uterus video
DESCRIPTION
These are the slides that accompany the video found on www.aboutcancer.comTRANSCRIPT

Cancer of the Uterus or Endometrium
Robert Miller MDwww.aboutcancer.com

Uterine cancer is the most common gyn malignancy with a 2.6 % lifetime risk
The average age is 61 years. The majority are diagnosed at an early stage (68 percent)

Anatomy

fundus
body
isthmus
cervix
vagina
Cervical canal
Endometrium
Myometrium
Internal Anatomy of the Uterus
Internalorifice

Cross section anatomy of the female pelvis

PET Scans may be more useful than CT scans in GYN cancers

1. Ovary, 2. Endometrial Cancer, 3. Uterus, 4. Urinary Bladder, 5.
Rectum, 6. Vagina
Endometrial cancer – adenocarcinoma of the lining of the uterus

Prognostic Factors in Endometrial Cancer
Stage (has it spread to the cervix, ovaries or lymph nodes)
Muscle Invasion (deep invasion in more serious)
Grade (higher grade is more serious) Histology (certain types like serous
cancer or sarcoma are more serious)

T and N Stage of Uterine Cancer
T1: confined to the uterus T1a : less than halfway into muscle T1b: deeper than halfT2: into cervix (stromal connective tissue)T3a: into serosa or adnexaT3b: into vagina or parametriumT4a: into bladder or rectum
N1: pelvic nodesN2: para-aortic nodes

Stages of Uterine Cancer
Stage I (T1N0) Stage II (T2N0) Stage IIIa (T3aN0) Stage IIIb (T3bN0) Stage IIIC1 (T1-3N1) Stage IIIC2 (T1-3N2) Stage Iva (T4) Stage IVb (M1)

Uterine cancer can spread to lymph nodes

PET Scan
Single area of metastases in right para-aortic lymph nodes
Biopsy confirmed recurrent cancer

Internal view (cross section) from PET

PET Scan = mets in para-aortic and pelvic nodes so stage IIIC endometrial cancer

Uterine cancer that has spread to para-aortic and pelvic nodes as seen on PET scan

5 Year Survival for Endometrial Cancer based on the Stage

5 Year Survival for Endometrial Cancer based on the histology of the cancer

Treatment of Endometrial Cancer
For most stages surgery (hysterectomy, TAH-BSO-PPLND) is performed and postOp radiation is indicated for high risk features:
•Deep muscle invasion (stage T1b)
•Involvement of cervix (stage T2)
•Spread to nodes, ovaries or tubes (Stage T3)
•High risk pathology: high grade, vascular invasion, serous or clear cell

•outer one-third myometrial invasion•grade 2 or 3 differentiation •lymphovascular invasion within the cancer.
Adverse prognostic factors are used to stratify women with intermediate-risk endometrial cancer:
High-intermediate risk – This is based on a combination of age and number of prognostic factors present:
•Patients of any age with all three factors•Patients 50 to 69 years old with two factors•Patients 70 years or older with only one factor



Guidelines for the use of radiation after a hysterectomy

Guidelines for the use of radiation after a hysterectomy

Dose Guidelines

CT scan is obtained at the time of simulation
CT images are then imported into the treatment planning computer

In the simulation process the CT and PET scan images are used to create a computer plan

In the treatment the lasers are used to line up the beam and the patient receives the radiation treatment

Radiation for advanced uterine cancer to treat pelvis plus para-aortic lymph nodes

Tomotherapy for Advanced Uterine Cancer

Computer reconstruction of radiation fields to cover groin and pelvic lymph nodes but avoid the bladder and rectum in vulva cancer patient

Combine a CT scan and linear accelerator to ultimate in targeting (IGRT) and ultimate in delivery (dynamic, helical IMRT) ability to daily adjust the beam (ART or adaptive radiotherapy)

Tomotherapy fields used to hit the groin and pelvic nodes but avoid the bladder and rectum

HDR = high dose rate machine that can run radiation through a tube that reaches the patient through vaginal applicators

Internal radiation devices
Procedure can be performed in hospital and the patient stays over night using a Cesium isotope applicator or the procedure can be done as an outpatient with a faster technique (called high dose rate or HDR) using an Iridium isotope source (Iridium 192 with half life of 74 days)

Vaginal cylinder is inserted into the vagina, the radiation tube or wire stays inside the tube and doesn’t touch the patient’s skin
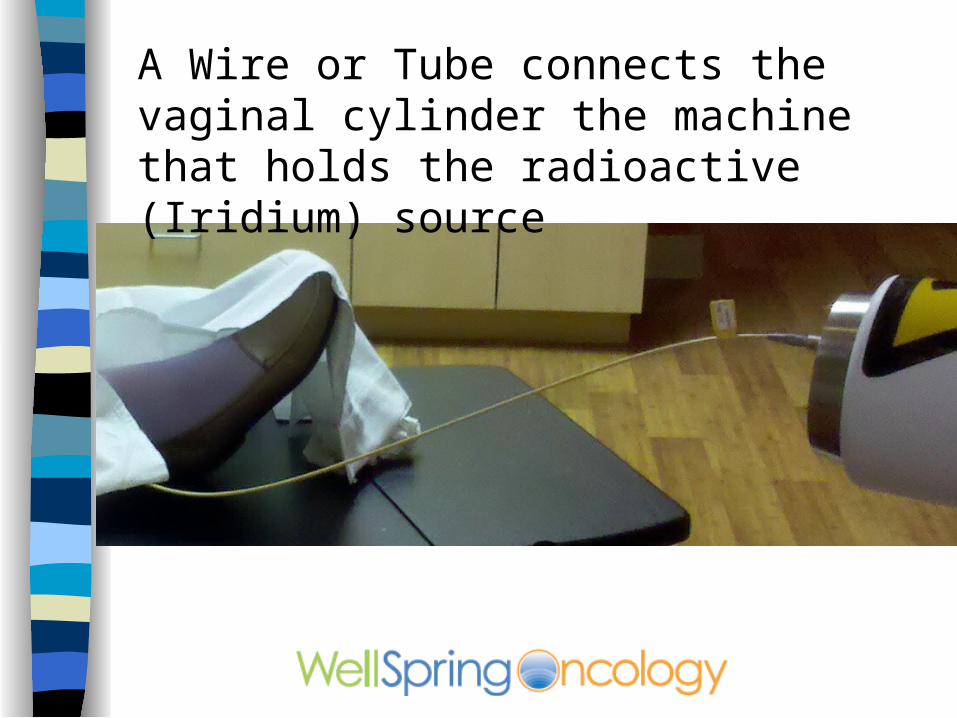
A Wire or Tube connects the vaginal cylinder the machine that holds the radioactive (Iridium) source

The woman lays on the radiation table and the treatment usually takes about 5 minutes and then the cylinder is removed

PostOp radiation for endometrial cancer is generally vaginal vault cylinder with HDR

Very little radiation reaches the bladder or rectum

Side Effects of Pelvic Radiation

Smallbowel

Rectum

Bone

Bladder

Vagina

Side Effects of Vaginal Cylinder HDR Radiation
•Vaginal irritation or discharge
•Bladder irritation or frequency
•Bowels more frequent, soft or mild rectal irritation

Cancer of the Uterus or Endometrium
Robert Miller MDwww.aboutcancer.com