utilizing the u.s. diabetes - c.ymcdn.comc.ymcdn.com/sites/ · from diabetes self-management...
TRANSCRIPT

Utilizing the U.S. Diabetes Conversation Map® Education Tools
with an Emphasis on Underserved Populations
AN IMPLEMENTATION
KIT
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm

This publication was developed and produced with funding from Merck and Company. Its contents are solely the
Photos on cover used with permission from Healthy Interactions, Inc.
March 2012

Torganization for chronic disease program directors of each state and U.S. territory. Founded in 1988, NACDD connects more than 3,000 members and chronic disease health professionals to advocate for preventive policies and programs, encourage knowledge sharing, and develop partnerships for health promotion. NACDD is a national leader in mobilizing efforts to reduce chronic diseases and their associated risk factors through state and community-based prevention strategies.
The NACDD Diabetes Council serves program managers and staff working in or with state and territorial Diabetes Prevention and Control Programs around the country, as well as partner organizations that support the work of the diabetes prevention and control programs.
National Association of Chronic Disease Directors2872 Woodcock Boulevard, Suite 220
Atlanta, GA 30341Phone: (770) 458-7400www.chronicdisease.org
Utilizing the U.S. Diabetes Conversation Map® Education Tools with an Emphasis on Underserved Populations
An Implementation Kit

Acknowledgments
The Diabetes Council of NACDD recognizes the following partners who participated in a pilot project, Evaluating Group Diabetes Education (EDGE), to utilize the U.S. Diabetes Conversation Map® education tools in underserved communities. Partners are listed by state/organization.
Merck and CompanyC. Victor Spain, DVM, PhDEpidemiologist, U.S Outcomes Research at Merck and Company.
National Association of Chronic Disease DirectorsTrish Herrmann, MS, RDDiabetes Consultant
Sue Ann Savas, MSWEDGE Program Evaluation ConsultantUniversity of Michigan
Denise Cyzman, MS, RDSenior Consultant for Diabetes and Chronic Kidney Disease
Earl W. SchurmanDiabetes Consultant
Marti Macchi, MEd, MPHSenior Consultant for Diabetes
Arizona EDGE ProjectSandra Leal, PharmD, CDEDirector of Clinical PharmacyEl Rio Community Health Center
Carmen RamirezCommunity Program CoordinatorDiabetes Prevention and Control Program Arizona Department of Health Services
Leticia Martinez, RD, MS, MPH, DC-ADMHealth EducatorEl Rio Community Health Center
Connecticut EDGE ProjectConnecticut Department of Public HealthChristian AndresenSection ChiefAIDS and Chronic DiseasesConnecticut Department of Public Health
Cindy Kozak, RD, MPH, CDEDiabetes Program ManagerConnecticut Department of Public Health
Valerie FisherDiabetes Program SupervisorConnecticut Department of Public Health

Advocate. Connect. Inspire
Stephanie M. Poulin, MPH, MT (ASCP)Epidemiologist Connecticut Department of Public Health
Julie Wagner, PhDAssociate ProfessorDivision of Behavioral Sciences and Community Health University of Connecticut Health Center
South Carolina EDGE ProjectSouth Carolina Department of Health and Environmental Control:
Michael D. Byrd, PhDDirector, Bureau of Community Health and Chronic Disease Prevention
Michelle Moody Community Partnership Coordinator
Rhonda Hill Division DirectorDiabetes Prevention and Control Program
Shelly-Ann BowenProgram EvaluatorDiabetes Prevention and Control Program
Melanie Robinson, RD, LD, CDERegistered Dietitian/Diabetes Educator
South Dakota EDGE ProjectSouth Dakota Department of Health:Linda Ahrendt, BA, M.EdAdministrator
Pamela Schochenmaier, RN, BSNDirector, Diabetes Prevention and Control Program
Zach ParsonsCoordinator, Diabetes Prevention and Control Program
A special thanks to Healthy Interactions and Barbara Eichorst, MS, RD, CDE for training partners on the Conversation Map tools.
In addition to the State Diabetes Prevention and Control Program reviewers, the following people reviewed this publication. Denise Cyzman, MS, RD; Nathan Morse, CHES, TTS-C (Maine Diabetes Prevention and Control Manager); Barbara Eichorst; Karen C. Barbone RN, CDE; and Melanie Robinson, RD, LD, CDE.

Table of Contents
Introduction
About the Evaluating Diabetes Group Education Program ................................................................................ 1
About the Diabetes Conversation Map Tools ................................................................................................. 2
About the Implementation Kit.................................................................................................................... 3
Guidelines for Implementation
Step 1: Planning and Pre-Implementation Assessment .............................................................................. 4
Step 2: Implementation of the Diabetes Conversation Map Tools ................................................................. 7
Step 3: Monitoring and Evaluating ............................................................................................................ 13
Role of Diabetes Prevention and Control Programs .............................................................................................. 14
Appendices
Appendix A: EDGE DPCP Project Partners .............................................................................................. 17
Appendix B: Resources for Organizations Beginning a Diabetes Self-Management
Education Program ........................................................................................................... 18
Appendix C: State DPCP Contact Information ........................................................................................ 19
Appendix D: Evaluation Detail to Apply for IRB Exemption ................................................................... 24
Appendix E: Participant Survey ................................................................................................................. 26
Appendix F: Participant Survey in Spanish ................................................................................................ 28
Appendix G: Diabetes Educator U.S. Diabetes Conversation Map Experience Survey ................................ 30
Appendix H: EDGE Focus Group Topics for Educators ........................................................................... 33
Appendix I: State Success Stories ............................................................................................................. 34
References ............................................................................................................................................................... 38

mm
1 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
The DPCP EDGE projects focused on serving people with diabetes who experience health disparities, with each state identifying priority populations, as follows:
Arizona: Hispanic/Latino, American Indian Connecticut: African American, Hispanic/Latino,
and low-income populations South Carolina: African American South Dakota: American Indian and rural popula-
tions
These four states conducted the demonstration project to assess and increase the use of the Diabetes Conversation Map tools within group diabetes self-management education. DPCPs partnered with DSME programs that implemented the Map tools and administered participant surveys after each session. Diabetes educator experiences using the Map tools were gathered using an educator survey. Interviews with DPCPs and partners were conducted following the demonstration project, contributing to a better understanding of the factors affecting use of Map tools. The lessons learned,
incorporated into the implementation steps outlined in this kit. While the EDGE project focused on health disparate populations, the implementation steps and much of what was learned can be applied to any DSME population.
About the Evaluating Diabetes Group Education Program
In 2010, the National Association of Chronic Disease Directors’ Diabetes Council received a two-year grant from Merck & Co., Inc. to launch the Evaluating Diabetes
Group Education (EDGE) Program. This program worked with four state Diabetes Prevention and Control Programs (DPCPs) and their partners on a demonstration project to implement and evaluate the U.S. Diabetes Conversation Map® education tools within American Diabetes Association-recognized and American Association of Diabetes Educators-accredited diabetes self-management education (DSME) programs. The four participating state DPCPs were Arizona, Connecticut, South Carolina, and South Dakota. For of list of state project partners, see Appendix A: EDGE DPCP Project Partners.
The EDGE Program had three primary goals: 1. To identify and enhance understanding of ways to
improve group diabetes self-management education programs using the Diabetes Conversation Map tools
2. To identify the role of state and territorial Diabetes Prevention and Control Programs (DPCPs) in foster-ing use of the Conversation Map tools to better serve those with diabetes-related health disparities
3. To explore the use of the Conversation Map tools for Spanish-speaking populations
Introduction

mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
2 mm
outcomes. Additional studies show that culturally and age-appropriate programs improve outcomes and that group education is effective.
Ongoing support is critical to sustain progress made by participants during the DSME program.
Behavioral goal setting is an effective strategy to sup-port self-management behaviors.
The U.S. Diabetes Conversation Map tools are available in English and Spanish. The Spanish language version is cultural relevant to Spanish speaking audiences. Merck also supported the development of a culturally-appropriate Conversation Map on healthy eating for Navajo participants. The Conversation Map tools and training are provided to health professionals at no cost. The Map tools meet the National Standards for Diabetes Self-Management Education2 and may be used as the curriculum to apply for ADA recognition or AADE accreditation. ADA recognition or AADE accreditation ensures that a program is comprehensive and meets the standards for DSME. It is also required in order to receive Medicare and other insurance reimbursement for provision of DSME services.
The training sessions for the Conversation Map tools are supported by Merck and Company; the Map tools are
non-branded.
About the Diabetes Conversation Map® Tools
The unique U.S. Diabetes Conversation Map® education tools were developed by Healthy Interactions, Inc. in collaboration with the American Diabetes Association
(ADA) with support provided by Merck and Company. The Conversation Map tools are used to educate people with diabetes and engage them in their own health with a series of face-to-face, dialogue-driven sessions guided by a trained diabetes educator. They help people with diabetes to relate what they learn in these sessions to their own experiences and to make plans to apply that learning in their everyday lives.
Healthy Interactions describes the Conversation Map tools as:
“…rooted in personalized, active engagement. Unlike traditional teaching methods, the Conversation Map methodology invites direct participation in the learning process. Participants focus on the information that relates to their own experiences. They then use face-to-face discussions to create the strategies and peer support needed to turn that information into meaningful behavior changes that can become lasting, positive habits.”1
The Map tool is a 3’ by 5’ visual with images that help generate discussion on diabetes education topics. The educator poses questions to start a discussion and discussion cards are used to further engage participants as they talk together about the topics. Five different Map tools are available. Four of these together can serve as a core diabetes
diabetes.
The Conversation Map tools support the National Standards for Diabetes Self-Management Education Guiding Principles established jointly by the American Association of Diabetes Educators (AADE) and the American Diabetes Association (ADA).2 Select principles include:
DSME has evolved from primarily didactic presen-tations to more theoretically based empowerment models.
There is no one “best” education program or ap-proach; however, programs incorporating behavioral and psychosocial strategies demonstrate improved

mm
3 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
Why Should I use the Conversation Map tools?The Conversation Map
The Map tools can enhance a current education pro-gram by adding a new method of learning through facilitated discussion and group activities.
The Map tools are available at no cost to licensed health professionals who participate in training on using the maps.
The Map tools are an approved curriculum for diabetes programs applying for ADA recognition or AADE accreditation.
The Conversation Map tools are a unique way for people with diabetes to learn more about diabetes and how to self-manage their disease. DSME programs that rely on lecture
from changing to the Map tools.
How do I begin to implement the Conversation Map Tools?Follow the steps in the “Guidelines for Implementation” section.
formal hospital-diabetes education programs; community based programs; Veterans Administration, Indian Health Service and other programs implementing a new diabetes education curriculum. The EDGE program worked with diabetes programs that are recognized or accredited by the American Diabetes Association or the American Association of Diabetes Educators. These programs were able to incorporate the Map tools effectively into their diabetes education programs.
About the Implementation Kit
What is the purpose of the implementation kit?This kit describes the experiences and lessons learned from diabetes self-management education programs that implemented the Conversation Map tools in their programs and outlines the best approach to use with underserved populations.
Who should use this implementation kit?This kit is designed for use in diabetes self-management education programs and diabetes programs in public health settings.
Diabetes self-management education programs in many settings—community based organizations, hospital systems, health clinics, or community health centers—provide direct diabetes education services. Examples of how these diabetes programs can implement the Conversation Map tools are discussed in the “Guidelines for Implementation” section. For organizations that currently do not have a diabetes self-management education program and wish to start one, resources are listed in Appendix B: Resources for Organizations Beginning a Diabetes Self-Management Education Program.
Diabetes programs in public health settings generally do not provide direct diabetes education services, but rather work with partners on public health core services.4 For example:
assuring that people with diabetes receive the rec-ommended care and treatment including diabetes education,
assessing the gaps in diabetes education programs, and
developing policies to improve access to diabetes education.
Examples of how public health programs can work with partners to implement the Map tools are discussed throughout the toolkit and in the “Role of Diabetes Prevention and Control Programs” section of this kit.
Where can the Conversation Map tools be implemented?The Conversation Map tools are intended for use by licensed health professionals and can be used in many settings:
The Conversation Map tools meet the requirements for a diabetes education program outlined by ADA and AADE. The tools can be used as a curriculum to apply for ADA
recognition or AADE accreditation.

mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
4 mm
4. Present the Map tools to the diabetes education advi-sory group for review.
5. Conduct focus groups with participants to gather feedback on the Map tools and the format for classes. Figure 2 highlights EDGE participant’s comments about the Map tools.
6. Pilot test one or two Map tools and use the feedback to identify any changes that may be needed.
7. Meet with diabetes educators who will be teaching classes and discuss concerns they may have about us-ing this new method.
Are you starting a diabetes self-management education program? If you need more information on establishing
and maintaining an effective diabetes program see Appendix B: Resources for Organizations Beginning a Diabetes
Self-Management Education Program.
Tools/Methods Meetings Focus groups and/or a pilot test Overview of U.S. Diabetes Conversation Map Tools Review Websites: www.healthyinterations.com and
www.journeyforcontrol.com
Step 1: Planning and Pre-Implementation Assessment
Gaining support for implementing a new curriculum is important for its success. You will want to ensure that your diabetes education advisory committee and the
diabetes educators are supportive and open to trying a new approach. You will also want to gather feedback from past or potential participants in self-management education. This will be especially important if your current curriculum is lecture format and is less interactive than the Map approach. An assessment will help you:
Identify potential hurdles Create awareness about the new curriculum Adapt the new curriculum for special populations, if
needed
Objective: To gain support for implementing a new curriculum Primary Activity: Gathering information to help implement the new curriculum Process: Facilitate meetings with those affected by potential change in curriculum; conduct interviews and or focus groups with diabetes educators and past/potential participants.
Process for Planning and Pre-Implementation Assessment:
1. Review information about the Conversation Map tools which can be found on the Journey for Control web-site (www.journeyforcontrol.com). The basic content of each map can be found in Figure 1: Content of Conversation Map Tools showing how the content re-lates to the 7 diabetes self-care behaviors outlined by the American Association of Diabetes Educators3.
2. Contact your state Diabetes Prevention and Control Program (see Appendix C: State DPCP Contact Informa-tion). The state DPCP may be able to help you reach out to other partners in the state who are currently using the Map tools since experienced partners can be a valuable resource for your team.
3. Have at least one educator get training on use of the Map tools.
Guidelines for Implementation

mm
5 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
Figure 1: Content of Conversation Map Tools
Name of Conversation Map Tool
Conversation Map Tool Content Diabetes Self-care Behaviors**
On the Road to Better Managing Your Diabetes*
Understanding what diabetes is and how it works Dealing with feelings about diabetes Checking your blood glucose levels Healthy eating Keeping active Diabetes medicines Your support network
All 7 Self-care behaviors
Diabetes and Healthy Eating*
The relationship between diabetes and food Feelings about food and healthy eating How what you eat, how much you eat and when you
eat can affect your blood glucose Meal planning and other strategies for healthy eating
Healthy eating
Monitoring Your Blood Glucose*
What blood glucose and insulin are Blood glucose targets and reactions to out of range
levels What can cause blood glucose to go up and down
and preventing high and low blood glucose Using your monitoring results to mange your
diabetes
Monitoring Healthy coping
Continuing Your Journey with Diabetes*
The natural course of diabetes The potential long-term complications of diabetes How to delay or reduce the risk of long-term
complications of diabetes Knowing your ABC’s
Taking medication Problem solving Reducing Risks
Caring for Gestational Diabetes
What gestational diabetes is Feeling about being diagnosed with gestational
diabetes and tying to manage it Caring for gestational diabetes What to expect after pregnancy and the risk of
getting type 2 diabetes
All 7 Self-care behaviors
* Together, the four starred Map tools serve as a core curriculum.**The AADE7TM self-care behaviors are healthy eating, being active, monitoring, healthy coping, taking medication, problem solving, and reducing risks.3

mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
6 mm
Figure 2: EDGE Participants on Why U.S. Diabetes Conversation Map ToolsWork Best for Them
Theme Illustrative Comments
“I can see what I need to know and go by the Map.” “Because the Map shows and the teacher explains. I feel as if I
learn more from someone teaching us.” “Hands-on” “Being able to visualize everything is always helpful.”
“You can ask questions. Because there are others in class, it brings up more relevant issues.”
“Greater participation” “Because the group is small and they could cover more questions.” “Conversations with other people with diabetes.” “Encourage conversation. Encourage interaction.” “Because we sat around and talked about our experience” “Because we participate more we ask questions about all of our
doubts that we have.”
“Because it explains and helps me categorize food consumed on a daily basis that wasn’t good for me. It indicated how to better metabolism and eat adequately.”
“Because there is better information.” “They explain all of your doubts. It helps me to take my meds.” “ It helps me understand what to expect- all the facts and myths.” “Expanded on the one-on-one education. Gave me a better under
standing about eating healthy.” “Gives examples and people put in what they eat daily”
The Map tool is a helpful visual
Interaction with group members
Informative

mm
7 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
2. Schedule the educator training considering these op-tions : a. Find out if there is a Conversation Map training
session in your area by going to the Journey for Control website, www.journeyforcontrol.com. On the Educator page, choose the Conversation Map Program (top menu) and then Conversation Map Training (left menu).
b. If no training is available, contact your local Merck Sales Representative to schedule an edu-cator training in your area. At least 10 licensed health professionals are needed to schedule a Conversation Map training session. You may need to contact other health systems, clinics or your state Diabetes Prevention and Control Program in or-der to identify others who would like to be trained (see Appendix C: State DPCP Contact Information).
c. Online training is also available for the Conversa-tion Map tools — contact your Merck Sales Rep-resentative for an invitation to be trained via this method.
Process for Implementing Conversation Map tools:
1. Decide who should be trained. Only licensed health professionals will receive a set of the Conversation Map
for community health outreach workers to attend a training to learn about the new curriculum and to garner their support and engagement.
Step 2: Implementation of the Diabetes Conversation Map Tools
Diabetes educators are very knowledgeable about diabetes and are trained to help people with diabetes make changes to improve their health. Some
diabetes educators are less knowledgeable about teaching methods and may have reservations about using a new format where participants are invited to discuss a wide range of issues. To successfully implement the Conversation Map tools diabetes educators must be skilled in facilitation techniques to ensure the conversation moves forward. Staff training on how to use the Map tools is a key component of implementation.
Another key component of successful implementation is making sure the Map tools are appropriate for the audience by adapting them, if necessary. Cultural considerations are especially important to address.
Objective: To implement the Conversation Map tools in a culturally appropriate wayPrimary Activities: Strengthen capacity of diabetes educators to teach in new format through assessment and training; ensure materials are culturally appropriate for the audience Process: Access trainings for educators and assess educator’s
Conversation Map tools in a group education format.
“I am a much better facilitator than a lecturer. I also feel that clients get more out of having conversations with others with
diabetes than to be lectured to.”
Diabetes Educator, EDGE Program
local Merck Sales Representative at 1-800-672-6372.
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
8 mm
South Carolina EDGE partners scheduled a brown bag lunch with educators to review successes, barriers, and lessons learned from conducting Conversation Map sessions and the development of an Action Plan for program implementation changes
South Carolina EDGE partners adapted the Map tools by:
Adding a new square to represent places of worship on the Diabetes and Healthy Eating Conversation Map tool in the “Challenges You Might Face” section.
Adding an additional hot air balloon graphic to the Monitoring Your Blood Glucose Map tool to represent the ABC’s of Diabetes.
Creating new cards to address local cultural is-sues, such as these added to “Myths and Facts” in the On the Road to Better Managing Your Diabetes Map:
Toasting bread gets rid of some starch in bread.
Drinking lots of water can wash away the extra sugar in my blood.
Putting Spanish Moss in your shoes helps bring your blood pressure down.
Daily does of vinegar helps lower blood sugar levels.
Washing rice before cooking gets rid of the starch.
And these added to “Oral Diabetes Agents” in the Continuing Your Journey with Diabetes Map:
Pronunciation instructions along with examples of each medication.
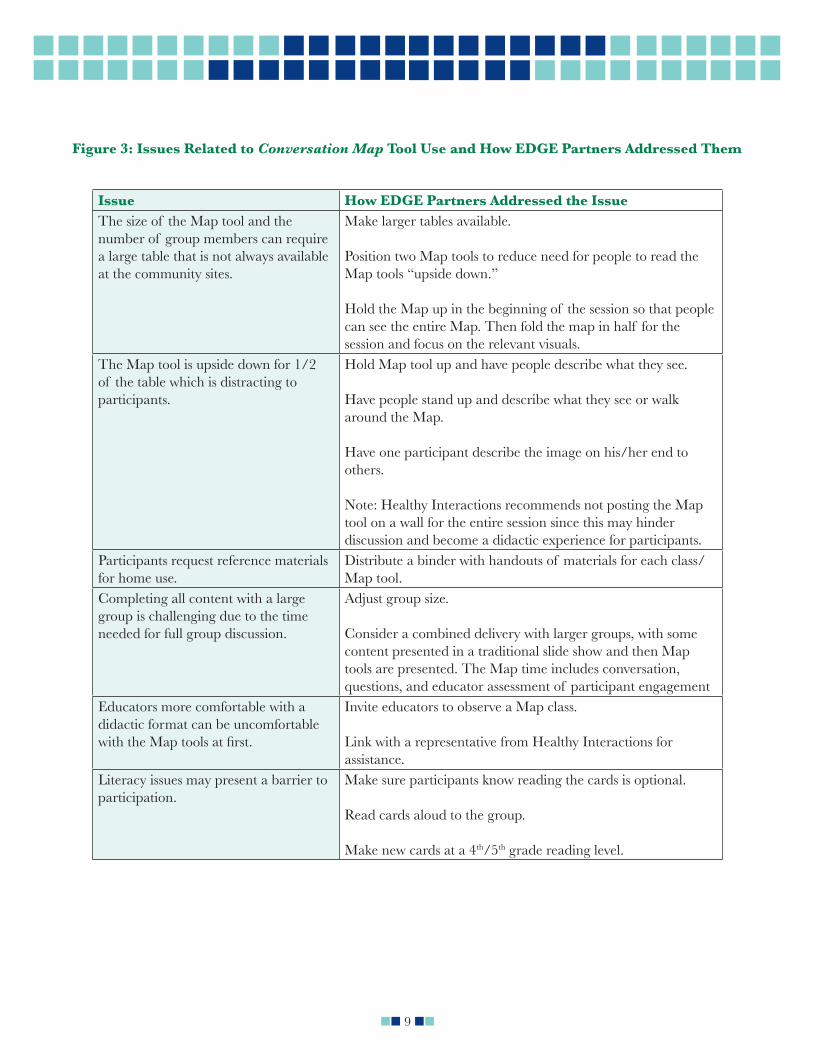
Lessons learned from EDGE partners using Map tools can be found in Figure 3: Issues Related to Conversation Map Tool Use and How EDGE Partners Addressed Them.
3. Adapt the Conversation Map tools and prepare to use Map tools. The core curriculum includes these four Map tools:
On the Road to Better Managing Your Diabetes
Diabetes and Healthy Eating Monitoring Your Blood Glucose Continuing Your Journey with Diabetes
language skills. For example, in South Carolina, images of a church and places of worship were
religious beliefs of the population served. Additional
to discussion cards or placed on the Map during the discussion. Viewing these visuals may spark additional discussion by participants on culturally
To ensure that the curriculum is responsive to local needs, the project team should:
Augment or adapt the curriculum using local information, if appropriate. New cards for the activities can be produced to suit your com-munity. Blank templates for some of the card topics are available online from Healthy Inter-
the templates, login as a facilitator and then choose “conversation card template” under U.S. Diabetes Resources.
Use the results from your local assessment in Step 1 to identify areas where cultural consider-ations or language issues need to be addressed.
“I think that the diabetes conversation map format is excellent for participants. They have the opportunity to learn from each other while being guided and provided with accurate information. I also like the way that all materials are provided and the content is scripted. This allows for minimal planning while still providing
excellent diabetes instruction.”
Diabetes Educator, EDGE Program
mm
9 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
Issue How EDGE Partners Addressed the IssueThe size of the Map tool and the number of group members can require a large table that is not always available at the community sites.
Make larger tables available.
Position two Map tools to reduce need for people to read the Map tools “upside down.”
Hold the Map up in the beginning of the session so that people can see the entire Map. Then fold the map in half for the session and focus on the relevant visuals.
The Map tool is upside down for 1/2 of the table which is distracting to participants.
Hold Map tool up and have people describe what they see.
Have people stand up and describe what they see or walk around the Map.
Have one participant describe the image on his/her end to others.
Note: Healthy Interactions recommends not posting the Map tool on a wall for the entire session since this may hinder discussion and become a didactic experience for participants.
Participants request reference materials for home use.
Distribute a binder with handouts of materials for each class/Map tool.
Completing all content with a large group is challenging due to the time needed for full group discussion.
Adjust group size.
Consider a combined delivery with larger groups, with some content presented in a traditional slide show and then Map tools are presented. The Map time includes conversation, questions, and educator assessment of participant engagement
Educators more comfortable with a didactic format can be uncomfortable
Invite educators to observe a Map class.
Link with a representative from Healthy Interactions for assistance.
Literacy issues may present a barrier to participation.
Make sure participants know reading the cards is optional.
Read cards aloud to the group.
Make new cards at a 4th/5th grade reading level.
Figure 3: Issues Related to Conversation Map Tool Use and How EDGE Partners Addressed Them

mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
10 mm
5. Begin using the Conversation Map curriculum in diabetes education classes. Several EDGE partners
allowing them to become comfortable with the new
to effectively facilitate the discussion. One partner assigned two educators per class, allowing one educa-tor to review and provide feedback on blood glucose and food logs while the other educator facilitated the class discussion. Healthy Interactions provides ongo-ing support to educators to increase their skills and
and participation is highly encouraged. Information about webinars can be found on the Healthy Interac-tions website (www.healthyinteractions.com) after logging in as a facilitator. Once logged in, educators
learner-centered approach to diabetes education.
4. Develop a class schedule. Each Conversation Map tool is intended for use in one 2-hour class session for a total of four classes. In rural communities where travelling distances can make attending four classes challenging,
combined. EDGE partners integrated the Conversation Map tools into their Diabetes Self-Management Edu-cation programs in various but similar ways.
Four program formats are presented in Figure 4: Examples of Class Formats/Schedules to illustrate how the Conversation Map sessions were implemented. All programs had participants meet for a 1-hour individual initial visit with the diabetes educator to assess their need for group education and review their current skills and knowledge about diabetes. One program also included a 30-minute individual partici-pant visit with a registered dietitian.
Suggestions for Implementing the Conversation Map tools from EDGE Partner Educators:
Practice asking open-ended questions. “Hold your tongue, wait for participants to answer.” “Need to plunge into it, instead of feeling totally
ready.” Have two educators facilitate a class to ease the fears
of staff. Let participants know that no one is obligated to say
or read anything. -
selves and answer a mini icebreaker question: For
diagnosed with diabetes?” Reinforce meal planning by counting carbohydrates
together using a participant’s breakfast, lunch, or din-ner meal as an example.
Tools/Methods Conversation Map tools Training Healthy Interactions (www.healthyinteractions.com)
and Journey for Control (www.journeyforcontrol.com) Web sites
Partners in Connecticut had not previously taught classes in
and/or Spanish speaking health professional who can be trained to use the Conversation Map tools.
Recruitment and Retention Strategies for Spanish Speaking Populations
Two partners implemented the Conversation Map tools for Spanish speakers. In Arizona most of the classes were taught in Spanish and in Connecticut a few of the classes were
partners shared strategies for recruitment outlined in Figure 5: Recruitment and Retention Strategies.
“The conversation maps offer the participants a chance to share their own thoughts, feelings and information about diabetes. This allows participants to learn from each other while the facilitator guides the conversation and validates or corrects information brought to the session by the participants.”
Diabetes Educator, EDGE Program

mm
11 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
Class Format/Schedule Description
3 Map Sessions (2 hours each)In Connecticut, one partner, used one Map tool at each of three sessions. These Map tools were On the Road to Better Managing Your Diabetes, Diabetes and Healthy Eating, and Continuing Your Journey with Diabetes. Occasionally, the Monitoring Your Blood Glucose tool was presented together with Continuing Your Journey with Diabetes tool.
3 Map Sessions (3 hours each)One South Dakota EDGE Project partner conducted three, 3-hour group classes using the following Map tools: On the Road to Better Managing Your Diabetes, Continuing Your Journey with Diabetes, and Monitoring Your Blood Glucose.
4 Map Sessions (2 hours each)Another Connecticut partner conducted four, 2-hour sessions using all four, core curriculum Map tools. They spent 15 minutes per class analyzing one participant’s meal to teach carbohydrate counting and ways to make
4 Group Sessions using 2 Map tools (2 hours each)
Another South Dakota EDGE partner presented one of two Map tools (On the Road to Better Managing Your Diabetes and the Continuing Your Journey with Diabetes) at Session 1 and Session 3 of their four sessions. The Diabetes Educator covered other material needed by participants at Sessions 2 and 4..
Figure 4: Examples of Class Formats/Schedules

mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
12 mm
Strategy DescriptionLet participants spread the word Participants brought friends, neighbors, and family
members with diabetes to classes as additional participants.
Educate providers Invite providers to observe classes.
to Map classes with providers.
Encourage participants to bring materials back to class
This allows participants to ask any questions they saved from the previous class. One partner felt this was “a useful strategy to ensure participants return to class.”
Use promotores or community health outreach workers
Promotores and other community health outreach workers can be very effective at recruiting and retaining participants.
Leverage participant satisfaction Positive feedback from participants is a great way to recruit new participants. As one EDGE project leader says, “Fortunately our patients have been a great source of advertising for us…”
Train health professionals in training (for example, students, interns, residents)
In Arizona, all pharmacy residents at the community health center were required to attend class and become trained to use the Map tools to increase their familiarity with tools and their comfort level in teaching using this format.
Adapt class schedules to participant needs Moving from weekday afternoons to weekend or evening classes increased participation for participants who work during the day.
Partner with a community health center Two hospital-based DSME programs partnered with nearby community health centers to offer Spanish language classes. One center trained a Spanish speaking LPN to use Map tools; another had their marketing
Provide in-service training for primary care staff
Educators provided an in-service to medical assistants
to increase their knowledge and awareness of program
Figure 5: Recruitment and Retention Strategies

mm
13 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
compared to previous curriculum, it may indicate sat-isfaction with curriculum.
2. Participant satisfaction - The participant sur-vey was administered following every class where a Conversation Map tool was used. If it is cumbersome for participants to complete a survey after each class, consider conducting one per quarter so that informa-
Appen-dix E: Participant Survey and Appendix F: Participant Survey in Spanish for sample surveys.
3. Educator Experience using Conversation Map tools - A Diabetes Educator survey was used to as-sess the educator’s use of the Map tools. The paper-pencil survey was administered quarterly throughout the project for the purpose of gathering information about educator’s methods and strategies in using the Map tools. See Appendix G: Diabetes Educator U.S. Diabe-tes Conversation Map Experience Survey.
4. Focus group with educators - The focus group allowed educators to describe barriers and facilitat-ing factors to using Map tools and any changes that needed to be made to improve/enhance the imple-mentation. See Appendix H: EDGE Focus Group Topics for Educators for topic examples.
Tools/Methods: Participant Surveys—Appendix E (English version)
and F (Spanish version) Educator Surveys—Appendix G EDGE Focus Group Topics for Educator—Appen-
dix H
Step 3: Monitoring and Evaluating
Evaluation should measure the effect of implementing the Conversation Map tools and the capacity of the educators to use the Map tools. Establish the
evaluation methods and plan before implementation begins and continually assess for appropriateness. When improvements based on evaluation are implemented, monitor the results of changes made.
The EDGE program evaluation focused on process measures. EDGE partners also collect outcome measures to meet the requirements for ADA recognition or AADE accreditation; these were not collected for the EDGE project evaluation.
Your agency may require IRB human subject protection approval before you administer surveys to participants. Appendix D: Evaluation Detail to Apply for IRB Exemption contains examples of IRB applications appropriate for a university or hospital–based review committee. All EDGE partners were required to receive an IRB research approval or secure a waiver as an evaluation study.
Objective: To gather information to improve, enhance, and sustain the Conversation Map tools curriculumPrimary Activities: Assessing diabetes educators’ satisfaction and capacity to use Map tools; assessing patient satisfaction with the Map tools; integrating evaluation results into program improvement planningProcess: Choose from a variety of quantitative and qualitative methods to assess the implementation, including: Tracking participation rate and number of participants who complete class series; participant surveys; educator surveys; focus groups with educators.
The key elements of the process evaluation with suggestions for Conversation Map tools to use are:
1. Class attendance - Class attendance is a proxy measure of satisfaction. If attendance rates increase
“Before [using Conversation Map tools] everyone . . . . was ready to go at the end of class; with the Maps we can’t get people to leave. Maps are more personalized.”
Diabetes Educator, EDGE Program

mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
14 mm
Role of Diabetes Prevention and Control Programs
Training Promotion of Map tools trainings to partners Linking health professionals with Conversation Map
tools resources Hosting or co-hosting trainings of licensed health
professionals on Map tools
Implementation Providing resources to address barriers to implemen-
tation Linking educators new to using the tools with experi-
enced educators Sharing methods programs can use to incorporate
Map tools into their curriculum Describing the way DSME programs adapted Map
Hosting conference calls for educators using the Map tools or interested in using the Map tools and facili-tating their experience-sharing
Developing Sustainable Models for DSME Disseminating the locations of current DSME pro-
for DSME Working with communities having a high incidence
or maintain a DSME program Providing assistance to new communities or new pro-
grams on starting a community-based DSME class by introducing the Conversation Map tools as a potential no cost curriculum
Sharing model DSME programs with other partners in the state
Using a Public Health Framework The U.S. Diabetes Conversation Map tools provide State Diabetes Prevention and Controls Programs and their partners with resources aimed at multiple levels of the socio-ecological model6 including community (for example, health
State and territorial Diabetes Prevention and Control Programs are funded by the Centers for Disease Control and Prevention and are public health programs
that work with partners—public, private and voluntary groups and community-based organizations —to positively impact diabetes health outcomes. DPCPs work primarily through their relationships with partners who work directly
coordinate the activities of partners, and serve as technical advisors for these activities. DPCP work aligns with the 10 Essential Public Health Services4, which include
monitoring the numbers of people with and at risk for diabetes,
informing, educating, and empowering people about diabetes prevention and control,
mobilizing community partners to action to identify and solve problems, and
linking people to needed personal health services and assume the provision of health care.
To contact your state DPCP, refer to Appendix C: State DPCP Contact Information.
The state DPCP staff served in many roles for this project, including:
Promotion of the Conversation Map Tools Sharing information about Conversation Map tools at
State Diabetes Coalition meetings Sending information about the Map tools in newslet-
ters to partners Outreach to priority populations to facilitate their
participation in DSME programs using the Map tools Introducing healthcare providers and community
partners to the DSME programs using Map tools Ongoing promotion and communication with health
care providers and community partners to encourage referrals to the DSME programs using the Map tools

mm
15 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
professional user groups), organizational (for example, AADE accreditation), and interpersonal and individual (for example, diabetes self-management education for people with diabetes and their families).
Example of State Roles in Applying the Conversation Map ToolsSuccess stories for the EDGE program are in included in Appendix I: State Success Stories. A few additional examples from the pilot follow:
Convening Educators in the State to Discuss Conversation Map Tools—South Dakota
The South Dakota DPCP convened educators from around the state and invited them to participate in conference calls to discuss the use of the Map tools. The educators expressed appreciation about learn-ing from others in the State who use the tools. As the State Coordinator noted, “The positive attitude of educators at one site about the EDGE program (tools) helps others to be more positive.” Educators also shared resources with one another; for example, one site sent a written script they used when asking participants to complete the participant survey.
State DPCPs can work with partners to identify areas in their state where DSME programs are needed. Mapping current
programs with an overlap showing diabetes prevalence is one way to assist communities in identifying areas of need.
Expanding Sustainable Diabetes Education Programs in States—Arizona
Diabetes self-management education is a standard of care for people with diabetes and yet there are many people with diabetes who do not receive educa-tion5. Some state DPCPs are working with partners to increase access to this important service. Assessing the gaps to education and developing sustainable programs and models of care is an appropriate role for DPCPs. The Conversation Map tools can be part of plans to increase access to services. For example, the
Center in Tucson, was able to receive AADE accred-itation for the provision of DSME services, increasing the likelihood they will be able to bill for services for certain participants and will increase revenue for this program focused on a highly-underserved popula-tion. This model program will be shared with other community health centers in Arizona coordinated by the state’s DPCP.

mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
16 mm
AppendicesAppendix A: EDGE DPCP Project PartnersAppendix B: Resources for Organizations Beginning a Diabetes Self-Management Education ProgramAppendix C: State DPCP Contact InformationAppendix D: Evaluation Detail to Apply for IRB ExemptionAppendix E: Participant SurveyAppendix F: Participant Survey in SpanishAppendix G: Diabetes Educator U.S. Diabetes Conversation Map® Experience SurveyAppendix H: EDGE Focus Group Topics for Educators Appendix I: State Success Stories

mm
17 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
DPCP DSME Partners
Arizona Conversation Map Intervention Site and Non-Map site: El Rio Health Center
Other Partner: Pascua Yaqui Tribe
Connecticut Conversation Map Intervention Sites: Norwalk Hospital Diabetes Education Center Windham Hospital Diabetes Education Program
Non-Map sites: Backus Hospital Diabetes Education Program Hospital of Central CT Joslin Diabetes Education Center
Other Partner: Julie Wagner, PhD (evaluator), University of Connecticut
South Carolina
Conversation Map Intervention Sites: Diabetes Educators Syndia Moultrie, MS, RD, LD and Montrese Edwards, BSN, RN,
CDE with REACH SEA:CEED Charleston Diabetes Coalition in partnership with St. James-Santee Family Center East Cooper Community Outreach Mt. Moriah Baptist Church Four Franklin C Fetter Community Health Center Sites SC DHEC Region 7 Diabetes Educators, Karen Warren, RN, MS and Melanie Robin-
son, RD, LD, CDE in partnership with Internal Medicine Associates Harvest Free Medical Clinic
Non-Map site: SC DHEC Region 8 Diabetes Educator, Sarah P. Smith, MAT, RD, LD, CDE in part-
nership with Health Care Partners
South Dakota Conversation Map Intervention Sites: Sanford Health in Sioux Falls, SD Avera McKennan in Sioux Falls, SD Avera Sacred Heart Hospital in Yankton, SD Rapid City Regional in Rapid City, SD
Non-Map site: Madison Community Hospital in Madison
Appendix A: EDGE DPCP Program PartnersJanuary 1, 2010-December 31, 2011

mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
18 mm
Appendix B: Resources for Organizations Beginning a Diabetes Self-Management Education Program
Partnership for Prevention. Diabetes Self-Management Education (DSME): Establishing a Community-Based DSME Program for Adults with Type 2 Diabetes to Improve Glycemic Control—An Action Guide. The Community Health Promotion Handbook: Action Guides to Improve Community Health. Washington, DC: Partnership for Prevention; 2008.
National Standards for Diabetes Self-Management Education. The standards are published jointly by the American Association of Diabetes Educators and the American Diabetes Association and can be found in The Diabetes Educator and Diabetes Care. These organizations recognize or accredit Diabetes Self-Management Education Programs. Information about this process can be found on their websites.
American Association of Diabetes Educators Diabetes Education Accreditation Program American Diabetes Association Education Recognition Programs

mm
19 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
Connecticut Department of Public Health Diabetes Prevention and Control Program 410 Capitol Avenue Hartford, Connecticut 06134-0308 Program phone number: (860) 509-7737 Program fax number: (860) 509-7855
Delaware Diabetes Prevention and Control Program Thomas Collins Building, Suite 10 540 S. DuPont Highway Dover, Delaware 19901 Program phone number: (302) 744-1020 Program fax number: (302) 739-2544
District of Columbia Diabetes Prevention and Control Program 825 N. Capitol St. NE 3rd Floor Washington, DC 20002 Program phone number: (202) 671-5000 Program fax number: (202) 442-4825
Florida Diabetes Prevention and Control Program Bureau of Chronic Disease Prevention and Health Promotion Department of Health 4052 Bald Cypress Way Bin # A-18 Tallahassee, Florida 32399-1744 Program phone number: (850) 245-4330 Program fax number: (850) 245-4391 E-mail address:
Georgia Diabetes Prevention and Control Program Georgia Department of Community Health Division of Public Health 2 Peachtree Street, Suite 16-262 Atlanta, Georgia 30303 Program phone number: (404) 657-6313 Program fax number: (404) 657-4338
Alabama Diabetes Prevention and Control Program State of Alabama Department of Public Health RSA Tower 201 Monroe Street, Suite 976 Montgomery, Alabama 36104 Program phone number: (334) 206-5300 Program fax number: (334) 206-5609
Alaska Diabetes Prevention and Control Program 3601 ‘C’ St., Suite 722 Anchorage, Alaska 99503 Program phone number: (907) 269-8035 Program fax number: (907) 269-5446
Arizona Diabetes Control & Prevention Coordinator Arizona Department of Health Services 150 North 18th Avenue, Suite 310 Phoenix, Arizona 85007 Program phone number: (602) 542-8261 Program fax number: (602) 542-0512
Arkansas Department of Health 4815 W. Markham, Slot #6 Little Rock, Arkansas 72205 Program phone number: (501) 661-2627 Program fax number: (501) 661-2070
California Department of Public Health Diabetes Prevention and Control Program, MS 7211 1616 Capitol Avenue, Suite 74.420 Sacramento, California 95814Mailing Address California Department of Public Health Diabetes Prevention and Control Program, MS 7211 P.O. Box 997377 Sacramento, California 95899-7377 Program phone number: (916) 552-9942 Program fax number: (916) 552-9988
Colorado Diabetes Prevention and Control Program Colorado Department of Public Health and Environment 4300 Cherry Creek Drive South #A-5 Denver, Colorado 80246 Program phone number: (303) 692-2577 Program fax number: (303) 691-7900
Appendix C: State DPCP Contact Information
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
20 mm
Kentucky Diabetes Prevention and Control Program Chronic Disease Prevention Branch 275 East Main Street, HS2W-E Frankfort, Kentucky 40621-0001 Program phone number: (502) 564-7996 Program fax number: (502) 564-4667
Louisiana Diabetes Program 628 North 4th Street, 2nd Floor Bienville Building Baton Rouge, Louisiana 70802Mailing Address 628 North 4th Street, P.O. Box 3118 Baton Rouge, Louisiana 79821-3118 Program phone number: (225) 342-2663 Program fax number: (225) 342-2652
Maine Diabetes Prevention and Control Program Division of Chronic Disease
11 State House Station Augusta, Maine 04333-0011 Program phone number: (207) 287-5380 Program fax number: (207) 287-7213
Maryland Diabetes Prevention and Control Maryland Department of Health and Mental Hygiene201 W. Preston Street, 3rd Floor Baltimore, Maryland 21201 Program phone number: (410) 767-3608 Program fax number: (410) 333-5030
Massachusetts Diabetes Prevention and Control Program (Search “diabetes”) Massachusetts Department of Public Health 250 Washington Street, 4th Floor Boston, Massachusetts 02108 Program phone number: (617) 624-5429 Program fax number: (617) 624-5075
Michigan Diabetes Prevention and Control Program Michigan Department of Community Health Washington Square Building, 7th Floor 109 W. Michigan Avenue Lansing, Michigan 48913 Program phone number: (517) 335-9892 Program fax number: (517) 335-9461
Hawaii State Department of Health Diabetes Prevention and Control Program 601 Kamokila Blvd, Room 344 Kapolei, Hawaii 96707 Program phone number: (808) 692-7462 Program Fax number: (808) 692-7461 Program email address (Hawaii Diabetes Prevention & Control Program) E-mail: [email protected]
Idaho Diabetes Control and Prevention Program Bureau of Community and Environmental Health Department of Health and Welfare 450 West State Street P.O. Box 83720 Boise, Idaho 83720-0036 Program phone number: (208) 334-4928 Program fax number: (208) 334-6573
Illinois Department of Public Health
Diabetes Prevention and Control Program 535 West Jefferson Street
Program phone number: (217) 557-3283 Program fax number: (217) 782-1235
Indiana Diabetes Prevention and Control Program Indiana State Department of Health 2 North Meridian Street, 6B Indianapolis, Indiana 46204 Program phone number: (317) 233-7755 Program fax number: (317) 233-7805
Iowa Diabetes Prevention and Control Program Iowa Department of Public Health 321 East 12th Street – Lucas Building Des Moines, Iowa 50319-0075 Program phone number: (515) 242-6204 Program fax number: (515) 281-6475
Kansas Diabetes Prevention and Control Program
Kansas Department of Health and Environment 1000 SW Jackson, Suite 230 Topeka, Kansas 66612 Program phone number: (785) 291-3739 Program fax number: (785) 296-8059

mm
21 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
New Hampshire Diabetes Education Program Division of Public Health Services NH Department of Health and Human Services 29 Hazen Drive Concord, New Hampshire 03301 Program phone number: (603) 271-5173 Program fax number: (603) 271-5199
New Jersey Department of Health & Senior Services Wellness and Chronic Disease Prevention Program 50 East State Street, PO Box 364 Trenton, New Jersey 08625 Program phone number: (609) 984-6137 Program fax number: (609) 292-9288
New Mexico Diabetes Prevention and Control Program New Mexico Department of Health 810 West San Mateo Road, Suite 200E Santa Fe, New Mexico 87505 Program phone number: (505) 476-7615 Toll-free telephone 1-888-523-2966 Program fax number: (505) 476-7622
New York State Department of Health Bureau of Chronic Disease Services Diabetes Prevention and Control Program 150 Broadway – Room 350 Albany, New York 12204-0678 Program phone number: (518) 474-1222 Program fax number: (518) 473-0642
North Carolina Diabetes Prevention and Control Program 5505 Six Forks Road (3rd Raleigh, North Carolina, 27609 Program phone number: (919) 707-5340 Program fax number: (919) 870-4801
North Dakota Diabetes and Prevention Program North Dakota Department of Health 600 E. Boulevard Avenue, Department 301 Bismarck, North Dakota 58505-0200 Program phone number: (701) 328-2367 Program fax number: (701) 328-2036
Minnesota Diabetes Program Minnesota Department of Health P.O. Box 64882 St. Paul, Minnesota 55164-0882 Program phone number: (651) 201-5423 Program fax number: (651) 201-5800
Mississippi Diabetes Prevention and Control Program 570 East Woodrow Wilson Drive Osborne Building, Suite 200 Jackson, Mississippi 39215-1700 Program phone number: (601) 576-7781 Program fax number: (601) 576-7444
Missouri Diabetes Prevention and Control Program Bureau of Cancer and Chronic Disease Control Section for Chronic Disease Prevention and Nutrition Services Missouri Department of Health and Senior Services 930 Wildwood, PO Box 570 Jefferson City, Missouri 65102 Program phone number: (573) 522-2861 Program fax number: (573) 522-2898 E-mail: [email protected]
Montana Diabetes Project 1400 Broadway, Room C314B PO Box 202951 Helena, Montana 59620-2951 Program phone number: (406) 444-6677 Program fax number: (406) 444-7465
Nebraska Diabetes Prevention and Control Program Nebraska Department of Health and Human Services 301 Centennial Mall South P.O. Box 95026 Lincoln, Nebraska 68509-5026 Program phone number: (1-800) 745-9311 Program fax number: (402) 471-6446
Nevada Diabetes Prevention and Control Program Nevada State Health Division 4150 Technology Way, Suite 101 Carson City, Nevada 89706 Program phone number: (775) 684-5996 Program fax number: (775) 684-5998

mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
22 mm
Columbia, South Carolina 29204 Program phone number: (803) 545-4471 Program fax number: (803) 545-4921
South Dakota Diabetes Prevention & Control Program South Dakota Department of Health 615 E Fourth Street Pierre, South Dakota 57501 Program phone number: (605) 773-7046 / toll-free number-1-800-738-2301 Program fax number: (605) 773-5509
Tennessee Diabetes Prevention and Control Program Tennessee Department of Health, Nutrition and Wellness 425 5th Avenue North Cordell Hull Building, 5th Nashville, Tennessee 37243 Program phone number: (615) 741-5379 Program fax number: (615) 532-8478
Texas Diabetes Prevention and Control Program Texas Department of State Health Services MC 1965 P.O. Box 149347 Austin, Texas 78714-9347Street Address for overnight mailing (UPS, Fed Ex, etc.) 1100 West 49th Street Austin, Texas 78756-3199 Program phone number: (512) 458-7490 Program fax number: (512) 458-7408
Utah Diabetes Prevention and Control Program Utah Department of Health PO Box 142107 Salt Lake City, Utah 84114-2107 Program phone number: (801) 1538-6141 or (888) 222-2542 Program fax number: (801) 538-9495
Vermont Diabetes Prevention and Control Program Vermont Department of Health 108 Cherry Street PO Box 70 Burlington, Vermont 05402-0070 Program phone number: (802) 865-7708 Program fax number: (802) 651-1634
Ohio Diabetes Prevention and Control Program Ohio Department of Health Diabetes Unit, 8th Floor 246 North High Street Columbus, Ohio 43266-0588 Program phone number: (614) 466-2144 Program fax number: (614) 644-7740
Oklahoma State Department of Health Diabetes Prevention and Control Program 1000 Northeast 10th Street Oklahoma City, Oklahoma 73117-1299 Program phone number: (405) 271-4072 Program fax number: (405) 271-6315
Oregon Diabetes Prevention and Control Program Health Promotion and Chronic Disease Prevention Program Oregon Department of Human Services, Public Health Division 800 N.E. Oregon Street, Suite 730 Portland, Oregon 97232-2162 Program phone number: (971) 673-0984 Program fax number: (971) 673-0994
Pennsylvania Diabetes Prevention and Control Program Administrators Pennsylvania Department of Health Division of Nutrition and Physical Activity Health & Welfare Building, Room 1000 7th and Forster Streets Harrisburg, Pennsylvania 17120 Program phone number: (717) 787-5876 Program fax number: (717) 783-5498
Rhode Island Diabetes Prevention and Control Program Rhode Island Department of Health 3 Capitol Hill, Room 409 Providence, Rhode Island 02908 Program phone number: (401) 222-6957 Program fax number: (401) 222-4415
South Carolina Diabetes Prevention & Control Program Bureau of Community Health and Chronic Disease Prevention SC Department of Health and Environmental Control 1800 St. Julian Place
mm
23 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
Virginia Department of Health Division of Chronic Disease Control and Prevention Diabetes Prevention and Control Project 109 Governor Street, 10th Floor Richmond, Virginia 23219 Program phone number: (804) 864-7877 Program fax number: (804) 864-7880
Washington State Diabetes Prevention and Control Program Washington State Department of Health 111 Israel Rd, SE, Box 47855 Tumwater, Washington 98501 Program phone number: (360) 236-3799 Program fax number: (360) 236-3708
West Virginia Diabetes Prevention and Control Program 350 Capitol Street, Room 206 Charleston, West Virginia 25301 Program phone number: (304) 558-0644 Program fax number: (304) 558-1553
Wisconsin Diabetes Prevention and Control Program1 W. Wilson/PO Box 2659 Madison, Wisconsin 53701-2659 Program phone number: (608) 261-9422 Program fax number: (608) 266-8925
Wyoming Department of Health Diabetes Prevention & Control Program 6101 Yellowstone Road, Suite 259A Cheyenne, Wyoming 82002 Program phone number: (307) 777-3579 Program fax number: (307) 777-8604

mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
24 mm
The survey data will not identify the participants nor can the survey responses be linked back to the individual participants.
Using a Diabetes Educator U.S. Diabetes Conversation Map® Experience Survey, this evaluation study will gather diabetes educator experiences with the Conversation Map tools. The survey is written at a 5th grade reading level and is anonymous. The survey data will not identify the participants nor can the survey responses be linked back to the individual participants. The survey captures educator experiences in using the Map tools, barriers to Map tool use, factors that facilitated Map tool use, and basic demographics. This survey will be developed in an electronic format using Survey Monkey and e-mailed to each educator for completion at the end of their Conversation Map facilitation experience.
Data Entry and AnalysisAt the end of each session, the participants will place their completed Participant Post-session Surveys in an envelope labeled with the date of session, the session location (including state), and the name of the educator. The envelope will be mailed to the project evaluator for data entry, analysis and evaluation reporting. The surveys will be shredded after
reported in aggregate format, not individually. The educator survey results will be gathered by Survey Monkey and submitted to the project evaluator using a spreadsheet format. The educator survey results will be reported in aggregate format, not individually.
Access to the DataThe project evaluator and National Association of Chronic Disease Directors (project administrator) will have access to the anonymous subject data.
The risk for participation in the completion of the surveys is minimal. Some participants may feel disappointed with their group diabetes education class after completing the post-
from the completion of the surveys in these ways: having an
the evaluators, and feeling as though their input was heard and valued.
Brief description of the project: The EDGE project was designed to expand and enhance use of the U.S. Diabetes Conversation Map® tools as part of group diabetes self-management education (DSME), and to increase reach for programs using these Conversation Map tools to serve people with diabetes (PWD) who experience the greatest diabetes-related health disparities. The project will focus on serving people with diabetes who experience diabetes-related
from racial/ethnic minority groups, (2) individuals who have low or inadequate incomes, (3) individuals who are un-insured or under-insured; and (4) individuals who are more comfortable using Spanish as their primary language.
Participant and educator experience with the U.S. Diabetes Conversation Map® tools has been documented and published in the literature with primarily white participants or participants
evaluation will gather session experiences from a group of participants and educators using the Maps compared to a group of participants who did not use the Maps in their group session.
Reason for Exemption The data are being collected to better understand subject experiences with an education class for the purposes of quality improvement. The data will be collected in such
completely anonymous.
Data CollectionUsing a Participant Post-session Survey, this evaluation will gather participant experiences from two groups: (1) participants who participated in the Conversation Map group diabetes education class, and (2) participants who participated in a group diabetes education class without the Conversation Map tools. The 2-page survey will be completed at the end of a group diabetes class. The survey captures class experiences, diabetes status, and demographics. The survey is at a 5th grade reading level and will be translated into Spanish for participants who are more comfortable using Spanish as their primary language. The survey is completed anonymously.
Appendix D: Evaluation Detail to Apply for IRB Exemption

mm
25 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
Informed ConsentFor a number of reasons, an informed consent is not necessary for this evaluation. The completion of the participant post-session survey and the educator experience survey is voluntary. The participants and educators can withdraw from participation by not completing the surveys.
survey results cannot be linked back to individual participants or educators. All data will be analyzed and reported in aggregate formats.

mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
26 mm
Appendix E: Participant Survey
U. S. Diabetes Conversation Map® Group Education Participant Survey
InstructionsThis survey should be completed by persons with Type 2 Diabetes who are enrolled in today’s diabetes group education Conversation Map class. Friends or family members of the person with diabetes attending today do not complete the survey.
Purpose of the SurveyThis survey is designed to capture your experiences, interactions and satisfaction with today’s class. Your feedback will be used to better understand diabetes education. Your responses will be kept . Please be honest.
Today’s Date: ________________________
1. Which U.S. Diabetes Conversation Map tool was used today in your group education class? ¨ On the Road to Better Managing Your Diabetes ¨ Diabetes and Healthy Eating ¨ Monitoring Your Blood Glucose Results ¨ Continuing Your Journey with Diabetes
2. Please mark (X) the response that best describes your experiences TODAY.
1 2 3 4 5a. The class was interactive, with lots of discussion
among the participants. Strongly Disagree
Disagree Not Sure Agree Strongly Agree
b. For the most part, the discussion was relevant to my own life.
Strongly Disagree
Disagree Not Sure Agree Strongly Agree
c. I learned new health facts that can be used to manage diabetes.
Strongly Disagree
Disagree Not Sure Agree Strongly Agree
d. I felt comfortable sharing with other people in the class.
Strongly Disagree
Disagree Not Sure Agree Strongly Agree
e. I learned a lot from the group discussion about how to manage diabetes.
Strongly Disagree
Disagree Not Sure Agree Strongly Agree
f. As a result of today’s class, I know that people can successfully manage their Type 2 Diabetes.
Strongly Disagree
Disagree Not Sure Agree Strongly Agree
g. Today’s class gave me ideas on how to reach my personal health goals.
Strongly Disagree
Disagree Not Sure Agree Strongly Agree
h. I would recommend this class to a friend or family member in need.
Strongly Disagree
Disagree Not Sure Agree Strongly Agree
mm
27 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
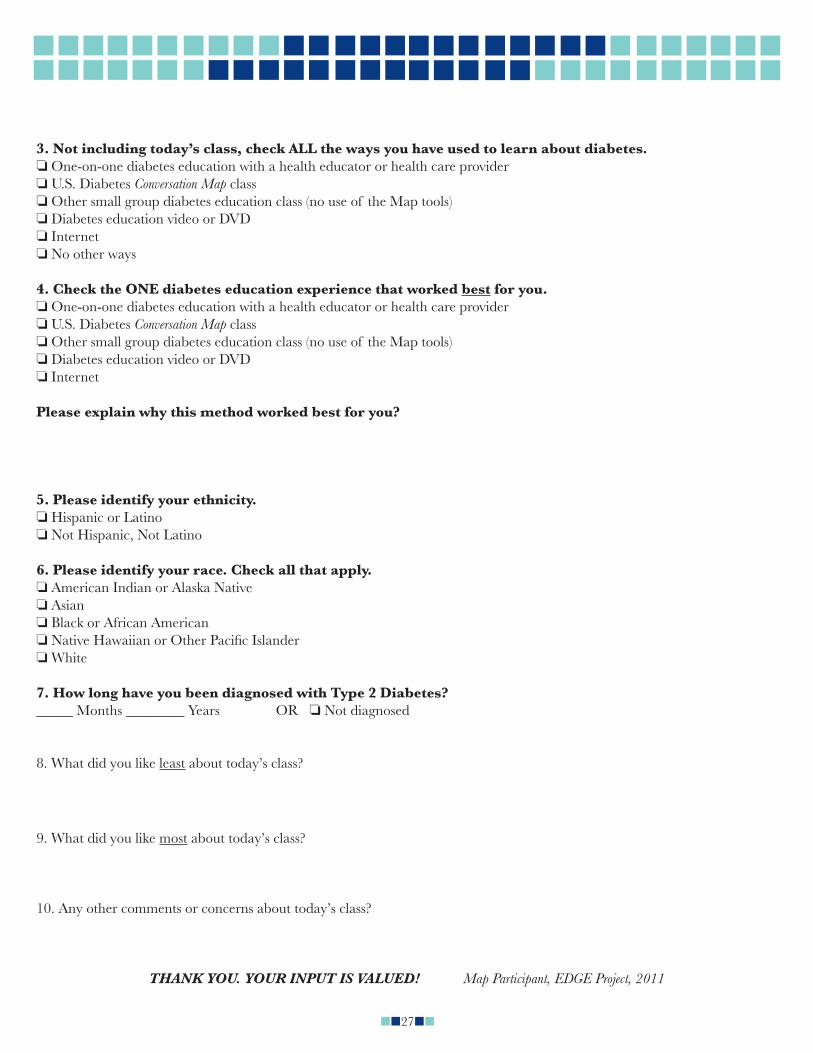
3. Not including today’s class, check ALL the ways you have used to learn about diabetes. One-on-one diabetes education with a health educator or health care provider U.S. Diabetes Conversation Map class Other small group diabetes education class (no use of the Map tools) Diabetes education video or DVD Internet No other ways
4. Check the ONE diabetes education experience that worked best for you. One-on-one diabetes education with a health educator or health care provider U.S. Diabetes Conversation Map class Other small group diabetes education class (no use of the Map tools) Diabetes education video or DVD Internet
Please explain why this method worked best for you?
5. Please identify your ethnicity. Hispanic or Latino Not Hispanic, Not Latino
6. Please identify your race. Check all that apply. American Indian or Alaska Native Asian Black or African American
White
7. How long have you been diagnosed with Type 2 Diabetes? _____ Months ________ Years OR Not diagnosed
8. What did you like least about today’s class?
9. What did you like most about today’s class?
10. Any other comments or concerns about today’s class?
THANK YOU. YOUR INPUT IS VALUED! Map Participant, EDGE Project, 2011
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
28 mm
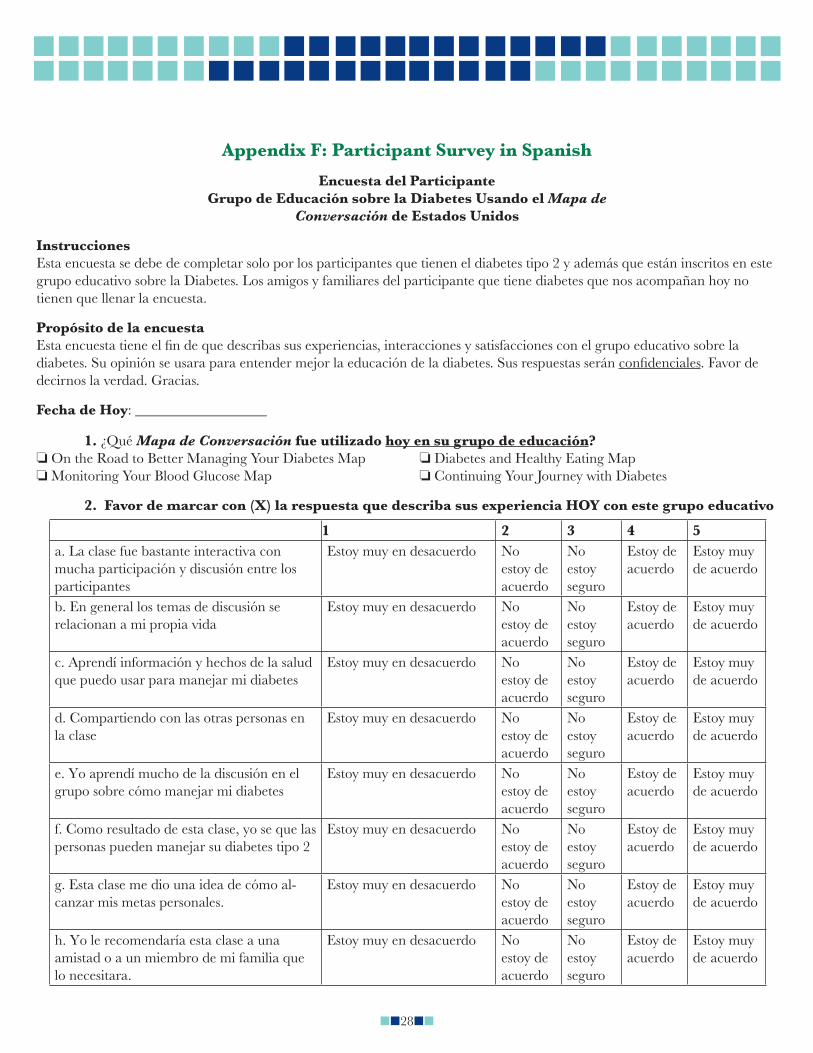
1 2 3 4 5a. La clase fue bastante interactiva con mucha participación y discusión entre los participantes
Estoy muy en desacuerdo No estoy de acuerdo
No estoy seguro
Estoy de acuerdo
Estoy muy de acuerdo
b. En general los temas de discusión se relacionan a mi propia vida
Estoy muy en desacuerdo No estoy de acuerdo
No estoy seguro
Estoy de acuerdo
Estoy muy de acuerdo
c. Aprendí información y hechos de la salud que puedo usar para manejar mi diabetes
Estoy muy en desacuerdo No estoy de acuerdo
No estoy seguro
Estoy de acuerdo
Estoy muy de acuerdo
d. Compartiendo con las otras personas en la clase
Estoy muy en desacuerdo No estoy de acuerdo
No estoy seguro
Estoy de acuerdo
Estoy muy de acuerdo
e. Yo aprendí mucho de la discusión en el grupo sobre cómo manejar mi diabetes
Estoy muy en desacuerdo No estoy de acuerdo
No estoy seguro
Estoy de acuerdo
Estoy muy de acuerdo
f. Como resultado de esta clase, yo se que las personas pueden manejar su diabetes tipo 2
Estoy muy en desacuerdo No estoy de acuerdo
No estoy seguro
Estoy de acuerdo
Estoy muy de acuerdo
g. Esta clase me dio una idea de cómo al-canzar mis metas personales.
Estoy muy en desacuerdo No estoy de acuerdo
No estoy seguro
Estoy de acuerdo
Estoy muy de acuerdo
h. Yo le recomendaría esta clase a una amistad o a un miembro de mi familia que lo necesitara.
Estoy muy en desacuerdo No estoy de acuerdo
No estoy seguro
Estoy de acuerdo
Estoy muy de acuerdo
Appendix F: Participant Survey in Spanish
Encuesta del ParticipanteGrupo de Educación sobre la Diabetes Usando el Mapa de
Conversación de Estados Unidos
InstruccionesEsta encuesta se debe de completar solo por los participantes que tienen el diabetes tipo 2 y además que están inscritos en este grupo educativo sobre la Diabetes. Los amigos y familiares del participante que tiene diabetes que nos acompañan hoy no tienen que llenar la encuesta.
Propósito de la encuesta
diabetes. Su opinión se usara para entender mejor la educación de la diabetes. Sus respuestas serán . Favor de decirnos la verdad. Gracias.
Fecha de Hoy: __________________
1. ¿Qué Mapa de Conversación fue utilizado hoy en su grupo de educación? On the Road to Better Managing Your Diabetes Map Diabetes and Healthy Eating Map Monitoring Your Blood Glucose Map Continuing Your Journey with Diabetes
2. Favor de marcar con (X) la respuesta que describa sus experiencia HOY con este grupo educativo

mm
29 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
3. Sin incluir la clase de hoy, marque todas las maneras que usted ha utilizado para aprender sobre el diabetes.
Clases de educación individual uno a uno con un educador de salud o un medico Clase del Mapa de Conversación Diabético de Estados Unidos Otro grupo pequeño de clases del diabetes (sin el uso del mapa) Video o DVD sobre la educación de la Diabetes Internet De ninguna clase
4. Cheque cual es la experiencia educativa de la diabetes que funciona mejor para usted (SOLO UNO) Clases de educación individual uno a uno con un educador de salud o un médico Clase de grupo de educación de diabetes usando el Mapa de Conversación de EEUU Otro grupo pequeño de clases del diabetes (sin el uso del mapa) Video o DVD sobre la educación de la Diabetes Internet
¿Por favor explique porque este método funciono mejor para usted?
5. Por favor indique su etnicidad. Hispano o Latino No soy Hispano o Latino
Indio Americano o Nativo de Alaska Asiático Negro o Áfrico Americano
Blanco
7. ¿Que tanto tiempo hace que le diagnosticaron el diabetes tipo 2? _____ Meses ________ Años O No me han diagnosticado
8. ¿Que es lo que menos que le gusto de la clase de hoy?
9. ¿Que es lo mas que le gusto de la clase de hoy?
10. ¿Cualquier comentario o preguntas sobre la clase de hoy?
¡Gracias! Valoramos su participación y su opinión. Map Participant, EDGE Project, 2010

mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
30 mm
Appendix G: Diabetes Educator U.S. Diabetes Conversation Map® Experience Survey
This survey is designed to capture your experiences and interactions related to your use of the U.S. Diabetes Conversation Map tools. Your feedback will be used to better understand diabetes group education using the Map tools. Your responses will be kept . Please be honest.
Today’s Date: _________________________
1. How long have you been using the U.S. Diabetes Conversation Map tools for diabetes education? ________________
2. When did you complete your Conversation Map training? _______(month, year)
3. How long have you been involved in the EDGE Project? __________________
4. Other than the Conversation Map classes, how have you taught diabetes education? Check ALL that apply. One-on-one diabetes education Other small group diabetes education class (no use of the Maps) Diabetes education video or DVD Other ways: __________________________________________ No other ways (Skip to Question 5)
5. Check the ONE diabetes education experience that works best for you as the educator. One-on-one diabetes education U.S. Diabetes Conversation Map session Other small group diabetes education class (no use of the Map tools) Diabetes education video or DVD Other ways: ___________________________________________
6. Explain why this education method works best for you?
THINK ABOUT YOUR USE OF THE CONVERSATION MAP TOOLS IN THE PAST 3 MONTHS
7. Rate the importance of each of these factors in your use of the Map tools.
Notimportant
Somewhat important
Important Extremely important
The large visual 1 2 3 4The information 1 2 3 4The conversation questions 1 2 3 4The group interaction 1 2 3 4The action plan 1 2 3 4
mm
31 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
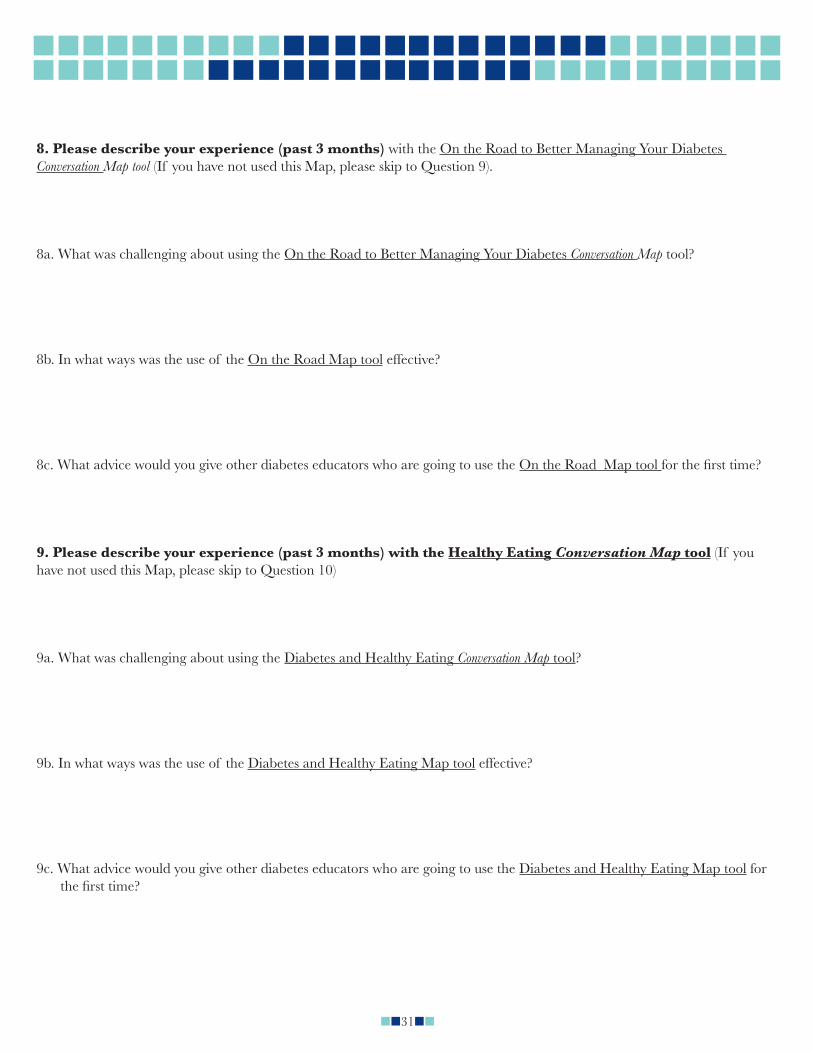
8. Please describe your experience (past 3 months) with the On the Road to Better Managing Your Diabetes Conversation Map tool (If you have not used this Map, please skip to Question 9).
8a. What was challenging about using the On the Road to Better Managing Your Diabetes Conversation Map tool?
8b. In what ways was the use of the On the Road Map tool effective?
8c. What advice would you give other diabetes educators who are going to use the On the Road Map tool
9. Please describe your experience (past 3 months) with the Healthy Eating Conversation Map tool (If you have not used this Map, please skip to Question 10)
9a. What was challenging about using the Diabetes and Healthy Eating Conversation Map tool?
9b. In what ways was the use of the Diabetes and Healthy Eating Map tool effective?
9c. What advice would you give other diabetes educators who are going to use the Diabetes and Healthy Eating Map tool for

mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
32 mm
10. Please describe your experience (past 3 months) with the Monitoring and Using your Blood Glucose Results Conversation Map tool (If you have not used this Map, please skip to Question 11)
10a. What was challenging about using the Monitoring Your Blood Glucose Conversation Map tool?
10b. In what ways was the use of the Monitoring Your Blood Glucose Map tool effective?
10c. What advice would you give other diabetes educators who are going to use the Monitoring Your Blood Glucose Map tool

mm
33 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
Appendix H: EDGE Focus Group Topics for Educators
Purpose of the Focus Group: To gather EDGE partner experiences on the implementation of the EDGE project. The
Introductions: Please introduce yourself and tell us how you are involved with the EDGE project.Suggested Topics/QuestionsPrevious Experience
How many of you used the Conversation Map tools prior to the EDGE project?
Barriers and Facilitating Factors Think about the EDGE project, what were some of the barriers and challenges to implementing maps? Did participants/patients get the information they needed from the Map sessions? How often do the participants ask if group will continue? Trying to get at the social support component of the Map groups… What made the Map program possible? What were the facilitating factors? What was the role of the DPCP in the project?
Adjustments accommodations to the Conversation Map tools? For example, were adjustments
made due to culture, or learning style or issues with vision or literacy? As a part of the EDGE project, were others trained besides the health professionals? For those who were already
trained before EDGE, did you get trained again? How did you orient health educators who were new to the Map tools? Did you try shadowing or pairing health educa-
tors who were new to the Map tools?
Sessions How did you integrate the Conversation Map sessions into your education program? For example, did you offer individ-
ual sessions and then the group session? How many and for how many hours? How many Map tools were covered? drop-out rate to be different with the Map groups compared to the other diabetes education groups?
groups?
Tool Kit What advice would you give to other programs that wish to start using the Conversation Map tools? We would add this
to our implementation tool kit? Any other experiences you would like to add to our discussion today?

mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
34 mm
Appendix I: State Success Stories
Diabetes Education in Arizona Reaches the Underserved Using the U.S. Diabetes Conversation Map® Education Tools
Public Health Issue Self-management education is vital for people with diabetes to help them prevent complications and hospitalizations
from their disease. Diabetes education programs accredited by recognized groups such as the American Association of Diabetes Educa-
tors (AADE) can receive reimbursement for their services, an important factor in sustainability. Enhancing access to delivery of culturally appropriate diabetes education is important in communities with popula-
tions where language and culture can be a barrier to care.
Program The Arizona Department of Health Services Diabetes Prevention and Control Program organized and hosted train-
ings on using the Diabetes Conversation Map education tools designed for Spanish language speakers. Working with a community partner, the El Rio Community Health Center, additional trainings were held.
Clinical pharmacists as well as staff of tribal health departments and the Indian Health Service were trained in using the Map education tools.
Community Health Advisors, community members serving as liaisons between their community and health/social service organizations, recruited health center patients, scheduled classes and encouraged participation as an extension of their wellness and prevention duties.
This work was funded by Merck and Company and the National Association of Chronic Disease Directors.
Impact
-imbursement that sustains provision of these essential education services. The Conversation Map tools serve as El Rio’s diabetes self-management education curriculum.
Community Health Advisors effectiveness in assisting implementation led the health center to add more Community Health Advisors and staff is using an expanded Community Health Advisor intervention model for all prevention education.
The health center now offers more diabetes group education, with patients reporting that this had been helpful in sup-porting their behavior change.
The Conversation Map training experience provided the seed for a proposal and award of $50,000 from the American Pharmacists Association Foundation to implement an IMPACT: Diabetes project in partnership with the Bristol-My-ers Squibb Foundation as part of their Together on Diabetes initiative. This new project will further integrate diabetes education and pharmacy services.
The integrated model resulting from this Conversation Map project helped the health center leverage National Com-mittee for Quality Assurance Patient-Centered Medical Home accreditation, an innovative program for improving primary care.
ContactsSandra Leal, PharmD, CDE Carmen Ramirez El Rio Health Center Arizona Department of Health Services520-302-5325 [email protected]@gmail.com

mm
35 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
Diabetes Group Education in Connecticut Enhanced through the Use of U.S. Diabetes Conversation Map® Education Tools
Public Health Issue Diabetes self-management education is cost-effective; investing a dollar can cut health care costs by as much as eight
dollars. Diabetes self-management education is also a key step in improving health outcomes and quality of life for people with
diabetes because it helps them apply lessons they learn to better control of their disease. Enhancing access to and delivery of appropriate diabetes self-management education is especially important for popu-
lations at higher risk for diabetes complications and with cultural barriers to care.
Program With funding from Merck and Company and the National Association of Chronic Disease Directors, the Connecti-
cut Department of Public Health Diabetes Prevention and Control Program partnered with two hospitals: Norwalk Hospital and Windham Hospital.
-age of African Americans (15 & 18 percent respectively) and Hispanics/Latinos (16 & 30 percent respectively).
Each hospital program implemented the Diabetes Conversation Map tools using an interactive, culturally appropriate approach to engage people with diabetes, including the use of Spanish-language version Map tools.
Ten clinic facilitators were trained in the use of the Conversation Map tools.
Impact
Increased access to diabetes education services in Spanish resulted from the Windham Hospital program providing a Licensed Practical Nurse as a Spanish language translator and the Norwalk Hospital program implementing a Span-ish language class at the Americares clinic, a free clinic for the uninsured, working poor.
The diabetes group educators who were trained to use the Conversation Map tools reported gaining a better understand-ing of diabetes and how to educate people about self-management. When the Conversation Map tools are used, facilita-tors noticed that the participants were engaged in the conversations, the group dynamic was positive, and participants were eager to share strategies to manage their diabetes with one another.
Educators used project evaluation data to improve their class content and processes.
Contact Cindy Kozak Connecticut Department of Public Health [email protected] 860-509-7737

mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
36 mm
Adapting the U.S. Diabetes Conversation Map® Education Tools for an African American Audience in South Carolina
Public Health Issue Diabetes self-management education helps people with diabetes prevent complications and hospitalizations from this
condition. Emergency Department visits by African Americans with diabetes in South Carolina are almost twice as high as in
others with diabetes. Culturally adapting diabetes self-management education for groups of participants subject to racial/ethnic health
disparities such as higher rates of disease complications makes it more likely that people with diabetes will apply the information and better control their disease.
Educational materials designed to accommodate the various learning styles of program participants are more likely to be effective.
Program With support from Merck and Company and the National Association of Chronic Disease Directors, the South Caro-
lina Department of Health and Environmental Control Diabetes Prevention and Control Program partnered with American Diabetes Association-recognized programs in rural Berkeley and Dorchester counties to use the Diabetes Conversation Map tools.
Both participating rural counties have a large African American population, are part of the REACH US SEA-CEED project, and are working to eliminate health disparities related to diabetes prevention and control.
-posed to the Conversation Map tools in their diabetes group education classes.
The Conversation Map tools were adapted for the African American participant population by expanding one carbohy-drate counting session to two sessions, adding several ‘myth’ cards, adding images of places of worship, and providing facilitation for the reading of the cards.
Impact Following the diabetes group education session with the Conversation Map tools almost all of the adults participating in
centers. According to the diabetes educators, the Conversation Map tools were effective in reaching an underserved group of
people by revealing and dispelling myths participants had about diabetes, removing barriers to participant’s self-care, and increasing the likelihood that the participant will take action to control their disease.
Diabetes educators are more likely to use the Conversation Map tools because the training and the tools are available at no-cost.
ContactsSyndia Moultrie Melanie Robinson Michelle Moody REACH SEA:CEED SC DHEC SC DHEC843-792-5872 843-792-3561 [email protected] [email protected] [email protected]

mm
37 mm
mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
U.S. Diabetes Conversation Map® Education Tools Promote Delivery of Diabetes Education in Rural South Dakota
Public Health Issue Diabetes self-management education prevents complications and hospitalizations from diabetes. One dollar invested
in education can cut health care costs by up to $8.76. It is a key step in improving health outcomes and quality of life for people with diabetes.
Educating groups of people with diabetes is not just cost-effective—it is also effective in helping people with diabetes apply the lessons they learn to better control their disease.
Enhancing access to and delivery of diabetes self-management education is especially important in rural states where long driving distances are a barrier.
Program With support from Merck and Company and the National Association of Chronic Disease Directors, the South Da-
kota Diabetes Prevention and Control Program implemented a demonstration project, Evaluating Diabetes Group Education, to increase the use of the Diabetes Conversation Map tools.
Diabetes educators trained in the Conversation Map tools, actively engaged participants in the learning process as a springboard for meaningful behavior change.
At the onset of the project, all providers of diabetes self-management education programs in South Dakota were in-vited to participate in a conference call on the topic of using the Conversation Map tools. For diabetes group educators in South Dakota, this informal networking group served as a forum for problem-solving and sharing lessons learned.
The public/private partners examined factors related to the increased use of the Conversation Map tools with recognized diabetes education programs, and explored the role of the state diabetes prevention and control programs in augment-ing the effort.
Impact This project led the state health department to organize diabetes educators into a ‘users group,’ a line of communi-
cation which is facilitating implementation and expansion of diabetes self-management education in South Dakota, including the use of the Conversation Map tools.
A large hospital system is now reaching out to their satellite sites around the state to coordinate and expand diabetes group education to more participants and to potentially use teleconferencing technology to extend education to more rural parts of the state.
More no-cost, unbranded resources are now available in the state for diabetes education. The contacts made through this project with developers of the Conversation Map tools will help additional diabetes group education programs be-come established.
State Program staff continues to promote the use of the Conversation Map tools, engage new diabetes educators in the users group, and provide access to the no-cost tools.
ContactsPamela Schochenmaier Zach ParsonsSouth Dakota Department of Health South Dakota Department of Health605-773-6744 [email protected] [email protected]

mm mmm m mm mmm mmm mmm mmm mmm m mm mmm m
mmmmmmmmmmmm mmmmmm mmmmmmmmmmmm
mm
38 mm
References.
1. Healthy Interactions. A More Direct Route to Personal Health Engagement®. Available at: http://www.healthyinter-actions.com/conversation-map-programs/conversation-map-learning-methodology.
2. Funnell MM, Brown TL, Childs BP, Haas LB, Hosey GM, Jensen B., et al. National standards for diabetes self-man-agement education. Diabetes Care. 2010; 33(Supplement 1): S89-S96.
3. AADE7™. Available at: http://www.diabeteseducator.org/ProfessionalResources/AADE7/.
4. Public Health Functions Steering Committee. Public Health In America,1994. Available at: http://www.health.gov/phfunctions/public.htm
5. U.S. Department of Health and Human Services. Healthy People 2020. Objective D-14 D-14 Increase the proportion of persons with diagnosed diabetes who receive formal diabetes education. Available from: http://www.healthypeople.gov/2020/topicsobjectives2020/objectiveslist.aspx?topicId=8.
6. McLeroy KR, Bibeau D, Steckler A, Glanz K. An ecological perspective on health promotion programs. Health Edu-cation Quarterly. 15:351–377, 1988.