uva-dare (digital academic repository) selecting ... filetechniques are still in use. in 1950, aubel...
TRANSCRIPT

UvA-DARE is a service provided by the library of the University of Amsterdam (http://dare.uva.nl)
UvA-DARE (Digital Academic Repository)
Selecting diagnostic strategies in primary pelvic organ prolapseGroenendijk, A.G.
Link to publication
Citation for published version (APA):Groenendijk, A. G. (2009). Selecting diagnostic strategies in primary pelvic organ prolapse.
General rightsIt is not permitted to download or to forward/distribute the text or part of it without the consent of the author(s) and/or copyright holder(s),other than for strictly personal, individual use, unless the work is under an open content license (like Creative Commons).
Disclaimer/Complaints regulationsIf you believe that digital publication of certain material infringes any of your rights or (privacy) interests, please let the Library know, statingyour reasons. In case of a legitimate complaint, the Library will make the material inaccessible and/or remove it from the website. Please Askthe Library: http://uba.uva.nl/en/contact, or a letter to: Library of the University of Amsterdam, Secretariat, Singel 425, 1012 WP Amsterdam,The Netherlands. You will be contacted as soon as possible.
Download date: 07 Jun 2019

1CHAPTER 1
General introduction and outlineof the thesis
9
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 9

10
Chapter 1
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 10

1INTRODUCTION
The subject of this thesis is the diagnostic process leading to the diagnosis andtreatment proposal of primary pelvic organ prolapse. Below we first give a briefimpression of the past, the epidemiology, the present care and etiology ofpelvic organ prolapse. Next, the functional anatomy is described to provide abetter understanding of the pathophysiology of pelvic floor symptoms, and toclarify the underlying principles of the various aspects of the diagnostic testsperformed in our study. After a discussion of the objectives and (dis)advantagesof the current diagnostic process of pelvic organ prolapse, the study aims aredescribed and a guide of the thesis is presented.
THE PAST
Pelvic organ prolapse is of all times. As long as women give birth, vaginalprolapse must have existed. The earliest descriptions on the prevention andtreatment of vaginal prolapse have been found in two medical papyri of theancient Egyptians 2000 years BC. In these records vaginal prolapse is referredto as “falling of the womb” and they contain ”remedies to allow the womb of awomen to slip into its place”1. In the days of Hippocrates (400 BC), successionwas employed as treatment for irreducible prolapse. After the uterus wasrubbed with ointments, the woman was tied upside down on a ladder likeframe, this frame was shaken back and forth for several minutes, hoping that thewomb would return in its proper position. Another popular treatment in theantique world was reposition of the womb with a half pomegranate soaked invinegar. This combination worked both mechanically and astringed2.
Until the 19th century, the diagnosis of vaginal prolapse was solely basedon inspection and palpation, often in standing position, while treatmentconsisted of reposition of the uterus by means of a pessary3 (Fig. 1a en b).Hysterectomy was occasionally performed in case of unbearable pain due to agangrenous womb. The surgery often ended in bad outcome as the anatomy ofa complete vaginal prolapse was poorly understood; it was no exception thatthe bladder instead of the uterus was removed4. From the second half of 19thcentury, after the introduction of anaesthesia and antiseptics, surgicaltreatments for vaginal prolapse were implemented and some of thesetechniques are still in use. In 1950, Aubel wrote in his thesis “Prolapsus Uteri etVaginae” that the diagnosis of vaginal prolapse is usually easy to make and thatonly the assessment of an enterocele posterior causes difficulties5. Like hiscontemporaries, he attributed the high rate of posterior wall recurrence to
11
General introduction and outline of the thesis
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 11

12
Chapter 1
Fig. 1a Gynecological exami-
nation in the Middle Ages
Fig. 1b Insertion of a pessary
in the Middle Ages
From Caspar Stromayr’s Die
Handschrift des Schnitt- und
Augenartzes. Kindly provided
by Prof. dr. F.B. Lammes
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 12

1inappropriate surgical interventions for alleged rectoceles, which in fact shouldhave been classified under posterior enteroceles.
Since the second half of the last century, as result of new technologicaldevelopments, advanced diagnostic tests are increasingly applied for therefinement of the diagnosis and to optimise treatment selection of pelvic organprolapse. Despite the currently sophisticated technical tests to identify pelvicfloor defects and disorders, the failure rate of surgical treatment is stillunacceptably high6.
THE PRESENT
Epidemiology and use of carePelvic organ prolapse (POP) is a common condition in women, especially athigher age. As there is no validated definition of pelvic organ prolapse, the exactprevalence of this condition in the female population is difficult to determine.According to epidemiological studies, up to 40% of women over the age of fiftyyears have some loss of pelvic organ support. Pelvic floor symptoms usually donot occur before the prolapse reaches the hymen7. Pelvic organ prolapse with adescent beyond the hymen has probably a prevalence between 3 and 6%8-11.Although pelvic organ prolapse rarely results in severe morbidity or mortality, itsassociated symptoms can affect daily activities12 and quality of life13, 14.
POP is also associated with use of medical care, particularly generalpractitioner, medical specialist and physiotherapist visits, but also medications,use of incontinence materials, and medical aids (e.g. pessarium, urethra plugs,Conveen/Femcare tampons).
13
General introduction and outline of the thesis
Annual incidence and prevalence rates of urinary incontinence and POP per 1000 womena
Patient age (years) Incidence PrevalenceUrinary incontinence POP Urinary incontinence POP
25-44 2.6 1.2 4.5 2.245-64 5.4 3.6 11.8 8.165-74 7.4 5.6 22.6 20.1>75 years 11.9 5.1 51.3 26.7Total 3.7 2.0 9.9 6.1a Van der Linden MW, Westert GP, De Bakker DH, Schellevis FG. Tweede Nationale Studie naar ziekten in de huisartsenpraktijk (NIVEL 2004, ISBN 9069056496) www.nivel.nl/nationalestudie/
Table 1 Yearly incidence and prevalence of urinary-incontinence at the general practitioner in the
Netherlands (2001)
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 13
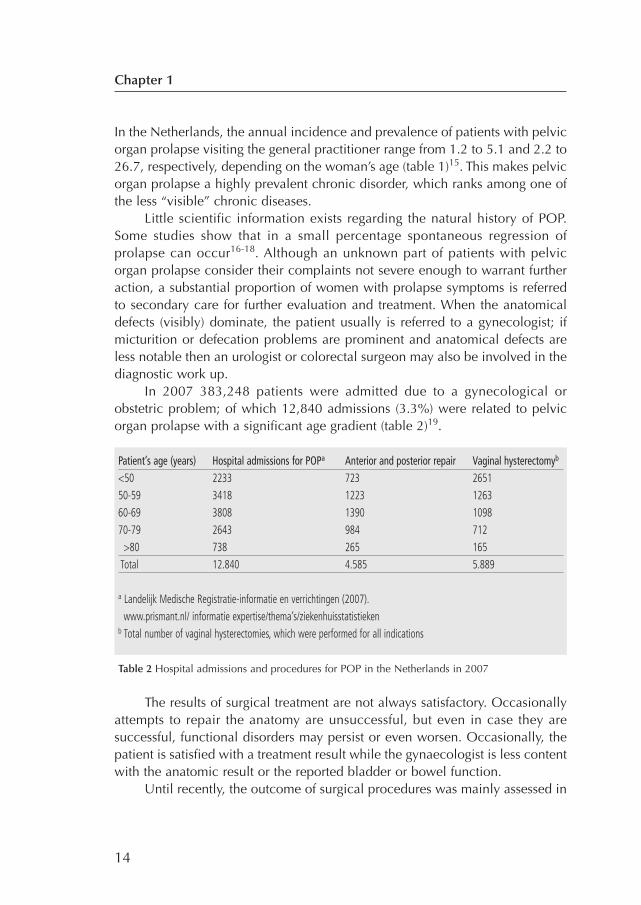
In the Netherlands, the annual incidence and prevalence of patients with pelvicorgan prolapse visiting the general practitioner range from 1.2 to 5.1 and 2.2 to26.7, respectively, depending on the woman’s age (table 1)15. This makes pelvicorgan prolapse a highly prevalent chronic disorder, which ranks among one ofthe less “visible” chronic diseases.
Little scientific information exists regarding the natural history of POP.Some studies show that in a small percentage spontaneous regression ofprolapse can occur16-18. Although an unknown part of patients with pelvicorgan prolapse consider their complaints not severe enough to warrant furtheraction, a substantial proportion of women with prolapse symptoms is referredto secondary care for further evaluation and treatment. When the anatomicaldefects (visibly) dominate, the patient usually is referred to a gynecologist; ifmicturition or defecation problems are prominent and anatomical defects areless notable then an urologist or colorectal surgeon may also be involved in thediagnostic work up.
In 2007 383,248 patients were admitted due to a gynecological orobstetric problem; of which 12,840 admissions (3.3%) were related to pelvicorgan prolapse with a significant age gradient (table 2)19.
The results of surgical treatment are not always satisfactory. Occasionallyattempts to repair the anatomy are unsuccessful, but even in case they aresuccessful, functional disorders may persist or even worsen. Occasionally, thepatient is satisfied with a treatment result while the gynaecologist is less contentwith the anatomic result or the reported bladder or bowel function.
Until recently, the outcome of surgical procedures was mainly assessed in
14
Chapter 1
Patient’s age (years) Hospital admissions for POPa Anterior and posterior repair Vaginal hysterectomyb
<50 2233 723 265150-59 3418 1223 126360-69 3808 1390 109870-79 2643 984 712
>80 738 265 165Total 12.840 4.585 5.889
a Landelijk Medische Registratie-informatie en verrichtingen (2007). www.prismant.nl/ informatie expertise/thema’s/ziekenhuisstatistieken
b Total number of vaginal hysterectomies, which were performed for all indications
Table 2 Hospital admissions and procedures for POP in the Netherlands in 2007
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 14

1retrospective studies, showing that recurrence rate of the prolapse after 5 yearsfollow-up is 8% to 36%. It is unclear whether this wide range is due to theinclusion criteria, differences in definition or a true difference. There are only alimited number of prospective (randomised controlled) studies on the outcomeof surgical prolapse repair. The reported recurrence rate in these studies isapproximately 40% which is comparable to the recurrence rates found inretrospective studies20-22. If therapy fails, the chronic state may be disturbingand demanding much care (e.g. disposables, physician time, repeat diagnostictest, re-operation).
EtiologyThe pathogenesis of pelvic organ prolapse is not fully understood but it seemsthe result of a weakening of the supporting tissue including pelvic floor muscles,ligaments and fascia. Childbirth, congenital factors and hysterectomy areconsidered to be important risk factors in the etiology of pelvic organ prolapse.Childbirth results in direct damage of the connective tissue and muscles of thepelvic floor and indirect damage by neuropathic injury, while caesarean sectionappears to protect against pelvic organ prolapse development23, 24. Some reportssuggest that a policy of routine elective caesarean section might prevent vaginalprolapse up to 46%25. Congenital inferior quality of connective tissue due tocollagen disorders may also be a factor and probably predominate in patientswith pelvic organ prolapse younger than 35 years of age26. Klutke et al. found asignificantly decreased desmosine content in the uterosacral ligament tissuefrom women with prolapse and more than two deliveries and from women withcomplete procidentia compared to matched controls27. Furthermore, somereports suggest that hysterectomy might increase the risk of subsequent vaginalprolapse as women with previous hysterectomy have a higher risk of prolapsesurgery28, 29. Finally, other described risk factors are increased intra-abdominalpressure in chronic pulmonary diseases, chronic constipation, diabetes andobesity30.
Functional anatomy of the pelvic floor Damage of the pelvic floor may result in a loss of support of the pelvic organsand to a compromised function of the urethra, bladder and anorectum. For along time the anatomy of the pelvic floor has been studied in elderly femalecadavers. The anatomical relationships in cadaver studies are quite differentfrom those found in health and diseased living women. This has resulted indisagreement about what is normal and in discussions about the importance offactors that determine the position of the pelvic organs.
15
General introduction and outline of the thesis
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 15

Bonney (1934) was the first to suggest that the organs were supported frombelow and suspended form above31. Last decades knowledge on the anatomyand function of the pelvic floor has increased due to dynamic magneticresonance imaging studies, defecography and 3-dimensional ultrasound32-34.The individual contributions of the ligaments, connective tissue and musclesinvolved in the pelvic floor function are now better understood and the conceptof a support and suspension system is generally being acknowledged. TheIntegral Theory of Papa Petros has further contributed to our understanding ofthe pelvic floor function35. The basic principles of the Integral Theory confirmBonney’s hypothesis that damage of the pelvic floor, especially of theconnective tissue and the ligaments, results in a loss of support of the pelvicorgans (pelvic organ prolapse) and to a compromised function of the urethra,bladder and anorectum. The ligaments (pubo-urethral ligament, uterosacralligaments and the arcus tendineus), fascia and connective tissue provide thesuspension of the pelvic organs. The uterosacral and cardial ligaments pull theupper part of the vagina and cervix backwards, which gives the vagina its
16
Chapter 1
Fig. 2 The relationship of the pelvic muscles to organs, ligaments and fascia
Bone:PS=pubic symphysisS=sacrum
Suspensory ligaments:PUL=pubourethral ligamentATFP=arcus tendineus fascia pelvisUSL= uterosacral ligament
Muscle forces:PCM= pubococcygeus muscleLP= levator plateLMA=longitudinal muscle of the anusPRM= puborectalis muscle
Supporting fascia:PCF=pubocervical fasciaRVF=rectovaginal fascia
Perineal anchoring structures:PB=perineal bodyEAS=external anal sphincter
Adapted from PE Papa Petros. The female pelvic floor. Function, dysfunction and management
according to the integral theory, p 4. With kind permission of PE Petros and Springer Science and
Business Media.
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 16

1horizontal and sacral position. The ligaments also serve to hold the cervix andupper vagina over the pelvic floor (Fig. 2)36. An increase in intra-abdominalpressure results in a narrowing of the angle between the vagina and the pelvicfloor and causes the organs to press upon the levator plate which acts as atrampoline, reflecting both the intra-abdominal pressures and the organs. Whenthe levator plate is damaged of attenuated, it becomes a loose hammock with alow tone. A damaged levator plate is not properly able to counteract increasesin intra-abdominal pressure. The intra-abdominal pressure becomes mainlydirected downward and as a result the levator plate gradually sags and tips bywhen the genital hiatus becomes larger37.
The pelvic floor contributes to urinary continence by providing anadditional occlusive force on the urethra wall. The intrinsic occlusive force of theurethra is generated by multiple structures like the mucosa lining of the urethrawall, the longitudinal and circular smooth muscles, the rhabdomyo sphincterand the peri-urethral part of the pubococygeus muscle, which encircles theurethra and acts as a sphincter. The extrinsic occlusive force is generated by theintra-abdominal pressure transmission to the bladder neck and proximal urethra.A prerequisite for adequate pressure transmission is that the bladder neck andproximal urethra are maintained in an intra-abdominal position during increasesof intra-abdominal pressure. Only then, increases in intra-abdominal pressureare borne by bladder and urethra alike, minimizing any differential pressuregradient that would favour the opening of the bladder neck.
This pressure-transmission theory has been challenged by Petros andUlmsten, who attribute stress-urinary incontinence to a mechanical imbalancedue to lax pubo-urethral ligaments and vagina38.
DeLancey also emphasized the importance of the urethral support by thepubo-urethral ligaments for the continence mechanism. The posterior pubo-urethrala ligaments prevent downward and posterior rotational displacement ofthe urethra during straining. Intra-abdominal pressure forces the urethra againstthe underlying pubo-urethral ligament and vaginal fascia and through thisupward and downward pressure the lumen of the urethra is squeezed andoccluded39. Thereby, the urethra holds its position while the bladder base maydescend up to 1.5 centimetre, but not below the pubic bone. As a result thebladder neck acts as a valve or ‘kink’, which also contributes to urinarycontinence40. Hypermobility of the bladder neck due to a laxed pelvic floor isassociated with an insufficient pressure transmission on the urethra, reducedocclusive force by the pubo-urethral ligaments and a loss of the normal valvularor ‘kinking’ mechanism. The disturbed pelvic floor mechanism finally results in
17
General introduction and outline of the thesis
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 17
urinary stress incontinence. On the other hand, in case of serious anteriorvaginal wall prolapse, impaired bladder emptying can occur due to extremekinking of the urethra. Bladder outlet obstruction might be one of the underlyingcauses of overactive bladder symptoms41. According to the Integral Theory ofPapa Petros, overactive bladder symptoms may also occur as result ofprematurely activated micturition stretch receptors in the ligaments due to adisturbed musculo-elastic control mechanism42.
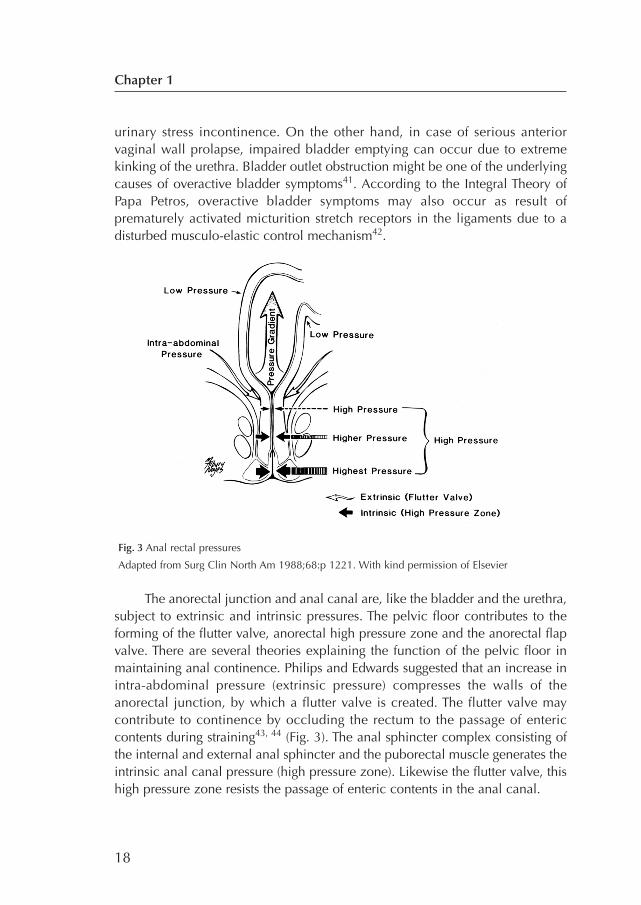
The anorectal junction and anal canal are, like the bladder and the urethra,subject to extrinsic and intrinsic pressures. The pelvic floor contributes to theforming of the flutter valve, anorectal high pressure zone and the anorectal flapvalve. There are several theories explaining the function of the pelvic floor inmaintaining anal continence. Philips and Edwards suggested that an increase inintra-abdominal pressure (extrinsic pressure) compresses the walls of theanorectal junction, by which a flutter valve is created. The flutter valve maycontribute to continence by occluding the rectum to the passage of entericcontents during straining43, 44 (Fig. 3). The anal sphincter complex consisting ofthe internal and external anal sphincter and the puborectal muscle generates theintrinsic anal canal pressure (high pressure zone). Likewise the flutter valve, thishigh pressure zone resists the passage of enteric contents in the anal canal.
18
Chapter 1
Fig. 3 Anal rectal pressures
Adapted from Surg Clin North Am 1988;68:p 1221. With kind permission of Elsevier
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 18
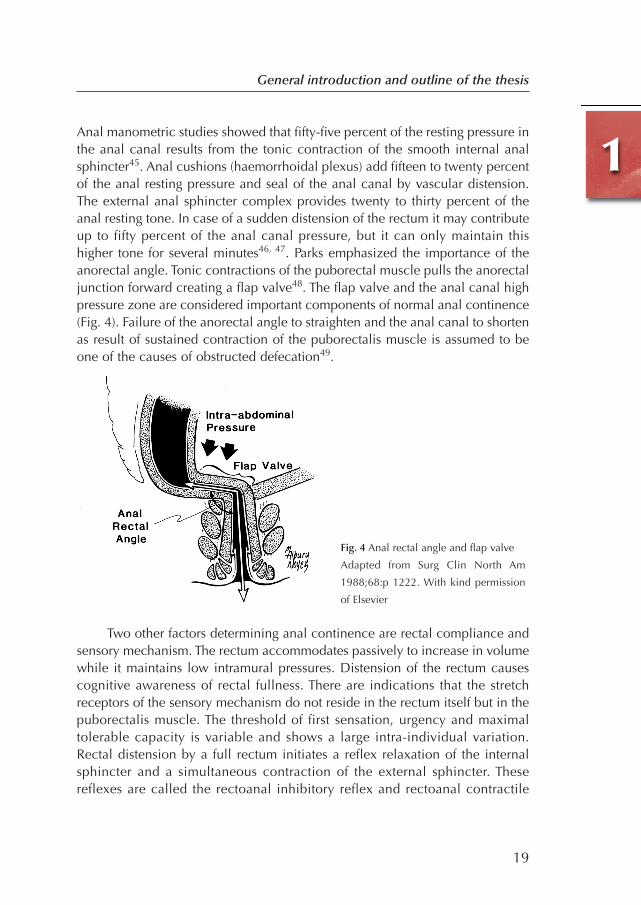
1Anal manometric studies showed that fifty-five percent of the resting pressure inthe anal canal results from the tonic contraction of the smooth internal analsphincter45. Anal cushions (haemorrhoidal plexus) add fifteen to twenty percentof the anal resting pressure and seal of the anal canal by vascular distension.The external anal sphincter complex provides twenty to thirty percent of theanal resting tone. In case of a sudden distension of the rectum it may contributeup to fifty percent of the anal canal pressure, but it can only maintain thishigher tone for several minutes46, 47. Parks emphasized the importance of theanorectal angle. Tonic contractions of the puborectal muscle pulls the anorectaljunction forward creating a flap valve48. The flap valve and the anal canal highpressure zone are considered important components of normal anal continence(Fig. 4). Failure of the anorectal angle to straighten and the anal canal to shortenas result of sustained contraction of the puborectalis muscle is assumed to beone of the causes of obstructed defecation49.
Two other factors determining anal continence are rectal compliance andsensory mechanism. The rectum accommodates passively to increase in volumewhile it maintains low intramural pressures. Distension of the rectum causescognitive awareness of rectal fullness. There are indications that the stretchreceptors of the sensory mechanism do not reside in the rectum itself but in thepuborectalis muscle. The threshold of first sensation, urgency and maximaltolerable capacity is variable and shows a large intra-individual variation.Rectal distension by a full rectum initiates a reflex relaxation of the internalsphincter and a simultaneous contraction of the external sphincter. Thesereflexes are called the rectoanal inhibitory reflex and rectoanal contractile
19
General introduction and outline of the thesis
Fig. 4 Anal rectal angle and flap valve
Adapted from Surg Clin North Am
1988;68:p 1222. With kind permission
of Elsevier
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 19

reflex, respectively. These reflexes are important as they allow the sensory richanal canal to come into contact with enteric contents and to discriminatebetween gas, liquid and solid stool in the rectum50. Other components ofnormal continence are the slow and ultra slow wave fluctuations in the analcanal generated by the internal sphincter muscle. The frequency of these slowwave contractions is larger distally than proximally, producing a gradientpropelling anal contents back into the rectum51.
The striated muscles of the pelvic floor, urethra and external anal sphincterare innervated by the somatic pudendal nerve, arising from the sacral roots S2-S4 and travelling over the cranial surface of the pelvic floor. The pudendal nervecan be damaged by descent of the pelvic floor due to excessive straining duringvaginal delivery or as result of chronic forceful straining at defecation, whichstretches the nerve as it emerges form Alcock’s canal24, 52. Stretching of a nerveby twelve percent of its length may cause permanent nerve injury. It is assumedthat pudendal nerve injury has an adverse effect on the strengths of the pelvicfloor muscles and results in atrophy of the external anal sphincter53. However,electromyographic studies do not always prove the presence of nerve injury,possibly because pundendal nerve terminal latency time measures theconduction in the fasted remaining nerve fibres, by which no significantdifferences in pathologic pudendal latencies between patients with and thosewithout external anal sphincter atrophy may be found54. Anal sphincter defectand atrophy are important structural causes of fecal incontinence.
An intact mature central nervous system is necessary to coordinate urineand fecal storage and when appropriate micturition and defecation. The bladderand anorectum are richly innervated by the autonomic nervous system. Theautonomic parasympathic and sympathic innervation of the bladder, urethra,anorectum and internal anal sphincter is supplied via the sacral pelvic plexus (S2-S4) and hypogastric nerve (Th11-L2), respectively. Parasympatic stimulation viathe acetylcholine receptors in the bladder wall mediates detrusor contraction.Sympathic innervation is associated with urinary storage; the sympathic beta-adrenergic pathway inhibits detrusor contraction, while the alpha-adrenergicpathway provides closure of the bladder neck55. The anal sphincter complex andrectum wall are also subject of intrinsic autonomic innervation. Stimulation of thealpha-adrenergic sympathic receptors has an excitatory effect on the internal analsphincter, whereas beta-adrenergic stimulation has inhibitory effect on of therectal wall. Parasympathic stimulation via the afferent nerves causes contractionof the rectal wall and relaxation of the internal anal muscle.
20
Chapter 1
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 20

1Disturbances in any of the above described physiologic mechanisms may lead tourinary or fecal incontinence, difficulties with bladder emptying, obstructeddefecation or mixed problems. Specific physiologic function testing and imagingmay be helpful to determine the cause of the bladder and bowel symptoms.
DIAGNOSTIC AND THERAPEUTIC GOALS IN THE MANAGEMENT OF PELVIC ORGAN PROLAPSE
Pelvic organ prolapse is a disease with a complex clinical picture. It may includevarious anatomical abnormalities and a wide variety of associated functionaldisorders. Signs of protrusion, pelvic heaviness, bladder and bowel complaints orsexual dysfunction are often the primary reason to visit the gynecologist, althoughmany of these complaints and symptoms may not necessarily be specific forvaginal prolapse. There is no agreement in the literature to what extent thesesymptoms are related to specific pelvic floor defects56. Studies reportcontradictory conclusions about the impact of vaginal prolapse on bladder, boweland sexual function. If pelvic floor symptoms were mainly related to anatomicalsupportive defects, a repair of these anatomical defects would suffice. If therelationship is less clear, it is unlikely that surgical prolapse repair will relievepatient’s urinary and defecatory symptoms. In that case, understanding whichother factors play a role in the pathogenesis of the function disorders, is the keyto tailor the diagnostic and therapeutic approach. Therefore, to optimise thediagnostic process it is mandatory to better understand the relationship betweenfunctional disorders and anatomical abnormalities of the pelvic floor.
The diagnostic processThe aim of surgical prolapse repair is thought to be twofold: one aim is torestore the normal anatomy, the other, more importantly, is to relieve symptomsand to achieve a normal function of the pelvic organs.
A correct diagnosis of the anatomical defect(s) and function disorders isessential for a valid description of the anatomic abnormality, explaining thenature of the symptoms and the selection of a proper therapy. The process ofdiagnosis is divided into two steps: the first consists of medical history takingand physical examination, the second step is to decide whether or not toinitiate additional testing in order to refine the diagnosis and/or to clarify thefunctional disorders.
Medical historyTo obtain a clear picture of the patient’s complaints and symptoms, thediagnostic process starts with a comprehensive, systematic medical review.
21
General introduction and outline of the thesis
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 21

Specific prolapse complaints e.g. vaginal bulging and pelvic pressure arerecorded along with bladder and defecation symptoms and the impact onsexual functioning.
In addition, ‘age’, co-morbidity, use of medication and previous pelvicsurgery are considered important factors in assessing the appropriateness of asurgical procedure57, 58. Medical history taking – a rather subjective andinformal method for the inventory of patient’s complaints and symptoms – maybe supplemented with validated questionnaires as a more formal andstandardized method to record patient’s health status. Studies report pooragreement between the results of medical history and validated questionnaires,probably because patients are inclined to minimize their complaints anddoctors tend to underestimate the complaints of their patients in a personalinterview59, 60. Rodríguez et al. reported that physicians underestimate patient'sbother from urinary symptoms in 25% to 37% of cases61. As validatedquestionnaires more reliably measure the patient’s clinical condition at first visitand subsequently at post-operative visits compared to medical history, they mayalso serve as a baseline measurement against which treatment outcome can beevaluated.
Clinical examinationThere are several methods to classify POP of which the half way system ofBaden and Walker62 and the Pelvic Organ Prolapse-Quantification (POP-Q)system are most well-known63. The aim of these classifications systems is toobtain a standardized, accurate and unequivocal staging of prolapse as thebasis for treatment decisions. Furthermore, a standardized classification systemfacilitates the comparison of therapeutic measures and allows the longitudinalevaluation of individual patient’s health status or treatment outcome. However,the commonly used classification systems reveal important differences ingrading results (Fig. 5)64. In 1996, the POP-Q system was designed because ofconcerns about the reliability of the existing classification systems and toimprove standardization and international communication. The POP-Q systemgives a quantitative description of pelvic organ support by measuring sixvaginal points in relation to the hymen and three fundamental landmarks i.e.genital hiatus, perineal body and total vaginal length, offering a more detaileddescription of the prolapse than the popular, easy to use, but less sensitive half-way system of Baden and Walker. The Baden and Walker classification systemmerely describes whether the descent of the various compartments is above, atthe level or beyond the level of the hymen. Despite efforts made by theInternational Continence Society (ICS), the implementation of the POP-Q
22
Chapter 1
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 22

1system in general clinical practice was hampered. Arguments put forwardagainst the POP-Q system were that it is too time consuming, too confusing,that colleagues do not use it and that it has ‘no clinical relevance’65. Since thesimilarities and discrepancies between the Baden and Walker and POP-Qsystem with regard to the clinical stages and its reliability (reproducibility) wereonly scarcely investigated66, we decided to study to what extent the reliabilityof both systems are comparable and to judge whether these systems areinterchangeable.
Additional diagnostic testingAlthough standardized classification systems enhance the description of theprolapse, physical examination may not always identify all the anatomicaldefects, which is needed for optimal treatment selection. One of the limitationsof physical examination is that only the vaginal side of the protrusion can beseen and that masked anatomical defects can be easily overlooked. Furthermore,in spite of a careful history taking and physical examination, the precise natureof the symptoms may not be explained and complaints may be inconsistent withclinical findings.
Additionally a wide variety of imaging techniques is available likemagnetic resonance imaging, defecography, ultrasound scanning, and functiontests e.g. urodynamic evaluation and anal manometry. There are no guidelines
23
General introduction and outline of the thesis
Fig. 5 Prolapse classification systems
Adapted from Theofratus JP, Swift SE. The clinical evaluation of pelvic floor dysfunction. Obstet
Gynecol Clin North Am 1998:25:4:p 790. With kind permission of Elsevier
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 23

to decide when and in whom one or more additional diagnostic tests should beinitiated in order to improve accuracy of diagnosis and treatment outcome.Some diagnostic labels can be reliably assigned after medical history andphysical examination have been completed, for example in case of a simpleone-compartment prolapse without functional disorders, while others requirespecific additional test information, for example when the prolapse is morecomplex and is accompanied with one or more functional symptoms. As theapplication of diagnostic tests is far form evidence based, a direct consequenceof this ‘diagnostic uncertainty’ may be that the patient is examined tooextensively, resulting in diagnostic burden without therapeutic benefit.Alternatively, it is equally possible that clinicians might be too restrictive evenif surgery is considered, resulting in incomplete or false diagnoses and lessoptimal treatment choices. Extended testing involves the risk of overdiagnosisand overtreatment of insignificant findings, while too restricted testing involvesthe risk of underdiagnosis and being too restrictive in treatment of significantdefects. Unnecessary tests should be avoided for being burdensome for thepatient and expensive for community, while no benefits can be expected interms of improved diagnosis, better understanding of the underlying cause ofthe symptoms, or selection of the optimal treatment. Although the InternationalContinence Society recommends the use of ancillary tests for appropriate pre-operative evaluation of POP patients63, no specific guidelines exist on the useof additional diagnostic testing to improve the description of pelvic floordefects. In the few official guidelines on the management of urinary stress-incontinence and the surgical management of vaginal vault prolapse, onlysparse recommendations are made for the application of additional testing incase of anterior compartment disorders, while recommendations for theevaluation of posterior compartment disorders are lacking67-73. Due to theabsence of evidence based guidelines on vaginal prolapse evaluation, localhospital routine, physician’s education and the availability of diagnostic toolswill play an important role in patient decision-making.
Treatment selectionThe results of treatment outcome studies are difficult to interpret due toconsiderable variation in the preoperative and postoperative evaluation of theprolapse74. The diagnostic classification on which therapy is based is oftenunclear and consensus regarding methods of outcome assessment is lacking75.The effect of surgery is mainly expressed in anatomic outcome and lessfrequently in terms of bladder, bowel and sexual function or health relatedquality of life. Often only short-term complications and recurrence rates are
24
Chapter 1
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 24

1reported. Most reports are based on case series or observational studies. Thereare only few prospective long term therapeutic outcome studies, recurrencerates and health-related quality of life. Only few randomised controlled trialsare available, obscuring the long-term outcome of various surgical treatments.A Cochrane review on the surgical management of pelvic organ prolapseidentified twenty-two randomised controlled trials: seven studies evaluated theoutcome of surgical repair of the upper vaginal prolapse (middle compartment),eleven studies the outcome of anterior vaginal wall repair and four studies theoutcome of posterior vaginal wall prolapse repair. The comparison of theclinical outcome of the various trials was hampered by heterogeneity inobjectives and study design e.g. the use of different surgical techniques, the useof mesh or not, definition of cure, the presence of incontinence after prolapsesurgery. Only in three trials the length of follow-up exceeded five years22.Therefore, even if the diagnosis is reliable and valid, it remains doubtful whichtherapy will be the most appropriate as several surgical approaches in theabsence of specific evidence may result in more or less equal therapeuticoutcome. Alternatively, it is also possible that one treatment is optimal fordifferent diagnoses or symptoms. Hence, on the one side of the diagnostic-therapeutic spectrum, there is one best therapy that specifically corresponds toone accurate diagnosis. At the other end, several treatment modalities areavailable for pelvic organ prolapse (complaints) for which the exact diagnosis isirrelevant. By this opacity, it is a rather complex task to optimise the diagnosticwork-up without knowing the short and long term outcome that may result fromthe treatment following the diagnostic work-up.
Standardization and validation of the diagnostic work-up is thereforeessential in order to realize a step forward in defining a scientifically baseddiagnostic work-up. Only then it is possible to validly measure the treatmentoutcome and allow comparative research into treatment modalities.
Rationale of this thesisPelvic organ prolapse is a prevalent disease, occasionally with a disappointingsurgical outcome and a high recurrence rate. Frequently, the accompanyingbladder and bowel disorders are not satisfactory resolved after therapeuticintervention. The cause of the disappointing therapeutic outcome may beunclear but inappropriate therapy due to insufficient diagnosis of the anatomyand function disorders may be one of the causes to be considered. Furthermore,mutual comparison of therapeutic interventions is hampered by the unstandar-dised method of diagnostic classification but also by the lack of consensus andoutcome assessment. Whether ancillary testing in the work-up of pelvic organ
25
General introduction and outline of the thesis
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 25

prolapse beyond a comprehensive medical history and physical pelvicexamination will improve treatment decisions is unclear. As currently noguidelines exist for the application of diagnostic tests, either alone orcombined, they are often arbitrarily initiated and the added value in theselection process of the optimal treatment is unclear.
Aim of the thesisThe aim of this thesis was to evaluate the diagnostic process leading to thediagnosis and treatment proposal in patients with primary pelvic organ prolapse. The following questions were addressed:
First, to what extent are bladder and bowel function disorders related tosite specific pelvic floor defects?Chapter 2 describes to what extent pelvic organ prolapse contributes to micturitionand defecatory symptoms. In 64 patients who visited the outpatient clinic forpelvic organ prolapse symptoms (study group) and 50 women who did not seekmedical care for these complaints (control group), we studied the relationshipbetween the presence of pelvic organ prolapse and the occurrence of pelvic floorsymptoms. All subjects were evaluated with validated questionnaires and POP-Qscores.
Second, how reliable is physical examination (clinical prolapse stagingsystems) in assessing the severity of POP? This aim is addressed in chapter 3. This chapter reports on the interobserveragreement of the halfway system of Baden and Walker (B&W) compared withthe interobserver agreement of the quantitative pelvic organ prolapse-quantification (POP-Q) system. The agreement between the Baden and Walkerand POP-Q systems is assessed in order to determine whether these twosystems are interchangeable.
Third, to what degree are various additional diagnostic tests useful in theclinical work-up of patients with primary pelvic organ prolapse? And inwhich cases does ancillary testing help in selecting treatment? This study aim is addressed in chapters 4, 5 and 6.
Chapter 4 reports a study on the pathophysiology of constipation and fecalincontinence in patients with primary pelvic organ prolapse, and the potentialrole of anorectal function testing and anal endosonography in the diagnosticwork-up of these patients.
26
Chapter 1
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 26

1Chapter 5 describes the diagnostic accuracy of clinical examination in detectingrectoceles and enteroceles, using defecography as (reference) standard.
Chapter 6 reports on the relative importance of four often initiateddiagnostic tests: magnetic resonance imaging, defecography, urodynamicexamination and anorectal function testing, including anal endosonography, foroptimal treatment selection in patients with primary pelvic organ prolapse.
Three expert-gynecologists individually as well as collectively duringexpert meetings defined the management plans of 53 patients before and afterfull results of the four tests were disclosed in addition to the results of historytaking and physical examination.
Chapter 7 contains the general discussion. The clinical relevance of thefour diagnostic tests evaluated in our study are discussed. Recommendationsfor the clinical work-up of patients with primary POP are presented.
Chapter 8 summarizes the results and conclusions presented in thepreceding chapters of this thesis.
Outline of the studyChapter 1 General Introduction and outline of the thesisChapter 2 The contribution of pelvic organ prolapse to micturition and
defecation symptomsChapter 3 Interobserver agreement and intersystem comparison of the
halfway system of Baden and Walker versus the Pelvic OrganProlapse-Quantitation prolapse classification system in assessingthe severity of pelvic organ prolapse
Chapter 4 Anorectal function testing and anal endosonography in the work-up of patients with primary pelvic organ prolapse
Chapter 5 Correlation between posterior vaginal wall defects assessed byclinical examination and by defecography
Chapter 6 Clinical-decision taking in primary pelvic organ prolapse; theeffect of diagnostic tests on treatment selection in comparisonwith a consensus meeting
Chapter 7 General discussionChapter 8 Summary and conclusions
27
General introduction and outline of the thesis
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 27

28
Chapter 1
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 28

1REFERENCES
1. Emge LA, Durfee RB. Pelvic Organ Prolapse: Four thousand years of treatment. Clin
Obstet Gynecol 1966;9:997-1032.
2. Shah SM, Sultan AH, Thakar R. The history and evolution of pessaries for pelvic organ
prolapse. Int Urogynecol J 2006;17:170-5.
3. Caspar Stromayr. Die Handschrift des Schnitt- und Augenartzes; Facsimile Berlin; Idra
Verlag 1925. Stromayer was chirurgijn, "ordinierte" rond 1550 in de Duitse stad Lindau.
4. Job Janszoon van Meekeren (ca 1611-1666); Heelmeester der Stad, Admiraliteit en 't
Gasthuis binnen Amsterdam; publiceerde in 1668 zijn Heel- en Geneeskonstige
Aenmerkingen.
5. Van Aubel A. Prolapsus Uteri et Vaginae. Thesis Amsterdam. Universiteits-
Vrouwenkliniek (Wilhelmina-Gasthuis) 1950.
6. Benson JT, Lucente V, McClellan E. Vaginal versus abdominal reconstructive surgery for
the treatment of pelvic support defects: a prospective randomized study with long-term
outcome evaluation. Am J Obstet Gynecol 1996:175:1418-21.
7. Gutman RE, Ford DE, Quiroz LH, Shippey SH, Handa VL. Is there a pelvic organ
prolapse threshold that predicts pelvic floor symptoms. Am J Obstet Gynecol 2008:199;
683.e1-7.
8. Hendrix SL, Clark A, Nygaard I, Aragaki A, Barnabei V, McTiernan A. Pelvic organ
prolapse in the Women´s Health Initiative: gravity and gravidity. Am J Obstet Gynecol
2002;86:1160-6.
9. Samuelsson EC, Victor FT, Tibblin G, Svärdsudd KF. Signs of genital prolapse in a
Swedish population of women 20-59 years of and possible related factors. Am J Obstet
Gynecol 1999;180:299-305.
10. Swift S, Woodman P, O’Boyle A, Kahn M, Valley M, Bland D, Wang W, Schaffer J.
Pelvic Organ Support Study (POSST): the distribution, clinical definition, and
epidemiologic condition of pelvic organ support defects. Am J Obstet Gynecol
2005;192:795-806.
11. Swift SE, Tate SB, Nicholas J. Correlation of symptoms with degree of pelvic organ
prolapse in a general population of women: what is pelvic organ prolaps? Am J Obstet
Gynecol 2003;189:372-7;discussion 377-9.
12. Nygaard I, Handa VL, Brubaker L, Borello-France D, Wei J, Wells E, Goode P; Pelvic
Floor Disorders Network. Changes in physical activity after abdominal sacrocolpopexy
for advanced pelvic organ prolapse. Am J Obstet Gynecol 2008;198:570.e1-5.
13. Jelovsek JE, Barber MD. Women seeking treatment for advanced pelvic organ prolapse
have decreased body image and quality of life. Am J Obstet Gynecol 2006;194:1455-61.
29
General introduction and outline of the thesis
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 29

14. Barber MD, Amundsen Cl, Paraiso MF, Weidner AC, Romero A, Walters MD. Quality of
life after surgery for genital prolapse in elderly women; obliterative and reconstructive
surgery. Int Urogynecol J 2007:18:799-806.
15. Van der Linden MW, Westert GP, De Bakker DH, Schellevis FG. Tweede Nationale
Studie naar ziekten in de huisartsen praktijk (NIVEL 2004, ISBN 9069056496)
www.nivel.nl/nationalestudie/
16. Bradley CS, Zimmerman MB, Qi Y, Nygaard IE. Natural history of pelvic organ prolapse
in postmenopausal women. Obstet Gynecol 2007:10:848-54.
17. Baessler K, O’Neill S, Battistutta D, Maher CF. Prevalence, incidence, progression and
regression and associated symptoms of pelvic organ prolapse. Int Urogynecol 2006;17
(Suppl.2):S70.
18. Handa VL, Garrett E, Hendrix S, Gold E, Robbins J. Progression and remission of pelvic
organ prolapse: a longitudinal study of menopausal women. Am J Obstet Gynecol
2004;190:27-32.
19. Landelijk Medische Registratie-informatie en verrichtingen (2006). www.prismant.nl/
informatie-expertise/thema’s/ziekenhuisstatistieken
20. Cruikshank SH, Kovac SR. Randomized comparison of three surgical methods used at
the time of vaginal hysterectomy to prevent posterior enterocele. Am J Obstet Gynecol
1999;180:859-65.
21. Miedel A, Tegerstedt G, Mörlin B, Hammarström M. A 5-year prospective follow-up
study of vaginal surgery for pelvic organ prolapse. Int Urogynecol J 2008;19:1593-601.
22. Maher C, Baessler K, Glazener CM, Adams EJ, Hagen S. Surgical management of pelvic
organ prolapse in women. Cochrane Database Syst Rev 2007;18:CD004014.
23. Bump RC, Norton PA. Epidemiology and natural history of pelvic floor dysfunction.
Obstet Gynecol Clin North Am 1998;25:723-46.
24. Weidner AC, Jamison, MG, Branham V, South MM, Borawski KM, Romero AA.
Neuropathic injury to the levator ani occurs in 1in 4 primiparous women. Am J Obster
Gynecol 2006;195;1851-6.
25. Lukacz ES, Lawrence JM, Contreras R, Nager CW, Luber KM. Parity, mode of delivery,
and pelvic floor disorders. Obstet Gynecol 2006;107:1253-60.
26. Crépin G, Cosson M, Lucot JP, Collinet P. Genital prolapse in young women: a topical
issue. Bull Acad Natl Med 2007;191:827-36.
27. Klutke J, Ji Q, Campeau J Starcher B, Felix JC, Stanczyk FZ, Klutke C. Decreased
endoplevic fascia elastin content in uterin prolapse. Acta Obstet Gynecol Scand 2008;
87:111-5.
28. Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically
managed pelvic organ prolapse and urinary incontinence. Obstet Gynecol
1997;89:501-6.
30
Chapter 1
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 30

129. Moalli PA, Jones Yvy S, Meyn LA, Zyczynski HM. Risk factors associated with pelvic
floor disorders in women undergoing surgical repair. Obstet Gynecol 2003;101:869-74.
30. Dietz HP. The aetiology of prolapse. Int Urogynecol 2008;19:1323-9.
31. Bonney V. The principles that should underlie all operations for prolapse. The Journal of
Obstetrics and Gynaecology of the British Empire 1934;41:669-83.
32. Lienemann A, Anthuber C, Baron A, Kohz P, Reiser M. Dynamic MRI
colpocystorectography assessing plevic floor descent. European Radiology
1997;7:1309-17.
33. Goei R, van Engelshoven J, Schouten H, Baeten C, Stassen C. Anorectal function:
defecografic measurements in asymptomatic subjects. Radiology 1989;173:137-41.
34. Dietz HP. Why pelvic floor surgeons should use ultrasound imaging. Ultrasound Obstet
Gynecol 2006;28:629-34.
35. Petros PE. Chapter 1: Overview. In: Petros PE. The female pelvic floor function,
dysfunction and management according to the integral theory. 2nd edition. Springer,
Berlin.Heidelberg.New York; 2006:1-12. ISBN 978-3-540-33663-1.
36. Nichols DH, Randall CL. Chapter 1: Pelvic anatomy of the living. In: Nichols DH,
Randall CL. Vaginal surgery. 3rd edition: Williams&Wilkins, Baltimore.Hong
Kong.London.Sydney;1989:1-46. ISBN 0-683-06494-0.
37. Berglas B, Rubin IC. Study of the supportive structures of the uterus by levator
myography. Surg Gynecol Obstet 1953;97;677-92.
38. Petros PE, Ulmsten U. Urethral pressure increase on effort originates from within the
urethra, and continence from musculovaginal closure. Neurourol Urodyn
1995;14:337-46; discussion 346-50.
39. DeLancy JO. The structural support of the urethra as it relates to stress incontinence: the
hammock hypothesis. Am J Obstet Gynecol 1994:170:1713-23.
40. Blaivas JG. Pathophysiology of lower urinary tract dysfunction. Clinics in Obstetrics and
Gynecology 1985;12:285-309.
41. Basu M, Duckett J. Effect of prolapse repair and the relationship to overactive bladder
and detrusor activity. Int Urogynecol Int Urogynecol 2009;4:25-30.42.
42. Petros PE, Ulmsten U. Bladder instability in women: A premature activation of the
micturition reflex. Neurourol Urodyn 1993;12:235-9.
43. Cherry DA, Rothenberger DA. Pelvic floor physiology. Surg Clin North Am
1988;68:1217-30.
44. Phillips SF, Edwards DA. Some aspects of anal continence and defaecation. Gut
1965;6:396-406.
45. Madoff RD, Parker SC, Varma MG, Lowry AC. Fecal incontinence in adults. Lancet
2004;364:621-32.
46. Rao SS. Pathophysiology of adult fecal incontinence. Gastroenterology 2004;126;S13-
14.
31
General introduction and outline of the thesis
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 31

47. Sangwan YP, Solla JA. Internal anal sphincter: advances and insight. Dis Colon Rectum
1998;42:1297-311.
48. Parks AG. Anorectal incontinence. Proceedings of the Royal Society of Medicine
1975;68:681-90.
49. Andromanakos N, Troupis T, Filippou D. Constipation of anorectal outlet obstruction. J
Gastroenterol Hepatol 2006;21:638-46.
50. Maxwell PR, Heriot AG, Davies DC, Kumar D. Anorectal sensation and continence
Scand J Gastroenterol 1999;34:113-6.
51. Read NW, Haynes WG, Bartolo DC, Hall J, Read MG, Donnelly TC, Johnson AG. Use
of anorectal manometry during rectal infusion of saline to investigate sphincter function
in incontinence patients. Gastroenterology 1983;85:105-13.
52. Jones PN, Lubowski DZ, Swash M, Henry MM. Relation between perineal descent and
pundendal nerve damage in idiopathic faecal incontinence. Int J Colorecal Dis
1987;2:93-5.
53. Snooks SJ, Swash M Setchell M, Henry MM. Injury of pelvic floor sphincter
musculature in childbirth. Lancet 1984;8:546-50.
54. Terra MP, Deutekom M, Beets-Tan RG. Engel AF, Janssen LW, Boeckxstaens GE,
Dobben AC, Baeten CG, de Priester JA, Bossuyt PM, Stoker J. Relationship between
external anal sphincter atrophy at endoanal MR imaging and clinical, functional, and
anatomic characteristics in patients with faecal incontinence. Dis Colon Rectum
2006;49:668-78.
55. Strohbehn K. Normal pelvic floor anatomy. Obstet Gynecol Clin North Am
1998;25;683-705.
56. Mouritsen L. Classification and evaluation of prolapse. Best Pract Res Clin Obstet
Gynecol 2005;19:859-911.
57. Whiteside JL, Weber AM, Meyn LA, Walters MD. Risk factors for prolapse recurrence
after vaginal repair. Am J Obstet Gynecol 2004;191:1533-8.
58. Daneshgari F, Moore C, Frinjari H, Babineau D. Patient related risk factors for recurrent
stress urinary incontinence surgery in women treated at a tertiary care center. J Urol
2006;176:1493-9.
59. Boer TA, Gietelink DA, Vierhout ME. Discrepancies between physician interview and a
patients self-assessment questionnaire after surgery for pelvic organ prolapse. Int
Urogynecol J 2008;19:1349-52.
60. Srikrishna S, Robinson D, Cardozo L, Gonzalez J. Is there a difference in patient and
physician quality of life evaluation of pelvic organ prolapse? Int Urogyencol J
2008;19:517-20.
61. Rodríguez LV, Blander DS, Dorey F, Raz S, Zimmern P. Discrepancy in patient and
physician perception of patient’s quality of life related to urinary symptoms. Urology
2003;62:49-53.
32
Chapter 1
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 32

162. Baden WF, Walker TA. Genesis of the vaginal profile: a correlated classification of
vaginal relaxation. Clin Obstet Gynecol 1972;15:1048-54.
63. Bump RC, Mattiasson A, Bø K, Brubaker LP, DeLancey JO, Klarskov P, Shull BL, Smith
AR. The standardization of terminology of female pelvic organ prolapse and pelvic floor
dysfunction. Am J Obstet and Gynecol 1996;175:10-7.
64. Theofrastous JP, Swift SE. The clinical evaluation of pelvic floor dysfunction. Obstet
Gynecol Clin North Am 1998;25;783-804.
65. Auwad W, Freeman RM, Swift S. Is the pelvic organ prolapse quantification system
(POPQ) being used? A survey of the members of the International Continence Society
(ICS) and the American Urogynecologic Society (AUGS). Int Urogynecol J
2004;15:324-7.
66. Kobak WH, Rosenberger K, Walters MD. Interobserver variation in the assessment of
pelvic organ prolapse. Int Urogynecol J 1996;7:121-24.
67. Royal College of Obstetricians and Gynaecologists (RCOG). Surgical treatment of
urodynamic stress incontinence. London (UK): Royal College of Obstetricians and
Gynaecologists (RCOG), 2003 Oct 9 (Guideline; no. 35).
68. Royal College of Obstetricians and Gynaecologists (RCOG) and British Society of
Urogynaecolgy (BSUG).The management of post hysterectomy vaginal vault prolapse.
2007 Oct (Green-top guideline; no. 46).
69. ACOG technical bulletin. Pelvic organ prolapse. American College of Obstetricians
and Gynecologists. Int J Gynaecol Obstet 1996;52:197-205.
70. ACOG Practice Bulletin no 79: Pelvic Organ Prolapse. Committee on Practice
Bulletins-Gynecology, American College of Obstetricians and Gynecologists. Obstet
Gynecol 2007;109:461-73. Withdrawal from literature.
71. Murphy M; Society of Gynecologic Surgeons Systematic Review Group. Clinical
practice guidelines on vaginal graft use from the society of gynecologic surgeons.
Obstet Gynecol 2008;112:1123-30.
72. Groenendijk AG, Vervest HAM, Van der Vaart CH, Van Geelen JM. NVOG richtlijn
urine-incontinentie. September 2004.
73. Ghoniem G, Stanford E, Kenton K, Achtari C, Goldberg R, Mascarenhas T, Parekh M,
Tamussino K, Tosson S, Lose G, Petri E. Evaluation and outcome measures in the
treatment of female urinary stress incontinence: International Urogynecological
Assocation (IUGA) guidelines for research and clinical practice. Int Urogynecol J
2008;19:5-33.
74. Brubaker L, Norton P. Current clinical nomenclature for description of pelvic organ
prolapse. J Pelvic Med Surg 1996;2:257-9.
75. Robinson D Anders K, Cardozo L. Outcome measures in urogynaecology: the
clinician’s perspective. Int Urogynecol J 2007:18:273-9.
33
General introduction and outline of the thesis
Proefschrift Groenendijk_proefschrift 19-10-09 10:35 Pagina 33