vaccination with irradiated autologous tumor cells mixed ... · (ctla-4) and the pdl/pd-l1 pathway...
TRANSCRIPT

Cancer Therapy: Clinical
Vaccination with Irradiated Autologous TumorCells Mixed with Irradiated GM-K562 CellsStimulatesAntitumor ImmunityandTLymphocyteActivation in Patients with Recurrent MalignantGliomaWilliam T. Curry, Jr1,2,3, Ramana Gorrepati1, Matthias Piesche4,9, Tetsuro Sasada5,Pankaj Agarwalla1, Pamela S. Jones1, Elizabeth R. Gerstner2,3, Alexandra J. Golby3,6,Tracy T. Batchelor2,3, Patrick Y.Wen3,7, Martin C. Mihm3,8, and Glenn Dranoff3,4,5
Abstract
Purpose: Recurrent malignant glioma carries a dismal prog-nosis, andnovel therapies are needed.We examined the feasibilityand safety of vaccination with irradiated autologous glioma cellsmixed with irradiated GM-K562 cells in patients undergoingcraniotomy for recurrent malignant glioma.
Experimental Design: We initiated a phase I study examiningthe safety of 2 doses of GM-K562 cells mixed with autologouscells. Primary endpointswere feasibility and safety. Feasibilitywasdefined as the ability for 60% of enrolled subjects to initiatevaccination. Dose-limiting toxicity was assessed via a 3þ3 dose-escalation format, examining irradiated tumor cells mixed with 5� 106 GM-K562 cells or 1 � 107 GM-K562 cells. Eligibilityrequired a priori indication for resection of a recurrent high-gradeglioma. We measured biological activity by measuring delayedtype hypersensitivity (DTH) responses, humoral immunityagainst tumor-associated antigens, and T-lymphocyte activation.
Results: Eleven patients were enrolled. Sufficient numbersof autologous tumor cells were harvested in 10 patients,all of whom went on to receive vaccine. There were nodose-limiting toxicities. Vaccination strengthened DTHresponses to irradiated autologous tumor cells in mostpatients, and vigorous humoral responses to tumor-associ-ated angiogenic cytokines were seen as well. T-lymphocyteactivation was seen with significantly increased expressionof CTLA-4, PD-1, 4-1BB, and OX40 by CD4þ cells and PD-1and 4-1BB by CD8þ cells. Activation was coupled withvaccine-associated increase in the frequency of regulatoryCD4þ T lymphocytes.
Conclusions: Vaccination with irradiated autologous tumorcells mixed with GM-K562 cells is feasible, well tolerated, andactive in patients with recurrent malignant glioma. Clin CancerRes; 22(12); 2885–96. �2016 AACR.
IntroductionRecent clinical research has demonstrated that some patients
with advanced malignancies have clinical and radiographicresponses to immune checkpoint inhibition with monoclonalantibody-based blockade of cytotoxic T-lymphocyte antigen—4
(CTLA-4; ref. 1) and the programmed cell death protein 1 (PD1;ref. 2) and its ligand (PD-L1; ref. 3). These clinically impactfulimmunotherapies come on the heels of Food and Drug Admin-istration approval of Sipleucel T, an autologous cellular vaccinethat prolongs survival for patients with advanced castration-resistant prostate cancer (4).
Vaccination with irradiated autologous tumor cells engi-neered to express granulocyte-macrophage colony stimulatingfactor (GM-CSF)—a strategy referred to as "GVAX"—has stim-ulated vigorous antitumor immunity in subjects with varioussolid and hematologic malignancies and has prolonged sur-vival in selected patients (5). Vaccination using whole tumorcells drives a polyclonal immune attack against multiple tumor-associated antigens and both reinforces existing humoraland cell-mediated immunity to antigenic epitopes and stimu-lates new responses to previously undetected tumor-associatedantigens.
Glioblastoma is an intracranial malignancy with medianoverall survival between 14 and 17 months, despite surgery,radiation, and chemotherapy (6, 7). A dire need exists foreffective treatments for patients with glioblastoma. Many clin-ical trials of targeted agents and angiogenesis inhibitors havefailed to show efficacy (8). Bevacizumab is the only FDA-approved drug for patients with recurrent glioblastoma, on the
1Department of Neurosurgery, Massachusetts General Hospital, Bos-ton, Massachusetts. 2Cancer Center, Massachusetts General Hospital,Boston, Massachusetts. 3Harvard Medical School, Boston, Massachu-setts. 4Department ofMedicine, Dana Farber Cancer Institute, Boston,Massachusetts. 5Cancer VaccineCenter, Dana Farber Cancer Institute,Boston, Massachusetts. 6Department of Neurosurgery, Brigham andWomen's Hospital, Boston, Massachusetts. 7Division of Neuro-oncol-ogy, Dana Farber Cancer Institute, Boston, Massachusetts. 8Depart-ment of Pathology, Brigham and Women's Hospital, Boston, Massa-chusetts. 9Department of Biomedicine, Aarhus University, Aarhus,Denmark.
Note: Supplementary data for this article are available at Clinical CancerResearch Online (http://clincancerres.aacrjournals.org/).
Corresponding Author: William T. Curry, Jr., Massachusetts General HospitalCancer Center, 55 Fruit Street, Y9E, Boston, MA 02114. Phone: 617 726 3779; Fax:617 726 3665; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-15-2163
�2016 American Association for Cancer Research.
ClinicalCancerResearch
www.aacrjournals.org 2885
on May 9, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2016; DOI: 10.1158/1078-0432.CCR-15-2163

basis of phase II clinical trials showing overall survival of 40weeks (9).
Despite the blood–brain barrier, brain tumors interact with theimmune system and provoke nascent antitumor immuneresponses. Pallasch has identified antibodies to tumor antigensin the sera of glioblastoma patients and has correlated the pres-ence of a subset of these with prolonged survival (10). Similarly,glioblastoma immunogenicity has been demonstrated by theidentification of circulating tumor-specific CD8þ T lymphocytesamong the peripheral bloodmononuclear cells (PBMC) of tumorpatients. The intratumoral ratio of effector T lymphocytes toregulatory T lymphocytes may independently affect survival inglioblastoma patients (11).
Preclinical evidence shows that vaccination can enhance anti-glioma immunity and can be effective in intracranial gliomamodels. In separate reports, Sampson andHerrlinger demonstrat-ed that subcutaneous vaccinationwith irradiated syngeneic tumorcells expressing cytokines improves survival in mice-bearingintracranial tumors. Although animals in these studies experi-enced enhanced survival, the treatments did not cure establishedtumors. However, vaccination in combination with immunecheckpoint blockade has been highly efficacious preclinically(12, 13) and shows promise in early clinical trials (14, 15) inpatients with solid tumors. Moving forwards with these combi-nation clinical studies, including for patients with glioma, is areasonable next step for the field.
The GVAX approach has not been reported in patients withmalignant brain tumors. Therefore, before proceeding with com-bination immunotherapy in these patients, we sought to dem-onstrate the feasibility and safety of vaccinating patients withrecurrent malignant glioma with irradiated autologous tumorcells in the context of local GM-CSF expression. The risk ofinducing autoimmune encephalitis via autologous whole gliomacell vaccination is a legitimate safety concern. Also, previousefforts at using autologous glioma cell vaccination in this pop-ulation have shown low feasibility because of tumor progressionduring vaccine preparation and the challenges inherent to main-taining glioma cells in culture (16).
We mixed irradiated autologous glioma cells with varyingnumbers of irradiated GM-K562 cells. GM-K562 has beendescribed previously as a GM-CSF producing bystander cell linefor use in the formulation of autologous tumor cell-based vac-cines (17). The use of a bystander cell line with low immunoge-nicity allows for in vivo expression of a defined and controllableamount of GM-CSF and permits the design of a true dose-esca-lation phase I study.
We confirm the feasibility and safety of vaccinating recurrentglioma patients with irradiated autologous tumor cells mixedwith up to 1 � 107 GM-K562 cells. Vaccination engenderedan active systemic immune response, as we documentenhanced tumor-specific immunity and generalized T-lympho-cyte activation.
Materials and MethodsThe clinical trial protocol was approved by the Institutional
Review Board of the Dana Farber-Harvard Cancer Center, and isregistered on ClinicalTrials.gov (NCT00694330).
PatientsPatients included adults undergoing elective craniotomy in the
setting of recurrent malignant glioma. Full inclusion/exclusioncriteria are listed in the supplementary materials.
GM-K562 cellsThe GM-K562 cell line was created at the Harvard Gene Vector
Laboratory by stably transfecting K562 cells with a plasmidencoding GM-CSF and a puromycin resistance gene. K562 isderived from chronic myelogenous leukemia cells in blast crisis,does not express MHC I and MHC II molecules, and is poorlyimmunogenic (17, 18). After 100 gray irradiation, GM-K562 cellsexpress 9 to 13 mg of GM-CSF/1 � 106 cells/24 hours.
Clinical trial designThis phase I trial was designed in a "3þ3" format for exami-
nation of the safety of administering up to 1� 107 GM-K562 cellsmixed with irradiated autologous glioma cells. The first dosecohort was treated with 5 � 106 GM-K562 cells per vaccination.The second cohort (1 � 107 GM-K562 cells) was expanded inorder to treat a total of 10 patients in the study. The number ofautologous glioma cells planned per vaccination was a factor ofhowmany were harvested at craniotomy. Vaccines were deliveredweekly for 3 weeks, then biweekly, up to a total of 6 vaccinations.Feasibility was defined as the ability to treat �60% of enrolledpatients with at least 4 vaccinations.
Vaccine preparationAutologous tumors were processed into single cell suspension
under GMP conditions using collagenase. Cells were aliquotedand cryopreserved at equal number into vials for 6 vaccines,ranging from 1 � 105 cells to 6 � 107 cells. If additional cellswere available, two vials of 1�106 cellswere set aside for delayed-type hypersensitivity (DTH) testing.
At time of vaccination, 1 vial of GM-K562 and 1 vial ofautologous tumor cells were thawed and extensively washed insaline. Quality control samples were collected for gram stain andsterility evaluation. According to protocol dose, the appropriatenumber of GM-K562 cells was mixed with the autologous tumorcells, and lethally irradiated at 100 Gray. The vaccine was then
Translational Relevance
Immune checkpoint inhibition withmonoclonal antibody-based blockade of cytotoxic T lymphocyte-associated antigen(CTLA-4) and the PDl/PD-L1 pathway have lead the clinicaltranslation of cancer immunotherapy. These therapies arelikely most active in subjects with preexisting immune recog-nition of tumor-associated antigens. Vaccination may be aneffective way to expand the repertoire of recognizable tumor-associated antigens and has been shown in preclinical studiesto be synergistic in combination with checkpoint blockade.We have demonstrated that, in patients with recurrent malig-nant glioma, vaccination with irradiated autologous tumorcells mixed with irradiated GM-K562 cells—a variation of the"GVAX" strategy—drives T lymphocyte activation and stimu-lates tumor-specific immune responses, perhaps setting thestage for combination immunotherapy with checkpoint inhi-bitors and/or with agents that negate the impact of regulatoryT cells.
Curry et al.
Clin Cancer Res; 22(12) June 15, 2016 Clinical Cancer Research2886
on May 9, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2016; DOI: 10.1158/1078-0432.CCR-15-2163

delivered to the patient via mixed subcutaneous and intradermalinjection.
DTH samples were thawed at time of the first and fourthadministration of vaccine, washed extensively in saline, thenlethally irradiated at 100 Gray. DTH samples were injected intra-dermally on the shoulders of consenting subjects.
ImmunophenotypingImmune cell phenotypes in blood were monitored by 5-color
flow cytometry. Freshly drawn samples were lysed and stainedusing monoclonal antibodies specific for T-cell costimulatorymolecules or regulatory T (Treg) cells. The combination of anti-bodies is listed in the supplementary data. The samples were runon a flow cytometer (FC500 MPL, Beckman Coulter), and datawere analyzed using the CXP (Beckman Coulter) software.
ELISA for anticytokine antibodiesDetails of the ELISA for angiogenic cytokines are as previously
described (19), and are also detailed in the supplementarymaterials.
BiostatisticsSurvival analysis was performed by the Kaplan–Meier method.
Change in expression of costimulatory molecules andmarkers onlymphocytes was analyzed by the nonparametric sign-rank test,accounting for small sample size and improbability of normalityassumption. P-values �0.05 were considered statisticallysignificant.
ResultsFeasibility
Feasibility was dependent upon the successful harvest andcryopreservation of a sufficient number of viable autologoustumor cells to generate vaccine for 6 injections. The lowestallowable number of tumor cells per vaccination was 1 � 105,equal to the lowest number of GM-CSF expressing autologoustumor cells associated with biological activity in clinical trialspreviously conducted at our center. The maximum number ofautologous tumor cells per vaccination was set at 6� 107, equalto the highest number of GM-CSF expressing tumor cells thathad been delivered in the aforementioned studies. Patients hadto maintain KPS �70% until the time of the initial treatment inorder to remain study-eligible. Eleven patients total wereenrolled and underwent craniotomy (Table 1). Median agewas 42 years (range 31–78). Sufficient cells were obtained andprepared in 10 of the 11 patients (Table 2). In a single subject(patient 7), pathology was consistent with treatment effect.Three patients were enrolled into the first dose cohort (patients1–3, 5 � 106 GM-K562 cells per vaccination) and 8 patientsinto the second (patients 4–11, 1 � 107 GM-K562 cells pervaccination).
All subjects maintained a KPS of at least 70% after surgery anduntil the time of the first vaccination. Treatment was initiated at amedian of 19.5 days (16–30 days) after craniotomy. All 10 treatedpatients received at least four vaccinations. Patients 1, 2, and 3received six, five, and four vaccinations, respectively. Patients 2and 3 were not treated with the full complement of six injectionsbecause of radiographic progression of disease and subsequentinitiation of bevacizumab. Vaccination of patients undergoingcraniotomy for recurrent malignant glioma with a mixture of
irradiated autologous tumor cells andGM-K562 cells was deemedfeasible by preset criteria.
SafetyAll subjects were followed closely for complications associated
with vaccine, including adverse neurological effects and autoim-munity. Toxicities were assessed by the National Cancer InstituteCommon Toxicity Criteria, version 3.0. Grades 1 and 2 skinreactions were observed at the vaccination sites in all patients,and all resolved spontaneously. There were no grade 3 or 4toxicities.
The first three patients were treatedwith 5� 106 irradiatedGM-K562 cells (50 mg GM-CSF/24 hours) mixed with irradiatedautologous tumor cells. There were no dose-limiting toxicities ofvaccination in this cohort.
The remaining seven patients were treated with 1 � 107 irra-diated GM-K562 cells (100 mg GM-CSF/24 hours) mixed withirradiated autologous glioma cells. Five of seven treated subjectsreceived six vaccinations. Two of seven were treated with fivevaccinations; in both cases, the sixth treatment was held becauseof concern for progressive disease and initiation of new therapy.There were no dose-limiting toxicities in patients treated atdose-level 2 of GM-K562 cells (1 � 107 cells).
Patient 5 was evaluated for a low-grade fever and a headache 1day after initial vaccination. The elevated temperature persistedfor 2 days.Work-up included a lumbar puncture, which revealed amildly elevated protein (124 mg/dL) and 50 white blood cells(58% polymorphonuclear cells, 27% lymphocytes), possiblyconsistent with aseptic meningitis. The patient defervesced, andthe second vaccination was delayed by 1 week. Repeat adminis-tration of vaccine went forwards without recurrence of fever orheadache. This episode was categorized as an adverse eventpossibly related to treatment, CTC grade 2.
After the fourth vaccination, patient 4 complained of head-ache and left hemiparesis. Brain MRI showed significantincreases in nodular gadolinium enhancement around the rightfrontal resection cavity and downward mass effect on the lateralventricles (Fig. 3B). Dexamethasone at 4 mg daily was initiatedwith resolution of symptoms, and vaccination continued onschedule. MRI 3 weeks later (week 7 after initiation of therapy)showed reduction in both enhancement and mass effect. Giventhe presence of central nervous system symptoms that requiredintervention with oral corticosteroids, this episode is catego-rized as an adverse event possibly related to therapy, CTCgrade 3.
Toxicity analysis demonstrated that vaccinating patients withsubcutaneous and intradermal injections of irradiated autologousglioma cells mixed with up to 1� 107 irradiated GM-K562 cells issafe in patients who have undergone craniotomy for recurrentmalignant glioma.
Tumor-associated immunityDelayed-type hypersensitivity. All patients were evaluated for clin-ical evidence (rash) of vaccination site and DTH reactionsbetween 48 and 72 hours after the first and fourth injections.Consenting patients underwent punch skin biopsies of bothvaccination sites and DTH sites, also 48 to 72 hours after the firstand fourth treatments.
Hematoxylin and eosin–stained specimens were evaluated bya senior dermatopathologist who was blinded to patient
GVAX for Recurrent Malignant Glioma
www.aacrjournals.org Clin Cancer Res; 22(12) June 15, 2016 2887
on May 9, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2016; DOI: 10.1158/1078-0432.CCR-15-2163

identification, the dose level, and the timing of the biopsy. Theintensity of the inflammatory infiltrates was assessed qualitativelyand semiquantitatively by assignation of a score of 1 to 4 (þ,þþ,þþþ, þþþþ), with 4 representing the highest degree of inflam-mation (Details of scoring presented in supplementary data).Results are summarized in Table 3.
There was a strong trend toward enhanced histopathologicallydetectable inflammation at the time of the fourth vaccination ascompared to the biopsy sites at the time of the first treatment. Thiswas true at the vaccination sites themselves, but was particularlymarked at the biopsied DTH sites. At the time of the first vacci-nation, there was essentially no inflammatory response to intra-dermal injection of irradiated autologous tumor cells into theshoulder contralateral to the vaccination site. Forty-eight to sev-enty-two hours after the fourth vaccination, however, clearincreases in the intensity of inflammatory cell infiltrates wereobserved in the DTH punch biopsy specimens of all patientsexcept for patient 9.
Histology examination of DTH sites suggested that by the timeof the fourth treatment, vaccination with irradiated autologousglioma cells mixed with irradiated GM-K562 cells has augmenteda systemic immune response against the patients' tumor cells.
Humoral antitumor immunity. To address the lack of antigen-specific immune monitoring associated with our whole cellapproach, we extended findings from our group that cancerpatients treated with GVAX alone (19) or in combination withCTLA-4 blockade (20) generate antibodies against multiple cyto-kines associated with tumor angiogenesis, including angiopoie-tins 1 and 2, as well as vascular endothelial growth factor (VEGF).
We established an ELISA panel of angiogenic cytokines andpeptides and analyzed reactivity with patient plasma. We studiedplasma reactivity to L1-CAM, DEL-1, Angiopoietin 1 (Ang 1),Angiopoietin 2 (Ang 2), hepatocyte growth factor (HGF), plateletderived growth factor (PDGF-BB), progranulin (PGLN), andvascular endothelial growth factor, as our prior work indicatedthat each may be the target of vaccine-induced antibodies. Peakchanges in plasma reactivity to these cytokines, measured byoptical density (OD), are shown in Table 4.
Vaccination increased antibody responses most consistentlyand significantly to Ang 1 (four/nine patients), Ang 2 (seven/ninepatients),HGF (six/nine patients), andPDGF (five/nine patients).Changes above baseline were compared to background levels inthe assay, and ranged from a minimum of 2.5-fold elevations tomore than eight-fold increases. Increases in response were mostvigorous for Ang 2. Reactivity tended to peak towards the end ofthe vaccination course or after it was complete (Fig. 1). In patients3, 4, and 5, peak responses to Ang 2 were most intense aftercommencement of treatmentwithbevacizumab,which startedonweeks 6, 10, and 10, respectively, possibly reflecting an immu-nostimulatory effect of VEGF-A blockade, consistent with priorstudies of combined bevacizumab and ipilimumab in advancedmelanoma patients (21).
T-lymphocyte activationFlow cytometry of leukocyte subsets reveals post-vaccination T lym-phocyte activation. We sought to identify trends in vaccination-associated leukocyte activation by performing flow cytometry ofwhite blood cell subsets, using freshly collected whole blood. Thefull flow cytometry panel is shown in the supplementary data.
Table 1. Clinical characteristics at enrollment for "bystander GVAX" subjects
Patient Age SexInitial
diagnosis KPSTime since initialdiagnosis (m) Recurrence
Pre-opsteroids (Y/N?)
1 32 M GBM 90 12 1st Y2 74 M GBM 70 9 1st Y3 31 M AA 100 91 1st N4 39 M GBM 90 43 3rd N5 63 M GBM 100 10 1st N6 42 F GBM 100 29 3rd N7 AOA8 51 M GBM 100 11 1st N9 32 M GBM 80 29 3rd N10 38 M GBM 90 18 2nd Y11 78 M GBM 80 17 1st N
Abbreviations: AA, anaplastic astrocytoma; AOA, anaplastic oligoastrocytoma; GBM, glioblastoma; RT, radiation therapy; SRS, stereotactic radiosurgery; TMZ,temozolomide.
Table 2. Pathology and therapy for "bystander GVAX" subjects undergoing craniotomy for resection of recurrent malignant glioma
PatientExtent ofresection Pathology
Viable tumorcells
Tumor cells/vaccination
Vaccinationsreceived
Initial post-vaccinationtherapy
1 Subtotal Glioblastoma 7.9 � 107 1.2 � 107 6 Bev/CPT-112 Subtotal Glioblastoma 1.9 � 108 1.6 � 107 5 Bev/CPT-113 Subtotal Glioblastoma 2.0 � 108 3.0 � 107 4 Bev4 Near total Glioblastoma 1.6 � 108 2.5 � 107 6 Bev5 Near total Glioblastoma 3.0 � 107 4.2 � 106 5 Bev/CPT-116 Near total Glioblastoma 9.4 � 107 1.4 � 107 6 Ang10057 Gross total Radiation Necrosis N/A N/A 08 Gross Total Glioblastoma 2.5 � 108 8.2 � 105 6 None9 Gross Total Glioblastoma 5.8 � 106 3.7 � 107 6 Unknown10 Near total Glioblastoma 2.5 � 109 3.4 � 107 5 Sirolimus and
Vandetanib11 Gross Total Glioblastoma 3.4 � 107 4.80 � 106 6 Bev
Abbreviation: N/A, not applicable.
Curry et al.
Clin Cancer Res; 22(12) June 15, 2016 Clinical Cancer Research2888
on May 9, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2016; DOI: 10.1158/1078-0432.CCR-15-2163

Expression levels for each marker were followed over time. Wecalculated the maximum percentage change as compared to thelevels measured from blood collected at the time of the initialvaccination, as not all subjects hadwhole bloodprocessed prior totreatment. We limited our analysis to blood that was collectedwithin the first 12 weeks after vaccination, in order to avoidconfounding of data by the impact of additional therapies.
For many of the cellular subsets, there were no distinguishablepatterns of change, including in natural killer (NK) cells, NKTcells, and dendritic cell subsets. However, with regard to systemicCD4þ and CD8þ T lymphocyte activation, several trends, some ofwhich were statistically significant and temporally related tovaccine initiation, emerged.
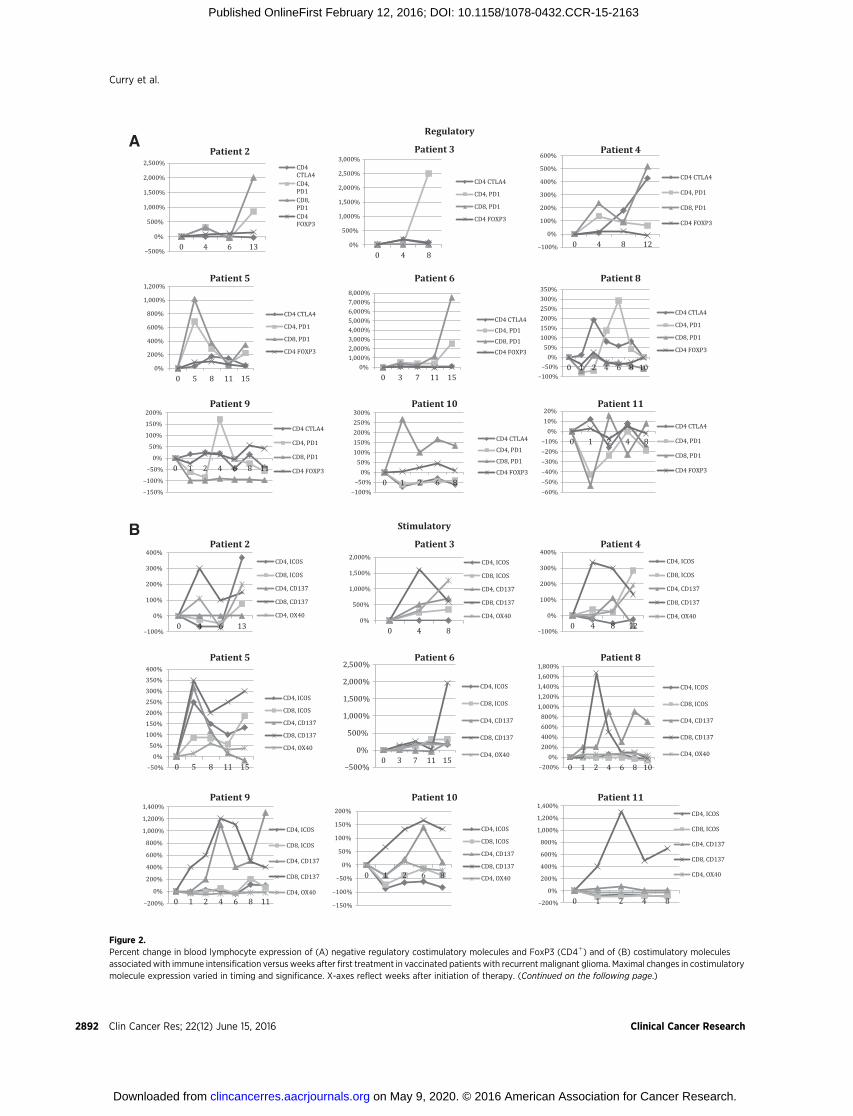
We identified changes in the expression of "activating" and"regulatory" costimulatory molecules by both CD4þ and CD8þ Tlymphocytes. Upregulation of these molecules is an indication ofinitial T-cell activation, and their ligation may be associated withfurther expansion of lymphocyte proliferation and memory dif-ferentiation ("activating") or fatigue and downregulation of anti-gen specific immune responses ("regulatory").
Sufficient blood for flow cytometry analysis was collected insubjects 2, 3, 4, 5, 6, 8, 9, 10, and 11. We measured lymphocyteexpression of ICOS, CD137, and OX40 (activating); also, asregulatory costimulatory molecules, we examined T-lymphocyteexpression of CTLA4 (CD4þ lymphocytes) and PD1, as well asFoxP3 expression on CD4þ cells. Expression of FoxP3 on CD4þ
lymphocytes serves as an identifier of the suppressive regulatory Tcell (Treg) subset, though it alsomay be present on some activatedconventional T cells.
CTLA-4 expression on CD4þ lymphocytes clearly increasedrelative to levels at the beginning of vaccination, typically withinthe first 10 weeks after the initial vaccination. Peak expression ofCTLA-4 for one patient (Patient 4), occurred at the 12thweek, andthe relative increase was particularly high (>5�). There was a clear
trend for increasedCTLA-4 expressiononCD4þ lymphocytes overthe course of the vaccination period, with the peak occurring after7 to 8 weeks, typically followed by subsequent decline.
Similarly, in 9 of 11patients, CD4þT-lymphocyte expression ofPD1 generally increased over time after vaccination. Althoughmost patients demonstrated peak PD1 expression by CD4þ Tlymphocytes between 4 and 6 weeks with a subsequent decline,three patients had marked elevations in PD1 expression (9.5�,26�, and 26.2�) in a delayed fashion (12, 12, and 15 weeks afterinitiation of vaccination).
The percentage of CD4þFoxP3þ T lymphocytes frequentlyincreased after the start of treatment, oftenpeaking, thendeclining(e.g., patients 3, 4, 5, 6, 8, and 10).
Activating costimulatory molecules were upregulated in theirexpression on CD4þ and CD8þ lymphocytes after vaccinationas well. Baseline levels of T-lymphocyte expression of CD137(4-1BB) were low in these patients. However, both CD4þ andCD8þ T lymphocytes more frequently expressed CD137 post-vaccination than at the outset. OX40 expression on CD4þ Tlymphocytes was also driven upward.
We quantified and depicted the change in CD4 lymphocyteexpression for Foxp3 and the above T-lymphocyte costimulatorymolecules (Fig. 2). Statistically significant changes were identifiedfor CD4CTLA4, CD4PD1, CD4FoxP3, CD4CD137, CD8CD137,and CD4OX40. The change in expression of PD1 on CD8þ Tlymphocytes trended upward, but did not achieve statisticalsignificance because of wide variation (Supplementary Data).
CD4þCD25þCD127� regulatory T lymphocytes. Although FoxP3expression is commonly used to define CD4þ regulatory T cells, itis also transiently expressed as an activation marker on conven-tional CD4þ T cells. The CD4þCD25þCD127� subset correlatestightly with FoxP3-expressing regulatory T lymphocytes and canbe used as an alternative marker. By 4 weeks after initiation of
Table 3. Semiquantitative assessment of inflammatory responses at punch biopsy sites
Patient GVAX 1 GVAX 4 DTH 1 DTH 4
1 ND þ Negative þþþ2 þþþ þþþ Trace þþ, Eos4 ND þþþ ND þþþ5 Focal þþ, Eos ND Trace ND6 þþ þþþþ Negative þþ9 Trace þ Negative Negative11 þþ þþþþ, eos þ þþþ, Eos, and
neutrophils
NOTE: GVAX 1,4, vaccination site biopsies 48 to 72 hours after first and fourth treatments, respectively; DTH 1,4, DTH-site biopsies 48 to 72 hours after first and fourthtreatments, respectively.Abbreviations: ND, not done; eos, eosinophils.
Table 4. Semiquantitative analysis of antibody response to angiogenic cytokines in vaccinated patients with recurrent malignant glioma
Patient number L1 DEL-1 Ang1 Ang2 HGF PDGF VEGF-Aa VEGF-A PGRN
2 þ þ þþþ3 þ þþþ þ þ þþþ þ4 þþ þþþ þþþ þ þ þþþ5 þþ þþþ þþþ þ þþþ þþþ þþþ6 þþþ þ þ8 þ þ þ þ9 þþþ þ10 þ þþþ þþ þþþ11 þþ þþþ þ þ þ þNOTE: þ, two and one half to five-fold increases; þþ five- to six-fold increases; þþþ, eight- and greater fold increases.Patients 2, 3, 4, 5, and 11 received bevacizumab at weeks 7, 6, 10, 10, and 10, respectively.aVEGF-A before bevacizumab. Patients 2 to 5 had blood sampled after bevacizumab administration.
GVAX for Recurrent Malignant Glioma
www.aacrjournals.org Clin Cancer Res; 22(12) June 15, 2016 2889
on May 9, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2016; DOI: 10.1158/1078-0432.CCR-15-2163

vaccination, seven of nine patients had marked increases in thepercentage of these cells within the CD4þ compartment, rangingfrom 162% to 385%, providing further indication that vaccina-tionwith irradiated autologous glioma cellsmixedwithGM-K562cells rapidly induces regulatory T-lymphocyte differentiation orsystemic mobilization (Fig. 2C and D).
SurvivalBy the MacDonald (17), criteria, each patient progressed radio-
graphically by the time of the first posttreatment MRI (7–9 weeks).For all patients, median overall survival was 35 weeks (range 21–92). Median overall survival for the 7 patients treated with 1� 107
GM-K562 cells was 53 weeks (range 30–92). Survival was notstatistically associatedwith any of the immune parameters studied.
Case examplesThe small number of patients treated in this phase I study and
the heterogeneous clinical presentations preclude meaningfulanalyses of associations between measured immune parametersand outcome. However, patients 4 and 5 reflect how clinical andradiographic responsesmay correlate with changes in cellular andhumoral immune responses in glioma patients undergoing autol-ogous tumor cell vaccination.
00.020.040.060.08
0.10.120.140.16
1710840
Pa�ent 2A
B C
Ang1
Ang2
0
0.2
0.4
0.6
0.8
1
1.2
1511730
Pa�ent 3
Ang1
Ang2
0
0.2
0.4
0.6
0.8
1
1.2
2723191511730
Pa�ent 4
Ang1
Ang2
0
0.2
0.4
0.6
0.8
1
1.2
1.4
22181410820
Pa�ent 5
Ang1
Ang2
00.10.20.30.40.50.60.70.8
191511730
Pa�ent 6
Ang1
Ang2
0
0.1
0.2
0.3
0.4
0.5
0.6
1210864320
Pa�ent 8
Ang1
Ang2
0
0.1
0.2
0.3
0.4
0.5
1310864320
Pa�ent 9
Ang1
Ang2
0
0.2
0.4
0.6
0.8
1
11975430
Pa�ent 10
Ang1
Ang2
0
0.5
1
1.5
2
1810864320
Pa�ent 11
Ang1
Ang2
0
0.2
0.4
0.6
0.8
1
1.2
302520151050
OD
450
Weeks
An�-angiopoie�n 1 an�bodies
Pa�ent 2Pa�ent 3Pa�ent 4Pa�ent 5Pa�ent 6Pa�ent 8Pa�ent 9Pa�ent 10Pa�ent 11
0
0.2
0.4
0.6
0.8
1
1.2
1.4
1.6
1.8
302520151050
OD
450
Weeks
An�-angiopoie�n 2 an�bodies
Pa�ent 2Pa�ent 3Pa�ent 4Pa�ent 5Pa�ent 6Pa�ent 8Pa�ent 9Pa�ent 10Pa�ent 11
Figure 1.A, measured absorbance of patient plasma in ELISA assay against angiopoietins 1 (Ang1) and 2 (Ang2) versus week from the time of initial vaccination in patientswith recurrent malignant glioma. The blue-dashed vertical lines denote the timepoint of the last dose of vaccine per patient. The aggregate time courseand magnitude of anti-Ang1 antibodies (B) and anti-Ang2 antibodies (C) are represented. Vaccinated patient plasma more consistently registered responsesto Ang2 peptide, and these were typically of greater intensity than responses to Ang1. Arrows denote delivery of vaccine.
Curry et al.
Clin Cancer Res; 22(12) June 15, 2016 Clinical Cancer Research2890
on May 9, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2016; DOI: 10.1158/1078-0432.CCR-15-2163

Patient 5. Patient 5 was a 62-year-old man treated with craniot-omy, radiation, and temozolomide chemotherapywho presentedwith nodular enhancement involving and surrounding his priorresection cavity in the right temporal lobe. Hewas enrolled on thevaccination protocol, and underwent near-total resection of themass. Substantial numbers of viable tumor cells were harvestedand vaccination was initiated, off of corticosteroids, 19 dayspostoperatively. As described previously, he presented with fever1 day after the first vaccination. The second treatment was post-poned by 1 week, without recurrent fever. After the fifth vaccina-tion (week 7.5), a regularly scheduledMRI demonstrated nodularenhancement, thought to be consistent with disease progression,and bevacizumab/irinotecan was started. Although brain MRI atthis point showed that the volume of gadolinium-enhancingtissue was increased, cerebral blood volume values and metabo-lites onMR spectroscopy were decreased, suggestive of treatment-associated changes.
Early imaging response after bevacizumab/irinotecan treat-ment showed reduced enhancement, which remained stable formore than a year until shortly before he passed away fromprogressive disease, 21 months after initiation of vaccination.
We retrospectively examined the patient's immune responses.At week 5 after vaccine initiation—the time of the fourth vaccineinjection—there was brisk upregulation of activating and regula-tory costimulatory molecules on both CD4þ and CD8þ lympho-cytes in the peripheral blood (Fig. 3A). The synchronous increasein CD4þFoxP3þ regulatory T lymphocytes was relatively modest.Subsequently, ELISAof the patient's plasma revealed abrisk rise inhumoral responses to angiopoietins 1 and 2, as well as HGF,PDGF, and Progranulin. These elevated responses began prior tothe initiation of bevacizumab/irinotecan at week 9, peaked atweek 14 after vaccination began, then persisted and partiallysubsided. Heightened lymphocyte activation, rising antitumorantibody titers, and advanced MR imaging suggestion of treat-ment effect raise the possibility that the week 7 scan representedpseudoprogression and that the durable tumor control thatfollowed was related to systemic antitumor immunity.
Patient 4.Patient 4's clinical course has been detailed in this reportin the section on safety of vaccination. During the fifth week,neurological deterioration lead to an MRI, which demonstratednewnodular enhancementwithmass effect. DTHanalysis at week5 revealed intense inflammatory infiltrates. Similarly, there wasbroad CD4þ and CD8þ T-lymphocyte activation with markedlyincreased expression of PD1, CTLA-4, CD137, and ICOS (Fig. 3B).The relative increase in the percentage of CD4þFoxp3þ cells was,as was the case for patient 5, modest. Patient 4 developed anti-bodies to multiple angiogenic cytokines, particularly againstangiopoietin 1 and angiopoietin 2. These antitumor antibodytiters continued to rise until week 14. The strength and polyva-lence of the immune response at week 5 and beyond supports ourretrospective belief that the synchronous MRI was an example ofvaccine-induced pseudoprogression. Subsequent MRIs are diffi-cult to interpret because of treatment with bevacizumab.
DiscussionIn this phase I study, we have achieved the primary objectives of
demonstrating safety and feasibility of combining autologousirradiated glioblastoma cells with up to 1� 107 GM-K562 cells asvaccination in patients that had undergone craniotomy for recur-
rent tumor. Feasibility was readily achieved, and there were noserious adverse events. Feasibility is a highly relevant issue forcellular glioma immunotherapy, particularly for patients withrecurrent disease. In a study examining the use of autologousglioma cells alongside patient fibroblasts engineered to expressIL4 (16),most enrolled patients did not receive treatment becauseof disease progression or clinical decline prior to initiation oftherapy. Similarly, in a recent phase I study of vaccination ofpatients undergoing craniotomy for recurrent glioblastoma withautologous tumor-derived peptides bound to the 96 kDa chap-erone protein derived from the tumor specimens (22), only 12 of28 enrolled patients were ultimately treated. Patient dropout wassecondary to inadequate harvest of viable tumor in nine patientsand progression or clinical deterioration prior to full vaccineadministration in four patients. In our series, the GM-K562bystander line facilitated the ready capacity to make vaccine andallowed rapid postoperative turnaround without the need toculture or genetically manipulate harvested specimens.
Consistent with other approaches to glioma immunotherapy(23), therewas no evidence of autoimmunity or encephalitis. Thisis significant for the use of autologous whole glioma cell vacci-nation, as, although the tumor specimens undergo enzymaticdigestion andmechanical separation, there is no process bywhichnormal glial or neuronal elements are excluded, and they may beincluded in the product.
Clinical useofGM-K562cells asbystanderproducersofGM-CSFhas been reported previously in the context of vaccination ofpatients with advanced lung cancer (24, 25) and in patients withchronic lymphocytic leukemia (CLL; ref. 25). In the CLL study, 22subjects were treated with irradiated autologous tumor cellsmixedwith 1 � 107 GM-K562 cells without adverse events. Vaccinationled to development of systemic tumor-specific T-cell responses.
Whole glioma cell vaccination has been examined previously,but not in amanner consistent with GVAX. Plautz, and colleaguesreported adoptive T-lymphocyte transfer in glioblastomapatients,using cells harvested from inguinal lymphnodes harvested 8 to 10days after a single subcutaneous injectionof irradiated autologoustumor cells mixed with 500 mg of recombinant GM-CSF (25).More recently, Ishikawa described safe treatment with autologousformalin-fixed tumor vaccine in patients with newly diagnosedglioblastoma (26). To the best of our knowledge, our study is thefirst report of the GVAX approach in patients with malignantgliomas.
Pseudoprogression by MRI is a well-known entity in glioblas-toma imaging (27) and may be relevant in patients treated withimmunotherapy aswell. In other solid tumors, standardCT-basedimaging criteria such as RECIST have been misleading, and analternative set of immune response assessment criteria have beenpromoted (28). We saw early appearance of new gadoliniumenhancement on MRI in some patients, followed by subsequentradiographic regression and/or lengthy stabilization of disease.Improved ability to differentiate tumor progression from toxic orinflammatory changes will help practitioners understand whichpatients are responding to treatment and which patients shouldbe directed towards another therapy. It is worth noting that in thetwo patient cases described in this report, whereas the MRIs and/or the clinical scenarios suggested progression, the accompanyingimmune studies showed treatment-driven activation, includingimproved ratios of activated T lymphocytes to regulatory T lym-phocytes. It is possible that immune parameters or biomarkerswill be more predictive of early response than standard imaging.
GVAX for Recurrent Malignant Glioma
www.aacrjournals.org Clin Cancer Res; 22(12) June 15, 2016 2891
on May 9, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2016; DOI: 10.1158/1078-0432.CCR-15-2163
Regulatory
–500%
0%
500%
1,000%
1,500%
2,000%
2,500%
0 4 6 13
Patient 2A
B
CD4
CTLA4
CD4,
PD1
CD8,
PD1
CD4
FOXP3
0%
500%
1,000%
1,500%
2,000%
2,500%
3,000%
0 4 8
Patient 3
CD4 CTLA4
CD4, PD1
CD8, PD1
CD4 FOXP3
–100%
0%
100%
200%
300%
400%
500%
600%
0 4 8 12
Patient 4
CD4 CTLA4
CD4, PD1
CD8, PD1
CD4 FOXP3
0%
200%
400%
600%
800%
1,000%
1,200%
0 5 8 11 15
Patient 5
CD4 CTLA4
CD4, PD1
CD8, PD1
CD4 FOXP3
0%
1,000%
2,000%
3,000%
4,000%
5,000%
6,000%
7,000%
8,000%
0 3 7 11 15
Patient 6
CD4 CTLA4
CD4, PD1
CD8, PD1
CD4 FOXP3
–100%
–50%
0%
50%
100%
150%
200%
250%
300%
350%
0 1 2 4 6 8 10
Patient 8
CD4 CTLA4
CD4, PD1
CD8, PD1
CD4 FOXP3
–150%
–100%
–50%
0%
50%
100%
150%
200%
0 1 2 4 6 8 11
Patient 9
CD4 CTLA4
CD4, PD1
CD8, PD1
CD4 FOXP3
–100%
–50%
0%
50%
100%
150%
200%
250%
300%
0 1 2 6 8
Patient 10
CD4 CTLA4
CD4, PD1
CD8, PD1
–60%
–50%
–40%
–30%
–20%
–10%
0%
10%
20%
0 1 2 4 8
Patient 11
CD4 CTLA4
CD4, PD1
CD8, PD1
CD4 FOXP3CD4 FOXP3
Stimulatory
–100%
0%
100%
200%
300%
400%
0 4 6 13
Patient 2
CD4, ICOS
CD8, ICOS
CD4, CD137
CD8, CD137
CD4, OX400%
500%
1,000%
1,500%
2,000%
0 4 8
Patient 3
CD4, ICOS
CD8, ICOS
CD4, CD137
CD8, CD137
CD4, OX40
–100%
0%
100%
200%
300%
400%
0 4 8 12
Patient 4CD4, ICOS
CD8, ICOS
CD4, CD137
CD8, CD137
CD4, OX40
–50%
0%
50%
100%
150%
200%
250%
300%
350%
400%
0 5 8 11 15
Patient 5
CD4, ICOS
CD8, ICOS
CD4, CD137
CD8, CD137
CD4, OX40
–500%
0%
500%
1,000%
1,500%
2,000%
2,500%
0 3 7 11 15
Patient 6
CD4, ICOS
CD8, ICOS
CD4, CD137
CD8, CD137
CD4, OX40
–200%
0%
200%
400%
600%
800%
1,000%
1,200%
1,400%
1,600%
1,800%
0 1 2 4 6 8 10
Patient 8
CD4, ICOS
CD8, ICOS
CD4, CD137
CD8, CD137
CD4, OX40
–200%
0%
200%
400%
600%
800%
1,000%
1,200%
1,400%
0 1 2 4 6 8 11
Patient 9
CD4, ICOS
CD8, ICOS
CD4, CD137
CD8, CD137
CD4, OX40
–150%
–100%
–50%
0%
50%
100%
150%
200%
0 1 2 6 8
Patient 10
CD4, ICOS
CD8, ICOS
CD4, CD137
CD8, CD137
–200%
0%
200%
400%
600%
800%
1,000%
1,200%
1,400%
0 1 2 4 8
Patient 11CD4, ICOS
CD8, ICOS
CD4, CD137
CD8, CD137
CD4, OX40CD4, OX40
Figure 2.Percent change in blood lymphocyte expression of (A) negative regulatory costimulatory molecules and FoxP3 (CD4þ) and of (B) costimulatory moleculesassociated with immune intensification versus weeks after first treatment in vaccinated patients with recurrent malignant glioma. Maximal changes in costimulatorymolecule expression varied in timing and significance. X-axes reflect weeks after initiation of therapy. (Continued on the following page.)
Curry et al.
Clin Cancer Res; 22(12) June 15, 2016 Clinical Cancer Research2892
on May 9, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2016; DOI: 10.1158/1078-0432.CCR-15-2163

Also, a relatively delayed onset of effective antitumor activity hasbeen observed previously in cancer vaccination, including in thephase 3 demonstration that Sipleucel-T improved overall survivalinpatientswith advancedhormone-refractory prostate cancer, butdid not change progression-free survival. As immunotherapyevolves andbecomesmore effective in patientswith brain tumors,management of inflammatory toxicity may have to move awayfrom the use of corticosteroids, which can downregulate T-cellresponses.
The tracking of relevant biomarkers for assessment of cancerimmunotherapies is a complex and dynamic process; the efficacyof the antitumor response is ultimately dependent upon interac-tions between variable factors related to the host, the tumor itself,and the treatments in question, in addition to any other therapiesthat may be used in combination or sequentially. Evaluation ofDTH sites provides a straightforward assessment of the biologicalactivity of any immunotherapy. In these glioma patients, histol-ogy evaluation of punch biopsies of DTH injection sites consis-tently demonstrated intensification of an inflammatory responsewithin the irradiated tumor deposits after 4 vaccinations. Thisresponse was fully lacking in each patient at the time of the firstvaccination, prior to the onset of biological effect of the vaccine.DTH studies assess systemic immunoreactivity to a given patient'stumor within the physical context of the host; however, they donot necessarily represent interactions within the actual tumormilieu and do not provide information about immune cellularfunction. With further progress in the field of glioma immuno-therapy, stereotactic biopsy of the actual tumor sites may becomenecessary if imaging and serologic biomarkers of response are notconsistently representative of antitumor effect.
Lymphocytes are effectors of adaptive antitumor immunity,and analysis of their differentiation and activation status, both assnapshots andover time,mayprovide associationswith responsesto immunotherapy (29–31). For better understanding of biomar-kers and predictors of immune and clinical response in glioma
patients, many more patients will have to be treated, including asignificant fraction with clinical responses.
In our patients, vaccination with irradiated autologous tumorcells mixed with GM-K562 cells seemed to impact the activationstatus of T lymphocytes, particularly in the CD4þ subset.Although activation of T lymphocytes requires major histocom-patibility complex engagement of the T-cell receptor coupled byCD80 or 86 binding of CD28 (32), numerous subsequent inter-actions occur at the APC/T-cell interface that fine-tune theimmune response; some are associated with further activationand clonal proliferation, whereas others are associated withhomeostatic negative immune regulation.We have demonstratedstatistically significant increases of CD4þ T-lymphocyte expres-sion of CTLA-4, PD-1, OX40, and CD137 within 12 weeks ofvaccination initiation. CD8þ T-lymphocyte expression of CD137was significantly increased and many patients saw elevations inPD-1 expression by CD8þ T lymphocytes as well. Overall, thesealterations imply a general treatment-associated activation ofperipheral lymphocyte responses that peaks after several roundsof vaccination have occurred. We also observed increased fre-quency of regulatory T lymphocytes within the CD4þ compart-ment, a phenomenon which has been described in preclinicalmodels of GM-CSF-expressing irradiated autologous tumor cells(33) and, clinically, in ipilimumab þ GM-CSF combinationtherapy (31). The efficacy of therapymay ultimately depend uponthe change in the ratio of effector T lymphocytes to regulatory Tlymphocytes (15), intratumorally and systemically; we did notcollect absolute lymphocyte counts, which precludes precisecalculation of these numbers. Nevertheless, it may be beneficialto combine vaccination with agents that counteract regulatory T-lymphocyte activity or suppress their induction, which is partiallydependent on GM-CSF levels (34). Furthermore, GM-CSF expres-sion in cancer vaccines has been shown to increase the number ofcirculating and intratumoral myeloid-derived suppressor cells(35). Combining vaccination with VEGF inhibition may be a
0
0.5
1
1.5
2
2.5
C D
Patient Patient Patient Patient Patient Patient Patient Patient Patient
0 Weeks
4 Weeks
Patient 2
Patient 3
Patient 4
Patient 5
Patient 6
Patient 8
Patient 9
Patient 10
Patient 11
% Change in CD4+CD25+CD127- T Lymphocytes
Patient 2
Patient 3
Patient 4
Patient 5
Patient 6
Patient 8
Patient 9
Patient 10
Patient 11
Figure 2.(Continued. ) C, frequency of CD4þCD25þCD127� T lymphocytes at the initiation of vaccination (week 0) and 4 weeks later. D, percent change in the frequencyof CD4þCD25þCD127� T lymphocytes between weeks 0 and 4 of treatment. Red color reflects percentage decrease.
GVAX for Recurrent Malignant Glioma
www.aacrjournals.org Clin Cancer Res; 22(12) June 15, 2016 2893
on May 9, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2016; DOI: 10.1158/1078-0432.CCR-15-2163

0%
200%
400%
600%
800%
1,000%
1,200%
1511850
Regulatory
CD4 CTLA4
CD4, PD1
CD8, PD1
CD4 FOXP3
–100%
0%
100%
200%
300%
400%
1511850
S�mula�ng
CD4, ICOS
CD8, ICOS
CD4, CD137
CD8, CD137
CD4, OX40
Post-Op
A
B
7 Weeks 11 Weeks(Post bevacizumab)
00.20.40.60.8
11.21.4
22181410820
Ang1
Ang2
An�-angiopoie�n an�bodies
–100%
–50%
0%
50%
100%
150%
200%
250%
300%
350%
400%
12840
S�mula�ng
CD4, ICOS
CD8, ICOS
CD4, CD137
CD8, CD137
CD4, OX40
–100%
0%
100%
200%
300%
400%
500%
600%
12840
Regulatory
CD4 CTLA4
CD4, PD1
CD8, PD1
CD4 FOXP3
Week 0 Week 4 Week 7
0
0.2
0.4
0.6
0.8
1
1.2
2723191511730
An�-angiopoie�n an�bodies
Ang1
Ang2
Figure 3.A, serial magnetic resonance imaging of patient 5 demonstrating increased nodular gadolinium enhancement around the resection cavity 7 weeks afterinitiation of vaccination, shortly after peak T lymphocyte activation and concurrent with rises in plasma antibodies to Ang1 and Ang2. B, for patient 4, increasedgadolinium enhancement at week 4 corresponded with increased expression of T lymphocytes costimulatory molecules and was detected just prior insignificant increases to anti-Ang1 and anti-Ang2 antibodies in the patient's plasma. Dexamethasone was administered and, within 3 weeks, the enhancementhad receded.
Curry et al.
Clin Cancer Res; 22(12) June 15, 2016 Clinical Cancer Research2894
on May 9, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2016; DOI: 10.1158/1078-0432.CCR-15-2163

way to strengthen antitumor immunity by reduction of MDSCinduction (36). Likewise, co-administration of toll-like receptor(TLR) ligands alongwithGM-CSF expressing vaccinesmay reverseMDSC induction and further promote antitumor immunity,driving stronger responses (37). In some clinical studies, however,GVAX immunotherapy has led to a reduction in circulatingMDSCs (38). The relationship between GM-CSF expression andimmunoregulatory mechanisms requires further study.
The time-dependent elevated expression of costimulatory andcoinhibitory molecules on the T-lymphocyte surface may high-light the optimal points at which to administer "checkpoint-active" therapies after vaccination. Along these lines, in a murineintracranial glioma model, we have demonstrated synergisticefficacy following syngeneic GM-CSF expressing tumor cell vac-cination with CTLA-4 blockade (12). In these studies, sequentialdelivery of these immunotherapies provoked stronger antitumoreffect than giving them concurrently (unpublished data). Block-ade of PD-1 function (39) and agonist ligation of OX-40 (40) and4-1BB (CD137; ref. 41) have shown promising activity in com-bination with vaccination in preclinical glioma models. Vaccine-associated activation and upregulation of these "druggable" tar-gets on T lymphocytes may provide an opportunity for increasingthe efficacy of these therapeutics.
Measuring T-lymphocyte activation, as above, does not clarifythe antigen specificity of the response. A whole-tumor cellapproach creates a challenge for antigen-specific immunomoni-toring. The CD137 expressing subset of T lymphocytes has beenshown to harbor specifically activated cells, and may serve as ameans of identifying the repertoire of the antigen-specific cellsamidst a heterogeneous population (42).
Our assay of humoral responses to angiogenic cytokines has thepotential to provide immunomonitoring across cancer types andimmunotherapies. Among vaccinated glioblastoma patients, werevealed increases in antibody titers to angiopoietins 1 and 2among other angiogenic cytokines. These antibody responseswere not detectable prior to vaccination. The induction of anti-body responses to angiogenic cytokines may have several rami-fications. Fundamentally, this illustrates the vaccine-driven pres-ence of humoral antitumor immunity, in temporal coordinationwith the T-lymphocyte activation catalogued by immunopheno-typing studies. Schoenfeld demonstrated that sera of vaccinatedcancer patientswith detectable antibodies to angiogenic cytokinesexhibits functional angiogenesis inhibition in vitro (20). Vacci-nated leukemia patients with early development of antibodies totwo or more angiogenic cytokines saw improved survival com-pared to those with measureable detection of one or fewercytokines on the same panel. Angiogenic cytokines, includingangiopoietins, may inhibit immune function, and their blockademay thereby further enhance intratumoral lymphocyte infiltra-tion, leading to increased antitumor cytotoxic effect and subse-quent immunogenicity. The immune targeting of multiple angio-
genic proteins may allow synergy with current angiogenesisinhibitors. The mechanism by which this vaccine-induced target-ing of the tumor vasculature occurs and its therapeutic conse-quences requires further investigation, but supports the rationalefor combination approaches with autologous cell-based vaccina-tion and angiogenesis inhibitors.
In summary, vaccination of patients undergoing craniotomyfor recurrent malignant glioma with irradiated autologous tumorcells mixed with GM-K562 cells was feasible and safe. Via histol-ogy evaluation of delayed-type hypersensitivity reactions, phe-notypic demonstration of T-lymphocyte activation, and the iden-tification of elevated titers of antibodies to angiogenic cytokines,"bystander GVAX" vaccination has biological activity in thesepatients, and we have strengthened the rationale for a variety ofcombination approaches. These strategies may include augment-ing vaccination with monoclonal antibodies targeting T-lympho-cyte costimulatory molecules, agents that suppress regulatory Tlymphocytes, and inhibitors of angiogenesis.
Disclosure of Potential Conflicts of InterestT. Batchelor reports receiving commercial research grants from Pfizer; speak-
ers bureau honoraria from Merck; and is a consultant/advisory board memberfor Oxigene, Roche, and Upsher. M.C. Mihm is a consultant/advisory boardmember for Caliber ID, MELASciences, and Wiley & Sons. G. Dranoff reportsreceiving commercial research grants from and is a consultant/advisory boardmember for Novartis. No potential conflicts of interest were disclosed by theother authors.
Authors' ContributionsConception and design: W.T. Curry Jr, G. DranoffDevelopment of methodology: W.T. Curry Jr, M. Piesche, G. DranoffAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): W.T. Curry Jr, R. Gorrepati, M. Piesche, T. Sasada,P. Agarwalla, E.R. Gerstner, A.J. Golby, T.T. Batchelor, P.Y. WenAnalysis and interpretation of data (e.g., statistical analysis, biostatistics,computational analysis): W.T. Curry Jr, R. Gorrepati, M. Piesche, T. Sasada,P.S. Jones, P.Y. Wen, M.C. MihmWriting, review, and/or revision of the manuscript:W.T. Curry Jr, M. Piesche,T. Sasada, P. Agarwalla, E.R. Gerstner, T.T. Batchelor, P.Y. Wen, M.C. Mihm,G. DranoffAdministrative, technical, or material support (i.e., reporting or organizingdata, constructing databases): W.T. Curry Jr, M. Piesche, P. AgarwallaStudy supervision: W.T. Curry Jr, G. Dranoff
Grant SupportW. Curry, MD, was partially supported by a grant from the Harold Amos
Faculty Development Program of the Robert Wood Johnson Foundation.The costs of publication of this articlewere defrayed inpart by the payment of
page charges. This article must therefore be hereby marked advertisement inaccordance with 18 U.S.C. Section 1734 solely to indicate this fact.
Received September 2, 2015; revised January 15, 2016; accepted February 4,2016; published OnlineFirst February 12, 2016.
References1. Hodi FS,O'Day SJ,McDermott DF,Weber RW, Sosman JA,Haanen JB, et al.
Improved survivalwith ipilimumab in patients withmetastaticmelanoma.N Engl J Med 2010;363:711–23.
2. Larkin J, Chiarion-Sileni V, Gonzalez R, Grob JJ, Cowey CL, Lao CD, et al.Combined nivolumab and ipilimumab or monotherapy in untreatedmelanoma. N Engl J Med 2015;373:23–34.
3. Sunshine J, Taube JM. PD-1/PD-L1 inhibitors. Curr Opin Pharmacol2015;23:32–8.
4. Kantoff PW, Higano CS, Shore ND, Berger ER, Small EJ, Penson DF, et al.Sipuleucel-T immunotherapy for castration-resistant prostate cancer.N Engl J Med 2010;363:411–22.
5. Dranoff G. GM-CSF-secreting melanoma vaccines. Oncogene 2003;22:3188–92.
6. Hegi ME, Diserens AC, Gorlia T, HamouMF, de Tribolet N, Weller M, et al.MGMT gene silencing and benefit from temozolomide in glioblastoma.N Engl J Med 2005;352:997–1003.
www.aacrjournals.org Clin Cancer Res; 22(12) June 15, 2016 2895
GVAX for Recurrent Malignant Glioma
on May 9, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2016; DOI: 10.1158/1078-0432.CCR-15-2163

7. Gilbert MR, Dignam JJ, Armstrong TS, Wefel JS, Blumenthal DT, Vogel-baum MA, et al. A randomized trial of bevacizumab for newly diagnosedglioblastoma. N Engl J Med 2014;370:699–708.
8. Jahangiri A, De Lay M, Miller LM, Carbonell WS, Hu YL, Lu K, et al. Geneexpression profile identifies tyrosine kinase c-Met as a targetable mediatorof antiangiogenic therapy resistance. Clin Cancer Res 2013;19:1773–83.
9. Vredenburgh JJ, Desjardins A, Herndon JE, Marcello J, Reardon DA, QuinnJA, et al. Bevacizumab plus irinotecan in recurrent glioblastoma multi-forme. J Clin Oncol 2007;25:4722–9.
10. Pallasch CP, Struss AK, Munnia A, K€onig J, Steudel WI, Fischer U, et al.Autoantibodies against GLEA2 and PHF3 in glioblastoma: tumor-associ-ated autoantibodies correlated with prolonged survival. Int J Cancer2005;117:456–9.
11. Sayour EJ, McLendon P, McLendon R, De Leon G, Reynolds R, Kresak J,et al. Increased proportion of FoxP3þ regulatory T cells in tumor infiltrat-ing lymphocytes is associated with tumor recurrence and reduced survivalin patients with glioblastoma. Cancer Immunol Immunother 2015;64:419–27.
12. Agarwalla P, Barnard Z, Fecci P, Dranoff G, Curry WT. Sequential immu-notherapy by vaccination with GM-CSF-expressing glioma cells andCTLA-4 blockade effectively treats established murine intracranial tumors.J Immunother 2012;35:385–9.
13. Quezada SA, Peggs KS, Curran MA, Allison JP. CTLA4 blockade and GM-CSF combination immunotherapy alters the intratumor balance of effectorand regulatory T cells. J Clin Invest 2006;116:1935–45.
14. Singh H, Madan R, Dahut W, Coyne G, Rauckhorst M, McMahon S, et al.Combining active immunotherapy and immune checkpoint inhibitorsin prostate cancer. In: Proceedings of the Genitourinary Cancers Sym-posium; 2015 Feb 26: Orlando, FL; 2015.
15. Hodi FS, Butler M, Oble DA, Seiden MV, Haluska FG, Kruse A, et al.Immunologic and clinical effects of antibody blockade of cytotoxic Tlymphocyte-associated antigen 4 in previously vaccinated cancer patients.Proc Natl Acad Sci U S A 2008;105:3005–10.
16. Okada H, Lieberman FS, Walter KA, Lunsford LD, Kondziolka DS, BejjaniGK, et al. Autologous glioma cell vaccine admixed with interleukin-4 genetransfected fibroblasts in the treatment of patients withmalignant gliomas.J Transl Med 2007;5:67.
17. Borrello I, Sotomayor EM, Cooke S, Levitsky HI. A universal granulocyte-macrophage colony-stimulating factor-producing bystander cell line foruse in the formulationof autologous tumor cell-based vaccines.HumGeneTher 1999;10:1983–91.
18. Burkhardt UE, Hainz U, Stevenson K, Goldstein NR, Pasek M, Naito M,et al. Autologous CLL cell vaccination early after transplant inducesleukemia-specific T cells. J Clin Invest 2013;123:3756–65.
19. PiescheM,Ho VT, KimH,Nakazaki Y, NehilM, Yaghi NK, et al. Angiogeniccytokines are antibody targets during graft-versus-leukemia reactions.Clin Cancer Res 2015;21:1010–8.
20. Schoenfeld J, JinushiM,Nakazaki Y,Wiener D, Park J, Soiffer R, et al. Activeimmunotherapy induces antibody responses that target tumor angiogen-esis. Cancer Res 2010;70:10150–60.
21. Hodi FS, Lawrence D, Lezcano C, Wu X, Zhou J, Sasada T, et al. Bevaci-zumab plus ipilimumab in patients with metastatic melanoma. CancerImmunol Res 2014;2:632–42.
22. Crane CA, Han SJ, Ahn B, Oehlke J, Kivett V, Fedoroff A, et al. Individualpatient-specific immunity against high-grade glioma after vaccinationwithautologous tumor derivedpeptides bound to the 96KDchaperone protein.Clin Cancer Res 2013;19:205–14.
23. Reardon DA, Freeman G, Wu C, Chiocca EA, Wucherpfennig KW, Wen PY,et al. Immunotherapy advances for glioblastoma. Neuro Oncol 2014;16:1441–58.
24. Nemunaitis J, Jahan T, RossH, StermanD, Richards D, Fox B, et al. Phase 1/2 trial of autologous tumor mixed with an allogeneic GVAX vaccine inadvanced-stage non-small-cell lung cancer. Cancer Gene Ther 2006;13:555–62.
25. Creelan BC, Antonia S, Noyes D, Hunter TB, Simon GR, Bepler G, et al.Phase II trial of a GM-CSF-producing and CD40L-expressing bystander cell
line combined with an allogeneic tumor cell-based vaccine for refractorylung adenocarcinoma. J Immunother 2013;36:442–50.
26. Ishikawa E,Muragaki Y, Yamamoto T,Maruyama T, Tsuboi K, Ikuta S, et al.Phase I/IIa trial of fractionated radiotherapy, temozolomide, and autolo-gous formalin-fixed tumor vaccine for newly diagnosed glioblastoma.J Neurosurg 2014;121:543–53.
27. Jahangiri A, Aghi MK. Pseudoprogression and treatment effect. NeurosurgClin N Am 2012;23:277–87, viii–ix.
28. Wolchok JD, Hoos A, O'Day S, Weber JS, Hamid O, Lebb�e C, et al.Guidelines for the evaluation of immune therapy activity in solidtumors: immune-related response criteria. Clin Cancer Res 2009;15:7412–20.
29. Fong B, Jin R, Wang X, Safaee M, Lisiero DN, Yang I, et al. Monitoring ofregulatory T cell frequencies and expression of CTLA-4 on T cells, beforeand after DC vaccination, can predict survival in GBM patients. PLoS One2012;7:e32614.
30. Santegoets SJ, StamAG, Lougheed SM,GallH, Scholten PE, ReijmM, et al. Tcell profiling reveals high CD4þCTLA-4 þ T cell frequency as dominantpredictor for survival after prostate GVAX/ipilimumab treatment. CancerImmunol Immunother 2013;62:245–56.
31. Kwek SS, Lewis J, Zhang L, Weinberg V, Greaney S, Harzstark A, et al. Pre-existing levels of CD4 T cells expressing PD-1 are related to overall survivalin prostate cancer patients treated with ipilimumab. Cancer Immunol Res2015;3:1008–16.
32. Schwartz RH. Costimulation of T lymphocytes: the role of CD28, CTLA-4,and B7/BB1 in interleukin-2 production and immunotherapy. Cell1992;71:1065–8.
33. LaCelleMG, Jensen SM, Fox BA. Partial CD4 depletion reduces regulatory Tcells induced by multiple vaccinations and restores therapeutic efficacy.Clin Cancer Res 2009;15:6881–90.
34. JinushiM,Nakazaki Y,DouganM,CarrascoDR,MihmM,DranoffG.MFG-E8-mediated uptake of apoptotic cells by APCs links the pro- and antiin-flammatory activities of GM-CSF. J Clin Invest 2007;117:1902–13.
35. Serafini P, Carbley R, Noonan KA, Tan G, Bronte V, Borrello I. High-dosegranulocyte-macrophage colony-stimulating factor-producing vaccinesimpair the immune response through the recruitment of myeloid sup-pressor cells. Cancer Res 2004;64:6337–43.
36. Guislain A, Gadiot J, Kaiser A, Jordanova ES, Broeks A, Sanders J, et al.Sunitinib pretreatment improves tumor-infiltrating lymphocyte expansionby reduction in intratumoral content of myeloid-derived suppressor cellsin human renal cell carcinoma. Cancer Immunol Immunother 2015;64:1241–50.
37. Fern�andez A, Oliver L, Alvarez R, Fern�andez LE, Lee KP, Mesa C. Adjuvantsand myeloid-derived suppressor cells: enemies or allies in therapeuticcancer vaccination. Hum Vaccin Immunother 2014;10:3251–60.
38. Lipson EJ, SharfmanWH, Chen S, McMiller TL, Pritchard TS, Salas JT, et al.Safety and immunologic correlates of Melanoma GVAX, a GM-CSF secret-ing allogeneic melanoma cell vaccine administered in the adjuvant setting.J Transl Med 2015;13:214.
39. Zeng J, See AP, Phallen J, Jackson CM, Belcaid Z, Ruzevick J, et al. Anti-PD-1 blockade and stereotactic radiation produce long-term survival inmice with intracranial gliomas. Int J Radiat Oncol Biol Phys 2013;86:343–9.
40. Schreiber TH, Wolf D, Bodero M, Gonzalez L, Podack ER. T cell costimula-tion by TNFR superfamily (TNFRSF)4 and TNFRSF25 in the context ofvaccination. J Immunol 2012;189:3311–8.
41. Lin X, Zhou C, Wang S, Wang D, MaW, Liang X, et al. Enhanced antitumoreffect against human telomerase reverse transcriptase (hTERT) by vacci-nation with chemotactic-hTERT gene-modified tumor cell and the com-bination with anti-4-1BB monoclonal antibodies. Int J Cancer 2006;119:1886–96.
42. Wolfl M, Kuball J, Ho WY, Nguyen H, Manley TJ, Bleakley M, et al.Activation-induced expression of CD137 permits detection, isolation, andexpansion of the full repertoire of CD8þ T cells responding to antigenwithout requiring knowledge of epitope specificities. Blood 2007;110:201–10.
Clin Cancer Res; 22(12) June 15, 2016 Clinical Cancer Research2896
Curry et al.
on May 9, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2016; DOI: 10.1158/1078-0432.CCR-15-2163
2016;22:2885-2896. Published OnlineFirst February 12, 2016.Clin Cancer Res William T. Curry, Jr, Ramana Gorrepati, Matthias Piesche, et al. Lymphocyte Activation in Patients with Recurrent Malignant GliomaIrradiated GM-K562 Cells Stimulates Antitumor Immunity and T Vaccination with Irradiated Autologous Tumor Cells Mixed with
Updated version
10.1158/1078-0432.CCR-15-2163doi:
Access the most recent version of this article at:
Material
Supplementary
http://clincancerres.aacrjournals.org/content/suppl/2016/02/12/1078-0432.CCR-15-2163.DC1
Access the most recent supplemental material at:
Cited articles
http://clincancerres.aacrjournals.org/content/22/12/2885.full#ref-list-1
This article cites 41 articles, 13 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/22/12/2885.full#related-urls
This article has been cited by 1 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/22/12/2885To request permission to re-use all or part of this article, use this link
on May 9, 2020. © 2016 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst February 12, 2016; DOI: 10.1158/1078-0432.CCR-15-2163