vaccine hesitancy: definition and background - sabin.org · vaccine hesitancy: definition and...
TRANSCRIPT
1
Vaccine Hesitancy:
Definition and Dimensions
Noni MacDonald MD, FRCPCDalhousie University,
Canadian Centre for VaccinologyHalifax , Canada
IAIM Joint Regional MeetingFeb 2, 2017
Conflicts of Interest
No relationship with commercial interests
i.e. no conflicts of interest
• Noni MacDonald:
professsor, Dalhousie University, Halifax Canada,
consultant and adviser to WHO EURO and WHO HQ
• Biases
I believe vaccines are safe, effective,
serious diseases can occur if not immunized
2
Vaccine HesitancyHesitancy: as old as vaccination itselfSince Jenner first scraped cow-pox blisters & innoculated people, see examples resistance to vaccination
Vaccine refusal:
associated with outbreaks many diseases in many different countries, including:
• Pertussis in the UK, US and Japan
• Measles in USA, Canada, France etc
• Polio in Nigeria
• Tetanus in Philippines and Kenya
Hesitancy can affect any vaccination program
Wolfe RM, Sharp LK. Anti-vaccinationists past and present. BMJ. 2002;325(7361):430-2.Dubé E, Vivion M, MacDonald NE. Vaccine hesitancy, vaccine refusal and the anti-vaccine movement:
influence, impact and implications. Expert Rev Vaccines. 2015;14(1):99-117.
www.freewebs.com/edward_jenner/the_cow_pock_
large_cartoon.jpg
3
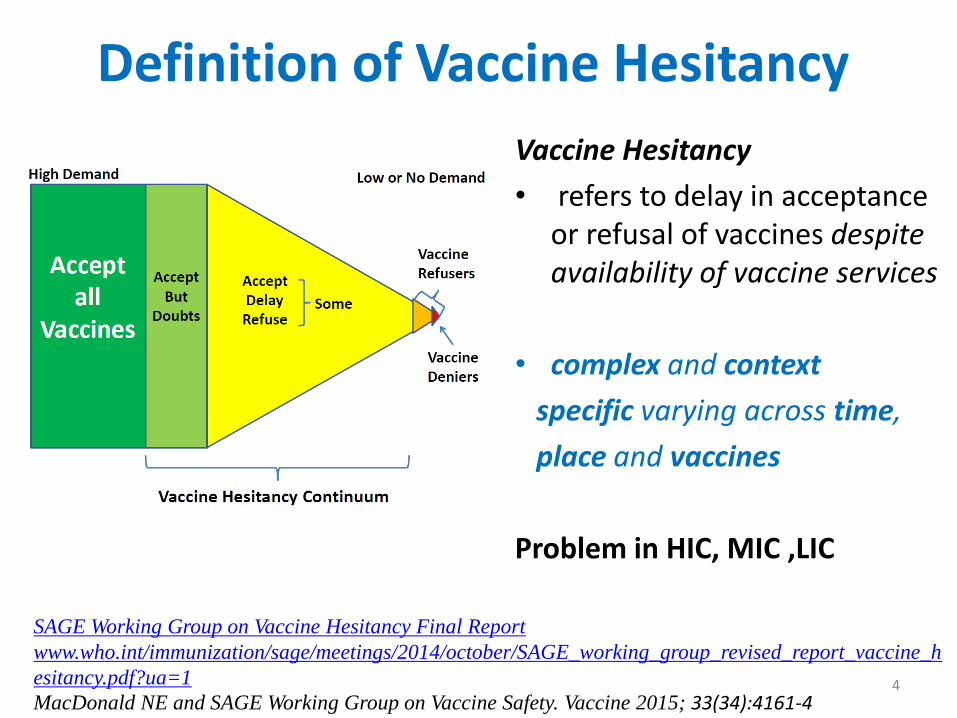
Definition of Vaccine Hesitancy
Vaccine Hesitancy
• refers to delay in acceptance or refusal of vaccines despite availability of vaccine services
• complex and context
specific varying across time,
place and vaccines
Problem in HIC, MIC ,LIC
SAGE Working Group on Vaccine Hesitancy Final Report
www.who.int/immunization/sage/meetings/2014/october/SAGE_working_group_revised_report_vaccine_h
esitancy.pdf?ua=1
MacDonald NE and SAGE Working Group on Vaccine Safety. Vaccine 2015; 33(34):4161-44
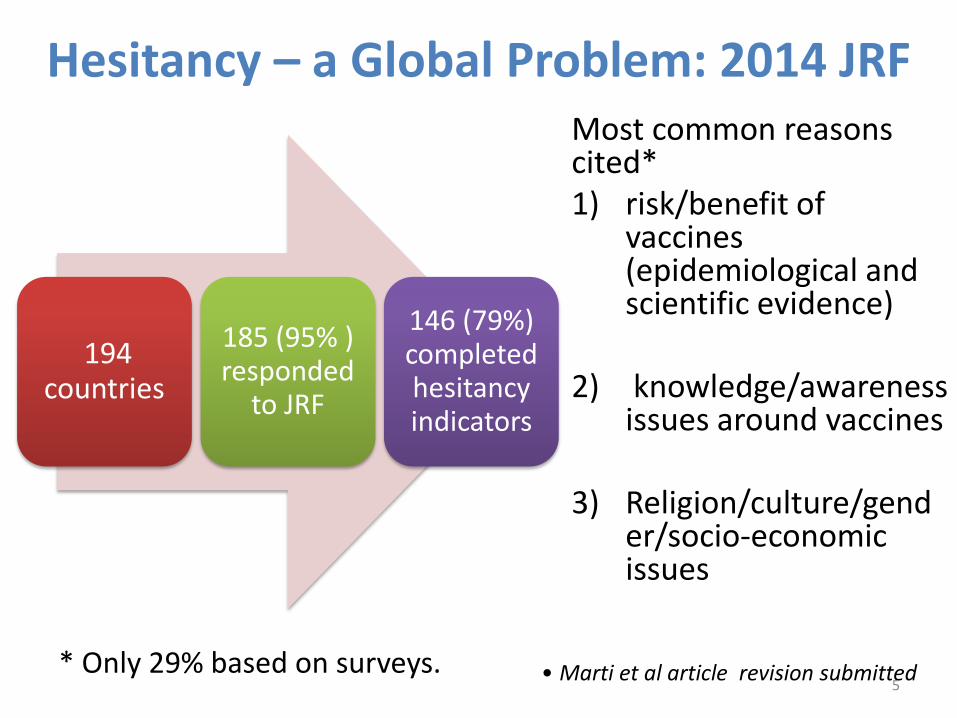
Hesitancy – a Global Problem: 2014 JRF
194 countries
185 (95% ) responded
to JRF
146 (79%) completed hesitancy indicators
Most common reasons cited* 1) risk/benefit of
vaccines (epidemiological and scientific evidence)
2) knowledge/awareness issues around vaccines
3) Religion/culture/gender/socio-economic issues
* Only 29% based on surveys. • Marti et al article revision submitted 5
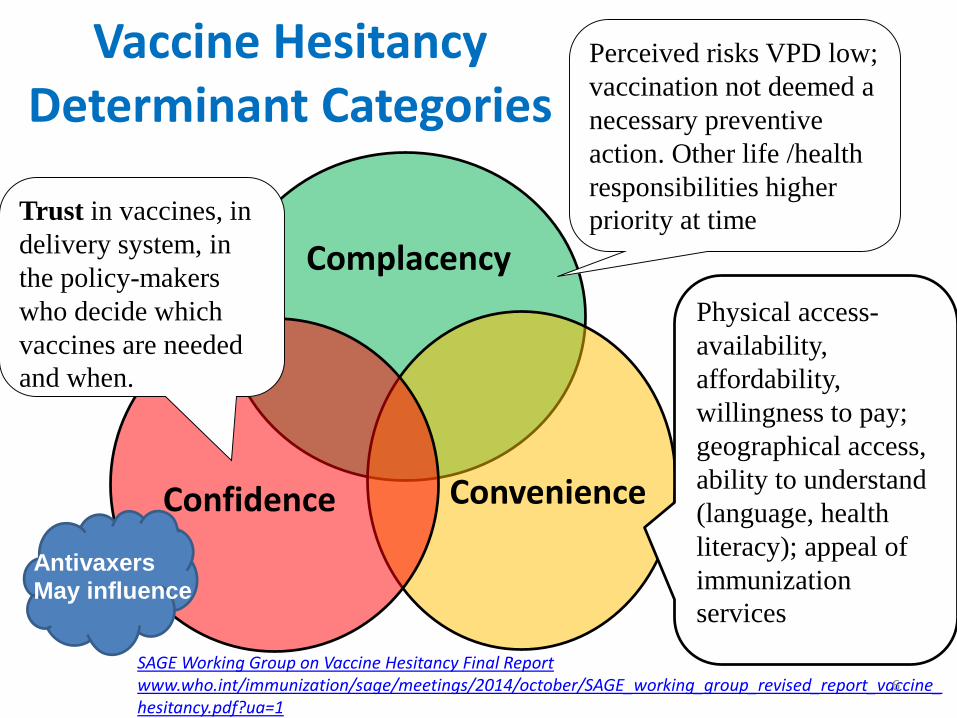
Vaccine HesitancyDeterminant Categories
Perceived risks VPD low;
vaccination not deemed a
necessary preventive
action. Other life /health
responsibilities higher
priority at timeTrust in vaccines, in
delivery system, in
the policy-makers
who decide which
vaccines are needed
and when.
Physical access-
availability,
affordability,
willingness to pay;
geographical access,
ability to understand
(language, health
literacy); appeal of
immunization
services
Confidence Convenience
Complacency
SAGE Working Group on Vaccine Hesitancy Final Report www.who.int/immunization/sage/meetings/2014/october/SAGE_working_group_revised_report_vaccine_hesitancy.pdf?ua=1
Antivaxers
May influence
6
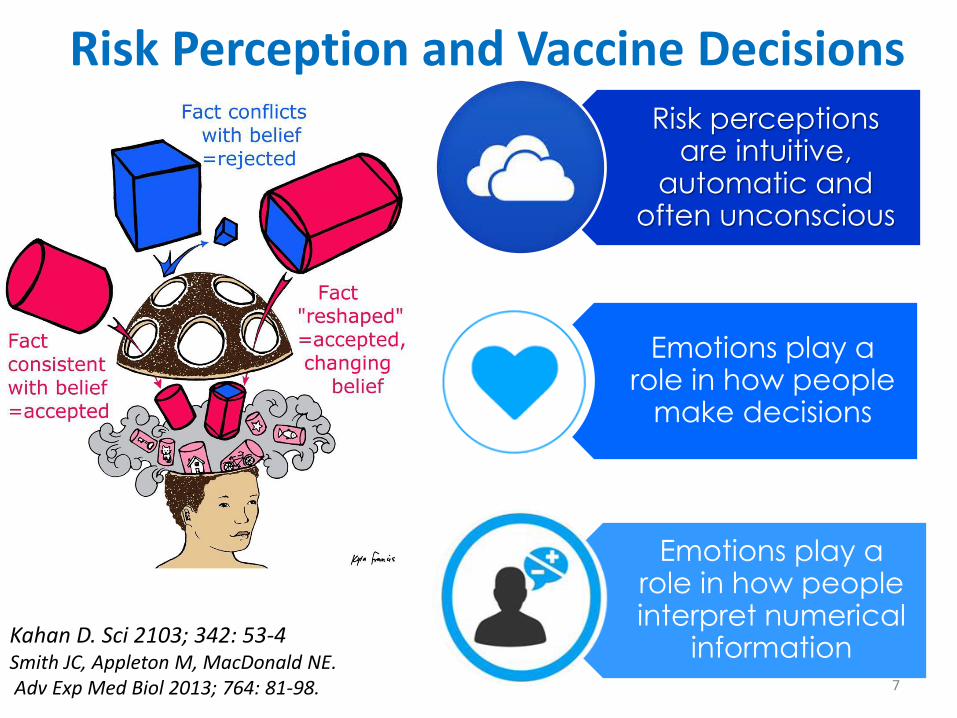
Risk perceptions are intuitive,
automatic and often unconscious
Emotions play a role in how people
make decisions
Emotions play a role in how people interpret numerical
information
Risk Perception and Vaccine Decisions
Kahan D. Sci 2103; 342: 53-4Smith JC, Appleton M, MacDonald NE.Adv Exp Med Biol 2013; 764: 81-98. 7

Vaccine Hesitancyinfluenced by many social, cultural, demographic and socio-psychological factors
• We are strongly influenced by what we think others around us are doing or expecting us to do
• We see causation in coincidences
• We see what we believe, rather than believing what we see
• We prefer anecdote and stories to data and evidence
• We are becoming increasingly hypervigilant to risk for our children
Dube E, MacDonald NE. Lancet ID 2016; 16(5):518-98
Addressing Dimensions ofVaccine Hesitancy
Systematic review of strategies peer-reviewed and gray literature (2007-2013) & Review of Reviews
Identified:
- no strategies to specifically overcome hesitancy in
all populations
- strategies that improved vaccine uptake
- multicomponent more effective than single
Jarrett C, Wilson R, O’Leary M, Eckersberger E, Larson HJ and the SAGE Working Group on Vaccine
Hesitancy Strategies for addressing vaccine hesitancy -a systematic review. Vaccine 2015;33(34): 4180-
90.
Dubé E, Gagnon D, MacDonald NE and the SAGE Working Group on Vaccine Hesitancy. Strategies
intended to address vaccine hesitancy: Review of published reviews. Vaccine 2015;33(34): 4191-203.
Complex not simple problem
9

10
12 Approaches to Enhance Vaccine Acceptance/Address Hesitancy
At Immunization Program Level
1. Detect and address hesitancy
2. Ensure HCW best immunization practices
3. Utilize evidence based strategies known to ↑ uptake
4. Effective Communication plan
5. Educating children, youth, adults on the importance immunization for health
6. Work collaboratively
At individual Level 7. HCP – key role in imm8. Don’t dismiss from practice
9. Use effective parental discussion techniques
10. Use clear language
11. Reinforce role community immunity
12. Address pain at immunization
Dube E, MacDonald NE. Lancet ID 2016;

1. Everyone is not Same: Detect and Address Vaccine Hesitant Subgroups
Reasons for hesitancy vary;
- not uniform over popn;
- may change over time
- vary by vaccine
- may be clustered
At program level: key to identify subgroups low immunization- hard if no immunization registry
WHO EUR: The Guide to Tailoring Immunization Program- “TIP”
Butler R, MacDonald N. Vaccine 2015;33:4176-9
outbreak started in anthroposophical schools in Ghent (Flanders) in February.
Geographical distribution of measles cases in Belgium Jan –
March 2011 n=151
Sabbe M et. Euro Surveill 2011; 16(16):pii=19848..
11
2. HCW Impact Vaccine Acceptance: Ensure HCW use Best Immunization Practices
HCW’s own immunization status: -reflects onto their patients’ status
HCW vaccine beliefs: - influences whether families will come forward and accept immunization
For optimal outcome patients need to hear from all HCW :
- consistent, accurate information: vaccine preventable disease risks, vaccine safety & benefits
- given in a respectful, positive manner
Zhang J et al Vaccine 2010, 28:7207-14; Collange F et al Hum Vac &Imm 2016; 12:1282-92 Favin M, et al International Health 2012; 4:229-238. Corace K et al Vaccine 2016; 34: 3235–3242
Shibli et al Vaccine online Dec 30, 2016
HCP immunization education key Ensure HCW immunization up to date
12
3. Multiple dimensions to hesitancy: Use Effective Strategies to ↑ Vaccine Uptake a) directly target
• unvaccinated or under-vaccinated populations
• specific populations: e.g. local community, HCW;
b) aim to increase knowledge, awareness about vaccination*;
c) engage community leaders, religious or other influential leaders to promote vaccination in the community.
d) improve convenience and access to vaccination;
e) employ reminder and follow-up;
f) mandate vaccinations / sanctions for non-vaccination,
$$ incentives;
Jarrett C, et al.Vaccine 2015; 33:4180-90; Dube E et; Vaccine. 2015 14;33:4191-203; Das et al Journal of Adolescent Health 2016; 59:S40eS48
13

Religion and Vaccines Review of major religions of world –
-most religious doctrines support
caring for others,
preserving life
having a duty to the community (family, neighbours, each other) i.e support vaccination
- exception Christian Scientists
- did not look at anthroposophical -
Polio scare Israel 2014: multi pronged approach- including work with IMA, IPA, rabbis, imams etc
Grabenstein JD. Vaccine 2013;31:2011-23
Kaliner E et al. Euro Surveill.
2014;19(7):pii=20703
WHO EURO Collaborative Project with Sweden: “Hard-To-Serve” pophttps://www.fhi.no/globalassets/migrering/dokumenter/pdf/tailoring-immunization-programmes-an-example-from-sweden-.pdfBystrom et al Vaccine 2014;32: 6752-7
14
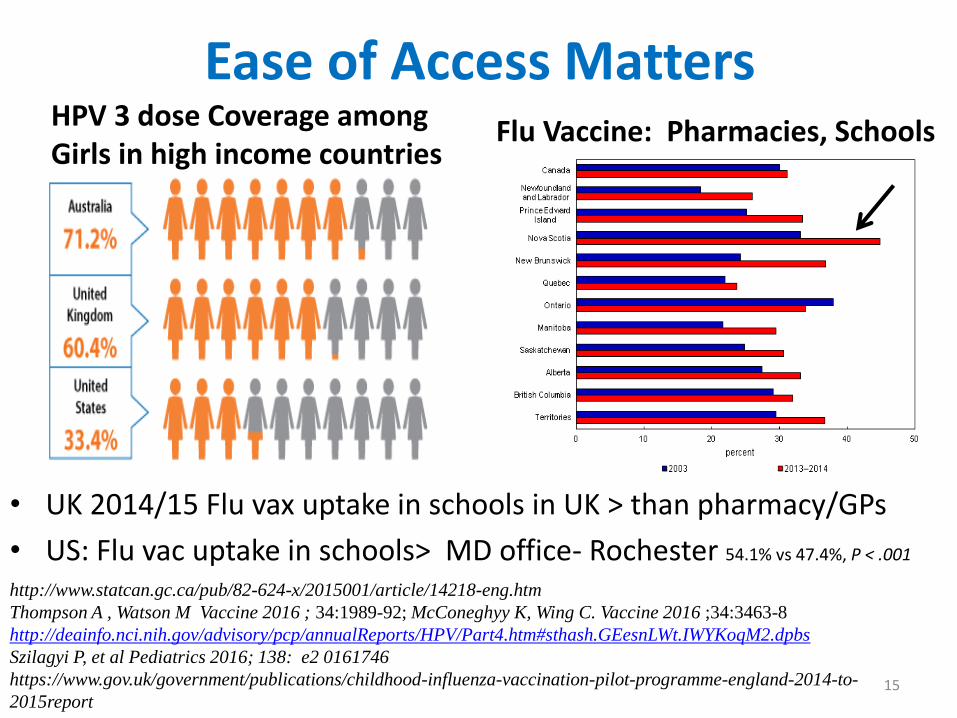
Ease of Access Matters HPV 3 dose Coverage among Girls in high income countries
Flu Vaccine: Pharmacies, Schools
http://www.statcan.gc.ca/pub/82-624-x/2015001/article/14218-eng.htm
Thompson A , Watson M Vaccine 2016 ; 34:1989-92; McConeghyy K, Wing C. Vaccine 2016 ;34:3463-8
http://deainfo.nci.nih.gov/advisory/pcp/annualReports/HPV/Part4.htm#sthash.GEesnLWt.IWYKoqM2.dpbs
Szilagyi P, et al Pediatrics 2016; 138: e2 0161746
https://www.gov.uk/government/publications/childhood-influenza-vaccination-pilot-programme-england-2014-to-
2015report
• UK 2014/15 Flu vax uptake in schools in UK > than pharmacy/GPs
• US: Flu vac uptake in schools> MD office- Rochester 54.1% vs 47.4%, P < .001
15
Reminders Make a Difference Systematic review: effect on 0-5 years imm; adolescents
- postal and telephone reminders help
Work in HIC, MIC, LIC
Text Messages in general practice for flu vax
Seniors
2 min video on pneumococal vaccines email link sent to seniors prior to clinic visit - uptake -
6 mo study: 116- 75% opened message, 64% viewed all
if viewed 3 X uptake
Cameron KA et al 2016 J Gen Int Med 2016; 31 Suppl 2 S174
*
Harvey H, Reissland N, & Mason J. Vaccine2015; 33(25): 2862-2880.SMS infant vax reminder LMIC(Guatamala City ) Domek et al Vaccine 2016; 34: 2437-2443Das JK et al Journal of Adolescent Health 2016; 59:S40eS48
Herret E et al BMJ Open 2016;6:e010069.
16

Mandatory Vaccination and $ Incentives Mandatory Immunization for school entry
Outcome: complex area
US- ↑rates non medical exemptions;
not always lead to high uptake -may backfire
UK- 150 years ago compulsory small pox vaccine: backlash
Canada Ont/ NB – not > imm uptake rates than other provinces no mandatory
Incentives:
HCW: UK -GP imm incentives ↑ uptake; US RCT Peds-no ↑
Patient incentives: sys review – not enough evidence but where done like: Australia
Dubov A, Phung C. Vaccine 2015;33: 2530-35; Salmon DA, et al. Lancet Infect Dis. 2015;15:872-3.
Dube E, MacDonald NE. CMAJ 2016 ;188:E17-8; Hull et al British Journal of General Practice.
2000;50:183-187; Fu LY et al. Pediatrics 2016; 137: e2 0154603Moss et al Pediatrics 2016;138(6): e20161414 ; Wigham et al Peds 2014; 134:e1117–e1128Lee, C., Robinson JL. J Infect 2016 72.6: 659-66.
www.dcclothesline.com
17
4. Effective Communication• Knowledge = Action• Knowledge is important but not = change behaviour• Be proactive NOT just reactive • Communication is a two-way process: listening is key • Choose knowledge to focus on carefully• Target audience- tailor plan to fit • Many communication tools available* Evaluate impact and adjust as need to mantra needs to be: communicate, communicate, and
then communicate some more…..but be sure fit audience targeting
Goldstein S et al Vaccine 2015;33: 4212-4
Shelby A, Ernst K. Hum Vac and Immuno 2013; 9:1795-1801
*Odone et al Hum Vaccin Immunother 2015;11(1):72-82 (review effectiveness new media )
Thompson A , Watson M Vaccine 2016; 34:1989–1992
Know
DoKnow
18

Impact of Vaccine Messages: VariesPro-vaccine messages: work for those +ve about vaccines: important for ↑ resiliencyif –ve about vaccines - not reduce vaccine misperceptions, nor
increase uptake-i.e. “backfire effect” reinforce negative views
Partisans see unfavorably slanted content as even more polarized than it is
Key: test messages in advance; tailor to fit
Nyhan B et al Pediatrics 2014;133; e835-42; Gunther AC et al Comm Res 2012;39: 439-57
Haase et al J Health Comm 2015:20:920-9 Nyhan & Reifler Vaccine 2015;33: 459-64 19
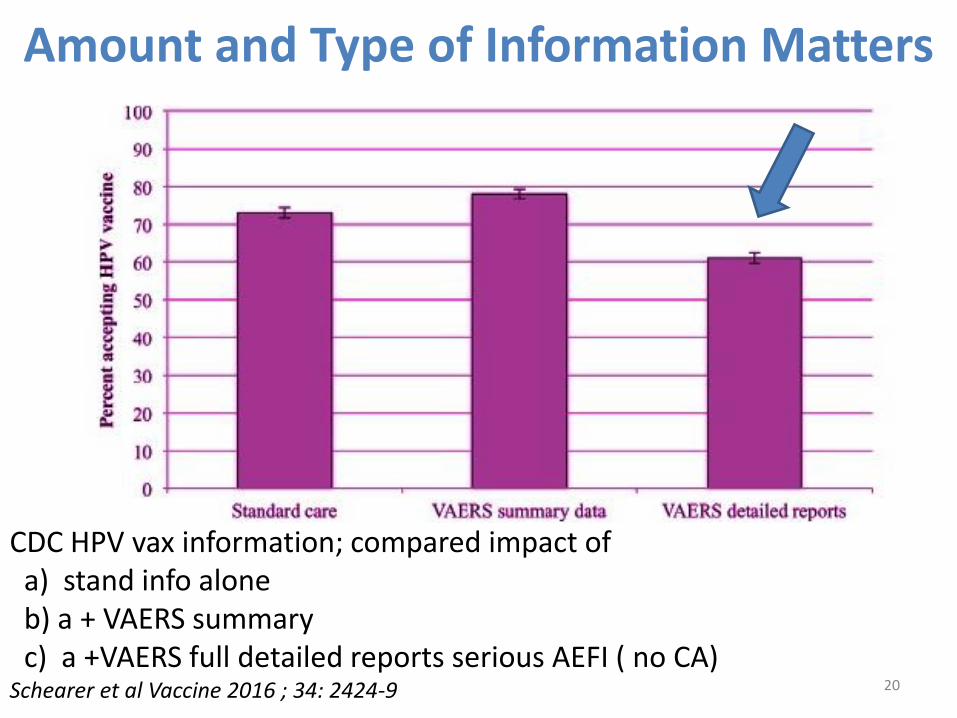
Amount and Type of Information Matters
CDC HPV vax information; compared impact ofa) stand info aloneb) a + VAERS summary c) a +VAERS full detailed reports serious AEFI ( no CA)
Schearer et al Vaccine 2016 ; 34: 2424-9 20
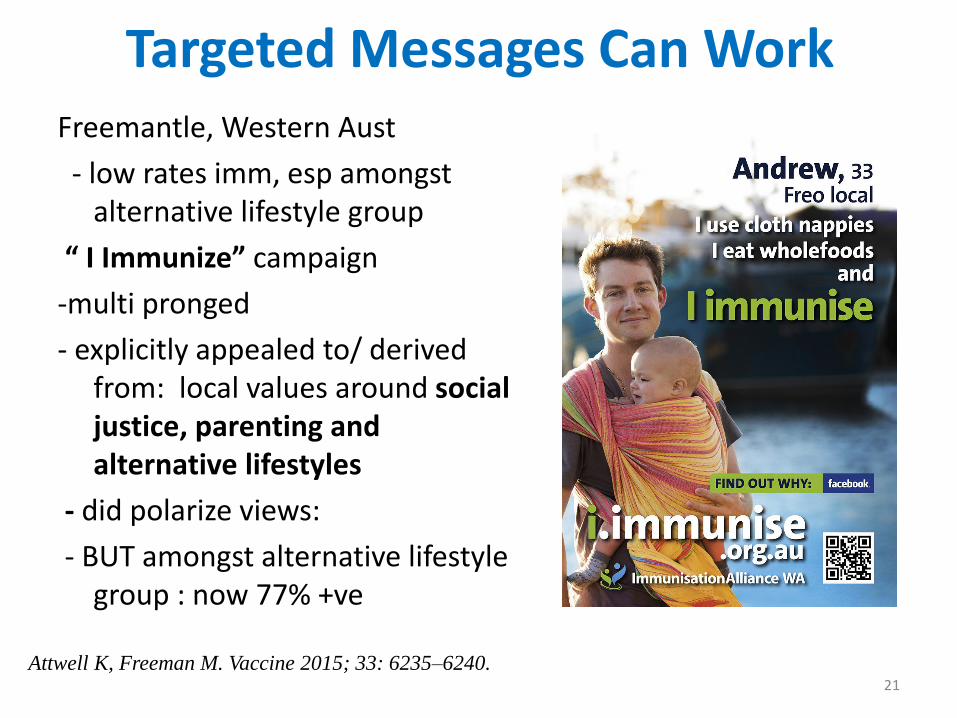
Targeted Messages Can WorkFreemantle, Western Aust
- low rates imm, esp amongst alternative lifestyle group
“ I Immunize” campaign
-multi pronged
- explicitly appealed to/ derived from: local values around social justice, parenting and alternative lifestyles
- did polarize views:
- BUT amongst alternative lifestyle group : now 77% +ve
Attwell K, Freeman M. Vaccine 2015; 33: 6235–6240.21
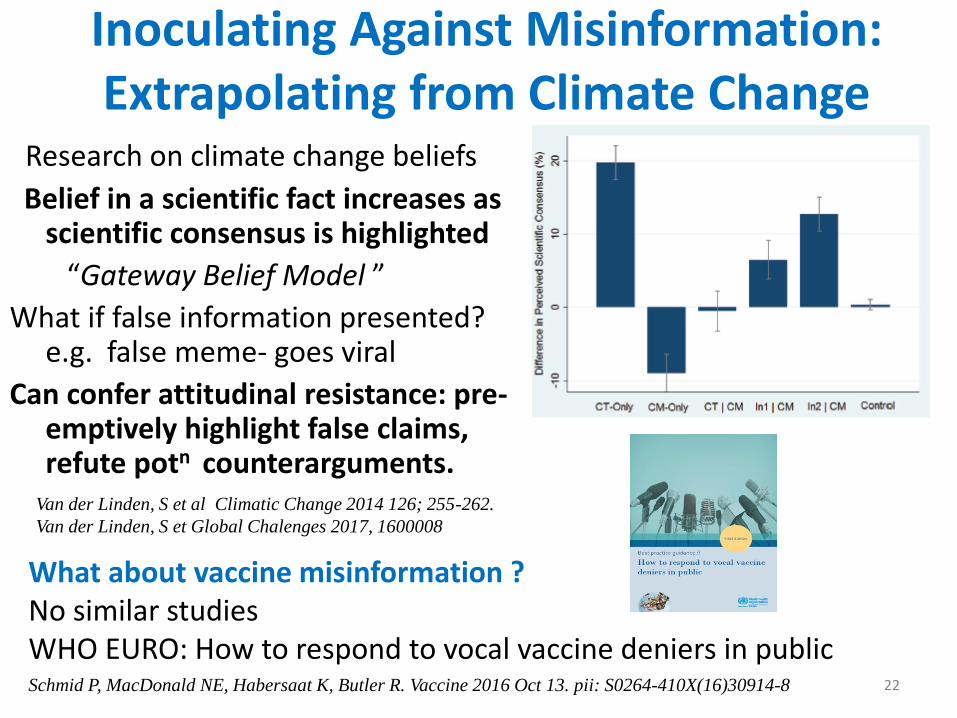
Inoculating Against Misinformation: Extrapolating from Climate Change
Research on climate change beliefs
Belief in a scientific fact increases as scientific consensus is highlighted
“Gateway Belief Model ”
What if false information presented? e.g. false meme- goes viral
Can confer attitudinal resistance: pre-emptively highlight false claims, refute potn counterarguments.
What about vaccine misinformation ? No similar studies WHO EURO: How to respond to vocal vaccine deniers in public
Van der Linden, S et al Climatic Change 2014 126; 255-262.
Van der Linden, S et Global Chalenges 2017, 1600008
22Schmid P, MacDonald NE, Habersaat K, Butler R. Vaccine 2016 Oct 13. pii: S0264-410X(16)30914-8

5. Shape Children’s Beliefs on
Vaccine Necessity, Benefits, Safety
Start early:
• Primary: what vaccines are, why needed, benefits, safety
• Secondary: weave into history, science and health
• Engage expert teachers and students - many resources
• Denmark- CPN – developing curriculum
• Canada -Ontario has included child and youth vacedu in 2020 Imm plan
Teachers Kit, National Immunization Poster Contest in Canada .
http://www.immunize.cpha.ca/en/events/imm-poster-contest.aspx
Opel D, Marcuse E. Human Vaccines & Immunotherapeutics 2013;9:2672–2673
http://www.health.gov.on.ca/en/common/ministry/publications/reports/immunization_2020/immunizati
on_2020_report.pdf
Nowak G, Gellin B, MacDonald NE, Butler R et al Vaccine 2015; 33: 4204–4211 23

6. Work Collaboratively Partnership: Key Asset
National immunization program
Public health
Academia
HCPs
HCP societies
Manufacturers *
Civil Society Organizations
Global agencies
Private Sector
NGOs
Shared objectives:
(i) communicate proactively on immunization,
(ii) prepare for issues that may arise
(iii) Understand challenges better through existing and future research
Thompson A , Watson M. Vaccine 2016; 34 :1989–92
saves time, resources, adds voice,
enhances credibility health worker vaccine message
24

7.Key Role HCP in Vaccine Acceptance; “For all vaccines, the attitude of the physician ……is very
influential in the decision to vaccinate a child…..”Favin et al . International Health 2012; 4:229-238
Suryadevara M et al Vaccine 2015; 33: 6629–6634.
Parents received vaccine information from MDs: < vac concerns vs from friends/family/books
Wheeler M, Buttenheim A. Human Vaccines & Immunotherapeutics2013; 9:1782–1789
Witteman HO. Addressing vaccine hesitancy with values Pediatrics 2015;136 :215-7
HCP information or assurances - main reason why parents who planned to delay or refuse a vaccine for their child changed their minds
Gust, D.A., et al., Parents with doubts about vaccines: which vaccines and reasons why. Pediatrics, 2008. 122(4): p. 718-25
Mother’s lack of uptake of flu vaccination in pregnancy
predicts infant immunization
25Fuchs EL. Self-reported prenatal influenza vaccination and early childhood vaccine series completion Prev Med 2016;88: 8-12
8.Vaccine Refusers and Hesitant Refusers: • Do Not dismiss • Build trust – caring and
competence • Not debate• Maybe able to determine
concerns with “ what would it take to move you to a yes to accept vaccines?
• Responsibilities for refusers WHO EURO
• Consider referral to “expert”
Hesitant:• Determine basis of hesitancy
– do not assume• Do not over estimate
parental concerns• Listen and listen • Tailor response to concerns
http://www.euro.who.int/en/health-topics/disease-prevention/vaccines-and-immunization/publications/2012/if-you-choose-not-to-vaccinate-your-child,-understand-the-risks-and-responsibilitiesHealyCM, Montesinos DP, Middleman AB. Vaccine
2014: 23;32(5):579-84Halperin B, Melnychuk R, Downie J, Macdonald N.
Paediatr Child Health 2007;12(10):843-5.
26
27
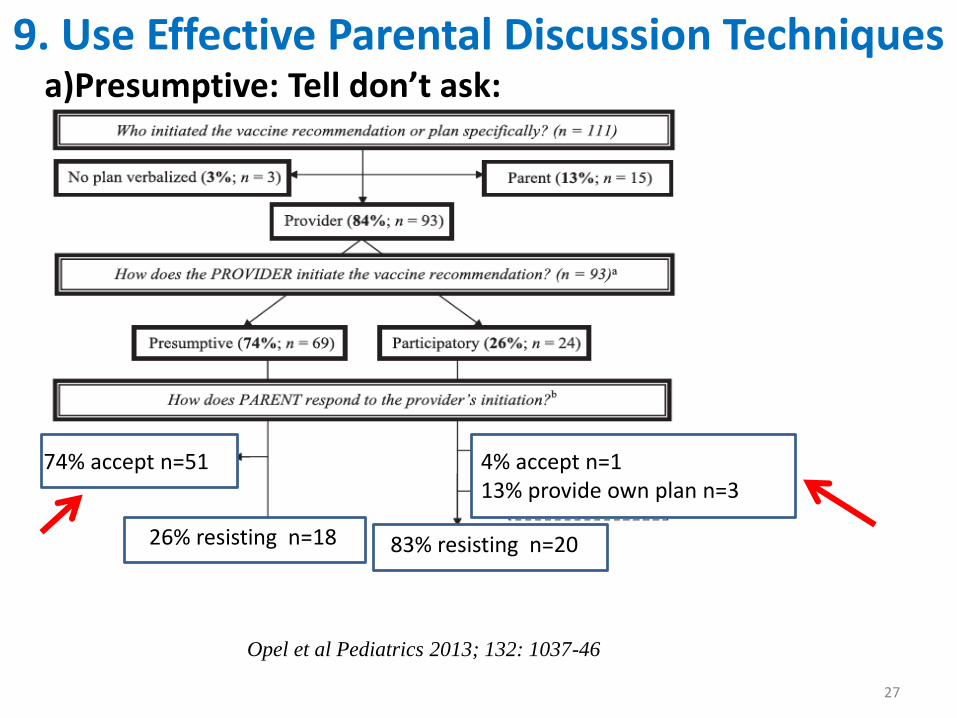
9. Use Effective Parental Discussion Techniquesa)Presumptive: Tell don’t ask:
Opel et al Pediatrics 2013; 132: 1037-46
74% accept n=51 4% accept n=113% provide own plan n=3
83% resisting n=2026% resisting n=18

28
9. Use Effective Parental Discussion Techniques
•client centred, semi-directive, aimed at changing behaviour•shift from •TALKING TO → WORKING WITH
“ What would it take to move you to a yes to accept vaccines?”
Tailor discussion to fit concerns
Healey CM and Pickering L. Pediatrics 2011;127: S127–S133
Leask et al. BMC Pediatrics 2012, 12:154
Open ended questions
• What do you think about vaccines?
Affirmation • I understand
Listen reflectively
• You are concerned by
Summarize • Let me summarize
b) Address Concerns : Motivational Interviewing

10. Use Effective Clear Language1. Standard vocabulary
2. Consistent denominator
3. Present risks/benefits
fairly: tell truth
4. Explain single event
probability (rain,not
rain) visual aides
5. Absolute numbers not relative risk or %
6. Frame your message *
7. Avoid using jargon **
1000 Children
Tetanus 10% die even with ICU care = 100 in 1000MacDonald NE et al. Help with Vaccine Hesitant Parents; an Update. Paediatrics & Child Health in press
Data graphics HPV & vaccine: www.informationisbeautiful.net/2011/is-the-hpv-vaccine-safe-v-2-0/
Peters, E.,Bjalkebring. 2015. J Pers Soc Psychol 108.5: 802-22 29
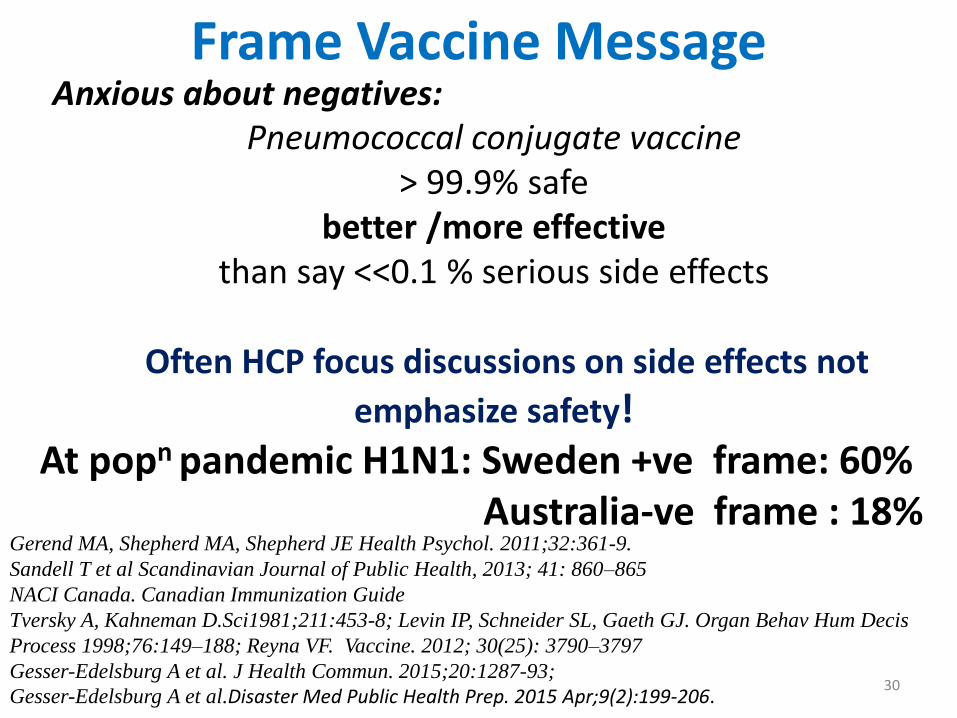
Frame Vaccine Message Anxious about negatives:
Pneumococcal conjugate vaccine > 99.9% safe
better /more effectivethan say <<0.1 % serious side effects
Often HCP focus discussions on side effects not
emphasize safety!At popn pandemic H1N1: Sweden +ve frame: 60%
Australia-ve frame : 18%Gerend MA, Shepherd MA, Shepherd JE Health Psychol. 2011;32:361-9.
Sandell T et al Scandinavian Journal of Public Health, 2013; 41: 860–865
NACI Canada. Canadian Immunization Guide
Tversky A, Kahneman D.Sci1981;211:453-8; Levin IP, Schneider SL, Gaeth GJ. Organ Behav Hum Decis
Process 1998;76:149–188; Reyna VF. Vaccine. 2012; 30(25): 3790–3797
Gesser-Edelsburg A et al. J Health Commun. 2015;20:1287-93;
Gesser-Edelsburg A et al.Disaster Med Public Health Prep. 2015 Apr;9(2):199-206.30

Focus on Gist Communication ( Fuzzy Trace Theory)
Evidence based fact or Statistic
Scripted phase Bottom line meaning
Verbatim Explicit Link GIST
Establishes credibility and expertise
Connects verbatim with GIST
Helps comprehension and recall
eg And the reason that’s important is…What that means to you is… So the thing to remember is… Bottom line -what I tell patients is……
Broniatowski D et al. Vaccine 2016; 34: 3225–3228 31
11. Present Concept:Community Protection/ImmunityNot use Jargon: Herd Immunity
https://www.ted.com/talks/romina_libster_the_power_of_herd_immunityBroniatowski DA, Hilyard KM, Dredze M.Vaccine. 2016;34(28):3225-8
32
• Reinforcing added value community immunity helpful
US in 2015 – first measles death in 12 years in
immunocompromised patient
• BUT: not at expense note personal benefit
not all VPD preventable with this e.g. tetanus
• Jargon: can be a problem
“ herd Immunity”
http://www.doh.wa.gov/Newsroom/2015NewsReleases/15119WAMeaslesRelatedDeath
12. Address Pain Mitigation 2015 Canadian Pain Guidelines ( GRADE):
HELPinKids&Adults
- Covers age range: neonates to adults
- Updated & new evidence, twice as many interventions assessed vs 2010
- Rotavirus vaccine-many have high sucrose content –study show benefit give just before injection vaccines
- Breast feeding during the injection
- Give most painful vax last ** need help - manufacturers
Taddio et al CMAJ 2015; 187:975-982.
WHO : Report to SAGE on Reducing pain and distress at the time of vaccination. ( reviewed using AGREE)http://www.who.int/immunization/sage/meetings/2015/april/1_SAGE_latest_pain_guidelines_
March_24_Final.pdf
www.youtube.com/watch?v=KgBwVSYqfps
33
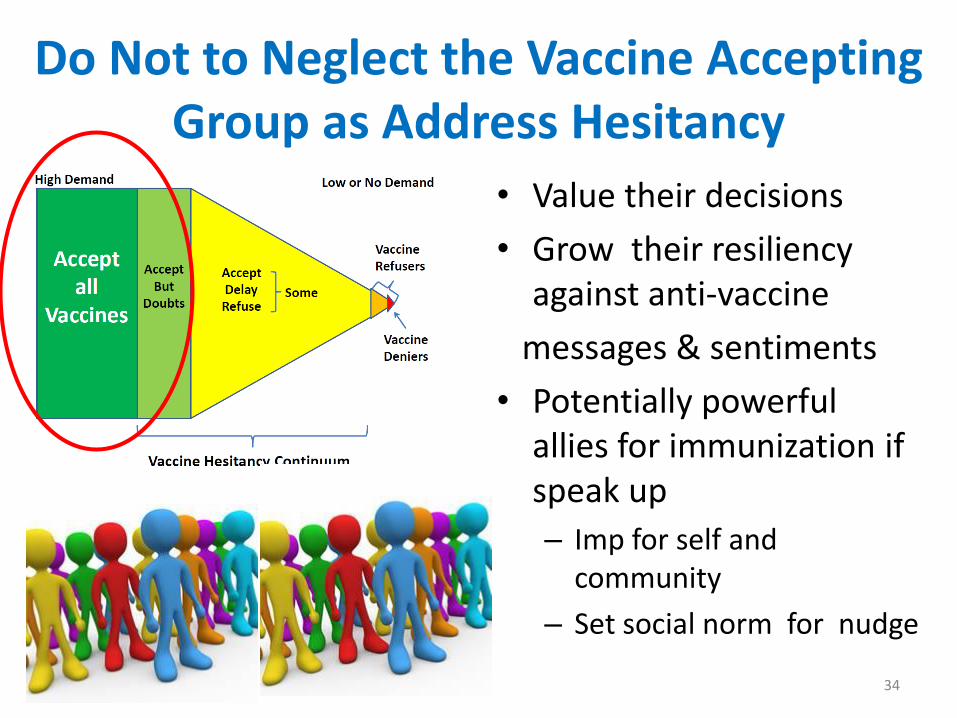
Do Not to Neglect the Vaccine Accepting Group as Address Hesitancy
• Value their decisions
• Grow their resiliency against anti-vaccine
messages & sentiments
• Potentially powerful allies for immunization if speak up
– Imp for self and community
– Set social norm for nudge
34