valvular heart disease eric j milie, d.o.. goals and objectives recognize which cardiac murmurs...
TRANSCRIPT
Valvular Heart Disease
Eric J Milie, D.O.
Goals and Objectives
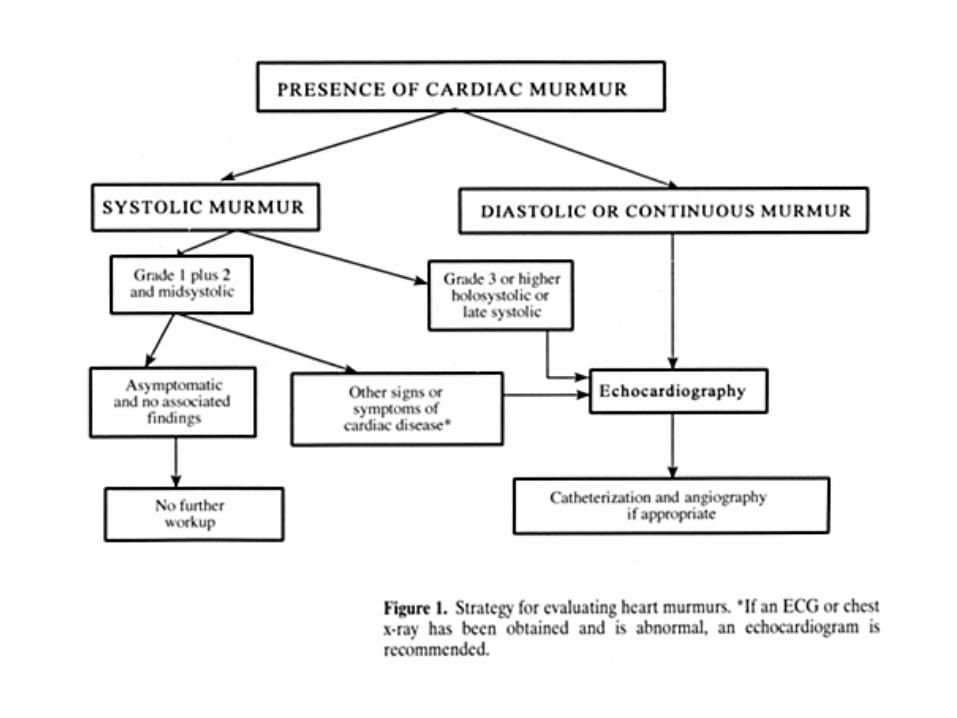
Recognize which cardiac murmurs warrant further evaluationUnderstand three cardinal signs of aortic stenosis and indications for surgical interventionOutline treatment plans for specific valvular heart lesions
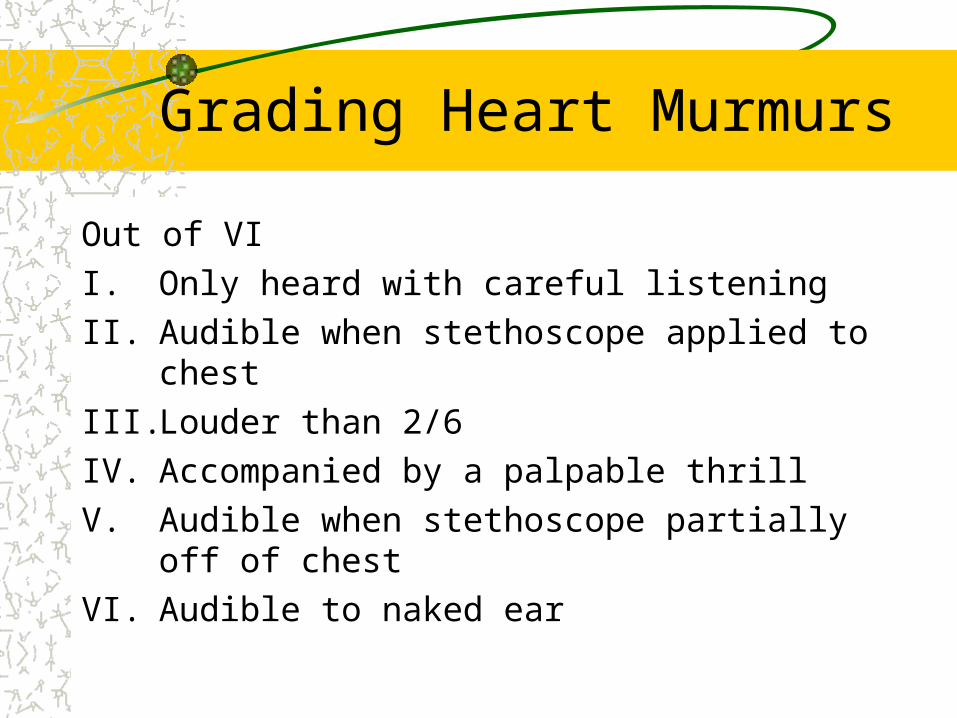
Grading Heart Murmurs
Out of VII. Only heard with careful listeningII. Audible when stethoscope applied to chestIII. Louder than 2/6IV. Accompanied by a palpable thrillV. Audible when stethoscope partially off of chestVI. Audible to naked ear
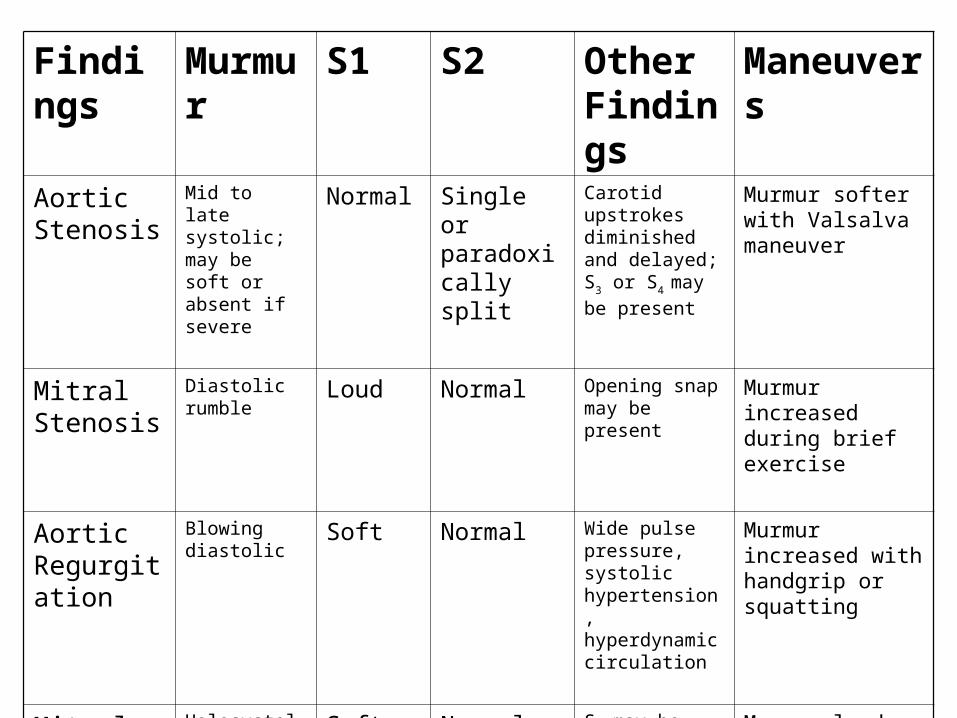
Findings Murmur S1 S2 Other Findings
Maneuvers
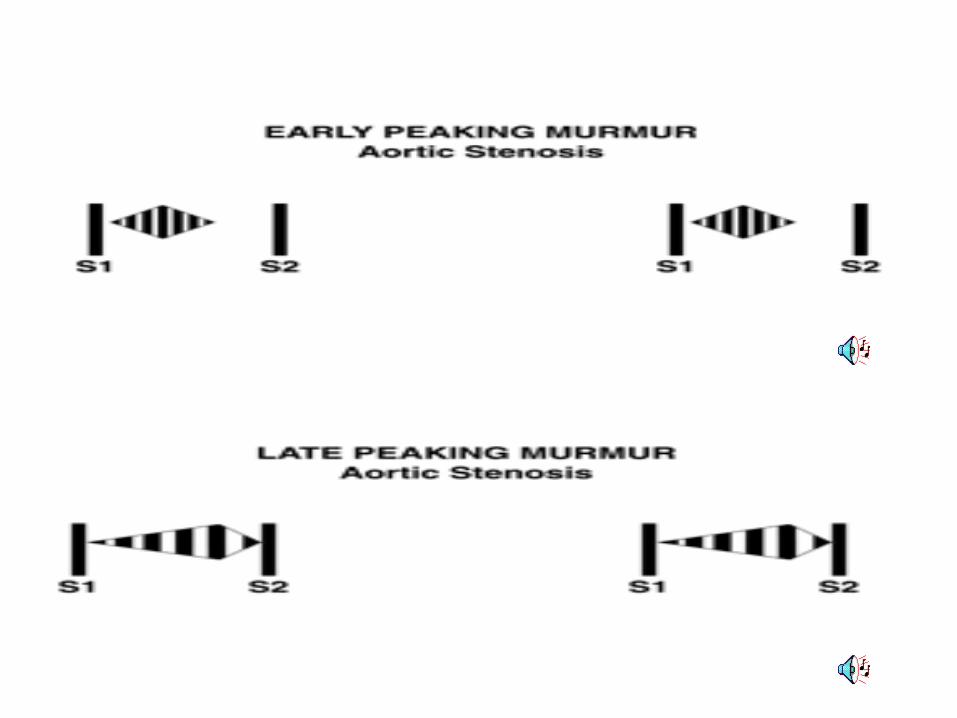
Aortic Stenosis
Mid to late systolic; may be soft or absent if severe
Normal Single or paradoxically split
Carotid upstrokes diminished and delayed; S3 or S4
may be present
Murmur softer with Valsalva maneuver
Mitral Stenosis
Diastolic rumble Loud Normal Opening snap may be present
Murmur increased during brief exercise
Aortic Regurgitation
Blowing diastolic Soft Normal Wide pulse pressure, systolic hypertension, hyperdynamic circulation
Murmur increased with handgrip or squatting
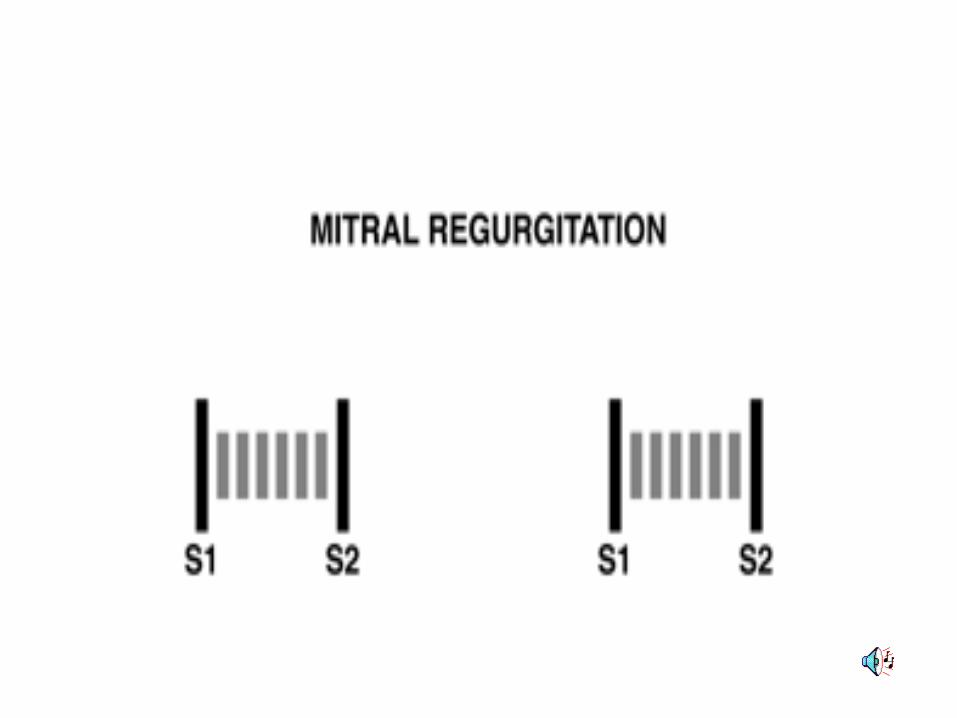
Mitral Regurgitation
Holosystolic Soft Normal or split
S3 may be present; cartoid upstrokes brisk
Murmur louder with Valsalva maneuver
MVP Mid to late systolic
Normal Normal Mid-systolic click Murmur increased with standing
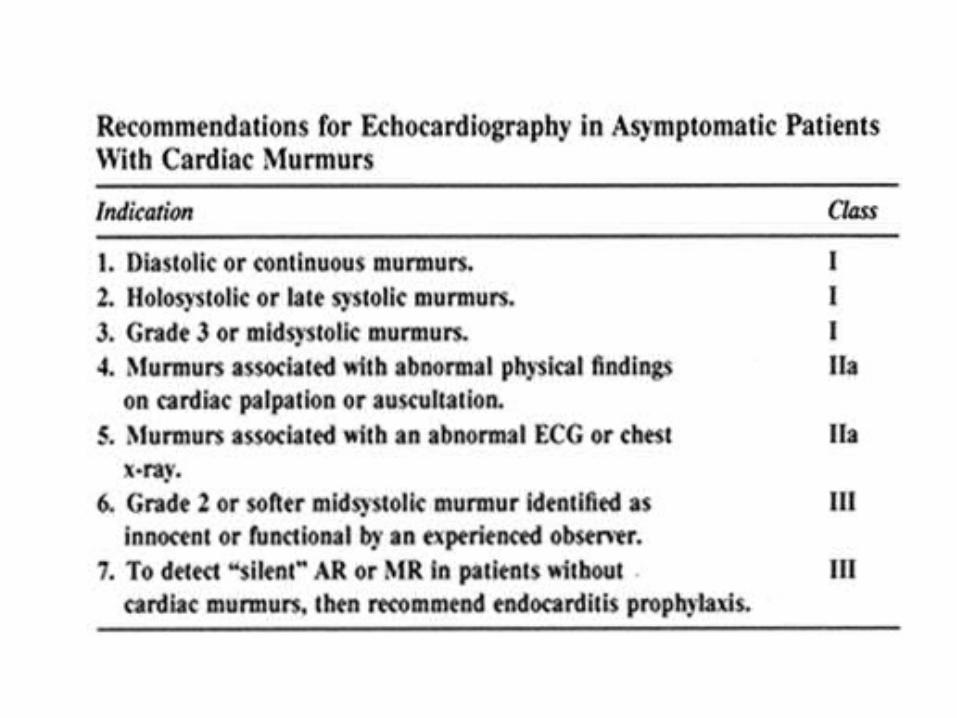
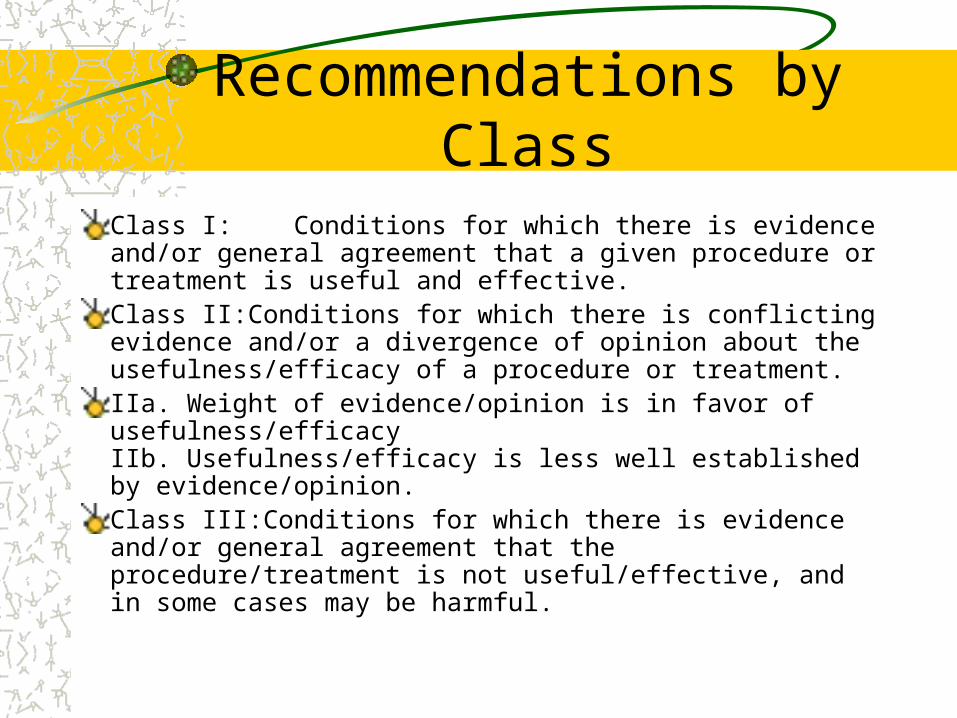
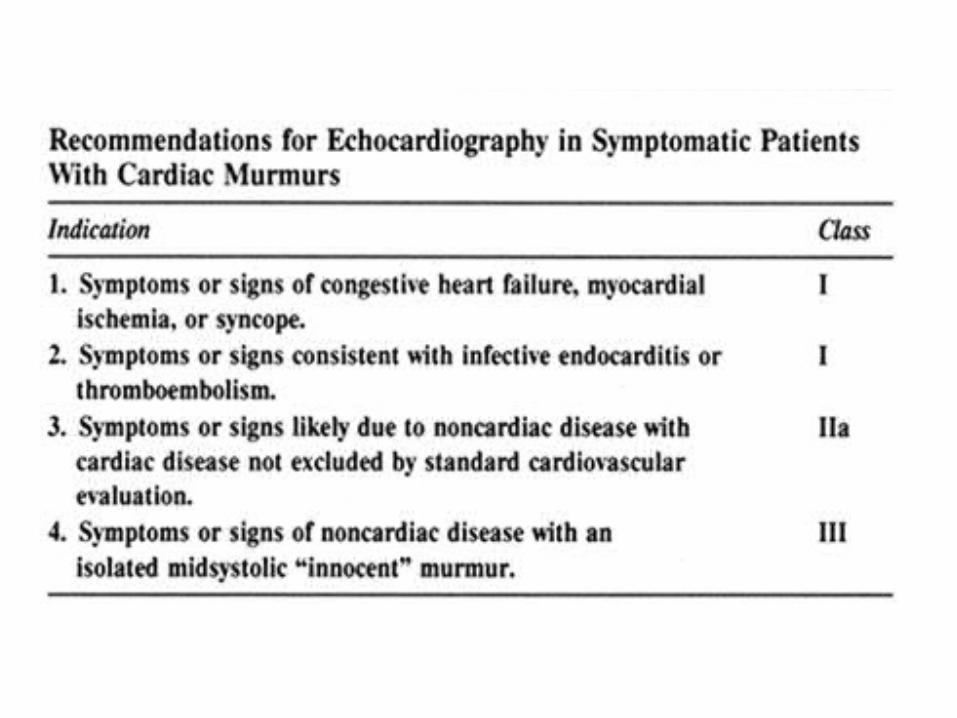
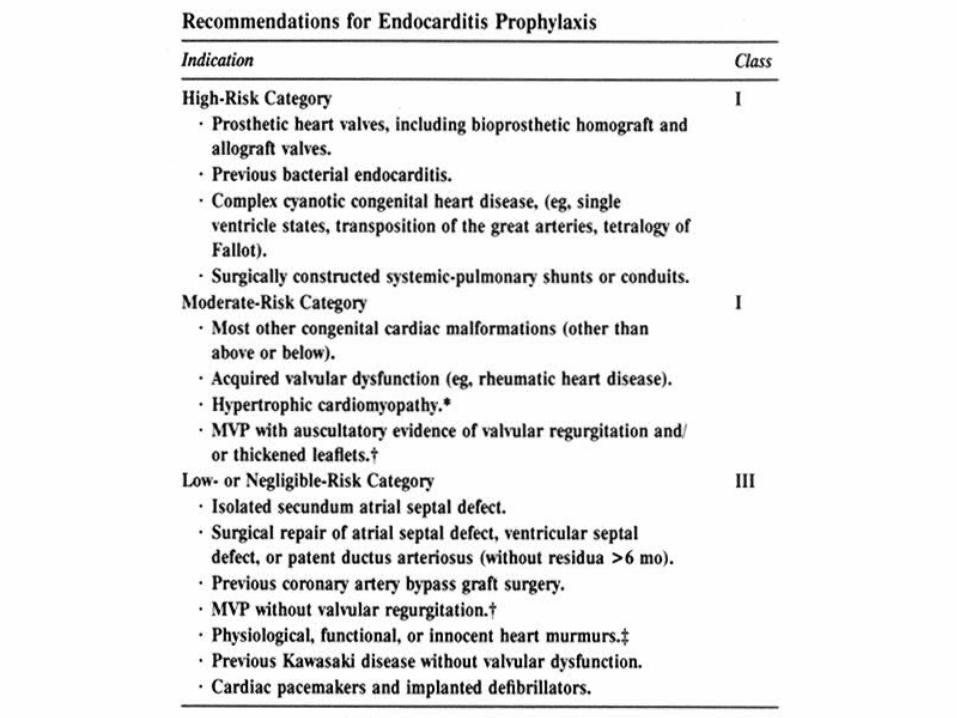
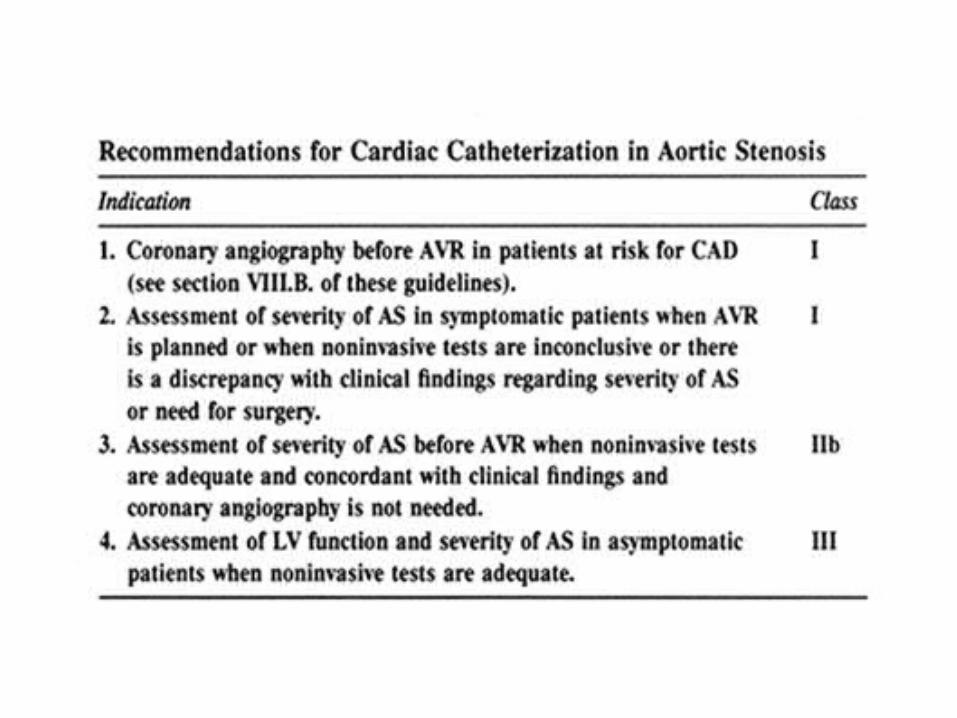
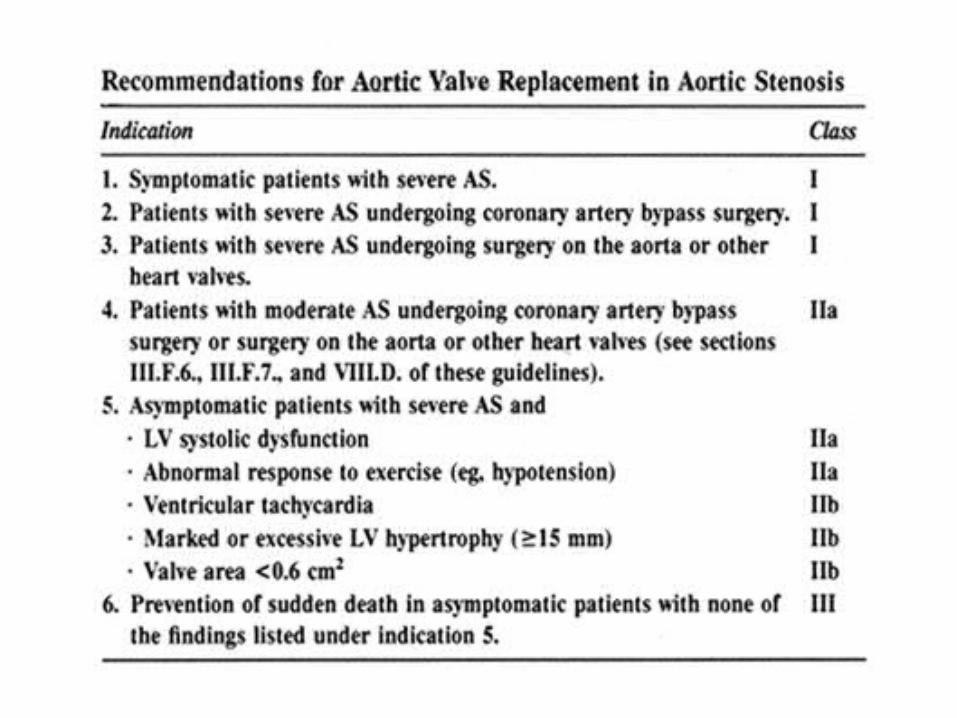
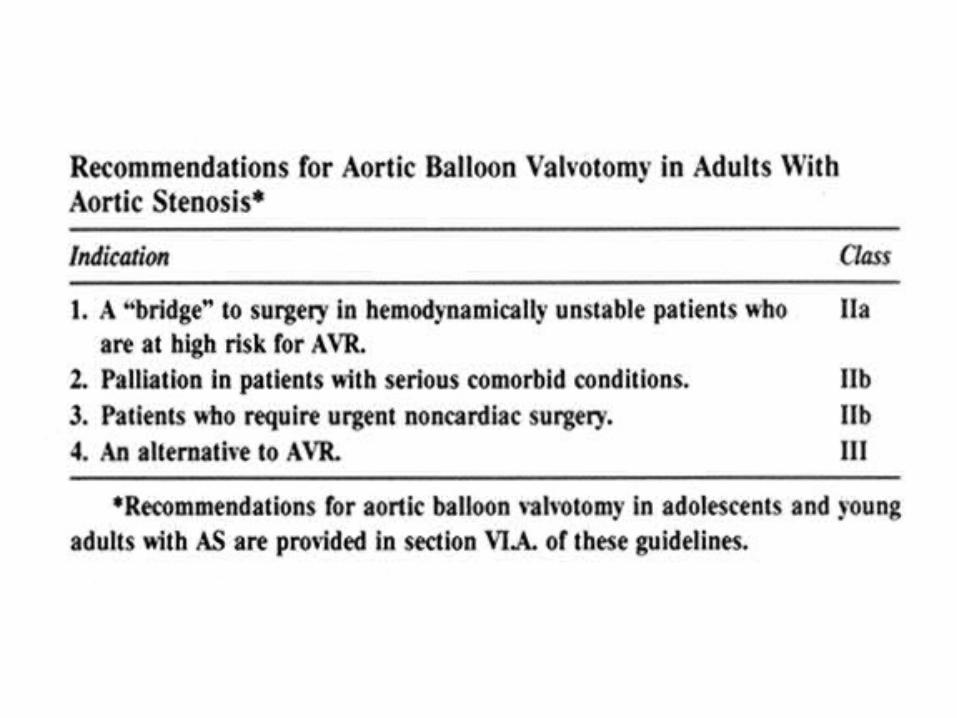
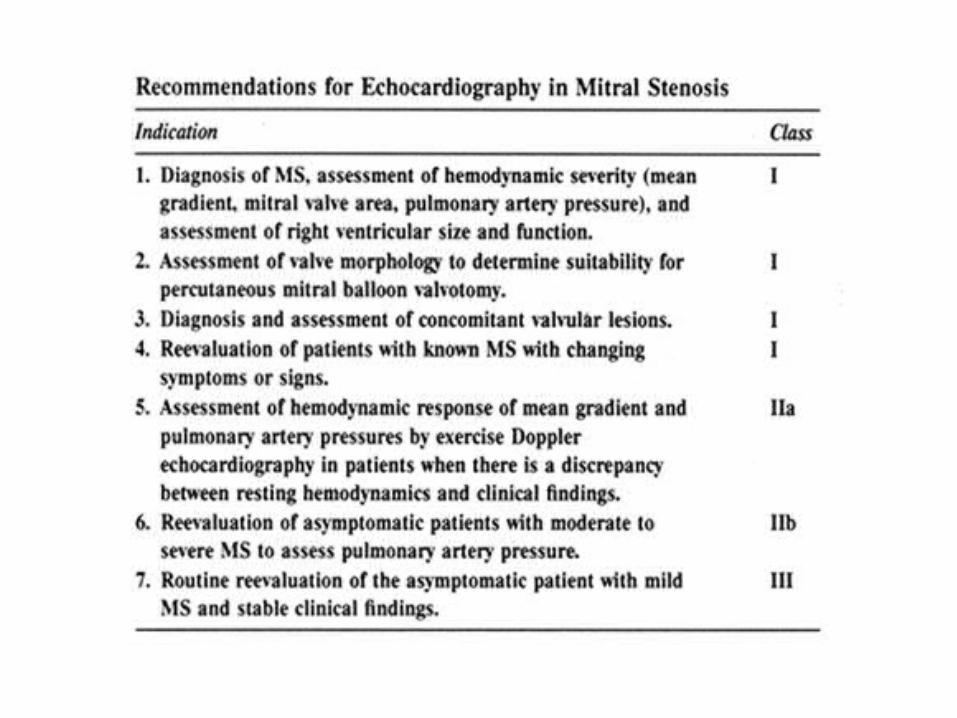
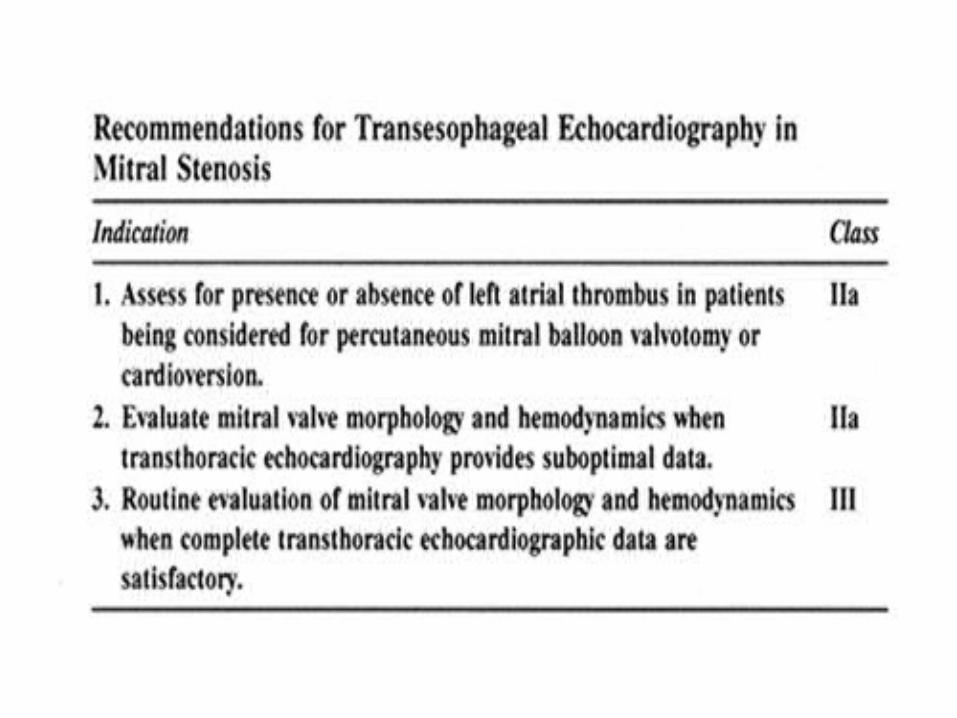
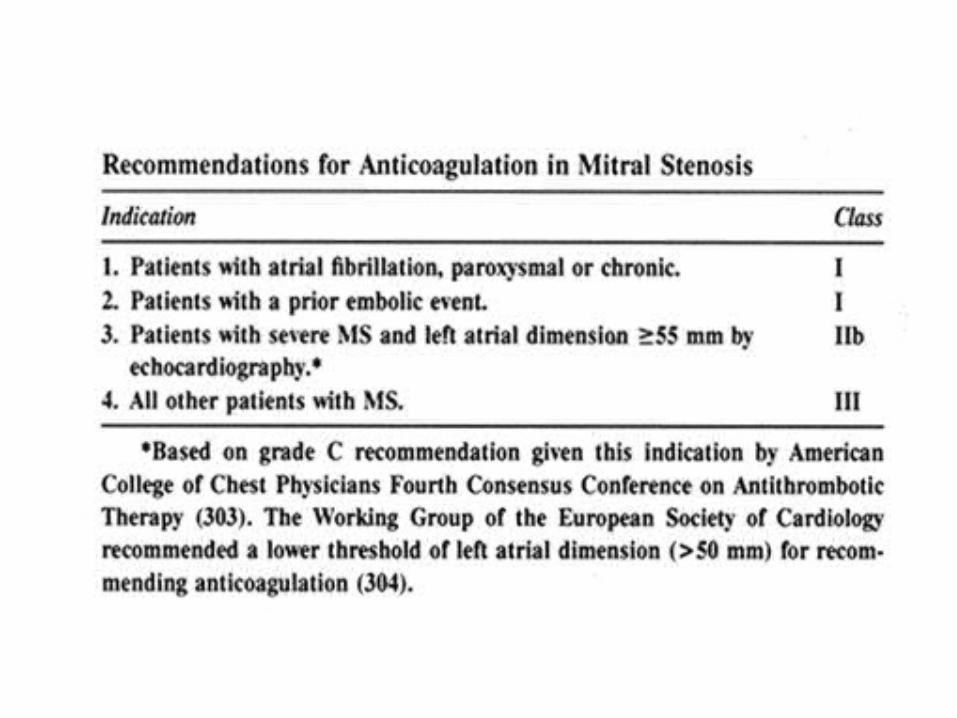
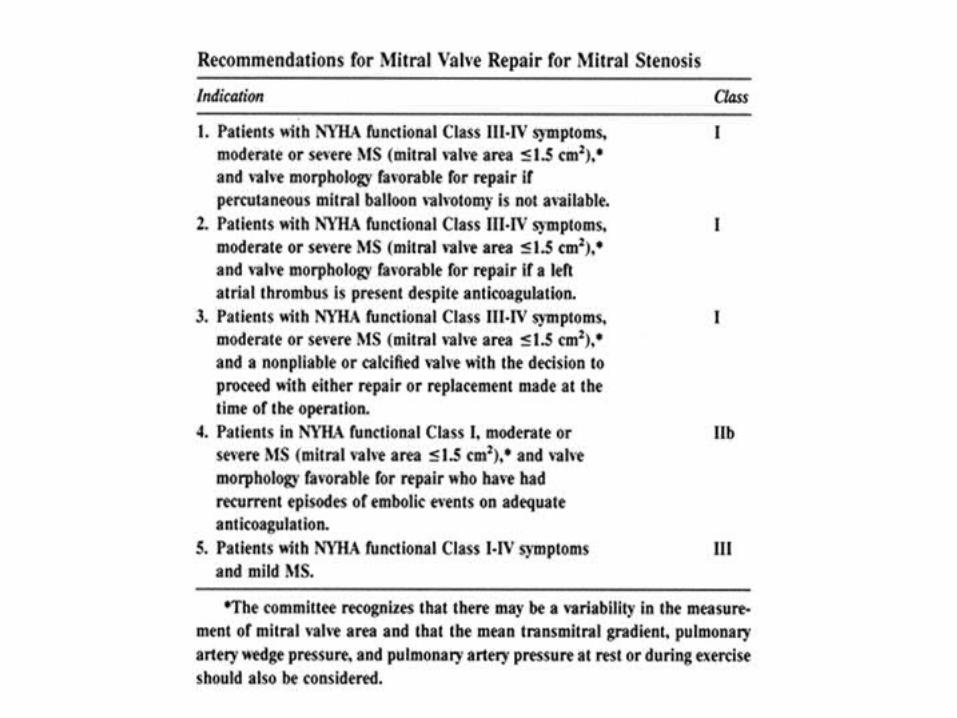
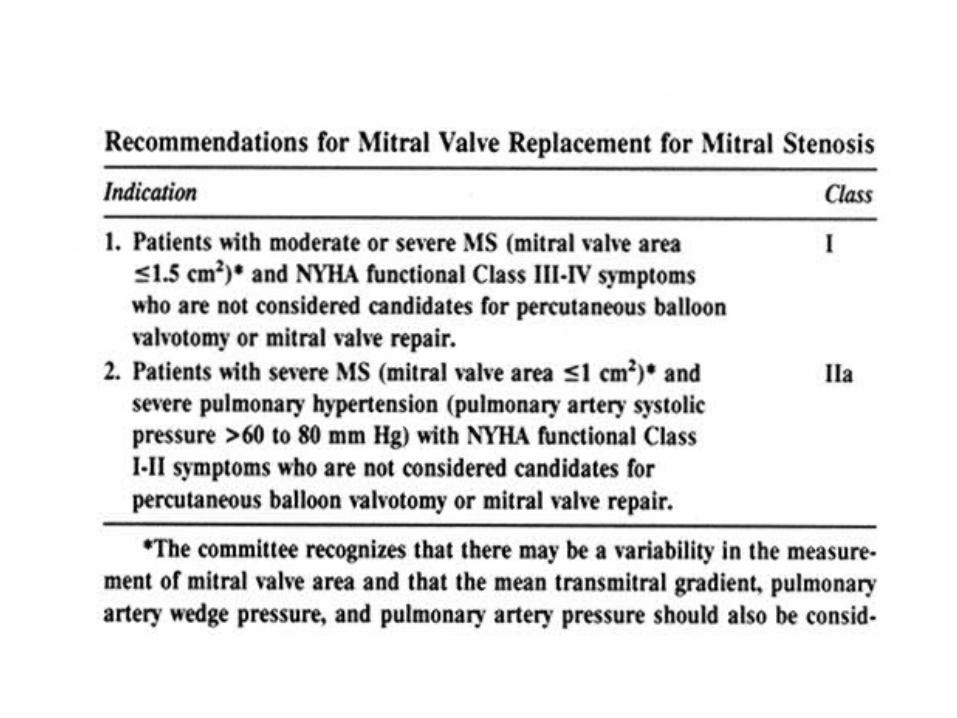
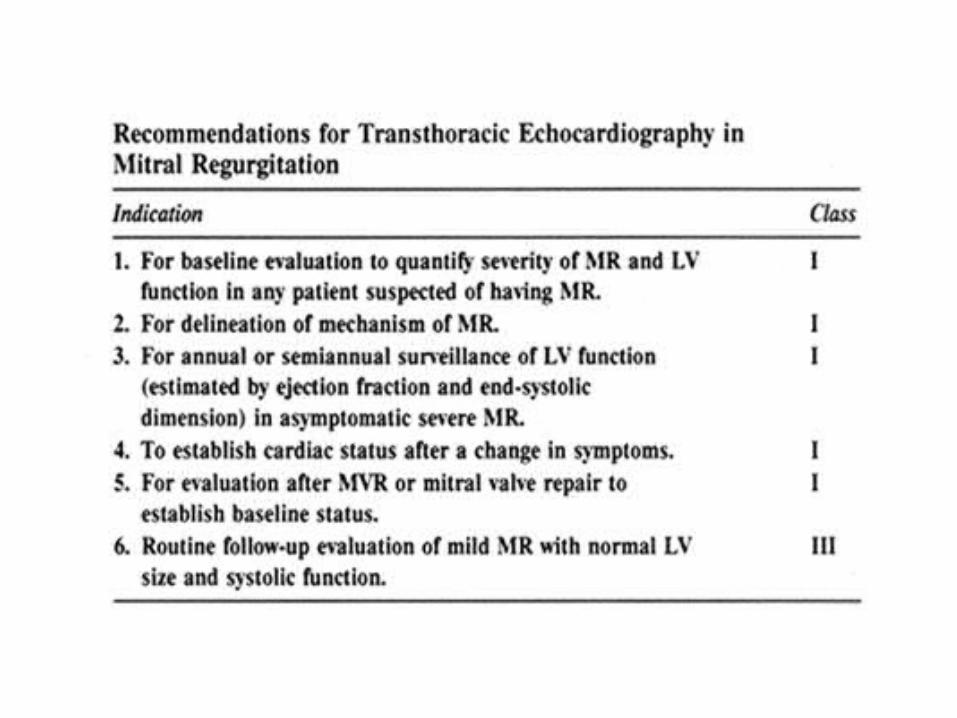
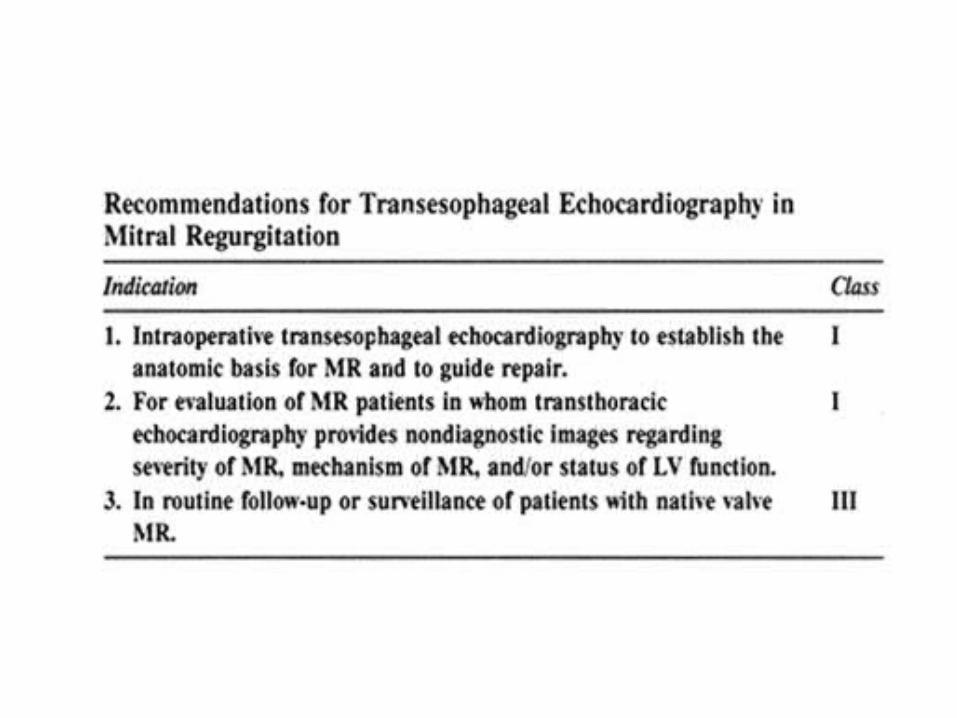
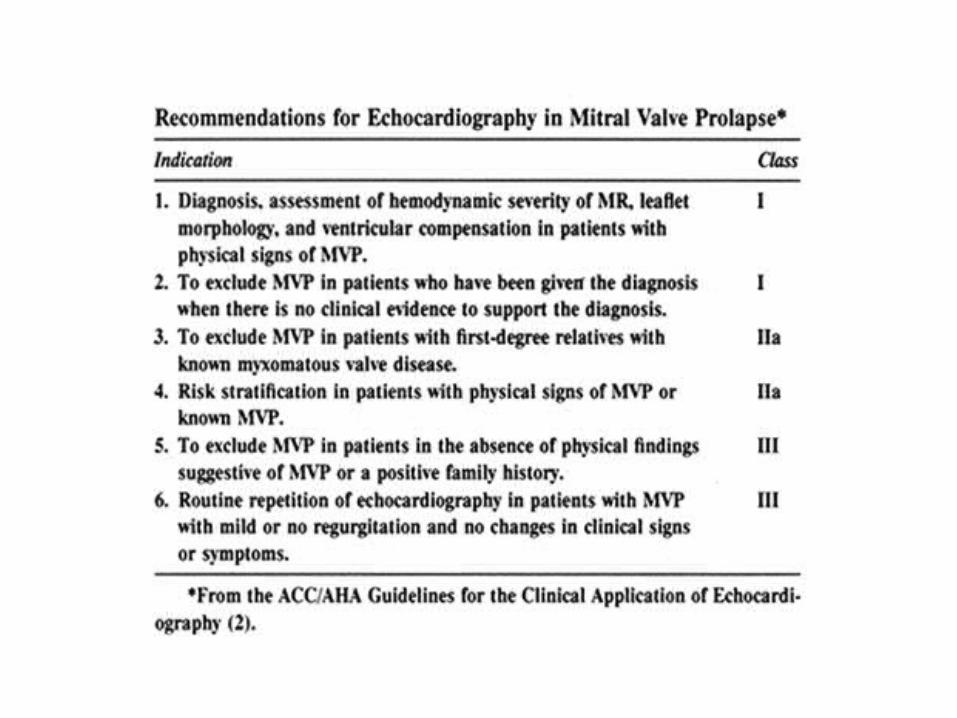
Recommendations by Class
Class I: Conditions for which there is evidence and/or general agreement that a given procedure or treatment is useful and effective. Class II:Conditions for which there is conflicting evidence and/or a divergence of opinion about the usefulness/efficacy of a procedure or treatment. IIa. Weight of evidence/opinion is in favor of usefulness/efficacyIIb. Usefulness/efficacy is less well established by evidence/opinion. Class III:Conditions for which there is evidence and/or general agreement that the procedure/treatment is not useful/effective, and in some cases may be harmful.
Aortic Stenosis: Etiology
Often congenitalRheumatic AS associated with previous rheumatic diseaseIdiopathic, calcific As associated with elderly, generally milder
AS: Symptoms
DyspneaAnginaSyncope
These are cardinal symptoms, occur late in disease, and are associated with mortality (usually 2-3 year survival after onset of symptoms)
AS: Physical Exam
Weak and delayed arterial pulses with carotid thrill (pulsus parvus et tardus)Double apical impulseS4 commonDiamond shaped systolic murmurUsually >3/6
AS: Echo
LV thickeningThickening and calcification of aortic valve cuspsDilatation, reduced LVEF poor prognosis

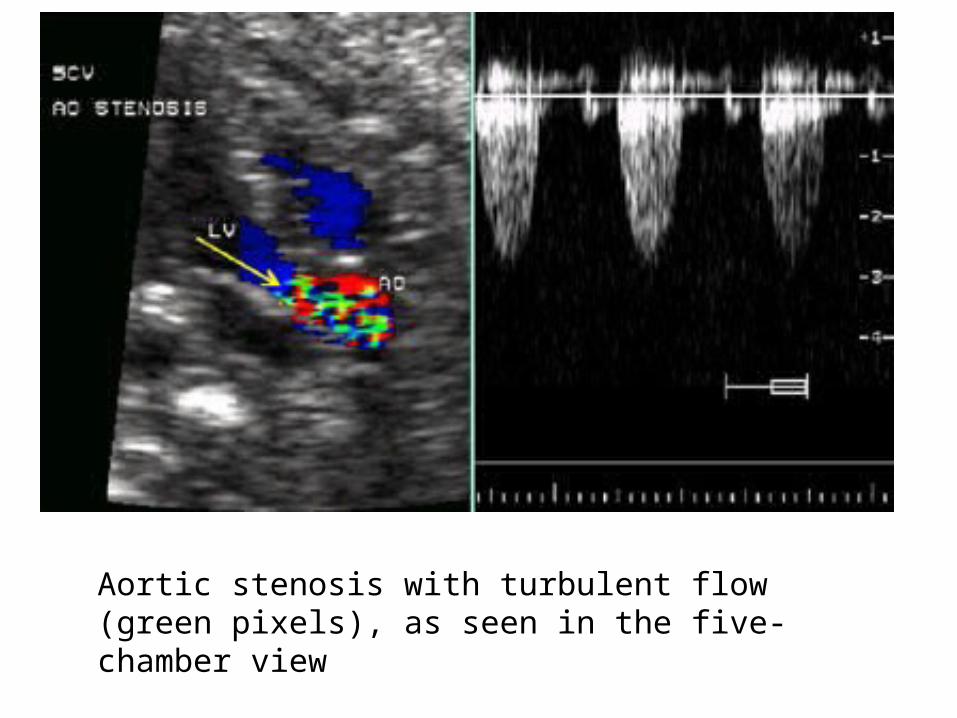
Aortic stenosis with turbulent flow (green pixels), as seen in the five-chamber view
AS: Classification of Severity
Mild: Valve Area >1.5cm²Moderate: Valve area 1.0cm² to 1.5cm²Severe: Valve area <1.0cm²
AS: Treatment
Avoid strenuous exercise in severe ASTreat CHF in standard fashion, but avoid afterload reductionStatin therapy to slow progression of leaflet calcificationBalloon valvotomy to reduce symptoms in patients who aren’t surgical candidatesValve replacement in adults who are symptomatic or with evidence of outflow obstructionSurgery optimally performed before frank heart failure develops
Aortic Regurgitation: Etiology
Rheumatic etiology commonHypertensionInfective endocarditisDilitation due to cystic medial necrosisMyxomatous infiltrationMarfan syndromePatients ¾ male
AR: Manifestations
Exertional dyspneaCardiac awarenessAnginaLV failureWide pulse pressureCapillary pulsations (Quincke’s sign)S3Blowing, decrescendo diastolic murmur heard best along left sternal border

AR: Lab
CXR- LV enlargementEKG- LV hypertrophyEcho: LA and LV enlarged, increased excursion of LV posterior wall
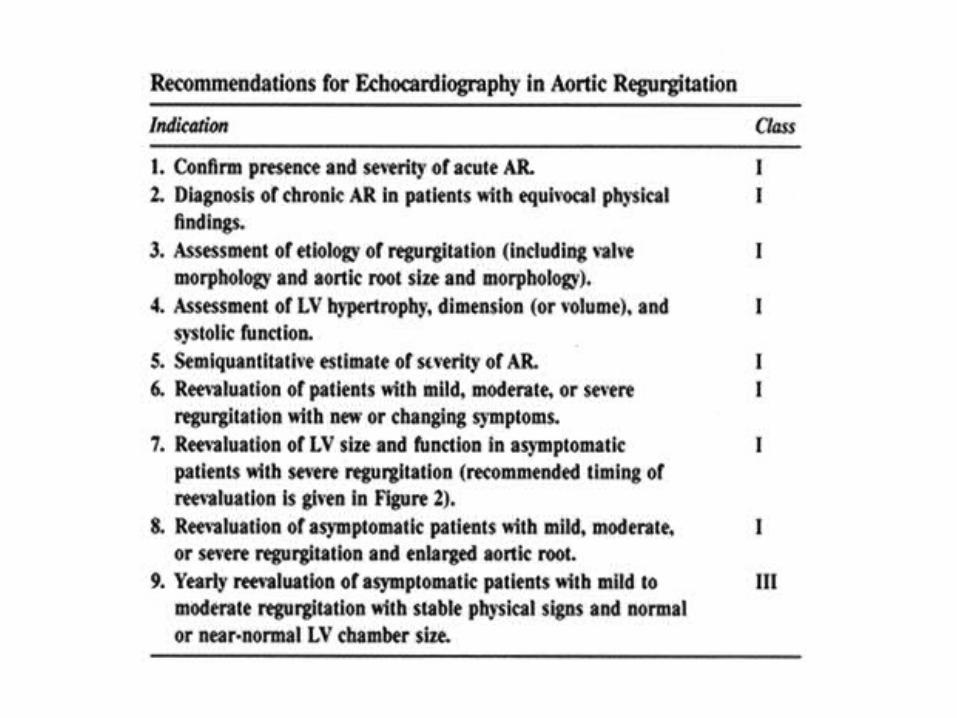
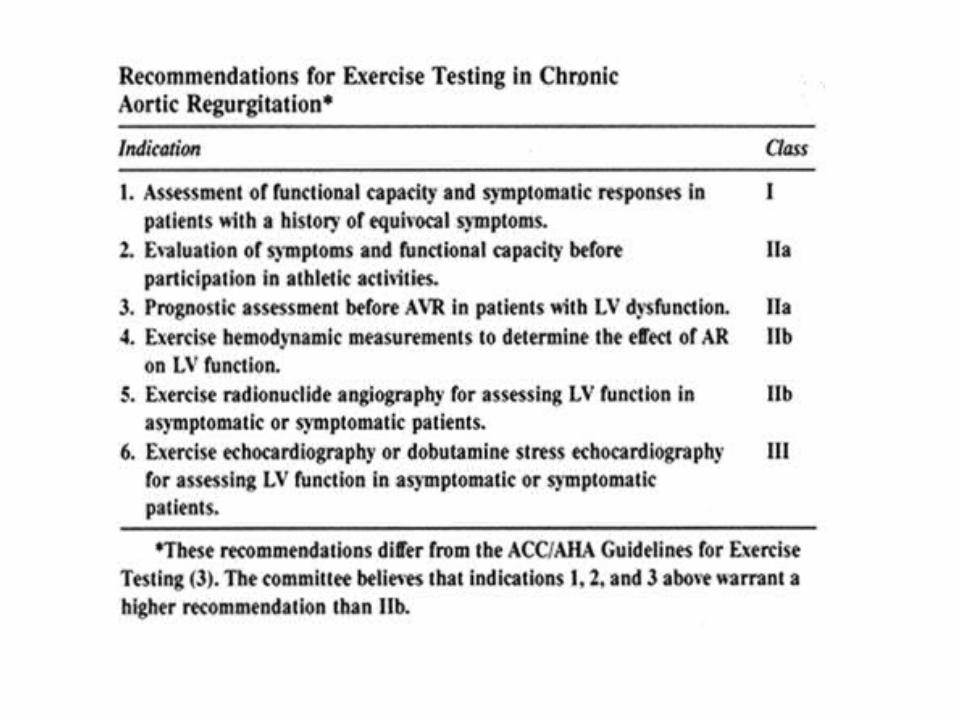

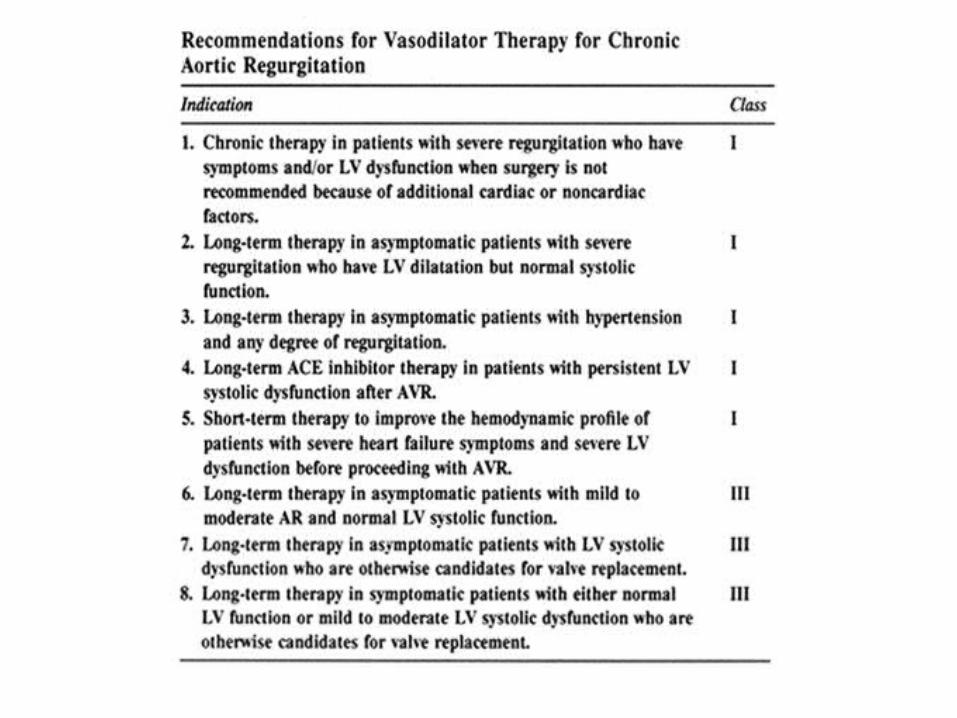
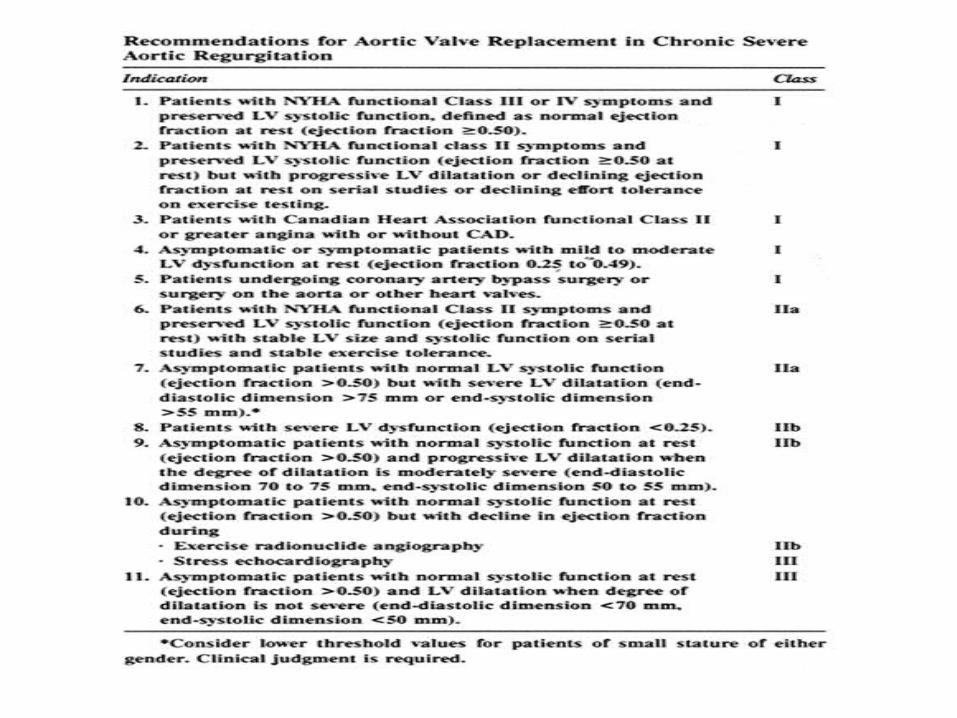
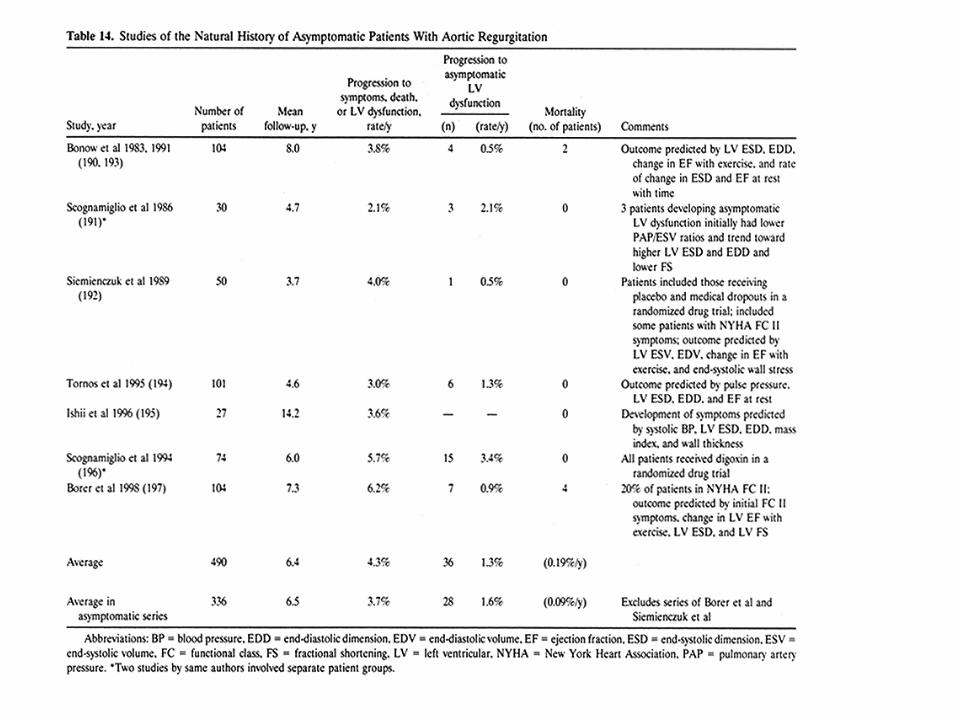
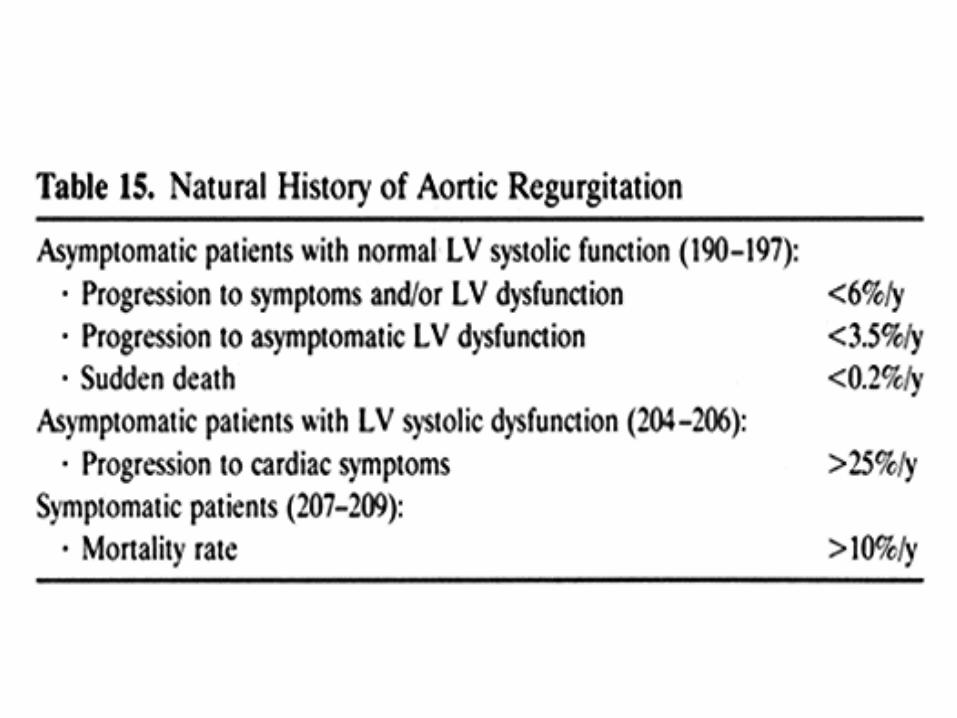
AR: Treatment
Standard therapy for LV failureVasodilators to delay need for surgical interventionSurgical intervention indicated in symptomatic patients with severe AR or in asymptomatic patients with LV dysfunction on echo (LVEF <55%)
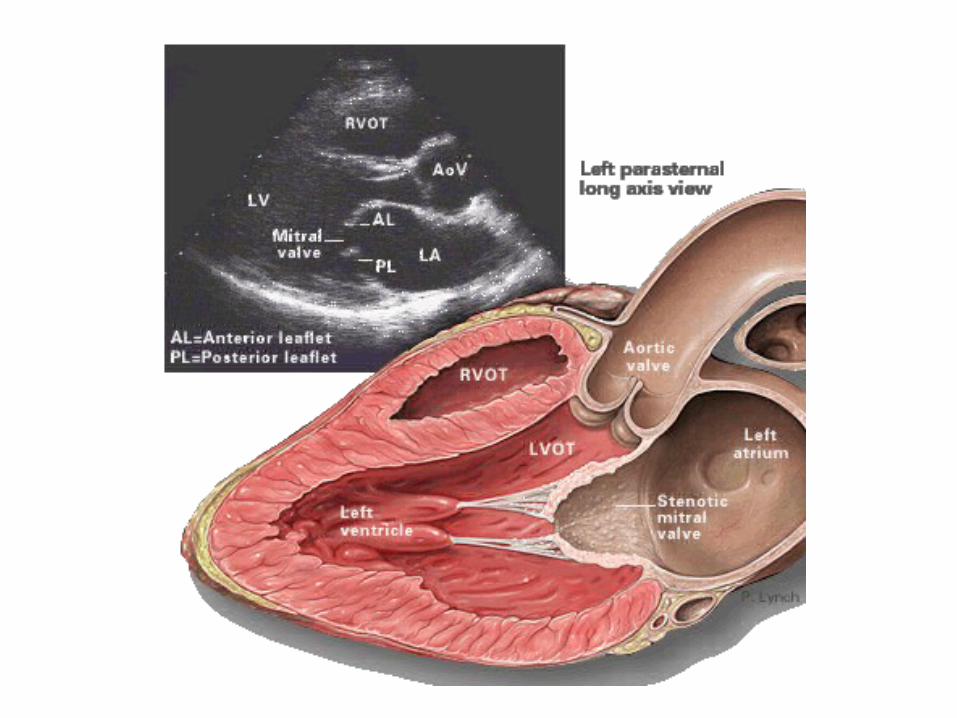
Mitral Stenosis: Etiology
Most commonly rheumatic (up to 40% of patients with rheumatic fever develop mitral stenosis, 99% of surgically removed mitral valves with rheumatic infiltration)Congenital MS rare
MS: History
Symptoms commonly begin in 4th decadeCan cause severe debility by age 20 in economically deprived areasPrincipal symptoms are dyspnea and pulmonary edema precipitated by exertion, anemia, fever, excitement pregnancy, sexual intercourse, etc.
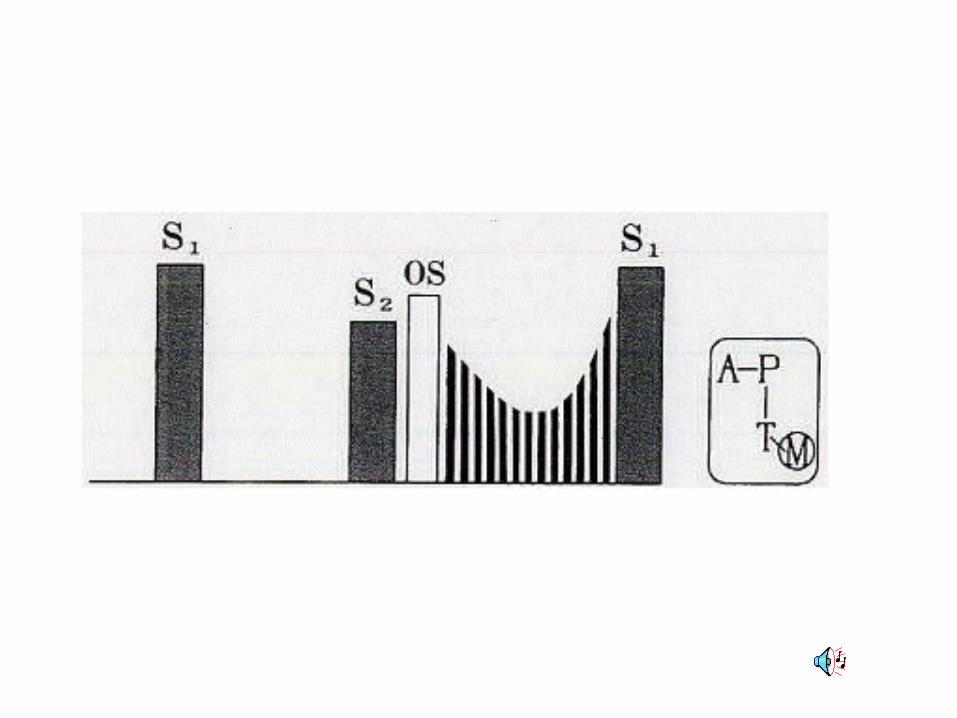
MS: Physical
Right ventricular liftPalpable S1Opening snap follows A2 by 0.06 to 0.12 secondsOS-A interval inversely proportional to severity of diseaseDiastolic rumbling murmur
MS: Complications
HemoptysisPulmonary embolismPulmonary infectionSystemic embolization
Endocarditis uncommon in pure MS
MS: Labs
EKG: Typically A. Fib or LA enlargement when sinus rhythm presentCXR: LA and RV enlargement, Kerley B linesEcho: calcification and thickening of valve leaflets and LA enlargement
MS: Treatment
Prophylaxis for rheumatic feverHeart failure treatment if presentDig, beta blockers to control ventricular rateValvotomy in presence of symptoms and mitral orifice <1.7cm²Anticoagulation if indicated
Mitral Regurgitation: Causes
Rheumatic heart disease in 33% of casesMVPIschemic heart disease with papillary muscle dysfunctionLV dilitationMitral annular calcificationHypertrophic cardiomyopathyInfective endocarditiscongenital
MR: Clinical Manifestations
FatigueWeaknessExertional dyspnea
MR: Physical Exam
Sharp upstoke of arterial pulseLV liftS1 diminishedWide splitting of S2Loud holosystolic murmur
MR: Echo
Enlarged LAHyperdynamic LVDoppler echocardiogram useful in diagnosing and assessing severity of MR
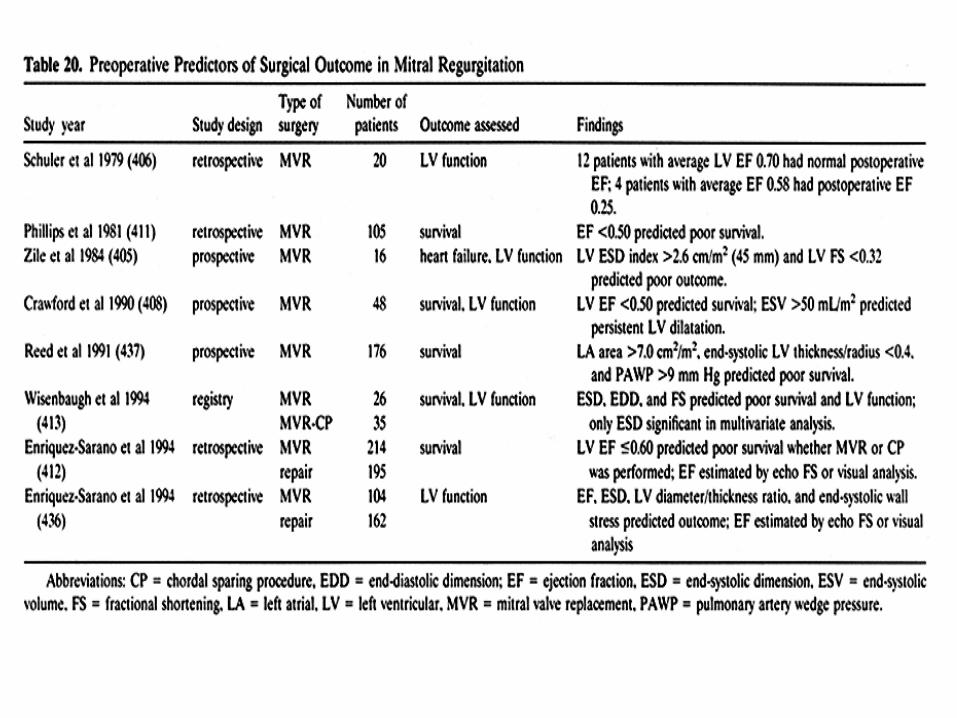
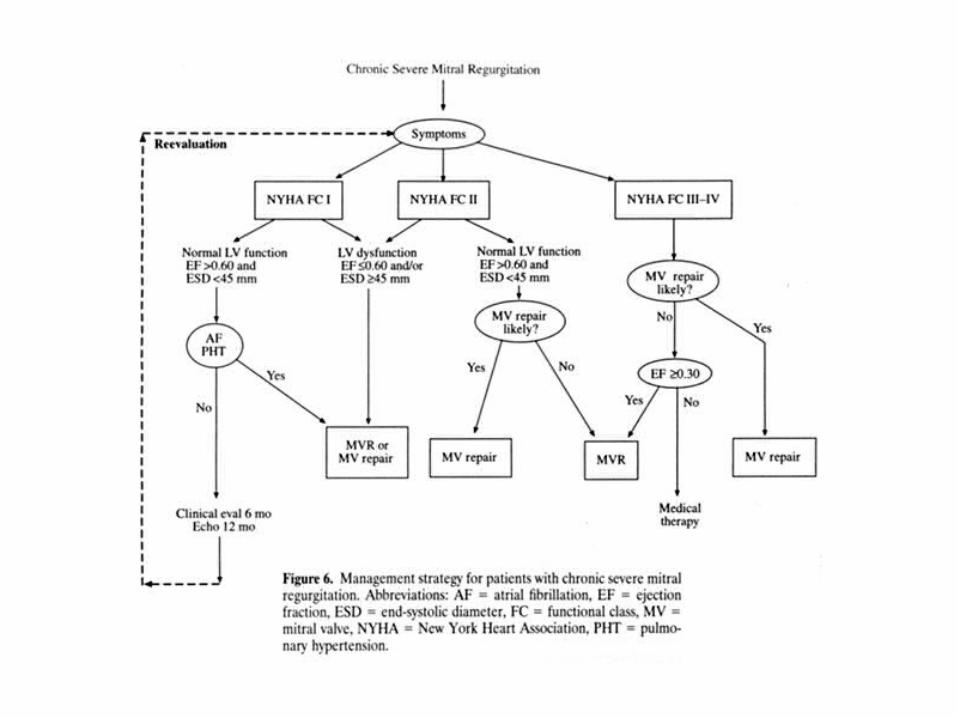
MR: Treatment
For severe/ decompensated MR, treat as heart failureEndocarditis prophylaxis is indicatedSurgical intervention warranted in symptomatic individuals or in evidence of progressive LV dysfunctionSurgery before decompensated heart failureAnticoagulation in face of atrial fibrillation

Mitral Valve Prolapse: Etiology
Most commonly idiopathic? FamilialIschemic heart diseaseAtrial septal defectMarfan syndromeMore common female>male
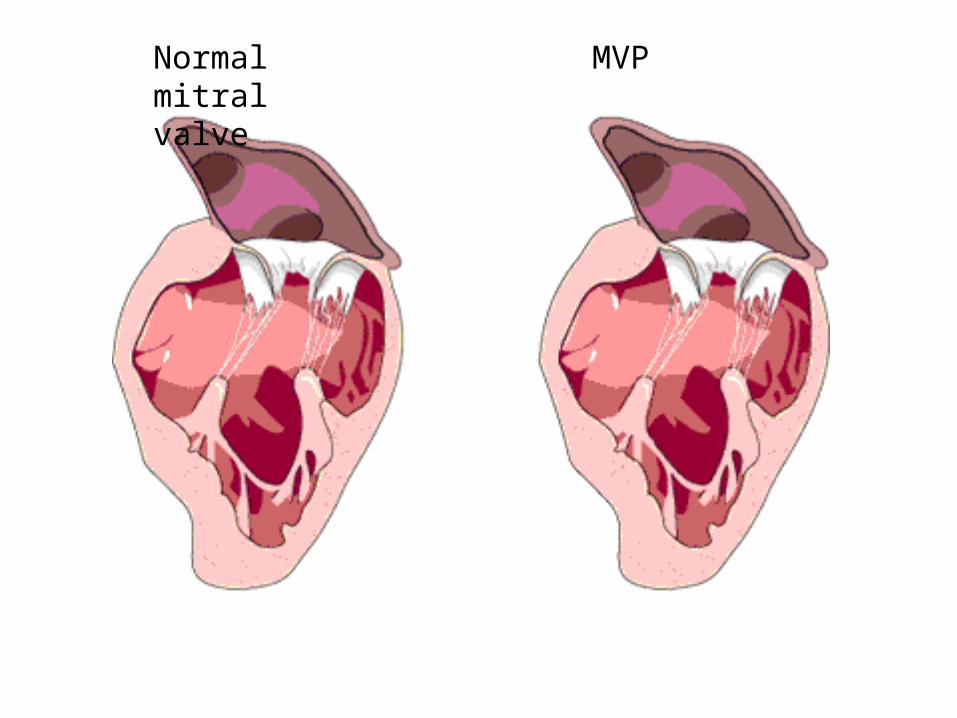
Normal mitral valve
MVP
MVP: Clinical Manifestations
Most patients asymptomatic and remain soChest pain (atypical)Supraventricular and ventricular arrhythmias
Most important complication of severe MR is LV failureSudden death is very rare
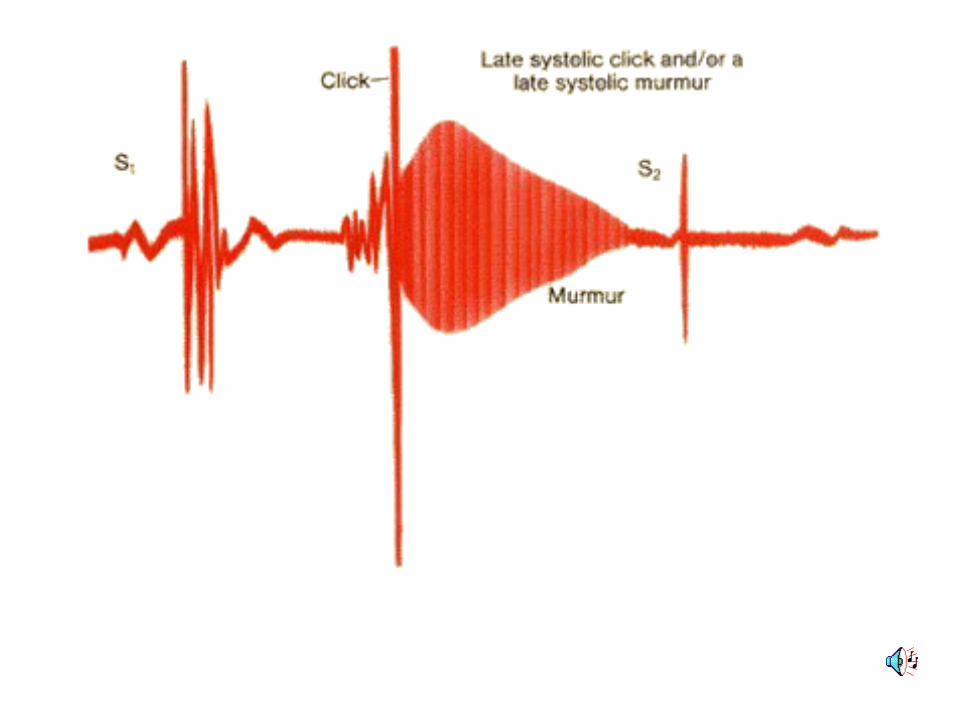
MVP: PE
Mid or late systolic click followed by late systolic murmurMurmur exaggerated by valsalva, reduced with squatting
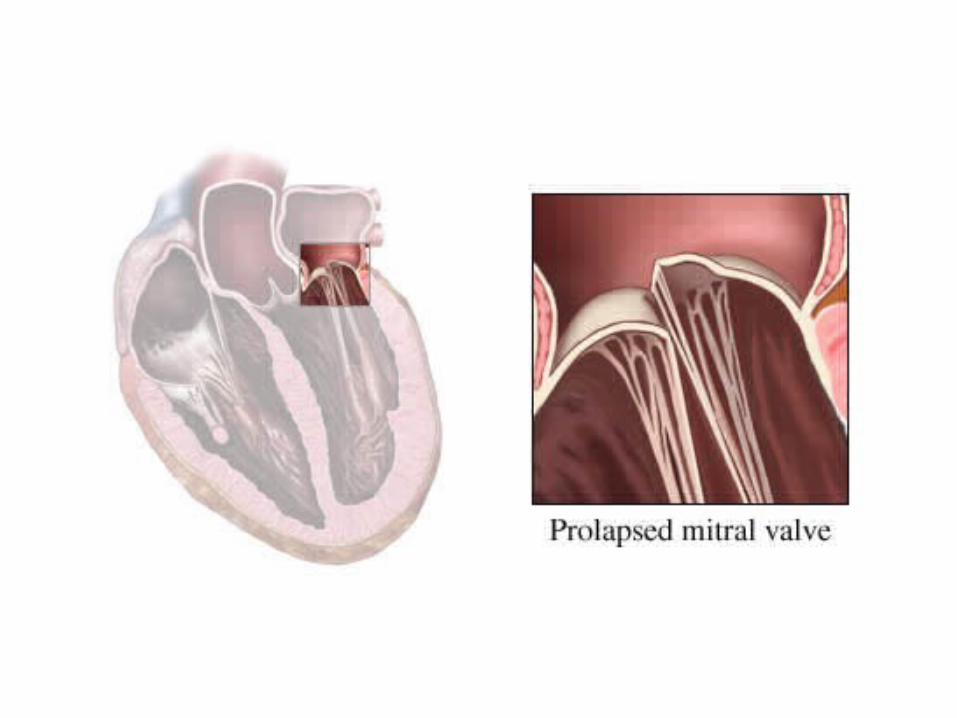
Echo shows displacement of one or both leaflets late in systole
MVP: Treatment
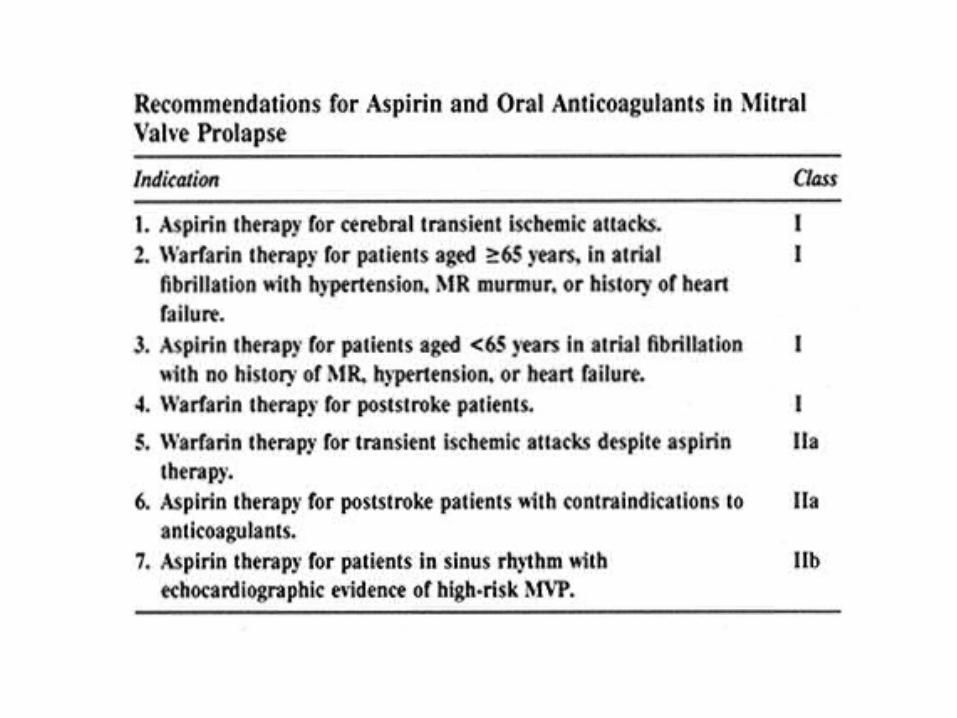
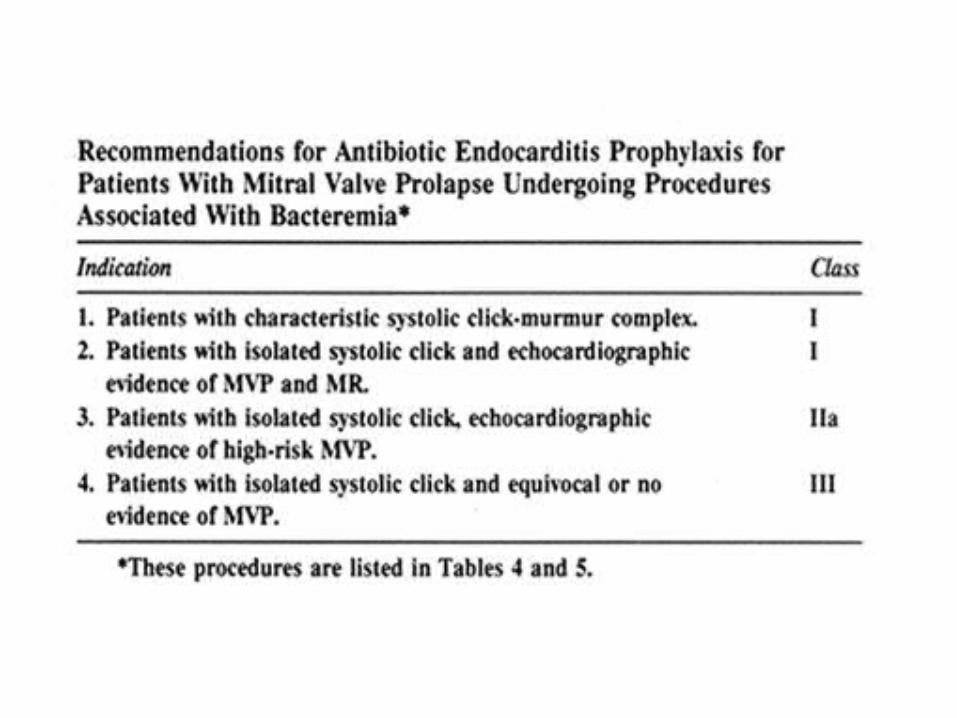
Asymptomatic patient: reassuranceProphylaxis for endocarditis indicatedValve repair for patients with severe MRASA or anticoagulation for patients with TIA or embolization
Question 1
A new patient comes to you for evaluation. He’s a 45 year old male whose only complaint is that of some dyspnea on exertion, which he attributes to old age. He doesn’t smoke or drink alcohol. He does admit to being “very ill as a child,” but has been relatively healthy since. On physical exam, a diastolic murmur is noted, but the remainder of the exam is within normal limits.
Question 1 continued
Which of the following is the next best step in this patient’s management?
a) Only routine preventative careb) Trial of beta blocker therapy to see if his shortness of
breath resolvesc) Echocardiogram for assessment of the diastolic
murmur, with further recommendations to followd) Cranial OMT for assessment of his CRI
Question 2
A 73 year old white male presents to the emergency department after a syncopal episode. He’s dyspnic, with air hunger at the bedside, and is complaining of chest discomfort radiating to his jaw and down his left arm. On exam, a III/VI crescendo-decrescendo murmur is appreciated.
Question 2 continued
Which of the following valvular pathologies is most likely responsible for this man’s presentation?
a) Aortic Stenosisb) Aortic Regurgitationc) Mitral Stenosisd) Mitral Regurgitatione) Mitral valve prolapse
Question 3
The most common cause of mitral stenosis is:a) Familialb) Idiopathicc) Sauerkraut ingestiond) Rheumatice) Alcohol induced