vanderbilt heart focus: heart failure and cardiac … · vanderbilt advanced heart failure and...
TRANSCRIPT

Vanderbilt Heart and Vascular Institute Semiannual Publication Spring 2010 Volume 5 Issue 7 VanderbiltHeart.com
In This Issue
4 Coronary Artery Calcium Scoring for Cardiovascular Risk Prediction in theAsymptomatic Patient
8 Cardiac Disease in Cancer Patients: More Common Than Realized
10 Study Reinforces Link Between Sleep Apnea and Cardiac Arrhythmias
By Mark A. Wigger, M.D., medical director, Adult Heart Transplant, assistant professor ofClinical Medicine
The last three years have seen revitalization, growth and success for theVanderbilt advanced heart failure and transplant programs. Since 2008,there have been 41 new adult heart transplant recipients and 24 pediatricrecipients. Cumulative patient survival rates have exceeded 97%.The transplant program is recognized as a Blue Distinction Center forTransplant and is in the LifeTrac Select Transplant Network, making ourservices available to a wider range of patients. As part of this network,patients are referred to Vanderbilt as a center of excellence for cardiactransplantation.
The Advanced Congestive Heart Failure program providesstate of the art consultation and longitudinal management ofour sickest patients with failing hearts. Patients should bereferred at the time of first hospitalization for heart failure,with the development of New York Heart Class III or foroptimization of care in difficult to treat heart failure patients.A cardiac-oncology clinic has been established, addressing theissues of chemotherapy-induced cardiomyopathy. Themetabolic management of these complex patients is enhanced
by vital support from faculty endocrinologists within the Cardiovascular Division. Critical tothe optimal care of these patients has been the recruitment of committed nurse practitioners,nurses, financial coordinators, and a social worker, all focused on maximizing heart failure andtransplant successes.
Enduring success requires training the next generation of leaders in heart failure andtransplant cardiology. Vanderbilt has established an advanced heart failure/transplantfellowship program, which now provides training, leadership development and guidance ofnew trainees. This endeavor has already manifested tremendous successes, with multipleabstracts and papers presented over the last two years, as well as two young investigator awardsfrom the American Heart Association in 2009 and the American College of Cardiology in2010. (Continued on page 3)
Mark A. Wigger, M.D.
Vanderbilt Heart Focus: Heart Failure and Cardiac Transplant
2009 Patient Survival Rate(Actuarial as of 1/05/2010)
Pediatrics Adults All
1 Month 93.33% 100.00% 97.22%
1 Year 93.33% 100.00% 97.22%
Txps# 15 21 36

Controversies swirl in the field of cardiology, but important questions continue to beaddressed through ongoing research. At the American College of Cardiology AnnualScientific Sessions in March, multiple important studies were reported with valuableclinical insights for us as practitioners. Several of these seem particularly relevant toour readership.
Should we perform early angiography in our patients presenting with acute coronarysyndromes? In patients with acute coronary syndromes (ACS), routine invasive therapy(coronary angiography +/- revascularization as indicated) proved superior to selective invasivetherapy (e.g., prompted by recurrent ischemia) in a meta-analysis of ~ 5,000 patients fromthree clinical trials: RITA-3, FRISC-II, and ICTUS. At five years there was a 19% reductionin death and myocardial infarction with the strategy of routine invasive therapy. This newdata strengthens the current recommendations for early invasive evaluation of patientspresenting with ACS. [Fox KAA. Long-term outcome of a routine versus selective invasivestrategy in patients with non ST elevation acute coronary syndrome: first meta-analysis of five-yearoutcomes based on individual patient data (FIR Trial Collaboration)].
How long should we continue dual antiplatelet therapy (DAPT) with aspirin (ASA) andclopidogrel (Plavix) in patients receiving a drug eluting stent (DES)? Researcherspresented combined results from two trials addressing this question: ZEST-LATE and REAL-LATE. In these studies 2,700 patients free of adverse cardiovascular complications one yearout from DES were randomized to continuing DAPT or to ASA alone at 100-200 mg/d. Attwo years, the composite endpoint of cardiac death and myocardial infarction (MI) was 1.8%with DAPT and 1.2% with ASA alone (p=NS). There was no significant difference inrevascularization rates, and the composite of death, MI, and stroke was higher with DAPT(3.2% vs 1.8%, p=0.051). There are many limitations to this study, including the fact that~6% of those randomized to ASA alone actually took clopidogrel as well. Many ongoingstudies are evaluating this important question. At present the consensus guidelines suggest atleast 12 months of DAPT after DES placement. [Park SJ. Optimal duration of dualantiplatelet therapy after drug-eluting stents implantation: a randomized, multi-center trial.]
How aggressively should we treat systolic blood pressure (SBP) in type II diabeticpatients at high risk for cardiovascular disease (CVD) complications? The Seventh Reportof the Joint National Committee on Prevention, Detection, Evaluation, and Treatment ofHigh Blood Pressure (JNC-7) currently recommends antihypertensive medication at SBP≥ 130 mm Hg in diabetic patients with a goal of lowering to < 130 mm Hg. The ACCORDBP Trial enrolled 4,733 patients with type II diabetes (HbA1c 7.5-11% ) at high risk forCVD events (prior event, subclinical CAD, or ≥2 additional CVD risk factors) and SBP>130. Patients were randomized to Intensive Therapy (treatment SBP goal of <120 mmHg)versus Standard Therapy (<140 mmHg). At 4.7 years of follow-up, there was no difference inmajor adverse clinical events (1.9% vs 2.1% ). While observational data suggests that lowerSBP is beneficial, treating with medication to achieve a SBP <130 mmHg in this high riskpopulation may not provide additional benefit. One preliminary expert panel reaction hassuggested perhaps treating to a SBP ~130 mmHg, but not adding additional medications forstricter control due to lack of demonstrated efficacy and increased cost. More aggressive non-pharmacologic lifestyle modification has been emphasized. [Cushman WC, ACCORD StudyGroup. Effects of intensive blood pressure control on cardiovascular events in type 2 diabetesmellitus: the Action of Control Cardiovascular Risk in Diabetes (ACCORD) Blood Pressure Trial.]
From the Editorby Robert N. Piana, M.D., professor of Medicine
Vanderbilt Heart Spring 2010
Robert N. Piana, M.D.
2

Vanderbilt Heart Focus: Heart Failure and Cardiac Transplant(Continued from page 1)
3
Vanderbilt has also developed multiple surgical andinterventional programs which have contributed to improvedoutcomes in patients with advanced heart failure. For very highrisk patients with ischemia complicating advanced heart failure,we have utilized short-term ventricular support in thecatheterization laboratory with Tandem Heart and the Impellasystems to facilitate successful percutaneous coronaryrevascularization procedures. A robust surgical program utilizingminimally invasive mitral valve replacement has also allowed usto relieve mitral regurgitation in advanced heart failure patientswho might not otherwise be approachable surgically.Intermediate term hemodynamic support with the ThoratecCentri-Mag ventricular assist device and axillary intra-aorticballoon pumps has also been successful in bridging patients torecovery or cardiac transplant over days to weeks. We also nowoffer the Thoratec Heart Mate II as long-term ventricularsupport, with the potential to be used as “destination therapy.”
A dedicated team of medical and surgical transplant physiciansensures optimal care when transplant is required. Clinical follow-
up after successful transplantation is evolving. We are now using peripheral bloodmolecular gene expression profile to monitor for rejection in place of more invasivetechniques. This has been a successful tool for surveillance monitoring and ispreferred by patients as indicated by our longitudinal Quality of Life Survey.
Clinical and basic science research opportunities are immense for staff and patients.Stem cell therapy for patients with chronic ischemic cardiomyopathy and newerpharmaceutical trials are ongoing. We also have an active cardiovascular inheriteddisease program evaluating genetic cardiomyopathies. Finally, we have recentlyestablished a heart failure registry database to support clinical research designed toimprove our patients’ outcomes.
We also understand that responsive longitudinal care is a critical component of thisprogram. We have established numerous outreach clinics in Middle and EastTennessee and Southern Kentucky over the past three years. We are providing patientsupport groups and CME opportunities locally and regionally to health careproviders on all aspects of advanced heart failure and transplant care. These clinicsprovide advanced heart failure consults and post cardiac transplant care with ongoingeducation to health care providers.
The advanced heart failure/cardiac transplant team will continue to expand ourrepertoire of therapeutic interventions for our patients. Our commitment to basic,clinical and translational cardiovascular medicine will facilitate far reachingopportunities for our patients and for physicians in training for generations to come.The more we know and share with our patients, the better recovery platform we canoffer for those impaired by this condition.
Contact Information:
Heart Failure andCardiac Surgery:(615) 343-9188
Cardiac Transplant Services:866-748-1494, extension 6-3500
Vanderbilt Heart Failureand Transplant OutreachLocations:East Tennessee Heart Consultants,
Knoxville, Tenn.East Tennessee State University
Heart, Johnson City, Tenn.Vanderbilt Heart, Lebanon, Tenn.and Murfreesboro, Tenn.
Advanced Heart Failure/Cardiac Transplant Physiciansand NursesThomas DiSalvo, M.D., DanielLenihan, M.D., Allen Naftilan,M.D., Doug Sawyer, M.D., Ph.D.,Mark Wigger, M.D.,and Connie Lewis, N.P.
Cardiac Transplant SurgeryPhysiciansJohn G. Byrne, M.D., Steve Hoff,M.D., and Rashid Ahmad, M.D.
Endocrinology PhysiciansJeffrey Boord, M.D.
Patient Mary Pat Andrews wears a Heart Mate IImechanical assist device that functions as a bridge to cardiactransplant. Advances in technology allow patients like her tomaintain quality of life while awaiting her new heart.

4
By Emily Graham Kurtz, M.D., assistant professor of Medicine
Atherosclerosis imaging, and cardiac computed tomography (CT) inparticular, has rapidly evolved over the past several years, primarily inresponse to the needs for accurate non-invasive coronary angiography andearly identification of subclinical coronary artery disease (CAD), allowingfor early aggressive modification of risk in those at increased risk for futurecardiovascular events (CVE).
Distinguishing between coronary artery calcium scoring and coronary CT angiography
There are two varieties of “cardiac CT.” Coronary artery calcium scoring (CACS) is arelatively low-radiation (radiation exposure: approximately 1-2 mSv), noncontrasted CT ofthe chest with dedicated evaluation of the coronary arteries. CACS is used as a screening testin asymptomatic patients in whom it has been extensively studied for risk stratification. Inthe absence of contrast, CACS is limited to visualization of calcified coronary artery plaque.Quantification of coronary calcium burden using an Agatston score is a helpful prognosticindicator for risk of future CVE (see Figure 1). By comparison, coronary CT angiography(cCTA) is a contrasted CT examination of the chest (radiation exposure: approximately 8-12mSv) which enables visualization of coronary arteries and reliable exclusion of coronary arterystenosis, especially in patients with chest pain and a low to intermediate pretest likelihood of
significant CAD. The use of contrast withcCTA allows detection of both calcified andnoncalcified atherosclerotic plaque (see Figure2). These distinctions between CACS andcCTA are important for clinical application ofthese imaging modalities. CACS is a screening,risk prediction tool whose high sensitivityrenders it most useful for ruling in thepresence of subclinical atherosclerosis inasymptomatic patients, whereas cCTA is adiagnostic modality whose high negativepredictive value renders it most effective forruling out obstructive CAD in symptomaticpatients.
Understanding these distinctions, the purposeof this article is to discuss the clinical utilityof CACS for cardiovascular risk prediction inthe asymptomatic patient. That is, how maywe appropriately use CACS to rule insubclinical atherosclerosis and thereforeidentify patients in whom more aggressivepreventive lifestyle and medical strategies arelikely to favorably influence long-termcardiovascular risk?
Coronary Artery Calcium Scoring for Cardiovascular RiskPrediction in the Asymptomatic Patient
Emily Graham Kurtz, M.D.
Figure 1. Coronary arterycalcium in a 57-year-oldasymptomatic patient witha family history ofpremature coronary arterydisease. The top imageshows the original axial CTimages, demonstrating acalcified plaque (bluearrow) within the proximalsegment of the left anteriordescending coronary artery(LAD). The softwarequantitates the coronaryartery calciumconcentration in thisproximal LAD plaque(bottom image; plaquecolor coded in red). Thetotal Agatston scores for theproximal LAD plaqueshown and for the entirestudy were 134 and 291,respectively. His coronaryartery calcium age-basedpercentile was 82% for age-matched men 55-59 years.
5
Coronary artery calcium scoring and risk prediction
CACS demonstrates independent and incremental prognostic value over traditional riskfactors for the prediction of all-cause mortality and cardiovascular events.1-7 Along with theemergence of novel serum biomarkers, coronary artery calcium scoring has improved theability to detect subclinical atherosclerosis and, more importantly, to appropriately risk stratifypatients and invoke aggressive preventive lifestyle and medical strategies accordingly.
The ACCF/AHA 2007 Expert Consenses Document on CACS compiled data from multipletrials comparing CACS and CV outcomes.8 From this data, a quantitative relative risk (RR)ratio scale based on coronary calcium density as measured by Hounsfeld units (HU) wasproposed, reflecting an incremental relationship in which higher coronary artery calciumscores are associated with higher event rates (CHD death or MI risk, over a 3-to-5-yearperiod) and higher RR ratios. Using a calcium score of zero as the referent, the RR ratio for acalcium score of 1-100 was 1.9 (95% CI 1.3-2.8, p = 0.001). For calcium scores of 100-399,400-999, and ≥1000, the RR ratios were 4.3, 7.2, and 10.8,respectively (p < 0.0001 for all).8
Similarly, Wayhs reported that a calcium score of >1000 on ascreening CACS in asymptomatic individuals portended a veryhigh risk (36%) of MI or death at 4-36 months.9 This riskappeared to be greater than the risk associated with a severeperfusion abnormality on nuclear stress testing (annualizedevent rate of 25% vs. 7.4%, respectively; p < 0.0001). At theother end of the spectrum, even the presence of minimalcoronary artery calcium (Agatston score: 1-10) doubles 10-year mortality risk, according to a study by Blaha et al.10
The absence of coronary calcification, however, does notnecessarily exclude obstructive coronary stenosis. A recentstudy by Gottlieb demonstrated that among patients with acoronary calcium score of zero, almost 20% had at least one≥50% non-calcified coronary stenosis at the time of cardiaccatheterization within 30 days of CACS.11
Which patients are appropriate candidates forCACS screening?
In their summary recommendations, the authors of theACCF/AHA Expert Consensus Document on CoronaryArtery Calcium Scoring specifically addressed the role ofCACS in asymptomatic patients with low, intermediate andhigh CHD risk (10-year event risks of <10%, 10-20%, and>20%, respectively). In intermediate CHD risk patients,CACS was considered reasonable, given that available evidencedemonstrates incremental risk prediction information in thisgroup. Evidence of coronary calcium would result inreclassification of these patients to a higher risk status,warranting modification of patient management. In high-riskpatients, CACS was not recommended, as these patients arealready judged to be candidates for intensive risk reduction(Continued on page 6)
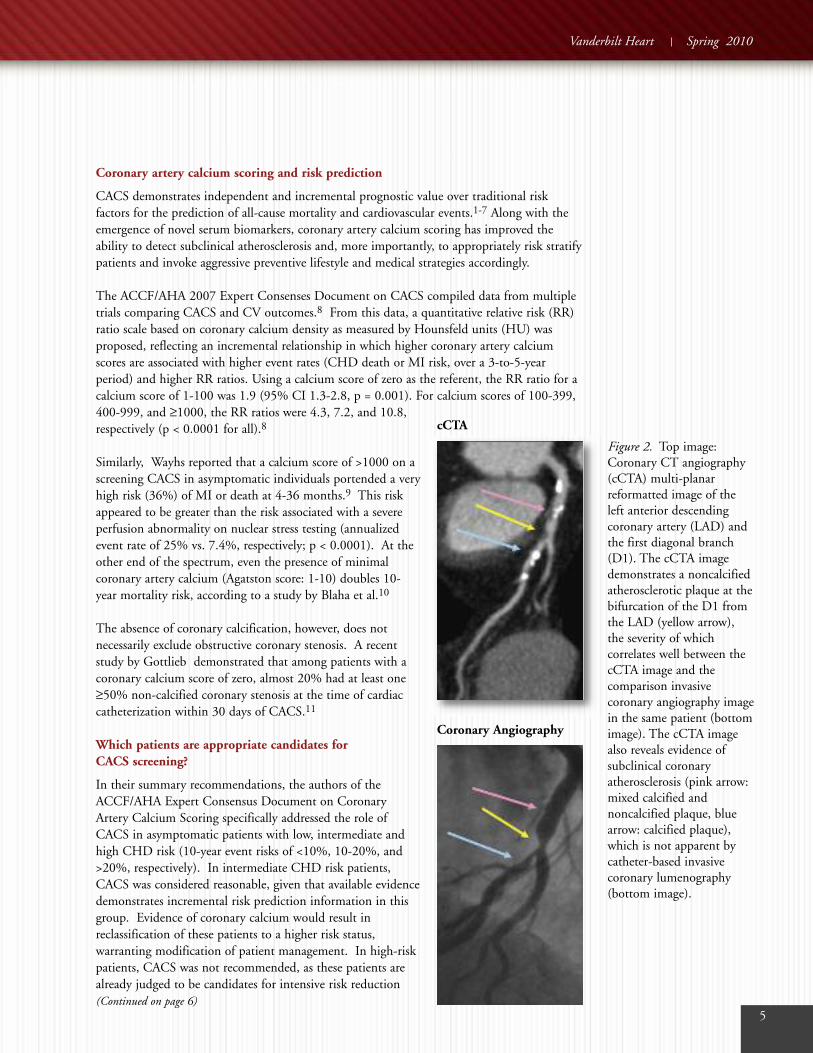
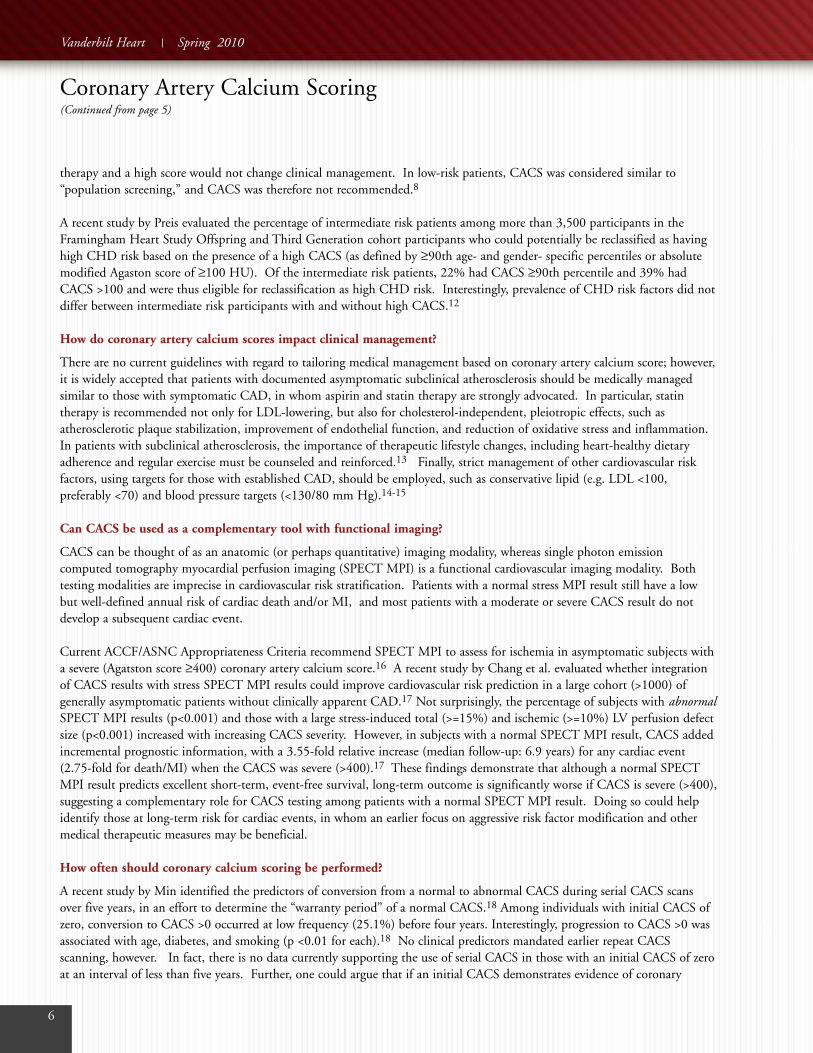
Figure 2. Top image:Coronary CT angiography(cCTA) multi-planarreformatted image of theleft anterior descendingcoronary artery (LAD) andthe first diagonal branch(D1). The cCTA imagedemonstrates a noncalcifiedatherosclerotic plaque at thebifurcation of the D1 fromthe LAD (yellow arrow),the severity of whichcorrelates well between thecCTA image and thecomparison invasivecoronary angiography imagein the same patient (bottomimage). The cCTA imagealso reveals evidence ofsubclinical coronaryatherosclerosis (pink arrow:mixed calcified andnoncalcified plaque, bluearrow: calcified plaque),which is not apparent bycatheter-based invasivecoronary lumenography(bottom image).
Coronary Angiography
cCTA
Vanderbilt Heart Spring 2010
6
therapy and a high score would not change clinical management. In low-risk patients, CACS was considered similar to“population screening,” and CACS was therefore not recommended.8
A recent study by Preis evaluated the percentage of intermediate risk patients among more than 3,500 participants in theFramingham Heart Study Offspring and Third Generation cohort participants who could potentially be reclassified as havinghigh CHD risk based on the presence of a high CACS (as defined by ≥90th age- and gender- specific percentiles or absolutemodified Agaston score of ≥100 HU). Of the intermediate risk patients, 22% had CACS ≥90th percentile and 39% hadCACS >100 and were thus eligible for reclassification as high CHD risk. Interestingly, prevalence of CHD risk factors did notdiffer between intermediate risk participants with and without high CACS.12
How do coronary artery calcium scores impact clinical management?
There are no current guidelines with regard to tailoring medical management based on coronary artery calcium score; however,it is widely accepted that patients with documented asymptomatic subclinical atherosclerosis should be medically managedsimilar to those with symptomatic CAD, in whom aspirin and statin therapy are strongly advocated. In particular, statintherapy is recommended not only for LDL-lowering, but also for cholesterol-independent, pleiotropic effects, such asatherosclerotic plaque stabilization, improvement of endothelial function, and reduction of oxidative stress and inflammation.In patients with subclinical atherosclerosis, the importance of therapeutic lifestyle changes, including heart-healthy dietaryadherence and regular exercise must be counseled and reinforced.13 Finally, strict management of other cardiovascular riskfactors, using targets for those with established CAD, should be employed, such as conservative lipid (e.g. LDL <100,preferably <70) and blood pressure targets (<130/80 mm Hg).14-15
Can CACS be used as a complementary tool with functional imaging?
CACS can be thought of as an anatomic (or perhaps quantitative) imaging modality, whereas single photon emissioncomputed tomography myocardial perfusion imaging (SPECT MPI) is a functional cardiovascular imaging modality. Bothtesting modalities are imprecise in cardiovascular risk stratification. Patients with a normal stress MPI result still have a lowbut well-defined annual risk of cardiac death and/or MI, and most patients with a moderate or severe CACS result do notdevelop a subsequent cardiac event.
Current ACCF/ASNC Appropriateness Criteria recommend SPECT MPI to assess for ischemia in asymptomatic subjects witha severe (Agatston score ≥400) coronary artery calcium score.16 A recent study by Chang et al. evaluated whether integrationof CACS results with stress SPECT MPI results could improve cardiovascular risk prediction in a large cohort (>1000) ofgenerally asymptomatic patients without clinically apparent CAD.17 Not surprisingly, the percentage of subjects with abnormalSPECT MPI results (p<0.001) and those with a large stress-induced total (>=15%) and ischemic (>=10%) LV perfusion defectsize (p<0.001) increased with increasing CACS severity. However, in subjects with a normal SPECT MPI result, CACS addedincremental prognostic information, with a 3.55-fold relative increase (median follow-up: 6.9 years) for any cardiac event(2.75-fold for death/MI) when the CACS was severe (>400).17 These findings demonstrate that although a normal SPECTMPI result predicts excellent short-term, event-free survival, long-term outcome is significantly worse if CACS is severe (>400),suggesting a complementary role for CACS testing among patients with a normal SPECT MPI result. Doing so could helpidentify those at long-term risk for cardiac events, in whom an earlier focus on aggressive risk factor modification and othermedical therapeutic measures may be beneficial.
How often should coronary calcium scoring be performed?
A recent study by Min identified the predictors of conversion from a normal to abnormal CACS during serial CACS scansover five years, in an effort to determine the “warranty period” of a normal CACS.18 Among individuals with initial CACS ofzero, conversion to CACS >0 occurred at low frequency (25.1%) before four years. Interestingly, progression to CACS >0 wasassociated with age, diabetes, and smoking (p <0.01 for each).18 No clinical predictors mandated earlier repeat CACSscanning, however. In fact, there is no data currently supporting the use of serial CACS in those with an initial CACS of zeroat an interval of less than five years. Further, one could argue that if an initial CACS demonstrates evidence of coronary
Coronary Artery Calcium Scoring(Continued from page 5)
Vanderbilt Heart Spring 2010

atherosclerosis (CACS >0), the patient need not ever undergo repeat CACS, as the resultswould not likely further influence clinical management, assuming that aggressive risk factormodification was offered at the time of first discovery of subclinical atherosclerosis.
In summary, coronary artery calcium scoring is an important noninvasive diagnostic tool thatadds independent and incremental prognostic value over traditional risk factors for theprediction of all-cause mortality and cardiovascular events, and can be effectively used to rulein the presence of subclinical atherosclerosis in asymptomatic patients, leading to earlyaggressive modification of risk in those at high risk for future cardiovascular events.
1. Raggi P. Cardiac CT in asymptomatic patients at risk. Cardiol Clin 2009; 27: 605-610.
2. Shaw LJ, Raggi P, Schisterman E, et al. Prognostic value of cardiac risk factors and coronary artery calciumscreening for all-cause mortality. Radiology 2003; 228(3): 826–33.
3. Greenland P, LaBree L, Azen SP, et al. Coronary artery calcium score combined with Framingham score for riskprediction in asymptomatic individuals. JAMA 2004; 291(2): 210–5.
4. Arad Y, Goodman kJ, Roth M, et al. Coronary calcification, coronary disease risk factors, C-reactive protein, andatherosclerotic cardiovascular disease events: the St. Francis Heart Study. J Am CollCardiol 2005; 46(1): 158–65.
5. LaMonte MJ, FitzGerald SJ, Church TS, et al. Coronary artery calcium score and coronary heart disease events ina large cohort of asymptomatic men and women. Am J Epidemiol 2005; 162(5): 421–9.
6. Taylor AJ, Bindeman J, Feuerstein I, et al. Coronary calcium independently predicts incident premature coronaryheart disease over measured cardiovascular risk factors: mean three-year outcomes in the Prospective Army CoronaryCalcium (PACC) project. J Am Coll Cardiol 2005; 46(5): 807–14.
7. Kondos GT, Hoff JA, Sevrukov A, et al. Electronbeam tomography coronary artery calcium and cardiac events: a37-month follow-up of 5635 initially asymptomatic low- to intermediate-risk adults.Circulation 2003; 107(20): 2571–6.
8. Greenland P, et al. ACCF/AHA Expert Consensus Document on Coronary Artery Calcium Scoring. J Am CollCardiol 2007; 49: 378-402.
9. Wayhs R, Zelinger A, and Raggi P. High Coronary Artery Calcium Scores Pose an Extremely Elevated Risk forHard Events. J Am Coll Cardiol 2002; 39(2): 225-230.
10. Blaha M, Budoff MJ, Shaw LJ, et al. Absence of coronary artery calcification and all-cause mortality. J Am CollCardiol Img 2009; 2: 692-700.
11. Gottlieb I, et al. The Absence of Coronary Calcification Does Not Exclude Obstructive Coronary Artery Diseaseor the Need for Revascularization in Patients Referred for Conventional Coronary Angiography. J Am Coll Cardiol2010; 55(7): 627-34.
12. Preis SR, Hwang SJ, Fox CS, Massaro JM, Levy D, Hoffmann U, O’Donnell CJ. Eligibility of individuals withsubclinical coronary artery calcium and intermediate coronary heart disease risk for reclassification (from theFramingham Heart Study). Am J Cardiol. 2009; 103(12): 1710-5.
13. Lichtenstein AH, Appel LJ, Brands M, Carnethon M, Daniels S. Franch HA, Franklin B, Kris-Etherton P, HarrisWS, Howard B, Karanja N, Lefevre M, Rudel L, Sacks F, Van Horn L, Winston M, and Wylie-Rosett Judith. AHA2006 Diet and Lifestyle Guidelines. Circulation 2006; 114: 82-96.
14. Grundy et al. Implications of Recent Clinical Trials for the National Cholesterol Education ProgramAdult Treatment Panel III Guidelines. Circulation 2004;110: 227-239
15. Rosendorff C. et al. Treatment of Hypertension in the Prevention and Management of Ischemic Heart Disease:A Scientific Statement From the American Heart Association Council for High Blood Pressure Research and theCouncils on Clinical Cardiology and Epidemiology and Prevention. Circulation. 2007;115:2761-2788.
16. Brindis RG, et al. ACCF/ASNC Appropriateness Criteria for SPECT MPI. J Am Coll Cardiol 2005; 46:1587-2150.
17. Chang AM, et al. The Coronary Artery Calcium Score and Stress Myocardial Perfusion Imaging ProvideIndependent and Complementary Prediction of Cardiac Risk. J Am Coll Cardiol 2009; 54: 1872-1882.
18. Min J, et al. Determinants of coronary calcium conversion among patients with a normal coronary calciumscan: What is the “warranty period” for remaining normal? J Am Coll Cardiol 2010; 55: 1110-7.
7
In summary, coronaryartery calcium scoringis an importantnoninvasive diagnostictool that addsindependent andincremental prognosticvalue over traditionalrisk factors for theprediction of all-causemortality andcardiovascular events,and can be effectivelyused to rule in thepresence of subclinicalatherosclerosis inasymptomatic patients,leading to earlyaggressive modificationof risk in those at highrisk for futurecardiovascular events.

8
By Daniel J. Lenihan M.D., professor of Clinical Medicine
There is tremendous overlap in the risk factor profiles of cardiology patientsand patients being treated for cancer.1 Fortunately, advances in cancer carehave yielded striking reductions in mortality in a host of malignancies, suchthat the five-year survival rate of all cancers has increased dramatically, from50% in the 1970s to 66% in the late 1990s. However, as survival rates haveincreased, so has recognition that these survivors face cardiac complicationsthat have a major impact on quality of life.2-3 Furthermore, the complexityof cancer therapeutics continues to rise, with many specialized molecularmarkers of uncontrolled cancer growth being targeted. Not surprisingly, suchtreatments may have at least transient important negative effects on themetabolically active cardiovascular tissues. As a result of these dynamics, itis imperative for cardiovascular specialists to have an understanding of theprevention, identification and treatment of cardiac disease in cancer patientsin order to optimize clinical outcomes.
Cardiologists broadly recognize the potential for anthracyclines or trastuzumab to inducecardiomyopathy. However, for us to provide optimal care to these complex patients we mustrecognize that there are actually many other cardiac complications to consider (see inset). Forinstance, significant rhythm disturbances including atrial fibrillation, are common duringcancer treatment and chemotherapy. Monitoring the QT interval is a required method todetect early toxicity with certain chemotherapeutic regimens. Agents such as arsenic trioxidecan have a profound effect on the QT interval or can result in bradycardia, requiring a
permanent pacemaker. Cardiac masses, either thrombus ortumor, are frequently detected on imaging, such asechocardiography and MRI (figures 1 and 2, respectively),and present challenging clinical decisions that require aninterdisciplinary approach. Cancer patients’ propensity forsystemic thrombi, including pulmonary emboli andmyocardial infarction, even in the face of thrombocytopenia,requires careful anticoagulation while balancing the risk ofbleeding.4 Cardiac valvular structures can also be involved,such as tricuspid regurgitation commonly seen withcarcinoid syndrome. Pericardial disease is a majorconsideration, sometimes progressing to life-threateningcardiac tamponade. The vasculature in general is greatlyaffected by systemic therapy. Radiation therapy is known topromote fibrosis and accelerated atherosclerosis in treatedareas. The effect of newer cancer therapies intended to beanti-angiogenic by limiting blood supply to the tumor islikely to have remote vascular effects that may be onlypartially recognized at present. Several reports havedemonstrated severe hypertension, heart failure and otherarterial thrombotic events during anti-vascular growth factorand anti-angiogenic based therapy.5-7
Cardiac Disease in Cancer Patients: More CommonThan Realized
Daniel J. Lenihan, M.D.
Common Cardiac Problems EncounteredDuring Cancer Therapy
• Arrhythmias (Atrial Fibrillation, Bradycardia)
• ECG Abnormalities (QT Prolongation, ST changes)
• Thrombi (arterial and venous)
• Myocardial Infarction
• Cardiomyopathy and Heart Failure(Chemotherapy-related, Stress Cardiomyopathy)
• Valvular disease (Tricuspid Regurgitation,Endocarditis)
• Pericardial Effusion and Tamponade
• Hypertension (Especially related toAnti-angiogenic therapies)
• Masses (tumors, either metastatic or primary, orintracardiac thrombi)
• Vascular compromise (radiation related oraccelerated atherosclerosis)

9
The optimal management of cardiac disease in cancerpatients clearly needs to emphasize prevention, detection andtreatment. The history of cardiac toxicity in cancer patientsduring a variety of therapies is often difficult to establishdefinitively. This is because there are often changingdefinitions of exactly what is considered cardiac toxicity andit is unclear how strongly the surrogate marker (typically leftventricular ejection fraction [LVEF] measured byechocardiography or nuclear imaging) used to detect thisdamage is related to the actual timing of chemotherapy.8
Several recent studies have utilized a sophisticated cardiacbiomarker approach to carefully identify patients developingcardiac toxicity. It is possible that this strategy will besuperior to serial LVEF measurements for the early detectionof cardiac toxicity to allow optimal preventive measures forthe development of cardiac disease.9-10 There is amulticenter study being initiated to test this strategy duringanthracycline chemotherapy to establish whether thisapproach is advantageous. Most importantly, if toxicity isidentified, this trial will help document the cardiac outcomeswith different cardiology-based treatment choices to guidefuture consensus recommendations. At this time, affectedpatients are treated using typical medications that are knownto be effective in preventing and optimally treating heartfailure.11-13 Unfortunately, the strategy for using cardiacbased biomarkers to detect cardiac toxicity early has not beenwidely adopted for a host of reasons, including difficulty inestablishing the exact timing for when the serum should bedrawn and a changing definition of toxicity across all ofthe studies.
Recent efforts have focused on achieving a consensusregarding important issues involving the overlap ofcardiology and oncology, and on developing strategies toimprove our collective knowledge in a clinically practicalmanner. We have developed the InternationalCardiOncology Society, whose primary goal is to eliminatecardiac disease as a barrier to effective cancer therapy and toextend and improve our knowledge of these complex clinicalsettings. We are organizing our fourth Annual InternationalMeeting to be held in Nashville, Oct. 7-9, in which the latestresearch, including developing basic and clinical studies, anda consensus document will be described and published.Several ongoing clinical trials, including a multicenterdatabase and registry, are being organized as part of thisconcerned group of providers which will help to answersome of the burgeoning clinical conundrums faced byproviders on a daily basis. (Continued on page 12)
Vanderbilt Heart Spring 2010
Echocardiogram showing a left ventricular thrombus in apatient with chemotherapy-related cardiomyopathy
MRI imaging showing an atrial mass resulting fromangiosarcoma
Figure 1
Figure 2

10
By Ken Monahan, M.D., assistant professor of Medicine
Sleep-disordered breathing (SDB) affects at least 5% of the adult population1 and isassociated with hypertension,2 cardiovascular disease3 and mortality.3-4 Typical symptomsinclude loud snoring and otherwise unexplained excessive sleepiness during waking hoursincluding unintentionally falling asleep during normal activities (reading, watching TV,having a conversation). Witnessed cessation of breathing while asleep is another key featureof SDB. During sleep, episodes of airway collapse lead to intermittent hypoxia and itssequelae (increased blood pressure, inflammation, endothelial dysfunction, sympatheticactivation), all of which can promote sustained hypertension, myocardial ischemia, andarrhythmias. Treatment of SDB with continuous positive airway pressure (CPAP) canfavorably impact not only the symptoms of SDB itself, but also ameliorate its downstreamconsequences.3,5
Over the past three decades,6-11 studies exploring the relationships between SDB and cardiacarrhythmias have shown that SDB increases the risk of atrial fibrillation (OR ~ 2-3)12 andventricular arrhythmias (OR ~ 3-4),13-14 which may relate to the increased risk of suddencardiac death (SCD) of those with SDB during overnight sleeping hours. However, whetherthe respiratory disturbances that are the hallmark of SDB are triggers for these arrhythmias isunknown.15
Our group set out to investigate this question.16 Working with an interdisciplinary team ofsleep physicians, biostatisticians, and cardiologists, we analyzed polysomnograms (sleepstudies) from the Sleep Heart Health Study, a large multicenter longitudinal study of sleep-disordered breathing.
We identified participants who experienced discrete episodes of AF and/or non-sustainedventricular tachycardia (NSVT) during their polysomnogram. We then used the case-crossover design to determine whether respiratory disturbances can trigger paroxysmal AF orNSVT. The case-crossover method analyzes the risk of an event occurring in the context of atemporary exposure, with subjects serving as their own controls. In our study, the ‘events’ arearrhythmias (PAF and NSVT), the ‘exposures’ are respiratory disturbances (apneas orhypopneas), and the three ‘control’ (or ‘referent’) periods are derived from time spent in sinusrhythm (Figure 1).
Our study showed that the odds of an arrhythmia following a respiratory disturbance werenearly 18 times the odds of an arrhythmia occurring following normal breathing. Thesefindings suggest a direct temporal link between respiratory disturbances and the developmentof PAF and NSVT. However, because the occurrence of arrhythmias in our cohort wasrelatively uncommon, we estimate that an individual with moderate sleep apnea who getseight hours of sleep per night would experience approximately two extra arrhythmias per year.
Given our findings, it is possible that undetected and/or untreated SDB could contribute tothe increasing prevalence of AF. Similarly, increased ventricular ectopy following apneas orhypopneas may lead to malignant arrhythmias that could explain the nocturnal predominanceof sudden death in those with SDB.
Future research will focus on testing the hypotheses that pharmacotherapy and/or SDBtreatment (with CPAP) can modify the SDB-arrhythmia relationships demonstrated in ourwork. Further studies are also needed to explore whether screening individuals with AF forSDB improves detection of sleep apnea and/or assists in the treatment of AF. It remains
Study Reinforces Link Between Sleep Apnea andCardiac Arrhythmias
Ken Monahan, M.D.
Vanderbilt Heart Spring 2010
Our study showed thatthe odds of anarrhythmia following arespiratory disturbancewere nearly 18 timesthe odds of anarrhythmia occurringfollowing normalbreathing. Thesefindings suggest adirect temporal linkbetween respiratorydisturbances and thedevelopment of PAFand NSVT.

11
unclear to what extent those with SDB should undergo dedicated cardiac evaluation, but furtherinvestigation of electrocardiographic abnormalities that occur during a sleep study seemsreasonable.
1. Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective.Am J Respir Crit Care Med 2002; 165: 1217-39.
2. Nieto FJ, Young TB, Lind BK, et al. Association of sleep-disordered breathing, sleep apnea, and hypertensionin a large community-based study. JAMA 2000; 283: 1829-36.
3. Marin JM, Carrizo SJ, Vicente E, Agusti AGN. Long-term cardiovascular outcomes in men with obstructivesleep apnea-hypopnea with or without treatment with continuous positive airway pressure: an observationalstudy. Lancet 2005; 365: 1046-53.
4. Yaggi HK, Concato J, Kernan WN, Lictman JH, Brass LM, Mohsenin V. Obstructive sleep apnea as a riskfactor for stroke and death. N Engl J Med 2005; 353: 2034-41.
5. Bradley TD, Floras JS. Obstructive sleep apnea and its cardiovascular consequences. Lancet 2009; 373: 82-93.
6. Tilkian AG, Guilleminault C, Schroeder JS, Lehrman KL, Simmons FB, Dement WC. Sleep-induced apneasyndrome: prevalence of cardiac arrhythmias and their reversal after tracheostomy. Am J Med 1977; 63: 348-58.
7. Zwillich C, Devlin T, White D, Douglas N, Weil J, Martin R. Bradycardia during sleep apnea: characteristicsand mechanism. J Clin Invest 1982; 69: 1286-92.
8. Guilleminault C, Connolly SJ, Winkle RA. Cardiac arrhythmia and conduction disturbances during sleep in400 patients with sleep apnea syndrome. Am J Cardiol 1983; 52: 490-4.
9. Hoffstein V, Sateika S. Cardiac arrhythmias, snoring, and sleep apnea. Chest 1994; 106: 466-71.Gami AS, Pressman G, Caples SM, et al.
10. Association of atrial fibrillation and obstructive sleep apnea. Circulation 2004; 110: 364-7.
11. Mehra R, Benjamin EJ, Shahar E, et al. Association of nocturnal arrhythmias with sleep-disorderedbreathing. Am J Respir Crit Care Med 2006; 173: 910-6.
12. Gami AS, Hodge DO, Herges RM, et al. Obstructive sleep apnea, obesity, and the risk of incident atrialfibrillation. J Am Coll Cardiol 2007; 49: 565-71.
13. Shepard JW Jr, Garrison MW, Grither DA, Dolan GF. Relationship of ventricular ectopy to oxyhemoglobindesaturation in patients with obstructive sleep apnea. Chest 1985; 88: 335-40.
14. Fichter J, Bauer D, Arampatzis S, Fries R, Heisel A, Sybrecht GW. Sleep-related breathing disorders areassociated with ventricular arrhythmias in patients with an implantable cardioverter-defibrillator. Chest 2002;122: 558-61.
15. Gami AS, Howard DE, Olson EJ, Somers VK. Day-night pattern of sudden death in obstructive sleep apnea.N Engl J Med 2005; 352: 1206-14.
16. Monahan K, Storfer-Isser A, Mehra R, et al. Triggering of nocturnal arrhythmias by sleep-disorderedbreathing events. J Am Coll Cardiol 2009; 54: 1797-1804.

12
VANDERBILT UNIVERSITYVanderbilt Heart CommunicationsMCE, 5th floor, Ste. 51401215 21st Ave. S.Nashville, TN 37232-8802
Non-Profit Org.U.S. Postage
PAIDNashville, TN
Permit No. 3432
Visit VanderbiltHeart.com for more information on Vanderbilt Heart programs
1. Driver, J.A., et al., Incidence of cardiovascular disease and cancer in advanced age: prospective cohort study. BMJ, 2008. 337: p. a2467.
2. Oeffinger, K.C., et al., Chronic health conditions in adult survivors of childhood cancer. N Engl J Med, 2006. 355(15): p. 1572-82.
3. Horner, M., et al., SEER Cancer Statistics Review, 1975-2006 2007, National Cancer Institute: Bethesda, MD.
4. Sarkiss, M.G., et al., Impact of aspirin therapy in cancer patients with thrombocytopenia and acute coronary syndromes. Cancer, 2007. 109(3): p. 621-7.
5. Khakoo, A.Y., et al., Heart failure associated with sunitinib malate: a multitargeted receptor tyrosine kinase inhibitor. Cancer, 2008. 112(11): p. 2500-8.
6. Telli, M.L., et al., Cardiotoxicity associated with the cancer therapeutic agent sunitinib malate. Ann Oncol, 2008. 19(9): p. 1613-8.
7. Chu, T.F., et al., Cardiotoxicity associated with tyrosine kinase inhibitor sunitinib. Lancet, 2007. 370(9604): p. 2011-9.
8. Bird, B.R. and S.M. Swain, Cardiac toxicity in breast cancer survivors: review of potential cardiac problems. Clin Cancer Res, 2008. 14(1): p. 14-24.
9. Cardinale, D., et al., Prognostic value of troponin I in cardiac risk stratification of cancer patients undergoing high-dose chemotherapy. Circulation, 2004.109(22): p. 2749-54.
10. Lenihan, D.J., et al., Superior Detection of Cardiotoxicity during Chemotherapy Using Biomarkers. J Card Fail, 2007. 13(6 Supp): p. S151.
11. Cardinale, D., et al., Prevention of high-dose chemotherapy-induced cardiotoxicity in high-risk patients by angiotensin-converting enzyme inhibition.Circulation, 2006. 114(23): p. 2474-81.
12. Cardinale, D., et al., Anthracycline-Induced Cardiomyopathy: Clinical Relevance and Response to Pharmacologic Therapy. JACC, 2010. 55(3): p. 213-20.
13. Kalay, N., et al., Protective effects of carvedilol against anthracycline-induced cardiomyopathy. J Am Coll Cardiol, 2006. 48(11): p. 2258-62.
Cardiac Disease in Cancer Patients: More Common Than Realized(Continued from page 9)