vasopressors and inotropes...update on the use of vasopressors and inotropes in the intensive care...
TRANSCRIPT
VASOPRESSORS AND INOTROPES
AMER ALJUNDI, PHARM D
Shock States and Vasoactive Agents

Disclosures
§ The author does not have financial or personal
relationships with entities that may have a direct or
indirect interest in the subject matter of this
presentation

Objectives
§ Define shock and list important physiological parameters for different types of shock states
§ Apply vasoactive drug fundamentals on
hemodynamic equations
§ Explain the differences between inoconstrictors, inodilators, and pure vasoconstrictors in terms of
hemodynamic effects and adverse effects
§ Recognize reasons for refractory shock and proper selection of vasoactive agents

Shock
§ Circulatory failure that can lead tissue hypoperfusionand inadequate O2 delivery to maintain cellular metabolism
§ Hypotension is the most common clinical manifestation of shock syndromes
§ Hypotension is due toú Low systemic vascular resistance (SVR) &/orú Insufficient cardiac output (CO)

Shock Progression

Hemodynamic Mechanisms
§ Hemodynamic Equations1. BP= CO X SVR2. CO= HR X SV
Preload Afterload Inotropy
+ +_
BP = blood pressure, CO = cardiac ouput,SVR = systemic vascular resistance,HR = heart rate, SV = stroke volume, MAP = mean arterial pressure, CVP = central venous pressure
3. CO X SVR = 80 (MAP-CVP)

Types of Shock
Cold shock
Inadequate CO
Compensatory ↑SVR
Cool extremities, weak distal pulses
Cardiogenic or Obstructive Shock
Warm shock
Vasodilation (↓SVR)
Compensatory ↑CO
Warm extremities, palpable pulses
Distributive (septic) Shock

Adrenoceptor types, locations, and physiological responses
Receptor Type Primary location (s) Response when stimulated
α1 Arteries, arterioles, veins Vasonstriction (↑SVR)
β1 Heart ↑ heart rate (chronotropy) ↑ force of contraction (inotropy)
β2 Skeletal muscle blood vessels Coronary arteries
Vasodilation (↓SVR)Vasodilation
Vasopressin (V) V1: VesselsV2: RenalV3: Pituitary gland
Vasoconstriction (↑SVR)Fluid retentionCortisol release

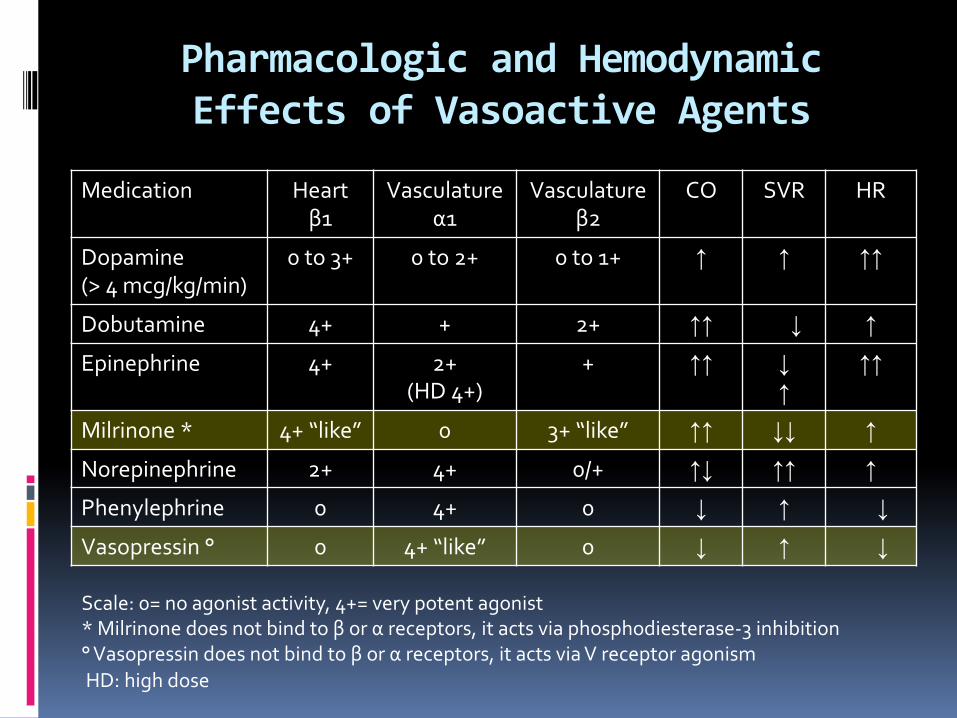
Pharmacologic and Hemodynamic Effects of Vasoactive Agents
Medication Heartβ1
Vasculatureα1
Vasculatureβ2
CO SVR HR
Dopamine (> 4 mcg/kg/min)
0 to 3+ 0 to 2+ 0 to 1+ ↑ ↑ ↑↑
Dobutamine 4+ + 2+ ↑↑ ↔↓ ↑
Epinephrine 4+ 2+ (HD 4+)
+ ↑↑ ↓↑
↑↑
Milrinone * 4+ “like” 0 3+ “like” ↑↑ ↓↓ ↑
Norepinephrine 2+ 4+ 0/+ ↑↓ ↑↑ ↑
Phenylephrine 0 4+ 0 ↓ ↑ ↔↓
Vasopressin ° 0 4+ “like” 0 ↓ ↑ ↔↓
Scale: 0= no agonist activity, 4+= very potent agonist* Milrinone does not bind to β or α receptors, it acts via phosphodiesterase-3 inhibition° Vasopressin does not bind to β or α receptors, it acts via V receptor agonismHD: high dose

Pharmacologic and Hemodynamic Effects of Vasoactive Agents
Medication Heartβ1
Vasculatureα1
Vasculatureβ2
CO SVR HR
Dopamine (> 4 mcg/kg/min)
0 to 3+ 0 to 2+ 0 to 1+ ↑ ↑ ↑↑
Dobutamine 4+ + 2+ ↑↑ ↓ ↑Epinephrine 4+ 2+
(HD 4+)+ ↑↑ ↓
↑↑↑
Milrinone * 4+ “like” 0 3+ “like” ↑↑ ↓↓ ↑Norepinephrine 2+ 4+ 0/+ ↑↓ ↑↑ ↑Phenylephrine 0 4+ 0 ↓ ↑ ↓Vasopressin ° 0 4+ “like” 0 ↓ ↑ ↓
Scale: 0= no agonist activity, 4+= very potent agonist* Milrinone does not bind to β or α receptors, it acts via phosphodiesterase-3 inhibition° Vasopressin does not bind to β or α receptors, it acts via V receptor agonismHD: high dose
Pharmacologic and Hemodynamic Effects of Vasoactive Agents
Medication Heartβ1
Vasculatureα1
Vasculatureβ2
CO SVR HR
Dopamine (> 4 mcg/kg/min)
0 to 3+ 0 to 2+ 0 to 1+ ↑ ↑ ↑↑
Dobutamine 4+ + 2+ ↑↑ ↓ ↑Epinephrine 4+ 2+
(HD 4+)+ ↑↑ ↓
↑↑↑
Milrinone * 4+ “like” 0 3+ “like” ↑↑ ↓↓ ↑Norepinephrine 2+ 4+ 0/+ ↑↓ ↑↑ ↑Phenylephrine 0 4+ 0 ↓ ↑ ↓Vasopressin ° 0 4+ “like” 0 ↓ ↑ ↓
Scale: 0= no agonist activity, 4+= very potent agonist* Milrinone does not bind to β or α receptors, it acts via phosphodiesterase-3 inhibition° Vasopressin does not bind to β or α receptors, it acts via V receptor agonismHD: high dose

Pharmacologic and Hemodynamic Effects of Vasoactive Agents
Medication Heartβ1
Vasculatureα1
Vasculatureβ2
CO SVR HR
Dopamine (> 4 mcg/kg/min)
0 to 3+ 0 to 2+ 0 to 1+ ↑ ↑ ↑↑
Dobutamine 4+ + 2+ ↑↑ ↓ ↑Epinephrine 4+ 2+
(HD 4+)+ ↑↑ ↓
↑↑↑
Milrinone * 4+ “like” 0 3+ “like” ↑↑ ↓↓ ↑Norepinephrine 2+ 4+ 0/+ ↑↓ ↑↑ ↑Phenylephrine 0 4+ 0 ↓ ↑ ↓Vasopressin ° 0 4+ “like” 0 ↓ ↑ ↓
Scale: 0= no agonist activity, 4+= very potent agonist* Milrinone does not bind to β or α receptors, it acts via phosphodiesterase-3 inhibition° Vasopressin does not bind to β or α receptors, it acts via V receptor agonismHD: high dose

Pharmacologic and Hemodynamic Effects of Vasoactive Agents
Medication Heartβ1
Vasculatureα1
Vasculatureβ2
CO SVR HR
Dopamine (> 4 mcg/kg/min)
0 to 3+ 0 to 2+ 0 to 1+ ↑ ↑ ↑↑
Dobutamine 4+ + 2+ ↑↑ ↓ ↑Epinephrine 4+ 2+
(HD 4+)+ ↑↑ ↓
↑↑↑
Milrinone * 4+ “like” 0 3+ “like” ↑↑ ↓↓ ↑Norepinephrine 2+ 4+ 0/+ ↑↓ ↑↑ ↑Phenylephrine 0 4+ 0 ↓ ↑ ↓Vasopressin ° 0 4+ “like” 0 ↓ ↑ ↓
Scale: 0= no agonist activity, 4+= very potent agonist* Milrinone does not bind to β or α receptors, it acts via phosphodiesterase-3 inhibition° Vasopressin does not bind to β or α receptors, it acts via V receptor agonismHD: high dose

Pharmacologic and Hemodynamic Effects of Vasoactive Agents
Medication Heartβ1
Vasculatureα1
Vasculatureβ2
CO SVR HR
Dopamine (> 4 mcg/kg/min)
0 to 3+ 0 to 2+ 0 to 1+ ↑ ↑ ↑↑
Dobutamine 4+ + 2+ ↑↑ ↓ ↑Epinephrine 4+ 2+
(HD 4+)+ ↑↑ ↓
↑↑↑
Milrinone * 4+ “like” 0 3+ “like” ↑↑ ↓↓ ↑Norepinephrine 2+ 4+ 0/+ ↑↓ ↑↑ ↑Phenylephrine 0 4+ 0 ↓ ↑ ↓Vasopressin ° 0 4+ “like” 0 ↓ ↑ ↓
Scale: 0= no agonist activity, 4+= very potent agonist* Milrinone does not bind to β or α receptors, it acts via phosphodiesterase-3 inhibition° Vasopressin does not bind to β or α receptors, it acts via V receptor agonismHD: high dose

Pharmacologic and Hemodynamic Effects of Vasoactive Agents
Medication Heartβ1
Vasculatureα1
Vasculatureβ2
CO SVR HR
Dopamine (> 4 mcg/kg/min)
0 to 3+ 0 to 2+ 0 to 1+ ↑ ↑ ↑↑
Dobutamine 4+ + 2+ ↑↑ ↓ ↑Epinephrine 4+ 2+
(HD 4+)+ ↑↑ ↓
↑↑↑
Milrinone * 4+ “like” 0 3+ “like” ↑↑ ↓↓ ↑Norepinephrine 2+ 4+ 0/+ ↑↓ ↑↑ ↑Phenylephrine 0 4+ 0 ↓ ↑ ↓Vasopressin ° 0 4+ “like” 0 ↓ ↑ ↓
Scale: 0= no agonist activity, 4+= very potent agonist* Milrinone does not bind to β or α receptors, it acts via phosphodiesterase-3 inhibition° Vasopressin does not bind to β or α receptors, it acts via V receptor agonismHD: high dose

Pharmacologic and Hemodynamic Effects of Vasoactive Agents
Medication Heartβ1
Vasculatureα1
Vasculatureβ2
CO SVR HR
Dopamine (> 4 mcg/kg/min)
0 to 3+ 0 to 2+ 0 to 1+ ↑ ↑ ↑↑
Dobutamine 4+ + 2+ ↑↑ ↓ ↑Epinephrine 4+ 2+
(HD 4+)+ ↑↑ ↓
↑↑↑
Milrinone * 4+ “like” 0 3+ “like” ↑↑ ↓↓ ↑Norepinephrine 2+ 4+ 0/+ ↑↓ ↑↑ ↑Phenylephrine 0 4+ 0 ↓ ↑ ↓Vasopressin ° 0 4+ “like” 0 ↓ ↑ ↓
Scale: 0= no agonist activity, 4+= very potent agonist* Milrinone does not bind to β or α receptors, it acts via phosphodiesterase-3 inhibition° Vasopressin does not bind to β or α receptors, it acts via V receptor agonismHD: high dose

Classification of Vasoactive Agents
InoconstrictiorsNorepinephrine
Epinephrine
Dopamine
Pure Vasoconstrictors
Phenylephrine
Vasopressin
InodilatorsDobutamine
Milrinone
VasodilatorsNitroglycerin
Nitroprusside
Nesiritide
Direct Inotropic Effects
Yes No
Perip
hera
l Vas
cula
r Eff
ects
Vas
odila
tion
Vas
ocon
stric
tion
Vasopressors
Inotropes

Classification of Vasoactive Agents
InoconstrictiorsNorepinephrine
Epinephrine
Dopamine
Pure Vasoconstrictors
Phenylephrine
Vasopressin
Inodilators
Dobutamine
Milrinone
Vasodilators
Nitroglycerin
Nitroprusside
Nesiritide
Direct Inotropic Effects
Yes No
Perip
hera
l Vas
cula
r Eff
ects
Vas
odila
tion
Vas
ocon
stric
tion
Vasopressors
Inotropes

Classification of Vasoactive Agents
Inoconstrictiors
Norepinephrine
Epinephrine
Dopamine
Pure Vasoconstrictors
Phenylephrine
Vasopressin
InodilatorsDobutamine
Milrinone
Vasodilators
Nitroglycerin
Nitroprusside
Nesiritide
Direct Inotropic Effects
Yes No
Perip
hera
l Vas
cula
r Eff
ects
Vas
odila
tion
Vas
ocon
stric
tion
Vasopressors
Inotropes

Classification of Vasoactive Agents
Inoconstrictiors
Norepinephrine
Epinephrine
Dopamine
Pure Vasoconstrictors
Phenylephrine
Vasopressin
Inodilators
Dobutamine
Milrinone
Vasodilators
Nitroglycerin
Nitroprusside
Nesiritide
Direct Inotropic Effects
Yes No
Perip
hera
l Vas
cula
r Eff
ects
Vas
odila
tion
Vas
ocon
stric
tion
Vasopressors
Inotropes

Classification of Vasoactive Agents
Inoconstrictiors
Norepinephrine
Epinephrine
Dopamine
Pure Vasoconstrictors
Phenylephrine
Vasopressin
Inodilators
Dobutamine
Milrinone
VasodilatorsNitroglycerin
Nitroprusside
Nesiritide
Direct Inotropic Effects
Yes No
Perip
hera
l Vas
cula
r Eff
ects
Vas
odila
tion
Vas
ocon
stric
tion
Vasopressors
Inotropes

Inodilators
§ Dobutamine§ Milrinone

Inodilator- Dobutamine
MOA Pros Cons
Agonist β1, β2 • ↑ SV/CO & ↓ afterload
• In septic or cardiogenic shock and myocardial dysfunction
• PK: Short t1/2, not excreted renally
• ↓ MAP in vasodilatory shock
• Doses>10 mcg/kg/min minimal ↑ CO d/t ↑ HR
• Tachyphylaxis
• β-Blockers impair response
• Tachyarrythmia>milrinone
MOA: mechanism of action

Inodilators- Milrinone
MOA Pros Cons
PD3 inhibitor • ↑ SV/CO
• ↓both SVR & PVR
• In patients Rx β blockers
• Less tachycardia and arrhythmia vs. dobutamine
• PK: long t1/2, renal excretion
• NOT in septic shock d/tvasodilation > dobutamine
PD3: phosphodiesterase 3PVR: pulmonary vascular resistance

Inoconstrictors
§ Norepinephrine (NE)
§ Epinephrine (EPI)
§ Dopamine (DA)

Inoconstrictors- General Info
§ 1st line vasoactive agents for majority shock statesvNorepinephrine preferredvEpinephrine & dopamine can be added when ↑CO and/or
↑HR is required

Inoconstrictors
Place in Therapy Receptor Affinity
NE 1st line in different shock states α1>> β1>>>β2
EPI •1st line: anaphylactic shock•2nd line: other shock states
•LD (β1, β2): ↑ CO/HR, ↓ SVR (inotrope)•HD (β1, β2,α1): ↑ CO/HR, ↑ SVR (vasopressor)
DA Alternative for patients with low risk of tachyarrhythmia or bradycardia induced hypotension
Low dose < 4 mcg/kg/min• Renal dose• Renal vasodilation→ ?↑ urine output
Moderate dose 4 – 10 mcg/kg/min• Inotropic/chronotropic dose• Effects on CO peak ~8 mcg/kg/min d/t ↑ SVR
High dose: >10 mcg/kg/min• Vasopressor dose• MAP increases without further CO increase
LD: low dose; HD: high dose

Inoconstrictors
Place in Therapy Receptor Affinity
NE 1st line in different shock states α1>> β1>>>β2
EPI •1st line: anaphylactic shock•2nd line: other shock states
•LD (β1, β2): ↑CO/HR, ↓ SVR (inotrope)•HD (β1, β2,α1): ↑CO/HR, ↑ SVR (vasopressor)
DA Alternative for patients with low risk of tachyarrhythmia or bradycardia induced hypotension
Low dose < 4 mcg/kg/min• Renal dose• Renal vasodilation→ ?↑ urine output
Moderate dose 4 – 10 mcg/kg/min• Inotropic/chronotropic dose• Effects on CO peak ~8 mcg/kg/min d/t ↑ SVR
High dose: >10 mcg/kg/min• Vasopressor dose• MAP increases without further CO increase
LD: low dose; HD: high dose

Inoconstrictors
Place in Therapy Receptor Affinity
NE 1st line in different shock states α1>> β1>>>β2
EPI •1st line: anaphylactic shock•2nd line: other shock states
•LD (β1, β2): ↑CO/HR, ↓ SVR (inotrope)•HD (β1, β2,α1): ↑CO/HR, ↑ SVR (vasopressor)
DA Alternative for patients with low risk of tachyarrhythmia or bradycardia induced hypotension
Low dose < 4 mcg/kg/min• Renal dose• Renal vasodilation→ ?↑ urine output
Moderate dose 4 – 10 mcg/kg/min• Inotropic/chronotropic dose• Effects on CO peak ~8 mcg/kg/min d/t ↑ SVR
High dose: >10 mcg/kg/min• Vasopressor dose• MAP increases without further CO increase
LD: low dose; HD: high dose

Inoconstrictors
Place in Therapy Receptor Affinity
NE 1st line in different shock states α1>> β1>>>β2
EPI •1st line: anaphylactic shock•2nd line: other shock states
•LD (β1, β2): ↑CO/HR, ↓ SVR (inotrope)•HD (β1, β2,α1): ↑CO/HR, ↑ SVR (vasopressor)
DA Alternative for patients with low risk of tachyarrhythmia or bradycardia induced hypotension
Low dose < 4 mcg/kg/min• Renal dose• Renal vasodilation→ ?↑ urine output
Moderate dose 4 – 10 mcg/kg/min• Inotropic/chronotropic dose• Effects on CO peak ~8 mcg/kg/min d/t ↑ SVR
High dose: >10 mcg/kg/min• Vasopressor dose• MAP increases without further CO increase
LD: low dose; HD: high dose

Pure Vasoconstrictors
§ Phenylephrine§ Vasopressin

Pure Vasoconstrictors- General Info
§ 2nd line in most shock statesvMainly with uncontrolled tachycardiavVasodilatory/distributive shock when SVR is low and CO
is adequate

Pure Vasopressor Place in Therapy Pearl
Phenylephrine • Should not be used for cardiogenic shock
• Septic shock ifo NE triggers serious arrhythmias
• Add on in persistent hypotension /hypoperfusion with high CO
Good choice• Left ventricular outflow
tract obstructiono Severe aortic stenosiso Hypertrophic obstructive
cardiomyopathy
Vasopressin Good choice•During acidemia•RV failure d/t ↑PVR•Fixed dose
(0.03-0.04 U/min)
RV: right ventricle; PVR: pulmonary vascular resistance; SSC: surviving sepsis campaign

Positive Inotropy
Vasoconstriction
Vasodilation
Dobutamine Milrinone
Phenylephrine Vasopressin Norepinephrine HD epinephrine
HD dopamine LD epinephrine/dopamine

Management of Shock and Refractory Shock
IV fluids
MAP <65 mm Hg &/or SB< 90 mm Hg• UOP >0.5 ml/kg/hour• Normal or ↓ lactate• Near-normal venous O2
saturation
No
Yes
No
YesCVP<12 mm Hg
Norepinephrine (NE)
MAP >65 mm Hg on NE <1mcg/kg/min Refractory shock
HypovolemiaHypocortisolismAcidosisHypocalcemia
Reversible causes
+ epinephrineWarm/cold
Cold (low CO)Warm (low SVR) + dobutamine+ vasopressin(+ phenylephrine)
Adequate organ perfusion
corrected

Potential Adverse Effects of Vasoactive Agents
Agent Tachy-arrythmia
Peripheralvasoconstriction (digital ischemia)
Gut mucosalHypoperfusion
(increased lactate)
Increasedmyocardial O2 demand (MI)
Dobutamine ++++ +/- +++ ++
Dopamine ++++ + + ++
Epinephrine +++ + +++ ++
Norepinephrine + +++ +/- +
Phenylephrine +/- + + +/-
Vasopressin +/- +++ +++ ++

References
1. Jentzer JC, Coons JC, Link CB, et al. Pharmacotherapy update on the use of vasopressors and inotropes in the intensive care unit. J Cardiovasc Pharmacol Ther. 2015 May;20(3):249-60.
2. Moranville MP, Mieure KD, Santayana EM. Evaluation and management of shock States: hypovolemic, distributive, and cardiogenic shock. J Pharm Pract. 2011 Feb;24(1):44-60

THANK YOU