veno-occlusive disease: “new perspectives” day... · veno-occlusive disease: “new...
TRANSCRIPT
Mairéad NíChonghaile
CNS HSCT
Dublin, Ireland
Veno-Occlusive Disease: “New Perspectives”
Veno-occlusive disease
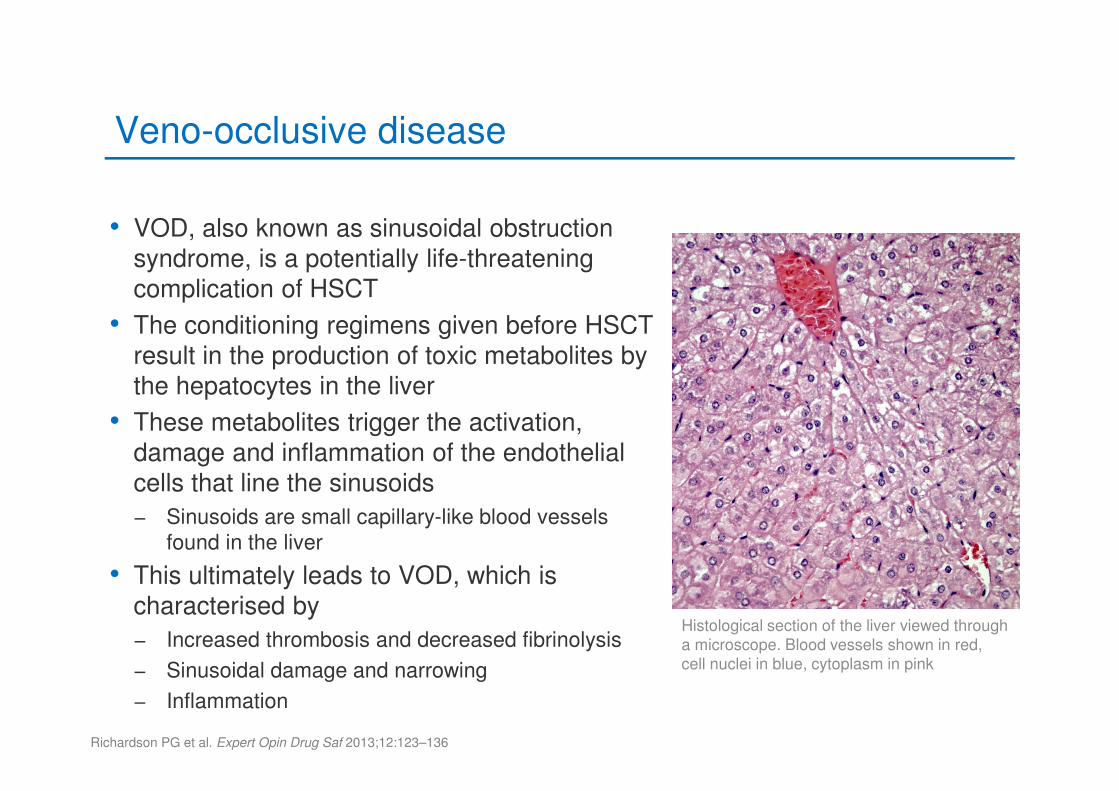
• VOD, also known as sinusoidal obstruction
syndrome, is a potentially life-threatening
complication of HSCT
• The conditioning regimens given before HSCT
result in the production of toxic metabolites by
the hepatocytes in the liver
• These metabolites trigger the activation,
damage and inflammation of the endothelial
cells that line the sinusoids
− Sinusoids are small capillary-like blood vessels
found in the liver
• This ultimately leads to VOD, which is
characterised by
− Increased thrombosis and decreased fibrinolysis
− Sinusoidal damage and narrowing
− Inflammation
Richardson PG et al. Expert Opin Drug Saf 2013;12:123–136
Histological section of the liver viewed through a microscope. Blood vessels shown in red, cell nuclei in blue, cytoplasm in pink
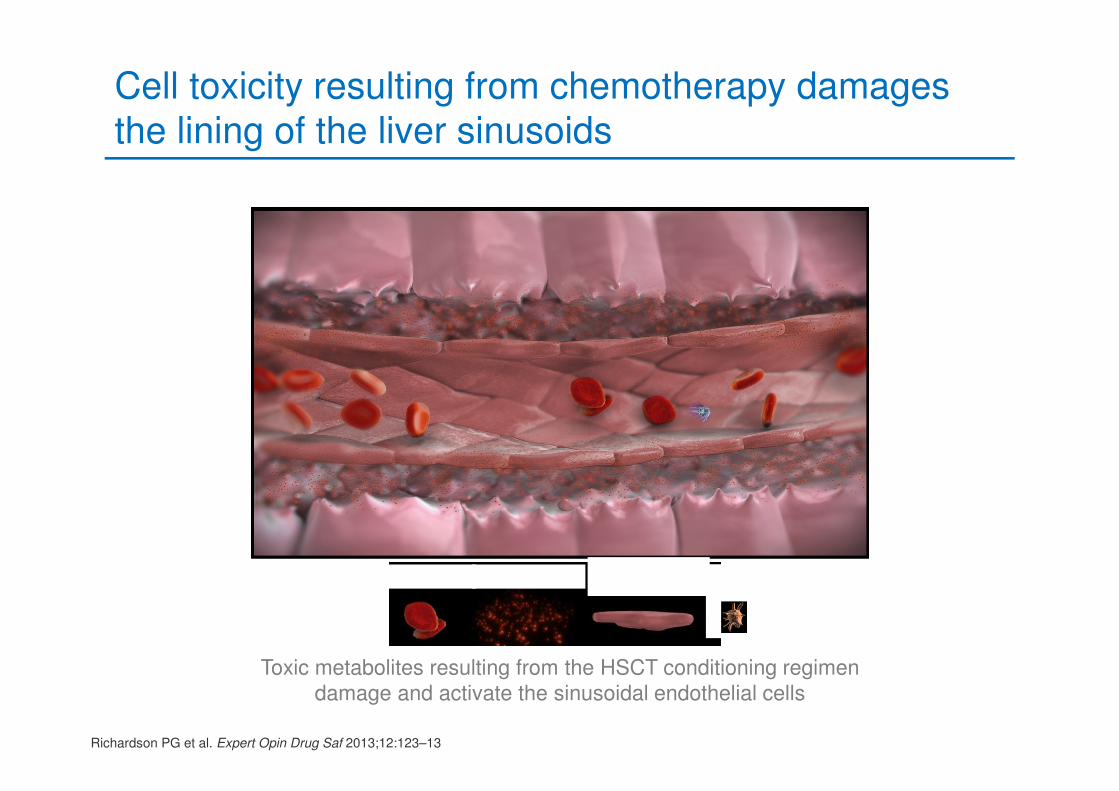
Cell toxicity resulting from chemotherapy damages the lining of the liver sinusoids
Toxic metabolites resulting from the HSCT conditioning regimen
damage and activate the sinusoidal endothelial cells
Richardson PG et al. Expert Opin Drug Saf 2013;12:123–13
Red blood cells Toxic metabolitesSinusoidal
endothelial cellsPlatelets
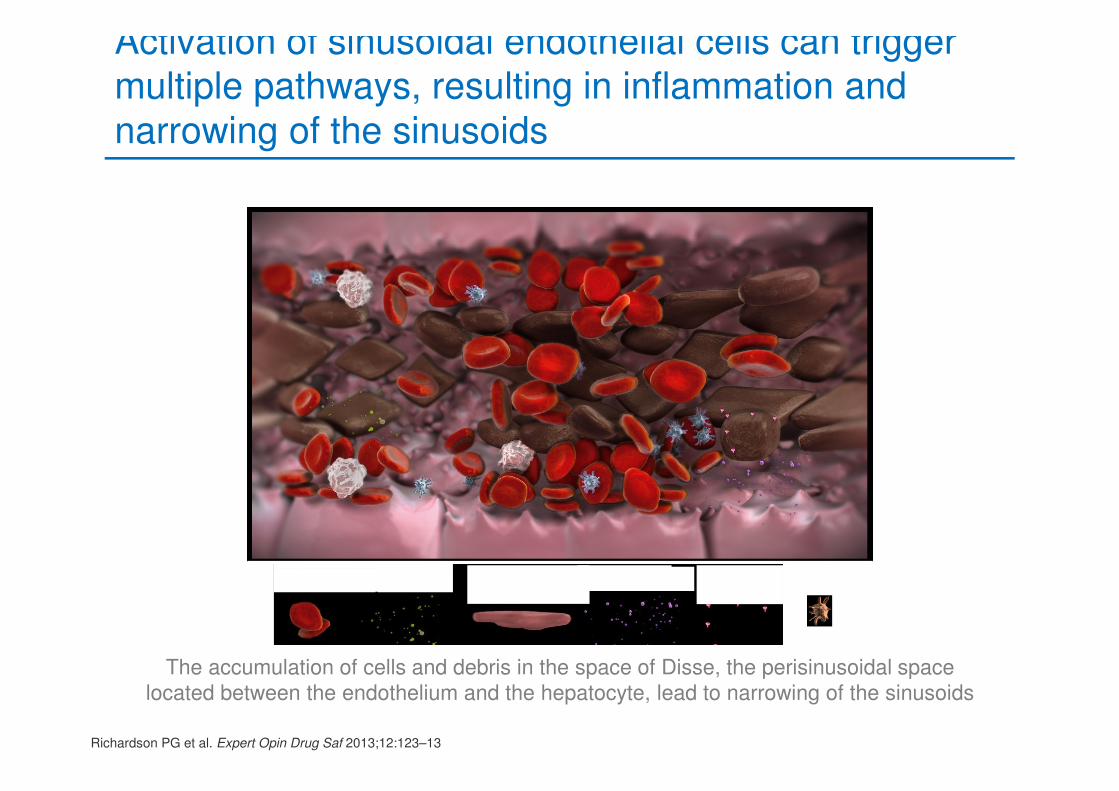
Activation of sinusoidal endothelial cells can trigger multiple pathways, resulting in inflammation and narrowing of the sinusoids
Richardson PG et al. Expert Opin Drug Saf 2013;12:123–13
The accumulation of cells and debris in the space of Disse, the perisinusoidal space
located between the endothelium and the hepatocyte, lead to narrowing of the sinusoids
Red blood cells Cytokines Sinusoidal endothelial cells
Cytokines Heparanase Adhesion molecules
Platelets
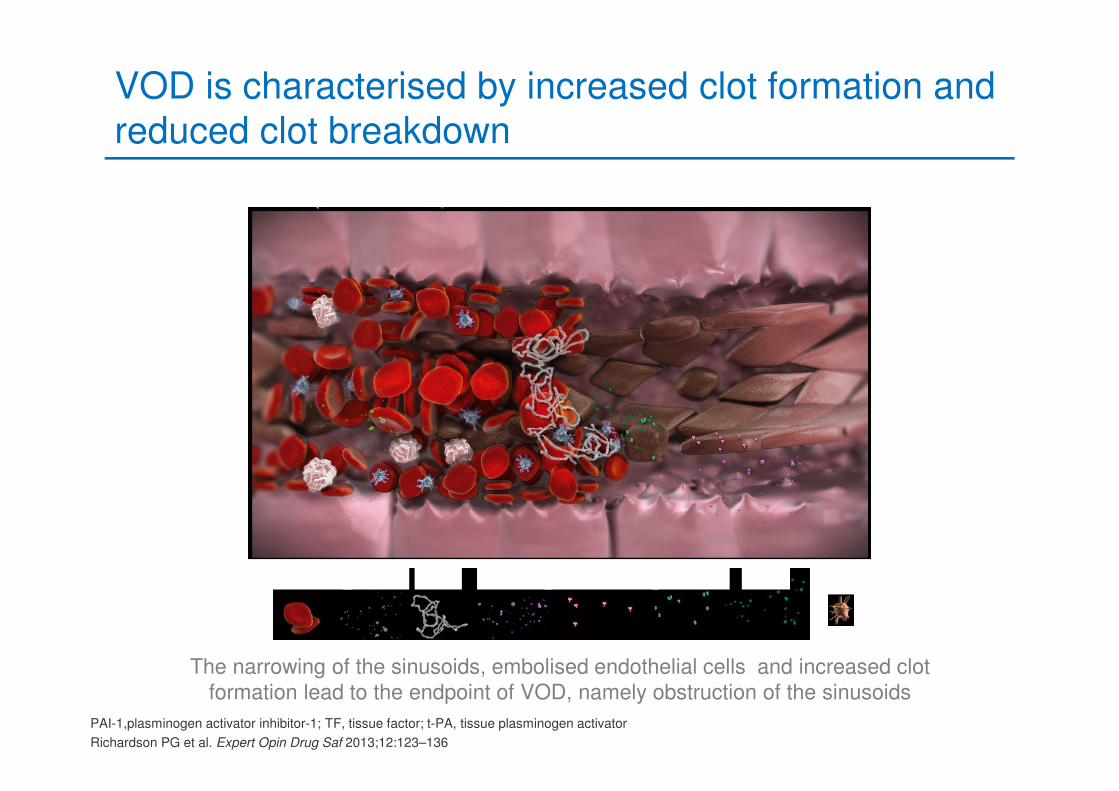
VOD is characterised by increased clot formation and reduced clot breakdown
PAI-1,plasminogen activator inhibitor-1; TF, tissue factor; t-PA, tissue plasminogen activator
Richardson PG et al. Expert Opin Drug Saf 2013;12:123–136
The narrowing of the sinusoids, embolised endothelial cells and increased clot
formation lead to the endpoint of VOD, namely obstruction of the sinusoids
Red blood cells Cytokines Fibrin Heparanase Adhesion molecules Tissue factor PAI-1 Platelets
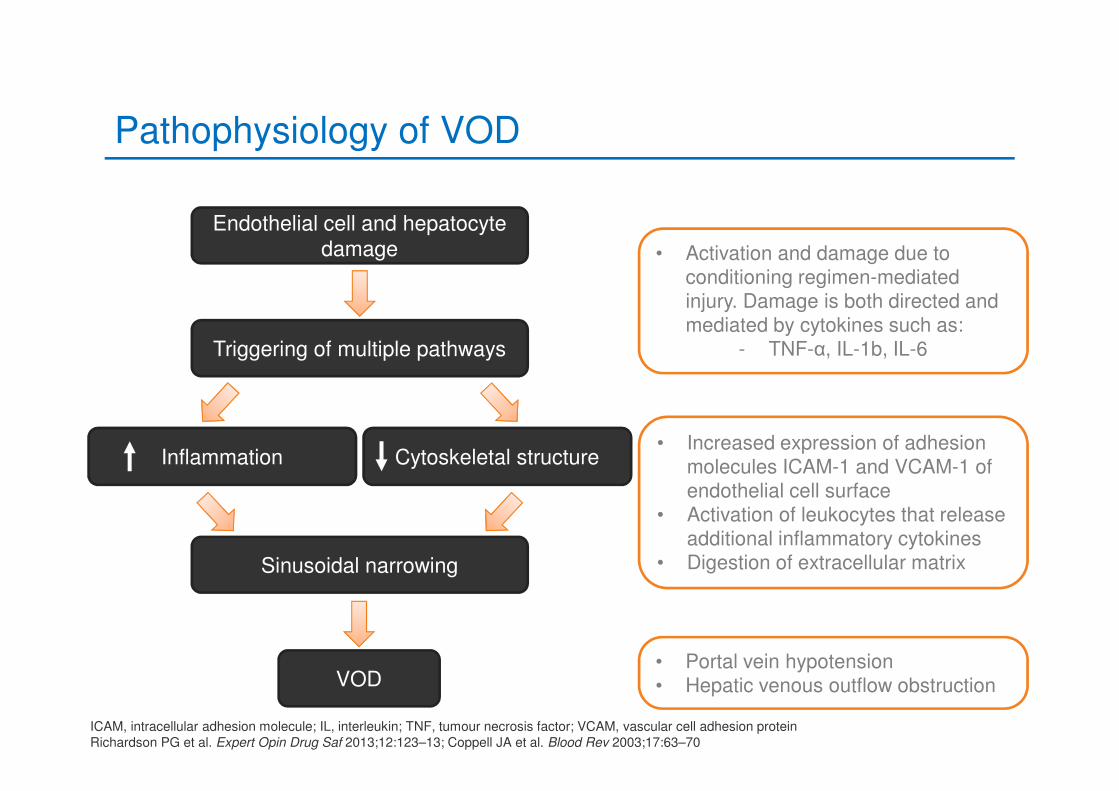
Pathophysiology of VOD
ICAM, intracellular adhesion molecule; IL, interleukin; TNF, tumour necrosis factor; VCAM, vascular cell adhesion protein
Richardson PG et al. Expert Opin Drug Saf 2013;12:123–13; Coppell JA et al. Blood Rev 2003;17:63–70
Triggering of multiple pathways
Inflammation Cytoskeletal structure
Sinusoidal narrowing
Endothelial cell and hepatocyte
damage
VOD
• Activation and damage due to conditioning regimen-mediated injury. Damage is both directed and mediated by cytokines such as:
- TNF-α, IL-1b, IL-6
• Increased expression of adhesion molecules ICAM-1 and VCAM-1 of endothelial cell surface
• Activation of leukocytes that release additional inflammatory cytokines
• Digestion of extracellular matrix
• Portal vein hypotension• Hepatic venous outflow obstruction
Summary of VOD pathophysiology
• The conditioning regimen given prior to HSCT increases endothelial cell activation, resulting in damage to the SECs and hepatocytes
• The accumulation of cells in the space of Disse (the perisinusoidal space), increased inflammation and formation of clots lead to narrowing of the sinusoids
• This results in VOD, which is characterised by blockage of the sinusoids, portal vein hypotension and reduced hepatic venous outflow
Severe VOD/SOS: Case study
• 37-year-old lady
• September 2008 – CML. p210 BCRABL
• Rx imatinib – haematological toxicity
• Switched to dasatinib – more haematological toxicity
• October 2009 Philadelphia chromosome negative
• September 2012 CML transforming to AML
VOD, Veno-occlusive disease; SOS, Sinusoidal obstruction syndrome; CML, Chronic myeloid leukaemia; Rx, Prescription; BM, Bone marrow; AML,
Acute myeloid leukaemia
Mairéad NíChonghaile, personal communication March 2014
Severe VOD/SOS: Case study
• September 2012 dasatinib stopped
• October 2012 Cycle 1 DAT 3+10
• December 2012 Cycle 2
• Conditioning – IV Busulfan/Cyclophosphamide
• February 2013 sibling allogeneic bone marrow transplant
DAT, Daunorubicin, cytarabine, thioguanine
Mairéad NíChonghaile, personal communication March 2014
Nursing assessment
• Weigh patients daily
• Measure abdominal girth
• Monitor urea and electrolytes
• Monitor fluids in/out
• Assess all sites for bleeding
• Assess pain level and source
• Blood tests
Helmy A et al. Aliment Pharmacol Ther 2006;23:11–25; Eisenberg S. Oncol Nurs Forum 2008;35:385–397; Sosa EC. Clin J Oncol
Nurs. 2012;16:507-13.
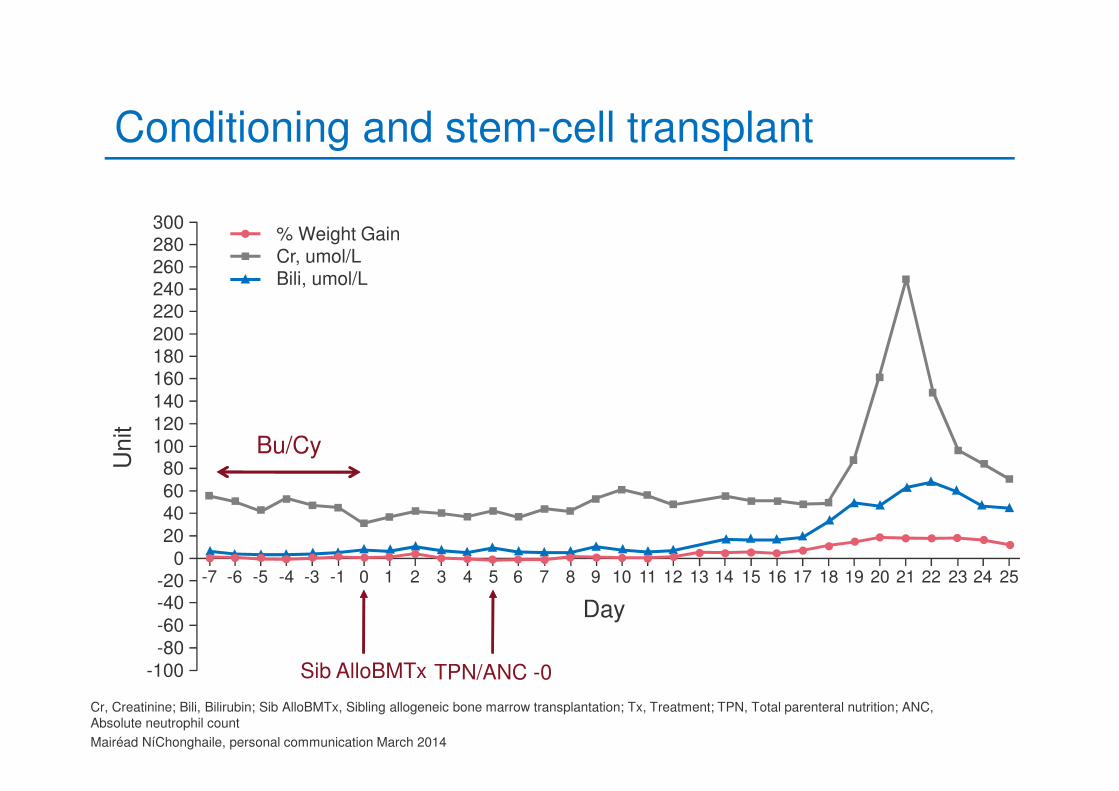
Conditioning and stem-cell transplant
Sib AlloBMTx
Bu/Cy
300% Weight GainCr, umol/LBili, umol/L
280260240220
200180160
140
120
10080
6040
20
0-20-40
-60
-80
-100
Unit
-7 -6 -5 -4 -3 -1 0 1 2 3 4 5 6 7 8
Day
9 10 11 12 13 14 15 16 17 2524232221201918
Cr, Creatinine; Bili, Bilirubin; Sib AlloBMTx, Sibling allogeneic bone marrow transplantation; Tx, Treatment; TPN, Total parenteral nutrition; ANC,
Absolute neutrophil count
Mairéad NíChonghaile, personal communication March 2014
TPN/ANC -0
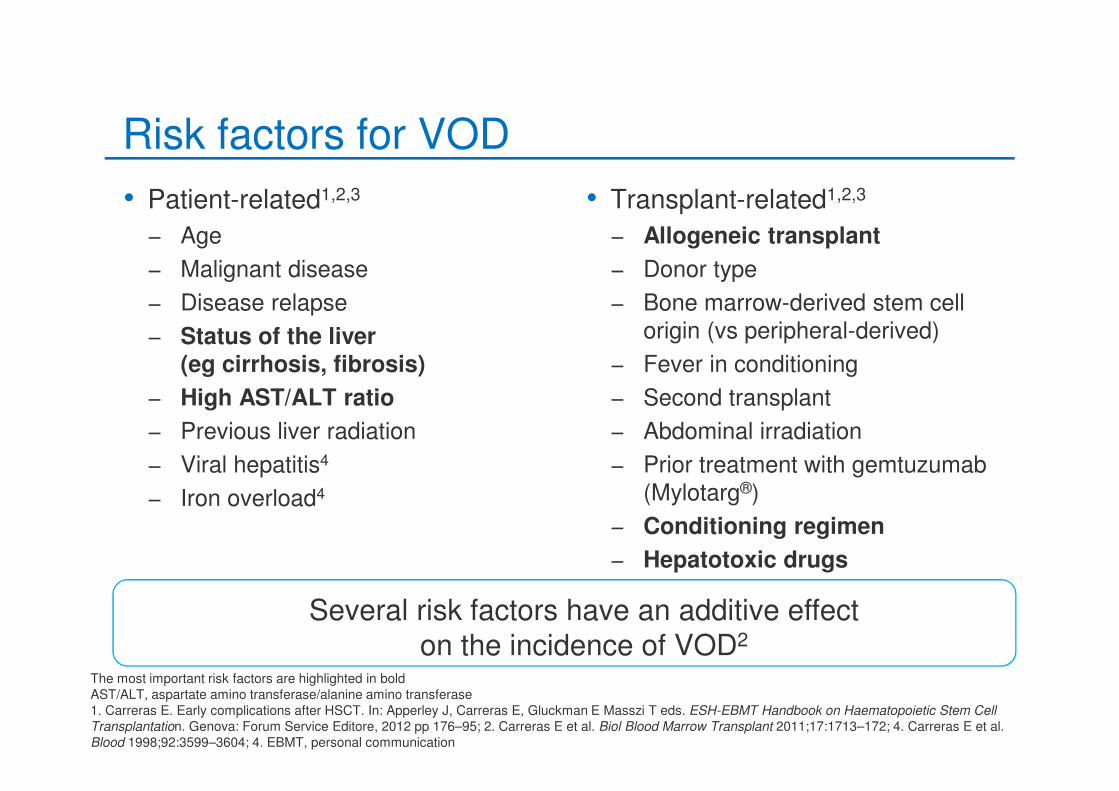
Risk factors for VOD
• Patient-related1,2,3
− Age
− Malignant disease
− Disease relapse
− Status of the liver(eg cirrhosis, fibrosis)
− High AST/ALT ratio
− Previous liver radiation
− Viral hepatitis4
− Iron overload4
• Transplant-related1,2,3
− Allogeneic transplant
− Donor type
− Bone marrow-derived stem cell origin (vs peripheral-derived)
− Fever in conditioning
− Second transplant
− Abdominal irradiation
− Prior treatment with gemtuzumab (Mylotarg®)
− Conditioning regimen
− Hepatotoxic drugs
The most important risk factors are highlighted in bold
AST/ALT, aspartate amino transferase/alanine amino transferase
1. Carreras E. Early complications after HSCT. In: Apperley J, Carreras E, Gluckman E Masszi T eds. ESH-EBMT Handbook on Haematopoietic Stem Cell
Transplantation. Genova: Forum Service Editore, 2012 pp 176–95; 2. Carreras E et al. Biol Blood Marrow Transplant 2011;17:1713–172; 4. Carreras E et al.
Blood 1998;92:3599–3604; 4. EBMT, personal communication
Several risk factors have an additive effect on the incidence of VOD2
Which of the following patient characteristics represent VOD risk factors?
• 1: Malignant disease
• 2: Conditioning with busulfan
• 3: Allogeneic transplantation
• 4: All of the above
37-year-old ladyCML. p210 BCRABLRx imatinib – haematological toxicity Switched to dasatinib – more haematological toxicity Philadelphia chromosome negativeCML transforming to AMLCycle 1 DAT 3+10Conditioning – IV Busulfan/CyclophosphamideSibling allogeneic transplant
Which of the following patient characteristics represent VOD risk factors?
37-year-old ladyCML. p210 BCRABLRx imatinib – haematological toxicity Switched to dasatinib – more haematological toxicity Philadelphia chromosome negativeCML transforming to AMLCycle 1 DAT 3+10Conditioning – IV Busulfan/CyclophosphamideSibling allogeneic transplant
0%
13%
10%
77%
� Malignant disease
� Conditioning with busulfan
� Allogeneic transplantation
� All of the above
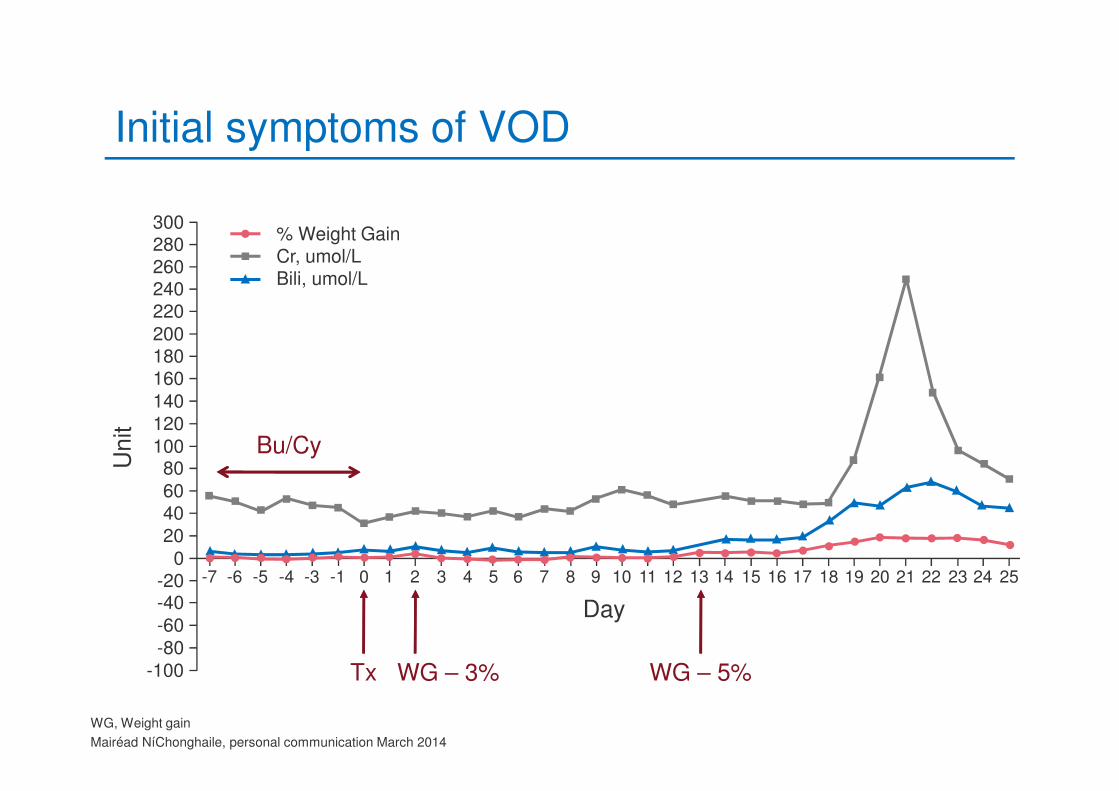
Initial symptoms of VOD
WG – 3% WG – 5%Tx
Bu/Cy
300% Weight GainCr, umol/LBili, umol/L
280260240220
200180160
140
120
10080
6040
20
0-20-40
-60
-80
-100
Unit
-7 -6 -5 -4 -3 -1 0 1 2 3 4 5 6 7 8
Day
9 10 11 12 13 14 15 16 17 2524232221201918
WG, Weight gain
Mairéad NíChonghaile, personal communication March 2014
What was the first symptom suggesting the development of VOD?
• 1: Post-transplant nausea
• 2: Neutropenic sepsis
• 3: Weight gain > 3%
• 4: CML transforming to AML
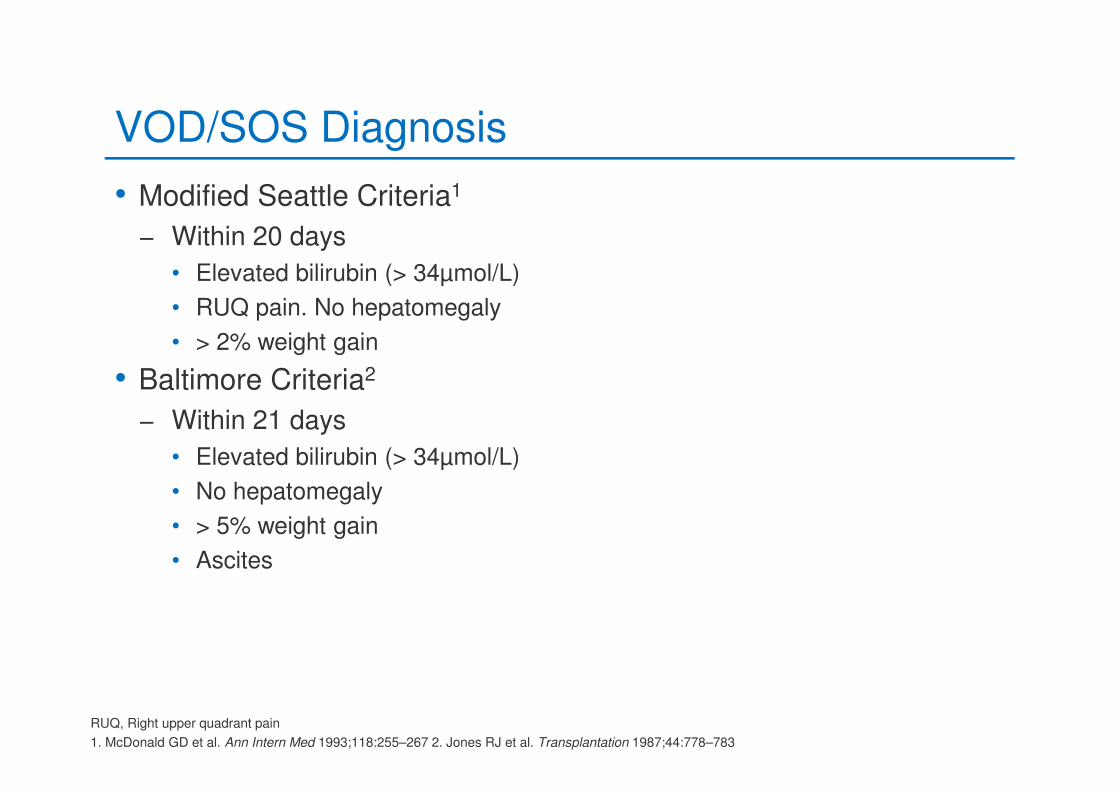
VOD/SOS Diagnosis
• Modified Seattle Criteria1
− Within 20 days
• Elevated bilirubin (> 34µmol/L)
• RUQ pain. No hepatomegaly
• > 2% weight gain
• Baltimore Criteria2
− Within 21 days
• Elevated bilirubin (> 34µmol/L)
• No hepatomegaly
• > 5% weight gain
• Ascites
RUQ, Right upper quadrant pain
1. McDonald GD et al. Ann Intern Med 1993;118:255–267 2. Jones RJ et al. Transplantation 1987;44:778–783
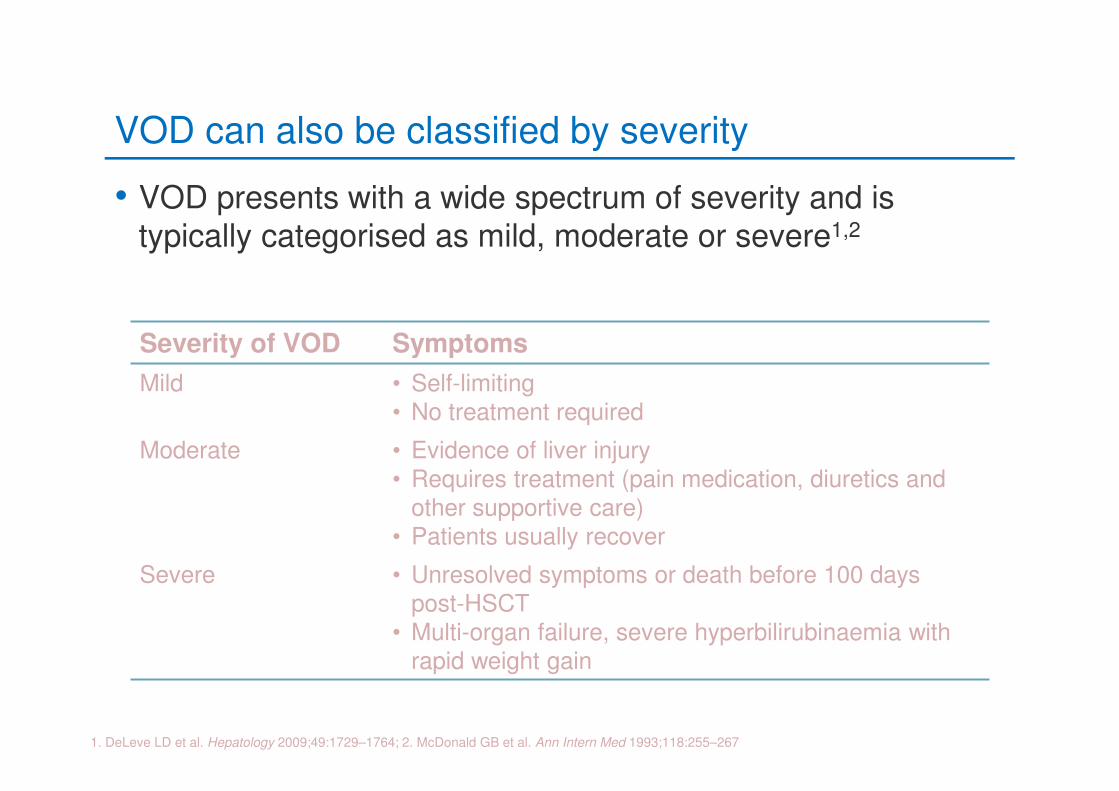
VOD can also be classified by severity
• VOD presents with a wide spectrum of severity and is typically categorised as mild, moderate or severe1,2
1. DeLeve LD et al. Hepatology 2009;49:1729–1764; 2. McDonald GB et al. Ann Intern Med 1993;118:255–267
Severity of VOD Symptoms
Mild • Self-limiting• No treatment required
Moderate • Evidence of liver injury• Requires treatment (pain medication, diuretics and
other supportive care)• Patients usually recover
Severe • Unresolved symptoms or death before 100 days post-HSCT
• Multi-organ failure, severe hyperbilirubinaemia with rapid weight gain
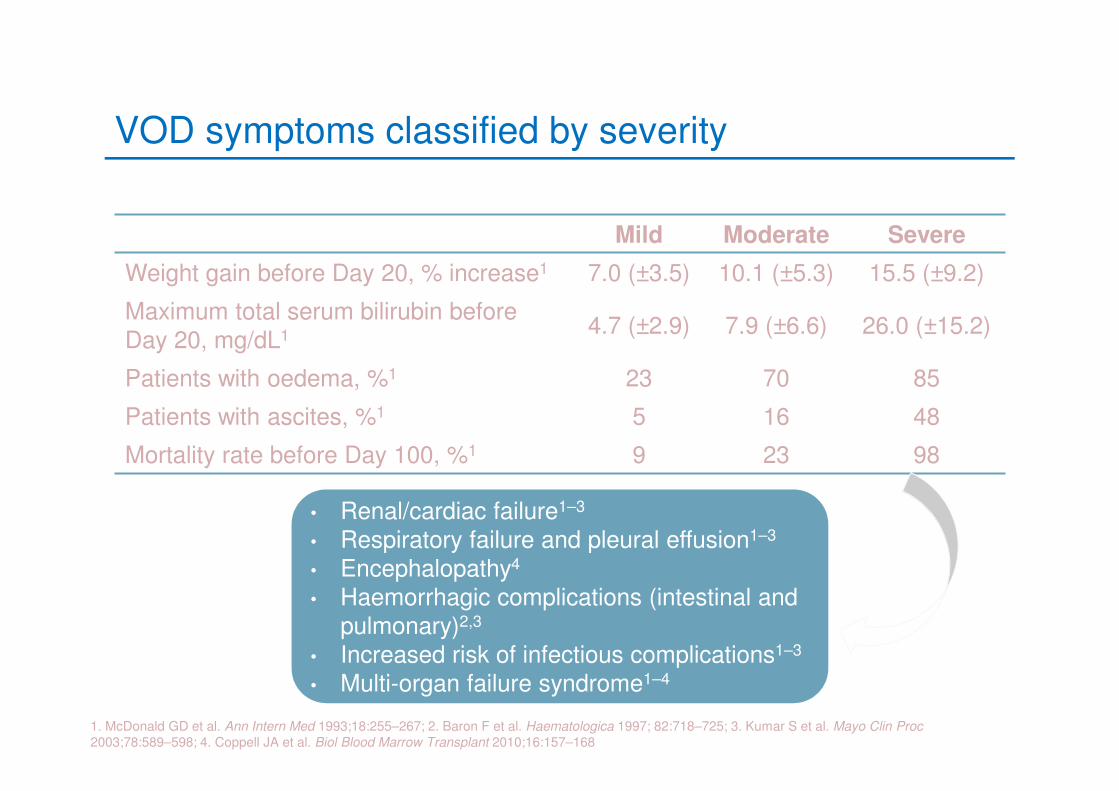
VOD symptoms classified by severity
Mild Moderate Severe
Weight gain before Day 20, % increase1 7.0 (±3.5) 10.1 (±5.3) 15.5 (±9.2)
Maximum total serum bilirubin beforeDay 20, mg/dL1 4.7 (±2.9) 7.9 (±6.6) 26.0 (±15.2)
Patients with oedema, %1 23 70 85
Patients with ascites, %1 5 16 48
Mortality rate before Day 100, %1 9 23 98
1. McDonald GD et al. Ann Intern Med 1993;18:255–267; 2. Baron F et al. Haematologica 1997; 82:718–725; 3. Kumar S et al. Mayo Clin Proc
2003;78:589–598; 4. Coppell JA et al. Biol Blood Marrow Transplant 2010;16:157–168
• Renal/cardiac failure1–3
• Respiratory failure and pleural effusion1–3
• Encephalopathy4
• Haemorrhagic complications (intestinal and pulmonary)2,3
• Increased risk of infectious complications1–3
• Multi-organ failure syndrome1–4
Nursing management of VOD
• Restrict fluid intake
• Administer analgesia
• Position patient comfortably
• Administer blood products
• Administer electrolytes
• Administer medications
• Provide psychological support
• Provide family support
Management of VOD is mainly supportive
Helmy A et al. Aliment Pharmacol Ther 2006;23:11–25; Eisenberg S. Oncol Nurs Forum 2008;35:385–397; Sosa EC. Clin J Oncol
Nurs. 2012;16:507-13.
Traditional treatment of VOD
Current management strategies: primarily
supportive measures1,2
Heparin + rt-PA
Diuresis to minimise oedema
Sodium and fluid restriction
Haemofiltration and haemodialysis
Analgesia
Response in up to 30% of patients, but overall survival is poor2,3,4
Associated with increased risk of life-threatening bleeding2,3
Not recommended in patients with sVOD who have already developed multi-organ failure3,4
Should be avoided in patients with pulmonary or renal failure2,4
rt-PA, recombinant tissue plasminogen activator, sVOD, severe VOD
1. DeLeve LD et al. Hepatology 2009;49:1729–1764; 2. Helmy A et al. Aliment Pharmacol Ther 2006;23:11–25; 3. Bearman SI et al. Blood 1997;89:1501–
1506; 4. Ho V et al. Bone Marrow Transplant 2007;3:373–388
Rationale for development of new therapiesfor VOD
• Traditional strategies are supportive, and treatments are associated with significant risk of bleeding1,2
• However, severe VOD remains a serious complication of HSCT with a high mortality rate (> 80%)3
Effective therapies are therefore required for both the prophylaxis and treatment of severe VOD
HSCT, haematopoietic stem cell transplantation
1. Helmy A. Aliment Pharmacol Ther 2006;23:11–25; 2. Bearman SI et al. Blood 1997;89:1501–1506; 3. Coppell JA et al. Biol Blood Marrow Transplant
2010;16:157–168
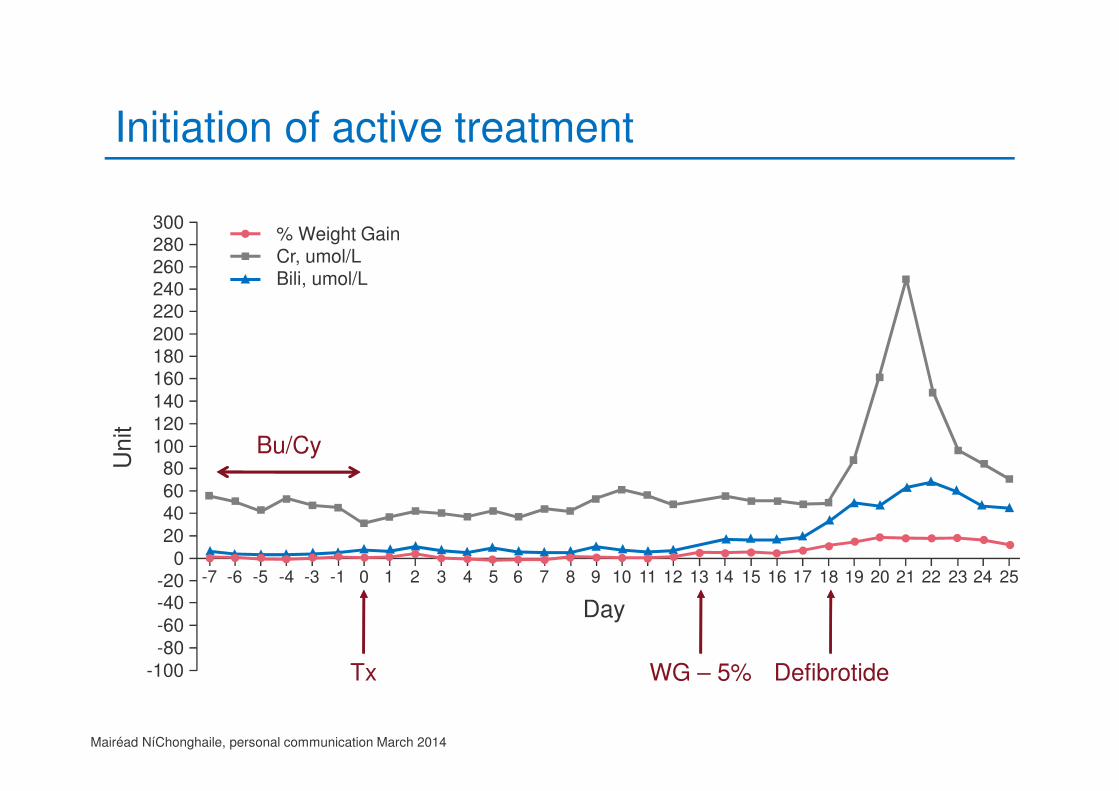
Initiation of active treatment
DefibrotideWG – 5%Tx
Bu/Cy
300% Weight GainCr, umol/LBili, umol/L
280260240220
200180160
140
120
10080
6040
20
0-20-40
-60
-80
-100
Unit
-7 -6 -5 -4 -3 -1 0 1 2 3 4 5 6 7 8
Day
9 10 11 12 13 14 15 16 17 2524232221201918
Mairéad NíChonghaile, personal communication March 2014
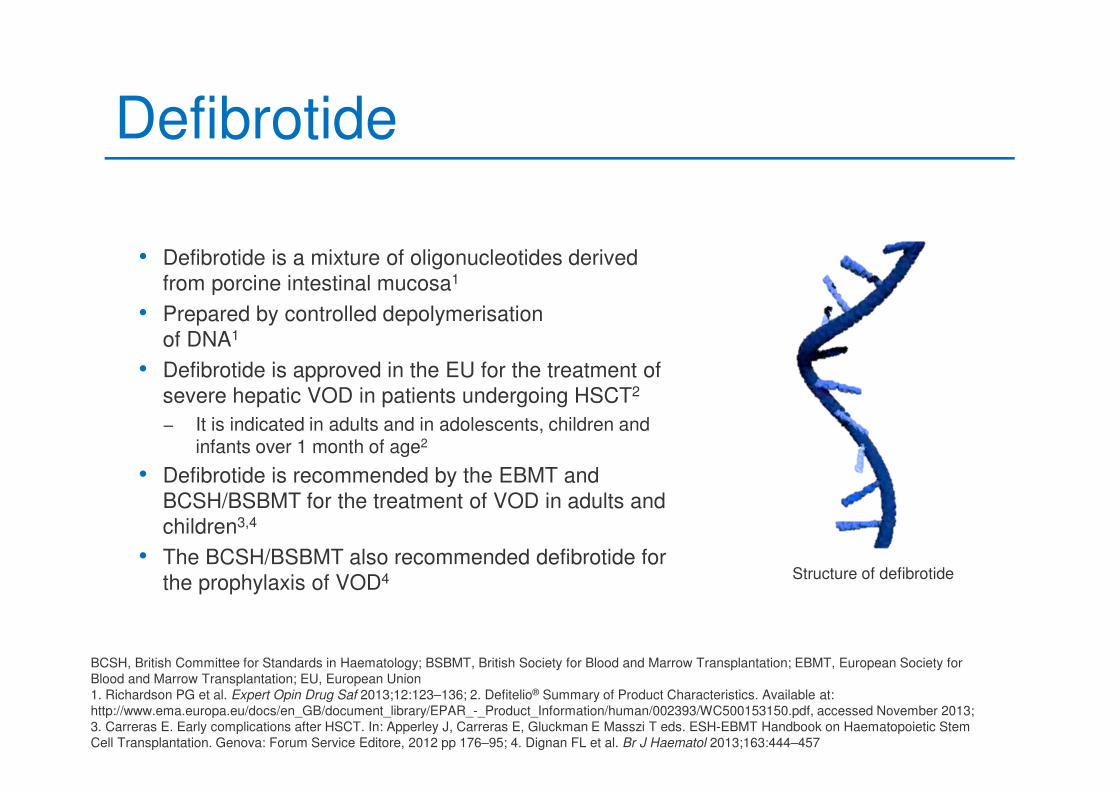
Defibrotide
• Defibrotide is a mixture of oligonucleotides derived
from porcine intestinal mucosa1
• Prepared by controlled depolymerisation
of DNA1
• Defibrotide is approved in the EU for the treatment of
severe hepatic VOD in patients undergoing HSCT2
− It is indicated in adults and in adolescents, children and infants over 1 month of age2
• Defibrotide is recommended by the EBMT and
BCSH/BSBMT for the treatment of VOD in adults and
children3,4
• The BCSH/BSBMT also recommended defibrotide for
the prophylaxis of VOD4
BCSH, British Committee for Standards in Haematology; BSBMT, British Society for Blood and Marrow Transplantation; EBMT, European Society for
Blood and Marrow Transplantation; EU, European Union
1. Richardson PG et al. Expert Opin Drug Saf 2013;12:123–136; 2. Defitelio® Summary of Product Characteristics. Available at:
http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002393/WC500153150.pdf, accessed November 2013;
3. Carreras E. Early complications after HSCT. In: Apperley J, Carreras E, Gluckman E Masszi T eds. ESH-EBMT Handbook on Haematopoietic Stem
Cell Transplantation. Genova: Forum Service Editore, 2012 pp 176–95; 4. Dignan FL et al. Br J Haematol 2013;163:444–457
Structure of defibrotide
Defibrotide – mechanism of action
Defitelio® Summary of Product Characteristics available at: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-
_Product_Information/human/002393/WC500153150.pdf, accessed November 2013; 2. Richardson PG et al. Expert Opin Drug Saf 2013;12:123–136;
3. Coppell JA et al. Biol Blood Marrow Transplant 2010;16:157–168
Restores thrombo-
fibrinolytic balance
Defibrotide
Protects endothelial
cells
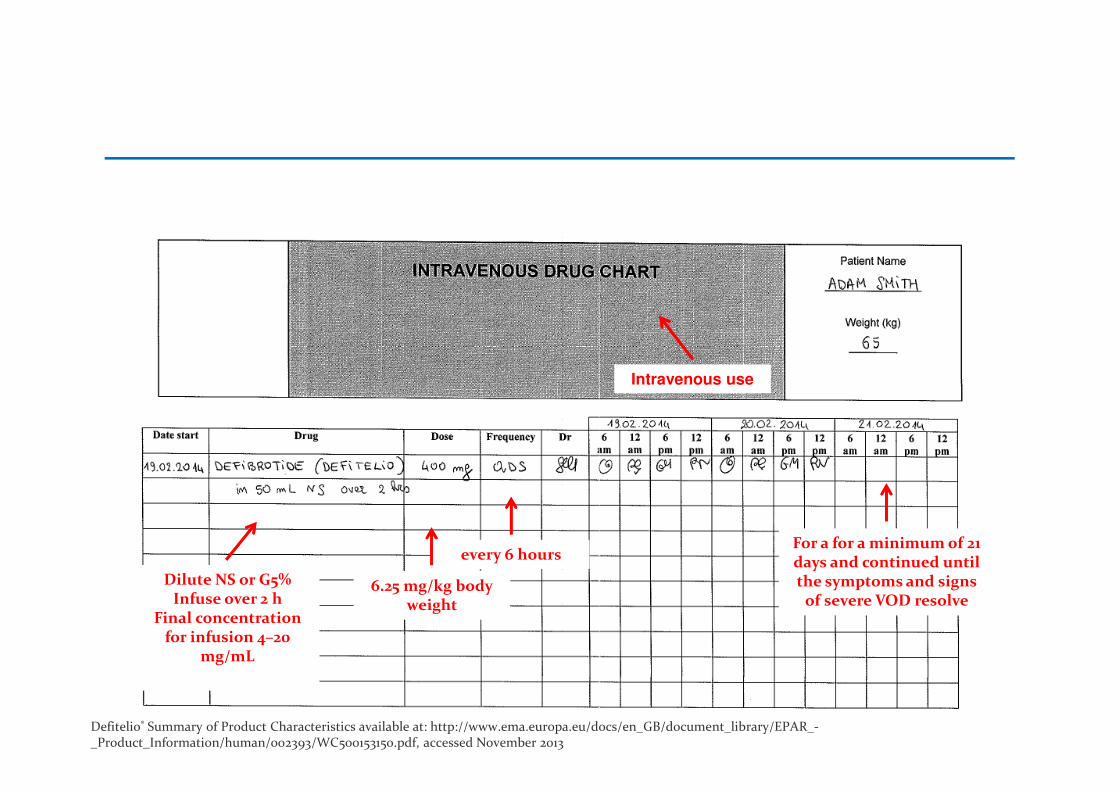
Intravenous use
6.25 mg/kg body weight
every 6 hours
Dilute NS or G5%Infuse over 2 h
Final concentration for infusion 4–20
mg/mL
For a for a minimum of 21 days and continued until the symptoms and signs
of severe VOD resolve
Defibrotide administration
Defitelio® Summary of Product Characteristics available at: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-_Product_Information/human/002393/WC500153150.pdf, accessed November 2013
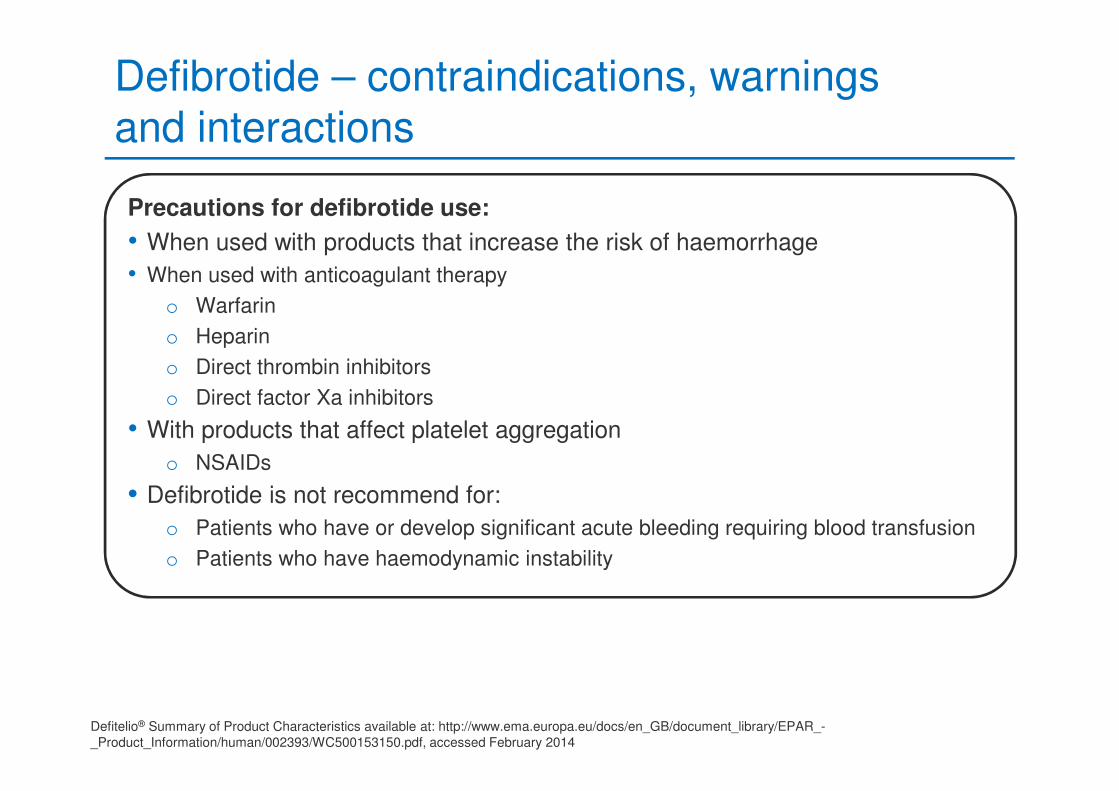
Defibrotide – contraindications, warningsand interactions
Precautions for defibrotide use:
• When used with products that increase the risk of haemorrhage
• When used with anticoagulant therapy
o Warfarin
o Heparin
o Direct thrombin inhibitors
o Direct factor Xa inhibitors
• With products that affect platelet aggregation
o NSAIDs
• Defibrotide is not recommend for:
o Patients who have or develop significant acute bleeding requiring blood transfusion
o Patients who have haemodynamic instability
Defitelio® Summary of Product Characteristics available at: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-
_Product_Information/human/002393/WC500153150.pdf, accessed February 2014
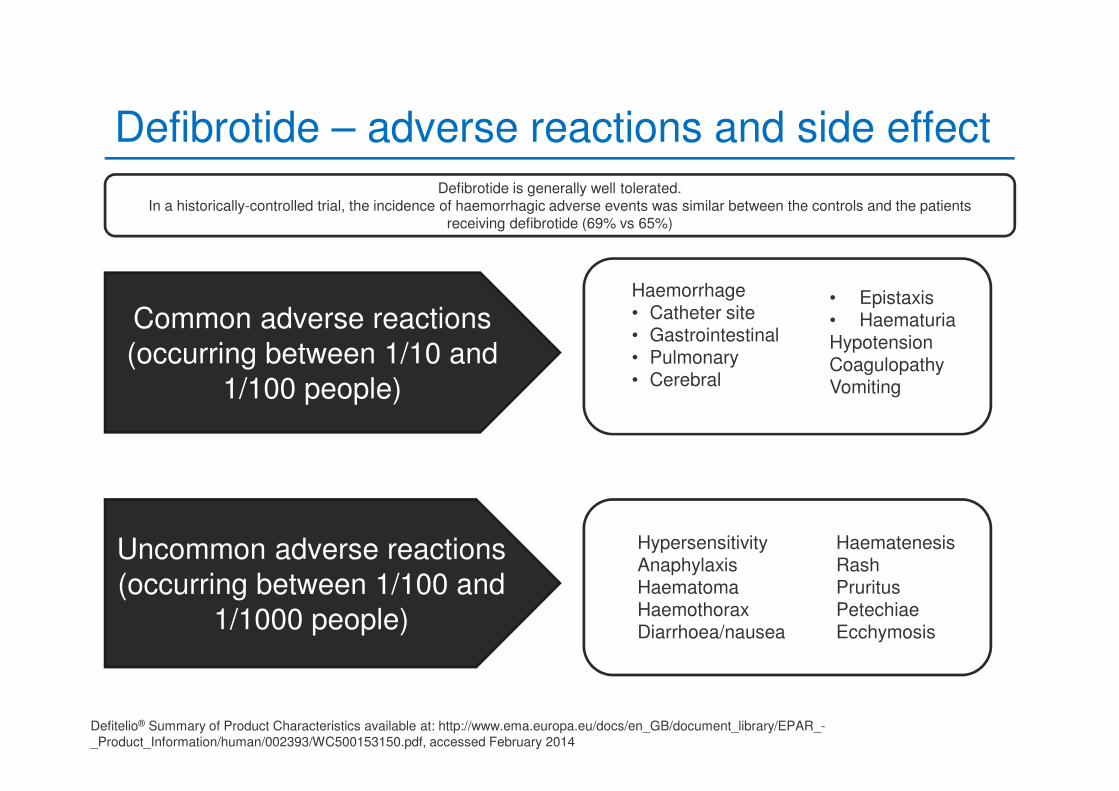
Defibrotide – adverse reactions and side effect
Common adverse reactions(occurring between 1/10 and
1/100 people)
Uncommon adverse reactions(occurring between 1/100 and
1/1000 people)
Defibrotide is generally well tolerated.In a historically-controlled trial, the incidence of haemorrhagic adverse events was similar between the controls and the patients
receiving defibrotide (69% vs 65%)
Haemorrhage• Catheter site• Gastrointestinal• Pulmonary• Cerebral
• Epistaxis• HaematuriaHypotensionCoagulopathyVomiting
HypersensitivityAnaphylaxisHaematomaHaemothoraxDiarrhoea/nausea
HaematenesisRashPruritusPetechiaeEcchymosis
Defitelio® Summary of Product Characteristics available at: http://www.ema.europa.eu/docs/en_GB/document_library/EPAR_-
_Product_Information/human/002393/WC500153150.pdf, accessed February 2014
Which of the following is not a precaution or contraindication when using defibrotide?
• 1: Anti-coagulant use
• 2: Haemodynamic instability
• 3: Right upper quadrant pain
• 4: NSAIDs
When used with products that increase the risk of haemorrhage
When used with anticoagulant therapy
With products that affect platelet aggregation
Patients who have or develop significant acute bleeding requiring blood transfusion
Patients who have haemodynamic instability
Resolution and post-VOD care
• Day +40 discharged from HSCT unit
− Attended day unit daily
− LFTs – bilirubin 23; Alk Phos 178; GGT 87; AST 30
• Day +43 bilirubin within normal range
− No clinical signs of VOD
• 10 months post-transplant all LFTs returned to normal
• One-year post-transplant
− In remission
− Normal FBC
− No GvHD
− Normal liver function tests
− Returning to work
LFT, Liver function test; Alk Phos, Alkaline phosphatase; GGT, Gamma glutamyl transpeptidase; AST, Aspartate transaminase; FBC, Full blood count;
GvHD, Graft-versus-host disease
Mairéad NíChonghaile, personal communication March 2014
Summary
• VOD remains a significant cause of morbidity and mortality following HSCT
• New treatment options give grounds for optimism
• Nurses play a major role
− Early recognition
− Supportive care
• We find defibrotide an effective treatment for severe VOD within our patient group
Mairéad NíChonghaile, personal communication March 2014
EBMT VOD Learning Programme
• Card in your binder
• Available at Eusapharma Booth