ventana hematopathology solutions comprehensive aids for ... · ventana hematopathology solutions...
TRANSCRIPT
VENTANA hematopathology solutionsComprehensive aids for detecting and subtyping
1 12/4/2015 9:47:24 AM
On the cover Top: Follicular lymphoma stained with BCL-2 (SP66) Rabbit Monoclonal Primary Antibody. Bottom: Classical Hodgkin lymphoma stained with CD30 (BER-H2) Mouse Monoclonal Primary Antibody.
2 Hematopathology diagnostic solutions
Contents
VENTANA hematopathology assays 3
Detecting and subtyping hematological cancers 4
The importance of immunohistochemistry as an aid in diagnosis 4
The challenge of hematopathology: many cancers and many tests 4
Guideline organizations and classification systems 5
Diagnostic approaches and key considerations 5
Mature B-cell lymphomas: the most commonly encountered cancers 6
Mature T-cell lymphomas: rare and aggressive cancers 7
Follicular lymphoma 8
Introduction: disease and epidemiology 8
Key diseases in the differential diagnosis 9
Key markers that aid diagnosis 9
Diffuse large B-cell lymphoma 10
Introduction: disease and epidemiology 10
Key diseases in differential diagnosis 11
Key markers that aid diagnosis 11
Chronic lymphocytic leukemia/small lymphocytic lymphoma 12
Introduction: disease and epidemiology 12
Key diseases in differential diagnosis 13
Key markers that aid diagnosis 13
Mantle cell lymphoma 14
Introduction: disease and epidemiology 14
Key diseases in differential diagnosis 14
Key markers that aid diagnosis 15
Hodgkin lymphoma 16
Introduction: disease and epidemiology 16
Key diseases in differential diagnosis 16
Key markers that aid diagnosis 18
VENTANA hematopathology solutions: comprehensive, robust, innovative 19
2 12/4/2015 9:47:24 AM
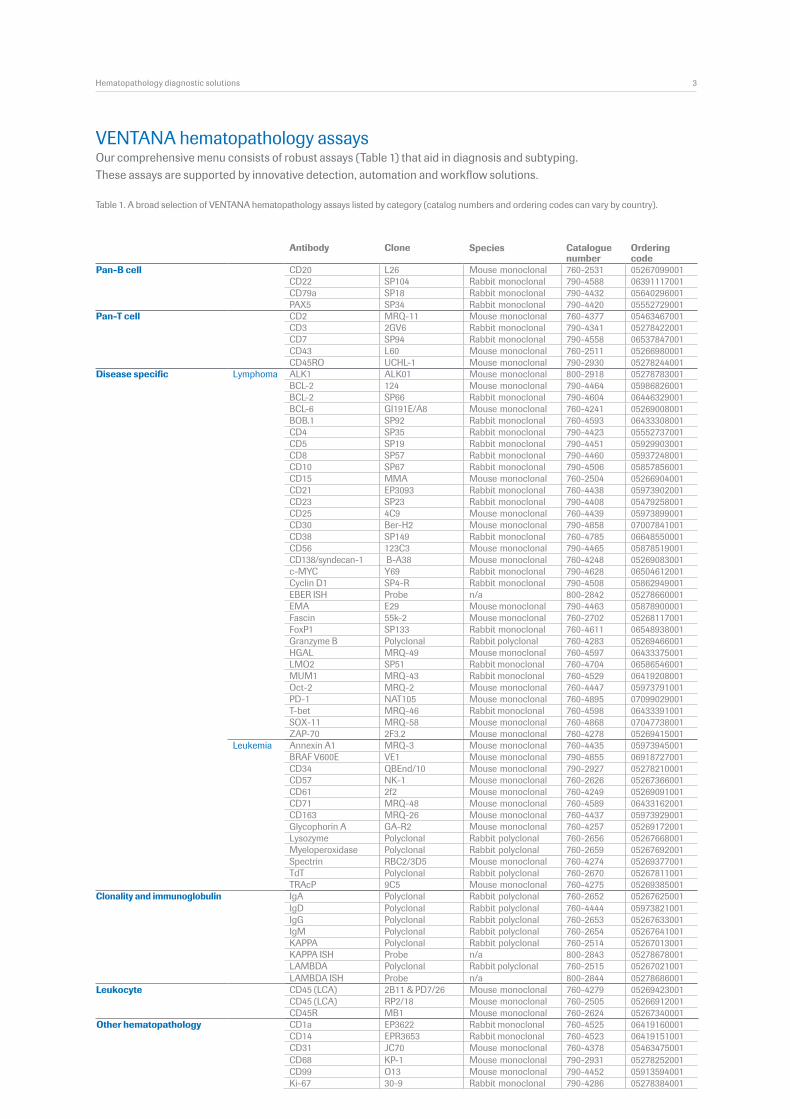
Table 1. A broad selection of VENTANA hematopathology assays listed by category (catalog numbers and ordering codes can vary by country).
Our comprehensive menu consists of robust assays (Table 1) that aid in diagnosis and subtyping. These assays are supported by innovative detection, automation and workflow solutions.
VENTANA hematopathology assays
Pan-B cell CD20 L26 Mouse monoclonal 760-2531 05267099001CD22 SP104 Rabbit monoclonal 790-4588 06391117001CD79a SP18 Rabbit monoclonal 790-4432 05640296001PAX5 SP34 Rabbit monoclonal 790-4420 05552729001
Pan-T cell CD2 MRQ-11 Mouse monoclonal 760-4377 05463467001CD3 2GV6 Rabbit monoclonal 790-4341 05278422001CD7 SP94 Rabbit monoclonal 790-4558 06537847001CD43 L60 Mouse monoclonal 760-2511 05266980001CD45RO UCHL-1 Mouse monoclonal 790-2930 05278244001
Disease specific Lymphoma ALK1 ALK01 Mouse monoclonal 800-2918 05278783001BCL-2 124 Mouse monoclonal 790-4464 05986826001BCL-2 SP66 Rabbit monoclonal 790-4604 06446329001BCL-6 GI191E/A8 Mouse monoclonal 760-4241 05269008001BOB.1 SP92 Rabbit monoclonal 760-4593 06433308001CD4 SP35 Rabbit monoclonal 790-4423 05552737001CD5 SP19 Rabbit monoclonal 790-4451 05929903001CD8 SP57 Rabbit monoclonal 790-4460 05937248001CD10 SP67 Rabbit monoclonal 790-4506 05857856001CD15 MMA Mouse monoclonal 760-2504 05266904001CD21 EP3093 Rabbit monoclonal 760-4438 05973902001CD23 SP23 Rabbit monoclonal 790-4408 05479258001CD25 4C9 Mouse monoclonal 760-4439 05973899001CD30 Ber-H2 Mouse monoclonal 790-4858 07007841001CD38 SP149 Rabbit monoclonal 760-4785 06648550001CD56 123C3 Mouse monoclonal 790-4465 05878519001CD138/syndecan-1 B-A38 Mouse monoclonal 760-4248 05269083001c-MYC Y69 Rabbit monoclonal 790-4628 06504612001Cyclin D1 SP4-R Rabbit monoclonal 790-4508 05862949001EBER ISH Probe n/a 800-2842 05278660001EMA E29 Mouse monoclonal 790-4463 05878900001Fascin 55k-2 Mouse monoclonal 760-2702 05268117001FoxP1 SP133 Rabbit monoclonal 760-4611 06548938001Granzyme B Polyclonal Rabbit polyclonal 760-4283 05269466001HGAL MRQ-49 Mouse monoclonal 760-4597 06433375001LMO2 SP51 Rabbit monoclonal 760-4704 06586546001MUM1 MRQ-43 Rabbit monoclonal 760-4529 06419208001Oct-2 MRQ-2 Mouse monoclonal 760-4447 05973791001PD-1 NAT105 Mouse monoclonal 760-4895 07099029001
T-bet MRQ-46 Rabbit monoclonal 760-4598 06433391001 SOX-11 MRQ-58 Mouse monoclonal 760-4868 07047738001 ZAP-70 2F3.2 Mouse monoclonal 760-4278 05269415001Leukemia Annexin A1 MRQ-3 Mouse monoclonal 760-4435 05973945001 BRAF V600E VE1 Mouse monoclonal 790-4855 06918727001 CD34 QBEnd/10 Mouse monoclonal 790-2927 05278210001 CD57 NK-1 Mouse monoclonal 760-2626 05267366001 CD61 2f2 Mouse monoclonal 760-4249 05269091001 CD71 MRQ-48 Mouse monoclonal 760-4589 06433162001 CD163 MRQ-26 Mouse monoclonal 760-4437 05973929001 Glycophorin A GA-R2 Mouse monoclonal 760-4257 05269172001 Lysozyme Polyclonal Rabbit polyclonal 760-2656 05267668001 Myeloperoxidase Polyclonal Rabbit polyclonal 760-2659 05267692001
Spectrin RBC2/3D5 Mouse monoclonal 760-4274 05269377001 TdT Polyclonal Rabbit polyclonal 760-2670 05267811001 TRAcP 9C5 Mouse monoclonal 760-4275 05269385001Clonality and immunoglobulin IgA Polyclonal Rabbit polyclonal 760-2652 05267625001 IgD Polyclonal Rabbit polyclonal 760-4444 05973821001 IgG Polyclonal Rabbit polyclonal 760-2653 05267633001 IgM Polyclonal Rabbit polyclonal 760-2654 05267641001 KAPPA Polyclonal Rabbit polyclonal 760-2514 05267013001 KAPPA ISH Probe n/a 800-2843 05278678001 LAMBDA Polyclonal Rabbit polyclonal 760-2515 05267021001 LAMBDA ISH Probe n/a 800-2844 05278686001Leukocyte CD45 (LCA) 2B11 & PD7/26 Mouse monoclonal 760-4279 05269423001 CD45 (LCA) RP2/18 Mouse monoclonal 760-2505 05266912001 CD45R MB1 Mouse monoclonal 760-2624 05267340001Other hematopathology CD1a EP3622 Rabbit monoclonal 760-4525 06419160001 CD14 EPR3653 Rabbit monoclonal 760-4523 06419151001 CD31 JC70 Mouse monoclonal 760-4378 05463475001 CD68 KP-1 Mouse monoclonal 790-2931 05278252001 CD99 O13 Mouse monoclonal 790-4452 05913594001 Ki-67 30-9 Rabbit monoclonal 790-4286 05278384001
Hematopathology diagnostic solutions 3
Antibody Clone Species Catalogue number
Ordering code
3 12/4/2015 9:47:24 AM
The importance of immunohistochemistry as an aid in diagnosis?The stated goal of the World Health Organization (WHO) classification of tumors of hematopoietic and lymphoid tissues is to define real diseases that appear to be distinct clinical entities by using all available information, including morphology, immunophenotyping, genetic features and clinical features.2 Thus, diagnosis of hematopathological cancers often requires the use of immunohistochemistry/immunophenotype information to aid in confirming or excluding a particular diagnosis. Ventana Medical Systems, Inc. (“Ventana”) is committed to assisting you in your quest to accurately diagnose and subtype hematopathological diseases (Table 1).?The challenge of hematopathology: many cancers and many tests?One of the key challenges in hematopathology is the growing number of types and subtypes of cancers and the plethora of available markers to assist in diagnosis and classification. So, the pathologist is faced with a large differential diagnosis and needs to manage adjunctive tests including immunohistochemistry (IHC) and in situ hybridization (ISH) effectively.?Hematological malignancies account for 6–7% of cancers globally, but constitute about 20–30% of IHC testing volume in anatomic pathology laboratories, which is a large volume of testing relative to the incidence of the disease.2 The extensive ability to type and subtype hematological cancers has been demonstrated to be clinically relevant. For example, survival and treatment response differ between a Burkitt’s lymphoma and a diffuse large B-cell lymphoma not otherwise specified (DLBCL, NOS), so making an accurate diagnosis is essential for optimal patient outcomes.2, 3
Detecting and subtyping hematological cancers
“Although morphologic examination of a well-fixed, well-stained, thin paraffin section remains the first prerequisite for the diagnosis of lymphoma, the burgeoning weight of the literature is that, with rare exceptions, morphology alone is not sufficient for today.”1
4 Hematopathology diagnostic solutions
4 12/4/2015 9:47:24 AM
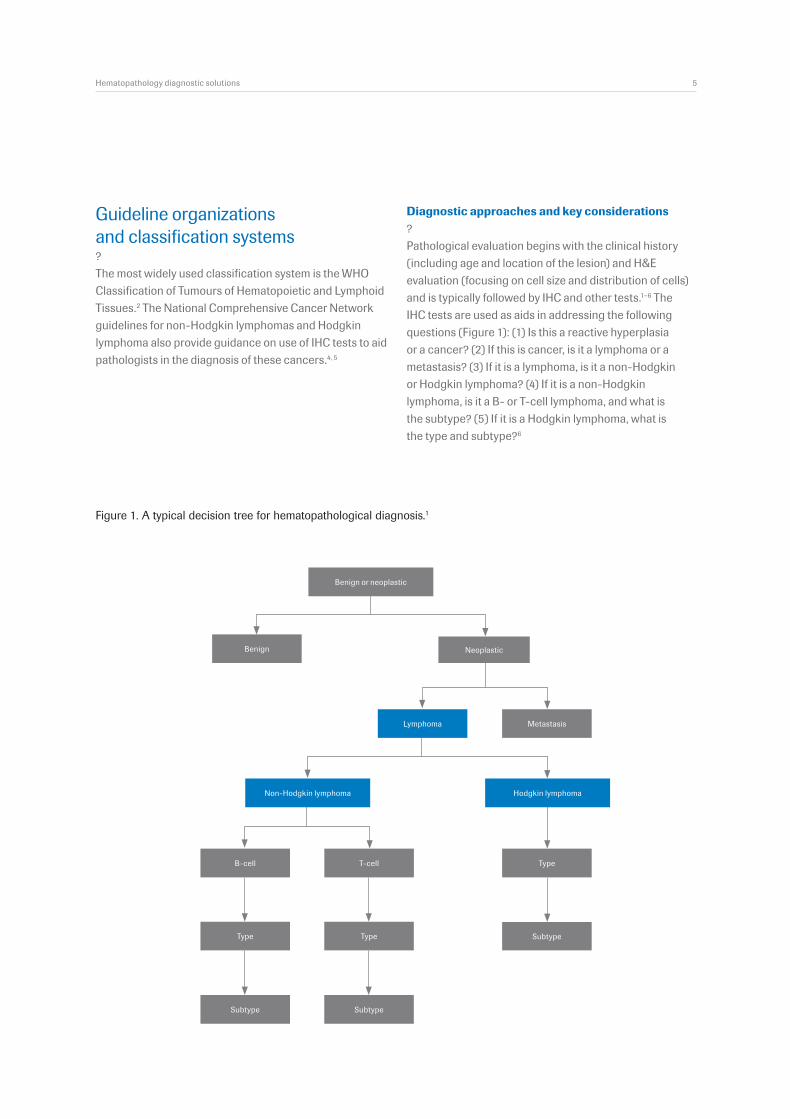
Figure 1. A typical decision tree for hematopathological diagnosis.1
Benign
Subtype
TypeB-cell
Type Type
Subtype Subtype
T-cell
MetastasisLymphoma
Non-Hodgkin lymphoma Hodgkin lymphoma
Neoplastic
Benign or neoplastic
Guideline organizations and classification systems ?The most widely used classification system is the WHO Classification of Tumours of Hematopoietic and Lymphoid Tissues.2 The National Comprehensive Cancer Network guidelines for non-Hodgkin lymphomas and Hodgkin lymphoma also provide guidance on use of IHC tests to aid pathologists in the diagnosis of these cancers.4, 5
Hematopathology diagnostic solutions 5
Diagnostic approaches and key considerations?Pathological evaluation begins with the clinical history (including age and location of the lesion) and H&E evaluation (focusing on cell size and distribution of cells) and is typically followed by IHC and other tests.1–6 The IHC tests are used as aids in addressing the following questions (Figure 1): (1) Is this a reactive hyperplasia or a cancer? (2) If this is cancer, is it a lymphoma or a metastasis? (3) If it is a lymphoma, is it a non-Hodgkin or Hodgkin lymphoma? (4) If it is a non-Hodgkin lymphoma, is it a B- or T-cell lymphoma, and what is the subtype? (5) If it is a Hodgkin lymphoma, what is the type and subtype?6
5 12/4/2015 9:47:24 AM
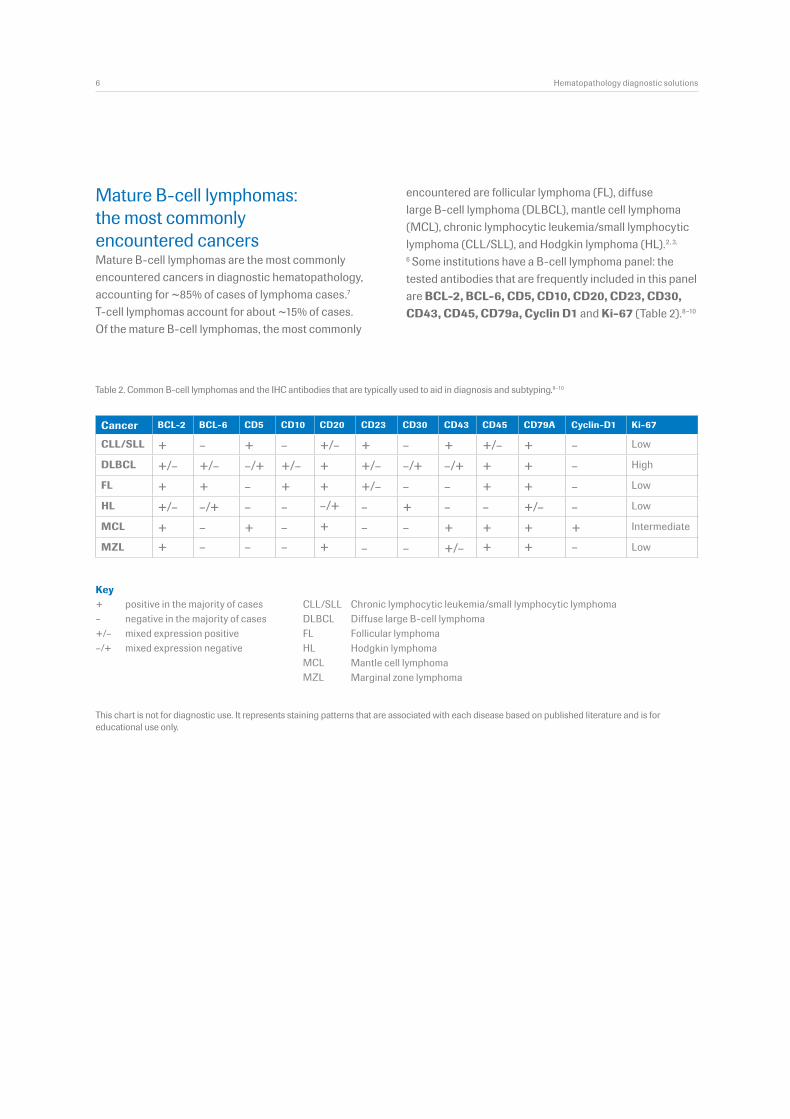
Mature B-cell lymphomas: the most commonly encountered cancersMature B-cell lymphomas are the most commonly encountered cancers in diagnostic hematopathology, accounting for ~85% of cases of lymphoma cases.7 T-cell lymphomas account for about ~15% of cases. Of the mature B-cell lymphomas, the most commonly
encountered are follicular lymphoma (FL), diffuse large B-cell lymphoma (DLBCL), mantle cell lymphoma (MCL), chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL), and Hodgkin lymphoma (HL).2, 3,
6 Some institutions have a B-cell lymphoma panel: the tested antibodies that are frequently included in this panel are BCL-2, BCL-6, CD5, CD10, CD20, CD23, CD30, CD43, CD45, CD79a, Cyclin D1 and Ki-67 (Table 2).8–10
Cancer BCL-2 BCL-6 CD5 CD10 CD20 CD23 CD30 CD43 CD45 CD79A Cyclin-D1 Ki-67
CLL/SLL + – + – +/– + – + +/– + – Low
DLBCL +/– +/– –/+ +/– + +/– –/+ –/+ + + – High
FL + + – + + +/– – – + + – Low
HL +/– –/+ – – –/+ – + – – +/– – Low
MCL + – + – + – – + + + + Intermediate
MZL + – – – + – – +/– + + – Low
+–+/––/+
Keypositive in the majority of cases Chronic lymphocytic leukemia/small lymphocytic lymphoma
Table 2. Common B-cell lymphomas and the IHC antibodies that are typically used to aid in diagnosis and subtyping.8–10
This chart is not for diagnostic use. It represents staining patterns that are associated with each disease based on published literature and is for educational use only.
6 Hematopathology diagnostic solutions
negative in the majority of cases Diffuse large B-cell lymphoma
Hodgkin lymphomamixed expression positive Follicular lymphoma
Mantle cell lymphomamixed expression negative
Marginal zone lymphoma
CLL/SLLDLBCLFLHLMCLMZL
6 12/4/2015 9:47:25 AM
+–+/––/+
Keypositive in the majority of cases Angioimmunoblastic T-cell lymphoma
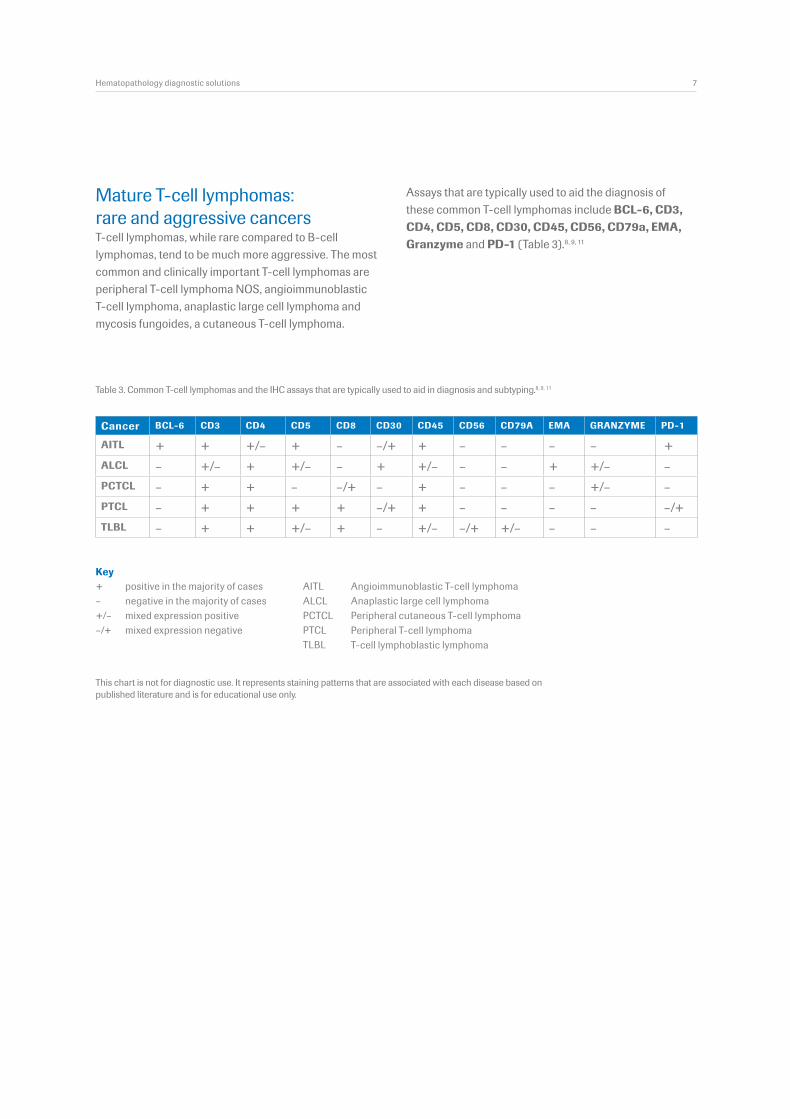
Table 3. Common T-cell lymphomas and the IHC assays that are typically used to aid in diagnosis and subtyping.8, 9, 11
Mature T-cell lymphomas: rare and aggressive cancersT-cell lymphomas, while rare compared to B-cell lymphomas, tend to be much more aggressive. The most common and clinically important T-cell lymphomas are peripheral T-cell lymphoma NOS, angioimmunoblastic T-cell lymphoma, anaplastic large cell lymphoma and mycosis fungoides, a cutaneous T-cell lymphoma.
Assays that are typically used to aid the diagnosis of these common T-cell lymphomas include BCL-6, CD3, CD4, CD5, CD8, CD30, CD45, CD56, CD79a, EMA, Granzyme and PD-1 (Table 3).8, 9, 11
Cancer BCL-6 CD3 CD4 CD5 CD8 CD30 CD45 CD56 CD79A EMA GRANZYME PD-1
AITL + + +/– + – –/+ + – – – – +ALCL – +/– + +/– – + +/– – – + +/– –PCTCL – + + – –/+ – + – – – +/– –PTCL – + + + + –/+ + – – – – –/+TLBL – + + +/– + – +/– –/+ +/– – – –
This chart is not for diagnostic use. It represents staining patterns that are associated with each disease based on published literature and is for educational use only.
Hematopathology diagnostic solutions 7
negative in the majority of cases Anaplastic large cell lymphoma
Peripheral T-cell lymphomamixed expression positive Peripheral cutaneous T-cell lymphoma
T-cell lymphoblastic lymphomamixed expression negative
AITLALCLPCTCLPTCLTLBL
7 12/4/2015 9:47:25 AM
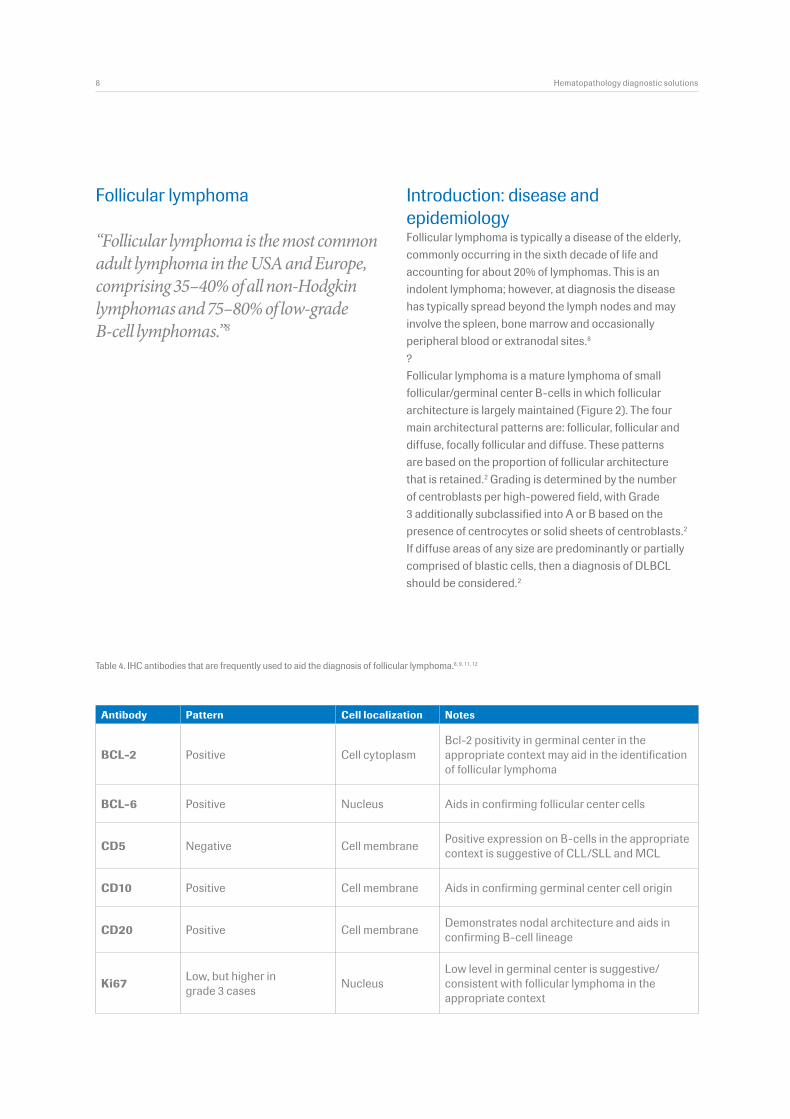
Introduction: disease and epidemiology Follicular lymphoma is typically a disease of the elderly, commonly occurring in the sixth decade of life and accounting for about 20% of lymphomas. This is an indolent lymphoma; however, at diagnosis the disease has typically spread beyond the lymph nodes and may involve the spleen, bone marrow and occasionally peripheral blood or extranodal sites.8
?Follicular lymphoma is a mature lymphoma of small follicular/germinal center B-cells in which follicular architecture is largely maintained (Figure 2). The four main architectural patterns are: follicular, follicular and diffuse, focally follicular and diffuse. These patterns are based on the proportion of follicular architecture that is retained.2 Grading is determined by the number of centroblasts per high-powered field, with Grade 3 additionally subclassified into A or B based on the presence of centrocytes or solid sheets of centroblasts.2 If diffuse areas of any size are predominantly or partially comprised of blastic cells, then a diagnosis of DLBCL should be considered.2
Follicular lymphoma
“Follicular lymphoma is the most common adult lymphoma in the USA and Europe, comprising 35–40% of all non-Hodgkin lymphomas and 75–80% of low-grade B-cell lymphomas.”8
Table 4. IHC antibodies that are frequently used to aid the diagnosis of follicular lymphoma.8, 9, 11, 12
Antibody Pattern Cell localization Notes
BCL-2 Positive Cell cytoplasm Bcl-2 positivity in germinal center in the appropriate context may aid in the identification of follicular lymphoma
BCL-6 Positive Nucleus Aids in confirming follicular center cells
CD5 Negative Cell membrane Positive expression on B-cells in the appropriate context is suggestive of CLL/SLL and MCL
CD10 Positive Cell membrane Aids in confirming germinal center cell origin
CD20 Positive Cell membrane Demonstrates nodal architecture and aids in confirming B-cell lineage
Ki67 Low, but higher in grade 3 cases Nucleus
Low level in germinal center is suggestive/consistent with follicular lymphoma in the appropriate context
8 Hematopathology diagnostic solutions
8 12/4/2015 9:47:25 AM
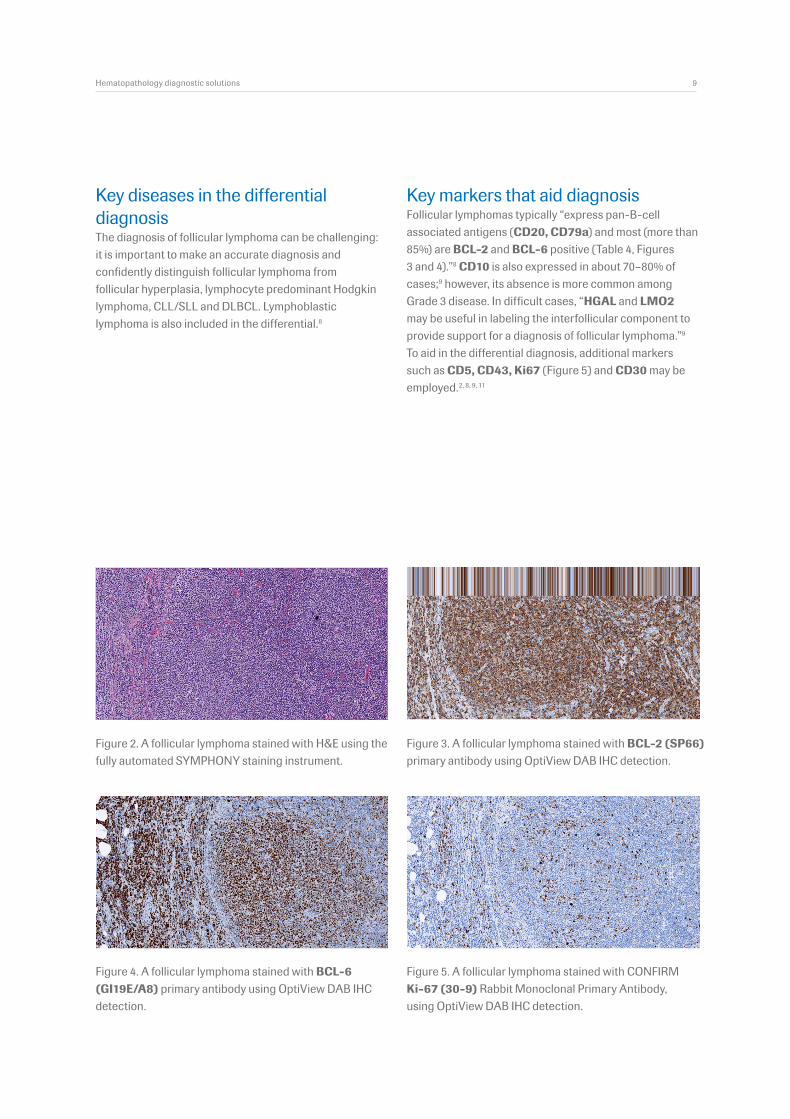
Figure 2. A follicular lymphoma stained with H&E using the fully automated SYMPHONY staining instrument.
Figure 3. A follicular lymphoma stained with BCL-2 (SP66) primary antibody using OptiView DAB IHC detection.
Figure 4. A follicular lymphoma stained with BCL-6 (GI19E/A8) primary antibody using OptiView DAB IHC detection.
Figure 5. A follicular lymphoma stained with CONFIRM Ki-67 (30-9) Rabbit Monoclonal Primary Antibody, using OptiView DAB IHC detection.
Key diseases in the differential diagnosisThe diagnosis of follicular lymphoma can be challenging: it is important to make an accurate diagnosis and confidently distinguish follicular lymphoma from follicular hyperplasia, lymphocyte predominant Hodgkin lymphoma, CLL/SLL and DLBCL. Lymphoblastic lymphoma is also included in the differential.8
Key markers that aid diagnosisFollicular lymphomas typically “express pan-B-cell associated antigens (CD20, CD79a) and most (more than 85%) are BCL-2 and BCL-6 positive (Table 4, Figures 3 and 4).”8 CD10 is also expressed in about 70–80% of cases;9 however, its absence is more common among Grade 3 disease. In difficult cases, “HGAL and LMO2 may be useful in labeling the interfollicular component to provide support for a diagnosis of follicular lymphoma.”9 To aid in the differential diagnosis, additional markers such as CD5, CD43, Ki67 (Figure 5) and CD30 may be employed.2, 8, 9, 11
Hematopathology diagnostic solutions 9
9 12/4/2015 9:47:34 AM
Diffuse large B-cell lymphoma
DLBCL can arise in follicular lymphoma, CLL/SLL, or marginal zone lymphoma. If present, the DLBCL component is the primary therapeutic target.13, 14
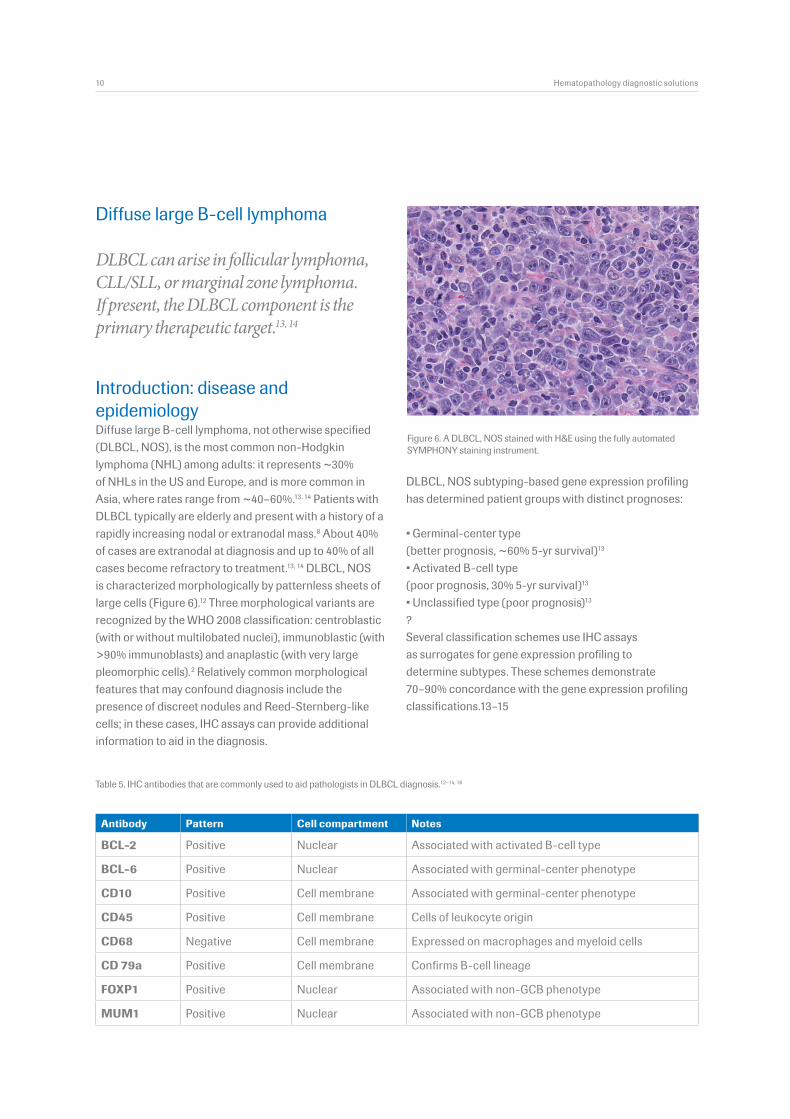
Introduction: disease and epidemiologyDiffuse large B-cell lymphoma, not otherwise specified (DLBCL, NOS), is the most common non-Hodgkin lymphoma (NHL) among adults: it represents ~30% of NHLs in the US and Europe, and is more common in Asia, where rates range from ~40–60%.13, 14 Patients with DLBCL typically are elderly and present with a history of a rapidly increasing nodal or extranodal mass.8 About 40% of cases are extranodal at diagnosis and up to 40% of all cases become refractory to treatment.13, 14 DLBCL, NOS is characterized morphologically by patternless sheets of large cells (Figure 6).12 Three morphological variants are recognized by the WHO 2008 classification: centroblastic (with or without multilobated nuclei), immunoblastic (with >90% immunoblasts) and anaplastic (with very large pleomorphic cells).2 Relatively common morphological features that may confound diagnosis include the presence of discreet nodules and Reed-Sternberg-like cells; in these cases, IHC assays can provide additional information to aid in the diagnosis.
Figure 6. A DLBCL, NOS stained with H&E using the fully automated SYMPHONY staining instrument.
Antibody Pattern Cell compartment Notes
BCL-2 Positive Nuclear Associated with activated B-cell type
BCL-6 Positive Nuclear Associated with germinal-center phenotype
CD10 Positive Cell membrane Associated with germinal-center phenotype
CD45 Positive Cell membrane Cells of leukocyte origin
CD68 Negative Cell membrane Expressed on macrophages and myeloid cells
CD 79a Positive Cell membrane Confirms B-cell lineage
FOXP1 Positive Nuclear Associated with non-GCB phenotype
MUM1 Positive Nuclear Associated with non-GCB phenotype
Table 5. IHC antibodies that are commonly used to aid pathologists in DLBCL diagnosis.12–14, 16
10 Hematopathology diagnostic solutions
DLBCL, NOS subtyping-based gene expression profiling has determined patient groups with distinct prognoses:
• Germinal-center type (better prognosis, ~60% 5-yr survival)13
• Activated B-cell type (poor prognosis, 30% 5-yr survival)13
• Unclassified type (poor prognosis)13
?Several classification schemes use IHC assays as surrogates for gene expression profiling to determine subtypes. These schemes demonstrate 70–90% concordance with the gene expression profiling classifications.13–15
10 12/4/2015 9:47:35 AM
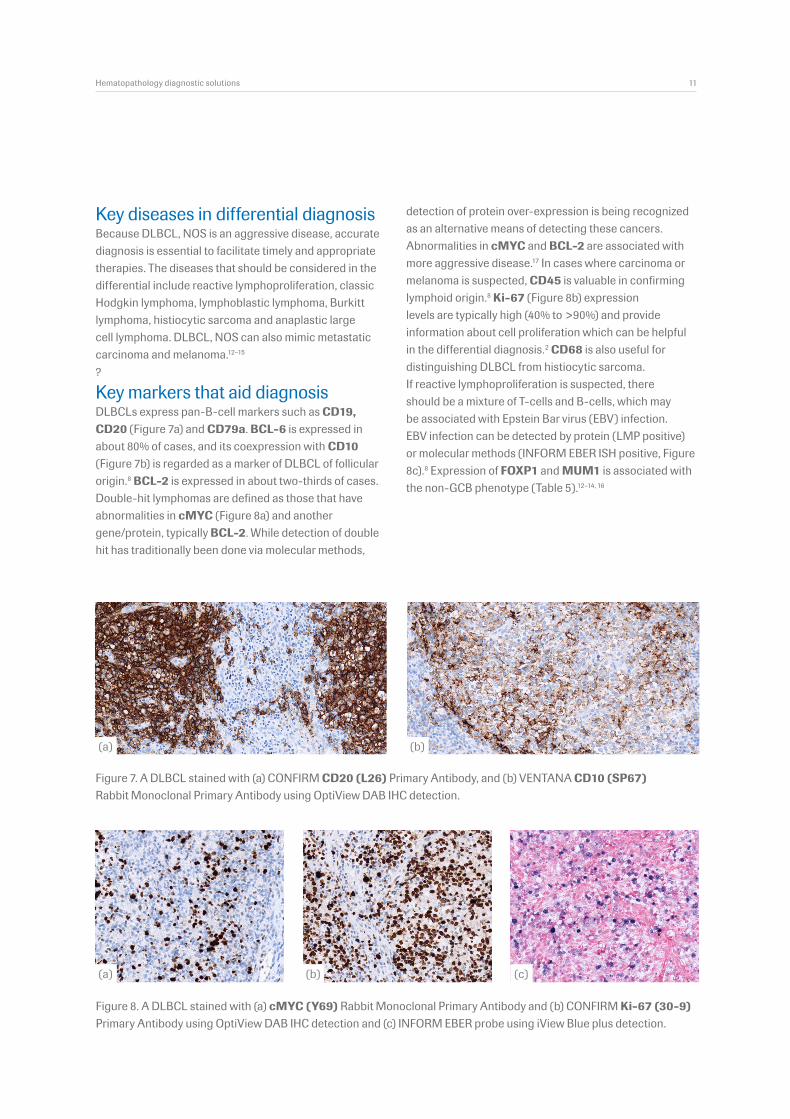
Figure 7. A DLBCL stained with (a) CONFIRM CD20 (L26) Primary Antibody, and (b) VENTANA CD10 (SP67) Rabbit Monoclonal Primary Antibody using OptiView DAB IHC detection.
Figure 8. A DLBCL stained with (a) cMYC (Y69) Rabbit Monoclonal Primary Antibody and (b) CONFIRM Ki-67 (30-9) Primary Antibody using OptiView DAB IHC detection and (c) INFORM EBER probe using iView Blue plus detection.
Key diseases in differential diagnosisBecause DLBCL, NOS is an aggressive disease, accurate diagnosis is essential to facilitate timely and appropriate therapies. The diseases that should be considered in the differential include reactive lymphoproliferation, classic Hodgkin lymphoma, lymphoblastic lymphoma, Burkitt lymphoma, histiocytic sarcoma and anaplastic large cell lymphoma. DLBCL, NOS can also mimic metastatic carcinoma and melanoma.12–15
?
Key markers that aid diagnosis DLBCLs express pan-B-cell markers such as CD19, CD20 (Figure 7a) and CD79a. BCL-6 is expressed in about 80% of cases, and its coexpression with CD10 (Figure 7b) is regarded as a marker of DLBCL of follicular origin.8 BCL-2 is expressed in about two-thirds of cases. Double-hit lymphomas are defined as those that have abnormalities in cMYC (Figure 8a) and another gene/protein, typically BCL-2. While detection of double hit has traditionally been done via molecular methods,
detection of protein over-expression is being recognized as an alternative means of detecting these cancers. Abnormalities in cMYC and BCL-2 are associated with more aggressive disease.17 In cases where carcinoma or melanoma is suspected, CD45 is valuable in confirming lymphoid origin.8 Ki-67 (Figure 8b) expression levels are typically high (40% to >90%) and provide information about cell proliferation which can be helpful in the differential diagnosis.2 CD68 is also useful for distinguishing DLBCL from histiocytic sarcoma. If reactive lymphoproliferation is suspected, there should be a mixture of T-cells and B-cells, which may be associated with Epstein Bar virus (EBV) infection. EBV infection can be detected by protein (LMP positive) or molecular methods (INFORM EBER ISH positive, Figure 8c).8 Expression of FOXP1 and MUM1 is associated with the non-GCB phenotype (Table 5).12–14, 16
(a)
(a) (b) (c)
(b)
Hematopathology diagnostic solutions 11
11 12/4/2015 9:47:37 AM
Antibody Pattern Cell compartment Notes
CD3 Negative Cell membrane T-cell marker, if negative excludes T-cell origin
CD5 Positive Cell membrane Co-expression on B-cells with CD43 is consistent with a diagnosis of CLL/SLL
CD20 Positive Cell membrane Confirms B-cell origin
CD23 Positive Cell membrane Typically positive, can be used to differentiate from mantle cell lymphoma
Ki67 Low-level expression Nuclear Proliferative marker
Table 6. IHC antibodies that are commonly used to aid in CLL/SLL diagnosis.1, 2, 8, 9, 12
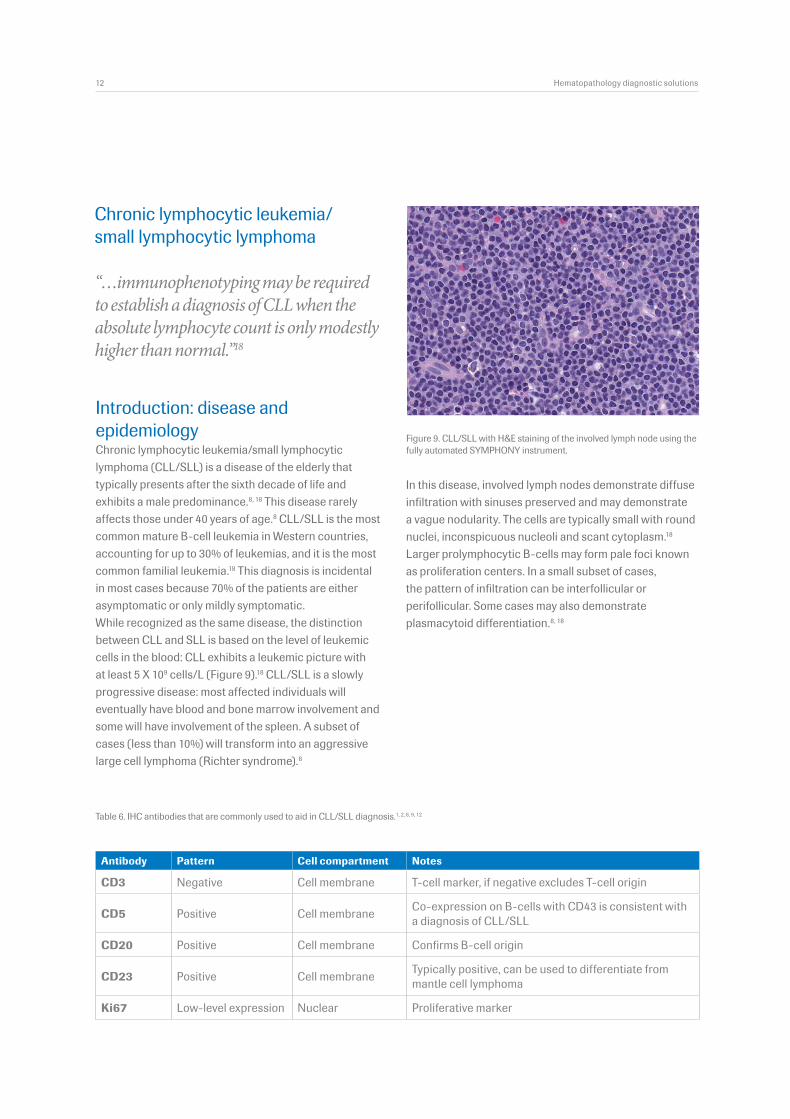
Introduction: disease and epidemiologyChronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL) is a disease of the elderly that typically presents after the sixth decade of life and exhibits a male predominance.8, 18 This disease rarely affects those under 40 years of age.8 CLL/SLL is the most common mature B-cell leukemia in Western countries, accounting for up to 30% of leukemias, and it is the most common familial leukemia.18 This diagnosis is incidental in most cases because 70% of the patients are either asymptomatic or only mildly symptomatic. While recognized as the same disease, the distinction between CLL and SLL is based on the level of leukemic cells in the blood: CLL exhibits a leukemic picture with at least 5 X 109 cells/L (Figure 9).18 CLL/SLL is a slowly progressive disease: most affected individuals will eventually have blood and bone marrow involvement and some will have involvement of the spleen. A subset of cases (less than 10%) will transform into an aggressive large cell lymphoma (Richter syndrome).8
Chronic lymphocytic leukemia/ small lymphocytic lymphoma
“…immunophenotyping may be required to establish a diagnosis of CLL when the absolute lymphocyte count is only modestly higher than normal.”18
Figure 9. CLL/SLL with H&E staining of the involved lymph node using the fully automated SYMPHONY instrument.
12 Hematopathology diagnostic solutions
In this disease, involved lymph nodes demonstrate diffuse infiltration with sinuses preserved and may demonstrate a vague nodularity. The cells are typically small with round nuclei, inconspicuous nucleoli and scant cytoplasm.18 Larger prolymphocytic B-cells may form pale foci known as proliferation centers. In a small subset of cases, the pattern of infiltration can be interfollicular or perifollicular. Some cases may also demonstrate plasmacytoid differentiation.8, 18
12 12/4/2015 9:47:38 AM

Figure 10. A CLL/SLL stained with (a) CONFIRM CD3 (2GV6) Rabbit Monoclonal Primary Antibody, and (b) CONFIRM CD5 (SP19) Rabbit Monoclonal Primary Antibody using OptiView DAB IHC detection.
Figure 11. A CLL/SLL stained with (a) CONFIRM CD23 (SP23) Rabbit Monoclonal Primary Antibody, and (b) ZAP70 (2F3.2) antibodies using OptiView DAB IHC detection.
Key diseases in differential diagnosis The differential diagnosis includes other small B-cell lymphomas such as mantle cell, marginal zone lymphoma and follicular lymphoma that share similar characteris-tic including patient presentation, symptoms, signs and morphology on H&E.8
Key markers that aid diagnosisCLL/SLL cells express B-cell markers including CD20 (Table 6) and CD79 and don’t express CD3 (Figure 10a). Most cells co-express CD43 and CD5 (this expression is often weaker than in the surrounding reactive T-cells) (Figure 10b).8 CD23 is typically positive and can be useful in differentiating between mantle cell lymphoma and marginal zone lymphoma (Figure 11a). Cyclin D1 is also useful for differentiation from mantle cell lymphoma as it is negative in CLL/SLL. CD21 may also be positive in these cancer cells but tends to be less intense compared to follicular dendritic cells. Ki-67 is low in these tumors (<5%), and kappa lambda restriction can be demonstrated. CLL with immunoglobulin gene mutations has a better prognosis than cases that are not mutated: ZAP-70 (Figure 11b) and CD38 have been used as surrogate markers to identify cases that have wild-type immunoglobulin genes.8
(a) (b)
(b)(a)
Hematopathology diagnostic solutions 13
13 12/4/2015 9:47:40 AM
Antibody Pattern Cell compartment Notes
CD3/CD7 Negative Membrane Positive on T-cells, not on neoplastic cells
CD5 Positive Membrane Most positive, a minority subset can be negative
CD20 Positive Membrane Pan-B-cell marker
Cyclin D1 Positive Nuclear Expression of this protein is part of the WHO 2008 definition of mantle cell lymphoma
Ki67 Proliferation index Nuclear Assesses growth/proliferation
Table 7. IHC antibodies that are commonly used to aid the diagnosis of mantle cell lymphoma.2;8;10
Mantle cell lymphoma
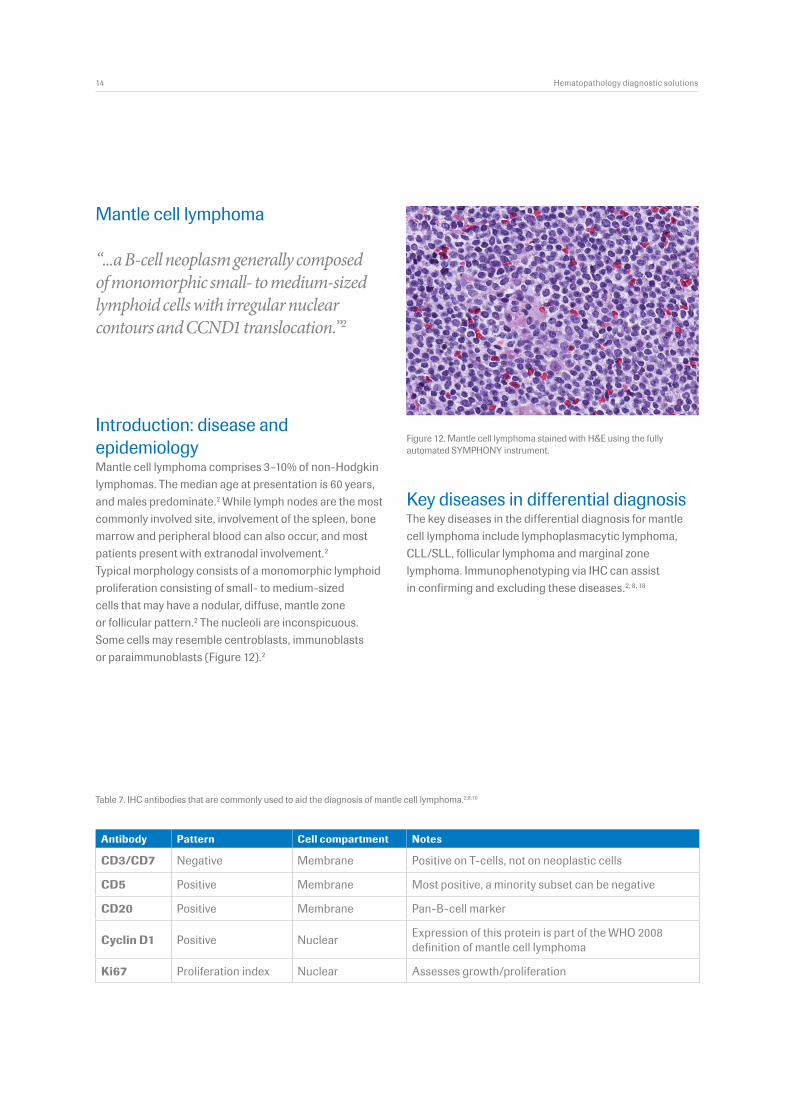
“...a B-cell neoplasm generally composed of monomorphic small- to medium-sized lymphoid cells with irregular nuclear contours and CCND1 translocation.”2
Introduction: disease and epidemiologyMantle cell lymphoma comprises 3–10% of non-Hodgkin lymphomas. The median age at presentation is 60 years, and males predominate.2 While lymph nodes are the most commonly involved site, involvement of the spleen, bone marrow and peripheral blood can also occur, and most patients present with extranodal involvement.2 Typical morphology consists of a monomorphic lymphoid proliferation consisting of small- to medium-sized cells that may have a nodular, diffuse, mantle zone or follicular pattern.2 The nucleoli are inconspicuous. Some cells may resemble centroblasts, immunoblasts or paraimmunoblasts (Figure 12).2
Figure 12. Mantle cell lymphoma stained with H&E using the fully automated SYMPHONY instrument.
14 Hematopathology diagnostic solutions
Key diseases in differential diagnosisThe key diseases in the differential diagnosis for mantle cell lymphoma include lymphoplasmacytic lymphoma, CLL/SLL, follicular lymphoma and marginal zone lymphoma. Immunophenotyping via IHC can assist in confirming and excluding these diseases.2, 8, 18
14 12/4/2015 9:47:41 AM
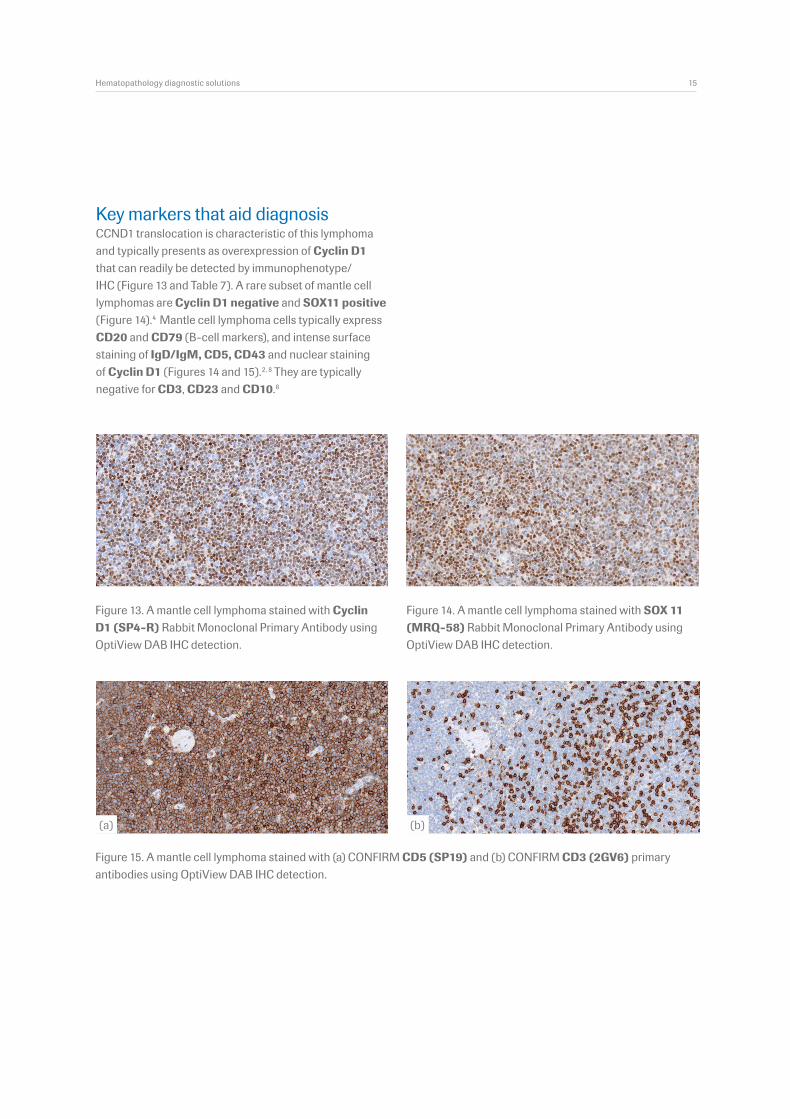
Figure 13. A mantle cell lymphoma stained with Cyclin D1 (SP4-R) Rabbit Monoclonal Primary Antibody using OptiView DAB IHC detection.
Figure 14. A mantle cell lymphoma stained with SOX 11 (MRQ-58) Rabbit Monoclonal Primary Antibody using OptiView DAB IHC detection.
Figure 15. A mantle cell lymphoma stained with (a) CONFIRM CD5 (SP19) and (b) CONFIRM CD3 (2GV6) primary antibodies using OptiView DAB IHC detection.
Key markers that aid diagnosisCCND1 translocation is characteristic of this lymphoma and typically presents as overexpression of Cyclin D1 that can readily be detected by immunophenotype/IHC (Figure 13 and Table 7). A rare subset of mantle cell lymphomas are Cyclin D1 negative and SOX11 positive (Figure 14).4 Mantle cell lymphoma cells typically express CD20 and CD79 (B-cell markers), and intense surface staining of IgD/IgM, CD5, CD43 and nuclear staining of Cyclin D1 (Figures 14 and 15).2, 8 They are typically negative for CD3, CD23 and CD10.8
(a) (b)
Hematopathology diagnostic solutions 15
15 12/4/2015 9:47:50 AM
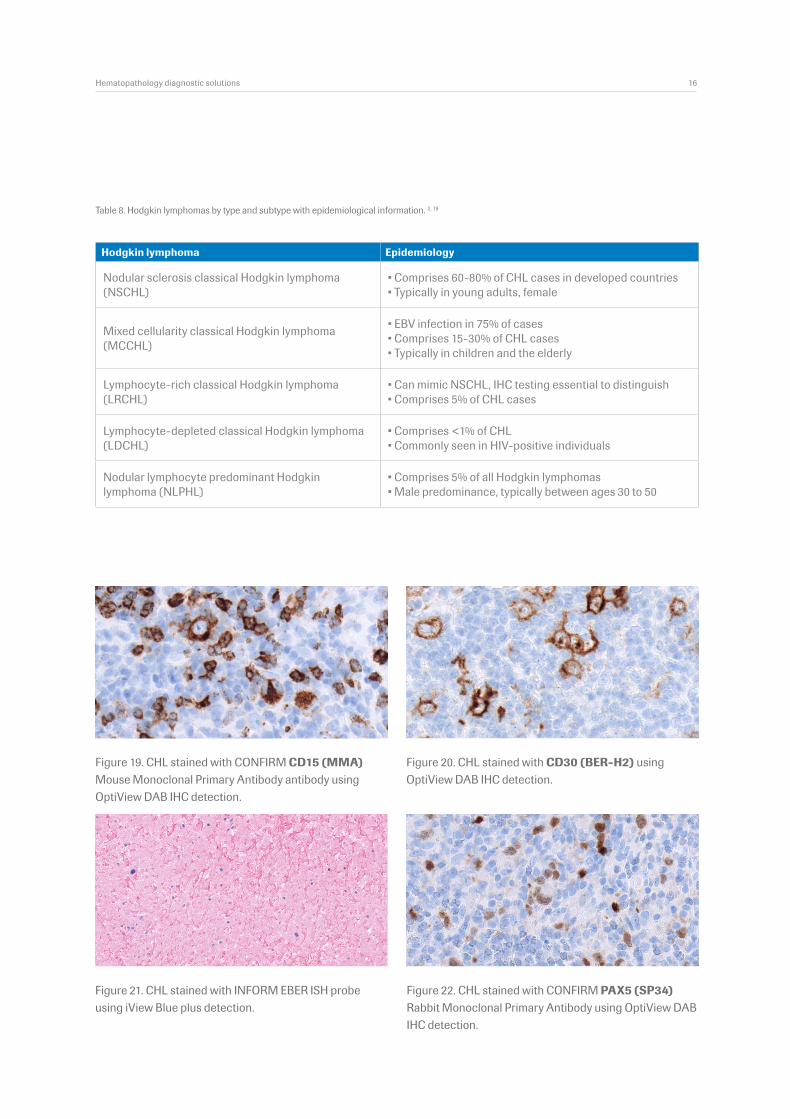
Table 8. Hodgkin lymphomas by type and subtype with epidemiological information. 2, 19
Nodular sclerosis classical Hodgkin lymphoma (NSCHL)
• Comprises 60-80% of CHL cases in developed countries• Typically in young adults, female
Mixed cellularity classical Hodgkin lymphoma (MCCHL)
• EBV infection in 75% of cases• Comprises 15-30% of CHL cases• Typically in children and the elderly
Lymphocyte-rich classical Hodgkin lymphoma (LRCHL)
• Can mimic NSCHL, IHC testing essential to distinguish• Comprises 5% of CHL cases
Lymphocyte-depleted classical Hodgkin lymphoma (LDCHL)
• Comprises <1% of CHL• Commonly seen in HIV-positive individuals
Nodular lymphocyte predominant Hodgkin lymphoma (NLPHL)
• Comprises 5% of all Hodgkin lymphomas• Male predominance, typically between ages 30 to 50
Figure 19. CHL stained with CONFIRM CD15 (MMA) Mouse Monoclonal Primary Antibody antibody using OptiView DAB IHC detection.
Figure 20. CHL stained with CD30 (BER-H2) using OptiView DAB IHC detection.
Figure 22. CHL stained with CONFIRM PAX5 (SP34) Rabbit Monoclonal Primary Antibody using OptiView DAB IHC detection.
Figure 21. CHL stained with INFORM EBER ISH probe using iView Blue plus detection.
Hematopathology diagnostic solutions 16
Hodgkin lymphoma Epidemiology
16 12/4/2015 9:47:52 AM
Hodgkin lymphoma
HIV infection increases the risk of developing CHL by 6- to 20-fold, and is almost always associated with Epstein-Barr virus (EBV) infection.18
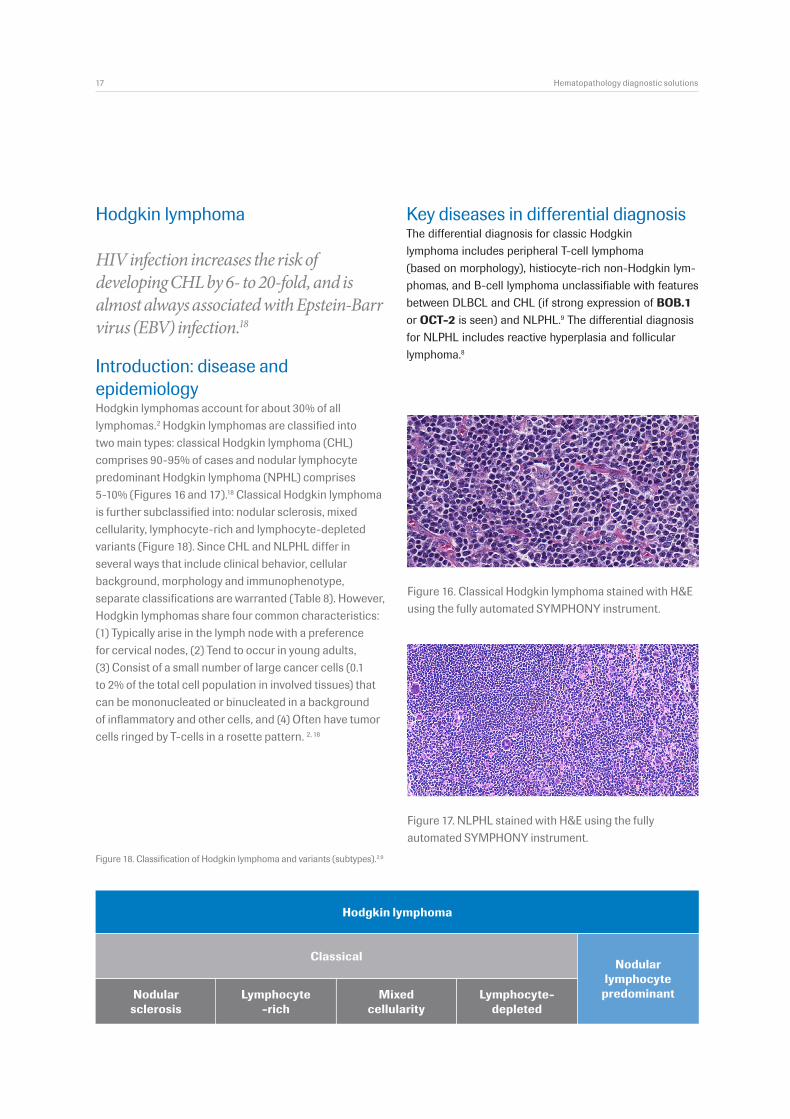
Introduction: disease and epidemiologyHodgkin lymphomas account for about 30% of all lymphomas.2 Hodgkin lymphomas are classified into two main types: classical Hodgkin lymphoma (CHL) comprises 90-95% of cases and nodular lymphocyte predominant Hodgkin lymphoma (NPHL) comprises 5-10% (Figures 16 and 17).18 Classical Hodgkin lymphoma is further subclassified into: nodular sclerosis, mixed cellularity, lymphocyte-rich and lymphocyte-depleted variants (Figure 18). Since CHL and NLPHL differ in several ways that include clinical behavior, cellular background, morphology and immunophenotype, separate classifications are warranted (Table 8). However, Hodgkin lymphomas share four common characteristics: (1) Typically arise in the lymph node with a preference for cervical nodes, (2) Tend to occur in young adults, (3) Consist of a small number of large cancer cells (0.1 to 2% of the total cell population in involved tissues) that can be mononucleated or binucleated in a background of inflammatory and other cells, and (4) Often have tumor cells ringed by T-cells in a rosette pattern. 2, 18
Figure 17. NLPHL stained with H&E using the fully automated SYMPHONY instrument.
Figure 16. Classical Hodgkin lymphoma stained with H&E using the fully automated SYMPHONY instrument.
Figure 18. Classification of Hodgkin lymphoma and variants (subtypes).2;9
Nodular sclerosis
Classical
Hodgkin lymphoma
Nodular lymphocyte predominantLymphocyte-
depletedMixed
cellularityLymphocyte
-rich
Key diseases in differential diagnosisThe differential diagnosis for classic Hodgkin lymphoma includes peripheral T-cell lymphoma (based on morphology), histiocyte-rich non-Hodgkin lym-phomas, and B-cell lymphoma unclassifiable with features between DLBCL and CHL (if strong expression of BOB.1 or OCT-2 is seen) and NLPHL.9 The differential diagnosis for NLPHL includes reactive hyperplasia and follicular lymphoma.8
17 Hematopathology diagnostic solutions
17 12/4/2015 9:47:54 AM
VENTANA hematopathology solutions: comprehensive, robust, innovativeIn hematopathology diagnosis, H&E is essential, but it is insufficient in most cases. Information from additional testing is often employed to confirm or exclude a diagnosis. IHC and ISH play an essential role in informing diagnosis.?Ventana is a full-service hematopathology provider: we offer fully automated solutions for H&E, and a comprehensive menu of robust assays supported by innovative detection, automation and workflow solutions. To learn more please visit us at ventana.com/hematopathology or contact your local representative.
References
1. Taylor CR. IHC and the WHO classification of lymphomas: cost effective immunohistochemistry using a deductive reasoning “decision tree” approach. Appl Immunohistochem Mol Morphol 2009;17:366-374.
2. Swerdlow SH, Campo E, Harris NL, et al. WHO Classification of Tumours of Haematopoietic and Lymphoid Tissues. 1 ed. Lyon: IARC Press, 2008.
3. Campo E, Swerdlow SH, Harris NL, Pileri S, Stein H, Jaffe ES. The 2008 WHO classification of lymphoid neoplasms and beyond: evolving concepts and practical applications. Blood 2011;117:5019-5032.
4. NCCN Guidelines Version 2.2013 Non-Hodgkin’s lymphomas. 2013. http://www.nccn.org/professionals/physician_gls/f_guidelines.asp
5. NCCN Guidelines Version 2.2013 Hodgkin lymphoma. 2013. http://www.nccn.org/professionals/physician_gls/f_guidelines.asp
6. Taylor CR. The WHO classification of lymphomas: cost-effective immunohistochemistry using a deductive reasoning “decision tree” approach: part II: the decision tree approach: diffuse patterns of proliferation in lymph nodes. Appl Immunohistochem Mol Morphol 2009;17:470-482.
7. Dotan E, Aggarwal C, Smith MR. Impact of Rituximab (Rituxan) on the Treatment of B-Cell Non-Hodgkin’s Lymphoma. P T 2010;35:148-157.
8. Gatter K, Delsol G, Warnke R, et al. The Diagnosis of Lymphoprolifera-tive Diseases.Wiley-Blackwell, 2011.
9. Jaffe ES, Harris NL, Vardiman JW, Campo E, Arber DA. Haematopathol-ogy. 1. 2011. Philadelphia, Saunders Elsevier.
10. Rimsza L, Grogan T. B-cell lymphomas related to B-cell development.
Hematopathology diagnostic solutions 18
2012. Tucson, AZ, Ventana Medical Systems, Inc.
11. Rimsza L, Grogan T, Marafioti T. T-cell lymphocyte development related to T-cell and natural killer-cell neoplasia. 2012. Ventana Medical Systems, Inc.
12. Lu J, Chang KL. Practical immunohistochemistry in haematopatholo-gy : a review of useful antibodies for diagnosis. Adv Anat Pathol 2011;18:133-151.
13. Choi WW, Weisenburger DD, Greiner TC et al. A new immunostain algorithm classifies diffuse large B-cell lymphoma into molecular subtypes with high accuracy. Clin Cancer Res 2009;15:5494-5502.
14. Xia Z, Xu Z, Zhao S et al. The prognostic value of immunohistochemi-cal subtyping in Chinese patients with de novo diffuse large B-cell lymphoma undergoing CHOP or R-CHOP treatment. Ann Hematol 2013;89:171-177.
15. Said JW. Aggressive B-cell lymphomas: how many categories do we need? Mod Pathol 2013;26 Suppl 1:S42-S56.
16. Barrans L, Fenton JAL, Ventura R, Smith A, Banhamn AH, Jack AS. Deregulated over expression of FOXP1 protein in diffuse large B-cell lymphoma does not occur as a result of gene rearrangement . Haemato-logica 2007;92:863-864.
17. Li S, Lin P, Young KH, Kanagal-Shamanna R, Yin CC, Medeiros LJ. MYC/BCL2 double-hit high-grade B-cell lymphoma. Adv Anat Pathol 2013 Sep;20(5):315-26. doi: 10.1097/PAP.0b013e3182a289f2
18. Jaffe ES, Harris NL, Stein H, Isaacson PG. Classification of lymphoid neoplasms: the microscope as a tool for disease discovery. Blood 2008;112:4384-4399.
19. Harris NL. Shades of gray between large B-cell lymphomas and Hodgkin lymphomas: differential diagnosis and biological implications. Mod Pathol 2013;26 Suppl 1:S57-S70.
18 12/4/2015 9:47:54 AM
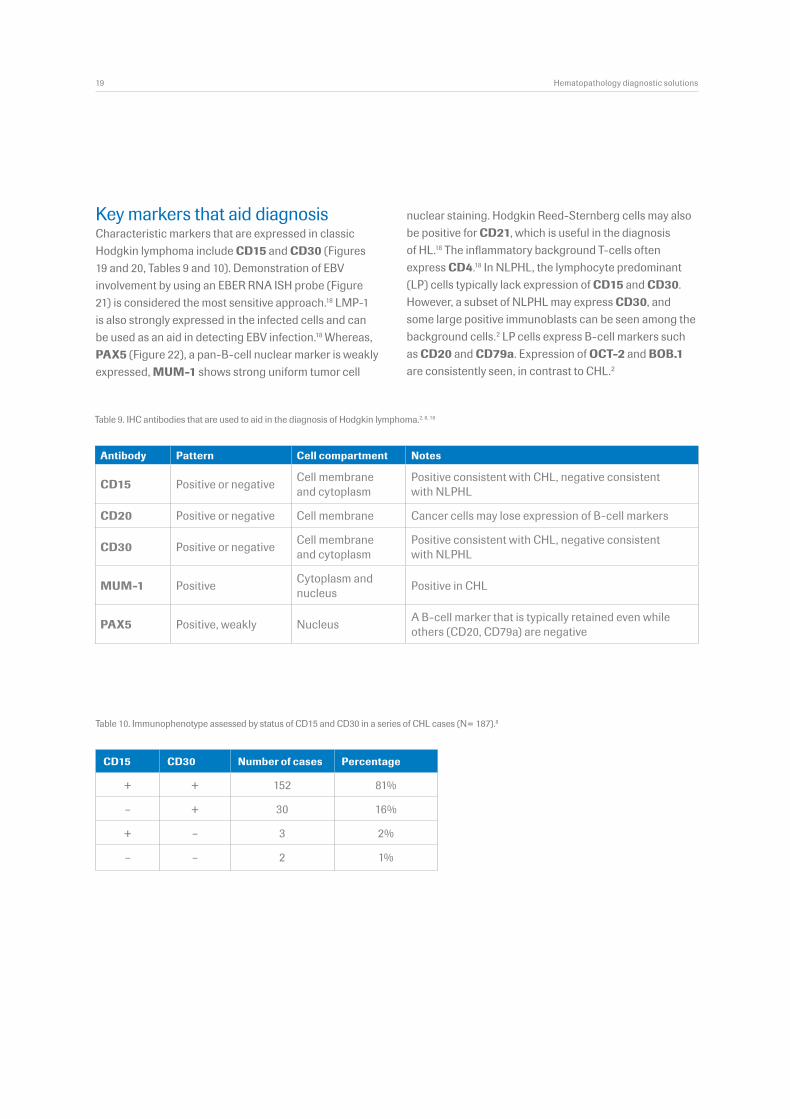
Table 10. Immunophenotype assessed by status of CD15 and CD30 in a series of CHL cases (N= 187).8
Antibody Pattern Cell compartment Notes
CD15 Positive or negative Cell membrane and cytoplasm
Positive consistent with CHL, negative consistent with NLPHL
CD20 Positive or negative Cell membrane Cancer cells may lose expression of B-cell markers
CD30 Positive or negative Cell membrane and cytoplasm
Positive consistent with CHL, negative consistent with NLPHL
MUM-1 Positive Cytoplasm and nucleus Positive in CHL
PAX5 Positive, weakly Nucleus A B-cell marker that is typically retained even while others (CD20, CD79a) are negative
Table 9. IHC antibodies that are used to aid in the diagnosis of Hodgkin lymphoma.2, 8, 18
Key markers that aid diagnosisCharacteristic markers that are expressed in classic Hodgkin lymphoma include CD15 and CD30 (Figures 19 and 20, Tables 9 and 10). Demonstration of EBV involvement by using an EBER RNA ISH probe (Figure 21) is considered the most sensitive approach.18 LMP-1 is also strongly expressed in the infected cells and can be used as an aid in detecting EBV infection.18 Whereas, PAX5 (Figure 22), a pan-B-cell nuclear marker is weakly expressed, MUM-1 shows strong uniform tumor cell
CD15 CD30 Number of cases Percentage
+ + 152 81%
– + 30 16%
+ – 3 2%
– – 2 1%
19 Hematopathology diagnostic solutions
nuclear staining. Hodgkin Reed-Sternberg cells may also be positive for CD21, which is useful in the diagnosis of HL.18 The inflammatory background T-cells often express CD4.18 In NLPHL, the lymphocyte predominant (LP) cells typically lack expression of CD15 and CD30. However, a subset of NLPHL may express CD30, and some large positive immunoblasts can be seen among the background cells.2 LP cells express B-cell markers such as CD20 and CD79a. Expression of OCT-2 and BOB.1 are consistently seen, in contrast to CHL.2
19 12/4/2015 9:47:55 AM
Company Name 1 Company Name 2 Address Line 1 Address Line 2 Address Line 3 Address Line 4 Address Line 5 Telephone Number 1 Telephone Number 2 Additional Tracking ID
www.roche.com www.ventana.com
© 2014 Ventana Medical Systems, Inc. All trademarks mentioned enjoy legal protection.VENTANA and the VENTANA logo are trademarks of Roche. All other trademarks are the property of their respective owners. E4340-1 0814A
VENTANA
Empowering | Innovation
Roche Diagnostics (Schweiz) AG Industriestrasse 7 CH-6343 Rotkreuz Schweiz Tel: +41 (0)41 799 61 00 Fax: +41 (0)41 799 65 45
www.roche.com www.ventana.com
© 2014 Ventana Medical Systems, Inc. All trademarks mentioned enjoy legal protection.
20 12/4/2015 9:47:55 AM