véronique leblond hôpital pitie …©ronique leblond hôpital pitie-salpetriere paris france how...
TRANSCRIPT
I FCR th t d d thI FCR th t d d thIs FCR the standard therapy for older cancer patients withIs FCR the standard therapy
for older cancer patients withfor older cancer patients with chronic lymphocytic
for older cancer patients with chronic lymphocytic
leukemia?leukemia?Véronique LEBLOND
Hôpital PITIE-SALPETRIEREPARISPARIS
FRANCE
How to treat chronic lymphocytic leukaemia ?y p y
FCR Fludarabine: 25mg m2 IV D1-3Fludarabine: 25mg m2 IV D1 3Cyclophosphamide 250mg/m2 IV D1-D3Rituximab: Cycle 1: 375 mg/m2, d 0Cycles 2 6: 500 mg/m2 d 1Cycles 2-6: 500 mg/m2, d 1
•FCR induces the highest remission rates ever reported
FCR h th t l f CLL• FCR may change the natural course of CLL
• FCR should be the treatment of first choice in• FCR should be the treatment of first choice in patients considered fit enough
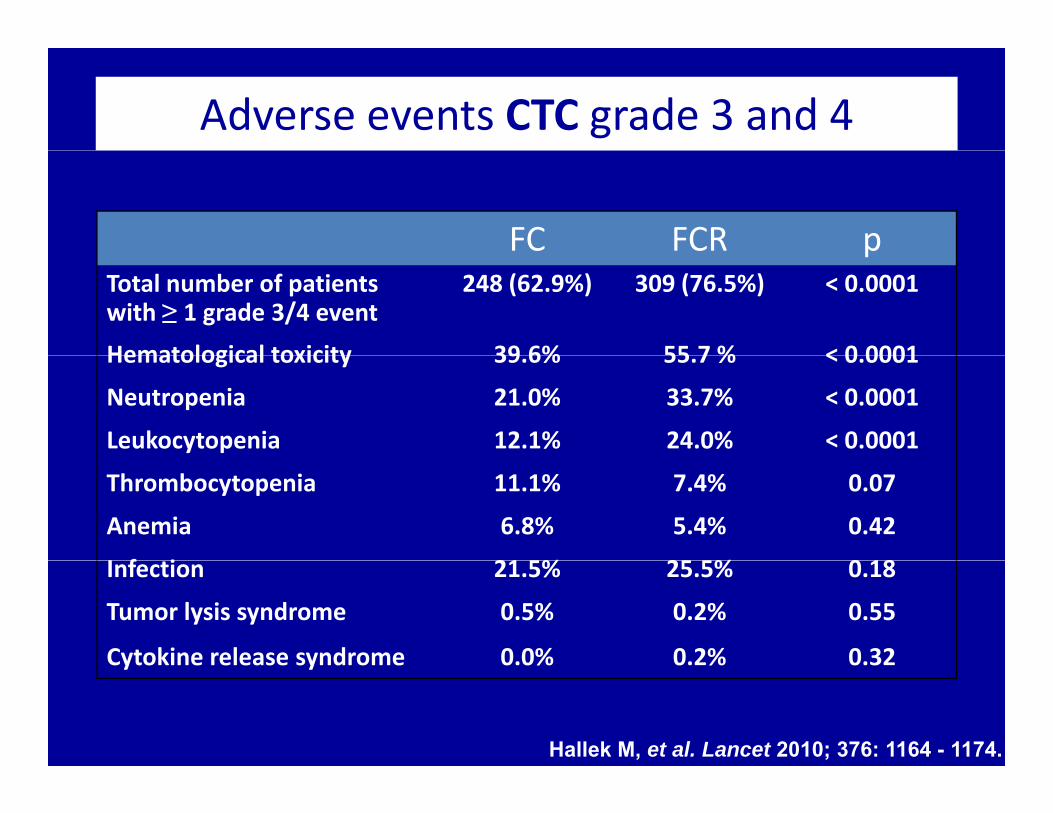
Adverse events CTC grade 3 and 4
FC FCR ppTotal number of patients with ≥ 1 grade 3/4 event
248 (62.9%) 309 (76.5%) < 0.0001
Hematological toxicity 39 6% 55 7 % < 0 0001Hematological toxicity 39.6% 55.7 % < 0.0001
Neutropenia 21.0% 33.7% < 0.0001
Leukocytopenia 12.1% 24.0% < 0.0001
Thrombocytopenia 11.1% 7.4% 0.07
Anemia 6.8% 5.4% 0.42
I f i 21 5% 25 5% 0 18Infection 21.5% 25.5% 0.18
Tumor lysis syndrome 0.5% 0.2% 0.55
Cytokine release syndrome 0.0% 0.2% 0.32Cytokine release syndrome 0.0% 0.2% 0.32
Hallek M, et al. Lancet 2010; 376: 1164 - 1174.
How to treat chronic lymphocytic leukaemia ?
• Only 11% of the patients were over 70 yearsy p y
• All others may receive Chlorambucil
So, do we need something else ?

Median age of patients in pivotal phase III CLL trialsphase III CLL trialsMedian age of diagnosis = 72
yrs)
F
CamFC
F
Age (
1. Goede V and Hallek M. Drugs Aging. 2011;28(3):163‐76
2. Hallek M, et al. Lancet. 2010;376: 1164–74
3. Robak T, et al. J Clin Oncol. 2010;28(10):1756‐65
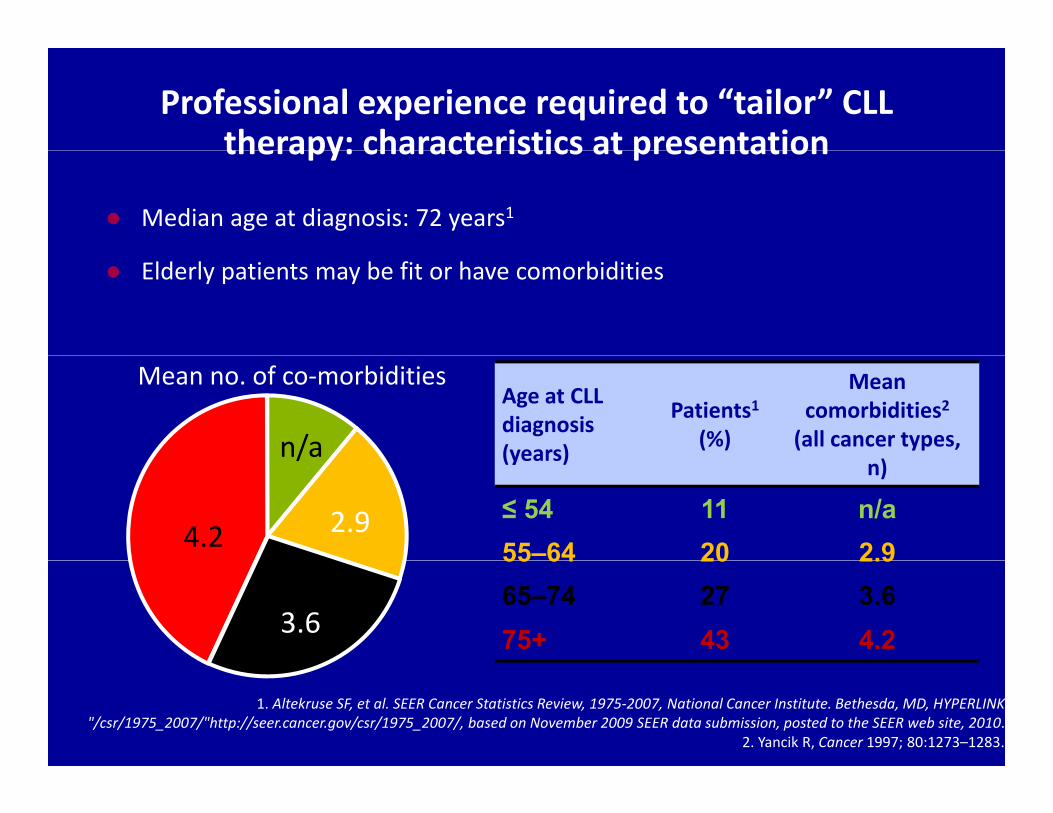
Professional experience required to “tailor” CLL therapy: characteristics at presentationtherapy: characteristics at presentation
● Median age at diagnosis: 72 years1
● Elderly patients may be fit or have comorbidities
Age at CLL diagnosis (years)
Patients1(%)
Mean comorbidities2(all cancer types,
Mean no. of co‐morbidities
n/a (years) n)
≤ 54 11 n/a55–64 20 2.9
2.94.2
/
55 64 20 2.965–74 27 3.675+ 43 4.23.6
1. Altekruse SF, et al. SEER Cancer Statistics Review, 1975‐2007, National Cancer Institute. Bethesda, MD, HYPERLINK "/csr/1975_2007/"http://seer.cancer.gov/csr/1975_2007/, based on November 2009 SEER data submission, posted to the SEER web site, 2010.
2. Yancik R, Cancer 1997; 80:1273–1283.
Who may not be eligible for fludarabine based therapy?fludarabine based therapy?
• Impaired renal function: debate exists: CrCl• Impaired renal function: debate exists: CrCl 30–70 ml/min mandates reduced dose
• Physically unfit (co morbidities, geriatric assessment)
• Risk for infection

Other chemoimmunotherapy combinations may allow therapy to be adapted tomay allow therapy to be adapted to
individual patients’ needs
‘Go-go’• Completely independent• No co-morbidity
‘No-go’• Severely handicapped• High co-morbidity
‘Slow-go’ • Some co-morbidity• Impaired organ functionNo co morbidity
• Normal life expectancy Aggressive
chemotherapy
High co morbidity• Reduced life expectancy Palliative care
Impaired organ function• Reduced performance
status Less aggressive
approachpp
Where to draw
What is thestandard of care?
Rituximab-FC is the standard of care to draw
the line?
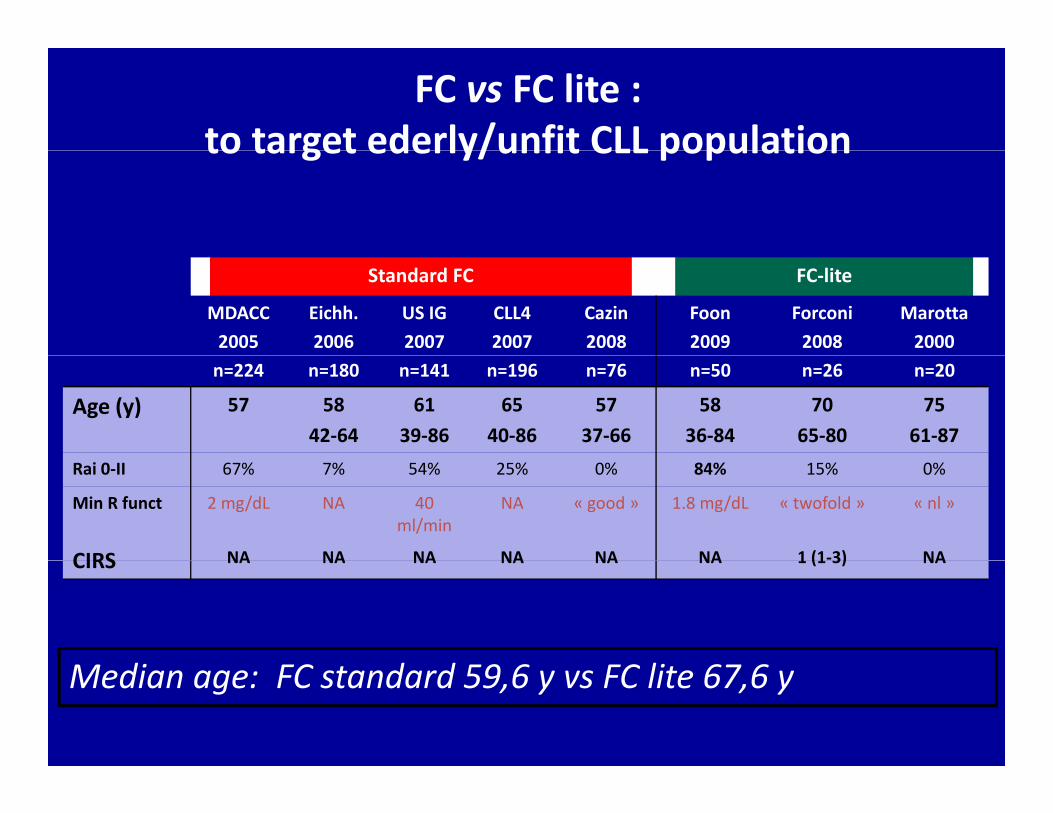
FC vs FC lite :to target ederly/unfit CLL populationto target ederly/unfit CLL population
Standard FC FC‐lite
MDACC2005
Eichh.2006
US IG2007
CLL42007
Cazin2008
Foon2009
Forconi2008
Marotta2000
n=224 n=180 n=141 n=196 n=76 n=50 n=26 n=20
Age (y) 57 5842‐64
6139‐86
6540‐86
5737‐66
5836‐84
7065‐80
7561‐87
Rai 0‐II 67% 7% 54% 25% 0% 84% 15% 0%
Min R funct 2 mg/dL NA 40 ml/min
NA « good » 1.8 mg/dL « twofold » « nl »
CIRS NA NA NA NA NA NA 1 (1‐3) NACIRS NA NA NA NA NA NA 1 (1 3) NA
d d d lMedian age: FC standard 59,6 y vs FC lite 67,6 y

CLL trials in the elderly and/or unfitCLL trials in the elderly and/or unfitStudy Treatment No. of patients CR (%) ORR (%) PFS (months) Comments
Chl b il 100 0 51 18Eichhorst et al, 2009
GCLLSG CLL5
Chlorambucil
Fludarabine
100
93
0
7
51
72
18
19
65 – 80 years of ageNo sig diff in PFS or OSMedian age 70‐71 yearsKnauf et al, 2009
Multicentre phase III
Chlorambucil
Bendamustine
157
162
2
31
31
68
8.3
21.6
Median age 64 years
No sig diff in ORR in <65 and >65 year olds
(BEN 71 6% 63 5% 0 3 CLB 28 4% 32 5%162 31 68 21.6 (BEN 71.6% vs 63.5%, p>0.3; CLB 28.4% vs 32.5%, p>0.06)
PFS not influenced by age >65 yearsHillmen et al, 2010
CLL208Chlorambucil + Rituximab
100 9 82 23.5
Hillmen et al, 2010
Median age 70 years (range 43–86)
F l 2010
Ph IICLB‐R +/‐ R
maintenance*54 20.4 81.4 NR
Foa et al, 2010
Median age 70.5 years (range 61–84)
NR = not reported * Interim analysis measuring tumour response at end of induction phase on ITT
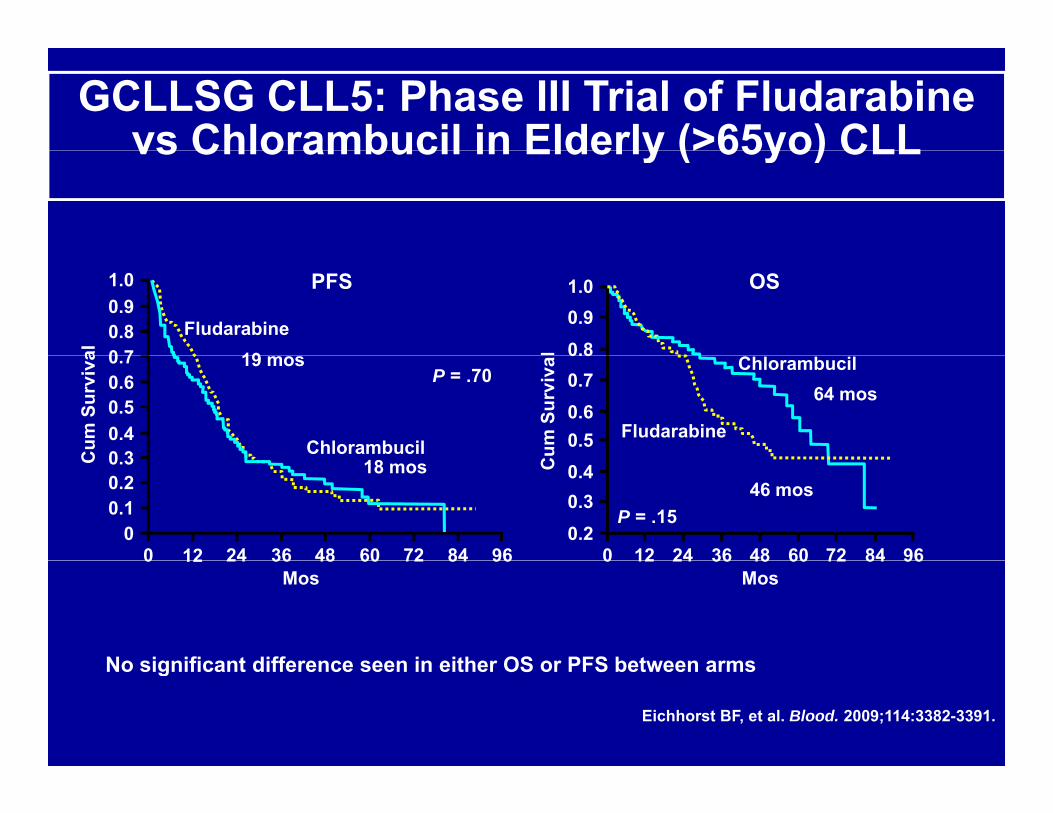
GCLLSG CLL5: Phase III Trial of Fludarabine vs Chlorambucil in Elderly (>65yo) CLLvs Chlorambucil in Elderly (>65yo) CLL
OS0.91.0
0.8l
PFS
19
0.91.0
0 70.8
al
Fludarabine
64 mos
0.50.60.70.8
Cum
Sur
viva
Fludarabine
ChlorambucilP = .7019 mos
0.40 3
0.5
0.7
Cum
Sur
viva
Chlorambucil
0.6
P = .1546 mos0.3
0.20 12 964836
0.4
24 60 72 84C
12
18 mos0.2
00 964836
0.3
24 60 72 84
C
0.1
No significant difference seen in either OS or PFS between arms
Mos 0 12 96483624 60 72 8412
Mos 0 96483624 60 72 84
No significant difference seen in either OS or PFS between arms
Eichhorst BF, et al. Blood. 2009;114:3382-3391.
Is chlorambucil an effective therapy s c o a buc a e ect e t e apyfor elderly/unfit patients with CLL?
• Outcome varies by dose and duration of treatment– Higher doses and longer duration of therapy lead to:
• Overall response rates >70% and CR rates 5‐10%• Median PFS ~18 months in front‐line CLLM di ll i l >5• Median overall survival >5 years
• Can we improve on chlorambucil?– alternative chemotherapy ?alternative chemotherapy ?– addition of monoclonal antibodies ?
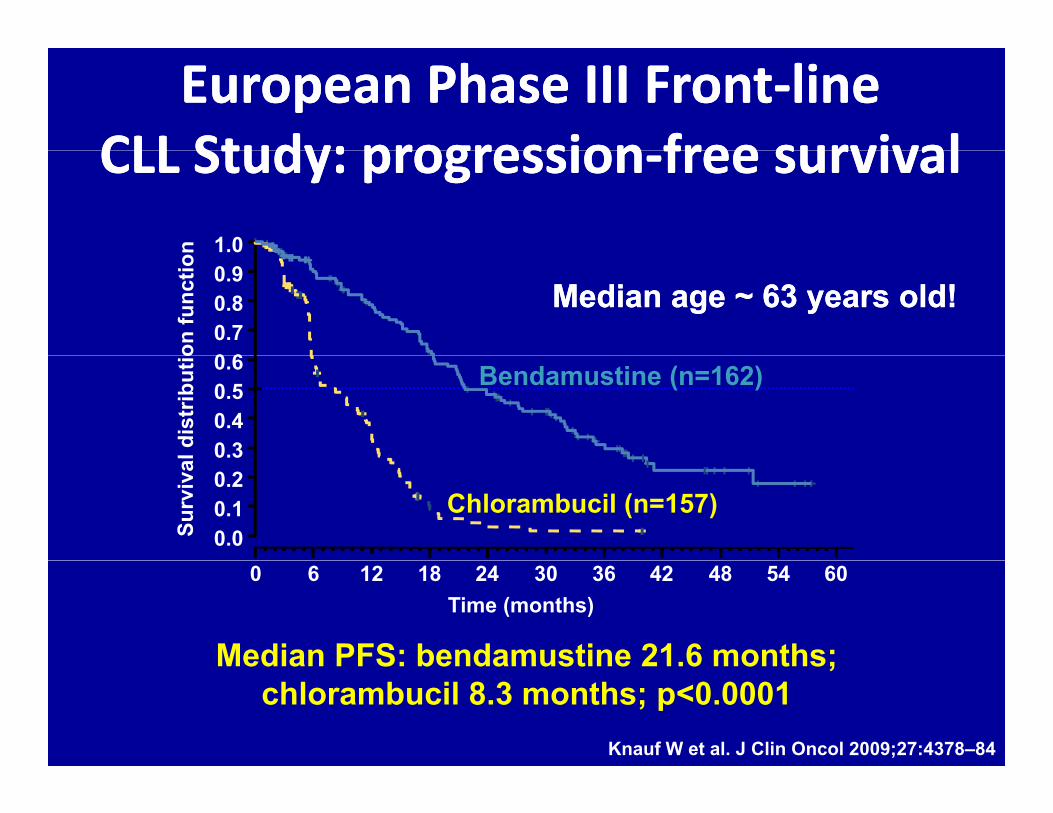
European Phase III FrontEuropean Phase III Front‐‐linelineCLL Study: progressionCLL Study: progression free survivalfree survivalCLL Study: progressionCLL Study: progression‐‐free survivalfree survival
1.0
0 60.70.80.9
Median age ~ 63 years old!Median age ~ 63 years old!
Bendamustine (n=162)
0.30.40.50.6
Chlorambucil (n=157)0.00.10.2
Median PFS: bendamustine 21.6 months;
0 6 12 18 24 30 36 42 48 54 60Time (months)
Median PFS: bendamustine 21.6 months; chlorambucil 8.3 months; p<0.0001
Knauf W et al. J Clin Oncol 2009;27:4378–84
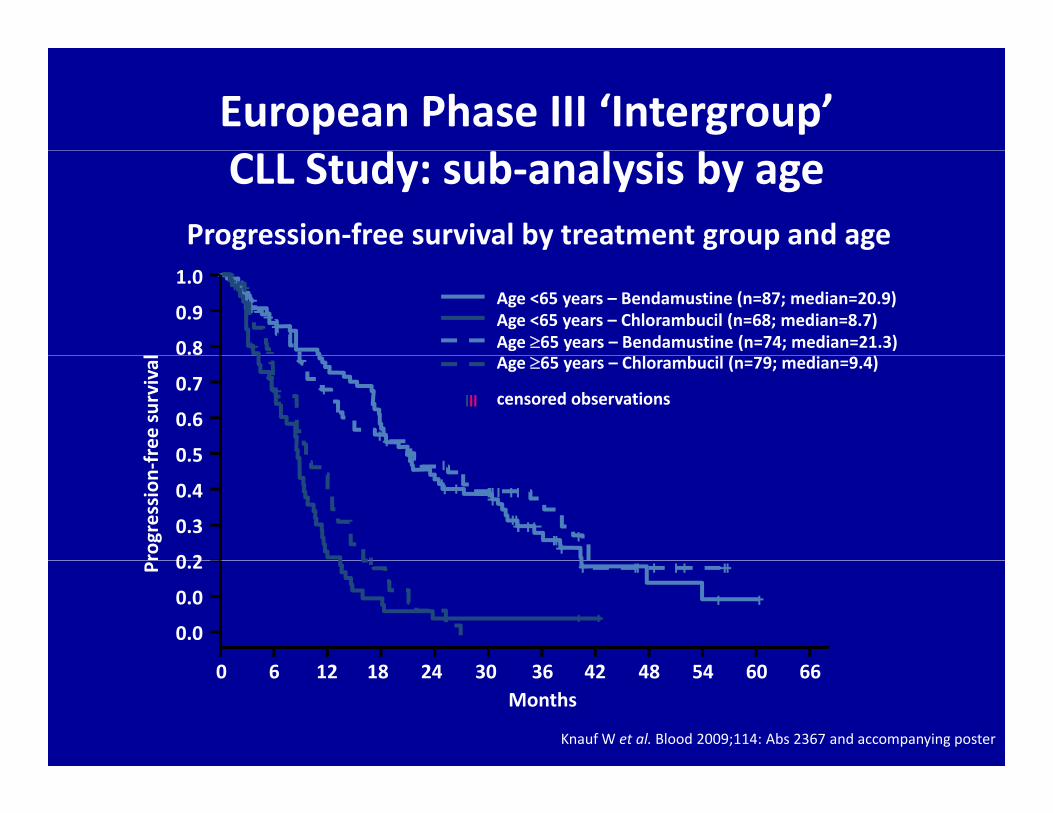
European Phase III ‘Intergroup’ CLL Study: sub‐analysis by age
Progression‐free survival by treatment group and age
0.8
0.9
1.0Age <65 years – Bendamustine (n=87; median=20.9)Age <65 years – Chlorambucil (n=68; median=8.7)Age 65 years – Bendamustine (n=74; median=21.3)
0 5
0.6
0.7
free
survival Age 65 years – Chlorambucil (n=79; median=9.4)
censored observations
0 2
0.3
0.4
0.5
rogression
‐f
0.0
0.0
0.2P
0 6 12 18 24 30 36 42 48 54 60 66Months
Knauf W et al. Blood 2009;114: Abs 2367 and accompanying poster
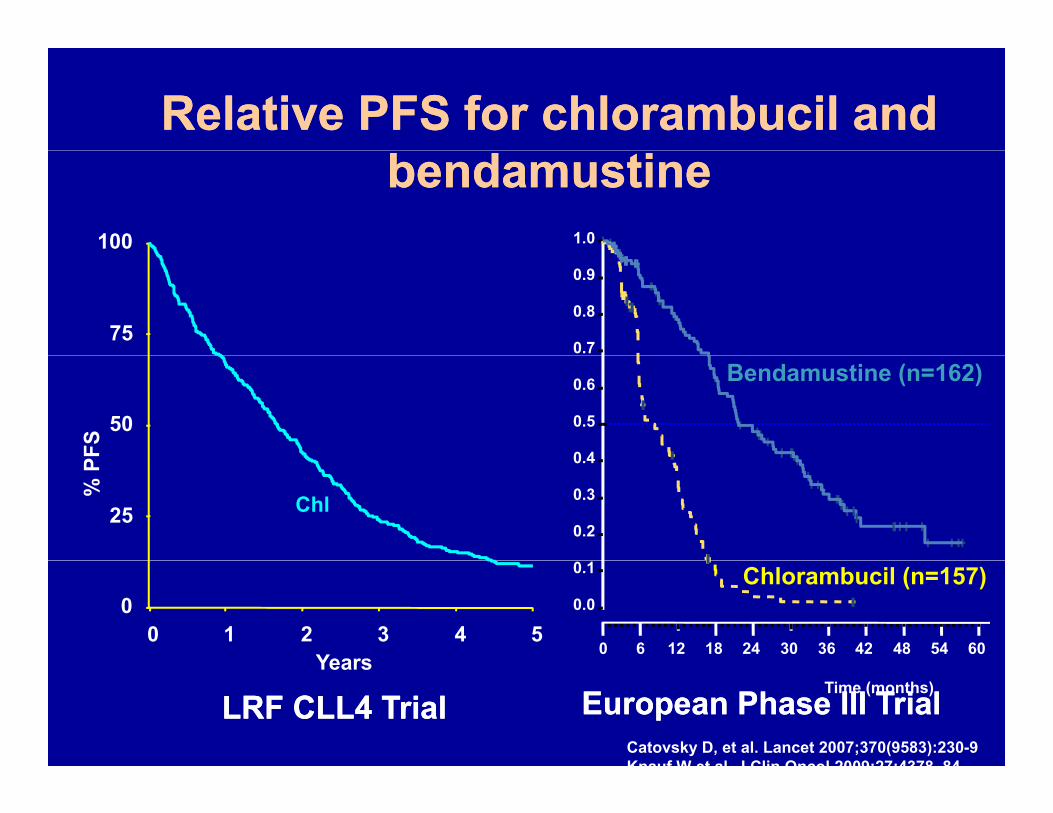
Relative PFS for Relative PFS for chlorambucilchlorambucil and and
100
bendamustinebendamustine1.0
750.7
0.8
0.9
50
FS
Bendamustine (n=162)
0 4
0.5
0.6
25
% P
Chl0.2
0.3
0.4
0 1 2 3 4 50
Years
Chlorambucil (n=157)0.0
0.1
0 6 12 18 24 30 36 42 48 54 60Years
Time (months)LRF CLL4 TrialLRF CLL4 Trial European Phase III TrialEuropean Phase III Trial
Catovsky D, et al. Lancet 2007;370(9583):230-9Knauf W et al J Clin Oncol 2009;27:4378 84
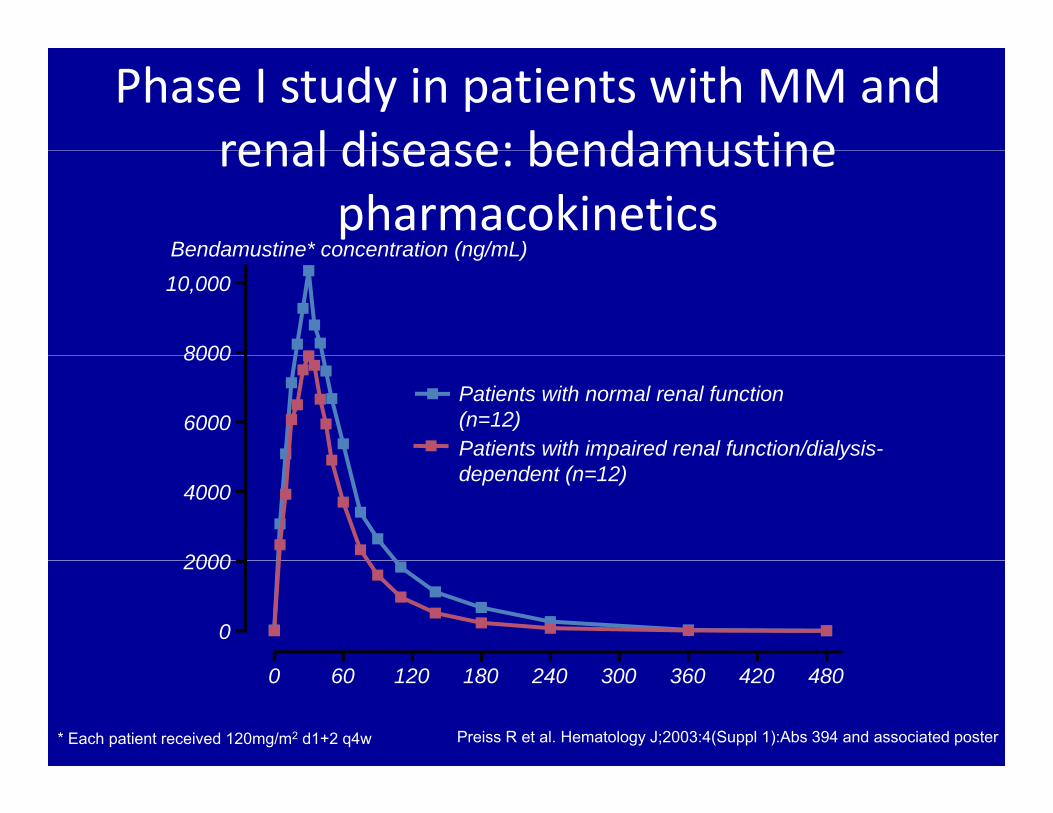
Phase I study in patients with MM and renal disease: bendamustinerenal disease: bendamustine
pharmacokineticsBendamustine* concentration (ng/mL)Bendamustine concentration (ng/mL)
8000
10,000
6000
8000
Patients with normal renal function (n=12)Patients with impaired renal function/dialysis-
2000
4000
p ydependent (n=12)
0
2000
Preiss R et al. Hematology J;2003:4(Suppl 1):Abs 394 and associated poster
0 60 120 180 240 300 360 420 480
* Each patient received 120mg/m2 d1+2 q4w
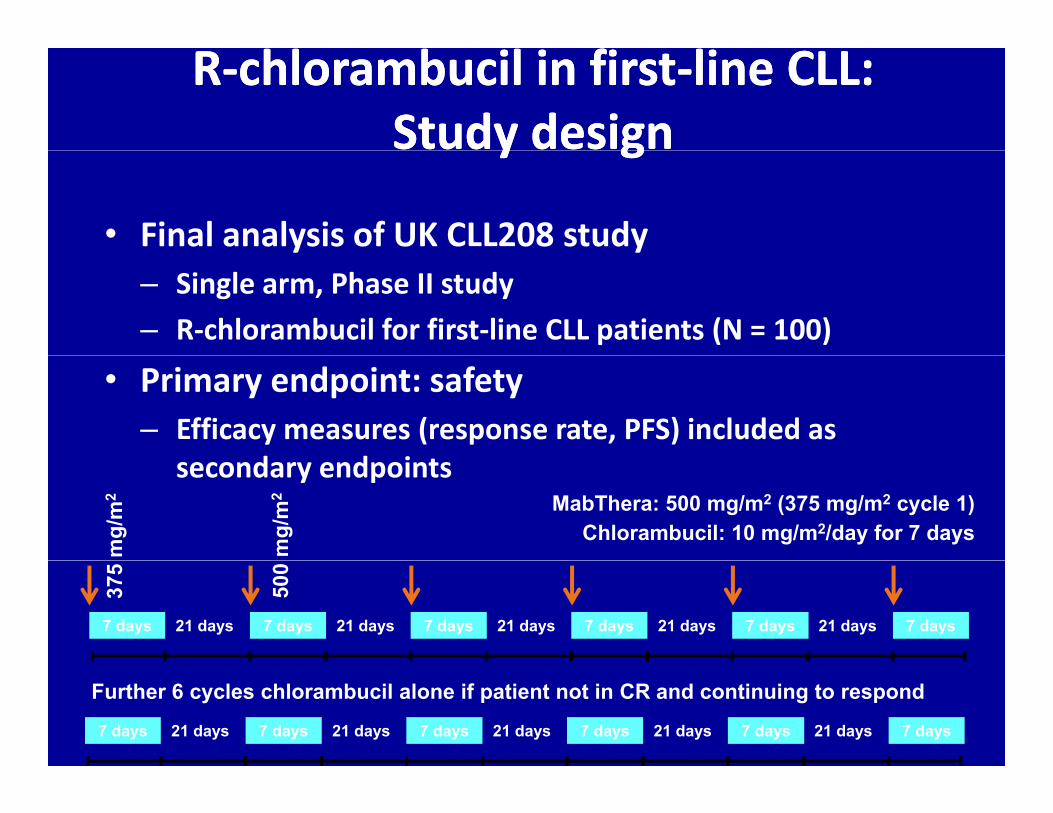
RR‐‐chlorambucil in firstchlorambucil in first‐‐line CLL:line CLL:Study designStudy designy gy g
• Final analysis of UK CLL208 study– Single arm, Phase II study– R‐chlorambucil for first‐line CLL patients (N = 100)
• Primary endpoint: safety– Efficacy measures (response rate, PFS) included as
d d isecondary endpointsMabThera: 500 mg/m2 (375 mg/m2 cycle 1)
Chlorambucil: 10 mg/m2/day for 7 days
mg/
m2
mg/
m2
375
500
7 days 7 days 7 days 7 days 7 days 7 days21 days 21 days 21 days 21 days 21 days
7 days 7 days 7 days 7 days 7 days 7 days21 days 21 days 21 days 21 days 21 days
Further 6 cycles chlorambucil alone if patient not in CR and continuing to respond

CLL208: Response ratesCLL208: Response ratesC 08: espo se atesC 08: espo se ates
CRCRMi iMi i
O %O %12%17%
3%CRCRSD/PDSD/PD
MissingMissing
ORR=80% ORR=80% 95% CI 70.895% CI 70.8––87.3 87.3
68%Median PFS: 23 months
N ti t h d MRD ti i i
PRPR23 months
No patients had an MRD negative remission
Hillmen P, presented at ASH 2010
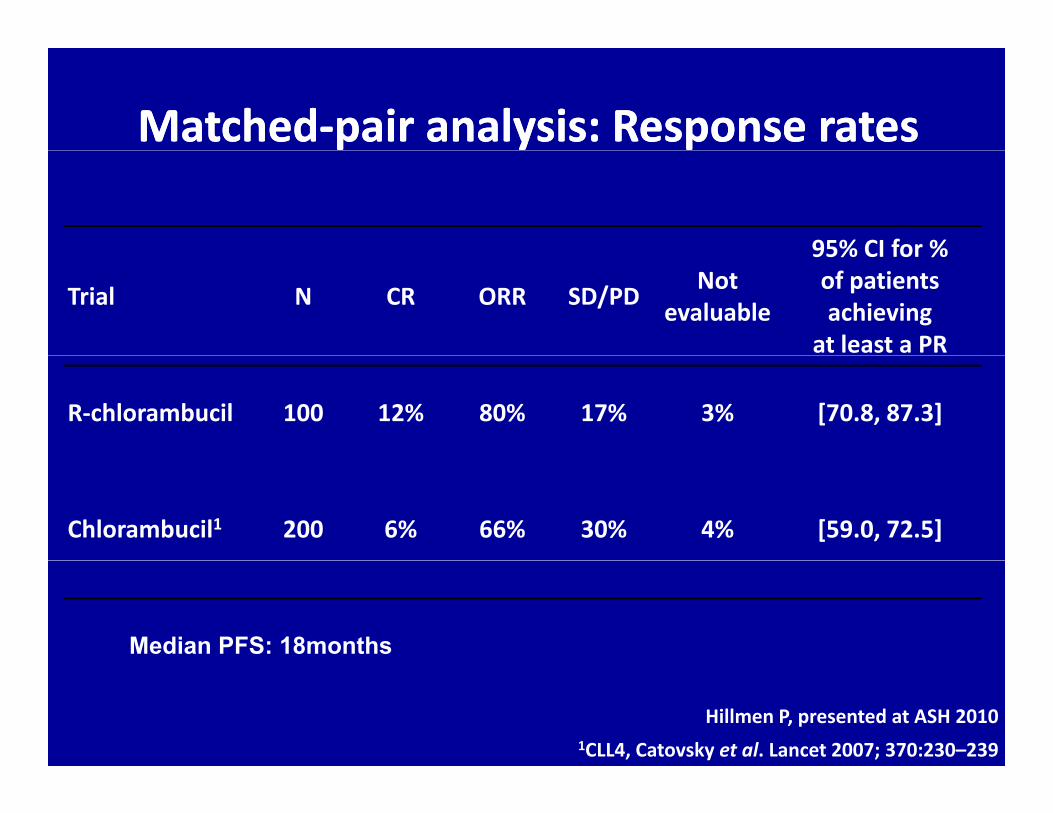
MatchedMatched‐‐pair analysis: Response ratespair analysis: Response rates
95% CI for %
Trial N CR ORR SD/PD Not evaluable
95% CI for % of patients achieving
at least a PR
R‐chlorambucil 100 12% 80% 17% 3% [70.8, 87.3]
Chlorambucil1 200 6% 66% 30% 4% [59.0, 72.5]
Median PFS: 18months
Hillmen P, presented at ASH 20101CLL4, Catovsky et al. Lancet 2007; 370:230–239

New monoclonal antibodies
GA101• CD20 monoclonal• CD20 monoclonal
• Glyco-engineered
• Humanized, type II
Ofatumumab
•CD20 monoclonal
•Humanized, type I

Ongoing CLL studies in the unfit and/or elderlyOngoing CLL studies in the unfit and/or elderlyStudy Phase Previous therapy Treatment RecruitmentStudy Phase Previous therapy Treatment Recruitment
MaBLe
(Roche)IIIb No and yes
Chlorambucil‐R
Bendamustine‐ROngoing
ChlorambucilCLL‐11
(Roche)III No
Chlorambucil
Chlorambucil‐R
Chlorambucil‐GA101
Ongoing
Complement‐1III N
ChlorambucilO i
(GSK)III No
Chlorambucil‐OOngoing
RIAltO(GSK)
III NoChlorambucil‐O
Bendamustine‐OPlanned
Origin(Celgene)
III NoChlorambucil
LenalidomideOngoing
GOELAMS and FCGCLL/WM
III No FCR +/‐ R maintenance OngoingFCGCLL/WM
GOELAMS and II N
Chlorambucil
Fludarabine+ cyclophosphamide lite
B d ti O Pl dFCGCLL/WM
II No Bendamustine‐O
Ofatumumab
Fludarabine‐O
Planned
Conclusion: CLL in Older Patients, Conclusion: CLL in Older Patients, a Problem in Search of Solutionsa Problem in Search of Solutionsa Problem in Search of Solutionsa Problem in Search of Solutions
• FCR improves survival and is the “gold-standard” for all patients p g pconsidered fit enough for therapy
• Evaluation of comorbidities and geriatric assessment • We need a validated, simple-to-use CLL comorbidity and fitness
scale• The most appropriate therapy for those unfit for FCR could be :The most appropriate therapy for those unfit for FCR could be :
– Chlorambucil monotherapy (appropriate dosing!!)• Combinations that are being tested include:g
– Chlorambucil + anti-CD20 (Rituximab, ofatumumab, GA-101)
C– Alternative chemotherapy Bendamustine + anti CD20 – FCR lite
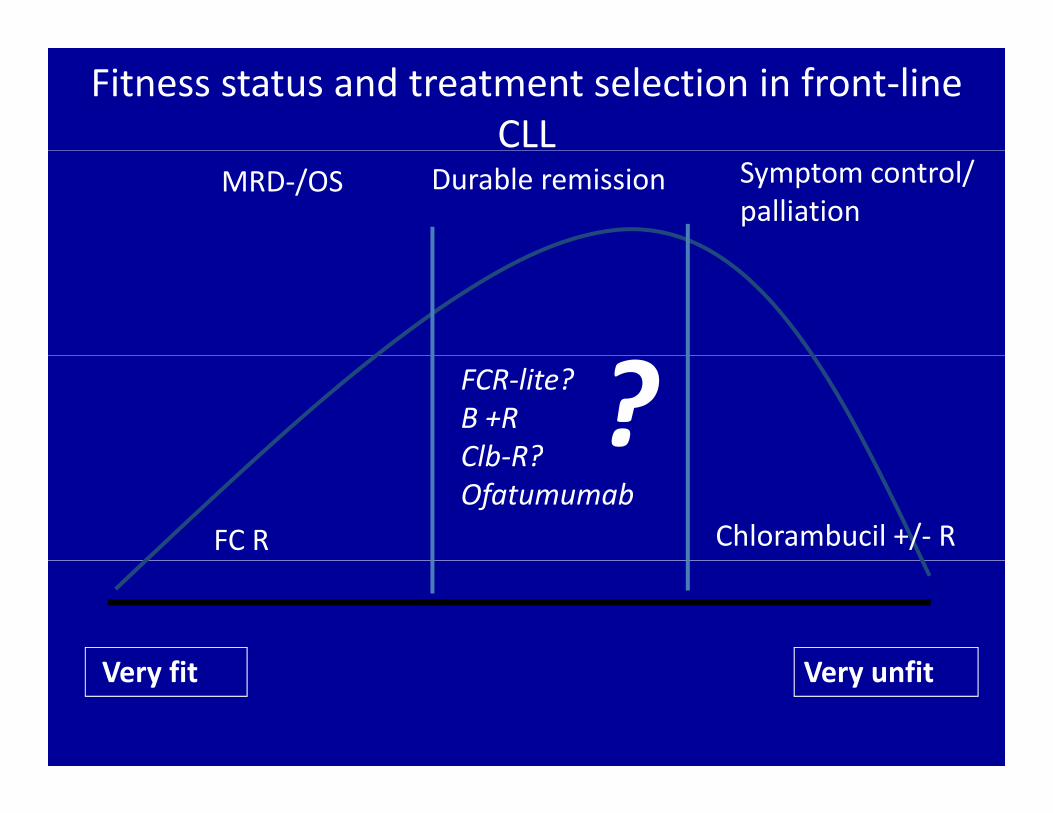
Fitness status and treatment selection in front‐line CLL
MRD‐/OS Symptom control/ palliation
Durable remission
?FCR‐lite?B +R Clb‐R?
FC R Chlorambucil +/‐ R
Clb‐R?Ofatumumab
V fi V fiVery fit Very unfit