victorian health policy and funding guidelines...
TRANSCRIPT

Department of Health
Victorian health policy and funding guidelines 2013–14
Part one: Key changes and new initiatives
Victorian health policy and funding guidelines 2013–14
Part one: Key changes and new initiatives

If you would like to receive this publication in an accessible format, please phone 9096 8422 using the National Relay Service 13 36 77 if required, or email: [email protected]
This document is available as a PDF on the internet at: www.health.vic.gov.au/pfg
© Copyright, State of Victoria, Department of Health, 2013
This publication is copyright, no part may be reproduced by any process except in accordance with the provisions of the Copyright Act 1968.
Authorised and published by Victorian Government, 50 Lonsdale Street, Melbourne.
Print managed by Finsbury Green. Printed on sustainable paper.
August 2013

Contents
Ministers’ foreword 1
Acronyms and abbreviations 2
Overview 3
1. Victorian Health Priorities Framework 2012–2022 5
2. Budget highlights 6 2.1 Competitive Elective Surgery Funding Initiative 6 2.2 State Health Budget structure and growth 8 2.3 Output initiatives 8 2.4 Asset initiatives 10
3. System improvements and innovation 12 3.1 Health Innovation and Reform Council 12 3.2 Commission for Hospital Improvement 13 3.3 Victorian Clinical Training Council 14 3.4 Clinical networks 14 3.5 Perinatal autopsy service 15 3.6 Specialist clinics and surgical waiting list public reporting 15 3.7 National Safety and Quality accreditation scheme 16 3.8 Reducing administrative overheads 16 3.9 Strategic procurement 17
4. Funding 18 4.1 National activity based funding model 18 4.2 State funding reforms 24 4.3 Data and reporting changes 26
5. Service performance 28 5.1 Health Service performance measures 28 5.2 Quality benchmarking 29 5.3 National performance measures 29
6. Improving patient experience 31 6.1 My health care experience 31 6.2 Patient safety 31 6.3 Infection control 32 6.4 Services Connect 32 6.5 Acute and subacute services 32 6.6 Mental Health Act Implementation 34 6.7 Ambulance services 35 6.8 Ageing, aged care and supported residential services 35 6.9 Community health services 35 6.10 Primary Care Partnerships 36

Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 5
6.11 Identification and management of vulnerable children 37 6.12 Health workforce 37 6.13 GLBTI Ministerial Advisory Committee 37 6.14 Intersex decision making principles 37 6.15 Tuberculosis Control Program 38 6.16 Emergency Preparedness Clients and Services Policy 38 Appendix 1: Summary of modelled budgets 2013–14 39 Appendix 2: Commonwealth funding reductions by Health Service 40


Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 1
Ministers’ foreword
The Victorian Government is committed to developing the Victorian health system so that it continues to perform to a high standard, is sustainable, responsive to people’s needs and accountable for performance in terms of health outcomes and taxpayer value. Increasing demand and an ageing population are continuing sources of pressure on the health system, while global and national factors impacting on the Victorian economy have required greater focus on efficiencies in government spending. The Victorian Government is confident that Victoria’s health system is well placed to address major challenges in the year ahead.
In the face of these pressures, the 2013–14 State Budget demonstrates the Victorian Government’s ongoing commitment to the health of Victorians, with health spending increasing to $14.3 billion this financial year, including:
• an additional $352 million for service growth in acute hospital services, and $629 million on new capital investment in the hospital building and redevelopment program
• investment of $420 million over four years to drive public elective surgery activity delivered through the Competitive Elective Surgery Funding initiative
• an additional $14.6 million for mental health and alcohol and drug initiatives including the ongoing operation of acute inpatient beds, including funding to operate new mental health beds
• an additional $238 million (over four years) clinical training package for the increased delivery of clinical training for undergraduate students, additional intern and new graduate places and increased training posts for rural general practitioners
• an additional $33.7 million for Home and Community Care services, to help keep senior Victorians living independently in the community
• $421 million for primary, community and dental health and more than more than $319 million for public health.
The 2013–14 State Budget takes a responsible approach to funding the Victorian health system. It ensures that high priority services can be maintained in difficult financial circumstances whilst still investing in the future of the health system. Despite the record investment in health by the Victorian Government, Health Services will have less funding from the Commonwealth than they were promised last year, with a $368 million reduction in Commonwealth funding over the next three years. For 2013-14, this equates to a $99.5 million savings being imposed on Health Services by the Commonwealth. The decision by the Commonwealth to remove funding is based on misleading demographic statistics that suggest Victoria’s population fell by 11,000 people in 2011. This decision by the Commonwealth will place even greater pressure on Victorian hospitals to meet growing community demand for elective surgery and emergency department treatment.
In these challenging times, the Victorian Government is committed to working with the health sector to deliver necessary whole-of-system reforms to ensure that services are delivered efficiently and are sustainable, and that our health system is enhanced and improved for the benefit of all Victorians. These include continuing support for better purchasing of goods and services through strategic procurement strategies, particularly through expansion in the operations of Health Purchasing Victoria and the competitive elective surgery funding initiative, to maximise the value of government funding for elective surgery and to build collaboration and competition within the public sector and with the private sector.
Hon David Davis MP Hon Mary Wooldridge MP Minister for Health Minister for Mental Health Minister for Ageing

Acronyms and abbreviations
ABF activity based funding
AN-SNAP Australian National Subacute and Non-Acute Patient Classification
AR-DRG Australian Refined Diagnosis Related Groups
DRG diagnosis related group
GEM Geriatric Evaluation and Management
GLBTI Gay, Lesbian, Bisexual, Transgender and Intersex
HACC Home and Community Care
HARP Hospital Admission Risk Program
IHPA Independent Hospital Pricing Authority
I-SNAC Interim-Subacute and Non-Acute Classification
LINK Leadership, Innovation, Networks and Knowledge
NEAT National Emergency Access Target
NEC national efficient cost
NEST National Elective Surgery Target
NEP national efficient price
NEPT non-emergency patient transport
NWAU national weighted activity unit
PRISM Program Report for Integrated Service Monitoring
SRHS Small Rural Health Service
VINAH Victorian Integrated Non-Admitted Health
VPCS Victorian Product Catalogue System
WIES weighted inlier equivalent separation
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 2

Overview
The Victorian Government is responsible for ensuring the delivery of a wide range of health services to the community. The state government is responsible for planning, policy development, funding and regulation of health service providers and activities to promote and protect Victorians’ health and wellbeing. The Department of Health (henceforth, ‘the department’) funds a large number of organisations to provide health services to the Victorian population including:
• healthcare delivered through public hospitals, community health services, ambulance services, public mental health, and drug and alcohol services
• provision of residential and community care for older people, support and assistance to enable people to function independently in their own homes, positive ageing programs, and healthy and active living
• health promotion and protection through emergency management, public health and related preventative services, education and regulation.
The Victorian health policy and funding guidelines 2013–14 (henceforth, ‘the guidelines’) sets out the requirements that funded organisations must comply with in addition to their contractual and statutory obligations. The guidelines detail the conditions of funding and key accountability requirements for all funded organisations.
The department regularly reviews its policies and programs, and continues to introduce a number of new initiatives to support implementation of the Victorian Health Priorities Framework 2012–2022. There will also be further changes to funding arrangements for Health Services this year, as Victoria continues to transition to the new national activity based funding model across admitted and non-admitted acute, subacute and mental health services.
The guidelines consist of three parts:
• Part one: Key changes and new initiatives, which provides an overview of the important policy, program, funding and reporting changes that come into effect this financial year. It outlines budget highlights and areas of focus for 2013–14, as well as significant policy or program changes introduced by the department.
• Part two: Health operations, which explains how funded organisations are expected to operate, and includes information on accountability, compliance, reporting and funding requirements.
• Part three: Technical guidelines, which sets out the technical aspects of the operation of Health Service funding models and payment rates.
In addition, a list of the key policy documents and guidelines for each portfolio area is available on the Policy and Funding Guidelines website, at: http://www.health.vic.gov.au/pfg
Funded organisations should always refer to the Policy and Funding Guidelines website for the most recent version of the guidelines, as items may be updated throughout the year.
Where these guidelines refer to a statute, regulation or contract, the reference and information provided in these guidelines is descriptive only. To the extent of any inconsistencies or ambiguities between these guidelines and any legislation, regulations and contractual obligations with the State of Victoria acting through the department or the Secretary of the Department of Health, the legislative, regulatory and contractual obligations will take precedence. Each funded organisation should refer to the relevant statute, regulation or contract in order to ascertain all the details of its legal obligations. If any funded organisation has any question in relation to its legal obligations it should seek independent legal advice.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 3

A note on terminology
For the purposes of these guidelines, the term ‘Health Services’ relates to public health services, denominational hospitals, metropolitan hospitals and public hospitals, as defined by the Health Services Act 1988, with regard to services provided within a hospital or a hospital-equivalent setting. Aspects of these guidelines that refer specifically to ‘Health Services’ are only applicable to these entities.
The term ‘funded organisations’ relates to all entities in receipt of funding from the department for the delivery of services. Aspects of these guidelines referring to funded organisations are applicable to all department-funded entities.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 4
1. Victorian Health Priorities Framework 2012–2022
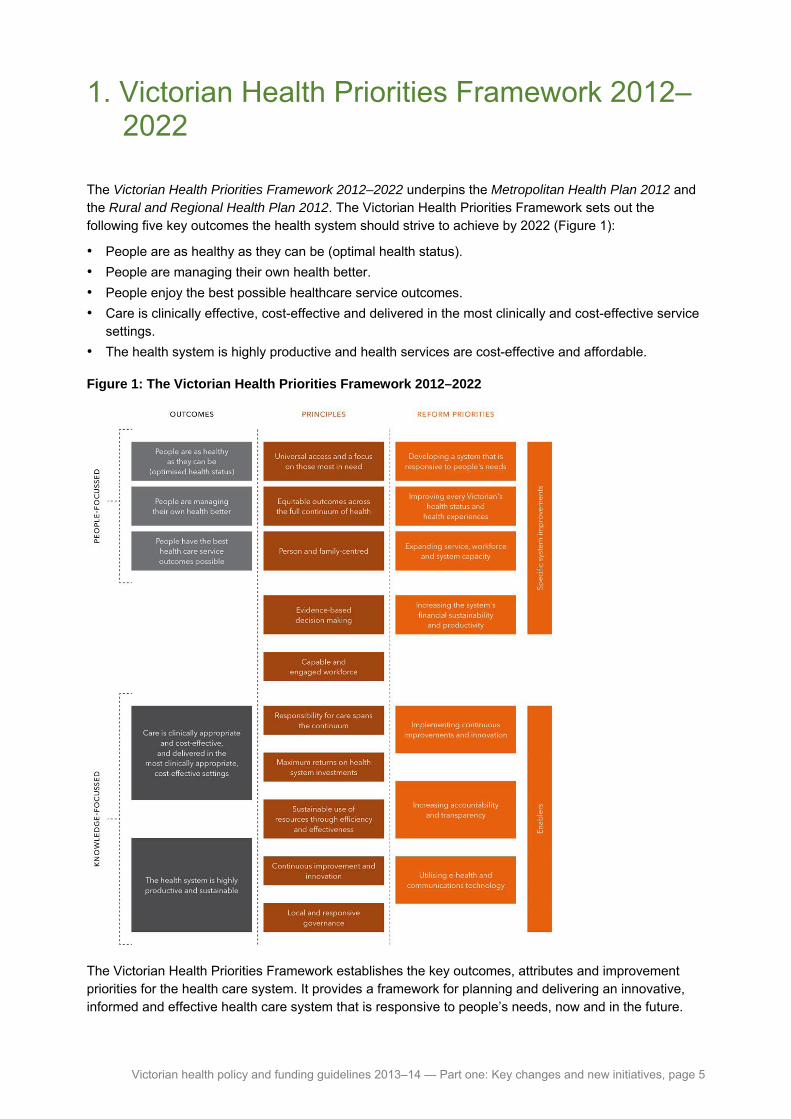
The Victorian Health Priorities Framework 2012–2022 underpins the Metropolitan Health Plan 2012 and the Rural and Regional Health Plan 2012. The Victorian Health Priorities Framework sets out the following five key outcomes the health system should strive to achieve by 2022 (Figure 1):
• People are as healthy as they can be (optimal health status).
• People are managing their own health better.
• People enjoy the best possible healthcare service outcomes.
• Care is clinically effective, cost-effective and delivered in the most clinically and cost-effective service settings.
• The health system is highly productive and health services are cost-effective and affordable.
Figure 1: The Victorian Health Priorities Framework 2012–2022
The Victorian Health Priorities Framework establishes the key outcomes, attributes and improvement priorities for the health care system. It provides a framework for planning and delivering an innovative, informed and effective health care system that is responsive to people’s needs, now and in the future.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 5
2. Budget highlights
The 2013–14 Victorian State Budget allocated $14.3 billion to the health, mental health and aged care sectors (Table 1), and invested $629 million in new health infrastructure projects. The Budget secures the Victorian health system, providing a solid base from which to deliver critical health services, support seniors to live healthy, active and independent lives, and provide better access to mental health and drug support services across the state.
The Victorian Government (henceforth, ‘the government’) has committed to support the health system deliver health and wellbeing outcomes for all Victorians in the face of growing demand and a tight fiscal environment. In 2013–14 funded initiatives include:
• treating more patients who require hospital care, including an expansion of the competitive elective surgery program and hospital substitution and diversion programs (Hospital Admission Risk Program, Hospital in the Home and Residential In-Reach)
• opening more mental health beds across Victoria
• sustaining and growing Victoria’s qualified health workforce by providing additional clinical training and medical intern positions
• additional services to meet the multiple and complex physical and mental health care needs of people from refugee backgrounds and asylum seekers settling in Victoria
• supporting senior Victorians through the joint Commonwealth- and state-funded Home and Community Care Program
• improving the health outcomes of Aboriginal Victorians through investment in targeted health promotion and prevention programs, and supporting the health sector to deliver high-quality, culturally responsive health services in local communities
• establishing programs that will improve hospital service quality and efficiencies, and reduce incidence of hospital-acquired infections
• boosting community-based health services by funding more services in growth areas.
A summary of modelled budgets for 2013–14 is provided at Appendix 1.
In 2012–13, the Commonwealth Government reduced funding to Victorian Health Services by $107 million. The Commonwealth reduction in health service funding was announced after Victorian Health Service budgets were set and took effect in November with an immediate impact on Health Service budgets. The Commonwealth Government’s decision to return funding of $107 million to Victorian Health Services was a one-off Commonwealth payment, leaving an ongoing Commonwealth shortfall in promised funding of $368 million over the next three years (see Appendix 2 for impact by Health Service). In 2013–14, this impact is $99.5 million less than promised. If the Commonwealth Government returns this funding during 2013-14, Health Service budgets will be revised accordingly in their Statement of Priorities.
2.1 Competitive Elective Surgery Funding Initiative One of the key investments in the 2013–14 State Budget was $101 million in funding allocated for public elective surgery to be delivered via the Competitive Elective Surgery Funding Initiative.
The objectives of the initiative are to:
• maximise the value of funding for elective surgery public patients over the long term
• drive efficiencies and innovation in elective surgery to improve access and maximise the number of public patients treated
• introduce contestability for the provision of elective surgery for public patients
• encourage partnerships between the public and private sector to develop new market approaches for the delivery of public elective surgery
• ensure learnings inform future approaches for treating elective surgery public patients.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 6

This initiative aims to build on the success of last year’s pilot of this program. In 2012-13, over 10,000 patients received their procedure through the initiative. This figure includes over 1,700 patients who were treated through the public private pool of the initiative.
The findings from the independent evaluation of the pilot program delivered in 2012–13 will be incorporated into the design of the initiative for 2013–14.
For 2013-14, the Competitive Elective Surgery Initiative will be split across three pools:
• a pool for Elective Surgery Information System reporting public providers
• a pool for the 10 public and private providers currently delivering surgery under the 2013 Elective Surgery Services Deed of Agreement
• a pool for public and private providers to be allocated via a new competitive Request for Submission process.
2.1.1 Public pool
Public Health Services reporting to the Elective Surgery Information System were invited by the department in June 2013 through an expression of interest process to submit bids for funding to be allocated through the public pool. Competitive funding will be provided at the full public Weighted Inlier Equivalent Separation (WIES) rate, with the discount captured as a negative specified grant. The WIES will be included within a Health Service’s total WIES targets and be monitored and funded in accordance with the 2013–14 Policy and Funding Guidelines.
Health Service Statement of Priorities will include the admissions agreed through this initiative in their elective surgery admission and waiting list targets for 2013–14. Progress against targets will be monitored through quarterly reporting and managed through the mid- and end-of-year review process.
2.1.2 Public private pool
Ten public and private providers are currently engaged to deliver surgery under the 2013 Elective Surgery Services Deed of Agreement. Nine of the 10 providers have agreed to continue delivering services until 31 December 2013. Under this arrangement, the department had the option to allocate twice the original volume to successful providers for the same procedures, subject to sufficient suitable patients and the providers agreeing to accept the additional work.
The department will seek submissions from all public and private providers of elective surgery in the second half of 2013. The submission process will be open to new public and private providers, as well as existing providers who participated in the 2012–13 pilot. The new agreements will facilitate the treatment of patients from January 2014. Further information will be released on this part of the initiative in the first quarter of 2013–14.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 7

2.2 State Health Budget structure and growth
Table 1: Victorian Health Budget details
Output group 2011–12 ($m) 2012–13 ($m) 2013–14 ($m) Percentage
increase 2012–13 to 2013–141
Acute health services2 8,956.6 9,332.3 9,836.0 5.4
Ambulance services 588.5 640.3 661.9 3.4
Mental health3 1,071.1 1,140.6 1,203.2 5.5
Ageing, aged and home care 1,112.0 1,168.1 1,216.1 4.1
Primary, community and dental health4 400.5 396.0 420.9 6.3
Small rural services 494.3 518.6 534.0 3.0
Public health5 299.9 341.3 319.3 -6.5
Drug services 143.2 146.4 153.5 4.9
Total 13,066.1 13,683.6 14,344.9 4.8
Notes
1. The movement in the Department of Health’s 2013–14 Budget compared with the 2012–13 Budget are primarily due to: - funding provided for government policy commitments, including the full-year effect of initiative funding announced in previous
years’ budgets; - output price increases arising from price escalation for anticipated cost increases; - output price increases for depreciation and capital asset charge costs associated with the approved asset investment program
for 2013–14; - increased Commonwealth funding due to the expansion of a number of programs; and - increases in anticipated income from sales of goods and services, particularly for public hospitals.
2. The movement in 2013–14 Budget reflects increased funding for government policy initiatives and output price increases arising from price escalation for anticipated cost increases.
3. The movement in 2013–14 Budget reflects increased funding for growth in mental health bed capacity. 4. The movement in 2013–14 Budget reflects increased funding for government policy initiatives and the implementation of the
equal remuneration order in the social and community services sector. 5. The movement in 2013–14 Budget reflects a revision to the anticipated expenditure of funding provided under the National
Partnership Agreement for Preventative Health.
2.3 Output initiatives The 2013-14 State Budget provides an additional $426 million ($1.8 billion over four years) in output funding to support the government’s commitment to the long-term outcomes and priorities set out in the Victorian Health Priorities Framework.
2.3.1 Acute hospital services
An additional $352 million in 2013–14 ($1.5 billion over four years) is allocated for acute hospital services output initiatives. This includes:
• $176 million in 2013–14 ($751 million over four years) to meet and manage growth in demand for essential hospital services. This includes additional emergency and inpatient capacity; outpatient, renal dialysis, chemotherapy, radiotherapy and maternity services; and cost-effective substitutes for acute care. Additional funding is also provided for critical care capacity in intensive care units and neonatal intensive care units.
• $101 million in 2013–14 ($421 million over four years) to expand the competitive elective surgery funding initiative to reduce waiting times for surgery and realise efficiencies through greater partnership with the private sector.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 8

• $55.6 million in 2013–14 ($238 million over four years) to train the future health workforce, including additional intern and new graduate places in medicine, nursing, midwifery and medical radiation, and increase to clinical training for undergraduate students, and an additional six procedural skills training posts (24 over four years) for rural general practitioners.
• $5 million in 2013–14 ($21.9 million over four years) to improve health outcomes associated with cardiovascular disease (including stroke). Funding will improve access to lifesaving treatment and medication, especially for Victorians living in rural and regional areas, and reduce readmission and disease progression rates by better managing and supporting people with chronic heart failure.
• $5 million in 2013–14 ($20 million over four years) to establish an innovation and improvement fund that will support improvements to health service efficiency, quality, safety and patient-centred care.
• $5 million over two years to establish an infection prevention and control strategy that will reduce the incidence of hospital-acquired infections in Victorian public Health Services, including a specific focus on hand hygiene.
• $1.6 million over three years (from 2012–13) to improve the health literacy of Victorian women and their families through the development of a statewide parenting kit (led by the Royal Women’s Hospital) and publishing of consumer information about having a baby.
2.3.2 Mental health and alcohol and drug services
An additional $14.6 million will be provided in 2013–14 ($67.7 million over four years) for mental health and alcohol and drug initiatives. This includes funding for the following initiatives:
• $10.2 million in 2013–14 ($42.5 million over four years) for the ongoing operation of acute inpatient beds, secure extended care units, adult and youth prevention and recovery care beds.
• $2.0 million in 2013–14 ($14.6 million over four years) to operate 16 new mental health beds.
• $2.0 million in 2013–14 ($9.4 million over four years) to operate three mother and baby units in regional Victoria for women with a mental illness and their infants. These units will be located at Latrobe Regional Hospital, Ballarat Health Service and the new Bendigo Hospital.
• $1 million over four years to expand community mental health services in East Gippsland to support access to coordinated mental health, drug and alcohol, welfare and social services.
2.3.3 Ageing, aged and home care
The 2013–14 Budget provides for $34.2 million ($142 million over four years) to support senior Victorians to remain living independently in their own homes and communities for longer by investing the following:
• $33.7 million in 2013–14 ($140 million over four years) to maintain the Home and Community Care services for senior Victorians and younger people with a disability.
• $0.5 million in 2013–14 ($2.0 million over four years) to establish the Senior Victorian Champion program, which will support senior Victorians to access information, tools and programs that will help them manage rising household costs, such as utilities.
2.3.4 Primary, community and dental health
The 2013–14 Budget provides $23.1 million in 2013–14 ($96.3 million over four years) to enhance and expand community-based services that will enable more Victorians, including Aboriginal people and refugees, to access expanded health services in their local areas. Investments include:
• $15.1 million in 2013–14 ($61.7 million over four years) to improve health outcomes for Aboriginal Victorians, by expanding the culturally-appropriate service options and building pathways to support increased use of Aboriginal community-controlled health organisations and mainstream services.
• $5.0 million in 2013–14, of which $3 million is for community health, ($22.2 million over four years) to provide timely intervention and preventative care for the increasing number of people from refugee backgrounds and asylum seekers settling in Victoria, many of whom have multiple and complex health needs that require a specialised health care response.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 9

• $3.0 million in 2013–14 ($12.5 million over four years) to boost community health services, especially in growth corridors, including allied health care, chronic disease management, post acute care and child health.
2.3.5 Public health
The 2013–14 Budget will invest $6.3 million over four years in health advancement strategies that will be delivered in partnership with communities; these include:
• $4 million over four years to improve the provision of shade through grants to local government, community groups and sporting clubs to install shade in public places, including natural shade (trees) and built shade (shade sails). This program, together with other policy and education activities, will work towards achieving the goals outlined in the Skin Cancer Prevention Framework 2013–17.
• $1.2 million in 2013–14 to establish a new and innovative pilot model designed to make Melbourne the world’s most active city, focusing on better utilisation of Melbourne’s parks and open spaces by city workers.
• $1.0 million over three years (from 2012–13) to pilot a community-based, rapid point-of-care HIV testing service as part of Victoria’s response to reducing the incidence of HIV/STI transmission.
2.4 Asset initiatives The 2013–14 State Budget commits $629 million1 (total estimated investment) to capital investment in the hospital building and redevelopment program. This includes funding for the initiatives set out in Table 2.
Table 2: Funding for asset initiatives
Initiative Description Funding
Critical care capacity expansion
Critical care capacity will be expanded with an additional four adult intensive care beds and five neonatal intensive care respiratory support beds, together with upgraded medical retrieval equipment for Health Services across Victoria. This will provide sophisticated technology and medical management to care for patients with complex illness and injuries.
$2.2 million
Health and medical precinct and community-based ambulatory care centre
A designated health and medical precinct will be established and facilitated through new planning tools and streamlined land-zoning. Streamlined land use zoning requirements for health care providers will promote private sector investment and partnerships between the private and public sectors in the provision of health services.
A community-based ambulatory care centre will be established in a health and medical precinct that promotes an integrated service model that will combine primary and secondary services.
$18.2 million
Monash Children’s Hospital A new purpose built paediatric hospital at the Monash Medical Centre in Clayton. The new hospital, delivering 230 beds, will provide capacity for increases in demand and improve access for the growing population in the south-east of Melbourne, the Mornington Peninsula and south-east Victoria.
Undisclosed2
Northern Hospital — inpatient capacity expansion
A new three-storey building will be built at Northern Hospital to accommodate 32 additional beds and support services. This investment will expand services at Northern Health to better meet the demands of the northern growth corridor.
$29.0 million
1 The total estimated investment for health projects includes funding for the Monash Children’s Hospital and the Royal Victorian
Eye and Ear Hospital redevelopment. 2 Details of the available funding are not being released prior to completion of the tender process, to ensure that the government is
able to achieve the best outcome from the market and accordingly, the best value for money for Victorians.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 10

Initiative Description Funding
Numurkah Hospital —reinstatement of acute services
This investment will re-establish a range of acute health services at Numurkah Hospital which was damaged extensively in the March 2012 floods. The new purpose-built facility includes ten acute beds, a two-bed high dependency unit, four beds for palliative or restorative care and a six-bed day procedure unit.
$18.3 million
Radiotherapy services in south-west Victoria — Stage 2
A radiotherapy service will be developed for south-west Victoria in Warrnambool. This will deliver the government’s election commitment, and enable residents to receive treatment locally instead of travelling long distances.
$10.0 million
Royal Victorian Eye and Ear Hospital redevelopment
This initiative funds the redevelopment of the Royal Victorian Eye and Ear Hospital. It will enable the hospital to meet current and future demand for specialist adult and paediatric ophthalmology and ear, nose and throat services on its existing site in East Melbourne. It will include major reconfiguration, upgrade and expansion of facilities for clinical services and significant improvements to the onsite teaching, training and research facilities.
Undisclosed2
Securing Our Health System — medical equipment replacement
The replacement of highest at-risk medical equipment in the health system will continue to be undertaken on a priority basis. This will enable Health Services to reduce risk to patients and staff and improve service availability. This initiative supports the integration of new technology by providing up-to-date replacement medical equipment that sustains acute clinical services essential for the delivery of responsive and appropriate services across Victorian metropolitan and rural public hospitals.
$35.0 million
Securing Our Health System — engineering infrastructure replacement
This initiative enables the systematic replacement of highest priority at-risk essential engineering services infrastructure to reduce risks to patients and staff and support the continued effective delivery of acute clinical services across Victorian metropolitan and rural public hospitals.
$25.0 million
Waurn Ponds Community Hospital
A new 32-bed community hospital will be built in the southern suburbs of Geelong. The new facility will provide same-day surgery, chemotherapy chairs, renal chairs and capacity for specialist clinics. This will increase services for the growing population of Geelong and the Surf Coast Shire.
$50.2 million
Werribee Mercy Hospital Mental Health expansion
New Werribee Mercy Hospital mental health facilities will be built through the construction of a new 54-bed acute mental health facility, including 25 additional beds. This investment will increase local access to mental health services and improve the efficiency of service delivery in the western suburbs of Melbourne.
$34.7 million
Western Region Health Centre — dental service redevelopment
Western Region Health Centre Dental Service will be redeveloped to enhance the provision of dental services for the inner west metropolitan area. The new 12-chair dental clinic will consolidate two existing dental service facilities and will be integrated with the community health centre.
$9.7 million
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 11

3. System improvements and innovation
The government is committed to strengthening the culture of continuous improvement and innovation across the health sector, to ensure that Victoria’s health system delivers the best possible value for the community.
The department and the sector together, through a systematic and integrated approach to creating, spreading and sustaining improvements in patient care, assists funded organisations to tackle local access, efficiency and service quality challenges as well as system-wide priorities.
In 2013–14, statewide priorities include implementing strategies to contain costs; reduce avoidable demand; better integrate planning, both vertically and horizontally; support engagement of clinicians and patients in the design of the delivery system; and provide greater clarity about the roles and responsibilities of all service providers within a system-wide framework.
System improvements and innovation are further supported by the Health Innovation and Reform Council and the department’s Commission for Hospital Improvement.
3.1 Health Innovation and Reform Council The Health Innovation and Reform Council is an independent advisory body that has been established in line with the provisions set out in the Health Services Amendment (Health Innovation and Reform Council) Act 2011.
The Council’s role is to provide advice to the Minister for Health and the Secretary on the effective and efficient delivery and management of quality health services and the continuing reform of the public health system.
The Council has established the Standing Committee on Health Quality, Safety and Outcomes.
In addition to the new areas of focus, the Council will continue to oversee the implementation and ongoing review of the Victorian Health Priorities Framework and will provide advice on range of issues referred by the Minister for Health.
More information can be found at the Health Innovation and Reform Council website: http://www.health.vic.gov.au/hirc
3.1.1 Readmissions
During 2012–13 a working group considered contemporary literature and available data on the Victorian hospital readmission rates and associated practices in order to provide advice on an effective approach to achieving improvements.
The Readmission Working Group found that for unplanned readmissions:
• Victoria’s 30-day readmission rate is consistent with comparable systems, such as Canada and the UK.
• Victoria’s 30-day readmission rate over the past five years has remained relatively unchanged.
In relation to emergency presentations following an admission, the working group found:
• In Victoria, approximately two per cent of patients discharged from Victorian hospitals returned to an emergency department within seven days of their discharge and were not subsequently admitted.
• Of all unplanned readmissions within 30-days, approximately 40 per cent were readmitted for a single day. Of these, half received their total admitted care in the emergency department, and the other 50 per cent had their care following their presentation in another location such as a short stay unit.
In 2011–12 the single-day readmissions utilised 45 public hospital emergency cubicles per day (seven per cent).
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 12
The working group concluded that focusing on strategies that support collaboration across the whole of the health system is more likely to reduce readmission rates, rather than focusing on improving hospital processes, including discharge processes, in isolation.
The Health Innovation and Reform Council has formulated a number of recommendations that aim to improve readmission performance across the Victorian health system which will be implemented:
• the Commission for Hospital Improvement will organise a Conference to showcase best practice and boost the provision of information to Health Services
• the development and launch of an online portal of key data supporting Health Services to improve their performance
• two trials of new service delivery models, with evaluation of results in 2014
• the measurement of outcomes year on year via Statements of Priorities.
3.1.2 Telehealth
A working group, consisting of clinical experts, information and communication technology experts and policy makers across the private and public sectors has reviewed existing telehealth activity levels across Victoria and contemporary evidence to understand the range of potential barriers that influence telehealth uptake. The review found that over the past decade implementation in Victoria has been predominantly driven at a local service level in response to specific health service challenges. Telehealth has often been used to address the lack of available local medical services and to reduce the travel requirements on patients and clinicians. However, it appears there has been a lack of consideration given to the deliberate use of telehealth as a genuine substitute for the more traditional face-to-face mode of service delivery.
Based on the advice of the Telehealth Working Group, the Health Innovation and Reform Council has formulated twelve recommendations that, when enacted together, should:
• lead to a more systematic and rapid uptake of telehealth technologies
• support improved access and outcomes for the Victorian community
• support cost-effective and clinically appropriate models of care.
Critically, the recommendations recognise that telehealth must not be seen as a standalone service stream, but must become embedded in everyday practice and form part of core business for all health care practitioners.
In May 2013, the Minister for Health released the government's response to the recommendations and announced innovation funding of $2.5 million for the 2013–14 period to support a number of telehealth projects across the state.
The full recommendations of the working group and further information about the announced telehealth projects can be found at the Health Innovation and Reform Council website: http://www.health.vic.gov.au/hirc
3.2 Commission for Hospital Improvement The Commission for Hospital Improvement was established in August 2012 by bringing together a number of areas in the department that focused on improvement and is responsible for supporting Health Services to deliver measurable improvement in the quality, safety, efficiency and effectiveness of the services that they provide. The Commission aims to build the capability and capacity of Health Services to drive improvement and innovation focusing on leadership, engagement, measurement, improvement methodologies, quality and safety.
The Commission uses a range of approaches and strategies to achieve this, including building leadership skill, dissemination of best practice and improvement lessons, facilitating a culture of change, networking and collaboration, providing access to expertise, and developing and implementing tools and other products. A range of online education resources on safety, quality and improvement will be made available to the sector.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 13

During 2013–14, the Commission will:
• Lead the development of the Victorian Quality Improvement Framework for Healthcare 2013–2022. The purpose of the framework is to guide and drive continuous improvement and consistency in the quality of healthcare provided in all health settings in Victoria. The framework is underpinned by consumer-centred care, including work to develop the capacity for consumers to be actively involved in treatment decisions.
• Continue to work collaboratively with clinical networks and program areas to support a range of redesign initiatives including efficiency through redesign. Health Services funded as part of the Redesigning Health Care Program will provide reports on progress and outcomes from the improvement work they undertake.
• Continue to roll out the National Health Service Productive Series tools and methodology. The Productive Series are focused on delivering meaningful results to both patients and staff in terms of quality and safety, patient experience and releasing clinicians' time to be redirected to patient care.
• Work collaboratively with Health Services and program areas to facilitate a range of leadership initiatives in 2013–14 including Clinical Leadership in Quality and Safety, the LINK in Health Leadership Strategy, and selected programs offered by its New Zealand partner, Ko Awatea.
3.3 Victorian Clinical Training Council The department has established a Victoria-wide governance system for clinical training. The stakeholder-led Victorian Clinical Training Council (the Council, previously the Victorian Clinical Placements Council) provides statewide leadership and strategic advice on issues associated with the continuum of the training pathway, inclusive of professional-entry, postgraduate, prevocational and specialist training. The work of the Council is complemented by Victoria’s Clinical Placement Networks which provide a platform for local partnership building and collaboration. From January 2014 these will be known as clinical training networks in recognition of their own expanded remit.
Consistent with an agreed emphasis on whole-of-system and interprofessional approaches, the Council includes representation from education providers (higher education and VET), Medicare Locals, public Health Services, aged care, and the private and not-for-profit sectors.
The Victorian Clinical Training Council structure includes three discipline-focused education planning groups (medicine, allied health, and nursing and midwifery). The first of these discipline-specific groups, the Medical Education and Planning Group has been established to address the issues associated with the pipeline of learners and trainees in medicine, acting as the Victorian conduit to the soon-to-be-established National Medical Training Advisory Network.
3.4 Clinical networks Clinical networks will continue to provide clinical leadership and support collaboration between clinicians, and with the department. The networks will work with the Commission for Hospital Improvement and departmental program areas to support service improvement.
In 2013–14, the focus of work will include the following:
• The Cardiac Clinical Network will take a major role in implementation of the government’s cardiac initiative and work to support hospitals meet evidence-based clinical guidelines for the management of time-critical cardiac events. The cardiac clinical network will take a major role in service development work for the Heart Health – improved services and better outcomes for Victoria plan to ensure hospitals meet evidence-based clinical guidelines for the management of time-critical cardiac events.
• The Renal Health Clinical Network will take a leading role in the implementation of a new framework, Renal directions — Better services and improved kidney health for Victorians. This outlines the objectives and priorities of the government to improve services for people both at risk of or currently experiencing chronic kidney disease.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 14
• The Stroke Clinical Network will be implementing clinical pathways across regional and tertiary services to streamline access to definitive care, and delivering evidence-based treatments, such as thrombolysis, where appropriate.
• The Paediatric Clinical Network will improve consistency and reduce variation from evidence-based clinical practice through continuing support for statewide clinical practice guidelines.
• The Palliative Care Clinical Network will consider clinical tools to assist with specialist palliative care provision, palliative care clinical indicators for pain, the development of Victorian bereavement standards, and support for implementing end-of-life care pathways in Victoria.
• The Emergency Care Improvement and Innovation Clinical Network will focus on the use of evidence-based care to reduce variation in clinical practice in areas such as the management of fever in children, atrial fibrillation with rapid ventricular response and the identification and management of the deteriorating patient.
• The Maternity and Newborn Clinical Network will focus on obesity and weight management in pregnancy, gestational diabetes, clinical deterioration in maternity patients, safe infant sleeping, perinatal mental health and the neonatal handbook.
• The Cancer Clinical Network will continue to work on patient-centred care (improved outcomes and patient experience), as well as systems-focused work to reduce variations in care and benchmark cancer services.
3.5 Perinatal autopsy service Following a review of the Perinatal Autopsy Service, in 2013–14 the department will establish a lead Health Service to provide administrative and clinical leadership under an integrated governance arrangement.
The Consultative Council on Obstetric and Paediatric Mortality and Morbidity is the advisory body to the Minister for Health on maternal, perinatal and paediatric mortality and morbidity. The Consultative Council is reliant on the information it obtains through the Perinatal Autopsy Services to fulfil its statutory functions under the Public Health and Wellbeing Act 2008. In circumstances where there is uncertainty about the precise cause of death, an expert perinatal autopsy and pathological examination of the placenta will often provide helpful information for the parents as well as for clinicians.
3.6 Specialist clinics and surgical waiting list public reporting In September 2011 the government established an expert panel to examine waiting list management and data reporting for elective surgery and specialist clinics services in Victoria's public hospitals.
In May 2013, the first quarterly data of specialist clinic activity in Victoria was released, which provided waiting time data by specialty for six Health Services. This represents a significant step forward in the public reporting of activity and performance for specialist clinics in public hospitals and represents the culmination of groundbreaking work being done by Health Services to establish this capability across the state.
In 2013–14 the department will continue to work with Health Services to:
• implement the recommendations of the expert panel’s report
• improve transparency of specialist outpatient clinic waiting list and waiting time information.
The report on specialist clinics activity and the elective surgery waiting list, as well as the recommendations of the expert panel report are accessible at: http://performance.health.vic.gov.au/Home/Publications.aspx
The department will also work with the sector to implement the Specialist Clinics Access Policy in 2013–14. The policy provides business rules and associated timeframes for specialist clinic processes. Key areas covered include referral management, clinical prioritisation, managing waiting lists, appointment scheduling and booking, patient flow and care coordination, discharge and performance monitoring.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 15
Health Services have responsibility for ensuring compliance with the policy by developing appropriate implementation processes. Health Services are expected to comply with the policy by 1 July 2015.
The department will also publish a specialist clinics service improvement guide to support the implementation of the policy. The service improvement guide will contain practical resources to assist in the management of specialist clinics, service redesign techniques and examples, and advice on the development of information for referrers.
3.7 National Safety and Quality accreditation scheme Effective from 1 January 2013 accreditation of Health Services falls under the Australian Health Service Safety and Quality Accreditation Scheme (the scheme). Under the scheme Health Services are required to be accredited against the National Safety and Quality Health Service Standards.
All eligible Victorian Health Services will be assessed against the National Safety and Quality Health Service Standards at their next accreditation assessment scheduled after 1 January 2013. This scheme applies to all Health Services, including small rural health services, clinical mental health services, as well as public dental services in community health services.
Under the scheme the department, as the jurisdictional regulator, has responsibility for verifying the accreditation status of public Health Services in Victoria.
Accreditation status will be monitored by the department in accordance with the Accreditation – Performance Monitoring and Regulatory Approach Business Rules 2013. These business rules detail the department’s approach to accreditation outcomes and provide health services with a clear understanding of the requirements of the new scheme and reporting obligations related to accreditation outcomes. The department’s response will be based on the outcome of the accreditation assessment and allow for escalation of monitoring and intervention.
Performance against accreditation will be reviewed at performance meetings with Health Services.
Further details on accreditation requirements and resources to support health services can be found at: http://www.health.vic.gov.au/accreditation
3.8 Reducing administrative overheads Hospital administrative costs are frequently considered as providing opportunities for efficiency improvement and cost savings and have been a focus of the National Health Service in the United Kingdom. Identified as a priority in 2012–13 all Health Services included within their Statement of Priorities actions to increase the financial sustainability and productivity through examining and reducing the variation in administrative overheads.
The department has established a health sector reference group which is working to determine indicators and benchmarks for measuring administrative structure efficiency within Health Services with a view to provide a benchmarking comparative tool to support health service decision making. Whilst it is anticipated that Health Services are performing well against administrative cost comparators and are generally efficient, it is expected that a range of cost saving opportunities will be identified across a range of non-clinical areas. An important element to consider in evaluating service provision and potential cost savings is the cost versus the quality of the service provided.
In 2013–14 the department will continue to work with the sector to develop a priority set of indicators for use by Health Services and collaborate with the Commission for Hospital Improvement to link activities to improving efficiency. Health Services Statement of Priorities will include an action in 2013–14 that will require each Health Service to develop deliverables that ‘Reduce variation in health service administrative cost'.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 16

3.9 Strategic procurement The government’s policy paper Securing Victoria's Economy identifies the importance of ensuring more efficient and productive delivery of health services in Victoria. Health system procurement reform will focus on enhancing hospital cost containment and improved procurement processes by:
• increasing the range of agencies able to procure from Health Purchasing Victoria (HPV) contracts and tenders
• increasing the number and value of tenders and contracts managed by HPV
• working with the sector to improve procurement processes.
The Health Services Act 1988 was amended during 2012–13 to enable community health centres and women’s health centres to access HPV contracts. HPV will focus on collective procurement, volume purchasing and further broadening the scope of agencies eligible to access Health Purchasing Victoria’s tenders and contracts.
This work includes ongoing implementation of the statewide contract for hip and knee prothesis, valued at approximately $45 million per annum and achieving 10 per cent cost reduction. Cost savings have been achieved by encouraging rationalisation of suppliers through commitment discount thresholds.
In 2013–14 HPV will focus on achieving further additional savings of $30 million and will undertake further expansion of tenders and contracts under its management. HPV and the department will work with the Victorian Competition and Efficiency Commission, the Victorian Department of Treasury and Finance and other stakeholders to ensure implementation of HPV’s expanded role.
HPV is committed to implementing the Victorian Product Catalogue System (VPCS). Stream 1 of VPCS was made operational during 2012–13. In December 2012 the VPCS went “live” containing all product and pricing information published by HPV suppliers to the National Product Catalogue, which is then synchronized with a number of HPV Pricing Schedules. It currently contains over 175,000 items from 135 suppliers.
With the VPCS now live for use by HPV, their next goal is to develop and implement a Victorian Common Catalogue. A Common Catalogue builds upon the VPCS synchronisation concept and will provide up-to-date product and pricing information, a centrally defined set of item descriptions, identifiers and categories for all Health Services.
HPV has also commenced scoping measurable end-to-end supply chain efficiencies, investigating various reform options and taking into account the practices of other jurisdictions and industries.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 17

4. Funding
4.1 National activity based funding model The implementation of a nationally consistent approach to activity based funding (ABF) for acute admitted services, emergency department services and non-admitted patient services began on 1 July 2012. From 1 July 2013, this approach will be extended to cover in-scope mental health and subacute services.
The timetable for implementation of national activity-based funding has been driven by the Commonwealth’s new growth funding methodology, which will commence in 2014-15, rather than the feasibility of producing mature models for the extension of activity-based funding to emergency departments, non-admitted and sub-acute care, and mental health services by July 2014. This has resulted in the development of a national funding model by IHPA which has been based on costing, classification and data systems which have serious gaps, and are therefore not yet fit for the purpose of supporting a national funding system which will enable states to effectively manage their public hospital systems.
The staged implementation of the national funding model will continue for 2013–14 to avoid major funding distortions for Health Services while the national models are still being developed and tested and until Victoria is satisfied the national model is robust and reliable. This will ensure consistency and predictability for Victorian Health Services to manage activity and funding under the new national models. Under this approach:
• Activity targets and prices will be set according to the existing Victorian funding models, which are supported by current information and financial systems.
• Activity targets will be translated by the department to National Weighted Activity Units (NWAUs). Funding will be flowed to Health Services through the National Funding Pool according to those targets.
• The volume and price of NWAUs will be adjusted to reflect each Health Service’s budget set through the existing Victorian model.
• Health Services will report activity and monitor revenue using the existing Victorian funding model in 2013–14.
• The department will convert activity data to an equivalent number of NWAU for reporting to the National Funding Pool Administrator.
A number of changes will ne made to Victorian funding models in 2013–14 to bring them closer to the national model and assist with the transition towards full implementation of the national approach into the future. Key changes are:
• Admitted subacute care: an interim funding and pricing model will be introduced that is uniform across all admitted subacute programs. The interim pricing model has one price and 17 classes, each with a price weight. There will be no changed data requirements for the interim model.
• Admitted mental health services: transition towards the national model will commence with the introduction of patient centred pricing using a ‘shadow’ weighted occupancy approach for non specialist inpatient services (acute adult, aged, child and adolescent mental health beds). This approach assumes 100 per cent occupancy and will not be adjusted for over or underperformance. Actual occupancy will be monitored to determine appropriate thresholds for 2014-15. An end of year process based on actual bed days and cost data analysis will be undertaken to realign funding between admitted and non-admitted (community) settings.
• Acute admitted services: WIES20 has been developed for use in 2013-14. The Diagnosis Related Group (DRG) version will be maintained as AR-DRG 6.0x and cost weights have been refreshed using 2011–12 cost data. The Victorian DRG modification for admitted non-sameday radiotherapy will be retained and a new Victorian DRG modification will be introduced for combined ventilatory support for neonates.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 18
• Funding for medical indemnity insurance will continue to be paid through the WIES price, with the exception of Small Rural Health Services which be funded via a specified grant. A manual adjustment has been made to the WIES 20 cost weights to fully capture the relative cost (risk) of medical indemnity insurance for the 19 obstetric DRGs. This change means that the previous adjustment for insurance costs made through specified grants is no longer required. Health Services will receive full funding for medical indemnity insurance through the WIES price.
• Non-admitted radiotherapy services: a reduced rate will be payable for non-admitted radiotherapy services, and Health Services will be able to retain revenue received from all other sources.
• Funding arrangements for emergency departments and non-admitted specialist outpatient services will continue as outlined in 2012–13.
• Non-admitted subacute services will be block funded in 2013–14.
• Indigenous adjustment: To improve consistency with the national approach to funding of Aboriginal and Torres Strait Islander patients, the 30 per cent indigenous patient adjustment will be extended to admitted subacute and mental health bed days for 2013–14. Further work will be undertaken during 2013–14 to look at further extending the co-payment to non-admitted services from 2014-15.
• Paediatric adjustment: a paediatric complexity grant will be provided to Monash Children’s Hospital to reflect the paediatric loading this hospital would receive under the national model. Current paediatric complexity funding for the Royal Children’s Hospital will be split to identify the proportion of this funding that would be received through the national paediatric loading.
4.1.1 Monitoring NWAUs
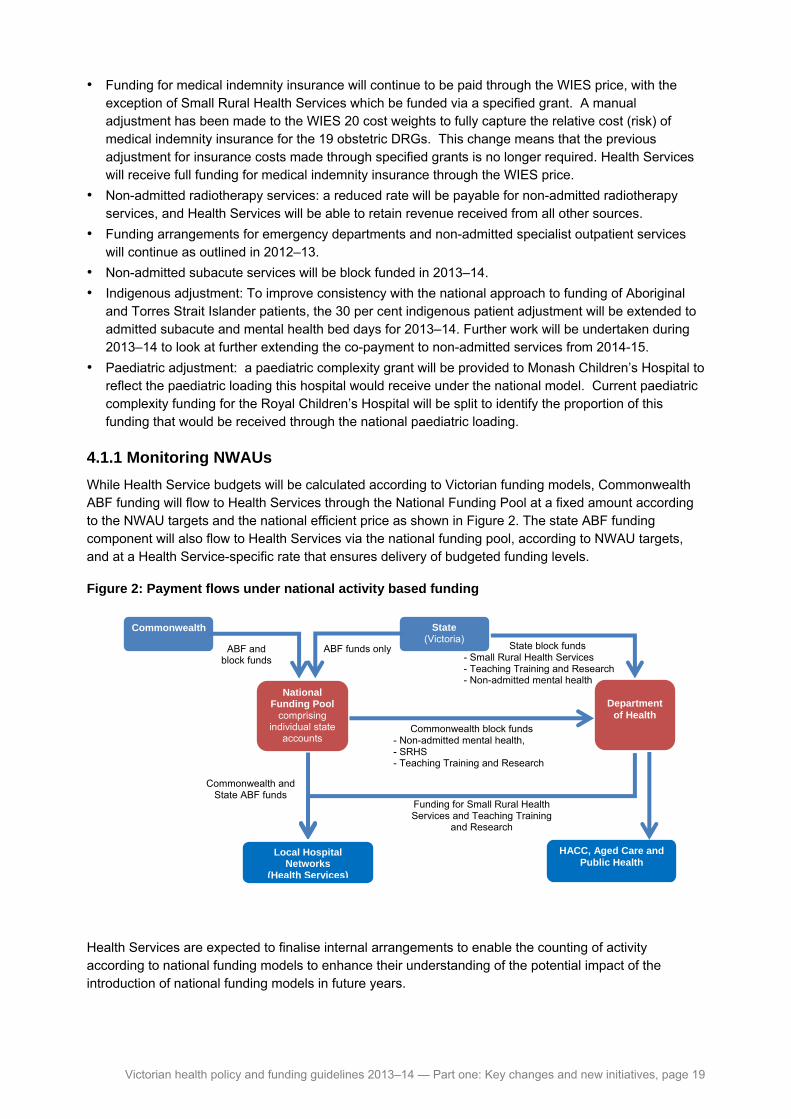
While Health Service budgets will be calculated according to Victorian funding models, Commonwealth ABF funding will flow to Health Services through the National Funding Pool at a fixed amount according to the NWAU targets and the national efficient price as shown in Figure 2. The state ABF funding component will also flow to Health Services via the national funding pool, according to NWAU targets, and at a Health Service-specific rate that ensures delivery of budgeted funding levels.
Figure 2: Payment flows under national activity based funding
National Funding Pool
comprising individual state
accounts
Commonwealth
ABF and block funds
State(Victoria)
ABF funds only
Department
of Health
Commonwealth and State ABF funds
Commonwealth block funds - Non-admitted mental health, - SRHS - Teaching Training and Research
State block funds - Small Rural Health Services - Teaching Training and Research - Non-admitted mental health
Funding for Small Rural Health Services and Teaching Training
and Research
HACC, Aged Care and Public Health
Local HospitalNetworks
(Health Services)
Health Services are expected to finalise internal arrangements to enable the counting of activity according to national funding models to enhance their understanding of the potential impact of the introduction of national funding models in future years.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 19

NWAU targets will be included in Health Services’ Statement of Priority process. Monthly reports will be provided to Health Services on NWAU activity. An additional field has been added to the F1 report to enable Health Services to report monthly activity in NWAUs along with the state-based funding models.
Workshops will be held for Health Services to provide guidelines and assistance to monitor NWAUs. Facts sheets are available on the department’s Activity Based funding website to provide guidelines and assistance for Health Services. NWAU calculators are available for download from the Independent Hospital Pricing Authority (IHPA) website: http://www.ihpa.gov.au/internet/ihpa/publishing.nsf
National recall policy
The National Health Funding Body is required to complete six monthly reconciliation against NWAU targets for each Local Hospital Network in Victoria. This reconciliation process is yet to be determined by the Administrator and it is unknown if this will impact Commonwealth payments for Health Services under the fixed funding arrangements for 2012-13 and 2013-14. The department will keep Health Services informed of any implications arising from the Administrator's determination.
National funding model specifications for 2013–14
In 2013–14, in-scope public hospital services which will be funded under the national ABF model are:
• all acute admitted patient services, including Hospital in the Home
• all emergency department services
• all admitted subacute services
• all admitted mental health services
• specified non-admitted acute and subacute patient services, as determined by IHPA.
In 2013–14:
• the national activity unit will be known as NWAU(13)
• the national efficient price is set by IHPA at $4,993. Costing information used to determine the national efficient price was drawn from the 2010–11 National Hospital Cost Data Collection Round 15.
The national model uses a number of classification systems to express the relative cost weights in terms of NWAUs for each ‘group’ of ABF services. The national classification systems used to group patients for each ABF service are:
• admitted patient services: Australian Refined Diagnosis Related Groups (AR-DRG) Version 6.X
• emergency department services: Urgency Related Groups Version 1.3 (for recognised emergency departments at Levels 3B-6) and Urgency Disposition Groups Version 1.3 (for recognised emergency departments at Levels 1-3A)
• non-admitted patient services: Tier 2 Outpatient Clinics Definitions Version 2.0.
• admitted mental health patient services: Modified version of AR-DRG Version 6.x
• admitted subacute patient services: Australian National Subacute and Non-Acute Patient Classification (AN-SNAP) Version 3.
The final price payable for an NWAU-funded activity will include a number of adjustments, including:
• paediatric adjustment: payable for patients aged up to and including 16 years (excluding newborn and neonates) who have spent time in an approved children’s hospital (Royal Children’s Hospital and Monash Children’s Hospital)
• outer regional and remote adjustment: payable for patients whose residential address is within an area that is classified by the Commonwealth as being ‘outer regional or remote’
• Indigenous adjustment: payable for patients who identify as being of Aboriginal and/or Torres Strait Islander origin
• intensive care unit adjustment: payable per hour spent by a patient in an approved intensive care unit
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 20

• private patient service adjustment: an adjustment to the price weights for private patients to take into account revenue received from third-party providers (such as Medicare Australia) for prostheses, pathology, imaging and medical costs
• private patient accommodation adjustment: an adjustment to the price for private patients to take into account revenue received from private health insurers.
More detailed technical information on the national ABF model is available on the IHPA website at: http://www.ihpa.gov.au
4.1.2 Transition arrangements for subacute care services
The IHPA has developed a national subacute funding model based on the AN-SNAP service classification.
For Victoria, it is proposed to commence the transition to AN-SNAP with the introduction of an interim pricing model that includes essential features of AN-SNAP and is uniform across all admitted subacute programs. Key components of the interim model are:
• The model will be called the Interim-Subacute and Non-Acute Classification (I-SNAC) and will incorporate funding for inpatient palliative care, rehabilitation, Geriatric Evaluation and Management (GEM) and maintenance care.
• I-SNAC comprises of one price and 17 weighted classes. The weighted classes are based on patient attributes. There are four classes for palliative care (based on Phase of Care), 11 classes for Rehabilitation (based on impairment) and one class each for GEM and maintenance (based on care type). The patient attributes differentiating classes are the same attributes being used for the national model.
• Funding will be provided on a bed day basis that is weighted by the class in which the activity is aligned. An activity loading will be applied based on indigenous status and the remoteness area of the patient’s usual accommodation.
• Funding for public nursing home type services will be discontinued from all Health Services except for Department of Veterans’ Affairs patients and Small Rural Health Services (SRHS).
• No new data collection burden is imposed for the model.
The National Minimum Data set definitions are found at the METeOR online registry at www.aihw.gov.au
Victoria has made changes to align subacute service delivery with the care type changes. The changes are consistent with the service expectations and levels detailed in the Subacute Capability Framework and include:
• Restorative care (R1 and R2) will be incorporated into GEM in all level 3 and above Health Services (excluding Swan Hill) as defined by the Subacute Capability Framework.
• Local Health Services delineated as Level 2 (and Swan Hill) in the Subacute Capability Framework will provide and report maintenance care only.
Health Independence Program consolidation
In 2013–14, the department will consolidate the funding for Post Acute Care, Subacute Ambulatory Care Services, Hospital Admission Risk Program (HARP) and Residential In-Reach services under a single funding stream and flow to Health Services as Health Independence Program funding. The consolidation will support the key objectives of the Health Independence Program guidelines and encourage Health Services to use their funds and workforce more flexibly based on client need.
4.1.3 Transition arrangements for mental health services
The IHPA is in the process of developing a new classification system for mental health care services, however, the model will not be ready for 2013–14. For 2013–14, IHPA has developed an interim model using an ‘enhanced’ AR-DRG-based model (including age-related loadings) for admitted inpatients.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 21

Victoria will not adopt the IHPA model for 2013–14 as it has not been completed or tested, and instead will commence the transition by introducing patient centred pricing using a ‘shadow’ weighted occupancy approach for non specialist inpatient services (acute adult, aged, child and adolescent, mental health beds). The model takes into account age, care delivered in a rural setting and care for Indigenous patients.
The department has also consolidated various bed-day payment rates and will introduce a single unit price for non specialist acute beds and some specialist acute beds for weighted occupancy. In addition, some of the funding provided historically as specified grants will now be rolled into the revised prices.
In 2013–14 funding assumes 100 per cent occupancy and will not be adjusted for over or underperformance. Actual occupancy will be monitored to determine appropriate thresholds for 2014–15. An end-of-year process based on actual bed days and cost data analysis will be undertaken to realign funding between admitted and non-admitted (community) settings.
Non-admitted mental health services will be block funded in 2013–14. Secure extended care, specialist and statewide mental health services, such as forensic inpatient services and eating disorder inpatient services, will continue to be funded on the existing basis.
Secure extended care, specialist and statewide mental health services, such as forensic inpatient services and eating disorder inpatient services, will continue to be funded on the existing basis.
4.1.4 Transition arrangements for Small Rural Health Services
The national model includes recognition that activity based funding may not always be practicable and that some services will need to be funded on a block grant basis. Under current arrangements SRHS will be funded nationally through block grants.
For 2013–14, the IHPA developed the following block funding criteria to determine which public hospital services are eligible for block funding:
• block funding will be required when it is not technically possible to use ABF
or
• when there is an absence of economies of scale that mean some services would not be financially viable under ABF.
The IHPA has determined ‘low volume’ thresholds for use in 2013–14. Under these thresholds, hospitals may be eligible for block funding if they are:
• in a metropolitan area, and provide ≤ 1,800 acute inpatient NWAU per annum
or
• in a rural area and provide ≤ 3,500 acute inpatient NWAU per annum.
The government provides advice to the IHPA on which services meet the criteria to be block funded. Services currently funded through the SRHS model will continue to be block funded. Those currently receiving output funding through the casemix model will be subject to ABF.
The IHPA has applied these criteria in developing the National Costing Model, and the National Efficient Cost (NEC) Determination for 2013–14 that applies to block funded services.
The IHPA block funding model incorporates two components, an availability payment and a service capability payment:
• availability payment: this component recognises that block funded hospitals have significant fixed costs. Availability payments are determined on the basis of total reported NWAU activity, and Australian Standard Geographical Classification Remoteness
• service capability payment: this payment recognises the costs related to the level of service provision. Hospitals in Groups F and G will receive an additional Service Capability payment of $498 per NWAU.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 22

The average cost of a block funded hospital in Australia in 2010–11 was $4.7 million (NEC), derived from in-scope expenditure data for 2010–11, which was reported to the National Public Hospital Establishment Database. The NEC is a benchmark price to guide governments about the level of funding which would meet the average cost of providing services in SRHS across Australia.
For more information on this and for categorisation of SRHS refer to the NEC determination available at: http://www.ihpa.gov.au/internet/ihpa/publishing.nsf/Content/nec-determination-2013-14
4.1.6 National Partnership Agreement on Improving Public Hospital Services Schedule E: Subacute bed guarantee funding information
Commonwealth funding through the National Partnership Agreement on Improving Public Hospital Services Schedule E will conclude on 30 June 2014. In 2013–14, Victoria is allocating final-year facilitation funding of $154.7 million to:
• capital expansion
• service expansion (admitted and non-admitted)
• specialist subacute equipment to enhance quality of current service provision and support expansion of subacute services
• enhance specialist subacute care workforce through supporting engagement in training and development
• improve access to subacute ambulatory care services
• redesign patient flow from acute to admitted subacute and to the community to enhance patient access and flow across the service system.
A national review of the lapsing funding, as committed by the Commonwealth in the National Health Reform Agreement, is expected to occur in 2013.
4.1.7 National Health Reform Agreement Schedule F: Aged Care and Disability Services
Victoria has agreed to the National Disability Insurance Scheme (DisabilityCare Australia). As a result, from 1 July 2015 there will be a split in the funding and management of the Home and Community Care (HACC) program in Victoria.
The Commonwealth will become solely responsible for services to people aged over 65, and services currently funded under HACC for those over 65 will be transferred to the Commonwealth. In 2013–14 and 2014-15, the HACC program will continue to be managed by the department, and service providers will be kept informed of all decisions and issues relating to the transition of their service agreements to the Commonwealth.
In negotiating details of the transition, the two governments have agreed to work together to retain the benefits of the current HACC system in Victoria.
Home and Community Care and DisabilityCare Australia
From 1 July 2013 some HACC clients in the Barwon launch site of DisabilityCare Australia will become DisabilityCare Australia participants. The relevant HACC service providers will need to plan for a progressive reduction in their HACC output targets for 2014-15 and beyond, to reflect the extent of migration of people aged under 65 from HACC to DisabilityCare Australia Scheme. Transition details will be discussed with relevant agencies during 2013–14.
In 2016-17 when the roll-out of the DisabilityCare Australia begins, a proportion of current HACC clients under 65 will be eligible and will progressively join that scheme.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 23

4.2 State funding reforms Ongoing funding reform is required to achieve longer term sustainability and adapt to new challenges. This task will require improving the funding arrangements between governments, greater flexibility in funding models and rigorous fiscal management. Health Services and government will need to work together to ensure effective and appropriate decisions are made about how resources are allocated and performance is measured.
4.2.1 Funding reviews for 2013–14
During 2013–14 the department will review funding related to Health Services' research grants and blood products.
Health Services currently receive annual funding for general research purposes. The department will undertake work during 2013–14 to clarify the intent of research funding, establish accountability mechanisms for use of research funding and review the allocation methodology to ensure funding is distributed in an appropriate manner.
Blood products are in scope under the national funding model. Under existing Victorian arrangements, blood and blood products are provided free of charge to public and private hospitals in Victoria. The department funds the National Blood Authority directly. Under the National Health Reform Agreement and costing standards, blood should be costed and included in price. This is not currently possible in Victoria (and some other jurisdictions). To adjust for the differing practice across jurisdictions, the IHPA currently makes a price-based adjustment to remove these costs from some jurisdictions' data. IHPA has indicated that the inclusion of the cost of blood and blood products in national funding models is an issue that will be considered in coming years. In time, it is likely that blood funding will be absorbed into the national pricing arrangements, thereby ensuring an appropriate Commonwealth contribution towards the cost of blood products. Work will be undertaken in 2013–14 to develop a process to transition Victoria’s funding approach for blood products to an activity basis, in anticipation of a similar change occurring at the national level.
4.2.2 Non-admitted radiotherapy and allied health
The non-admitted patient radiotherapy funding model has previously incorporated a premium for associated department costs, including allied health services provided to radiotherapy patients.
In 2013–14 an amount of $1.8 million will be removed from the non-admitted radiotherapy budget and will be paid to radiotherapy hub hospitals for allied health service events as defined under the IHPA Tier 2 non-admitted services definitions manual. Health Services will be required to report aggregate service event activity on the Agency Information Management System S10 form against appropriate allied health clinics registered on the Non-Admitted Clinic Management System.
The non-admitted radiotherapy price per weighted activity unit will be discounted to effect this change and overall funding will remain neutral.
4.2.3 Victorian Artificial Limb Program
From 1 July 2013 the Victorian Artificial Limb Program will no longer be funded under general WIES equivalents and funding will be provided as a block grant to Health Services as a non-admitted subacute service. Funding will also be incorporated into the budget model, rather then being paid through prior year adjustments. This is likely to be an interim arrangement as the Victorian Artificial Limb Program will transition to activity based funding in the future.
From 1 July 2013 Victorian Artificial Limb Program services will be required to report client-level data. The unit of count for client-level activity will be a non-admitted service event. Service events will be reported on the S11 form with the view to reporting on Victorian Integrated Non-Admitted Health (VINAH) dataset from 1 July 2014.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 24

To monitor maintenance of effort the pre-existing annual activity statement of provision of limbs and repairs including expenditure will also be required for 2013–14.
4.2.4 Provision of aids and equipment and domiciliary oxygen
A comprehensive set of guidelines has been developed that clarifies the responsibilities of Health Services in the provision of aids, equipment and domiciliary oxygen, for patients being discharged from hospital. The guidelines are available at: http://www.health.vic.gov.au/feesman/
4.2.5 Payments to Health Services and treatment of variations to throughput
In 2013–14 the department will introduce single monthly payments through the Hospital Budget and Payments System (apart from July where two payments will be made), with standard cash flow percentages for all Health Services. The department will monitor hospital cash-flows as reported monthly in the finance return.
Actual throughput against target will continue to be monitored on a monthly basis by the department. Annual targets will be subject to a mid-year review, and any reallocation of throughput will result in adjustments to the original monthly targets.
4.2.6 Recall policy
The standard Health Service recall, which uses a progressive scale of funding recalled based on the level of underperformance, will be extended to apply to local peer group (price) Health Services.
4.2.7 Renal WIES targets
For 2013–14, renal activity and WIES will no longer be paid to actual and will be incorporated within total agency public and private WIES activity targets (excluding Small Rural Health Services which will continue to be funded to actual activity). Renal WIES will be subject to the prior year adjustment process for public and private activity.
4.2.8 Private Patient accommodation charges
Section 72.1(2) of the Private Health Insurance Act 2007 states that an insurance policy covering hospital treatment must provide at least the ‘minimum benefit’ for that treatment. The Commonwealth Minister for Health stipulates the minimum benefits payable by private health insurers for shared ward accommodation in public hospitals through the Private Health Insurance (Benefit Requirements) Rules. The Commonwealth does not set a minimum benefit for single room accommodation.
Health services are able to make their own determination on accommodation fees to be charged to private patients who receive treatment at their campuses. In coming to this decision, health services should consider the following:
• the benefit that private health insurance funds will assign to the public hospital in their health insurance products
• any copayment a patient may be willing to pay as a private patient
• the amount of any copayment or excess the hospital can viably forego.
To assist health services with this decision, the department provides a recommended fee schedule for private patient accommodation in the department’s Fees and Charges Manual available at: http://www.health.vic.gov.au/feesman/index.htm.
Recent analysis by the department has shown that the actual cost of providing accommodation to private patients is significantly higher than the Commonwealth’s minimum benefits. Table 3 outlines the Commonwealth’s 2013–14 default minimum benefits for shared ward accommodation in Victorian public hospitals, and the average public hospital accommodation costs per bed day for private overnight patients (based on the 2010 Victorian Cost Data Collection). At a minimum, these rates would be expected to be charged to private patients in public hospitals.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 25

The Commonwealth Department of Health and Ageing has committed to undertaking a review of private patient accommodation rates and indexation methodology during 2013-14. The department will engage nationally in this review to seek a fair and appropriate price for Victorian Health Services which better reflects the costs incurred in treating private patients.
Table 3: 2013–14 Private patient accommodation fees
Account Class
Commonwealth default minimum benefit for shared
ward accommodation 2013–14
Shared ward average actual
cost per bed day (2010–11)
Single room average actual
cost per bed day (2010–11)
Advanced surgical patient:
• first 14 days
• over 14 days
$394
$273
$569
$528
$666
$518
Surgical or obstetric patient:
• first 14 days
• over 14 days
$365
$273
$558
$522
$760
$604
Psychiatric patient:
• first 42 days
• 43-65 days
• over 65 days
$365
$317
$273
$624
$612
$642
$811
$936
$901
Rehabilitation patient:
• first 49 days
• 50-65 days
• over 65 days
$365
$317
$273
$414
$467
$415
$503
$496
$543
Other patient:
• first 14 days
• over 14 days
$317
$273
$533
$512
$597
$586
4.2.9 Specified grants
The following changes to specified grants will occur in 2013-14:
• Funding for Emergency Medihotels will be rolled into the WIES price.
• Trauma Appropriateness Payments will cease from 2013-14. Funding has been redistributed to relevant Health Services through their emergency department or urgent care centre funding streams based on average Trauma Appropriateness Payment activity over the past three years. Funding will be also be used to improve trauma education across the State.
4.3 Data and reporting changes
4.3.1 Revisions to the Victorian Hospital Admission Policy
The Victorian Hospital Admission Policy has been revised for 2013–14 to reflect the following:
• For criterion for admission Type E, the current requirement of four hours of continuous active management will remain in place. However, an additional component has been added to also permit admissions for patients transferred to a Short Stay Unit who have a documented clinical management plan or pathway.
• Same-day undifferentiated IV therapy may no longer be admitted as a Type C procedure. Same-day admission for IV infusion that has a code on the automatically admitted procedure list will still be eligible for admission under criteria for admission Type B.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 26

• Aligning the definition of qualified newborns to match the Commonwealth definition (in particular the criteria that the newborn is admitted to an intensive care facility in a hospital approved by the Commonwealth Minister for Health for the purpose of the provision of special care).
• Aligning criteria for admission with accommodation type where appropriate.
• Clarification that the criteria for admission are based on intent at time of admission.
• Admission time for patients admitted via the emergency department now begins when a patient departs from the emergency department.
The revised admission policy is in effect as of 1 July 2013. It can be downloaded at: http://www.health.vic.gov.au/hdss/
4.3.2 Hospital data collection changes
Victorian Admitted Episodes Dataset
Phase of care reporting for Palliative Care episodes has been clarified including two additional data elements for final phase of care. In addition, admission time has been amended for admission from non-admitted service to exclude time spent in non-admitted service from the admitted episode.
Victorian Integrated Non-Admitted Health Dataset
Seven data elements have had modifications and some codeset changes have been made to enhance data utility and improve data quality. The validation of many data elements collected at the ‘patient’ level has been linked to the date of contact in order to ensure code values are current.
Agency Information Management System
The S11 Subacute Non-Admitted Services form will collect aggregate data for non-admitted subacute activity that is in scope for Activity Based Funding.
Modifications have been made to the S2_305 form to remove information no longer required. The following forms have been discontinued:
• Waste Management
• S6 Dialysis Patients.
4.3.3 Health Service environmental management planning and reporting
The requirement to develop and implement a whole-of-organisation environmental management plan and report publicly on environmental performance is being expanded to all Public Health Services. This will continue to assist Public Health Services to manage their environmental impacts and increase operational efficiencies.
For more information on environmental programs and reporting go to: http://www.health.vic.gov.au/sustainability/programs.htm
4.3.4 Health Services and the Victorian Carers Recognition Act 2012
The Victorian Carers Recognition Act came into effect on 1 July 2012 and applies to organisations funded by government that are responsible for providing services affecting people in care relationships.
Health Services are now required to report in their annual report on their compliance with obligations under the Act. Further details are contained in Part two: Health operations and at www.dhs.vic.gov.au/carersact
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 27

5. Service performance Continuous improvement requires systems to be in place to collect, link, analyse, benchmark and report safety and quality data within and across health settings. Armed with this information or ‘business intelligence’, clinicians, consumers and policy makers can more effectively use this knowledge and evidence in decision making.
The government is committed to further developing public reporting of health service performance, outcomes and consumer experience. This includes ensuring that reporting measures are fit for purpose and, where appropriate, consistent across jurisdictions.
Key initiatives underway in 2013–14 are outlined below.
5.1 Health Service performance measures
5.1.1 Health care experience
The Victorian Patient Satisfaction Monitor will cease at the end of 2012–13, after the delivery of the final six-monthly results (January to June 2013 data) in October 2013 and the publication of the final annual report in December 2013. The Health Services’ final score from the Victorian Patient Satisfaction Monitor will be reported in the first two quarters of 2013–14.
The new healthcare experience survey will be rolled out in 2013–14. New targets will be developed once sufficient data to establish benchmarks has been obtained.
5.1.2 Health care worker immunisation — influenza
Health Services should take all reasonable steps to ensure staff members are protected against vaccine-preventable diseases. High coverage rates for immunisation in health care workers are essential to reduce the risk of transmission in healthcare settings. In response to this, the department has increased the health care workers influenza immunisation target to 75 per cent in 2013–14. The target will require 75 per cent of health service Category A and B healthcare worker's (as outlined in table C2.1 of the National Guidelines for the Prevention and Control of Infection in Health Care) who are permanently, temporarily or casually (i.e. bank staff) employed by the health service throughout the influenza period, to be immunised.
The National Guidelines are available at: http://www.nhmrc.gov.au/book/australian-guidelines-prevention-and-control-infection-healthcare-2010/c2-2-1-staff-health-scre
This will be reflected as a new indicator in the 2013–14 Statement of Priorities. Details about this indicator can be found in the Victorian Health Service performance monitoring framework 2013–14 business rules at: http://www.health.vic.gov.au/hospital-performance/
5.1.3 Hospital mortality measures
The department is developing three new performance measures for 2013–14 specific to in-hospital mortality for major provider, regional, sub-regional and local peer group Health Services. The mortality measures will be based on specifications developed by the Australian Commission on Safety and Quality in Healthcare in association with the Australian Institute of Health and Welfare, clinician groups and jurisdictions.
The mortality measures are designed to reveal where observed patient outcomes are within the expected range for peer hospitals, are significantly better than expected, or are potentially in need of improvement.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 28

The three in-hospital mortality measures are:
• hospital standardised mortality ratio
• death in low mortality diagnostic related groups
• death following treatment for the following conditions:
– acute myocardial infarction
– pneumonia
– stroke
– fractured neck of femur.
These performance measures are to be used by Health Services as a screening tool, rather than being assumed to be definitively diagnostic of poor quality and/or safety. The indicator is intended to signal that an issue may exist and that further detailed investigation is required by the Health Service. There will be no aggregate targets or benchmark rates for these performance measures.
5.2 Quality benchmarking Providing comparative data which enables Health Services to compare and benchmark their performance on a variety of quality measures beyond formal performance indicators is an important component of improving the quality of healthcare.
The department PRISM reporting tool provides information to Health Services on a range of quality indicators based on the core hospital-based outcome indicators specified by the Australian Commission in Safety and Quality.
In 2013–14 this information will be supplemented through an agreement with Doctor Foster Intelligence, a UK company part-owned by the UK Department of Health, which provides British health service providers with a range of tools to benchmark and monitor the quality and efficiency of service provision.
This agreement will encompass
• membership of the Doctor Foster Intelligence Global Comparators Club for the four largest Victorian tertiary Health Services (Alfred Health, Austin Health, Melbourne Health, Monash Health). They join thirty-eight other hospitals from across the United States, United Kingdom, Europe and Australia
• creation of a Victorian quality benchmarking group using the Doctor Foster Intelligence tool ‘Quality Investigator’ for ten Victorian Health Services (Barwon Health, Ballarat Health, Bendigo Health, Eastern Health, Goulburn Valley Health, Latrobe Regional Hospital, Northern Health, Peninsula Health, St Vincent’s Health and Western Health).
These products will provide the listed Victorian Health Services with an interactive tool to both benchmark and investigate and understand the reasons for their performance, on the quality measures of hospital standardised mortality ratios, hospital readmissions and relative length of stay.
Agreements will be put in place for one year and a review at the end of this period will determine whether the use of the Doctor Foster tools will continue and in what form.
5.3 National performance measures
5.3.1 National Emergency Access Target
The National Emergency Access Target (NEAT) was included in Health Services’ Statements of Priorities in 2012–13 in response to the National Partnership Agreement on Improving Hospital Services. Implementation of the NEAT has been staged incrementally, and will ultimately require 90 per cent of patients presenting to a public hospital emergency department either to physically leave the emergency department for admission to hospital, be referred to another hospital for treatment, or be discharged within four hours.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 29

The NEAT to be included in relevant Health Services’ Statements of Priorities for 2013–14 has increased to a target of 75 per cent, applying in 2013 and increasing to 81 per cent in 2014.
5.3.2 National Elective Surgery Target
The National Elective Surgery Targets (NEST) was included in Health Services’ Statements of Priorities in 2012–13 in response to the National Partnership Agreement on Improving Hospital Services.
Implementation has been incremental and requires a portion of Urgency Category 2 and 3 elective surgery patients to be treated within clinically recommended timeframes.
The NEST Part 1 to be included in relevant Health Services’ Statements of Priorities for 2013–14 are as follows:
• for Urgency Category 1, a target of 100 per cent will apply in the 2013 calendar year
• for Urgency Category 2 patients, a target of 80 per cent will apply in 2013 (calendar year) and will increase to 88 per cent in 2014 (calendar year)
• for Urgency Category 3 patients, a target of 94.5 per cent will apply in 2013 (calendar year) and will increase to 97 per cent in 2014 (calendar year).
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 30

6. Improving patient experience
In 2013–14, the focus of the department’s policy and program reforms is to ensure patients obtain the most effective form of care for their needs; they make informed decisions about that care; and their care is coordinated and timely.
The reforms consider the specific needs of various groups within our community to promote services that are targeted, responsive and culturally and gender appropriate. The health system needs to anticipate people’s needs by promoting health and managing risks for specific population groups.
The reforms also address system planning including: health service operation, clinical-effectiveness, cost-effectiveness and fiscal management.
Key initiatives underway in 2013–14 are outlined below.
6.1 My health care experience During 2013–14, Community and Health Services will be invited to participate in a range of strategies to improve patient’s health care experiences. The establishment of a new measurement and public reporting process under the Victorian Health Experience Measurement Instrument will include moving from continuous surveying of patient satisfaction to patient experience data for adult in-patients, maternity and adult emergency department patients. Note, the adult in-patient cohort includes sub-acute (rehabilitation) consumers. Importantly the department will commence paediatric and parent/guardian patient experience surveys for in-patients and emergency department service users. The adult in-patient survey is based on the UK's National Health Service's (NHS) survey and is inclusive of the National Research Corporation’s (US) in-patient patient experience questions. The adult maternity and emergency department patient experience surveys are based on the UK's NHS surveys for these health service groups. The paediatric and parent/guardian surveys are based on the Picker Europe surveys.
Under the Victorian Health Experience Measurement Instrument four new patient experience surveys are also being developed for the following cohorts:
• community health service clients (primarily includes non-GP primary health care clients) will be surveyed using a tool based on the NHS primary care survey
• specialist clinic patient experience data will be collected using a tool based on the NHS adult outpatient survey and the Picker Europe paediatric and parent/guardian outpatient survey
• public residential aged care residents and carers will be surveyed using a tool developed on the NHS primary care survey and Australian patient experience surveys.
These four new surveys will be conducted annually from 2014–15 over a staggered three month period.
All surveys are being developed with funded agencies, consumer and carer working groups; cognitively tested with consumers (and where appropriate carers); piloted through a sample of the appropriate funded agency; and will include verbatim comments thematically streamed from survey respondents. Importantly the results of all surveys will be publicly reported on a new Victorian Department of Health website.
6.2 Patient safety Health services have a responsibility to provide a safe environment for all people. Health Services should develop local policies and procedures to facilitate gender-sensitive and safe practice, to promote sexual safety and guide staff in preventing sexual activity and responding appropriately to allegations of sexual assault or harassment.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 31

The department has developed the following documents to provide guidance to services:
• service guideline for gender sensitivity and safety: http://docs.health.vic.gov.au/docs/doc/Service-Guideline-for-Gender-Sensitivity-and-Safety
• the chief psychiatrist guideline Promoting sexual safety, responding to sexual activity and managing allegations of sexual assault in adult acute inpatient units: http://docs.health.vic.gov.au/docs/doc/Promoting-sexual-safety-responding-to-sexual-activity-and-managing-allegations-of-sexual-assault-in-adult-acute-inpatient-units--June-2012
6.3 Infection control Effective prevention, monitoring and control of infection are an integral part of the quality, safety and clinical risk management operations of any Health Service.
Incorporated in the 2013-14 budget is a commitment of $5 million over two years for infection control. With this additional resource a statewide infection prevention and control strategy will be implemented aimed at improving patient outcomes and reducing the cost burden of health associated infections. The strategy will include a specific focus on hand hygiene and antimicrobial stewardship.
Health Service hand hygiene performance is measured against the national benchmark rate of 70 per cent. For submission criteria see: www.hha.org.au
Public reporting of individual hospital/Health Service hand hygiene compliance is via the My Hospitals website http://www.myhospitals.gov.au/
6.4 Services Connect Services Connect is a new initiative. Managed through the Department of Human Services, Services Connect aims to be Victoria’s integrated client service system to assist disadvantaged and vulnerable individuals and families, connecting them in a streamlined way with the full range of supports they require and managing delivery of support at the right level of intensity and case coordination.
Psychiatric disability rehabilitation support services and alcohol and drug services are within scope for Services Connect. The cooperation of clinical mental health services will also be required where Services Connect clients experience severe mental illness.
Pilot sites have been established in Geelong, South West Coast and Dandenong. The focus has been on testing intake, screening, client streaming and needs identification processes, particularly for the managed support component. A screening tool for drug treatment need, developed for the department by Turning Point, is being trialled in the pilot sites.
6.5 Acute and subacute services
6.5.1 Cardiac services
The department will work with Health Services, ambulance and community service providers to implement the government’s commitment of $21.9 million over four years to improve access to treatment for heart disease and stroke (cardiovascular disease), especially in rural and regional Victoria; reduce readmission and representation rates for these chronic diseases; and improve access to specialist advice. Key actions include:
• Heart Health – improve services and better outcomes for Victoria plan will be released during 2013-14 to guide this work
• access to urgent blood clot dissolving drugs pre-hospital for people experiencing a heart attack in rural and remote areas of Victoria
• establish specialist advice capacity
• improve triage and referral pathways for access to specialist cardiac surgical services
• new or strengthened models of care to improve outcomes of chronic heart failure.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 32
6.5.2 Emergency department care
A range of general and hospital-specific initiatives designed to improve and extend emergency access and improve the responsiveness of emergency care are being implemented across Victoria. The department continues to support hospital service improvement initiatives that include optimising alternatives to hospital admission, ensuring provision of earliest definitive treatment, using evidence to reduce variation in care, optimising acute patient flow and overall system coordination.
The timely transfer of ambulance patients in emergency departments is essential to delivering responsive and safe emergency care. Improving this process will positively impact patient outcomes, patient flow in the emergency departments and ambulance response times.
A key focus in 2013–14 will be to reinforce the responsibility of Health Services for the care of ambulance patients upon arrival in the emergency department. The department will work with Health Services and Ambulance Victoria to reduce variation in the ambulance patient transfer process, improve data collection and reporting and clearly define the escalation processes for use when delays in ambulance transfers occur.
Staff safety in Victorian Health Services
The government will invest $1.4 million in 2013–14 ($5.8 million over four years) to improve safety and security in Victorian Health Services, particularly in emergency departments. The majority of recommendations from the Drugs and Crime Prevention Committee’s Inquiry into Violence and Security Arrangements in Victorian Hospitals are targeted specifically to Health Services. Health Services are required to develop strategies to ensure they meet the recommendations arising from the inquiry, and report to the department on their progress at performance meetings and through written reports.
6.5.3 Maternity and neonatal services
In 2013–14 there will continue to be a focus on enhancing the sustainability of rural maternity and neonatal services through regional and sub-regional approaches to planning. This will be supported by the government’s commitments to improve rural obstetric data, support rural midwifery and provide postgraduate training for specialist rural general practitioners, with a focus on obstetrics.
The department, in collaboration with key stakeholders, will continue to explore a range of strategies to manage increasing demand for maternity and neonatal services. This will be supported by five additional neonatal intensive care unit cots in 2013–14.
The establishment of a formal arrangement between the Royal Women’s Hospital and Alfred Health will result in maternity and gynaecology services at Sandringham Hospital operating as a satellite service under the governance of the Royal Women’s Hospital. This will enable service expansion and an increase in the number of births undertaken at Sandringham Hospital. This example of voluntary collaboration is supported and will be monitored as a means on increasing service access, quality and clinical development.
In consultation with the Perinatal Services Advisory Committee, the department will explore options for the expansion of publicly funded homebirth in Victorian public Health Services. This follows the outcomes of an independent evaluation of the pilot program at Sunshine and Casey hospitals.
The Koori Maternity Services program will continue to work to improve access to culturally appropriate maternity care for Aboriginal women. Recent expansion of the program means there are now 14 sites across Victoria, 11 located in Aboriginal community controlled health organisations and three located in public Health Services. In 2013–14, the department will develop guidelines to support delivery of the Koori Maternity Services Program with a view to strengthening clinical governance arrangements and relationships between services.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 33

6.5.4 Renal health — kidney care
A new plan to support the continuing development of renal services, Renal directions — Better services and improved kidney health for Victorians was released in May 2013, and includes the following four strategic directions:
• promote healthy living and reduce renal risk factors
• improve early detection and management of kidney disease
• improve services for people with chronic kidney disease
• strengthen and sustain renal services.
In 2013–14, specific projects will focus on these strategic directions to deliver:
• improved capacity in primary care to recognise and manage early signs of kidney disease
• improved screening for kidney disease
• improved health literacy through provision of consistent and comprehensive information for people with deteriorating kidney function
• increased patient independence and improved health outcomes through continuing support for home dialysis as the first option for dialysis
• improved coordination of care through statewide implementation of consistent patient pathways for chronic kidney disease, kidney transplantation, dialysis and supportive patient care
• structural reform of renal services, through development and promulgation of a service capability framework
• promotion of workforce sustainability.
6.5.5 Advance care planning implementation strategy
In 2013–14 all Victorian funded Health Services are expected to implement formal advance care planning structures and processes that provide patients with opportunities to develop, review and have their expressed preferences for future treatment and care enacted if the person becomes unable to communicate or participate in decision making. Advance care planning is included as a key action area in Health Services’ Statement of Priorities for 2013–14.
6.5.6 Clinical Leadership Group on the Care of Older People in Hospital
In 2013–14 the Clinical Leadership Group on the Care of Older People in Hospital will focus specifically on achieving optimum clinical outcomes and reduce harm for older people in hospital by identifying and developing resources, tools and measures that support Health Services to meet the requirements of the National Safety and Quality Health Service Standards.
6.6 Mental Health Act Implementation The new Mental Health Act is anticipated to commence in 2014. The legislation intends to introduce supported decision making, increase safeguards to rights and encourage recovery-oriented service delivery and innovation. Health services will have to comply with new Act when this is introduced.
The department will be providing part-year funding to Health Services in 2013–14 (the amount will depend on when new legislation commences) for additional staff to meet the new and changed requirements in the legislation. Funding in following years will be recurrent to support implementation of new mental health legislation.
Funding of $3.1 million in 2013–14 will be provided as a specified one-off grant for the recruitment of mental health act implementation project officers to assist Health Services to prepare for new mental health legislation.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 34

6.7 Ambulance services
6.7.1 Emergency and non-emergency transport
In 2013–14 the department will continue to work with Ambulance Victoria to implement the government’s election commitments to improve ambulance services, including continued expansion of the paramedic workforce, capital and service upgrades. These developments will improve ambulance services for Victorians, particularly those residing in outer metropolitan and regional and rural areas.
Two new quality key performance indicators will be reported in 2013–14 to monitor the timely arrival of patients to stroke treatment units and cardiac arrest survival rates.
The department is also working with Ambulance Victoria to improve the interface with Health Services on a range of strategies to improve ambulance response times and patient transfers at public hospital emergency departments.
The department will continue to progress a range of ambulance reforms including a study of Victoria’s non-emergency transport sector and a review of Ambulance Victoria’s funding model.
The non-emergency transport sector study explores the scope and objectives of Victoria’s non-emergency patient transport services and its patient population and will provide advice on the most effective, efficient and sustainable means of providing and regulating non-emergency patient transport services to meet the needs of patients and the health sector.
The ambulance funding model project aims to provide a clear basis to price and fund ambulance services, as well as establish an appropriate and sustainable policy framework for setting and charging transport fees.
6.8 Ageing, aged care and supported residential services In 2013–14, the department will focus on the directions and work priorities for the Home and Community Care Program set out in the Home and Community Care Triennial Plan 2012–2015, which incorporates the national community care reform agenda.
The department will also:
• conduct a census of all Supported Residential Services (SRS) which will provide data about resident and staff profiles and the SRS sector in general, as well as specific detail about the profile of those SRS participating in the SRS Supporting Accommodation for Vulnerable Victorians Initiative
• develop the Victorian Senior Champions initiative to improve senior Victorians’ access to information, tools and programs that will help in reducing household cost pressures ($2 million over four years)
• work with the commissioner and the Ministerial Advisory Committee for Senior Victorians to develop a whole-of-government older persons action plan
• develop a Victorian dementia action plan informed by consultation with key stakeholders, service providers and interested and relevant private sector businesses. The action plan will identify gaps, potential growth and innovations in service types and delivery models and provide opportunities for new partnerships, potentially in public and private sectors.
6.8.1 Growing non-government provision of aged care beds
During 2013–14, the department will work with Health Services to implement the government’s December 2012 budget update initiative, which will seek to reallocate public sector residential aged care places to non-government providers in Melbourne.
6.9 Community health services In order to consolidate the initiatives of recent years and to further strengthen the work of the sector, the following initiatives will be introduced in 2013–14 and beyond:
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 35

• the community health integrated program guidelines to provide direction and improve consistency in planning, program design and service delivery as well as to clarify expectations for integrated service provision
• community health indicators to support continuous quality improvement and contribute to the evidence of the quality and impact of services provided by the sector
• improvements to the community health data set to assist with performance monitoring and support community health program management and continuous quality improvement
• collaborative research with universities and a range of programs (HARP, HACC and Community Health) to develop a response framework that assists health and community services to identify and respond appropriately to the health literacy needs of their local populations
• adoption of the 2012 Service Coordination Tool Templates
• a requirement for all community health services to participate in the People Matter survey
• the streamlining of processes for how community health services make Department of Veterans’ Affairs claims.
6.10 Primary Care Partnerships
6.10.1 Integrated planning
From July 2013 Primary Care Partnerships will follow a four-year planning cycle covering 2013-17. This alignment of Primary Care Partnerships, Community and Women’s Health and Municipal Public Health and Wellbeing planning cycles will facilitate greater integration in planning and avoidance of duplication of effort. Primary Care Partnerships requirements for 2013-17 are articulated in the Primary Care Partnerships Program Logic 2013-17.
The 2013-17 Program Logic consists of three key domains: early intervention and integrated care, consumer empowerment and prevention. This encompasses the system level work of Primary Care Partnerships including service coordination, e-health, integrated disease management, integrated health promotion and strategic partnership development. Further information can be found at: http://www.health.vic.gov.au/pch/commhealth/improvement.htm.
6.10.2 Service coordination
Service coordination aims to place consumers at the centre of service delivery, and ensure that they have access to the services they need, early intervention and coordinated care.
The focus of work in 2013–14 will include:
• implementation of the revised statewide common service coordination practice standards, with particular focus on the development of local agreements to progress inter-agency shared care planning
• continuation of 2012–13 work around a sustainable approach to workforce development for service coordination practice.
Major work will also include the implementation of the Service Coordination Tool Templates 2012. The 2012 review resulted in a number of improvements and changes including more support for managing accommodation and safety issues, drug, alcohol and tobacco issues and health and social needs. Amendments have been introduced to better support people with a disability, carers and Aboriginal and Torres Strait Islanders. A final change is the inclusion of a consumer-completed profile form to enable consumers to identify their key areas of need.
Further details are available at http://www.health.vic.gov.au/pcps/coordination/index.htm
The Statewide Service Coordination Survey will recommence in 2013. The survey will generate an analysis of individual organisations’ level of service coordination practice and benchmark them against regional and statewide results. This is an opportunity for services to identify areas that require further focus to ensure that they are delivering client-centred and coordinated care.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 36

6.11 Identification and management of vulnerable children
The Vulnerable babies, children and young people at risk of harm — Best practice framework for acute health services will be updated and expanded to include a broader range of services, including community and mental health services, and to reflect relevant recommendations from the Protecting Victoria’s Vulnerable Children Inquiry.
The department will also partner with key funded organisations to implement the Pathway to Good Health comprehensive health assessments for children in out-of-home care, in order to identify their health needs and enable them to access services. This has commenced with a rollout in the North West Metropolitan Region of Melbourne.
6.12 Health workforce
6.12.1 Clinical training
The Best Practice Clinical Learning Environment Framework will be rolled out to all 86 public Health Services from 2013–14 to 2016–17.
Health Services will be required to implement the Framework utilising the Best Practice Clinical Learning Environment tool. The Best Practice Clinical Learning Environment tool will facilitate future reporting against a number of key indicators that demonstrate and monitor commitment to the delivery of high quality clinical placements.
The department will also be conducting a scoping exercise to identify options towards creating a specific clinical training body for Victoria.
6.12.2 Credentialling and defining scope of clinical practice
The department has a suite of clinical engagement policies to support Health Services to facilitate safe, high-quality healthcare.
The Credentialling and defining the scope of clinical practice for medical practitioners in Victorian health services policy applies to all senior medical staff (including dentists) and eligible midwives appointed to a Victorian Health Service.
In 2013–14 the department is undertaking a review of the implementation of the Credentialling and defining the scope of clinical practice for medical practitioners in Victorian health services policy and the Partnering for performance framework.
Further information is available at: http://www.health.vic.gov.au/clinicalengagement/credentialling/index.htm
6.13 GLBTI Ministerial Advisory Committee
In 2013, the Gay, Lesbian, Bisexual, Transgender and Intersex (GLBTI) Health and Wellbeing Ministerial Advisory Committee was established to provide advice to the Victorian Minister for Health and Ageing and the Victorian Minister for Mental Health, incorporating the health, ageing and aged care, mental health and drug services portfolios.
The committee will advise on the delivery of election commitments related to the health of the GLBTI Victorians and appropriate health service and program responses for the GLBTI community.
6.14 Intersex decision making principles In 2013 the department published decision-making principles for the care of infants, children and adolescents with intersex conditions, which was developed in collaboration with leading experts in the field.
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 37

Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 38
The resource synthesises the advice of medical, human rights, ethical and legal experts and community advocates, and outlines best-practice principles to be applied to decision making. It is intended to assist decision makers to safeguard the best interests of the patient.
6.15 Tuberculosis Control Program In 2013–14 the department is proposing to transfer the Tuberculosis Control Program to an external service provider. This program provides direct patient case management to ensure compliance with treatment, as well as traditional public health measures such as contact tracing and screening to determine any spread of infection. An expression of interest process is proposed to take place with relevant Health Services in early 2013–14. It is proposed that the service will transfer to the successful service provider in early 2014.
6.16 Emergency Preparedness Clients and Services Policy The department works with funded organisations to prepare for, respond to and recover from emergencies that impact or affect funded organisations and the health of Victorians. The department has developed the Emergency Preparedness Clients and Services Policy — Summer 2012–13 to assist funded organisations to prepare for external hazards that may occur during the period of heightened risk associated with summer, thereby better protecting and enhancing the health and safety of clients.
This policy describes responsibilities and considerations for emergency planning and preparedness. It takes into account recommendations from the Victorian Bushfire Royal Commission and the Review of the 2010–11 Flood Warnings and Response and aligns with the overarching direction in Victoria’s emergency management arrangements requiring organisations to include an ‘all hazards approach’ in their planning.
This policy also encourages a consistent health sector-wide approach to emergency management planning which takes into consideration local conditions, resources and environmental circumstance.
Departmental services are defined as those that are:
• delivered from department-owned or managed facilities
• provided through departmental funding
• Supported Residential Services regulated by the department.
Further information is available at: http://www.dhs.vic.gov.au/facs/bdb/fmu/service-agreement/4.departmental-policies-procedures-and-initiatives/4.19-emergency-preparedness-clients-and-services-policy

Appendix 1: Summary of modelled budgets 2013–14
Table 4: Summary of modelled budgets 2012–13 and 2013–14
2012–13 expenditure budget 2013–14 expenditure budget
Acute health
services*
Ageing, aged & home care
Drug services
Mental health
Primary commu-
nity & dental health
Public health Total
Acute health
services*
Ageing, aged & home care
Drug services
Mental health
Primary commu-nity & dental health
Public health Total
Provider type $’000s $’000s $’000s $’000s $’000s $’000s $’000s $’000s $’000s $’000s $’000s $’000s $’000s $’000s
Health Services 6,722,756 193,170 33,559 758,475 46,795 17,302 7,772,057 7,120,944 196,840 34,823 782,146 47,959 17,644 8,200,354
Small Rural Health Services
195,995 56,256 - 322 11,089 - 263,661 201,566 57,101 - 331 11,331 - 270,329
Non-Government Organisations
50,248 223,021 56,275 89,212 22,539 116,161 557,456 53,040 234,010 65,711 92,355 23,253 120,508 588,877
Local Government Authorities
- 226,500 44 82 1,836 13,635 242,098 - 236,853 110 316 1,643 13,546 252,468
Community Health Centres
5,610 84,074 19,874 20,840 81,745 1,943 214,087 5,857 91,689 23,614 22,547 85,353 1,847 230,908
Health Consortiums
- 83 - - 1,250 - 1,332 - 85 - - 929 - 1,014
Other Organisations
390,269 5,946 - 40,569 136,373 - 573,156 411,214 6,103 - 41,369 190,297 - 648,984
Total State 7,364,878 789,049 109,753 909,500 301,627 149,041 9,623,848 7,792,620 822,682 124,257 939,063 360,766 153,544 10,192,933
*Includes the budget for Ambulance services
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 39

Appendix 2: Commonwealth funding reductions by Health Service
Table 5: Commonwealth reductions in promised funding 2013-14 to 2015-16
Commonwealth cuts to promised funding ($'000)
Health Service 2013-14 2014-15 2015-16 3 Year Total
Albury Wodonga Health 1,005 1,226 1,481 3,713
Alfred Health 7,185 8,766 10,584 26,536
Austin Health 6,185 7,546 9,111 22,842
Bairnsdale Regional Health Services 582 710 858 2,151
Ballarat Health Services 2,600 3,172 3,829 9,601
Barwon Health 4,484 5,471 6,606 16,561
Bass Coast Regional Health 340 415 501 1,257
Benalla & District Memorial Hospital 184 224 271 678
Bendigo Health Care Group 2,693 3,286 3,968 9,947
Castlemaine Health 221 270 326 817
Central Gippsland Health Service 586 715 864 2,165
Colac Area Health 232 282 341 855
Djerriwarrh Health Services 351 428 517 1,296
East Grampians Health Service 164 200 241 604
Eastern Health 7,689 9,381 11,326 28,396
Echuca Regional Health 371 452 546 1,369
Gippsland Southern Health Service 167 204 246 618
Goulburn Valley Health 1,701 2,075 2,506 6,282
Kyabram & District Health Services 133 163 196 492
Latrobe Regional Hospital 2,015 2,458 2,968 7,442
Maryborough District Health Service 157 192 232 582
Melbourne Health 7,680 9,369 11,313 28,362
Mercy Public Hospitals 2,749 3,354 4,049 10,151
Mildura Base Hospital 1,059 1,291 1,559 3,909
Northeast Health Wangaratta 1,011 1,233 1,489 3,733
Northern Health 3,661 4,467 5,393 13,522
Peninsula Health Care Network 4,471 5,455 6,586 16,512
Peter Maccallum Cancer Institute 1,166 1,423 1,718 4,306
Portland District Health 234 285 344 864
Royal Children's Hospital 3,306 4,033 4,870 12,209
Royal Victorian Eye & Ear Hospital 900 1,098 1,326 3,323
Royal Women's Hospital 1,873 2,285 2,759 6,918
South West Healthcare 1,296 1,581 1,909 4,786
Monash Health 12,412 15,144 18,285 45,841
St Vincent's Hospital 4,677 5,706 6,890 17,273
Stawell Regional Health 153 186 225 564
Swan Hill District Health 344 420 507 1,270
West Gippsland Health Care Group 616 752 908 2,277
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 40

Commonwealth cuts to promised funding ($'000)
Health Service 2013-14 2014-15 2015-16 3 Year Total
Western District Health Service 395 483 583 1,461
Western Health 6,020 7,345 8,868 22,233
Wimmera Health Care Group 547 667 806 2,020
Alexandra District Hospital 70 85 103 257
Alpine Health 133 162 195 489
Beaufort & Skipton Health Service 52 63 76 191
Beechworth Health Service 88 107 129 324
Boort District Health 27 33 40 100
Calvary Health Care Bethlehem 312 381 460 1,154
Casterton Memorial Hospital 46 56 67 169
Cobram District Health 72 88 106 266
Cohuna District Hospital 61 75 91 227
Dunmunkle Health Services 13 16 19 47
East Wimmera Health Service 122 149 180 452
Edenhope & District Memorial Hospital 44 53 64 162
Heathcote Health 25 31 37 94
Hepburn Health Service 98 120 144 362
Hesse Rural Health Service 24 29 35 88
Heywood Rural Health 29 35 43 107
Inglewood & Districts Health Service 22 27 33 83
Kerang & District Health 76 93 112 281
Kilmore & District Hospital 127 155 187 470
Kooweerup Regional Health Services 61 75 90 226
Kyneton District Health Service 107 131 158 395
Lorne Community Hospital 28 34 41 104
Maldon Hospital 14 17 21 53
Mallee Track Health & Community Service 46 56 67 168
Mansfield District Hospital. 74 90 109 274
Moyne Health Services 43 53 64 160
Nathalia District Hospital 25 31 38 94
Numurkah District Health Service 79 97 117 293
Omeo District Health 20 25 30 76
Orbost Regional Health 74 90 109 273
Otway Health & Community Services 31 38 46 115
Robinvale District Health Services 67 82 99 247
Rochester & Elmore District Health Service 59 72 87 217
Rural Northwest Health 101 124 149 374
Seymour District Memorial Hospital 145 177 214 536
South Gippsland Hospital 61 75 90 227
Tallangatta Health Service 47 57 69 174
Terang & Mortlake Health Service 65 79 95 238
Timboon and District Healthcare Service 45 55 66 167
Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 41

Victorian health policy and funding guidelines 2013–14 — Part one: Key changes and new initiatives, page 42
Commonwealth cuts to promised funding ($'000)
Health Service 2013-14 2014-15 2015-16 3 Year Total
Upper Murray Health & Community Services 45 55 67 168
West Wimmera Health Service 157 191 231 578
Yarram & District Health Service 62 76 92 230
Yarrawonga District Health Service 92 112 35 338
Yea & District Memorial Hospital 29 35 42 106
Victorian Institute Of Forensic Mental Health 574 701 846 2,121
Public Health Adjustment 2,330 3,030 3,840 9,200
Total 99,540 121,630 147,040 368,210
Notes:
Calculations based on the reduction in National Health Reform funding to Victoria as outlined in the
Commonwealth Government’s 2013-14 Mid-Year Economic and Fiscal Outlook
Albury Wodonga Health excludes the NSW funding contribution. Health Service allocation of the Commonwealth cuts to promised funding has been nominally determined
using a pro-rata allocation based on budgets published in the Policy and Funding Guidelines in July
2012.