video assisted thoracic surgery api tripura
TRANSCRIPT

8/14/2019 Video Assisted Thoracic Surgery API Tripura
http://slidepdf.com/reader/full/video-assisted-thoracic-surgery-api-tripura 1/11
Video Assisted Thoracic Surgery (VATS)
Role in Pulmonary Medicine.
Dr L.M.Darlong.MS(AIIMS)
Fellow Thoracic Surg (KUMC Seoul)
. Key Words: Video Assisted Thoracic Surgery (VATS), Thoracoscopy,
Minimal access Surgery.
Introduction;
Medicine is both science and art and sometimes there are more than one way to solve the problem. Ever since the evolution of the endoscopy the medical profession has tried to
duplicate and perform surgical skills which had been done in the traditional open waysand thus reduce the suffering of the patients. In pulmonary medicine and thoracic surgery
this has resulted in the evolution of various techniques as we know today as medical
thoracoscopy, Video assisted thoracic surgery (VATS) minimal access surgery. This is
unlike the open thoracic surgery where for any procedure ranging from diagnostic totherapeutic a liberal skin incision had to be given across the chest wall between the ribs
and the ribs spread apart for access to organ site and not to forget the associated
postoperative morbidity, pain and ugly scar. (Fig 1, 2).
Medical thoracoscopy which was first practiced by jacobeus way back in 1913 for the
treatment of pulmonary Koch when he introduced the cystoscope into the pleural cavityto lyse adhesion for facilitating pneumothorax is done under local anesthesia withsedation. 1 Medical thoracoscopy is mainly used as a diagnostic tool for the disease of
pleura.
This is unlike VATS which is a minimal access procedure which is done under generalanaesthesia for diagnostic as well as therapeutic indications. The therapeutic indication of
VATS has not limited itself to the disease of lung pleura and mediastinum but is also
being increasingly used for dorsal spine, esophagus and cardiac surgery since the
development of better video and endoscopic imaging system along with endostapplingdevices since the 1990s. Ever since the introduction of endoscopic surgery the dictum
“big surgeons big incision” is slowly giving way to “no scopy no scope” with a limited
small incision.

8/14/2019 Video Assisted Thoracic Surgery API Tripura
http://slidepdf.com/reader/full/video-assisted-thoracic-surgery-api-tripura 2/11
Fig 1 Thoracotomy wound
Fig 2. VATS wound
Indications of Video assisted thoracic surgery:
The various indications of VATS can be briefly classified as Diagnostic and Therapeutic.VATS has been mainly utilized by thoracic surgeons for pulmonary and mediastinal
diseases however it has also been used for disorders of the spine by spine surgeons and ina few centres for cardiac surgery. The various indications of VATS are shown in table 1.

8/14/2019 Video Assisted Thoracic Surgery API Tripura
http://slidepdf.com/reader/full/video-assisted-thoracic-surgery-api-tripura 3/11
Table 1.
LUNG
PARENCHYMA
PLEURA MEDIASTINUM ESOPHAGUS
/SPINE
Biopsy Biopsy Lymph node biopsy Benign tumor
Bulla/bleb excision Drainage Cyst/mass excision Myotomy
Wedge ressection /
Metastatectomy
Pleurectomy Sympathectomy Diverticulectomy
Segmentectomy Pleurodesis Thymectomy Esophagectomy
Lobectomy Decortication PDA ligation Spine abcess
drainage / Fixation
Pneumonectomy Drain empyema Pericardial window
VATS Procedure:The VATS procedure is basically an access procedure with all the surgical techniquesremaining the same as in open surgery and only the access route being smaller and
operative field viewed on a monitor. The procedure is done under General anesthesia in
the lateral decubitis , supine or prone position based on the area of interest. A doublelumen tube endotracheal tube is required so as to collapse the ipsilateral lung on the area
of interest and thus provide a working space for instrumentation and coduct of surgery.
Some centres use CO2 insufflation to achieve pneumothorax on the side of surgery to
obtain working space with the disadvantage of possible air leak during instrument
withdrawl and loss of space and the need for specific endoscopic instruments. However in our center the preferred approach is to collapse the ipsilateral lung with a double lumen
endotracheal tube (Fig 3). This is crucial as most of the instruments used are long versionof open surgical instruments (Fig 4) like sponge holding forceps ,long scissors,
disposable suctioncannula etc. It is always necessary to have a set of open thoracotomy
instruments aside in case of the need for conversion to open thoracotomy.

8/14/2019 Video Assisted Thoracic Surgery API Tripura
http://slidepdf.com/reader/full/video-assisted-thoracic-surgery-api-tripura 4/11
As in any procedure VATS also has its contraindication. The only absolute
contraindication 2 is the patients inability to tolerate single lung ventilation and
hemodynamic instability. The other relative contraindications are :1. Pleural symphysis.
2. Previous history of thoracotomy.
3. Tumor beyond a certain size or stage.
Fig 3. Double lumen tube with tube insitu at trachea and left main bronchus.
Fig 4. Instruments used in VATS.
Diagnostic indications in pulmonogy:

8/14/2019 Video Assisted Thoracic Surgery API Tripura
http://slidepdf.com/reader/full/video-assisted-thoracic-surgery-api-tripura 5/11
PLEURAL DISEASE
For pleural effusions, thoracentesis is the first line of management. A biochemical,
cytological and microbiological analysis of fluid is done and further studies depending onwhether the fluid is an exudate or a transudate. Exudates can be infectious and non-
infectious and require further investigation. A combination of thoracoscopy and lung
//pleural
biopsy usually reaches the final diagnosis where others have failed. Malignant pleural effusions, primary or metastatic, are particularly suited for diagnosis by
thoracoscopy, as the disease is focal rather than uniform and blind biopsies tend to have a
low yield.3-5
INTERSTITIAL LUNG DISEASE
Despite diagnostic efforts by sputum analysis, bronchoscopy, bronchoalveolar lavage,
and transbronchial biopsy, some parenchymal infiltrates remain idiopathic. In suchinstances surgical biopsy is indicated, the thoracoscopic approach being generally
superior to the open techniques.4-6
PULMONARY NODULESSolitary pulmonary nodules can be malignant in up to a third of cases and tissue
diagnosis is therefore a mandatory end point. Percutaneous biopsy aided by variouslocalisation techniques still produces a too high rate of false negative results. The data of
Calhoun et al showed that after a fine needle percutaneous biopsy a specific diagnosis of
benignity is reached in less than 5% of cases.7 It follows logically that surgical excision is
a safer option, with thoracoscopy ideally suited for nodules in the outer third of the parenchyma. Nodules that appear to be seated deeper in the parenchyma on imaging can
actually be very close to the surface in a fissure and these too are readily accessible. 8 In
cases where frozen section histology of a thoracoscopically extracted specimen confirmsmalignancy, the surgeon can proceed to excision via thoracoscopy or thoracotomy.
MEDIASTINAL MASSESlymph node mass in the Paratracheal and subcarinal areas are accessible by cervical
mediastinoscopy, however masses and lymph nodes situated in the aortopulmonary
window and pulmonary hila are not accessible by mediastinoscopy and anterior mediastinotomy (the Chamberlain procedure) was the standard in such cases. VATS has
made this areas accessible and is superior to mediastinotomy, in that it is less invasive and
provides access to other areas too, such as the posterior mediastinum. Routine
prethoracotomy mediastinal exploration with thoracoscopy in patients with confirmedlung cancer is advocated by some groups, especially if multifocal lesions are suspected or
to assess invasion of chest wall or other adjacent structures. This policy reduces the
number of "open and close" thoracotomies to a minimum.8
Therapeutic procedures in pulmonology:
PLEURAL DISEASE
Benign effusions usually disappear when the underlying disease is successfully dealt
with. Malignant effusions are by definition associated with unresectable disease (T4 inthe tumour, node, metastases (TNM) classification). If the lung retains the capacity to re-

8/14/2019 Video Assisted Thoracic Surgery API Tripura
http://slidepdf.com/reader/full/video-assisted-thoracic-surgery-api-tripura 6/11
expand, tube thoracostomy and chemical pleurodesis with tetracycline / Talc can be
sufficient. If the diagnosis is established by thoracoscopy, additional options include
mechanical abrasion, instillation of talc or other sclerosants, and pleurectomy.4 Themagnitude of the latter makes it unsuitable for this group of debilitated patients. In more
advanced disease the effusion recurs or the lung becomes trapped. The same measures of
tube
thoracostomy, or thoracoscopy in better risk cases, can be reapplied
but the chancesof success are less as the disease progresses.
VATS is most useful in the intermediate phase of empyema, before the lung is encased in
a thick fibrous peel that would require decortication.9 In this fibropurulent phase tubedrainage is unsuccessful if loculations are present, and thoracoscopic drainage and
decortication is indicated. (Fig 5,6)
Fig 5 Thickened pleura in VATS Decortication.
Fig 6 Fibrinopurulent phase with loculation.
8/14/2019 Video Assisted Thoracic Surgery API Tripura
http://slidepdf.com/reader/full/video-assisted-thoracic-surgery-api-tripura 7/11
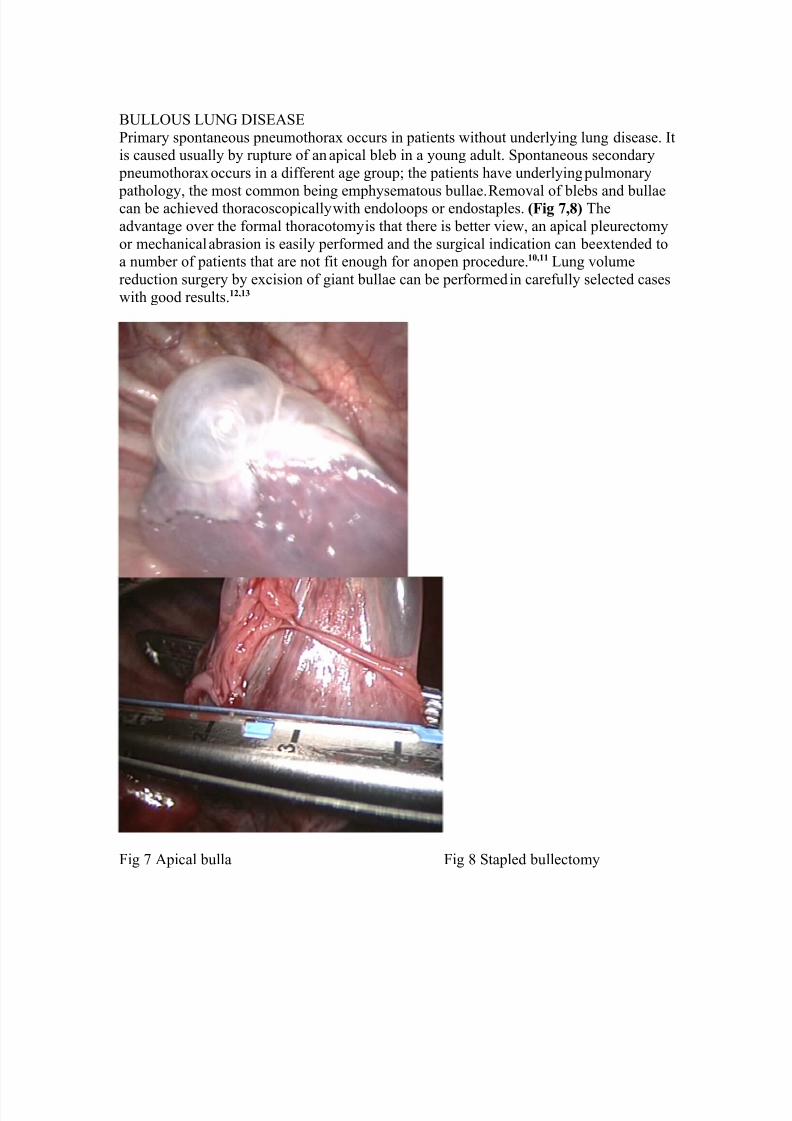
BULLOUS LUNG DISEASE
Primary spontaneous pneumothorax occurs in patients without underlying lung disease. Itis caused usually by rupture of an apical bleb in a young adult. Spontaneous secondary
pneumothorax occurs in a different age group; the patients have underlying pulmonary
pathology, the most common being emphysematous bullae.
Removal of blebs and bullaecan be achieved thoracoscopically with endoloops or endostaples. (Fig 7,8) The
advantage over the formal thoracotomy is that there is better view, an apical pleurectomy
or mechanical abrasion is easily performed and the surgical indication can be extended toa number of patients that are not fit enough for an open procedure.10,11 Lung volume
reduction surgery by excision of giant bullae can be performed in carefully selected cases
with good results.12,13
Fig 7 Apical bulla Fig 8 Stapled bullectomy

8/14/2019 Video Assisted Thoracic Surgery API Tripura
http://slidepdf.com/reader/full/video-assisted-thoracic-surgery-api-tripura 8/11
LUNG RESECTION
The principal roles of VATS in lung cancer are diagnosis of the indeterminate pulmonary
nodule, staging of the pleura and mediastinum, wedge resection of early tumours indebilitated patients, lobectomy/pneumonectomy, and treatment of malignant pleural
effusion.14
Some of the above indications have already been discussed. The data from the LungCancer Study Group showed that for stage I lung cancer there is no survival benefit of
lobectomy over non-anatomical wedge resection.15 However, there is a significantly
higher rate of local recurrence after wedge resection, so this procedure is reserved for patients who are too debilitated to tolerate a formal oncological resection. Resection of
solitary metastases is a good indication for VATS, but excision of multiple metastases as,
for example, those of osteogenic sarcoma is best accomplished via a conventional
thoracotomy that allows palpatory detection of small nodules.Lobectomy and pneumonectomy can now be performed thoracoscopically, with the
possibility of excising the ipsilateral lymph notes as necessary. Ideally the tumour should
be small, located peripherally, preferentially in the lower lobes.14 It cannot be
overemphasised that there should be no compromise
in the extent of resection by theminimal access route and a conversion to thoracotomy should be considered sound
judgment and not failure of VATS in case adequate clearance of tumour and lymph nodescannot be achieved.14
MEDIASTINUM
It has already been mentioned that VATS is complementary to cervical mediastinoscopyin assessing lymphadenopathy in the mediastinum. Mediastinal masses can be removed
thoracoscopically from different locations in the mediastinum.16 Likewise, thymic
tumours can be excised thoracoscopically,
Conclusion:
The advantage of VATS over thoracotomy lies in the reduction of both acute and chronic
postoperative pain with improved chest physiotherapy and recovery, together with earlier return to normal activity and better cosmesis. (Fig 9,10) In terms of costs, VATS is
expensive but several studies demonstrated a reduced high dependency and hospital stay
which probably neutralise the expense.17 Table 2 shows a comparative chart of thenormally asked questions when comparing VATS with Thoracotomy. Adequate exposure
and a long learning curve is essential before performing on complex procedures. The
complications of thoracoscopy are by and large related to the surgical complications of the treated condition and are similar to those that follow conventional open operations.
The necessity to convert
a thoracoscopic procedure to an open one usually arises fromone of the following: significant adhesions, uncontrollable bleeding, inadequate view,inability to obtain single lung ventilation, removal of large lesions, and inability to
perform an adequate excision.2Conversion thus should be taken as a wise decision and
not a failure as the ultimate aim is a completion of the procedure with no mortality and
minimal morbidity.It can be seen from this overview that most thoracic operations can betackled in this day and age thoracoscopically. The available studies suggest that simple
parenchymal sampling, wedge resection, and pneumothorax surgery are best performed

8/14/2019 Video Assisted Thoracic Surgery API Tripura
http://slidepdf.com/reader/full/video-assisted-thoracic-surgery-api-tripura 9/11
thoracoscopically. Selected cases of lung volume reduction are also suitable for VATS.
More controversial is the role of VATS in cancer resection, but the minimal access route
and conventional techniques should be seen as complimentary and not opposed. Theminimal access approach is best reserved for peripheral early tumours, while the more
advanced and central lesions will be managed by open resection. The debate over patient
outcomes and cost effectiveness will
continue until the practice becomes morestandardized and thoracoscopic surgery widely accessible.
Table 2 18
Questions VATS ThoracotomySize of incision 1 inch 10-14 inch
Average hospital stay 2 days 10-12 days
Return to work 7-10 days 6-8 weeks
Fig 9 VATS scar.

8/14/2019 Video Assisted Thoracic Surgery API Tripura
http://slidepdf.com/reader/full/video-assisted-thoracic-surgery-api-tripura 10/11
Fig 10 Open thoracotomy scar.
References:
1. Loddenkemper R. Thoracoscopy state of the art. Eur Respir J 1998;11:213-221
2. Dieter RAJ, Kuzycz GB. Complications and contraindications of thoracoscopy. Int Surg 1997;82:232-239
3. Boutin C, Astoul PH, Seitz B. The role of thoracoscopy in the evaluation andmanagement of pleural effusions. Lung 1990;168:S1113-S1121.
4. Reddy LC, Monson JR, Cowen ME. Role of video thoracoscopy in managementof malignant pleural effusion. Int Surg 1996;81:325-326
5. Ravini M, Ferraro G, Barbieri B, et al . Changing strategies of lung biopsies in
diffuse lung diseases: the impact of video-assisted thoracoscopy. Eur Respir J
1998;11:99-1037.
6. Carnochan FM, Walker WS, Cameron EWJ. Efficacy of video-assisted
thoracoscopic lung biopsy: a historical comparison with open lung biopsy.Thorax 1994;49:361-363
7. Calhoun P, Feldman PS, Armstrong P, et al . The clinical outcome of needleaspirations of the lung when cancer is not diagnosed. Ann Thorac Surg
1985;41:592-596
8. Yim AP. Routine video-assisted thoracoscopy prior to thoracotomy. Chest
1996;109:1099-1100
9. Silen ML, Naunheim KS. Thoracoscopic approach to the management of
empyema thoracis. Indications and results. Chest Surg Clin N Am 1996;6:491-499
10. Dumont P, Diemont F, Massard G, et al . Does a thoracoscopic approach for
surgical treatment of spontaneous pneumothorax represent progress? Eur J
Cardiothorac Surg 1997;11:27-31
11. Waller DA. Video-assisted thoracoscopic surgery (VATS) in the management of
spontaneous pneumothorax. Thorax 1997;52:307-308
12. Menconi GF, Melfi FM, Mussi A, et al . Treatment by VATS of giant bullous
emphysema: results. Eur J Cardiothorac Surg 1998;13:66-70.

8/14/2019 Video Assisted Thoracic Surgery API Tripura
http://slidepdf.com/reader/full/video-assisted-thoracic-surgery-api-tripura 11/11
13. Weder W, Schmid RA, Russi EW. Thoracoscopic lung volume reduction surgery
for emphysema. Int Surg 1996;81:229-23420.
14. Landreneau RJ, Mack MJ, Dowling RD, et al . The role of thoracoscopy in lung
cancer management. Chest 1998;113:S6-12
15. Thomas P, Rubinstein L, the Lung Cancer Study Group. Cancer recurrence after
resection: T1N0 non-small cell lung cancer. Ann Thorac Surg 1990;59:242-247.
16. Rieger R, Schrenk P, Woisetschlager R, et al . Videothoracoscopy for the
management of mediastinal mass lesions. Surg Endosc 1996;10:715-717
17. Hazelrigg SR, Nunchuck SK, Landreneau RJ, et al . Cost analysis for
thoracoscopy: thoracoscopic wedge resection. Ann Thorac Surg 1993;56:633-635
18. www.thoracicgroup.com