vincenzo ficarra 1,2,3 - over group provider ecm · vincenzo ficarra1,2,3 1director department of...
TRANSCRIPT

Vincenzo Ficarra1,2,3
1Di t D t t f U l U i it f Udi It l1Director Department of Urology – University of Udine, Italy2Associate Editor BJU International33Scientific Director OLV Robotic Surgery Institute, Aalst, Belgium
Best papers on kidney cancerBest papers on kidney cancer
Vincenzo Ficarra1,2,3
1Director Department of Urology – University of Udine, Italy2A i t Edit BJU I t ti l2Associate Editor BJU International3Scientific Director OLV Robotic Surgery Institute, Aalst, Belgium

Urological topicsUrological topics
• Renal tumour biopsy
• Active surveillance and ablative therapies
• Nephrometry systems and Partial Nephrectomy
• Adjuvant therapies
• Cyteruductive nephrectomy
• Treatment for single metastasis

International GuidelinesInternational Guidelines

Renal Mass biopsy stratificationp y
Rahbar H et al J Urol 2014; 192: 1337-1342

Multi institutional multicenter prospective non• Multi-institutional, multicenter prospective, non-randomized study
• Period 2009 to 2014: 497 patients with solid renal masses ≤ 4 0 cmmasses ≤ 4.0 cm
• Intervention: Primary intervention (PI) or ActiveIntervention: Primary intervention (PI) or Active Surveillance (AS)
Pierorazio PM et al Eur Urol 2015; (in press)

Pierorazio PM et al Eur Urol 2015; (in press)

Pierorazio PM et al Eur Urol 2015; (in press)

Pierorazio PM et al Eur Urol 2015; (in press)

Pierorazio PM et al Eur Urol 2015; (in press)

AS Vs PIAS Vs PIMedian follow-up: 2.1 yr (IQR 0.9–3.8);161 (32%) patients had follow up > 3 yr161 (32%) patients had follow-up > 3 yr
Pierorazio PM et al Eur Urol 2015; (in press)

AS V PI l iAS Vs PI: conclusions
• In a well-selected cohort with up to 5 yr of prospective follow-up, AS was not inferior to PI
• Discussion of active surveillance should becomepart of the standard discussion for management of small renal masses
Pierorazio PM et al Eur Urol 2015; (in press)

Zargar H et al Eur Urol 2015; (in press)

C bl ti f ll lCryoablation for small renal masses
S l ti• Selection: - for patients with contraindications for extirpative approach s ch as medical comorbidities pre io sapproach such as medical comorbidities, previous renal procedures, or purely due to patient choice
• Further data are needed before CA utility in general patient populationpatient population
Zargar H et al Eur Urol 2015; (in press)
Cryoablation for small renal massesCryoablation for small renal masses
• Complications: - range from 7 8% to 20% with most complicationsrange from 7.8% to 20% with most complications being minor
• Functional results: - minimal decline in renal function postoperativelyp p y
• Oncologic results: g- the rate of recurrence-free survival for CA is lower than extirpative surgery.
Zargar H et al Eur Urol 2015; (in press)

I t ti l G id liInternational Guidelines
• In the elderly and/or comorbid patients with small renal masses and limited life expectancy activerenal masses and limited life expectancy, active surveillance, radiofrequency ablation and cryotherapy can be offered (EAU 2015)cryotherapy can be offered (EAU, 2015)
• Active surveillance and ablative techniques such asActive surveillance and ablative techniques such as cryo- or radiofrequency ablation are alternative strategies for selected patients particularly thestrategies for selected patients, particularly the elderly and those with competing health risks (NCCN, 2015)(NCCN, 2015)

Surgical treatments for localized RCCgClinical NCCN, 2015 EAU, 2015stage
, ,
T1a • PN preferred • PN is recommended in patients ith T1 t(≤4 cm)
• RN if PN not technically feasible, or central location
with pT1a tumors
T1b • PN or RN (whenever PN
(4-7 cm) technically not feasible) • PN should be preferred over RN in patients with T1b tumours when technically feasibley
T2 • Radical Nephrectomy • Radical Nephrectomy

The impact of nephrometry scores on counseling patientsscores on counseling patients and outcome reports after partial nephrectomy
Vincenzo Ficarra1Director Department of Urology – University of Udine, Italy
2Associate Editor BJU International

R.E.N.A.L. Nephrometry scorep y
Kutikov A. et al. J Urol 2009; 182, 844-853,

1 31 3 12
2 21
2
1 1
2
Polar location Exophytic rate Rim location
2 1
2
2
2
12
2
Renal sinus involvement UCS involvement Tumour size
11 3
Renal sinus involvement UCS involvement Tumour size
Ficarra V. et al. Eur Urol 2009; 56, 786-793,

C index systemy
• C-index provides a single score based entirely on tumor size and tumor depth.
• C-index does not communicate geographic location data, and is therefore limited compared to the categorical systems
• To provide information about its i it t th kid tproximity to the kidney center.
Simmons M. et al J Urol 2010; 183: 1708-1713

Reference Cases Complications Ischemia time Blood loss
Hayn 2011 141 LPN NS + +R Hayn, 2011 141 LPN NS + +Simhan, 2011 216 OPN
174 RPN+ + +
Hew 2011 134 PN + + NA
R.E. Hew, 2011 134 PN + + NA
Mufarrij, 2011 92 RPN NS NS NSBruner, 2011 155 PN + NA NAOkhunov, 2011 101 LPN NS + NS
N.A O u o , 0 101 LPN NS + NS
Kruck, 2012 81 LPN NS NS +Lavallée, 2012 78 OPN NA + NABylund, 2012 124 LPN NA + +
A.L. y
25 RPN13 OPN
Png, 2012 83 RPN NS + NSS Stroup, 2012 153 OPN100 LPN31 RPN
NS NA NASC
Mayer, 2012 55 RPN12 LPN
NA + NS
Altunrende, 2012 181 RPN NA NS NA
OR
Liu, 2013 128 LPN53 RPN
+ + NS
Long, 2013 159 OPN NS NS NS
RE
g 59 O18 LPN
S S S
modified from Klatte T, Ficarra V et al Eur Urol (in press)

PADUA scoreReference Cases Complications Ischemia time Blood loss
Waldert , 2010 186 OPN54 LPN
+ + NA
Hew 2011 134 PN + + NAHew, 2011 134 PN + + NA
Okhunov, 2011 101 LPN NS + NSKruck , 2012] 81 LPN + NS +Lavallée, 2012 78 OPN NA + NABylund, 2012 124 LPN
25 RPNNA + NS
13 OPNFicarra , 2012 347 RPN + + +Kong, 2012 136 OPN + + NS
59 LPNMottrie, 2012 62 RPN + + +
Tyritzis, 2012 74 OPN + NA NAMinervini, 2013 244 OPN + NA NA
modified from Klatte T, Ficarra V et al Eur Urol (in press)

C index systemy
Reference Cases Complications Ischemia time Blood loss
Okhunov, 2011 101 LPN NS + NS
Lavallée, 2012 78 OPN NA NS NA
Bylund, 2012 124 LPN25 RPN
NA + NS
13 OPN
modified from Klatte T, Ficarra V et al Eur Urol (in press)

Leslie S. et al. Eur Urol 2014; 66: 884-893

Renal Tumor Contact Surface Area
Leslie S. et al. Eur Urol 2014; 66: 884-893

ConclusionsConclusionsN h t ff ti t l t di t• Nephrometry scores are effective tools to predict perioperative outcomes in patients who underwent PNPN
• These classifications can be considered as useful• These classifications can be considered as useful tools to improve patients counseling and selection for PNfor PN
• Nephrometry scores could allow a realNephrometry scores could allow a real comparison between the tumor characteristics of the different seriesof the different series

Scosyrev E et al. Eur Urol 2014; 65: 372-377

PN Vs RN: renal functionPN Vs RN: renal function
Scosyrev E et al. Eur Urol 2014; 65: 372-377

PN Vs RN: renal functionPN Vs RN: renal function
Scosyrev E et al. Eur Urol 2014; 65: 372-377

PN Vs RN: renal functionPN Vs RN: renal function
Scosyrev E et al. Eur Urol 2014; 65: 372-377

PN Vs RN: renal functionPN Vs RN: renal function
• Compared with RN, NSS substantially reduced the incidence of at least moderate renalthe incidence of at least moderate renal dysfunction(eGFR < 60), although with available follow up the incidence of advanced kidneyfollow-up the incidence of advanced kidney disease (eGFR < 30) was relatively similar in the two treatment arms and the incidence of kidneytwo treatment arms, and the incidence of kidney failure (eGFR < 15) was nearly identical.
• The beneficial impact of NSS on eGFR did not result in improved survival in this study populationresult in improved survival in this study population
Scosyrev E et al. Eur Urol 2014; 65: 372-377

• 113 PN and 59 RN
• Function and parenchymal mass specifically in the operated and contralateral kidneys.
• renal scans to provide split renal function preoperatively and postoperativelypreoperatively and postoperatively.
• All studies were done less than 2 monthsAll studies were done less than 2 months preoperatively and 4 to 12 months postoperatively
Takagi T. et al. J Urol 2015; 192: 16121619
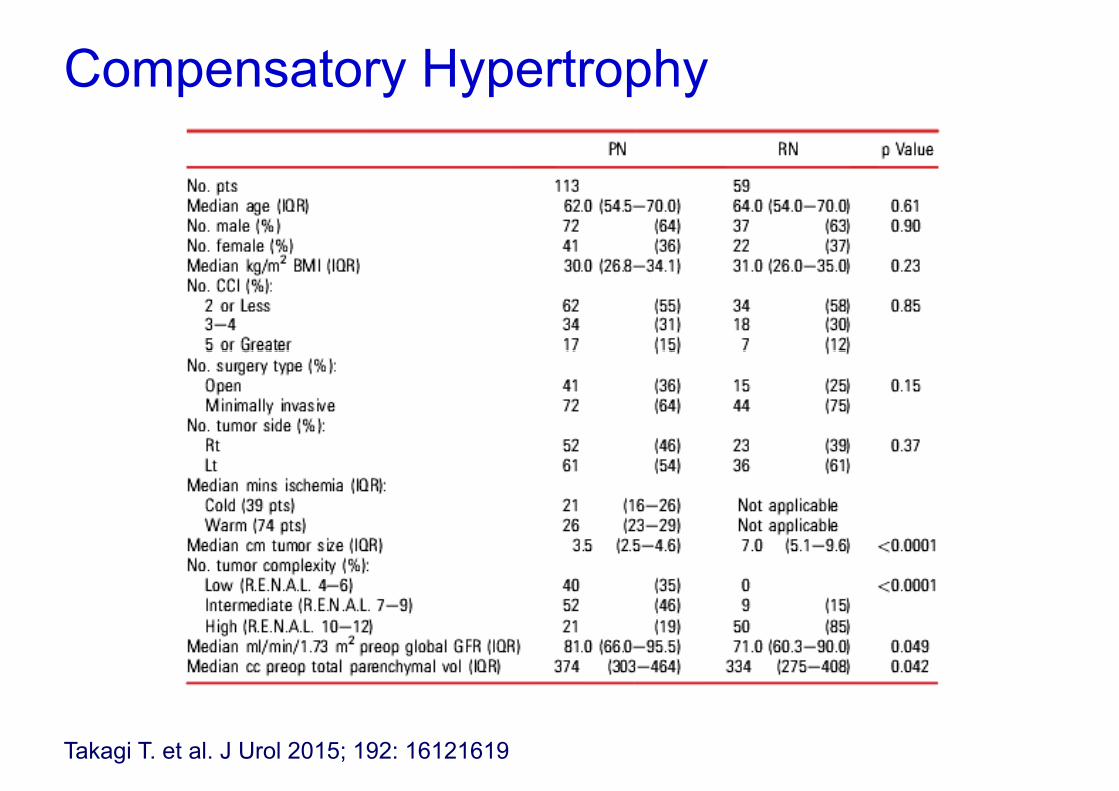
Compensatory Hypertrophyp y yp p y
Takagi T. et al. J Urol 2015; 192: 16121619

Compensatory Hypertrophyp y yp p y
Takagi T. et al. J Urol 2015; 192: 16121619

• 973 patients operated at 9 academic institutions were retrospectively analyzedinstitutions were retrospectively analyzed
• Glomerular filtration rate (GFR) before andGlomerular filtration rate (GFR) before and after surgery was calculated with the abbreviated Modifi cation of the Diet in Renalabbreviated Modifi cation of the Diet in Renal Disease equation.
Pignot G et al Urol Oncol 2014; 32: 1024 1030Pignot G. et al. Urol Oncol 2014; 32: 1024-1030

Preserving renal function: PN Vs RNg
Pignot G. et al. Urol Oncol 2014; 32: 1024-1030

Preserving renal function: PN Vs RNg
≤4 cm >4 cm
Pignot G. et al. Urol Oncol 2014; 32: 1024-1030

Preserving renal function: PN Vs RNPreserving renal function: PN Vs RN
Pignot G. et al. Urol Oncol 2014; 32: 1024-1030

• Multi institutional Australian study• Multi-institutional, Australian study
• 488 consecutive procedures
• Period 2005-2012
• 156 PN and 332 RN• 156 PN and 332 RN
Satasivam P. et al. BJU Inter 2015; (available online)

PN in patients with medical risk factorsPN in patients with medical risk factors
Satasivam P. et al. BJU Inter 2015; (available online)

PN in patients with medical risk factorsPN in patients with medical risk factors
Satasivam P. et al. BJU Inter 2015; (available online)

PN in patients with medical risk factorsPN in patients with medical risk factors
Satasivam P. et al. BJU Inter 2015; (available online)

f• Retrospective analysis of 44 consecutive cases
• PADUA score ≥ 10
• Single Center, single surgeon studysurgeon study
Volpe A. et al. BJU Inter 2014; 114: 903-909

RAPN f hi h i k tRAPN for high risk category
Volpe A. et al. BJU Inter 2014; 114: 903-909

RAPN for high risk categoryRAPN for high risk category
Volpe A. et al. BJU Inter 2014; 114: 903-909

RAPN for high risk categoryRAPN for high risk category
Volpe A. et al. BJU Inter 2014; 114: 903-909

Ficarra V. et al. BJU Inter 2014; 113: 936-944

RAPN Vs OPNRAPN Vs OPN
Ficarra V. et al. BJU Inter 2014; 113: 936-944

RAPN Vs OPNRAPN Vs OPN
Ficarra V. et al. BJU Inter 2014; 113: 936-944
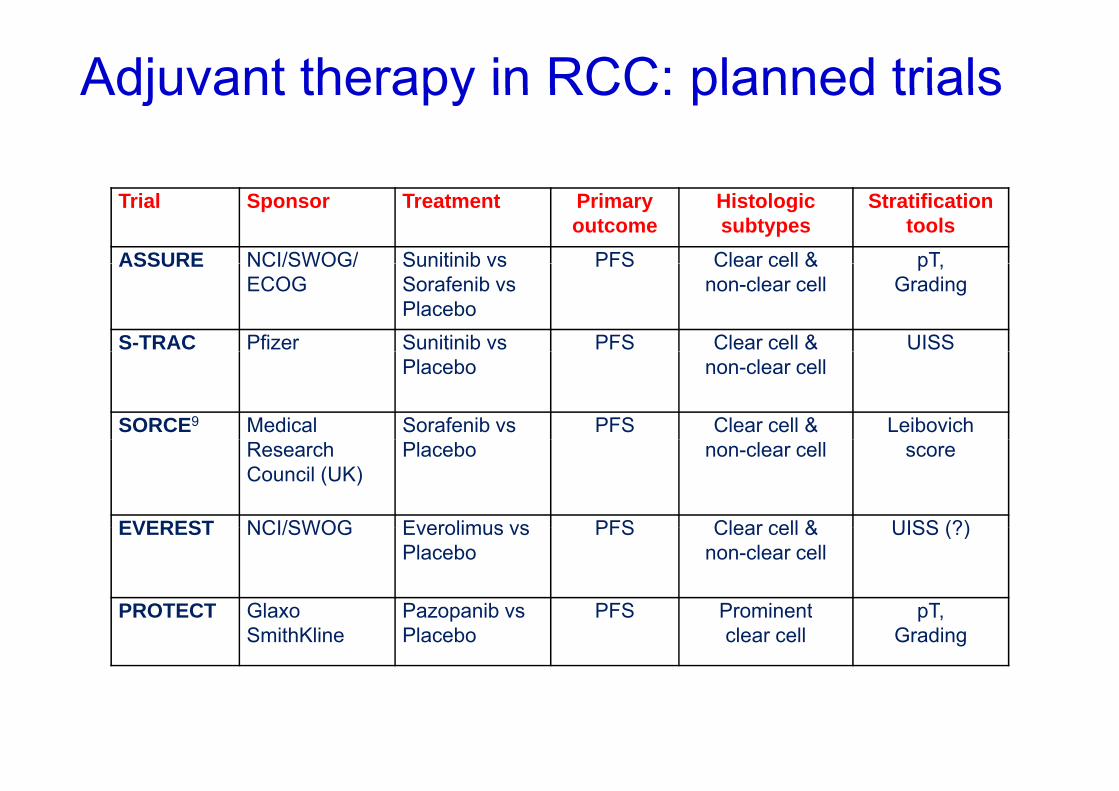
Adjuvant therapy in RCC: planned trialsAdjuvant therapy in RCC: planned trials
Trial Sponsor Treatment Primaryoutcome
Histologicsubtypes
Stratificationtools
ASSURE NCI/SWOG/ Sunitinib vs PFS Clear cell & pTASSURE NCI/SWOG/ECOG
Sunitinib vsSorafenib vsPlacebo
PFS Clear cell & non-clear cell
pT,Grading
S-TRAC Pfizer Sunitinib vs PFS Clear cell & UISSPlacebo non-clear cell
SORCE9 Medical Sorafenib vs PFS Clear cell & LeibovichResearchCouncil (UK)
Placebo non-clear cell score
EVEREST NCI/SWOG Everolimus vs PFS Clear cell & UISS (?)EVEREST NCI/SWOG Everolimus vsPlacebo
PFS Clear cell & non-clear cell
UISS (?)
PROTECT Glaxo Pazopanib vs PFS Prominent pTPROTECT GlaxoSmithKline
Pazopanib vsPlacebo
PFS Prominentclear cell
pT, Grading

Adjuvant therapy in RCC: ASSURE trialAdjuvant therapy in RCC: ASSURE trial

Adjuvant therapy in RCC: ASSURE trialAdjuvant therapy in RCC: ASSURE trial
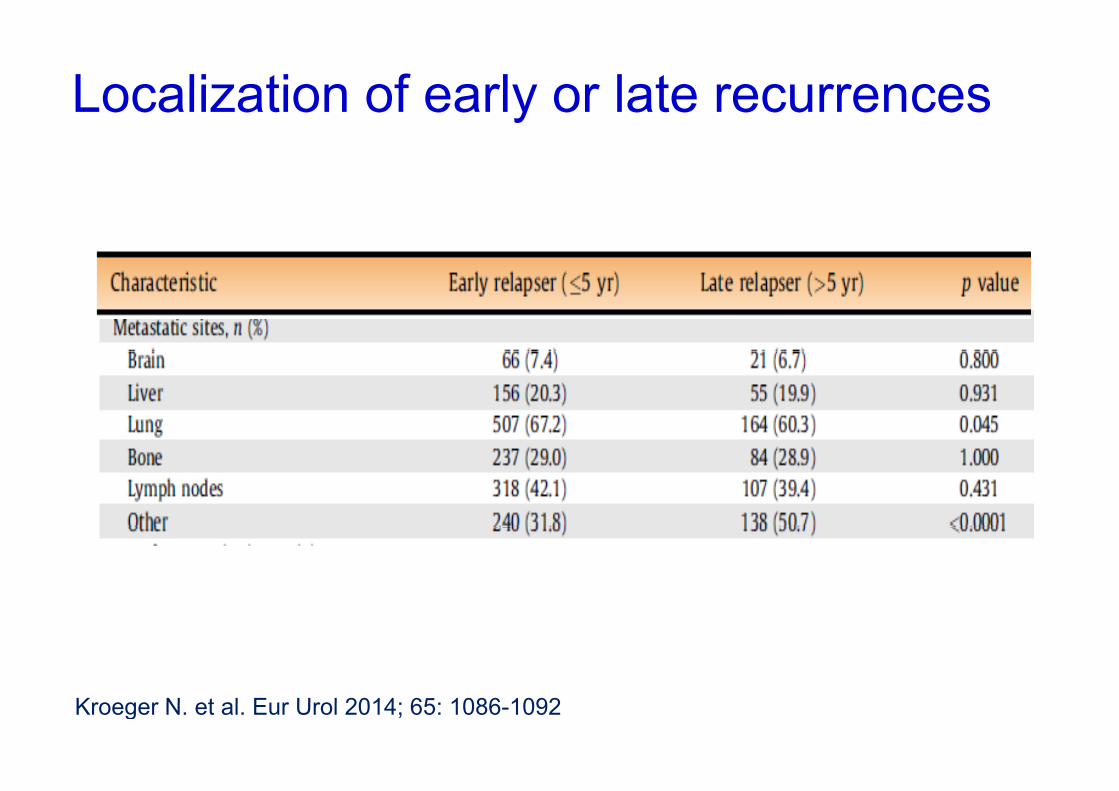
Localization of early or late recurrencesLocalization of early or late recurrences
Kroeger N et al Eur Urol 2014; 65: 1086 1092Kroeger N. et al. Eur Urol 2014; 65: 1086-1092

Localization of early or late recurrencesLocalization of early or late recurrences
Brookman S. et al. BJU Inter 2013; 112: 909-916

Active surveillance for recurrent RCC
• Potential first-line approach in asyntomatic or minimally symptomatic patients with good y y p p gperformance status without liver metastases.
• “spontaneous” disease stabilization should be considered before initiation of any active treatmentconsidered before initiation of any active treatment
Park I. et al. J Cancer Res Clin Oncol 2014; 140:1421–1428

Lung recurrencesLung recurrences
Active surveillance for recurrent RCC
• Subcentimeter Pulmonary Nodules are not• Subcentimeter Pulmonary Nodules are not associated with disease progression
• Patients with subcm indeterminate pulmonary nodules would be unlikely to benefit from extensivenodules would be unlikely to benefit from extensive postoperative chest imaging surveillance, which h ld b d f ti t ith d lshould be reserved for patients with nodules
greater than 1 cm
Mano RI. et al. J Urol 2015; 193: 776-782

Metastasectomy in mRCCMetastasectomy in mRCC
• Ideal candidates are patients - with solitary recurrence after a prolonged DFSwith solitary recurrence after a prolonged DFS
from nephrectomy
• The decision to resect metastases has to be taken foreach site and on a case-by-case basis; performanceeach site, and on a case-by-case basis; performance status, risk profiles, patient preference and alternative techniques to achieve local control mustalternative techniques to achieve local control, must be considered (GR C)
• Multidisciplinary decision

Metastasectomy in mRCCMetastasectomy in mRCC
Dabestani S et al Lancet Oncology 2014; 15: 549-561

Stereotactic radiotherapy for boneStereotactic radiotherapy for bone metastases
Thoracic spine Pelvic bone

Stereotactic radiosurgery for brainStereotactic radiosurgery for brain metastases

• Retrospective study including 1658 cases from the International Metastatic Renal Cell Carcinoma te at o a etastat c e a Ce Ca c o aDatabase Consortium (IMDC)
• Comparison between 982 patients who had a CN• Comparison between 982 patients who had a CN with and 676 mRCC patients who did not.
Heng DYC et al Eur Urol 2014; 66: 704-710

Cytoreductive nephrectomy in the targeted therapy era
Heng DYC et al Eur Urol 2014; 66: 704-710

Heng DYC et al Eur Urol 2014; 66: 704-710

Cytoreductive nephrectomy in theCytoreductive nephrectomy in the targeted therapy era
Heng DYC et al Eur Urol 2014; 66: 704-710

Cytoreductive nephrectomy in theCytoreductive nephrectomy in the targeted therapy erag py
• CN is beneficial in synchronous mRCC patients treated with targeted therapy even after adjusting fortreated with targeted therapy, even after adjusting for prognostic factors.
• Patients with estimated survival times < 12mo or four or more IMDC prognostic factors may not benefit fromor more IMDC prognostic factors may not benefit from CN.
Heng DYC et al Eur Urol 2014; 66: 704-710

International GuidelinesInternational Guidelines
• CN is currently recommended in mRCC patients• CN is currently recommended in mRCC patients with good PS, large primary tumours, and low metastatic volume In patients with poor PS ormetastatic volume. In patients with poor PS or IMDC risk, those with small primaries and high metastatic volume and/or asarcomatoidmetastatic volume and/or asarcomatoidtumour, CN is not recommended. (EAU, 2015)
• Data from IMRDMC suggest that CN continues to play a role in patients treated with targeted-p y p gtherapies. Patients with mRCC who present with hematuria or other symptoms related to primary y ytumor should be offered palliative nephrectomy if they are surgical candidate (NCCN, 2015)

Precision Medicine for mRCC: “the right gmedication for the right patient”
Sonpavde G et al. Urol Oncol. 2014; 32: 5-15
Precision Medicine for mRCC: “the rightPrecision Medicine for mRCC: the right medication for the right patient”
• Conducting clinical trials withConducting clinical trials with
1) prospective incorporation of promising1) prospective incorporation of promising candidate predictive molecular biomarkers
2) novel biomarkers endpoints, and
3) mandatory biopsies of metastatic sites at diff t ti i t thdifferent time points on therapy
Sonpavde G et al. Urol Oncol. 2014; 32: 5-15