visit our booth at
TRANSCRIPT
Page | 1 October 2014
Thank you to everyone who joined us for our Annual Health Fair on September 18th. It was truly an enjoyable experience for both AccuScripts and the attendees. The positive feedback was overwhelming and we hope to continue to exceed expectations in our educational offerings. We sincerely thank all of our excellent presenters for sharing their knowledge and expertise with our attendees. Our goal with all of our educational offerings is to improve the quality of care and expand awareness and knowledge of trending topics. We look forward to seeing you at our future events.
As of October 6th, 2014 ALL HCP have been moved from a Schedule III to Schedule II (with the exception of Zohydro-ER, a pure hydrocodone sustained-release product already assigned to Schedule II). All ordering processes that long-term care facilities have been undertaking in procuring Schedule II medications are now in effect for ordering such products as Vicodin, Vicoprofen, Lorcet, Lortabs, Norco, Hycodan (Hydromet) syrup, Tussionex Pennkinetic ER suspension, TussiCaps and the like. Regrettably, legislation of this rescheduling mandate has come about secondary to the vast hydrocodone diversion that has been plaguing the United States for some time now. The DEA has also enacted more guidelines to make more options available for the safe and secure return of all controlled drugs from long-term care facilities. We will not delve into this now, as AccuScripts long-time protocol that has been and is currently being followed by our customers for the return of controls continues to remain an approved process by the DEA and State Board of Pharmacy.
IN THIS ISSUE:
Medicare Part D Plans & MyCare Ohio in 2015 2
Continuous Quality Improvement 2-3
New CDC Recommendations for Aged 65+ 3-4
Atypical Antipsychotics May Cause AKI 4
NSAIDs Linked to Venous Thromboembolism 5
Cataract Surgery May Help Prevent Cognitive Decline 5
Probiotic + Antibiotic Therapy Reducing C. Diff 5
New FDA Approved Medications 6-7
Pharmacotherapy of Anxiety Disorders 7-11
VISIT OUR BOOTH AT
October 21-22
Dublin, OH
Page | 2 October 2014
Effective January 1, 2015 the following Medicare Part D plans will no longer be a zero-premium plans and any residents that are enrolled in them will need to enroll into a new Part D plan or be charged a premium effective January 1st (NOTE: Any resident who is a dual (Medicare/Medicaid) and/or lives in a long-term care facility can change plans any time of the year. Any resident, who does not have Medicaid coverage and does not live in a long-term care facility, must enroll into a new plan by December 7th). The plans that will not be zero premium in 2015 are:
Advantage-Plus Meridian (S7230-002) Anthem Blue MedicareRx Standard (S5596-013) United American-Select (S5755-085) SecureAdvantage Rx – Option 1 (S9014-001)
The 2015 Medicare Part D zero-premium plans are:
EnvisionRxPlus Silver (S7694-014) by RxOptions/Envision AARP MedicareRx Saver Plus (S5921-359) by OptumRx SilverScript Choice (S5601-028) by SilverScript Aetna MedicareRx Saver CVS/pharmacy Prescription Drug Plan (S5810-048) by
Aetna Humana Walmart-Preferred Rx Plan (S5884-137) by Humana Symphonix Rite Aid ValueRx (S0522-020) WellCare Classic (S5967-151)
Ohio initiated the MyCare Ohio managed care program in 2014 to unite Medicare and Medicaid benefits for DUAL eligible recipients. This year the beneficiary was only auto-enrolled in the Medicaid benefits and automatically opted out of the Medicare portion. Unfortunately that will
change in 2015. If you do not want a resident to receive the Medicare benefits from MyCare, they will need to opt out of the Medicare portion by December, 2014. Once the decisions have been made please forward a list of residents’ names, benefit information (MyCare/Traditional Medicare), and ID numbers for MyCare Medicare to your billing representative.
Any questions regarding Medicare Part D and MyCare Ohio can be directed to Sarah Partlo, Director of Financial Accounts at AccuScripts Pharmacy: [email protected].
Your AccuScripts leadership team has been dedicated to improving the quality of our services and customizing to your unique needs. Your feedback is always vital to initiating and guiding our services. Here are some areas we developed better service in the third quarter…
Page | 3 October 2014
Additions to Cycle Fill. Even more products have been added to cycle fill to reduce the need to reorder and reduce the risk of running out of a medication. Examples of the additions include more patches including Lidoderm/lidocaine, and more monthly injections. These products have a distinct, specified use and dosing that can accurately be measured and counted like routine oral solids.
MobilexUSA Partnership. We are looking forward to working with Mobilex to bring you more IV support services as well as education. As a nursing CEU provider, we are preparing to provide LPN IV certification classes taught by the experts at MobilexUSA’s Vascular Access Division. Look for future announcements of educational opportunities and services coming soon!
Software Integration. New regulations coming from the federal government is halting software integration in long term care. An integration known as HL7 interface, which is a direct link between a facility’s EHR software and the pharmacy software, will become invalid as of November 1, 2014. New ways of software communication are underway to compensate for this delay. AccuScripts Pharmacy is in contact with software vendors to ensure that we continue to move forward with electronic orders. Drug Allergy, Interaction & Duplicate Therapy Communication Forms. You will have noticed more paper records of issues usually discussed over the phone with the pharmacists. To ensure proper record-keeping and documentation, a communication form will be issued to the customer staff stating the issue, the resolution and who discussed it with whom. Cold Seal Blister Cards. Certain products would be compromised by using the standard packaging method of heat sealing blister cards. For example, it may melt the contents or cause them to disintegrate. In the past, these products were dispensed in vials. The unfortunate effect was that the top drawer of the med cart became crowded and it slowed down med pass. By using the cold seal cards, the products’ integrity remains intact, the cards can be placed in the cart with the rest of the blister card meds, and credit can be issued for returns because of tamper evident packaging.
As we are all aware, seniors aged 65 and over are regarded within the medical community as being high risk when it comes to being exposed to the influenza virus, (along with other groups such as kids four years of age and under, pregnant women, Native Americans, Alaskan natives and patients with chronic lung and heart diseases). The CMS regulations require institutionalized residents to be vaccinated against both the flu and pneumonia unless the resident (or POA) refuses, or a condition contraindicates the administration of either of these vaccines. This having been said, we do have a very high rate of vaccinated residents living in the institutionalized setting, much higher than the young to middle aged adults (18 to 64) who are community dwellers. This group has fallen to a vaccination rate of about 33% which bodes very poorly for preventing a possible epidemic outbreak nationwide.

Page | 4 October 2014
Now the C.D.C. has issued a few new guidelines and recommendations: adults 65 and older are now urged to get two (2) vaccines against pneumococcal disease, a potential complication of the flu that can cause morbidity and mortality including pneumonia, meningitis and toxemia. If the patient (65 and over) has never been vaccinated against pneumococcal disease, a 1st dose of the pneumococcal conjugate vaccine is indicated, followed (6-12 months later) by a second vaccine, the pneumococcal polysaccharide vaccine. One dose of each is all that is required in a lifetime, and either of these can be given simultaneously with the influenza vaccine, says William Schaffner, M.D., past president of the National Foundation for Infectious Diseases and current medical professor at Vanderbilt University School of Medicine.
Some ‘food’ (or ‘vaccine’) for thought: The Publication, ‘Annals of Long-Term Care’ has published an article touting the benefits of Fluzone high-dose vaccine. About one year ago, Sanofi Pasteur, the manufacturer of Fluzone high-dose vaccine, announced the results of an efficacy trial stating that this new, high powered vaccine (indicated only in the 65 and older population) had a 24.2% more efficacious rate in preventing influenza in more than 30,000 participants (aged 65 and older) than did the standard-dose Fluzone vaccine. Additionally, the results showed that Fluzone high-dose delivered consistent clinical benefit across influenza virus types, clinical illness definitions, and laboratory methods of confirming influenza diagnosis.
Now the question may be: how involved do long-term care facilities want to be in replacing the standard-dose vaccine with the high-dose vaccine? With one’s immune system being enhanced to better ward off the onslaught of incoming influenza viruses, this latest innovation among flu vaccine products may be very worthwhile for looking in to. For more information re: Fluzone high-dose (including federal/state guidelines for billing Medicare/Medicaid or questions you may have [& can submit re: billing]), visit www.fluzone.com/health-care-professionals/fluzone-high-dose-vaccine.cfm.
It isn’t enough that atypicals have come under fire on many fronts, especially when not used judiciously among the elderly population, we now have one more potentially negative risk factor that has been discovered in the prescribing of these agents. A large population-based study conducted by Y. Joseph Hwang, MSC, Case Western Reserve School of Medicine in Cleveland, and colleagues have found that the use of atypical antipsychotics also increases the risk of acute kidney injury (AKI) in adults aged 65 years and older. This study was very comprehensive and informative as the duration of the study continued from 2004 through 2011 involving a population of 97,777 adults aged 65 and older, approximately half of whom received new outpatient prescriptions for an oral atypical with matched adults who did not receive such prescriptions. The team of investigators measured the number of hospitalizations due to AKI within 90 days of dissemination of the atypical medications to patients vs the number of hospitalizations due to the same cause (of AKI) of those not prescribed an atypical agent. The results of the analysis revealed the use of atypical antipsychotics was associated with a significantly higher risk of being hospitalized with AKI compared with nonuse. Atypical use was also associated with hypotension, acute urinary retention and all-cause mortality. A periodic look at a resident’s serum creatinine value by the consultant pharmacist may now be prudent for those being managed routinely on an atypical agent.

Page | 5 October 2014
Nonsteroidal anti-inflammatory drugs (NSAIDS) may almost double the risk for venous thromboembolism (VTE) including deep venous thrombosis and pulmonary embolism, according to an article published online September 24, 2014 in the journal, Rheumatology. Physicians should be especially aware of this association where patients at high baseline risk of VTE are concerned, and are being prescribed an NSAID. This is the first systematic review and meta-analysis of published observational studies to examine the association between NSAID use and VTE. At the conclusion of these multiple studies, the pooled risk ratio among NSAID users was 1.8-fold for emerging VTE, and for the population using the specific COX-2 inhibitor, celecoxib (Celebrex), an almost 2.0-fold (was actually 1.99) risk factor was ascertained. Both of these findings were statistically significant. There are theorized versions of why NSAIDS may cause an increased risk of VTE formation, but the true, known mechanism for increased VTE risk remains unclear. Obviously, any patient with a current or historical status of presenting with VTE is at substantially high risk for the re-occurrence or exacerbation of this condition when administered an NSAID.
Though these two entities may seem totally unrelated, if one steps back and looks at the ‘big picture,’ there may be some real rationale as to why cataract surgery may slow cognitive decline. In older adults with or without dementia, the presence of cataracts and visual impairment can compromise the ability to perform ADLs and increase the risk of falls, thereby increasing the risk of institutionalization and contributing to an overall decline in cognitive function and quality of life. Cataract surgery has an extremely low rate of postop complications and is considered a type of surgery that almost always is successful in terms of improving vision. However, many older persons and their caregivers opt not to undergo the procedure due to cost, anxiety, doubt of a good or satisfactory outcome, and doubt that improvement in the quality of life will ensue. However, results from an ongoing clinical trial presented at the Alzheimer’s Assn International Conference in 2014 in Copenhagen revealed that cataract surgery not only improves vision, but may also slow cognitive decline and reduce neuropsychiatric symptoms. “This was actually a very important finding for us,” said Tatiana Riedel, research project manager, Case Western Reserve University, Cleveland, in an interview with ‘Annals of Long-Term Care: Clinical Care and Aging.’ “We have found that vision loss contributes to confusion, depression, and delusion in the dementia patient, and that these symptoms were reduced after surgery.”
The Annals of Long-Term Care journal has published a condensed version of a systematic review and meta-analysis to evaluate the efficacy of coadministering probiotics and antibiotics in preventing Clostridium difficile infection (CDI) which was fully published in the journal, Open Medicine. Reena Pattani, MD and colleagues from the University of Toronto, Canada, included 16 studies, the majority of which were based in the United States and the United Kingdom which involved many patients aged between 33 and 80 years, and were examined for efficacy of probiotics when administered simultaneously with antibiotics. Among patients randomly assigned to coadministration of probiotics, pooled analyses

Page | 6 October 2014
revealed significant reductions in the risks of antibiotic-associated diarrhea. In the subgroup analyses, the authors noted that significant reductions in rates of both antibiotic-associated diarrhea and C-Diff infections being the outcome within these trials of coadministration. These trials assessed primarily lactobacillus-based probiotic formulations; the authors recommended future investigations of whether a greater benefit can be realized using combined probiotic therapy vs single-species probiotic formulations when antibiotics are prescribed.
On June 20th, 2014 the FDA approved the antibiotic Sivextro (tedizolid) available as an oral tablet or IV solution to eradicate organism(s) being chiefly identified as Streptococcus species,
Enterococcus faecalis, Staph Aureus (both methicillin-resistant and susceptible strains) and other gram-positive bacteria involved in skin and skin-structure infections. The two dosage forms (200mg IV once daily X 6 days or one 200mg tablet daily X 6 days) work as a protein synthesis inhibitor and belong to the class of antibiotics known as oxazolidinones, of which this is the 2nd approved agent (Zyvox [linezolid] being the 1st). Sivextro is marketed by Cubist Pharmaceuticals.
Jardiance (empagliflozin) researched and marketed by Boehringer Ingelheim has been approved by the U.S. FDA as an adjunct to diet and exercise to improve glycemic control in adults with
type 2 diabetes. The once-daily drug, a sodium-glucose cotransporter 2 (SGLT2) inhibitor has a mechanism of action of blocking the reabsorption of glucose by the kidney, thereby increasing glucose excretion and lowering blood glucose levels. Rather common adverse reactions include UTI’s and vaginal yeast infections. In and of itself, empagliflozin should not cause hypoglycemia, but may in combination with other glucose-lowering agents. This agent may also cause some degree of dehydration which in turn may lead to a drop in blood pressure & result in dizziness or faintness which can be especially hazardous in older, ambulatory residents. This medication is contraindicated in the presence of severe or end-stage renal disease and dialysis patients.
Trulicity (dulaglutide – Eli Lilly & Co) has been approved as a once-weekly injection for the treatment of type 2 diabetes. This glucagonlike peptide-1 (GLP-1) receptor agonist joins
liraglutide (Victoza), exenatide (Byetta) and albiglutide (Tanzeum) on the U.S. market. The most prevalent side effects of dulaglutide are similar to these other agents within the same class which are nausea, diarrhea, vomiting, abdominal pain and decreased appetite. This agent is also not to be considered as 1st line therapy in managing DM-II.
Striverdi Respimat (Boehringer Ingelheim) was approved in July 2014, and its generic name, olodaterol may reveal this agent to be some kind of a beta2 agonist which indeed it is. This is a
very long-acting orally inhalable aerosol mist which has been approved for managing COPD with a dosage regimen of two inhalations administered orally once daily. Each actuation releases 2.5mcg of olodaterol within an aerosol solution and the respimat cartridges are available as either a 28 or 60 metered actuation size. In the elderly, no dosage adjustment is necessary, even in the presence of impaired hepatic or renal function. However, the patient must exhibit the ability to slowly inhale and hold his breath for 10 or more seconds to adequately receive a full, therapeutic dose. Various priming procedures as described in the patient leaflet need to be followed when this metered dose aerosol is not being routinely used; the cartridge has an expiration date of 90 days after being inserted into the inhaler.

Page | 7 October 2014
Spiriva (tiotropium) is now available also as an inhalation spray, and Boehringer Ingelheim has named this dosage form Spriva Respimat. Indicated for the management / maintenance treatment
of COPD, this drug is already available as an inhalation powder. The clinical indications and dosage regimen are the same as the Spiriva Handihaler, but is easier to use than its companion handihaler because it requires minimal inhalation effort by the patient. The scheduled release for the Spiriva Respimat will be some time at the very end of December, 2014.
And finally, the U.S. Food and Drug Administration has approved apremilast (Otezla, by Celgene) for treating patients with moderate to severe plaque psoriasis who are candidates for
phototherapy or systemic therapy. This approval comes on the heels of FDA’s approval (of apremilast) last March to treat adults with active psoriatic arthritis which occurs in 10 to 20% of patients with plaque psoriasis. This type of psoriasis is the most common manifestation, appearing as raised, red patches of skin covered with silvery white scales.
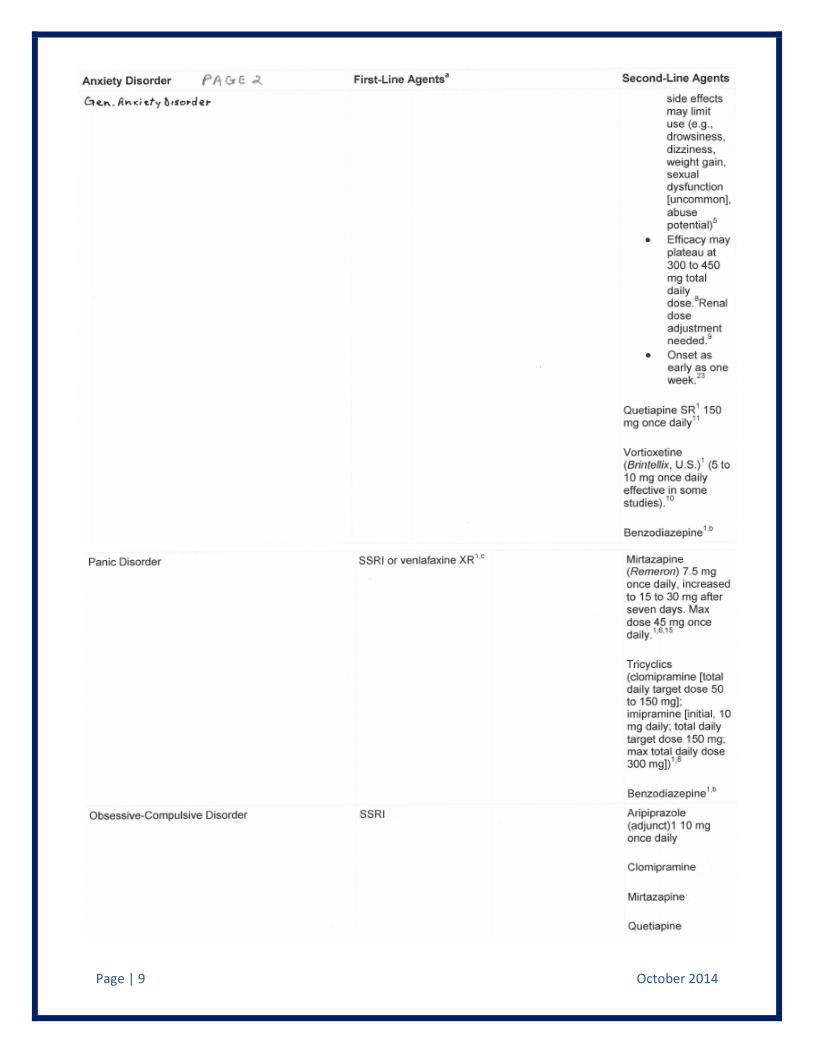
As was done in our last quarterly newsletter in which an informative table was presented as a reference guide in ‘Choosing and Switching Antidepressants,’ this quarter a reference guide is going to be included (see the following four pages) regarding the Pharmacotherapy of Anxiety (and related) Disorders. We hope this serves as a good reference works in selecting 1st line and 2nd line therapies in managing generalized anxiety disorder, panic disorder, obsessive-compulsive disorder, social anxiety disorder and post-traumatic stress disorder. The international on-line service of Medscape has presented the following tables which have been printed on the following four pages:
24340 Sperry Dr
Westlake, OH 44145
Phone: 800-726-5920
Fax: 800-779-3822

Page | 8 October 2014
Page | 9 October 2014

Page | 10 October 2014

Page | 11 October 2014
Images via Medscape.