vol. 13, no. 1, spring 2006 association of staff physician ...c.ymcdn.com/sites/ · jama careernet...
TRANSCRIPT

VOL. 13, NO. 1, Spring 2006
A S P R THE ONLY INTERNATIONAL ORGANIZATION EXCLUSIVELY FOR IN-HOUSE PHYSICIAN RECRUITERS
Association of Staff Physician Recruiters
FIVE KEYS TO MAXIMIZING YOURRECRUITMENT ADVERTISINGDOLLARSby Elaine Starling
(Maximizing Advertising Dollars - cont'd on p. 36)
As a staff recruiter, you face significant pressures whencompeting with hospitals, group practices, and medicalresearch establishments for top-flight physiciancandidates. These challenges are particularly acute ifyou are in a rural or underserved area where the demandfor healthcare is often greater, but the resources are fewer.
The state of your recruitment expenditures may revealthat your advertising dollars are simply not going as faras they used to. In fact, you may be facing significant pressure from medical staffexecutives to demonstrate a return-on-investment for your dollars spent. Yourgoal of achieving cost effective results is significantly complicated by all of thesales pitches, inflated statistics, and confusing and misleading promises made byvendors seeking to gain a piece of your advertising budget. Not a week goes bywithout some news of a new recruitment advertising source that purports to be theultimate, cost-effective panacea for filling physician openings.
The truth of the matter is that physician advertising can evolve into a very expensiveproposition if not managed properly. Fortunately, by incorporating a few simple practicesinto your media strategy, you can maximize the impact of your recruitment budget.
There is an old saying that 70% of an advertising campaign’s success comes asa direct result of placing your ad in the right forms of media. In fact, the mostcritical decision you’ll make is where to place your advertising, as media placementrepresents the largest percentage of your advertising budget. The right mediavenues will generate highly qualified, interested prospects —the results of whichcan be tracked over time to assist in optimizing your spending further. Followingare five keys to maximizing your advertising budget at a time when you may befacing increased pressures to demonstrate a return on investment.
Elaine Starling
Articles: PageASPR Educational Forum Program .................. 30Book Review ........................................................ 6Great Places ......................................................... 9High Cost of Malpractice Insurance ThreatensSupply of Ob/Gyns ............................................. 13How Can We Make Our Interviews Flow .......... 11The Impact and Influence of PhysicianRecruitment on the Revenue Stream ................ 28Maximizing Recruitment Advertising Dollars ...... 1Silence Kills ........................................................ 16Skyrocketing Malpractice Premiums Causeof Ob/Gyn Crisis? ............................................... 15
ASPR Updates/Features/Other:ASPR Member Profiles ........................................ 8Board of Directors & Committee Chairs ............ 44Calendar ............................................................... 4Committee Chat ................................................... 4Corporate Contributor Features ........................ 36Corporate Contributor Listing .............................. 2Discount Purchasing Program ............................. 3Executive Director Report .................................... 3Job Hotline ......................................................... 41New Members .................................................... 38Notes from the Board Room ................................ 5President's Corner ............................................... 2Regional Programs ............................................ 27
Guide to Advertisers:AAFP .................................................................. 22AAOS .................................................................. 21A. Arnold ............................................................. 12Adkisson ............................................................. 21American College of Physicians ........................ 40Bernard Hodes ................................................... 14Cejka ................................................................ 7,29Delta Medical ..................................................... 26Doc-in-a-Box ...................................................... 26Dowden Health Media ....................................... 29Endocrine Society .............................................. 29Health eCareers ................................................. 37JAMA .................................................................. 24Medical Doctor Associates ................................ 12MMS ................................................................... 11NAS ...................................................................... 9NEJM ............................................................. 23,25PhysicianWork .................................................... 19PracticeLink ........................................................ 18Profiles ................................................................ 20Radworking ........................................................ 15Surgeons Link .................................................... 10Vista ............................................................... 14,43
Editor Judy BrownAssociate Editor Laura Screeney
Publisher Bonnie Young Edu
c. F
orum
Rec
ruiti
ng 1
01
Rec
ruiti
ng 2
01 ASPR Annual ConferenceAugust 13-16, 2006Hyatt Regency Hotel
Minneapolis, MN
Info on
Pages
30-32

Vol 13 NO. 1, Spring 2006PAGE 2 A S P R
Shortly before starting to write this updateI made my monthly calls to a few of thenew ASPR members. All ASPR boardmembers make these calls to offer awelcome and to remind them of the manybenefits they receive by being a part ofthis organization. I feel that ASPRprovides many valuable resourcesincluding; the chat@ASPR, quarterlynewsletters, the discount vendorprogram, Educational Forum, and others.The benefit that I believe is the mostvaluable is the networking that occursamongst members. I never hesitate tocontact a fellow member with a question,when seeking information or when I’m
looking for advice. I hope all of you take advantage of this benefit.
I am very pleased to announce after much review and discussion, ASPRhas signed a letter of agreement with Castle Worldwide, Inc. to helpdevelop the first part of our fellowship program. Castle Worldwide, Inc.has a great deal of experience in working with organizations and societiesin developing, administering, and maintaining knowledge basedcompetency exams. We are planning on offering the 101 fellowship examthis fall and are continuing to develop the 201 and 301 exams to beoffered in the coming years. This will be not only a significant financialcommitment for ASPR but also a huge time commitment by strategicplanning committee members. We feel that in the interest of our members,we as the leading physician recruitment organization are the best onesto develop a program, which measures competency in the field.
ASPR held a Board and Committee Chair strategic planning retreat, March4-5 2006 in Minneapolis. The reason we do this is to make certain thedirection and goals of the organization are in line with what ourmembership requires to continue to make this the leading physicianrecruiter organization. During this meeting there were several key areasidentified to improve ASPR not only for our current members, but in orderto attract new members as well. We also agreed we must continue toeducate physicians on the benefits of working with ASPR members. Youwill be hearing more about these in the coming months but some of ourinitiatives include; increased communication to our members through thewebsite and a monthly e-newsletter; redesign of the website to takeadvantage of technological improvements; increasing awareness in theindustry by partnering with corporate contributors on projects; andattracting new members who may do some recruitment as a part of theirposition (ie. Practice Managers, Hospital Presidents, etc.) to name a few.
Hope everyone is enjoying spring and looking forward to networking withyou this summer in Minneapolis!
PRESIDENT'S CORNERASPR Recognizes &Thanks our 2005Corporate ContributorsFor product and contact information on thesecompanies, go to the "Members Only" page ofthe ASPR website (www.aspr.org).
Gold ContributorAdkisson ConsultantsArlington HealthcareCompHealthElsevierJAMA CareerNetNew England Journal of MedicinePhysicianWorkPracticeLink.com & Web CVPracticeMatchVista Staffing Solutions
Silver ContributorBernard Hodes GroupWeatherby Locums
Bronze ContributorA Arnold World Class RelocationAccuCheck InvestigationsAmerican Academy of Family PhysiciansAmerican College of PhysiciansAmerican Medical AssociationAmerimed ConsultingBarrett Moving & StorageDelta MedicalDoc-in-a-BoxDowden Health MediaLocumTenens.comMedical Doctor AssociatesMedical Marketing ServiceMedicus PartnersMedstaff National Medical StaffingPacific CompaniesProfilesStaff Care Inc.Stevens Worldwide Van LinesStrategy HouseTimeline RecruitingUnique Opportunities
ASPR Reprint Policy
Permission must be obtained beforereprinting any article appearing in theASPR newsletter. To obtain thispermission, please contact Bonnie Youngin the ASPR office directly. 800-830-2777.
David Nyman

Vol 13 NO. 1, Spring 2006 PAGE 3A S P R
MESSAGE FROM THE EXECUTIVE DIRECTOR
The ASPR Newsletter is publishedquarterly for members of ASPR by theAssociation of Staff Physician Recruitersand Office Enterprises, Inc., 1711 W.County Road B, Suite 300N, Roseville,MN 55113Phone: 800-830-2777 or 651-635-0359Fax: 651-635-0307Email: [email protected]
Unless stated, comments in thispublication do not necessarily reflect theendorsement or opinion of ASPR or OEI.The publisher is not responsible forstatements made by the authors,contributors, or advertisers. Thepublisher reserves the right to finalapproval of editorial and advertising copyin this publication.
ASPR members are eligible for specialdiscounts on services from participatingadvertising, direct mail, and other serviceproviders. For a complete listing, go to themembers only section of our website andclick on the Discount Purchasing Program.
Call Bonnie at the ASPR office at 800-830-ASPR (2777) if you have questions or needadditional information.
Discount PurchasingProgram
ASPR Endorsement PolicyASPR recognizes and appreciates thesupport of members of the CorporateContributor Program. This affiliation withASPR provides a unique opportunity forexposure to ASPR members that includesname recognition and goodwill. WhileASPR recognizes and acknowledgesCorporate Contributors, it in no waydirectly or indirectly endorses thecorporation, its products, or services.Corporate Contributors, who advertise orpromote an endorsement or impliedendorsement by ASPR, will automaticallybe terminated from the CorporateContributor Program.
Dana Butterfield
Even though it is only early May, the ASPRBoard of Directors and numerous committeemembers and chairs have been hard at workthis year. I would like to thank a long list ofindividuals for their time and efforts that wentinto a very successful strategic planningretreat, held in Minneapolis on March 4-5,2006. For those of you who don’t have yourcalendars in front of you, those dateshappened to fall over a weekend in March.So yes, your ASPR officers are willing togive of their own personal time in order tomake progress on strategic planning issuesthey feel are critical to the growth andvibrancy of this organization. The officersand leaders who attended were; DaveNyman, Marci Jackson, Lynne Peterson,Dana Reed, Kathie Lee, Rich Lynch, Brett Walker, Jerry Hess, Scott Lindblom,Laura Screeney, Judy Brown, Cindy Bagwell, Mike Hesch, Dana Butterfield, andJohn Arlandson. We discussed a number of issues and ideas in one and one halfdays. We had an opportunity to very thoroughly go over the current strategic planand make changes and additions for 2006. I would also like to thank John Arlandsonfor doing an excellent job of facilitating the two-day meeting. As you have probablyalready noted from the President’s report that there are a number of items we wantto focus on this year. Communication is one of the key items. We need to be moreeffective in communicating to and with new members, as well as the healthcareindustry. We have made progress, but it remains a challenge and something weare improving upon. Additional areas we intend to focus on are membershipretention, membership growth, broadening membership, and strategic partnerships.
I have been involved in making some initial steps in getting the “word” out aboutASPR. This year alone, I have had the opportunity to attend a number of differentconferences, some of which I have been given time on the program to shareinformation about our Association. PracticeMatch held its annual conference inFebruary, and was gracious enough to ask me to make a presentation at the meeting.I have also exhibited at the APDIM (Association of Program Directors in InternalMedicine), NAPR (National Association of Physician Recruiters), UMPR (the UpperMidwest Physician Recruiters), and attended the CompHealth symposium. TheSGIM (Society of General Internal Medicine) asked me to participate on a paneldiscussion for residents and fellows about finding a job after training. I do hope thatwe, as an association, have more opportunities to present at various medicalconferences in the very near future. I’m looking forward to the days when ASPRbecomes a “household word” in the healthcare community. You can affect that veryeasily at your own organizations, starting this process at a grass roots level. Themore you share with your administration and resident training programs, the morecredibility and visibility we as an organization have. Our corporate contributorsneed to be thanked because they do an outstanding job of sharing information withnew members about ASPR. We receive numerous calls from potential membersbecause they have been directed to ASPR by our corporate contributors.
Another important area of growth that has been a long time in the works is thatof the ASPR Education Fellowship Program. During the April 2006 Board ofDirectors meeting, the Board voted to award the fellowship development programcontract to Castle Worldwide, a widely respected provider of high-quality testingservices for trade and professional associations, based in North Carolina. Initialwork has begun on this project and the first meeting with Castle Worldwide and
(Executive Director - cont'd on p. 5)

Vol 13 NO. 1, Spring 2006PAGE 4 A S P R
CALENDAR
2006
May 21-23 MRRN - Michigan Annual ConferenceGrand Traverse Resort, Traverse City, MIBi-monthly meetings in Lansing for education & networking.Information: www.mrrn.org or Deb Collier 800-206-8706
August 13-16 18th Annual ASPR Educational ForumThe Hyatt Hotel, Minneapolis, MinnesotaInformation: 800-830-2777
September TBD Indiana Recruiters Network Job FairInformation: Brett Walker - [email protected]
November 2-5 ISPR - Illinois Annual Conference & Job FairDowntown ChicagoQuarterly meetings for education and networking.Information: www.isprnet.org
2007August 12-15 19th Annual ASPR Educational Forum
The Hyatt Denver Convention Center, Denver, ColoradoInformation: 800-830-2777
Greetings, all-
Once again, we hope you enjoy this issue ofthe ASPR Newsletter.
Now that spring is here, it is time for us to beginmaking our summer plans. Where are youheaded for summer vacation? Maybe a familyreunion at the lake house, some down time atthe seashore, or camping in the wilderness?Plus, before you know it, the 18th Annual ASPREducational Forum will be taking place. Thisyear, we are headed back to lovely Minneapolis,Minnesota. Yes, Minneapolis is the home ofMary, Rhoda, Phyllis, and Mr. Grant, the Mall ofAmerica, and ASPR’s corporate headquarters.
For more information on the Annual Forum,there is a copy of the program (includingregistration form) and an article from the ASPREducation Committee starting on page 30 of thisnewsletter issue.
For many of us, the ASPR Annual Forum is atime to regroup regarding our physicianrecruitment and retention functions, catch upwith old friends, take home some new ideas,maybe even take the Physician Recruitment101 course as a refresher; and, of course, jumpin on the brand new Physician Recruitment201 session. It is also a time to visit the ExhibitHall to test out the latest and greatest toolsavailable to assist us with our physicianrecruitment responsibilities.
Lastly, and most important to me, is thenetworking that takes place during the AnnualForum. My ASPR colleagues provide aninvaluable resource to me on a daily basis.When I think back to my first year in physicianrecruitment (yes, disco was in back then), I hadno idea where to begin. ASPR did not exist,but I met a neat group of folks at a conferencewho were happy to share their ideas andexperiences with me. This group eventuallybecame ASPR and has been my “go-to” groupever since. Unlike most other industries, mostof us are in a department of one person. Whenyou are in a solo department, you can miss thecamaraderie of a larger department. Lucky forus, we can get what we need from our ASPRbuddies. This group has been my rock, mycolleagues, the predictors of industry trends, myresource for all things healthcare, and myfriends. Let’s face it--this is the group of experts.Did you ever pick up a copy of “Modern
COMMITTEE CHAT / LETTERS TO THE EDITOR“All I Really Need to Know I Learned in Kindergarten”
Healthcare” or any trade journal and read a story about the latest trends, realizingthat you already knew about it because one of your ASPR buddies had sharedit with you?
Networking is an unbelievable tool in our industry. As recruiters, networkingcomes naturally to us. It’s in our DNA. We network without realizing it and welove it! As recruiters, networking is a daily part of our lives both personally andprofessionally. I was networking when I was in kindergarten, by introducing theshy kid in class to my new group of friends during snack time. I just didn't knowit was called networking at the time. And, let’s face it, networking is lots of fun!
I guess it really is true, everything I really need to know I did learn in kindergarten!
We look forward to networking with you in Minneapolis!
Best Regards,Laura Screeney and your ASPR Newsletter Team
P.S. In the last issue of the ASPR Newsletter we inadvertently stated that Mr.Rogers' keds were white, when, in fact, they were navy blue. We apologize forthe error.

Vol 13 NO. 1, Spring 2006 PAGE 5A S P R
Partnering Opportunities – In January and February,the Board reviewed information for a partnering opportunitybetween ASPR and our Corporate Contributor, Vista StaffingInc., for providing educational materials for the Recruitment101 educational program. The Board at the February 14thmeeting approved a formal nondisclosure agreement.
Educational Testing – Since January, the Board andStrategic Planning Committee have been reviewingproposals for examination development, testing, analysisand administrative services for the Recruitment 101 programas part of the ASPR Educational Fellowship Program. TheBoard made a final selection and approval of CastleWorldwide Inc. at the April 11 meeting. President DaveNyman has more information in his article this month.
Strategic Planning – The Board and Committee Chairsheld a weekend retreat in Minneapolis in March to reviewthe ASPR Strategic Plan, set priorities and action plan forthe future of the organization. All agreed that it was anexcellent meeting with a lot of ideas for new opportunitiesas well as challenges.
ASPR NOTES FROM THE BOARD ROOM
the Fellowship Program Committee will occur later thismonth. As part of our ASPR Fellowship we will be offeringa test after completion of the Recruiter 101 course. Thattest will be available for participants to take after the August2006 annual ASPR conference in Minneapolis. Please bewatching your email for additional announcements anddetails about the program. The Board and StrategicPlanning Committee are very excited about the opportunityto continue to enhance our educational offerings to ourmembership. We look forward to your comments andsuggestions about the fellowship, as well as suggestionsfor future programming.
More recently, I have also had the pleasure of working withsome of our corporate contributors on special projects that willbenefit our members. Some of the projects I would like tomention involve CompHealth, Vista Staffing, and New EnglandJournal of Medicine. CompHealth has offered to make somechanges to an existing document, which they have called the“Best Friends Guide.” It will be co-branded by them and ASPR.This is a booklet that helps walk a physician through the varioussteps he/she needs to take when looking for a new position.We look forward to using this guide at conferences and medicalmeetings where we are exhibiting and talking with physicians.I would like to thank CompHealth for their very generous offer,and look forward to completing this project and beginningothers. I would also like to thank Vista Staffing, who hasenthusiastically agreed to help create a Recruiting 101 StudyGuide for those who will be taking the 101 test this summer. Ihad an opportunity to meet with some of their seniormanagement to discuss this, and we are hopeful there maybe subsequent study guides for the 201 and 301 as well.
Board Recruitment – In February and March the Board discussedproviding a waiver of annual conference fees for board members.President Dave Nyman noted that this would help offset the additionallodging/travel costs Board members incurr to attend the meetings theyare required to attend prior to the annual conference. At the March 14meeting the following policy was adopted:
The ASPR Board of Directors conducts monthly board meetings;periodic special meetings and members serve as officers andliaisons to committees with additional duties. The members serveas volunteers and receive no compensation. In recognition of thetime and commitment of the board members and as an incentive inrecruiting members to serve on the board, a policy is established towaive the two-day registration fee for the ASPR Annual EducationalConference for all board members attending the conference. To beeligible for this benefit, board members must attend a minimum of 80%of the board meetings each year.
Other Actions – At each Board meeting members hear reportsfrom the President, Executive Director, Treasurer and committeechairs or liaisons. These reports are usually informational with noformal action required. Executive Director Dana Butterfield has moreinformation on some of these activities in her article this month.
(Executive Director - cont'd from p. 3)
The NEJM has offered to conduct extensive research on a topicthat will be very valuable to physician recruiters. This summer, atour annual conference NEJM will be conducting an initial survey togarner suggestions from our membership on possible topics. Youwill hear more about this at our conference, but be aware that it willbe coming up, and please plan on participating in the survey. Theywill then be sharing the results with us at our annual conference inDenver, August of 2007. This is a fantastic opportunity for ASPR topartner with NEJM, and we are really excited about it. I would like tothank all three of these companies for looking at innovative ways tohelp support our membership. We greatly value our corporatecontributors and their active support of our membership.
Lastly, I hope that by now you have all had a chance to review theASPR Member Survey Summary Report. An email was sent out toall of our 799 members, notifying them that the survey results couldbe accessed in the "Resource Directory" in the Member section ofthe ASPR website. We had a response rate of 28.5% for the survey.I hope next time we will be closer to a 50% response rate, given thevalue of this information. There were a number of interesting findingsabout salary, bonus programs, lack of retention budgets, number ofcurrent opening, and large percentage of ASPR members whobelong to state and/or regional groups. Please watch for additionalinformation about the survey and for a report from our President,Dave Nyman, at the ASPR Annual Conference this summer .
I’m looking forward to our conference, and would appreciate hearingfrom all of you with suggestions or comments about the work I amdoing. My role is to further this organization and to meet the needsof its membership. Please drop me an email,[email protected] or call me at 651-288-3432, and letme know how I am doing.

Vol 13 NO. 1, Spring 2006PAGE 6 A S P R
Most of what I read is divided into two basic categories: what Ishould read for education/work, and what I read for pleasure. Ifeel disciplined and virtuous when I can soldier through articlesor books that will improve my knowledge base in the field ofphysician recruitment and healthcare. In my limited free time, Iam entertained and even transported when I can sneak in a fewchapters of a novel. (I suggest Dean Koontz’s Life Expectancy;you will laugh aloud, hold your breath in suspense, and justgenerally find yourself staying up late to read past your bedtime.Way past.) Occasionally, a book comes along that defies mydichotomous categorization of reading material. Atul Gawande’sComplications: A Surgeon’s Notes on an ImperfectScience (2002, Picador, Henry Holt andCompany, New York), is just such a book. Itis both educational and a good read.
Atul Gawande,M.D., M.P.H., isa general surgeonwho specializes inendocrine tumors and research onsurgery and public health. He splitshis clinical time between the Brighamand Women’s Hospital in Boston andHarvard Vanguard MedicalAssociates, where he is a physicianin our multispecialty group practice.He wrote Complications whilefinishing his residency. (Who writesa book during residency?) For a briefbiography of his training, visit the
Physician Directory at our website: www.harvardvanguard.org.
I did not encounter Complications through the practice wherewe both work. Instead, I stumbled across it quite by accident asI was running through a bookstore at Logan airport. I figured Ihad time to quickly grab something off the bestseller rack beforethe final boarding call. I was thinking juicy novel but instead wasattracted to the silver sticker that marked this book a NationalBook Award Finalist. As I read Complications on that red eyeflight, I resisted sleep and was drawn into the writer’s world ofresidency training and the mysteries, miracles, and mayhem ofmodern medicine. Dr. Gawande’s storytelling capabilities areespecially showcased in both the first and last chapters ofComplications, Education of a Knife and The Case of the RedLeg. You will never look at residents (or a case of cellulitis) inquite the same way again.
Dr. Gawande’s book, however, is much more than a kiss-and-tellabout the tribulations of residency, or the titillations of unusualmedical cases. The scope of the material is wider and richerthan that. He explains his reasons for writing the book as follows:
BOOK REVIEW:Complications: A Surgeon's Notes on an Imperfect ScienceReviewed by Brenda Reed, Physician Recruiter, Harvard Vanguard Medical Associates
We look for medicine to be an orderly field of knowledgeand procedure. But it is not. It is an imperfect science,an enterprise of constantly changing knowledge,uncertain information, fallible individuals, and at the sametime lives on the line. There is science in what we do,yes, but also habit, intuition, and sometimes plain oldguessing. The gap between what we know and what weaim for persists. And this gap complicates everythingwe do.
Dr. Gawande uses dramatic experiences from his residencytraining for illustration, but what makes his writing
so compelling is his ability to maintain anexchange-student-like quality of lookingat medicine as both insider andoutsider. He can write about theelephant in the room that most people
like to pretend isn’t there. Moreimportantly, he humanely engages other folks
in the conversation so the elephant isn’t sodestructive.
One such potentially avoided topic is the “uncomfortable truthabout teaching.” He openly writes about the practice of residentstesting their fledgling skills on human patients. Teaching hospitalsadvance progress and expertise, but not without trial and error onthe part of physicians in training. While attending physicianspassionately believe in the advancement of medicine throughtraining programs, if they are honest with themselves, most willconfess to not wanting residents to treat them or their familymembers. They prefer the services of an experienced colleague.Dr. Gawande sensitively summarizes this contradiction withoutascribing blame for the hypocrisy it embodies: “As patients, wewant both expertise and progress. What nobody wants to face isthat these are contradictory desires.”
The book is divided into three sections: “Fallibility,” “Mystery”and “Uncertainty.” Two chapters of the book that are probablymost directly linked to physician recruitment are in the sectioncalled “Fallibility:” Nine Thousand Surgeons, and When GoodDoctors Go Bad.
Nine Thousand Surgeons is the viewpoint from the other side ofthe booth; what it is like for physicians to attend a professionalconvention and the experience of the exhibit hall (trinkets, boothbait, and networking).
In the chapter entitled When Good Doctors Go Bad, Dr. Gawandejolts the reader when he reports that “estimates are that, at anygiven time, 3 to 5 percent of practicing physicians are actuallyunfit to see patients.” Perhaps a physician recruiter reader isnot so much shocked as startled, both for the grim statistic itrepresents, and for the frankness of the disclosure. The only
...at any given time, 3 to 5percent of practicing
physicians are actuallyunfit to see patients.
Atul Gawande, MD, MPH

Vol 13 NO. 1, Spring 2006 PAGE 7A S P R
other statistic in the book that equally engaged my squirm factorwas the fact that autopsy reveals misdiagnosis 40% of the time,a rate that hasn’t improved since 1938. (From the chapter entitledFinal Cut.)
Many of us are aware of the amount of angst that a practicesuffers when dealing with an unfit physician. Dr. Gawande writes:
As is often the case, the people who are in the bestposition to see how dangerous a physician has becomeare in the worst position to do anything about it: juniorphysician, nurses, ancillary staff. In such circumstances,the support staff will often take measures to protectpatients. Nurses find themselves quietly directingpatients to other doctors. Receptionists suddenly havetrouble finding openings in a doctor’s schedule.
Dr. Gawande acknowledges that practice partners are often slowto take action to remove an unfit colleague from practice. Notso much by way of defense as by explanation, Gawande citesresearch from sociologist Marilyn Rosenthal: “People have calledthis a conspiracy of silence, but Rosenthal did not find plottingso much as a sorry lack of it…the dominant reaction wasuncertainty, denial, and dithering, feckless intervention…” Headds, “When people try to help, they do it quietly, privately. Theirintentions are good; the result usually isn’t.” (As a healthcareprofessional, does this observation make you uneasy, perhapsfrom firsthand experience?)
Complications: A Surgeon’s Notes on an Imperfect Science is anexpansion of a number of articles and columns that Dr. Gawandeoriginally wrote for Slate and The New Yorker magazines. Thebook has won numerous awards, details of which are listed underAtul Gawande’s name at www.leighbureau.com. Besides beinga talented writer, Dr. Gawande is also a well-published researcherin the area of surgery and public health. For an in-depth profile ofhis research, visit the Brigham and Women’s webpage(www.brighamandwomens.org) and select Research Information,then search under Research Profiles.
Lastly, you should know that Dr. Gawande is an engaging publicspeaker and a great clinician. His medical assistant, Janice,positively beams when talking about their working relationship.The adjective she uses most frequently to describe him is“humble.” Describing patients seeing him for first time consults,she says, “There is a tenseness when they come in, and it is justgone when they leave. It’s like they have hope.” She likes theway he takes the time to teach in laymen’s terms. Dr. Gawandealso speaks to large audiences. He has been a Keynote Speakerat conferences, and gave the 2005 Commencement Address atHarvard Medical School.
Dr. Atul Gawande connects with people from all walks of lifethrough compelling storytelling and a self-deprecating sense ofhumor. He can hold the audience’s attention even when theydon’t necessarily understand all of the complex technological
(Book Review - continued on p. 8)

Vol 13 NO. 1, Spring 2006PAGE 8 A S P R
Megan Landgraf - CaliforniaMegan was born andraised in the Bay areaaround San Francisco,and now lives and worksnot too far fromSacramento. She juststarted working part timeas a Physician Recruiterwith Woodland Healthcarein 2005, and continues towork for a market ingagency promotingMontessori schools.Woodlands is an 80+provider multi-specialtygroup. She received herBS from UC Davis in 2004in Managerial Economics
with a minor in Spanish.
Her biggest challenges in recruitment include recruiting to asmall town and learning the ropes of working with doctors(good luck on that one…). She enjoys finally meeting thedoctors in person after talking on the phone so many times,and plans to stay with this as a career long term.
Megan’s goal with ASPR is to gain valuable knowledge frommore experienced ASPR recruiters. She is already active inASPR as a member of the illustrious Regional DevelopmentCommittee, and is a valued asset bringing the Californiacontingent into the mix.
On her off time, Megan likes to travel, cook, and ski (snowand water). And she is a painter; soon to be as famous asDejas, Wood, Seurat, and Dali.
Welcome to the world of recruitment, Megan, and to ASPR.
ASPR MEMBER PROFILESby Dennis Burns
Cherith Chapman - ColoradoCherith has been floatingaround various statesgrowing up and gettingeducated, from Illinois toNew York to Kentucky andColorado. She saved thebest for last – Colorado!This is now her home. Afew years ago, Cherithspent t ime in Japanteaching English as asecond language, andhaving her fun t imevolunteering with theChristian Surfing Club.Surfing is big in Japanand she loves i t !(Hey…she l ives inColorado. Weird). Not to be outdone by the mountains, shenow loves to hike and snowboard in all the beauty. She alsohas a creative side to her, and has a knack for drawing. Shehas taken art classes at the Art Institute of Colorado, andreceived her BS degree in Business Administration fromBerea College in Kentucky.
Cherith has worked at a number of for-profit companies andnon-profits. She prefers the non-profits, and thereforeaccepted the job as physician recruiter for Colorado RuralHealth in July 2005. She loves what she does, and plans tostay with it long term. One of her challenges at ColoradoRural Health is matching candidates and families to the morerural practices and communities – she has some toughsearches in some remote places – but her joy comes frommaking that great match and seeing the fruit of her efforts.She enjoys talking in-depth with the candidates, and buildingrelationships over time. Cherith has about 40 searches goingon at any point in time, and most of them are in Primary Care.She has been busy the past year reaching out proactively toColorado’s residents and medical education programs.
Cherith is great at connecting with people, so she will do wellin her new role, and we will be seeing her around ASPRconnecting with all of us! We're glad you are part of theteam, Cherith.
By the way, her unusual name comes from the Bible: it is thename of the brook where the Prophet Elijah was fed by theravens. So far, she has determined that there are about adozen other “Cheriths” around the country. Rare, indeed, onmany levels.
nuances of his subject matter. He is a great example of how toengage people in the difficult, but necessary, conversations thatwill begin to narrow the “gap between what we know and whatwe aim for” in the imperfect science of medicine. Go read thebook for yourself and begin the conversation with friends andcolleagues in your practice.
About the author:Brenda Reed is Physician Recruiter, Harvard Vanguard MedicalAssociates, 275 Grove Street, Suite 3-300, Newton, MA. Phone 800-222-4606, email [email protected].
(Book Review - continued from p.7)
Cherith ChapmanMegan Landgraf

Vol 13 NO. 1, Spring 2006 PAGE 9A S P R
IntroductionSuccessful recruitment of physicians and other medicalprofessionals to rural areas requires a blending of communitydevelopment and medical staff development. Iowa is one statethat developed a program connecting community andrecruitment issues in a unique partnership.
“Great Places” is designed to make good places great througha partnership between 18 state agencies, and build capacity incommunities, regions, neighborhoods, or districts. The initiativewas introduced by Iowa’s governor in early 2005. Under thenew Great Places collaboration, the application and grant cycleusing multiple state agencies is replaced by a “one stop shop”proposal opportunity.
For communities, Great Places streamlines access to stategrants and technical assistance, stimulates ideas and planning,and helps leverage local and private resources. For stateagencies, Great Places introduces an innovative technique tocombine existing resources for measurable impact in regionsand communities.
Great PlacesLast year, the Iowa Department of Cultural Affairs in partnershipwith 18 state agencies, issued a call for invitations to participatein a brand new initiative called Iowa Great Places.
GREAT PLACES -- A Developmental Model for Other Statesby Anita Walker, Director, Iowa Department of Cultural Affairs
(Great Places - continued on p. 10)
Anita Walker
We received 146 invitationsfrom 94 counties. If you wantto take a trip to every cornerof Iowa and all that’s inbetween, past, present, andfuture, take a reading tour ofour Great Places invitations(www.iowagreatplaces.gov).
Iowans were challenged tothink about what is genuineand authentic about the placewhere they live, and what itwould take to make that agreat place. Great placeshave a special identity, andcome in all sizes, urban and rural. So did our invitations.
Some of the great places were as big as the 10-county GreatRiver Road along the Mississippi, the length of the Loess Hillsfrom Plymouth to Fremont Counties along the Missouri, andanother captured two tiers of counties on our southern borderin the Historic Hills Corridor, from Clarke and Decatur to VanBuren.

Vol 13 NO. 1, Spring 2006PAGE 10 A S P R
They envisioned the revitalization of historic corridors like theWhite Pole Road, a historic trail marked by white polesconnecting Adair, Casey, Menlo, Stuart, and Dexter.
They were compact, well-defined sections of our cities that seethemselves as cultural magnets or shopping districts, likeBeaverdale, East Village, and Ingersoll in Des Moines, and SiouxCity’s Floyd Boulevard market that wants to attract people withauthentic, locally-grown organic food. Some invitations camefrom small towns that have experienced rebirth before and areconfident they can do it again.
Pomeroy was “nearly wiped off the face of the earth by adevastating tornado in 1893,”writes Denita Luke. “The spirit ofthe people prevailed,” she continues. Now the community wantsto attract artisans to live and work in Pomeroy making it acultural destination.
Riceville survived a fire that destroyed the town in 1901. It wantsto reclaim its place as “Gateway to Mitchell County.”
Olin wants a town square instead of the vacant lot in the middleof town. City Clerk Jean McPherson envisions benches, bikeracks, picnic tables, and a fountain as a resting spot for hikersand cyclists who travel a nearby trail.
Albia, which has one of the few town squares on the NationalRegister of Historic Places, wants to focus now on Buxton andits mining history, recreating an authentic experience with trainrides and a trip down a coal shaft.
Lake City has “everything but a lake,” but knows how to “dreambig and deliver on those dreams,” writes Paul Iverson.
Iowans seem perfectly content without the proverbial “mountainsand oceans.” They write of the vineyards and wine country inAvoca, musical heritage in Mason City and Clear Lake, anequestrian paradise in Warren County, and the “golfing, camping,picnicking, paddling, shooting, birding, hiking, hunting, biking…”in Polk County.
Iowans know that a great quality of life is essential if we aregoing to keep or lure back our talented young people. And ouryoung people must think so too. They were behind a number ofour Great Places invitations.
U of I Student Body President Mark Kresowik is the primarycontact for the Creative Corridor invitation. The YoungProfessionals group authored the invitation from Ft. Dodge. Andthe ISU Greek Community wants to build a better relationshipwith Ames and Campustown as a Great Place.
More than 75 coaches were dispatched last summer to everyplace that submitted a Great Places invitation. They workedwith the local teams to move the vision forward. The GreatPlaces Citizens Advisory Board visited 74 places to hearpresentations. In October, the Board selected Clinton, CoonRapids, and Sioux City as pilot places.
On Tuesday – Cultural Advocacy Day – Governor Tom Vilsackwill sign letters of agreement with the pilot places. Theagreement creates a work plan for each community that bringstogether state resources and local assets to turn vision into reality.
Overall, however, every one of the 146 places that extended aninvitation to Great Places will benefit from this initiative throughthe coaching process, new training opportunities, and the chanceto come together as a community and focus on the future.
That’s happening already in Davenport, which calls itself Iowa’sfront porch; in Council Bluffs, where Donna Kinney writes, “HereI am, just another Iowan who loves to brag about the beautifulhills, trails, and of course the friendly people who live here inCouncil Bluffs, Iowa.”
Iowans have set aside their signature modesty, thought aboutwhat’s good and great about our state, and with the brass of 76trombones, blown their own horns. That takes confidence,creativity, and vision. And that is the first step towardtransforming what’s good to Great Places in Iowa.
Please visit www.iowagreatplaces.gov or contact CyndiPederson at 515-281-3223 or [email protected] formore information about the Iowa Great Places program.
About the Author:Anita Walker is Director of the Iowa Department of Cultural Affairs,600 E. Locust Street, Des Moines, IA 50319; 515-281-7471;[email protected].
(Great Places - continued from p.9)

Vol 13 NO. 1, Spring 2006 PAGE 11A S P R
Medical Marketing ServiceASPR Bronze Contributor
Pinpoint perfect prospects for your promotions with thebest lists of physicians, health professionals, pharmacists,and managers for direct mail, Med-E-MailSM, broadcast faxand telemarketing, including:
Physicians• American Medical Association (AMA)• American Osteopathic Association (AOA)• American Academy of Pediatrics (AAP)• Physicians Willing to Relocate
Health Professionals• American Academy of Physician Assistants (AAPA)• Nurse Practitioners from Verispan
Pharmacists• American Pharmaceutical Association (APhA)• American Society of Health-System Pharmacists (ASHP)
Managers• America’s Health Insurance Plans (AHIP)• American Society of Medical Administrators (AAMA)
Our NOWW system lets you run counts and downloadAMA physician lists on the Web 24/7/365.
For more information:Call 1-800-MED-LIST (633-5478)E-mail [email protected]
© 2006 Medical Marketing Service, Inc. Pinpointing perfect prospects for more than 75 years.
HOW CAN WE MAKE OUR INTERVIEWS FLOW AS WELL AS THECONVERSATIONS AT THE LOCAL STARBUCKS?by Laura Screeney, CMSR
As I look back at all of the interviews I've conducted over the years,I begin to think, “Why do some interviews have the same type ofgreat rhythm that I would have with a friend, over a cup of coffee/tea; while others bring back memories of my worst blind dates?”
Now, we all know that to conduct an effective interview, we needto pay attention to the key elements: Be prepared, develop agood rapport, ask good questions, listen to the answers, andfollow up in a timely manner.
Lately, I am trying to concentrate on effective and attentive listening.I am working on turning off the other million and one tasks that arefloating around in my head and giving the candidate, and mystaff, my undivided attention. I am re-evaluating the questions Iask. Do I formulate my questions as I am reviewing the CV inadvance, or do I just wing it? And, am I effectively communicatingto my staff on how our interviews can run more fluidly?
I was recently participating in an interview with a departmentthat I had not worked with in a while. As the interview movedforward, the staff used a set of standard interview questions thatwere on a sheet of paper that most had placed on the table infront of them. As they asked our candidate questions, most ofour staff were reading verbatim from their notes, rarely lookingthe candidate in the eye, and then scribbling the candidate’sresponses intently on their notepads while the candidate wasspeaking. I was so busy watching the staff that I am sure I misseda lot of what the candidate had to say, and I am not really sure
how much the staff was activelylistening either.
Our interviews should be as wellchoreographed as the NYC Ballet.We should make sure everyparticipant knows his/her role in theinterview. And, if we are lucky enoughto have a department that is stable, itis our responsibility as recruitmentprofessionals to remind all involved oftheir roles in the process and howimportant it is to actively listen. We alsoneed to be able to continue theconversation in the car, the airport, thehotel lobby, etc, and, don’t forget, we need to do the same with his/her spouse or significant other during the site visit, as well. So,how do we keep that fresh interview after interview?
How can I prevent myself from zoning out? Sometimes I getupset with myself because I am thinking about my “to do” list,grocery shopping, the weekend, or if we have enough articlesfor the ASPR newsletter this quarter. So, did I zone out becauseI have a lot on my mind, did not get a good night’s sleep the nightbefore, or is the candidate someone with whom we (the practice)have nothing in common, thus, not a “good fit” for our Group?
Laura Screeney
(Interviews - continued on p. 12)

Vol 13 NO. 1, Spring 2006PAGE 12 A S P R
We need to find some common ground with each person weinterview, and we need to work with our staff to do the same.Maybe we grew up in the same geographic area, went to thesame college, have some of the same interests? We both likemovies, baseball, have kids, ski, like to travel, have attended aconference in their town/city. When we connect with a candidate,it helps the candidate feel more comfortable, thus allowing thecandidate to be himself/herself, which helps us to get to knowhim/her better.
The reality is that every candidate is not a good fit for the practiceswe represent, and we are not always the ideal practice for everycandidate we meet. However, if we pay attention to our listeningskills and work with our “recruiting team” to do the same, ourodds of finding a good, long term employee for our practiceincreases. If a physician is not going to work out, hopefully theinterview was enjoyable and he/she is one more person we hadthe pleasure to meet, and the honor of spending time with. Let’sface it, didn’t we all choose the recruitment profession becausewe are social, enjoy meeting new people, and are fulfilled bymatching an outstanding candidate with an excellent practice?
So, let us continue to enjoy each new candidate as if we are havinga cup of coffee with a friend at Starbuck’s…happy listening…
About the Author:Laura Screeney is a physician recruiter based in Santa Monica, CA.She has been in recruiting for close to 20 years, has been a member ofASPR since its inception, and is Co-chair of the ASPR NewsletterCommittee. [email protected].
(Interviews- continued from p.11)

Vol 13 NO. 1, Spring 2006 PAGE 13A S P R
The high cost of malpractice insurance for some medicalspecialties affects not only how many doctors are entering thefield of obstetrics and gynecology, but also where they offer theirwidely needed obstetric, prenatal, and gynecological care,according to new University of Michigan Health System research.
Their study, published in the June 2005 issue of journalObstetrics & Gynecology, (vol. 105, issue 6) gives a forebodingprognosis for the supply of doctors specializing in the fieldbecause of the rising costs of malpractice premiums.
“The high cost of malpractice premiums is beginning to leadproviders to drop or reduce obstetrical services. Our studypresented evidence that high malpractice premiums affect wherenew obstetricians are locating and it may affect the supply inthe future,” says Scott B. Ransom, D.O., M.B.A., M.P.H.,associate professor of obstetrics and gynecology at the U-MMedical School and of health management and policy at the U-M School of Public Health, and senior author of the paper.
“Our study shows that there is legitimate reason for concernabout patients’ access to obstetric care and prenatal care in thefuture,” he says.
Some of the potential problem areas include states with thehighest malpractice premiums, including Florida, Nevada,Michigan, New York, and the District of Columbia. Researchersalso found signs for problematic future supply of obstetriciansin several counties containing populous cities such as DadeCounty, FL, Wayne County, MI, and Cook County, IL, which allhave high costs of malpractice insurance.
Ransom says he hopes this study and others dealing with similarissues can inspire policy changes and tort reform that help reignin the cost of liability insurance for obstetrics/gynecology andother fields.
“Something has to be done about the skyrocketing cost ofmalpractice premiums in our field,” says Ransom, also thedirector of women’s health and gynecology at the Ann Arbor VAHealthcare Center and director of the U-M Program forHealthcare Improvement and Leadership Development. “Weare going to lose some of the best and brightest young doctorswho otherwise might enter this field, and we are going to faceshortages in many areas of the country if something isn’t done.”
The researchers compared the rates of births per fellow andjunior fellow members of the American College of Obstetriciansand Gynecologists (ACOG) in states that have the highest costof malpractice insurance and states at the other end of thespectrum.
HIGH COST OF MALPRACTICE INSURANCE THREATENSSUPPLY OF OB/GYNS, ESPECIALLY IN SOME URBAN AREAS
UMHS study finds premium rates affect where ob/gynschoose to practice; could have major impact on urban areas
Reprinted with permission of the University of Michigan Health System.
They found that the rate of increase in births-per-junior fellow inthe 10 highest-premium states was far greater (a median of28.5 percent) than the rate of increase in the 10 lowest-premiumstates (a median of 5 percent) from 1995 to 2002. That indicatesthat the supply of obstetricians is not keeping up with the needfor doctors in this specialty in the highest-premium states, sayslead author Pamela Robinson, M.B.A., a student at the U-MMedical School.
The researchers also found that in general, most counties inthe United States experienced decreases in the number of birthsper ob/gyn, indicating an improvement in the supply of doctorsin the field. But they also found that the six highest-premiumcounties had a slightly lower rate of decrease in births per ob-gyn than the other counties in the nation. While not statisticallysignificant, this result could hint at a worse situation in meetingthe ob/gyn needs in these areas.
Malpractice insurance premiums vary widely from state to state.Florida is the highest-premium state, with an average 2004premium of more than $195,000, followed by Nevada, Michigan,the District of Columbia, Ohio, Massachusetts, West Virginia,Connecticut, Illinois, and New York.
The 10 lowest-premium states are Oklahoma, at about $17,000on average, and Nebraska, South Dakota, Minnesota, Indiana,Idaho, North Dakota, Wisconsin, Arkansas, and South Carolina.
Many areas of the country, especially around major metropolitanareas, are experiencing large increases in the average costs ofpremiums. Between 2003 and 2004, Dade County in Florida,which includes the city of Miami, went from $249,000 to$277,000, an increase of about 11 percent.
In that same period, Cook County in Illinois, which includesChicago, jumped about 67 percent from $138,000 to more than$230,000. Wayne County in Michigan, which includes Detroit,went up 18 percent, from almost $164,000 to nearly $194,000.
The issue of how rising malpractice rates are impacting theobstetrics and gynecology profession has been a topic ofnational concern in recent years. It has received widespreadattention both in the media and in the discussions and writingsof health care professionals.
The reasons for the rising costs in this specialty are myriad, butRansom notes that a partial explanation is that “everybody wantsand expects a perfect baby,” leading many people to sue whenthe reality doesn’t match their expectation.
(Malpractice - continued on p. 14)

Vol 13 NO. 1, Spring 2006PAGE 14 A S P R
Another facet of the discussion relates to patient safety. Thiswas the subject of an editorial in Obstetrics & Gynecology inMay, written by Mark D. Pearlman, M.D., professor and vicechair in the Department of Obstetrics and Gynecology andprofessor of surgery at the U-M Medical School; and Paul A.Gluck, M.D., of the University of Miami School of Medicine.
Pearlman and Gluck wrote about the threat to the supply of ob/gyns, and said that doctors in the specialty should focus onincreasing patient safety.
“As a specialty, we are threatened. Rising malpracticepremiums, lower job satisfaction, intrusion of policy makers andinsurance companies demanding better service and accesswhile providing fewer resources, and decreased interest inobstetrics and gynecology among senior medical students poseformidable challenges,” Pearlman and Gluck wrote.
“Our specialty should position itself among the leaders of thepatient safety movement. Engaging ourselves fully in this effortis not only our moral imperative, it will bring us back to whatmotivated us to go into obstetrics and gynecology—to helpwomen get well and stay well.”
Funding for the research was provided in part by the U-M MedicalSchool Summer Biomedical Research Program and theDepartment of Obstetrics and Gynecology.
Reprinted with permission of the Univ. of Michigan Health System
Talent Matters.
I N T E G R A T E D T A L E N T S O L U T I O N S f o r H E A L T H C A R E
Physician recruiting challenge? We’ll help you find the answer.
In today’s competitive market, the challenges facing physician recruiting professionals often require unique solutions. And, people who can come up with the right answers. Enter Karen Hart, Hodes Health Care Division leader. As a former executive director of NAHCR, director of nurse recruitment, and a nurse who held clinical staff and management positions, Karen is adept at solving the most puzzling of health care recruiting problems. With the support of hundreds of local Hodes recruitment specialists across the country, she’ll deliver the right answer - no matter how difficult the question.
www.hodes.com/healthcare 800 582 4668Marketing Metrics Retention Consulting Benchmarking Interviews Research Mystery Shops
Karen Hart, RN, BSN
SVP, Hodes Health Care Division
Crossword Connoisseur
(Malpractice - continued from p. 13)

Vol 13 NO. 1, Spring 2006 PAGE 15A S P R
SKYROCKETING MALPRACTICE PREMIUMS CAUSE OFOB/GYN CRISIS?by Kathie Lee, Conway Medical Center, Conway, SC
Think Again, says Civil Justice Advocacy Group.
Not everyone is convinced that climbing malpractice premiumsare forcing OB/GYNs to relocate or leave the profession entirely.The Center for Justice & Democracy, a not-for-profit publicinterest organization based in New York City says the facts tella different story.
According to CJ&D, obstetricians and gynecologists are thesecond highest paid professionals in the country. They cite theU.S. Department of Labor’s most recent report that listsobstetricians and gynecologists as the second highest paidoccupation, behind surgeons. “The seven highest-payingoccupations . . . were all doctors,” out-ranking both corporateCEOs and lawyers.1
The net income of obstetricians and gynecologists is more eachyear - $256,020 – than the lifetime cap they seek to impose onvictims of medical malpractice. Moreover, the group says, theamount that ob/gyns pay for medical malpractice insurance is,on average, only 12.4 percent of their gross income.2
CJ&D says the U.S. General Accounting Office has found thatob/gyns have made false or wildly exaggerated claims abouthow their malpractice problems have limited access to healthcare.3 CJ&D says a 2003 report by the General AccountingOffice disputes physicians’ claims of a crisis due to the currentlegal system:
In Florida, “hospital association representatives reported thataccess to newborn delivery services in Florida had beenreduced due to the closures of five hospital obstetrics units.However, GAO contacted each of these facilities anddetermined that . . . for each now closed obstetrics facilityhad been low and that nearby facilities provided obstetricalservices.”
In Nevada, “34 ob/gyns reported leaving, closing practices,or retiring due to malpractice concerns; however, confirmatorysurveys conducted by the Nevada State Board of MedicalExaminers found nearly one-third of these reports wereinaccurate – 8 were still practicing and 3 stopped practicingdue to reasons other than malpractice. Random calls GAOmade to 30 ob/gyn practices in Clark County found that 28were accepting new patients with wait times for appointmentsof three weeks or less.”
In West Virginia, “although access problems reportedlydeveloped because two hospital obstetrics units closed dueto malpractice pressures, officials at both of these hospitalstold GAO that a variety of factors, including low service volumeand physician departures unrelated to malpractice,contributed to the decisions to close these units. One of thehospitals recently reopened its obstetrics unit.”
The Center For Justice & Democracy is a tax-exempt non-profit,non-partisan public interest organization that works to educatethe public about the importance of the civil justice system andthe dangers of so-called “tort reforms.”
NOTES:1 U.S. Department of Labor, Bureau of Labor Statistics, OccupationalEmployment and Wages, 2002 (Nov. 19, 2003); see also “Feds SayYou’re Well Paid,” American Medical Association News, Nov. 17,2003, at http://www.ama-assn. Org/amednews/2003/11/17/prca1117.htm.
2 American Medical Group Management, 2003 Medical GroupCompensation and Productivity Survey. Average grosscompensation is typically approximately 200% of net compensation.Average gross compensation is based on expense data by specialtyin Practice Expenses, Medical Economics, Nov. 7, 2003.
3 General Accounting Office, Medical Malpractice: Implication of RisingPremiums on Access to Health Care, GAO-03-836 (Aug. 8, 2003),http://www.gao.gov/new.items/d03836.pdf.
About the Author:Kathie Lee is Director, Medical Staff Development, Conway MedicalCenter, 200 Singleton Ridge Road, Conway, SC 29526. Phone 843-234-5139; Email [email protected].

Vol 13 NO. 1, Spring 2006PAGE 16 A S P R
NASA employs some of the smartest and most dedicatedprofessionals in the world. Individually they are the cream ofthe crop in their various science, engineering, and administrativedisciplines. Their collective achievements have dramaticallyexpanded the boundaries of our knowledge of both our universeand our world. And yet, in spite of their individual dedicationand collective brilliance, on February 1, 2003, seven astronautsdied—perhaps unnecessarily—when the Columbia ShuttleMission STS-107 incinerated on reentry into the earth’satmosphere. The reason? A key contributor to the tragedy wasa culture that “prevented effective communication of criticalsafety information and stifled professional differences ofopinion.”1 People’s inability to confront risky topics allowed risksto go unaddressed contributing to the loss of seven lives.
Those who serve daily in U.S. hospitals could be described assimilarly intelligent and dedicated. In the aptly titled report ToErr is Human2, the Institute of Medicine acknowledges both theindividual dedication and collective contributions of those whogive their all to improve and save the lives of patients in ourhealthcare institutions. And yet, as the report points out, eachyear hundreds of thousands of patients are brought to harm inthe course of their healing because of fundamental problems inthe collective behavior of these caring professionals. Theseproblems are not unlike those that contributed to the loss ofColumbia. For example, each year one in twenty in-patients athospitals will be given a wrong medication, 3.5 million will getan infection from someone who didn’t wash his or her hands ortake other appropriate precautions3, and 195,000 will diebecause of mistakes made while they’re in the hospital.4
Hospitals are responding aggressively to this crisis with newtechnologies, quality improvement systems, and methods oforganizing. However, though the healthcare community is takingneeded action on a number of fronts, there is a deeper problemthat must be resolved before acceptable levels of improvementwill be attainable.
As with NASA personnel, key problems that contribute to thesetragic errors are often known far in advance. And yet, few peopletalk about them. Every day, many healthcare workers standnext to colleagues and see them cut corners, make mistakes,or demonstrate serious incompetence. But only a smallpercentage speak up and discuss what they have seen—eventhough they’re standing only a few feet away. As a result,problems go on for years—contributing to avoidable errors, highturnover, decreased morale, and reduced productivity. Just asthe unwitting behavior of well-intended NASA personnel servedto suppress key information that might have escalated risks,many healthcare workers tend to act in ways that allow risksand problems to remain unaddressed—sometimes for years.
A group of eight anesthesiologists agree a peer isdangerously incompetent, but they don’t confront him.
Instead, they go to great efforts to schedule surgeriesfor the sickest babies at times when he is not on duty.This problem has persisted for over five years. (FocusGroup of Physicians)
A group of nurses describe a peer as careless andinattentive. Instead of confronting her, they double checkher work—sometimes running in to patient rooms to retakea blood pressure or redo a safety check. They’ve “workedaround” this nurse’s weaknesses for over a year. Thenurses resent her, but never talk to her about theirconcerns. Nor do any of the doctors who also avoid andcompensate for her. (Focus Group of Nurses)
Past studies have indicated that more than 60 percent ofmedication errors are caused by mistakes in interpersonalcommunication. The Joint Commission on Accreditation ofHealthcare Organizations suggests that communication is a topcontributor to sentinel events.5 This study builds on thesefindings by exploring the specific concerns people have a hardtime communicating that may contribute to avoidable errors andother chronic problems in healthcare.
The study we report here suggests that there are seven crucialconversations that people in healthcare frequently fail to holdthat likely add to unacceptable error rates. The nationwide studywas conducted by VitalSmarts in partnership with the AmericanAssociation of Critical-Care Nurses. This study suggests thatimprovement in these seven crucial conversations could notonly contribute to significant reductions in errors, but also toimprovements in quality of care, reduction in nursing turnover,and marked improvement in productivity.
In addition, we will offer healthcare leaders a simple method formeasuring their current performance in these seven crucialconversations, as well as an action plan for making measurableimprovement in this key competency.
The StudyResearchers conducted dozens of focus groups, interviews, andworkplace observations, and then collected survey data frommore than 1,700 respondents, including 1,143 nurses, 106physicians, 266 clinical-care staff, and 175 administrators during2004. Their research sites included thirteen urban, suburban,and rural hospitals from across the U.S. These included a mixof teaching, general, and pediatric hospitals. Although this is amodest sample, the findings fit together in a significant andcompelling way.
The study identified the categories of conversations that areespecially difficult and, at the same time, especially essentialfor people in healthcare to master. The study showed that thequality of these crucial conversations relates strongly withmedical errors, patient safety, quality of care, staff commitment,
SILENCE KILLS: The Seven Crucial Conversations forHealthcare (2005 VitalSmarts Research Study)by David Maxwell, Joseph Grenny, Ron McMillan, Kerry Patterson, Al SwitzlerReprinted with permission from VitalSmarts, 282 West River Bend Lane, Suite 100, Provo, Utah, 84604. www.silencekills.com.

Vol 13 NO. 1, Spring 2006 PAGE 17A S P R
employee satisfaction, discretionary effort, and turnover. Wegrouped these concerns into seven areas: Broken Rules,Mistakes, Lack of Support, Incompetence, Poor Teamwork,Disrespect, and Micromanagement.
More than half of the healthcare workers surveyed in this studyhad occasionally witnessed broken rules, mistakes, lack ofsupport, incompetence, poor teamwork, disrespect, andmicromanagement. Many had seen some of their colleaguescutting corners, making mistakes, and demonstrating seriousincompetence. However, even though they had these concerns,fewer than one in ten fully discussed their concerns with thecoworker. Furthermore, most healthcare workers neither believeit’s possible, nor even their responsibility, to call attention tothese issues.
About half of respondents say the concerns have persisted fora year or more. And a significant number of those who havewitnessed these persistent problems report injuriousconsequences. For example, one in five physicians say theyhave seen harm come to patients as a result of these concerns,and 23 percent of nurses say they are considering leaving theirunits because of these concerns.
On the positive side, this study shows that healthcare workerswho are confident in their ability to raise these crucial concernsobserve better patient outcomes, work harder, are moresatisfied, and are more committed to staying. About 10 percentof the healthcare workers surveyed fall into this category. Whileadditional confirming research is needed, the implication is thatif more healthcare workers could learn to do what this influential10 percent seem to be able to do systematically, the result wouldbe significantly fewer errors, higher productivity, and lower turnover.
Prevalence of the Seven Most Crucial ConcernsParticipants were asked to indicate the percentage of theircoworkers with whom they had each of the seven crucialconcerns. They had to indicate that at least 10 percent of theircoworkers were in violation to be categorized as “seeing theconcern.” It is important to point out that respondentsconsistently report that the vast majority of healthcare workersdo not exhibit the problems described below. And yet, the vastmajority of healthcare workers do see some number who notonly exhibit the problems, but also continue to do so for longperiods of time without being held accountable.
1. Broken Rules: 84 percent of physicians and 62 percent ofnurses and other clinical care providers see some numberof their coworkers taking shortcuts that could be dangerousto patients. This concern was focused on a relatively smallnumber of their colleagues. The median was 10 percent,meaning that they were comfortable with 90 percent of theircolleagues’ ability.
“A phlebotomist in a neonatal unit would slip on hergloves and immediately tear the tip of the index fingeroff her glove, so she could feel the baby’s vein betterand wouldn’t miss. I talked to her about it twice. FinallyI said, ‘If I ever see you tear the finger out of anotherglove I will write you up for a willful violation.’ Now shefollows the rules.” (Nurse Manager)
2. Mistakes: 92 percent of physicians and 65 percent ofnurses and other clinical-care providers work with somepeople who have trouble following directions; 88 percent ofphysicians and 48 percent of nurses and other clinical careproviders see some colleagues show poor clinical judgmentwhen making assessments, doing triage, diagnosing,suggesting treatment, or getting help. Again, theserespondents are pointing to a relatively small minority oftheir colleagues—the median was again just 10 percent.
“Some docs can make incorrect orders. We let it slide—especially if it is a jerk . . . For example, one physicianprescribed a drug that you should give three times aday, but he said to give it twice a day. I let it go, becauseit was just a pain pill. It wasn’t going to make the childany sicker.” (Pharmacist.)
3. Lack of Support: 53 percent of nurses and other clinicalcare providers report that 10 percent or more of theircolleagues are reluctant to help, impatient, or refuse toanswer their questions. 83 percent have a teammate whocomplains when asked to pitch in and help. On the positiveside, 76 percent say that half or more of their colleaguesgive them emotional support when they are down, and 64percent say that half or more of their colleagues pick up ashare of their work when they need help. It’s clear thatmost people provide support. The problem is with a smallminority who don’t.
“Some people here are burnt out. They’ve lost theexcitement or have some personal issue in their life . . .People have to cover for them, pick up their slack.People get mad at them, isolate them, don’t offer to helpthem, shy away from them. If they need extra help,they don’t get it. They don’t call or ask for it.” (Nurse)
4. Incompetence: 81 percent of physicians and 53 percentof nurses and other clinical care providers have concernsabout the competency of some nurse or other clinical careprovider they work with; 68 percent of physicians and 34percent of nurses and other clinical care providers haveconcerns about the competency of at least one physicianthey work with.
“There is a cardiologist who everybody feels isincompetent. He makes himself very accessible togeneral practitioners, so he gets a lot of referrals, butthose of us who have to work with him—the thoracicsurgeons, the anesthesiologists, the othercardiologists—would never put someone under hiscare.” (Physician)
5. Poor Teamwork: 88 percent of nurses and other clinicalcare providers have one or more teammate who gossips oris part of a clique that divides the team. 55 percent have ateammate who tries to look good at others’ expense.
“We have a nurse who is like your eccentric aunt—she’sa bully. She makes unreasonable demands like, ‘I won’ttake any more patients today.’ She gets away with it.
(Silence Kills - continued on p. 18)

Vol 13 NO. 1, Spring 2006PAGE 18 A S P R
(Silence Kills - continued from p.17)
She’s a very good nurse, but she’s ornery and a bully.She doesn’t do her fair share. It ticks all of us off. We’velost a couple of good nurses here because they weresick of putting up with her and our supervisor won’t dealwith her.” (Nurse)
6. Disrespect: 77 percent of nurses and other clinical careproviders work with some who are condescending, insulting,or rude. 33 percent work with a few who are verballyabusive—yell, shout, swear, or name call.
“A group of physicians went right into the patient’s roomwithout gowns, masks, or gloves. This was a patientwho was supposed to be in isolation. We didn’t confrontthem because that cardiosurgeon has a reputation. Hebelittles nurses by saying things like, ‘Do they have anynurses on this unit who aren’t stupid?’ If you questionhim, he starts yelling, and turns it into a war.” (Nurse)
7. Micromanagement: 52 percent of nurses and other clinicalcare providers work with some number of people who abusetheir authority—pull rank, bully, threaten, or force their pointof view on them.
“We have a charge nurse who . . . pages us to come tothe desk so she can tell us what to do . . . She will comeinto the room where we have a sick patient and she’lltake over . . . She’ll say, ‘Do it because I say so.’Sometimes, when she bosses me around I feel less
inclined to correct her when she’s wrong about how totreat the child. I’m sure I’ve gone along with somethingI shouldn’t have because I resent her. But basically,I’ve started looking at other hospitals for a job.” (Nurse)
The Impact of these Crucial ConversationsMost healthcare respondents are happy in their careers andbelieve their organizations do good work. And yet, mostrespondents report that a number of their colleagues createproblems that are common, frequent, persistent, and dangerous.And, most important, the data show these problems are rarelyaddressed.
The study focused in detail on three of the seven crucialconversations: incompetence, poor teamwork, and disrespect.In these three areas the study mapped the frequency, duration,and impacts of people’s concerns. It also measured whetherand how these concerns were addressed.
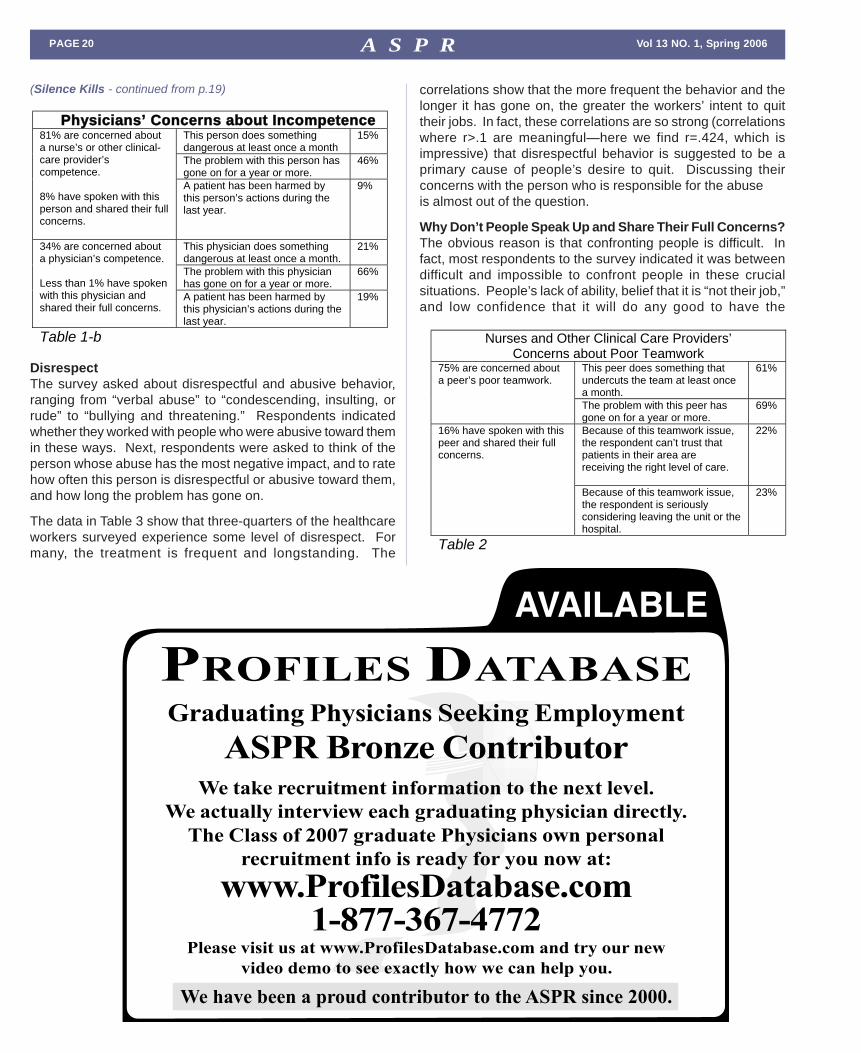
IncompetenceThe survey asked about a variety of competency issues, rangingfrom “poor clinical judgment” to “making decisions beyond theircompetency level,” to “missing basic skills.” Respondentsindicated whether they had coworkers who are incompetent inthese areas. Next, respondents were asked to think of thecoworker with the worst competency problem, and to rate howoften this person does something dangerous, how long theproblem has gone on, and how the person’s competency hasimpacted patient health and safety.

Vol 13 NO. 1, Spring 2006 PAGE 19A S P R
The data in tables 1-a and 1-b reveal the scope of the problem.Most healthcare workers have serious concerns about thecompetence of some of their coworkers. In fairness, a person’sperceptions of another’s competence can sometimes be just adifference of judgment—and nowhere more than in a field ascomplex and often ambiguous as healthcare. And yet, theprevalence of the perceptions, along with strong anecdotal datafrom focus group interviews, suggest that real problems exist.Many cite a coworker who does something dangerous as oftenas every month. Nearly half report the problem has continuedfor a year or more. Some have witnessed the person causingharm to patients. And yet, only a small percentage discusstheir concerns with the person.
The data show it is much tougher to confront a physician thanto confront a nurse or other clinical care provider. Interestingly,the data also show physicians are about as unlikely to confrontnurses and other clinical-care providers as they are to confrontphysicians, even though their clinical authority would seem tomake it an easier discussion.
Poor TeamworkThe survey examined a variety of teamwork concerns, rangingfrom “gossiping” to “making themselves look good at yourexpense” to “not doing their fair share of the work.” Respondentsindicated whether they had coworkers who demonstrated poorteamwork in these areas. Next, respondents were asked to thinkof the coworker whose poor teamwork has the most negativeimpact, and to rate how often this person does something thatundermines the team, how long the problem has gone on, andhow the person’s poor teamwork has impacted patient care andemployee morale.
The data in Table 2 show a widespread problem. Three-quartersof the healthcare workers surveyed are concerned about ateamwork issue, and more than two-thirds say this problem hasgone on for over a year. A smaller—yet significant—number(one-fifth) say the teamwork issue is so severe they can’t trustthat patients are getting the right level of care, and even moreare seriously considering leaving their jobs because of theteamwork issue. And yet, relatively few ever discuss theirconcerns with the person involved.
Nurses and Other Clinical Care Providers’
Concerns about Incompetence
This peer does something dangerous at least once a month.
27%
The problem with this peer has gone on for a year or more.
48%
53% are concerned about a peer’s competence. 12% have spoken with this peer and shared their full concerns.
A patient has been harmed by this person’s actions during the last year.
7%
This physician does something dangerous at least once a month.
19%
The problem with this physician has gone on for a year or more.
54%
34% are concerned about a physician’s competence. Less than 1% have spoken with this physician and shared their full concerns.
A patient has been harmed by this physician’s actions during the last year.
8%
Table 1-a (Silence Kills - continued on p. 20)
Vol 13 NO. 1, Spring 2006PAGE 20 A S P R
Nurses and Other Clinical Care Providers’
Concerns about Poor Teamwork
This peer does something that undercuts the team at least once a month.
61%
75% are concerned about a peer’s poor teamwork.
The problem with this peer has gone on for a year or more.
69%
Because of this teamwork issue, the respondent can’t trust that patients in their area are receiving the right level of care.
22% 16% have spoken with this peer and shared their full concerns.
Because of this teamwork issue, the respondent is seriously considering leaving the unit or the hospital.
23%
Table 2
(Silence Kills - continued from p.19)
Physicians’ Concerns about Incompetence
This person does something dangerous at least once a month
15%
The problem with this person has gone on for a year or more.
46%
81% are concerned about a nurse’s or other clinical-care provider’s competence. 8% have spoken with this person and shared their full concerns.
A patient has been harmed by this person’s actions during the last year.
9%
This physician does something dangerous at least once a month.
21%
The problem with this physician has gone on for a year or more.
66%
34% are concerned about a physician’s competence. Less than 1% have spoken with this physician and shared their full concerns.
A patient has been harmed by this physician’s actions during the last year.
19%
Table 1-b
DisrespectThe survey asked about disrespectful and abusive behavior,ranging from “verbal abuse” to “condescending, insulting, orrude” to “bullying and threatening.” Respondents indicatedwhether they worked with people who were abusive toward themin these ways. Next, respondents were asked to think of theperson whose abuse has the most negative impact, and to ratehow often this person is disrespectful or abusive toward them,and how long the problem has gone on.
The data in Table 3 show that three-quarters of the healthcareworkers surveyed experience some level of disrespect. Formany, the treatment is frequent and longstanding. The
correlations show that the more frequent the behavior and thelonger it has gone on, the greater the workers’ intent to quittheir jobs. In fact, these correlations are so strong (correlationswhere r>.1 are meaningful—here we find r=.424, which isimpressive) that disrespectful behavior is suggested to be aprimary cause of people’s desire to quit. Discussing theirconcerns with the person who is responsible for the abuseis almost out of the question.
Why Don’t People Speak Up and Share Their Full Concerns?The obvious reason is that confronting people is difficult. Infact, most respondents to the survey indicated it was betweendifficult and impossible to confront people in these crucialsituations. People’s lack of ability, belief that it is “not their job,”and low confidence that it will do any good to have the

Vol 13 NO. 1, Spring 2006 PAGE 21A S P R
conversation are the three primary obstacles to directcommunication.
Other obstacles include time and fear of retaliation. The surveyasked respondents to indicate the reasons they didn’t confrontpeople when they had these important concerns. The reasonsthey selected were similar for each concern, with the mostcommon reasons being: “There wasn’t a time or opportunity,”“It’s not my role,” “I’ve seen them get angry,” and “I thought theywould retaliate.” People don’t want to make others angry orundercut their working relationships, so they leave difficultdiscussions to others or to another time, and never get back tothe person.
However, some people don’t remain silent about the problemsthey see. They talk about them with others. Depending on thenature of the problem, a quarter to half of the respondentsdiscussed the problem with coworkers or with the person’smanager. In interviews, participants suggested that the purposefor discussing these problems with coworkers is not to solveproblems. Instead, it’s to work around them, warn others aboutthem, and blow off steam. The comments below, taken fromfocus groups, illustrate these workarounds, warnings, andventing sessions.
“We all know who I’m talking about. She has bad habits,or is missing good ones. She gets busy and leaves therails down on an infant bed or the door open on anincubator. We all check on her patients just to makesure about things.” (Nurse)
Nurses and Other Clinical Care Providers’
Concerns about Disrespect and Abuse
This person is disrespectful or abusive toward them in at least a quarter of their interactions.
28%
77% are concerned about disrespect they experience.
The behavior has gone on for a year or more.
44%
Correlation between the frequency of mistreatment and intent to quit their job.
r = .424, p < .001
7% have spoken with this peer and shared their full concerns.
Correlation between the duration of abuse and intent to quit their job.
r = .190, p < .001
Table 3
“People give you the word. A nurse will call from surgeryand say, ‘He’s in a mood.’ If something goes wrong insurgery, he’ll come in yelling at people. You are justwaiting for your turn.” (Nurse)
“She can’t be trusted with cases. She can give meds,but she won’t ever get it. She’s been there for sevenmonths. This nurse would do fine in a doctor’s office,but won’t make it in the hospital. The other nurses allagree.” (Nurse)
Most respondents also say going to the person’s managercreates problems.
(Silence Kills - continued on p. 22)
EEExxxccceeeppptttiiiooonnnaaalll RRReeecccrrruuuiiitttiiinnnggg... EEExxxccceeelllllleeennnttt RRReeesssuuullltttsss...
Adkisson Consultants
PO Box 5643 Bloomington IL 61702
Phone: 309-452-7200 ••• Toll Free: 866-311-0000
wefinddocs••• com

Vol 13 NO. 1, Spring 2006PAGE 22 A S P R
“I’m embarrassed. I saw a nurse cutting corners andinstead of talking to her I talked to her boss. Here’s thesituation. I used to be this nurse’s boss, but now she’straining me and we are peers. I should have gone toher, but I was concerned about our relationship and Iwent to her boss instead. It was a bad move.” (NursePractitioner)
The data suggest that going to the person’s manager is, indeed,a bad move. Although managers are somewhat more likelythan employees to confront the person and fully discuss theproblem, they are still very unlikely to do so. Taking a concernto a manager was often a dead end.
People Who Do Step Up to these Crucial ConversationsWithin each hospital there is a fascinating minority, 5–15 percentof healthcare workers, depending on the issue, who step up tothese crucial conversations. They work in the same units ordepartments as the 85–95 percent of their coworkers who don’tfeel able to speak up. Are they crazy? Are they destroyed by theunsafe environment? No; these people prove that it’s possible todiscuss serious concerns in almost any environment and succeed.
The significant correlations in Table 6 show that people who areconfident in their ability to have crucial conversations achievepositive outcomes for their patients, for the hospital, and forthemselves. This is counterintuitive. Most of those who don’tspeak up believe that to do so would lead to disaster. Theopposite seems to be the case for this critical minority ofinterpersonally skilled individuals. Again, the correlations of from.2 up to .465 suggest that these peoples’ ability to deal withtough interpersonal challenges is highly related to all of theoutcomes described. The “p<.001” means that the odds thatthis strong relationship is due to chance is less than 1 in 1000.
When the
Concern Is…
Percentage Saying It Is Difficult to
Impossible to Confront the Person
Incompetence 56% of Physicians 72% of Nurses and other Clinical-Care Providers
Poor Teamwork 78% of Nurses and other Clinical-Care Providers
Disrespect or Abuse 59% of Nurses and other Clinical-Care Providers
Table 4
These correlations make sense. People who feel able toconfront and resolve the problems they see, take action, andimprove the environment for everyone. Consider the twoexamples below. The first involves a physician who wasn’t ableto confront a peer.
“One surgeon actually left because of another’s lousywork ethic. You’d call him at one in the morning, andhe’d say, ‘It can wait till morning.’ The best member ofhis practice quit over it. No one ever made him shapeup or confronted him over it. Docs would talk about it,but not to him.” (Physician)
When problems are allowed to fester, morale and productivitysuffer, and patients are put at risk. Following is a contrastingexample from a physician who is comfortable confronting hispeer.
“I have a guy in my practice who is (acting in aninappropriate way) . . . It meant that his other partnersand I would have to work more nights. I spoke to him.It wasn’t easy, but he agreed to change.” (Physician)
People who are able to speak up and address the problemsthey see make a positive difference. This finding isn’t a bigsurprise. The surprise is how few healthcare workers speakup. The confident physician in the example above representsless than one in a hundred of the physicians in our sample.The other 99 percent live with their concerns and the badoutcomes they see around them.
When the
Concern Is…
Percentage of
Non-Supervisory
Employees Who
Confront the
Person
Percentage of
Supervisors Who
Confront the
Person
Competence of a Nurse or other Clinical-Care Provider
3%
16%
Competence of a Physician
Less than 1%
Less than 1%
Poor Teamwork 5%
9%
Disrespect or Abuse 2%
5%
Table 5
(Silence Kills - continued from p.21)

Vol 13 NO. 1, Spring 2006 PAGE 23A S P R
ConclusionsThe majority of the healthcare workers in this study have seriousconcerns about someone they work next to. Some share theseconcerns with coworkers and managers, but rarely speak directlyto the people they are concerned about. Few of their coworkersand managers approach these people either, so the problemscontinue with a high frequency and for a long time.
It is critical for hospitals to create cultures of safety, wherehealthcare workers are able to candidly approach each otherabout their concerns. The added benefits in productivityimprovement, reduction in nursing turnover, and physiciancooperation make improvement in this core competence anoverwhelmingly high leverage objective. However, it would bedangerous to conclude that the responsibility for breaking thispervasive culture of silence depends solely on making it saferto speak up. There are those in every hospital who are alreadyspeaking up, and they are not suffering for their outspokenness.Although they are only 5 to15 percent of the total, they are themost effective, satisfied, and committed in the organization.
Hospitals need to learn from this skilled minority. VitalSmartshas spent 10,000 hours observing these opinion leaders andcan recommend a series of steps for spreading their capabilitiesacross a hospital.
RecommendationsThe medical and business leaders of a hospital need to makeimproving crucial conversations one of their top two or three
Observe better patient outcomes (Spearman correlation = -.336, p < .001) Are more satisfied with their workplace (Spearman correlation = -.267, p < .001) Exhibit more discretionary effort6—work beyond the minimum required (Spearman correlation = -.240, p < .001)
Nurses and other clinical-care providers who are confident in their ability to confront people when the concern is Incompetence
Intend to stay in their unit and hospital (Spearman correlation = -.335, p < .001) Observe better patient outcomes (Spearman correlation = -.307, p < .001) Are more satisfied with their workplace (Spearman correlation = -.309, p < .001)
Physicians who are confident in their ability to confront people when the concern is Incompetence Exhibit more discretionary effort—work
beyond the minimum required (Spearman correlation = -.263, p < .001) Observe better patient care (Spearman correlation = -.310, p < .001) Have higher morale (Spearman correlation = -.465, p < .001) Exhibit more discretionary effort—work beyond the minimum required (Spearman correlation = -.297, p < .001)
Nurses and other clinical-care providers who are confident in their ability to confront people when the concern is Poor Teamwork
Intend to stay in their unit and hospital (Spearman correlation = -.460, p < .001) Are more satisfied with their workplace (Spearman correlation = -.271, p < .001) Exhibit more discretionary effort—work beyond the minimum required (Spearman correlation = -.203, p < .001)
Nurses and other clinical-care providers who are confident in their ability to confront people when the concern is disrespect or abuse
Intend to keep their job (Spearman correlation = -.258, p < .001)
Table 6
(Silence Kills - continued on p. 24)

Vol 13 NO. 1, Spring 2006PAGE 24 A S P R
(Silence Kills - continued from p.23)
priorities for at least a year. The reluctance to confront is sodeeply rooted in the healthcare culture that it will take this levelof attention to create lasting improvements. The AmericanAssociation of Critical Care Nurses points out that lasting changein challenging interpersonal communication practices like thesewill require the combined commitment of nurses and healthcareprofessionals as well as healthcare organizations.7
Enabling crucial conversations may involve a variety ofinterventions, depending on the obstacles and inertia presentin a hospital. Here we will focus on four steps that have providedrapid payoffs in many organizations.
Establish a Baseline and a Target for ImprovementThe fundamental principle of organizational attention is: If youdon’t measure it you don’t care about it. Survey the hospital toestablish a baseline measure of the seven crucial conversations,and set a clear target for improvement.8 A public goal for 25percent improvement in a one-year period is achievable, andwill concentrate attention on the issue. Update the baseline atleast four times a year so people can be rewarded and heldaccountable for progress.
Conduct Focus Group InterviewsForm interview teams that include top administrators and keyphysicians, and have these interview teams lead focus groups.It is important to have leaders, not staff, conduct these interviews.Leaders need to hear about the problems and their causesdirectly, and they need to demonstrate their willingness to listen.
The purpose of these interviews is to learn about the obstaclespreventing crucial conversations. The most common obstacleyou will hear is “safety;” people feel it is unsafe to confront.9
Leaders need to take this safety concern to heart, because it isa criticism aimed at them. The interviews should solicit specificfeedback about the kinds of behaviors and experiences peoplehave that lead them to conclude they should not step up tothese crucial conversations—or vice versa in areas where theconversations are happening.
“Everybody knows the cardiac surgeons can dowhatever they want because they bring in a lot of dollars.I was warned not to confront them.” (Nurse)
If a cardiac surgeon is preventing nurses from confronting himor her, it is only because a manager or another physician ispermitting it. These focus groups are an opportunity for leadersto learn about their role in allowing problems to continue.
Focus on Problem AreasUse the baseline survey to focus your efforts. The survey willshow you where conversations aren’t happening or aren’thappening well. Often, these are high-stress, high-impact areassuch as the emergency room, operating rooms, and intensivecare units. Focus on the intersection of “poor conversations”and “high impact.”
Form teams within these problem areas, and have medical andadministrative leaders participate. These teams should identifykey obstacles and develop solutions to test.

Vol 13 NO. 1, Spring 2006 PAGE 25A S P R
Implement TrainingA handful of the people in your hospital are already speaking upand resolving the problems they see around them. Trainingcan be a powerful way to help others speak up, but its successis far from guaranteed. Below are the most critical elements indetermining whether training will result in significantimprovements.
• Leaders teach. Leaders need to conduct the training.Research shows that line managers, even those selectedfor their poor teaching abilit ies, achieve greaterimprovements than highly rated professional trainers.10 Inaddition, having a leader teach a set of skills guarantees heor she will master them, and goes a long way towardensuring he or she will “walk the talk” and model the skills.
• Quality Materials. The training must employ an effectiveinstructional design. Participants need to be able tounderstand the concepts and master the behaviors. Theskills taught should be valid in the highly emotional and riskyconfrontations we’re asking people to step up to. Generic“communication” training will not suffice as the rules andchallenges change when these seven emotionally andpolitically risky topics emerge. In addition, the trainingactivities need to include emotionally compellingexperiences that cause participants to examine themselvesand recognize the need to change.11
• Spaced learning. Smaller chunks spaced a week or twoapart are far better than longer, more intensive chunks. Two-hour or four-hour workshops avoid the cognitive overload
so common in many training programs, and spaced learningallows people to apply and test the skills between sessions.
• Sustained attention. Some training interventions seemlike a race to the finish—as if the goal were to get everyonethrough the course as quickly as possible. In fact, sustaininga skill-building effort over time is more important than“finishing” it on deadline. Unless people stay in the learningprocess for four to six months, it won’t penetrate to theirdaily experience.
• Relevant. Obviously, the content of the training must relatedirectly to risky situations people need to confront. Generictraining in listening and feedback won’t help participantshandle the tough situations measured in our study. Practicesbuilt into the training should focus on the specific crucialconversations the individuals involved need to master.
The problem described in this study is severe. 1) People seeothers make mistakes, violate rules, or demonstrate dangerouslevels of incompetence 2) repeatedly 3) over long periods oftime 4) in ways that hurt patient safety and employee morale 5)but they don’t speak up and 6) the critical variable thatdetermines whether they break this chain by speaking up istheir confidence in their ability to confront. These results givehospitals a powerful tool for improving patient safety andemployeeperformance. The inability to speak up is an informationbottleneck. Finding and removing the bottlenecks will release acascade of benefits. Leaders can begin this process immediately,and achieve rapid and substantial progress.
(Silence Kills - continued on p. 26)

Vol 13 NO. 1, Spring 2006PAGE 26 A S P R
(Silence Kills - continued from p.25)
About the SponsorsVitalSmartsA global leader in organizational performance and leadership,VitalSmarts provides training and consulting services tothousands of organizations, including more than 300 of theFortune 500. For more than twenty-five years, the companyprincipals have researched methods for bringing aboutsystematic and lasting change. Crucial Conversations®,(including The New York Times bestselling book of the sametitle—McGraw-Hill 2002) delivers a set of influence tools thatvitalize companies, strengthen teams, improve communities,and enrich relationships. Borrowing from more than twenty-five years of research, VitalSmarts introduces its newest WallStreet Journal and New York Times bestselling title, CrucialConfrontations (McGraw-Hill 2004), as well as a new set oftraining tools that teach organizations, teams, and individualsto effectively deal with violated expectations in a way that solvesthe problem at hand and strengthens the relationship in the
process. VitalSmarts also offers other services includingkeynote speaking, on-site consulting, customized development,and executive mastery retreats.
AACNThe American Association of Critical-Care Nurses (AACN) isthe world’s largest specialty nursing organization. Representingthe interests of more than 400,000 nurses who care for criticallyill patients, AACN is dedicated to creating a healthcare systemdriven by the needs of patients and their families, where criticalcare nurses make their optimal contribution.
AACN defines critical care nursing as that specialty withinnursing that deals with human responses to life threateninghealth problems. The purpose of AACN is to promote the healthand welfare of those experiencing critical illness or injury byadvancing the art and science of critical care nursing andpromoting environments that facilitate comprehensiveprofessional nursing practice.
Endnotes1 Columbia Accident Investigation Board Report Volume 1 August
2003) 9.2 L. Kohn, J. Corrigan, M. Donaldson, eds., To Err is Human: Building
a Safer Health System (Washington, DC: National Academy Press,2000) 127.
3 Richard P. Wenzel and Michael B. Edmond, “The Impact of Hospital-Acquired Bloodstream Infections,” Emerging Infectious Diseases7, no. 2 (March–April 2001)
4 HealthGrades Quality Study: Patient Safety in American Hospitals,(HealthGrades, Inc., July, 2004).
If you'd like to find out what your style is when it comes to"crucial conversations," go to
http://www.crucialconversations.com.Click on the “Free Stuff” tab at the top of the Home Page.Next, click on “Sign up to take the Crucial ConversationsStyle Under Stress Test”. You will need to enter some de-mographic information and create a password.

Vol 13 NO. 1, Spring 2006 PAGE 27A S P R
5 Joint Commission on Accreditation of Healthcare Organizations,Root Causes of Medication Errors 1995-2003. http://www.jcaho.org/accredited+organizations/ambulatory+care/sentinel+events/rc+of+medication+errors.htm
6 “Discretionary effort” is a concept first introduced by DanielYankelovich in 1983 (Yankelovich and Immerwahr, Putting the WorkEthic to Work, Public Agenda Foundation). It is the engine ofproductivity in any knowledge-intensive organization. Discretionaryeffort is the gap between the least amount a worker can put inwithout being sanctioned or fired and the most they could put in ifthey chose to. In many professions this “discretionary effort” canaccount for productivity improvements of 100–500 percent whenan employee chooses to offer it.
7 AACN Standards for Establishing and Sustaining Healthy WorkEnvironments: A Journey to Excellence (American Association ofCritical Care Nurses: 2005) 40.
8 A downloadable survey of these seven crucial conversations isavailable at www.silencekills.com along with usage requirements.
9 A downloadable script and suggested structure for these interviewsis available at www.silencekills.com.
10 VitalSmarts research on using leaders as teachers.11 For information on VitalSmarts’ approach to Crucial Conversations,
www.silencekills.com.
Reprinted with permission from VitalSmarts, 282 West RiverBend Lane, Suite 100, Provo, Utah, 84604.www.silencekills.com.
CASPR - Canadian Recruiters Gather in MontrealOver 70 physician recruiters from hospitals and communitiesacross Canada met in Montreal on February 21st and 22nd forthe second annual conference of the recently-establishedCanadian Association of Staff Physician Recruiters’ (CASPR)conference. Organizers received very positive feedback onconference speakers, and topics. Attendees came from BritishColumbia, Newfoundland, the provinces in between and evenfrom as far away as Yellowknife.
Dr. Dale Dauphinee, Executive Director, Medical Council ofCanada, the conference’s keynote speaker, shared his thoughtson the evolution of Medical Workforce Policy Making in Canadaover recent years. Other guest speakers covered CulturalDiversity, Media Training, and How to engage your communityin physician recruitment. In addition, Dr. Tim Zmijowskyj, Headof the Division of Clinical Sciences, for the new Northern OntarioSchool of Medicine (NOSM), Canada’s first new medical schoolin 30 years, shared some of his exciting challenges and vastopportunities with the audience.
Organizers were strategic in selecting material and speakersfor the conference entitled “Today’s Physician Recruiter – ATool Kit for Success”. We felt it important to present speakersand topics that would provide relevant, hands-on informationthat could be applied to a physician recruiter’s daily challenges,”says Joan Hatcher, CASPR Chair, and Specialist PhysicianRecruiter for the Niagara Region. “The challenges recruitersface tend to be universal regardless of province, region orcatchment area.”
CASPR thanks its 2006 conference sponsors for their generoussupport and participation without which these annual eventswould not be possible.
One of the highlights of the Conference was the ProgressiveDinner held on Tuesday evening. Participants were taken bycoach bus to trendy Crescent Street in Montreal for an eveningof food, fun and networking with colleagues and sponsors.Appetizers at the Hard Rock Café and dinner at Weinstein andGavino’s was appreciated by all. The group then moved on toNewton, an upscale new restaurant owned by race car driverJacques Villeneuve for dessert and winding down. Some tookadvantage of the great weather to continue the night with newfriends at other spots on the street. CASPR is looking forwardto continuing with our professional growth and building on thenew friendships we’ve made at the recent Conference. It mayhave been cold, but we had a hot time!
REGIONAL PROGRAMS
Progressive dinner at Weinstein and Gavino's - Members having fun!
CASPR executives (L-R): Angela Sugden-Praysner, MargaretKennedy, Jill Cappa,Wayne Heide, Joan Hatcher. Missing: FrancesRoesch.
Conference CommitteeCo-chairs -Angela Sugden-Praysnerand Margaret Kennedy.
Vol 13 NO. 1, Spring 2006PAGE 28 A S P R
As our organization’s fiscal year is based upon the academicyear (July 1 – June 30), we are in the midst of the budget season.At this time of year, I am always surprised by the reality of theimpact of physician recruitment on our entire organization.Physician recruitment has a tremendous impact on budgetedrevenues and potentially the budgets of each of my colleaguesin the organization.
There are many different ways for a healthcare organization todevelop a budget and project revenues. The process at ourorganization seems to be one that many other organizationsutilize. Our budget process is to initially determine our projectedrevenues and then match our department budgets (expenses)to those budgeted revenues.
If you go back to school and look at basic business theory, ourphysicians and providers are our widgets. Without physiciansand other providers, we have limited revenue streams.
It is important to know how your employer develops itsorganization-wide budgets. What are the expectations for thenext year and what role does physician recruitment play in thoseexpectations?
1. What are the expectations of physician productivity,whether measured in visits, wRVUs, or charges?Are there expectations that each physician must meet aminimum level of productivity? If so, how will that impactthe physicians you are recruiting?
A physician you have been interviewing who spends 30minutes per scheduled patient may not meet the needs ofyour organization in terms of productivity. In turn, thatphysician may find your organization is not a good fit fortheir expectations either.
2. What are the expectations of total number of physiciansin the organization including the current provider staffand anticipated recruits?These projections on newly recruited physicians need tobe realistic. Are you going to hire 10 new primary carephysicians out of the 10 searches for a particular cliniclocation? Is it realistic that this next fiscal year you will behiring the trauma orthopedic surgeon you have been tryingto recruit for the past two years?
It is important that the Physician Recruitment Departmentis aware of these expectations. If some of the projectionsare not realistic, it is better to say so at the beginning of thebudget process versus being in the midst of the fiscal yearand finding out the organization is going to have budgetwoes based upon miscalculated projections.
THE IMPACT AND INFLUENCE OF PHYSICIAN RECRUITMENTON THE REVENUE STREAM AND BUDGET FOR AHEALTHCARE ORGANIZATIONby Judy Brown
3. When are these new providers budgeted (and expected)to join the organization?At the beginning of the new fiscal year is not very realistic.Most groups will project out expected revenues andexpenses for new providers for a partial year based uponprojections of when a new provider is anticipated to begintheir practice.
A new clinic start-up may have difficulties in meeting projectedbudgets if not all of the new physicians have been recruitedand begin in the timeframes projected. These differencesbetween projected start dates for new physicians and the realityof the start dates could mean the difference in thousands andsometimes hundreds of thousands of dollars in the revenuestream. That impact could be enormous.
Knowing how your organization develops its budget plan isimportant to you as a recruiter. If your organization’s budgetplan is based in part upon projections of physician placements,there is an implied expectation of your own performance. Arethese expectations realistic? Can you live up to theseexpectations? What is the impact of these expectations to youand your department?
Individuals on all levels of the organization, from CEO to ClinicManagers, could be basing in part their individual or organization-wide budgets upon the success of your recruitment program.
The assumption that you will place an orthopedic surgeoninfluences the projected budget for the Orthopedic DepartmentManager and Clinic Manager who may also be budgeting toadd support staff to accommodate this new physician, equipmentand rooms, and other related overhead. The RadiologyDepartment Manager may be budgeting to expand the radiologydepartment based upon anticipated increase in usage of theimaging equipment. On and on the cycle could go affectingalmost every department within an organization.
If you are not actively involved in your organization’s budgetprocess, I encourage each and every one of you to at least findout what assumptions are being made every budget year aboutphysician placements. It is one thing to budget for recruitmentand searches as many of us do with our own departmentalbudgets, it is another thing to budget and plan based upon theplacements (whether real or anticipated). The overall knowledgeof how the organizational budget is developed and theexpectations of physician recruitment will hopefully help you tobe successful in your recruitment efforts.
About the Author:Judy Brown is a Physician Recruiter at Columbia Park Medical Centerin Columbia Park, MN. She is also a member of ASPR and Co-Chairof the Newsletter Committee

Vol 13 NO. 1, Spring 2006 PAGE 29A S P R
The Endocrine Society Can Help Your Recruiting Efforts
WE OFFER:■ Classified Advertising ■ Web Advertising■ Free CV Database ■ Job Fair in June
To learn more, call 800.361.3906 or visitwww.endo-society.org/placementservices
We are at your service!
Can’t Find AnEndocrinologist?HERE’S WHERE TO LOOK

Vol 13 NO. 1, Spring 2006PAGE 30 A S P R
Minneapolis, here we come!
Spring is in the air and once again it istime to think about adding to yourrecruitment foundation by attending the
annual ASPR education conference. This year we return toMinneapolis which gives us the opportunity to access theamazing resources found in this medical corridor. We arefortunate to be able to tap into a wealth of healthcare expertswho are found in the Minneapolis area. Dr. Keith Lindor of theMayo Clinic is our keynote speaker, and he will talk to us abouteducating physicians to practice in a changing environment.We were also lucky to get the President/CEOs from three of thelargest health systems in the Minneapolis market to participatein a panel discussion on the future of healthcare.
Please take a close look at the brochure, as we have changedsome of the format to make the sessions more user friendlyand address the needs of our growing membership. We areoffering an afternoon breakout session on Monday, giving ourattendees three options to chose from, in addition to two optional
early bird breakfast meetings on Tuesday. It is our hope thateach attendee can choose topics that best fit his/her recruitingenvironment.
This year, in addition to the 101 course for new recruiters (andrefresher course for the more seasoned recruiter), we arelaunching the 201 course for the more seasoned recruiter. Bothof these programs are components of the ASPR fellowshipcertification.
And, we mustn’t forget the fun we have socializing with friendsold and new, and networking with members from across the USand Canada. Monday evening will find us at the Mill CityMuseum, enjoying good food and music while we learn aboutthe history of Minneapolis. Plus, there is a fabulous view of theMinneapolis skyline from the observatory!
Once again, ASPR is offering you a chance to “Add New Blocksto Your Recruitment Foundation”. We look forward to seeingyou in Minneapolis, August 13-16, 2006.
ASPR ANNUAL CONFERENCEby Cindy Bagwell and Michele Burke, Conference Committee Co-chairs
General Information
HotelHyatt RegencyROOM RATE: $141 SINGLE/DBL PLUS TAX --- ROOM RATE
1300 NICOLLET MALL
JULY 21, 2006 --- CUTOFF DATE
MINNEAPOLIS, MN 55403
PHONE: 800-233-1234AFTER 3:00 PM --- CHECK-IN
NO LATER THAN 12:00 NOON --- CHECK-OUT
ADDITIONAL ROOMS AVAILABLE ACROSS THE STREET AT:
Millennium Hotel1313 NICOLLET MALL
MINNEAPOLIS, MN 55403PHONE: 800-522-8856 OR 612-332-6000
Call the hotel directly for reservations. Mention ASPR toget the special room rate listed above.
*Reservations received after the cutoff date will beaccepted on a space and rate availability basis.
Shuttle ServiceSuper Shuttle is the recommended shuttle service betweenthe airport and the Hyatt. Estimated time is 20 minutes. Costis $14 one way or $20 round trip. Go to the Super Shuttlecounter on the baggage claim level of the airport fortransportation arrangements.
Directions From the Airport Exit the airport and followsigns to 494 West. Continue on 494 West to 35W North.Take the downtown 11th Street exit. Follow 11th Street to2nd Avenue. Take a left at 2nd Avenue. Turn right at NicolletAvenue.
Car RentalFor car rental discounts from Avis, call 800-331-1600 andrefer to our discount number J099683.
For More InfoContact Laurie at the ASPR office at 800-830-2777, or emailher at [email protected].

Vol 13 NO. 1, Spring 2006 PAGE 31A S P R
Adding New Blocks toYour Recruitment Foundation
The Eighteenth Annual Educational Forum
August 13-16, 2006The Hyatt Regency
Minneapolis, MN
Who should attend:New physician recruiters can lay the foundation for theirprofession by attending the 101 sessions. This also servesas a refresher and re-energizer for seasoned recruiters.
why you should attend this session:Network with colleagues from around the country.Training for in-house recruiters by in-house recruiters.State-of-the-art information about our industry.Tools for your recruiting toolbox.Find the best way to source candidates.Learn the secrets of an effective site visit.Obtain proven methods in screening candidates.Begin to create your own personal recruitment resourcelibrary.The 101 is one of the three components of the ASPRFellowship Program.
Here's what you'll get:A "how to" workbook.In-depth instruction from seasoned in-house recruitersand other experts in the field.A certificate of completion for "Physician Recruitment101."
What attendees have said:"Wonderful conference--very educational, great fornetworking!"
"Excellent day for validating what I have done in mycareer."
"Great conference for new recruiters.""Excellent planning and great handouts!""Very informative."
7:15 am Registration and Continental Breakfast
8:00 am Welcome ........ David Nyman, ASPR President
Moderators: Cindy Bagwell & Michele Burke
8:15 am Getting Organizedfor Recruiting ......................... Scott Lindblom
9:30 am Break
9:45 am Sourcing Candidates ............. Carol Sullivan,Donna Loy
11:30 am Lunch
12:00 pm Screening Candidates ............ Michael Griffin
1:00 pm Itinerary/Site Visit .......... Christine Bourbeau,Dana Butterfield
1:45 pm Break
2:00 pm Physician Immigration Primer . Greg Siskind
3:00 pm How to Determine Your RecruitingCosts Per Physician ............... Chris Kashnig
3:30 pm Panel: Questions for the Presenters
4:30 pm Adjourn and Exhibit Hall opens
6:00 pm Reception and hors d’oeuvres with theexhibitors in the Exhibit Hall
Physician Recruitment 101Sunday, August 13Jumpstart your recruitment process;
learn how to increase your effectiveness and productivity.

Vol 13 NO. 1, Spring 2006PAGE 32 A S P R
Monday, August 14
7:15 am ASPR Committee Meetings7:45 am Registration, Continental Breakfast with
Exhibitors
Main Sessions8:30 am Welcome ......... David Nyman, ASPR President
Moderators: Cindy Bagwell & Michele Burke
9:00 am KEYNOTE: EDUCATING PHYSICIANSTO PRACTICE IN A CHANGINGENVIRONMENT ..................... Keith Lindor, MDThis session will address the impetus for curricularchanges, and our evolving plans.
10:00 am Break in Exhibit Hall
10:30 am PANEL: HEALTHCARE EXPERTSMary Brainerd, President & CEO, HealthPartnersDavid Page, President & CEO, FairviewDick Pettingill, President & CEO, AllinaJeffrey Korsmo, Chief Administrative Officer,
Mayo ClinicHow can you prepare to get ahead of the curve?Listen to what these healthcare experts have tosay about changes they see for the future in thehealthcare environment.
12:00 pm Lunch in Exhibit Hall
1:30 pm CULTURALLY COMPETENT INTERVIEWING........................................................... Lila KellyThis will stimulate participants to expand their wayof perceiving the employment interview process.It will give insight into cultural misunderstandingsand unconscious biases that exist, and how diverseapplicants perceive that these play out in aninterview.
3:00 pm Break in Exhibit Hall
3:30 pm Simultaneous SessionsDEVELOPING MARKETING MATERIALS FORRECRUITMENT ................... Susan WadhwaniWhat information should you have on your table at anexhibit? How do you develop marketing materialsyourself? How do you work better with your marketingdepartment? Do you want to jazz up your brochureand make a better impact? Learn the who, what, when,where, and why of developing marketing materials forrecruitment.
RURAL RECRUITENTION ........... Tim SkinnerThis session emphasizes that successful recruitmentand retention of medical professionals to smallercommunities relies on the connection betweencommunity development and physician development.Physician recruitment is not an event that stands alone.In rural areas, a strategic process is essential.
REGIONAL DEVELOPMENTROUNDTABLES .........................Dennis BurnsJoin others who are interested in discussing stateand regional networks.
4:30 pm ADJOURN
Monday Evening Event5:30 pm The Monday evening dinner and social event is being
held at the Mill City Museum in Minneapolis. Bring yourdancing shoes, and join us in the Mill Ruins Courtyardfor some live music. Built within the limestone ruins ofthe Washburn A Mill - the National Historic Landmarkthat was once the centerpiece of the world's flour millingindustry - the museum tells the story of a mighty river, ayoung city, and how one product - flour - fueled thegrowth of Minnesota. It's a tale of hard and sometimesdangerous work, innovative technologies, big money,brilliant advertising campaigns, and even internationalespionage.
Enjoy a fabulous view of the Minneapolis skyline fromthe ninth floor observatory on a warm summer night!
Sign up on registration form. Note July 1 deadline.
Tuesday, August 15
7:15 am Early Bird SessionsSTARK ...................................... Ryan Johnson
IMMIGRATION ...... Bob Aronson, Greg SiskindLearn more about Stark and immigration laws forphysicians.
Main Sessions7:45 am Continental Breakfast in Exhibit Hall
Moderators: Cindy Bagwell & Michele Burke
8:45 am PHYSICIAN COMPENSATION............................................... Bradley VaudreyLearn more about compensation--the differenttypes and different ways physicians arecompensated; compensation for call and who’sasking for it, etc.
Educational ForumMonday - Tuesday, August 14-15

Vol 13 NO. 1, Spring 2006 PAGE 33A S P R
10:15 am Break
10:30 am PANEL: RESIDENTS AND NEWLYRECRUITED PHYSICIANSIncluded in this panel are a family physician whohas been in rural practice for 1 year, a residentjust out of training, a dermatologist in practice for2 years, and a general surgeon who has been inpractice for 8 years. Find out what worked inrecruiting them to their current positions, as wellas how they were sourced, what attracted them,what ads and websites caught their interest, howthey chose which job fairs to attend, and more.
11:30 am Break
Who should attend:The “101” has laid the foundation for recruiters. Now recruiterscan build on that base with the “201” program, which isdesigned to address topics important to compensation,orientation, relocation, and retention. This is also a part ofthe ASPR Fellowship program.
why you should attend this session:Network with colleagues from around the country.Training for in-house recruiters by in-house recruiters.Hear state-of-the-art information about our industry.Obtain tools for your recruiting toolbox.Find the best ways to court, close, and keep aphysician.Learn ways to develop a relocation policy while workingwithin the IRS guidelines.Review physician compensation and what’s necessaryto be competitive while remaining within your budget.Add to your personal recruitment resource library.The 201 is one of the three components of the ASPRFellowship Program.
Here's what you'll get:A "how to" workbook.In-depth instruction from seasoned in-house recruitersand other experts in the field.A certificate of completion for "Physician Recruitment201."
7:15 am Registration and Continental Breakfast
8:00 am Welcome ........ David Nyman, ASPR President
Moderators: Cindy Bagwell & Michelle Burke
8:15 am Provider Compensation & Incentive Plans;Salary Surveys ............. Deborah Pennington
9:30 am Break
9:45 am The Deal--Opening It, DevelopingRelationships, & Keeping itClosed .......... Marci Jackson, Denise Siemers
11:30 am Lunch
12:30 pm Specialty Accreditations &Certifications ......................... Scott Lindblom
1:30 pm Recruitment of Mid-levels & Non-physicianRelated Positions .................. Scott Lindblom
2:15 pm Break
2:30 pm Provider Orientation .... Deborah Pennington
3:30 pm How to Develop a RelocationPolicy & Procedure for YourDepartment .................... Christine Bourbeau,
Dana Butterfield
4:00 pm Retention Matters ....................... Tim Skinner
5:00 pm Adjourn
Program subject to change.
Physician Recruitment 201Wednesday, August 16
Broaden and enhance your knowledge base for recruitment.
11:45 am Lunch & ASPR Business Meeting
12:45 pm Prize Drawings in the meeting room
1:30 pm Break
1:45 pm PHYSICIAN SATISFACTION ..... David RowleeHow do you keep physicians satisfied? Do youneed more retention ideas? If you answered yes,this session is for you.
2:30 pm Break
2:45 pm PHYSICIAN SATISFACTION - cont’d
3:45 pm Adjourn

Vol 13 NO. 1, Spring 2006PAGE 34 A S P R
Enrollment is limited--register early. Early registration deadline is July 1.
NAME: _________________________________________________________
POSITION/TITLE: __________________________________________________
ORGANIZATION: ___________________________________________________
ADDRESS: ______________________________________________________
CITY/STATE/ZIP: __________________________________________________
PHONE: ___________________________ FAX: ________________________EMAIL: ____________________________
Eighteenth Annual Educational Forum ~ August 13-16, 2006
Adding New Blocks to YourRecruitment Foundation
For office use only.
Please complete all 5 sections below:
1-Monday - CONCURRENT SESSION SIGNUP - check 1:3:30 Developing Marketing Materials for Recruitment
Rural RecruitentionRegional Development Roundtables
2-Monday - RESERVATION - Evening Event at Mill City Museum - check 1:(JULY 1 RESERVATION DEADLINE)
5:30 Yes, I PLAN TO ATTEND
No, I AM UNABLE TO ATTEND
3-Tuesday - EARLY BIRD SESSION SIGNUP - check 1:7:15 Yes, I PLAN TO ATTEND (check one): ......... Stark .. Immigration
No, I DON’T PLAN TO ATTEND
4-REGISTRATION FEES: (Early registration deadline is July 1)Member Non-Member
Early Late Early LateSunday only .................. $300 ..... $330 .......... $525 .... $555Sunday-Tuesday ........... $475 ..... $505 .......... $700 .... $730Sunday-Wednes. .......... $625 ..... $655 .......... $850 .... $885Monday-Tuesday .......... $350 ..... $380 .......... $575 .... $605Monday-Wednes. ......... $500 ..... $530 .......... $725 .... $755Wednesday only ........... $325 ..... $355 .......... $550 .... $585
Early registrations must be Postmarked By 7/1. $ ____________Registrations postmarked after 7/1 are at the late rate
5-PAYMENT INFO: (Payment must be received to guarantee registration)Enclosed is $ _________ in payment of the meeting. Check payable to “ASPR.”Please charge my: Visa, Master Card $ _____ in payment of the meeting.
Card # _________________________________________ Exp. Date _________Credit Cardholder’s Name ____________________________________________Signature__________________________________________________________
Join ASPR Nowand attend for the member price. Get amembership application off the website.Mail your membership application withdues, and conference registration formwith registration fee to the ASPR office.
*Non-memberRegistrations:Individuals registering in the “non-member” category must be eligible formembership, but need not be a memberto attend.
Multiple RegistrationDiscount:A $15 per person discount may beapplied when four or more registrationsare sent together from the samecompany.
Registrations sent individually are notdiscounted.
Cancellation Policy:80% refund for cancellations made byAugust 8. No refunds after that date.
Please call the ASPR office if you havea special physical, sensory, or dietaryneed.
Registration Options:Recruiting 101 ................... Sun101 & Educ. Forum ........... Sun - Tues101, Educ. Forum, & 201 ... Sun - WedEducational Forum ............ Mon - TuesEducational Forum & 201 .. Mon - WedRecruiting 201 ................... Wed

Vol 13 NO. 1, Spring 2006 PAGE 35A S P R
ROBERT ARONSON, Attorney at Law, Ingber and Aronson,PA, Minneapolis, MN.
CINDY BAGWELL, Manager, Physician and SpecialtyRecruitment, Moses Cone Health System, Greensboro, NC;Co-Chair, ASPR Education Committee.
CHRISTINE BOURBEAU, Director, Physician Recruitment,Bristol Hospital, Bristol, CT; ASPR Member.
MARY BRAINERD, President and CEO, HealthPartners,Minneapolis, MN.
MICHELE BURKE, Physician Recruiter, Hammond Clinic,Munster, IN; Co-Chair, ASPR Education Committee.
DENNIS BURNS, Physician Outreach and ServicesSpecialist, St. John Health, Warren, MI; Chair, ASPRRegional Development Committee.
DANA BUTTERFIELD, Executive Director, Association ofStaff Physician Recruiters, Roseville, MN.
MICHAEL GRIFFIN, Vice President of Physician Recruitment,Cogent Healthcare, Inc, Irvine, CA; ASPR Past President.
MARCI JACKSON, Manager, Physician and ProviderRecruitment and Retention, Southwest Medical Associates/Sierra Health Services, Las Vegas, NV; ASPR Member.
RYAN JOHNSON, Attorney at Law, Fredrikson & Byron, PA,Minneapolis, MN.
CHRIS KASHNIG, Director of Physician Recruiting, ChristieClinic Association, Champaign, IL; ASPR member.
LILA KELLY, Principal Trainer and Consultant, Lila KellyAssociates, Roseville, MN.
JEFFREY KORSMO, Chief Administrative Officer, MayoClinic, Rochester, MN.
SCOTT LINDBLOM, Director, Medical Staff Services, DeanHealth Systems, Madison, WI; ASPR Past President.
KEITH LINDOR, MD, Dean, Mayo Medical School, Rochester,MN.
DONNA LOY, Medical Staff Coordinator/Staff DevelopmentManager, St. Joseph Medical Center, Reading, PA; ASPRPast President.
DAVID NYMAN, Physician Recruiter, St. Vincent Hospital/Prevea Clinic, Green Bay, WI; ASPR President.
DAVID PAGE, President and CEO, Fairview Health Services,Minneapolis, MN.
DEBORAH PENNINGTON, Assistant Vice President,Professional Staffing, Geisinger Health System, Danville,PA; ASPR Member.
DICK PETTINGILL, President and CEO, Allina Hospitals andClinics, Minneapolis, MN.
DAVID ROWLEE, Vice President, Research andDevelopment, Morehead Associates, Charlotte, NC.
DENISE SIEMERS, Physician Recruitment Leader, MercyMedical Center Northern Iowa, Mason City, IA; ASPRMember.
GREG SISKIND, Attorney at Law, Siskind Susser ImmigrationLawyers, Memphis, TN.
TIM SKINNER, Executive Director, National Rural Recruitmentand Retention Network, LaCrosse, WI; ASPR Member.
CAROL SULLIVAN, Executive Director, Healthcare Services,Nationwide Advertising, St. Louis, MO.
BRADLEY VAUDREY, CPA, Manager, R.S.M. McGladreyPullen, Minneapolis, MN.
SUSAN WADHWANI, Director of Recruitment, Sutter Health,Sacramento, CA; ASPR Member.
Speakers SponsorshipsMonday Lunch ($20,000)
PracticeLink.com
Evening Event ($10,000)
PhysicianWork.comVista Staffing
101 Lunch ($7500)
Medical Doctor Associates
Diamond ($7500)
NEJM
Ruby ($2500)
PracticeMatch
OpalJAMA ($1500)
CompHealth ($1000)
ReceptionDelta Locum Tenens ($3000)
Vista Staffing ($1000)
CompHealth ($1000)
Interim Healthcare ($1000)
Linde Healthcare ($1000)
Locumtenens.com ($1000)
Staff Care ($1000)
101 General sponsorDowden Health ($500)

Vol 13 NO. 1, Spring 2006PAGE 36 A S P R
ASPR FEATURED BRONZE CONTRIBUTOR AMERICAN MEDICAL ASSOCIATION
Help young physicians plan their future with the Green Book
As a recruiter, where do you turn to verify the education and trainingof physicians seeking employment? How do you keep track of theever-growing number of specialties/subspecialties? Need info on thelicensure requirements in given state(s), or the latest board certificationrequirements?
Then you need the “Green Book,” or Graduate Medical EducationDirectory, the only complete printed list of all ACGME-accredited andABMS board-approved residency/fellowship programs. The new 2006-2007 edition includes:
• Contact information for 8,390 ACGME-accredited and combinedprograms in 143 specialties/subspecialties and 1,700 GME teachinginstitutions
• New: Descriptions of and data for specialties/subspecialties, andexpanded information on the NRMP, ERAS, ECFMG, AAMC,ACGME, and more.
• ABMS medical specialty board certification requirements
• Medical licensure information
Also available soon is the GME Library on CD-ROM, which offersadvanced search functions to help you find the program or institutionyou’re seeking, an intuitive Web browser interface—no installationrequired, and an innovative XML format allowing for quick data sortsand program comparison.
To order or for more information, call 800 621-8335 or visit http://www.ama-assn.org/go/mededproducts
1. Strategy: Physician recruitment has traditionally taken on a“shoot from the hip” approach, one that overlooks the importanceof strategy and direction. What can ensue from this is a streamof dollars spent on advertising that yields little in the way oftangible outcomes. Your success in maximizing your advertisingresults is largely predicated on having clear objectives for yourefforts including budgets, timeframes, advertising targets, anda framework for evaluating the responses your ad generates.Revisiting this strategy often and making important courseadjustments is critical to ensuring that your efforts achieve theobjectives you desire.
2. Research: Stretching your recruitment advertising dollarsinvolves doing your homework on potential media vendors. Itis critical to acquire key information that will better allow you toleverage your resources and make more informed decisionsregarding your options. This involves contacting various mediavenues to learn more about their target audience, advertisingrates, and results history. You can also request that they provideyou with client references from other advertisers. You’ll want tofind out whether there are any standard advertising packagesavailable that guarantee leads. In general, this evaluationprocess will allow you to better identify the most cost-effectivemedia for achieving your recruitment objectives.
3. Diversification: Recruitment efforts which rely primarily onmedical journals and recruitment websites, will often limit yourresults. Boosting your return-on-advertising investment involvesmoving beyond one-dimensional exposure and employing avariety of strategies that, in the long run, are cost effective andyield better results.
(Maximizing Advertising Dollars - cont'd from p.1) It is important to consider every opportunity available to impressa potential candidate whether at a medical conference, publicevent, or through a newsletter. How you communicate yourmessage in welcoming physician candidates is a key factor toensuring successful outcomes.
From a pure advertising standpoint, there are a number of waysto diversify your efforts. For example, marketplace/classifiedsections that are available in some specialty medical journalsare often priced much lower than “Run-Of-The-Book” advertisingsections and can achieve equal or better returns in generatingqualified candidates. Advertising on niche boards for tough tofill positions in areas like gastroenterology, cardiology, andorthopedic surgery provide exclusive access to a very targetedgroup of candidates.
4. Negotiation: Receiving favorable advertising terms involvesleveraging your negotiation efforts in a way that allows maximumreturn on your recruitment dollars. Always keep in mind thefollowing rules of thumb:
• The more targeted the media venue, the higher the price; thelarger your budget and the more flexible the timing, the moreflexible the price.
• Make sure to convey to media vendors that you areconsidering multiple advertising venues and are seeking thebest package for your objectives and advertising budget.Letting them know you have more than one media option can goa long way toward positioning yourself for a good rate.
• Be clear about your objectives and ask the media vendor foradvice on the most efficient way to accomplish your goal within
(Maximizing Advertising Dollars - cont'd on p.37)
Profiles DatabaseGraduating Physician Seeking Employment
ASPR Bronze ContributorWe take recruitment information to the next level. We actuallyinterview each graduating physician directly. The Class of 2007graduate physicians' own personal recruitment info is ready foryou now at: www.ProfilesDatabase.com
Please visit us at www.ProfilesDatabase.comand try our new video demo to see exactlyhow we can help you.
We have been a proud ASPRcontributor since 2000.
ASPR FEATURED BRONZE CONTRIBUTOR PROFILES

Vol 13 NO. 1, Spring 2006 PAGE 37A S P R
(Maximizing Advertising Dollars - cont'd from p.36)
a specified time frame and budget range. Media vendorsknow their market and audience well, so enlist their supportin achieving your goals.
• Do not reveal your total budget. Instead, provide a reasonablerange for the media vendors to work with. Then request a coupleof scenarios from the vendor at varying budget levels so youhave the flexibility to choose one that is right for your needs.
• Once you are familiar with the standard rates, ask for a betteroffer than you expect to get. Request a first time advertisingdiscount (if appropriate), as well as frequency discounts inorder to see what the media vendor responds to. It’s notuncommon for them to come back with a rate that is lowerthan the original price.
• It is wise to request a trial run or test ad from a vendor prior tocommitting to an extended schedule. As a part of this, makesure you have procedures in place that allow you to capturethe unique results generated by each vendor. This will allowyou the opportunity to better determine which media vehicleis most conducive to your situation.
• If your overall advertising expenditures are in the range of$500,000 or more, you may want to consider partnering witha media strategy firm. They can assist you with strategicinput, quickly develop media recommendations, and negotiateadvantageous rates and positioning. In fact, a good mediastrategy firm may save you upwards of 40%-50% off ofpublished advertising rates.
5. Evaluation: An often overlooked yet important key toattracting top physician talent is having a process in place tomonitor your advertising activity and evaluate its effectiveness.A successful evaluation process is predicated on having a setof indicators, that offer you tangible evidence as to whichadvertising venues are producing the best results. Thisinformation is key to making important decisions about futureadvertising options and expenditures. It is also useful as aleverage point when negotiating future media agreements witha particular vendor.
A growing number of media vendors now offer some basictracking tools that can capture key data regarding youradvertising campaign effectiveness. This value added servicecombined with your own tracking efforts better allow you tomanage your advertising budget and ensure optimum returnson your investment.
There is no denying that physician recruitment is a competitiveundertaking these days. However, a well thought out processfor managing your advertising dollars can greatly enhance yoursuccess. Achieving maximum return on your recruitmentadvertising involves an integrated approach that uses acombination of research, strategy, diversification, negotiation,and evaluation to achieve a favorable outcome.
About the AuthorElaine Starling is the President of Starling Media, Inc. a NorthernCalifornia media strategy and negotiation firm that assists clients inachieving cost effective advertising. She can be reached [email protected].

Vol 13 NO. 1, Spring 2006PAGE 38 A S P R
WELCOME NEW ASPR MEMBERSAmy ArntsonPhysician RecruiterThe Duluth Clinic - SMDC400 E 3rd StDuluth, MN 55805Phone: 218-786-3181Toll Free: 800-342-1388FAX: 218-722-9952Email: [email protected]
Nicole BeckHealth Professional RecruiterOffice of Rural Health207 E Missouri Ave Ste 1APierre, SD 57501Phone: 605-773-2679Toll Free: 800-738-2301FAX: 605-773-2680Email: [email protected]
Amanda BolanderPhysician Services ManagerRush-Copley Medical Center2000 Ogden AveAurora, IL 60504Phone: 630-898-3456FAX: 630-898-3796Email: [email protected]
Ann Marie BowmanMedical RecruiterBrant Community Hlthcare Sys.200 Terrance Hill StBrantford, Ont, Canada N3R 1G9Phone: 519-751-5544 x2354FAX: 519-751-5575Email: [email protected]
Angie Boyd-ChambersPhysician Recruit & Bs. Dev.Stonecrest Medical Center200 Stonecrest BlvdSmyrna, TN 37167Phone: 615-768-2507FAX: 615-768-2707Email: angie.boyd-chambers@
hcahealthcare.com
Nadene BradburnDirector of Physician RecruitmentOur Lady of Lourdes Mem. Hosp.169 Riverside Dr, Ste 307Binghamptom, NY 13905Phone: 607-798-5837FAX: 607-798-5093Email: [email protected]
Debbie BrimerPhysician RecruiterCook Children’s Phys. Network750 -8th Ave, Ste 600Fort Worth, TX 76104Phone: 682-885-7434Toll Free: 877-532-6657FAX: 682-885-6729Email: [email protected]
Paul BrosorPractice AdministratorSun Health Corporation13950 W Meeker BlvdSun City West, AZ 85375Phone: 623-544-5079FAX: 623-544-5093Email: [email protected]
Julie BurgerPractice Development ManagerHealth Point Medical Group406 Reo St, Ste 200Tampa, FL 33609Phone: 813-636-2087FAX: 813-635-2050Email: [email protected]
Debbie BurriesPhysician RecruiterTri Health Hospitals619 Oak StCincinnati, OH 45206Phone: 513-569-6385FAX: 513-569-3620Email: debbie_burries@
trihealth.com
Louis CaligiuriPhysician Contracting & RecruitingNorth Shore Medical Center81 Highland AveSalem, MA 01970Phone: 978-354-2581FAX: 978-740-1803Email: [email protected]
Karen CranfordDirector of Ref. Dev. & PhysicianRecruitmentEast Texas Medical Center815 S BeckhamTyler, TX 75701Phone: 903-535-6859FAX: 903-596-3760Email: [email protected]
Kathy Cumming O’Hara, RNPhysician ServicesHealth Partners Central MN Clinics1245 -15th St NSt. Cloud, MN 56303Phone: 320-203-2007Toll Free: 800-370-0570 x2007FAX: 320-203-2068Email: kcummingohara@
hpcmc.com
Jonell Dailey, RHIADirector, Professional RelationsHardin Memorial Hospital913 N Dixie AveEllizabethtown, KY 42701Phone: 270-706-1728FAX: 270-706-1012Email: [email protected]
Misty DanielsPhysician RecruiterPikeville Medical Center911 Bypass RdPikeville, KY 41501Phone: 606-218-4915FAX: 606-218-4599Email: misty.daniels@
pikevillehospital.org
Rachelle DaughertyPhysician RecruiterProvidence Health & Services1235 NE 47th Ave, Ste 299Portland, OR 97213Phone: 503-215-2217Toll Free: 866-504-8178FAX: 503-215-6561Email: rachelle.daugherty@
providence.org
Charlene DavisDirectorProvidence Phys. Relations & Recr.PO Box 196604Anchorage, AK 99519Phone: 907-743-2631FAX: 907-743-2799Email: [email protected]
David DeSimone, CHEPhysician Development AdministratorThe Nebraska Medical Center987400 Nebraska Medical CenterOmaha, NE 68198Phone: 402-559-4679FAX: 402-552-3484Email: ddesimone@
nebraskamed.com
Gail DonovanPhysician RecruiterHarrison Medical Center2520 Cherry AveBremerton, WA 98310Phone: 360-473-4914FAX: 360-475-8530Email: gdonovan@
harrisonmedical.org
Lori DyeMedical Staff RecruiterWellmont Health System999 Executive Park Blvd, Ste 210Kingsport, TN 37660Phone: 423-230-8506Toll Free: 888-296-7358FAX: 423-230-8502Email: [email protected]
Brenda ElliottAdmin. Asst./Physician RecruiterPerson Memorial Hospital615 Ridge RdRoxboro, NC 27573Phone: 336-503-5796FAX: 336-503-5765Email: [email protected]
Mark GallucciPhysician RecruiterSt. Peter’s Hospital310 S Manning BlvdAlbany, NY 12208Phone: 518-525-2354Email: mgallucci@ stpetershealthcare.org
Deanna GrangePhysician RecruiterIntermountain Healthcare36 South State StSalt Lake City, UT 84111Phone: 801-442-3280Toll Free: 800-888-3134FAX: 801-442-2999Email: deanna.grange@
intermountainmail.org
John GravetteDirector of RecruitingCalifornia Emergency Physicians2100 Powell St, Ste 920Emeryville, CA 94608Phone: 510-350-2665Toll Free: 800-842-2619FAX: 510-879-9064Email: gravettej@
medamerica.com
Janna HansonDirector, Phys Recr/CompensationCharleston Area Medical Center511 Brooks StCharleston, WV 25156Phone: 304-388-6401Toll Free: 866-551-8927FAX: 304-388-6297Email: [email protected]
Marianne HayesExecutive AssistantMartin’s Point Healthcare331 Veranda StPortland, ME 04104Phone: 207-791-3813FAX: 207-828-2446Email: marianneh@
martinspoint.org
Gwen Hinton-StinsonPhysician RecruiterPeace Health1615 DelawareLongview, WA 98632Phone: 360-414-7596FAX: 360-636-7243Email: [email protected]
Stephanie HutchinsPhysician RecruiterValley Health Plan706 S Main StHarrisonburg, VA 22801Phone: 540-564-7000Toll Free: 800-250-3401FAX: 540-564-7010Email: shutchens@
valleyhealthplan.com

Vol 13 NO. 1, Spring 2006 PAGE 39A S P R
NEW MEMBERS - continued
Susan KutacPhysician RecruiterValley Baptist Medical Center2101 Pease StHarlingen, TX 78550Phone: 956-389-6774Toll Free: 800-471-9743FAX: 956-389-6746Email: susan.kutac@
valleybaptist.net
Bonita LancasterPhysician RelationsBaptist HealthPO Box 244001Montgomery, AL 36124-4001Phone: 334-273-4527FAX: 334-273-4204Email: [email protected]
Dalia LevyPhysician RecruiterValley Baptist Medical Center1040 W.JeffersonBrownsville, TX 78520Phone: 956-698-5220Toll Free: 866-383-5220 x6FAX: 956-698-5005Email: [email protected]
Kristin LuciaBusiness Development SpecialistSt. Margaret Mercy HealthcareCenters5454 Hohman AveHammond, IN 46320Phone: 219-933-2117FAX: 219-933-2634Email: [email protected]
Bryan MacLeanProgram CoordinatorMaritime Physician RecruitmentInitiative460 -5991 Spring Garden RdHalifax, NS, Canada B3H 1Y6Phone: 902-404-3598FAX: 902-404-3599Email: [email protected]
Lauren MainesPhysician RecruiterUnited Medical Center214 E 23rd StCheyenne, WY 82001Phone: 307-432-2649FAX: 307-432-3181Email: [email protected]
Jan McCleeryProvider Staff RecruiterKewanee Hospital719 Elliott StKewanee, IL 61443Phone: 309-853-6081Toll Free: 800-369-6771FAX: 309-852-6428Email: jmccleery@
kewaneehospital.com
Alethea McCulloughDirector Physician RecruitmentForsyth Medical Center3333 Silas Creek PkwyWinston-Salem, NC 27103Phone: 336-277-0390FAX: 336-277-9641Email: awmccullough@
novanthealth.org
Brenda McGinnCMSRBryanLGH Health System1600 S 48th StLincoln, NE 68506Phone: 402-481-8543Toll Free: 800-563-8289FAX: 402-481-8549Email: [email protected]
Kathy MembersPhysician Services RepresentativeVia Health1425 Portland AveRochester, NY 14621Toll Free: 877-838-7571FAX: 585-922-9422Email: [email protected]
Jason MeyerDirector of Practice DevelopmentChildren’s Acute Care3281 N Decatur Blvd, Ste 210Las Vegas, NV 89130Phone: 702-395-5945Toll Free: 800-923-2393FAX: 702-395-3502Email: jmeyer@
childrensacutecare.com
Tanya MullenPhysician RecruiterFremont-Rideout Health Group989 Plumas StYuba City, CA 95991Phone: 530-751-4243FAX: 530-751-4226Email: [email protected]
Gail NegronPhysician RecruiterCape Cod Healthcare, Inc27 Park StHyannis, MA 02601Phone: 508-862-5357FAX: 508-862-7316Email: [email protected]
Donna NewmanDirector Physician RecruitmentOhio Health Physician Recruiting3732 Olentangy River Rd, Ste EColumbus, OH 43214Email: [email protected]
Helene OyamaPhysician RecruiterKauai Medical Clinic3-3420 Kuhio Hwy, Ste BLihue, HI 96766Phone: 808-246-2951FAX: 808-246-1645Email: [email protected]
Mariann PangPhysician RecruitmentBorgess Medical1521 Gull RdKalamazoo, MI 49048Phone: 269-226-7420Toll Free: 800-695-6737FAX: 269-226-5966Email: [email protected]
Michael PetersonMedical Provider RecruiterMultiCare Health System737 S FawcettTacoma, WA 98415Phone: 253-459-7978Toll Free: 800-621-0301FAX: 800-264-2818Email: [email protected]
Jennifer PizzolatoPhysician RecruiterWellstar Health System805 Sandy Plains RdMarietta, GA 30066Phone: 770-792-5222FAX: 770-792-1738Email: [email protected]
Kimberli PoorDirector of OperationsHealthServe Medical Group, LLC2939 Kenny Rd, Ste 200Columbus, OH 43221Phone: 614-442-2431Toll Free: 877-442-2431FAX: 614-442-2426Email: [email protected]
Jennell PrenticeHealth Services ConsultantWashington Recruitment GroupPO Box 47834Olympia, WA 98504Phone: 360-236-2814Toll Free: 877-776-1824FAX: 360-664-9273Email: [email protected]
Steven RichardsonPhysician RecruiterWVU School of MedicinePO Box 897Morgantown, WV 26507Phone: 304-293-0765FAX: 304-293-4200Email: richardson@
rcbhsc.wvu.edu
Krista RobertsDirector Strategic DevelopmentSt. Mary’s Regional Medical Ctr305 S FifthEnid, OK 73701Phone: 580-249-3781FAX: 580-249-3982Email: [email protected]
Denise RomandMedical Staff/Practice LiaisonSaratoga Hospital211 Church StSaratoga Springs, NY 12866Phone: 518-583-8465FAX: 518-580-2605Email: [email protected]
Kathleen SchmelzleAssistant to VP of Medical AffairsEPIC Management, LP10393 Enterprise DrRedlands, CA 92374Phone: 909-478-5116FAX: 909-796-0417Email: [email protected]
Chad SelenskePhysician Recruiting LiaisonMarshfield Clinic2727 Plaza DrWausau, WI 54401Phone: 715-847-3426Toll Free: 800-847-0016FAX: 715-847-3329Email: selenske.chad@
marshfieldclinic.org
Reid SmithPhysician RecruiterHCA Physician Recruitment300 Arboretum Pl, Ste 370Richmond, VA 23236Phone: 804-237-7763Toll Free: 866-422-3627FAX: 877-430-2303Email: reid.smith@
hcahealthcare.com
Michelle SteffenPhysician Recruiter/Development& RetentionWichita Clinic3311 E MurdockWichita, KS 67208Phone: 316-689-9852Toll Free: 800-876-5111 x9852FAX: 316-689-9742Email: [email protected]
Cheryl VanderlaanPhysician RecruiterSherman Hospital1019 E Chicago StElgin, IL 60120Phone: 847-429-5428FAX: 847-429-6117Email: cheryl.vanderlaan@
shermanhospital.org

Vol 13 NO. 1, Spring 2006PAGE 40 A S P R
Lisa WatersPhysician Specialty RecruiterHCA Physician Services7400 Fannin Ste 650Houston, TX 77054Email: lisa.waters@
hcahealthcare.com
Kelly WhitmarshSenior RecruiterChristiana Care Health System200 Hygeia DrNewark, DE 19713Phone: 302-623-0319Toll Free: 866-562-4767 x0319FAX: 302-623-0324Email: kwhitmarsh@
christianacare.org
Monica YoungPhysician Relations SpecialistSouthern Illinois Healthcare1239 East Main StCarbondale, IL 67017Phone: 618-457-5200 X62901Toll Free: 800-333-1929FAX: 618-529-0568Email: [email protected]
NEW MEMBERS - continued
Linda DwyerDirector of Physician ServicesSt. Joseph Medical Center7601 Osler DrTowson, MD 21204Phone: 410-337-1215FAX: 410-337-1569Email: [email protected]
Kim LanzillottiRecruitment Services CoordinatorThe Southeast Permanente MedicalGroup3495 Piedmont Rd NE, Bldg 9Atlanta, GA 30305Phone: 404-364-7178FAX: 404-364-4984Email: [email protected]
Lisa LewisDirector Physician DevelopmentHealthfirst/St Anthony Hospital1110 N Classen Blvd, Ste 100Oklahoma City, OK 73106Phone: 405-272-7952FAX: 405-272-7937Email: [email protected]
Debra MountsMngr Physician Recruiting/MedicalStaff ServicesKelsey-Seybold Clinic8900 Lakes @ 610 DriveHouston, TX 77054Phone: 713-448-0212FAX: 713-442-5115Email: drmounts@
kelsey-seybold.com
Frank PickeringManager of Physician RecruitmentEmergency Medical Services, Inc.920 Main St, Ste 300Kansas City, MO 64105Phone: 816-559-6333Toll Free: 800-821-5147FAX: 816-753-4647Email: [email protected]
Andrea TworekPhysician Recruitment CoordinatorOregon Anesthesiology Group, P.C.120 NW 14th Ave, Ste 300Portland, OR 97209Phone: 503-299-9906Toll Free: 800-282-6864FAX: 503-295-2232Email: [email protected]
WELCOMEBACK!
The following people wereprevious members ofASPR, and have nowrejoined. Welcome Back!

Vol 13 NO. 1, Spring 2006 PAGE 41A S P R
ASPR EMPLOYMENT HOTLINEComplete current job &"where to apply" info can be found
in the "Members Only" section of the ASPR website.
If you hear about a recruiting position available, call Bonnie in theASPR office at 800-830-ASPR (2777). For information on the mostrecent job listings, and for contact/application information on theselisted opportunities, check the members only section of the ASPRwebsite.
Regional Recruiting ManagerIPC - The Hospitalist Company, Houston TX
Founded by physicians in 1995, IPC - The Hospitalist Company hasgrown to become the nation’s leading hospitalist company. IPC’sphysicians, support staff, operations, and technology are all focusedon driving the health care delivery system towards better, more efficientand more patient-friendly inpatient care. IPC has taken a leadershiprole in the emergence of this new medical specialty, and today IPC’sphysicians work with more than 12,000 referring physicians and over1,000 health plans to manage more than $1 billion in healthcareexpenditures annually.
Due to accelerating growth, IPC – The Hospitalist Company has animmediate opening for an experienced recruiter for its regional officein Houston, TX. This position will report to the Vice President ofPhysician Staffing and have complete responsibility for managing theregion’s physician recruitment needs. The ideal candidate will havea BA/BS degree, demonstrated career progression, along with aminimum of five years of successful physician recruiting experience.Experience in a multi-facility/multi-state system is preferred, moderatetravel required. Our team has grown to a total of nine experiencedstaffing professionals, supporting over 500 physicians in more than100 practice groups in 14 states. If you have an interest in workingwithin a fast-paced organization that is dedicated to excellence –please email your resume to Timothy Lary at, [email protected] or call800-680-2492.
Physician RecruiterProvidence Health and Services, Portland, OR
Working in collaboration with service area leadership teams andphysicians, the Physician Recruiter plans and implements physicianrecruitment activities for Providence Health System, located primarilyin Portland, Oregon. The Physician Recruiter is responsible for allsourcing functions including: outreach visits, advertising/marketing,initial contact, reference checking, orchestrating visits and finalizingrelationships to meet physician needs within the system. The PhysicianRecruiter works in close collaboration with service area leadershipteams, Human Resources, and the Regional Physician SupportServices team. The ideal candidate will possess a BA/BS as well as3 to 5 years recruitment and/or healthcare management experience.Preference will be given to candidates having previous experienceworking with physicians. The ideal candidate will also possessknowledge of physician practice operation and strong negotiatingskills. Working out of Providence Office Park as a member of theRegional Physician Support Services Team, this position is full-time,with some travel required. Current OR driver’s license and vehicle isalso required. Minimum $25.75/hr to Maximum $38.63/hr. withcomprehensive benefits and retirement package.
Interested persons are encouraged to send resume to:[email protected]
Physician RecruiterNemours, based out of Wilmington, DE or Jacksonville, FL
Nemours is one of the nation’s largest organizations dedicated tomaintaining and improving the health of children, operating the A I.duPont Hospital for Children in Wilmington, DE and pediatric primaryand outpatient specialty offices in DE, FL, NJ and PA. We serve morethan 220,000 children and provide nearly 900,000 visits annually. Weare seeking a Physician Recruiter to recruit for pediatric subspecialtyphysicians in DE, NJ, PA and FL.Responsibilities:• Implement both immediate and pipeline physician recruitment strategies• Utilize proactive recruitment methods (lead generation/sourcing,
networking, and referral programs)• Develop text for physician recruitment advertising• Manage relationships in collaboration with HR business partner with
physician leaders, candidates, and external physician recruitmentagencies
• Ensure early and timely contact and screening of candidates• Arrange pre-screening of candidate background checks in cooperation
with Corporate Credentialing• Arrange and host on-site physician recruitment visits• Extend and negotiate offers of employment• Coordinate relocation issues with candidates• Collaborate with the HR Employment Manager and other recruiters to
build long- and short-term strategies for developing a Center ofExcellence in Recruiting
• Travel requiredRequirements:• BS/BA degree in business, marketing, human resources, health care
or related field• Minimum five (5) years experience as a physician recruiter• Certification as CMSR (Certified Medical Staff Recruiter), CPC
(Certified Personnel Consultant) or COCRC (Certified PersonnelConsultant Physician Recruiter) preferred
• Demonstrated success in developing and implementing recruitingstrategies, policies, and programs .
We offer 100% in-network health coverage for children of full-timeNemours Associates! Please apply online at www.Nemours.org. EOE
Physician Recruitment ConsultantSuburban Health Organization, Indianapolis, IN
Suburban Health Organization, a physician and hospital networkserving central Indiana, is seeking a full-time Physician RecruitmentConsultant to join its Recruitment Team. The Recruiter will direct theidentification, qualification and placement of healthcare providers intothe company’s owner physician groups and medical facilities bymatching physician skill level, licenses, preferences, board status,and credentials to the client’s needs. Qualified candidates willpossess:• Bachelor’s Degree in Business or Health Administration• 5 to 7 years experience in physician recruiting or physician relations
(Job Hotline - continued on p. 42)

Vol 13 NO. 1, Spring 2006PAGE 42 A S P R
EMPLOYMENT HOTLINE - continued• Knowledge of central Indiana medical community preferred• Ability to work independently and as a team player• Excellent customer service• Must possess solid judgment skills and contribute as a team player• Display exceptional communication skills, oral and written• Well-developed listening skillsWe offer excellent benefits including Medical, Dental, Vision, 401Kand a generous vacation package. Please send or fax your resumeand salary requirements to: Suburban Health Organization, ATTNKeisha Underwood, 2780 Waterfront Parkway East Drive, Suite 300,Indianapolis, IN 46214; Fax 317/692-5233
Manager, Professional Staff Recruitment & AffairsPeaceHealth Medical Group, Eugene, OR
An exciting leadership opportunity at PeaceHealth Medical Group tojoin our dynamic team of talented professionals in Eugene, OR.Eugene-Springfield is a community of 200,000+ that boasts the culturalamenities associated with being home to a major university as wellas Pac-10 football and world-class track. We are currently seeking aseasoned individual to work closely with the Senior Leadership Teamand Medical Staff. Primary responsibil ity is development,administration, and management of a comprehensive physicianrecruitment and retention program for a growing 120-physician multi-specialty group. Successful candidate must have a Bachelor’s degreeand/or a minimum of 5 years professional level experience with atleast 3 years in management preferably in Physician Recruitment orHuman Resources within a multi-specialty medical group. Must alsopossess strong strategic leadership skills and progressive humanresources. To apply online, visit www.peacehealth.org (OregonRegion). For more info, please contact Alice @ 800-365-8990, ext.1791. PeaceHealth is an EOE/Affirmative Action Employer.
Physician RecruiterThe Permanente Medical Group, Inc./Kaiser Permanente, Oakland, CA
The Permanente Medical Group, Inc. in Northern California has anexciting opportunity for an in-house physician recruiter. TPMG is aquality leader in healthcare with over 6,000 physicians in the medicalgroup providing care to over 3.2 million Kaiser Foundation HealthPlan members throughout Northern California. Based at the regionaloffices in Oakland, CA, the physician recruiter will recruit and securethe placement of physicians for the entire Northern California region.Responsibilities will include: All steps of the recruitment process. Developsuccessful relationships with candidates, chiefs, and leadership. Partnerwith colleagues on marketing strategies to bring in the top physicians inthe nation. The position calls for strong communication, presentation,and consulting skills. Must be familiar with database technology. Localand out-of-area travel is expected. Successful candidates must possessan enthusiastic professional demeanor and a strong service mind-set.Qualifications: Bachelor's degree preferred in human resources, businessadmin., or other related field. Good working knowledge of recruitmentpractices, marketing strategies, and techniques preferred. For moreinformation or to apply: Contact Mazie Blanks at 800-777-4912 or byemail at [email protected]. To find out more about The PermanenteMedical Group, Inc., visit our website at http://physiciancareers.kp.org.ncal
Physician RecruiterTeam Health West, Phoenix, AZ
Team Health, Western Division office, has an opening for anexperienced Physician Recruiter in its Phoenix, AZ office. Focus willbe recruiting physicians and mid-level practitioners to staff hospitals/
clinics. Candidates should possess confident communication andinterpersonal skills, as well as the ability to handle multiple tasks/deadlines. BA/BS in Business, Communication, and 5+ years relevantexperience, preferably in physician recruiting or medical sales.Excellent compensation/benefits package. EOE. Fax resume to 925/924-0506 ATTN: Mike Engle or email to: [email protected]. Team Health West, 5000 HopyardRoad, Suite 100, Pleasanton, CA 94588; phone 925-924-1600 x 6940
Pediatric Subspecialty RecruiterHCA Physician Services, Nashville, TN
We seek a physician recruiter who is an expert in recruiting pediatricsubspecialists. This recruiter would work with the current regionalrecruiters, our pediatric hospital CEOs and hospital personnel. Thisrecruiter would focus exclusively on pediatric subspecialties. We wantsomeone who can identify and develop relationships with the besttraining programs across America. Working through either the programcoordinators, program directors or fellows and residents to personallyknow the candidates in training and assist them with their long-termcareer planning and practice search. This recruiter would attend theappropriate pediatric-focused conferences to meet and network withcandidates. Our plan would include opportunities for the recruiter toemail, call, and meet with the candidates proactively, and funnelcandidates to the regional recruiters. We have five high-qualitypediatric facilities around our network: Sunrise Children’s Hospital,Presbyterian/St Luke’s Medical Center, Methodist Children’s Hospitalof South Texas, Women’s & Children’s Hospital (Lafayette, LA), andMedical City Children’s. Each of these facilities faces similarchallenges in recruiting the specialists needed to offer the best inpediatric care. The recruiter would focus on finding candidates neededin each of the specified communities that are fellowship-trained inareas such as Pediatric Orthopedics, Pediatric Cardiology, PediatricGastroenterology, Pediatric Anesthesiology, Pediatric Intensivists,Pediatric Surgery and more. This recruiter could be based in ourNashville office, or work from any other area of the country. Qualifiedindividuals should email their resumes to: [email protected].
Physician RecruiterHCA, Tallahassee, FL
HCA is committed to a compassionate attitude towards others and toproviding quality service. Our 180 hospitals include over 50,000doctors on their medical staffs, and satisfaction scores for thesedoctors have never been higher. Join us in this key role recruitingoutstanding physicians to maintain our high standards. Use yourexceptional interpersonal skills and knowledge of physician recruiting/healthcare operations to manage the recruitment database, generateleads, and pre-screen and follow up with candidates, as well asdevelop and coordinate effective recruitment strategies/campaigns.In addition, you’ll coordinate physician facility/community site visitsand work with Fellowship and Residency programs to make residentsaware of great practice opportunities for our market area. To qualify,you must have at least three years of experience in physician recruitingor physician relations, and proficiency with recruiting software suchas Recruiter Magic, Practice Track, or Goldmine. Knowledge of theWorld Wide Web as related to job postings and recruitment researchrequired. Your professionalism, diplomacy, discretion, sound judgment,and flexibility, and the ability to maintain confidentiality are essentialfor this key role. Bachelor’s degree and some travel required. Forimmediate consideration and to apply, please visit: www.resjobs.com/hcajobs HCA is an Equal Opportunity Employer.

Vol 13 NO. 1, Spring 2006 PAGE 43A S P R
Physician RecruiterVisiting Physicians Association (VPA), Farmington Hills, MI
VPA is a large multi-state group practice with offices throughout theMidwest and in the South. Headquartered in Farmington Hills,Michigan, VPA has an immediate opening for an experiencedPhysician Recruiter to focus on recruiting full-time salaried physiciansto staff multiple offices. The ideal candidate must possess the skillsand experience to handle all aspects of physician recruitment. Thisposition is a hands-on role which requires excellent communication/interpersonal skills to deal effectively with physicians andadministrators. We seek a confident and motivated candidate whoperforms well under stress and welcomes challenge and growth.Candidates must be familiar in the initiation and development ofrecruitment programs including but not limited to advertising, directmail, telephone, networking, exhibiting, etc.
Knowledge, Skills and Abilities:• Physician Recruitment experience required (min. 3-5 yrs.)• Bachelors degree is preferred, not required• Sales experience and/or clinical background preferred, not required• Excellent computer skills, especially MS Office products
This position offers exceptional growth for the right candidate. VPAoffers competitive salary and excellent benefits including health anddental insurance, short-term disability, paid time off, holidays, 401/kand flexible spending accounts. Please apply online by emailing:[email protected] or send resume via fax: 248-324-1532. Visit our website at: www.visitingphysicians.com
Director, Physician RecruitmentMeridian Health, Neptune, NJ
Meridian Health seeks an experienced professional to take a leadrole in the development and management of a system-wide physicianrecruitment department. Meridian Health is among the largest healthcare providers in New Jersey. It is a three hospital system with morethan 7,500 employees, 1,400 affiliated physicians, 1,219 licensedpatient care beds, and annual revenues of over $820 million.Immediate responsibilities will include initial business for the newdepartment planning, addressing such areas as service offerings,target clients, staffing, capital requirements, budget, fee structure,and development of the department’s policies and procedures. Thesuccessful candidates will have experience and knowledge in allaspects of physician recruitment and will have demonstrativeexperience in developing and/or effectively managing a large in-houserecruitment department or having had a high degree of successworking for a for-profit search firm. The position reports to the VicePresident of Physician Services and will collaborate with other seniorlevel managers in the areas of strategic planning and businessdevelopment, marketing and communications, legal affairs, andinformation technology. Preferred candidates will be self motivated,demonstrate the ability to develop strong relationships with seniormanagement, medical staff and physician candidates and haveknowledge of various computer software systems. Excellent writtenand oral communication skills are essential. A college degree requiredwith a minimum of 5 years of successful experience in the physicianrecruitment field. Qualified candidates should submit their resumeto: Frank Goldstein, Vice President of Physician Services,[email protected]
Physician LiaisonDelnor-Community Hospital, Geneva, IL
Delnor-Community Hospital has an opening for a Physician Liaison.General Summary: To build supportive relationships with physiciansand their office staff that lead them to making Delnor their first choiceas a place to practice medicine.
Knowledge, Skills, and Abilities:• Bachelors Degree required• Sales experience and/or clinical background preferred• Masters Degree preferred• Minimum 3 to 5 years of healthcare experience with direct physician
contact required.Interested candidates can contact Jojy Schless at Phone 630-208-4360; Fax 630-208-3085; email [email protected],www.delnor.com
Director of Physician Recruitment and RetentionSaint Vincent Health System, Erie, PA
Exciting new opportunity at Saint Vincent Health System inNorthwestern Pennsylvania for a seasoned professional to workclosely with the Medical Staff and Senior Leadership Team. Primaryresponsibility is development and administration of a comprehensivephysician recruitment and retention program for the entire healthsystem. The ideal candidate is required to have 10 years of healthcare recruitment/retention experience along with a Bachelor’s Degreein a health care concentration, Master’s Degree preferred. Thesuccessful candidate must also possess strong strategic leadershipskills and progressive human resource experience. Saint VincentHealth System was recently named in the top 20 of Pennsylvania’stop 100 employers. Saint Vincent is an integrated health care deliverynetwork, which includes 14 distinct on-campus centers of excellence,12 primary care medical practices, 11 specialty medical practices,and strategic affiliations with numerous community hospitals andmedical providers, serving a population base of 1.2 million arearesidents. For more information regarding Saint Vincent HealthSystem and this outstanding career opportunity, please visit ourwebsite at saintvincenthealth.com and send a resume and cover letterto John Mashinski, Senior Vice President of Human Resources [email protected].

BOARD OF DIRECTORS
Education/Conference Planning Committee Cindy Bagwell & Michelle BurkeMarketing/Membership Committee Rich Lynch
Newsletter Judy Brown & Laura ScreeneyRegional Development Dennis Burns
Strategic Planning/Bylaws Scott LindblomWebsite Michael Hesch
PRESIDENTDavid NymanPhysician RecruiterSt. Vincent Hospital/Prevea ClinicPO Box 13508Green Bay, WI 54307Phone: 920-433-8076Toll Free: 800-236-3030 x8076FAX: 920-431-3043Email: [email protected]
VICE PRESIDENTMarci JacksonManager, Physician & Provider Recruitment& RetentionSouthwest Medical AssociatesPO Box 15645Las Vegas, NV 89114Phone: 702-240-8944Email: [email protected]
SECRETARYLynne PetersonManager, Physician RecruitmentFairview Health Services2450 Riverside Ave, F 101 West BldgMinneapolis, MN 55454Phone: 612-672-2285Toll Free: 800-842-6469Fax: 612-672-2986Email: [email protected]
TREASURERDana ReedDirector of Professional RecruitingOchsner Clinic Foundation9001 Summa AvenueBaton Rouge, LA 70809Phone: 225-761-5893Toll Free: 800-488-2240Fax: 225-761-5441Email: [email protected]
BOARD MEMBER AT LARGEKathleen LeeDirector, Medical Staff DevelopmentConway Medical Center300 Singleton Ridge RoadConway, SC 29526Phone: 843-234-5139Fax: 843-347-80056Email: [email protected]
BOARD MEMBER AT LARGERich LynchMedical Staff RecruiterFort Atkinson/Watertown Memorial Hospitals611 Sherman Avenue EFort Atkinson, WI 53538-1998Phone: 920-568-5121Fax: 920-568-6045Email: [email protected]
Association of Staff Physician Recruiters1711 West County Road B, Suite 300 N
Roseville, MN 55113
Spring 2006
See page 30 for information onthe ASPR Annual Conference.
BOARD MEMBER AT LARGEBrett WalkerDirector, Physician RecruitmentClarian Health1633 N. Capitol Ave, Suite 102Indianapolis, IN 46202Phone: 317-962-6688Toll Free: 866-394-4138Email: [email protected]
PAST PRESIDENTJerry HessMedical Staff DevelopmentGundersen Lutheran Health System1900 South Avenue, H02-009ILaCrosse, WI 54601Phone: 608-775-6314Toll Free: 800-362-9567Fax: 608-775-5594Email: [email protected]
ASPR EXECUTIVE DIRECTORDana Butterfield1711 W. County Road B, Suite 300NRoseville, MN 55113Toll Free: 651-635-0359Phone: 800-830-2777Fax: 651-635-0307Email: [email protected]