volume 21 . number 3 . december 2010 rivista … · volume 21 . number 3 . december 2010 rivista...
TRANSCRIPT

VOLUME 21 . NUMBER 3 . DECEMBER 2010
RIVISTA ITALIANA DI CHIRURGIA MAXILLO-FACCIALE
EDIZIONI MINERVA MEDICA
IT J MAXILLOFACSURG 2010;21:155-60
Clinical and radiological characteristicsof a severe form of cherubism: case report
P. PIOMBINO 1, A. SPINZIA 1, S. PARASCANDOLO 2, V. ABBATE 1, L. CALIFANO 1
Cherubism is a rare, inherited condition characterizedby fibro-osseous lesions of the maxilla and mandible.It has recently been localized in chromosome 4p16.3.The fullness of the lower half of the face and retraction of the lower lids gives the characteristic "eyesraised to heaven" cherubic appearance. A case reportof a ll-year old boy with extensive orbital involvement of cherubism is presented. The patient has orbital manifestations including lower lid retraction, proptosis, diplopia and globe displacement. Taking intoaccount the severity of the disease based on the modified Motamedi grading system, we decided to treat theorbit surgically and to pIace the patient under a postsurgery weekly follow-up to assess the spontaneousregression of the extra-ocular disease in accordancewith the data reported in literature. We maintain thatdecompressive surgery on the orbit is desirable in severe cases of the disease to avert the risk of irreversible ocular lesions.
KEY WORDS: Cherubism - Orbit - Ophthalmologic surgicalprocedures.
Cherubism was described for the first time in 1933by Jones as a "familial multilocular cystic diseaseof the jaws".l-l0
It is a benign fibro-osseous dysplasia, characterized by an involvement of the mandible, the maxillaor both. The incidence of cherllbism is unknown,but the age of onset is between 2 and lO years.2
Cherubism is a disease transmined \\-ith an autosomal dominant inheritance, ,Ùth variable penetrance and expressiveness, presenting a penetranceof 100% in males and from 50% to,,70%in females4
Received on October 4. 2010.
Accepred for publicarion on '\o\'ember 26. 2010.
Corresponding aurhor: A. Spinzia. via Pansini 5. 80131 '\aples. Irah'.E-mai!: [email protected]
10epartment of Maxillofacial SurgeryFederico /I University, Naples, Italy
20epartment of Maxillofacial SurgeryA. Cardarelli Hospital of Naples, Italy
Even so, many sporadic cases are reported in literature.ll-r
It has been associated, after the mapping ofchromosome 4p16, with a mutation of the geneSH3BP2.18-20 Starting from this discovery, a pathogenetic hypothesis has been formulated: the Gain-offunction mutation (SH3BP2) causes a disregulationof the gene Msx-l that is involved in the morphogenetic processes causing the fullness of the face.2, 5, 8
Cherubism is characterized by an asymptomatic bilateral expansion of the mandible, maxilla orboth.4 This becomes evident in early infancy andincreases progressively until puberty, after which agraduaI resolution of the disease is reported at different times in the patient's development.5
The uncontrolled growth of the superior maxillapushes the orbita I floor upwards, which leads to adislocation of the eyeball with a consequent exposure of the lower part of the scIera (scIeraI show).
AlI this gives to the patient the upward-Iookingappearance typical of this disease ("eyes raised toheaven").13 Based on such characteristics, the term"cherubism" was used for the first time in 1938,becallse the disease confers to the patients, whopresent a symmetrical swelling of the cheeks witha rounded face and an upward gaze, an appearance similar to that of the cherubs of Renaissanceart (Figure 1).
The dentition is often anomalous and the patientspresent agenesis, ectopia and dental incIusions,radicular reabsorption and malocclusions. Radiolog-
VoI. 21 - No.3 ITAlIN' JOL~,Al OF ~[A.,\ILLOFACl-USCRGERY 155

PIOMBINO
Figure l.-Cherubs - Engel V (Detail from Raphaers Sistine Madonna).
Figure 2.-Bilateral mandibular and maxillary expansion.
SEVERE FORNI OF CHERUBISM
Figure 3.- Typical appearance "eyes raised lO heaven·'.
Figure 4.-Subversion of the normal conformation of the mandibleand maxilla
ically, the expansive lesions appear as radiolucentmultilocular cysts, that is initially localized at thejunction with the mandibular angle and then extendto the horizontal branch and the ramus. Lesions onthe superior maxilla can present at the same time.These lesions are often associated with a dislocationof the teeth and dental germs.5
A definitive diagnosis is confirmed histologically bythe idemification of giam multinuclear cells, distributed randomly, associated with the presence of aeosinophilic collagen peri\-ascular cuffin, that could beinterpreted as a pathognomonic sign of the disease,immersed in a fibrous connective tissue stroma2,4
The multinuclear giam cells are positive to oste 0clasts specific markers and appear to be pathologi-
156 !TAli, .., ]OCR-,Al OF \LA.,\JLLOFAClAl SCRGERY Oecember 2010
SEVERE FOR.ì'vl OF CHERUBIS.\I PIOMBINO
cerning the presence of cherubism in other members of hisfamil)'.
Extra-oral clinical examination revealed a bilateral expansion of the mandibular region, oral mucosa and maxilla, moreeYident on the left side of the face, which conferred to theface of the patient a rounded appearance (Figure 2).
The excessive growth of the right superior maxilla with signifìcant involvement of the homolateral orbital floor resultedin the appearance of a false esophthalmus, with a consequentexposure of the sclerae beneath the eyeballs (scleral show).This gave the young patient the upward looking appearance,typical of cherubism ("eyes raised to heaven") (Figure 3).
The patient reported the presence of dip!opia in the upward gaze, caused by the presence of a misa!ignment of theinterpupillary !ine.
An objective intra-oral examination revealed a dentalmalocclusion, associated with the absence of some penllanent teeth and the persistence of some deciduous teeth, someof ",-hich in an ectopic position.
Additionally, it revealed a painless swelling, at the leve! ofthe mucosa hanging over the superior and inferior alveolarridges, caused by an expansion of the underlying osseoustissue.
Orthopamomography revealed radiological signs characteristic of cherubism: the presence of multiple radiolucentmultilocular cystic lesions occupying the entire mandibularand maxillary osseous area to the exclusion of the mandibular condyles; deciduous and permanent teeth in osseousinclusion. some of which having erupted but in an ectopicposition; and the presence of dental germs and radicularreabsorption.
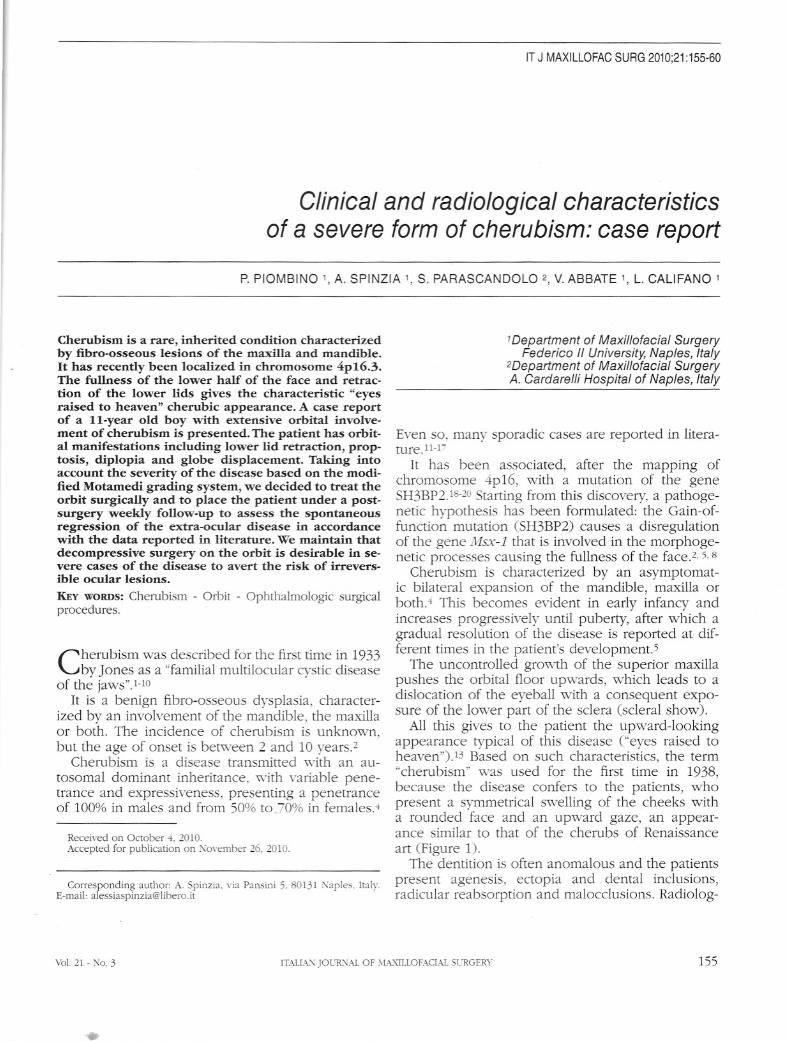
CT radiological examination revealed a signifìcant morphostructural alteration of the mandible and maxilla. Theyappeared markedly increased in volume, showing a subversion of the norma I conformation due lo the deposit of thenon-ossifÌed osteoid matrix and the interruption of the osseous cortex (Figure 4). The massive growth of the superiormaxilla caused a reduction of the air cavities of the maxillary sinuses and a signifìcant involvement of the right orbitalfloor (Figure 5).
Osseous scintigraphy (555MBq 99m CT-MDP) revealed aclear alteration caused in the fullness of the face with a disomogeneous hyperaccumulation on the mandible and themaxillae.
Figure 5.-Significant right orbita! l100r im-oh-emem.
cally activated inside the expanding lesions2 Thesecharacteristics are similar to those of other osseouspathologies, such as the brown tumour of hyperparathyroidism, giant cell tumour and centraI andperipherai giant cell granuIoma.5
The treatment of cherubism is controversial.The therapies recommended include observation,
calcitonin therapy, Iiposuction, radiotherapy and/orsurgery.2-4,13
Many surgeons assume an attitude of "wait andsee", limiting surgicai intervention to decompressionof the orbits or removai of any teeth in an ectopicposition. Although some surgeons suggest that surgery corrects the osseous deformities of cherubism,it is rareIy recommended and can itself cause thegrowth of quiescent lesions2
Case report
An ll-year old patient came under oùr obseryation in May2007, after having been treated pre\'ioush-. at the age of 9. inanother hospital. On leaving that hospital. he ,',as diagnosedas suffering from a suspected dysplasia of the superior andinferior maxilla.
Familial anamnesis did not bring to !ight anv data con-
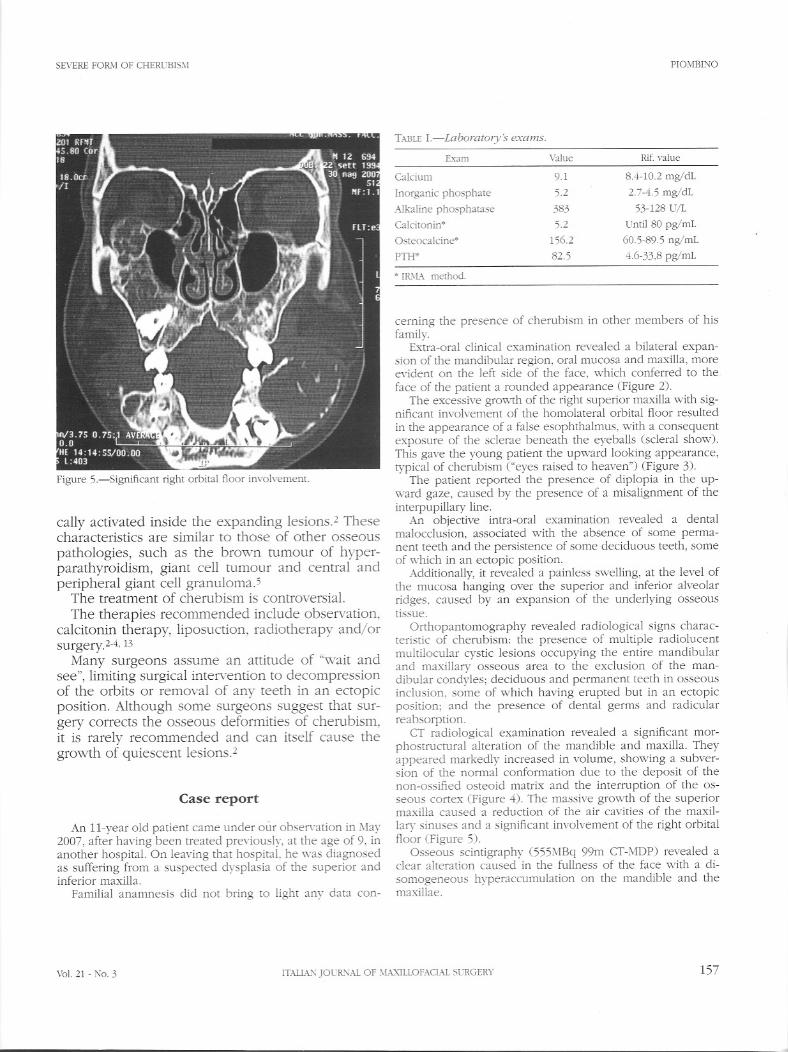
TWlE I.-LaboratOlY~'i exams.
Exam
Calcium
Inorganic phosphate
.,>JkalinephospharaseCalcitonin*
Osreocalcine*
Fili*
• IR.\L\ merhod.
Yalue
9.1
52
38352
156.2
82.5
Rif. value
8.4-10.2 mg/dL
27-4.5 mg/dL
53-128 U/L
Unti! 80 pg/mL
60.5-89.5 ng/mL
4.6-33,8 pg/mL
Val. 21 - No.3 ITAIL\_'\ JOUR.'\Al OF \L","\1LLOFACL\l SL'RGERY 157

PIOMBINO SEVERE FOR/0 OF CHERUBISM
Figure 6.-A, B) Curettage of the orbital floor ,Yitha transconjuncti,-alapproach.
Figure 7.-Postoperative resolution of the ophthalmopaù1y.
Hematochemical examinations reyealed an elevated levelof alkaline phosphatase and inorganic phosphatase, norma lcalcaemia and phosphoremia and slightly elevated osteocalcin and parathormone levels CTable I).
On the base of this clinical and radiological assessment. anincisional biopsy was performed at the mandibular junction toestablish a definitive diagnosis.
The histological examination of the lesion produced a positive result for cheIUbism.
As the patienr presenred esophthalmus and diplopiaand there was a risk of loss of vision due to the compression on the optic nerve only the right orbita l ,yassurgically treated. A decompression of the orbit ,,-ascarried out by means of a curettage of the floor ",-ith atransconjunctival approach (Figure 6). At the first postsurgical follow-up the clinica l and radio logica l reportsshowecl a resolution of the ophthalmopathy (Figure 7),a restoration of the orbital volume (Figure 8) and animprovement of the esthetic appearance of the face. A
Figure 8.-Postoperati\-e radiological outcome: restoration of theorbital yolume.
158 ITALIA."\ ]OURl'iAL OF MAXILLOFACIAL SURGERY Oecember 2010

SEVERE FORM OF CHERUBISi\1 PIOMBINO
TABLE II.-Modified Motamedi system.
Grade
Il
III
IV
v
VI
Definition
Lesion of the mandible "'ithout signs of rom resorption
Lesions involYing the mandible and maxilla "'ithout signsof rom resorption
Aggressive lesion of the mandible "'ith signs of rom resorption
Lesions iI1\'oIYingthe mandible and m~'illla "'ith signs ofrom resorption
The rare. massive!\' gro,,·ing. aggressive. and extensi\'elvdeforming juvenile lesions in\'o!\'ing the maxilla and themandible
The rare. massi\'ely gro,,·ing. aggressi\e. and extensi\'e!\'deforming juvenile lesions in\'o!\'ing the maxilla. mandible, and orbits
ourselves to an attitude of "wait and see", in accordance with the data found in internationalliteraturethat reports, in the majority of cases,6.9 a spontaneous resolution of the disease after puberty,s· 7,15,17,18
Conclusions
The results obtained in the postsurgical follow-upsuggest that an immediate decompressive surgicalapproach on the orbit should be taken into consideration for the resolution of ophthalmopathy andthe associated risks, while waiting for the spontaneous regression of the eÀ1:ra-orbitallesions.
References
weekly follow-lIp was planned to check the expectedspontaneolls resollltion of the pathology.
Discussion
Cherubism is a rare non neoplastic fibro-osseousdysplasia related to genetic mutations, for which,unti! today, definitive epidemiological data does notexist. Approximately 280 cases of cherubism havebeen reported in literature.13 Numerous grading systems have been proposed to define the severity ofthe disease.14. 16In 1998, Motamedi described fivegrades of the disease, defining as severe Cgrade V)the profile characterized by a contemporaneous involvement of the mandible and the superior maxilla.11CE. Raposo-Amaral et al. in 20072 suggested theaddition of a grade VI to the Motamedi classification to describe the orbital involvement, in additionto that of the mandible and the superior maxilla,which had not previously been taken into consideration CTableII). According to such a classllcation,our patient is to be attributed to a severe form ofthe disease Cgrade VI). He presented, in fact, a significant involvement of the orbita l floor that causedthe appearance of a false esophthalmus associatedwith diplopia and a serious risk 9f a loss of visiondue to optic atrophy.1. 7 12Based on these considerations surgical treatment involved exclusively theright orbital floor to decompress the orbit, to resolvethe ophthalmopathy and to avert the risk of opticatrophy. As for the extra-ocular lesions, we limited
l. Carroll AL, SlIllivan T). Orbital involvement in chembism. Clinical and Experimemal Ophùlalmology 2001;29:38-40.
2. Raposo-Amaral CE, de Campos Guidi M, Warren SM, Almeida AB. Amstalden E,\1, Tiziane V et al. Two-stage surgicaltreatment of severe cherubism. Ann Plast Surg 2007;58:6455I.
3. de Lange J, Rosenberg Al van den Akker HP, Koole R, Wirds JJ,
van den Berg H. Treatment of centrai giant cell granuloma ofthe jaw with calcitonin. Int J Oral Maxillofac Surg 1999;28:3726.
4. De Lange J, Van den Akker HP, Scholtemeijer M. Cherubismtreated with calcironin: report of case. J Oral Maxillofac Surg2007:65:1665-67.
5. Carvalho Silva E, Carvalho Silva GC, Vieira Te. Chembism clinicoradiographic features, treatmem, and long term follow-up of8 cases. J Oral Maxillofac Surg 2007;65:517-22.
6. Hamner JE 3rd, Ketcham AS. Chembism: an analysis of treatmenI. Cancer 1969;23:1133-43.
7. Ha,,'es M). Cherubism and its orbita! manifestations. OphthalPlast Reconstr Surg 1989;5:133-40.
8. Hyckel P, Berndt A, ScWeier P, Clemem JH, Beensen V, PetersH el al. Cherubism new hypotheses on pathogenesis and therapeutic consequences. J Craniomaxillofac Surg 2005;33:61-8.
9. Regezi JA, Scuiba J). Oral pathology. Philadelphia, PA: Saunders: 1989. p. 439.
lO. Jones WA. Familial multilocular cystic disease of the jaws. Am JCancer 1933;17:946-50.
Il. Kalantar Motamedi MH. Treatment of cherubism with locallyaggressive behavior presenting in adu!thood: report of four
cas~s and .~ propose~ of new grading system. J Oral MaxillofacSur", 1998,)6:1336-4_.12. .'.1arck PA, Kudryk WllL.Chembism. J OtolaryngoI1992;21:84-7.13. Ozkan Y. Varol A. Turker K. Aksakalli N. Basa S. Clinical and
radiological e\'aluation of cherubism: a sporadic case reportand reYie'" of the literature. 1m J Pediatr Otorhinolaryngol2003:67:1005-12.
14. Ramon Y, Engelberg IS. An unusually extensive case of cherubism. J Oral Maxillofac Surg 1986;44:325-8.
15. Roginsk-y VV.h'anov AL, Ovtchinnikov lA, Khonsari RH. Familial cherubism: the experience of me iVloscow CentraI Institutefor Stomarologv and -"1~"\.il!o-FacialSurgery. Int J Oral Maxillofac Surg 2009:38:218-23.
16. Se"'ard GR, Hankey GT. Cherubism. Oral Surg Ora! Med OralPathoI1957:10:952-747
VoI. 21 - No.3 ITAlL"-.l'\lJOUR1'\Al OF MAXILLOFAClAL SURGERY 159

PIOMBINO
17. Silva GC, Gomez RS, Vieira TC, Silva EC. Cherubism: long-termfollow-up of 2 patiems in whom it regressed without treatment.Br J Oral Maxillofac Surg 2007;45:567-70.
18. Timosca Gc. Cherubism: regression of the lesions and spontaneous bone regeneration. Rev Stomatol Chir Maxillofac1966;97: 172-7.
SEVERE FORJ\1 OF CHERUBISM
19. Tiziani V, Reichenberger E, Buzzo CL, Niazi S, Fukai N, Stiller Met al. The gene for cherubism maps to chromosome 4p16. AmJ Hum Genet 1999;65:158-66.
20. Ueki Y. Tiziani V, Sanranna C et al. Mutations in the gene encoding c Abl binding protein SH3BP2 cause cherubism. NatGenetic 2001:28:125-6.
160 ITAll,,-" JOUR"Al OF HAXILLOFACL>\l SCRGERY December 2010