vs vs a comparison of accuracy and efficiency among different techniques for measuring cardiac...
TRANSCRIPT

vs vs
A comparison of accuracy and efficiency among different techniques for measuring cardiac output
Alex Yartsev, 10-05-2011

Cardiac Output
• Volume of blood pumped by the left ventricle over 1 minute• Measured in litres per minute
• Expresed as Q
Q = stroke volume x heart rate
Measurement of Cardiac Output
• Holy grail of physiology• Numerous methods tried• Each has strengths• Each has weaknesses

The Gold Standard
There is no gold standard.
The “practical gold standard” is the PA catheter,
which uses
The Fick Principle
Pugsley et al. Cardiac output monitoring: is there a gold standard and how do the newer technologies compare? Seminars in Cardiothoracic & Vascular Anesthesia. 14(4):274-82, 2010 Dec.

The Fick Principle– First described by Adolf Eugen Fick in 1870
BASIC PREMISE: Blood flow out of the heart can be calculated using oxygen as
a marker, provided you know how much oxygen is being consumed by the whole body.
Requires several technically complex measurements to be taken
Guyton and Hall Textbook of Medical Physiology - 10th ed.The ICU Book by Paul L Marino, 3rd ed.

The Fick Principle
VO2 = (Q x CA) – (Q x CV)
Human BodyConcentration of oxygen in
arterial blood(CA)
Concentration of oxygen in
venous blood(CV)
Oxygen consumption in ml/min(VO2)
Guyton and Hall Textbook of Medical Physiology - 10th ed.The ICU Book by Paul L Marino, 3rd ed.

The Fick Principle
Or…
Q =
Human BodyConcentration of oxygen in
arterial blood(CA)
Concentration of oxygen in
venous blood(CV)
Oxygen consumption in ml/min(VO2)
VO2
CA - CVGuyton and Hall Textbook of Medical Physiology - 10th ed.The ICU Book by Paul L Marino, 3rd ed.

The Fick Principle
Or…
Q =
Human BodyConcentration of oxygen in
arterial blood(CA)
Concentration of oxygen in
venous blood(CV)
Oxygen consumption in ml/min(VO2)
VO2
CA - CV
Assumed:125ml O2
per minute per m2 of body surface area
Guyton and Hall Textbook of Medical Physiology - 10th ed.The ICU Book by Paul L Marino, 3rd ed.

Comparing Indirect Measurement of Cardiac Output
• Pulmonary Artery Thermodilution (PAC)
• Pulse Contour measurement (PiCCO)
• Observation of signs of adequate / inadequate cardiac output

The Swan-Ganz Pulmonary Artery Catheter
• Measurement of Q with trans-right-heart thermodilution• Modification of the Fick principle
Guyton and Hall Textbook of Medical Physiology - 10th ed.The ICU Book by Paul L Marino, 3rd ed.Swan HJ, Ganz W, Forrester J, Marcus H, Diamond G, Chonette D (August 1970). "Catheterization of the heart in man with use of a flow-directed balloon-tipped catheter". N. Engl. J. Med. 283 (9):
Jeremy Swan 1922-2005 William Ganz 1919-2009
Swan-Ganz catheter, 1970 -
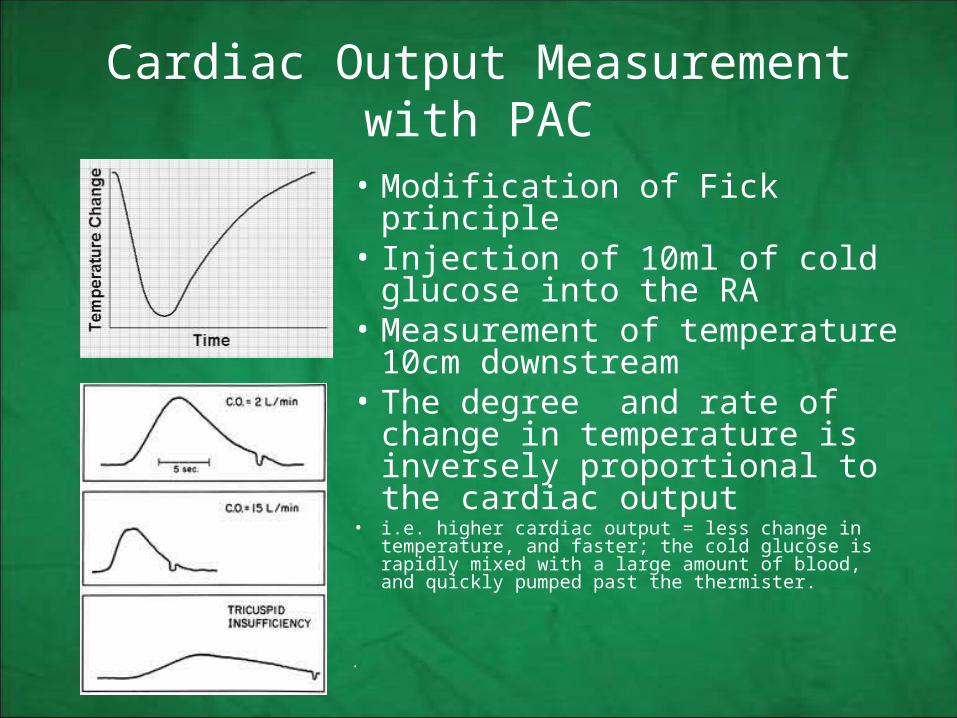
Cardiac Output Measurement with PAC
• Modification of Fick principle• Injection of 10ml of cold glucose
into the RA• Measurement of temperature
10cm downstream• The degree and rate of change
in temperature is inversely proportional to the cardiac output
• i.e. higher cardiac output = less change in temperature, and faster; the cold glucose is rapidly mixed with a large amount of blood, and quickly pumped past the thermister.
•

Limitations of PAC• Despite using correction factors, heat transfer to catheter wall and right heart
tissues leads to overestimation of cardiac output
• Other sources of error:– Rate of cold fluid infusion– Hematocrit – Intracardiac shunts– Fluctuation in pulmonary artery temperature in a humidified
heated circuit– Variation in cardiac output due to positive pressure ventilation
…Also, it kills people
Gomez CM, Palazzo MG. Pulmonary artery catheterization in anaesthesia and intensive care. Br J Anaesth 1998; 81: 945–5
PiCCO: pulse contour cardiac output monitoring• Area under aortic flow curve• Continuous monitoring• Requires frequent calibration:
properties of the vessels are constantly changing
• Calibrated with transpulmonary thermodilution
Wesseling KH, Jansen JR, Settels JJ, Schreuder JJ (May 1993). "Computation of aortic flow from pressure in humans using a nonlinear, three-element model". J. Appl. Physiol. 74 (5): 2566–73.

PiCCO: pulse contour cardiac output monitoring
• Bottom line: The area under the curve correlates with the stroke volume• Cardiac output is calculated from stroke volume and heart rate.
Wesseling KH, Jansen JR, Settels JJ, Schreuder JJ (May 1993). "Computation of aortic flow from pressure in humans using a nonlinear, three-element model". J. Appl. Physiol. 74 (5): 2566–73.
http://www.creaghbrown.co.uk/anae/hdmon.htm#PiCCO

Limitations of PiCCO
• If poorly calibrated, yields garbage data• Copes poorly with sudden changes of vascular tone• Relies on OPTIMAL arterial pressure signal
• Pulse contour cannot be interpreted in– IABP– Severe aortic regurgitation– Sustained arrhythmias
• Essentially, you need a normal-looking arterial waveform, and a hemodynamically stable patient. ? Defeats the purpose.
Wesseling KH, Jansen JR, Settels JJ, Schreuder JJ (May 1993). "Computation of aortic flow from pressure in humans using a nonlinear, three-element model". J. Appl. Physiol. 74 (5): 2566–73.
Intensive Care Medicine: Annual Update 2008 By Jean-Louis Vincent

Clinical assessment of cardiac output
• Externally obvious or non-invasively measurable markers of cardiac performance and tissue perfusion– Capillary refill– Peripheral temperature– Palpated pulse pressure– Heart rate– Noninvasive blood pressure– Cardiac auscultation– History, rumour and intuition
.Shephard JN et al Bedside assessment of myocardial performance in the critically ill. Intensive Care Med. 1994 Aug;20(7):513-21Conway J. Clinical assessment of cardiac output. Eur Heart J. 1990 Dec;11 Suppl I:148-50.

“What is his cardiac output, doctor?• Nobody will give you that at the bedside.
• “is this patient shocked” is a better question
• Most of us wont reliably answer even that
• Disagreement between any two clinicians
Stevenson LW, Perloff JK. The limited reliability of physical signs for estimating hemodynamics in chronic heart failure. JAMA. 1989;261:884-888.Joly HR, Weil MH. Temperature of the great toe as an indication of the severity of shock. Circulation. 1969;39:131-138.Butman SM, Ewy GA, Standen JR, et al. Bedside cardiovascular examination in patients with severe chronic heart failure: importance of rest or inducible jugular venous distension. J Am Coll Cardiol. 1993;22:968-974.EMST course (ATLS handbook 2009), RACS

Limitations of Bedside Cardiac Output Assessment
• Blood pressure and heart rate are of minimal use in shock• Cap refill assessment has large variability between clinicians
– We only seem to agree when its normal or SIGNIFICANTLY delayed
• Proportional pulse pressure correlates well with cardiac index ….in at least one study…– PPP = (systolic minus diastolic, divided by systolic) – PPP ≤25% = 91% sensitive for a cardiac index ≤2.2 L/min/m2.
Stevenson LW, Perloff JK. The limited reliability of physical signs for estimating hemodynamics in chronic heart failure. JAMA. 1989;261:884-888WO, CHARLES C. J et al Unreliability of blood pressure and heart rate to evaluate cardiac output in emergency resuscitation and critical illness Crit Care Med 1993; 21:218-22H Otieno et.al. Are bedside features of shock reproducible between different observers? Arch Dis Child. 2004 October; 89(10): 977–979

How do they compare?
What do you compare?… Accuracy? versus which gold standard?…Safety?…influence on hard outcomes?
Which is “better”, in a non-specific sense?
Pugsley et al. Cardiac output monitoring: is there a gold standard and how do the newer technologies compare? Seminars in Cardiothoracic & Vascular Anesthesia. 14(4):274-82, 2010 Dec.

PAC vs. human
• Connors (1996): 5735 patients prospective cohort, 1989-1994– PAC increases mortality in first 24 hrs
• Sandham (2003): RCT, 3800 pts, – goal directed PAC-guided mx vs non-PAC care – Surgical ICU for the over-60s– No survival benefit, no mortality increase. PAC doesn’t seem to matter.
• Harvey (2006): Cochrane meta-analysis: PAC vs no PAC.– PAC does not influence length of stay or mortality, but increases cost.
Uchino et.al Pulmonary Artery Catheter Versus Pulse Contour Analysis: A Prospective Epidemiological Study Crit Care. 2007;10(6)Harvey S, Young D, Brampton W, Cooper A, Doig GS, Sibbald W, Rowan K. Pulmonary artery catheters for adult patients in intensive care. Cochrane Database of Systematic Reviews 2006, Issue 3Sandham JD, Hull RD, Brant RF. A Randomized, Controlled Trial of the Use of Pulmonary-Artery Catheters in High-Risk Surgical Patients. Indian J Crit Care Med [serial online] 2003 [cited 2011 May 10Connors AF Jr, Speroff T, Dawson NV, et al. The effectiveness of right heart catheterization in the initial care of critically ill patients. JAMA 1996; 276: 889–97

PiCCO vs Human
• De Waal (2007) – post cardiac surgery patients – Acceptable assessment of CO in closed-chest conditions and in stable ICU patients
• Belda (2010) compared PiCCO to TTE: – good correlation to systolic function
No studies comparing PiCCO vs no PiCCO?
Belda et. al. Clinical validation of minimally invasive evaluation of systolic function; Rev Esp Anestesiol Reanim. 2010 Nov;57(9):559-64.de Waal EE Validation of a new arterial pulse contour-based cardiac output device. Crit Care Med. 2007 Aug;35(8):1904-9.

PiCCO vs PAC
• Cecconi (2010) : PiCCO accuracy, as compared to PAC gold standard– CO measurements were in excellent agreement when PiCCO is well calibrated
• Uchino & Bellomo (2007) : 331 pts, prospective epidemiological study– PiCCO fluid balance was more positive, ventilator free days were fewer– “Choice of monitoring did not influence major outcomes”
All these studies have excluded patients with permanent arrhythmias.
All agree: in hemodynamically unstable patients, PiCCO becomes less reliable than PAC
Uchino et.al Pulmonary Artery Catheter Versus Pulse Contour Analysis: A Prospective Epidemiological Study Crit Care. 2007;10(6)Cecconi M. Dawson D. Casaretti R. Grounds RM. Rhodes A. A prospective study of the accuracy and precision of continuous cardiac outputmonitoring devices as compared to intermittent thermodilution. Minerva Anestesiologica. 76(12):1010-7, 2010 Dec.Mayer J, Boldt J, Schöllhorn T, et al. Semi-invasive monitoring of cardiac output by a new device using arterial pressure waveform analysis: a comparison with intermittent pulmonary artery thermodilution in patients undergoing major cardiac surgery. Br J Anaesth 2007; 98:176–182.

A doctor’s intuition vs invasive measurements, specifically for CO estimation.
• No RCTs or even large studies
• Eisenberg (1984) : – 113 doctors asked to assessed CO before insertion of PAC– Correctly guessed CO 50% of the time– Changed their therapy based on PAC 58% of the time– Added unanticipated therapy 30% of the time
Eisenberg PR, Jaffe AS, Schuster DP. Clinical evaluation com pared to pulmonary artery catheterization in the hemody namic assessment of critically ill patients. Crit Care Med. 1984;12(7):549-553.

The bottom line:• PAC remains the “gold standard”, in absence of an actual gold standard
• PAC and PiCCO in stable patients agree often enough to be interchangeable in assessing cardiac output
• PAC reserved for abnormal aortas, balloon pumps arrhythmias and changing vascular tone
• PiCCO is safer in every other situation
• Humans are 50% accurate in estimating cardiac output

No further questions, please.