vt chapter apta cervico-thoracic spine assessment … · vt chapter apta cervico-thoracic spine...
TRANSCRIPT

10/13/14
1
! Hand towel ! Wear tank top (not sports bra) ! SW bring
" Coloured spine " Dynadjust " Mulligan straps " Hand towel " Ipad (fully charged) " Mob wedges
VT Chapter APTA Cervico-thoracic spine assessment and
treatment (patient in the seated position)
Sonya Anderson Worth, PT, PGDipHSc, OCS, FAAOMPT [email protected]
Sonya Anderson Worth, PT, PGDipHSc, OCS, FAAOMPT ! Physical Therapist in the Outpatient Physical Therapy team at Fletcher
Allen Health Care in Burlington, VT where I treat patients with a variety of neuromusculoskeletal dysfunctions with a focus on treatment for patients with spinal, shoulder and hip pain.
! Lab Instructor in the musculoskeletal curriculum of the UVM entry-level Doctorate of Physical Therapy Program since 2001.
! Co-leader of PT 352 an International Manual Therapy Collaboration Class. This is an elective class for DPT students and licensed Physical Therapists. The class is taught at Auckland University of Technology and collaborates with AUT’s Post Graduate Diploma in Manipulative Physiotherapy in 2015, in 2016 the class is taught at Bond University, Australia and collaborated with Bond’s DPT students.
! As a native New Zealander, I received my Physical Therapy undergraduate training at Otago University, Dunedin, New Zealand, and my advanced training in Manual and Manipulative Therapy from Auckland University of Technology, New Zealand.

10/13/14
2
! Your patient has neck and/or upper thoracic symptoms but you don't have a treatment table.
! During this 2 hour session you will learn cervical and upper thoracic spine evaluation and treatment techniques to use when the patient is seated. " Cervical Assessment " Thoracic Assessment " Differentiation between Cervical and Thoracic " Cervical Treatment options " Thoracic Treatment options " Cervico-thoracic treatment options
Cervical Spine Assessment ! Refer to separate pdf file Advanced Cervical Spine
Examination Template ! Most of a Cervical Spine examination is performed in
sitting " Accessory motion testing can be performed in sitting " Palpation can be performed in sitting " Most MMTs can be modified to a sitting position, be sure to
document the alternative test position
Cervical Assessment ! Seated Cervical PPIVMs ! In neutral
" Seated NAGs central " Seated NAGs unilateral
! At end of available physiological range " NAGs " Unilateral NAGs

10/13/14
3
PPIVMs …. What are they? ! Passive Physiological Inververtebral Movements
" Flexion " Extension " Rotation " Sidebending " Palpate an intervertebral segment while passively moving the
spine " Assess for hyper-, hypo, or normal motion with or without pain
provocation " Use this information to localize your accessory motion testing
NAGs (mid CSP and upper TSP) NAG (natural apophyseal glide)
! NAGs are weight bearing joint accessory mobilisations for the spine! ! Useful as an assessment and a treatment technique. ! Essentially a PA
" Posterior to anterior glide along the plane of the facet. ! These are a precursor to MWM (mobilization with movement) for the spine ! Mid to end range techniques for:
" Pain relief " Improvement in intersegmental and regional ROM (especially flexion)
! Patient is weight bearing ! Therapist applies NAG along facet plane using spinous process or transverse
processes as bony contact ! The spinal level being moved will flex/gap/open/slide anterior & superiorly with
respect to the level below ! Inferior facets of C6 move superiorly and anteriorly on superior facets of C7
NAGs (mid CSP and upper TSP) Weight bearing Accessory Mobilisation for the Spine
! Patient sitting ! Therapist
" Stand to side of patient. " Cradle patient’s head and neck, maintain head in midline. " Hook R) pinky finger around spinous process, support
suboccipital region with rest of hand ! Procedure
" Lateral border of L) thenar eminence is under R) pinky and delivers NAG.
" Rhythmic oscillations. ! Indications
" Assess intersegmental motion & pain provocation/alleviation. " Treat segmental movement loss &/or pain.
! Comments " Gentle cervical traction can be added " Can be performed unilaterally over articular pillar to promote
rotation

10/13/14
4
NAGs (mid CSP and upper TSP)
! NAGs can be performed bilaterally over articular pillar if spinous process is painful
! Especially useful in upper thoracic spine
! NAGs can be performed unilaterally on the articular pillar to assess rotation
Thoracic assessment ! Refer to separate pdf file Advanced Thoracic Spine Examination
Template ! Most of a Thoracic Spine examination can be performed in sitting
" Accessory motion testing can be performed in sitting " Palpation can be performed in sitting " Most MMTs can be modified to a sitting position, be sure to document the
alternative test position ! NAGs
" See Cervical Assessment slide ! Seated PPIVMs
" Flexion " Extension " Rotation " Sidebending
PPIVMs …. What are they? ! Passive Physiological Inververtebral Movements
" Flexion " Extension " Rotation " Sidebending " Palpate an intervertebral segment while passively moving the
spine " Assess for hyper-, hypo, or normal motion with or without pain
provocation " Use this information to localize your accessory motion testing

10/13/14
5
Differentiation between lower cervical and upper thoracic spine ! Many times patients present with pain or dysfunction at the end of
their available cervical range of motion ! Commonly the symptoms and loss of function are felt during cervical
rotation, extension or side bending ! The motion segment at fault may be lower cervical or upper thoracic ! Differentiating the level at fault directs your treatment to the
appropriate level ! First, attempt to differentiate between the cervical and thoracic
regions (regionalization) …. Next slide ! If the cervical spine is the region at fault, use NAGs to localize the
specific motion segment …. See Cervical slides ! If the thoracic spine is the region at fault, use thoracic
segmentalisation to localize the specific motion segment ….Next slides
Is it Cervical or Thoracic Spine? Regionalisation using provoking/alleviating tests ! Axial compression is painful (distraction relieves)
" Could be CSp or TSp " Differentiate by comparing with TSp compression (still painful?
TSp) ! R) Rotation CSp in neutral is painful
" Could be CSp or upper TSp " Differentiate by rotating trunk & neck to the L) to end range, fix
TSp at this end range, then rotate CSp to R), (still painful? CSp) ! CSp extension is painful
" Could be CSp or upper TSp " Differentiate with full C & T spine flexion (slump), fix both 1st ribs
(preventing TSp extension), now slowly extend CSp (still painful? CSp)
! Segmentalisation using provoking/alleviating testing (in sitting):(Regionalisation testing has implicated the CT junction) " R) rotation into pain, then back off “just a bit” " Then test segmentally from below to avoid irritating segments prior to
testing them " Fix T5 (thumb on Left side of sp pr) " Move T4 into R) rotation (thumb on right side of sp pr) " By default T3 will slightly rotate L) " Move up the spine until pain is provoked, this is the dysfunctional
segment " Confirm by performing a L) rotation to same segment while head/neck
is rotated into pain (pain should be alleviated)
When rotation regionalization implicates the CT junction, Segmentalisation can be done seated (or prone, or side lying)

10/13/14
6
Practice time! ! Cervical PPIVMs ! Thoracic PPIVMs ! Regionalisation between cervical and thoracic spine ! Segmentalisation in thoracic spine ! NAGS to assess Cervical and upper Thoracic accessory
motion
Cervical treatment ! CSP NAGs ! CSP unilat NAGs ! CSP flexion SNAG ! CSP extension SNAG ! CSP rotation SNAG ! Self SNAGs ! Deep cervical flexor strengthening
NAGs (mid CSP and upper TSP) Weight bearing Accessory Mobilisation for the Spine
! Patient sitting ! Therapist
" Stand to side of patient. " Cradle patient’s head and neck, maintain head in midline. " Hook R) pinky finger around spinous process, support
suboccipital region with rest of hand ! Procedure
" Lateral border of L) thenar eminence is under R) pinky and delivers NAG.
" Rhythmic oscillations. ! Indications
" Assess intersegmental motion & pain provocation/alleviation. " Treat segmental movement loss &/or pain.
! Comments " Gentle cervical traction can be added " Can be performed unilaterally over articular pillar to promote
rotation

10/13/14
7
NAGs (mid CSP and upper TSP)
! NAGs can be performed bilaterally over articular pillar if spinous process is painful
! Especially useful in upper thoracic spine
! NAGs can be performed unilaterally on the articular pillar to assess rotation
SNAGs (Sustained Natural Apophyseal Glides) “MWMs for the spine”
! SNAGs are a sustained facet joint upslope, combined with active cervical movements
! SNAGs are useful in all regions of the spine, but demonstrated tonight for the Cervical and upper thoracic spine
! Facet joint mobilisation is sustained while the patient performs active “movement”
! The “movement” is active spinal motion performed with end range overpressure
! SNAGs are always performed in a weight bearing position (sit or stand)
! Central SNAGs on spinous processes are used to treat flexion or extension
! Unilateral SNAGs (on transverse process or lamina) or transverse SNAGs (on lateral aspect of spinous process) are used to treat rotation
Cervical Extension SNAGs ! Patient sitting ! Therapist
" Stand behind the patient. " Medial border of one thumb on inferior aspect of C7
spinous process, other thumb reinforces this. ! Procedure
" Glide C7 spinous process cranially along the line of the facets.
" While maintaining this glide ask the patient to extend their head.
" Repeat 3-6 times, then reassess before continuing if indicated.
! Indications " Treat cervical extension movement loss &/or pain
! Comments " Note that no overpressure is applied during a
Cervical extension SNAG. The weight of the head falling behind the line of gravity provides adequate overpressure.
10/13/14
8
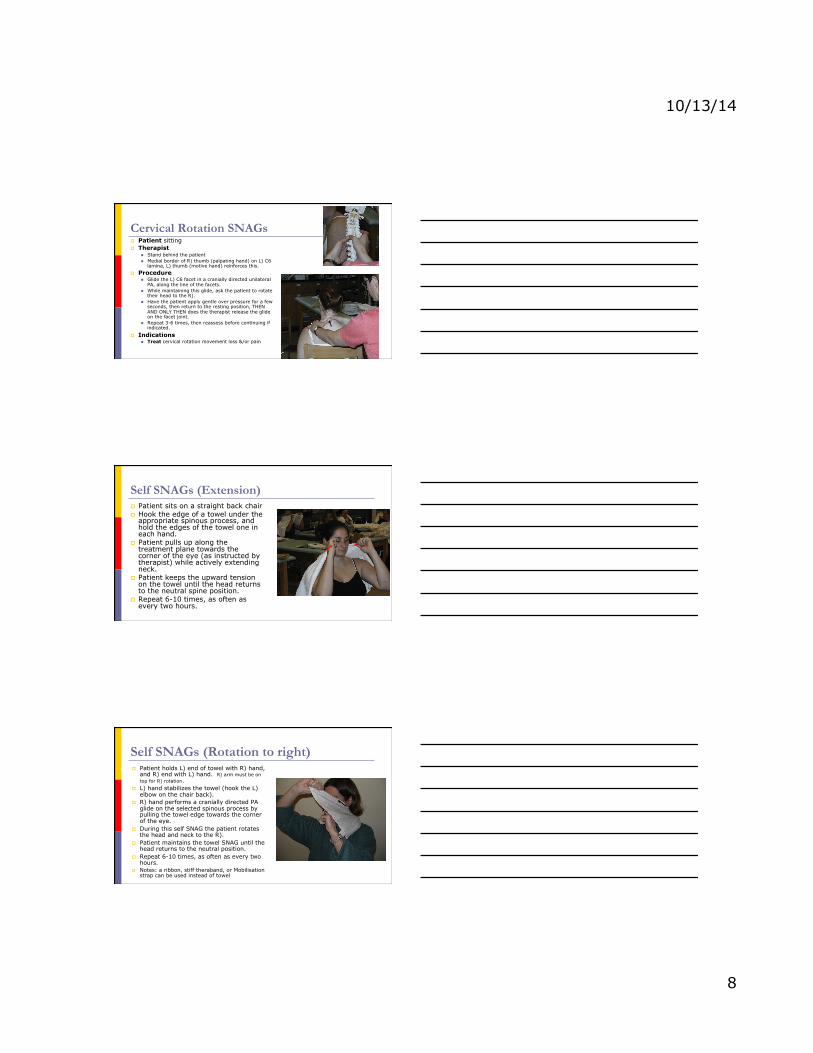
Cervical Rotation SNAGs ! Patient sitting ! Therapist
" Stand behind the patient " Medial border of R) thumb (palpating hand) on L) C6
lamina, L) thumb (motive hand) reinforces this. ! Procedure
" Glide the L) C6 facet in a cranially directed unilateral PA, along the line of the facets.
" While maintaining this glide, ask the patient to rotate their head to the R).
" Have the patient apply gentle over pressure for a few seconds, then return to the resting position, THEN AND ONLY THEN does the therapist release the glide on the facet joint.
" Repeat 3-6 times, then reassess before continuing if indicated.
! Indications " Treat cervical rotation movement loss &/or pain
Self SNAGs (Extension) ! Patient sits on a straight back chair ! Hook the edge of a towel under the
appropriate spinous process, and hold the edges of the towel one in each hand.
! Patient pulls up along the treatment plane towards the corner of the eye (as instructed by therapist) while actively extending neck.
! Patient keeps the upward tension on the towel until the head returns to the neutral spine position.
! Repeat 6-10 times, as often as every two hours.
Self SNAGs (Rotation to right) ! Patient holds L) end of towel with R) hand,
and R) end with L) hand. R) arm must be on top for R) rotation.
! L) hand stabilizes the towel (hook the L) elbow on the chair back).
! R) hand performs a cranially directed PA glide on the selected spinous process by pulling the towel edge towards the corner of the eye.
! During this self SNAG the patient rotates the head and neck to the R).
! Patient maintains the towel SNAG until the head returns to the neutral position.
! Repeat 6-10 times, as often as every two hours.
! Notes: a ribbon, stiff theraband, or Mobilisation strap can be used instead of towel

10/13/14
9
Patient Handout – permission to copy is granted by Sonya Worth PT PGDipHSC OCS FAAOMPT Self MWM Lower cervical rotation left (to improve right rotation do the opposite)
! Sit well supported, head aligned over trunk ! RIGHT middle finger grasps LEFT side of neck bones at level of
skin crease ! Apply gentle pressure to assist this bone to turn left WHILE
turning head to left ! If full rotation is not painfree, move your middle finger up or
down slightly and try again until rotation is painfree
! Add gentle over stretch, hold 3 seconds ! KEEP pressure with right hand while returning head to midline ! Repeat 5-10 times, as often as every 2 hours.
! IF turning head to right is uncomfortable … ! use this same technique with the opposite hand placements and turn head to right
Deep Neck Flexor Training ! Deep neck flexors are:
" Upper cervical spine ! rectus capitus anterior ! rectus capitus lateralis
" Lower cervical spine ! longus capitus ! longus colli
! Extrinsic neck flexors are: " sternocleidomastoid " anterior and middle scalene
often the extrinsic muscles are the dominant muscle group during cervical flexion causing anterior translation of the head and cervical spine with diminished anterior sagittal plane rotation (true cervical spine flexion).
Retraining of the Deep Neck Flexors helps normalise the forces in the cervical spine and restore painfree function.
Deep neck flexors

10/13/14
10
Extrinsic neck flexors
Beer A, Treleaven J & Jull G. Can a functional postural exercise improve performance in the cranio-cervical flexion test? – A preliminary study. Manual Therapy. 2012;17:219-224
! A pilot study, n=20 patients with persistent neck pain and poor performance on CCFT
! Investigated effects of training the DCF in functional position (neutral spine sitting with added neck lengthening)
! This neck lengthening maneuver strongly activates the longus colli
! Exercise effect was assessed by changes (pre and post training) in SCM EMG activity during CCFT
Interventions Beer A, Treleaven J & Jull G. Can a functional postural exercise improve performance in the cranio-cervical flexion test? – A preliminary study. Manual Therapy. 2012;17:219-224.
! 1 visit to teach seated DCF exercise " Neutral lumbopelvic position " Gently “lift the base of the skull from the top of the
neck” as if to lengthen the neck " Scapula position correction if needed
! 2 further visits within 2 week study to check performance of the exercise and compliance with exercise program
! HEP prescription " 10 seconds hold every 15-20 minutes of every waking
hour for 2 weeks ! 2 weeks chosen for this pilot study as a change in muscle
behaviour can be expected in this time frame
" Record exercise frequency in log book

10/13/14
11
Results Beer A, Treleaven J & Jull G. Can a functional postural exercise improve performance in the cranio-cervical flexion test? – A preliminary study. Manual Therapy. 2012;17:219-224
! After 2 weeks of daily seated DCF exercise " SCM EMG activity in CCFT was significantly reduced at 1st and 3rd stages of
CCFT " SCM EMG activity at 2nd, 4th and 5th stages was reduced but did not reach
statistical significance " These findings infer an increase in DCF activity
! Earlier invasive studies (Fountain et al 1966! In Beer et al 2012) have shown this neck lengthening exercise strongly activates longus colli
! Jull et al 2009 (In Beer et al 2012) saw reduced SCM activity and increased in DCF activity when training the DCF in supine using CCFT
! This pilot study suggests a functional seated DCF exercise can improve DCF recruitment in the CCFT
Clinical Implications Beer A, Treleaven J & Jull G. Can a functional postural exercise improve performance in the cranio-cervical flexion test? – A preliminary study. Manual Therapy. 2012;17:219-224
! Motor learning research tells us that repetition is critical for motor learning " We all know our most compliant patients will lie supine 2-4 times a day at best to
complete any exercise! ! On average the functional seated DCF exercise in this study was performed 15
times per day during the 2 weeks of the study " Enough repetitions for motor learning and behaviour change AND it is functional
! Clinically, even greater improvement might be expected with a combination of functional seated DCF AND formal hook lying CCFT training
! There is enough support in this study for us to confidently include BOTH hook lying AND seated DCF exercises in our evidence based treatment of patients with neck pain
Cervico-thoracic junction treatment ! Seated 1st rib ! Seated 2nd rib ! MWM bilateral transverse glide with CSP rotation ! Rotation SNAGs (refer to Cervical Treatment slides) ! Self rotation SNAGs (refer to Cervical Treatment slides)

10/13/14
12
1st & 2nd rib indirect mobilisation ! Patient
" Seated, arms loosely crossed, hand cupped under elbow of side to be treated
! Therapist " Standing behind and slightly to side to be treated
! Procedure " Palpate posterior angle of 1st rib (use C7 as reference) " Hypothenar eminence fixes posterior angle of 1st rib " Motive hand cups under patient’s elbow/hand " Lift patient’s arm up and down in a slow oscillating motion
approximately 1 per second " Keep 1st rib fixed firmly, lock out the elbow of your mobilising hand,
use a shoulder shrug action ! Indications
" Improve mobility of 1st or 2nd rib " Treat soft tissue tension in upper trapezius " Improve end range cervical rotation
" To treat 2nd rib: stabilise 2nd rib with hypothenar eminence. Patient’s treated arm will be out from the body to create direction of thrust perpendicular to rib 2.
MWM (bilateral transverse glide) CSp/TSp with CSp rotation ! Patient sitting ! Therapist
" Stand behind patient ! Procedure
" Perform a transverse glide at C7 and T1 spinous processes
! to restore L) rotation: mob C7 to R) and T1 to L) " Combine this with the patient performing active
cervical L) rotation and adding over pressure at end of range.
" Maintain the mobilization until the patient has returned to the neutral position.
! Indications " Another method to restore rotation " Most effective in the lower CSP and upper TSP
Upper thoracic treatment ! Seated distraction ! Seated extension in forward lean ! Upper thoracic NAGs (see Assessment slides) ! MWMs (see previous slides) ! Self MWMs (see previous slides)
" Variations for upper thoracic spine ….. ! Mobilisation strap ! Back of chair

10/13/14
13
! TSpine responds well to HVT to restore motion, and to manual techniques in general
! Most used HVT technique is facet traction/gapping " Seated thoracic HVT distraction is an effective gapping technique (taught
tonight) " “Thoracic DOG”, a PA to the inferior partner of the motion segment by dorsal
fixation and thrust from A-P, patient in supine (not taught tonight, we need tables!!)
! TSpine HVT used to treat: " TSpine dysfunctions " mid and lower cervical dysfunctions " Shoulder girdle dysfunctions " Lumbar dysfunctions " Rib dysfunctions
Thoracic Spine Treatment
Examples: ! Acute locking of TSP facet joint (HVT only) ! Chronic joint and muscle stiffness, gradual loss of mobility over time (HVT, joint
and soft tissue stretching, deep massage, exercises) ! Hypermobile lower CSP segment aggravated by loss of upper TSP motion (HVT
TSP, stretch mobilisation of hypomobile TSP and shortened muscles, stabilisation exercises for CSP – deep neck flexors, posture ed ….)
! Chronic shoulder impingement due to improper scapular dynamic control, and loss of thoracic extension (HVT TSP, stabilisation of GHJ joint, motor control of GHJ and STJ …)
! Hypermobile lumbar segments aggravated by loss of lower TSP motion (HVT TSP, stabilisation of lumbar segments)
! Ribs, HVT TSP, stretch mobilisation, correct positional fault of rib.
Seated Thoracic distraction manipulation ! Patient
" seated in front of therapist " Patient’s hands behind lower neck (for upper
thoracic treatment) " Patient’s arms across chest, grasping shoulders
if able (for middle thoracic treatment)
! Therapist " Behind patient " upper chest level with patient’s mid thoracic
spine " grasps patient’s elbows
! Procedure " Perform high velocity thrust in upward and
slightly posterior direction (using legs to deliver force)
! Indications " Treat mid thoracic hypomobility &/or pain
10/13/14
14
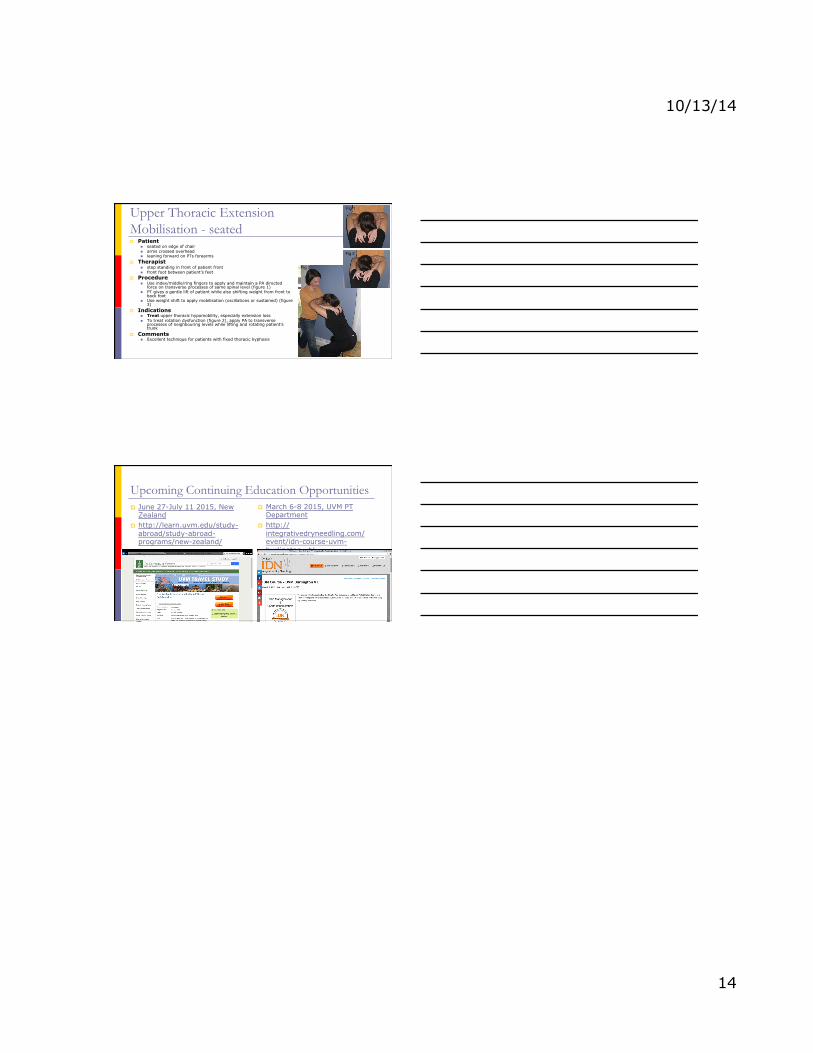
Upper Thoracic Extension Mobilisation - seated ! Patient
" seated on edge of chair " arms crossed overhead " leaning forward on PTs forearms
! Therapist " step standing in front of patient front " front foot between patient’s feet
! Procedure " Use index/middle/ring fingers to apply and maintain a PA directed
force on transverse processes of same spinal level (figure 1) " PT gives a gentle lift of patient while also shifting weight from front to
back foot " Use weight shift to apply mobilisation (oscillations or sustained) (figure
3) ! Indications
" Treat upper thoracic hypomobility, especially extension loss " To treat rotation dysfunction (figure 2), apply PA to transverse
processes of neighbouring levels while lifting and rotating patient’s trunk
! Comments " Excellent technique for patients with fixed thoracic kyphosis
Fig 2
Fig 1
Fig 3
Upcoming Continuing Education Opportunities ! June 27-July 11 2015, New
Zealand ! http://learn.uvm.edu/study-
abroad/study-abroad-programs/new-zealand/
! March 6-8 2015, UVM PT Department
! http://integrativedryneedling.com/event/idn-course-uvm-burlington-vt/