vyanga varnya samhita
DESCRIPTION
A STUDY ON THE CONCEPT OF VARNYA VIS-À-VIS CLINICAL EVALUATION OF EFFICACY OF VARNYA GANA LEPA IN VYANGA, PALLAVI.G, DEPARTMENT OF POST GRADUATE STUDIES IN AYURVEDA SIDDHANTA, GOVERNMENT AYURVEDA MEDICAL COLLEGE, MYSORE.TRANSCRIPT
i
“A STUDY ON THE CONCEPT OF VARNYA VIS-À-VIS CLINICAL
EVALUATION OF EFFICACY OF VARNYA GANA LEPA IN VYANGA”
By
Dr. PALLAVI.G, B.A.M.S.
Dissertation submitted to the
Rajiv Gandhi University of Health Sciences,
Karnataka, Bangalore.
In the partial fulfillment of the requirements for the degree of
DOCTOR OF MEDICINE (AYURVEDA)
in
AYURVEDA SIDDHANTA
Under The Guidance of
Dr. D.L. BALAKRISHNA M.D. (Ayu)
Professor and Head of the Department
Department of Panchakarma
Government Ayurveda Medical College,
Mysore – 570021
Co-Guide
DR.VASUDEV ANANDRAO CHATE M.D. (Ayu)
Lecturer,
Department of Post Graduate Studies in Ayurveda Siddhanta
Government Ayurveda Medical College,
Mysore – 570021
DEPARTMENT OF POST GRADUATE STUDIES IN AYURVEDA
SIDDHANTA,
GOVERNMENT AYURVEDA MEDICAL COLLEGE,
MYSORE.
2012

ii

iii

iv

v

vi

vii
ACKNOWLEDGEMENT
I bow to the sacred feet of Almighty, without the blessings of whom this study
would not have been completed.
I am highly thankful to Dr. Naseema K. Akhtar, Professor and HOD,
Department of PG Studies in Ayurveda Siddhanta, Government Ayurveda Medical
College, Mysore, for her constant guidance & continuous supervision at every stage
of this study.
I sincerely express my indebtedness and profound gratitude to my Former
Guide Late Dr. Shakunthala G.N, Professor and Former HOD, Department of PG
Studies in Ayurveda Siddhanta, Government Ayurveda Medical College, Mysore for
her constant guidance which helped me in selecting this study.
I sincerely express my indebtedness and profound gratitude to my Guide
Dr. D.L Balakrishna, Professor, Department of Panchakarma, Government
Ayurveda Medical College, Mysore whose, valuable guidance, timely remarks, and
helpful suggestions in this dissertation are beyond capacity of my words to reciprocate
with thankfulness
I sincerely convey my respect and gratitude to my Co-Guide Dr. Vasudev
Anandrao Chate , Lecturer ,Department of P.G Studies in Ayurveda Siddhanta ,
Government Ayurveda Medical College, Mysore, for his valuable guidance &
encouragement throughout my PG studies.
I am grateful to Principal Dr.B.A.Venkatesh, Professor, Department of Shalakya
tantra, Government Ayurveda Medical College, Mysore for his support and
encouragement.
I sincerely express my indebtedness and profound gratitude to Dr.Aruna
Mangalgi ,former Principal Government Ayurveda Medical College, Mysore for her
everlasting support and inspiration.
I sincerely express my indebtedness and profound gratitude to
Dr.K.Shivaram Prasad, Professor & Head of the Department, Department of
Panchakarma ,Shri Jagadguru Gavisiddeshwara Ayurvedic Medical College &
Hospital, Koppal, Karnataka who has extended enormous help in literary collection as
well as critical analysis.

viii
I owe my deep sense of gratitude to all my teachers Dr.T.D.Ksheerasagar,
Dr.Rajendra.V Dr.Shreevathsa ,Dr. Anand Katti and all other teaching faculty and
hospital staff for their support in this study.
I thank Dr.Lancy D’souza for his valuable help and guidance in the statistical
analysis and interpretations.
I am thankful to my senior colleagues Dr. Aparna, Dr.Geetha.P, Dr.Ranjith
Kumar Shetty, Dr.Ramesh Kumar. K.L ,Dr.Kalyani Bhusane & Dr. Kavitha.S. I owe
my special thanks to my classmates Dr.Aravind.B.S, Dr.Athika Jan, Dr.Rekha
Prabakar and Dr.Preetha R. .I thank my younger colleagues Dr. Divya Rani, Dr.
Arhanth Kumar, Dr. Atul Subramanian, Dr.Arun Chandran & Dr.Sapna.D,
Dr.Aloknath, Dr.Asha Gowda, Dr.Bhavana, Dr.Nagaraj, Dr.Megha for their timely
help.
I also owe my heartfelt gratitude to my teachers of under graduation who
initiated and instilled in me the knowledge of this holy science.
I convey my heartfelt thanks to Govindraj Shetty & Sons, Devraj urs Road
Mysore, G.Abdur Ravoof Pansari, Unani and Ayurvedic Druggists ,Lashkar Mohalla,
Mysore Jogappa Shenoy Pansari, Near Venkataramana temple, Rathabeedi Udupi
who have helped me in procuring the drugs for my dissertation.
This acknowledgement would not be complete without paying obeisance to
my parents Mr. Rama Mohan .G and Smt. Punyavathi. G.R. Their constant
encouragement and guidance propelled me to achieve my goal.
I convey my special thanks enveloped with affection to my beloved husband
Dr.K.L Virupaksha Gupta and beloved elder brother for their constant
encouragement and valuable guidance.
I wish to convey my thanks to U.G. and PG Librarian Smt Varalakshmi, Sri
Mahesh and Sri Somasundar ,for providing library facilities. I thank Madhu
Computers, Mysore, for bringing this work in a documented form.
Last but not the least, I express my thanks to everyone who helped me directly
or indirectly in my studies with apologies for my inability to identify and thank them
individually.
Date:
Place Dr. Pallavi.G

ix
LIST OF ABBREVATIONS
ACTH :-Adreno Cortico Trophic Hormone
AH:- Astanga Hridaya
AS :-Astanga Sangraha
AT :-After Treatment
B.P:- Bhavaprakasha
BR :- Bhaishajya Ratnavali
BST :- Baumann Skin Typing
BT :-Before Treatment
CD: Clinically deteriorated
CI :-Clinical Improvement
CS : Clinically Stable
CS : Charaka Samhita
CSC :-Constitutive Skin Colour
FU:-Follow up
FSC :-Facultative Skin Colour
HA:-Hyaluronic acid
HRT :–Hormone Replacement Therapy
HPA: –Hypothalamic Pituitary Adrenal
HS :–Haritha Samhita
KS:-Kashyapa Samhita
M.N :-Madhava Nidana
MASI :-Melasma Area Severity Index Score
MSH :-Melanocyt e Stimulating Hormone
NMF:- Natural Moisturising Factor
OCP :-Oral Contraceptive Pills
PIH:-Post Inflammatory Hyperpigmentation
SC:- Stratum Corneum
Sha.sam:- Sharangadhara Samhita
SS:-Sushruta Samhita
SPF:- Sun Protective Factor
SLE :-Systemic Lupous Eryhmatosus
UV, A/B:- Ultra Violet, Alpha/Beta
YR :- Yoga Ratnakara

x
KEY FOR TRANSLITERATION
अ a क ka ट ṭa ऩ pa
आ ā ख kha ठ ṭha प pha
इ i ग ga ड ḍa फ ba
ई ī घ gha ढ ḍha ब bha
उ u ङ ṅa ण ṇa भ ma
ऊ ū च ca त ta म ya
ऋ ṛ छ cha थ tha य ra
ऌ ḷ ज ja द da र la
ए e झ jha ध dha व va
ऐ ai ञ ् ñ न na श śa
ओ o ष ṣa
औ au स sa
ह ha

xi
CONTENTS
Particulars Page No.
Introduction 1
Objectives of the Study 3
Review of literature- Chapter 1
Historical review on Varṇa
4-7
Varṇa , Prabhā ,Chāyā ,Pratichāyā 8-10
Types of Varṇa 10-13
Varṇa adhiṣṭhāna 13-14
Varṇa māna, Varṇa utpatti 15
Factors governing formation of Varṇa
Factors contributing in the process of Varṇotpatti during foetal life
Factors contributing in the process of Varṇotpatti after birth
16
16-21
22-26
Anatomy & Physiology of skin 27-30
Complexion, Skin type classification, 31-37
Melanin 38-46
Chapter -2-Varṇya 47-56
Complexion Promoters 57-61
Disease review-Vyaṅga 62-69
Melasma 70-81
Drug Review -Varṇya Gaṇa 82-86
Materials and methods 87-97
Observations 98-112
Results 113-125
Discussion 126-164
Conclusion 165-166
Recommendations For Further Study 167
Summary 168-169
Bibliographic references 170-180
Annexure I, II, III, IV I-XV

xii
LIST OF TABLES
Table No Particulars Page No.
1 Types Of Chāyā 10
2 Types Of Prākṛta Varṇa 11
3 Subtypes Of Prākṛta Varṇa 12
4 Types Of Vaikṛta Varṇa 12
5 Similies For Vaikṛta Varṇa 13
6 Difference Between Bāhya Twcha &Anta Tvacā 13
7 Different Layers Of Skin And Their Respective Diseases. 14
8 Varṇa Utpatti Kāla 16
9 Mahābhūta Composition Of Different Varṇas 17
10 Different Varṇas With Similies 17
11 Relation Of Śārīrika Prakṛti & Varṇa 18
12 Relation Of Mānasika Prakṛti. &Varṇa 18
13 Relation Of Guṇa &Varṇa 18
14 Relation Of Śukra Varṇa & Garbha Varṇa 20
15 Relation Of Deśa & Varṇa 21
16 Relation Of Rasa & Varṇa 22
17 Relation Of Vihāra & Varṇa 23
18 Relation Of Dhātu Sāra Lakṣaṇas & Varṇa 25
19 Fitzpatrick‟s Skin Phototyping System 32
20 Baumann Skin Typing System 33
21 Various Events From Origin To Migration Of Melanocytes 38
22 The Difference Between Immediate And Delayed Tanning 45
23 Various Dinacharyā And Their Effect On Varṇa 48

xiii
Table No Particulars Page No.
24 Āhāra Vargās Which Are Varṇya 49
25 Different Types Of Lepa 53
26 Difference Between Types Of Lepa 53
27 Dietary Needs Of Different Skin Types 57
28 Classification Of Topical Formulations 59
29 Sāmānya Nidāna Of Vyaṅga 64
30 Rūpa Of Vyaṅga 64
31 Samprāpti Ghaṭakas Of Vyaṅga 67
32 Treatment Modalities Of Vyaṅga 69
33 Śamana Yoga In Vyaṅga 69
34 The Histological Types Of Melasma 76
35 Topical Applications And Their Probable Mode Of Action 80
36 Drug Review 82
37 The Grades Of MASI Score 96
38 Age Group Incidence 98
39 Sex Wise Distribution 98
40 Religion Wise Distribution 99
41 Educational Status Wise Distribution 99
42 Marital Status Wise Distribution 99
43 Socio Economic Status Wise Distribution 100
44 Nature Of Work Wise Distribution 100
45 Diet Wise Distribution 101
46 Koṣṭha Wise Distribution 101
47 Agni Wise Distribution 101
xiv
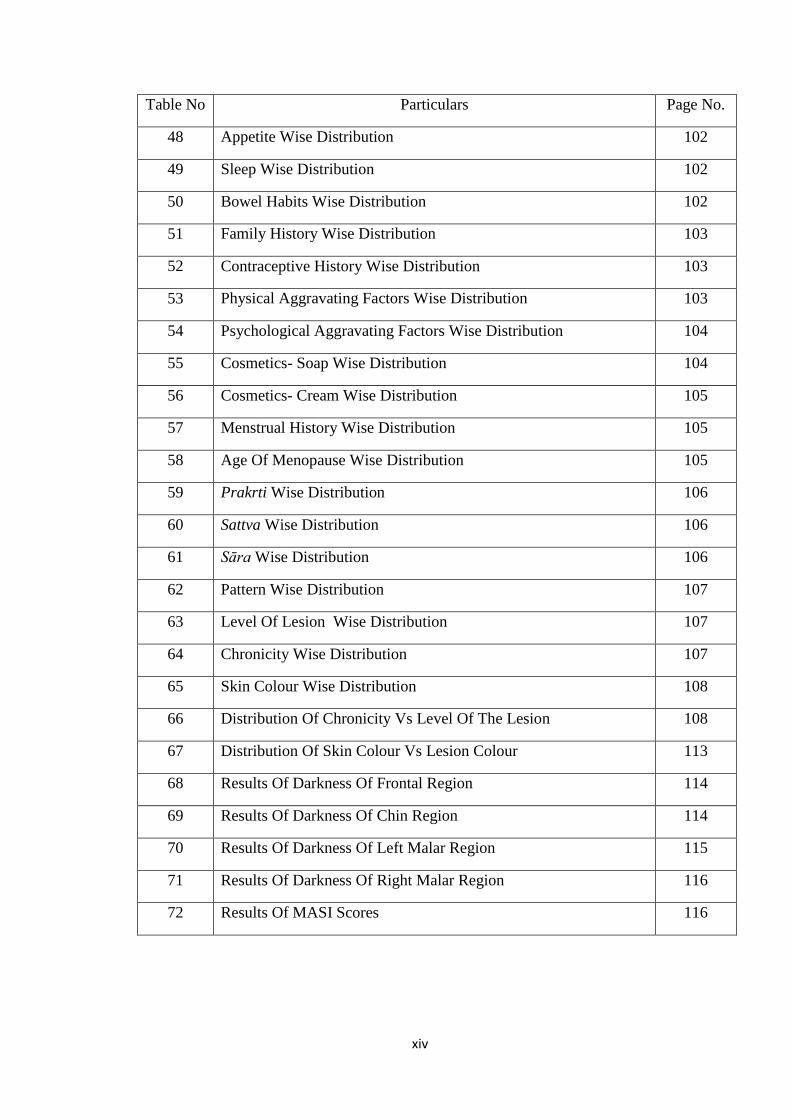
Table No Particulars Page No.
48 Appetite Wise Distribution 102
49 Sleep Wise Distribution 102
50 Bowel Habits Wise Distribution 102
51 Family History Wise Distribution 103
52 Contraceptive History Wise Distribution 103
53 Physical Aggravating Factors Wise Distribution 103
54 Psychological Aggravating Factors Wise Distribution 104
55 Cosmetics- Soap Wise Distribution 104
56 Cosmetics- Cream Wise Distribution 105
57 Menstrual History Wise Distribution 105
58 Age Of Menopause Wise Distribution 105
59 Prakrti Wise Distribution 106
60 Sattva Wise Distribution 106
61 Sāra Wise Distribution 106
62 Pattern Wise Distribution 107
63 Level Of Lesion Wise Distribution 107
64 Chronicity Wise Distribution 107
65 Skin Colour Wise Distribution 108
66 Distribution Of Chronicity Vs Level Of The Lesion 108
67 Distribution Of Skin Colour Vs Lesion Colour 113
68 Results Of Darkness Of Frontal Region 114
69 Results Of Darkness Of Chin Region 114
70 Results Of Darkness Of Left Malar Region 115
71 Results Of Darkness Of Right Malar Region 116
72 Results Of MASI Scores 116

xv
Table No Particulars Page No.
73 Results Of Dryness And Oilyness 117
74 Results Of Itching And Burning Sensation 118
75 Results Of Size And Number Of Lesions 118
76 Results Of Skin Lustre 119
77 The Assessment Of Clinical Improvement In All The Parameters. 119
78 Results Of Overall Assessment 120
LIST OF ILLUSTRATIONS
Ilustn.No Particulars P No.
1 Incidence Of Age And Sex 109
2 Incidence Of Sex 109
3 Incidence Of Marital Status 109
4 Incidence Of Family History 109
5 Incidence Of Contraceptive History 110
6 Incidence Of Physical Aggravating Factors 110
7 Incidence Of Psychological Aggravating Factors 110
8 Incidence Of Use Of Soaps 110
9 Incidence Of Menstual History 110
10 Incidence Of Age Of Menopause 110
11 Incidence Of Prakriti 111
12 Incidence Of Pattern Of Lesion 111
13 Incidence Of Level Of Lesion 111
14 Incidence Of Chronicity 111
15 The Distribution Of Skin Colour 111
16 The Distribution Of Chronicity Vs Level Of Lesion. 112
17 Distribution Of Skin Colour Vs Lesion Colour 121
18 Darkness Of Frontal Region And Chin 121
xvi
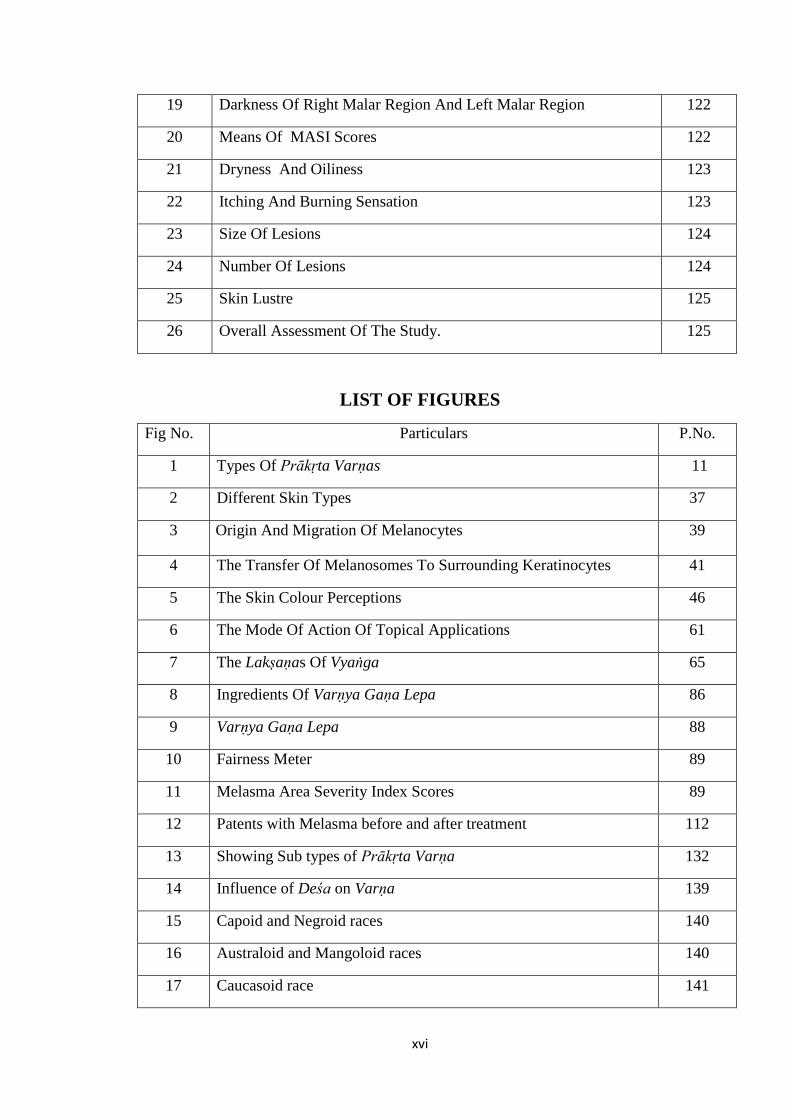
19 Darkness Of Right Malar Region And Left Malar Region 122
20 Means Of MASI Scores 122
21 Dryness And Oiliness 123
22 Itching And Burning Sensation 123
23 Size Of Lesions 124
24 Number Of Lesions 124
25 Skin Lustre 125
26 Overall Assessment Of The Study. 125
LIST OF FIGURES
Fig No. Particulars P.No.
1 Types Of Prākṛta Varṇas 11
2 Different Skin Types 37
3 Origin And Migration Of Melanocytes 39
4 The Transfer Of Melanosomes To Surrounding Keratinocytes 41
5 The Skin Colour Perceptions 46
6 The Mode Of Action Of Topical Applications 61
7 The Lakṣaṇas Of Vyaṅga 65
8 Ingredients Of Varṇya Gaṇa Lepa 86
9 Varṇya Gaṇa Lepa 88
10 Fairness Meter 89
11 Melasma Area Severity Index Scores 89
12 Patents with Melasma before and after treatment 112
13 Showing Sub types of Prākṛta Varṇa 132
14 Influence of Deśa on Varṇa 139
15 Capoid and Negroid races 140
16 Australoid and Mangoloid races 140
17 Caucasoid race 141

xvii
18 African Americans 141
LIST OF FLOW CHARTS
Sl. No. Particular P.No.
1 Showing Samprāpti of Vyaṅga 66

xviii
ABSTRACT
The concept of beauty is as old as mankind and civilization. A fair complexion
is a desirable and decisive component of beauty. The concept of Varṇa dealt in
Āyurveda is an innate entity of beauty .Varṇa represents all the parameters for healthy
and radiant skin. In this aesthetic era, people are getting more and more beauty
conscious, so to cope with their cosmetic demands, it becomes invariably essential to
resort to Varṇya upakramas. Vyaṅga is a Varṇa vikāra (hyper pigmentation) which
has been selected for this study. It accounts for a great deal of anxiety and stress.
Treatment modalities for hyper pigmentation are usually unsatisfactory due to its
frequent exacerbation and remission. Hence the need for its evaluation through
Varṇya upakramas. With this background the present study was undertaken so as to
analyze the concept of Varṇya and its application in the patients of Vyaṅga.
The 2 important objectives with which this study was designed were -To
systematically compile and review the literature on the concept of Varṇa, Varṇya
and Vyaṅga & To clinically evaluate the efficacy of Charakokta Varṇya Gaṇa Lepa
in Vyaṅga.
The study was a randomized single blind clinical trial with pre test, post test,
follows up assessment. 40 patients of Vyaṅga belonging to 16-60yrs of age group
were selected from OPD and IPD of GAMC & Hospital Mysore. They were assigned
into a single group. Varṇya Gaṇa Lepa was given for external application along with
luke warm water to all patients for 15 days twice daily in a sufficient quantity. The
different parameters of the study (Skin colour, Lesion colour, Skin texture-
dryness/oiliness, Skin lustre, Number and Size of the lesions, Darkness, Area and
Homogeneity of lesion, Itching, Burning sensation, MASI Score) were recorded
before treatment, after treatment, and after follow up.

xix
The data was analyzed by means of Descriptive statistics, Chi-square test,
Paired sample„t‟ test, Repeated measure ANOVA and Contingency Co efficient for
statistical significance.
There was statistically highly significant improvement in the MASI Scores but
in overall assessment 64.5% patients had mild improvement. Clinical improvement
was more evident in Darkness parameter when compared to other parameters.
Varṇa incorporates the entities like colour, texture, lustre, appearance and
nourishment (plumpness) . Dermatological parameters such as Skin hydration
(Dryness-Oiliness), Skin Pigmentation (Pigmented Non pigmented) , Skin Sensitivity(
Sensitive –resistant), Skin wrinkling (Wrinkled-tight) also come under the purview of
Varṇa. It is evident from the study that application of Varṇya Gaṇa Lepa in Vyaṅga
could bring a mild improvement in colour and texture parameters of Varṇa along with
other symptoms like itching and burning sensation. Greater extent of improvement
could have been expected in all the parameters if the duration of intervention is
extended.
Key words-
Varṇa
Varṇya
Varṇya gana lepa
Vyaṅga
Complexion
Melasma

20
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
INTRODUCTION
The Concept of beauty is as old as mankind and civilization and it has been admired
since time immemorial. Beauty is that quality or combination of qualities which afford
keen pleasure to the senses or which charms the intellectual or moral faculties. The word
Sundara (Saundarya) is derived from the saṁskṛta word „ārdrīkaroti cittam iti’ which
means to please the mind. Skin colour is one of the most conspicuous ways in which
humans vary and has been widely used to define human races. Colour and complexion of
the individual are the innate entities of this beauty which is depicted by the term Varṇa in
Āyurveda. In a broader perspective it includes all the parameters of healthy and radiant
skin. It reflects the equilibrium of dhātus and is one among the signs of good health. Any
unhealthy state of the psyche or physique is reflected by the skin as beauty manifests
through the complexion of the skin. Importance of beauty and personality is at its bloom in
this era of aesthetics as it determines the social perceptions, value judgments and
interpersonal relationships.
Melasma is one such personality detrimenting hyper pigmentation disorder which is
selected for this study. It is a chronic, acquired cutaneous, relapsing hypermelanosis
characterized by hyperpigmented patches on sun-exposed areas of the face, neck, and
forearms. Exposure to UV radiation is believed to be the leading factor in its development.
Āyurveda refers this condition as Vyaṅga where in vāta pitta doṣa as well as mānasika
nidānas such as krodha, śoka, āyasa are the main culprits. Melasma should not be
dismissed as simply a cosmetic entity because it often evokes emotional distress.

21
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Additionally, stigma may be associated, particularly in Asian cultures .It is known for
causing significant psychosocial stress. The treatment modalities and other management
strategies for hyper pigmentation are usually unsatisfactory as it shows exacerbation and
remission from time to time because of various influencing factors such as frequent
exposure to sun rays, pollution, stress and hormonal variations.
The task of enhancement of Varṇa (restoring the natural hue and tone of the skin) is
termed as Varṇya. Cosmetic science has caught the attention of majority of the population
since centuries. The whole of cosmetic science deals with the idea of promoting
complexion and appearance and thus is based on the principle of Varṇya karma. Hence it is
high time to resort to Varṇya upakramas of Āyurveda in order to discover a better
alternative.It mainly deals with the correction of innate entities responsible for maintanace
of Varṇa along with various mehods of bahi parimārjana cikitsā. Therefore it is the need
of the hour to fulfill the cosmetic demand of people.
In accordance with the preference attitude of the society, the present study was
aimed at building a concept on Varṇa and Varṇya and evaluating the efficacy of Varṇya
Gaṇa lepa in Vyaṅga.

22
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
OBJECTIVES OF THE STUDY
The study includes Conceptual and Clinical part.
The Conceptual part deals with the following objective
To systematically compile and review the literature on the concept of Varṇa,
Varṇya and Vyaṅga
The Clinical part deals with the following objective
To clinically evaluate the efficacy of Carakokta Varṇya Gaṇa Lepa in Vyaṅga.
23
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
HISTORICAL REVIEW ON VARNA
History forms the basis to remember and cherish the milestones achieved by
mankind from the time of evolution till the present era. Many evidences from the history
reveals the special attention paid towards the Concept of Varṇa. The Vedas Purāṇas
Upaniṣads, Saṁhitās, Epics form the main historical sources. The word Varṇa appears in
these literatures at various instances which can be understood as follows:-
Vedic Kāla - Atharvaveda
The Vedās are said to be the oldest treasure of knowledge. In Atharvaveda, many
mantrās highlight the significance of improving the Varṇa of the body. Use of
Maṇībandhana is indicated to purify the deranged colour and complexion, i.e. certain herbs
were used for restoring the beauty which is vitiated by Viṣa.
Rāmāyaṇa & Mahābhārata
An important reference states that, when Lakṣmaṇa was in unconscious stage,
Hanumān was advised to bring some drugs from Gandhamardana, where he found certain
Savarṇakarā drugs (drugs which brings the vitiated colour to normal one and which gives
normal features to abnormal one) among the drugs on Sanjīvanī Parvata
Saṁhitā kāla:- Caraka Saṁhitā:
Caraka Saṁhitā is the first and foremost Āyurvedic source for the detailed description of
this subject. Varṇa has been described from various view points, such as, as a sign of
health, as a parameter to evaluate the status of body elements and also as a premonitory

24
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
symptom as described in Indriyasthāna.A group of drugs known as„Varṇya Daśemāni‟ is
also described, which are known as complexion promoters.
The description of Dinacaryā, like Abhyaṅga , Snāna Anulepana, etc are stated to have an
effect on Varṇa. The concept of Rasāyana therapy is highly suggestive of its importance.
In „Astauninditīya adhyāya the description of Atigaura and Atikṛṣṇa explains its
significance
Suśruta Saṁhitā:
Suśruta Saṁhitā gives prime importance to Agni Mahābhūta in the manifestation of
Varṇa. Instead of a separate group of Varṇya dravyas , Elādi Gaṇa dravyas have been
described and are said to possess Varṇaprasādana karma .Under the heading of
„Vaikŗtāpaha‟, the ‟22 Upkramas‟ are explained, among them „Kṛṣṇa karma‟ and
„Pāndukarma‟ etc. directly suggests the importance of Varņaprasādana .
Saṁgraha Kāla:
In Aştāṅga Saṁgraha, Varṇa Māna has been described, which includes Āhāra,
Vihāra, Deśa, Kula, Jāti, Bhutādhikya. In both texts Aştāṅga Hṛdaya and Aştāṅga
saṁgraha, two groups of herbs labeled as „Rodhrādi Gaņa‟ and „Elādi Gaņa‟ are attributed
to „Varņya‟
Madhya Kāla: Cakradatta, Mādhava Nidāna, Vaṅgasena:
In all these texts certain Mukhakāntikara and Mukhasaundaryakara lepas, various
taila and ghṛta preparations are described for better colour and complexion .The Varṇa
vikāras like Vyaṅga ,Nīlikā, Tilakālaka, Maṣaka, etc. have been described with their
management in the chapter Kşudra Rogādhikāra .
25
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Śārṅgadhara Saṁhitā:
Śārṅgadhara Saṁhitā explains about certain Varņya Lepas, which enhances the
colour and complexion. In Vraņopkramas, seventh and last Upkrama is named as
„Savarņakaraņa‟, which itself suggests the importance.
Vātsyāyana Kāmasūtra:
In Kāmasūtra, a chapter named Subhagaṁ karaṇam is described in which many
herbs are indicated for enhancing the Beauty. In this chapter anulepana, anjana,
tailābhyaṅga, saundaryavardhaka lepa etc. are stated.1.
Ādhunika Kāla:
Skin colour is a subject that throughout history has been shrouded in mystery,
misconception, mystique and misunderstanding since antiquity, people have sought
answers to questions such as where skin colour comes from? What was the colour of the
first humans and why humans developed different skin colours?
Myths about Skin Colour
Myth and religion provided the earliest explanations of skin colour. According to an
early African myth, early humans quarreled over the first ox slaughtered for food. The
colour of their descendants thus was determined by the distribution of the meat. Those who
ate the liver had black children, those who took the lungs and blood had red children, and
those who ate the intestines had white children.
Ultra violet Radiation and Skin Colour-Hypothesis
26
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
There is a close association between latitude and skin colour. The amount of UV
received at the earth's surface is inversely related to latitude - the higher the latitude, the
lower the UV. From a geographical standpoint the darker the skin pigmentation the greater
is the ambient UV.
Vitamin D hypothesis
According to this hypothesis human beings could only have survived the low UV
availability of northern climates by evolving a de-pigmented skin to enable the scant
available UV to traverse the stratum corneum (and beneath) and induce the formation of
Vitamin D. Hence arose fair-skinned people of Scandinavia and northern Europe.
Genetic hypothesis and Evolutionary time
Emergence of skin colour was based on evolution. Livingstone (1969) constructed a
computer model on the assumption that four genes were involved in the determination of
skin colour. According to it certain human physical characteristics such as skin colour have
been accomplished in a matter of 30 generations (750 years).2
Melanosome theory
Modern research has finally led to an understanding of the biological process that
produces skin colour. According to Fitzpatrick and Quevedo (2003), pigmentation of the
skin is related to four biologic processes: 3
Formation of melanosomes in melanocytes
Melanization of melanosomes in melanocytes
Secretion of melanosomes into keratinocytes
Transportation of melanosomes by keratinocytes to the epidermal surface.

27
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
VARNA
Introduction
The concept of beauty has an age old origin & one of the ways of expression of
beauty is through the skin. Complexion is the manifest form of beauty. Āyurveda refers it
as Varṇa. It is incorporated among the signs of health as it reflects the equilibrium of all the
dhātus & acts as a barometer of individual‟s health. Varṇa has various physiological and
pathological implications, hence the need for its extensive study and proper understanding.
Derivation
Varṇa is an Akārānta napuṁsakaliṅga śabda
uÉhÉï+ AcÉç -The word Varṇa is derived from the root Varṇa with suffix Ach. 4
Definition
It can be understood under 2 headings. They are Sāmanya artha and Viśeṣa artha
MÑüƒ¡ÓûqÉå | oÉëɼhÉÉÌSeÉÉiÉÉæ zÉÑYsÉÉÌSÃmÉuÉhÉåï AMüÉUɱ¤ÉUå cÉ | 5
Sāmanya Artha- The word Varṇa refers to Kuṁkuma, Brahmaṇādi Jāti, Śuklādi Rūpa and
Akārādyakṣara. The literal meaning of the word Varṇa is the outward appearance, exterior
form, figure, shape, colour, colour of the face, good colour or complexion, lustre beauty
etc.6
Viśeṣa Artha
uÉhÉïrÉÌiÉ mÉëÌiÉqÉÉÇ zÉÑYsÉÉÌSuÉhÉï MüUÉãiÉÏirÉjÉïÈ |
To colour any substance. 7

28
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
uÉhÉï xiÉÑiÉÉæ ÌuÉxiÉÉUå zÉÑYsÉÉÌSuÉhÉïMüUhÉå E±ÉåaÉå SÏmÉlÉå cÉ |8
The word Śuklādi Varṇa karaṇe refers to whiten or enlighten any substance.
uÉhÉï zÉoSålÉ uÉhÉï xÉWûcÉËUiÉɶɤÉÑaÉëÉï½É UÉæ¤rÉÉSrÉÉåÅÌmÉ aÉ×½liÉå | 9
Varṇa refers to all those qualities which can be recognized by cakṣurindriya.
uÉhÉï zÉUÏUMüÉÎliÉÈ |10
Varṇa refers to the lustre of the body.
uÉhÉÉåï aÉÉæUÉÌS | 11
Varṇa refers to gaura śyāmādi Varṇa.
uÉhÉïpÉåSålÉ asÉÉÌlÉWûwÉïUÉæ¤rÉxlÉåWû urÉÉZrÉÉiÉÉÈ | 12
Varṇa refers to glāni, harṣa, raukṣya, sneha reflecting the health of the skin.
Samānārtha śabda
Rūpa, Śuklādi rūpa, Vilepana, Saṁsthāna, Kānti Ākṛti, Pramāṇa, Aṅgarāga, Prabhā. 13
Saṁbandhita śabda
Prabhā
pÉÉxiÉÑ uÉhÉï mÉëMüÉÍzÉlÉÏ |14
Prabhā is the highlighter of the complexion and it is recognizable from a distance .All
sorts of Prabhā are the components of tejo mahābhūta . It is said to be of 7 types. They
are Rakta, Pīta, Śyāva, Harita, Pāndura, Asita.
Chāyā
uÉhÉÉïlÉÉqÉÉ¢üqÉÌiÉ NûÉrÉÉ |

29
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
AÉxɳÉÉ sɤrÉiÉå NûÉrÉÉ |
NûÉrÉÉ uÉhÉïmÉëpÉÉ´ÉrÉÉ |15
Chāyā is the one which circumscribes Varṇa and which is recognizable from near (Short
distance). Chāyā depends on Varṇa and Prabhā 5 types of Chāyā have been explained.
They are Vāyavī, Āgneyī, Nābhasī, Āṁbhasī & Pārthivī.
Table 1:- Types of Chāyā
Chāyā Characteristics
Nābhasī Nirmala, nīla, sasneha, saprabhā.
Vāyavī, Rūkṣa, śyāva, aruṇa, hataprabhā.
Āgneyī Viśuddharakta, dīptābha, darśanapriya
Āṁbhasī Śuddha vaiḍūrya vimala, susnigdha
Pārthivī Sthira, snigdhāyata, ślakṣṇa, śyāma, śveta
Pratichāyā
mÉëqÉÉhÉ xÉÇxjÉÉlÉ xÉSØzÉiÉrÉÉ eÉsÉÉÌSwÉÑ rÉÉ NûÉrÉÉ xÉÉ mÉëÌiÉcNûÉrÉÉ | 16
The reflection of the body similar to its Pramāna & Saṁsthāna is termed as Pratichāyā
Types of Varna-
It is of 2 types
Prākṛta Varṇa
Vaikṛta Varṇa
Prākṛta Varṇa- It is defined as Deha samāna Varṇa or Sāhajika Varṇa.17
Caraka Saṁhitā
clearly states 4 different types of Prākṛta Varṇa of the body, 18
where as Aṣṭāṅga
saṁgraha explains 5 Prākṛta deha Varṇas .19
These are as follows:-

30
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Table 2 :-Types of Prākṛta Varṇa
Varṇa
C.S
Meaning as per
Monier Williams
Varṇa Meaning as per
Monier Williams S.S A.S H.S
Kṛṣṇa Black, dark blue Gaura Gaura Gaura White/Yellowish
Śyāma Brown - Śyāma Śyāma Brown
Śyāma
avadāta
Blackish white/
dazzling black
Kṛṣṇa Kṛṣṇa Kṛṣṇa Black, dark, dark blue
Avadāta Dazzling white/
white
Gaura
Śyāma
Blackish
white/dazzling black
Kṛṣṇa
Śyāma
Blackish brown
Piṅgala Reddish brown, golden
Hārīta Saṁhitā explains about an additional one by name Piṅgala Varṇa which is
constituted by Pitta and Rakta. 20
Avadāta Varṇa Śyāma Avadāta Varṇa Śyāma Varṇa Kṛṣṇa Varṇa
Figure No1. Different types of Prākṛta Varṇas

31
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
The Sub types of the Prākṛta Varṇa have been explained in Indukara commentary on
Aṣṭāṅga Saṁgraha Śārīra sthāna. They are as follows21
Table 3:- Subtypes of Prākṛta Varṇa
Varṇa Gaura Śyāma Kṛṣṇa Gaura Śyāma Kṛṣṇa Śyāma
1 Padma Gaura Kapittha
Śyāma
Kajjala
Kṛṣṇa
Priyaṅgu Śyāma Atasī Kṛṣṇa
Śyāma
2 Candra
Gaura
Dūrvāṅkura
Śyāma
Kokoila
Kṛṣṇa
Jala Śyāma Tamāla Kṛṣṇa
Śyāma
3 Śara Gaura Nabha
Śyāma
Saṭpada
Kṛṣṇa
Ghṛta
Śyāma
Vaikṛta Varṇa
5 types of Vaikṛta Varṇa which manifests in the body have been described in Caraka
Saṁhitā22
and Aṣṭāṅga Saṁgraha with a slight difference in terminology.
Table 4 :-Types of Vaikṛta Varṇa
Varṇa-C.S A.S Meaning as per Monier Williams
Nīla Nīla Dye dark/Blackish
Śyāva Śyāva Dark brown/ brown
Tāmra Tāmra Coppery red
Harita Haridra Harita -Green /pale yellow Haridra - yellow
Śukla Śukla White/bright/whitish
Some similies have been quoted for each type of Varṇa in Indukara commentary of
Aṣṭāṅga Saṁgraha. They are:- 23

32
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Table 5 :-Similies for Vaikṛta Varṇa
Varṇa Similie
Nīla Nīla
śyāva Aruṇa lohita sama
Tāmra Agni prakhya
Harita Haritāla sama
Śukla Śankhakundādi prakhya
Varṇa Adhiṣṭhāna
iuÉcÉÉ- iuÉcÉç xÉÇuÉUhÉå |
The word Tvacā is derived from Twach saṁvaraṇe dhātu 24
which means the covering of
body and it is the main basis for Sparśanendriya, Swedavaha srotas Roma & Romakūpa 25
Tvacā pramana is said to be Yava Pramāna 26
and Vāyu is the adhidevatā for tvacā.27
It is divided into 2- They are
Bāhya Tvacā &
Ābhyantara /Anta Tvacā28
Table 6 :-Difference between Bāhya Tvacā & Anta Tvacā
Bāhya Twcā- Anta Tvacā-
It is Tanu It is sthūla
Ādhāra for kṛṣṇa gaurādi Varṇa It does Śarīra Rakṣaṇa
33
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
It is the seat for diseases such as ploṣa and
Pidaka
It maintains the texture and compactness ie
it does Snehādi Karṣaṇa
Formation of Tvacā
The process of formation of Tvacā in the developing foetus is due to Pāka of Rakta Dhātu
by its dhātvāgni in the foetus, it dries up to form Tvacā just like the deposition of cream
over the surface of boiled milk.
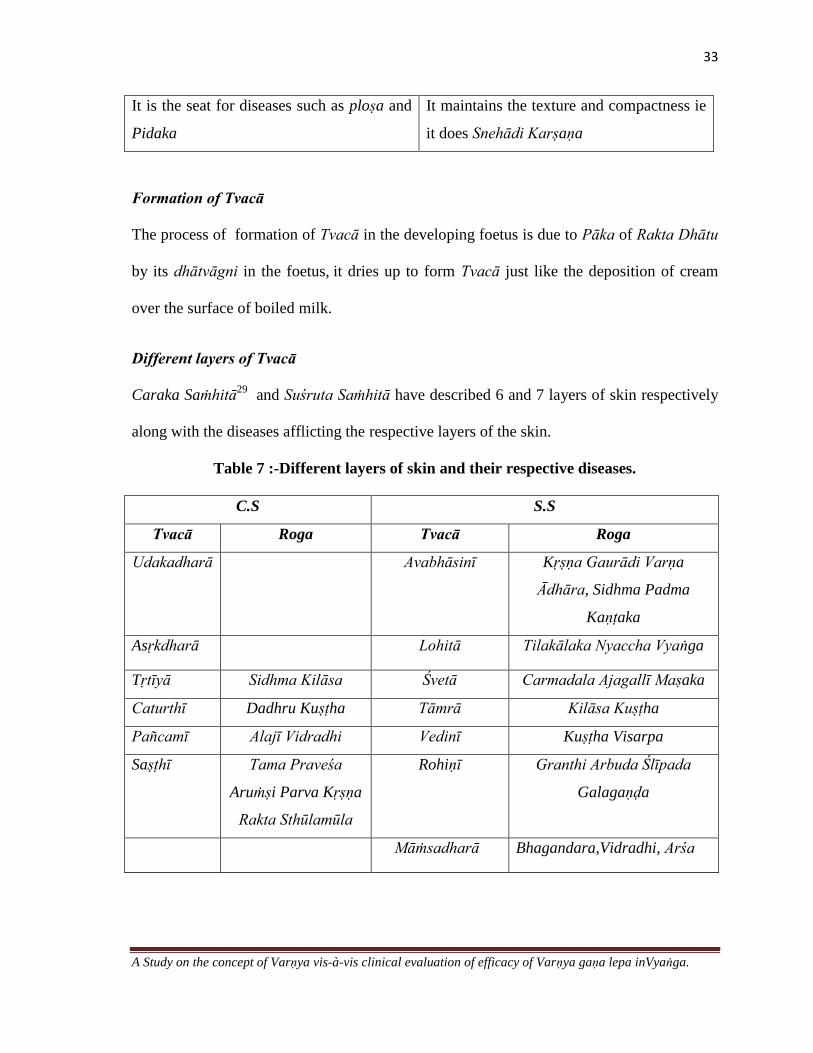
Different layers of Tvacā
Caraka Saṁhitā29
and Suśruta Saṁhitā have described 6 and 7 layers of skin respectively
along with the diseases afflicting the respective layers of the skin.
Table 7 :-Different layers of skin and their respective diseases.
C.S S.S
Tvacā Roga Tvacā Roga
Udakadharā Avabhāsinī Kṛṣṇa Gaurādi Varṇa
Ādhāra, Sidhma Padma
Kaṇṭaka
Asṛkdharā Lohitā Tilakālaka Nyaccha Vyaṅga
Tṛtīyā Sidhma Kilāsa Śvetā Carmadala Ajagallī Maṣaka
Caturthī Dadhru Kuṣṭha Tāmrā Kilāsa Kuṣṭha
Pañcamī Alajī Vidradhi Vedinī Kuṣṭha Visarpa
Saṣṭhī Tama Praveśa
Aruṁṣi Parva Kṛṣṇa
Rakta Sthūlamūla
Rohiṇī Granthi Arbuda Ślīpada
Galagaṇḍa
Māṁsadharā Bhagandara,Vidradhi, Arśa
34
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Avabhāsinī is the ādhāra for Kṛṣṇa and Gaurādi Varṇa.30
It manifests all the Varṇas and
highlights the 5 types of Chāyā.31
Varṇa Māna
The factors which determine/decides Varṇa significantly are Āhāra, Vihāra, Deśa, Kula,
Bhutādhikya. The various permutations and combinations among these factors result in
variation in Varṇa like Gaura, Avadāta, Kṛṣṇa32
Varṇa as Ārogya Lakṣaṇa
Ārogya lakṣaṇas are characterized by Annābhilāṣā, Sṛṣṭaviṇmūtravāta, Prasanna indriya,
Śarīra lāghava, Sukha swapna prabodhana etc. Varṇa lābha is also considered as an
important Ārogya lakṣaṇa
Shubha lakṣaṇa yukta Shareera
Śubha lakṣaṇa yukta śarīra is characterized by Snigdha Varṇa and Sthira Prabhā .33
Varṇa prabhava
Tejo dhātu is said to be prabhava or mūla for Varṇa utpatti.34
Varṇa Utpatti
The physiological phenomenon of Varṇa Utpatti is basically governed by many factors ie
some contribute in the formation of Varṇa in Garbhāvasthā and some others contribute in
the process after birth and later stages of life.
Varṇa Utpatti kāla
35
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
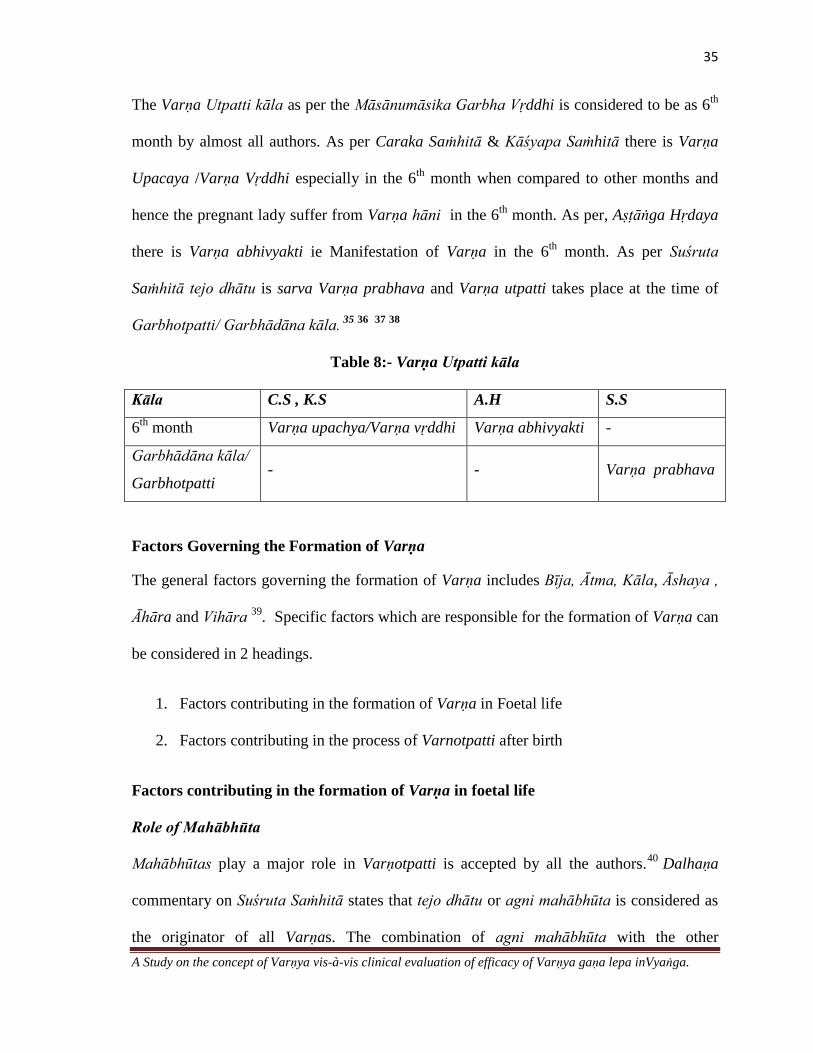
The Varṇa Utpatti kāla as per the Māsānumāsika Garbha Vṛddhi is considered to be as 6th
month by almost all authors. As per Caraka Saṁhitā & Kāśyapa Saṁhitā there is Varṇa
Upacaya /Varṇa Vṛddhi especially in the 6th
month when compared to other months and
hence the pregnant lady suffer from Varṇa hāni in the 6th
month. As per, Aṣṭāṅga Hṛdaya
there is Varṇa abhivyakti ie Manifestation of Varṇa in the 6th
month. As per Suśruta
Saṁhitā tejo dhātu is sarva Varṇa prabhava and Varṇa utpatti takes place at the time of
Garbhotpatti/ Garbhādāna kāla. 35 36 37 38
Table 8:- Varṇa Utpatti kāla
Kāla C.S , K.S A.H S.S
6th
month Varṇa upachya/Varṇa vṛddhi Varṇa abhivyakti -
Garbhādāna kāla/
Garbhotpatti - - Varṇa prabhava
Factors Governing the Formation of Varṇa
The general factors governing the formation of Varṇa includes Bīja, Ātma, Kāla, Āshaya ,
Āhāra and Vihāra 39
. Specific factors which are responsible for the formation of Varṇa can
be considered in 2 headings.
1. Factors contributing in the formation of Varṇa in Foetal life
2. Factors contributing in the process of Varnotpatti after birth
Factors contributing in the formation of Varṇa in foetal life
Role of Mahābhūta
Mahābhūtas play a major role in Varṇotpatti is accepted by all the authors.40
Dalhaṇa
commentary on Suśruta Saṁhitā states that tejo dhātu or agni mahābhūta is considered as
the originator of all Varṇas. The combination of agni mahābhūta with the other

36
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
mahābhūtas is responsible for the various Varṇas in the individuals such as gaura, kṛṣṇa
etc. 41 42
Table 9:- Mahābhūta composition of different Varṇas
C.S & A.S S.S H.S
Varṇa Mahābhūta Varṇa Mahābhūta Varṇa Doṣa
Gaura Teja+Ap+ Ākāśa Gaura Teja + Ap Gaura Pitta
Kṛṣṇa Teja +Vāyu +Pṛthvī Gaura
Śyāma
Teja+Ap+Ākāśa Kṛṣṇa Vāta+ Rakta
Śyāma Teja +Ap+ Vāyu
+Ākāśa +Pṛthvī
Kṛṣṇa
Śyāma
Teja+ Pṛthvī
+Ākāśa
Śyāma Kapha +Rakta
Kṛṣṇa Teja + Pṛthvī Piṅgala Pitta + Rakta
Gangādhara commentary on Caraka Saṁhitā narrates various combinations of
Mahābhūtas resulting in different Varṇas with similies.43
They are as follows:-
Table 10:- Different Varṇas with similies
Varṇa Mahābhūta
Haridrābha Gaura Udaka bahula panca bhūta
Palāśābha harita Ākāśa bahula panca bhūta
Pakva jaṁbūpama Kṛṣṇa Pṛthvī bahula panca bhūta
Rūkṣa /Kṛṣṇa/ Nīla Vāyu bahula panca bhūta
Kajjala Kṛṣṇa Pṛthvī + Vāyu bahula panca bhūta
Kṛṣṇa śyāma Pṛthvī + Ākāśa bahula panca bhūta

37
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Role of Prakṛti
Prakṛti is one among the important factors influencing the formation of Varṇa in the
foetus. 44
45
46
47
Table 11:- Relation of Śārīrika Prakṛti & Varṇa
Prakṛti C.S S.S A.S H.S
Vāta
Paruṣa vadana
pāṇi, sphuṭita
avayava
Sphuṭita
karacaraṇa
Dhūsara Śyāma
Asita Chavi
Pitta
Sukumāra
avadāta
Tāmra pāṇi,
pāda
Gaura aṅga, tāmra
hasta
Gaura
Peeta prabha
Kapha Sukumāra,
avadāta, prasanna
snigdha
Dūrvā, indīvara
ariṣṭaka,
śarakanda Varṇa
Padmasu Varṇa,
priyaṅgu,
śarakanda,
indīvara gorocana
Snigdha,
śyāma
Sita, śyāma
Chavi
Varṇa of an individual is also determined by the Mānasika Prakṛti. The text Rāja nighaṇṭu
describes about the colour of individuals belonging to different Mānasika Prakṛtis in
Sattvādi Varga. 48
Table 12:- Relation of Mānasika Prakṛti. &Varṇa
Mānasika Prakṛti Varṇa
Sāttvika Gaura Śyāma Tanu
Rājasika Gaura kanakādi dīpti
Tāmasika Sita itara
Role of Guṇa
By virtue of a particular guṇa a specific Varṇa is attributed to the body 49
Table 13 Relation of Guṇa &Varṇa

38
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Guṇa Varṇa
Mṛdu Sukumāra avadāta gātra
Accha Prasanna snigdha varṇa
Uṣṇa Gaura sukumāra avadāta gātra
Rūkṣa Rūkṣa apchita , vaivarṇya varṇa hāni
Paruṣa Paruṣa vadana pāṇi pāda
Viṣada Sphuṭita aṅga avayava
Snigdha Snigdha aṅga
Ślakṣṇa Ślakṣṇa aṅga
Drava Varṇa utkarṣa
Ūṣṇa, Tīkṣṇa, Sūkṣma, Laghu, Rūkṣa, Viṣada Prabhā prākāśa ,varṇa kara
Role of Garbhotpādaka bhāvas
Śadbhāvas are the most important prerequisite for the formation and development of
Garbha. Each one has its own role to play in the process of Garbha Utpatti. Amidst these
various factors Ātmaja and Sātmyaja Bhāvas are assigned for the manifestation of colour
and complexion in the foetus.
Ātmaja Bhāvas
Atma is responsible for the birth in a particular Yoni due to its past actions. Manas,
Preraṇa, Dhāraṇa Ākṛti, Swara and Varṇa in the foetus50
and are mainly due to Ātmaja
bhāvas. All the physical attributes are derived from the deeds of past life. Hence Ātma also
has a role on account of the karmas of the previous birth.51
Sātmyaja Bhāvas
Sātmyaja Bhāvas have an important role to play in the formation of Varṇa. Among various
Satmyaja Bhavas, Varṇa sampat is also one, hence the diet and regimen of pregnant
woman has a strong influence on the Varṇa of the offspring.52

39
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Role of Śukra
The colour of the Śukra has an influence on the colour of the foetus. If the Śukra resembles
Ghṛta manda then it produces a progeny of Gaura Varṇa. If Śukra resembles Taila then
garbha would be of Kṛṣṇa Varṇa and if it resembles Madhu then it would produce a
progeny of Śyāma Varṇa. 53
Table 14 :-Relation of Śukra Varṇa & Garbha Varṇa
Śukra Varṇa Garbha Varṇa
Ghṛtamaṇḍābha /Śukla Gaura
Tailābha Kṛṣṇa
Madhvābha Śyāma
Role of manasthiti
Caraka Saṁhitā and Astaṅga Hṛdaya have clearly accepted the role of manah sthiti of
mother on the Varṇa of the offspring. Rūpa and Varṇa of the offspring born will be in
accordance with the thoughts of the lady during her pregnancy. 54
Role of Āhāra and Vihāra of the mother
Āhāra and Vihāra of the mother has a very evident influence on the colour and complexion
of the offspring as per Aṣṭāṅga saṁgraha. Excessive use of Madhura āhāra, Jala krīḍā
(moving around in water is the cause) produces Gaura Varṇa of the progeny. Excessive
intake of tila and vidāhi anna leads to Kṛṣṇa Varṇa and mixed diets leads to an offspring of
Śyāma Varṇa.55
. Nutrition of the foetus is mainly derived from the āhāra rasa which is
consumed by the mother and traverses the placenta. This āhāra rasa reaches the foetus
though Upasnehana and Upaswedana and thus provides strength and complexion to the
foetus56
. Caraka Saṁhitā and Suśruta Saṁhitā have established the relationship between

40
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
the Varṇa and Āhāra in the context of Puṁsavana saṁskāra, Putreṣṭi yajña and homa
vidhi are also said to bestow Varṇa .It is stated that Varṇa of the foetus is determined by
the Varṇa of the food consumed by the mother57
.
Among the various Garbha upaghātakara bhāvās the excessive use of kaśāya rasa
by the mother has been told to produce a progeny of Śyāva Varṇa. And thus it is advised
that the woman desiring excellent progeny should particularly abstain from the
unwholesome diet and behaviour. Along with the mother, the role of Puruśa has also been
justified in Suśruta Saṁhitā by the statement,- The āhāra and cheṣṭā into which the strī
,puruṣa indulge ,the offspring born will be endowed with similar qualities.
Role of Deśa
Deśa has considerable influence on the determination of Varṇa of the individual. Aṣṭāṅga
Saṁgraha states that the colour of the individual is determined by the geographical
condition58
.
Table 15 :- Relation of Deśa & Varṇa
Deśa Varṇa
Outtar Pathika Gaura Varṇa
Dakshina, āndhra draviḍa, uśara Deśa Kṛṣṇa Varṇa
Madhya Deśa Śyāva Varṇa
Role of Kula and Jāti
As per Aṣṭāṅga Saṁgraha, Kula and Jāti also have a key role in influencing Varṇa.
Indukara commentary on Aṣṭāṅga Saṁgraha states that based on various occupations such
as Śilpī etc colour of the individuals may vary accordingly ie Gaura, Kṛṣṇa, Śyāva. 59

41
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Factors Contributing in the Process of Varṇotpatti after Birth
Many factors have been found to be influencing Varṇa after the birth of the offspring
Role of Jaṭharāgni
Caraka Saṁhitā and Aṣṭāṅga Saṁgraha describes the evident role of Jaṭharāgni as a
causative factor for Varṇa ,Bala ,Swāsthya,Utsāha, Upacaya, Prabhā ,Oja, Teja etc60
Role of Āhāra (Rasa)
Caraka Saṁhitā opines that Varṇa prasādana, suswara, jīvana, pratibhā, sukha are mainly
attributed to Āhāra. Suśruta Saṁhitā also considers Āhāra as mūla for bala Varṇa and
ojas.61
Madhura rasa is said to enhance Varṇa along with other functions like
strengthening the dhātus, indriya and enhances ojas and is suitable for bāla, vṛddha ,kṣata,
kṣīṇa62
.Specific rasās and types of food have certain effects on Varṇa,
Table 16:-Relation of Āhāra Rasa & Varṇa
Role of Āhāra Vidhi
Āhāra Rasa Varṇa
Kaśāya Śyāva 63
Lavana Vaivarṇya
Madhura Varṇa Prasādana 64
Asātmya Āhāra Varṇa hāni
Viruddha Āhāra Varṇa hāni
42
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
The dietary pattern also has equal importance as that of āhāra. Caraka Saṁhitā has
emphasised on rules for intake of food. Wholesome food consumed in the prescribed
manner is said to be a complexion promoter. Among the various rules of intake of food
Snigdham aśnīyāt is one such entity which is attributed to Varṇa prasādana guṇa along
with other benefits such as agni dīpana, vātanulomana, indriya dārḍhya, bala, vṛddhi etc.65
It has also been mentioned by Āchārya Caraka that the appropriate quantity of food
certainly helps the individual to maintain the Varṇa without disturbing the Prakṛti. Hence
āhāra vidhi also has an impact on Varṇotpatti. 66
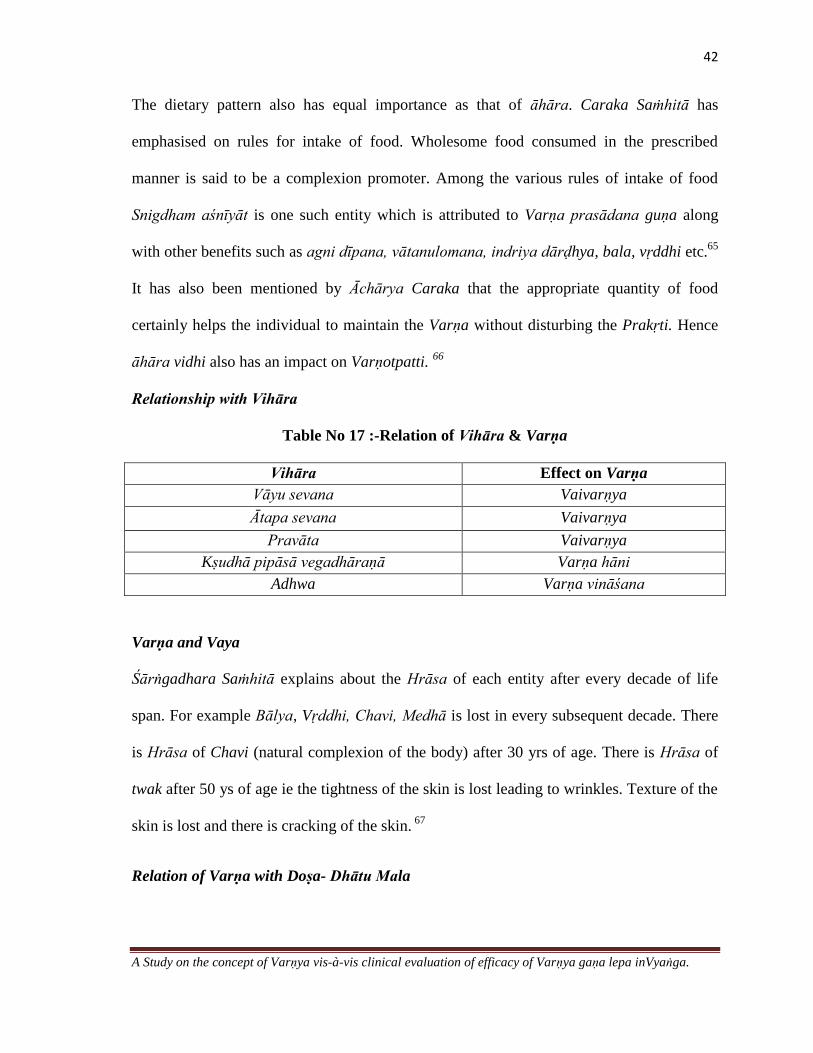
Relationship with Vihāra
Table No 17 :-Relation of Vihāra & Varṇa
Vihāra Effect on Varṇa
Vāyu sevana Vaivarṇya
Ātapa sevana Vaivarṇya
Pravāta Vaivarṇya
Kṣudhā pipāsā vegadhāraṇā Varṇa hāni
Adhwa Varṇa vināśana
Varṇa and Vaya
Śārṅgadhara Saṁhitā explains about the Hrāsa of each entity after every decade of life
span. For example Bālya, Vṛddhi, Chavi, Medhā is lost in every subsequent decade. There
is Hrāsa of Chavi (natural complexion of the body) after 30 yrs of age. There is Hrāsa of
twak after 50 ys of age ie the tightness of the skin is lost leading to wrinkles. Texture of the
skin is lost and there is cracking of the skin. 67
Relation of Varṇa with Doṣa- Dhātu Mala
43
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Contribution of doṣas in Varṇotpatti is considerably important. Caraka Saṁhitā quotes that
Tridoṣas in the state of eqillibrium brings about Upacaya, Bala and Varṇa.
Relationship with Vāta
Caraka Saṁhitā opines that a physician should admire the quality of Vāta as a promoter of
Varṇa Among the 5 types of Vāyu, Udāna Vāyu is responsible for Varṇa utpatti. 68
Udāna vāta
With complete effort, initiation (vega /utsāha) Udāna vāyu supplies anna rasa to all the
śarīra ghaṭakas or sūkṣma avayavas and nourishes it and hence endows the body with
Bala, Swara and Varṇa. It refers to the complete nourishment of the Rasa dhātu or
enrichment of rasa dhātu69
.
Relationship with Pitta
Pitta which is the main seat of agni in its normalcy and abnormalcy is responsible for
Prākṛta Varṇa (Utpatti/ Prākāśana) and Vaikṛta Varṇas.Along with other functions like
darśana, pakti, ūṣma, kṣudhā, tṛṣṇā 2 important functions are Deha mārdava- Maintains
the texture / softness of the body and Prabhā - the Complexion of the body70
. Prabhā is an
entity which is held responsible for the radiance in the skin which is expressed through
Varṇa.
Bhrājaka Pitta
The pitta seated in the tvacā is termed as Bhrājaka agni. This digests the auṣadha which is
applied on the skin in the form of Abhyaṅga, Pariṣeka, Avagāha, Ālepa and is responsible

44
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
for the luminescence or radiance. (Chāyā is Varṇa Prabhāśrayā – Chāyā depends on
Varṇa and Prabhā and hence Bhrājaka pitta determines Varṇa prākāśana.) It is
responsible for Varṇa utkarṣa ie which enhances Varṇa71
.
Relationship with kapha
In the context of Prakṛti lakṣaṇas it is clearly mentioned that individuals belonging to
Kapha Prakṛti possess Sukumāra, avadāta gātra and Prasanna snigdha varṇa which
indirectly proves that kapha has a major role in the utpatti of varṇa.
Relationship with Dhātu
Varṇa is basically an outcome of equilibrium of all the dhātus. Each dhātu has unique role
in the formation and maintenance of Varṇa.72
Table 18 :-Relation of Dhātu Sāra lakṣaṇas & Varṇa
Dhātu Sāra lakṣaṇas pertaining to Varṇa
Rasa Snigdha, ślakṣṇa, mṛdu, prasanna, saprabhā twak
Rakta Varṇa prasāda, Mukha pāni pāda, snigdha rakta varṇa
Meda Snigdha varṇa
Majja Mṛdu aṅga, snigdha varṇa
Śukra Prasanna snigdha ,varṇa
This clearly indicates that most of the dhātus are directly linked to varṇa and their
normalcy results in prākṛta varṇa utpatti

45
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Relationship with Malas
These are the entities which does the śarīra dhāraṇa. Direct relationship between ,Purīṣa,
Mūtra and Varṇa is not identified where as some relationship between sweda and tvacā
/Varṇa is identified. Sweda is held responsible in maintaining the moisture and skin
texture/ softness of the body.73
Relationship with ojas
Ojas has a definite role in imparting Prākṛta Varṇa to the body. Ojas bestows strength,
imparts firm integrity to the māmsa, exercises unbounded conrol over all the acts of
vitality, improves Swara and Varṇa, helps both external and internal sense organs, in duly
performing their natural functions.
Relationship with Bala
Prākṛta karma of bala is Varṇa prasādana, Hence Varṇa is an indicator of the status of
health and strength of an individual. 74

46
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
ANATOMY OF SKIN
Skin is a large and complex tissue that interfaces with the hostile environment. It is
called the Integument which covers the entire surface of the human body.
The Skin is composed of three primary layers. They are Epidermis, Dermis,
Hypodermis/ Subcutaneous tissue.
Epidermis
Epidermis is the most superficial layer of the skin. It is very important from a cosmetic
standpoint because it is the layer that gives the skin its texture, moisture and contributes
to the skin colour.
The Epidermis is mainly divisible into 2 main systems.
o Keratinising or Malphigian system (keratinocytes) which forms the bulk and
o Pigmentary system (melanocytes which produces the pigment)
Interlaced among the keratinocytes at various levels are the immigrant resident cells –
Melanocytes, Langerhan Cells, Merkel Cells. Other cells such as lymphocytes are
transient inhabitants of the Epidermis.
The main layers of the Epidermis which can be made out microscopically in a section are
o Stratum Germinativum /Stratum Basale / Basal Layer
o Stratum Malpighi /Prickle Cell Layer / Stratum Spinosum
o Stratum Granulosum
o Stratum Lucidum
o Stratum Corneum.
47
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
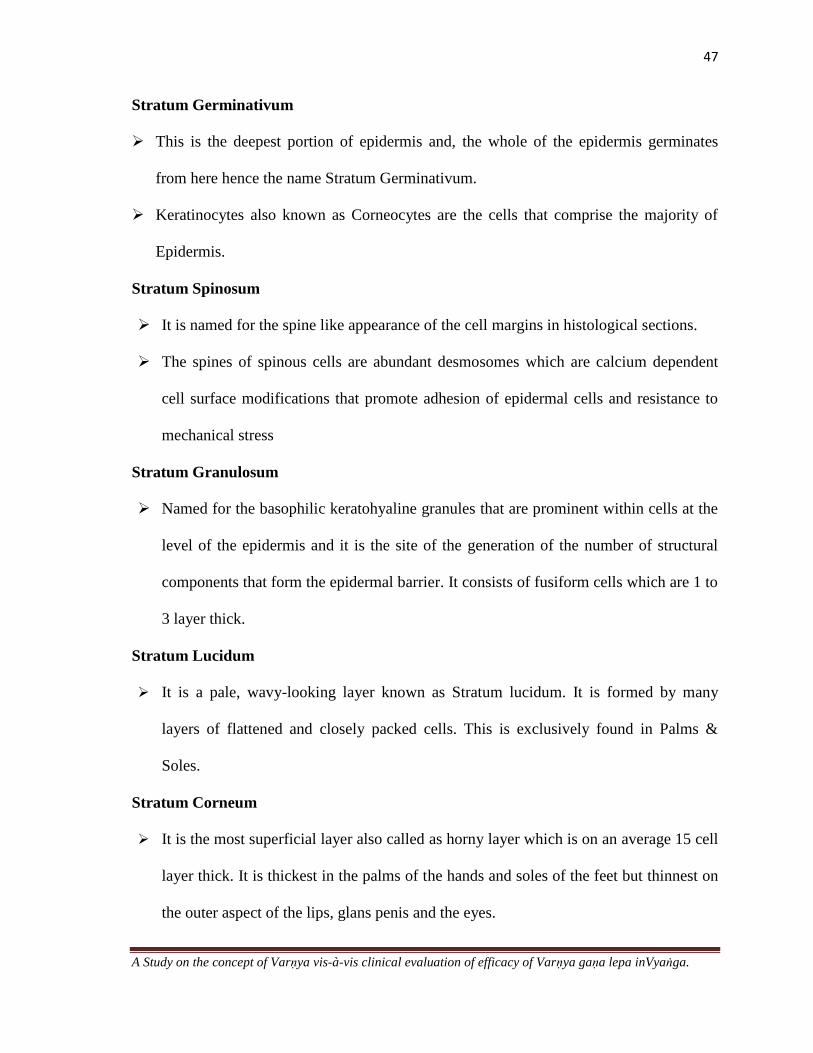
Stratum Germinativum
This is the deepest portion of epidermis and, the whole of the epidermis germinates
from here hence the name Stratum Germinativum.
Keratinocytes also known as Corneocytes are the cells that comprise the majority of
Epidermis.
Stratum Spinosum
It is named for the spine like appearance of the cell margins in histological sections.
The spines of spinous cells are abundant desmosomes which are calcium dependent
cell surface modifications that promote adhesion of epidermal cells and resistance to
mechanical stress
Stratum Granulosum
Named for the basophilic keratohyaline granules that are prominent within cells at the
level of the epidermis and it is the site of the generation of the number of structural
components that form the epidermal barrier. It consists of fusiform cells which are 1 to
3 layer thick.
Stratum Lucidum
It is a pale, wavy-looking layer known as Stratum lucidum. It is formed by many
layers of flattened and closely packed cells. This is exclusively found in Palms &
Soles.
Stratum Corneum
It is the most superficial layer also called as horny layer which is on an average 15 cell
layer thick. It is thickest in the palms of the hands and soles of the feet but thinnest on
the outer aspect of the lips, glans penis and the eyes.

48
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Dermis
The dermis is an integrated system of fibrous filamentous diffuse and cellular connective
tissue elements.
The dermis makes up the majority of the skin and provides its pliability, elasticity and
tensile strength.
The dermis is arranged into 2 major regions
o Upper pappilary dermis
o Deeper reticular dermis
Hypodermis
The hypodermis, or subcutis located beneath the dermis is composed mostly of fat and
one of the largest tissues in the human body which are mainly comprised of adipocytes
fibrous tissue and blood vessels.
It is important for dermatologists and cosmetically oriented physicians to pay close
attention to this tissue because it has many roles in cosmetic dermatology and general
appearance.
49
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
PHYSIOLOGY OF SKIN
Introduction
Skin is a dynamic complex, integrated arrangement of cells, tissues and matrix elements
that mediates a diverse array of functions. Three important functions with respect to this
study are
Barrier Functions - Epidermis and the Stratum Corneum as the Barrier
Prevents evaporative water loss from the aqueous interior cell layers and it also protects
against mechanical insults, foreign chemicals, micro organisms and Ultra violet light.
The knowledge of the skin as a barrier is important from the point of view of the
delivery of topical treatments for skin diseases to plan a logical approach to the
management.
Protection from Ultra-Violet Radiation
The skin has 2 barriers to U V radiation, a melanin barrier in the epidermis and a
protein barrier, concentrated in the stratum corneum. Both function by absorbing
radiation there by minimizing absorption by DNA and cellular constituents.
The mechanism of delayed tanning provides partial protection from U.V.
Percutaneous Absorption
The anatomically distinct layers have a different diffusion constant.
Healthy Adult human skin allows some-permeation of almost every substance .Rates of
permeation of different materials differs by 10,000 fold.
Other functions of skin include
Protection from Micro organisms, Mechanical Functions,Temperature Regulation
Immunological functions,Elimination/ Excretion,Sensory and Autonomic functions

50
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
COMPLEXION
The word "Complexion" is derived from the Late Latin complexi, which initially referred in
general terms to a combination of things, and later in physiological terms, to the balance of
humors. The four humours were four fluids that were thought to permeate the body and
influence its health. Contexually the term Complexion refers to the natural colour, texture
and appearance of the skin. These form an important basis for the classification of skin
Skin Type Classification
Human Skin (Homo Sapiens) has been classified into 3-6 racial taxons since the 18th
century before the development of Genetics and Evolutionary biology .These are based on
phenotypic characteristics, geographic origin and even psychological impressions. .
The modern races include:-
Caucasoid(Europians, Arabs, Indians, Pakistanis)
Mongoloid(Asians)
Australoid(Austalian,Aborigines)
Congoid/Negroid(Africans, Afro carribeans, African Americans)
Capoid(Kung san tribe of Africa)
Ethnic skin or skin of colour refers to the broad range of skin type and complexions
that characterize individuals with darkly pigmented skin.
Fitzpatrick Skin Typing System
The Fitzpatric Scale is a numerical classification scheme for determining the skin
colour based on a questionnaire related to an individuals genetic constitution, reaction to
sun exposure and tanning habits. The response to each question is measured on a scale of
51
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
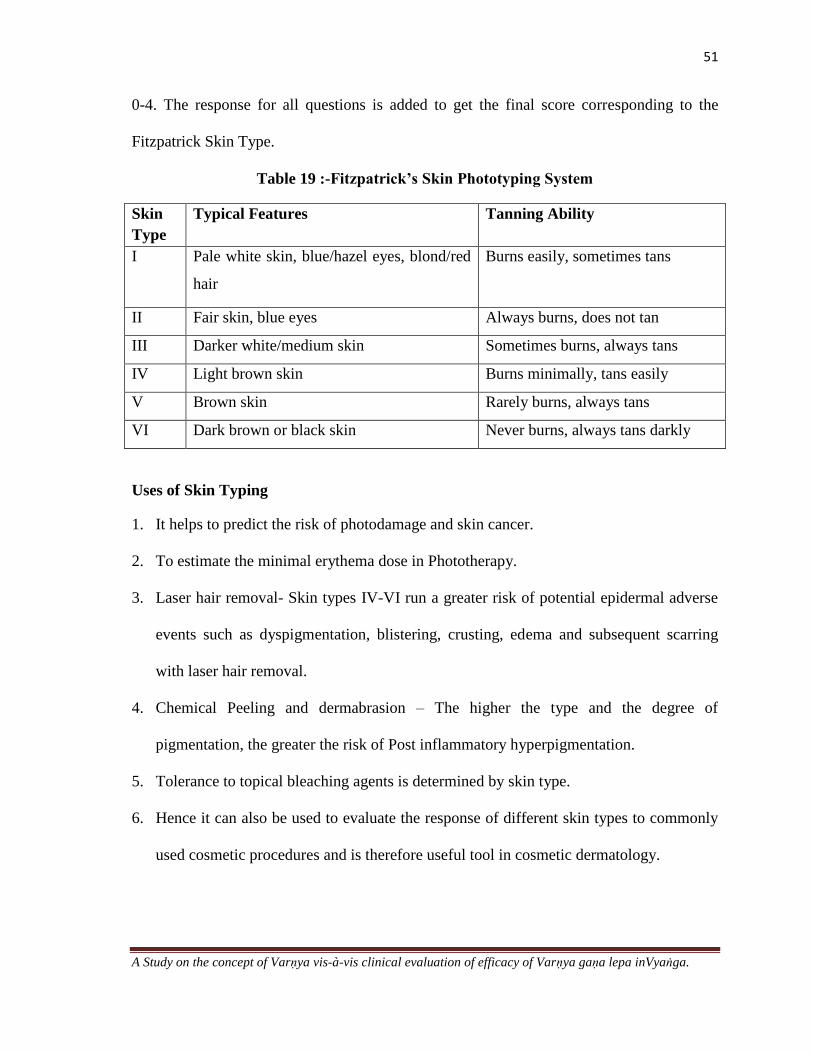
0-4. The response for all questions is added to get the final score corresponding to the
Fitzpatrick Skin Type.
Table 19 :-Fitzpatrick’s Skin Phototyping System
Skin
Type
Typical Features Tanning Ability
I Pale white skin, blue/hazel eyes, blond/red
hair
Burns easily, sometimes tans
II Fair skin, blue eyes Always burns, does not tan
III Darker white/medium skin Sometimes burns, always tans
IV Light brown skin Burns minimally, tans easily
V Brown skin Rarely burns, always tans
VI Dark brown or black skin Never burns, always tans darkly
Uses of Skin Typing
1. It helps to predict the risk of photodamage and skin cancer.
2. To estimate the minimal erythema dose in Phototherapy.
3. Laser hair removal- Skin types IV-VI run a greater risk of potential epidermal adverse
events such as dyspigmentation, blistering, crusting, edema and subsequent scarring
with laser hair removal.
4. Chemical Peeling and dermabrasion – The higher the type and the degree of
pigmentation, the greater the risk of Post inflammatory hyperpigmentation.
5. Tolerance to topical bleaching agents is determined by skin type.
6. Hence it can also be used to evaluate the response of different skin types to commonly
used cosmetic procedures and is therefore useful tool in cosmetic dermatology.
52
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
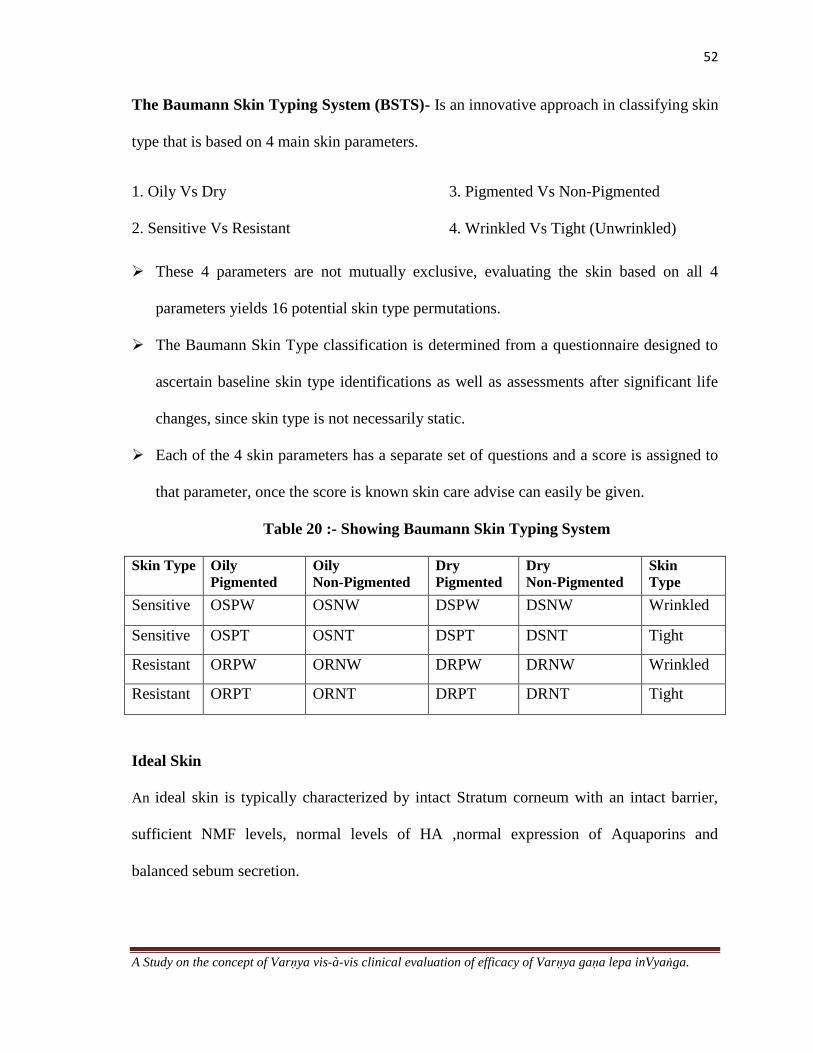
The Baumann Skin Typing System (BSTS)- Is an innovative approach in classifying skin
type that is based on 4 main skin parameters.
1. Oily Vs Dry
2. Sensitive Vs Resistant
3. Pigmented Vs Non-Pigmented
4. Wrinkled Vs Tight (Unwrinkled)
These 4 parameters are not mutually exclusive, evaluating the skin based on all 4
parameters yields 16 potential skin type permutations.
The Baumann Skin Type classification is determined from a questionnaire designed to
ascertain baseline skin type identifications as well as assessments after significant life
changes, since skin type is not necessarily static.
Each of the 4 skin parameters has a separate set of questions and a score is assigned to
that parameter, once the score is known skin care advise can easily be given.
Table 20 :- Showing Baumann Skin Typing System
Skin Type Oily
Pigmented
Oily
Non-Pigmented
Dry
Pigmented
Dry
Non-Pigmented
Skin
Type
Sensitive OSPW OSNW DSPW DSNW Wrinkled
Sensitive OSPT OSNT DSPT DSNT Tight
Resistant ORPW ORNW DRPW DRNW Wrinkled
Resistant ORPT ORNT DRPT DRNT Tight
Ideal Skin
An ideal skin is typically characterized by intact Stratum corneum with an intact barrier,
sufficient NMF levels, normal levels of HA ,normal expression of Aquaporins and
balanced sebum secretion.

53
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
The Stratum corneum is composed of three primary groups of compounds
o Ceramides- constitute 40% of the Stratum corneum lipids in humans
o Fatty acids and
o Cholesterol.
Natural moisturizing factor (NMF) derived from the breakdown of the protein flaggrin,
is integral in maintaining water within skin cells.
Hyaluronic acid which can bind 1000 times its weight in water is another substance
found in the skin that may help in retain and maintaining water.
Aquaporins are members of homologous water channels that facilitate fluid transport in
various organs such as skin, renal tubules ,eyes, digestive tract and even the brain.
Amount of sebum production also determines the skin hydration by producing glycerol
which is necessary for an intact barrier
Skin Hydration- The spectrum of Oily to Dry (O) to (D)
Dry skin/ Oily Skin
Dry skin describes skin that is characterized by dull colour, rough texture and an
elevated number of ridges. Dry skin is characterized by either an impaired barrier , lack of
natural moisturizing factor or decreased sebum production whereas Oily Skin exhibits
increased sebum production.
Combination skin
It is characterized by dry on the cheeks and oily in the T-Zone.
A higher score in the BSTS corresponds with increased sebum production and low
score with decreased skin hydration.
Skin that falls in the middle of this range would be considered as normal skin.

54
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Skin Sensitivity- The spectrum of Sensitive (S) and Resistant (R)
Sensitive Skin
Sensitive skin is characterized by inflammation and manifests as acne, rosacea,
burning and stinging, or skin rashes.
Resistant skin
Resistant skin is characterized by a robust stratum corneum (SC) that strongly
protects the skin from allergens, other environmental irritants, and water loss. Individuals
with resistant skin rarely experience erythema or acne. A high score on the S/R spectrum
correlates with sensitive skin while a low score represents resistant skin.
Skin Pigmentation-The Spectrum of Pigmented (P) to Non- Pigmented (N)
Skin Colour is not the focus here. Rather, the P/N parameter measures the tendency to
develop hyperpigmentation.
This segment of the BSTS determines those with a history or current presentation of
pigmentary alterations that can be prevented or improved with skin care products as
well as dermatologic procedures, and includes conditions such as melasma,
postinflammatory hyperpigmentation, and solar lentigos .
Although darker skin types are more likely to exhibit the P (pigmented) skin type, this
parameter does not refer to ethnicity.
The individual with a propensity to develop unwanted pigmentary changes is classified
as having the „P‟ Skin types in the BSTS system, a person not exhibiting this tendency
has Type N Skin.

55
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Skin Aging- The Spectrum of Wrinkled (W) to Tight (T)
This portion of the BST‟s identifies the risk for wrinkles. The questionnaire deals about
habits such as sun exposure smoking etc, the skin of ancestors to ascertain the genetic
influence on wrinkled skin.
The „W‟ types may not necessarily have wrinkles at the time that they complete the
BST but in time they will need to begin prevention methods because they are at risk.
Individuals with lighter skin are more likely to manifest „W‟ type skin than those with
dark skin.
Utility of Baumann Skin Typing System
1. The BST‟s can lend valuable assistance in the process of treating particular skin
problems and selecting the most appropriate products as well as dermatologic procedures
for an individuals particular skin type.
2. It is recommended that individuals take a baseline BST questionnaire and retake the test
at times of stress, change or when experiencing cutaneous symptoms because skin types are
not necessarily static.
3. Skin type alterations can be elicited by stress and marked fluctuations in stress,
pregnancy, and menopause, exposure to variable climates or moving to different climate or
various other significant exogenous or endogenous changes.

56
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Other Scales
Various other scales which are used are
Japanese Skin Type scale, Lancer Ethnicity Scale,
Pigmentation Scales- Taylor‟s hyperpigmentation Scale ,Melasma Area and Severity
Index, Skin Sensitivity- Acne Quality of Life Scale, Wrinkles and Photoaging Scales.
The ideal Scale is uncomplicated, easy to use and reliable with well defined categories.
An ideal Scale should also be reliable for use in daily practice in addition to clinical
trials.75
Figure No 2:-Different Skin types

57
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
MELANIN
Historical aspects of pigment cell biology
Human skin colour is predominantly based on the pigment melanin and influenced to a
minor extent by pigments such as carotene, reduced haemoglobin and oxyhaemoglobin.
Melanin is a term derived from the Greek word melas (black).
Robin is claimed to have been the first to use the term melanin when, in 1873, he
named the pigment in the pigment cells of animals 'pigment melanique’.
It was also revealed that tyrosine was the first compound in the melanin pathway and
that it was oxidized by the enzyme tyrosinase to dopa, which was then converted to
melanin through a series of intermediates.
Melanocytes- Origin and Migration
Melanocytes are neural crest derived, pigment synthesizing dendritic cells that reside
primarily in the basal layer.
Melanin is synthesized in the cytoplasm of specific dendritic cells which discharges
melanosomes into the surrounding keratinocytes through the dendrites.
Table 21 :- Various events from origin to migration of melanocytes 76
Time Event
8 weeks Melanoblasts arise from neural crest, they migrate along either side
of the spinal cord to the skin
10-12 weeks Population of melanocytes increase in the dermis
12-14weeks First appearance in the epidermis
16-20weeks Melanin synthesis starts
After 24 weeks They become established at the epidermal-dermal junction.
58
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
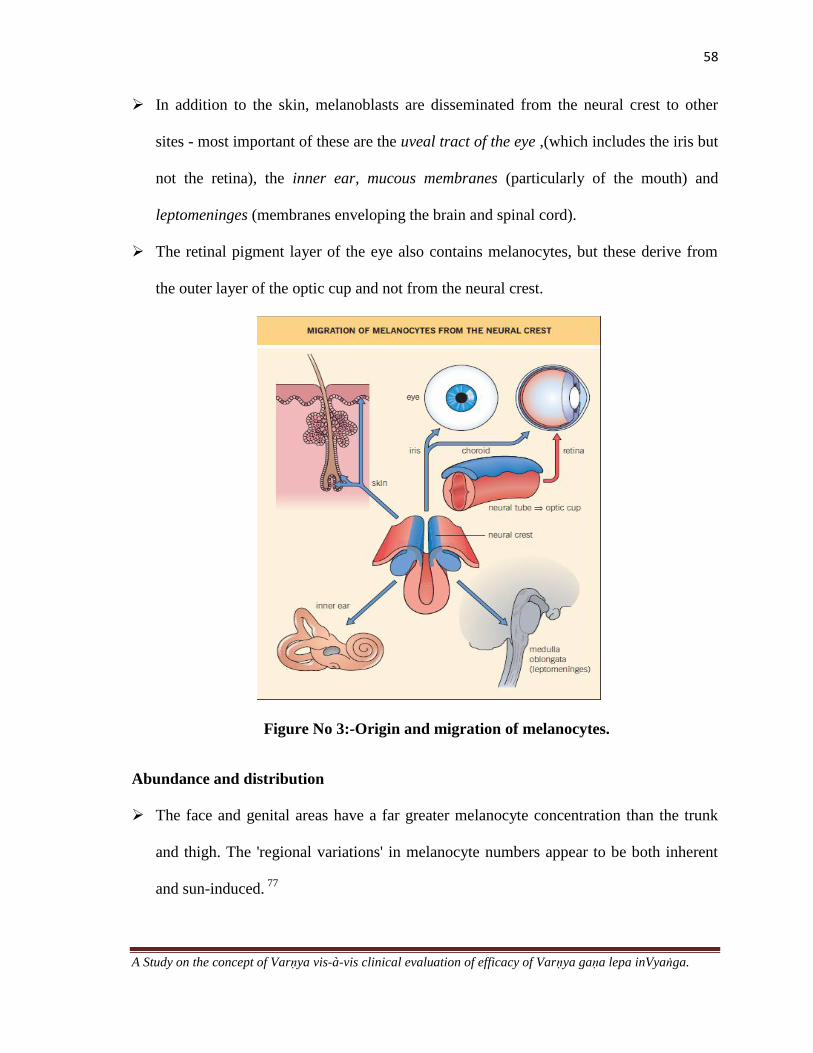
In addition to the skin, melanoblasts are disseminated from the neural crest to other
sites - most important of these are the uveal tract of the eye ,(which includes the iris but
not the retina), the inner ear, mucous membranes (particularly of the mouth) and
leptomeninges (membranes enveloping the brain and spinal cord).
The retinal pigment layer of the eye also contains melanocytes, but these derive from
the outer layer of the optic cup and not from the neural crest.
Figure No 3:-Origin and migration of melanocytes.
Abundance and distribution
The face and genital areas have a far greater melanocyte concentration than the trunk
and thigh. The 'regional variations' in melanocyte numbers appear to be both inherent
and sun-induced. 77
59
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Melanosomes
The basic currency of mammalian pigmentation is a cytoplasmic organelle called as
melanosome which contains the enzyme tyrosinase. 78
Melanosomes in human skin undergo four stages of development while inside the
melanocyte. In stage I, premelansomes are characterized by their spherical structure and
amorphous matrix. During stage II, they become more oval shaped with no apparent
melanin. In stage III, following tyrosinase activity, melanin production starts and the
melanization continues to stage IV, at which point the organelle contains high
concentrations of melanin. The melanosomes are then transferred along microtubules to
the dendritic structures of melanocytes and transferred to the keratinocytes
Melanocyte-keratinocyte relationship
The association of melanocyte and keratinocyte constitutes a functionally-active
partnership. These two cell types are mutually dependent and are considered as
structural and functional units which are termed as the epidermal melanin unit.
An epidermal melanin unit consists of one epidermal melanocyte in association with
20-40 keratinocytes to which it donates melanosomes.
The process of melanosome transfer from melanocyte to keratinocyte is a crucial one
because skin will not appear pigmented unless melanosomes are present within the
keratinocytes.
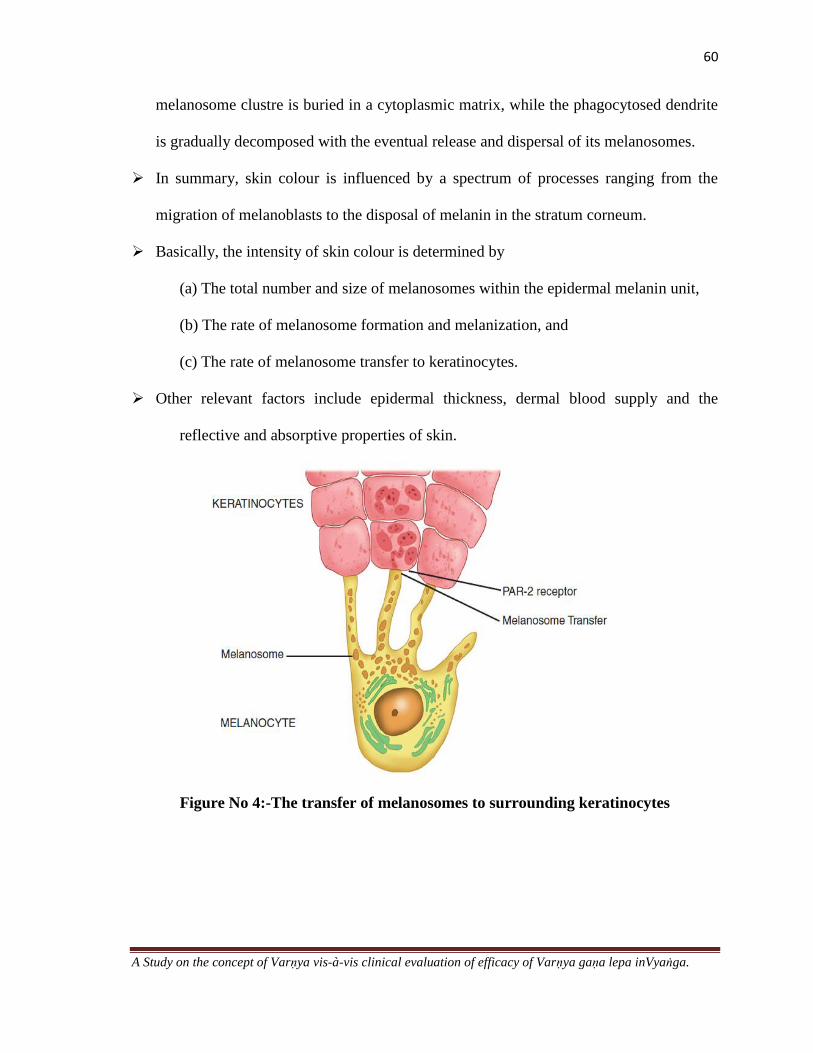
The modus operandi of this transfer has been intensively studied, and several models
were proposed. A popular model states that the tip of a melanocyte dendrite (containing
melanosomes) becomes enfolded in the recipient keratinocyte. This tip is then nipped
off together with its clustre of melanosomes by a process similar to phagocytosis. The
60
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
melanosome clustre is buried in a cytoplasmic matrix, while the phagocytosed dendrite
is gradually decomposed with the eventual release and dispersal of its melanosomes.
In summary, skin colour is influenced by a spectrum of processes ranging from the
migration of melanoblasts to the disposal of melanin in the stratum corneum.
Basically, the intensity of skin colour is determined by
(a) The total number and size of melanosomes within the epidermal melanin unit,
(b) The rate of melanosome formation and melanization, and
(c) The rate of melanosome transfer to keratinocytes.
Other relevant factors include epidermal thickness, dermal blood supply and the
reflective and absorptive properties of skin.
Figure No 4:-The transfer of melanosomes to surrounding keratinocytes
61
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Biochemical control of Pigmentation
Plant melanins have a different biochemical derivation from animal melanins. The
animal melanins originate from the amino acid tyrosine, and they are characterized by a
brown-black colour, a high molecular weight and a polymeric structure.
Biochemistry- Melanogenesis
Tyrosinase is the enzyme responsible for the formation of melanin within the
melanosomes, a process which will be referred to as melanogenesis. It is a copper-
containing enzyme which is stimulated by ultraviolet (UV) radiation, and other factors
such as melanocyte-stimulating hormone
There are two main types of melanin important in human biology: –
o Eumelanin - is the black-brown compound, which is found in the skin, hair and all the
other melanocyte-bearing tissues
o Phaeomelanin.- is the yellow-to reddish- brown pigment which has been identified in
mammalian hair (including human red hair) and in the feathers of chickens
o The relative amounts of these two types determine hair colour and skin tone.
Individuals with darker skin tones have mostly eumelanin and a lesser amount of
pheomelanin, while the opposite is true in people with a light skin colour
Hormonal Control of pigmentation
MSH and ACTH causes increase in tyrosinase activity with resultant stimulation of
melanogenesis.
Melatonin- MSH darkens the skin, where as melatonin lightens. It apparently acts by
inhibiting the later stages of melanin biosynthesis without affecting tyrosinase itself.

62
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Sex hormones- Oestrogen and progesterone have their strongest pigmentary impact on
the sexual skin and in the areolae.
Modifications in hormonal balance
Pregnancy- One of the early signs of pregnancy is darkening of the nipples and areolae
and, to a lesser extent, of the face, anterior abdominal wall and genitalia. These changes
are known collectively as the chloasma (or melasma) of pregnancy and they increase as
the pregnancy advances. During pregnancy there is a great increase in melanin
formation by the epidermal melanocytes, and melanocyte counts are higher than in
nonpregnant women of the same age group.
Oral contraceptives- The use of oral contraceptives has been associated with the
development of discolouration of the cheeks, forehead and nose similar to the chloasma
of pregnancy.
Menstrual cycle- There is some evidence that, like pregnancy, a similar but less marked
chloasma occurs during the menstrual cycle although menstrual chloasma is not an
established entity; the above evidence indicates that some skin discolouration does
occur in the premenstrual phase.
Other pigments responsible for skin colour- Melanoid- A pigment related to melanin
but having different absorption band of visible light.
Carotene- A yellow orange pigment is found in liquid rich areas such as stratum
corneum and the fat of the subcutaneous tissue.
Oxyhemoglobin- This imparts a red component to skin colour and is especially evident
in areas where there is a rich arterial supply, such as skin of the face, neck , palm , soles
and nipples.

63
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Reduced hemoblobin -It contributes a bluish or purple character to skin colour and is
more evident in lower part of the trunk. Factors such as melanin concentration and skin
thickness tend to suppress the hemoglobin pigment colour component effect.
Ultraviolet Light and Skin Colour
UV irradiation is a major source of environmental influence and damage to the skin.
There are 2 types of skin colour with respect to UV radiations.They are
o Constitutive skin colour (CSC) -refers to the genetically influenced colour and
melanin production without the impact of UV light or environmental factors.
o Facultative skin colour (FSC) denotes the colour influenced by UV light and
hormones. When exposed skin is subjected to UV light, melanogenesis or “tanning”
occurs, representing the skin‟s major defense against further UV damage. This
darkening results when the UV radiation provides a positive signal to the exposed
epidermal melanin units.
o Subsequent to UVA exposure, the skin develops an immediate pigmentary darkening
provoked by the oxidation of the existing melanin. This effect appears within a few
minutes of exposure to UVA and lasts for approximately 6 to 8 hours.
o Both UVB and UVA are involved in the process of delayed tanning. It is seen in 2 to
3 days after exposure and lasts for approximately 10 to 14 days.
o In this process, tyrosinase enzyme activity and the number of melanocytes that are
actively producing melanin increase. In addition, melanosome transfer from the
melanocytes to the keratinocytes is enhanced. The resulting increase in melanin
protects against further UV damage by surrounding the cell nucleus and absorbing
UV photons and UV-generated free radicals before they can react with DNA and

64
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
other critical cellular components. It was also demonstrated that DNA damage or
DNA repair intermediates can stimulate melanogenesis in the absence of UV light.
Table 22 :- Difference between Immediate and Delayed tanning
Immediate Delayed
Onset Minutes 3-4days
Peak Intensity Minutes to a few hours 10-28days
Fading Within 24 hours Weeks
Mechanism Redistribution
of melanosomes
Increased Tyrosinase level and activity,
Melanin Synthesis, Melanocyte dendricity,
Melanosome number, Melanosome transfer,
Melanocyte proliferation
Photo
protection
Unchanged Increased
Change in skin
Colour
Undetectable in fair
skin
Obvious in most light skinned and all dark
skinned individuals
Skin Colour Perceptions
Visible light reaches the skin surface and is either reflected back to the eye from the
stratum corneum or enters the skin and is then reflected back to the eye from collagen
fibers, blood vessels, and melanosomes. In ethnic skin, the desquamating corneocytes
contain pigment. This brown skin scale appears grey when viewed, as a result of the air
interface behind the scale and gives rise to the term “ashy,” which is used to describe the
appearance of dry skin in darker complexioned population. Ashy skin is equated with dry
skin and is considered unattractive because of the suboptimal skin colour viewed as light
bounces off of the stratum corneum.

65
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Visible light may also enter ethnic skin, which contains abundant pigment, for
subsequent reflection to the eye. If the pigment is evenly distributed, the skin appears an
even brown colour. If the melanin is present in clumps, the skin will appear unevenly
lighter and darker depending on the pigment distribution. In Fitzpatrick skin types I, II, and
III unevenness in skin colour is caused by the irregular distribution of vascular structures
and collagen, giving the skin undesirable red and yellow colours. The effects of collagen
breakdown and the formation of telangiectatic vascular structures are not of primary
concern in ethnic skin, making pigmentary change the single most important measure of
skin attractiveness. 79
Figure No 5 :-Skin colour perceptions –
Light is reflected from the skin surface and within the skin from hemoglobin, collagen,
and melanin.
66
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
VARNYA
Introduction
Complexion which is the manifest form of beauty is enhanced by various means.
This task of enhancement of complexion is termed as Varṇya. Various treatment modalities
such as Nasya, Raktamokṣana and Lepas have been mentioned by different authors which
are attributed to Varṇya Karma. Varṇya upakramas seems to be a ray of hope to fulfill the
cosmetic demands of this aesthetic era. Hence there is a need for its extensive study.
Definition
uÉhrÉï- uÉhÉÉïrÉ ÌWûiÉqÉç CÌiÉ uÉhrÉïqÉç || 80
That which is beneficial for Varṇa is said to be as Varṇya
uÉhrÉïÈ qÉÑZÉurÉ…¡ûÉÌSuÉhÉïMüU | 81
That which enhances Varṇa and which imparts physiological colour in mukha vyaṅga
uÉhrÉïÈ uÉhMïüUÈ |82
That which enhances Varṇa is termed as Varṇya
Synonyms
Varṇa prasādana, Varṇa vaiśadyakaram, Varṇa vaimalya, Varṇa śuddhi 83
, Varṇa karam,
Varṇa utkarṣa, Varṇa dārḍhya Varṇa upacaya, Varṇaprasannatvakara
84
Dinacaryā and their effect on Varṇa
Classical literature reveals that most of the procedures which are followed as a part of
dinacaryā are said to have an impact on the colour and complexion of the individual.

67
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Table 23 :-Dinacaryā and their effect on Varṇa
Sl.No Dinacaryā Effect On Varṇa
1. Abhyaṅga Varṇa Balaprada, Sutvak, Twachya,
Upachita Aṅga
2. Śiro'bhyaṅga Mūrdhni Taila Sutvak
3. Vyāyāma Kānti Gātraanām
4. Udvartana Twak Prasādana
5. Tāṁbūla Sevana Kānti Sauṣṭhavakāraka
6. Utsādana Kāntimat Mṛjā
7. Udgharṣana Twak Gatasya Agni Tejana
8. Anulepana Varṇakaram , Vaivarṇyaghnam
9. Snāna Varṇya
10. Bāṇāvara Varṇa Vivardhana
11. Āsyā Varṇa Soukumāryakari
12. Kṣaura Karma Kāntikara
13. Chatra Dhāraṇa Varṇya
14. Puṣpa Dhāraṇa Pāṭalī, Punnāga,
Kunda Vāsantikā, Ketakī, Bakula,
Kunda
Kāntikarakam
15. Nidrā Varṇa Dīpti
16. Saṁvāhana Twak Prasādakaram
17. Valkala Dhāraṇa Kāntikaram
18. Kārpāsa Uṣṇīśa Twak Roukshyāhāram Varṇyam
19. Bhūṣaṇa Dhāraṇa Kāntidam
20. Mouktika Dhāraṇa Kāntidam
21. Phala Dhāraṇa - Uduṁbara,Kadalī
Sugandhī , Kapittha, Mātuluṅga
Kāntikaram, Varṇyam
22. Tāmra Pātra Bhojana, Kānta Pātra,
Roupya Pātra, Veṇu Pātra
Kanikaram, Varṇyam
23. Pāda Saṁvāhana Twak Prasādkaram
24. Nasya Prasanna Twak
25. Taila Gaṇḍūṣa Vadana Upacaya

68
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Āhāra Vargās which are Varṇya
Certain Āhāra dravyās are said to promote the colour and complexion and are also
indicative of importance of food in creating and maintaining Varṇa.
Table 24 :-Āhāra vargās which are Varṇya
Sl. No Āhāra varga Dravya
1 Shāli varga Yava, lohita
2 Śiṁbivarga Makuṣṭha, masūra ,tila
3 Māmsa varga Barhi ,Rohita Tittira, haṁsa, mayūra , māmsa rasa
4 Shāka varga Tila
5 Phala varga Baddha kesara, āmra with kṣīra,Pakva āmra
6 Harita varga Rasona
7 Madhya varga Madhya, pakva rasa madhya, Apakva rasa madhya
8 Gorasa varga Kṣīra, kṣīrottha navanīta, Catu Sneha, ghṛta
9 Ikṣu varga Śarkara ,madhu , ikṣu
10 Taila varga Tila taila, Eraṇḍa taila
11 Kritānna varga Mantha, ghṛta taila pakva bhakṣya, yūṣa of sthavira
and jīraka
Dietary pattern:
It is mentioned that Diet taken in appropriate quantity certainly helps the individual in
bringing out complexion without disturbing the Prakŗti.Also the wholesome food
consumed according to rules is said to be complexion promoter 85
.It is stated that unctuous
food taken by an individual brings out the brightness of complexion. According to
Kashyapa Saṁhitā, Āhāra taken with Sneha dravya stimulates the „Varṇya‟ process. Lustre
of skin gets increased by the suitability of diet and regimen as per the season. Similarly;
„Anupāna‟ promotes the complexion.

69
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Role of Rasās
Madhura rasa and kasāya rasa are said to possess Varṇa prasādana karma
Role of Guṇas
Mṛdu, Accha, Ūṣṇa, Snigdha, Ślakṣṇa, Drava guṇas play a major role. These result in
Sukumāra avadāta gātra, Prasanna snigdha Varṇa, Gaura, Snigdha, Ślakṣṇa aṅga
Trividha Cikitsā
Classical literature of Āyurveda basically deals with 3 types of Cikitsā. They are
Antah Parimārjana
Bahi Parimārjana
Śastra Praṇidhāna
Antah Parimārjana
Cikitsā which basically aims at entering the Antah śarīra and mainly cures the Āhāra jāta
vyādhi is termed as Antah Parimārjana Cikitsā
Antah parimārjana as Varṇya
Samśodhana Therapy
Caraka Saṁhitā states that Normal complexion is restored by Samśodhana therapy and
Basti given in a prescribed manner improves complexion and strength. Aṣṭāṅga Saṁgraha
and Astaṅga Hṛdaya also explains the role of Elimination therapy in promoting the colour
and complexion. 86
70
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Śamana Cikitsā
Rasāyana
The Rasāyana therapy improves both the lustre and complexion. The four herbs which are
mentioned as Medhya Rasāyana also improve colour and complexion.87
Some yogas like
Laśuna kalpa and Śatāvarī Rasāyana are prescribed for improving the Varṇa. 88
Similarly
in Bhāvaprakāśa Samhitā the Yogas such as Guḍāṣṭaka, Vidārī ghṛta are stated to have an
action on the Varṇa. Vṛṣya Ghṛta and Takrāriṣṭa are also said to promote complexion. 89
Yogas like Āmalaka ghṛta and Aindra rasāyana
90and other Yogas like Amrtaprāśa ghṛta
and Sarpirmodaka 91
are mentioned.
Bahi Parimārjana as Varṇya
Cikitsā which mainly aims to cure the diseases which are localized in the skin through
Abhyaṅga, Sweda, pradeha, pariśeka, unmardana etc is termed as Bahi Parimārjana
Cikitsā.
Varṇya Upakramas:
In „Vraṇa Śotha Cikitsā‟, under the heading of „Vaikṛtāpaha’ twenty two Upkramas are
explained, among them „Kṛṣṇakarma‟ and „Pāndukarma’ are meant to change the
abnormal colour of healed wound. 92
Gaṇas
The herbs belonging to these Gaṇas are said to promote complexion.
Varṇya Gaṇa,93
Elādi Gaṇa –Varṇya,
Rodhrādi Gaṇa- Varṇa prasādana

71
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Herbs which promote complexion mainly includes
Candana, Tuṅga ,Padmaka ,Uśīra ,Madhūka ,Mañjiṣṭhā ,Sāriva ,Payasya ,Sitā ,Latā
constitute Varṇya Gaṇa
Ela, Tagara, Kuṣṭha, Māṁsī, Dhyāmaka, Tvakpatra, Puṣpa, Priyaṅgu, Hareṇuka
Vyaghranaka, Śukti, Canda, Sthauṇeyaka, Śrīveṣṭaka, Coca, Coraka ,Vāluka, Guggulu
Sarja Rasa, Kunduruka, Taruṣka, Aguru, Spruk, Uśīra, Bhadradāru, Kumkuma
Punnāga, Kesara constitute Elādi Gaṇa.
Lodhra, Savara Lodhra, Palāśa Kuṭannaṭa, Aśoka, Phañjī, Kaṭphala, Elavāluka,
Śallakī Jiṅginī, Kadalī, Kadamba, Sāla constitute Rodhrādi Gaṇa.
Bahi Parimārjana producing Varṇya effect
Bahi parimārjana cikitsā as the name indicates is mainly intended for external use only.
Hence different forms of external applications are described in the context of treatment of
different diseases. They are Lepa Kalpanā Upanāha, Malahara kalpanā etc.
Lepa kalpanā
Synonyms: Ālepa, Lipta, lepa, Lepana.
Medicines in the form of a paste used for external application are called lepas. Wet
medicinal drugs are made into kalka (paste form), if drugs are in dry state they are
converted into kalka (paste) by adding little quantity of water and grinding. This kalka is
used as external application and is called lepa kalpanā. Water, cow‟s urine, oil and ghee
are some of the media used for mixing.
Pharmaceutically lepa kalpanā is a form of kalka kalpanā. While clinically lepa
kalpana is only meant for external application where as kalka is very commonly used for
internal administration.

72
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Various classical literatures of Āyurveda have explained different types of lepas on the
basis of the drugs used for preparation and mode of administration and its usage.
According to Suśruta Saṁhitā Lepa is of 3 varieties.
Śaraṅgadhara Saṁhitā categorises Lepa Kalpanā on the basis of the drugs used for the
preparation and their action. Śaraṅgadhara Saṁhitā also categorises lepa kalpanā into
varieties on the basis of mode of administration and its usage
According to Aṣṭāṅga Saṁgraha lepas are of 10 types. Among these first five lepas are
most useful formulations for the treatment of Vraṇa Śotha. Rest of the five lepas are
useful for the treatment of secondary stage of vraṇa.
Table 25:- Different ypes of lepa
S.S Sha.Sam A.S
Pralepa Doṣaghna Lepa Pralepa Snaihika Pācana,
Pradeha Viṣaghna Lepa Pradeha Nirvāpaṇa Pīḍana
Ālepa Varṇya Lepa Prasādana Śodhana
Staṁbhana Śoṣaṇa
Vilayana Savarṇīkaraṇa
Table 26 :- Difference between Types of lepa
Pralepa Pradeha Ālepa
Shīta lepa (with Shīta guṇa
dravyas) without heating
Uṣṇa lepa (with Uṣṇa
vīrya drayas)
The action, thickness etc of
this lepa will be moderate
(Madhyama ālepa)
Tanu lepa (thin) Bahala (thick) Useful in Rakta and Pitta
doṣa pradhāna twak vikāra.
May or may not be dry
(Viśoṣī or Aviśoṣī)
Aviśoṣī (Remains moist
for long ime)
Indicated in Pittadoṣa
Pradhāna Twak rogās

73
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Rules of Application of lepa and Mechanism of its absorption
1. Lepas should always be applied in the opposite direction of the hair follicles. The drugs
get absorbed through their hair roots, sweat glands and capillaries.
2. While applying the lepas Snehas are said to be added. Their quantity has to be decided
as per the doṣa vitiated.
Vātaja vyādhi- 1/4th
part of Sneha dravya
Pittaja Vyādhi-1/6th
part of Sneha dravya
Kaphaja Vyādhi-1/8th
part of Sneha dravya
3. The lepa should not be left in situ after drying. It must be removed as soon as it dries
up. Because lepās in wet state help to cure the diseases , where as on drying they lose
their potency and irritate the skin.
4. Lepas should be prepared freshly and used.
5. They should be used only once.
6. Over the previous lepa fresh one should not be applied.
7. Lepas should not be applied at night. If applied, it causes skin diseases by suppressing
the local temperature and disturbing the local circulatory system.
8. Pralepa should not be applied at nights nor should it be allowed to stay on after it dries
up. Where as Pradehas can be allowed to stay on in order to cause constriction or
pressure over the part of the body.
9. The thickness of the lepas is said to be of that of wet skin of buffaloes
General actionsof Lepa
1. Vraṇa Śodhaka
2. Vraṇa Ropaka

74
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
3. Dāha Śāmaka
4. Kaṇḍūhara
5. Sandhāna Kara
6. Śothahara
7. Śūlahara
8. Staṁbhaka (Ex-Niruddha lepana-A thick paste of drugs applied to check the
bleeding).
Preservation of Lepas:- Vegetable lepa churnas will preserve their potency for 30 days
if kept in airtight containers. Minerals and Metallic preparations last indefinitely.
Mode of action of Lepas
When an auṣadha or kriyā dravya is applied on the skin, it enters the romakūpa, reaches
swedavaha srotas and thus the rasa tarpaṇa occurs and the applied drug is metabolized
by the auśṇya of bhrājaka pitta present in the skin.94

75
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
COMPLEXION PROMOTERS.
Complexion of an individual can be promoted by 2 ways. One is by oral administration of
dietary ingredients which are beneficial for skin and other way is by topical applications.
Nutritional Cosmetics
Nutritional cosmetics, more commonly referred to as nutricosmetics, embraces
the idea that beauty can be enhanced through the consumption of functional dietary
products that may support healthier and thus more beautiful skin. The term
nutricosmetics appears to borrow from the terms nutraceuticals and cosmeceuticals to
reflect the goal of these products, that is, to provide health and beauty benefits to the skin
via nutritional products consumed on a regular basis. This concept encompasses a unique
amalgamation of the nutrition and personal care industries. 95 It is said that “Let food be
your medicine and let medicine be your food”- It is from such a perspective that good
nutrition is a fundamental building block of good general health and healthy skin.
One of the more important aspects of healthy looking skin is a smooth
appearance. However, a smooth appearance can be difficult to maintain without a firm
foundation and proper hydration. A Variey of Natural dietary ingredients support a firm
skin foundation and proper skin hydration. The various skin types according to BST
classification have unique requirements. 96

76
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Table 27 :- Dietary needs of different skin types97
Skin Type Ingredient Source
Dry
Skin
Cholesterol,
Hyaluronic acid,
Omega 3 fatty acids,
Glucosamine,
Niacinamide(Vitamin B3 )
Animal fats,cheese, egg yolks, fish, shrimp, flax seeds
Fresh fruits vegetables,
Fish, flax seed, walnuts
Shells of shell fish
Peanuts, yeast, fish , meat
Oily &
Sesitive
Vitamin A
Omega 3 fatty acids,
Carrots, dried apricots, spinach, milk, oats
Fish, flax seed, walnuts
Resistant Nothing Specific -
Pigmented Glucosamine
Pycnogenol
Vitamin C
Shells of shell fish
Pomogranate, grapes Soy
Non
Pigmented
Nothing Specific
Wrinkled Mono unsaturated fatty acids
Co enzyme Q 10
Red meat ,olives, cashew
fish ,shell, fish, spinach , nuts
Asparagus, Garlic Spinach
Tight Nothing Specific -
Principles of Topical Therapy
Sensible topical drug therapy involves not only the selection of an appropriate agent, but
also a thoughtful consideration of the :-
Areas of the body affected,
The state of the diseased skin,
The concentration of the drug,
The type of vehicle (e.g ointment cream lotion)
The method of application and
77
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
A defined duration of use that both maximizes efficacy and minimizes adverse side
effects.
Cutaneous Drug Delivery
The therapeutic efficacy of a topical drug relates to both its inherent potency and the
ability of that drug to penetrate the skin. Percutaneous absorption necessitates passage
through the stratum corneum, epidermis, papillary dermis and into blood stream.
General Guidelines for Topical Therapy
Vehicle
The vehicle is the inactive part of a topical preparation that brings a drug into contact
with the skin.
The vehicle of a topical formulation often has beneficial non-specific effects by
possessing cooling, protective, emollient occlusive or astringent properties.
Rational topical therapy matches an appropriate vehicle that contains an effective
concentration of the drug.
The vehicle functions optimally when it is stable both chemically and physically and
does not inactivate the drug.
The vehicle also should be non irritating, non allergenic, cosmetically acceptable and
easy to use. Additionally the vehicle must release the drug into the pharmacologically
important compartment of the skin.
Finally the patient must accept using the vehicle or else compliance will be poor.
Dosage: An amount of topical medication sufficient to cover affected body surfaces in
repeated applications must be dispensed to the patient.

78
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Regional Anatomic Variation
Permeability generally is inversely proportional to the thickness of the stratum
corneum. Drug penetration is higher on the face, in intertriginous areas, and especially in
the perineum. Consequently, the skin in these regions may be more susceptible to irritant
and allergic contact reactions.
Altered Barrier Function
In many dermatological diseases, such as psoriasis, the stratum corneum is
abnormal, and barrier function is compromised. In these conditions, percutaneous
absorption may be increased to the point that standard drug doses can result in systemic
toxicity (e.g., hypothalamic-pituitary-adrenal axis suppression can result from systemic
absorption of potent topical glucocorticoids).
Hydration
Drug absorption is increased with hydration, defined as an increase in the water
content of the stratum corneum that is produced by inhibiting transepidermal loss of
water. Methods of hydration include occlusion with an impermeable film, application of
lipophilic occlusive vehicles such as ointments, and soaking dry skin before occlusion.
Classification of Topical formulations
Table 28 :- Classification of Topical formulations
Powders
Jellies
Thickening
agents
Ointments-Hydrocarbon bases, Absorption
bases,Water in oil emulsions (creams) , Oil in water
emulsions, water soluble bases
Poultices
Cerates
Stabilisers
Liquids-Solutions, Suspensions, Shake lotions
Pastes Plasters
Aerosols-

79
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Mode of action of Topical Applications98
Following the application of the drug to the skin surface, its subsequent passage through
the skin barrier into the underlying skin layers and its distribution into systemic
circulation is as follows.
Penetration pathways
The surface of the stratum corneum presents more than 99% of the total skin surface
available for percutaneous drug absorption. In order to undergo percutaneous absorption
the compound must penetrate the stratum corneum, diffuse into and through the viable
epidermis, into the dermis, finally gain access to the systemic compartment through the
vascular system. 3 Penetration pathways are possible. They are;-
Intercellular ( inside the lipid layers around corneocytes)
Follicular
Intracellular penetration.
The major steps involved in percutaneous absorption include
The establishment of a concentration gradient, which provides the driving force for
drug movement across the skin;
Release of drug from the vehicle (partition coefficient); and Drug diffusion across the
layers of the skin to reach the systemic circulation. (Diffusion coefficient).99

80
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Figure No 6 :-The mode of action of topical applications

81
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
VYANGA
Introduction
Kṣudra Rogas are those group of disorders which are basically characterized by Alpa
rūpa or these are also termed as Alpa Vyādhi (Shabda kalpa druma) The diseases which
manifest in children are also termed as Kṣudra rogas. They are also known by the terms
Swalpa, Adhama or Krūra Vyādhis Diseases which are caused by Adharma are also
termed as Kṣudra rogas. Vyaṅga is a disease which belongs to Swalpa variety of Kṣudra
Roga Prakaraṇa.
Kṣudra roga swa rūpa
Kṣudrarogas are characterised by both mandavega or mahāvega & some are
alparujāyukta and others are adhika pīḍā yukta, some are mahān and some are alpa
vyādhis.
Vyaṅga
ÌuÉM×üiÉÉÌlÉ ½…¡ûÉÌlÉ rÉxrÉ |
ÌuÉaÉiÉ ÌuÉMüsÉ A…¡û mÉëÉÍkÉMüqÉï |
Any sort of deformity is termed as Vyaṅga
urÉ…¡ûÈ zrÉÉqÉuÉhÉï qÉhQûsÉÇ qÉÑZÉå| 100
The word Vyaṅga literally means - Spotted, speckled, freckles on the face, a blot or
blemish.- (Monier Williams Dictionary)

82
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Historical Review
RigVeda
There is description of historical event - Śyāva Roga, (Discolouration) as a consequence
of kuṣṭha which was cured by Lord Indra and later he was blessed with a beautiful wife.
Saṁhitā kāla
CarakaSaṁhitā, Suśruta Saṁhitā, Astaṅga Hṛdaya
Vyaṅga has been described by all the bṛhat trayī. A detailed and separate description of
Vyaṅga in the chapter of „Kṣudra Roga’ is available in Suśruta Saṁhitā which includes
Nidāna, lakṣaṇa, samprāpti and sāpekṣa nidāna Both Caraka Saṁhitā and Suśruta
Saṁhitā considers Vyaṅga as a „Raktaja Roga’& a common samprāpti for Tilakālaka,
Piplu, Vyaṅga and Nīlikā in Triśothīya Adhyāya has been given.101
Individuals who
belong to Pitta Prakṛti are said to be prone to Vyaṅga. Social importance for the
appearance of the individual is also clear from the reference that the qualities of an ideal
Śiṣya and Dhātrī (wet nurse) are to be devoid of Vyaṅga. More elaborate description is
available in Astaṅga Hṛdaya Uttaratantra, in the „Kṣudra Roga Prakaraṇa where in the
Dośānusāra Lakṣaṇas of the disease are explained in detail.
Madhyakāla
Madhava Nidāna, Śarangadhara Saṁhitā, Bhavaprākāśa , Cakradatta, Yogaratnākar
have described about the disease Vyaṅga in the context of Kṣudra roga.
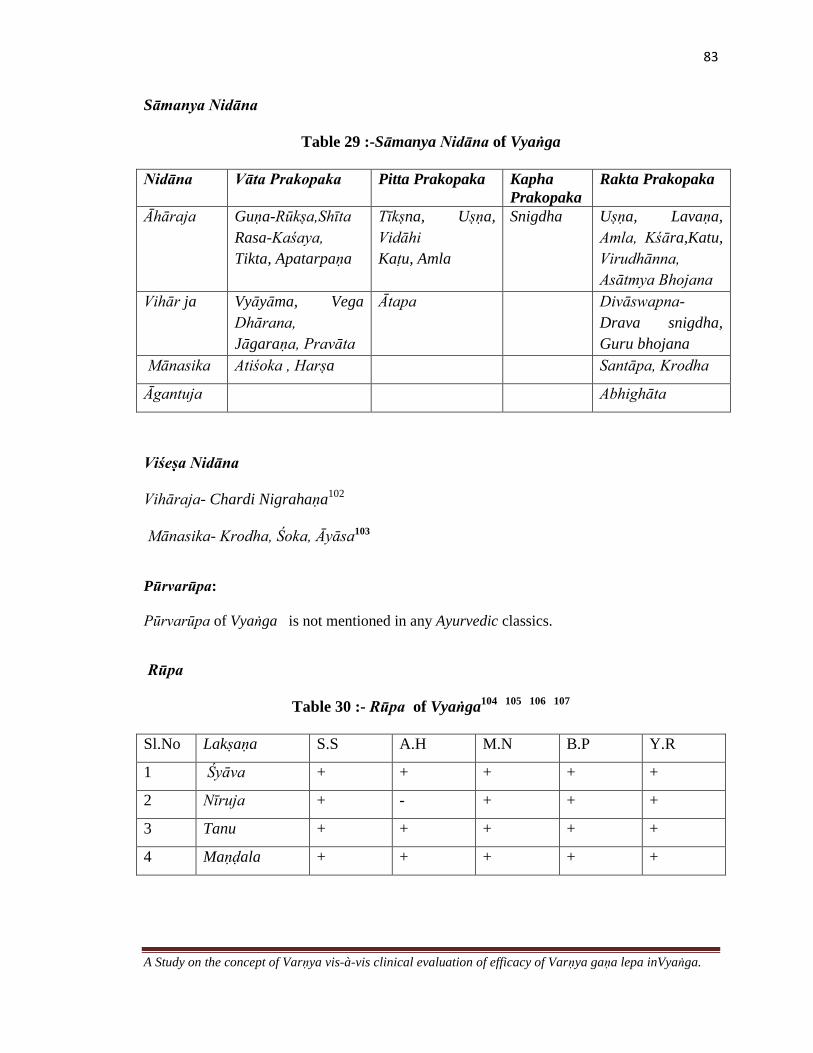
83
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Sāmanya Nidāna
Table 29 :-Sāmanya Nidāna of Vyaṅga
Nidāna Vāta Prakopaka Pitta Prakopaka Kapha
Prakopaka
Rakta Prakopaka
Āhāraja Guṇa-Rūkṣa,Shīta
Rasa-Kaśaya,
Tikta, Apatarpaṇa
Tīkṣna, Uṣṇa,
Vidāhi
Kaṭu, Amla
Snigdha Uṣṇa, Lavaṇa,
Amla, Kśāra,Katu,
Virudhānna,
Asātmya Bhojana
Vihār ja Vyāyāma, Vega
Dhārana,
Jāgaraṇa, Pravāta
Ātapa Divāswapna-
Drava snigdha,
Guru bhojana
Mānasika Atiśoka , Harṣa Santāpa, Krodha
Āgantuja Abhighāta
Viśeṣa Nidāna
Vihāraja- Chardi Nigrahaṇa102
Mānasika- Krodha, Śoka, Āyāsa103
Pūrvarūpa:
Pūrvarūpa of Vyaṅga is not mentioned in any Ayurvedic classics.
Rūpa
Table 30 :- Rūpa of Vyaṅga104
105
106
107
Sl.No Lakṣaṇa S.S A.H M.N B.P Y.R
1 Śyāva + + + + +
2 Nīruja + - + + +
3 Tanu + + + + +
4 Maṇḍala + + + + +

84
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Types
According to the Doṣa predominance, the disease Vyaṅga may be categorized into four
subtypes as,
(1) Vātika: The maṇḍalas are charecterised by Śyāva Varṇa. On sparśa maṇḍalas are
Khara or Paruśa.
(2) Paittika: The Varṇa of maṇḍalas may be either Tāmra or Nīla.
(3) Kaphaja: The maṇḍalas are of Śweta Varṇa and it may be associated with kaṇḍū
(4) Raktaja: The maṇḍalas are Rakta or Tāmra Varṇa and may be with dāha. 108
Figure No 7 :- Lakṣaṇas of Vyaṅga
Samprāpti
Due to the intake of Āhāraja, vihāraja, Mānasika nidāna (Āyāsa, Krodha), there is
vitiation of Vāta along with pitta. The vitiated doṣas lodge in the twak of mukha
producing Nīruja, tanu, śyāva maṇḍalas which is termed as Vyaṅga 109
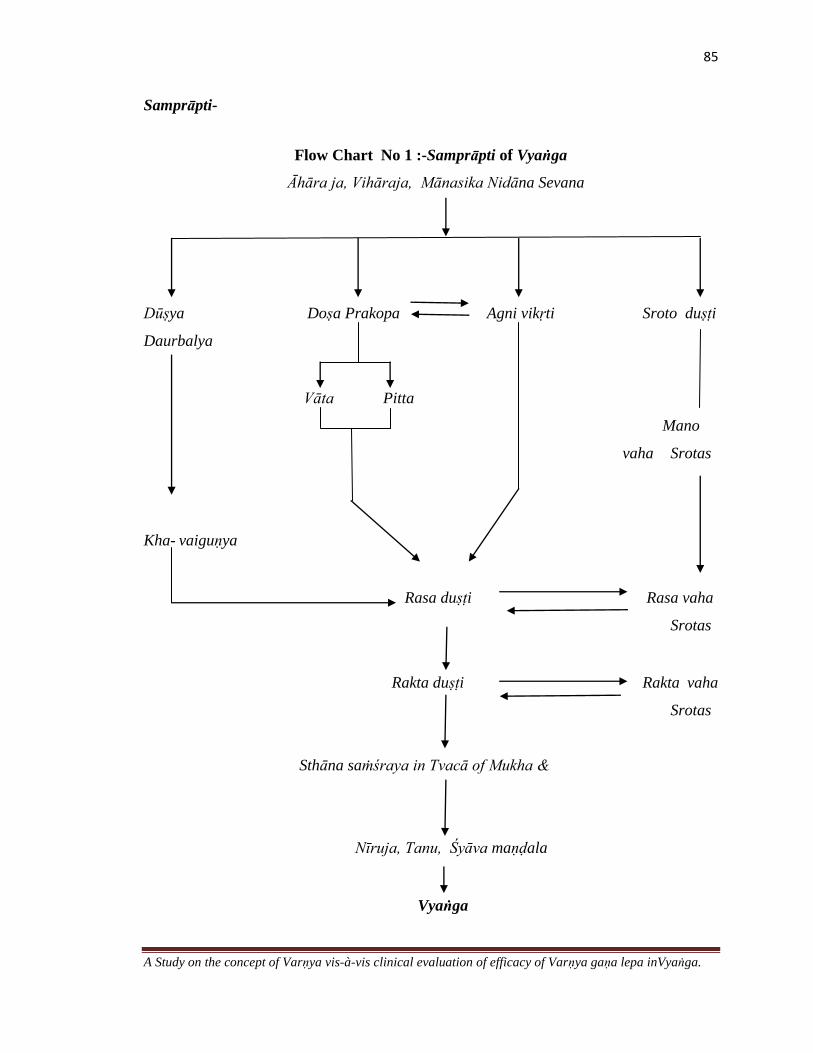
85
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Samprāpti-
Flow Chart No 1 :-Samprāpti of Vyaṅga
Āhāra ja, Vihāraja, Mānasika Nidāna Sevana
Dūṣya Doṣa Prakopa Agni vikṛti Sroto duṣṭi
Daurbalya
Vāta Pitta
Mano
vaha Srotas
Kha- vaiguṇya
Rasa duṣṭi Rasa vaha
Srotas
Rakta duṣṭi Rakta vaha
Srotas
Sthāna saṁśraya in Tvacā of Mukha &
Nīruja, Tanu, Śyāva maṇḍala
Vyaṅga

86
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Samprāpti Ghaṭaka
Table 31 :-Samprāpti Ghatakas of Vyaṅga
Doṣa Vāyu (Udāna, Vyāna) ,Pitta (Bhrājaka)
Dhātu Rasa, rakta,
Upadhātu Tvak
Dūṣya Rasa, Rakta, Manas
Srotas Rasavaha , Raktavaha, Manovaha
Sroto duṣṭi prakāra Saṅga, Vimārgagamana
Adhiṣṭhāna Tvacā
Swabhāva Mṛdu
Agni Jatharāgni ,Dhatvāgni (Rasāgni, Raktāgni)
Roga Mārga Bāhya rogamārga (śākha)
Vyakta Sthāna Tvak
Rugviniścaya:
1. Nyaccha: Broad or small, grey or dark discoloured, painless patches on the skin of the
body are called Nyaccha.
2. Nīlikā: Similar black discolouration as Vyaṅga appearing in other parts of the body is
known as Nīlikā
3. Jatumaṇi:- A congenital, slightly elevated, even, smooth, slightly reddish in colour
and painless patch on the skin caused by kapha and rakta is known as Jatumaṇi.
4. Maṣaka: Painless, immovable, black, round nodules on the skin resembling blackgram
caused by Vāta is called Maṣaka.
5. Tilakālaka: Black, painless spots resembling sesamum seeds, not raised above the
level of the skin, caused by vāta, pitta and kapha together is known as Tilakālaka. 110

87
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Cikitsā
Ayurvedic classics advocate the use of various formulations in the treatment of Vyaṅga in
addition to that certain formulations are indicated which alleviates the discolouration and
enhances the complexion of the face.
Mainly two types of the therapies are found to be advised for the disease Vyaṅga
A. Śodhana therapy like Vamana, Virecana, Nasya, Raktamokṣhana etc.
B. Śamana therapy in the form of internal medicines and external application of drugs in
the form of Lepa, Taila etc111
A. Śodhana Therapy
Though Vyaṅga is a Kṣudraroga and locally manifested disease, it also requires Śodhana
in chronic stage of the disease. Many classical texts indicated Śodhana therapy for the
disease Vyaṅga .112
B. Śamana Therapy
Various dosage forms are advocated for both external and internal use in Vyaṅga
Treatment Modalities of Vyaṅga mentioned by different Authors

88
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Table 32 Showing Treatment modalities of Vyaṅga113
Treatment
Modalities
C.S S.S A.H A.S B.P Y.R B.R
Mukha prakṣālana - + - - - - -
Lepa - + + + + + +
Abhyaṅga - - + + + + +
Pradeha - + - - - - -
Pāna - - - - + - -
Nasya - - + + - - -
Raktamokṣana - + + + + + -
Vamana - - - + - - -
Virecana + - - + - - -
Śamana yoga
Table 33 Showing Śamana yogas in Vyaṅga
Ghṛta Nīlinyādi Ghṛta, Varṇaka Ghṛta
Ariṣṭa Abhayāriṣṭa, Paṭolāriṣṭa
Taila for Abhyaṅga Kuṅkumādi Taila, Kaṭu Taila, Abhyaṅga
Taila for Nasya Aṇu Taila
Cūrṇa for Udvartana Tribhuvanādi Chūrṇa
Lepa
Mukha Kāntikara lepa, Śaśa Asṛk lepa, Jātī Phala Kalka lepa
Sādhyāsādhyata-Vyaṅga is a Sādhya vyādhi. & it has has no upadravas.
Vyaṅga as Ariṣṭa lakṣaṇa- akasmāt prādurbhāva of Vyaṅga is considered as ariṣṭa
lakṣaṇa

89
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
MELASMA
Introduction
Acquired hyper pigmentation disorders of the skin are among the most common
complaints in a general dermatology clinic. Among those, melasma is known for causing
significant impact on quality of life, including a negative effect on the patients emotional
well being and social life .Despite the advent of powerful pigment-targeting lasers, the
treatment for melasma remains challenging. In the United States alone, approximately 5
to 6 million individuals are afflicted with melasma of which majority are females (90-
95%). In Asia, it is a common diagnosis in any dermatology clinic and can reach an
incidence of 0.25% to 4% of cases seen in any dermatology institution. Melasma should
not be dismissed as simply a cosmetic entity because it often evokes emotional distress.
Additionally, stigma may be associated with melasma, particularly in Asian cultures.
Hence there is need for its extensive study.
Definition
Melasma is a chronic acquired cutaneous hypermelanosis which is classically
characterized by symmetric facial hyperpigmented macules and patches commonly
affecting the forehead, malar eminences, periorbital areas, and the upper lip.
Synonyms
Melasma, Chloasma (derived from the Greek cloazein, meaning greenish), Mask of
Pregnancy.
90
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Incidence
Melasma is much more commonly seen in women, although men can also be affected
(reported 10%), suggesting a hormone-related etiology.
This strong linkage between melasma and hormones is demonstrated by an increased
incidence in the onset of pregnancy, and is termed as chloasma, or “the mask of
pregnancy.”
In addition, the use of birthcontrol pills or estrogen replacement therapy, ovarian or
thyroid dysfunction, and ovarian tumors has also been associated with the onset of
melasma.
Although all skin types can be affected, melasma is seen at a much higher incidence
in darker skin phototypes (Fitzpatrick Skin Phototypes IV to VI) with extensive
ultraviolet radiation (UV) exposure.
Medications and other systemic illnesses have also been reported to be associated
with the onset of melasma, including phototoxic and photoallergic medications,
antiepileptic medications, cosmetics, altered nutrition, and hepatic disease.
Pathophysiology
Although the exact cause of melasma is unknown, it is strongly associated with 6 factors:
Hormonal influences,
Ultraviolet (UV) radiation,
Genetic predisposition
Immunology
Use of Cosmetics and
Use of Medication
91
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Hormonal Influences
Melasma occurs commonly during pregnancy, with data suggesting an incidence of
50–70% in pregnant women.
It occurs frequently in women using oral contraceptives.
Women taking hormone-replacement therapy (HRT) that includes progestational
hormones may develop melasma.
Menopausal and postmenopausal women receiving HRT were found to have lesions
on the forearms.
It may be triggered by nutritional supplements, especially those that have estrogen-
and progesterone-like properties.
Although progesterone, estrogen, melanocyte-stimulating hormone (MSH), and
luteinizing hormone have been implicated as a trigger of melasma, levels have not
been consistently elevated in these patients.
Ultraviolet Radiation
Exposure to UV radiation is believed to be the leading factor in the development of
melasma. Supporting this observation is the predominance of melasma is observed in
geographic areas with high levels of UV light.
Patients whose melasma has improved or nearly resolved may relapse completely or
develop darkening of existing lesions from one episode of UV exposure (minimum 5-
15min).
Melasma lesions tend to improve or fade during winter months with less UV
exposure. It is well known that skin darkening is a result of UVA exposure and to a
lesser extent UVB, which trigger increased melanocyte activity and melanogenesis.

92
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Genetic Predisposition
The common occurrence of melasma in families (ie 54% of the patients have a family
history of melasma) supports a hereditary component to this disorder.
It has been suggested that the increase in pigmentation following exposure to UV
radiation is a consequence of DNA repair.
Immunology
Immunohistochemical findings suggest that a strong immunoreactivity to α-MSH on
skin with melasma is one of the leading factors in the genesis of this disease.
There are evidences of a strong expression of α-MSH antigen in the keratinocytes of
the skin affected with melasma, suggesting that α-MSH plays a key role in the
hyperpigmentation of skin with melasma.
Use of Cosmetics
Ingredients in cosmetics that were selectively implicated as causative factors for
dermal melanoses include certain fatty acids, photoactive contaminants of mineral
oils, petrolatum, beeswax, certain dyes, para-phenylenediamine, and perfume
ingredients.
Use of Medication
A wide variety of medications produce hyperpigmentation. These include metals such
as arsenic, iron, copper, bismuth, silver, gold, phototoxic and antiseizure drugs.
Clinical features
The primary lesions of melasma are
Bilateral,

93
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Symmetric,
Hyperpigmented macules and patches that may vary in colour from tan to blue-gray.
The colour variations are attributed to several factors, including the amounts of melanin
pigment produced, the size of the melanosomes, and the location of melanin and
melanophages within the epidermis and dermis.
Types
Melasma occurs most often on the upper lip, nose, cheeks, forehead, chin, mandible,
neck, chest, and forearm areas. Three patterns of facial melasma have been described:
1. Depending on the Site of the lesion
Centro- facial with lesions involving the cheeks, forehead, upper lip, nose, and chin.
This pattern was seen in the majority of patients (63%). Melasma on the upper lip
typicallyoccurs in women taking oral contraceptives.
Malar with lesions involving the cheeks and nose only, which is seen in 21% of
patients.
Mandibular with involvement of the ramus of the mandible, which is seen in 16%.
Less often, the perioral and mental areas are involved. 114
2. Depending on the natural history of lesions 115
Transient -The transient types disappear within 1 year of cessation of hormonal
stimuli like pregnancy or oral contraceptive pills.
Persistent types. -The persistent types continues to be present more than 1 year after
the hormonal stimulus is removed and is caused by the UV rays and other factors.

94
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Histopathology of Melasma
Histologically, increased melanin can be seen in the basal and suprabasal
keratinocytes (epidermal pigmentation) and in the dermis (dermal pigmentation).
With the use of a Wood‟s lamp and light microscopy, Sanchez and colleagues
classified melasma into three histopathologic categories with the following features
1. Epidermal type (70–90% of all melasma cases)
Location of pigmentation: Melanin deposition in the basal and suprabasal layers through
the stratum corneum.
Woods lamp - Pigment is intensified
2. Dermal type
Location of pigmentation: Melanin deposition within the superficial dermis and in the
middermis. Imparts a blue grey colour to the overlying skin
Woods lamp- Pigment is not intensified under Wood‟s lamp
3. Compound (mixed) type
Features of both epidermal and dermal types (recently reported at 24% of all cases).
4. Indeterminate: inapparent under Wood's light
A Slight variation in the clinical features of these 3 histological types has been observed.
They are as follows

95
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Table 34 :-Histological types of Melasma
Epidermal type Dermal type- Mixed Type
Well-defined border Ill-defined border Combination of light and
brown patches
Dark brown colour Light brown colour Partial improvement with
treatment
Appears more obvious
under black light
Unchanged under black
light
Responds well to treatment Responds poorly to
treatment
Ultrastructural Features of Melasma
Increased number of melanocytes, melanocyte activity, melanosome size,
melanosome formation, melanosome transfer
High percentage of melanosomes individually dispersed within the keratinocyte
Differential Diagnosis
Freckles: These are pigmented macules, usually with reddish tan, observed in
sunexposed area on the skin. Seen mostly in children scattered across their cheeks and
nose, and macules darken following exposure to ultraviolet light.
Solar lentigo: Patients with history of chronic sun exposure develop solar lentigines,
usually after puberty and after age of 40 years. These are called liver spots or old-age
spots.Lentigens are moderately dark brown and large. With irregular borders.They
occur on chronically sun exposed surfaces, on the face, and dorsum of hand.
Riehl’s melanosis: Histopathology demonstrates an inflammatory infiltrate at the
epidermal dermal junction. Favours sites of application of cosmetics causing contact
dermatitis especially cosmetics, May be reticulated, Brown–grey colour due to dermal

96
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
melanin deposits, Histologic features- vacuolar degeneration of basal layer and
lichenoid infiltrate in early lesions
Bilateral nevus of ota: This is a blue to gray-brown pigmented patch located on the
face, usually within the distribution of the ophthalmic and maxillary branches of the
trigeminal nerve. Discolouration may be limited to the zygomatic arch or forehead or
may cover half the face, Associated with ocular and mucosal melanosis.
Post inflammatory hyperpigmentation (PIH): Usually lacks the symmetric
component, and history reveals a preceding inflammatory or traumatic event such as
acne vulgaris or contact dermatitis.
Incontinentia pigmenti: May be associated with developmental defects of the eye,
skeletal system and central nervous system.
Hypermelanosis in Endocrinal disorders: such as Addison‟s diseases, Cushing‟s
syndrome, Hyperthyroidism etc.
Hypermelanosis in Systemic disorders: such as Chronic Infections, Systemic lupus
erythematosus, Renal failure, Hepatic failure etc.
Hypermelanosis due to Nutritional Deficiencies: such as in Vitamin A Deficiency,
Pellagra
Prognosis
The predominantly epidermal type of melasma responds better than the predominantly
dermal type. Melasma of pregnancy fades away within a few months of delivery.116

97
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Treatment
Melasma is a chronic, relapsing disorder that can be managed effectively but not
cured. Effective treatment of melasma often has a prolonged course, and the patient
must be aware of the “long-term commitment” necessary to achieve a successful
outcome.
The goals of melasma therapy are basically twofold: the removal of existing pigments
and the prevention of the formation of new pigments.
Melasma therapy is based on four mechanisms of action
o Minimizing UV exposure
o Minimizing contributing hormonal Influences
o Preventing melanin production
o Removing melanin
Minimizing UV Exposure
Sun Avoidance
Geographic location often places a patient at risk for UV exposure from ordinary
daily activities. Avoidance of peak times of UV exposure, especially between the
hours of 10 a.m. and 3 p.m. should be emphasized. Sunbathing and sporting activities
are contraindicated, as are without sun-protective clothing and hats.
Sun Protection
Broad-spectrum sunblock with UVA and UVB protection and a skin protection factor
(SPF) of 30 or higher is a critically important adjunct to first-line melasma therapy
makeup.

98
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Sun-protective clothing, especially broad-brimmed hats, high-collared shirts, and
sunglasses, add additional coverage for melasma patients.
Avoid Photosensitizers
Medications and supplements that have photosensitization characteristics should be
avoided
Some of the drugs which cause Photosensitivity include Acetominophen, Acyclovir,
Captopril, Chloroquine, Ibuprofen, Oral Contraceptive Pills, Doxycycline etc.
These induce Photosensitivity reactions that will trigger melasma and /or darken
existing lesions.
Minimizing Contributing Hormonal Influences
It is important to remove hormonal stimulus such as OCP‟s
Preventing Melanin Production & Removing Melanin
By Topical and Procedural therapies
Topical Therapy
Topical preparations of lightening agents for the treatment of melasma are numerous
and constitute first-line therapy either as monotherapy or as combination therapy.
A variety of topical agents are used to treat melasma.

99
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Table 35 :-Topical applications and their probable mode of action
Formulations Mode of action
Hydroquinone, Azelaic acid, Kojic
acid, Arbutin, licorice extracts,
mulberry, bearberry
These agents act as tyrosinase inhibitors, degrades
melanosomes and destroys melanocytes.
Nicotinic acid, Niacinamide, Soy,
Tretinion
It decreases the rate of transfer of melanosomes to
the keratinocytes.
Alphahydroxyacids,
Betahydroxyacids, tretinoin
These accelerate cell turnover in the epidermis,
Topical corticosteroids Suppresses melanin formation without destroying
the melanosomes.
Chemical peels such as Glycolic
acid, Salicylic acid, Trichloracetic
acid, Tretinoin
Keratinocyte removal.
Procedural Therapy
Melasma is a therapeutic challenge for a dermatologist. Since most patients with
melasma have both epidermal and dermal pigmentation. Topical therapy alone is often
insufficient to clear their melasma.
Chemical Peels-
The two most common peeling agents used in treating melasma are glycolic acid and
salicylic acid, but are to be used in lower concentrations for superficial peeling in order to
avoid risk of causing post inflammatory hyperpigmentation.

100
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Other procedures include
Microabrasion
Vitamin C Iontophoresis
Laserss
Intense Pulse light along with topical Therapy
Melasma and Nurition
Vitamins C and E have been reported to suppress the spread of UV-induced
hyperpigmentation.
Oral Consumption of Pomogranate extract, grape seed extract, Pycnogenol (Pine
bark extract ) are said to be effective and safe nutritional supplements for melasma
by virtue of suppressing melanocyte proliferation and melanin production by
tyrosinase in melanocytes117
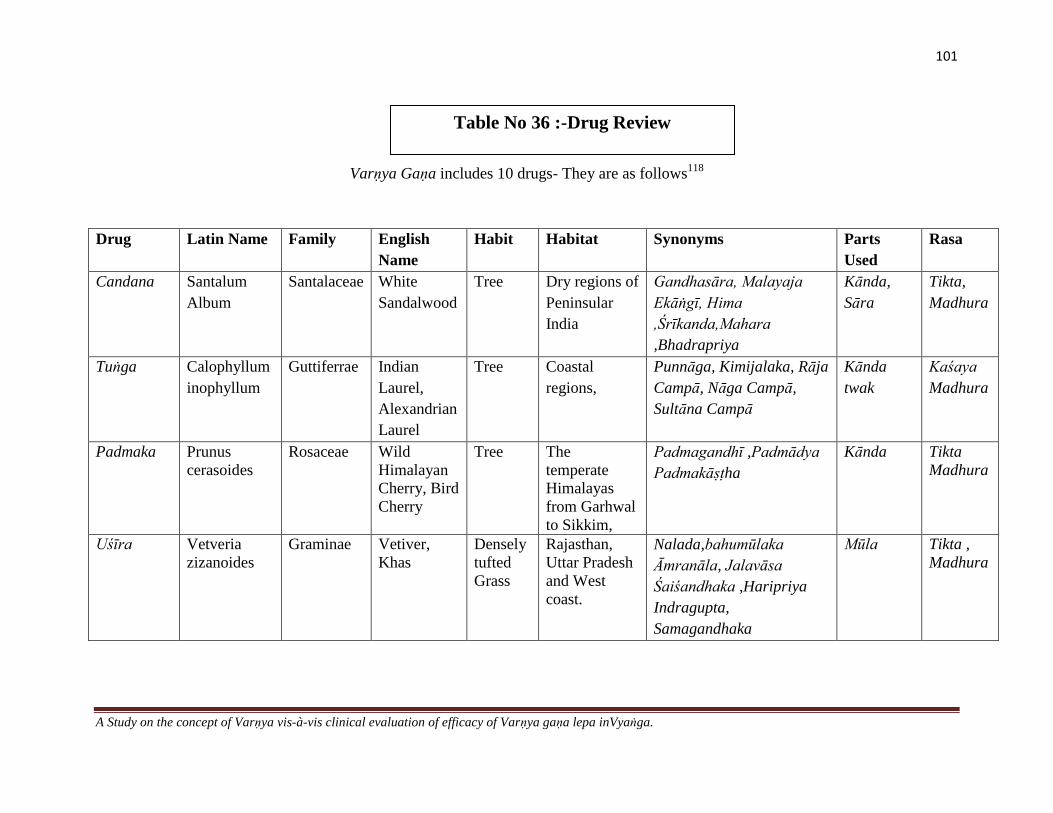
101
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Varṇya Gaṇa includes 10 drugs- They are as follows118
Drug Latin Name Family English
Name
Habit Habitat Synonyms Parts
Used
Rasa
Candana Santalum
Album
Santalaceae White
Sandalwood
Tree Dry regions of
Peninsular
India
Gandhasāra, Malayaja
Ekāṅgī, Hima
,Śrīkanda,Mahara
,Bhadrapriya
Kānda,
Sāra
Tikta,
Madhura
Tuṅga Calophyllum
inophyllum
Guttiferrae Indian
Laurel,
Alexandrian
Laurel
Tree Coastal
regions,
Punnāga, Kimijalaka, Rāja
Campā, Nāga Campā,
Sultāna Campā
Kānda
twak
Kaśaya
Madhura
Padmaka
Prunus
cerasoides
Rosaceae Wild
Himalayan
Cherry, Bird
Cherry
Tree
The
temperate
Himalayas
from Garhwal
to Sikkim,
Padmagandhī ,Padmādya
Padmakāṣṭha
Kānda Tikta
Madhura
Uśīra Vetveria
zizanoides
Graminae Vetiver,
Khas
Densely
tufted
Grass
Rajasthan,
Uttar Pradesh
and West
coast.
Nalada,bahumūlaka
Āmranāla, Jalavāsa
Śaiśandhaka ,Haripriya
Indragupta,
Samagandhaka
Mūla Tikta ,
Madhura
Table No 36 :-Drug Review

102
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Drug Latin Name Family English
Name
Habit Habitat Synonyms Parts
Used
Rasa
Madhūka Glycyrrhiza
glabra
Leguminac
eae
Licorice,
Liquorice
Herb/
Under
Shrub
Native to the
Mediterranean
regions.
Klītaka ,Madhuyaṣṭhī
,Jalayaṣṭhī, Madhūlika
Mūla Madhura
Mañjiṣṭhā Rubia
cordifolia
Rubiaceae Indian
Madder
Climber Throughout
India
Jinghinī ,Vastraranjinī
Vikāsa ,Raktāṅga
Mūla Madura
Tikta
Sāriva Hemidesmus
indicus
Asclepedia
ceae
Indian
Sarsaparilla
Semi-
erct
shrub
Bengal ,
Maharashtra
Anantā ,Anantamūla
Āsphoṭa, Gopī
Mūla Madhura
Tikta
Payasya Pureaeria
tuberosa
Leguminac
eae
Indian
kudze
Creeper Central India,
Punjab
Vidārī ,Svādugandhā
Ikṣugandhā ,Kandapalāśa
Kānda Madhura
Sitā Cynodon
dactylon
Poaceae Bermuda
Grass
Grass Throughout
India
Śataparva ,Dūrvā ,Anantā
Tiktaparvā
Pañchāṅg
a
Kaśaya
Madhura
Latā Cynodon
linearis
Poaceae Bermuda
Grass
Grass Throughout
India
Śataparva Dūrvā Anantā
Tiktaparvā
Pañchāṅg
a
Kaśaya
Madhura

103
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Drug Guṇa Vīrya Vipāka Karma Doṣaghnatā Chemical Composition
Candana Laghu,Rūkṣa Shīta Kaṭu Dāhapraśamana
Raktaprasādana
Kaphapittahara Santalol, Santene, Santalenes,
Santelenon, Teresantalol, Nor
Tricyclockasantalal, 1-santenone ,
Teresantalic acid.
Tuṅga Laghu,Rūkṣa Shīta Madhura Dāhapraśamana Kapha
pittahara
Friedelin, Sitosterol,
Canopylol,Callophylloids,
Inophyllid, Inophyllum A, B &D ,
Calophylin B
Padmaka Laghu,
Snigdha
Shīta Kaṭu Garbhasthāpana
Vedanāsthāpanā
Vṛṣya , Varṇya
Kaphapittahara Pudumin A, Genistein, Pruneitin,
Genkwanin, Cerasinone, Cerasidin,
Cerasin.
Uśīra Ruksha Laghu Shīta Kaṭu Pācana,
Stabhana
Kapha
Pittahara
Allokhusiol, Benzoic acid,
Epizizanol,Eudesmol, Eugenol,
Isokhusenoloxide, Isovalenic acid,
Khusimis acetate, Vanilin, zizanol.
Madhūka Guru Snigdha Shīta Madhura Pācana
Stambhana
Rasāyana Vṛṣya
Cakṣuṣya
Tridoṣahara Glycyrrhiza, Glycyrrhizic acid,
Liquertin, Glabrin, Licuraside,
Hispaglabradin, Glabrene.

104
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Drug Guṇa Vīrya Vipāka Karma Doṣaghnatā Chemical Composition
Mañjiṣṭhā Guru
Snigdha
Uṣṇa Kaṭu Svarya ,Varṇya Kapha pittahara Anti tumor cyclic hexapeptides,
Anthraquin,Munjistin,
Purpuroxantin, Rubiatriol,
Rubiofolic acid, Rubiadin,
Purpurin, Ruberythric acid.
Sāriva Guru
Snigdha
Shīta Madhura Grāhi ,Śukrala Tridoṣahara Hyperoside, Hexatriacontane,
Sitisterol, Hemidesminine
Payasya Guru
Snigdha
Shīta Madhura Balya ,Snehopaga
Bṛṁhaṇīya ,Varṇya
Kaṇṭhya
Vāta Pitta
Shāmaka
Purarin, Diadzein, Genestein,
Genistin
Tuberosin
Sitā Laghu Shīta Madhura Varṇya ,
Prajāsthāpana
Kapha pittahara Methoxy propionic acid,
Benzoic acid, Phytol, Sitosterol
Latā Laghu Shīta Madhura Varṇya
,Prajāsthāpana
Kaphapittahara Methoxy propionic acid,
Benzoic acid, Phytol, Sitosterol
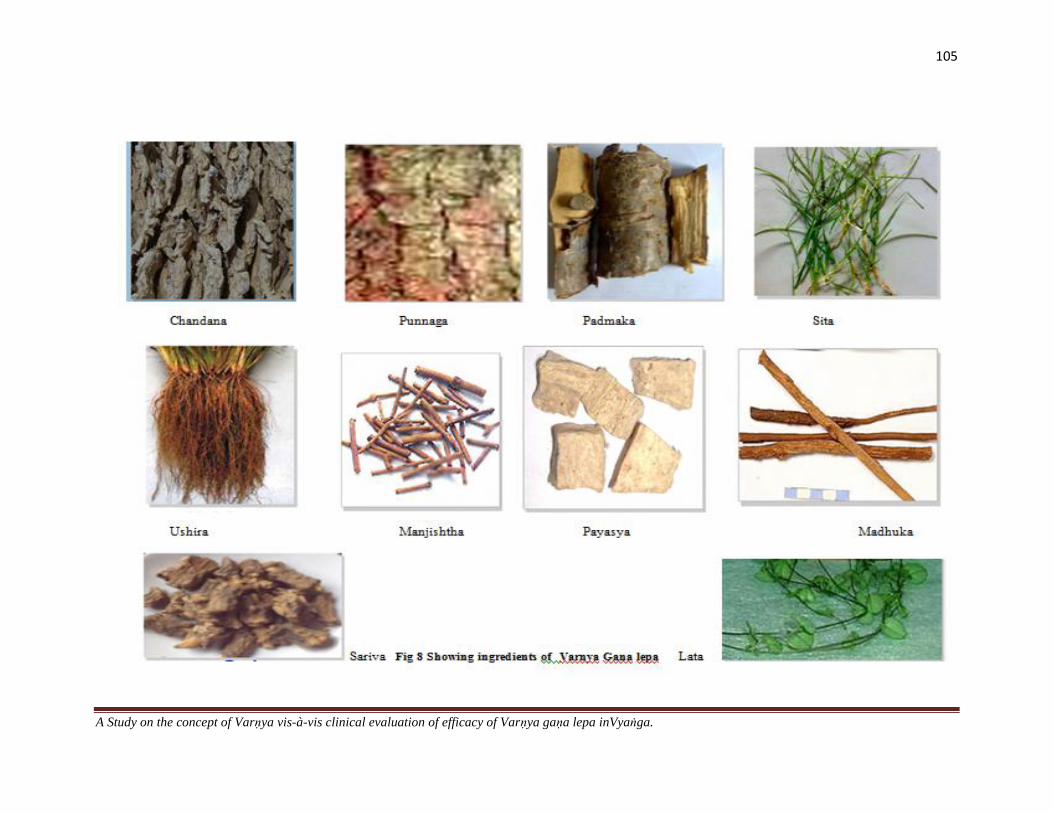
105
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
106
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
MATERIALS AND METHODS
MATERIALS
The materials used for the study can be categorized as follows
1. Literary
2. Drugs
3. Assessment tools (Instruments)
Collection of Materials
1. Literary Sources:- The primary sources of literature were different classical texts
books of Ayurveda, related information was compiled from other sources such as
Vedic and Upaniṣad scripts,. Information was also gathered from the texts books of
contemporary medical science, other allied texts. Other sources include various
journals, research works and retrospective studies carried out at different universities
and other research centers. Information available on internet was also incorporated.
Drugs:- Candana, Tuṅga, Padmaka, Uśīra, Madhūka, Mañjiṣṭhā, Sāriva, Payasya,
Sitā, Latā are the 10 drugs which were used in the form of lepa (ālepa) with water as
the media for the present study. The raw drugs were procured from Govind Raj
Shetty and Sons, Devraj Urs Road, Mysore, Abdul Ravoof Pansari Shop, Mandi
Mohalla, Mysore and Jogappa Shenoy Pansari Shop, Rathabeedi, Udupi

107
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa inVyaṅga.
Varnya Gana lepa Churna Luke warm water
Varnya Gana lepa
Figure No 9 ;- Varnya Gana lepa
Assessment tools (Instruments)
o Colour Grading Scale- Fair and lovely fairness meter was used to measure the Skin
Colour as well as the Lesion colour. It comprises of 26 grades of colour

108
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Fig No 10:-Fairness Meter
o Melasma Area Severity Index Scores- The Melasma Area and Severity Index
(MASI),was developed by Kimbrough-Green et al, based on a scoring system devised
for psoriasis .The MASI score is calculated by subjective assessment of 3 factors:
Area (A), Darkness (D), and Homogeneity (H) of involvement where in Forehead(f)
constitutes 30%, Right malar region (rm)- 30%, Left malar region (lm) 30% and
Chin (c)-10% .
Fig No 11:- Melasma Area Severity Index Scores

109
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
METHODOLOGY
1. Literary- Literary materials for the study were collected from different classics and
were analysed critically and comparatively with the help of tantra yuki.
2. Method to assess the Skin Colour and Lesion Colour through the Colour
Grading Scale.
The Colour Grading Scale has 26 grades. The number corresponding to the skin
colour of each patient was noted and in the same way, the number corresponding to
the lesion colour was noted before treatment. Lesion colour was assessed after the
intervention period and follow up period. The difference between the grades were
analysed to assess the improvement.
3. Method to assess the Area and Severity of Melasma through MASI Score
MASI Scoring System is used to assess 3 parameters .They are Area (A), Darkness
(D), and Homogeneity (H) of involvement. The MASI score is calculated by adding
the sum of the severity ratings for darkness and homogeneity, multiplied by the value
of the area of involvement, for each of the 4 facial areas [frontal (f), left malar(lm),
right malar(rm), chin(c)]: The following formula is used for calculation.
MASI total score =0.3A (f)[D(f)+H(f)]+ 0.3A (lm) [D(lm)+H(lm)] + 0.3A(rm)
[D(rm)+H(rm)] + 0.1A (c) [D(c)+H(c) ]. The total score range is 0 to 48. Higher the
score, higher is the severity.
4. Selction of the drugs
Varnya gaṇa mahakashaya dravyas are selected and administered in the form of lepa
(bahi parimārjana cikitsā)

110
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
5. Method of Preparation of Lepa
The raw drugs were procured from the source. They were cleaned and fine powder of
all the 10 drugs was prepared using a pulveriser. Patient was advised to add sufficient
quantity of luke warm water to the powder (lepa chūrna) and a thick paste was
prepared out of it.
6. Method of Application
Patients were advised to apply lepa from medial to lateral direction (opposite to the
direction of hair follicles) in a sufficient quantity, so as to cover the affected areas
(moderate thickness) effectively. Patients were advised to apply freshly prepared
lepa, not to apply over the previous lepa, & not to apply at night times.Patients were
instructed to apply lepa twice daily (morning and evening).They were advised to
wash the face with luke warm water once the lepa gets dried (after about 15-20 min).
They were instructed not to go to sun during the period of treatment.cxix
METHODS
Aim
To analyze the concept of Varṇya by evaluating the efficacy of Varṇya Gaṇa Lepa in
Vyaṅga.
Objectives
1. To systematically compile and review the literature on the concept of Varṇa , Varṇya,
and Vyaṅga
2. To clinically evaluate the efficacy of Carakokta Varṇya Gaṇa Lepa in Vyaṅga

111
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Source of Data
Sample
40 Patients irrespective of sex, caste, religion, and socio-economic status who were
diagnosed to have Vyaṅga were selected from the O.P.D and I.P.D of GAMC Hospital
Mysore and registered for the study. Out of 40 patients, 5 were drop outs and 35 patients
continued with the study.
Diagnostic Criteria
Objective Parameters
1. Syāma
2. Maṇḍala
3. Tanu
Inclusion Criteria
1. Patients with clinical signs of the disease Vyaṅga as per ayurvedic classics were
included.
2. Patients between age group 16-60years were selected for the study
3. Patients irrespective of sex, religion, occupation and chronicity were selected for the
study.
Exclusion Criteria
1. Hyperpigmentation caused due to any systemic diseases like Addison‟s disease,
Cushing Syndrome and SLE.
2. Hyperpigmentation since birth like Neavus.
3. Hyperpigmentation caused by tumors like malignant melanoma.
112
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Sampling Method
Sampling Method was the simple random sampling technique.
3. Research Design
1. A Literary study of Ayurvedic literature on Varṇa, Varṇya, and Vyaṅga with current
updated view (western medicine) was undertaken.
2. The study design was a Clinical –Interventional Study with a pre , post and follow up
assessment.
3. Patients were selected incidentally and 35 patients were assigned to a single group
Intervention
1. Initially the patient was advised to clean the face with luke warm water.
2. Varṇya Gaṇa Lepa was given for application on the affected areas.
3. It was advised that Quantity and thickness of Lepa was sufficient enough to cover the
lesion completely.
4. Duration of Each Application -Until the Lepa gets dried and once it dries the patient
was asked to wash the face with warm water.
5. Intervention period- For 15 days twice daily
6. Post test assessment-After 15 days
Assessment Criteria
The improvrment provided by the therapy was assessed on the basis of following
parameters:-

113
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Objective criteria
Skin /Lesion Colour
Texture (Dry/Oily)
Skin lustre
Number of Lesions
Size of Lesions
Darkness of the lesion
Area of involvement
Homogeneity of the lesion
Subjective criteria
Itching
Burning Sensation
Assessment Variables
The assessment of Clinical improvement was based on the assessment of individual
parameters which were framed as follows
Grading for the Objective Variables
1. Colour
Colour of Skin and lesion are graded with the help of Fair and Lovely Colour
Grading Scale .There are 1-26 grades
2. Texture- Dry Skin
Absent 0
Mild Dryness (Not seen but felt) 1

114
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Moderate Dryness (Stretching of the skin that a person feels) 2
Severe dryness (Visible dryness chapping of skin (hardness of Skin) 3
Oily skin
Absent 0
Mild oiliness(Not seen with naked eye) 1
Oiliness felt by touch (No need to wash face frequently
only 1-2 times)
Moderate oiliness (Oiliness is visible on skin, 2
Need to wash face frequently)
Severe Oiliness (Excessive Oiliness, Formation of Acne 3
Need to wash face more frequently)
3. Skin Lustre
Poor Lustre 1
Mild Lustre 2
Moderate Lustre 3
Good Radiant Lustre 4
4. Number of Lesions
1-2 1
2-4 2
4-6 3
>6 4

115
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
5. Size of the lesions
0-2cm 1
2-4cm 2
4-6cm 3
>6cm 4
When lesions or patches are multiple, the size of the largest lesion is taken into
consideration
6. MASI Score – To assess Area of Involvement, Darkness and Homogeneity of the
lesions
Table 37 :-Grades of MASI Score
The area of involvement Darkness Homogeneity
0 = no involvement; 0 = absent 0 = absent
1 =10% 1 = slight 1 = slight
2 = 10%-29% 2 = mild 2 = mild
3 =30%-49% 3 =marked 3 =marked
4 = 50%-69% 4 = maximum 4 = maximum
5 = 70%-89%
6 = 90%- 100%.

116
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Subjective variables
1. Itching
No itching 0
Mild Itching (Occasional itching, does not disturb routine) 1
Moderate itching (Frequent itching, disturbs routine activity but not sleep)- 2
Severe itching (Disturbs both routine and sleep) 3
2. Burning Sensation
No Burning 0
Mild Burning (Occasional Burning Sensation mostly when exposed to sun)- 1
Moderate Burning (Frequent Burning which increases when exposed to sun ) 2
Severe Burning (Continous Burning without sun exposure) 3
Assessment on Clinical Improvement
Overall assessment was done on the basis of following criteria.
CD- Clinically deteriorated ie increase in severity score against initial score
CS- Clinically Stable- Severity of Score remains same as against initial score
CI-1- Clinical improvement -Mild- 1 grade reduction against initial score
CI-2 – Clinical improvement Moderate -2 grade reduction against initial score
CI-3- Clinical improvement Good- 3 grade reduction against initial score
Statisical Analysis
The results of the present study will be analyzed statistically using Descriptive Statistics,
Frequencies and Percentages, Cross tabulation (Contingency Table Analysis), Chi-Square
test, Repeated measure ANOVA using SPSS for windows (version 16.0 ).

117
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
OBSERVATIONS AND RESULTS
OBSERVATIONS
The study registered 40 patients out of which 5 were drop outs and 35 continued with the
study. Observations of the patients are tabulated below.
Table 38 :-Age group incidence
Age in years Frequency Percent P. Value
21-30 9 25.7 0.122
31-40 14 40
41-50 8 22.9
51-60 4 11.4
Total 35 100.0
Out of 35 patients 14 patients (40%) were from the age group 31-40 yrs, 9 patients
( 25.7%) were from the age group 21-30 yrs, 8 patients (22.9%) were from the age group
41-50 yrs and only 4 patients (11.4%) were from the age group 51-60 yrs
Table 39 :-Sex wise distribution
Sex Frequency Percent P.Value
Male 4 11.4 0.000
Female 31 88.6
Total 35 100.0
Out of 35 patients 31 patients (88.6%) were females and only 4 patients (11.4%) were
males

118
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Table 40 :-Religion wise distribution
Religion Frequency Percent P.Value
Hindu 30 85.7 0.000
Muslim 4 11.4
Christian 1 2.9
Total 35 100.0
Out of 35 patients 30 patients (85.7%) were Hindus, 4 patients (11.4%) were Muslims
and only 1 patient (2.9%) was a Christian
Table 41:- Educational Status wise distribution
Educational Status Frequency Percent P.Value
Primary School 4 11.4 0.001
Middle School 6 17.1
High School 17 48.6
Graduate 4 11.4
Post Graduate 4 11.4
Total 35 100.0
Out of 35 patients 17 patients (48.6%) were educated upto high school, 6 patients
(17.1%) middle school and 4 patients (11.4%) each upto primary school, Graduation and
Post Graduation.
Table 42 :-Marital Status wise distribution
Marital Status Frequency Percent P.Value
Married 33 94.3
0.000 Un married 2 5.7
Total 35 100.0
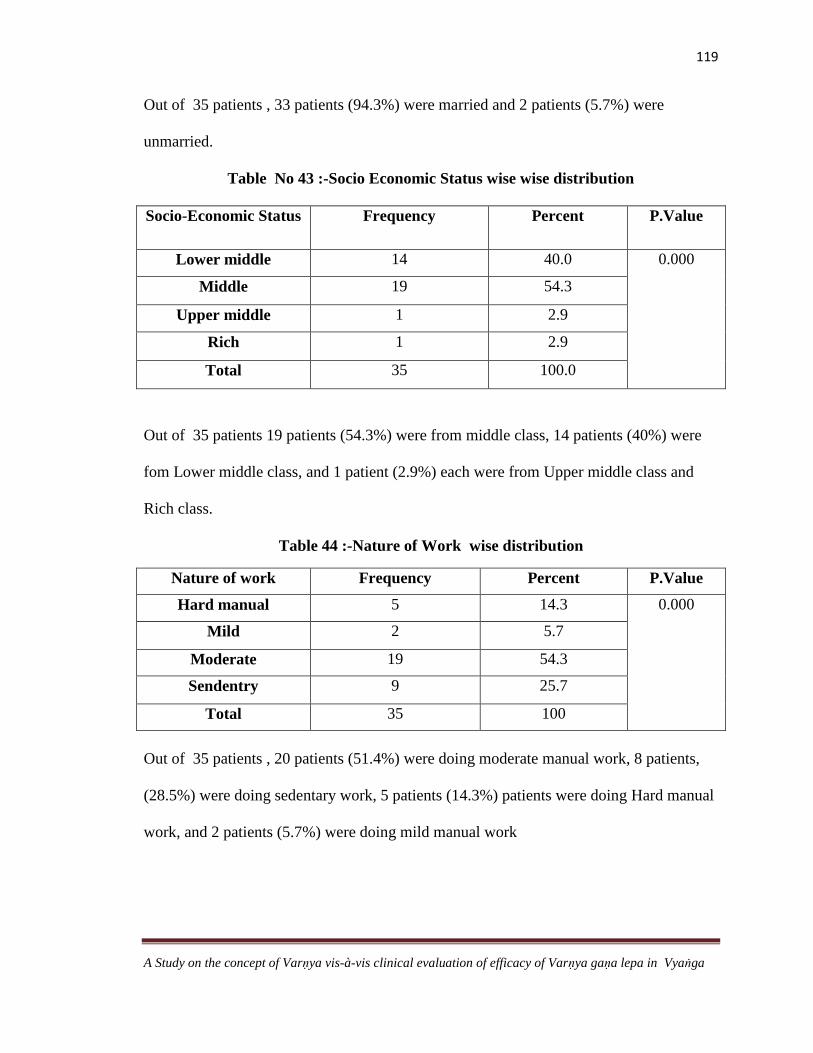
119
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Out of 35 patients , 33 patients (94.3%) were married and 2 patients (5.7%) were
unmarried.
Table No 43 :-Socio Economic Status wise wise distribution
Socio-Economic Status Frequency Percent P.Value
Lower middle 14 40.0 0.000
Middle 19 54.3
Upper middle 1 2.9
Rich 1 2.9
Total 35 100.0
Out of 35 patients 19 patients (54.3%) were from middle class, 14 patients (40%) were
fom Lower middle class, and 1 patient (2.9%) each were from Upper middle class and
Rich class.
Table 44 :-Nature of Work wise distribution
Nature of work Frequency Percent P.Value
Hard manual 5 14.3 0.000
Mild 2 5.7
Moderate 19 54.3
Sendentry 9 25.7
Total 35 100
Out of 35 patients , 20 patients (51.4%) were doing moderate manual work, 8 patients,
(28.5%) were doing sedentary work, 5 patients (14.3%) patients were doing Hard manual
work, and 2 patients (5.7%) were doing mild manual work
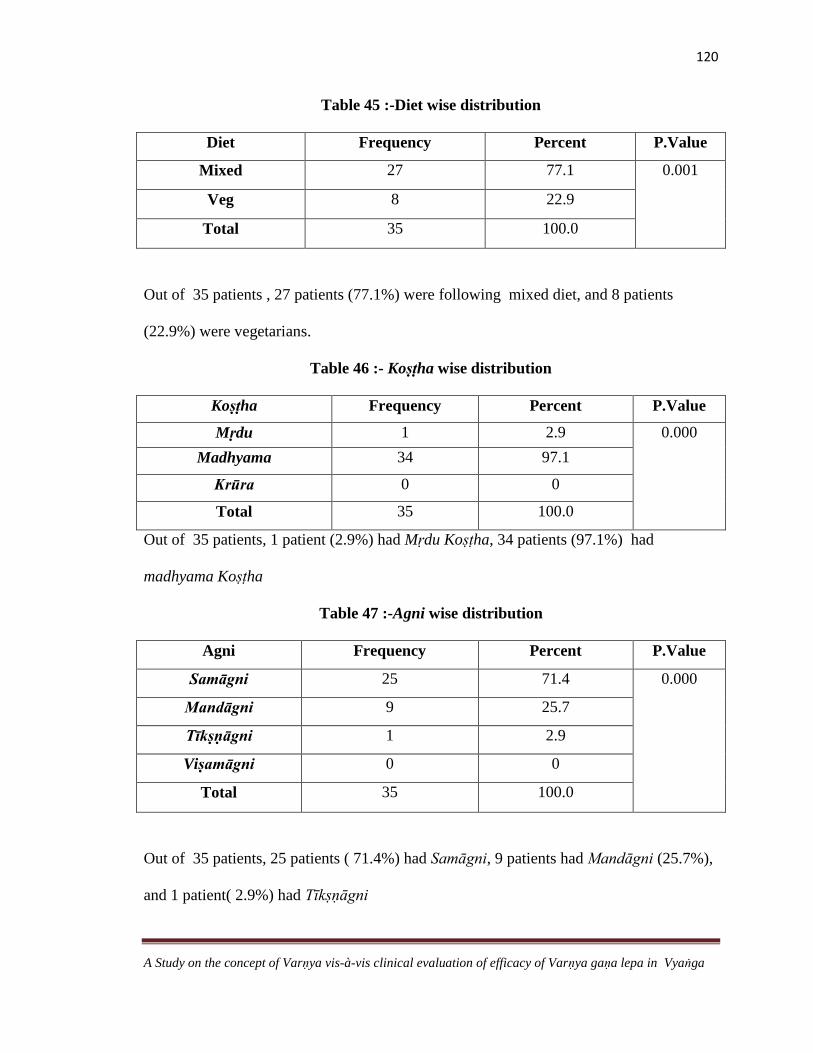
120
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Table 45 :-Diet wise distribution
Diet Frequency Percent P.Value
Mixed 27 77.1 0.001
Veg 8 22.9
Total 35 100.0
Out of 35 patients , 27 patients (77.1%) were following mixed diet, and 8 patients
(22.9%) were vegetarians.
Table 46 :- Koṣṭha wise distribution
Koṣṭha Frequency Percent P.Value
Mṛdu 1 2.9 0.000
Madhyama 34 97.1
Krūra 0 0
Total 35 100.0
Out of 35 patients, 1 patient (2.9%) had Mṛdu Koṣṭha, 34 patients (97.1%) had
madhyama Koṣṭha
Table 47 :-Agni wise distribution
Agni Frequency Percent P.Value
Samāgni 25 71.4 0.000
Mandāgni 9 25.7
Tīkṣṇāgni 1 2.9
Viṣamāgni 0 0
Total 35 100.0
Out of 35 patients, 25 patients ( 71.4%) had Samāgni, 9 patients had Mandāgni (25.7%),
and 1 patient( 2.9%) had Tīkṣṇāgni

121
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Table 48 :-Appetite wise distribution
Appetite Frequency Percent P.Value
Poor 4 11.4 0.000
Moderate 5 14.3
Good 25 71.4
Extreme 1 2.9
Total 35 100.0
Out of 35 patients, 25 patients (71.4%) had Good Appetite, 5 patients (14.3%) had
moderate appetite, 4 patients (11.4%) had Poor Appetite, and 1 patient (2.9%) had
extreme appetite.
Table 49:- Sleep wise distribution
Sleep Frequency Percent P.Value
Satisfactory 23 65.7 0.063
Unsatisfactory 12 34.3
Total 35 100.0
Out of 35 patients, 23 patients (65.7%) had Satisfactory Sleep and 12 patients (34.3%)
had unsatisfactory sleep
Table 50:- Bowel Habits wise distribution
Bowel Habits Frequency Percent P.Value
Regular 27 77.1 0.001
Irregular 8 22.9
Total 35 100.0
Out of 35 patients, 27 patients (77.1%) had Regular Bowel Habits, 8 patients (22.9%) had
Irregular Bowel Habits.

122
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Table 51:- Family History wise distribution
Family History Frequency Percent P.Value
Present 15 42.9 0.398
Absent 20 57.1
Total 35 100.0
Out of 35 patients, 20 patients (57.1%) had no Family History of vyaṅga, and 15 patients
(42.9%) had a Family History of vyaṅga
Table 52:- Contraceptive History wise distribution
Contraceptive History Frequency Percent P.Value
Present 3 8.6 0.000
Absent 28 80.0
Not Applicable 4 11.4
Total 35 100.0
Out of 35 patients, 28 patients (80%) had no Contraceptive History and 3 patients (8.6%)
had a positive Contraceptive History
Table 53 :-Physical Aggravating Factors wise distribution
Physical Agg.Factors Frequency Percent P.Value
Sun rays 16 45.7 0.000
Excessive work 2 5.7
Multiple AF 2 5.7
Nothing specific 15 42.9
Total 35 100.0
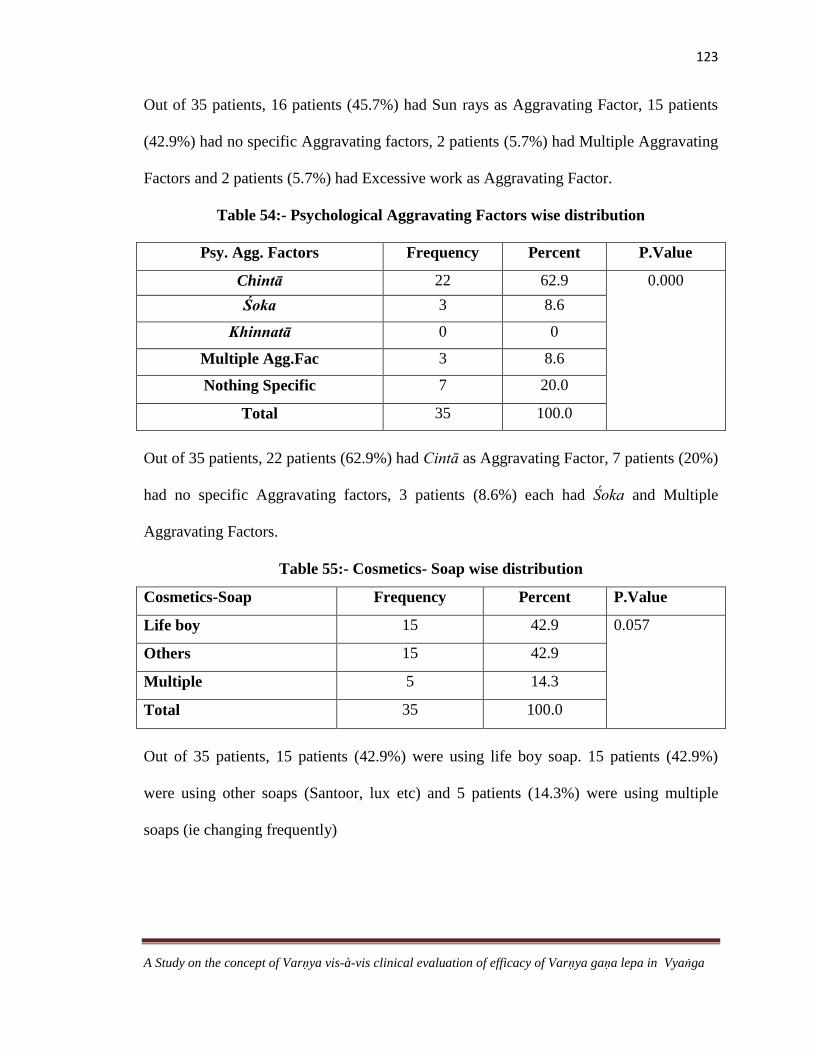
123
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Out of 35 patients, 16 patients (45.7%) had Sun rays as Aggravating Factor, 15 patients
(42.9%) had no specific Aggravating factors, 2 patients (5.7%) had Multiple Aggravating
Factors and 2 patients (5.7%) had Excessive work as Aggravating Factor.
Table 54:- Psychological Aggravating Factors wise distribution
Psy. Agg. Factors Frequency Percent P.Value
Chintā 22 62.9 0.000
Śoka 3 8.6
Khinnatā 0 0
Multiple Agg.Fac 3 8.6
Nothing Specific 7 20.0
Total 35 100.0
Out of 35 patients, 22 patients (62.9%) had Cintā as Aggravating Factor, 7 patients (20%)
had no specific Aggravating factors, 3 patients (8.6%) each had Śoka and Multiple
Aggravating Factors.
Table 55:- Cosmetics- Soap wise distribution
Cosmetics-Soap Frequency Percent P.Value
Life boy 15 42.9 0.057
Others 15 42.9
Multiple 5 14.3
Total 35 100.0
Out of 35 patients, 15 patients (42.9%) were using life boy soap. 15 patients (42.9%)
were using other soaps (Santoor, lux etc) and 5 patients (14.3%) were using multiple
soaps (ie changing frequently)

124
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Table 56 :-Cosmetics- Cream wise distribution
Cream Frequency Percent P.Value
Fair & lovely 22 62.9 0.000
Others 6 17.1
Multiple 5 14.3
Does not use 2 5.7
Total 35 100.0
Out of 35 patients, 22 patients (62.9%) were using Fair and Lovely, 6 patients (17.1%)
were using other creams (vico turmeric, everyuth etc ), 5 patients (14.3%) were using
multiple creams ( ie changing frequently ) and 2 patients ( 5.7%) were not using any
creams.
Table 57:- Menstrual History wise distribution
Menstrual History Frequency Percent P.Value
Regular 19 54.3 0.015
Irregular 5 14.3
Not applicapable 11 31.4
Total 35 100.0
Out of 35 patients, 19 patients (54.3%) had regular menses, 5 patients ( 14.3%) had
irregular menses and for 11 patients ( 31.4%) it was not applicable (males , those who
underwent Hysterectomy and post menopausal women )
Table 58 :-Age of Menopause wise distribution
Age of Menopause Frequency Percent P.Value
Attained 7 20.0 0.000
Not attained 23 65.7
Not Applicable 5 14.3
Total 35 100.0

125
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Out of 35 patients, 23 patients (65.7%) had not attained menopause, 7 patients (20%) nad
attained menopause and for 5 patients (14.3% ) it was not applicable (males and women
who underwent Hysterectomy)
Table 59 :- Prakṛti wise distribution
Prakṛti Frequency Percent P.Value
Vpk 11 31.4 0.114
Pvk 17 48.6
Kpv 7 20.0
Total 35 100
Out of 35 patients, 17 patients (48.6%) were of Pitta prakṛti, 11 patients (31.4%)
were of Vāta prakṛti and 7 patients (20%) were of kapha prakṛti.
Table 60-Showing Sattva wise distribution
Sattva Frequency Percent P.Value
Pravara 14 40.0 0.000
Madhyma 20 57.1
Avara 1 2.9
Total 35 100.0
Out of 35 patients, 20 patients (57.1%) had Madhyama Sattva and 14 patients
(40%) had Pravara sattva and 1 patient (2.9%) had Avara Sattva.
Table 61 :- Sāra wise distribution
Sāra Frequency Percent P.Value
Pravara 5 14.3 0.000
Madhyma 30 85.7
Avara 0 0
Total 35 100.0

126
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Out of 35 patients, 30 patients (85.7%) had Madhyama Sattva and 5 patients (14.3%)
had Pravara Sattva
Table 62 :-Pattern wise distribution
Pattern Frequency Percent P.Value
Centro facial 15 42.9 0.398
Malar 20 57.1
Mandibular 0 0
Total 35 100.0
Out of 35 patients, 20 patients (57.1%) had malar pattern and 15 patients (42.9%)
had Centro facial pattern.
Table 63 :-Level of Lesion wise distribution
Level of Lesion Frequency Percent P.Value
Dermal 21 60.0 0.237
Epidermal 14 40.0
Total 35 100.0
Out of 35 patients, 21 patients (60%) had Dermal Melasma and 14 patients (40%)
had epidermal melasma.
Table 64 :-Chronicity wise distribution
Chronicity Frequency Percent P.Value
0-4yrs 22 62.9 0.001
4-8yrs 7 20.0
>8 yrs 6 17.1
Total 35 100.0

127
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Out of 35 patients, Chronicity of 22 patients (62.9%) was between 0-4 yrs, 7
patients ( 20%) was between 4-8 yrs and 6 patients ( 17%) was more than 8 yrs.
Table 65 :-Skin colour wise distribution
Skin colour Frequency Percent P Value
1-5 3 8.6 0.000
6-10 17 48.6
11-15 13 37.1
15-20 2 5.7
Total 35 100.0
Out of 35 patients, skin colour of 3 patients (8.6%) was between 1-5 grade, Skin
colour of 17 patients (48.6%) was between 6-10grade, Skin colour of 13 patients (37.1%)
was between 11-15grade and skin colour of 2 patients (5.7%) was between 15-20 grade.
Table 66 :-Distribution of Chronicity vs level of the lesion
Chronicity Level Total P. Value
Dermal Epidermal 0.294
0-4yrs 12 10 22
57.1% 71.4% 62.9%
4-8yrs 6 1 7
28.6% 7.1% 20.0%
>8 yrs 3 3 6
14.3% 21.4% 17.1%
Total 21 14 35
100.0% 100.0% 100.0%
Out of 35 patients, among the 22 patients whose chronicity was between 0-4yrs, 12
patients (57.1%) had dermal type of melasma, 10 patients (71.4%) had epidermal type,
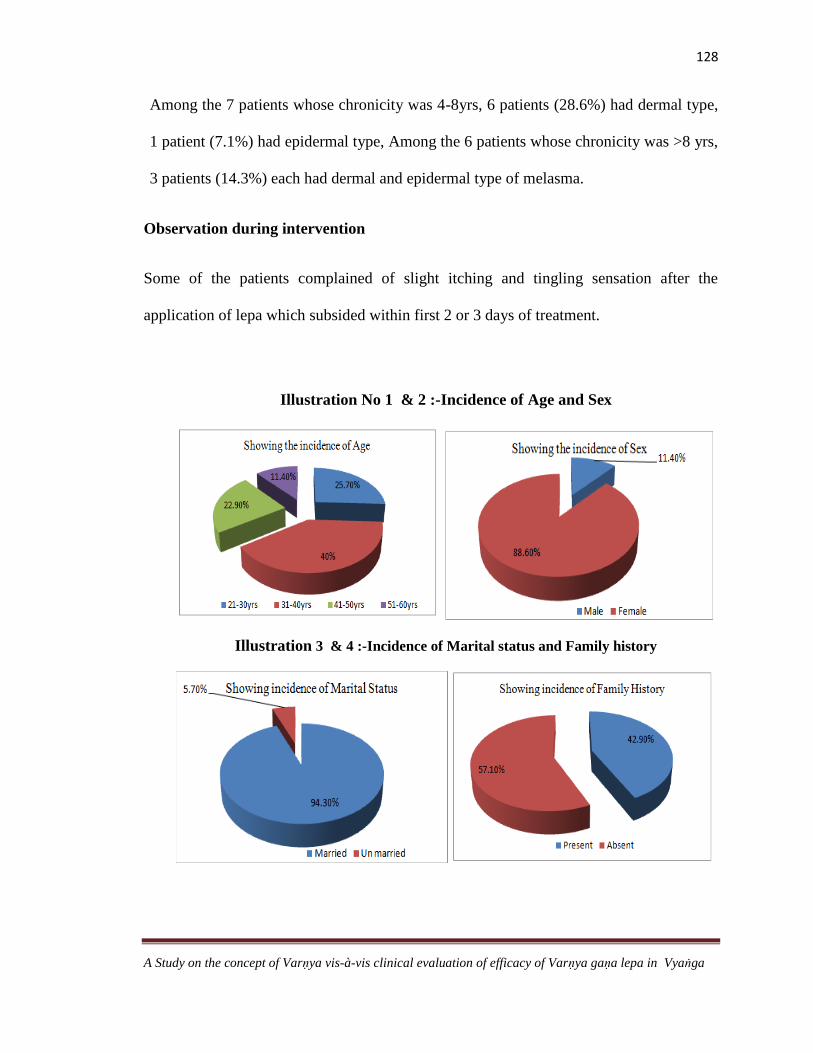
128
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Among the 7 patients whose chronicity was 4-8yrs, 6 patients (28.6%) had dermal type,
1 patient (7.1%) had epidermal type, Among the 6 patients whose chronicity was >8 yrs,
3 patients (14.3%) each had dermal and epidermal type of melasma.
Observation during intervention
Some of the patients complained of slight itching and tingling sensation after the
application of lepa which subsided within first 2 or 3 days of treatment.
Illustration No 1 & 2 :-Incidence of Age and Sex
Illustration 3 & 4 :-Incidence of Marital status and Family history

129
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Illustration No 5 & 6 :-Incidence of Contraceptive history &Physical Aggravating
factors
Illustration No 7 & 8 :-Incidence of Psychological Aggravating factors & use of Soaps
Illustration No 9 & 10 :-Incidence of Menstual history and age of menopause

130
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Illustration No 11 & 12 :-Incidence of prakṛti and Pattern of lesion
Illustration No 13 & 14 :-Incidence of Level of lesion and chronicity
Illustration No15 :-Distribution of skin colour

131
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Illustration No 16 :-Distribution of Chronicity vs level of lesion.
Figure No 12:- Patients with melasma before and after treatment

132
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
RESULTS
Table 67 :-Distribution of Skin Colour Vs Lesion Colour
Skin Colour Mean Std. Deviation N
Lesion
Colour
BT
1-5 22.3333 2.08167 3
6-10 20.5294 4.37489 17
11-15 22.7692 2.20431 13
16-20 24.5000 2.12132 2
Total 21.7429 3.56736 35
Lesion
Colour
AT
1-5 19.6667 2.08167 3
6-10 16.7059 4.11954 17
11-15 18.3077 1.70219 13
15-20 20.5000 .70711 2
Total 17.7714 3.27275 35
Lesion
Colour
FU
1-5 19.6667 2.08167 3
6-10 16.7059 4.11954 17
11-15 18.3077 1.70219 13
16-20 20.5000 .70711 2
Total 17.7714 3.27275 35
Colour P.Value
Only Lesion Colour 0.000
Lesion colour vs Skin colour 0.735
The total mean of the Lesion colour before treatment was 21.7429 , and it was 17.7714
after treatment and follow up.

133
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Table 68 :-Results of Darkness of Frontal region
Darkness-Frontal Region Total
Absent Slight Mild
Marked Maximum
BT 24 0 5 4 2 35
68.5% .0% 14.2% 11.4% 5.7% 100%
AT 24 1 6 3 1 35
68.5% 2.85% 17.14% 8.5% 2.85% 100%
FU 24 1 6 3 1 35
68.5% 2.85% 17.14% 8.5% 2.85% 100%
P Value-0.815
Out of 35 patients, 5 patients (14.2%) had mild darkness, 4 patients (11.4%) had marked
darkness, 2 patients (5.7%) had maximum darkness before treatment and 1 patient (2.85%) had
slight darkness, 6 patients (17.14%) had mild darkness, 3 patients (8.5%) had marked darkness
and1 patient (2.85%) had maximum darkness in the frontal region after treatment and after
follow up.
Table 69:- Results of Darkness of Chin region
Darkness-Chin Total
Absent Slight Mild
Marked
BT 29 3 2 1 35
82.8% 8.5% 5.7% 2.8% 100%
AT 29 5 1 0 35
82.8% 14.2% 2.8% 0% 100%
FU 29 5 1 0 35
82.8% 14.2% 2.8% 0% 100%
P Value-0.608
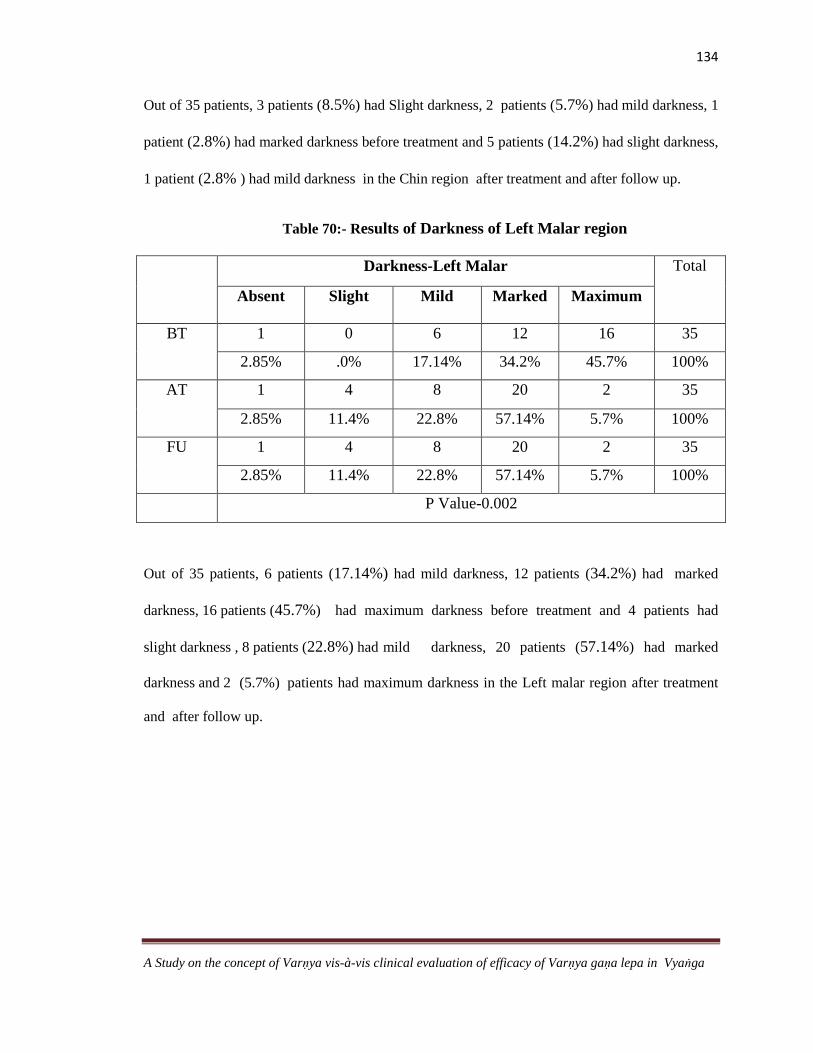
134
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Out of 35 patients, 3 patients (8.5%) had Slight darkness, 2 patients (5.7%) had mild darkness, 1
patient (2.8%) had marked darkness before treatment and 5 patients (14.2%) had slight darkness,
1 patient (2.8% ) had mild darkness in the Chin region after treatment and after follow up.
Table 70:- Results of Darkness of Left Malar region
Darkness-Left Malar Total
Absent Slight Mild
Marked Maximum
BT 1 0 6 12 16 35
2.85% .0% 17.14% 34.2% 45.7% 100%
AT 1 4 8 20 2 35
2.85% 11.4% 22.8% 57.14% 5.7% 100%
FU 1 4 8 20 2 35
2.85% 11.4% 22.8% 57.14% 5.7% 100%
P Value-0.002
Out of 35 patients, 6 patients (17.14%) had mild darkness, 12 patients (34.2%) had marked
darkness, 16 patients (45.7%) had maximum darkness before treatment and 4 patients had
slight darkness , 8 patients (22.8%) had mild darkness, 20 patients (57.14%) had marked
darkness and 2 (5.7%) patients had maximum darkness in the Left malar region after treatment
and after follow up.
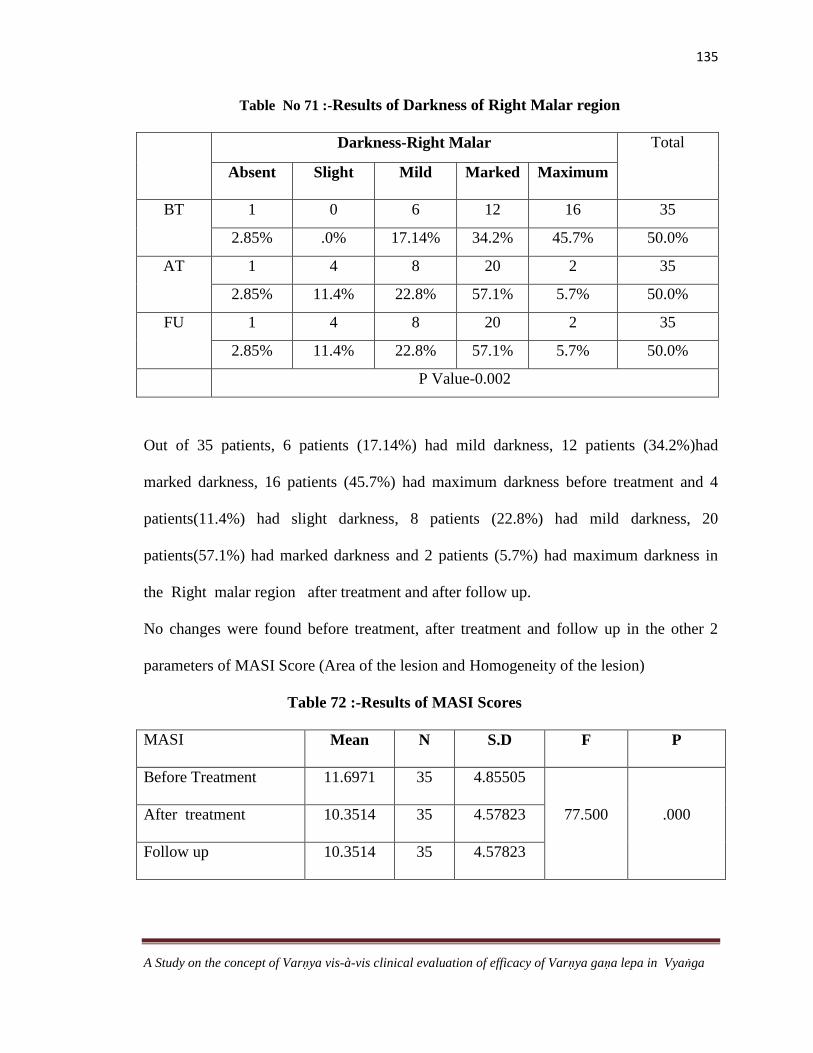
135
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Table No 71 :-Results of Darkness of Right Malar region
Darkness-Right Malar Total
Absent Slight Mild
Marked Maximum
BT 1 0 6 12 16 35
2.85% .0% 17.14% 34.2% 45.7% 50.0%
AT 1 4 8 20 2 35
2.85% 11.4% 22.8% 57.1% 5.7% 50.0%
FU 1 4 8 20 2 35
2.85% 11.4% 22.8% 57.1% 5.7% 50.0%
P Value-0.002
Out of 35 patients, 6 patients (17.14%) had mild darkness, 12 patients (34.2%)had
marked darkness, 16 patients (45.7%) had maximum darkness before treatment and 4
patients(11.4%) had slight darkness, 8 patients (22.8%) had mild darkness, 20
patients(57.1%) had marked darkness and 2 patients (5.7%) had maximum darkness in
the Right malar region after treatment and after follow up.
No changes were found before treatment, after treatment and follow up in the other 2
parameters of MASI Score (Area of the lesion and Homogeneity of the lesion)
Table 72 :-Results of MASI Scores
MASI Mean N S.D F P
Before Treatment 11.6971 35 4.85505
77.500 .000 After treatment 10.3514 35 4.57823
Follow up 10.3514 35 4.57823

136
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
The mean of MASI Scores of 35 patients, before treatment was 11.69 and after treatment
and follow up it reduced to 10.8314
Table 73:- Results of dryness and oilyness
D/O Dryness Oilyness
Mild Mod Sev Total Mild Mod Sev Total
BT 5 10 8 23 3 6 3 12
21.7% 43.5% 34.8% 100.0% 25.0% 50.0% 25.0% 100.0%
AT 11 10 2 23 8 4 0 12
47.8% 43.5% 8.7% 100.0% 66.7% 33.3% 0% 100.0%
FU 11 10 2 23 8 4 0 12
47.8% 43.5% 8.7% 100.0% 66.7% 33.3% 0% 100.0%
P value-0.070 P Value-0.056
Out of 35 patients, 5 patients(21.7%) had mild dryness, 3 patients(25.0%) had mild
oilyness, 10 patients (43.5%) had moderate dryness, 6 patients(50.0%) had moderate
oilyness, 8 patients (34.8%) had severe dryness and 3 patients had severe oilyness
(25.0%) before treatment. After treatment and follow up duration 11 patients (47.8%)
had mild dryness, 8 patients (66.7%) had mild oilyness, 10 patients (43.5%) had
moderate dryness 4 patients (33.3%) had moderate oilyness, 2 patients (8.7%) had severe
dryness, none had severe oilyness.
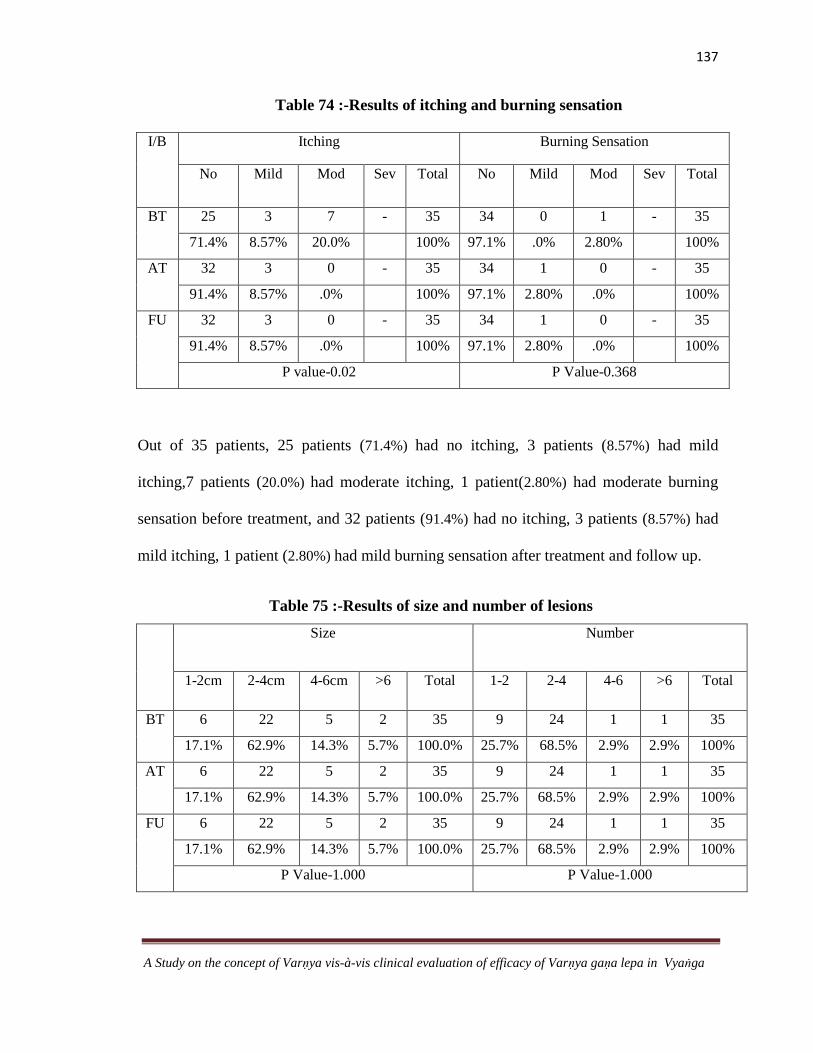
137
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Table 74 :-Results of itching and burning sensation
I/B Itching Burning Sensation
No Mild Mod Sev Total No Mild Mod Sev Total
BT 25 3 7 - 35 34 0 1 - 35
71.4% 8.57% 20.0% 100% 97.1% .0% 2.80% 100%
AT 32 3 0 - 35 34 1 0 - 35
91.4% 8.57% .0% 100% 97.1% 2.80% .0% 100%
FU 32 3 0 - 35 34 1 0 - 35
91.4% 8.57% .0% 100% 97.1% 2.80% .0% 100%
P value-0.02 P Value-0.368
Out of 35 patients, 25 patients (71.4%) had no itching, 3 patients (8.57%) had mild
itching,7 patients (20.0%) had moderate itching, 1 patient(2.80%) had moderate burning
sensation before treatment, and 32 patients (91.4%) had no itching, 3 patients (8.57%) had
mild itching, 1 patient (2.80%) had mild burning sensation after treatment and follow up.
Table 75 :-Results of size and number of lesions
Size Number
1-2cm 2-4cm 4-6cm >6 Total 1-2 2-4 4-6 >6 Total
BT 6 22 5 2 35 9 24 1 1 35
17.1% 62.9% 14.3% 5.7% 100.0% 25.7% 68.5% 2.9% 2.9% 100%
AT 6 22 5 2 35 9 24 1 1 35
17.1% 62.9% 14.3% 5.7% 100.0% 25.7% 68.5% 2.9% 2.9% 100%
FU 6 22 5 2 35 9 24 1 1 35
17.1% 62.9% 14.3% 5.7% 100.0% 25.7% 68.5% 2.9% 2.9% 100%
P Value-1.000 P Value-1.000

138
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
There was no change in the size and number of lesions before treatment, after treatment and after
follow up
Table 76 Results of Skin Lustre
Skin Lustre
Poor Mild Moderate Total
BT
15 18 2 35
42.9% 51.4% 5.7% 100.0%
AT
14 19 2 35
40.0% 54.3% 5.7% 100.0%
FU 15 18 2 35
42.9% 51.4% 5.7% 100.0%
P Value-0.999
Out of 35 patients, 15 patients(42.9%) had poor lustre, 18 patients (51.4%) had mild lustre
and 2 patients (5.7%)had moderate lustre before treatment and 14 patients (40.0%) had
poor lustre, 19 patients (54.3%) had mild lustre and 2 patients(5.7%) had moderate lustre
after treatment and follow up
Table 77:-The Assessment of Clinical improvement in all the parameters.
Criteria CD CS CI-1 CI-2 CI-3
Skin colour - - 51.4% 42.8% 5.7%
Skin Texture (Dryness) - 43.47% 56.5 - -
Oilyness - 33.3% 66.7% - -
Lustre - 97.14% 2.87% - -
No of Lesions - 100% - - -
Criteria CD CS CI-1 CI-2 CI-3

139
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Size of lesions - 100% - - -
Itching - - 60% 40% -
Burning - - 100% - -
MASI SCORE - - 100% - -
Area - 99.28% 0.7% - -
Darkness - 60.7% 39.3% - -
Homogeneity - 100% - - -
Table 79 :-Results of overall assessment
The overall assessment of the study reveals that 10 patients (28.9%) were said to be
clinically stable, 23 patients (64.34%) had mild improvement, 2 patients (6.7%) had
moderate improvement.
Clinical Improvement No of Patients Percentage P.Value
Clinically Deteriorated 0 0% 0.000
Clinically Stable 10 28.9%
Mild improvement 23 64.34%
Moderate improvement 2 6.7%
Good improvement 0 0%
Total 35 100%

140
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Illustration No 17 :-Distribution of Skin Colour Vs Lesion Colour
Illustration No 18 :- Darkness of Frontal region and Chin
0
5
10
15
20
25
1-5grade 6-10 grade 11-15grade 16-20grade
Mea
ns
Grades
Mean BT Mean AT Mean FU
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
BT AT FU BT AT FU
% o
f p
ati
ents
Darkness -Frontal region Darkness- Chin
Absent Sligt Mild Marked Maximum

141
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Illustration No 19 :-Darkness of Right Malar region and Left Malar region
Illustration No 20:- Means of MASI Scores
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
BT AT FU BT AT FU
% o
f p
ati
ents
Darkness- Right Malar region Darkness-Left Malar Region
Absent Sligt Mild Marked Maximum
9.5
10
10.5
11
11.5
12
Before Treatment After treatment Follow up
Mea
n M
AS
I v
alu
es
Duration of treatment

142
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Illustration No 21 :- Dryness and Oiliness Skin
Illustration No 22:- Itching and Burning Sensation
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
BT AT FU BT AT FU
% o
f p
ati
ents
Dryness Oilyness
Mild Moderate Severe
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
90.00%
100.00%
BT AT FU BT AT FU
% o
f p
ati
ents
Itching Burning sensation
Absent Mild Moderate

143
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Illustration No 23 :-Size of lesions
Illustration No 24 :- Number of lesions
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
BT AT FU
% o
f p
ati
ents
Duration of treatment
1-2cm 2-4cm 4-6cm >6cm
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
BT AT FU
% o
f p
ati
ents
Duration of Treatment
1-2n 2-4n 4-6n >6n

144
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
llustration No 25-Showing the Skin Lustre
Illustration No 26 :-Overall assessment of the study.
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
BT AT FU
% o
f p
ati
ents
Duration of Treatment
Poor Mild Moderate
0%
10%
20%
30%
40%
50%
60%
70%
Clinically Deteriorated
Clinally Stable Mild Imp Moderate Imp
Good Imp
% o
f P
ati
ents
Clinical improvement
% of Patients

145
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
DISCUSSION
Discussion is the platform to analyze the concept appropriately, to unveil the rationality
behind facts and finally to successfully accomplish the conceptualization. In this section
both conceptual study and clinical trial will be discussed.
Title
Skin is one of the important ways of expression of beauty. Complexion is the
manifest form of beauty .A fair complexion is a desirable component and indigenous
criterion for beauty since decades. In the present era it is the most decisive and the most
abused of all the attributes of mankind. It determines the social perceptions, value
judgements and interpersonal relationships and it can wreak havoc on individual‟s sense
of dignity and self esteem. Complexion and Colour in Āyurveda is referred to as Varṇa. It
represents all the parameters of healthy and radiant skin. From a physiological
perspective it is a barometer of an individual‟s health as it reflects the equilibrium of the
body entities.
The task of enhancement of Varṇa (or bringing back the abnormal colour
to normalcy or to improve the existing complexion) is termed as Varṇya .Various
treatment modalities such as Anu Lepana, Nasya, Virecana etc are said to be Varṇya. In
this era of aesthetics, it is the need of the hour to fulfill the cosmetic demand of people.
Āyurveda has its own detail and deeper sense regarding the subject but all the literature
concerned with Varṇa and Varṇya is scattered throughout and very minimum research
works have been done till date with this theme. So an attempt is made in this study to
analyse the relevant literature.

146
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Among the various Varṇa Vikāras the prevalent and representative disorder
considered in this study is Vyaṅga (Melasma), a hyperpigmentation disorder which
accounts for a great deal of anxiety and stress. There are not many statistics to prove the
exact frequency of skin diseases in this country but the general impression is 10-20
percent of patients seek medical advise for skin diseases. Treatment modalities for
hyperpigmentation are usually unsatisfactory as it shows exacerbation and remission
from time to time. It has various side effects such as contact dermatitis and complete
depigmentation. Hence there is a need for its evaluation through an Ayurvedic
perspective.
Since a fairer complexion is the preference attitude of the society, Varṇya
upakramas may prove to be a ray of hope for those who are desirous of it .Hence the
present study was focused on this concept applied in Vyaṅga thus entitled as “ A Study
on the concept of Varṇya vis-a vis Clinical evaluation of Varṇya Gaṇa Lepa in Vyaṅga.”
Definition of Varṇa
The Sāmānya arthas of the term Varṇa include Brahmaṇādi Jāti, Śuklādi Rūpa and
Akārādyakṣara. By Padārtha tantrayuki it can be said that Śuklādi Rūpa is the most
relevant meaning in this context.
Viśeṣa artha- Varṇa can be interpreted and understood in the following way.
Varṇa as Skin Colour:-
By the definition Varno gaurādi the term Varṇa literally refers to the colour component
of skin health i.e. gaura, śyāma, avadāta etc colours of the skin.

147
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Varṇa as Skin texture
By the definition Varṇa Śabdena Cakṣurgrāhya Raukṣādayopi Gṛhyante the term Varṇa
has been used to designate skin texture in this context. Raukṣādi refers to rūkṣa and
snigdha guṇas i.e. (dryness or oiliness of the skin) which are perceived by the
cakṣurindriya and are in association with Varṇa.
Varṇa as Skin Lustre/natural glow
By the definition Varṇaḥ śarīra kānti, Varṇa refers to the lustre or the radiance of the
skin. When the light falls on the skin, there is reflection (radiance) of light at the surface
of skin (caused by skin oil), and from the sub-layers under the skin from pigments such
as melanin and blood haemoglobin. This reflection produces kānti in the skin.
Varṇa as -Plumpness (sign of good nourishment)
By the definition Varṇa bhedena glāni harṣa raukṣya sneha vyākhyātā, it is clear that the
other parameters such as glāni, harsha, roukshya, snigdhata also refers to Varṇa. Here
glani refers to māṁsa apacaya and harsha refers to the māṁsa upacaya which can be
understood as plumpiness or the sign of good nourishment.
Varṇa as Appearance-
The term Prasanna Varṇa has been used in many contexts, for example, the individual
with kapha Prakṛti is said to possess Prasanna Varṇa. The term prasanna refers to clear,
bright and pure, hence Varṇa also refers to the appearance of skin.

148
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
In a broader perspective ,Varṇa mainly refers to skin colour, but the deeper
understanding of the term with the help of other contextual references reveals that Varṇa
is colour (śyāma, gaurādi), texture (rūkṣa, snigdhādi), lustre (kānti),
appearance/complexion (prasanna varṇa), Nourishment (harsha upacaya). In the context
of Vraṇa Upakrama Savarṇakaraṇa also refers to Māṁsa janana karma. In
dermatological parlance the parameters such as Skin hydration (Dryness-Oilyness), Skin
Pigmentation (Pigmented Non pigmented), Skin Sensitivity (Sensitive –resistant), Skin
wrinkling (Wrinkled-tight) also come under the perview of Varṇa. Therefore Varṇa can
be understood from different perspectives. Hence by ekavṛntagataphala dvaya nyāya it
can be said that Varṇa has wider dimensions.
Saṁbaṁdhita Śabda
Prabhā, Chāyā and Varṇa are used synonymously at different contexts. There is a very
narrow margin between these 3 entities and hence the exact difference between these 3
entities can be understood as follows.
Chāyā- Chāyā is a broader aspect which incorporates many entities into it. The 3 main
characteristic features of Chāyā include Varṇānāmākramati Chāyā, Āsannā lakṣyate
Chāyā, Chāyā Varṇaprabhāśrayā i.e. Chāyā circumscribes Varṇa ie Varṇa is not
perceived clearly when circumscribed by Chāyā, it is recognizable from near and Chāyā
is dependent on Varṇa and Prabhā. 5 types of Chāyā have been explained in classics.
Vāyavī, Āgneyī, Nābhasī, Āṁbhasī, Pārthivī ie classification of Chāyā are based on 5
mahābhūtas.
149
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
It is said that Saṁsthāna Pramāṇa Varṇa Prabhā Rūpa Vividha Lakṣaṇāḥ120cxx
ie the
description of 5 types of Chāyā is mainly based on these 5 parameters
Samsthana refers to Ākṛti (form or appearance). It is of 2 types Suṣamā (Pleasant) and
Viṣamā (Unpleasant). Sthira Saṁsthāna is a lakṣaṇa of Pārthivī Chāyā.
Pramana is considered as (weight or the measure of physical strength) . It is classified
into Madhya, Alpa and Mahat Pramāṇa. Dīrgha āyata Pramāṇa is a lakshana of
Pārthivī Chāyā.
Varṇa refers to colour ie Gaurādi. Vāyavī Chāyā is characterized by shyāva aruṇa
Varṇa, Nābhasī Chāyā is characterised by Nīla Varṇa
Prabhā is the radiance or lustre which does the Varṇa prakāśaṇa. Āgneyī Chāyā as
dīptābha prabhā, but Vāyavī Chāyā has hata prabhā.
Rupa- It is the beauty (saundarya, cakṣurindriya gata bhāva) of an individual. Āṁbhasī
Chāyā is said to have śuddha vaiḍūrya vimalā rūpa where as Āgneyī Chāyā is said to
have viśuddha rakta rūpa
In a broader sense together these 5 entities constitute Chāyā Varṇa and Prabhā are the
important and significant contributory factors for Chāyā .
For example An individual has a dark skin type, but has a lustrous skin, good built,
impressive appearance. Inspite of having dark skin type it is masked by other personality
traits and still the overall personality of the individual remains unaffected. That is the
reason it is said that Varṇa is circumscribed by Chāyā (varṇānām ākramati
pratidvaṁdvībhūteva Varṇasya ātmānaṁ prakāśayati). Bahiparimārjana dravyās

150
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
basically cause prakāśaṇa of neelādi Varṇa and sapta vidha prabhā which indirectly
refers to the Varṇa and Prabhā components of Chāyā
Prabhā -Prabhā is an entity which is characterized by prakāśana of Varṇa (bhāstu
Varṇa prakāśakaḥ). It is identified from a distance. It is the innate lustre which gives
radiance to the skin irrespective of the skin colour. It is said to be produced only because
of teja. It is divided into 7 types ie rakta, pīta, sita, śyāva, harita, pāndura, asita. All
these are grouped into śubha and aśubha varieties in the context of ariṣṭa lakṣaṇa .These
types of Prabhā when they are vikāsī ,vimala, āśuprasāriṇī then these are termed as
śubha Prabhā but when they are rūkśa malina saṁkliṣṭa & utpatita then they are
termed as aśubha.
Existence of Prabhā is completely independent of Varṇa (Skin colour) as
invariably individuals of either type of skin colours can have a good radiant and lustrous
skin. But the type of Prabhā out of these 7 types can be in accordance to the Varṇa. For
example gaura varṇa may be associated with sita or pāndura Prabhā , śyāma Varṇa with
śyāva Prabhā etc. An extensive study of the concept of Prabhā is necessary to
understand the practical application of the types of Prabhā .
Classification of Prākṛta Varṇa
It is observed that a tāratamyatā in avadāta varṇa is the basis for classification
i.e. (śyāmavadāta and avadāta) according to Caraka samhita and tāratamyatā in śyāma
varṇa i.e. (Gaura śyāma and Kṛṣṇa śyāma) according to Aṣṭāṅga Saṁgraha.
Hārīta saṁhitā has a unique explanation of prākṛta varṇas with an addition of piṅgala
varṇa to the 3 prākṛta varṇas i.e. (Gaura, Śyāma, Kṛṣṇa). In this classification the

151
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
association of rakta is explained along with pittādhikya. As per the author, combination
of 2 doṣas produces prākṛta Varṇa and the classification is according to this idea. It is a
unique concept different from all other authors.
Hence 6 Prākṛta Varṇas are observed as per different authors. They are Kṛṣṇa, Śyāma,
Avadāta (Gaura), Gauraśyāma, Kṛṣṇa Śyāma, & Piṅgala
Sub types of Prākṛta Varṇa
The main basis for classification of Prākṛta Varṇas is the tāratamyatā among each type
of Varṇa. For example padma gaura, candra gaura and śara gaura are the tara tama
Varṇas of Gaura Varṇa. Similarly it can be understood for other Varṇas also. The
modern races such as Mongoloid, negroid etc correspond to the different varieties of
Prākṛta Varṇa. The different gradients of Varṇas can also be a guideline to design and
develop a standardized Colour grading scale useful for both diagnostic and therapeutic
purposes.
Figure 13- Sub types of Prākṛta Varṇa
152
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Vaikṛta Varṇa
5 Varṇas have been considered as Vaikṛta Varṇa according to both Caraka Saṁhitā and
Aṣṭāṅga Saṁgraha .They are nīla, śyāva ,tāmra ,harita, śukla. Ācārya Gangādhara’s
commentary on Vaikṛta Varṇa reveals that there are 3 Vaikṛta Varṇas. They are nīla
śyāma (nīlavat śyāma), tāmra, haritaśukla (palāśavad gaura). The similies given in
Indukara commentary for Vaikṛta Varṇas such as śankha kundādi prakhya (śukla), Agni
prakhya (taamra) helps to acquire clarity regarding the colours. A difference of opinion
exists with Ācārya Gangādhara.According to him nīla varṇa is produced by vāyu bahula
panca mahābhūta and is considered as rūkṣa kṛṣṇa (prākṛta varṇa). Haridrābha gaura
(Udaka bahula pancabhūta) and palāśābha harita (Ākāśa bahula pancabhūta) are
considered as prākṛta varṇas. It seems that there is a narrow margin between prākṛta
varṇa and vaikṛta varṇa. Vaikṛta Varṇa has significance in the context of diseases and
ariṣṭa lakṣaṇa. Prākṛta Varṇa can at times become vaikṛta varṇa, and if vaikṛta varṇa is
present since birth then it can be considered as prākṛta itself. Only a sudden shift from
prākṛta to vaikṛta can be considered under ariṣṭa lakṣaṇa.
When an individual who is basically of Śyāma Varṇa consumes rasāyana for some
duration and attains gaura varṇa, and after discontinuation of rasāyana therapy he again
attains śyāma varṇa, in this context, though gauratva is a different varṇa from that of his
original colour but it cannot be considered as doṣa and śyāvatva which is attained back is
not considered as ariṣṭa lakṣaṇa or vaikṛta varṇa.
153
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Tvacā
Tvacā is said to be the adhiṣṭhāna for Varṇa. The term avabhāsinī refers to the reflection
or presentation or manifestation of all the Varṇas, 5types of Chāyā and 7 types of
Prabhā. Avabhāsinī tvacā is main ādhāra for kṛṣṇa gaurādi Varṇa. Upto the 3 or 4th
layer of skin, it it can be included under bāhya tvacā and various Varṇa vikāras like
nyaccha, vyaṅga, maṣaka, kilāsa etc afflict the 3rd
or 4th
layer of skin which shows the
Varṇa takes adhiṣṭhāna in these layers.
The different layers of tvacā i.e. avabhāsinī, lohitā, vedinī etc can be co related to the 7
layers of skin as per the contemporary science (i.e. Stratum corneum, lucidum etc)
Varṇa Utpatti kāla
Varṇa utpatti occurs mainly in the garbhādāna kāla. And it is manifested in the 6th
month and according to Kāśyapa Saṁhitā and Caraka Saṁhitā Varṇa upacaya /Varṇa
vṛddhi takes place in 6th
month. The contemporary research on the skin colour reveals
that only after 24 weeks of gestation the melanocytes become established at the
epidermal-dermal junction, thus Āyurveda proves itself to be a most scientific science.
Factors responsible for the formation of Varṇa- General factors
Bīja, ātmā, āśaya, kāla, āhāra ,vihāra in general play a significant role in determination
of Varṇa. Bīja, ātmā & āśaya can be roughly considered as the hereditary factors and
kāla, āhāra &vihāra can be considered as influencing factors. But kāla has still more
significance since it is the factor which is completely out of the range of human control.
ṛtu also has a significant role to play,as per few studies, due to seasonal transformations
there is decreasing photo-period in autmn and early winter generates increased melatonin

154
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
secretion which in turn has inhibitory effects on the pigmentary hormones of the
pituitary.
Factors of foetal life- Role of Pancamahābhūtas in the formation of Varṇa
Tejo dhātu is said to be mainly responsible for variation in Varṇa. It is a known fact that
Ap is said to possess ayvakta rasa similarly teja is said to possess Avyakta rūpa, any
colour is determined by the combination of other mahābhūtas with teja. Varṇa utpatti is
influenced by Pancamahābhūta during the avayava āraṁbha kāla .Any change in the
guṇas of mahābhūtas produces different variations in Varṇa. Teja alone or other
mahābhūtas alone cannot produce any colour thus the saṁyoga here plays an important
role. For example
The avyakta rūpa of tejas in combination with śuklatva of Ap and viśada guṇa of Ākāśa
produces Avadāta Varṇa
Teja (Avyakta)+ Ap (śukla) + Ākāśa(viśada)- Avadāta Varṇa
Variations in bāhulya –In the same combination if there is
Udaka bahula pancabhūta – It produces Haridrābha gaura
Ākāśa bahula pancabhūta –It produces Palāśābha harita
The avyakta rūpa of tejas in combination with Kṛṣṇatva of Pṛthvī and vishada guṇa of
Vāyu produces Kṛṣṇa Varṇa
Teja (Avyakta)+ Pṛthvī (Kṛṣṇa) + Vāyu (viśada)- Kṛṣṇa Varṇa
In the same combination if there is
Pṛthvī bahula pancabhūta – It produces Pakva jaṁbūpama kṛṣṇa Varṇa
Vāyu bahula pancabhūta – It produces Ruksh kṛṣṇa , Nīla Varṇa
Śyāma- śukla kṛṣṇa miśrī bhāva

155
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Similarly it should be understood for other Varṇas. Tāratamyatā in mahābhūtas will
result in rakta, pīta, aruṇādi varṇas.
Role of Guṇa
During the formation of varṇa, the guṇas play an important role and thus determine the
colour, The viśada guṇa of ākāśa mahābhūta produces avadāta varṇa, The khara and
cala guṇas produces kṛṣṇatva, snigdha guṇa is responsible for sukumara, snigdha aṅga
uṣṇa tīkṣṇa sūkṣma, laghu, rūkṣa, viśada physiologically are said to be responsible, for
Prabhā prākāśa and varṇa. But when these guṇayukta āhāra are consumed in excess
they produce varṇa vikṛti. For example increase in viśada guṇa causes sphuṭita aṅga,
excess of rūkṣa guṇa causes varṇa hāni and vaivarṇya.
Role of Śukra
Ghṛtamaṇḍābha, tailābha & madhvābha are the terms used to designate the śukra .
These correspond to Gaura kṛṣṇa and Śyāma Varṇa of the offspring. These similies are
used to depict the tāratamyatā in the Varṇa of śukra. On observation it also reveals that
similarity in mahābhautic composition also may be the reason for mentioning these
similies. The colour of healthy semen usually varies from a white to pale yellow colour.
A lighter colour of śukra would lead to a fairer complexion of the offspring and a darker
one leads to a dark coloured offspring. Similarly the quality of strī bīja may also
influence the varṇa of the foetus. But śukra alone cannot determine the colour of the
foetus.Only in combination of all other factors it may manifest its effect.

156
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Role of Garbhotpādaka bhāvas
Ātmaja bhāvas- These are the main determining factors. They include indriya preraṇa
dhāraṇa, swara Varṇa etc. All the ātmaja bhāvas are under the control of ātma
pratibaddha karmās as the karma and triguṇas of previous birth are carried by ātma
There are many instances where in the couples are kṛṣṇa or śyāma Varṇa but the
offspring is of avadāta varṇa or vice versa with a contrast colour of the offspring.
Though the answer for this may be the genetic control according to the modern scientists
but since even these factors are far from the control of humans, they can be included
under the ātmaja bhāvas. This is clear evidence of the effect of ātma pratibaddha karmās
and their effects are reflected by these bhāvas.
Sātmyaja Bhāvas.- Varṇa can be modulated to some extent by the intake of āhāra which
are varṇya and by rasāyana upayoga. The āhāra is pancabhoutic and the dominant
mahābhūta influences the corresponding varṇa. Here Sātmya refers to the āhāra vihāra
of mother before and during garbhāvasthā and āhāra, vihāra influences the quality of
śukra in males. For example excess kashāya rasa causes shyāvatva.
Out of these 2 factors, ātmaja bhāvas are far from control of humans where as sātmyaja
bhāvas are under the control of humans where in slight modulation of Varṇa is possible.
Role of Āhāra
Āhāra plays a very important role to determine the Varṇa of the individual. The careful
observation of garbhiṇī paricaryā reveals that the āhāra which is advised in the 6th
month of pregnancy is sarpi, since Varṇa upacaya takes place in the 6th
month, sarpi is

157
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
said to be śreṣṭha varṇya dravya hence that may be rationality behind advising sarpi as
pathya in the 6 th month of pregnancy.
Role of vihāra
An important vihāra which is said to be as varṇya is Jala krīda.The reason for this may
be attributed to frequent contact with Jala (Ap mahābhūta) which is constituted mainly
by śukla guṇa.
Factors responsible for the formation of Varṇa after the birth.- Varṇa and Vaya
There is Hrāsa of Chavi after 30 yrs and Hrāsa of twak is seen after 50 yrs. Here the skin
attains śithilatā (wrinkling), since the parameters such as (wrinkling –tightness) (dryness-
oiliness) (pigmented-non pigmented) etc are included under the purview of varṇa it can
be said that vaya has a significant effect on maintenance and deterioration of varṇa.
Elderly people often display dry scaled skin. This is because of the loss of barrier
function that occurs with increasing age. Thus Roughness, wrinkling, and the appearance
of dark and light spots also affect the appearance and texture of aged skin.
Role of Deśa
Deśa has a significant influence on varṇa. A person from a colder region has a
characteristic varṇa in accordance to his deśa. But when he moves from the cold region
to the hotter regions his varṇa will definitely show a change to suit the climate there. The
same can be said about a person from a hot region migrating to a cooler region. But this
change will not be more than a particular degree from his normal colour. Hence though
the colour and complexion of a person is genetically determined, the deśa does influence

158
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
it to a certain extent. So, the geographical conditions have their contribution in their
respect.
The close association between latitude and skin colour was confirmed in a recent
and more comprehensive survey which found a positive correlation of 0.82 between skin
reflectance and distance from the equator. The amount of U.V received at the earth‟s
surface is inversely related to latitude the higher the latitude the lower the U.V.It seems
that from a geographical stand point the darker the skin pigmentation the greater is the
ambient U.V.
Fig No 14:- Influence of Deśa on Varṇa.
Role of Kula and Jāti
Kula also has a significant role in the determination of Varṇa, It is a known fact that
prakṛti determines varṇa, among the various types of prakṛti, Kula prasaktā prakṛti
suggests the importance of Kulaja bhāvas in the determination of varṇa. Genetic factors
which really contributed to skin colour were also the ones that determined race-genetic
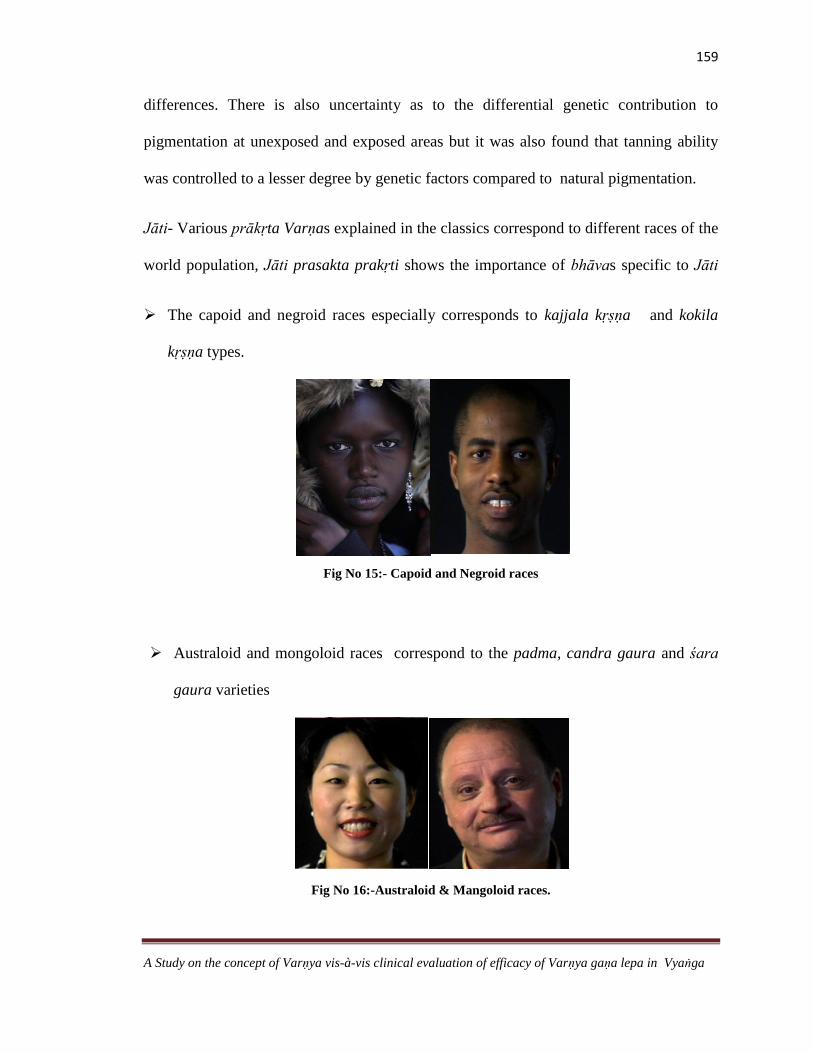
159
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
differences. There is also uncertainty as to the differential genetic contribution to
pigmentation at unexposed and exposed areas but it was also found that tanning ability
was controlled to a lesser degree by genetic factors compared to natural pigmentation.
Jāti- Various prākṛta Varṇas explained in the classics correspond to different races of the
world population, Jāti prasakta prakṛti shows the importance of bhāvas specific to Jāti
The capoid and negroid races especially corresponds to kajjala kṛṣṇa and kokila
kṛṣṇa types.
Fig No 15:- Capoid and Negroid races
Australoid and mongoloid races correspond to the padma, candra gaura and śara
gaura varieties
Fig No 16:-Australoid & Mangoloid races.
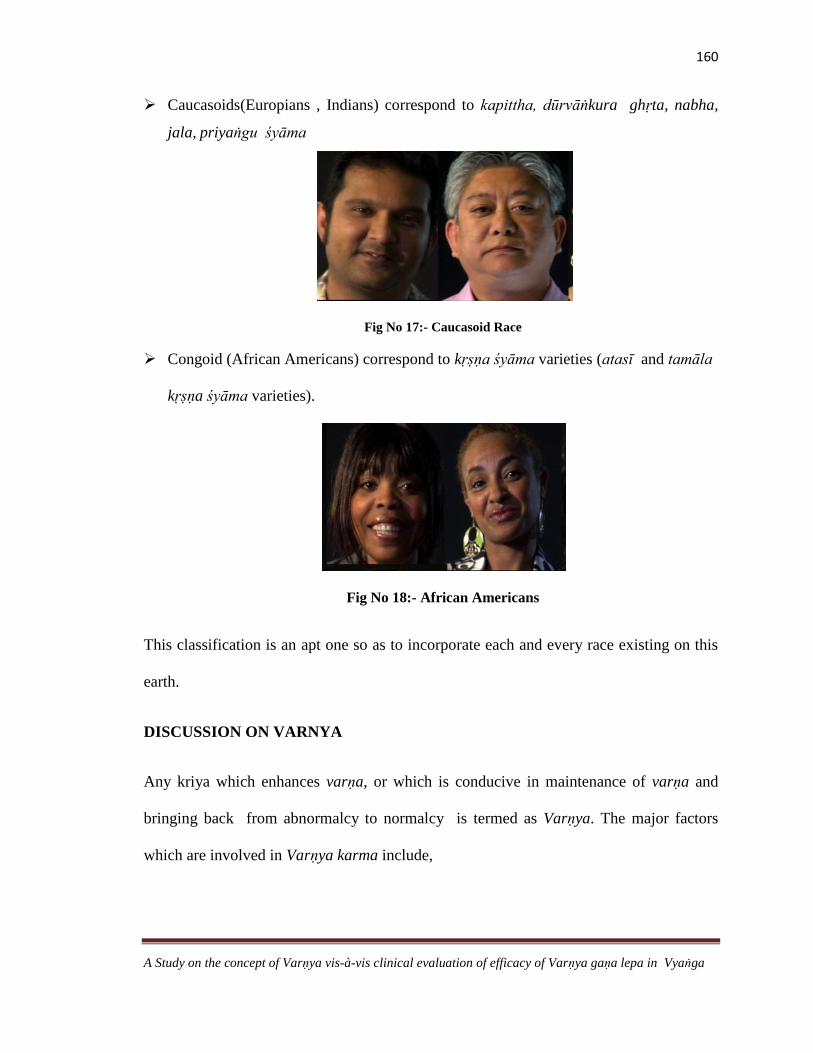
160
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Caucasoids(Europians , Indians) correspond to kapittha, dūrvāṅkura ghṛta, nabha,
jala, priyaṅgu śyāma
Fig No 17:- Caucasoid Race
Congoid (African Americans) correspond to kṛṣṇa śyāma varieties (atasī and tamāla
kṛṣṇa śyāma varieties).
Fig No 18:- African Americans
This classification is an apt one so as to incorporate each and every race existing on this
earth.
DISCUSSION ON VARNYA
Any kriya which enhances varṇa, or which is conducive in maintenance of varṇa and
bringing back from abnormalcy to normalcy is termed as Varṇya. The major factors
which are involved in Varṇya karma include,
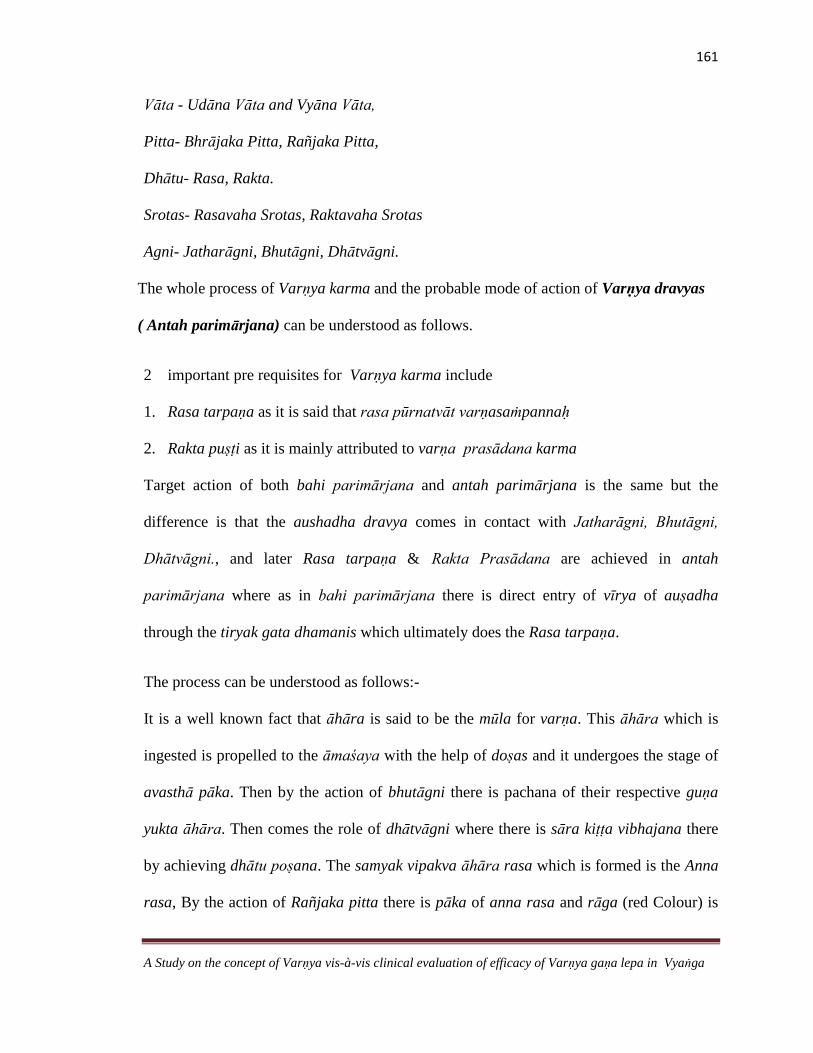
161
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Vāta - Udāna Vāta and Vyāna Vāta,
Pitta- Bhrājaka Pitta, Rañjaka Pitta,
Dhātu- Rasa, Rakta.
Srotas- Rasavaha Srotas, Raktavaha Srotas
Agni- Jatharāgni, Bhutāgni, Dhātvāgni.
The whole process of Varṇya karma and the probable mode of action of Varṇya dravyas
( Antah parimārjana) can be understood as follows.
2 important pre requisites for Varṇya karma include
1. Rasa tarpaṇa as it is said that rasa pūrnatvāt varṇasaṁpannaḥ
2. Rakta puṣṭi as it is mainly attributed to varṇa prasādana karma
Target action of both bahi parimārjana and antah parimārjana is the same but the
difference is that the aushadha dravya comes in contact with Jatharāgni, Bhutāgni,
Dhātvāgni., and later Rasa tarpaṇa & Rakta Prasādana are achieved in antah
parimārjana where as in bahi parimārjana there is direct entry of vīrya of auṣadha
through the tiryak gata dhamanis which ultimately does the Rasa tarpaṇa.
The process can be understood as follows:-
It is a well known fact that āhāra is said to be the mūla for varṇa. This āhāra which is
ingested is propelled to the āmaśaya with the help of doṣas and it undergoes the stage of
avasthā pāka. Then by the action of bhutāgni there is pachana of their respective guṇa
yukta āhāra. Then comes the role of dhātvāgni where there is sāra kiṭṭa vibhajana there
by achieving dhātu poṣana. The samyak vipakva āhāra rasa which is formed is the Anna
rasa, By the action of Rañjaka pitta there is pāka of anna rasa and rāga (red Colour) is
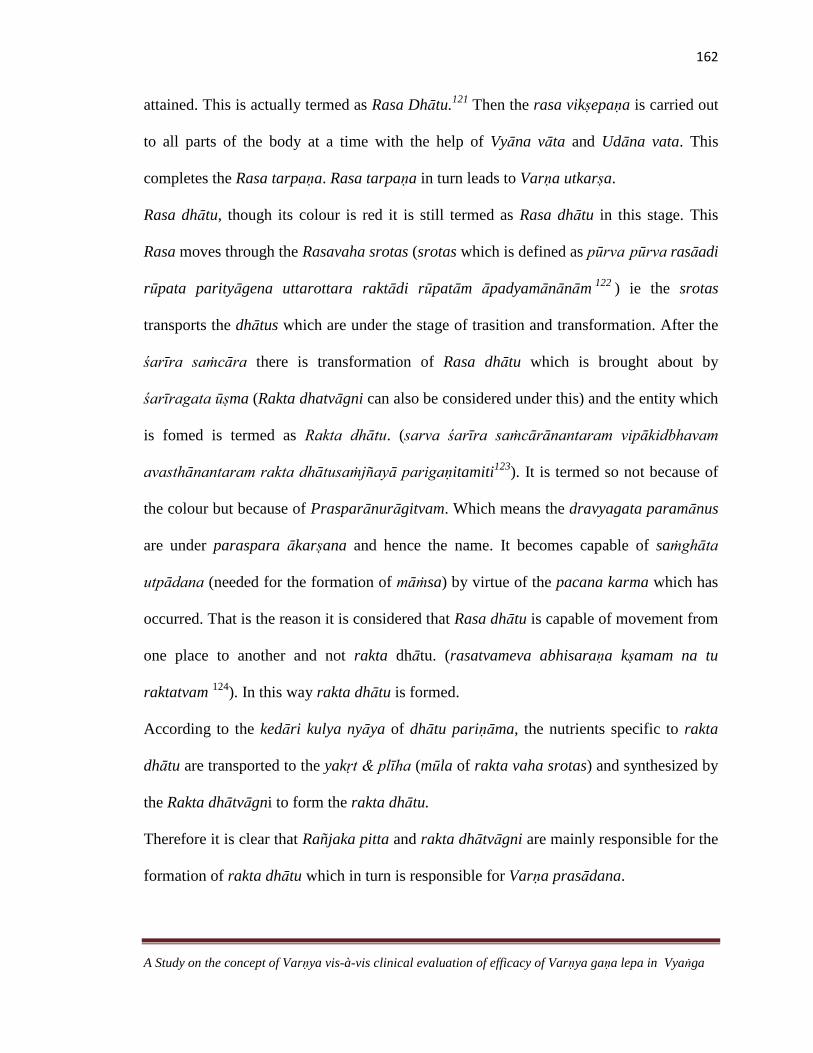
162
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
attained. This is actually termed as Rasa Dhātu.121
Then the rasa vikṣepaṇa is carried out
to all parts of the body at a time with the help of Vyāna vāta and Udāna vata. This
completes the Rasa tarpaṇa. Rasa tarpaṇa in turn leads to Varṇa utkarṣa.
Rasa dhātu, though its colour is red it is still termed as Rasa dhātu in this stage. This
Rasa moves through the Rasavaha srotas (srotas which is defined as pūrva pūrva rasāadi
rūpata parityāgena uttarottara raktādi rūpatām āpadyamānānām122
) ie the srotas
transports the dhātus which are under the stage of trasition and transformation. After the
śarīra saṁcāra there is transformation of Rasa dhātu which is brought about by
śarīragata ūṣma (Rakta dhatvāgni can also be considered under this) and the entity which
is fomed is termed as Rakta dhātu. (sarva śarīra saṁcārānantaram vipākidbhavam
avasthānantaram rakta dhātusaṁjñayā parigaṇitamiti123
). It is termed so not because of
the colour but because of Prasparānurāgitvam. Which means the dravyagata paramānus
are under paraspara ākarṣana and hence the name. It becomes capable of saṁghāta
utpādana (needed for the formation of māṁsa) by virtue of the pacana karma which has
occurred. That is the reason it is considered that Rasa dhātu is capable of movement from
one place to another and not rakta dhātu. (rasatvameva abhisaraṇa kṣamam na tu
raktatvam 124
). In this way rakta dhātu is formed.
According to the kedāri kulya nyāya of dhātu pariṇāma, the nutrients specific to rakta
dhātu are transported to the yakṛt & plīha (mūla of rakta vaha srotas) and synthesized by
the Rakta dhātvāgni to form the rakta dhātu.
Therefore it is clear that Rañjaka pitta and rakta dhātvāgni are mainly responsible for the
formation of rakta dhātu which in turn is responsible for Varṇa prasādana.
163
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
The Varṇa Prasādana of Rakta dhātu need not necessarily be linked to melanin or
melanogenesis. It may also be understood as the oxy hemoglobin pigment, a red
component which is especially evident in the areas where there is a rich arterial supply
such as skin of the face, neck palm and soles.
Paka of rakta dhatu in the foetal life produces twaca which is the seat for Bhrājaka
Pitta125
Bhrājaka Pitta- The quantitative and qualitative variations of ūṣma and Varṇa are the
main functions of bhrājaka pitta. This digests the auṣadha which is applied on the skin in
the form of abhyaṅga, pariṣeka, ālepa, avagāha and (Chāyā depends on Varṇa and
Prabhā and hence bhrājaka pitta determines Varṇa prākāśana)126
This ūṣma (Bhrājaka
Pitta) present in lasīkā, rasa, rakta, tvacā, maintains the dravatva in rasa and rakta
which in turn are responsible for Varṇa utkarṣa.
Rañjaka Pitta, by converting the rasa dhātu forms rakta, which in turn supplies to the
tvacā. It also nourishes the Varṇa, as tvacā is adhisthāna of Varṇa. Morever, rakta dhātu
is Varṇa prasādakara hence; it influences the Varṇa through forming the rakta. By virtue
of its function and colour it can be said to participate in the formation of Haemoglobin. It
is observed in the Vyādhi Pāńdu, where there is vitiation of the Rañjaka Pitta thus
causing Pāńduta or vaivarņya in the skin.
Role of Ojas
Ojas is the essence of all the dhātus. It is termed as Param teja or utkṛṣṭa teja or sāra.
Various references of ojas reveal that it can be considered as;-
164
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
1. Sarva dhātu sneha,
2. Rasa dhātu
3. Jīva śoṇita
4. Śarīra ūṣma
When we keenly observe the dhātu sāra puruṣa lakṣaṇas it is very evident that except the
māṁsa and asthi sāra puruṣa lakṣaṇas. Mṛdu aṅga, ślakṣṇa aṅga snigdha varṇa prasanna
varṇa are the terms which are used in all the other dhātu sāra puruṣa lakṣaṇas This
snigdhata is mainly due to dhātu gata sneha. The combined effect of all the dhātu gata
sneha thus produces an utkṛṣṭa sneha or teja thus varṇa is very closely related to the status
of ojas. The role of Rasa dhātu, Jīva śoṇita, Śarīra ūṣma have already been dealt and Thus
every component of oja predominantly determines varṇa
Bala is a form of ojas whose normalcy produces prasanna varṇa and hence varṇa bheda
is a cardinal symptom which is mainly seen in Bala vyāpad lakṣaṇa.
Probable mode of action of Varṇya dravyās (bahi parimarjana)
All the kriyās such as Abhyaṅga, Pariṣeka, Ālepa, Avagāha, Snāna act mainly on the
bhrājaka pitta which resides in the tvacā.
Lepa is applied to the tvacā which is ādhāra for sparśanendriya, sweda vaha srotas
and romakūpa. Bāhya tvacā is the ādhāra for kṛṣṇa gaurādi varṇa also. The mode of
acttion can be analysed in 3 steps

165
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Step 1
Lepa comes in contact with the roma and romakūpa which in turn are connected to
the tiryak gata dhamanīs which perform the function of sweda vahana ie the active
drug enters the sweat ducts and hair follicles.
Hair follicles represent a reservoir that may store topically applied
substance.Differences in the follicular penetration were observed in different ethnic
groups. Hair follicles appear to present an important pathway for percutaneous
absorption in non diseased skin. Even solid particles may enter deep into the follicular
orifice, a phenomenon that lends itself to the concept of follicular targeting of drugs.It
was found that nano particles were stored 10 times longer in the hair follicles than in
the stratum corneum, it should be noted that when topically applied substances
penetrate into the hair follicles, they do not necessarily penetrate through the skin
barrier into the living tissue because hair follicles also have barrier properties.
Step 2
After the contact of the drug there is pāka of dravya in tvacā. Pāka refers to the
action of Bhrājaka agni and rasa dhātvāgni It occurs by virtue of uṣṇa guṇa of
bhrājaka pitta ie it takes up and metabolises the kriyā dravya (bahi parimārjana
dravya)
This ūṣma present in lasīkā, rasa, rakta, tvacā, maintains the dravatva in rasa and
rakta which in turn are responsible for Varṇa utkarṣa. 127

166
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Pathway across stratum corneum
Stratum corneum-It is The Primary compartment that limits the percutaneous
absorption of compounds is the stratum corneum and it determines diffusion of
compounds across the skin.
Viable tissue
Although the primary barrier to percutaneous absorption of compounds is the stratum
corneum diffusion through viable tissue as well as metabolism and resorption also
influence the bio availability of compounds in specific skin compartments.The
passage of compounds from the stratum corneum into the viable epidermis results in
substantial dilution.
Skin Metabolism
Metabolism in skin compartments plays a significant role in determining the fate of a
topically applied active compound. Metabolic activity is found in skin surface,
appendages, the stratum corneum, viable epidermis. The level of many enzymes is
highest in the epidermis. The relatively large size of the dermal component may result
in a significant role in the metabolism of topically applied substances.
Step 3
These steps finally lead to Rasa tarpaṇa which is mainly achieved by Udāna Vāta &
Vyāna Vāta which supplies anna rasa to the concerned śarīra ghaṭaka or avayava
and Varṇa utkarṣa is thus achieved. Hence it is quoted that Varṇasaṁpannaḥ
rasapūrṇatvāt.

167
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
General concept of Varnya
Varṇya refers to enhancing the normal complexion (the terms Varṇa dārḍhya, Varṇa
prasādana Varṇa utkarṣa are used) and it also refers to bringing back the abnormal
colour to the normalcy which includes the pathological aspect ie( hyperpigmentation
and hypopigmentation) hence the synonyms Varṇa vaimalya, Varṇa vaiśadya, Varṇa
śuddhi are used. By these modalities just the modulation of Varṇa can be achieved,
where in the qualitative parameters can be improved such as the texture, radiance etc.
The colour parameter cannot be changed to a very significant extent such as from
kṛṣṇa to gaura varṇa by the usage of varṇya upakramas ( āhāra, vihāra, rasāyana
etc), but śyāma to gaura can be expected, that is the reason Ācārya Cakrapāṇi has
considered that when rasāyanas are used there may be change of varṇa from śyāma
to gaura (where as kṛṣṇa varṇa is not considered) but when discontinued the same
śyāma varṇa is attained back, and this is not included under the perview of vaikṛta
varṇas. A shift to a complete contrast colour is also not explained inspite of usage of
rasāyana. Hence varṇya upakramas help in modulation of Varṇa (parameters such as
colour (Skin pigmentation – Pigmented/ Non pigmented), texture (Skin Hydration –
Dry/Oily), appearance (Skin Sensitivity- Sensitive/Resistant), (Skin wrinkling –
Wrinkled/Tight) radiance, plumpness (sign of nourishment) to some extent.
The concept of varṇya thus incorporates the Correction of innate entities influencing
Varṇa. An oral administration of varṇya dravyas along with bahi parimārjana cikitsā
may definitely bring a marked improvement in all the parameters included under
Varṇa
168
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
DISCUSSION ON DISEASE- VYANGA/ MELASMA
Melasma is a disease in the general population that causes great impact on the
quality of life of patients and drives great efforts to clinical and pharmaceutical research
for the development of treatments. However, the knowledge of its physiopathogenesis is
still very limited.128
Incidence
An important factor in the etiology of melasma in females is female sex hormone
activity, usage of Oral Contraceptive pills, and hormonal changes in post menopausal
period, where as the main associated factors among men appear to be sun induced
aggravation and a significant family history of the condition129
.
Etiology/ Nidāna
Mānasika Nidāna for Vyaṅga is mainly stated to be as Krodha, and Āyasa which in turn
vitiate Pitta and Vāta respectively. An emotional stress is a prime factor in causation of
Vyaṅga, The main quality of life domains that showed to be affected by melasma were
social life, recreation, leisure, and emotional well being.130
Stress is an influential factor in pigmentary disorders and it can also precipitate or
contribute to the etiologic pathway of a cutaneous manifestation. Melanocyte stimulating
hormone (MSH) levels have been shown to be influenced by a rise in adrenocorticotropic
hormone (ACTH) levels, which increases with stress. Through this pathway, MSH may
play a role in aggravating melasma and other dyspigmentations in stressed patients.
Although the nature of the association between stress and the exacerbation of certain skin
conditions have not been fully elucidated.

169
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Two traditional explanations have been offered. That is, the activation of two
stress axes, the hypothalamic-pituitary-adrenal (HPA) axis, which elevates cortisol levels,
and the sympathetic nervous system axis, which increases adrenaline levels, are thought
to alter immune balance and facilitate cutaneous manifestation. Recently, a third stress
axis has been suggested. Specifically, Pavlovic et al. have demonstrated that peripheral
neuropeptidergic nerve fibers transmit stress to the skin, exacerbating cutaneous
inflammation. The investigators showed that the number of cutaneous nerve fibers
containing the stress neuropeptide substance P was increased significantly by sound
stress.
Also the neural crest gives rise to different types of cells, including the dorsal root
ganglia of the spinal cord, the adrenal medulla and certain components of peripheral
nerve fibres (Schwann cells). The neural crest also generates those cells that are destined
to differentiate into the melanocyte series known as melanoblasts. Since both adrenal
medulla and the melanoblasts share a common origin, the influence of MSH by ACTH is
justified and thus causing hyperpigmentation.
Clinical features
The clinical features of Vyaṅga are mainly based on 4 parameters ie Shape of the lesion
(maṇḍala), Thickness of the lesion (macule- Tanutva), colour of the lesion ( Nīla, Syāva,
Kṛṣṇa) and Pain (nīruja -Painless)
Reason for involvement of specific sites
Melasma involves only specific sites of the body. Wade et al. 131
have suggested
the reason why only certain body areas, but not the entire body, are affected by

170
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
hyperpigmentation is that melanocytes in the areas affected are more sensitive to
hormonal stimulation. Another explanation may be the greater population of melanocytes
in the affected sites. One investigation showed that there is a greater population of
melanocytes in the skin of the face and forehead, with the population density of
melanocytes being 2–4 times greater than in the skin of the thigh and arms
Samprāpti / Pathogenesis
Mānasika nidānas such as krodha śoka āyasa & harṣa, basically vitiate vāta and pitta
doṣa significantly. Ātapa & anala sevana are also said to cause vaivarṇya or varṇa hāni.
By these nidānas there is duṣṭi of Rasa vaha srotas (aticintana) and Rakta vaha srotas
(ātapa and Anala) along with manovaha srotas (Krodhadi). All the nidānas mentioned,
have fourfold effect upon Doṣa, dūṣya, Agni and Srotas. The śyāva varṇa maṇḍala
indicate the involvement of vāta, and since there is derangement in bhrājaka pitta leading
to discolouration, it shows the involvement of Pitta. Though there is no direct
involvement of Kapha, it is evident from the fact that twacā is adhiṣṭhāna for varṇa as
well as site for rasa dhātu, so by āśraya āśrayī bhāva, it can be said that kapha is also
involved, Presence of associated features such as kaṇḍū shows the active involvement of
kapha. Direct involvement of jaṭharāgni is not recognized clinically. But only dhātvāgni
vikṛti can be recognised mainly. This is possible only after the jaṭharāgni vikṛti hence its
involvement can be inferred. The vitiated Vāta doṣa along with Rakta and Pitta doṣa
produces Syāva, (blackish) nīruja maṇḍala. At this stage exact clinical features of the
disease are evident according to the involvement of the doṣas
171
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
Pathogenesis of pigmentation
Melasma is more commonly seen in Pregnancy. Hyperpigmentation in pregnancy
is attributed by some investigators to an increased output of some combination of
placental, pituitary, and ovarian hormones.132
An increased amount of MSH of the
pituitary was postulated in the past to be the cause of hyperpigmentation. Other factors
which were suggested to be related to hyperpigmentation in pregnancy are progesterone
and estrogen, the levels of both of which are increased during pregnancy. 133
Blood levels
of progesterone increase throughout pregnancy, and estrogen production rises from the
eighth week and begins to decrease after the 30th week of pregnancy. This pattern
follows the progression of hyperpigmentation .Hyperpigmentation of the face occurs in
women taking oral contraceptives or during the menstrual cycle, supporting the idea that
estrogen and progesterone are involved. 134
Recently, investigators found that a lipid extraction from the placenta had a
pigment inducing activity both in vivo and in vitro. The placenta was found to be rich in
bioactive sphingolipids, which were found to induce melanogenesis by upregulating the
expression of various melanogenic enzymes – tyrosinase and tyrosinase-related proteins 1
and 2 at the translational and transcriptional levels. 135
Vyaṅga cikitsā
The treatment modalities which have been mainly explained for Vyaṅga other than bahi
parimārjana cikitsā basically aim at correcting the innate entities such as doṣā duṣṭi,
rakta duṣṭi, agni ,vikṛti & sroto vaiguṇya by which the whole system is cleansed paving
a way for better improvement in varṇa. This method of treatment of vyaṅga was not the
option till recent days as per the contemporary science inspite of the fact that there is a

172
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
systemic involvement such as hormonal imbalance which needs correction at first. They
mainly concentrated on the different modes of transdermal drug delivery system till
recent years. And now even they have emerged with the concept of Nutritional Cosmetics
somewhat mimicking the antah parimārjana cikitsā hence Āyurveda has a detailed and
deeper sense of understanding regarding the subject.
Vyaṅga Sādhyāsādhyatā
Vyaṅga is considered as a kṛcchrasādhya vyādhi. Though it is a kṣudra roga it could have
been a sukhasādhya vyādhi, but due to involvement of various factors such as the
mānasika nidāna, exposure to sun rays, hormonal disturbances from time to time, all
these cannot be controlled effectively at a time because of which the treatment becomes
difficult.
DISCUSSION ON DRUGS
The main chemical constituents of the Lepa of 10 drugs which were used include
Santalol, Genistein, glabridin, Liquertin, Glycyrrhizin, benzoic acid etc. Many studies
have been undertaken to evaluate the efficacy of these chemical constituents on various
skin parameters.
Candana - Santalol is the main chemical constituent of Candana -. It may be effective in
controlling the oxidative stress caused by ultraviolet radiation.136
Padmaka, Payasya- Genistein is an important chemical constituent of these 2 drugs.
Genistein, either topically applied or orally supplemented, has been shown to
substantially block the subacute and chronic UVB-induced cutaneous damage and
histologic alterations related to photoaging .Genistein is already included in various

173
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
products such as facial moisturizers, sunscreens, and several skin care formulations
claiming antiaging effects.
Madhūka- Glabridin and Liquertin are said to have tyrosinase inhibitory and anti
inflammatory properties. Polyphenols and polysaccharides possess antioxidant activities.
Uśīra ,sitā & latā- The compounds such as Benzoic acid helps in balancing the secretion
of sebum. It is also a useful antiseptic and is slightly stringent. It is used in lotions,
compresses and baths for the treatment of oily skin, acne and weeping sores 137
Sāriva :-The plant is used against various skin diseases and in the treatment of acne
vulgaris.The ethanolic extract was reported to be effective chemo protective agent and
prevented oxidative stress and tumour in skin. 138
Manjiṣṭha -Munjistin and purpurin are the important anthraquinones present in Manjiṣṭha
The cell culture preparation exhibits antiinflammatory activity, as well as wound healing
properties.-
Probable mode of action on Vyaṅga/Melasma
Varṇya mahākaṣāya dravyās are administered both for bahi parimārjana and antah
parimārjana ie (ubhaya parimārjana). The probable mode of action based on rasa, guṇa
vīrya, vipāka may be as follows.
Any rasa basically is said to possess 2 important karmas ie Chedana and
upaśamana. The drugs which are administered in the form of lepa mainly are of madhura
tikta, kaṣāya rasās. These rasās does the Chedana of prakupita vāta and pitta (chedanaṁ
doṣāṇāṁ bhāgaśaḥ karaṇam)139
and upaśamana (doṣānām anutkleśena samīkaraṇam )

174
A Study on the concept of Varṇya vis-à-vis clinical evaluation of efficacy of Varṇya gaṇa lepa in Vyaṅga
which means does not allow the utkleśa of doṣas and maintains the equilibrium and thus
pacifies pitta which is the main culprit in the causation of vyaṅga.
Out of these 10 drugs some of drugs possess snigdha guṇa and others possess
laghu rūkṣa guṇas. Snigdha guṇa is responsible for mārdava and varṇa prasādana where
as laghu rūkṣa are the properties of āgneya dravya which in turn are responsible for
prabhā, prākāśa and varṇa.
Almost all the drugs selected are of śīta vīrya and śīta vīrya dravyās are endowed
with rakta prasādana karma. While explaining the direction of application of Lepa, it is
said that (sirā mukhaih vīryam prāpnoti) hence after the entry of the drug by virtue of
vīrya it enters the circulation.
The selected drugs mainly are of madhura vipāka. Vipāka is basically defined as
karma niṣṭhayā, here the term niṣṭhā incorporates jaṭharāgni dhātvāgni & bhūtāgni
irrespective of their order. Madhura vipāka by virtue of its snigdha guṇa and kapha
vardhana karma is responsible for Varṇa utkarṣa. By the term twaci vipakva it can be
said tha the drug is absorbed by virtue of vipāka into the circulation.
As per the modern paralance these drugs may be assumed to minimize pigmentation by
following mechanisms in Melasma.
1. Reducing tyrosinase activity
2. Copper chelation
3. Thining of Statum corneum
4. Keratinocyte proliferation and
epidermal turn over
5. Absorb U V B
6. Dop quinine to dopa transfer
7. Melanosome transfer
8. Free radical scavenger

CLXXV
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
Water –Luke warm water has been used here as the vehicle, Water is the most
widely used and safest method to increase skin penetration .It is a non irritant and
is suitable for all skin types. It is cosmetically acceptable and easy to use. Luke
warm water also facilitates the thermodynamic activity and diffusion by vaso –
dilation and this temperature does not vitiate the pitta. The water content of the
stratum corneum is around 15 to 20% of the dry weight but can vary according to
humidity of the external environment. Additional water within the stratum
corneum could alter permeant solubility and thereby modify movement from the
vehicle into the membrane. In addition, increased skin hydration may swell and
open the structure of the stratum corneum leading to an increase in penetration,
although this has yet to be demonstrated experimentally. There is variation in
permeability in different regions of the body for example- The scrotum is
particularly permeable and the face forehead and dorsa of the hands may be more
permeable to water than the trunk arm and legs. The palms are particularly
impermeable to nearly all molecules except water
Water is well known to permeate through the lipid bilayers of epidermal skin.
Untilrecently, simple diffusion was the only presumed mechanism for water
conduction through epidermis. Aquaporins (AQPs), which are a form of water
channel, are integral membrane proteins that facilitate water transport in various
organs such as skin, renal tubules, eyes, the digestive tract, and even the brain
CLXXVI
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
DISCUSSION ON MATERIALS AND METHODS
Assessment tools
Colour grading scale-There are 26 grades in this scale, the skin colour is recorded in
the beginning, then the lesion colour of the patient was noted before, after treatment
and after follow up, the difference in the grades gives the extent of improvement.
Though darkness of the lesion is graded in MASI Score also, the rationality behind
using this scale is that the minor changes in the lesions can be noted due to wide range
of gradients in colour and the skin colour is also recorded, which enables us to analyse
whether people with fair or dark complexion are more prone to vyaṅga.
Lepa
3 important types of Lepa have been explained in the classics, they are Pradeha,
Pralepa and Ālepa. Pradeha, as per the definition it is characterized by śīta tanu
aviśoṣi or viśoṣi ex- Candana Lepa (śīta and tanu) . When piṇḍīkṛta kalka is placed
on the affected area then it is termed as Pradeha, and instead of piṇḍīkṛta kalka if
cūrṇa is used then it is termed as cūrṇa pradeha. It can be considered as prayoga
bheda of pradeha.
Pralepa- It is characterized by ūṣṇa bahala or abahu, viśoṣi. The thickness is said to
be as bahala or abahu, abahu is alpabahala (not very thick).
Here in this study the type of lepa used is ālepa. Ālepa is considered as the ādya
upakrama as it is śreṣṭha for both bahi parimārjana and antah parimārjana because
of its āśupīdāharatvāt guṇa (quick relief from the peeda). Ālepa is said to be agrya in
twak prasādana hence it is selected.cxl

CLXXVII
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
Method of application
Lepa should be applied in the opposite direction of the hair follicles so as to facilitate
the entry of auṣadha dravya through the roma kūpa, sweda vaha srotas and thus
reaches the sirā mukha. If the applied lepa dries and if still it is kept for some more
time, it yields no result. It is also said that yāvad ārdro bhavati tāvad vyādhiharo
bhavati .Until it is wet it is said to possess vyādhiharatva. Regarding the pramāna or
the thickness of the lepa it is said that mahiṣa ārdracarmavat, but this is considered as
the parama pramāna (highest thickness of lepa) since thickness of ālepa is between
pradeha and pralepa, hence the madhyama pramāna can be used.cxli
Inclusion criteria
The prevalence of the disease melasma is more in the child bearing age of the women,
but there are also few studies which reveal that, it occurs in young girls due to
menstrual irregularities and older women in post menopausal period. Hence the age
group 16-60yrs was selected.
Assessment Criteria
Skin/Lesion Colour ,Texture (Dry/Oily), Skin lustre, Number of Lesions, Size of
Lesions, Darkness of the lesion, Area of involvement, Homogeneity of the lesions are
the 8 parameters which have been assessed in the patients, in this study. Among these,
Darkness Area and Homogeneity constitute the Melasma Area Severity Index. All
these are assessed separately. Size of the lesions can be incorporated under the Area
of involvement; Number of lesions can be incorporated under the homogeneity of
involvement. Though they can be incorporated under these, they are assessed
separately so as to get accurate results and to analyse the exact extent and parameters
on which the formulation is effective.

CLXXVIII
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
DISCUSSION ON OBSERVATIONS
The observations were based on the clinical trial conducted on 35 patients registered
on the study.
Age- In the study maximum number of patients (40%) belonged to the age group 31-
40yrs followed by 21-30yrs (25.7%), 41-50yrs, 51-60yrs which suggests that melasma
is more prevalent in child bearing age where in there is maximum role of hormonal
influence which is the root cause for the disease.
Sex- In the study (88.6%) of patients (p value-0.000) were females of different age
groups which supports the fact of global incidence of melasma associated with
hormonal variations
Religion: In this study maximum numbers of patients (85..7%) were Hindus
indicating geographical predominance of Hindus among the selected population.
Educational Status- In this study (48.6%) of patients (P value-0.001) were educated
only upto high school, which shows the low level of literacy, because of which most
of them had to opt the labour job for living, which involves, excess of exposure to sun
and exertion which are the causes of melasma.
Marital Status- In the present study 94.3% of patients (P.Value 0.000) were married.
Though there is no direct link of the disease with Marriage, married women who had
children had a history of melasma during their pregnancy, which disappeared with
time, and in some others was persistent since years.
Socio economic status-In the study (54.3%) of patients were of middle class followed
by 40% of patients who belonged to lower middle class. Because of low levels of
immunity due to unaffordability to nutritional foods, this may be a cause for
prevalance of melasma in lower middle class.

CLXXIX
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
Diet -The present study revealed that, the patients who were consuming mixed diet
were more susceptible (77.1%) to melasma. The study however could not generalize
the fact that vegetarians are on safer side from the disease as the sample size taken
was very small.
Family history- In the present study 42.9% patients had a family history of melasma
which supports the presence of hereditary component in the manifestation of disease.
Contraceptive history- In the study though only 8.6% of patients had the history of
use of contraceptives still it supports the role of contraceptives in the causation of
melasma
Physical aggravating factors- In the study 45.7% of patients (P value-0.000) had
exposure to sun rays as Physical aggravating factor which suggests the important role
of Ultra violet radiation in the causation of melasma.
Psychological aggravating factors- In the study 62.9% of the patients (P value-
0.000) had stress and worries as aggravating factors which clearly suggests that Stress
is an important etiological factor in causation of melasma.
Use of soap- In the study 42.9% of the patients had the history of use of Lifeboy soap
since years even before the onset of the disease. There may be some association
between the causation of melasma and its usage; This cannot be confirmed by this
study because of small sample size.
Cosmetics-cream use-In the study 62.9% of the patients had the history of use of fair
and lovely cream since years even before the onset of the disease. Though the
ingredients prevent hyperpigmentation, there may be some association between the
causation of melasma and its usage, Use of Chemicals and artificial colours in the
preparation can trigger the causation of melasma. This cannot be confirmed by this
study because of small sample size.

CLXXX
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
Menstrual history- in the study 14.3% of the patients had irregular menstruation
accounting to the fact that hormonal disturbances are the causative factors for
melasma.
Age of menopause- In the study 20% of the patients had attained menopause
supporting the fact that post menopausal women are also prone to melasma to some
extent.
Prakṛti-In the study 48.6% patients were of pitta prakṛti followed by 31.4% patients
were of vāta prakṛti suggesting the fact that individuals of pitta prakṛti are more
prone to vyaṅga.
Patter of lesion- In the study 57.1% of the patients had malar type of melasma
followed by centro facial type (42.9%), suggesting the site of involvement and
somewhat supporting the global incidence to some extent.
Level of lesion- In the study 60% of the patients had dermal lesions which suggest the
severity of the disease and the depth of involvement.
Chronicity- In the study the chronicity of 62.9% patients (pvalue-0.001) was between
0-4 yrs. This may be because since melasma is an aesthetic disease which is a major
cause of concern to patients and before it becomes chronic they approach the hospital.
Skin colour- In the study the skin colour of 57.2% patients (p value-0.000) was
between 1-10 grade suggesting the fair complexion, supporting the fact that those
with fair complexion are more prone to melasma, but it cannot be told with certainity
due to small sample size.
Distribution of Chronicity vs level of the lesion- In the study 57.1% of patients had
dermal lesions in the group 0-4yrs ,28.6% patients had dermal lesions in the group 4-8
yrs and 14.3% patients had dermal lesions in the group 8 and above yrs chronicity.
The more and more chronic the lesions are, the deeper will be the level of
CLXXXI
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
involvement ie (dermal). The study does not signify this fact; it may be because of
smaller sample size and less number of patients in the very chronic group.
DISCUSSION ON RESULTS
Distribution of skin colour vs lesion colour – In the study the lesion colour is
compared with the skin colour with the help of fair and lovely colour grading scale.
The total mean of the Lesion colour before treatment was 21.7429, and it was
17.7714 after treatment and follow up. When only Lesion colour is observed, a mean
difference of around 4 is highly significant statistically (Pvalue-0.000) but in
comparison to skin colour is insignificant with P value 0.735. Duration of intervention
has a significant role in this disease, since the duration is 15 days the expected results
were not observed.
Darkness of the lesion- The subjective criteria of syāma maṇḍala is also assessed by
this parameter. Darkness of 4 regions were assessed, Frontal, left malar, right malar
and chin , among the 4 regions there was no statistically significant improvement in
frontal and chin regions where as in left malar and right malar regions there was
statistically significant improvement (P value-0.002) . Only one grade reduction was
observed after the treatment in most of the patients, this may be because of very less
duration of intervention period ie 15 days. For any of the dermatological changes to
appear it requires atleast a minimum of 30-45days duration, administration of external
application along with oral medicines. The disease is of a stubborn variety, and
because of the chronicity and influence of hormones which is variable from time to
time, all the causative factors cannot be controlled effectively and hence only one
grade reduction is observed.

CLXXXII
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
Area and Homogeneity of the lesions- There was no improvement in the area of
lesion as well as homogeneity of the lesions before treatment and after treatment and
follow up. This includes the size and number of lesions. It is assumed that a
minimium of 3 to 4 months duration is mandatory so as to observe significant
dermatological changes in number and size of lesions , as these are are influenced by
many factors such as exposure to sun, too much of stress and presence of other
physical and psychological aggravating factors which causes delay in relief.
MASI Scores:- The mean of MASI Scores of 35 patients, before treatment was 11.69
and after treatment and follow up it reduced to 10.8314 with a high statistical
significance (p value-0.000) MASI score is influenced by all the 3 factors. Since there
are no changes in area and homogeneity and only 1 grade improvement in darkness,
overall score is affected and thus only a mean difference of 0.9 is observed where in
really a difference of atleast 15 points is mandatory to assume a good clinical
improvement.
Dryness and oilyness- A statistically significant improvement was not found in
Dryness parameter where as statistically significant improvement was seen in oilyness
parameter. The formulation is said to have an evident effect on the texture (oilyness)
parameter of Varṇa. This may be because the formulation is in the form of chūrna
which is basically rūkṣa and moreover some of the drugs have rūkṣa guṇa which may
possibly have a role in reducing the oiliness of the skin. It is also clear that out of 35
patients 23 patients had dryness of different extent which supports the fact that
vyaṅga is a Varṇa vikāra with a deranged colour and texture component of Varṇa(
especially vātaja vyaṅga) .

CLXXXIII
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
Itching and burning sensation- These 2 parameters were evaluated to find out the
prevalence of kaphaja as well as raktaja vyaṅga where in kaṇḍū and dāha are
observed as associated symptoms. Only 20% of patients complained of kaṇḍū and
2.8% of patients complained of dāha and is not conclusive since the sample taken is
very less. The formulation also shows mild effect on the itching and burning
sensation. It may have a better effect possibly when the intervention period is
prolonged.
Skin lustre- There are no changes observed in the skin lustre before and after
treatment and follow up, It may be possibly because of the fact that lustre is not just a
physical entity where in a change can be brought about just by an external
application for 15 days, It is an innate entity influenced by numerous factors.
Results of overall improvement
The overall assessment of the study reveals 23 patients (64.34%) had mild
improvement,
CLXXXIV
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
CONCLUSION
1. Varṇa refers to different parameters of skin. They are colour (śyāma, gaurādi),
texture (rūkṣa, snigdhādi), lustre (kānti) , appearance/complexion (prasanna
varṇa), Nourishment (harśa upacaya) and dermatological parameters such as Skin
hydration(Dryness-Oilyness), Skin Pigmentation (Pigmented Non pigmented) ,
Skin Sensitivity( Sensitive –resistant), Skin wrinkling (Wrinkled-tight) also come
under the purview of Varṇa..
2. Though the terms Prabhā and Chāyā are used synonymously with Varṇa they are
different entities .Classification of Chāyā is mainly based on 5 important
parameters, They are Saṁsthāna Pramāṇa Varṇa Prabhā & Rūpa. Varṇa and
Prabhā are the important and significant contributory factors for Chāyā .
3. Existence of Prabhā is completely independent of Varṇa (Skin colour). But the
type of Prabhā out of 7 types can be in accordance with the Varṇa.
4. Various factors govern the formation of Varṇa. General factors include Bīja,
Ātma, Kāla, Āśaya, Āhāra and Vihāra. Specific factors contribute in the formation
of Varṇa in foetal life and in the process of varṇotpatti after birth. They are
Mahābhūta, Prakṛti, Guṇa, Garbhotpādaka bhāvas, Manasthiti, Āhāra and
Vihāra ,Deśa ,Kula and Jāti, Jaṭharāgni, Dośa- Dhātu Mala, Ojas.,Bala.
5. Varṇya refers to enhancing the normal complexion hence the terms Varṇa
dārḍhya, Varṇa prasādana Varṇa utkarṣa are used. It also refers to bringing back
the abnormal colour to the normalcy hence the synonyms Varṇa vaimalya, Varṇa
vaiśadya, Varṇa śuddhi are used.
6. Bhrājaka pitta has a major role in metabolizing the lepa which is applied to skin
,which takes entry through romakūpa, tiryakgata dhamanis and finally reaches the
circulation ending up with rasa tarpaṇa and Varṇa utkarṣa
CLXXXV
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
7. Rasa tarpaṇa and rakta puṣṭi are the major pre requisites in the enhancement of
Varṇa .These processes are aided mainly by udāna vāta, vyāna vāta, bhrājaka
pitta & rañjaka pitta
8. Varṇya upakramas does not completely change the Varṇa but they help in
modulation of physical & dermatological parameters of Varṇa to some extent.
9. Most of the drugs used had madhura tikta kaśāya rasa, snigdha guṇa, śīta vīrya,
and madhura vipāka which helps in pacifying vāta, pitta, rakta doṣa which are the
main culprits in causation of Vyaṅga.
10. In the study there was statistically highly significant improvement in the MASI
Scores but in overall assessment 64.5% patients had mild improvement. This
could be because of short intervention period.
11. Varṇya gaṇa lepa is a safe and effective formulation which can be prescribed in
Vyaṅga.
CLXXXVI
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
RECOMMENDATIONS FOR FURTHER STUDY
1. The various parameters for assessment of Varṇa needs to be tested for its
objectivity so as to evolve standard assessment parameters for Varṇa
2. An extensive study on Prabhā & Chāyā, are needed so as to differentiate and help
in conceptualization.
3. An extensive study on the Āyurvedic perspective of Transdermal Drug Delivery
System needs to be evaluated.
4. Study involving a combination of external application with oral administration of
Varṇya dravyas can be carried out to assess efficacy of combination.
5. The same study can be carried out in a larger sample size and an extended
intervention period for better accuracy in results.
6. The same formulation can be tried in other skin diseases to evaluate its effect on
the parameters such as skin hydration, skin pigmentation, skin sensitivity, skin
wrinkling.

CLXXXVII
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
SUMMARY
The present study entitled“ A Study on the concept of Varṇya vis-a vis
Clinical evaluation of Varṇya Gaṇa Lepa in Vyaṅga.” was aimed at understanding the
concept of Varṇa and Varṇya and its application in Vyaṅga in order to evaluate its
effect on pigmentation. MASI scores and other parameters were used to assess and
analyse the results.
The study had 2 components. The conceptual study included the analysis of
concept of Varṇa, and relevant concepts like Prabhā and Chāyā, Concept of Varṇya
,analysis of role of Varṇya yogas in improving the Varṇa in patients of Vyaṅga. The
Varṇa can be more likely compared with colour, texture, lustre, appearance,
nourishment (plumpness). The dermatological parameters such as Skin
hydration(Dryness-Oilyness), Skin Pigmentation (Pigmented Non pigmented) , Skin
Sensitivity( Sensitive –resistant), Skin wrinkling (Wrinkled-tight) also come under the
perview of Varṇa.The different factors influencing Varṇa, role of Varṇya yogas in
improving Varṇa, their mode of action etc were dealt in the conceptual part.
The second component of the study was a clinical study consisting of sample
size of 40 patients of Vyaṅga. All the patients were assigned to a single group
.Different parameters were used as assessment criterias . They were Skin colour,
Lesion colour, Skin texture-dryness/oilyness, Skin lustre, Number and Size of the
lesions, Darkness, Area and Homogeneity of lesion, Itching, Burning sensation,
MASI Score. Varṇya gaṇa lepa was administered for 15 days followed by same
duration of follow up. The different parameters of the study were observed and
recorded before treatment, after treatment and after the follow-up. The results were
CLXXXVIII
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
analyzed statistically based on the scores obtained from MASI and other assessment
parameters for statistical significance.
There was statistically highly significant improvement in the MASI Scores but in
overall assessment 64.5% patients had mild improvement. Clinical improvement was
more evident in Darkness parameter when compared to other parameters.
The conclusion derived on the basis of detailed observation & deep study is
submitted under the chapter on Conclusion. Future perspective of the study is
highlighted as an aid for the future research workers.

CLXXXIX
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
BIBLIOGRAPHIC REFRENCES
1. Shilpa Savalia, Process and principles of varnotpatti and assessment of the
varnaprasādana in tvakvaivranya. Department of Basic Principles IPGT &
RA.Jamnagar. 2008
2. Ashley.H.Robins.Biological Perspectives On Human Pigmentation. 1st Edition
Cambridge University Press New York 1991 PP- 211
3. Fitzpatrick TB, Quevedo WC, Szabo G, Seiji M. Biology of the melanin
pigmentary system, Dermatology in General Medicine. McGraw-Hill
Publications New York, 1971, PP 117-146.
4. Taranath Bhattacharya.Vachaspatyam, Bruhat Sanskrutabhidhanam.3rd
Edition,
Chaukhamba Sanskrit series office, Vidya Vilas Press, Varanasi 1962, Volume
6PP 4850
5. Taranath Bhattacharya.Vachaspatyam, Bruhat Sanskrutabhidhanam. 3rd
Edition,
Chaukhamba Sanskrit series office, Vidya Vilas Press, Varanasi 1962, Volume 6
PP 4850
6. Sir Monier Monier Williams. A Sanskrit English Dictionary. 1st Edition,
Motilalal Banarsidas Publishers Pvt ltd Delhi, Oxford University Press 2005 PP
924
7. Raja Radha Kanta Deva .Shabda kalpa Druma. 3rd
Edition , Chaukhambha
Sanskrit Series office, Vidya Vilas Press ,Varanasi 1967 ,Volume 4 PP 277
8. Taranath Bhattacharya. Vachaspatyam Bruhat Sanskrutabhidhanam. 3rd
Edition
Chaukhamba Sanskrit series office, Vidya Vilas Press, Varanasi 1962, Volume
6,PP 4850
9. Acharya Yadavji Trikamji.Charaka samhita .5th
Edition ,Chaukhamba Sanskrit
Sansthan ,Varanasi 2001 PP 353
10. Venimadhav Shastri Joshi. Narayana hari Joshi. Ayurvedeeya Mahakosha /
Shabdakosha Prathama khanda, Nirnay Sagar Press, Mumbai 1968 PP 725
11. Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha
Orientalia, Varanasi 2005 PP 7
12. Acharya Yadavji Trikamji- Charaka samhita 5th
Edition Chaukhamba Sanskrit
Sansthan Varanasi 2001 page 355

CXC
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
13. Taranath Bhattacharya. Vachaspatyam Bruhat Sanskrutabhidhanam. 3rd
Edition
Chaukhamba Sanskrit series office, Vidya Vilas Press, Varanasi 1962, Volume 6
PP 4850
14. Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition ,Chaukhamba Sanskrit
Sansthan ,Varanasi 2001 PP 365
15. Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan ,Varanasi 2001 PP 365
16. Acharya Yadavji Trikamji.Charaka samhita 5th
Edition Chaukhamba Sanskrit
Sansthan Varanasi 2001 PP 365
17. Kaviraj Shri Narendranath Sen Gupta, Kaviraj Shri Balaichandra Sen Gupta.
Charaka Samhita., 1st Edition, Saptati Sankhya Bhavana, Shri Rangalal Printers,
Calcutta 1850 Volume 2 PP 2154
18. Acharya Yadavji Trikamji. Charaka samhita, 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 355
19. Pandit. Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha
Sanskrit series, Varanasi 2000 PP 334
20. Vaidya Jaymini Pandey. Harita samhita. 1st edition, Chaukhambha Vishwabharati
, Varanasi 2010 PP 539
21. Pandit. Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha
Sanskrit series, Varanasi 2000 PP 334
22. Acharya Yadavji Trikamji.Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan Varanasi 2001 PP 355
23. Pandit. Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha
Sanskrit series, Varanasi 2000 PP 335
24. Taranath Bhattacharya. Vachaspatyam Bruhat Sanskrutabhidhanam., 3rd
Edition
Chaukhamba Sanskrit series office, Vidya Vilas Press, Varanasi 1962, Volume 4
PP 3401
25. Acharya Yadavji Trikamji. Charaka Samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 337
26. Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha
Orientalia, Varanasi 2005 PP 355
27. Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha
Orientalia, Varanasi 2005 PP 339
CXCI
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
28. Gaṇanath Sen Sharma Saraswati. Pratyaksha shareera :A text book of Human
Anatomy in Sanskrit, Kṛṣṇa das Academy Oriental Publishers and distributors
Varanasi 2007 Volume 1 PP 6
29. Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 337
30. Pratyaksha shareera- Gaṇanath Sen Sharma Saraswati-A text book of Human
Anatomy in Sanskrit Reprint 2007 Kṛṣṇa das Academy Oriental Publishers and
distributors Varanasi Volume 1 PP 6
31. Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha
Orientalia, Varanasi 2005 PP 355
32. Pandit Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha Sanskrit
series, Varanasi 2000 PP 274
33. Pandit Hari Sadashiva Shastri Paradakara. Astanga Hrudaya. 9th
edition,
Chaukhamba Surabharati Prakashan, Varanasi 2005 PP 406
34. Acharya Yadavji Trikamji.Suśruta Samhita. 8th
Edition, Chaukhambha
Orientalia, Varanasi 2005 PP 348
35. Acharya Yadavji Trikamji.Charaka samhita .5th
Edition, Chaukhamba Sanskrit
Sansthan Varanasi 2001 PP 320
36. Pandit Hemarajasharma Sharma. Kashyapa Samhita, Chaukambha Sanskrit
Samsthan, Varanasi 2009 PP 71
37. Pandit Hari Sadashiva Shastri Paradakara. Astanga Hrudaya. 9th
edition,
Chaukhamba Surabharati Prākāśa, Varanasi 2005 PP 371,372
38. Acharya Yadavji Trikamji-Suśruta Samhita 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 PP 348
39. Acharya Yadavji Trikamji. Charaka samhita .5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 305
40. Pandit Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha
Sanskrit series, Varanasi 2000 PP 273
41. Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha
Orientalia, Varanasi 2005 PP 348
42. Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 342

CXCII
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
43. Kaviraj Shri Narendranath Sen Gupta, Kaviraj Shri Balaichandra Sen Gupta.
Charaka Samhita., 1st Edition, Saptati Sankhya Bhavana, Shri Rangalal Printers,
Calcutta 1850 Volume 2 PP 2075, 2076
44. Acharya Yadavji Trikamji. Charaka samhita .5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 277
45. Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha
Orientalia, Varanasi 2005 PP 361
46. Pandit Hari Sadashiva Shastri Paradakara. Astanga Hrudaya. 9th
edition,
Chaukhamba Surabharati Prākāśa, Varanasi 2005 PP 402
47. Vaidya Jaymini Pandey. Harita samhita. 1st edition, Chaukhambha Vishwabharati
, Varanasi 2010 PP- 538
48. Indradev Tripathi. Raja Nighantu, 2nd
edition, Kṛṣṇadas Academy Chaukhamba
Press Varanasi 1998 PP 639
49. Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 277
50. Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan ,Varanasi 2001 PP 312
51. Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan ,Varanasi 2001 PP 305
52. Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 312
53. Pandit Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha
Sanskrit series, Varanasi 2000 PP 273
54. Pandit Hari Sadashiva Shastri Paradakara Astanga Hrudaya 9th
edition
Chaukhamba Surabharati Prākāśan 2005 PP 368
55. Pandit Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha
Sanskrit series, Varanasi 2000 PP 273
56. Acharya Yadavji Trikamji- Charaka samhita 5th
Edition Chaukhamba Sanskrit
Sansthan Varanasi 2001 page 334
57. Acharya Yadavji Trikamji- Charaka samhita 5th
Edition Chaukhamba Sanskrit
Sansthan Varanasi 2001 page 344
58. Pandit Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha
Sanskrit series, Varanasi 2000 PP 273

CXCIII
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
59. Pandit Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha
Sanskrit series, Varanasi 2000 PP 273
60. Pandit Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha
Sanskrit series, Varanasi 2000 PP 315
61. Acharya Yadavji Trikamji-Suśruta Samhita 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 page 7
62. Pandit Hari Sadashiva Shastri Paradakara Astanga Hrudaya 9th
edition
Chaukhamba Surabharati Prākāśa n 2005 PP 175
63. Acharya Yadavji Trikamji. Charaka samhita .5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 145
64. Pandit Hari Sadashiva Shastri Paradakara Astanga Hrudaya 9th
edition
Chaukhamba Surabharati Prākāśan 2005 PP 175
65. Acharya Yadavji Trikamji- Caraka samhita 5th
Edition Chaukhamba Sanskrit
Sansthan Varanasi 2001 PP 237
66. Acharya Yadavji Trikamji- Charaka samhita 5th
Edition Chaukhamba Sanskrit
Sansthan Varanasi 2001 PP 38
67. Pandit Parashuram Shastri. Śarangadhara Samhita. 7th
Edition ,Chaukhamba
orientalia Charu printers ,Golghar Varanasi 2008 PP 72,73
68. Pandit Hari Sadashiva Shastri Paradakara. Astanga Hrudaya. 9th
edition
,Chaukhamba Surabharati Prākāśan 2005 PP 193
69. Purushottama Sharma, Shareera Tatva darshana nama vātadidosha vijnana, P.S
Hirlekar. Bharateeya Ayurvidya Shikshan Samiti Amraoti. Saraswati
Mudranalaya , Shri Hanuman Vyayam Prasarak Mandal Amraoti ,1942 PP 236
70. Acharya Yadavji Trikamji- Charaka samhita 5th
Edition Chaukhamba Sanskrit
Sansthan Varanasi 2001 PP 109
71. Acharya Yadavji Trikamji-Suśruta Samhita 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 PP 101
72. Acharya Yadavji Trikamji- Charaka samhita 5th
Edition Chaukhamba Sanskrit
Sansthan Varanasi 2001 PP 278
73. Acharya Yadavji Trikamji-Suśruta Samhita 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 PP 68
74. Acharya Yadavji Trikamji-Suśruta Samhita 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 PP71

CXCIV
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
75. Leslie Baumann, Sogol Saghari, Edmund Weisberg. Cosmetic Dermatology
Principles And Practice, 2nd
edition, Mc Graw Hill Companies New York , 2009
PP 69-73
76. Sagebiel, R. W. & Odland, G. F. Ultrastructural identification of melanocytes in
early human embryos. In Pigmentation: Its Genesis and Control, New York:
Appleton-Century-Crofts, 1972 PP. 43-50.
77. Rosdahl, I. & Rorsman, H. . An estimate of the melanocyte mass in humans.
Journal of Investigative Dermatology1983, Issue 81, PP 278-8
78. Seiji, M., Fitzpatrick, T. B. & Birbeck, M. S. C. . The melanosome: a distinctive
subcellular particle of mammalian melanocytes and the site of melanogenesis.
Journal of Investigative Dermatology, 1961 Issue 36,,PP 243-52.
79. Murad Alam Ashish C. Bhatia, Faad Roopal V. Kundu Simon S. Yoo, Henry
Hin-Lee Chan, Cosmetic Dermatology For Skin Of Colour Mc Graw Hill
Publications -PP 105
80. Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 21
81. Pandit Parashuram Shastri. Śarangadhara Samhita. 7th
Edition ,Chaukhamba
orientalia Charu printers ,Golghar Varanasi 2008 PP 346
82. Pandit Parashuram Shastri. Śarangadhara Samhita. 7th
Edition ,Chaukhamba
orientalia Charu printers ,Golghar Varanasi 2008 346
83. Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 96
84. Pandit Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha
Sanskrit series, Varanasi 2000 PP 134
85. Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 152 ,174
86. Pandit Hari Sadashiva Shastri Paradakara Astanga Hrudaya 9th
edition
Chaukhamba Surabharati Prākāśan 2005 PP 58
87. Pandit Hari Sadashiva Shastri Paradakara Astanga Hrudaya 9th
edition
Chaukhamba Surabharati Prākāśan 2005 PP 926
88. Pandit Hemarajasharma Sharma. Kashyapa Samhita, Chaukambha Sanskrit
Samsthan, Varanasi 2009 PP 175 ,185
89. Brahma Shankara Mishra ed. Bhavaprākāśa , Madhyama Khanda 61/37
2nded.2005, Choukambha Orientalia PP 371

CXCV
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
90. Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 385
91. Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 480
92. Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha
Orientalia, Varanasi 2005 PP 397
93. Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 24
94. Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha
Orientalia, Varanasi 2005 PP 385
95. Aaron Tabor and Robert M. Blair. Nutritional Cosmetics: Beauty from Within
,1st edition, William Andrew Publications, United States of America 2009 PP 13
96. Leslie Baumann , Sogol Saghari, Edmund Weisberg. Cosmetic Dermatology
Principles And Practice, 2nd
edition, Mc Graw Hill Companies New York , 2009
PP 45-62
97. Paul Kelly Susan C. Taylor - Dermatology for Skin of Colour. Mc Graw hill
companies, New York 2009 PP 45- 65
98. Klauss Wolff, Lowel A Goldsmith ,Stephen I Katz. Fitzpatrick‟s dermatology in
General Medicine. 7th
edition ,Mc graw Hill Companies , Unites States of
America
99. Lindy P. Fox, Hans F. Merk, ,David R. Bickers. Dermatological Pharmacology. -
Good Man And Gillmans Pharmacology
100. Acharya Yadavji Trikamji Charaka Samhita 5th EditionVaranasi Chaukhamba
Sanskrit Samsthan 2001 PP 50
101. Acharya Yadavji Trikamji Charaka Samhita 5th EditionVaranasi Chaukhamba
Sanskrit Samsthan 2001 PP-107
102. Acharya Yadavji Trikamji Charaka Samhita 5th EditionVaranasi Chaukhamba
Sanskrit Samsthan 2001 PP-49
103. Acharya Yadavji.Trikamji Suśruta Samhita 8th
Edition Varanasi Chaukhamba
Orientalia, 2005 PP-324
104. Pdt. Harish Shastri ed. Astanga Hridaya, Uttara tantra, 31/29, 2nd
ed. 2000,
Kṛṣṇadas Āyurveda series, Varanashi, PP 889.
105. Yadunandan Upadhyaya ed. Madhava Nidāna, 55/ 39, 31st ed. 2002,
Choukambha Sanskrit series, Varanashi, PP210.

CXCVI
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
106. Brahma Shankara Mishra ed. Bhavaprākāśa , Madhyama Khanda 61/37
2nded.2005, Choukambha Orientalia PP 588
107. Indradev Tripati ed. Yoga Ratnakar , kshudrarogadhikar /42,43 1st ed. 1998,
Choukambha orientalia, PP 695
108. Pdt. Shivprasad Sharma. Aṣṭāṅga saṁgraha , Uttara tantra, 36/29,2nd
ed. 2000,
Varanashi, pp Choukambha Sanskrit series, PP 815.
109. Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha
Orientalia, Varanasi 2005 PP 324
110. Acharya Yadavji.Trikamji Suśruta Samhita 8th
Edition Varanasi Chaukhamba
Orientalia, 2005 PP-323
111. Pdt. K. R. Shrikantha Murthy, Aṣṭāṅga saṁgraha , Uttara tantra, 37/26,29,33,1st
ed. 1996, Choukambha orientalia, PP 325,326.
112. Dr.Ambikadatt Shastri ed. Suśruta Cikitsā, vol- 1, 30/33, 2nded. 2005,
Choukambha,publication,Varanashi, PP 94.
113. Dr.Ambikadatt Shastri ed. Suśruta Cikitsā, vol- 1, 20/34,36, 2nded. 2005,
Choukambha,publication,Varanashi, PP 94.
114. Wade TR, Wade SL, Jones HE. Skin changes and diseases associated with
pregnancy. Obstet Gynecol 1978 52:233–242
115. Katiyar Shweta , Saify Khozema , Rai Meenu , Sharma Anupama , Singh S.K. ,
Singh Neelima A Systemic Review on Melasma: International Journal of Current
Biological and Medical Science- A Review 2011; 1(2): 63 – 68. Journal home:
www.currentscidirect.com
116. R. G. Valia. Text book of Dermatology, 1st edition, Bhalan Publication House,
1994,Volume 1 PP 552.
117. Paul Kelly Susan C. Taylor - Dermatology for Skin of Colour Mc Graw hill
companies PP 332
118. Acharya Priyavrat Sharma. Dravya Guna Vijnana.2nd
edition, Chaukhambha
Bharati Academy Varanasi, 2005 Volume 2 PP 43, 114, 253, 580, 715, 738, 786,
798, 800
119. Pandit Parashuram Shastri. Śarangadhara Samhita. 7th
Edition ,Chaukhamba
orientalia Charu printers ,Golghar Varanasi 2008 PP 355
120. Kaviraj Shri Narendranath Sen Gupta, Kaviraj Shri Balaichandra Sen Gupta.
Charaka Samhita., 1st Edition, Saptati Sankhya Bhavana, Shri Rangalal Printers,
Calcutta 1850 Volume 2 PP 2204

CXCVII
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
121. Purushottama Sharma, Shareera Tatva darshana nama vātadidosha vijnana, P.S
Hirlekar. Bharateeya Ayurvidya Shikshan Samiti Amraoti. Saraswati
Mudranalaya , Shri Hanuman Vyayam Prasarak Mandal Amraoti ,1942 276
122. Acharya Yadavji Trikamji Charaka Samhita 5th EditionVaranasi Chaukhamba
Sanskrit Samsthan 2001 PP 249
123. Purushottama Sharma, Shareera Tatva darshana nama vātadidosha vijnana, P.S
Hirlekar. Bharateeya Ayurvidya Shikshan Samiti Amraoti. Saraswati
Mudranalaya , Shri Hanuman Vyayam Prasarak Mandal Amraoti ,1942 PP 275,
276
124. Purushottama Sharma, Shareera Tatva darshana nama vātadidosha vijnana, P.S
Hirlekar. Bharateeya Ayurvidya Shikshan Samiti Amraoti. Saraswati
Mudranalaya , Shri Hanuman Vyayam Prasarak Mandal Amraoti ,1942 PP 287
125. Acharya Yadavji Trikamji-Sushruta Samhita 8th
Edition, Chaukhambha
Orientalia, Varanasi 2005 PP 101
126. Purushottama Sharma, Shareera Tatva darshana nama vātadidosha vijnana, P.S
Hirlekar. Bharateeya Ayurvidya Shikshan Samiti Amraoti. Saraswati
Mudranalaya , Shri Hanuman Vyayam Prasarak Mandal Amraoti ,1942 PP 243
127. Grimes PE, Yamada N, Bhawan J. Light microscopic, immunohistochemical, and
ultrastructural alterations in patients with melasma. Am J Dermatopathol.
2005;27: 96-101.
128. Vazquez M, Maldonado H, Benmaman C, Sanchez JL. Melasma in Men: a
clinical and histological study. Int J Dermatol 1988 27: 25-7
129. Dominguez AR, Balkṛṣṇan R, Ellzey AR, Pandya AG. Melasma in Latina
patients: cross-cultural adaptation and validation of a quality-of-life questionnaire
in Spanish language. J Am Acad Dermatol. 2006;55:59-66.
130. Wade TR, Wade SL, Jones HE .Skin changes and diseases associated with
pregnancy. Obstet Gynecol 1978 52:233–242
131. Wong RC, Ellis CN Physiologic skin changes in pregnancy. J Am Acad
Dermatology 1984 10:929–940
132. Errickson CV, Matus NR. Skin disorders of pregnancy. Am Fam Physician 1994
49:605–610
133. Parmley T, O‟Brien TJ. Skin changes during pregnancy. Clin Obstet Gynecol
1990 33: PP 713–717

CXCVIII
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
134. Mallick S, Singh SK, Sarkar C et al (2005) Human placental lipid induces
melanogenesis by increasing the expression of tyrosinase and its related proteins
in vitro. Pigment Cell Res 18:25–33
135. Rakesh K.Sindhu, Upma et al. Santalum album linn: a review on morphology,
phytochemistry and pharmacological aspects, IJPRIF Jan-Mar 2010 Vol.2, No.1,
PP 914-919
136. Narong Chomchalow. The Utilization of Vetiver as Medicinal and Aromatic
Plants with Special Reference to Thailand . Curtis 1996
137. Satheesh George, K. V Tushar et al. Hemidesmus indicus (L).R.Br. A Review,
Journal of Plant sciences 2002 , Issue 3(2) PP 146-156
138. Pandit Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha
Sanskrit series, Varanasi 2000 PP 136
139. Acharya Yadavji Trikamji-Sushruta Samhita 8th
Edition, Chaukhambha
Orientalia, Varanasi 2005 PP 85, 86
140. Acharya Yadavji.Trikamji Suśruta Samhita 8th
Edition Varanasi Chaukhamba
Orientalia, 2005 PP 84
CXCIX
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
ANNEXURE- CASE SHEET
DEPARTMENT OF POST GRADUATE STUDIES IN AYURVEDA SIDDHANTA
GOVERNMENT AYURVEDA MEDICAL COLLEGE,
MYSORE.
“A STUDY ON THE CONCEPT OF VARNYA VIS-À-VIS CLINICAL
EVALUATION OF EFFICACY OF VARNYA GANA LEPA IN VYANGA”
HEAD OF THE DEPARTMENT : Dr. Naseema Akhtar M.D. (Ayu)
GUIDE : Dr. Balakrishna D .L. M.D. (Ayu)
CO-GUIDE : Dr. Vasudev Anandrao Chate M.D. (Ayu)
RESEARCHER : Dr. Pallavi.G BAMS
Case No: Date:
Name of the patient : O.P.D. No:
Age : I.P.D No:
Sex : Ward. No.
Religion : Bed .No.
Education : Date of
Commencement: Occupation
Dateof Completion:
Socioeconomic status :
Marital Status :
Address :
Phone No:

CC
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
1. Chief complaints Duration
Vaivarnya (Shyaava)
Mandala
Others
2. Associated complaints
3. History of present illness
Aggravating factors:
Specific foods-
Physical :
Exposure to sunrays Heat
Cold Chemical contact
Frequent cleaning Rubbing
Excessive air Excessive work
Others
Pschychological
Krodha (anger) Harsha
Bhaya (fear) Chinta (Worries)
Shoka (Sorrow) Khinnata (Depression)
Others
H/o of use of cosmetics:
Chemical /Herbal
Frequency of use
Duration of use

CCI
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
Drug and Contraceptive history
4. History of past illness :
5. Family history :
6. Personal history :
a. Diet : ( ) Veg / ( ) Mixed
Frequency :
b. Ashana Prakara : Samasana / Visamasana / Adhyasana / Virudhasana
c. Pradhana rasa :
d. Appetite: Poor / Moderate / Good / Extreme
e. Sleep:
Nature: Satisfactory/ Unsatisfactory
Duration: Day: Night:
f. Habits- Coffee /Tea / Smoking / Alcohol/ Tobacco / Others
7. Occupational History
Nature of work:
Working conditions:
Working Hours:
Other Details:
8.Menstrual History :
Regularity : Reg. / Irreg.
Quantity : Scanty / Moderate / Excessive
Duration : ____days
Interval :_____ days

CCII
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
Asso. symps. :
Age of menarche :
Age of Menopause
9. Obstetric History :
No of pregnancies : ________ F.T.N.D/Ceaserian
GPALD
History of Hysterctomy, Tubectomy/Any other surgeries
10. Samanya Pareeksha
Asta sthaana Pareeksha
a. Nadi:
b. Mutra:
c. Mala:
d. Jihwa:
e. Shabda:
f. Sparsha:
g. Drik:
h. Akriti:
DashaVidha Pareeksha
Prakriti:-
Vikriti:
Sara: Pravara/ Madhyama/Avara
Sattva:- Pravara/ Madhyama/Avara
Samhanana:- Pravara/ Madhyama/Avara
Saatmya:- Pravara/ Madhyama/Avara
Ahara Shakti:- Pravara/ Madhyama/Avara
o Agni: Sama/Vishama/Manda/Teekshna
o Abhyavarana Shakti: Pravara( ) Madhyama( ) Avara( )
o Jarana Shakti: Pravara( ) Madhyana( ) Avara( )
o Koshtha: Mrudu( ) Madhyama( ) Krura( )
Vyayama Shakti: Pravara/ Madhyama/Avara
CCIII
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
Pramana:
Vaya : Bala/Madhyama/Vruddha
11. Vishesha Pareeksha
Anana
Darshana Pareeksha
Vyakta Sthana
Cheek-
Forehead-
Temporal region-
Nasal region-
Varna
Mandala Ayama (Pramana) – No of lesions____ Dimensions in _________cm
Lustre
Sparshana Pareeksha
Snigdha-Ruksha
Ushna-Sheeta
Sensory Examination
Touch sensation: Pain:
Pressure: Temperature:

CCIV
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
12. Chikitsa –
Bahya- Lepana chikitsa
Yoga- Varnya Gana lepa
Purvakarma- Patient is asked to wash face with luke warm water using chickpea
(Besan) flour.
Pradhana karma- Varnya Gana Lepa churna is mixed with appropriate quantity of
water and made into thick paste and applied externally on the affected areas.
Quantity- Quantity sufficient
Duration of each application-Retained until it gets dried.
Pashchat karma- After the lepa dries ,patient is asked to wash the face with luke
warm water.
Duration-15days, twice daily (morning and evening), From _________to
___________
Follow up-15days , From________to _________
Pathya- Avoid chemicals, soaps and patient is advised to use chickpea flour for
facewash.
Apathya- Exposure to sunlight
SIGNATURE OF RESEARCHER SIGNATURE OF OBSERVER
CCV
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
Scoring Systems
Visual assessment remains one of the „„gold standard‟‟ methods of assessing
skin color and a number of tools are currently available to reduce the inter observer
variability Dermatologists have the privilege of examining the largest organ of the
body. However unlike other organs, there are hardly any tests of clinical significance
that measure skin function. In dermatological practice methods of evaluating the
severity of skin diseasesare often crude, subjective and not reproducible, which
creates discrepancy in results and inter- individual variations. Hence to maintain
objectivity in observations,and to quantify the subsequent changes following
treatment, scores are used to evaluate the severity of skin diseases.
This is particularly important for monitoring the response to therapy and for
evaluating the efficacy of new drugs. Over the years scoring systems have been
developed for number of skin diseases. One among them is the Melasma Area
Severity Index (MASI) which has helped the cause of clinical practice and clinical
Research.
Melasma Area and Severity Index MASI
Melasma as already described, is a common, persistent disorder of
hyperpigmentation affecting a significant portion of the population, Conventional
treatment of melasma includes elimination of any causative factors coupled with the
use of sunscreens and hypopigmenting agents, often in combination with other
therapies. Despite the availability of these measures, melasma is often recalcitrant to
treatment and frustrating for both patients and clinicians. To develop new agents for
melasma, valid and reliable outcome measures are critical to determining clinical
severity of disease and the significance of treatment results when performing clinical
trials. These outcome measures should be easy to learn, responsive, inexpensive, and
applicable worldwide. Unfortunately, no such measure exists for melasma The
Melasma Area and Severity Index (MASI), an outcome measure developed to provide
a more accurate quantification of the severity of melasma and changes during therapy,
was developed by Kimbrough-Green et al,who based it on a similar scoring system
devised for psoriasis

206
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
The MASI score is calculated by subjective assessment of 3 factors:
Area (A) of involvement, Darkness (D), and Homogeneity (H),
Forehead(f), - 30%,
Right malar region (rm),- 30%,
Left malar region (lm), 30%, and
Chin (c), 10%
The MASI score is calculated by adding the sum of the severity ratings for darkness
and homogeneity, multiplied by the value of the area of involvement, for each of the 4
facial areas:
MASI total score
=0.3A (f)[D(f)+H(f)]+ 0.3A (lm) [D(lm)+H(lm)] + 0.3A(rm) [D(rm)+H(rm)] + 0.1A
(c) [D(c)+H(c) ]
The total score range is 0 to 48.
Grades of Assessment
The area of involvement Darkness
Homogeneity
0 = no involvement;
0 = absent
0 = absent
1 =10%
1 = slight
1 = slight
2 = 10%-29%
2 = mild
2 = mild
3 =30%-49%
3 =marked
3 =marked
4 = 50%-69%
4 = maximum
4 = maximum
5 = 70%-89%
6 = 90%- 100%.

CCVII
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
MASTER CHART

CCVIII
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga

CCIX
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga

CCX
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga

CCXI
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
Key to Master Chart
1. SL.NO- Serial No
2. Age- 21-30yrs- 1
31-40yrs- 2
41-50yrs- 3
51-60yrs- 4
3. Sex Male- 1
Female- 2
4. Religion Hindu- 1
Muslim- 2
Christian- 3
5. Education Primary School- 1
Middle School- 2
High School-PUC-3
Graduate- 4
Post Graduate- 5
6. Socio-economic status-
Lower Middle Class-1
Middle Class- 2
Upper Middle Class-3
Rich Class- 4
7. Marital Status Married- 1 Unmarried- 2
8. Nature of work
Hard Manual- 1
Mild manual work- 2
Moderate manual work-3
Sedentary work- 4
9. Diet Mixed-diet- 1
Vegetarian- 2

212
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
10. Appetite
Poor- 1
Moderate- 2
Good- 3
Extreme- 4
11. Agni
Samagni- 1
Mandagni- 2
Teekshnagni 3
Vishamagni- 4
12. Koshtha
Mrudu Koshtha- 1
Madhyama koshtha- 2
Krura Koshtha 3
13. Sleep
Satisfactory- 1
Unsatisfactory-2
14. Bowel Habits (B.H)
Regular- 1
Irregular- 2
15. Family History (F.H)
Present- 1
Absent- 2
16. Contraceptive History (C.H)
Present- 1
Absent- 2
17. Aggravating Factors
a. Physical Aggravating Factors
Sun rays- 1
Chemical contact- 2
213
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
Excessive work- 3
Multiple Agg Fact- 4
Nothing specific- 5
b. Psychological Aggtng Factors
Chinta- 1
Shoka- 2
Khinnata- 3
Any2 or all 3- 4
Nothing specific- 5
18. Use of Cosmetics
a. Soap
Lifeboy- 1
Others(Santoor Lux etc)- 2
Multiple (Keeps Changing)-3
b. Creams
Fair and Lovely- 1
Others- 2
Multiple- 3
Do not Use creams- 4
19. Menstrual History
a. Regularity
Regular- 1
Irregular- 2
b. Age of Menopause
Attained- 1
Not attained- 2
Not Applicable- 3
20. Prakriti
VATA, pitta,kapha- 1
PITTA, kapha, vata- 2
KAPHA, pitta, vata- 3

214
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
21. Sattva
Pravara- 1
Madhyama- 2
Avara- 3
22. Sara
Pravara- 1
Madhyama- 2
Avara- 3
23. Skin Colour 1-26 Grades
24. Lesion Colour
BT-Before Treatment
AT-After Treatment
FU-Follow up
25. No of Lesions
1-2- 1
2-4- 2
4-6- 3
>6 4
26. Size of Lesions
0-2cm-1
2-4cm-2
4-6cm-3
>6cm-4
27. Pattern
Centro facial- 1
Malar- 2
Mandibular- 3
28. Level of Lesion
Dermal- 1
Epidermal- 2
29. Skin Lustre

215
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
Poor Lustre- 1
Mild Lustre- 2
Moderate Lustre- 3
Good Lustre- 4
30. Chronicity
0-4 years- 1
4-8 years- 2
>8 years- 3
31. Area of Discolouration
0%- No involvement
<10%- 1 Af-Area Frontal
10-29%-2 Alm-Area Left Malar
30-49%-3 Arm-Area Rt Malar
50-69%-4 Ac-Area Chin
70-89%-5
90-100%-6
32. Darkness of Discolouration
Absent-0 Df-Darkness frontal
Slight- 1 Dlm-Darkness lft Malar
Mild-2 Drm-Darkness Rt Malar
Marked-3 Dc- Darkness Chin
Maximum-4
33. Homogenesity of Discolouration
Absent-0 Hf- Hmgnsity frontal
Slight-1 Hlm- Hmgnsity lft Malar
Mild-2 Hrm- Hmgnsity Rt Malar
Marked-3 Hc- Hmgnsity Chin
Maximum-4
34. MASI Score- 1-48
35. Skin Texture
Dryness/Oiliness

216
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
Absent- 0
Mild- 1
Moderate- 2
Severe- 3
36. Other Symptoms
a. Itching
No itching- 0
Mild Itching- 1
Moderate itching- 2
Severe itching- 3
b. Burning Sensation
No burning - 0
Mild Burning- 1
Moderate Burning- 2
Severe Burning- 3

217
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
1
Shilpa Savalia, Process and principles of varnotpatti and assessment of the
varnaprasādana in tvakvaivranya. Department of Basic Principles IPGT & RA.Jamnagar.
2008 2
Ashley.H.Robins.Biological Perspectives On Human Pigmentation. 1st Edition
Cambridge University Press New York 1991 PP- 211 3 Fitzpatrick TB, Quevedo WC, Szabo G, Seiji M. Biology of the melanin pigmentary
system, in Fitzpatrick TB et al (eds), Dermatology in General Medicine. New York,
McGraw-Hill, 1971, PP 117-146. 4
Taranath Bhattacharya.Vachaspatyam, Bruhat Sanskrutabhidhanam.3rd
Edition,
Chaukhamba Sanskrit series office, Vidya Vilas Press, Varanasi 1962, Volume 6PP 4850 5
Taranath Bhattacharya.Vachaspatyam, Bruhat Sanskrutabhidhanam. 3rd
Edition,
Chaukhamba Sanskrit series office, Vidya Vilas Press, Varanasi 1962, Volume 6 PP 4850 6 Sir Monier Monier Williams. A Sanskrit English Dictionary. 1
st Edition, Motilalal
Banarsidas Publishers Pvt ltd Delhi, Oxford University Press 2005 PP 924 7 Raja Radha Kanta Deva .Shabda kalpa Druma. 3
rd Edition , Chaukhambha Sanskrit
Series office, Vidya Vilas Press ,Varanasi 1967 ,Volume 4 PP 277 8
Taranath Bhattacharya. Vachaspatyam Bruhat Sanskrutabhidhanam. 3rd
Edition
Chaukhamba Sanskrit series office, Vidya Vilas Press, Varanasi 1962, Volume 6,PP 4850 9 Acharya Yadavji Trikamji.Charaka samhita .5
th Edition ,Chaukhamba Sanskrit Sansthan
,Varanasi 2001 PP 353 10
Venimadhav Shastri Joshi. Narayana hari Joshi. Ayurvedeeya Mahakosha /
Shabdakosha Prathama khanda, Nirnay Sagar Press, Mumbai 1968 PP 725 11
Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 PP 7 12
Acharya Yadavji Trikamji- Charaka samhita 5th
Edition Chaukhamba Sanskrit Sansthan
Varanasi 2001 page 355 13
Taranath Bhattacharya. Vachaspatyam Bruhat Sanskrutabhidhanam. 3rd
Edition
Chaukhamba Sanskrit series office, Vidya Vilas Press, Varanasi 1962, Volume 6 PP 4850 14
Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition ,Chaukhamba Sanskrit
Sansthan ,Varanasi 2001 PP 365 15
Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan ,Varanasi 2001 PP 365 16
Acharya Yadavji Trikamji.Charaka samhita 5th
Edition Chaukhamba Sanskrit Sansthan
Varanasi 2001 PP 365

218
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
17
Kaviraj Shri Narendranath Sen Gupta, Kaviraj Shri Balaichandra Sen Gupta. Charaka
Samhita., 1st Edition, Saptati Sankhya Bhavana, Shri Rangalal Printers, Calcutta 1850
Volume 2 PP 2154 18
Acharya Yadavji Trikamji. Charaka samhita, 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 355 19
Pandit. Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd Edition, Chaukambha Sanskrit
series, Varanasi 2000 PP 334 20
Hareeta samhita 21
Pandit. Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd Edition, Chaukambha Sanskrit
series, Varanasi 2000 PP 334 22
Acharya Yadavji Trikamji.Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan Varanasi 2001 PP 355 23
Pandit. Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd Edition, Chaukambha Sanskrit
series, Varanasi 2000 PP 335 24
Taranath Bhattacharya. Vachaspatyam Bruhat Sanskrutabhidhanam., 3rd
Edition
Chaukhamba Sanskrit series office, Vidya Vilas Press, Varanasi 1962, Volume 4 PP 3401 25
Acharya Yadavji Trikamji. Charaka Samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 337 26
Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 PP 355 27
Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 PP 339 28
Gaṇanath Sen Sharma Saraswati. Pratyaksha shareera :A text book of Human Anatomy
in Sanskrit, Kṛṣṇa das Academy Oriental Publishers and distributors Varanasi 2007
Volume 1 PP 6 29
Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 337 30
Pratyaksha shareera- Gaṇanath Sen Sharma Saraswati-A text book of Human Anatomy
in Sanskrit Reprint 2007 Kṛṣṇa das Academy Oriental Publishers and distributors
Varanasi Volume 1 PP 6 31
Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 PP 355 32
Pandit Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd Edition, Chaukambha Sanskrit
series, Varanasi 2000 PP 274 33
Pandit Hari Sadashiva Shastri Paradakara. Astanga Hrudaya. 9th
edition, Chaukhamba
Surabharati Prākāśa, Varanasi 2005 PP 406 34
Acharya Yadavji Trikamji.Suśruta Samhita. 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 PP 348 35
Acharya Yadavji Trikamji.Charaka samhita .5th
Edition, Chaukhamba Sanskrit
Sansthan Varanasi 2001 PP 320 36
Pandit Hemarajasharma Sharma. Kashyapa Samhita, Chaukambha Sanskrit Samsthan,
Varanasi 2009 PP 71 37
Pandit Hari Sadashiva Shastri Paradakara. Astanga Hrudaya. 9th
edition, Chaukhamba
Surabharati Prākāśa, Varanasi 2005 PP 371,372 38
Acharya Yadavji Trikamji-Suśruta Samhita 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 PP 348

219
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
39
Acharya Yadavji Trikamji. Charaka samhita .5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 305 40
Pandit Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha Sanskrit
series, Varanasi 2000 PP 273 41
Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 PP 348 42
Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 342 43
Kaviraj Shri Narendranath Sen Gupta, Kaviraj Shri Balaichandra Sen Gupta. Charaka
Samhita., 1st Edition, Saptati Sankhya Bhavana, Shri Rangalal Printers, Calcutta 1850
Volume 2 PP 2075, 2076 44
Acharya Yadavji Trikamji. Charaka samhita .5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 277 45
Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 PP 361 46
Pandit Hari Sadashiva Shastri Paradakara. Astanga Hrudaya. 9th
edition, Chaukhamba
Surabharati Prākāśa, Varanasi 2005 PP 402 47
Hariita samhita 48
Indradev Tripathi. Raja Nighantu, 2nd
edition, Kṛṣṇadas Academy Chaukhamba Press
Varanasi 1998 PP 639 49
Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 277 50
Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan ,Varanasi 2001 PP 312 51
Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan ,Varanasi 2001 PP 305 52
Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 312 53
Pandit Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha Sanskrit
series, Varanasi 2000 PP 273 54
Pandit Hari Sadashiva Shastri Paradakara Astanga Hrudaya 9th
edition Chaukhamba
Surabharati Prākāśan 2005 PP 368 55
Pandit Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha Sanskrit
series, Varanasi 2000 PP 273 56
Acharya Yadavji Trikamji- Charaka samhita 5th
Edition Chaukhamba Sanskrit Sansthan
Varanasi 2001 page 334 57
Acharya Yadavji Trikamji- Charaka samhita 5th
Edition Chaukhamba Sanskrit Sansthan
Varanasi 2001 page 344 58
A,s 273 59
A,s 273 60
Pandit Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha Sanskrit
series, Varanasi 2000 PP 315 61
Acharya Yadavji Trikamji-Suśruta Samhita 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 page 7 62
Pandit Hari Sadashiva Shastri Paradakara Astanga Hrudaya 9th
edition Chaukhamba
Surabharati Prākāśa n 2005 PP 175

220
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
63
Acharya Yadavji Trikamji. Charaka samhita .5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 145 64
Pandit Hari Sadashiva Shastri Paradakara Astanga Hrudaya 9th
edition Chaukhamba
Surabharati Prākāśan 2005 PP 175 65
Acharya Yadavji Trikamji- Caraka samhita 5th
Edition Chaukhamba Sanskrit Sansthan
Varanasi 2001 PP 237 66
Acharya Yadavji Trikamji- Charaka samhita 5th
Edition Chaukhamba Sanskrit Sansthan
Varanasi 2001 page 38 67
Pandit Parashuram Shastri. Śarangadhara Samhita. 7th
Edition ,Chaukhamba orientalia
Charu printers ,Golghar Varanasi 2008 PP 72-73 68
Pandit Hari Sadashiva Shastri Paradakara. Astanga Hrudaya. 9th
edition ,Chaukhamba
Surabharati Prākāśan 2005 PP 193 69
Purushottama Sharma- Shareera Tatva darshana nama vātadidosha vijnana –published
by P.S Hirlekar. Bharateeya Ayurvidya Shikshan Samiti Amraoti(Berar) . Printed by T.M
Patil Manager Saraswati Mudranalaya of Shri Hanuman Vyayam Prasarak Mandal
Amraoti 1942 uttarardha page 236 2nd
darshana 70
Acharya Yadavji Trikamji- Charaka samhita 5th
Edition Chaukhamba Sanskrit Sansthan
Varanasi 2001 page 109 71
Acharya Yadavji Trikamji-Suśruta Samhita 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 page 101 72
Acharya Yadavji Trikamji- Charaka samhita 5th
Edition Chaukhamba Sanskrit Sansthan
Varanasi 2001 page 278 73
Acharya Yadavji Trikamji-Suśruta Samhita 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 page 68 74
Acharya Yadavji Trikamji-Suśruta Samhita 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 page 71 75
Leslie Baumann , Sogol Saghari, Edmund Weisberg. Cosmetic Dermatology Principles
And Practice, 2nd
edition, Mc Graw Hill Companies New York , 2009 PP 69-73 76
Sagebiel, R. W. & Odland, G. F. Ultrastructural identification of melanocytes in early
human embryos. In Pigmentation: Its Genesis and Control, New York: Appleton-
Century-Crofts, 1972 PP. 43-50. 77
Rosdahl, I. & Rorsman, H. . An estimate of the melanocyte mass in humans. Journal of
Investigative Dermatology1983, Issue 81, PP 278-8 78
Seiji, M., Fitzpatrick, T. B. & Birbeck, M. S. C. . The melanosome: a distinctive
subcellular particle of mammalian melanocytes and the site of melanogenesis. Journal of
Investigative Dermatology, 1961 Issue 36,,PP 243-52. 79
Murad Alam Ashish C. Bhatia, Faad Roopal V. Kundu Simon S. Yoo, Henry Hin-Lee
Chan, Cosmetic Dermatology For Skin Of Colour Mc Graw Hill Publications -PP 105 80
Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 21 81
Pandit Parashuram Shastri. Śarangadhara Samhita. 7th
Edition ,Chaukhamba orientalia
Charu printers ,Golghar Varanasi 2008 PP 346 82
Pandit Parashuram Shastri. Śarangadhara Samhita. 7th
Edition ,Chaukhamba orientalia
Charu printers ,Golghar Varanasi 2008 346

221
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
83
Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 96 84
Pandit Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha Sanskrit
series, Varanasi 2000 PP 134 85
(Ca.Sū.27/3 & 349). 86
Pandit Hari Sadashiva Shastri Paradakara Astanga Hrudaya 9th
edition Chaukhamba
Surabharati Prākāśan 2005 PP 58, 87
Pandit Hari Sadashiva Shastri Paradakara Astanga Hrudaya 9th
edition Chaukhamba
Surabharati Prākāśan 2005 PP 926 88
Pandit Hemarajasharma Sharma. Kashyapa Samhita, Chaukambha Sanskrit Samsthan,
Varanasi 2009 PP 175 ,185 89
Brahma Shankara Mishra ed. Bhavaprākāśa , Madhyama Khanda 61/37 2nded.2005,
Choukambha Orientalia PP 371 90
Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 385 91
Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 480 92
Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 PP 397 93
Acharya Yadavji Trikamji. Charaka samhita. 5th
Edition, Chaukhamba Sanskrit
Sansthan, Varanasi 2001 PP 24 94
Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 PP 385 95
Aaron Tabor and Robert M. Blair. Nutritional Cosmetics: Beauty from Within ,1st
edition, William Andrew Publications, United States of America 2009 PP 13 96
Leslie Baumann , Sogol Saghari, Edmund Weisberg. Cosmetic Dermatology Principles
And Practice, 2nd
edition, Mc Graw Hill Companies New York , 2009 PP 45-62 97
A. Paul Kelly Susan C. Taylor - Dermatology for Skin of Colour Mc Graw hill
companies PP 45- 65 98
Klauss Wolff, Lowel A Goldsmith ,Stephen I Katz. Fitzpatrick‟s dermatology in
General Medicine. 7th
edition ,Mc graw Hill Companies , Unites States of America 99
Lindy P. Fox, Hans F. Merk, And David R. Bickers. Dermatological Pharmacology. -
Good Man And Gillmans Pharmacology 100
Acharya Yadavji Trikamji Charaka Samhita 5th EditionVaranasi Chaukhamba
Sanskrit Samsthan 2001 PP 50 101
Acharya Yadavji Trikamji Charaka Samhita 5th EditionVaranasi Chaukhamba
Sanskrit Samsthan 2001 PP-107 102
Acharya Yadavji Trikamji Charaka Samhita 5th EditionVaranasi Chaukhamba
Sanskrit Samsthan 2001 PP-49 103
Acharya Yadavji.Trikamji Suśruta Samhita 8th Edition Varanasi Chaukhamba
Orientalia, 2005 PP-324 104
Pdt. Harish Shastri ed. Astanga Hridaya, Uttara tantra, 31/29, 2nd ed. 2000, Kṛṣṇadas
Āyurveda series, Varanashi, pp 889. 105
Yadunandan Upadhyaya ed. Madhava Nidāna, 55/ 39, 31st ed. 2002, Choukambha
Sanskrit series, Varanashi, pp 210.

222
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
106
Brahma Shankara Mishra ed. Bhavaprākāśa , Madhyama Khanda 61/37 2nded.2005,
Choukambha Orientalia pp 588 107
Indradev Tripati ed. Yoga Ratnakar , kshudrarogadhikar /42,43 1st ed. 1998,
Choukambha orientalia, pp 695 108
Pdt. Shivprasad Sharma. Aṣṭāṅga saṁgraha , Uttara tantra, 36/29,2nd ed. 2000,
Varanashi, pp Choukambha Sanskrit series, pp 815. 109
Acharya Yadavji Trikamji. Suśruta Samhita. 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 PP 324 110
Acharya Yadavji.Trikamji Suśruta Samhita 8th Edition Varanasi Chaukhamba
Orientalia, 2005 PP-323 111
Pdt. K. R. Shrikantha Murthy, Aṣṭāṅga saṁgraha , Uttara tantra, 37/26,29,33,1st ed.
1996, Choukambha orientalia, pp 325,326. 112
Dr.Ambikadatt Shastri ed. Suśruta Cikitsā, vol- 1, 30/33, 2nded. 2005,
Choukambha,publication,Varanashi, pp 94. 113
Dr.Ambikadatt Shastri ed. Suśruta Cikitsā, vol- 1, 20/34,36, 2nded. 2005,
Choukambha,publication,Varanashi, pp 94. 114
Wade TR, Wade SL, Jones HE (1978) Skin changes and diseases associated with
pregnancy. Obstet Gynecol 52:233–242 115
Katiyar Shweta , Saify Khozema , Rai Meenu , Sharma Anupama , Singh S.K. , Singh
Neelima A Systemic Review on Melasma: International Journal of Current Biological
and Medical Science- A Review 2011; 1(2): 63 – 68. Journal home:
www.currentscidirect.com 116
R. G. Valia. Text book of Dermatology, 1st edition, Bhalan Publication House, 1994
,Volume 1 PP 552. 117
A. Paul Kelly Susan C. Taylor - Dermatology for Skin of Colour Mc Graw hill
companies PP 332 118
Acharya Priyavrat Sharma. Dravya Guna Vijnana.2nd
edition, Chaukhambha Bharati
Academy Varanasi, 2005 Volume 2 PP 43, 114, 253, 580, 715, 738, 786, 798, 800 cxix
Pandit Parashuram Shastri. Śarangadhara Samhita. 7th
Edition ,Chaukhamba orientalia
Charu printers ,Golghar Varanasi 2008 PP 355 cxx
Kaviraj Shri Narendranath Sen Gupta, Kaviraj Shri Balaichandra Sen Gupta. Charaka
Samhita., 1st Edition, Saptati Sankhya Bhavana, Shri Rangalal Printers, Calcutta 1850
Volume 2 PP 2204 121
Purushottama Sharma.Shareera Tatva darshana nama vatadidosha vijnana. published
by P.S Hirlekar. Bharateeya Ayurvidya Shikshan Samiti Amraoti (Berar) . Printed by
T.M Patil Manager Saraswati Mudranalaya of Shri Hanuman Vyayam Prasarak Mandal
Amraoti 1942 PP 276 122
Charaka vimana 5th
chapter 123
Purushottama Sharma.Shareera Tatva darshana nama vatadidosha vijnana. published
by P.S Hirlekar. Bharateeya Ayurvidya Shikshan Samiti Amraoti (Berar) . Printed by
T.M Patil Manager Saraswati Mudranalaya of Shri Hanuman Vyayam Prasarak Mandal
Amraoti 1942 PP 124
Purushottama Sharma.Shareera Tatva darshana nama vatadidosha vijnana. published
by P.S Hirlekar. Bharateeya Ayurvidya Shikshan Samiti Amraoti (Berar) . Printed by
T.M Patil Manager Saraswati Mudranalaya of Shri Hanuman Vyayam Prasarak Mandal
Amraoti 1942 PP

223
A Study on the Concept of Varnya Vis-à-vis Clinical evaluation of efficacy of varnya gana lepa in vyanga
125
Pandit Hari Sadashiva Shastri Paradakara Astanga Hrudaya 9th
edition Chaukhamba
Surabharati Prākāśa n 2005 page 387 126
Acharya Yadavji Trikamji-Sushruta Samhita 8th
Edition, Chaukhambha Orientalia,
Varanasi 2005 PP 101 127
Purushottama Sharma.Shareera Tatva darshana nama vatadidosha vijnana. published
by P.S Hirlekar. Bharateeya Ayurvidya Shikshan Samiti Amraoti (Berar) . Printed by
T.M Patil Manager Saraswati Mudranalaya of Shri Hanuman Vyayam Prasarak Mandal
Amraoti 1942 PP 243 128
Grimes PE, Yamada N, Bhawan J. Light microscopic, immunohistochemical, and
ultrastructural alterations in patients with melasma. Am J Dermatopathol. 2005;27:
96-101. 129
Vazquez M, Maldonado H, Benmaman C, Sanchez JL. Melasma in Men: a clinical
and histological study. Int J Dermatol 1988 27: 25-7 130
Dominguez AR, Balkṛṣṇan R, Ellzey AR, Pandya AG. Melasma in Latina patients:
cross-cultural adaptation and validation of a quality-of-life questionnaire in Spanish
language. J Am Acad Dermatol. 2006;55:59-66. 131
Wade TR, Wade SL, Jones HE .Skin changes and diseases associated with pregnancy.
Obstet Gynecol 1978 52:233–242 132
Wong RC, Ellis CN Physiologic skin changes in pregnancy. J Am Acad Dermatology
1984 10:929–940 133
Errickson CV, Matus NR .Skin disorders of pregnancy. Am Fam Physician 1994
49:605–610 134
Parmley T, O‟Brien TJ . Skin changes during pregnancy. Clin Obstet Gynecol 1990
33: PP 713–717 135
Mallick S, Singh SK, Sarkar C et al (2005) Human placental lipid induces
melanogenesis by increasing the expression of tyrosinase and its related proteins in vitro.
Pigment Cell Res 18:25–33 136
Rakesh K.Sindhu, Upma et al. Santalum album linn: a review on morphology,
phytochemistry and pharmacological aspects, IJPRIF Jan-Mar 2010 Vol.2, No.1,
PP 914-919 137
Narong Chomchalow. The Utilization of Vetiver as Medicinal and Aromatic Plants
with Special Reference to Thailand . Curtis 1996 138
Satheesh George, K. V Tushar et al. Hemidesmus indicus (L).R.Br. A Review,
Journal of Plant sciences 2002 , Issue 3(2) PP 146-156 139
Pandit Shivprasad Sharma. Aṣṭāṅga saṁgraha. 2nd
Edition, Chaukambha Sanskrit
series, Varanasi 2000 PP 136 cxl
Sushruta vrana bandhana cxli
Acharya Yadavji.Trikamji Suśruta Samhita 8th Edition Varanasi Chaukhamba
Orientalia, 2005 PP 84