war psychiatry, chapter 11, educating mental health workers
TRANSCRIPT
Educating Mental Health Workers
193
Chapter 11
EDUCATING MENTAL HEALTHWORKERS
RONALD J. KOSHES, M.D.,* JOHN M. PLEWES, M.D.,† BRIAN G. MCCAUGHEY, D.O.,‡ AND JAMES STOKES, M.D.§
INTRODUCTION
ESSENTIALS OF COMBAT PSYCHIATRYSituational AspectsIndividual/Role AspectsEducational Principles
SPECIFIC AUDIENCES
METHODS OF TEACHINGMedical StudentsPsychiatric ResidentsField Training Exercises
SUMMARY AND CONCLUSION
*Medical Director, Adult Services Administration, Commission on Mental Health Services, Department of Human Services, District ofColumbia, Washington 20032; Guest Scientist, Department of Military Psychiatry, Walter Reed Army Institute of Research, Washington,D.C.; Clinical Assistant Professor of Psychiatry, Uniformed Services University of the Health Sciences, Bethesda, Maryland; President, Societyof American Military Psychiatrists
†Lieutenant Colonel, Medical Corps, U.S. Army; Chief, Department of Psychiatry, Fort Bragg, North Carolina, and Clinical Assistant Professorof Psychiatry, Uniformed Services University of the Health Sciences, Bethesda, Maryland 20889–4799
‡Captain (ret), Medical Corps, U.S. Navy; Naval Health Sciences Education and Training Command, and Assistant Professor of MilitaryMedicine and Psychiatry, Uniformed Services University of the Health Sciences, Bethesda, Maryland 20889–4799
§Colonel, Medical Corps, U.S. Army; Chief, Psychiatry and Neurology Branch, Behavioral Sciences Division, Academy of Health Sciences, FortSam Houston, Texas 78234–6133

Military Psychiatry: Preparing in Peace for War
194
program and requested that their units remain in-volved in the subsequent years. That program hasnot continued, but a conceptually similar programhas been sustained at Schofield Barracks, Hawaii.
Although these special courses are novel andimportant, they are often carried forward by theenthusiasm and drive of their originators. The mili-tary unit consultation training must compete fortime with other parts of the psychiatric curriculumthat are required for accreditation of the residencyprogram. The training may lapse unless other fac-ulty members support it actively.
New army doctrine has been written that re-quires the intimate involvement of mental healthpersonnel in the work of units. The Army MedicalDepartment operational concept for combat stresscontrol (CSC) and Field Manual 8–513 specify thateach maneuver brigade in a division needs a dedi-cated brigade CSC team consisting of one mentalhealth officer and one behavioral science noncom-missioned officer (NCO) from the division mentalhealth section. Before combat, the brigade CSC teammust be proficient in field and survival skills andknowledgeable about combat stress reactions andgeneral mental health issues. The CSC personnelmust know the equipment and mission of the sup-ported units. They must interact with and teach allof the brigade’s leaders, chaplains, and medicalpersonnel to enhance combat performance and con-trol stressors. The officer-NCO team from the divi-sion mental health section must be trusted as acohesive part of the brigade and participate early inall operational planning.
If the mental health section officers and NCOsare to accomplish these requirements, they cannotremain in a clinic. They must go out and meet theunit leaders and soldiers in their work areas, motorpools, and barracks. They must sometimes takephysical training with those units early in the morn-ing. They must meet with the unit’s spouses in thefamily support group meetings. They must livewith the units overnight in field exercises. Theymust ride in the unit’s vehicles and go with thesoldiers as observers in their lines training and livefire drills. They must practice conducting unit sur-vey interviews (structured small group discussions)to assess unit morale, horizontal and vertical bond-ing, trust and information flow, and the strengthsand shortfalls of leadership. Based on these inter-
INTRODUCTION
Mental health workers play a unique role inmilitary organizations. They work with families,military units, individual soldiers, sailors, and air-men to promote cohesive working and family rela-tionships, improve morale, and maximize unit ef-fectiveness. They also provide direct services toindividuals with psychiatric or emotional prob-lems. Finally, mental health workers consult withleaders about effective strategies to support mili-tary units during war and peace. In these variedroles, military mental health workers focus espe-cially on occupational health.
Military and civilian mental health professionalsdiffer in many respects. For one, the arena of prac-tice is different. Military mental health profession-als must not only aggressively intervene with unitsand individuals during war but also provide agreater focus on families, assist in stress reductionwithin units, raise morale issues, and explore otherpreventive mental health concerns during peace-time. Civilian practice provides few models formilitary mental health workers. The calmness ofgarrison life may be interrupted at any time by anational emergency, requiring mobilization of indi-vidual units or entire armies that must face danger-ous missions and uncertain futures. Mental healthworkers are often part of the mobilization and sharethe same risks and uncertainties of their client popu-lation. In addition, practitioners of various disci-plines are required to work together within themilitary rank system. Mental health professionals,although experts in their field, often work under thejurisdiction of higher ranking officers in commandof the fighting forces.
Stress is inevitable in combat and often decidessuccess or failure. This recognition makes the mili-tary mental health provider unique from his civil-ian counterpart. Training, therefore, must reflectthis difference in preparation for battle.1 To im-prove training of psychiatrists to work with infan-try commanders, Lee devised a course for psychia-try residents to participate in the activities of lightcombat infantry battalions at Fort Ord, California.2
The first residents in the course (Leamon and Sutton)found that familiarity with the mission of the unitshelped them in providing effective psychiatric in-terventions.2 The equally impressive finding wasthat all three battalion commanders involved in theproject expressed “enthusiastic support” for the

Educating Mental Health Workers
195
views, the CSC teams provide consultation to theunit leaders on how they can capitalize on theirunits’ strengths and fix the shortfalls—being care-ful to safeguard the confidentiality of the sources.
Ultimately, the brigade CSC teams must deploywith their brigades’ rotations to the National Train-ing Center (NTC), Fort Irwin, California; the JointReadiness Training Center (JRTC), Fort Polk, Loui-siana; or the Combat Maneuver Training Center(CMTC), Hohenfels, Germany. These 2- to 3-weekexercises have the realism, fast pace, and high stressprovided by a highly trained and experienced op-posing force (OPFOR) and the Multiple IntegratedLaser Engagement System (MILES), which tellswhen each vehicle or soldier has been hit by enemy(or friendly) “fire.” These exercises provide suffi-cient real-world fatigue and stress (including, some-times, fatal training accidents) for the CSC teams topractice their real-world combat consultation andtreatment missions under tactical conditions. Fullinvolvement of the division mental health sectionsin these exercises must become standing operatingprocedure.
With this preparatory training accomplished, themission of the mental health workers can be focusedwith specific emphasis on combat readiness. Thefollowing standards must be part of the workingagenda for combat: provide far-forward triage andintervention to immediately return to duty over50% of battle fatigue cases and prevent misconductas a result of combat stress; supervise recovery ofthe battle fatigue cases with rest, nutrition, andexpectancy of return to duty in their own units;supervise restoration or referral of battle fatiguecasualties at the forward support medical companyto assure 70 to 85% return to duty within 3 days;assure that recovered battle fatigue casualties arereturned quickly to their units and keep relapsebelow 15%; assist units who have lost soldiers tobattle fatigue in reconstitution to rapidly restorecombat power; supervise or conduct unit after-action stress debriefings to prevent disabling post-traumatic stress disorder in effective soldiers; andserve as point of contact for other medical person-nel assigned to the CSC teams from the echelonabove division who will reinforce the brigades.
The army’s new active and reserve componentmedical CSC detachments and companies, at theechelon above division, should also coordinate tosend teams to reinforce the exercises at the NTC,JRTC, and CMTC (as well as to lesser field trainingexercises at the division and brigade posts). Theseunits are discussed in the second part of this chap-
ter. The air force’s four-person combat stress unitsfrom the 50-bed air transportable hospitals couldalso receive excellent training at the JRTC; theycould work at the Fort Polk airfield, which serves asthe entry point into the exercise. Navy mentalhealth teams might also have the opportunity towork with marine or army units at the JRTC. Allservices’ combat stress teams should be deployed inthe major joint field exercises, such as Team Spirit inKorea and Ocean Venture in the Atlantic Command.
In peacetime and military operations other thanwar, as well as in war, the cohesion, trust, andinvolvement of mental health personnel with lineunits (both active and reserve) are important forcontrolling stress and maintaining readiness in theevolving post-Cold War force. This can only beaccomplished by close working relations with thoseunits and their unit families. The driving modelmust be one of proactive, primary and secondaryprevention, conducted on the line unit’s own ground,rather than the reactive patient-care model in aclinic or hospital.
One problem with achieving the required capa-bility is that the military and civilian professionaltraining programs do not provide sufficient hands-on experience with the military community and theprevention model. Therefore, most graduates donot overcome their initial hesitancy about trying it.No one likes to feel and appear ignorant or incom-petent—especially not physicians or other mentalhealth professionals. The graduates naturally feelmore comfortable with, and gravitate to, the famil-iar direct patient care model in which they havetrained. This occurs even when the graduates areassigned to division mental health or CSC unit slotswhere the community-oriented mission should bethe highest priority. Their own natural tendency isreinforced by the pressure of full clinic appoint-ment schedules and the natural desire of short-staffed garrison medical facilities to coopt the unitmental health personnel onto their clinic and oncallrosters. We must give the future practitioners suffi-cient baseline knowledge and confidence about CSCand preventive unit consultation during training sothat they take the first steps toward learning to doby doing.
This chapter examines the unique role of militarymental health providers and delineates the processof teaching them the principles of combat psychia-try. The essentials of combat psychiatry, the type ofpractitioners involved in treating combat victims,and suggested methodologies for teaching combatpsychiatric principles are also presented.

Military Psychiatry: Preparing in Peace for War
196
ESSENTIALS OF COMBAT PSYCHIATRY
been the particular history of the unit throughoutits command and leadership? Insight into theseparticular features of the military organization canmake the mental health worker more effective. Theprocess of finding out this information can alsopromote effective liaison between caregiver andunit personnel.
During the time-consuming process of informa-tion gathering, the worker has an opportunity to getto know the people who make up the unit and tolearn what their jobs are and the problems they face.A military police unit, for instance, may have fre-quent, short-term deployments that come unex-pectedly and have high visibility within the com-munity. This may predispose them to higher ratesof alcoholism or other dysfunctional ways of deal-ing with stress. This instability will be stressful fortheir family members. A personnel agency mayhave a high degree of stress during mobilizationsbut be bored the rest of the time. This can promotejob dissatisfaction and frequent work conflicts.
A failure of the mental health worker to under-stand the work environment of the personnel he isresponsible for can result in distrust and anxiety onthe part of the unit. Recommendations concerningmanagement style or retention of personnel may beignored. As a result, mental health workers maydeal more with the frustrations and emergencies ofa unit, leaving little time to deal with morale or uniteffectiveness.
Mental health workers in the military must alsodeal with unique administrative issues. They mustbe familiar with key regulations9–11 to be able toeffectively provide militarily unique services, suchas forensic evaluations, clearances for specialtyschools, or how to initiate the removal of command-ers from their positions because of alcohol or drugabuse or psychiatric illness.
Understanding the importance of what consti-tutes good military leadership is crucial to the workof the mental health worker. While many for-profit,civilian organizations emphasize individual andcentral responsibilities to increase productivity, amilitary organization needs cooperation among itsmembers for it to function properly. Effective mili-tary leaders understand this principle. During peace-time as well as during conflict, effective communi-cation among members of the unit is paramount.The training and relationship building that occursduring peacetime within the unit prepares that or-ganization for rapid assumption of its mission dur-
The practice of military mental health is groundedin the principles of community mental health thatemphasize primary prevention, group dynamics,healthcare delivery system issues, and individualtreatment.4,5 Most military mental health profes-sionals are trained in nonmilitary settings wherethey primarily learn to diagnose and treat individu-als. Most military mental health practitioners mustaugment their training to be effective in a militarysetting. In the early European mobilizations of WorldWar II, it was evident that while the number ofmilitary psychiatrists (most of whom were on-the-job trainees with 90 days of education) was ad-equate, most did not have the background to pre-vent what we now call combat exhaustion.6 This isbecause the psychiatrists, most of whom had noprior psychiatric training and had been draftedfrom civilian practices, were not trained to dealwith this problem. Because of this, dysfunctionalsoldiers were inappropriately evacuated from com-bat zones to the United States, which decreased unitmorale, cohesion, and fighting strength and causedlong-term morbidity among these psychiatric pa-tients.6,7 Under the leadership of Roy Halloran,William Porter, and William Menninger, programswere established to train on-the-job psychiatrists totriage and treat military psychiatric casualties.8
The following sections describe the unique prin-ciples of combat psychiatry. Not merely a collectionof techniques, the field of combat psychiatry in-volves the training of the mental health worker as amilitary professional whose knowledge-base andattitudes reside within the military organizationalstructure.
Situational Aspects
Anyone who has taken a course in either creativewriting or public speaking knows the importance ofunderstanding one’s audience. If asked to give abanquet speech, the logical questions are, “Whowill be in attendance and what is their level ofinterest in this subject matter?” Likewise, mentalhealth professionals must know their military orga-nization to be effective. “How large is the unit; whatis its mission, location, composition, and recentdeployments?” These are just some beginning ques-tions to ask. More sophisticated ones include: Whatare the demographics of the group? Are most mar-ried? Single? Is this the first assignment for most ofthe members? Where do they come from? What has

Educating Mental Health Workers
197
ing armed conflict or mobilization. Mental healthworkers can help leaders to maximize cooperationamong their personnel and consequently improveproductivity.
An understanding of leadership also allows thehead of a mental health team to deliver servicesmore efficiently to the unit. For all military organi-zations, strict adherence to the chain of command,as well as obedience to leadership, is essential forthe morale and effectiveness of that organization.Mental health workers cannot act as individualparties in the treatment of patients, but they mustrecognize the responsibilities and authority of theunit’s commander and be able to work effectivelywith him. In this way, the mental health workerfunctions as a consultant.
Individual/Role Aspects
Mental health workers often function as liaisonsto units and advisors to commanders, in addition tobeing individual caregivers. The mental healthworker must be knowledgeable of the principles ofprimary prevention and community psychiatry,including the importance of stress reduction tech-niques, as well as the importance of family andother support structures available at the base orpost. Often, a mental health worker can learn a greatdeal about the functioning of the unit by readingpolice reports, knowing the number of referrals foralcohol and drug treatment, and learning aboutdisciplinary actions. At training sites, the pass rateof a particular unit may reflect not only the diffi-culty of the subject matter but the general morale ofthe group.
During combat, the liaison role is especially im-portant and onsite presence of the mental healthworker is essential. Contrary to most civilian men-tal health practices, military workers have an onsitemission, and they must be proactive; they shouldnot wait for patients to come to them. These prin-ciples have been most clearly articulated in contem-porary community psychiatry doctrine12 that ap-plies to working with chronic mental illness in thecommunity, as well as the management of disastervictims that requires an onsite intervention ap-proach. A mental health worker must give up hisoffice for the onsite field environment.
Mental health workers can be troubled by theirown anxieties and frustrations during combat. Theleader of the mental health team is responsible forthe morale of his workers and must emphasize theneed for debriefing, rotations, rest time, and proper
medical and nutritional support during these peri-ods. Mental health workers are at risk for burnout;they must monitor themselves for signs and symp-toms of decreased effectiveness and personal stress.
Perhaps the most difficult of the mental healthworker’s roles is being a command adviser. Com-manders may excessively depend on the advice thatis given by mental health workers, placing unreal-istic demands and expectations on them, and therebyabdicating their own responsibility as leaders. An-other possibility is that mental health workers maybe branded as causing the problem rather thancontributing to the solution. In the case of militarytrainees, a rising number of suicide attempts wasblamed on the presence of a mental health workeroperating on the training post. Only after discus-sion with commanders were a variety of environ-mental stresses identified as the actual causes of theincreased suicide attempts, namely a war mobiliza-tion, incapacity of several drill sergeants due toalcohol and drug problems, unrealistic expecta-tions of soldiers during the war effort, and an in-creased training mission and increased standardsfor training.13
In much the same way that a unit’s commanderand executive staff may depend on a mental healthworker, so too can command actions and decisionsbe delayed until the counsel of the worker is ob-tained. While in many instances information pro-vided by the workers may directly impact com-mand decisions, some military leaders may excusetheir own inability to make decisions based on“expert advice” from mental health workers. Spe-cific aspects of this point are well documented byBion in his work with leaderless groups during the1950s.14–21 He found that in a leaderless situation,group members can become dependent on eachother, suspicious and distrustful, or apathetic. Bion’sthesis was that in the work group, certain basicassumptions such as dependency, paranoia, andexpectancy decrease the efficiency and effective-ness of the group.
Mental health workers may be the first to identifydysfunctional groups. There are several examples.In dependency groups, commanders will make de-cisions that can be made by the first sergeants orother operational personnel. A “fight or flight”group may have members that are so competitivethat they are paranoid. A “pairing group,” or onethat is incompetent without a leader, will push offdecisions until a commander returns from vacationor temporary duty, thereby paralyzing any workprogress within that group. An essential element in

Military Psychiatry: Preparing in Peace for War
198
all these situations is that the group leader’s anxietywill determine how effective the unit can be. Themental health worker may be chiefly responsiblefor relieving the leader’s anxiety through whatevermeans are available.
Educational Principles
The principles of immediacy, proximity, and ex-pectancy in managing combat stress casualties de-serve another airing. Removing an individual fromstress is the goal of modern psychiatric hospitaliza-tion. In contrast, during combat, rest and return ofthe individual to his military unit have been shownto decrease long-term psychiatric morbidity, im-prove morale, and promote unit cohesiveness andeffectiveness.22–25
There are important differences in the kinds ofcasualties that occur during various types of com-bat. High-intensity conflict, in which there iseither a rapidly mobile land force or a staticbattlefield, tends to produce combat exhaustioncharacterized by anxiety and confusion disor-ders. Low-intensity garrison warfare can pro-duce “nostalgic” types of combat reactions thatinclude alcohol and drug abuse, depression, andsuicide. The mental health worker needs to be
aware of the variety of stress responses that re-sult from the different types of combat.26–28
Command consultation is another essential prin-ciple of combat psychiatry. The process of getting toknow a unit and providing effective consultationinvolves a slow, steady progression of meetings,often held weekly with key leaders in a militaryunit, to discuss the needs of those leaders. Just asmedical consultants would behave improperly ifthey took over complete care of a consultee’s pa-tient, it would also be inappropriate if the mentalhealth worker attempted to gain control of the unit.Mental health workers, although they possessunique professional abilities, must be replaceable atany time during the life of a unit. A unit cannotgrow too dependent on the worker, nor can theworker see the unit as his command. Specific tech-niques to be used in command consultation includeinvolving the chain of command in any presenta-tion made to the organization, deferring to the au-thority of the command structure in any decisionregarding personnel retention or separation, allow-ing commanders to initiate requests for consulta-tion, being available as consultant on a regular orpredictable basis, responding aggressively and ap-propriately to a commander’s request for help, andproviding feedback to commanders on referrals ortreatment of an individual unit member as needed.
SPECIFIC AUDIENCES
The education of mental health personnel occursin a variety of settings and utilizes many tech-niques. This section will describe the specific audi-ences for which training in combat psychiatry isnecessary.
The most often neglected individual who needsto be properly educated to maintain the mentalhealth of a unit is the individual soldier, sailor, orairman. Several pamphlets have been producedthat emphasize the need for the “buddy system” inpromoting unit morale and cohesiveness. Simplyput, each soldier should look for dysfunction in hiscomrades. Isolation, decreasing attention paid touniform cleanliness and personal hygiene, and in-subordination may indicate that a problem exists.Unit members may often be the first ones a troubledsoldier turns to, and education of all unit membersabout the importance of referring him to appropri-ate personnel within the command is essential.
Medics, those enlisted personnel who functionmostly as licensed practical nurses, medical techni-
cians, and orderlies, are also part of the militarymental health team. While these medics are notalways practicing in the field of mental health, it isimportant that they understand the basics of psy-chiatric triage. Important concepts for them to learnare the difference between neurotic and psychoticbehavior, the characteristics of psychiatric illnessthat can masquerade as physical illness, manage-ment of anxiety, management of suicide, manage-ment of combat stress reactions, and substance abusedisorders. For the most part, the medics who spe-cialize in mental health will learn how to work withpatients in their first assignment while under thesupervision of a psychiatrist or social worker.
Psychologists and social work officers workclosely with psychiatrists in the care of emotionallydisturbed patients. Although these individuals maybe credentialed to provide unsupervised care, thecare of patients on medications and those who re-quire hospitalization must be supervised by a phy-sician. The psychologist and social worker should

Educating Mental Health Workers
199
have a working knowledge of the latest Diagnosticand Statistical Manual of Mental Disorders (DSM),be able to conduct a comprehensive interview of apatient, make a provisional diagnosis, and developa diagnostic or treatment plan. By the nature of theireducation and training, the psychologists and so-cial workers will have an advanced academic de-gree in the field of mental health.
Medical students are often challenged by learn-ing psychiatry. For a military medical student popu-lation, introducing the concepts of battlefield man-agement of combat stress reactions is crucial.Participating in field exercises that realistically in-clude battle fatigue cases and cases that mimic battlefatigue will prepare the practicing physician to makecogent and useful referrals to his psychiatric col-league. A model program for the education of medi-cal students is described in the next section.
Nonpsychiatric physicians are the usual sourceof referrals for psychiatrists, and they may be thefirst physician practitioners to come in contact with
combat stress casualties. Educating these profes-sionals must be an ongoing enterprise.
Psychiatric residents can learn about combat psy-chiatry by first learning how a military unit func-tions. Electives should focus on field placement ofresidents for a realistic experience in the practice ofmilitary mental health. In the next section, a modelfor the education of psychiatric residents is pro-posed. Residency is also an opportune time toteach the techniques of psychiatric debriefing, aprocess by which survivors of trauma or combatbegin a reintegration into their communities andunits.29
Nursing staff have the most contact with patientswhen hospitalized, and during combat this contactis probably increased. Military nurses in all areas ofspecialty should be taught how to recognize andtreat combat stress reactions. Part of any militarynursing continuing education conference shouldinclude update, review, and latest techniques formanaging these disorders.
METHODS OF TEACHING
be done. Even with a very limited amount ofequipment, a worthwhile field exercise can stillbe conducted.
The planning faculty includes a course directorand several other faculty members who can act asadvisers to help develop and revise the course asneeded. They should be motivated to teach and beknowledgeable about battle fatigue or be willing tolearn. Initially, they need to meet to establish thegoals and objectives of the battle fatigue course anddecide how it is going to be taught in their institu-tional setting. Later, they should meet periodicallyto look for ways to implement improvements.
The teaching faculty conducts the teaching. Train-ing them properly is critical to the success of thecourse. This group will present the lecture andconduct the case discussions groups and testing inthe classroom and the field. Like the planners, theyshould have an interest and ability to teach andshould be knowledgeable about battle fatigue. Thisgroup may include members of the planning fac-ulty. This course was originally designed to teachmedical students, but if modified, it could be usedto teach other groups.30,31
If others are to be included, the next step is toidentify the students and construct a course thatwill fit their background, needs, and interests. Thecourse can be basic and still benefit a group with
The following section describes three programsdesigned to educate military personnel in the fieldof combat psychiatry. The first is primarily aimed atmedical students, the second is for psychiatric resi-dents, and the third is a field exercise that tests theoverall medical and mental health capabilities of amedical unit. While these programs are far fromideal, we feel these are the best educational modelstested to date.
Medical Students
A course for medical students concerning thepractice of medicine during combat was designedby McCaughey at the Uniformed Services Univer-sity of the Health Sciences. A basic concept aboutthe course is that there is a stepwise approach to thetraining.30,31 Exhibit 11–1 is a comprehensive de-scription of this course that gives students the abil-ity to learn basic concepts, practice them, and makeevaluation and management decisions under simu-lated wartime conditions.
Some institutions may not be able to adapt allaspects of this course because of their limited capa-bilities. For instance, it may not be possible to get allof the equipment that is necessary to conduct cer-tain parts of this course in the field. But this shouldnot prevent the faculty from doing the best that can
Military Psychiatry: Preparing in Peace for War
200
EXHIBIT 11–1
PSYCHIATRY TRAINING COURSE
Phase One: Providing Information
Information should be provided in three forms: hand-out, lecture, and videotape presentation.
1. Handout. The handout should include informa-tion about battle fatigue and how the coursewill be conducted. Information about battlefatigue should include published articles fromvarious perspectives, one of which is historical.It is important to convey to the students thatbattle fatigue is not just a recent problem butthat it has been around as long as wars them-selves. There should be case examples from theAmerican Civil War, Russo-Japanese War, WorldWars I and II, the Korean and Vietnam conflicts,and the Arab-Israeli wars. The various namesthat have been given to designate battle fatigue(nostalgia, shell shock, and so forth) and how itwas managed for each of these wars should beincluded. Other topics should include how todeal with battle fatigue management and pre-vention today and the application of battle fa-tigue management principles in other settings,such as civilian disasters.
The handout should be distributed well in ad-vance of the course so that the students have enoughtime to read the background material. Any addi-tional instructions, such as the name and tele-phone number of a person to contact if there arequestions, should also be included with thehandout.
2. Lecture. The lecture should include the followingtopics: types of battlefield stressors and the reac-tions of service personnel to these stressors; de-scription of battle fatigue and its extremely vari-able presentations; physical and psychologicalsymptoms associated with battle fatigue; a samplecase; theories about the cause of battle fatigue;battle fatigue epidemiology; importance of battlefatigue to the serviceman, combat unit, and medi-cal facilities; a list of the groups of medical person-nel that need to be informed about battle fatigue;management of battle fatigue; prevention; and usesof the battle fatigue management principles in thepeacetime setting.
3. Videotape presentation. The videotape presentationis given immediately following the lecture. Itshould show various types of actual battle fatiguecasualties. After each case is shown, the pre-senter should stop the tape and discuss the case
with the students. A suitable videotape, editedfrom a World War II documentary black andwhite film, is entitled World War II U.S. ArmyBattle Fatigue Cases—Combat Exhaustion (A1701–90–0059). It is available from the Army MedicalDepartment Center and School for restricteduse in training military and medical and mentalhealth workers.
Phase Two: Practicing
The students use the information they have learnedabout battle fatigue in the following settings: pretest,case discussion groups, and the classroom testing.
1. Pretest. The pretest is taken after the lecture andgraded by the students. It is then discussed in aclassroom setting.
2. Case discussion groups. Five to seven studentsmeet with a mental health professional for about2 hours. Individual cases, found in the handout,are discussed. The focus is on the identificationof battle fatigue, differentiation of battle fatiguefrom other problems, management, and return-ing to duty. Students, in pairs, also practiceinterviewing skills by having one student con-duct the interview while the other one plays therole of a battle fatigue casualty. The rest of thegroup has the opportunity to observe the inter-view and participate in the critique.
3. Classroom testing. Just before going on to thefield exercise, the students are tested in a class-room setting. This is a pass-fail test whosepurpose is to see if the students have gained thebasic skills and knowledge they need to effec-tively evaluate and manage battle fatigue cases.The students are tested in pairs. They alternateroles as an interviewing physician or a battlefatigue casualty while a faculty member evalu-ates the interaction. The faculty member alsoasks general questions about battle fatigue. Ifthe students demonstrate that they have mini-mal competence, they can go to the next phase.
Phase Three: Testing
There are two parts for the testing: written test in theclassroom and practical testing of simulated battlefatigue casualties in the field.

Educating Mental Health Workers
201
EXHIBIT 11–1 (continued)
PSYCHIATRY TRAINING COURSE
mixed backgrounds, such as one that includes physi-cians, nurses, physician assistants, corpsmen, medicalservice personnel, and so forth. Alternatively, thecourse can be designed for specialized groups, such asjust psychiatrists, just psychiatric residents, or anyone of the other groups mentioned above.
All courses, no matter who the audience is, shoulduse a phased approach, in which each phase pre-pares the students for the next phase. The firstphase provides information through reading mate-rial (handout), lectures, and videotapes. In the nextphase, the students practice the use of battle fatigueidentification and management techniques using theinformation they have learned. The last phase is test-ing, which occurs in the classroom and in the field.
The students should be given the opportunity toprovide feedback about the course. This feedback isbest done at the end of the course. Forms with open-ended questions and or scales that indicate howwell teaching objectives were met can be used.The feedback should be submitted anonymously.Changes to the course should be based on thefaculty’s observations and the student feedback.
Psychiatric Residents
The following is a model for a residency electivein community psychiatry. The goals of the electiveare to attain the skills necessary to function as amilitary psychiatrist, especially during combat, and
TABLE 11–1
ELECTIVE IN COMMUNITY AND MILITARYPSYCHIATRY
Component Comments
Course Directors Insert names of individuals who willbe responsible for the training: one amember of the medical center faculty,the other the onsite director.
Place Provide the exact location of facility.
Duration This will usually be 2 weeks to 2months depending on extent of mate-rial covered.
Participants Will be selected from appropriate levelpsychiatry residents.
Housing Arranged by the onsite director.
Cost Per diem costs and transportation ex-penses will be covered.
Rationale While military psychiatrists functionin a variety of settings (divisions, re-search, and hospitals), most graduat-ing residents are assigned to commu-nity hospital/clinic settings. Thistraining prepares them for their initialpractice experience.
1. Written test. The test includes material from thelecture, reading material, videotapes, and the casediscussion groups.
2. Testing in field under simulated wartime conditions. Afield exercise is the last part of the training program.The students are evaluated on their ability to evalu-ate and manage simulated battle fatigue cases. Ifpossible, this should be part of a larger field medicalexercise that includes a variety of other surgical andmedical problems to add to the realism.
Simulated battle fatigue casualties are trained be-fore the field operation starts. They are introducedinto the medical care system and, through triage,are sent to a combat stress center that is manned by
students who are supervised by faculty. The inter-view of the battle fatigue casualty is observed by afaculty member. After this, the faculty membermeets with the student to discuss the case and askgeneral questions about battle fatigue. The stu-dent is evaluated on the following points: orient-ing the casualty to the interview, identifying thereason for referral, conducting past history andmental status examinations (adapted for the battlefatigue situation), formulating the problem (diag-nosis and differential diagnosis), developing theintervention, ability to elicit information, and gen-eral knowledge about battle fatigue and leader-ship. Students should be evaluated individuallyand feedback given at the end of their rotation atthe combat stress center.

Military Psychiatry: Preparing in Peace for War
202
army surgical hospitals). The hospitals do not come atfull strength and usually are staffed for 50 to 100medical and surgical beds.32–38
Each medical group headquarters also usuallycontrols one or more medical clearing companies(with 50 to 100 of its 250 patient cots). The medicalbattalion, or an evacuation battalion headquarters,also controls several helicopter and ground ambu-lance companies and detachments.32–38
Additional medical and surgical specialty de-tachments augment the hospitals. Preventive medi-cine, dental, and veterinary detachments are as-signed to the medical brigade or the medical groupsto provide area support. Simulated and actual medi-cal supply and logistics for the many medical unitsare provided as they would be in a combat zone bymedical supply units.
In all of these FTXs between 1984 and 1992, therehas been at least one U.S. Army Reserve “OM team”
to develop strong collegial relationships with com-manders and other unit personnel. Tables 11–1 and11–2 are examples of a proposal that could be devel-oped for this elective, along with a discussion of theaspects of the field setting.
Field Training Exercises
The U.S. Army usually conducts one large-scalemedical field exercise each summer except when worldevents such as the Persian Gulf War or budget limita-tions have taken precedence. Since 1984, these fieldtraining exercises (FTXs) have rotated among severalmedical brigades (headquarters units). Each of theseFTXs has involved between 3,000 and 9,000 medicaltroops. The medical brigade headquarters commandstwo or three medical group headquarters. Each medi-cal group controls two to four hospitals (usually evacu-ation hospitals, combat support hospitals, and mobile
TABLE 11–2
ASPECTS OF THE FIELD SETTING
Component Comments
Background Describe the training site and its unique features.
Elective Experience Residents working under the chief of psychiatry will experience all levels of patient care toinclude consultation-liaison, outpatient and inpatient evaluations and treatment, supervision ofsocial workers, psychiatric technicians, and the psychologists. Emphasis will be placed onproviding the resident with an opportunity to observe and participate in the operation of a full-scale, multiservice psychiatric practice, as well as interact with crucial hospital personnelsupporting that practice. The resident will attend the usual departmental meetings, as well ashospital governance boards, and meet with officers in logistics, administration, resource man-agement division, and clinical support.
A major feature of this field elective will be command consultations and unit visits. This will beaccomplished under the auspices of the community mental health service. If timely, the resident canparticipate in the post’s chief of staff briefings.
Patient Population The profile of the patient population should be described here.
Supervision and All patient care supervision will be provided by the chief of the department of psychiatry. AEvaluation meeting of all practitioners in the department will be scheduled at the end of the resident’s stay
to gather performance data. The final rating of the resident will be done by the chief, departmentof psychiatry, and returned to the training director at the medical center in a timely fashion.Additionally, the resident will have the opportunity to rate the program as a part of his or hersemi-annual evaluations conducted by the medical center staff.
Requirements The training director at Medical Center X will review this proposal and contact the chief, departmentof psychiatry, regarding appropriateness for training and seek clarification if needed.
The training director and chief, department of psychiatry, at Medical Center X must formallyapprove the elective and schedule the first resident participant(s).
Time Table Give time that the program will be operational.
References Provide pertinent references for the proposal.

Educating Mental Health Workers
203
(the designation for a psychiatric medical detach-ment) to fulfill the CSC mission. The OM teamsserved in the Persian Gulf War but have since con-verted to the new CSC companies or detachments.An OM team at full strength had 48 persons. Itincluded five psychiatrists, six social workers, twopsychiatric nurses, a clinical psychologist, enlistedpsychiatric and behavioral sciences specialists, andadministrative support personnel. In practice, mostOM teams came to these FTXs with between 20 and35 personnel with only one psychiatrist and nopsychologist. They were augmented by volunteersfrom the other OM teams and by active duty, U.S.Army Reserve, and U.S. Air Force occupationaltherapists and by occupational therapist enlistedspecialists. The occupational therapists were espe-cially eager to demonstrate their field role in pro-moting return to duty of battle fatigue casualties.The OM teams also had some (but usually notenough) vehicles, tents, and equipment.32–38
One of the best features of these field exercises isthe opportunity they provide for individuals orsmall teams from other organizations to reinforceor fill out the CSC unit that has been programmedinto the FTX. The operational concept for CSC callsfor the capability to concentrate CSC personnel andexpertise rapidly at sites of acute need by havingthem temporarily reinforce the small CSC teamsalready near the site. The CSC personnel them-selves need to be highly adaptable and able tointegrate new team members quickly. Cross-attach-ing personnel among active duty or reserve CSCunits in FTXs practices this critical skill. It has theadded benefit of sharing (“cross-fertilizing”) prac-tical experience and initiating networking. The FTXsalso provide an economical way for mental healthinterns, residents, and practicing clinicians who areslotted as PROFIS (Professional Filler System) fill-ers in CSC units to receive high-quality, emotion-ally positive, field experience.
In most of the FTXs, the OM teams operatedaccording to evolving U.S. Army CSC doctrine. TheOM team headquarters were assigned directly tothe medical brigade headquarters. The detachmentdivided into smaller, dispersed teams. Dependingon the numbers of each professional discipline andthe vehicles available, the CSC unit tried to provideCSC support to one or all of the subordinate medi-cal groups in the medical brigade.
Because these FTXs were played at the level ofthe medical brigade in support of a corps, theOM(CSC) detachment had as one mission the staff-ing of a reconditioning center. Reconditioning bydefinition3,39,40 is the 4 to 14 day treatment of battle
fatigue casualties who do not return to duty in thefirst 3 days of restoration treatment. Recondition-ing cannot be simulated in real time in a 4 to 5 dayFTX. However, the staff can do the admissionsworkup and then go through the daily schedule ofstructured activities in “quick time” or “time com-pression” in which 10 minutes equals 4 or 6hours.3,39,40
In the FTXs, as in evolving doctrine, the OM(CSC)reconditioning facilities collocated with an evacua-tion or combat support hospital. They were depen-dent on the hospital for food, water, fuel, medicalrecords, and often tents and cots. This was as itwould be in real combat. The CSC teams mustestablish duty-sharing arrangements with thehost hospital without letting their personnel andequipment be absorbed into that hospital. Ab-sorption would rightly happen to a hospital-aug-mentation detachment like a neurosurgery team,which becomes an integral part of the hospital,but must not happen to a mobile CSC team. TheCSC team uses the hospital as a base of operationbut must deploy its teams elsewhere, often onshort notice. Even those treatment functions suchas restoration and reconditioning must, by doc-trine,3 maintain a separate “nonhospital” iden-tity and atmosphere.
Experience has shown that the reconditioningcenter is best set up in the hospital staff quartersarea, near the kitchen and mess hall, laundry, andmotor pool. It should not be among the triage orward tents, and it must maintain a nonpatient,soldiering milieu. The patient role players simulat-ing battle fatigue can be assigned to assist the hosthospital with real work details, as well as being fed,showered, rested, and involved in recreational,physical fitness, and group debriefing activities.
In these FTXs, other subteams of the OM detach-ment were normally deployed to one or more of themedical clearing companies under the medical bat-talion in the medical groups. These teams usuallyattached to the medical company for support andremained with it 24 hours a day to triage, evaluate,and provide restoration treatment for locally gener-ated battle fatigue cases (both simulated and “real”).Restoration, by definition,3,39,40 is the 1- to 3-dayinitial treatment of battle fatigue soldiers and is bestdone at the medical treatment or clearing companyclosest to the soldier’s own unit, not at a “hospital.”Restoration requires a reasonably sized tent, prefer-ably with cots, dedicated to the recovering battlefatigue casualties.
The CSC teams at the clearing companies alsoprovided actual preventive consultation, education,

Military Psychiatry: Preparing in Peace for War
204
and case evaluations to the medical company andall other nearby units. In some FTXs, when therewere too few CSC personnel to provide a continu-ous presence at the medical companies, the CSCteam instead provided a regular schedule of circuit-riding. The team spent the night at the OM teamheadquarters or reconditioning center (base camp)and drove to visit one clearing company in themorning, then on to another each afternoon. Theteams were prepared to spend the night at a clear-ing company as the workload or the tactical situa-tion required. In this situation, the patient-holdingsections and medical treatment teams of the clear-ing company were trained to manage and restore allbut the problem cases. The problem cases wereevaluated by the CSC team each day, and, if neces-sary, they were taken back to the reconditioning(and restoration) center by the team as it completedits daily rounds.
The medical FTXs also routinely included non-medical combat support and combat service sup-port units, especially signal battalions and detach-ments to set up and operate the communicationsequipment. Some FTXs also had military policecompanies to provide rear area security and man-age enemy prisoners of war. Engineer units may beavailable to assist with hospital site preparationand personnel replacement elements to coordinatethe return to duty of simulated casualties.
At some of these FTXs the U.S. Air Force providesC141 and/or C130 aircraft to conduct simulated airevacuation from the combat zone (taking off withthe simulated patients, flying around, and landingnearby so that the patients can be “recycled”). Theair force also provides a mobile air staging facilitywith medical and nursing staff to hold and preparethe patients for the flight. In the future, it may bepossible to involve a navy hospital ship in theseexercises.41 Having a hospital ship offshore wasconsidered for Wounded Warrior ’92, part of whichtook place at Camp Pendleton and involved a ma-rine medical battalion working under an army medi-cal group headquarters. However, it was not fea-sible then because of expense.
A few of the FTXs in California and Missis-sippi have combined the medical brigade’s exer-cises with the annual training of the states’ na-tional guard division or separate brigade. In someinstances, the maneuver brigade or division medi-cal companies and organic battalion assets wereincluded in the medical evacuation play.33,34,36 Onthose occasions, the OM team has fulfilled itsforward CSC mission by sending mobile teams
forward to reinforce the division and brigademedical companies.
The virtue of such large-scale medical exercisesfor training in CSC is that the exercises suggest themagnitude and complexity of the real combat mis-sion. The FTXs illustrate the real-world problems ofexercising command and control through multiplelayers of headquarters, communicating with dis-persed teams over other units’ overworked andbreakdown-prone field switchboards and radionets,41 traveling and navigating to find unfamiliarunits, and negotiating allocation or loan of scarceresources such as tents, food, water, and vehiclemaintenance. All of these problems must be over-come in the combat theater.
The larger FTXs provide actual supported unitsand audiences for staff briefings, command consul-tation advice, and preventive educational presenta-tions. They may provide extensive patient play thatcan include simulated stress and neuropsychiatriccases. Invariably, they also provide actual over-stressed soldiers who need individual case evalua-tion and, when appropriate, onsite treatment. Exer-cises of this size also always provide one or moretrue neuropsychiatric cases, usually with a preex-isting disorder, who decompensate and must beevacuated to the supporting hospital system.
The shortfall of these FTXs is that, large as theyare, they are still only a small-scale model of a realU.S. Army area of operations. The medical units arenot surrounded by the many more nonmedical com-bat service support units with which they would beaggregated into base defense areas and base de-fense clusters. The distances between clusters dur-ing actual combat would be much greater than canbe achieved at some of the posts hosting the FTXs.The rear battle threat may be simulated by OPFORattacks, but there is little real danger or difficultywhen going from unit to unit, which may create afalse sense of security. Still, such FTXs are muchbetter preparation for learning to live and functionin the field as part of a huge system than are purelyindividual or small unit training exercises.
The major medical FTX typically has between 300and 600 personnel assigned to play the simulatedcasualties. The FTXs generally try to achieve a mix-ture of simulated surgical wounds and injuries plusnonbattle diseases (including neuropsychiatric dis-orders), which conforms roughly to the expectedincidence in mid- to high-intensity conflict. Theymay include battle fatigue casualties. Chemical ca-sualties are usually included and nuclear casualtiesmay be included.

Educating Mental Health Workers
205
Role players who simulate soldiers who havediseases or minor injuries can be briefed quickly atthe FTX patient operations center (POC). Role play-ers with simulated surgical wounds must receiveextensive make-up (“moulage”) from a trainedmoulage team at the POC. Make-up artists do aremarkable job of mimicking serious and evengrossly deforming wounds.
The realism of the moulage is one of the factors(along with sleep loss, field sights, sounds andsmells, and sometimes the sound of actual artilleryfiring in the distance) that has provoked distressingand even temporarily disabling post-traumatic stresssyndrome symptoms in some medical personnelwho have had previous combat experience in Viet-nam or other conflicts. Such persons may requesthelp themselves or be referred to the CSC teams tohelp them deal with their memories. Many moremay simply “tough it out” and then perhaps decideto leave the army, national guard, or reserves ratherthan face another painful training exercise. This isone of the reasons why the CSC teams have activeand visible outreach programs.
Most of the simulated patients are picked up atthe patient moulage center and taken directly to oneof the medical treatment facilities by the helicopteror ground ambulances that are dispatched to trans-port them. A few patients may be taken by truck toremote field sites, where the ambulances must findthem. The patient players in these FTXs may bemade up and sent out once, twice, or even threetimes in a 12-hour shift. The number of times de-pends on how extensive their make-up is and theprognosis of the injury. Those who can be treatedand released quickly, or who are “dead on arrival”or “die” soon after they reach the clearing company,can be returned to the POC by a shuttle service andbe recycled quickly. For the role players, the expe-rience can be tiring and uncomfortable. They arecovered with make-up and prosthetic rubber orplastic, strapped to a litter, and then transported inthe summer heat in a vibrating helicopter or bounc-ing ground ambulance to one or more medical fa-cilities where they may wait for minutes to hours tobe examined. It is a demanding job.
The patient players are often members of anothermedical unit within the medical brigade’s area (suchas a general hospital) that has been tasked to pro-vide “patients” as its part in the FTX. They usuallyserve as patients for the entire 4 to 5 days of continu-ous scenario operations. They are “guaranteed”time to eat and sleep, but that guarantee may bedisrupted by transportation difficulties or the in-
hospitable field or barracks environment. In otherFTXs, the patient players may be borrowed from theparticipating hospitals and other medical units on aday-by-day basis. When national guard divisionsor brigades have been involved in the FTX, someline unit soldiers may be declared casualties and beevacuated through their organic medical platoonsand companies to the corps facilities one time only.These soldiers will not have extensive moulagemake-up unless a moulage team is deployed for-ward. In some FTXs, there may also be volunteerrole players from other organizations, such as thestate’s national guard cadet program. These detailsof where and how the role players are obtainedhave proved very relevant to the real-world stresscontrol missions of the CSC teams.
A recurrent finding32–38 is that both the role play-ers and the medical units become involved in thescenario portion of the FTX with enthusiasm. How-ever, for the medical units the novelty of realisti-cally moulaged patients wears off after a whilebecause the triage and surgical teams only pretendto start the intravenous infusions and insert thenasogastric and chest tubes and only get to ex-plain what surgical procedure they would bedoing. The triagers, operating room teams, andward staffs themselves become progressivelymore s leep deprived, hot , d ir ty , anduncomfortable.They become increasingly short-tempered with and even negligent toward therole-playing patients. That increases the stressand undermines the motivation of the alreadyuncomfortable patients.
Those role players who have been assigned toserve the full duration of the FTX (and even some ofthe volunteers) begin to grow weary of the exercise.Some may actually require the attention of mentalhealth workers for the transient exercise fatiguethey suffer. They begin to find ways to delay orevade being made up and sent out again. By the lastnight, a few may even become “combat refusers,”flatly declaring to the POC (or telephoning hometearfully to family) that they will resign from thearmy if forced to go out again as surgical patients.The result has been that the CSC teams have per-formed excellent service treating the battle fatiguedsurgical moulage players.
Anecdotes from actual exercises help to under-score important points about these experiences.During MEDEX [medical exercise] ’86 (Camp Shelby,Mississippi, 1986), the OM team elements at theclearing companies established ongoing “ventila-tion/gripe” sessions for the surgical and medical

Military Psychiatry: Preparing in Peace for War
206
role players. These sessions were reported by therole players as being very helpful to them. A memo-rable moment in the FTX occurred during a briefafternoon thundershower when lightning struck apine tree that fell and barely missed the tent inwhich such a session was going on.
During the Dusty Bull FTX (Fort Hood, Texas,1988),35 the OM team is credited by the 807th Medi-cal Brigade’s chief of the patient operations (mou-lage) center with “saving” the FTX.42 The moulagerole players became very disgruntled by the eveningof the fourth day, and the corps surgeon and POCleader consulted the OM team. They immediatelyimplemented the recommendations to call a tempo-rary halt to give all role players food and sleep.Meanwhile, the OM team sent a contingent on nightconvoy to the POC and, early in the morning, initi-ated a concentrated schedule of debriefing sessionsmixed with entertainment that had the role playersready to continue the FTX soon after sunrise.
Wounded Warrior ’92 (Camp Roberts, Califor-nia, 1992) provided an even more dramatic real-world demonstration of the value of a multidisci-plinary, multipurpose stress control team. The12-person CSC team was composed of a psychia-trist, psychiatric nurses, social workers, and en-listed behavioral and psychiatry specialists fromthree reserve OM teams. No simulated combat stresscasualties were scheduled among the surgical andmedical patient play because there was a shortageof patient role players. The “patients” were maleand female members of a state cadet organization,aged 11 to 19 years. The cadets had been enlistedinitially to play only a 1-day, joint military/civiliandisaster medical assistance team earthquake sce-nario. They had agreed to continue through a 4-daycontinuous (12-hour shifts) battle casualty scenario.By the first day of the army exercise, it was clear thatthe cadets’ cadre were not able to keep the adoles-cent cadets sufficiently occupied (on an old armypost) while they were offshift. A social workerand two technicians from the CSC team, who hadcivilian expertise with adolescents, were pulledin from the field to advise and train the cadetcadre, to establish a program of recreational ac-tivities, and to maintain order in the barracks’dormitories.
One of the young female cadets became extremelyagitated while she was being driven out to the fieldin an ambulance as a surgical wound case. She hadasked to be allowed to use one of the portablelatrines and had then perceived the behavior of themale medics as a sexual assault. The cadet reported
this perception by telephone to her mother, and thepost provost marshall was notified. Fortunately forall, the female social worker was able to work thera-peutically with the cadet that evening. Several yearsearlier, that cadet had been molested in a publicrestroom, which made her especially sensitive tothe threat of sexual assault. The next day, when theformal hearing was held, the girl’s testimony ofwhat the ambulance medics had done and the testi-mony of the medics themselves were sufficient toconvince everyone that only poor judgment, notwrongful intent, had been involved. The timelyassistance of a trained mental health worker helpedthe cadet work through a psychological trauma—and also arguably saved the careers of more thanjust the ambulance medics if the accusations hadreached the news media.
Thus, the psychiatric (stress control) detachmentscan be fully and profitably occupied in these FTXsby concentrating on their real-world preventiveand treatment missions. Unlike the surgical teams(and like the dental, preventive medicine, and vet-erinary food inspection teams), they have plenty ofreal-world missions, provided they are proactive,mobile, and helpful. They must not remain in theirtents waiting for “patients” to be sent to them.Indeed the people who would send such cases tothem (or come on their own behalf) are more likelyto misunderstand and mistrust the mental healthteams if those teams are relying only on their pro-fessional reputations.
In fact, too much simulated stress casualtyplay may actually be counterproductive. It maykeep the mental health teams so busy (doingwhat they already know fairly well how to do)that they put off undertaking the new challengesof going out, meeting, and forming trusting pro-fessional relationships with all of the units thatthey should be supporting. They need to becomefully familiar with the missions and stressors ofthe supported units.
The major medicine FTXs (especially the earlierones—Dusty Bull ’84 and ’88, Wounded Warrior’85, and MEDEX ’86) did have extensive simulatedstress casualty play. A mobile training team (MTT)from the Behavioral Sciences Division, Academy ofHealth Sciences, U.S. Army (San Antonio, Texas),was requested through command channels41 by themedical brigades to assist in training the OM teamsand guiding their employment. The MTT also as-sured that a suitable number and variety of simu-lated battle fatigue and neuropsychiatric casualtieswere played.

Educating Mental Health Workers
207
The moulage source book43 provides very fewneuropsychiatric and combat stress roles (withsample field medical cards). The battle fatigue casesare mostly the dramatic (but actually rare) andproblematic cases. The recommended treatment(contrary to current doctrine) is to prescribediazepam (Valium) or chlorpromazine (Thorazine).The neuropsychiatric cases are also rather limited.For example, the alcoholic with impending deliriumtremens has physical findings (such as a large andtender liver with ascites). That would be common,perhaps, in a big city hospital emergency room butwould not be typical of the heavy drinking butotherwise successful army NCO or officer who mightgo into delirium tremens if he suddenly cuts backfrom his regular heavy daily drinking. The soldier-alcoholic’s general health and physical fitness mightappear good with only the more subtle signs ofheavy alcohol use.41 The army’s programs of physi-cal fitness testing, weight control, the mandatoryphysical periodic examination, annual performanceappraisals with interim counseling sessions, plusthe Alcohol and Drug Abuse Prevention and Con-trol Program are usually sufficient to detect thegross signs of chronic physical deterioration be-cause of alcohol abuse.41
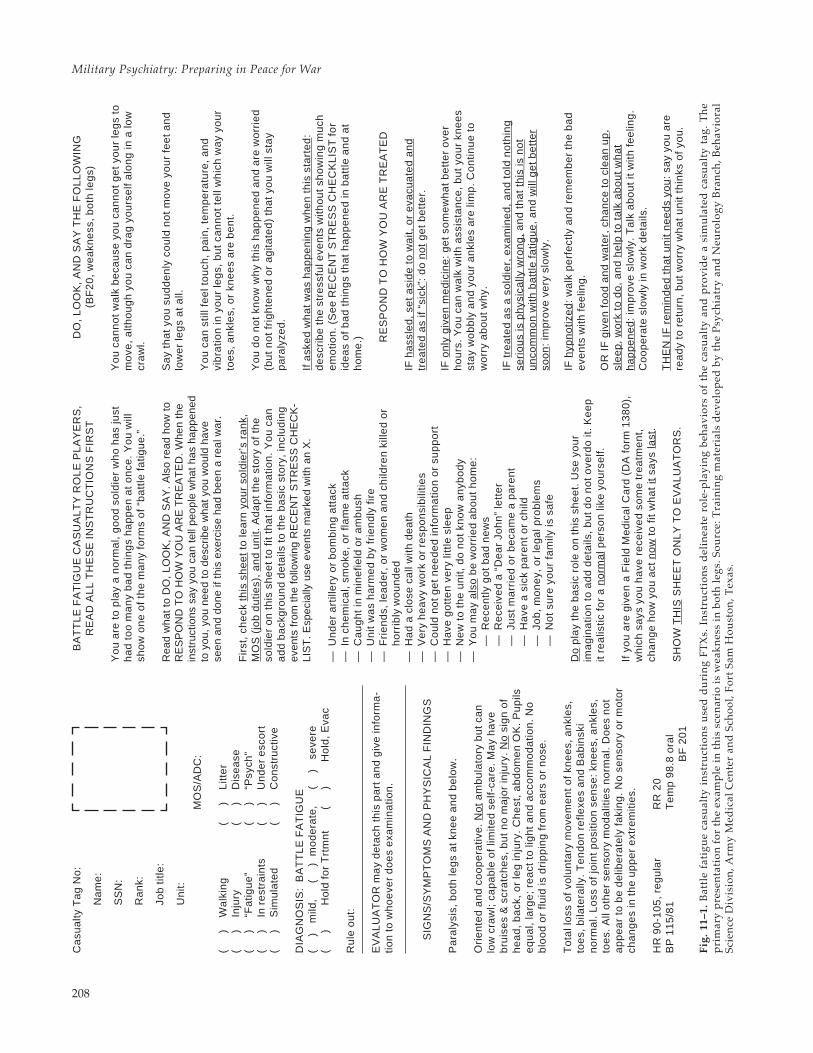
To provide a wider variety and more representa-tive sample of battle fatigue and neuropsychiatriccases, the MTT has fielded and tested a set of roleplayer instruction sheets. Examples are given inFigures 11–1, 11–2, and 11–3.
Each instruction sheet included the field medicalcard (DA Form 1380) entries and physical findings.It included general instructions to the role playersplus a checklist of recent stress events they shouldincorporate into their story about themselves. Itgives specific instructions on what to do, how tolook, and what to say, plus further instruction onhow to change or not change the scenario based onhow they are treated.
The battle fatigue cases have been written in setsof 20 cases. Each case is unique, but in each set, thereare three simple exhaustion/sleep deprivation cases,five with primarily anxiety symptoms, five withprimarily depressive and/or survivor guilt symp-toms, three variations on dissociative (memory loss)symptoms, and four variations on conversion symp-toms. This breakout still somewhat favors the dra-matic and problematic end of the battle fatiguespectrum at the expense of the more common ex-hausted, anxious, and depressed forms. However,that shift is appropriate for corps-level or divisionrear-level exercises, where most of the simpler cases
can be assumed to have been treated and releasedfurther forward.
The instructions deliberately omit the stereotypi-cal “pseudopsychotic,” “acting out,” and potentialviolent types of battle fatigue cases. This omissionwas done for two reasons. First, they are actuallyrare, and it is important to counteract that stereo-type lest it become a self-fulfilling prophecy assoldiers become overly suggestible with battle fa-tigue. Second, there will always be a few role play-ers who will overact or use this opportunity ofplaying a stress casualty as a license to play“psycho,” in spite of warnings not to.
In addition to the 60 variations on battle fatigue,instructions were written for neuropsychiatric cases,including a manic episode, paranoid schizophrenic-like psychoses, acute organic brain syndromes (at-ropine or anticholinergic type), alcohol withdrawal,and other substance abuse problems. Some of thesecases require additional administrative or legal ac-tion. Some of these cases do provide for the playersto become threatening and disruptive. This willgive the medical or psychiatric triagers and treatersthe opportunity to practice safe management andrestraining techniques without erroneously target-ing battle fatigue as the likely cause. The players ofthese roles must be strongly instructed not to con-tinue their resistance to the point where they orothers get hurt.
Interestingly, there was a case during MEDEX‘8634 when one of the nonviolent battle fatiguecases—a soldier with psychogenic deafness whowas pretending to be unable to hear instructions orquestions—was wrestled to the ground and his eyeglasses broken by overzealous triage and securitypersonnel who mistakenly identified him as either a“psycho” or an enemy infiltrator. All of the observerand controller personnel in the FTXs must be trainedto intervene to prevent such unnecessary safety viola-tions by the role-playing patient or the treaters.
Several “special combat stress cases” that in-volve misconduct and other legal issues have alsobeen prepared as role player instruction sheets.Examples are the soldier who confesses that theguilt he is feeling comes from having participated inthe commission of an atrocity or the “combat refuser”who describes a pacifistic religious conversion ex-perience while under extreme stress. These casesprovide training not only in clinical managementbut also in the administrative actions that should beinitiated and followed through the system.
The role player instruction sheets are sufficientlydetailed that a reasonably literate and motivated
Military Psychiatry: Preparing in Peace for War
208
DO
, L
OO
K,
AN
D S
AY
TH
E F
OL
LO
WIN
G(B
F2
0,
we
akn
ess
, b
oth
leg
s)
Yo
u c
an
no
t w
alk
be
cau
se y
ou
ca
nn
ot
ge
t yo
ur
leg
s to
mo
ve,
alth
ou
gh
yo
u c
an
dra
g y
ou
rse
lf a
lon
g in
a lo
wcr
aw
l.
Sa
y th
at
you
su
dd
en
ly c
ou
ld n
ot
mo
ve y
ou
r fe
et
an
dlo
we
r le
gs
at
al l.
Yo
u c
an
sti l
l fe
el t
ou
ch,
pa
in,
tem
pe
ratu
re,
an
dvi
bra
tion
in y
ou
r le
gs,
bu
t ca
nn
ot
tel l
wh
ich
wa
y yo
ur
toe
s, a
nkl
es,
or
kne
es
are
be
nt.
Yo
u d
o n
ot
kno
w w
hy
this
ha
pp
en
ed
an
d a
re w
orr
ied
(bu
t n
ot
frig
hte
ne
d o
r a
gita
ted
) th
at
you
wil l
sta
yp
ara
lyze
d.
If a
ske
d w
ha
t w
as
ha
pp
en
ing
wh
en
th
is s
tart
ed
:d
esc
rib
e t
he
str
ess
ful e
ven
ts w
itho
ut
sho
win
g m
uch
em
otio
n.
(Se
e R
EC
EN
T S
TR
ES
S C
HE
CK
LIS
T f
or
ide
as
of
ba
d t
hin
gs
tha
t h
ap
pe
ne
d in
ba
ttle
an
d a
th
om
e.) R
ES
PO
ND
TO
HO
W Y
OU
AR
E T
RE
AT
ED
IF h
ass
led
, se
t a
sid
e t
o w
ait,
or
eva
cua
ted
an
dtr
ea
ted
as
if “s
ick”
: d
o n
ot
ge
t b
ett
er.
IF o
nly
giv
en
me
dic
ine
: g
et
som
ew
ha
t b
ett
er
ove
rh
ou
rs.
Yo
u c
an
wa
lk w
ith a
ssis
tan
ce,
bu
t yo
ur
kne
es
sta
y w
ob
bly
an
d y
ou
r a
nkl
es
are
lim
p.
Co
ntin
ue
to
wo
rry
ab
ou
t w
hy.
IF t
rea
ted
as
a s
old
ier,
exa
min
ed
, a
nd
to
ld n
oth
ing
seri
ou
s is
ph
ysic
ally
wro
ng
, a
nd
th
at
this
is n
ot
un
com
mo
n w
ith b
att
le f
atig
ue
, a
nd
will
ge
t b
ett
er
soo
n:
imp
rove
ve
ry s
low
ly.
IF h
ypn
otiz
ed
: w
alk
pe
rfe
ctly
an
d r
em
em
be
r th
e b
ad
eve
nts
with
fee
ling
.
OR
IF
giv
en
fo
od
an
d w
ate
r, c
ha
nce
to
cle
an
up
,sl
ee
p,
wo
rk t
o d
o,
an
d h
elp
to
ta
lk a
bo
ut
wh
at
ha
pp
en
ed
: im
pro
ve s
low
ly.
Ta
lk a
bo
ut
it w
ith f
ee
ling
.C
oo
pe
rate
slo
wly
in w
ork
de
tails
.
TH
EN
IF
re
min
de
d t
ha
t u
nit
ne
ed
s yo
u:
say
you
are
rea
dy
t o r
et u
rn,
bu
t w
orr
y w
ha
t u
nit
t hin
ks o
f yo
u.
BA
TT
LE
FA
TIG
UE
CA
SU
AL
TY
RO
LE
PL
AY
ER
S,
RE
AD
AL
L T
HE
SE
IN
ST
RU
CT
ION
S F
IRS
T
Yo
u a
re t
o p
lay
a n
orm
al,
go
od
so
ldie
r w
ho
ha
s ju
sth
ad
to
o m
an
y b
ad
th
ing
s h
ap
pe
n a
t o
nce
. Y
ou
will
sho
w o
ne
of
the
ma
ny
form
s o
f “b
att
le f
atig
ue
.”
Rea
d w
hat t
o D
O, L
OO
K, A
ND
SA
Y. A
lso
read
how
toR
ES
PO
ND
TO
HO
W Y
OU
AR
E T
RE
AT
ED
. Whe
n th
ein
stru
ctio
ns s
ay y
ou c
an te
l l pe
ople
wha
t has
hap
pene
dto
you
, you
nee
d to
des
crib
e w
hat y
ou w
ould
hav
ese
en a
nd d
one
if th
is e
xerc
ise
had
been
a r
eal w
ar.
Fir
st,
che
ck t
his
sh
ee
t to
lea
rn y
ou
r so
ldie
r’s
ran
k,M
OS
(jo
b d
utie
s),
an
d u
nit.
Ad
ap
t th
e s
tory
of
the
sold
ier
on
th
is s
he
et
to f
it th
at
info
rma
tion
. Y
ou
ca
na
dd
ba
ckg
rou
nd
de
tai ls
to
th
e b
asi
c st
ory
, in
clu
din
gev
ents
from
the
fol lo
win
g R
EC
EN
T S
TR
ES
S C
HE
CK
-LI
ST
. Esp
ecia
l ly u
se e
vent
s m
arke
d w
ith a
n X
.
—U
nd
er
art
i l le
ry o
r b
om
bin
g a
tta
ck—
In c
he
mic
al,
smo
ke,
or
flam
e a
tta
ck—
Ca
ug
ht
in m
ine
field
or
am
bu
sh—
Un
it w
as
ha
rme
d b
y fr
ien
dly
fir
e—
Fri
en
ds,
lea
de
r, o
r w
om
en
an
d c
hild
ren
kill
ed
or
ho
rrib
ly w
ou
nd
ed
—H
ad
a c
lose
ca
ll w
ith d
ea
th—
Ve
ry h
ea
vy w
ork
or
resp
on
sib
ilitie
s—
Co
uld
no
t g
et
ne
ed
ed
info
rma
tion
or
sup
po
rt—
Ha
ve g
ott
en
ve
ry li
ttle
sle
ep
—N
ew
to
th
e u
nit,
do
no
t kn
ow
an
ybo
dy
—Y
ou
ma
y a
lso
be
wo
rrie
d a
bo
ut
ho
me
:—
Re
cen
tly g
ot
ba
d n
ew
s—
Re
ceiv
ed
a “
De
ar
Joh
n”
lett
er
—Ju
st m
arr
ied
or
be
cam
e a
pa
ren
t—
Ha
ve a
sic
k p
are
nt
or
child
—Jo
b,
mo
ne
y, o
r le
ga
l pro
ble
ms
—N
ot
sure
yo
ur
fam
ily is
sa
fe
Do
pla
y th
e b
asi
c ro
le o
n t
his
sh
ee
t. U
se y
ou
rim
ag
ina
tion
to
ad
d d
eta
ils,
bu
t d
o n
ot
ove
rdo
it.
Ke
ep
it re
alis
tic f
or
a n
orm
al p
ers
on
like
yo
urs
elf.
If y
ou
are
giv
en
a F
ield
Me
dic
al C
ard
(D
A f
orm
13
80
),w
hic
h s
ays
yo
u h
ave
re
ceiv
ed
so
me
tre
atm
en
t,ch
an
ge
ho
w y
ou
act
no
w t
o f
it w
ha
t it
says
last
.
SH
OW
TH
IS S
HE
ET
ON
LY
TO
EV
AL
UA
TO
RS
.
Fig.
11–
1. B
attl
e fa
tigu
e ca
sual
ty i
nst
ruct
i on
s u
sed
du
rin
g FT
Xs.
In
stru
cti o
ns
del
i nea
te r
ole-
pl a
yin
g be
hav
i ors
of
the
casu
alty
an
d p
rovi
de
a si
mu
l ate
d c
asu
alty
tag
. T
he
pri
mar
y p
rese
nta
tion
for
th
e ex
amp
l e i n
th
i s s
cen
ari o
i s w
eakn
ess
i n b
oth
l egs
. Sou
rce:
Tra
i ni n
g m
ater
i al s
dev
elop
ed b
y th
e P
sych
i atr
y an
d N
euro
l ogy
Bra
nch
, Beh
avi o
ral
Sci e
nce
Di v
i si o
n, A
rmy
Med
i cal
Cen
ter
and
Sch
ool ,
Fort
Sam
Hou
ston
, Tex
as.
Ca
sua
lty T
ag
No
:
Na
me
:
SS
N:
Ra
nk:
Job
title
:
Un
it:
MO
S/A
DC
:
(
)
Wa
lkin
g(
)L
itte
r(
)In
jury
(
)
Dis
ea
se(
)“F
atig
ue
”(
)“P
sych
”(
)In
re
stra
ints
(
)
Un
de
r e
sco
rt(
)S
imu
late
d(
)C
on
stru
ctiv
e
DIA
GN
OS
IS:
BA
TT
LE
FA
TIG
UE
(
)
mi ld
,
(
)
m
od
era
te,
(
)
se
vere
(
)
Ho
ld f
or
Trt
mn
t(
)H
old
, E
vac
Ru
le o
ut:
EV
AL
UA
TO
R m
ay
de
tach
th
is p
art
an
d g
ive
info
rma
-tio
n t
o w
ho
eve
r d
oe
s e
xam
ina
tion
.
SIG
NS
/SY
MP
TO
MS
AN
D P
HY
SIC
AL
FIN
DIN
GS
Pa
raly
sis,
bo
th le
gs
at
kne
e a
nd
be
low
.
Ori
en
ted
an
d c
oo
pe
rativ
e.
No
t a
mb
ula
tory
bu
t ca
nlo
w c
raw
l; ca
pa
ble
of
limite
d s
elf-
care
. M
ay
ha
veb
ruis
es
& s
cra
tch
es,
bu
t n
o m
ajo
r in
jury
. N
o s
ign
of
he
ad
, b
ack
, o
r le
g in
jury
. C
he
st,
ab
do
me
n O
K.
Pu
pils
eq
ua
l, la
rge
; re
act
to
lig
ht
an
d a
cco
mm
od
atio
n.
No
blo
od
or
fluid
is d
rip
pin
g f
rom
ea
rs o
r n
ose
.
To
tal l
oss
of
volu
nta
ry m
ove
me
nt
of
kne
es,
an
kle
s,to
es,
bila
tera
lly. T
en
do
n r
efle
xes
an
d B
ab
insk
in
orm
al.
Lo
ss o
f jo
int
po
sitio
n s
en
se:
kne
es,
an
kle
s,to
es.
All
oth
er
sen
sory
mo
da
litie
s n
orm
al.
Do
es
no
ta
pp
ea
r to
be
de
libe
rate
ly f
aki
ng
. N
o s
en
sory
or
mo
tor
cha
ng
es
in t
he
up
pe
r e
xtre
miti
es.
HR
90
-10
5,
reg
ula
rR
R 2
0B
P 1
15
/81
Te
mp
98
.8 o
ral
BF
20
1
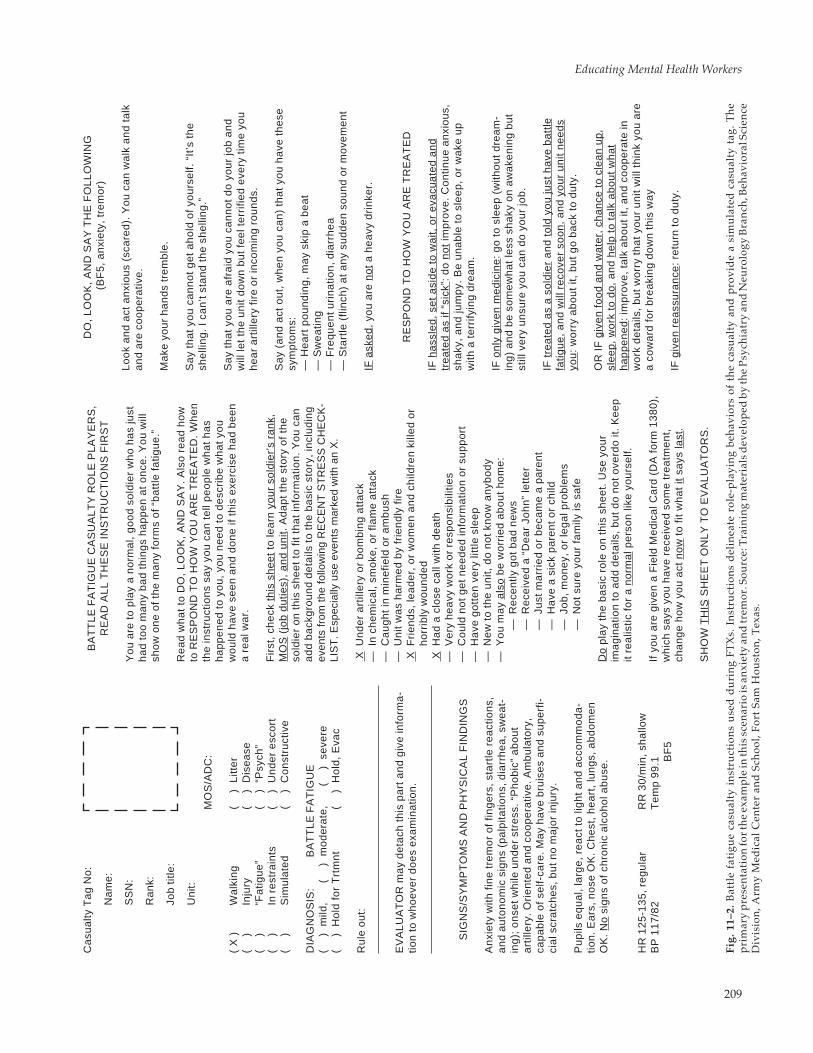
Educating Mental Health Workers
209
Ca
sua
lty T
ag
No
:
Na
me
:
SS
N:
Ra
nk:
Job
title
:
Un
it:
MO
S/A
DC
:
( X
)W
alk
ing
(
)
Litt
er
(
)In
jury
(
)
Dis
ea
se(
)
“Fa
tigu
e”
(
)
“Psy
ch”
(
)In
re
stra
ints
(
)
Un
de
r e
sco
rt(
)
Sim
ula
ted
(
)
Co
nst
ruct
ive
DIA
GN
OS
IS:
BA
TT
LE
FA
TIG
UE
(
)
mi ld
,
(
) m
od
era
te,
(
)
se
vere
(
)
Ho
ld f
or
Trt
mn
t(
)
H
old
, E
vac
Ru
le o
ut:
EV
AL
UA
TO
R m
ay
de
tach
th
is p
art
an
d g
ive
info
rma
-tio
n t
o w
ho
eve
r d
oe
s e
xam
ina
tion
.
SIG
NS
/SY
MP
TO
MS
AN
D P
HY
SIC
AL
FIN
DIN
GS
An
xie
ty w
ith f
ine
tre
mo
r o
f fin
ge
rs,
sta
rtle
re
act
ion
s,a
nd
au
ton
om
ic s
ign
s (p
alp
itatio
ns,
dia
rrh
ea
, sw
ea
t-in
g);
on
set
wh
ile u
nd
er
stre
ss.
“Ph
ob
ic”
ab
ou
ta
rtill
ery
. Ori
en
ted
an
d c
oo
pe
rativ
e. A
mb
ula
tory
,ca
pa
ble
of
self-
care
. M
ay
ha
ve b
ruis
es
an
d s
up
erf
i-ci
al s
cra
tch
es,
bu
t n
o m
ajo
r in
jury
.
Pu
pils
eq
ua
l, la
rge
, re
act
to
lig
ht
an
d a
cco
mm
od
a-
tion
. E
ars
, n
ose
OK
. C
he
st,
he
art
, lu
ng
s, a
bd
om
en
OK
. N
o s
ign
s o
f ch
ron
ic a
lco
ho
l ab
use
.
HR
12
5-1
35
, re
gu
lar
RR
30
/min
, sh
allo
wB
P 1
17
/82
Te
mp
99
.1 BF
5
BA
TT
LE
FA
TIG
UE
CA
SU
AL
TY
RO
LE
PL
AY
ER
S,
RE
AD
AL
L T
HE
SE
IN
ST
RU
CT
ION
S F
IRS
T
Yo
u a
re t
o p
lay
a n
orm
al,
go
od
so
ldie
r w
ho
ha
s ju
sth
ad
to
o m
an
y b
ad
th
ing
s h
ap
pe
n a
t o
nce
. Y
ou
will
sho
w o
ne
of
the
ma
ny
form
s o
f “b
att
le f
atig
ue
.”
Re
ad
wh
at
to D
O,
LO
OK
, A
ND
SA
Y.
Als
o r
ea
d h
ow
to R
ES
PO
ND
TO
HO
W Y
OU
AR
E T
RE
AT
ED
. W
he
nth
e in
stru
ctio
ns
say
you
ca
n t
el l
pe
op
le w
ha
t h
as
ha
pp
en
ed
to
yo
u,
you
ne
ed
to
de
scri
be
wh
at
you
wo
uld
ha
ve s
ee
n a
nd
do
ne
if t
his
exe
rcis
e h
ad
be
en
a r
ea
l wa
r.
Fir
st,
che
ck t
his
sh
ee
t to
lea
rn y
ou
r so
ldie
r’s
ran
k,M
OS
(jo
b d
utie
s),
an
d u
nit.
Ad
ap
t th
e s
tory
of
the
sold
ier
on
th
is s
he
et
to f
it th
at
info
rma
tion
. Y
ou
ca
na
dd
ba
ckg
rou
nd
de
tai ls
to
th
e b
asi
c st
ory
, in
clu
din
gev
ents
from
the
fol lo
win
g R
EC
EN
T S
TR
ES
S C
HE
CK
-LI
ST
. Esp
ecia
l ly u
se e
vent
s m
arke
d w
ith a
n X
.
XU
nd
er
art
ille
ry o
r b
om
bin
g a
tta
ck—
In c
he
mic
al,
smo
ke,
or
flam
e a
tta
ck—
Ca
ug
ht
in m
ine
field
or
am
bu
sh—
Un
it w
as
ha
rme
d b
y fr
ien
dly
fir
e X
Fri
en
ds,
lea
de
r, o
r w
om
en
an
d c
hild
ren
kill
ed
or
ho
rrib
ly w
ou
nd
ed
XH
ad
a c
lose
ca
ll w
ith d
ea
th—
Ve
ry h
ea
vy w
ork
or
resp
on
sib
ilitie
s—
Co
uld
no
t g
et
ne
ed
ed
info
rma
tion
or
sup
po
rt—
Ha
ve g
ott
en
ve
ry li
ttle
sle
ep
—N
ew
to
th
e u
nit,
do
no
t kn
ow
an
ybo
dy
—Y
ou
ma
y a
lso
be
wo
rrie
d a
bo
ut
ho
me
:—
Re
cen
tly g
ot
ba
d n
ew
s—
Re
ceiv
ed
a “
De
ar
Joh
n”
lett
er
—Ju
st m
arr
ied
or
be
cam
e a
pa
ren
t—
Ha
ve a
sic
k p
are
nt
or
child
—Jo
b,
mo
ne
y, o
r le
ga
l pro
ble
ms
—N
ot
sure
yo
ur
fam
ily is
sa
fe
Do
pla
y th
e b
asi
c ro
le o
n t
his
sh
ee
t. U
se y
ou
rim
ag
ina
tion
to
ad
d d
eta
ils,
bu
t d
o n
ot
ove
rdo
it.
Ke
ep
it re
alis
tic f
or
a n
orm
al p
ers
on
like
yo
urs
elf.
If y
ou
are
giv
en
a F
ield
Me
dic
al C
ard
(D
A f
orm
13
80
),w
hic
h s
ays
yo
u h
ave
re
ceiv
ed
so
me
tre
atm
en
t,ch
an
ge
ho
w y
ou
act
no
w t
o f
it w
ha
t it
says
last
.
SH
OW
TH
I S S
HE
ET
ON
LY
TO
EV
AL
UA
TO
RS
.
DO
, L
OO
K,
AN
D S
AY
TH
E F
OL
LO
WIN
G (
BF
5,
an
xie
ty,
tre
mo
r)
Lo
ok
an
d a
ct a
nxi
ou
s (s
care
d).
Yo
u c
an
wa
lk a
nd
ta
lka
nd
are
co
op
era
tive
.
Ma
ke y
ou
r h
an
ds
tre
mb
le.
Sa
y th
at
you
ca
nn
ot
ge
t a
ho
ld o
f yo
urs
elf.
“It
’s t
he
she
ll in
g.
I ca
n’t
sta
nd
th
e s
he
ll in
g.”
Sa
y th
at
you
are
afr
aid
yo
u c
an
no
t d
o y
ou
r jo
b a
nd
wil l
let
the
un
it d
ow
n b
ut
fee
l te
rrifi
ed
eve
ry t
ime
yo
uh
ea
r a
rti l l
ery
fir
e o
r in
com
ing
ro
un
ds.
Sa
y (a
nd
act
ou
t, w
he
n y
ou
ca
n)
tha
t yo
u h
ave
th
ese
sym
pto
ms:
— H
ea
rt p
ou
nd
ing
, m
ay
skip
a b
ea
t—
Sw
ea
ting
— F
req
ue
nt u
rin
atio
n, d
iarr
he
a—
Sta
rtle
(fli
nch
) a
t a
ny
sud
de
n s
ou
nd
or
mo
vem
en
t
IF a
ske
d,
you
are
no
t a
he
avy
dri
nke
r.
RE
SP
ON
D T
O H
OW
YO
U A
RE
TR
EA
TE
D
IF h
ass
led
, se
t a
sid
e t
o w
ait,
or
eva
cua
ted
an
dtr
ea
ted
as
if “s
ick”
: d
o n
ot
imp
rove
. C
on
tinu
e a
nxi
ou
s,sh
aky
, a
nd
jum
py.
Be
un
ab
le t
o s
lee
p,
or
wa
ke u
pw
ith a
te
rrify
ing
dre
am
.
IF o
nly
giv
en
me
dic
ine
: g
o t
o s
lee
p (
with
ou
t d
rea
m-
ing
) a
nd
be
so
me
wh
at
less
sh
aky
on
aw
ake
nin
g b
ut
still
ve
ry u
nsu
re y
ou
ca
n d
o y
ou
r jo
b.
IF t
rea
ted
as
a s
old
ier
an
d t
old
yo
u ju
st h
ave
ba
ttle
fatig
ue
, a
nd
will
re
cove
r so
on
, a
nd
yo
ur
un
it n
ee
ds
you
: w
orr
y a
bo
ut
it, b
ut
go
ba
ck t
o d
uty
.
OR
IF
giv
en
fo
od
an
d w
ate
r, c
ha
nce
to
cle
an
up
,sl
ee
p,
wo
rk t
o d
o,
an
d h
elp
to
ta
lk a
bo
ut
wh
at
ha
pp
en
ed
: im
pro
ve,
talk
ab
ou
t it,
an
d c
oo
pe
rate
inw
ork
de
tails
, b
ut
wo
rry
tha
t yo
ur
un
it w
ill th
ink
you
are
a c
ow
ard
fo
r b
rea
kin
g d
ow
n t
his
wa
y
IF g
ive
n r
ea
ssu
ran
ce:
retu
rn t
o d
uty
.
Fig.
11–
2. B
attl
e fa
tigu
e ca
sual
ty i
nst
ruct
i on
s u
sed
du
rin
g FT
Xs.
In
stru
cti o
ns
del
i nea
te r
ole-
pl a
yin
g be
hav
i ors
of
the
casu
alty
an
d p
rovi
de
a si
mu
l ate
d c
asu
alty
tag
. T
he
pri
mar
y p
rese
nta
tion
for t
he
exam
pl e
i n th
i s s
cen
ari o
i s a
nxi
ety
and
trem
or. S
ourc
e: T
rai n
i ng
mat
eri a
l s d
evel
oped
by
the
Psy
chia
try
and
Neu
rol o
gy B
ran
ch, B
ehav
i ora
l Sci
ence
Di v
i si o
n, A
rmy
Med
i cal
Cen
ter
and
Sch
ool ,
Fort
Sam
Hou
ston
, Tex
as.
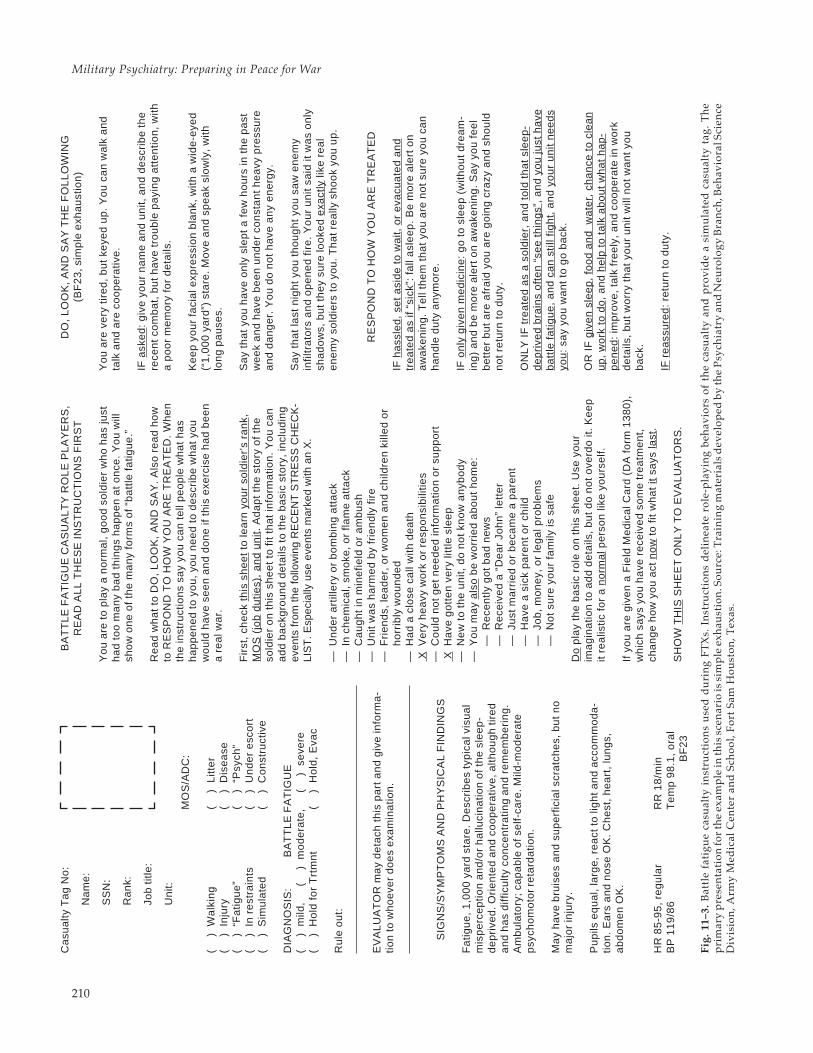
Military Psychiatry: Preparing in Peace for War
210
Ca
sua
lty T
ag
No
:
Na
me
:
SS
N:
Ra
nk:
Job
title
:
Un
it:
MO
S/A
DC
:
(
)
Wa
lkin
g(
)
L
itte
r(
)
In
jury
(
)
Dis
ea
se(
)
“F
atig
ue
”(
)
“P
sych
”(
)
In
re
stra
ints
(
)
Un
de
r e
sco
rt(
)
S
imu
late
d(
)
C
on
stru
ctiv
e
DIA
GN
OS
IS:
BA
TT
LE
FA
TIG
UE
(
)
mi ld
,
(
)
m
od
era
te,
(
)
seve
re(
)
H
old
fo
r T
rtm
nt
(
)
Ho
ld,
Eva
c
Ru
le o
ut:
EV
AL
UA
TO
R m
ay
de
tach
th
is p
art
an
d g
ive
info
rma
-tio
n t
o w
ho
eve
r d
oe
s e
xam
ina
tion
.
SIG
NS
/SY
MP
TO
MS
AN
D P
HY
SIC
AL
FIN
DIN
GS
Fa
tigu
e,
1,0
00
ya
rd s
tare
. D
esc
rib
es
typ
ica
l vis
ua
lm
isp
erc
ep
tion
an
d/o
r h
allu
cin
atio
n o
f th
e s
lee
p-
de
pri
ved
. Ori
en
ted
an
d c
oo
pe
rativ
e, a
ltho
ug
h ti
red
an
d h
as
diff
icu
lty c
on
cen
tra
ting
an
d r
em
em
be
rin
g.
Am
bu
lato
ry; c
ap
ab
le o
f se
lf-ca
re. M
ild-m
od
era
tep
sych
om
oto
r re
tard
atio
n.
Ma
y h
ave
bru
ise
s a
nd
su
pe
rfic
ial s
cra
tch
es,
bu
t n
om
ajo
r in
jury
.
Pu
pils
eq
ua
l, la
rge
, re
act
to
lig
ht
an
d a
cco
mm
od
a-
tion
. E
ars
an
d n
ose
OK
. C
he
st,
he
art
, lu
ng
s,a
bd
om
en
OK
.
HR
85
-95
, re
gu
lar
RR
18
/min
BP
11
9/8
6T
em
p 9
8.1
, o
ral
BF
23
BA
TT
LE
FA
TIG
UE
CA
SU
AL
TY
RO
LE
PL
AY
ER
S,
RE
AD
AL
L T
HE
SE
IN
ST
RU
CT
ION
S F
IRS
T
Yo
u a
re t
o p
lay
a n
orm
al,
go
od
so
ldie
r w
ho
ha
s ju
sth
ad
to
o m
an
y b
ad
th
ing
s h
ap
pe
n a
t o
nce
. Y
ou
will
sho
w o
ne
of
the
ma
ny
form
s o
f “b
att
le f
atig
ue
.”
Re
ad
wh
at
to D
O,
LO
OK
, A
ND
SA
Y.
Als
o r
ea
d h
ow
to R
ES
PO
ND
TO
HO
W Y
OU
AR
E T
RE
AT
ED
. W
he
nth
e in
stru
ctio
ns
say
you
ca
n t
el l
pe
op
le w
ha
t h
as
ha
pp
en
ed
to
yo
u,
you
ne
ed
to
de
scri
be
wh
at
you
wo
uld
ha
ve s
ee
n a
nd
do
ne
if t
his
exe
rcis
e h
ad
be
en
a r
ea
l wa
r.
Fir
st,
che
ck t
his
sh
ee
t to
lea
rn y
ou
r so
ldie
r’s
ran
k,M
OS
(jo
b d
utie
s),
an
d u
nit.
Ad
ap
t th
e s
tory
of
the
sold
ier
on
th
is s
he
et
to f
it th
at
info
rma
tion
. Y
ou
ca
na
dd
ba
ckg
rou
nd
de
tai ls
to
th
e b
asi
c st
ory
, in
clu
din
gev
ents
from
the
fol lo
win
g R
EC
EN
T S
TR
ES
S C
HE
CK
-LI
ST
. Esp
ecia
l ly u
se e
vent
s m
arke
d w
ith a
n X
.
—U
nd
er
art
i l le
ry o
r b
om
bin
g a
tta
ck—
In c
he
mic
al,
smo
ke,
or
flam
e a
tta
ck—
Ca
ug
ht
in m
ine
field
or
am
bu
sh—
Un
it w
as
ha
rme
d b
y fr
ien
dly
fir
e—
Fri
en
ds,
lea
de
r, o
r w
om
en
an
d c
hild
ren
kill
ed
or
ho
rrib
ly w
ou
nd
ed
—H
ad
a c
lose
ca
ll w
ith d
ea
th X
Ve
ry h
ea
vy w
ork
or
resp
on
sib
ilitie
s—
Co
uld
no
t g
et
ne
ed
ed
info
rma
tion
or
sup
po
rt X
Ha
ve g
ott
en
ve
ry li
ttle
sle
ep
—N
ew
to
th
e u
nit,
do
no
t kn
ow
an
ybo
dy
—Y
ou
ma
y a
lso
be
wo
rrie
d a
bo
ut
ho
me
:—
Re
cen
tly g
ot
ba
d n
ew
s—
Re
ceiv
ed
a “
De
ar
Joh
n”
lett
er
—Ju
st m
arr
ied
or
be
cam
e a
pa
ren
t—
Ha
ve a
sic
k p
are
nt
or
child
—Jo
b,
mo
ne
y, o
r le
ga
l pro
ble
ms
—N
ot
sure
yo
ur
fam
ily is
sa
fe
Do
pla
y th
e b
asi
c ro
le o
n t
his
sh
ee
t. U
se y
ou
rim
ag
ina
tion
to
ad
d d
eta
ils,
bu
t d
o n
ot
ove
rdo
it.
Ke
ep
it re
alis
tic f
or
a n
orm
al p
ers
on
like
yo
urs
elf.
If y
ou
are
giv
en
a F
ield
Me
dic
al C
ard
(D
A f
orm
13
80
),w
hic
h s
ays
yo
u h
ave
re
ceiv
ed
so
me
tre
atm
en
t,ch
an
ge
ho
w y
ou
act
no
w t
o f
it w
ha
t it
says
last
.
SH
OW
TH
I S S
HE
ET
ON
LY
TO
EV
AL
UA
TO
RS
.
DO
, L
OO
K,
AN
D S
AY
TH
E F
OL
LO
WIN
G(B
F2
3, s
imp
le e
xha
ust
ion
)
Yo
u a
re v
ery
tir
ed
, b
ut
keye
d u
p.
Yo
u c
an
wa
lk a
nd
talk
an
d a
re c
oo
pe
rativ
e.
IF a
ske
d:
giv
e y
ou
r n
am
e a
nd
un
it, a
nd
de
scri
be
th
ere
cen
t co
mb
at,
bu
t h
ave
tro
ub
le p
ayi
ng
att
en
tion
, w
itha
po
or
me
mo
ry f
or
de
tai ls
.
Ke
ep
yo
ur
faci
al e
xpre
ssio
n b
lan
k, w
ith a
wid
e-e
yed
(“1
,00
0 y
ard
”) s
tare
. M
ove
an
d s
pe
ak
slo
wly
, w
ithlo
ng
pa
use
s.
Sa
y th
at
you
ha
ve o
nly
sle
pt
a f
ew
ho
urs
in t
he
pa
stw
ee
k a
nd
ha
ve b
ee
n u
nd
er
con
sta
nt
he
avy
pre
ssu
rea
nd
da
ng
er.
Yo
u d
o n
ot
ha
ve a
ny
en
erg
y.
Sa
y th
at
last
nig
ht
you
th
ou
gh
t yo
u s
aw
en
em
yin
fi ltr
ato
rs a
nd
op
en
ed
fir
e.
Yo
ur
un
it sa
id it
wa
s o
nly
sha
do
ws,
bu
t th
ey
sure
loo
ked
exa
ctly
l ike
re
al
en
em
y so
ldie
rs t
o y
ou
. T
ha
t re
al ly
sh
oo
k yo
u u
p.
RE
SP
ON
D T
O H
OW
YO
U A
RE
TR
EA
TE
D
IF h
ass
led
, se
t a
sid
e t
o w
ait,
or
eva
cua
ted
an
dtr
ea
ted
as
if “s
ick”
: fa
ll a
sle
ep
. B
e m
ore
ale
rt o
na
wa
ken
ing
. T
ell
the
m t
ha
t yo
u a
re n
ot
sure
yo
u c
an
ha
nd
le d
uty
an
ymo
re.
IF o
nly
giv
en
me
dic
ine
: g
o t
o s
lee
p (
with
ou
t d
rea
m-
ing
) a
nd
be
mo
re a
lert
on
aw
ake
nin
g.
Sa
y yo
u f
ee
lb
ett
er
bu
t a
re a
fra
id y
ou
are
go
ing
cra
zy a
nd
sh
ou
ldn
ot
retu
rn t
o d
uty
.
ON
LY
IF
tre
ate
d a
s a
so
ldie
r, a
nd
to
ld t
ha
t sl
ee
p-
de
pri
ved
bra
ins
oft
en
“se
e t
hin
gs”
, a
nd
yo
u ju
st h
ave
ba
ttle
fa
tigu
e,
an
d c
an
stil
l fig
ht,
an
d y
ou
r u
nit
ne
ed
syo
u:
say
you
wa
nt
to g
o b
ack
.
OR
IF
giv
en
sle
ep
, fo
od
an
d w
ate
r, c
ha
nce
to
cle
an
up
, w
ork
to
do
, a
nd
he
lp t
o t
alk
ab
ou
t w
ha
t h
ap
-p
en
ed
: im
pro
ve,
talk
fre
ely
, a
nd
co
op
era
te in
wo
rkd
eta
ils,
bu
t w
orr
y th
at
you
r u
nit
will
no
t w
an
t yo
ub
ack
.
IF r
ea
ssu
red
: re
turn
to
du
ty.
Fig.
11–
3. B
attl
e fa
tigu
e ca
sual
ty i
nst
ruct
i on
s u
sed
du
rin
g FT
Xs.
In
stru
cti o
ns
del
i nea
te r
ole-
pl a
yin
g be
hav
i ors
of
the
casu
alty
an
d p
rovi
de
a si
mu
l ate
d c
asu
alty
tag
. T
he
pri
mar
y p
rese
nta
tion
for
the
exam
pl e
i n th
i s s
cen
ari o
i s s
i mp
l e e
xhau
sti o
n. S
ourc
e: T
rai n
i ng
mat
eri a
l s d
evel
oped
by
the
Psy
chi a
try
and
Neu
rol o
gy B
ran
ch, B
ehav
i ora
l Sci
ence
Di v
i si o
n, A
rmy
Med
i cal
Cen
ter
and
Sch
ool ,
Fort
Sam
Hou
ston
, Tex
as.

Educating Mental Health Workers
211
soldier could take one out of his pocket, read itcarefully, and know how to play a fairly detailedcase using his imagination to fill in the necessarydetails. However, experience shows that it is best toinvest more effort in the selection and training ofbattle fatigue and neuropsychiatric role players.
If there are psychiatric nurses as members of themoulage team, they may be recruited and trainedto choose only those role players who are them-selves mentally stable and able to act the part.Otherwise, members of the MTT must be detailedto do this.
SUMMARY AND CONCLUSION
Military mental health providers function differ-ently from their civilian counterparts. During peace-time missions, they may deal with service memberswho are lonely and frustrated and have any numberof family, occupational, or financial problems. Dur-ing combat, the provider is likely to provide care topatients who are acutely anxious and exhausted.Therefore, not only does the scene of practice changefor the military mental health provider, but the typeof pathology is likely to be different depending onthe setting.
Taken together, this situation means that thepractice of military mental health is grounded in theprinciples of community mental health. The pro-viders perform an occupational health role, focus-ing on preventing combat stress casualties and de-termining the fitness of the individual to function athis given job.
Training military mental health providers startsat the entry level. For specialists, technicians, socialworkers, and psychologists, training is available inthe recognition and treatment of combat stress ca-sualties. Most other providers, such as physicians,and specifically psychiatrists, often have not beentrained in medical school to treat battle fatiguecasualties. An innovative course for medical stu-dents has been described in this chapter. In addi-tion, a model proposal to teach psychiatry residentshow to interact with commanders and hospital per-sonnel in the field is included. Last, the major medi-
cal FTXs have been described in detail. These FTXsare important in the preparation and training of allhealthcare personnel in the proper management ofbattlefield stress casualties. For most mental healthpersonnel, on-the-job training is the best possibleway to learn about the practice of military mentalhealth.
Recommendations for training must take intoaccount military structure. Put simply, the manage-ment of combat stress cannot be taught in the medi-cal center. Psychiatric residents and allied mentalhealth professionals must have exposure to officersand enlisted service members in a variety of mili-tary settings.
With this in mind, the following four specificrecommendations can be made: (1) Develop a shortcourse and training packages in combat stress man-agement that are mandatory for personnel assignedto troop mental health support slots. Include asmany allied healthcare personnel as needed. To besure, nurses, chaplains, and hospital commandersshould be specifically asked to participate in thistraining. (2) Require inclusion of brigade combatstress teams in FTXs, especially at combat trainingcenters. (3) Increase combat stress training in corecareer courses armywide to the level of applicationin practical exercises. (4) Train and program unitmedical and mental health personnel to givesustainment training to unit leaders in the garrisonand field.
REFERENCES
1. Wise MG. The past, present, and future of psychiatric training the U.S. Armed Services. Milit Med.1987;152:550–553.
2. Leamon MH, Sutton LK, Lee RE. Graduate medical educators and infantry commanders: Working together totrain Army psychiatry residents. Milit Med. 1990;155:430–432.
3. US Department of the Army. Combat Stress Control in a Theater of Operations. Washington DC: DA; In press, 1994.Field Manual 8–51.

Military Psychiatry: Preparing in Peace for War
212
4. Hausman W, Rioch DMck. Military psychiatry: A prototype of social and preventive psychiatry in the UnitedStates. Arch Gen Psychiatry. 1967;16:727–739.
5. Bushard B. The U.S. Army’s mental hygiene consultation service. In: Symposium on Preventive and Social Psychiatry.Washington, DC: Walter Reed Army Institute of Research, Walter Reed Army Medical Center, and the NationalResearch Council, 15–17 April 1957.
6. Glass AJ. 1966; Lessons learned. In: Zone of the Interior. Vol 1. In: Glass AJ, Bernucci RJ, eds. Neuropsychiatry inWorld War II. Washington, DC: Office of The Surgeon General, US Department of the Army; 1966: 735–759.
7. Glass AJ. Army psychiatry before World War II. In: Zone of the Interior. Vol 1. In: Glass AJ, Bernucci RJ, eds.Neuropsychiatry in World War II. Washington, DC: Office of The Surgeon General, US Department of the Army;1966: 3–23.
8. Menninger W. Psychiatry in a Troubled World. New York: McMillan; 1948.
9. US Department of the Army. Neuropsychiatry and Mental Health. Washington, DC: DA; 10 August 1984. ArmyRegulation 40–216.
10. US Department of the Air Force, Army, and Navy. Psychiatry in Military Law. Washington, DC: DAF, DA, DN; 25September 1981. Training Manual 8–240.
11. US Department of the Army. Alcohol and Drug Abuse Prevention and Control Program. Washington, DC: DA; 21October 1988. Army Regulation 600–85.
12. Goldman HH, Morrissey JP. The alchemy of mental health policy: Homelessness and the fourth cycle of reform.Am J Public Health. 1985;75:727–731.
13. Koshes RJ., Rothberg JM. Parasuicidal behavior on an active duty Army training post. Milit Med. 1992;157:350–353.
14. Bion WR. Experiences in groups, I. Human Relations. 1948;1(3):314–320.
15. Bion WR. Experiences in groups, II. Human Relations. 1948;1(4):487–496.
16. Bion WR. Experiences in groups, III. Human Relations. 1949;2(1):1322.
17. Bion WR. Experiences in groups, IV. Human Relations. 1949;2(4):295–303.
18. Bion WR. Experiences in groups, V. Human Relations. 1950;3(1):3–14.
19. Bion WR. Experiences in groups, VI. Human Relations. 1950;3(4):395–402.
20. Bion WR. Group dynamics: A Re-view. Int J Psychoanal. 1952;33(2):235–247.
21. Bion WR. Experiences in Groups and Other Papers. New York: Basic Books; 1961.
22. Artiss KL. Military combat and social psychiatry. Presented to the Psychiatry Staff, Tripler Army Medical Center,Honolulu, Hawaii; 12 December 1984.
23. Artiss KL. Human behavior under stress. Milit Med. 1963;128(10):1011–1015.
24. Hibler RJ. Battlefield stress: Management techniques. Milit Med. 1984;149:5–8.
25. Solomon Z. Benbenishty R. The role of proximity, immediacy and expectancy in frontline treatment of combatstress reactions among Israelis in the Lebanon War. Am J Psychiatry. 1986;143(5):613–617.
Educating Mental Health Workers
213
26. Jones FD, Crocq L, Adelaja O, et al. Psychiatric casualties in modern warfare: I. Evolution of treatment. In: PichotP, Berner P, Wolf R, Thau K, eds. Psychiatry: The State of the Art. Vol 6. New York: Plenum Publishing Corporation;1985: 459–464.
27. Jones FD, Johnson AW. Medical and psychiatric treatment policy and practice in Vietnam. J Soc Issues.1975;31(4):49–65.
28. Jones FD. Lessons of war for psychiatry. In: Pichot P, Berner P, Wolf R, Thau K, eds. Psychiatry: The State of the Art.Vol 6. New York: Plenum Publishing Corporation; 1985: 515–519.
29. Hales RE, Jones FD. Teaching the principles of combat psychiatry to Army psychiatry residents. Milit Med.1983;148:24–27.
30. McCaughey BG. Role players: A brief intensive training program to portray acute psychological distress.J Traumatic Stress. 1991;4(4):595–599.
31. McCaughey BG. Observations about battle fatigue: Its occurrence and absence. Milit Med. 1991;156:694–695.
32. Stokes J. Personal Observations, June 1984. Fort Hood, Tex: Dusty Bull ’84.
33. Stokes J. Personal Observations, June 1985. Camp Roberts, Calif: Wounded Warrior ’85.
34. Stokes J. Personal Observations, June 1986. Camp Shelby, Miss: MEDEX ’86.
35. Stokes J. Personal Observations, June 1988. Fort Hood, Tex: Dusty Bull ’88.
36. Stokes J. Personal Observations, June 1988. Camp Roberts, Calif: Wounded Warrior ’88.
37. Stokes J. Personal Observations, 1989. Camp Shelby, Miss: MEDEX ’89.
38. Stokes J. Personal Observations, 1992. Camp Roberts and Camp Pendleton, Calif: Wounded Warrior ’92.
39. US Department of the Army. Health Service Support in a Theater of Operations. Washington DC: DA; 1991. FieldManual 8–10.
40. US Department of the Army. Leader’s Manual for Combat Stress Control. Washington DC: DA; In press, 1994. FieldManual 22–51.
41. Stokes J. Personal Observations.
42. Boatright C. Personal Communication, June 1988.
43. US Department of the Army. Patient Play in Exercises. Washington, DC: DA; Year? GTA 8–12–3(17).