wchob 2011 cpr procedures infant & neonate radiology techs, surgical techs, ot, pt, speech, eeg...
TRANSCRIPT
WCHOB 2011 CPR WCHOB 2011 CPR ProceduresProcedures
InfantInfant & & NeonateNeonate
Radiology Techs, Surgical Techs, OT, PT, Speech, EEG Techs, NA’s
ObjectivesAfter completing this self-learning packet the reader will be
able to:
1. Identify how infant and newborn CPR techniques differ from those of older patients.
2. Apply the American Heart Association's performance
guidelines to case scenarios requiring:
-Infant one rescuer CPR-Infant/newborn Foreign Body Airway Obstruction (FBAO) Management-Newborn CPR
A B CA B C (NEWBORNS) or C A B (C A B (INFANTSINFANTS)) The guidelines 2010 identify specific
differences in CPR techniques for infants and newborns.
InfantsInfants are defined as approximately 1 year of age or less.
NewbornsNewborns are identified as any infant from the time they are born until discharge from WCHOB.
The differences in CPR techniques are outlined in the following program.
So, what else is important ? Breathing for an infant or newborn is extremely important as
arrest issues are frequently related to respiratory issues .
BUT: Ventilation - More breaths are NOT better!
We often over inflate the lungs!
Blood flow to the lungs is decreased in an arrest, therefore, lower respiratory rates/volumes still maintain adequate cardiac function.
Hyperventilation (over inflating the lungs) is Harmful!
Forceful or excessively large breaths given by rescuers can cause the stomach to bloat. This can cause vomiting and aspiration, it can restrict lung movement.
So, what is important for infants and newborns?In a Cardiac Arrest compressions are key!
Compressions need to be hard enough Fast - appropriate to victim’s age Started as soon as the cardiac arrest or
imminent arrest is recognized Maintained with minimal interruption
Initial Steps of Infant CPR No longer will we be doing the A, B, Cs. To emphasize initiation of early
compressions, the steps are now C-A-B:
1. C - compressions
2. A - airway
3. B - breathing
Steps for Infant CPR for Support Staff1. Assess unresponsiveness and absence of normal
breathing.
2. Call for help and a defibrillator.
3. If patient is unresponsive and has no signs of normal breathing, begin CPR compressions.
4. After 30 compressions, open airway and give 2 breaths.
5. Continue CPR at a ratio of 30 compressions to 2 breaths for 2 minutes.
Steps for Infant CPR for Support Staff1. Assess unresponsiveness and observe for
normal breathing.
Tap victim, shout out, “Are you ok?” while simultaneously looking for any signs of normal breathing.
Steps for Infant CPR for Support Staff Assess unresponsiveness and observe for normal
DO NOT Look, Listen and Feel for breathing.
Abnormal breathing is frequently mistaken as presence of respirations.
Cardiac arrest victims may present or initially have a short period of seizure like activity or agonal gasps - this should not be identified as normal
breathing.
Steps for Infant CPR for Support Staff2.2. Call for bystanders to get help and the defibrillator- do not
leave the patient*.*.
Note the time for recording on the code blue documentation form. ** If no one is present to activate the emergency response
team, do CPR for 2 minutes and then call for help.
In any of the Kaleida Hospitals, direct helpers to call 79117911 and inform the operator of your location and Code Blue.
The Code Cart with advanced equipment and defibrillator is essential.
Steps for Infant CPR for Support Staff33.Begin chest compressions to maintain forward blood flow.
Just below the nipple line. Push Hard & Fast! Push Hard enough - at least 1/3 the diameter of the chest or
about 1 ½ inches in an infant. At least a rate of 100 per minute Allow full re-expansion (or recoil) of chest wall between
compressions. Avoid the xiphoid process and ribs. Place bed board under patient to facilitate chest
compressions.
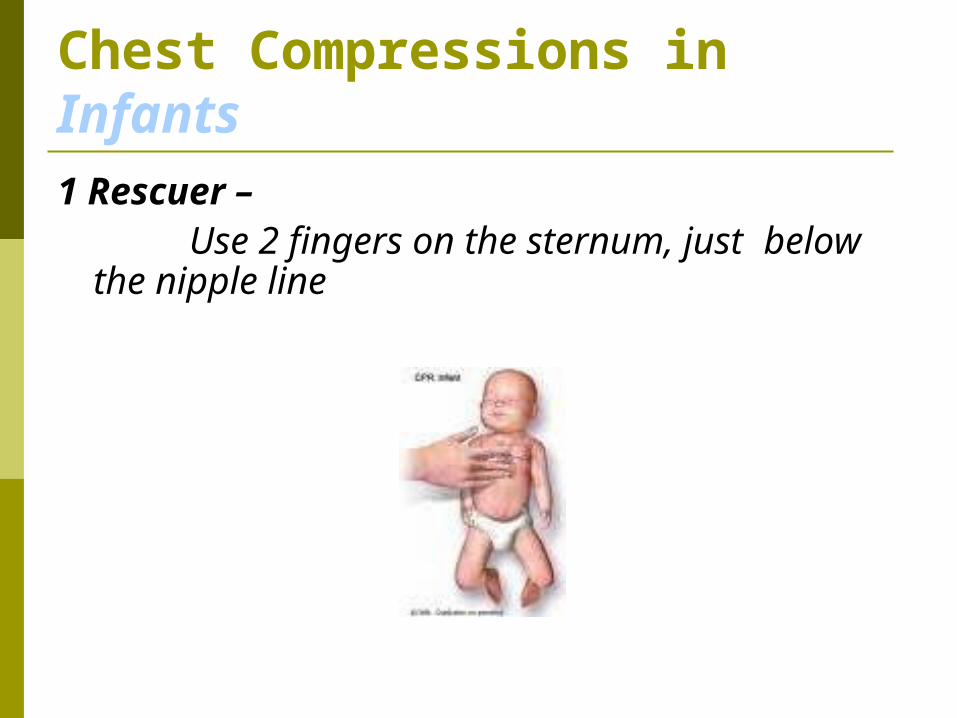
Chest Compressions in Infants1 Rescuer –
Use 2 fingers on the sternum, just below the nipple line
Steps for Infant CPR for Support Staff4.4. Following the first 30 chest compressions, deliver 2 breaths.
Use gentle head-tilt/chin-lift position to maintain open airway.
If the chest does not rise with ventilation attempt, reposition the head, make a better seal and try again.
Healthcare workers in employment situation should always have available and use a barrier device to deliver mouth to mouth ventilations.
Deliver only enough air to cause a visible chest rise – MORE IS NOT BETTER!
Deliver each breath over only 1 second.
Steps for Infant CPR for Support Staff Continue CPR in cycles of 30 compressions
to 2 ventilations.
Pause no more often than every 5 cycles or 2 minutes for a 5 second pulse check.
If an infant is not breathing but has a pulse above 60, give rescue breaths – one breath every 3 – 5 seconds or 12 – 20 breaths/minute.
Steps for Newborn CPR for Support Staff For the purposes of CPR resuscitation - the
guidelines identify a newborn as: Any Any newbornnewborn from birth until discharge from birth until discharge
from the hospital.from the hospital.
Important Considerations in Newborn CPR Make every effort to keep the newborn warm.
Too much oror too little oxygen can be harmful to the newborn.
Assisted Ventilation in the Newborn Breathing is the most effective action in
newborn resuscitation!
Breaths should be given at a rate of 40-60 breaths per minute.
Steps for Newborn CPR for Support Staff Assess unresponsiveness and for absence of normal breathing.
Call for help and a code cart/defibrillator.
Open the airway and deliver 2 breaths.
Begin cycles of CPR compressions and ventilations.
As soon as a defibrillator is available, assess for need to defibrillate.
Newborns still follow the A-B-C method:
A – Airway
B – Breathing
C – Circulation (compressions)
Steps for Newborn CPR for Support Staff Begin chest compressions:
Lower third of sternum.
Push Hard and Fast.
Push hard enough - at 1/3 the dimension of the chest.
Allow full re-expansion (or recoil) of chest wall between compressions.
Do not compress the xiphoid process or ribs.
Use 2 fingers on the sternum, just below the nipple line as in Infant CPR.
Coordinating Chest Compressions and Ventilation in a Newborn Ratio=3 compressions to 1 ventilation Rate=120 events per minute (90
compressions and 30 breaths) Each compression or breath takes only 1/2
second Compressions and ventilations CANNOT be
delivered simultaneously
Foreign Body Airway Obstruction (FBAO) Infants/Newborn
Management of choking is different for infants/newborns than adults and older children!
Definition=sudden onset of respiratory distress with coughing, gagging, stridor and or wheezing.
Mild=can cough forcefully or make some sounds-let the baby cough on her own.
Severe=victim unable to make sounds-use the steps outlined on the next slide.
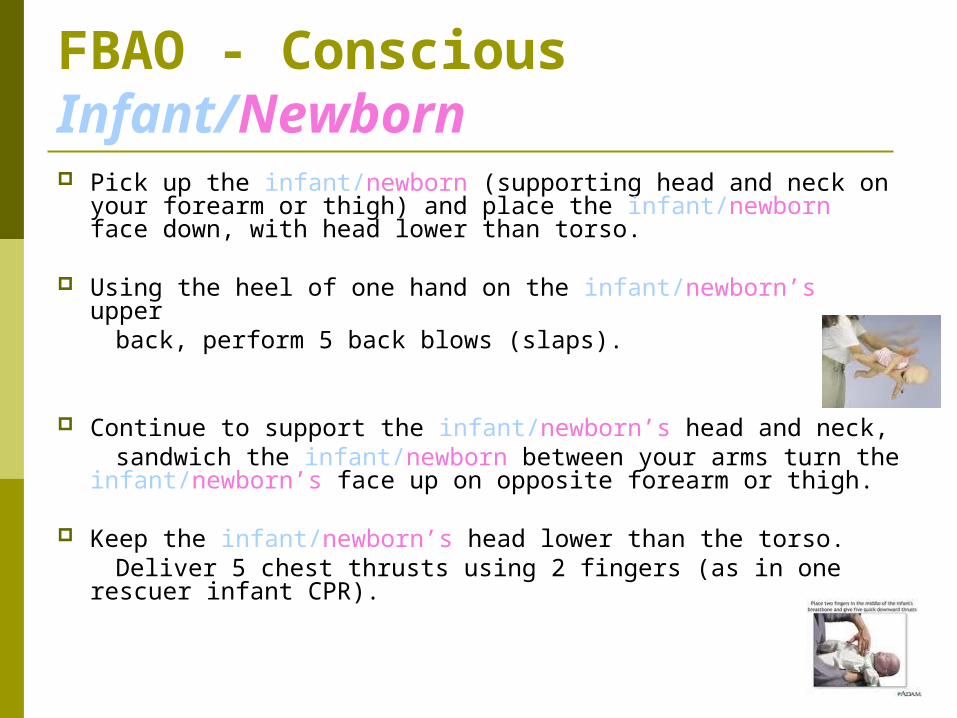
FBAO - Conscious Infant/Newborn Pick up the infant/newborn (supporting head and neck on
your forearm or thigh) and place the infant/newborn face down, with head lower than torso.
Using the heel of one hand on the infant/newborn’s upper back, perform 5 back blows (slaps).
Continue to support the infant/newborn’s head and neck, sandwich the infant/newborn between your arms turn the
infant/newborn’s face up on opposite forearm or thigh.
Keep the infant/newborn’s head lower than the torso. Deliver 5 chest thrusts using 2 fingers (as in one rescuer
infant CPR).
FBAO- Unconscious Infant/NewbornFor a choking baby who becomes unresponsive
Ask bystanders to call for help (if not done already).
1. Start CPR chest compressions.2. After 30 compressions, open the airway
and look for a foreign object. If a foreign object is seen - remove it. NO blind finger sweeps!
3. Attempt 2 breaths. 4. Continue with cycles of compressions and
breaths.