wear of enamel antagonist against ceramic restorative ... · pdf filewear of enamel antagonist...
TRANSCRIPT

i
WEAR OF ENAMEL ANTAGONIST AGAINST CERAMIC RESTORATIVE
MATERIALS
by
TANEET GHUMAN
JOHN O. BURGESS, COMMITTEE CHAIR
DANIEL A. GIVAN
MARK. S. LITAKER
AMJAD JAVED
A THESIS
Submitted to the graduate faculty of The University of Alabama at Birmingham,
in partial fulfillment of the requirements for the degree of
Master of Science
BIRMINGHAM, ALABAMA
2010

ii
Copyright by
Taneet Ghuman
2010
iii
WEAR OF ENAMEL ANTAGONIST AGAINST CERAMIC RESTORATIVE
MATERIALS
Taneet Ghuman
MASTER OF SCIENCE IN CLINICAL DENTISTRY
ABSTRACT
Tooth wear is an ever-increasing problem, and is likely to continue as patients' de-
mands and expectations rise and as more natural teeth are retained into old age. Demands
for esthetic alternatives have led to increased development of new generations of ceramic
materials. Dental ceramics are known for their excellent chemical and optical properties.
The wear of human enamel and the restorative material are often a functional and estheti-
cal concern when selecting a restorative material for clinical restorative treatment. Ce-
ramic restorations have been known to cause wear of opposing enamel. Some restorative
materials wear the opposing tooth while some have significant wear. Wear of restorative
materials and enamel is often determined by wear simulators. These machines have limi-
tations and most have not been calibrated to in vivo wear. Additional controversy centers
around the force exerted by these simulators on the esthetic restorative material. General-
ly the load used is similar to the forces generated during mastication. Validation of the
wear machines should be done by comparing their results with published in vivo studies.
The objectives of this study were (1) to evaluate volumetric wear and depth loss of
the antagonist surface (1) to evaluate the volumetric wear and depth loss of occlusal ena-
iv
mel investigated at baseline and 200,000 cycles.
Impressions, employing a polyvinyl siloxane, were made of the shaped enamel styli and
poured with improved dental stone and separated. Both the enamel styli casts and the ce-
ramic restorative materials were scanned with a non-contact Profilometer for before and
after 200,000 cycles in the wear simulator to determine loss of volume and depth of the
restorative material.
Superimposition of imaged casts was done to evaluate wear volume loss. The data was
statistically analyzed for volume loss of the 3 ceramic restorative materials compared to
enamel styli by ANOVA and Tukey-Kramer post hoc test. Lava Core showed higher in
vitro volumetric wear loss than all other groups (p<0.0001). There was no in vitro volu-
metric wear or depth loss for antagonist surfaces in any of the groups (p>0. 6209). There
were no differences for enamel wear depth for any of the groups (p>0.2757).
Keywords: Wear, enamel, ceramic restorative materials, wear volume loss, depth
loss, 3-D Non-contact Profilometer.

v
ACKNOWLEDGEMENTS
I am grateful to the many individuals who contributed to my education, culminat-
ing in achieving this Master‘s degree.
First, I wish to recognize Dr. John O.Burgess, Chair of my graduate committee.
Without his vision and guidance, this work could not have been completed. I convey my
earnest appreciation and gratitude for his invariable support, patience and motivation. I
am highly honored to have worked under his guidance and would love to work with him
in the future.
I would like to express my sincere thankfulness to my committee members, Dr.
Daniel A. Givan, Dr. Mark S. Litaker, Dr. Amjad Javed, for their invaluable advice over
the period of my research project. They were very tolerant and determined to see me
through. They all provided helpful assistance and advice for this work
I wish to extend my utmost gratitude to Mr. Preston Beck, without whose exper-
tise, I would not have been able to finish this study in time. I cannot thank him enough
for all that he has done for me.
I also wish to thank Dr. Deniz Cakir whose thoughtful & meticulous organization
of my research project allowed me to be consistent.
Many others have provided support and encouragement, especially Dr.Pranita Kadam,
Dr. Arjun Sarof, Dr. Ramtin Sadid Zadeh and Dr. Prabhavati Jampani my friend‘s from
the Master‘s program.
Finally, I thank all my friends and the biomaterials residents, without the moral
support of whom I would not have been able to achieve this.

vi
I am grateful to all these individuals and countless others with whom I have had
the privilege of interacting during the past years, and this dissertation is dedicated in part
to them.
Ivoclar Vivadent and 3M ESPE generously donated the materials for the study.
vii
DEDICATION
I dedicate my thesis to parents,
Mrs. Simran and Mr. Gurvinder Ghuman.
Thank you for your unconditional love and devotion with which you have raised me into
this world. Thank you for giving me a chance to prove and improve myself through all
walks of life. I am honored to have you as my parents.
I dedicate my thesis to my grandparents, sister and brother,
Ameet and Jaikaran Ghuman.
Thank you for believing in me; for allowing me to further my studies. I would not have
been at this stage without your unvarying encouragement and support.

viii
TABLE OF CONTENTS
Page
ABSTRACT...................................................................................................................... iii
ACKNOWLEDGMENTS.................................................................................................. v
DEDICATION...................................................................................................................vii
LIST OF TABLES............................................................................................................. x
LIST OF FIGURES............................................................................................................xi
INTRODUCTION...............................................................................................................1
Ceramics Background......................................................................................................... 1
Dental Ceramics.................................................................................................................. 2
Wear Background............................................................................................................. 11
Clinical Significance of wear............................................................................................ 13
Mechanism of Wear...........................................................................................................15
Wear Simulating Devices................................................................................................. 18
ACTA wear machine........................................................................................................ 20
Oregon Health Sciences University Oral Wear Simulator............................................... 21
University of Alabama Dental Wear Simulator................................................................ 21
Zurich computer-controlled masticator............................................................................. 22
BIOMAT wear Simulator................................................................................................ 23
Minnesota wear Simulator............................................................................................... 23
Willytec Wear Simulator................................................................................................. 25
Contributing factors for in-vitro wear simulation............................................................. 27
Alabama Chewing Simulators......................................................................................... 31
OBJECTIVES AND HYPOTHESES.............................................................................. 33
MATERIALS and METHODS........................................................................................ 35
Specimen preparation........................................................................................................ 36
Determination of Wear..................................................................................................... 39
Impression protocol.......................................................................................................... 40
Casts.................................................................................................................................. 41

ix
TABLE OF CONTENTS
Page
Determination of volumetric wear & depth loss............................................................... 43
RESULTS ........................................................................................................................ 47
DISCUSSION................................................................................................................... 50
CONCLUSIONS ............................................................................................................. 58
SUGGESTIONS FOR FUTURE RESEARCH................................................................ 59
REFERENCES................................................................................................................. 60
APPENDIX
A IRB APPROVAL FORM ........................................................................................... 67
B Tables -Repeated measure ANOVA & Tukey-Kramer test.......................................... 69
C In vitro enamel styli scan at baseline & 200,000 cycles.............................................. 76
D In vitro scan of Ceramic surfaces…………..………………………………………… 80
E Superimposed Images of Enamel Styli at Baseline & 200,000 cycles……………...... 84
F Superimposed Images of Ceramic surfaces at Baseline & 200,000 cycles…..………. 88
x
LIST OF TABLES
Page
1. Commonly used Dental Ceramics.................................................................................. 3
2. Materials used............................................................................................................... 36
3. Wear on Antagonist Ceramic Surfaces......................................................................... 47
4. Wear on Enamel Styli................................................................................................... 47
xi
LIST OF FIGURES
Figure Page
1 IPS e.max crystals ............................................................................................................5
2 Two-Body Wear..............................................................................................................16
3 Three-Body Wear............................................................................................................17
4 Fatigue Wear...................................................................................................................18
5 ACTA Wear machine.................................................................................................... 20
6 Oregon Oral Wear Simulator......................................................................................... 21
7 University of Alabama Dental Wear Simulator............................................................. 22
8 BIOMAT wear simulator............................................................................................... 23
9 Minnesota wear simulator.............................................................................................. 24
10 Willytec Wear Simulator............................................................................................ 25
11 Study Design............................................................................................................... 35
12 Stainless Steel Holders................................................................................................ 36
13 Carbide Burs................................................................................................................ 37
14 Mounted Maxillary Premolar....................................................................................... 37
15 Ceramic Blocks............................................................................................................ 38
16 Mounted ceramic specimen......................................................................................... 39
17 Modified UAB Chewing Simulator............................................................................ 40
18 PVS Impressions.......................................................................................................... 41

xii
LIST OF FIGURES
Figure Page
19 Stone replicas of styli removed from PVS Impressions.............................................. 42
20 Proscan 2000............................................................................................................... 44
21 Scanned specimens using Proscan................................................................................45
22 Superimposition of Images ..........................................................................................46
23 Original Alabama wear machine................................................................................ 54
24 Modified Alabama Wear Machine............................................................................. 55
1
INTRODUCTION
Ceramics Background
Land introduced the first feldspathic porcelain crown in 1886 (1). Since then, ce-
ramic crowns have been a focus of interest in patients and clinicians because of their nat-
ural appearance. Several types of ceramics have been introduced for producing all-
ceramic reconstruction. The first attempt was not until 1965; when McLaren and Hughes
introduced a technique strengthen conventional feldspathic porcelain with aluminous
porcelain, that a more common use of ceramic restorations was seen (2). However, ce-
ramic crowns were mostly used to restore anterior teeth because of their brittleness and
low tensile strength. In order to combine good optical results with enhanced stability,
glass-infiltered alumina (Inceram alumina) was developed. By adding glass the optical
quality was improved, however the high crystals content led to high opacity. Therefore,
alumina was adopted as a core material. Despite its enhanced mechanical stability, high
failure rates were reported with glass-infiltered alumina in posterior regions.
More recently, densely sintered high strength ceramics with mechanical
properties superior to conventional ceramics have been developed for restorative denti-
stry. Zirconia, the most stable of these high strength ceramics has flexural strength and
fracture toughness values of 900-100 MPa and 9 MPa/m1/2
. These values are twice as
high as glass-ceramics and glass-infiltered alumina. Using cores with alumina or zirconia
2
veneered with feldspathic porcelain, it is now possible to make a ceramic crown with im-
proved mechanical properties (3).
Increased patient demand for esthetic dentistry has encouraged interest in all-
ceramic dental restorations. Improved materials and innovative techniques have led many
dentists to use all-ceramic crowns and inlays for the restoration of posterior occlusal sur-
faces (4).
Introduction of alumina and zirconia as high strength core materials for all ce-
ramics crowns has significantly increase their use. Ceramic crowns can now be used in
posterior teeth successfully. When selecting a restorative material for dental practice, a
major consideration is its mechanical properties. Since restorative materials are used to
replace missing tooth structure, it must have adequate strength to withstand the forces
generated during mastication.
Dental Ceramics
Ceramics are probably the best materials available for matching the esthetics of a
complex human tooth. Dental ceramics are basically oxide based glass-ceramic systems.
Sintered ceramics and glass-ceramics are widely used as biomaterials for dental restora-
tion, especially as dental inlays, onlays, veneers, crowns or bridges. Ceramic materials
have been extensively employed in the clinical practice of dentistry mostly as an esthetic
restorative material. Different types of glass-ceramics and ceramics are available and ne-
cessary today to fulfill customers' needs (patients, dentists and dental technicians) regard-
ing the properties of the biomaterials and the processing of the products.

3
Glass-ceramics are particularly suitable for fabricating inlays, crowns and small
bridges, as these materials achieve very strong, esthetic results. High-strength ceramics
are preferred in situations where the material is exposed to high masticatory forces. A
well designed and fabricated ceramic crown is often indistinguishable from the adjacent
nature tooth. Although commonly used to replace decayed tooth structure, the esthetic
ceramic material is also used to cover pathological conditions of the enamel and dentin
such as unsightly stains, malformations of the teeth, or improper calcification. They are
used to close spaces (diastemae) existing between teeth and as enamel/dentin bonded par-
tial or total coverage without macro-retention.
Table 1: Commonly used Dental Ceramics
FLEXURAL
STRENGTH (MPa)
FRACTURE
TOUGHNESS (Mpa-m1 / 2
)
Feldspathic Porcelain
80
1.1
IPS Empress 120 1.2
IPS Empress 2 350 2.5
IPS e.max 350-400 2.5
In Ceram Alumina 400 4.5
In Ceram Zirconia 550 5.5
Procera (Alumina) 600 6.0
Zirconia (CERCON, LAVA) 900-1100 7-11
Tooth: Enamel
65-75 1
Tooth: Dentin
16-20 2.5
4
Conventional prosthetic treatment options such as porcelain-fused-to-metal
(PFM) are increasingly being replaced by all-ceramic restorative systems. Long-term
clinical studies have shown that the survival rates of Porcelain fused to Metal (PFM) sin-
gle crowns are 59% to 84% after an observation period of 15 years (5). In 2000, Ker-
schbaum reported a survival rate of 29% for cast metal crowns after an observation pe-
riod of more than 25 years (6). Scurria et al and Creugers et al reported a survival rate of
conventional fixed partial dentures (FPD) ranging from 69% to 74% after 15 years of ob-
servation period (7, 8). All- ceramic materials exhibit high level of translucency and lu-
minousness resembling those of natural teeth (9).
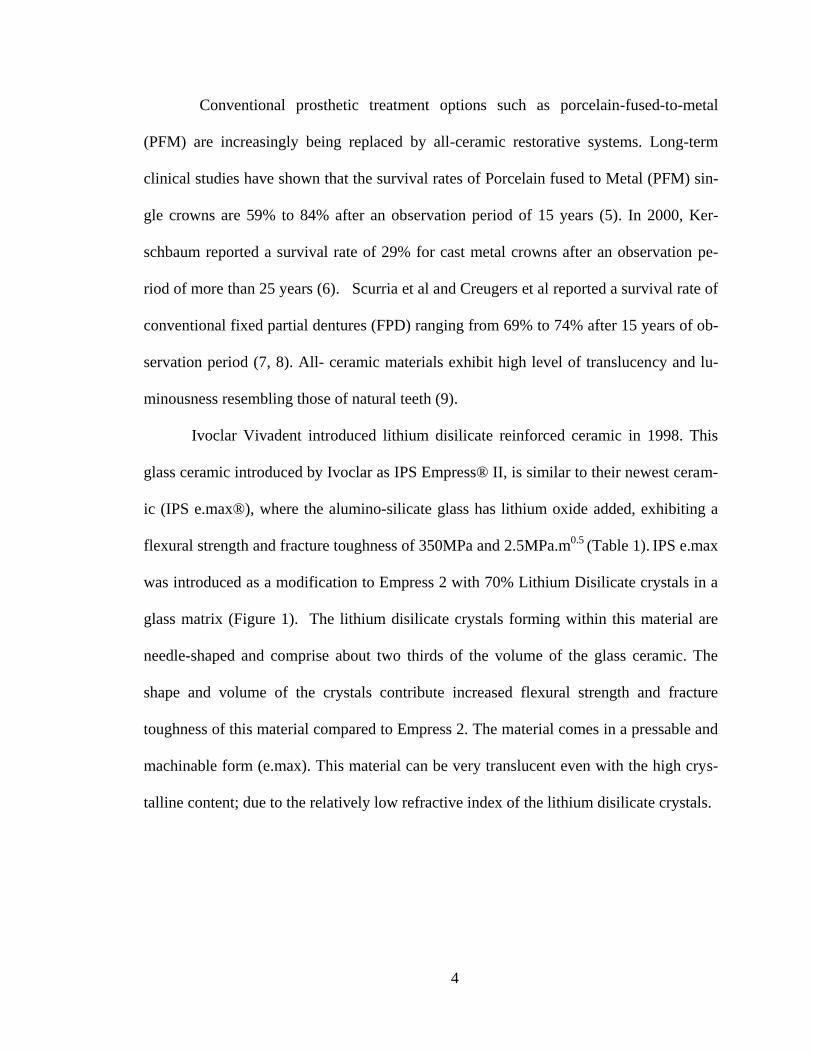
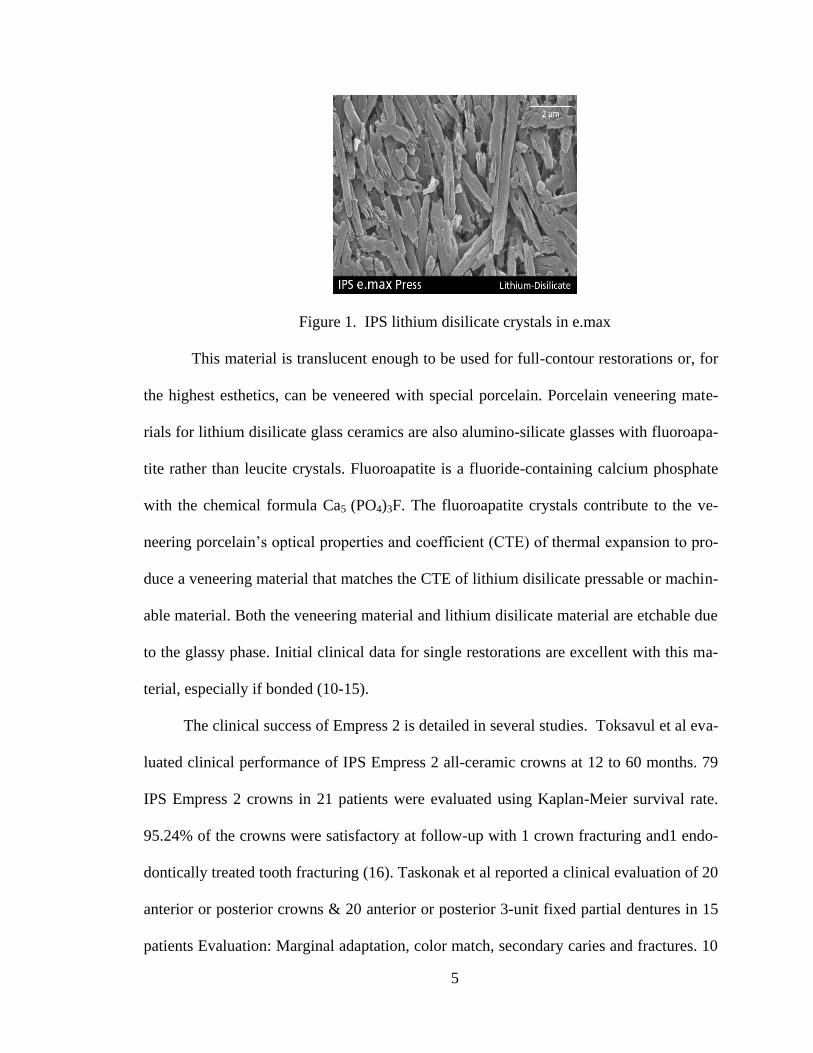
Ivoclar Vivadent introduced lithium disilicate reinforced ceramic in 1998. This
glass ceramic introduced by Ivoclar as IPS Empress® II, is similar to their newest ceram-
ic (IPS e.max®), where the alumino-silicate glass has lithium oxide added, exhibiting a
flexural strength and fracture toughness of 350MPa and 2.5MPa.m0.5
(Table 1). IPS e.max
was introduced as a modification to Empress 2 with 70% Lithium Disilicate crystals in a
glass matrix (Figure 1). The lithium disilicate crystals forming within this material are
needle-shaped and comprise about two thirds of the volume of the glass ceramic. The
shape and volume of the crystals contribute increased flexural strength and fracture
toughness of this material compared to Empress 2. The material comes in a pressable and
machinable form (e.max). This material can be very translucent even with the high crys-
talline content; due to the relatively low refractive index of the lithium disilicate crystals.
5
Figure 1. IPS lithium disilicate crystals in e.max
This material is translucent enough to be used for full-contour restorations or, for
the highest esthetics, can be veneered with special porcelain. Porcelain veneering mate-
rials for lithium disilicate glass ceramics are also alumino-silicate glasses with fluoroapa-
tite rather than leucite crystals. Fluoroapatite is a fluoride-containing calcium phosphate
with the chemical formula Ca5 (PO4)3F. The fluoroapatite crystals contribute to the ve-
neering porcelain‘s optical properties and coefficient (CTE) of thermal expansion to pro-
duce a veneering material that matches the CTE of lithium disilicate pressable or machin-
able material. Both the veneering material and lithium disilicate material are etchable due
to the glassy phase. Initial clinical data for single restorations are excellent with this ma-
terial, especially if bonded (10-15).
The clinical success of Empress 2 is detailed in several studies. Toksavul et al eva-
luated clinical performance of IPS Empress 2 all-ceramic crowns at 12 to 60 months. 79
IPS Empress 2 crowns in 21 patients were evaluated using Kaplan-Meier survival rate.
95.24% of the crowns were satisfactory at follow-up with 1 crown fracturing and1 endo-
dontically treated tooth fracturing (16). Taskonak et al reported a clinical evaluation of 20
anterior or posterior crowns & 20 anterior or posterior 3-unit fixed partial dentures in 15
patients Evaluation: Marginal adaptation, color match, secondary caries and fractures. 10

6
(50%) catastrophic failures of fixed partial dentures were reported, with 5 (25%) failures
within 1-year and (25%) by 2 years (17). Fasbinder et al reported a clinical evaluation of
IPS e.max crowns 2 yrs 62 IPS e.max crowns were cemented with 2 types of adhesive
resin cements, Multilink sprint & experimental self-adhesive cement by Ivoclar Vivadent
evaluated at baseline, 6 months, 1year and 2 yrs. No clinically identified cases of crown
fracture or surface chipping. No reported sensitivity at 1 or 2 years with either cement
with an Alfa score: 86.9 percent for crowns cemented with Multilink sprint & experimen-
tal self-adhesive cements (18). Early results indicate that IPS e.max crowns may be an
effective option for all-ceramic crowns (18). In a three year clinical study, Etman et al
cemented 90 posterior teeth crowns in 48 patients randomized into 3 groups. IPS e.max,
Procera AllCeram & Metal ceramic veneered with IPS Classic Porcelain. Data was ana-
lyzed using the modified USPHS criteria. Crowns that developed visible cracks were sec-
tioned and removed, and the surfaces were analyzed using a scanning electron micro-
scope (SEM). The data were analyzed using the Kruskal-Wallis nonparametric statistical
test, followed by the Mann-Whitney test with Bonferroni correction (α=.05). IPS e.max
& metal ceramic crowns showed fewer clinical changes than Procera All Ceram. Visible
roughness, wear & deformity noticed in occlusal contact areas of Procera AllCeram
crowns. SEM images showed well defined wear facets in both ceramic crown systems.
IPS e.max's clinical behavior was comparable to Procera AllCeram & metal ceramic
crowns but wear resistance superior to the Procera AllCeram crowns (19).
While early ceramics had a failure mechanism of bulk fracture however newer ce-
ramic materials using aluminum oxide and zirconia-based frameworks exhibit very good
clinical data and superior esthetics.

7
Zirconia holds a unique place amongst oxide ceramics due to its excellent me-
chanical properties the most recognizable names is Lava, Vita YZ, and Cercon®. These
materials were designed as a PFM alternative for single crowns and three-unit bridges
anywhere in the mouth. Larger bridges have been discussed but no large sample clinical
documentation exists for this application. Solid-sintered, monophase ceramics are mate-
rials that are formed by directly sintering crystals together without any intervening matrix
to from a dense, glass-free, polycrystalline structure.
Solid-sintered ceramics (polycrystalline glass-free) have the highest potential for
strength and toughness, but because of high firing temperatures and sintering, shrinkage
techniques were not available until only recently to use as high-strength frameworks for
crowns and fixed partial dentures. Zirconia has unique mechanical properties that provide
flexural strength for this ceramic range from over 900 MPa to 1,100 MPa (Table 1) (20).
It is important to note there is no direct correlation between flexural strength (modulus of
rupture) and clinical performance. With all things being equal, it is better to have an inhe-
rently stronger material than a weaker one. A more important physical property is frac-
ture toughness, a measure of a material‘s ability to resist crack growth ranges from 8 MPa
and 10 MPa for zirconia (21). This is significantly higher than any previously reported
ceramic ranging from 1-3 MPa, and roughly twice the amount reported for the alumina
materials (4-6 MPa). Zirconia has the apparent physical properties to be used for post-
erior three-unit fixed partial dentures (Table -1). Clinical studies for zirconia fixed partial
dentures have not demonstrated a problem with the zirconia framework (22-24). Unfortu-
nately, veneered zirconia had some problems associated with chipping and cracking of
porcelain. McLaren et al and his team did a pilot study testing the cracking resistance of
8
porcelain fired to zirconia. Using a slow-cooling protocol at the glaze bake to equalize
the heat dissipation from the zirconia and porcelain increased the fracture resistance of
the porcelain by 20% (25).
More than 1,200 Lava or Vita YZ restorations have been placed at the UCLA Cen-
ter for Esthetic Dentistry over the last 5 years, with less than < 1% per year failure rate
for core fracture. Chipping of the porcelain was noted in > 6% of the restorations that
could be recalled that required replacement, with many more showing chipping not re-
quiring replacement. The slow-cooling firing treatment on the glaze bake has minimized
or almost eliminated this problem. McLaren et al concluded from his clinical data that if
the proper porcelain firing protocol is used, single restorations anywhere in the mouth
and three-unit bridges (specifically Lava and Vita YZ) have performed well as a PFM
substitute (25). Inherent brittleness, low flexural strength & fracture toughness of con-
ventional glass and alumina ceramics have been the main obstacles for its use. While still
in its infancy, zirconia technology advances the fabrication of new biocompatible all-
ceramic restorations with improved physical properties for a wide range of promising
clinical applications. In clinical studies, zirconia core showed an overall success rate of
about 90-100% where as Zirconia Veneer material has problems with the veneer chipping
or cracking with minor loss of material after only 1–2 years. Schmitt et al conducted a 3
year clinical evaluation of 3 or 4 unit Lava fixed partial dentures for 30 patients and re-
ported veneering fractures of 4% and no framework fracture (26). Raigrodski et al re-
ported veneer fracture of 25% at 3 years, and Sailer et al reported 13% veneer chipping at
3 years & 15.2% at 5 years (24, 27, 28).
9
In the search for alternative and esthetic restorative materials, many all-ceramic
systems have been introduced for the general practitioner. However, dentists have re-
mained suspicious of the structural longevity, potential abrasivity, and fit of ceramic res-
torations, although facture and wear are the main concerns and reasons for failure of all-
ceramic crowns and fixed partial dentures (29). Newer reinforced ceramics showed better
durability then the earlier fired ceramic materials. Ceramics are more enamel abrasive
than other restorative materials such as gold, composites or amalgam.
Full contour zirconia crowns have been marketed which reduce the occlusal re-
duction of the tooth from 2-2.5mm to one mm a significant clinical advantage. However,
there has been considerable concern as to how these materials, formulated for improved
strength, wear the opposing dentition compared to other materials. An esthetic restoration
should not wear an opposing enamel surface. In a survey of members of the American
Academy of Esthetic Dentistry, in 1986 Christensen found "less wear on opposing teeth"
to be the single most desirable need for change in posterior tooth-colored crowns (30). In
1971 Mahalick et al. reported in vitro enamel-porcelain wear to be 2.4 times greater than
enamel-acrylic resin wear and 17 times greater than enamel-gold (31). Monasky and Tay-
lor tested a variety of surface finishes of porcelain against tooth substance and concluded
that the rate of enamel wear was a function of porcelain roughness (32). Ekfeldt and 0ilo
et al, using a bruxing subject, studied occlusal wear of porcelain, gold, and resin in vivo
(33). They also verified that enamel surfaces exhibited the greatest loss when opposed by
feldspathic porcelain. These and other studies have led some clinicians to caution against
the use of porcelain occlusal surfaces where rapid enamel attrition might be predicted,

10
such as for a bruxer or complete-denture wearer having porcelain opposed by natural
teeth.
A ceramic restorative material that combines good strength without the disadvan-
tage of increased enamel wear would be a significant addition to clinical dental practice.
Lambrechts et al. using clinical measurements reported that enamel vertical wear was be-
tween 20 m to 40 m per year when opposing enamel in the premolar and molar re-
gions, respectively (34). Dental wear, at first considered a pathological condition, is now
regarded as a physiological mechanism of teeth adaptation to continuous masticatory
stresses. (35). Enamel is the main tissue subjected to wear; however, advanced enamel
wear exposes increasingly large areas of dentin. Enamel hardness and anisotropy are the
major factors contrasting wear and micro fractures. Anisotropy is mainly related to the
different orientation of prism bundles and of hydroxyapatite crystals. Enamel wear devel-
opment is also related to differences in microhardness, density, mineral composition and
protein distribution. Masticatory loads distributed along the enamel-dentin junction un-
iformly disperse in the underlying dentin (35). As with enamel or dentin, restorative ma-
terials wear, and the wear mode depends on the type of restorative material. The various
dental materials may be grouped in four different categories: metal alloys, ceramics,
composites and unfilled polymers. Clinical studies have shown that metal alloys and ce-
ramic materials are generally very wear-resistant, whereas composites and unfilled poly-
mers have lower wear resistance (36, 37).
Ceramic materials may damage the opposing enamel. In vivo studies have shown
that the enamel wear depends on the ceramic material used (38, 39) internal porosities
and surface defects (40). Staining ceramic materials on the occlusal surface can influence

11
the wear of a ceramic material, as metal oxides used in the ceramic stains are abrasive to
enamel (40). Furthermore, patient-related factors such as dietary habits, dysfunctional
occlusion, biting force and bruxism contribute to accelerated enamel antagonist loss. Ce-
ramic wear testing remains difficult to assess in both in vitro and in vivo. Ceramic inves-
tigations are often studied using flat ceramic specimens opposing either human cusps in
their natural anatomic state or flattened (ground) enamel. It has been noted that the sum
of the vertical loss of enamel and of the restorative material can be a key to evaluating
wear characteristics relative to clinical performance. Evaluating the wear of restorative
materials requires that both the material of interest and the opposing material be consi-
dered. Clinically, it is the combined wear that is important; especially if the opposing ma-
terial is enamel. For example, in an in vitro study done using the University of Minnesota
artificial oral environment, significant differences were found in the ranking of material
wear depending on whether the material alone or the combined wear of the material and
enamel were considered. Enamel wear was measured when it opposed enamel, amalgam,
and porcelain. If only the material was considered, then enamel wore more than porce-
lain, which wore more than amalgam. Combining material wear with the opposing ena-
mel wear found that the enamel–porcelain combination wore more than the enamel–
enamel combination and that both wore significantly more than the enamel–amalgam
combination (29).
Wear Background
Mastication is defined as the act of chewing foods. Muscles of mastication pro-
duce active forces that are perpendicular and tangential to the occlusal surfaces of teeth
12
by guiding the movement of the mandible in relation to the functional movements with
the upper jaw. These forces are responsible, in part, for the wear of restorative materials
in the mouth. The ratio of the force of friction between the two surfaces and the force
pressing them together is the coefficient of friction (41). The coefficient of friction
changes with materials, and during mastication, the coefficient can be lower due to lubri-
cation from foods, drinks, and saliva (42). Wearing of tooth surfaces has significant clini-
cal consequences both esthetically and functionally. Increasing levels of tooth wear are
significantly associated with age. The predicted percentage of adults presenting with se-
vere tooth wear increased from 3% at 20 years to 17% in patients 70 years old and older
(43). The teeth most severely affected by wear are mandibular molars, but the most
commonly affected teeth are anteriors (43).
Several facts about biting forces are important while restoring the chewing capa-
bilities of patients. While evaluating the effect of tooth contacts on structures of mastica-
tory system, two factors must be considered: magnitude and duration of contacts. Both
chewing and swallowing activities must be evaluated. Estimates indicate that during
chewing, an average of 58.7lb of force is applied to teeth in 115ms. This yields
6.75lb/sec/chew. People swallow approximately 146 times a day while eating. An esti-
mated 66.5lb of force is applied during each swallow; this comes to 5068 lb/sec/day. The
total force activity for chewing and swallowing is about 17,200 lb/sec/day (42). Chewing
speed ranges about 49 to 120 cycles/minute. The usual chewing rate is 70 to 80 chews per
minute. It is important to consider that while the average chewing forces are about 22 Kg,
some individuals have biting forces as high as 360 Kg (42).
13
Materials wear is a complex and unpredictable phenomenon. The experiences
from the past decade prove that tooth wear occurs in an increasing number of cases in
dental practice. Tooth surface losses or ‗tooth wear‘ refers to the pathological loss of
tooth tissue by a disease process other than dental caries. The different wear mechanisms
are involved with the biomechanical factors of mastication. An ideal wear simulation
would incorporate both abrasion and attrition since mastication involves both processes.
Abrasion occurs in the presence of food as the jaw closes. It begins when both mandibu-
lar and maxillary teeth contact the food bolus and ends when the two teeth contact each
other. Because the teeth do not come in direct contact during abrasion, this stage is
termed the contact free area (CFA) region of wear. This stage of wear involves abrasive,
adhesive and corrosive wear (39). Attrition begins when the mandibular and maxillary
teeth directly contact and ends when they separate. This is termed the occlusal contact
area (OCA) region of wear (44). This stage of mastication involves abrasive; adhesive
and fatigue wear (44). The primary variables affecting the mechanism of wear include
the properties of the two contacting materials and the surrounding and interfacial media.
The rehabilitation of the lost tooth material is often very difficult, irrespectively of
whether it is needed because of functional or esthetic causes.
Clinical Significance of wear
Clinical wear bears a multifactorial etiology, understanding the mechanism of ac-
tion is an important step in an appropriate restoration material selection. Each material
selected should meet the individual wear behavior and needs. Individual factors may en-
hance the wear rates: aggressive tooth brushing, parafunctions, diet, acidic/aqueous envi-
14
ronment, surface geometry, and diminished tooth support. Failure of ceramic restoration
due to creation of micro cracks/flaws, poor masticatory function (29), impaired aesthetic
appearance (45), sensitivity, secondary caries and systemic effects through ingested wear
products (44). Teeth wear has significant clinical consequences both esthetically and
functionally. As teeth wear, they continue to erupt, which led to the concept of ―wearing
into occlusion‖. Physiological wear is surface degradation that results in progressive, but
very slow loss of convexity of the cusps, which manifests as a flattening of cusp tips on
the posterior teeth and incisal edges of mammelons on the anterior teeth. Excessive wear
results in unacceptable damage to the occluding surfaces and alteration of the functional
path of masticatory movement (40). It may also destroy anterior tooth structure that is
essential to acceptable anterior guidance function or esthetics, resulting in increased hori-
zontal stresses on the masticatory system and associated temporomandibular joint re-
modeling. If wear continues unabated, the enamel will eventually be breached. Once
breached, both the enamel and exposed dentin wear at accelerated rates. Excessive wear
on multiple teeth can have disastrous consequences. Biological consequences are related
to pain of the temporomandibular joint (TMJ), elongation of antagonists, loss of peri-
odontal ligament and tilting and movement of adjacent teeth. In spite of it being frequent-
ly mentioned as possible consequences, there is little evidence that occlusal wear as such
leads to the dysfunction of the TMJ, to muscle pain or periodontal disease (46-51). Sup-
portive treatment following restoration is important to monitor wear rates such as the res-
toration and nightguards.
A major concern in clinical practice is the wear resistance of resin materials used
in restorations especially involving posterior occlusion. Two types of wear have been de-
15
scribed by Leinfelder (52). One of these is wear initiated by generalized conditions (the
type of wear generated by a food bolus during mastication) and the other is wear generat-
ed under localized conditions (represented by direct tooth to materials contact). Some au-
thors have suggested that localized wear may be a more important contributor to the
breakdown of a material and contact wear may be more than two times as great as that in
non-contact areas. Clinical studies offer the most meaningful data on the performance of
a given material the time involved and costs associated with clinical studies have caused
manufacturers to have a strong interest in the use of wear simulator to test of prototype
materials during development and as a predictor of clinical performance. Leinfelder et al
developed a laboratory simulator capable of evaluating both generalized and localized
wear (52). This system transfers masticatory stresses to a composite specimen by means
of a flattened polyacetal stylus (generalized wear) or a stainless steel conical stylus (loca-
lized wear) in the presence of slurry of polymethylmethacrylate beads (PMMA). This de-
vice has facilitated the development of in vitro studies capable of predicting in vivo per-
formance. Previous work showed a correlation between in vitro wear and in vivo genera-
lized wear of dental restorative materials.
Mechanisms of Wear
Wear takes place at two surfaces: occlusal surface and proximal surface
Wear at contact-free occlusal area- CFOA
Wear at the occlusal contact area- OCA
While chewing, opposing dentition traps a layer of food and grinds it as the teeth
move past one another. The chewing forces produced during this phase are modeled
16
ranges between 10-20N (53, 54). At the end of chewing cycle, sliding motion stops as the
teeth reach centric occlusion. The chewing force ranges between 50-150N (55).
Wear is defined as a complex phenomenon and an ‗overall effect‘ of a number of
inter-related processes. It is further described these with five terms.
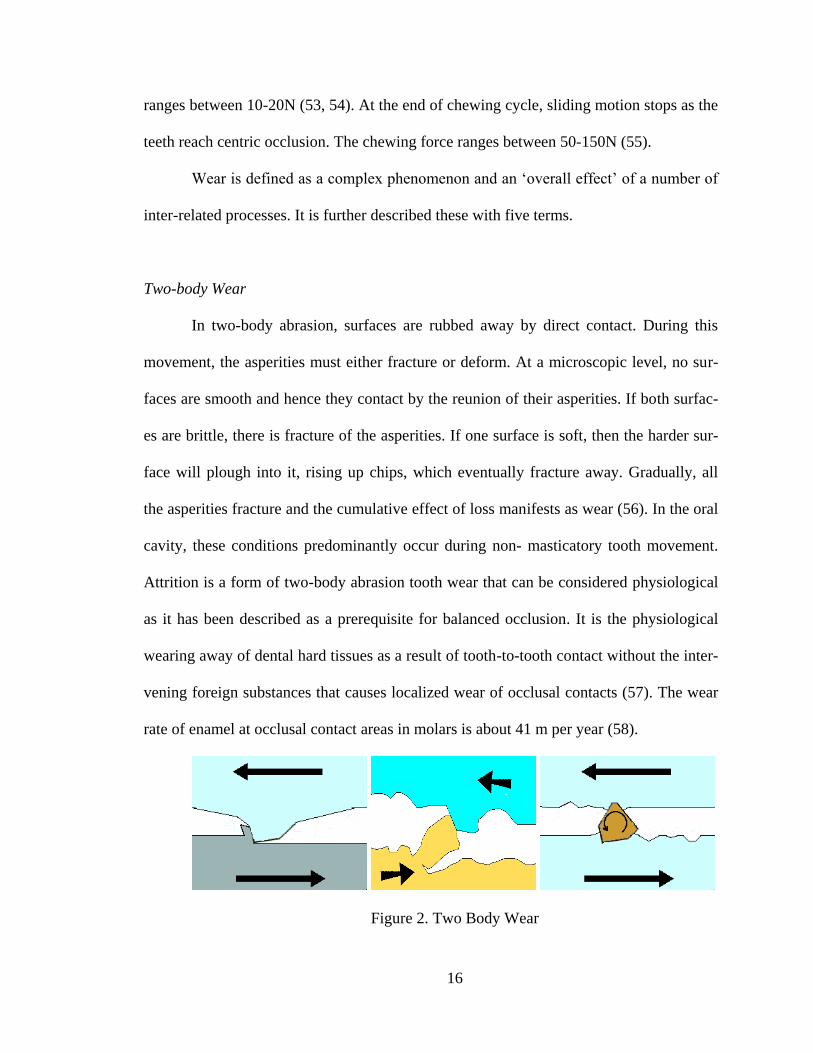
Two-body Wear
In two-body abrasion, surfaces are rubbed away by direct contact. During this
movement, the asperities must either fracture or deform. At a microscopic level, no sur-
faces are smooth and hence they contact by the reunion of their asperities. If both surfac-
es are brittle, there is fracture of the asperities. If one surface is soft, then the harder sur-
face will plough into it, rising up chips, which eventually fracture away. Gradually, all
the asperities fracture and the cumulative effect of loss manifests as wear (56). In the oral
cavity, these conditions predominantly occur during non- masticatory tooth movement.
Attrition is a form of two-body abrasion tooth wear that can be considered physiological
as it has been described as a prerequisite for balanced occlusion. It is the physiological
wearing away of dental hard tissues as a result of tooth-to-tooth contact without the inter-
vening foreign substances that causes localized wear of occlusal contacts (57). The wear
rate of enamel at occlusal contact areas in molars is about 41 m per year (58).
Figure 2. Two Body Wear

17
Three Body Wear
In three body wear surfaces are rubbed away by intervening slurry of abrasive
particles. The pressure between the surfaces is transferred to the particles, which then cut
away the asperities. In the oral cavity, this type of wear occurs during mastication and is
common in patients who eat an abrasive diet. During the early stage, when the occlusal
surfaces are separated by the food bolus, the abrasive particles act as a slurry and abrade
the whole surface as in generalized wear. They abrade the surface in the food shedding
pathways because of the shearing action of food on contact stress. This process is very
common in restorations with buccal or palatal extensions, as these absorb the main force
of the masticatory slurry in the escape root of the groove. This process tends to hollow
out the softer regions on a surface producing the chipping defects seen in occlusal molar
dentin (56). As the teeth begin to approximate during the later stages of mastication, the
remaining slurry particles get trapped between the asperities, in pits and in surface
grooves. If both surfaces have similar morphology then the abrasive particles may trans-
fer between scratches and cause more or less equal loss of both surfaces (56).
Figure 3. Three Body Wear
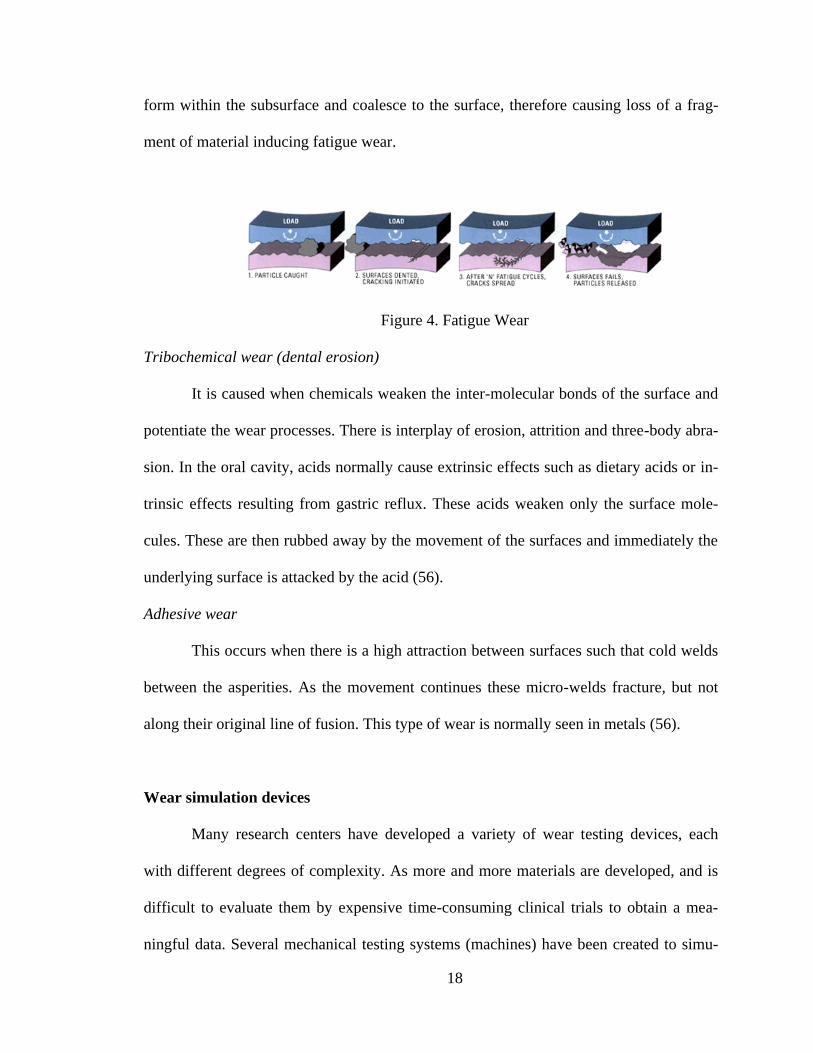
Fatigue wear
Some of the movement of the surface molecules is transferred to the subsurface
causing rupture of intermolecular bonds and a zone of subsurface damage. Micro cracks
18
form within the subsurface and coalesce to the surface, therefore causing loss of a frag-
ment of material inducing fatigue wear.
Figure 4. Fatigue Wear
Tribochemical wear (dental erosion)
It is caused when chemicals weaken the inter-molecular bonds of the surface and
potentiate the wear processes. There is interplay of erosion, attrition and three-body abra-
sion. In the oral cavity, acids normally cause extrinsic effects such as dietary acids or in-
trinsic effects resulting from gastric reflux. These acids weaken only the surface mole-
cules. These are then rubbed away by the movement of the surfaces and immediately the
underlying surface is attacked by the acid (56).
Adhesive wear
This occurs when there is a high attraction between surfaces such that cold welds
between the asperities. As the movement continues these micro-welds fracture, but not
along their original line of fusion. This type of wear is normally seen in metals (56).
Wear simulation devices
Many research centers have developed a variety of wear testing devices, each
with different degrees of complexity. As more and more materials are developed, and is
difficult to evaluate them by expensive time-consuming clinical trials to obtain a mea-
ningful data. Several mechanical testing systems (machines) have been created to simu-
19
late in vivo occlusal wear on the influence of test materials on natural enamel. The FDA
established guidelines for non-clinical laboratory studies including: equipment should be
calibrated and its maintenance defined and ensured so that the generation, measurement,
and assessment of data should be adequately tested, calibrated, and/or standardized (58).
In vitro models are easier than measuring in patient‘s mouth and do not depend on
patient compliance. In vitro models can provide reproducible chewing patterns for wear
evaluation where force profile, gliding path, medium and number of chewing cycles are
controlled. The machines and support systems offer controls to vary pH, temperature, an-
tagonist material, contact area, frequency of load cycles, load/force, third body medium,
lubrication and friction, duration of tooth contact, sliding speed, and wear measurement
technique.
All of which have been shown to affect wear rates. However, available machines
do not take into account the presence/absence of a periodontal ligament, which absorbs
some of the forces and influences motions during mastication. Due to the complexities of
recreating the mechanisms and properties of the oral cavity, no in vitro device can fully
simulate in vivo conditions. Hence, an important purpose of these machines is to serve as
a comparison of materials and to rank restorative materials according to their wear resis-
tance.
Many wear simulator research centers are trying to mimic the oral environment
and biological variables intending to rank restorative material according to their wear re-
sistance in comparison to reference materials.
20
ACTA wear machine (59-64)
The ACTA device has two metal wheels rotating in different directions with a dif-
ference of about 15% in the circumferential speed while being in close contact with each
other. The test specimens are placed on the circumference of one wheel whereas the other
wheel serves as antagonist. The force with which the two wheels contact is adjusted with
weights or springs. The stylus is a textured and hardened steel counter-wheel. The typical
medium used rice/millet seed shells suspension. A sliding movement with 15–20 N of
modifiable force (ranging between 0–50 N), 1.0Hz frequency and 100,000-200,000
cycles is used. Set-up: sample chamber with multi-chambered sample wheel, holding up
to 12 sample materials. The rotational speed of both motors ranges between 0–170 rpm
and is independently adjustable. Variables are contact stress, moving speed, and mutual
slip (15%). Although this machine does not closely simulate the biomechanical processes
of dental wear and forces applied are not high enough to produce fatigue wear, this ma-
chine is highly automated and provides a significant amount of screening data in a rela-
tively short time.
Figure 5. ACTA Wear Machine

21
Oregon Health Sciences University Oral Wear Simulator (OHSU) (65-67)
The OHSU device was a breakthrough device incorporating a sliding load which
duplicated the forces measured on a regular basis with a force sensor of a 10Hz measur-
ing frequency. This system is a multi-mode simulator. Stylus is enamel and conical, Me-
dium used is poppy seeds and PMMA beads. Movement is impact + sliding, and loading
is electro-magnetic. Frequency is 1.2 Hz with 50,000–100,000 no. of cycles, does not
have an integrated force sensor and the forces for abrasion testing (20 N) from one device
to another (65). The sliding distance varies from 5.36 to 6.24mm, producing variation in
the contact time. There is no systematic force/time measurements carried out with the
OHSU device.
Figure 6. Oregon Oral Wear Simulator
University of Alabama Dental Wear Simulator (52, 68-69)
The Alabama wear simulator in vitro wear device is the most cited as determined
by literature review. The Alabama wear simulator uses springs to generate an appropriate
22
force. The stylus is a flat of polyacetal cylinder or conical stainless steel styli. A variety
of materials were used for localized occlusal contact wear simulation and the medium
used is PMMA beads. The stylus movement is impact and rotation of 30°. Force exerted
is variable but generally is set at 75.6 N, vertical with a frequency of 1.2 Hz. It is a four-
station device with number of cycles ranging from 100,000–200,000–400,000. In this
wear set-up, multiple wear patterns can be seen. Generalized wear as simulation of the
wear during mastication.
Antagonistic enamel wear is simulated by wear of enamel created by direct con-
tact with the restorative materials. Vertical wear is measured as enamel height loss, ma-
terial stylus height loss, and total vertical height loss (the sum of the enamel height loss
and the restorative material height loss).
Figure 7. University of Alabama Dental Wear Simulator
Zurich computer-controlled masticator (70)
The stylus in this simulator is enamel. Medium is water (+alcohol + tooth brush-
ing). Movement: impact (+sliding) with a lateral movement of 0.2 mm, Force: 49 N with
23
a frequency of 1.7 Hz. Loading is electro-magnetic. Number of cycles range from
120,000, 240,000, 640,000 and 1,200,000 load cycles. Set-up: masticator. Variable:
toothbrush/toothpaste abrasion and chemical degradation. Zurich masticator has a rubber
socket that simulates the periodontal ligament and produces a sliding movement of the
sample, leading to a softening effect during wear simulation. The elastic modulus of the
rubber dam changes over time and these changes are accelerated by thermocycling.
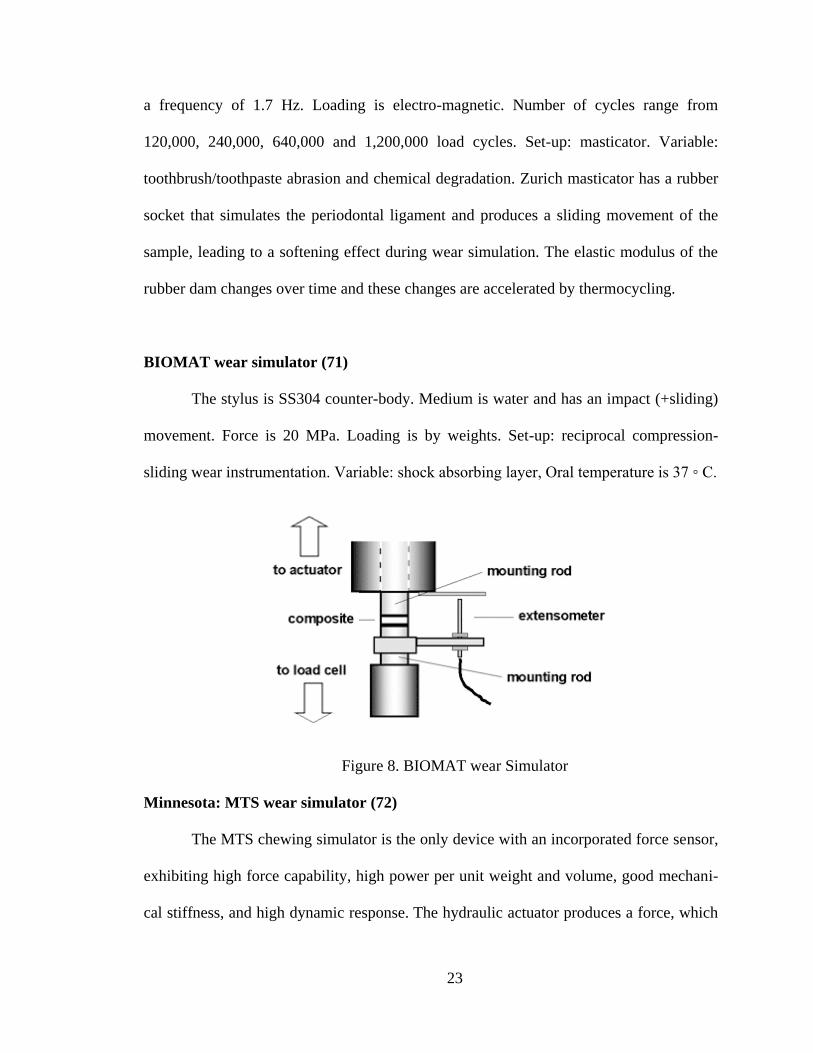
BIOMAT wear simulator (71)
The stylus is SS304 counter-body. Medium is water and has an impact (+sliding)
movement. Force is 20 MPa. Loading is by weights. Set-up: reciprocal compression-
sliding wear instrumentation. Variable: shock absorbing layer, Oral temperature is 37 ◦ C.
Figure 8. BIOMAT wear Simulator
Minnesota: MTS wear simulator (72)
The MTS chewing simulator is the only device with an incorporated force sensor,
exhibiting high force capability, high power per unit weight and volume, good mechani-
cal stiffness, and high dynamic response. The hydraulic actuator produces a force, which

24
is controlled within narrow limits in the descent/lifting and lateral movements; In addi-
tion, the force profile (―haversine waveform‖) is highly reproducible. Simulator control-
lers regulating the force (load cell), force profile (dual trace oscilloscope) and vertical and
lateral movements are incorporated into the testing device. The MTS chewing simulator
is an adapted version of the MTS device, which is widely used by medical companies for
the biomechanical testing of artificial hip and knee joints and implants. Stylus used is a
tooth, Medium: water giving a Movement: sliding. Force is 13.35 N and loading is hy-
draulic Number of cycles vary from 120,000, 240,000, 640,000 and 1,200,000 load
cycles. Set-up: masticator. Variables are contact stress, moving speed, mutual slip, and
third-body composition.
Figure 9. MTS wear Simulator

25
Willytec Wear simulator (73)
The Willytec chewing simulator has been commercially available since 1997.
This simulator is utilized to load crowns and bridges for fracture tests and to evaluate the
deterioration of the marginal integrity of restorations placed in extracted teeth. Stylus
used is enamel, empress (diameter 2.36 mm). Medium is water. Movement: gnashing,
slippage, striking with lateral movement of 0.7 mm. Force: 50 N with Loading by
weights. Number of cycles is 120,000 cycles. Set-up: masticator with programmable
Thermocycling (5–55 ◦ C). Variables: speed of impact, intensity of the impact, impact
and sliding load path.
Figure 10. Willytec Wear simulator
Simulators have been developed to measure the in vitro wear of dental materials;
each of these machines has their advantages and limitations.
In 2006, Heintz conducted a round robin study correlating the results of the dif-
ferent wear simulating devices with ACTA, OHSU, Willytec and Zurich wear devices on
eight different composites. Specimens were prepared at the Ivoclar Vivadent laboratories,
26
and sent to different testing sites and collected and data was analyzed (45). Heinz con-
cluded that the relative ranks of the materials differed significantly between the wear de-
vices. This is the only published paper to date in relation to validation of all systems. The
major limitation of the study was that the testing protocol and the method for measuring
wear at the individual test sites were not standardized. Variation would also arise from
the differences in antagonist material, number of cycles, temperature, pH, slurry medium,
and wear measurement technique. Each of these variables has been proven to affect wear
rates of composite materials. An accurate comparison is done between wear rankings for
the testing devices based on the load profiles and wear patterns, which differentiate the
wear devices. The Minnesota wear device is more expensive and complex than the other
devices and is located in only one test site. The BIOMAT wear device simulates only
two body wear. The Alabama wear simulating device has been used prolifically in the
United States. Existing oral wear devices have varying methods of simulating the abra-
sion and attrition phases of wear. The BIOMAT, OHSU, Minnesota and Willytec devic-
es have a stylus that impacts the specimen and slides a certain distance. The Leinfelder
wear testing device stylus impacts the specimen and rotates 30 degrees. These devices all
incorporate both the abrasion and attrition phases of mastication. The ACTA device has
two wheels, a wheel containing composite specimens and one steel counter surface wheel
that rotate next to each other at slightly different speeds. This device measures only the
abrasion phase of mastication. A round-robin test with the ACTA, OHSU, and Willytec
revealed that these devices measure different wear mechanisms. Despite prolific wear
testing by industry and academia with these devices, the International Standards Organi-
zation (ISO) has not specified a standard wear testing system.

27
Broadly, oral wear simulating devices incorporate three methods of producing
wear: sliding, sliding with impact, and rotation with impact. The effects of sliding wear
(abrasive and adhesive mechanisms) were compared with impact wear (abrasive, adhe-
sive and fatigue mechanisms) using a BIOMAT simulator. The comparative rankings of
seven restorative materials (including two composites) differed significantly between the
two methods, and the study concluded that ―there is no correlation between impact-cum-
sliding wear and non-impact sliding wear‖. There has not been a study that has analyzed
the effect of wear produced with impact and rotation to wear produced with impact and
sliding.
Contributing factors for in-vitro wear simulation
1. Standardization of the antagonist: Counter sample materials
The choice of the counter sample is a critical factor in establishing the pattern of
wear and in achieving an efficient in vitro wear testing system. A variety of factors in-
cluding hardness, wear surface evolution and frictional coefficients have to be consi-
dered, relative to the tribology of the in vivo situation. Assessment of potential counter
sample materials should be based on the essential tribological simulation supported by
investigations of mechanical, chemical and structural properties (74). Antagonists stan-
dardized for shape and size and according to materials should show mean values similar
to those found in natural, non-standardized cusps. Krejci et al. measured the shapes and
sizes of palatal cusps of non-erupted human upper third molars (74). Natural enamel an-
tagonists are preferable for the simulation of wear in the occlusal contact area.
2. Composition of the antagonist
28
A variety of antagonists have been used which include enamel, gold, ceramics,
stainless steel, annealed chromium-steel counter bodies, Alumina ball: diameter 10 mm
and Dental porcelain. A study by Heintz concluded that enamel provided similar wear
results as two different ceramic antagonists and produced no more variation in the wear
data (56).
3. Shape of the antagonist
A variety of antagonist such as flat, ball or rounded, flattened enamel surfaces,
enamel harvested from extracted human third molars and machined into cusps with a 5
mm spherical radius or hemi- spherically and Standardized human enamel cusps with a
uniform contact area have been used (75).
4. Load/force
In the load/force diagram several variations are possible. Static and/or sinusoidal
cyclic and dynamic, Contact loads ranging from 1, 10, 20, 25, 50, 75, 100 N, Contact
loads ranging from 1.7, 3.2, 4, 6.7, 9.95, 16.2 kgf/cm 2. Chewing force of 53 or 75.6 N
maximum force, Abrasion load: 20 N and attrition load: 90 N and Resiliency of the peri-
odontal ligament.
5. Contact area size: force per unit surface area. Facet area
The importance of the effect of contact area dimensions on the wear of composite
specimens and their opposing enamel cusps was evaluated in vitro by Krejci et al (74)
6. Number of cycles
In order to compare results different studies, number of cycles should be taken in-
to consideration. Ranging from 5000, 10,000, 25,000, 50,000, 100,000 to 120,000.
7. Chewing frequency: frequency of load cycles
29
The chewing frequency used in vitro studies varies from 1.2 to 1.7 Hz
8. Duration of tooth contact
The duration of tooth contact during the in vitro loading should mimic the in Vivo
situation. Load and time significantly influence wear.
9. Sliding speed: relative speed of opposing surfaces
The sliding speed (2.5 mm/s) during the in vitro simulation should be comparable
with the in vivo situation (40).
10. Temperature
Temperature plays a plasticizing effect. Constant temperature (20, 37 ◦ C) or
thermocycling (5–55 ◦ C) should be maintained.
11. Food bolus during mastication
Variety of food bolus or slurry can be used during mastication movement simulat-
ing such as Slurry of water and unplasticized PMMA beads, PMMA powder, hydroxya-
patite slurry and millet-seed/PMMA-beads mixture.
12. Lubricant and friction
Oral lubricants consist of saliva, plaque and pellicle. Together they form a boun-
dary lubrication system, because the thickness of the lubricant layer is insufficient to pre-
vent asperity contact through the film. Effectiveness of boundary lubricants is influenced
by their chemical properties than their viscosity. The buffering capacity of saliva and pla-
que is important in minimizing the corrosive effects of acids (thickness of 100–500 nm)
may act as a protective layer. Several liquids are incorporated in the three-body wear ma-
chines, like: Water, alcohol, acids, olive oil, olive oil/CaF slurry, artificial saliva, yes or
no inclusion of bacteria.

30
13. pH
pH conditions seem to influence dramatically the wear conditions and therefore
they should be controlled carefully during In vitro wear testing. Following pH levels (1.2,
3.3, and 7.0) are frequently used during wear simulation. They should mimic plaque ac-
ids, gastric acids and dietary acids. If human enamel is used as counter body, acidity of
the medium has an impact on the wear behavior. Interplay of abrasion, attrition and ero-
sion of human enamel under several different pH conditions has been tested. Combina-
tion of erosion and abrasion resulted in significantly greater wear than erosion alone. Si-
multaneous erosion and abrasion resulted in about 50% more wear than alternating ero-
sion and abrasion. Chewing of acidic foods with some abrasive properties might cause
enhanced tooth wear. Dentin is more susceptible than enamel to erosion and abrasion
alone or combined. Load and time significantly influence enamel wear both in acid and
neutral conditions. Depth of dentine erosion significantly increases non-linearly with time
and significantly decreases with increasing pH. Dentin is susceptible to erosion even at
relatively high pH, the tubule system is readily exposed and dentine, unlike enamel,
shows little propensity to remineralize (75-76).
14. Enzymes
Enzymes seem to have the potential to degrade the samples during in vitro testing.
de Gee et al. (55) used esterase solution in the ACTA wear machine. Chemical cycling
can induced a generalized swelling of the composite samples and a modified wear curve.
These enzymes can be generated in saliva and by bacterial metabolism.
15. Enamel structure and physiology related to microwear

31
Enamel structure has an effect on microwear. The micro structural element is im-
portant in direction of shearing force relative to enamel prisms and crystallite orientation.
The different responses of prismatic and non prismatic enamels to abrasion reflect the
influence of structure at the level of organization of crystallites rather than prisms per se.
Variation in crystallite orientation in prismatic enamels may contribute to optimal dental
function through the property of differential wear in functionally distinct regions of teeth
(77).
16. Wear debris
Impact of wear debris at the zone of impact and friction should be examined more
carefully.
Alabama Chewing Simulators
The original Alabama wear simulator in vitro wear device is the most cited as de-
termined by literature review. The University of Alabama Wear Simulator is a modifica-
tion of the Leinfelder type three-body wear device. Over the years there have been many
modifications of the original machine. In the first publication in 1989, a polyethylene
tape was used as intermediate substance, driven by a tape advancing system. The tape
was subsequently replaced by PMMA slurry. PMMA beads have been shown to produce
the maximum loss of material in the shortest amount of time. Also, they do not degrade in
water and they transfer the masticatory energy to the surface of the composite resin rather
than absorb it. The initial force used was 55N (12.4 lbs), which was increased to 75N
(16.8 lbs) during each cycle. This was consistent with conventional biting forces of 16.0
lbs. A 30° clockwise rotation was initiated as soon as the stylus touched the specimen
which was staged with the loading cycle. Originally, the restorative materials were incor-
32
porated into extracted molars that were trimmed flat, which simulated generalized wear.
More recently, localized wear has been simulated by using ceramics (alumina and zirco-
nia) and stainless steel balls as the actuator against 4mm deep restorations that are set into
brass holders filled with acrylic resin (68-69). Most studies using the Alabama wear ma-
chine are run from 100,000 to 400,000 cycles.
A new modified chewing simulator has been developed to simulate occlusal im-
pact overcoming the gradual loading and unloading of the Alabama Dental Wear Simula-
tor. Occlusal contact between opposing cusps may be considered as an impact loading of
two inelastic bodies. The Alabama Dental Wear Simulator utilizes a spring-loaded stylus
to apply a load, which is dissimilar to clinical occlusal contacts.
The modified Alabama chewing simulator brings a stylus into contact with a spe-
cimen at a controlled rate of sliding displacement with a axial load. The modified Ala-
bama chewing simulator can vary loads, antagonist material, No. of cycles, pH, thermo-
cycling and medium used. In the configuration proposed for this study, allows the stylus
to contact and slide up to 2 mm of translation with a 40 N axial load. This simulation is
thought to model deflective occlusal contact, and is under investigation for study beyond
this study.
33
OBJECTIVES AND HYPOTHESIS
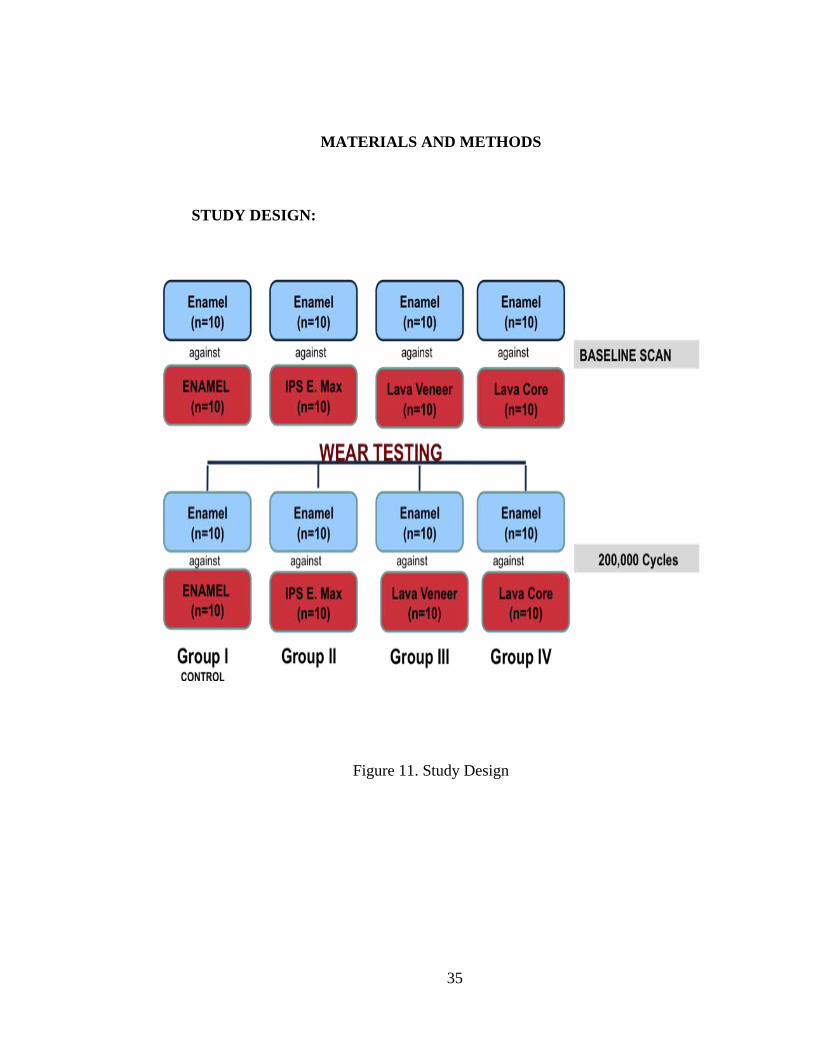
The objective of this study is to evaluate the wear of occlusal enamel and ceramic
restorative materials. Both the wear of the stylus and the wear of the specimen surface
will be investigated.
Hypothesis I:
There is no difference in the volumetric wear & wear depth of Lava core, IPS
e.max, Lava veneer material against enamel styli after 200,000 cycles.
Specific Aim I:
To measure by non-contact 3D profilometry and compare the volumetric wear &
wear depth of three ceramic materials against enamel styli after 200,000 cycles using a
modified-UAB simulator for an impact-sliding load without rotation. Differences be-
tween groups were determined by repeated-measures ANOVA and Tukey-Kramer‘s post-
hoc tests.
Hypothesis II:
There is no difference in the volumetric wear & wear depth of enamel styli after
200,000 cycles when against Lava core, IPS e.max, Lava veneer materials.
Specific Aim II:
To measure by non-contact 3D profilometry and compare the volumetric wear &
wear depth of enamel styli after 200,000 cycles when against three ceramic materials us-
ing a modified-UAB simulator for an impact-sliding load without rotation. Differences
34
between groups were determined by repeated-measures ANOVA and Tukey-Kramer‘s
post-hoc tests.
35
MATERIALS AND METHODS
STUDY DESIGN:
Figure 11. Study Design
36
Table 2
Materials used:
Product Type Manufacturer
Enamel Control Maxillary Premolars
IPS e.max Lithium Disilicate Ivoclar Vivadent
Lava Veneer Feldspathic Porcelain 3M ESPE
Lave Core Yttrium stabilized Zirconia 3M ESPE
Specimen preparation
Enamel Styli
10 samples per group were prepared for each enamel styli. Forty caries-free ex-
tracted human maxillary premolars were selected for each antagonist material and stored
them in a 2 percent solution of sodium azide. Stainless Steel Holders (Figure 12) were
designed and milled in the UAB Machine Shop to mount the coronal portion of caries-
free maxillary premolars.
Figure 12. Stainless Steel Holders

37
The coronal portions of maxillary premolars were mounted on screw in tips using
Panavia F 2.0 resin cement. In order to standardize the size and shape of each stylus, a
carbide bur was used to assure parallel shaping of the cusp to the long axis of the cusp to
assure similar geometry (Figure 13).
Figure 13. Carbide Burs
The styli were mounted on the Modified UAB Chewing Simulator and secured
parallel to the long axis of the wear simulator plunger (Figure 14).
Figure 14. Mounted Maxillary Premolar

38
Antagonist Molar, Control group
Ten caries-free extracted mandibular human molars for each material studied and
stored them in a 2 percent solution of sodium azide. Coronal portions of the mandibular
molar were mounted in a brass specimen holder using a self-cured acrylic resin. Ten flat-
specimens were prepared of molar enamel. Molars were standardized; assuring flat shap-
ing of the cusps to maintain similar geometry. The teeth were polished with a series of
400-, 600- & 1200-grit SiC paper under water-spray. Specimens were wet-finished with
0.05µm-alumina slurry/polishing cloth using a rotational polishing device (Buehler Ltd.,
IL, USA) and cleaned in an ultrasonic bath (5min) in distilled water and rinsed with wa-
ter. The specimens will then be stored for 24hrs at 37° C.
Antagonist restorative materials
Ten flat-specimens were prepared of each material, IPSe-max porcelain, Yttria-
stabilized Zirconia LAVA core, LAVA veneering porcelain (Table 2).
Figure 15. Ceramic Blocks
Specimens were mounted it in a brass specimen holder using a self-cured acrylic
resin and polished with a series of 400-, 600-, and 1200-grit SiC paper under water-spray.
39
Specimens were wet-finished with 0.05µm-alumina slurry/polishing cloth using a rota-
tional polishing device (Buehler Ltd., IL, USA) and cleaned in an ultrasonic bath (5min)
in distilled water and rinsed with water (Figure 16). The specimens will then be stored for
24hrs at 37° C.
Figure 16. Mounted ceramic specimen
This procedure ensured that the flat occlusal surface was parallel to a horizontal
plane, as well as to the flat surface of the energy-generating stylus.
Determination of Wear
The specimens were then subjected to wear on the modified UAB Chewing simu-
lator (Figure 17). A load of 40N was applied using enamel styli for 200,000 cycles. The
styli were set such that upon impact with the specimen a 2 mm slide across the specimen
surface under the constant 40 N load will occur. As soon as the maximum load was
achieved, the stylus rotated clockwise 30 degrees and then counter-rotated. Then the sty-
lus moved vertically up into its original position. At this point, the surfaces of the sam-
ples were covered with slurry of water and PMMA beads. Testing was performed in a
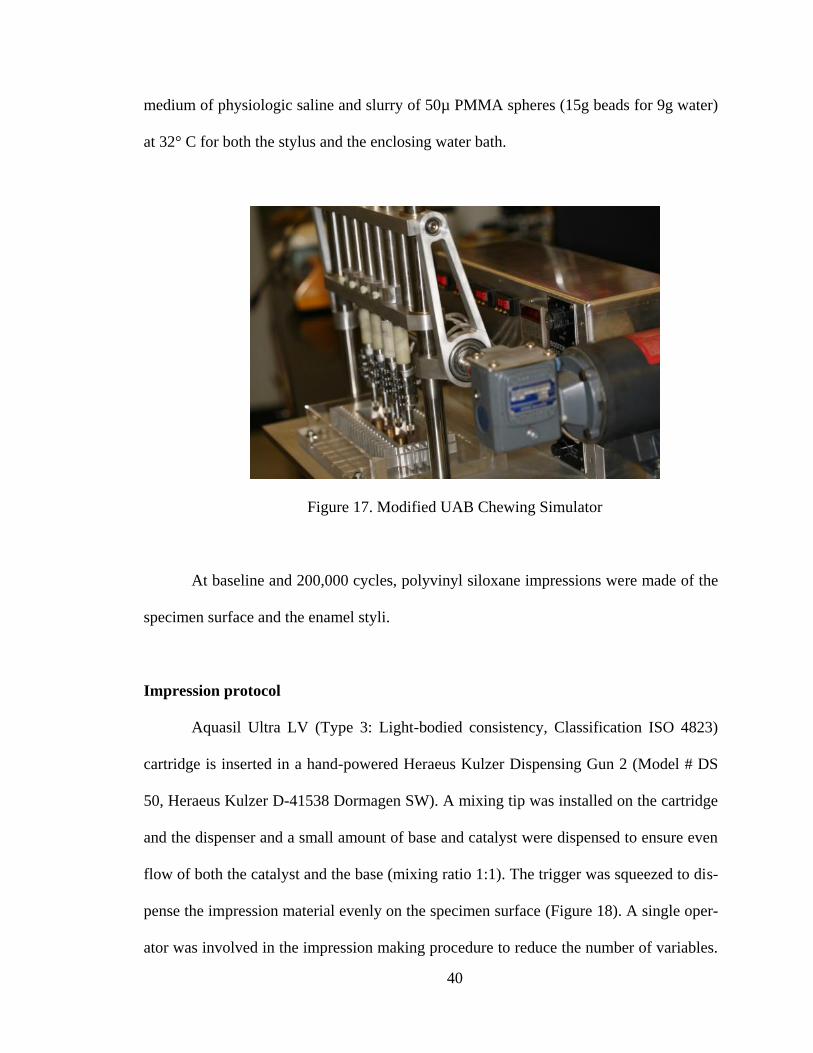
40
medium of physiologic saline and slurry of 50µ PMMA spheres (15g beads for 9g water)
at 32° C for both the stylus and the enclosing water bath.
Figure 17. Modified UAB Chewing Simulator
At baseline and 200,000 cycles, polyvinyl siloxane impressions were made of the
specimen surface and the enamel styli.
Impression protocol
Aquasil Ultra LV (Type 3: Light-bodied consistency, Classification ISO 4823)
cartridge is inserted in a hand-powered Heraeus Kulzer Dispensing Gun 2 (Model # DS
50, Heraeus Kulzer D-41538 Dormagen SW). A mixing tip was installed on the cartridge
and the dispenser and a small amount of base and catalyst were dispensed to ensure even
flow of both the catalyst and the base (mixing ratio 1:1). The trigger was squeezed to dis-
pense the impression material evenly on the specimen surface (Figure 18). A single oper-
ator was involved in the impression making procedure to reduce the number of variables.

41
Vinyl gloves were worn during manipulation of the material because latex gloves inhibit
the polymerization of polyvinyl siloxane (PVS) materials. The impression was allowed to
polymerize for 5 minutes after seating at an ambient temperature of 21 ± 2° C and humid-
ity of 33%. At this temperature the setting time of the impression material would be in-
creased. According to the manufacturer at 72° F (22° C) Aquasil Ultra Regular Set Im-
pression Materials have a minimum work time of 2 minutes 15 seconds and a minimum
removal time of 5 minutes from start of mix. In this study the impression was seated on
the enamel styli for 6 minutes and 10 seconds.
Figure 18. PVS Impressions
Casts
All the impressions were poured to scan in the order they were tested. The im-
pressions were washed thoroughly with tap water, to remove any remaining slurry and
dried with air water syringe to ensure no excess liquid remained. 32 ml distilled water,
accurately measured in a measuring cylinder at 23 ± 2° C was placed in a wet vacuum
42
bowl (Whip Mix Corporation, Model #6500, Louisville, US). 140 grams of Silky-Rock
type IV die stone powder (Whip Mix Corporation, Louisville, US) was added to the wa-
ter. The mixture was hand spatulated for 10 seconds to incorporate the powder in the wa-
ter and then vacuum mixed for another 30 seconds under 27 psi/Hg in a Whip Mix Com-
bination unit (Whip Mix Corporation, Louisville, US). The mix was poured at an ambient
temperature of 23 ± 2° C and humidity of 34 ± 1%. Using a stone vibrator set in a slow
mode the mixed stone was slowly poured in the impressions, and care taken to prevent
distortion. A new enamel stylus was used for each wear simulation. The samples were
retrieved after one hour (30 minutes recommended by the manufacturer). They were in-
spected for bubbles and other visible defects in the area of the preparation (Figure 19).
Specimens with such defects were discarded and new impressions were made. The spe-
cimens were then carefully sectioned to obtain the desired occlusal surface, the margin of
the maxillary premolar were evaluated for any defects during sectioning. The samples
were sectioned to make it easier to scan the sample with the non-contact 3D profilometer.
Samples were kept in a sealed plastic container at room temperature to avoid moisture
contamination.
Figure 19. Stone replicas of styli removed from PVS Impressions

43
Determination of volumetric wear & depth loss
A highly accurate non-contact surface profilometer, the Proscan 2000 (Scantron
Industrial Products Ltd., England), was used to scan the surfaces of the antagonist surfac-
es and enamel styli impressions made thereof. The Proscan 2000 is capable of 3D surface
profiling down to 10 nm depth of field and a submicron resolution at a rate of 1000 points
per second. The use of the (S-Type) chromatic sensor allows examination of dark and
rough surfaces with the object viewed in any orientation or auto-leveled using the pro-
prietary software Proscan and Proform. It scans any surface over an area up to 150mm x
100mm. It uses a focal multiplexing sensor with up to 0.005μm resolution. Safe white
light is transmitted through a lens, which has a built in spectral aberration. Takes the
white light and divides it into the full spectral field, focusing each different color fre-
quency at a slightly different point through a defined measuring range. When an object is
placed within this range, only one particular color frequency reflects back from the sur-
face. Information passes back into processor where a spectrometer analyzes the signal
and converts it to a measurement. Proscan combines these measurements with the precise
location of a moving X and Y linear table, giving three co-ordinates from which a three
dimensional profile is created. Results of the surface profile appear immediately on the
computer monitor and an image of the graphical 3-D representation can be saved on the
computer (Figure 20).
44
Figure 20. Proscan 2000
Impressions of each of the enamel styli, made with the Aquasil LV impression
material, were scanned using the same scanning parameters used for substrates. A partic-
ular substrate-impression-condition group was placed on a flat metal block affixed to the
flat scanning platform of the Proscan 2000 by modeling wax. Impressions were aligned in
a straight line such that each horizontal line on the impression met its corresponding hori-
zontal line on the adjacent impression in a straight line. This would enable the Proscan
software to read off designated random points on the lines, which were determined using
the matrix scan feature of the Proscan software (Figure 21). The step size was set at 20
μm. Then the sample rate was set at 300Hz. The S29/12 sensor model was chosen be-
cause that is the best sensor for measuring multiple teeth or a full arch. The S29/12 sensor
has a measuring range 0.12mm, resolution of .28μm, and uses chromatic, no triangula-
tion, technology.

45
Figure 21. Scanned specimens using Proscan
Therefore, the total samples were scanned at baseline and after 200,000 cycles
using the Proscan software (Figure 21). Wear volumetric loss differences between base-
line impression and 200,000 cycles were obtained using the Proform software by supe-
rimposition of the original (baseline) scans over the modified (200,000 cycles) scans
(Figure 22). For an impression to be dimensionally accurate and reproduce surface details
of the original model precisely, we determined that the closest value obtained in terms of
volume loss and the least difference obtained in terms of volume loss, to the original
sample/specimen would indicate the best adaptation of the impression material over its
substrate. This technique reduced the error along the XY axes. The measurements were
repeated two times on the same tooth and recorded to check the operators‘ reliability.
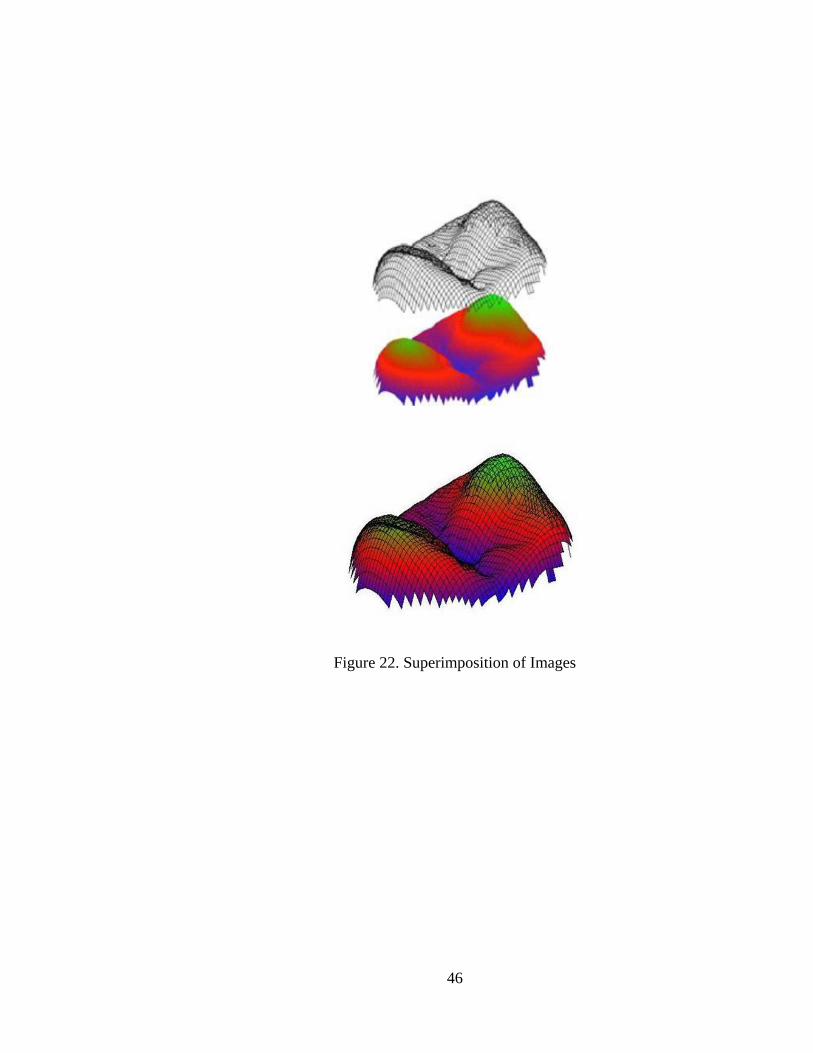
46
Figure 22. Superimposition of Images
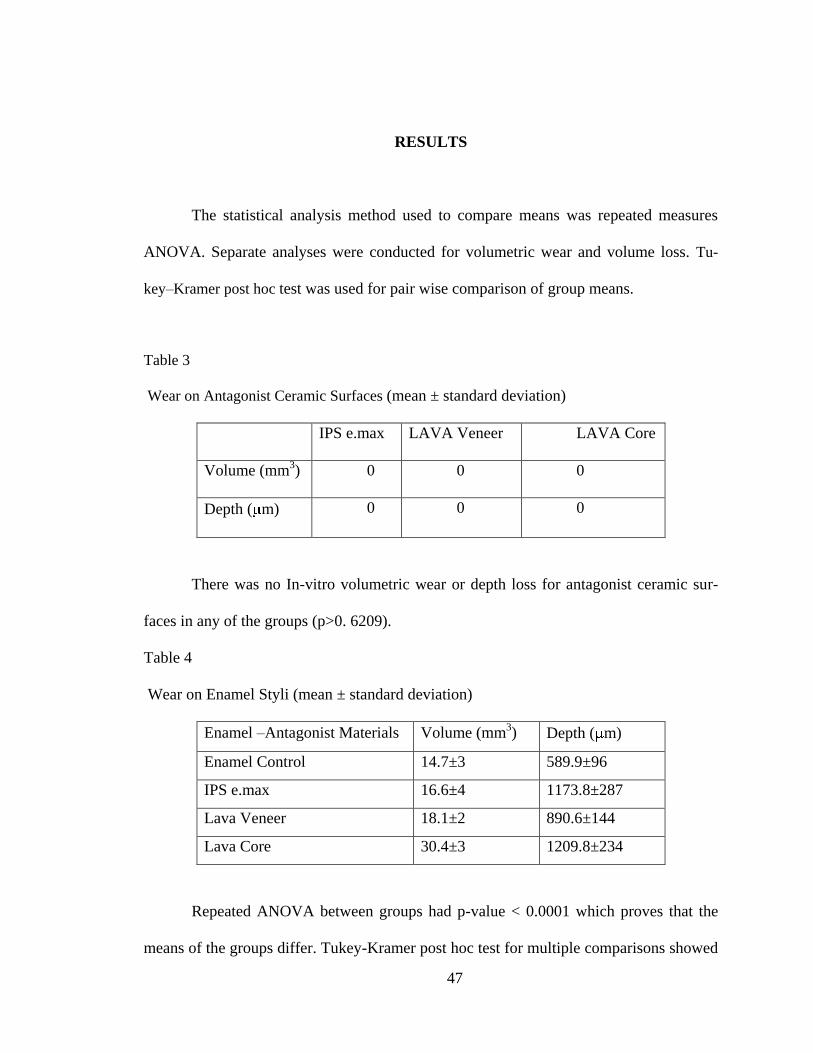
47
RESULTS
The statistical analysis method used to compare means was repeated measures
ANOVA. Separate analyses were conducted for volumetric wear and volume loss. Tu-
key–Kramer post hoc test was used for pair wise comparison of group means.
Table 3
Wear on Antagonist Ceramic Surfaces (mean ± standard deviation)
IPS e.max LAVA Veneer LAVA Core
Volume (mm3) 0 0 0
Depth ( m) 0 0 0
There was no In-vitro volumetric wear or depth loss for antagonist ceramic sur-
faces in any of the groups (p>0. 6209).
Table 4
Wear on Enamel Styli (mean ± standard deviation)
Enamel –Antagonist Materials Volume (mm3) Depth ( m)
Enamel Control 14.7±3 589.9±96
IPS e.max 16.6±4 1173.8±287
Lava Veneer 18.1±2 890.6±144
Lava Core 30.4±3 1209.8±234
Repeated ANOVA between groups had p-value < 0.0001 which proves that the
means of the groups differ. Tukey-Kramer post hoc test for multiple comparisons showed

48
that Lava core showed higher In-vitro volumetric wear loss than rest of the groups (p<
.0001) There was no differences for enamel wear depth for any of the groups (p>0.2757).
The results of this study are divided into two parts:
A. To measure by non-contact 3D profilometry and compare the volumetric wear
& wear depth of three ceramic materials against enamel styli after 200,000 cycles using a
modified-UAB simulator for an impact-sliding load without rotation.
B. To measure by non-contact 3D profilometry and compare the volumetric wear
& wear depth of enamel styli after 200,000 cycles when against three ceramic materials
using a modified-UAB simulator for an impact-sliding load without rotation.
Differences between groups were determined by repeated-measures ANOVA and
Tukey-Kramer‘s post-hoc tests.
Study I: Mean differences were measure and compare using repeated ANOVA
and Tukey-Kramer post-hoc test. There was no difference between the means in the
groups (p>0. 6209). Hence, we accept the null hypothesis stating that there is no differ-
ence in the volumetric wear & wear depth of Lava core, IPS e.max, Lava veneer material
against enamel styli after 200,000 cycles.
Study II: Mean differences were measure and compare using repeated ANOVA
and Tukey-Kramer post-hoc test. There was a difference between the means in the groups
(p< .0001). Hence, we failed to reject the null hypothesis stating that there is no differ-

49
ence in the volumetric wear & wear depth of enamel styli after 200,000 cycles when
against Lava core, IPS e.max, Lava veneer materials.

50
DISCUSSION
The three materials tested have each been developed to restore the anatomic form
and clinical function of human teeth. Under the limitations of the present study, the find-
ings indicate that ceramic materials are wear-resistant and caused wear of opposing ena-
mel occurred against all ceramic materials. IPS e.max & Lava Veneer material showed
no difference in terms of enamel wear compared to the Lava Core material (Zirconia)
To date only minimal data have been published regarding wear characteristics of
the ceramics evaluated. In a study by Suzuki et al IPS Empress (IPS e.max) is described
as having mechanical properties similar to those of enamel (78). Ratledge et al. report no
significant difference between in vitro wear data of unglazed IPS Empress opposing
enamel from their control: enamel opposing enamel (79). Seghi et al conducted a study
using OHSU oral wear simulator using enamel cusps (3rd
Molars) to the ceramic sub-
strates with the wear parameters: 20-N load, 1.0Hz, 8mm sliding action, 50,000 cycles,
Food-like slurry and concluded that IPS Empress 2 wear rate similar to Enamel (80).
Heintz et al evaluated the wear of enamel against IPS e.max using the Willytec chewing
simulator using enamel cusps (Maxillary Premolars) to the ceramic substrates with the
wear parameters: 120,000 cycles, 5 kg weight, 0.7 mm sliding action, 1.6 Hz; Speed was
60 mm/sec, Thermocycling and showed similar results as IPS. emax wear as similar to
enamel (81). Ceramic wear testing remains difficult to assess in both in vitro and in vivo
controlled evaluations.
Wear is a complex process that involves the removal of material and antagonist

51
material as a consequence of direct contact of the material and the stylus. Contributing
variables affecting wear volume loss can be mostly determined by factors as number of
cycles, sliding, surface hardness, surface roughness as well as resistance to fatigue and
fracture (82).
Number of cycles: 200,000 cycles were used in this study. According to Flanagan
et al swallowing cycle occurs approx. 590 times during a 24-hour period with 146 cycles
during eating, 394 cycles between meals while awake and 50 cycles during sleep. Hence,
200,000 cycles may represent 9.2 months swallowing tooth contacts (83, 84).
Sliding motion: According to Heintz et al the sliding distance in vivo has been rec-
orded as 0.3 mm in the anterior direction and 0.18 mm in the bucco-lingual direction. In
vitro devices have used sliding distances ranging from 0.2 mm – 8.0 mm. The slide in our
machine is about 2 mm. There is a lot of variation with other wear simulators, and we
know that during mastication, the grinding contact is much shorter than 2mm and tends
last about 0.2 seconds (81). Therefore, we felt this device would give a better approxima-
tion to the oral condition.
Hardness: Enamel has a Vickers hardness number of 336 VHN, IPS e.max: 591
VHN, Lava Veneer: 530 VHN & Lava Core: 1250 VHN. When considering the ceramic
materials in this study, they all are similar in physical and mechanical properties in that
they are hard and brittle. However, they also differ significantly in their hardness. Note,
that enamel is less hard than all the other materials. In wear simulation, the enamel was
worn while the ceramics demonstrated no measurable wear. Further, the enamel wear
against the zirconia ceramic was twice the volume of the lithium disilicate or the
feldspathic porcelain. This may be explained by a fundamental relationship of Tribology,

52
which is the study of wear.
The Archard wear equation describes the sliding abrasive wear of two surfaces as
they are worn.
Archard Wear Equation:
V= Volume of Wear Loss
W= Normal Load
H= Hardness of the softest contacting surfaces
K= Dimensional Constant
L= Sliding Length
Therefore, Hardness and Wear loss are inversely proportional. Enamel, being of
less hardness is more readily worn. However, this simplified equation does not account
for wear differences noted in this study.
Surface Roughness: All ceramic specimens were treated with the same finishing
and polishing protocol. However, the Zirconia ceramic has much higher hardness than the
other two materials. As finishing and polishing is in itself a wear process to progressively
reduce surface roughness to obtain a smoother surface, then, treatment of the Lava Core
material in the same way as a Feldspathic or a Lithium Disilicate will result in a rougher,
higher hardness surface, to oppose the enamel stylus. Therefore, because this material has
been proposed to be used for full contour restorations, this research demonstrates the
need for uniquely different finishing and polishing procedures for Zirconia.
Anisotropic Behavior of Enamel: The wear of the enamel should have a uniquely
VkWL
H
53
different mechanism of wear. Enamel is formed with rods or prisms in an organized ar-
rangement on a bed of lower modulus dentin. Translational forces which follow impact,
which we hypothesize are more similar to intraoral conditions, appeared to be effective in
degradation of enamel in wear testing. The ceramic materials do not have this type of mi-
crostructure, and this as well as the higher hardness, contributes to their excellent wear
resistance.
However, there is not so much work being done on the evaluation of effect of
these factors on wear of ceramic materials. It was expected that enamel styli would show
patterns of wear. This wear pattern could have been attributed to strength and hardness of
these materials in combination to the original shape of the enamel styli. As wear occurs,
the wear facet increases in size, the force per unit area decreases, and the potential wear
decreases. As wear facets increase in size, the wear pattern may be changing.
Majority of the existing wear simulators do not have consensus about the amount
of force exerted during mastication (81). With regard to the agreement of obtained results
in relation to certain ceramic materials, a comprehensive analysis cannot be performed, as
the test parameters contribute to their differences. These new materials have only been in
the market past few years and studies are still determining their survival rates. Clinical
trials are expensive and time consuming, so companies rely on results from laboratory
testing. It is easier and less expensive yet less accurate to work outside of the mouth
where conditions are standardized. Researchers cannot take wear results straight from in
vitro studies and use them to predict the amount of in vivo wear. Results from in vitro
studies can only be used to rank and compare materials.
The modified UAB Chewing Simulator is a new machine developed to closely
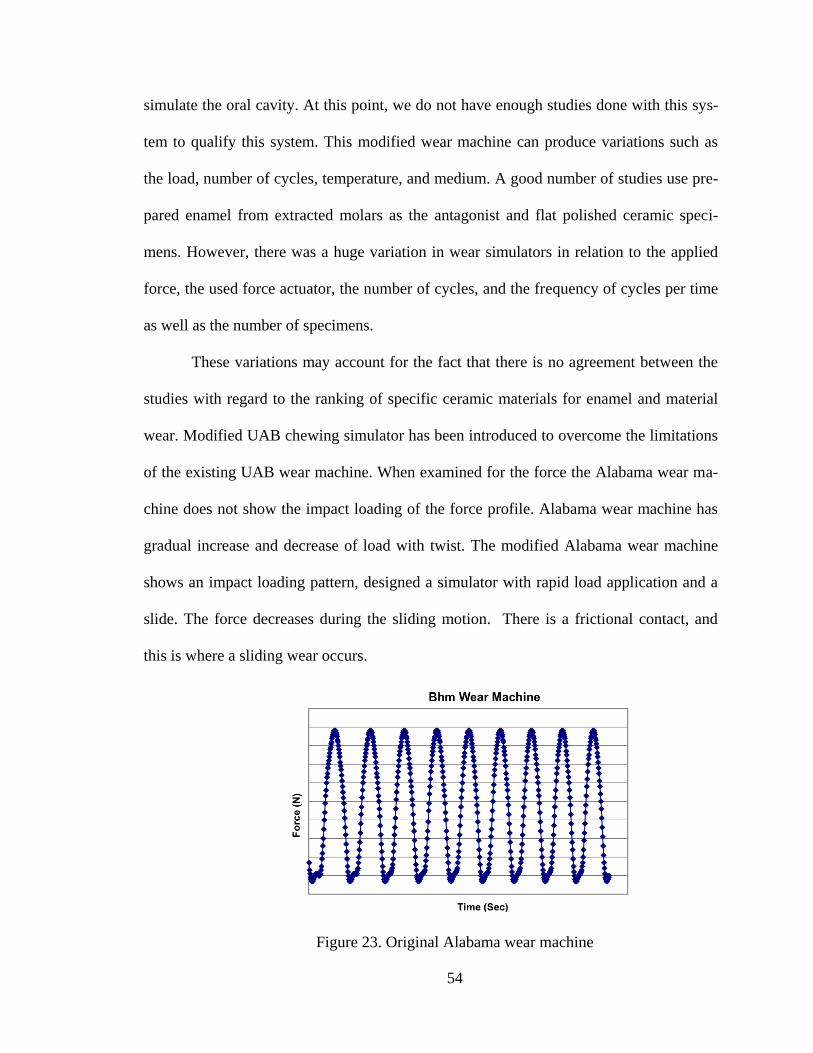
54
simulate the oral cavity. At this point, we do not have enough studies done with this sys-
tem to qualify this system. This modified wear machine can produce variations such as
the load, number of cycles, temperature, and medium. A good number of studies use pre-
pared enamel from extracted molars as the antagonist and flat polished ceramic speci-
mens. However, there was a huge variation in wear simulators in relation to the applied
force, the used force actuator, the number of cycles, and the frequency of cycles per time
as well as the number of specimens.
These variations may account for the fact that there is no agreement between the
studies with regard to the ranking of specific ceramic materials for enamel and material
wear. Modified UAB chewing simulator has been introduced to overcome the limitations
of the existing UAB wear machine. When examined for the force the Alabama wear ma-
chine does not show the impact loading of the force profile. Alabama wear machine has
gradual increase and decrease of load with twist. The modified Alabama wear machine
shows an impact loading pattern, designed a simulator with rapid load application and a
slide. The force decreases during the sliding motion. There is a frictional contact, and
this is where a sliding wear occurs.
Figure 23. Original Alabama wear machine
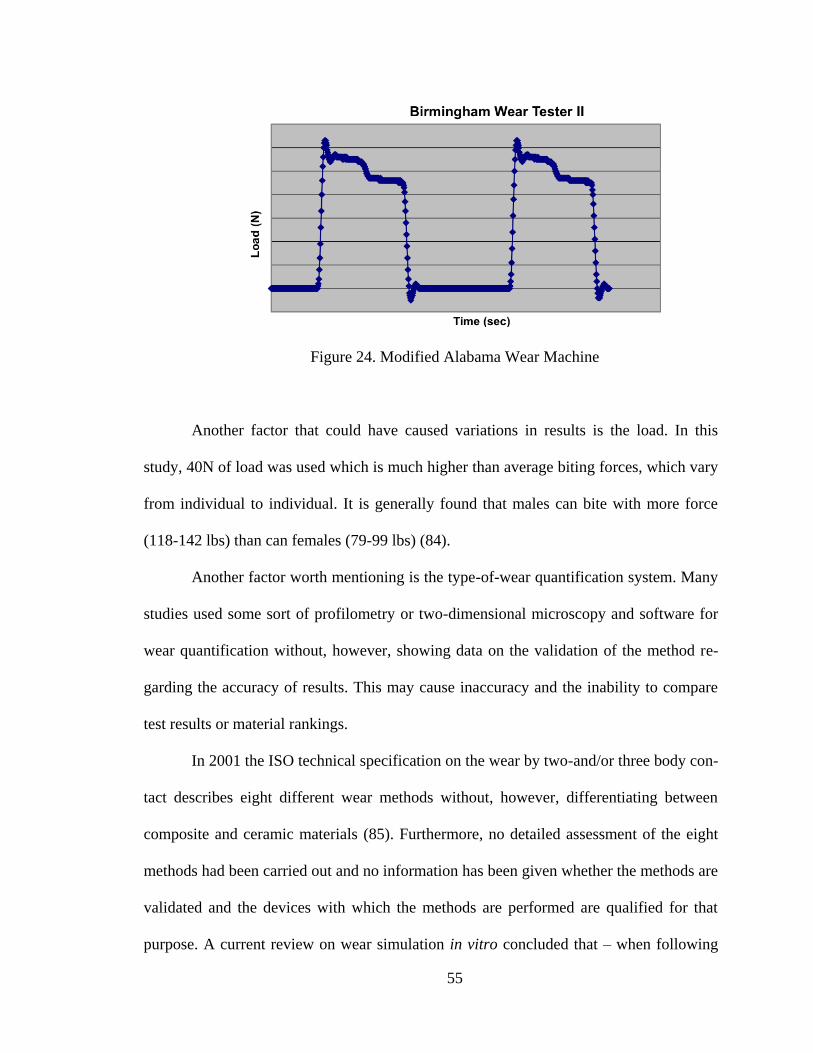
55
Figure 24. Modified Alabama Wear Machine
Another factor that could have caused variations in results is the load. In this
study, 40N of load was used which is much higher than average biting forces, which vary
from individual to individual. It is generally found that males can bite with more force
(118-142 lbs) than can females (79-99 lbs) (84).
Another factor worth mentioning is the type-of-wear quantification system. Many
studies used some sort of profilometry or two-dimensional microscopy and software for
wear quantification without, however, showing data on the validation of the method re-
garding the accuracy of results. This may cause inaccuracy and the inability to compare
test results or material rankings.
In 2001 the ISO technical specification on the wear by two-and/or three body con-
tact describes eight different wear methods without, however, differentiating between
composite and ceramic materials (85). Furthermore, no detailed assessment of the eight
methods had been carried out and no information has been given whether the methods are
validated and the devices with which the methods are performed are qualified for that
purpose. A current review on wear simulation in vitro concluded that – when following
56
the FDA guidelines on good laboratory practice (GLP) (86) – only the expensive MTS
wear simulator (Minnesota method) is a qualified machine for testing wear in vitro. The
force exerted by the hydraulic actuator is controlled and regulated during all movements
of the stylus. All the other simulators lack control and regulation of force development
during dynamic loading of the flat specimens. This may be an explanation for the high
coefficient of variation of the results in some wear simulators and the poor reproducibili-
ty of wear. A round robin test evaluating the wear of 10 dental materials (eight composite
materials, one ceramic and one amalgam) with five wear simulation methods (ACTA,
Munich, OHSU, Zurich, Ivoclar) showed that the results were not comparable, as all the
methods follow different wear testing concepts (87). There are concerns and problems
with different wear simulating devices as they exhibit different testing protocols & me-
thod for measuring wear is not standardized. There are variations in terms of differences
in antagonist material, number of cycles, temperature, pH, slurry medium, wear mea-
surement technique procedures. There is no standardization and consistency between Va-
riables: Force profile, number of cycles, medium, with very little correlation – Most wear
devices lack scientific evidence to correlate in vitro wear with in vivo wear. A good com-
promise with regard to costs, practicability and robustness is the Willytec chewing simu-
lator (88), which uses weights as the force actuator and stepping motors for vertical and
lateral movements (88). There is no clear tendency, which could lead to a sensible expla-
nation for the inconsistencies. We strived for standardizing as much of the test parameters
as possible, such as geometry of crowns and flat specimens, chewing simulator parame-
ters, etc. Most wear machines use test pieces with a flat surface, where as teeth and resto-
rations have complicated shapes which cause different stresses at various sites on the res-

57
toration surface. Kunzelmann et al. who used unprepared enamel cusps in their investiga-
tion described in their paper that preliminary unpublished tests showed that grinding and
polishing of enamel increased the wear properties of the antagonist compared to unpre-
pared cusps (89). This statement is in line with the results of the present study as more
variation of the results was detected for the prepared cusps. Furthermore, test results that
involved prepared cusps were inconsistent and sometimes illogical. As many of the re-
viewed studies concerning enamel wear for ceramic materials used prepared and polished
enamel cusps this fact may explain the different ranking of the same materials from one
study to another. The lack of correlation between clinical and laboratory studies should
not discourage the use of wear machines; but they should be used to investigate the un-
derlying mechanisms rather than to rank the potential clinical performance. All wear me-
thods lack the evidence of their clinical relevance because prospective studies correlating
in vitro with long-term in vivo results with identical materials are not available. In vivo
studies measuring enamel wear opposing ceramic materials with adequate equipment are
scarce. All wear methods lack the evidence of their clinical relevance because prospec-
tive studies correlating in vitro with long-term in vivo results with identical materials are
not available. In the beginning of this study, the goal was to have a larger sample size and
scan samples at baseline, 100,000 cycles and 200,000 cycles. Due to technical and time
issues, in the end, a representative sample was included in this study.

58
CONCLUSIONS
Within the limitations of this study, we conclude:
1) Enamel wear depends on antagonist restorative material used.
2) The modified UAB Wear Simulator appears to be effective in wear evaluation of
enamel against ceramic materials.
59
SUGGESTIONS FOR FUTURE RESEARCH
Future investigations should more closely duplicate the conditions in the oral cav-
ity and produce comparable wear variables to the ones found in vivo. By controlling va-
riables such as number of cycles, medium, force, temperature, and pH will do this. Anta-
gonist combinations found in the oral cavity as ceramics against ceramics, ceramics
against other restorative materials can be evaluated. Quality of the ceramic surface would
be another interesting factor to study. Future investigators should also look at changing
the mechanisms of a twist and slide rotation that would closely simulate the chewing pat-
terns in the oral cavity, and also in vitro studies on different chewing simulators with sim-
ilar variables & identical materials. Future investigations can try to assess differences in
clinical and in vitro wear and that the generations of the Alabama Wear Testing Devices
used to correlate to what is occurring in the mouth, and studies correlating in vitro with
long-term in vivo results with identical materials.
60
REFERENCES
1. Anusavice KJ, Soderholm KJ. Grossman DG. Implications of amalgam and ceramic
degradation in oral environment. MRS Bull 1993; Sept; 64-72.
2. McLean J. The future for dental porcelain. In: McLean JW, editor. Dental ceramics.
Proceedings of the first International Symposium on Ceramics. Chicago: Quintessence;
1983.p.13-40.
3. Reiger W. Medical applications of ceramics. In: Kostorz, G., eds. High-Tech Ceram-
ics-View points and Perspectives, 1291-228.London: Academic Press.
4. Seghi RR, Rosenstiel SF, Bauer P. Abrasion of Human Enamel by Different Dental
Ceramics In vitro. J Dent Res. 1991 Mar; 70(3):221-5.
5. KerschbaumTH, Paszyna GH, Klapp S, Meyer G,Verweilzeit und Risikoanalyse von
Kronen und Brucken.Dtsch Zanharztl 1991;46:20-24.
6. Kerschbaum T. Quitessenz 2004; 55:1126.
7. Scurria MS, Bader JD, Shugars DA. Meta-analysis of fixed partial dentures survival:
Prostheses and abutments. J Prosthet Dent 1998; 79; 459-464.
8. Creugers NH, Kayser AF,van‘t Hof MA. Ameta-analysis of the durability data on con-
ventional fixed bridges. Community Dent Oral Epidemiol 1994; 22:448-452.
9. Pjetursson BE, Tan K, Lang NP, Bragger U,Egger M, Zwahlen M. Asystemic review
of the survival rate and complication rates of fixed partial dentures after an observation
period of 5 years. Clin Oral Implants Res 2004; 15:667-676.
10. Albakry M, Guazzatto M, Swain MV. Fracture toughness and hardness evaluation of
three pressable all-ceramic dental materials.J Dent. 2003; 31:181-188.
11. Albakry M, Guazzalo M, Swain MV. Biaxial flexural strength, elastic moduli, and x-
ray diffraction characterization of three pressable all-ceramic materials. J Prosthet
Dent.2004; 89(4):374-380.
12. Guazzato M, Albakry M, Ringer SP, Swain MV. Strength, fracture toughness and mi-
crostructure of a selection of all-ceramic materials.Part I. Pressable and alumina glass-
infiltrated ceramics. Dent Mater. 2004; 20.441-448.
61
13. Holand W, Schweiger M, Frank M, Rheinberger V. A comparison of the microstruc-
ture and properties of the IPS Empress 2 and the IPS Empress Glass Ceramics. J Biomed
Mat Res.2000; 53 (4):297-303.
14. Della Bona A, Mecholsky JJ Jr, Anusavice KJ. Fracture behavior of Lithia disilicate
and leucite based ceramics. Dent Mater. 2004; 20:956-962.
15. Piwowarczyk A, Lauer HC, Sorensen JA. In vitro shear bond strength of cementing
agents to fixed prosthodontic restorative materials. J Prosthet Dent. 2004; 92(3):265-273.
16. Toksavul S, Toman M.A short-term clinical evaluation of IPS Empress 2 crowns. Int
J Prosthodont. 2007; 20(2):168-72.
17. Tastonak B, Sertgoz A. Two-year clinical evaluation of lithia-disilicate-based all-
ceramic crowns and fixed partial dentures. Dent Mater. 2006; 22(11):1008-13. Epub 2005
Dec 20.
18. Fasbinder DJ, Dennison JB, Heys D, Neiva G. A clinical evaluation of chairside li-
thium disilicate CAD/CAM crowns: a two-year report. J Am Dent Assoc. 2010 Jun; 141
Suppl 2:10S-4S.
19. Etman MK, Woolford MJ. Three-year clinical evaluation of two ceramic crown sys-
tems: a preliminary study. J Prosthet Dent. 2010 Feb;103(2):80-90.
20. Brochu JF, El-Mowafy O. Longevity and clinical performance of IPS-Empress ce-
ramic restorations – a literature review: J Can Dent Assoc. 2002; 68(4):233-237.
21. Guazzato M, Albakry M, Ringer SP, Swain MV. Strength, fracture toughness and mi-
crostructure of a selection of all-ceramic materials. Part I. Pressable and alumina glass-
infiltrated ceramics. Dent Mater. 2004; 20.441-448.
22. Sailer I, Feher A, Filser F, et al. Five year clinical results of zirconia frameworks for
posterior fixed partial dentures. Int J Prosthodont. 2007;20 (4):383-388.
23. Christensen RP, Eriksson KA, Ploeger BJ. Clinical performance of PFM, zirconia,
and alumina three-unit posterior prostheses. Available at:
http://iadr.confex.com/iadr/2008Toronto/techprogram/abstract_105962.htm.
24. Raigrodski AJ, Chiche GJ, Potiket N. The efficacy of posterior three-unit zirconium
oxide- based ceramic fixed partial dental prostheses: A prospective clinical pilot study. J
Prosthet Dent. 2006; 96 (4):237-244.
25. Edward A. McLaren, Phong Tran Cao. Ceramics in Dentistry—Part I: Classes of Ma-
terials. Inside Dentistry. October 2009. Insidedentistry.net
62
26. Schmitt J, Holst S, Wichmann M, Reich S, Göllner M, Hamel J. Zirconia Posterior
Fixed Partial Dentures: A Prospective Clinical 3-year Follow-up. Int. Journal of Prostho-
dontics 2009. November/December /Volume 22, Issue 6.
27. Sailer I, Fehér A, Filser F, Lüthy H, Gauckler LJ, Schärer P, Franz Hämmerle CH.
Prospective clinical study of zirconia posterior fixed partial dentures: 3-year follow-up.
Quintessence Int. 2006 Oct; 37(9):685-93.
28. Sailer I, Fehér A, Filser F, Gauckler LJ, Lüthy H, Hämmerle CH. Five-year clinical
results of zirconia frameworks for posterior fixed partial dentures. Int J Prosthodont. 2007
Jul-Aug; 20(4):383-8
29. Delong R. Intra-oral restorative materials: Rethinking the current approaches: How
to measure wear. Dent Mater 2006; 22: 702-711.
30. Christensen GJ. The use of porcelain-fused-to-metal restorations in current dental
practice: a survey. Journal of Prosthetic Dentistry, 1986; 56:1-3.
31. Mahalick JA, Knap FJ, Weiter EJ. Occlusal Wear in Prosthodontics, J Am Dent As-
soc 1971; 82:154-159.
32. Monasky GE, Taylor DF.Studies on the Wear of Porcelain, Enamel, and Gold, J Pros-
thet Dent 1971; 25:299-306.
33. Ekfeldt A, 0ilo G. Occlusal Contact Wear of Prosthodontic Materials, Acta Odontol
Scand 1988; 46:159-169.
34. Lambrechts P, Braem M, Vuylsteke-wauters, Vanherle MG, Quantitative In Vivo
wear of human enamelJ Dent Res 68(12):1752-1754,Dec,1989
35. Villa G, Giacobini G. Dental microwear. Morphological, functional and phylogenetic
correlations. Ital J Anat Embryol. 1998 Jul-Sep;103(3):53-84.
36. Ekfeldt A, Fransson B, Soderlund B, Oilo G. Wear resistance of some prosthodontic
materials In Vivo. Acta Odontol Scand 1993;51:99–107.
37. CRA. Posterior full crowns 2001, Part 3: 2-year clinical performance of CAD-CAM
copings & full crowns. CRA Newslett 2001;25:1–3.
38. Etman MK, Ferenczi L, Woolford MJ. Tooth wear and wear of ceramic restorations:
prospective clinical study. J Dent Res2006;85 (Special Issue A): Abstract 215.
39. Esquivel-Upshaw JF, Young H, Jones J, Yang M, Anusavice KJ.In Vivo wear of
enamel by a lithia disilicate-based core ceramic used for posterior fixed partial dentures:
first-yearresults. Int J Prosthodont 2006;19:391–6.
63
40. Oh WS, Delong R, Anusavice KJ. Factors affecting enamel and ceramic wear: a lite-
rature review. J Prosthet Dent 2002;87:451–9.
41. Szeri AZ, In: Larson RW, Dorfman M, editors. Tribology friction, lubrication,
and wear. McGraw-Hill Book Company; 1980, ISBN 0-07-062663-4.
42. Rabinowicz E. Friction and wear of materials. New York: John Wiley; 1965. p
167-179.
43. Spijker AV, Rodriguez M, Kreulen C, Bronkhorst E, Bartlett DW, Creugers NHJ.
Prevalence of Tooth Wear in Adults. Int J Prosthodont 2009; 22(1):35-42.
44. Lewis.G. Predictors of clinical wear of restorative dental composite materials. Bio-
med Mater Eng. 1993 Fall;3(3):167-74.
45. Heintze SD. How to qualify and validate wear simulation devices and methods. Dent
Mater 2006; 22: 712-34.
46. Genco RJ. Current view of risk factors for periodontal diseases. J Periodontol
1996;67:1041–9.
47. Carlsson GE, Egermark I, Magnusson T. Predictors of signs and symptoms of tempo-
romandibular disorders: a 20-year follow-up study from childhood to adulthood. Acta
Odontol Scand 2002; 60:180–5.
48. John MT, Frank H, Lobbezoo F, Drangsholt M, Dette KE.No association between
incisal tooth wear and temporomandibular disorders. J Prosthet Dent 2002;87:197–203.
49. Seligman DA, Pullinger AG, Solberg WK. The prevalence of dental attrition and its
association with factors of age,gender, occlusion, and TMJ symptomatology. J Dent Res
1988; 67:1323–33.
50. Bernhardt O, Gesch D, Splieth C, Schwahn C, Mack F,Kocher T, et al. Risk factors
for high occlusal wear scores in a population-based sample: results of the Study of Health
in Pomerania (SHIP). Int J Prosthodont 2004; 17:333–9.
51. Gesch D, Bernhardt O, Kirbschus A. Association of malocclusion and functional oc-
clusion with temporomandibular disorders in adults: systematic review of population-
based studies. Quintessence Int 2004; 35:211–21.
52. Leinfelder KF, Beaudreau RW, Mazer RB. An In vitro device for predicting clinical
wear. Quintessence Int 1989;20 (10):755–61.
53. De Gee AJ, Pallav P, Davidson CL, J.Dent. Res.19 (1994) 39-45.

64
54. R.L.Sakaguchi, W.H.Douglas, R.Delong, M.R.Pintado, Dent. Mater.2 (1994) 235-
240.
55. Bates JF, Stafford GD, Harrison A, J.Oral Rehabil.2 (1994) 281-301.
51. Mair LH. Wear in the mouth: the tribological dimension.: Tooth wear and sensitivity.
Clinical advances in restorative dentistry. Martin Dunitz Ltd.; 2000.
56. S.D. Heintze, G. Zellweger, A. Cavalleri, J. Ferracane. Influence of the antagonist
material on the wear of different composites using two different wear simulation me-
thods. Dent Mater. 2006 Feb; 22 (2):166-75. Epub 2005 Aug 8.
57. Lambrechts P, Braem M, Vuysteke-Wauters M, Vanherle G.Quantitative In Vivo
wear of human enamel. J Dent Res 1989; 68:1752–4.
58. FDA, Center for Devices and Radiological Health. Good Laboratory Practice (GLP)
(PART 58 52 FR 33780, 1978. Last revision 2004); 1978.
59. de Gee AJ, Pallav P, Davidson CL. Effect of abrasion medium on wear of stress-
bearing composites and amalgam In vitro. J Dent Res 1986;65 (5):654–8.
60. Pallav P, Davidson CL, de Gee AJ. Wear rates of composites, an amalgam, and ena-
mel under stress-bearing conditions. J Prosthet Dent 1988; 59 (4):426–9.
61. Pallav P, de Gee AJ, Davidson CL, Erickson RL, Glasspoole EA. The influence of
admixing microfiller to small-particle composite resin on wear, tensile strength, hardness,
and surface roughness. J Dent Res 1989; 68(3):489–90.
62. de Gee AJ, Wendt SL, Werner A, Davidson CL. Influence of enzymes and plaque
acids on In vitro wear of dental composites. Biomaterials 1996; 17(13):1327–32.
63. Graf K, Johnson GH, Mehl A, Rammelsberg P. The influence of dental alloys on
three-body wear of human enamel and dentin in an inlay-like situation. Oper Dent 2002;
27(2):167–74.
64. de Gee AJ, Pallav P. Occlusal wear simulation with the ACTA wear machine. J
Dent. 1994; 22 Suppl 1:S21-7.
65. Condon JR, Ferracane JL. Evaluation of composite wear with a new multi-mode oral
wear simulator. Dent Mater 1996; 12(4):218–26.
66. Freiberg RS, Ferracane JL. Evaluation of cure, properties and wear resistance of
Artglass dental composite. Am J Dent 1998; 11(5):214–8.
67. Ferracane JL, Condon JR. In vitro evaluation of the marginal degradation of dental
composites under simulated occlusal loading. Dent Mater 1999; 15 (4):262–7.
65
68. Suzuki S, Leinfelder KF, Kawai K, Tsuchitani Y. Effect of particle variation on wear
rates of posterior composites. Am J Dent 1995; 8(4): 173–8.
69. Ramp MH, Ramp LC, Suzuki S. Vertical height loss: an investigation of four restora-
tive materials opposing enamel. J Prosthodont 1999; 8(4):252–7.
70. Gohring TN, Schonenberger KA, Lutz F. Potential of restorative systems with simpli-
fied adhesives: quantitative analysis of wear and marginal adaptation In vitro. Am JDent
2003; 16(4):275–82
71. Yap AU, Ong LF, Teoh SH, Hastings GW. Comparative wear ranking of dental res-
toratives with the BIOMAT wear simulator. J Oral Rehabil 1999; 26 (3):228–35.
72. Sakaguchi RL, Douglas WH, DeLong R, Pintado MR. The wear of a posterior com-
posite in an artificial mouth: a clinical correlation. Dent Mater 1986; 2:235–40.
73. Lambrechts P, Debels E, van Landuyt K, Peumans M, van Meerbeek B. How to si-
mulate wear? Overview of existing methods. Dent Mater 2006; 22:693-701.
74. Krejci I, Albert P, Lutz F.The influence of antagonist standardization on wear. J Dent
Res 1999; 78(2):713–9.
75. Eisenburger M, Addy M. Erosion and attrition of human enamel In vitro. Part II. In-
fluence of time and loading. JDent 2002; 30(7/8):349–52.
76. Shabanian M, Richards LC. In vitro wear rates of materials under different loads and
varying pH. J Prosthet Dent 2002; 87(6):650–6.
77. Maas MC. Enamel structure and microwear: an experimental study of the response of
enamel to shearing force. Am J Phys Anthropol 1991; 85(1):31–49.
78. Ramp MH, Suzuki S, Cox CF, Lacefield WR, Koth DL, Evaluation of wear: Enamel
opposing three ceramic materials and a gold alloy. Prosthet Dent I997; 77:523- 30.
79. Ratledge DK, Smith BG, Wilson RF. The effect of restorative materials on the wear
of human enamel. J Prosthet Dent 1994; 72:194-203.
80. Seghi RR. Wear of enamel opposing low-fusing and conventional ceramic restorative
materials. J Prosthodont. 2001 Mar; 10 (1):8-15.
81. Heintz SD. Wear of ceramic and antagonist—A systematic evaluation of influencing
factors in vitro. Dent Mater. 2008 Apr; 24(4):433-49. Epub 2007 Aug 27.
82. Ferracane JL. Is the wear of dental composites still a clinical concern? Is there still a
need for In vitro wear simulating devices? Dent Mater 2006; 22:689–92.
66
83. Flanagan JB: The 24-hour pattern of swallowing in man, J Dent Res 42(abstr
#165):1072, 1963.
84. Okeson JP. Management of temporomandibular disorders and occlusion. St Louis:
CV Mosby, 1989:259-60.
85. ISO. Dental materials—Guidance on testing of wear. Part 2: Wear by two-and/or
three body contact. Techn Specific 2001. No. 14569–2.
86. FDA. Good Laboratory Practice (GLP). (PART 58 52 FR 33780), 1978, last revision
2004.
87. Heintze SD, Zappini G, Rousson V. Wear of 10 dental restorative materials in five
wear simulators—Results of a round robin test. Dent Mater 2005; 21:304–17.
88. Willytec. Multifunctional chewing simulator—Instructions of use 2001:1–39.
89. Kunzelmann KH, Jelen B, Mehl A, Hickel R. Wear evaluation of MZ100 compared
to ceramic CAD/CAM materials. Int J Comput Dent 2001; 4:171–84.
67
Appendix 1
IRB Approval Form
68
69
Appendix 2
Tables-Repeated Measure ANOVA &Tukey-Kramer post hoc test

70
Table 1
Table 2

71
Table 3
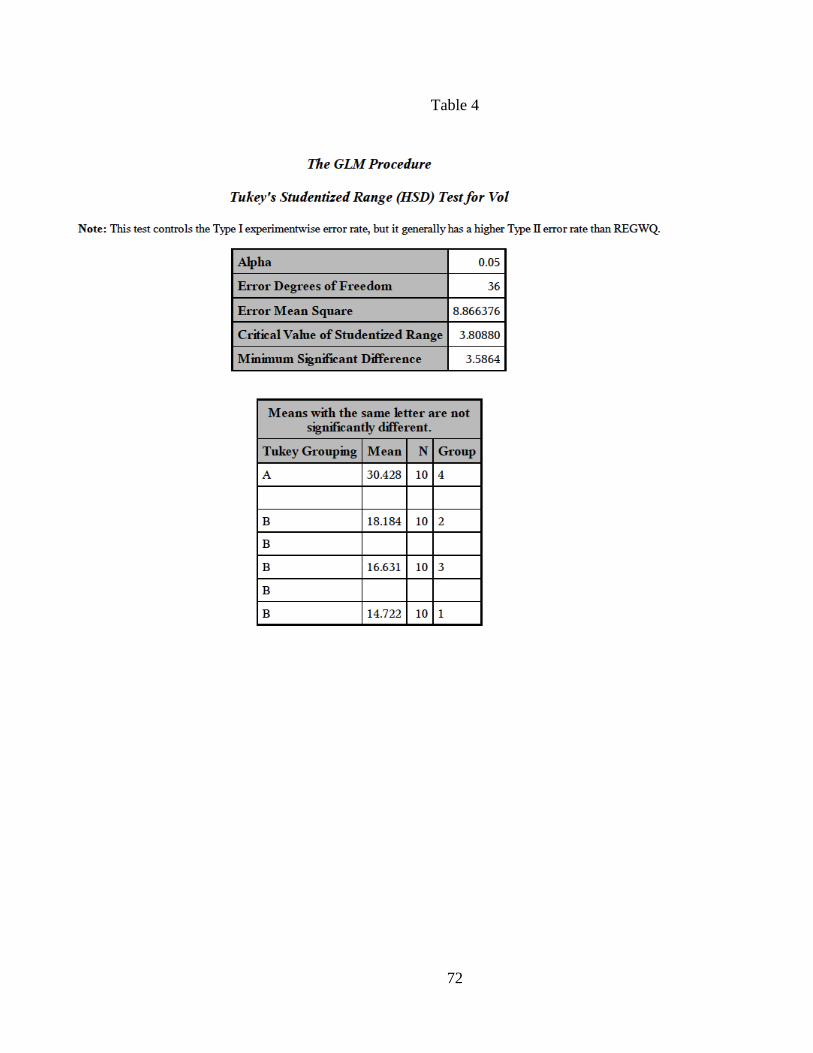
72
Table 4
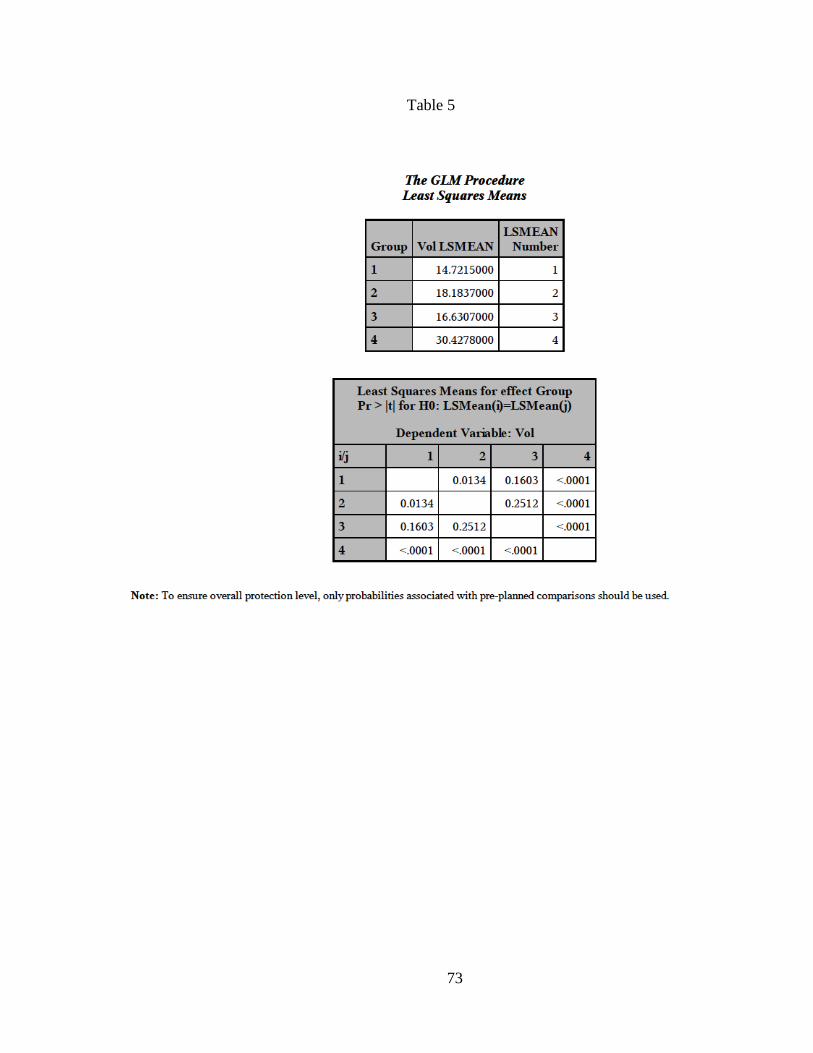
73
Table 5
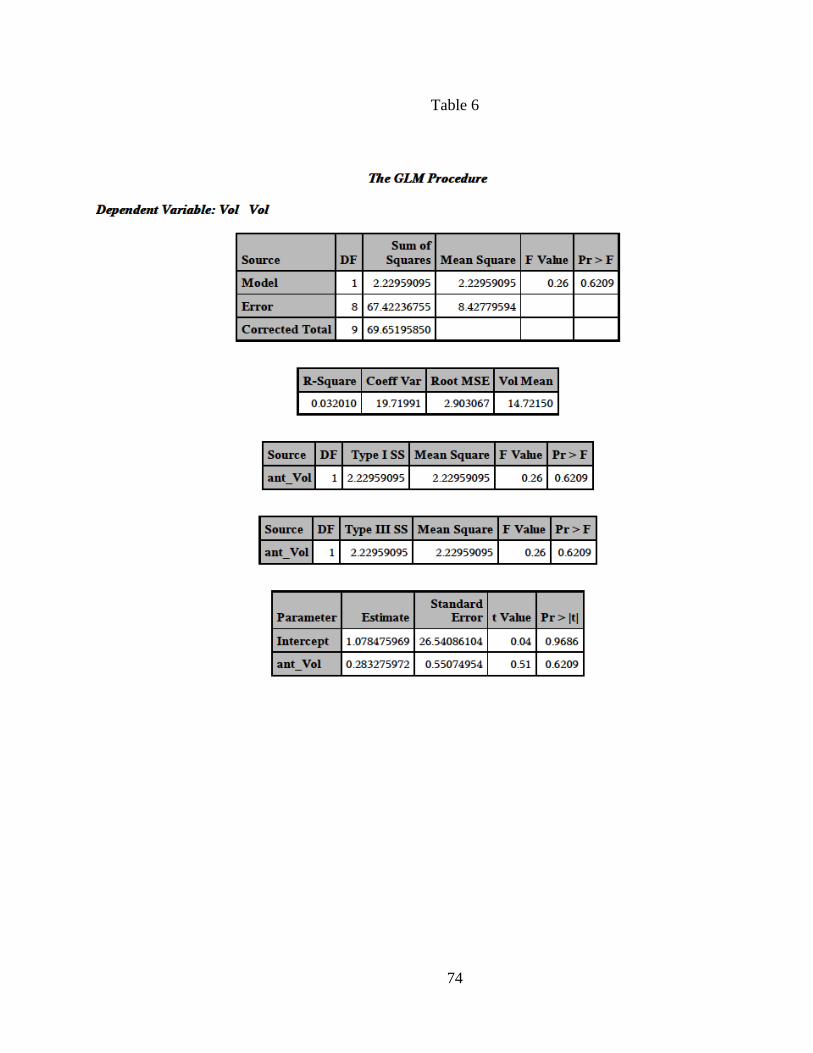
74
Table 6
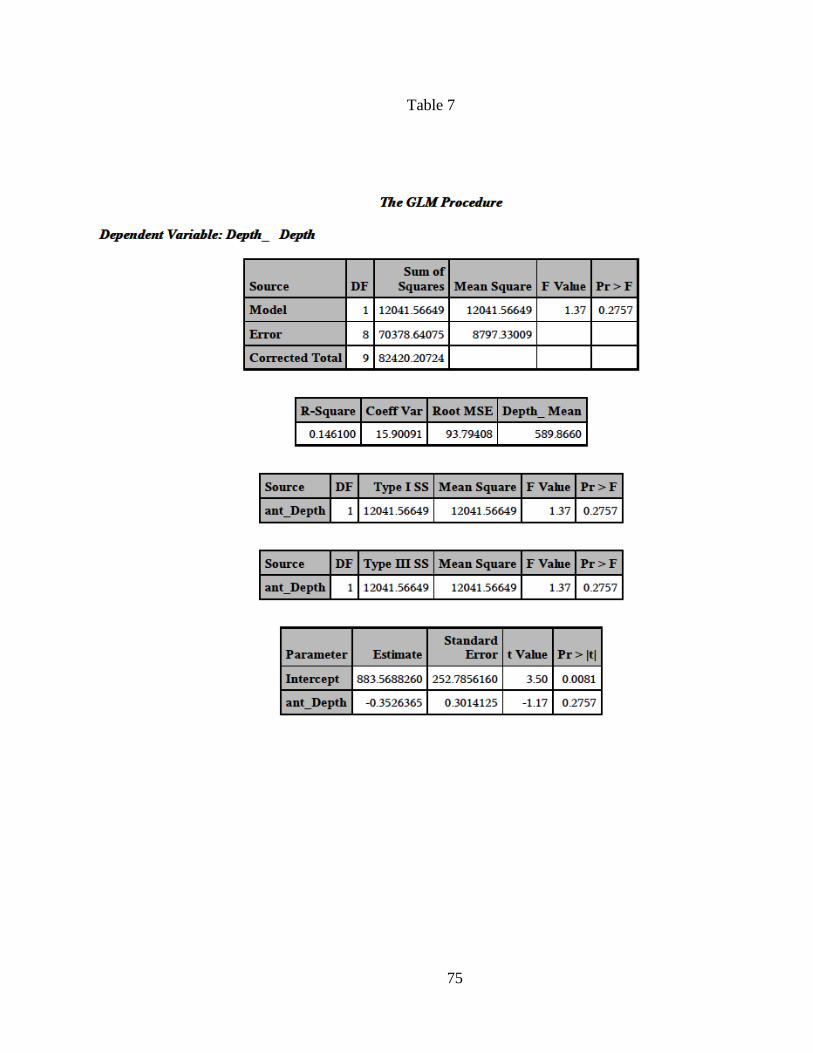
75
Table 7

76
Appendix 3
In Vitro Enamel styli Scans at Baseline & 200,000 cycles
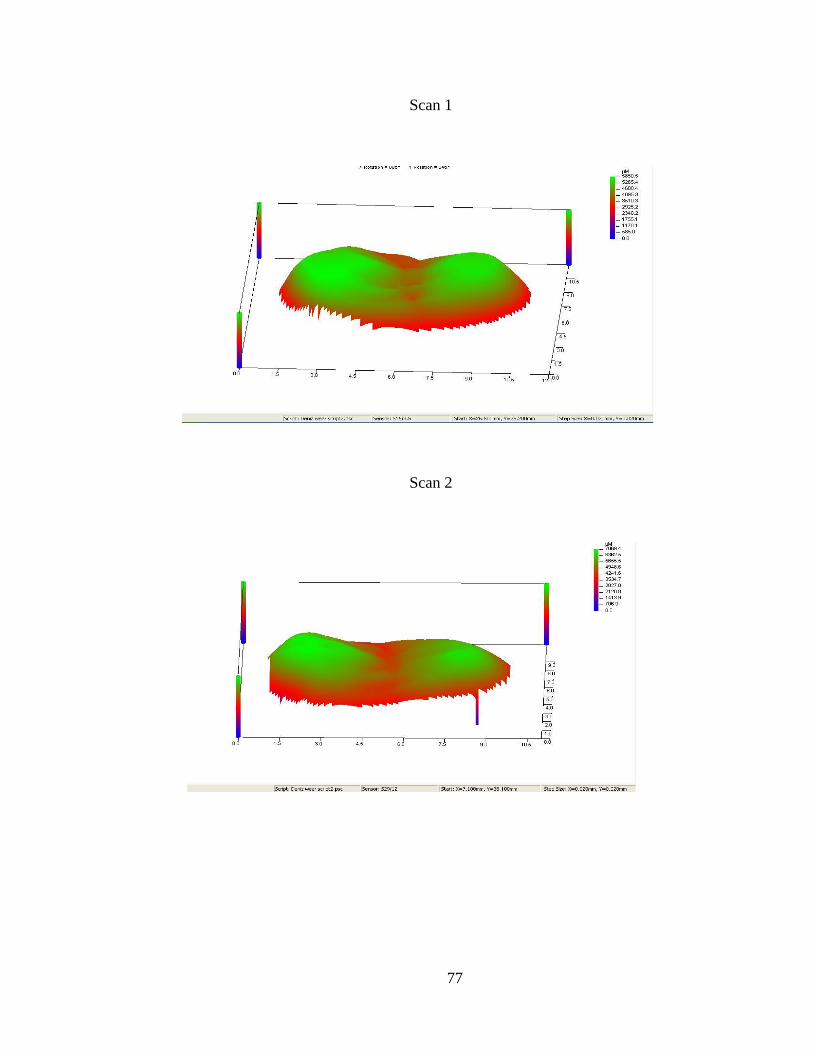
77
Scan 1
Scan 2
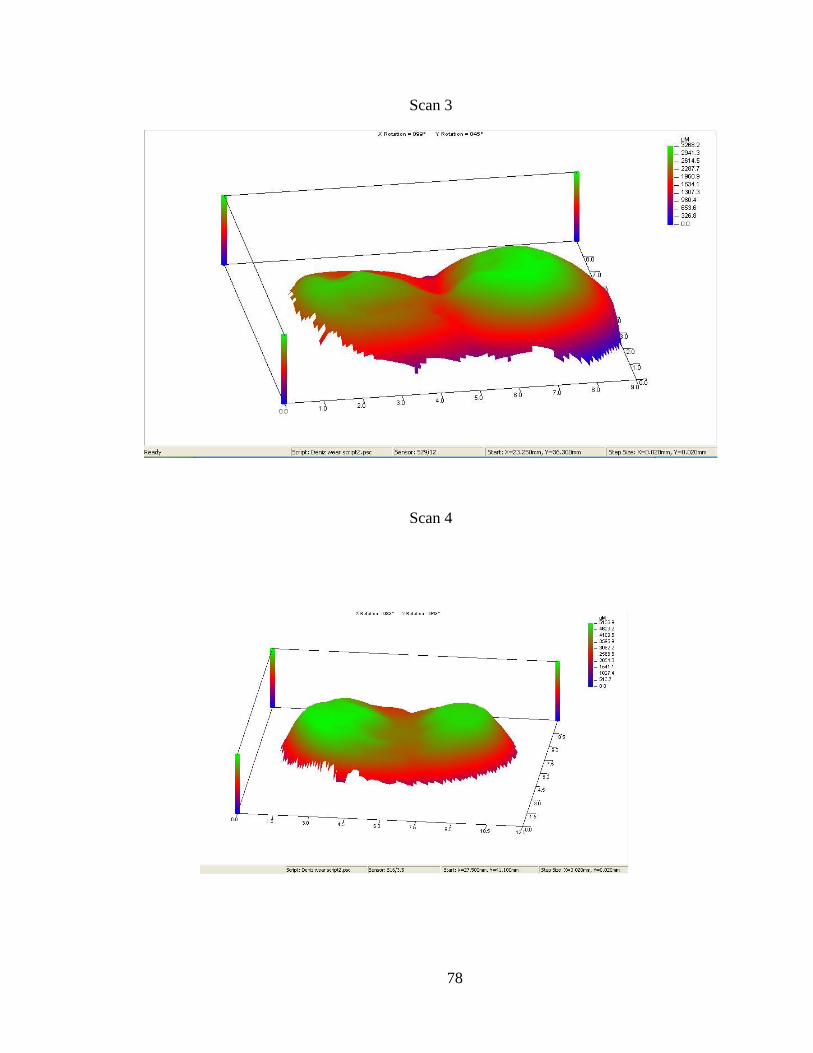
78
Scan 3
Scan 4
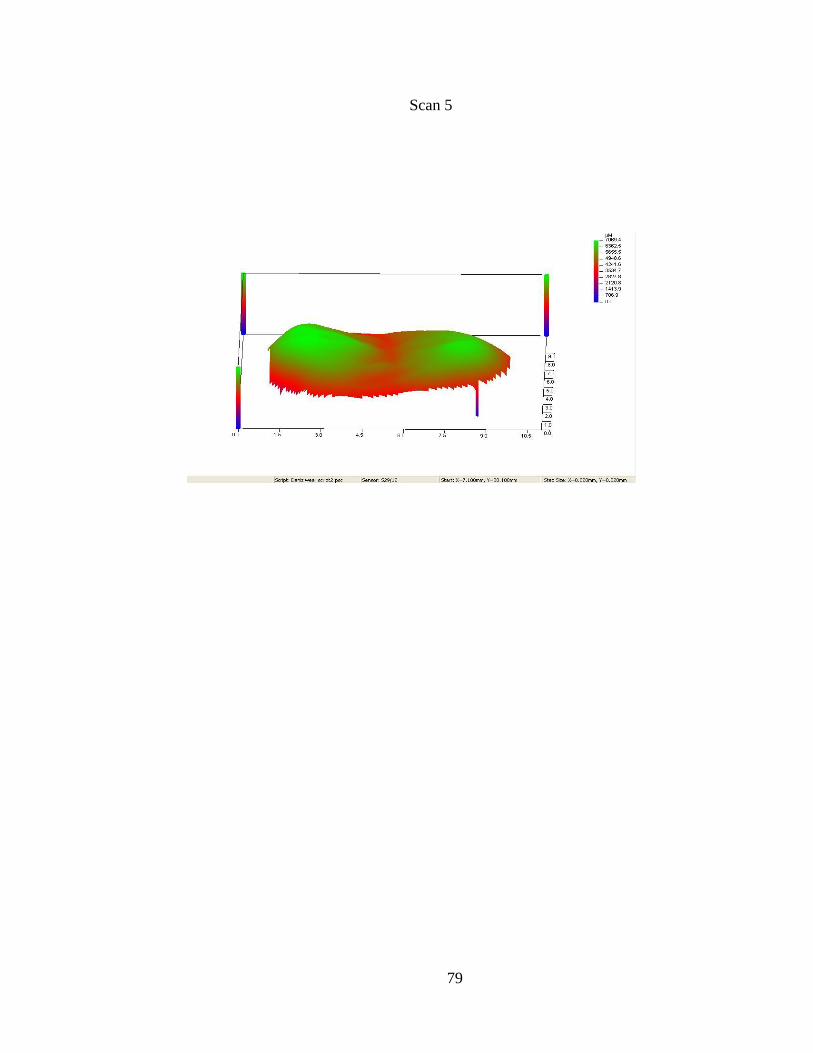
79
Scan 5

80
Appendix 4
In Vitro scans of Ceramic surfaces

81
Scan 1
Scan 2
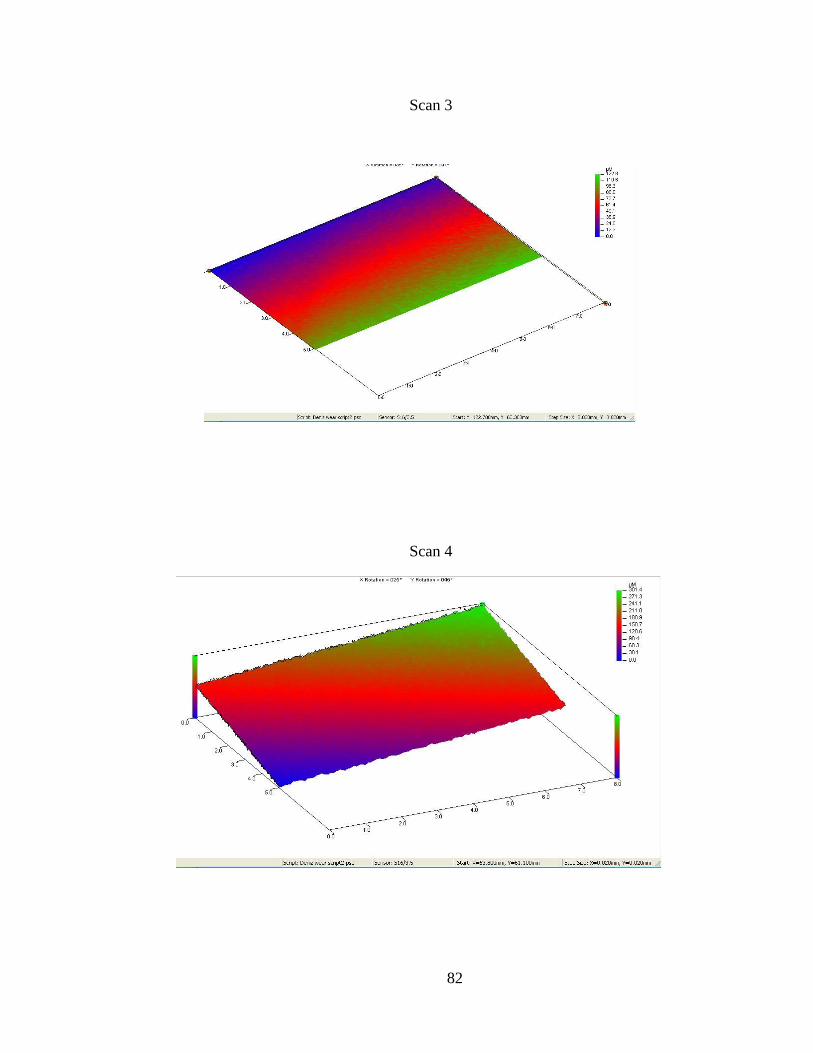
82
Scan 3
Scan 4
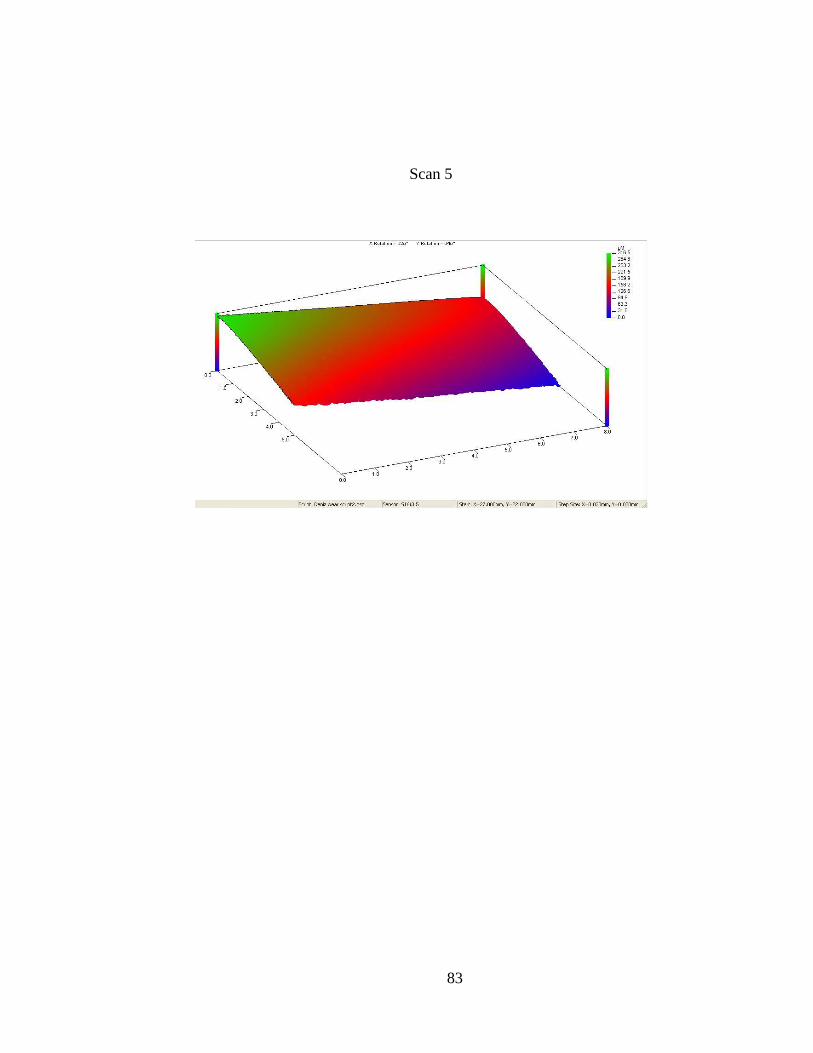
83
Scan 5

84
Appendix 5
Superimposed Images of Enamel Styli at Baseline & 200,000 cycles
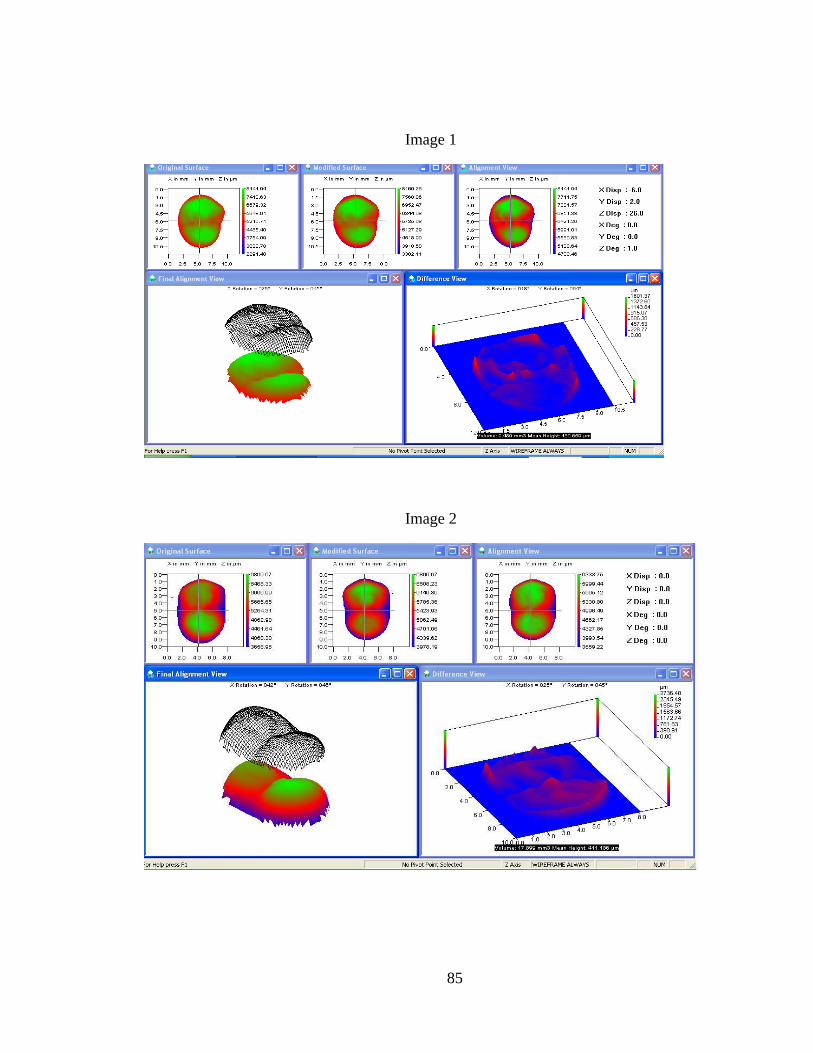
85
Image 1
Image 2
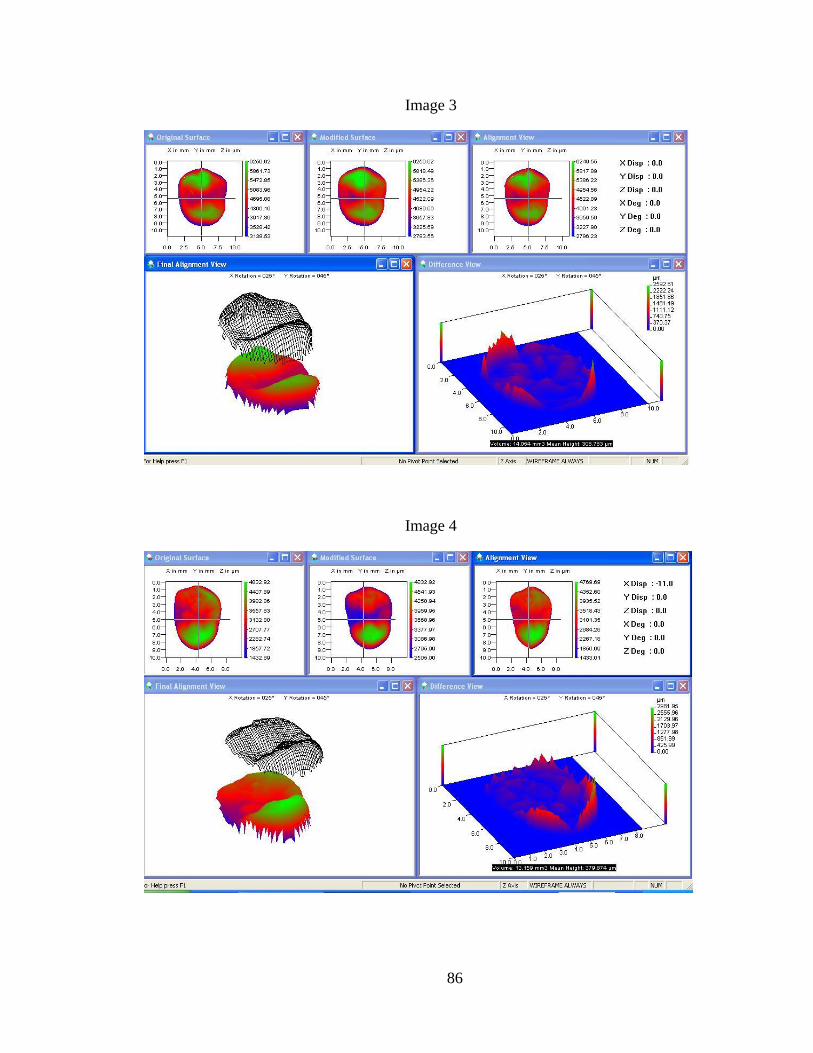
86
Image 3
Image 4
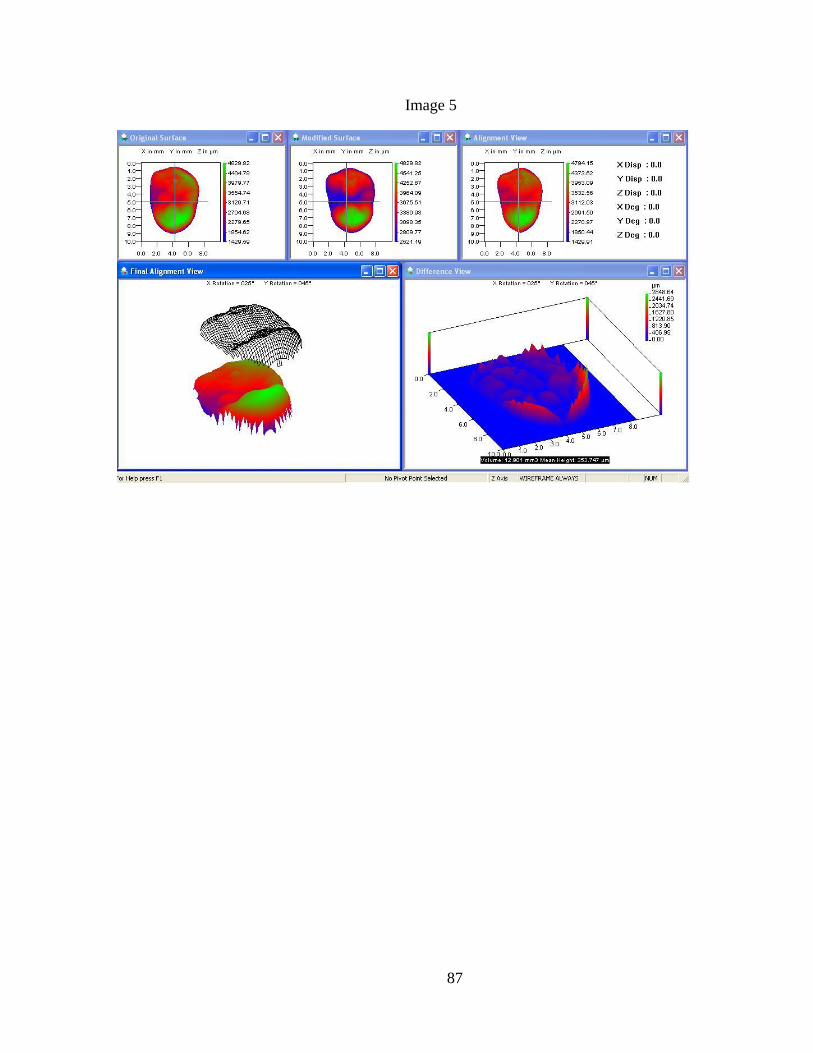
87
Image 5

88
Appendix 6
Superimposed Images of Ceramic surfaces at Baseline & 200,000 cycles
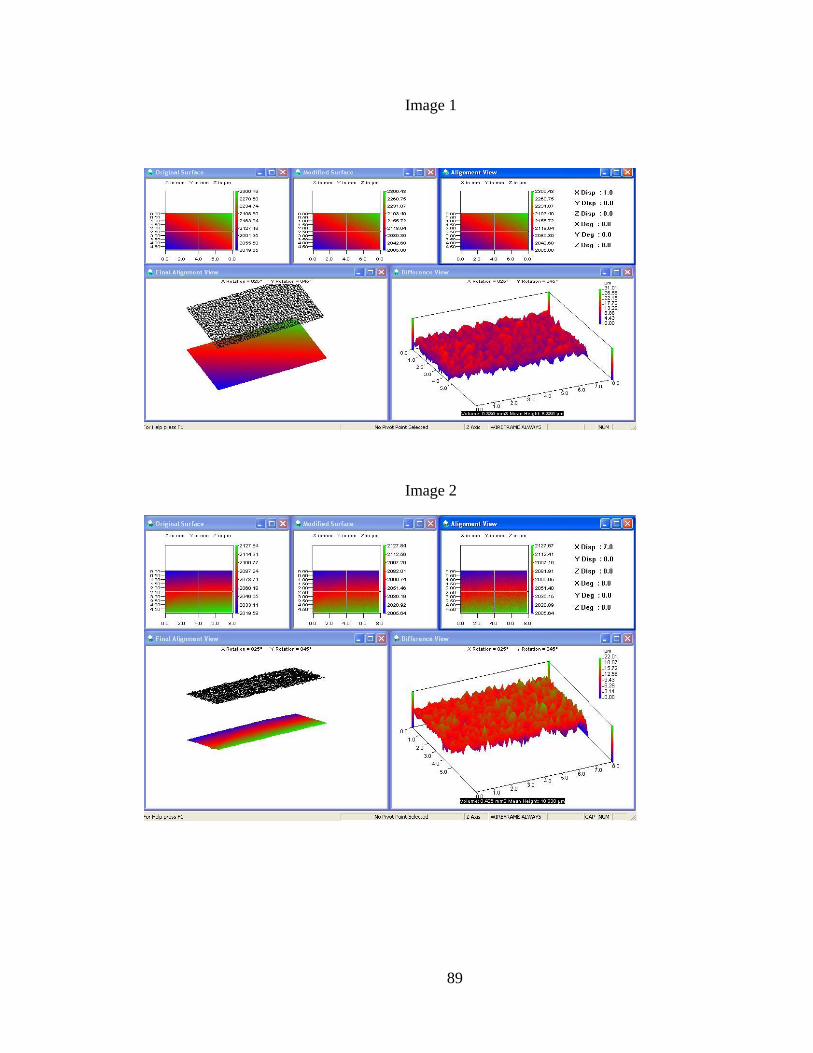
89
Image 1
Image 2

90
Image 3
Scan 4

91
Image 5