welcome to new employee orientation vcmc and … · welcome to new employee orientation vcmc and...
TRANSCRIPT

1
WelcometoNewEmployeeorientationVCMCandSPHJuly2016
ServingthecommunityofVenturaCounty

2
AboutVenturaCountyMedicalCenterandSantaPaulaHospital
VCMCisafullservice223bedAcuteCareHospitalincludinga43bedinpatientpsychiatricunit.WeareassociatedwithUCLAschoolofMedicineandhaveanationallyrecognizedFamilyMedicineResidencyprogramandhavebeen
educatingphysiciansheresince1928.VCMCresidentsaretrainedinbothinpatientandoutpatientmedicine,surgery,OB,ICU,ERandpediatrics.WehaveoneoftheoldestNICU’sinVenturaCountywhichwasopenedin1974.In2010,VCMCbecameaLevelIITraumaCenterforWestVenturaCountyprovidingcomprehensiveandcomplexcaretocriticallyinjuredpatientsinVenturaCounty.Notonlydowehavesomeofthetoptraumaphysicians,
surgeonsandnurses,wealsohaveawidevarietyofscreeningandpreventionprogramstodecreasetherisksofinjurywithinourcommunity.
SPHisafullservice49bedAcuteCareHospital.SPHisacampusofVCMCandservestheruralcommunitiesofSantaPaula,Fillmore,Piru,Saticoy,VenturaandOjai.SPHisavitalruralhealthcareaccesspointsituatedinthebeautifulhillsofSantaPaulaoverlookingthefertileSantaPaulaValley.Thesamehighqualityscreeningand
preventionprogramsarealsoavailableatourSantaPaulasite.
BothVCMCandSPHhavereceivedtheprestigiousBabyFriendlyHospitaldesignation.
OURMISSIONSTATEMENT
Providecomprehensive,responsible,compassionatehealthcareforourdiversecommunity,includingthosefacingbarriers,througheducation,anexceptionalworkforce,andforwardthinkingleadership.
Vision
ProviderofChoiceforIntegratedQualityHealthCare
PhilosophyofNursing
Webelieveinpatient/familyfocusedcare.Webelieveinpromotinghealthierlivinginourcommunity.Webelieveinacollaborative/multidisciplinaryapproachguardinganindividual’srighttoconfidentialityoftheirmedicalinformation.Webelieveinrespectingculturaldiversityandindividualityofeachpatient.Webelieveeach
professionalisaccountableandresponsiblefortheirindividualnursingjudgmentsandactions.
NewHospital
Ournewhospital,the“NorthTower,”iscurrentlyonscheduleformove-inattheendof2016.Theemergencydepartmentwillbethefirsttotransitionintothenewhospital.Priortotransitioningintothenewbuilding,there
willbescheduledtoursandcompetenciesforallstaff.

3
ImportantPhonenumbers
VCMC SPHVCMCMain 652-6000 Admitting/Paging 933-8632Admitting 652-6071 NursingOffice 933-8620AncillaryServices 652-6693 AncillaryServices 652-6693Lab 652-6037 PatientAdvocate 652-6691NursingOffice 652-6001 PatientRep 933-8605PatientAdvocate 652-6691 SocialServices 933-8637Paging 652-6075PalliativeCare 652-6093Payroll 677-5133Radiology 652-6080SocialServices 652-3280
CodesorRapidResponse
VCMC 7-6666 SPH 7-8666
UnitSpecific
Unit Manager ManagerPhone# UnitPhone#DOU CristinaMartinez 652-3254 7-6054ER SarahMelgoza 652-6658 7-6165ICU CristinaMartinez 652-3254 7-6195IPU JeffHawkins 652-6032 7-6729MedSurg-2west GracieDiaz 652-5704 7-6244 MedSurg-3west GracieDiaz 652-5704 7-6271 Peds KurtPeifer 652-5763 7-6224Surgery GregAnderson 652-6067 7-6237Telemetry CristinaMartinez 652-3254 7-6572NICU JennyBaarstad 652-6084 7-6088OB LisaMcPheeters 652-6704 7-6090L&D LisaMcPheeters 652-6704 7-6090SPHDOU CarrieHolt 933-8632 7-8689SPHER CarrieHolt 933-8632 7-8663SPHICU CarrieHolt 933-8632 7-8689SPHMedSurg BeaFrias 933-8603 7-8487SPHOB LisaMcPheeters 933-8620 7-8620SPHSurgery AzelaOconer 933-8637 7-8637

4
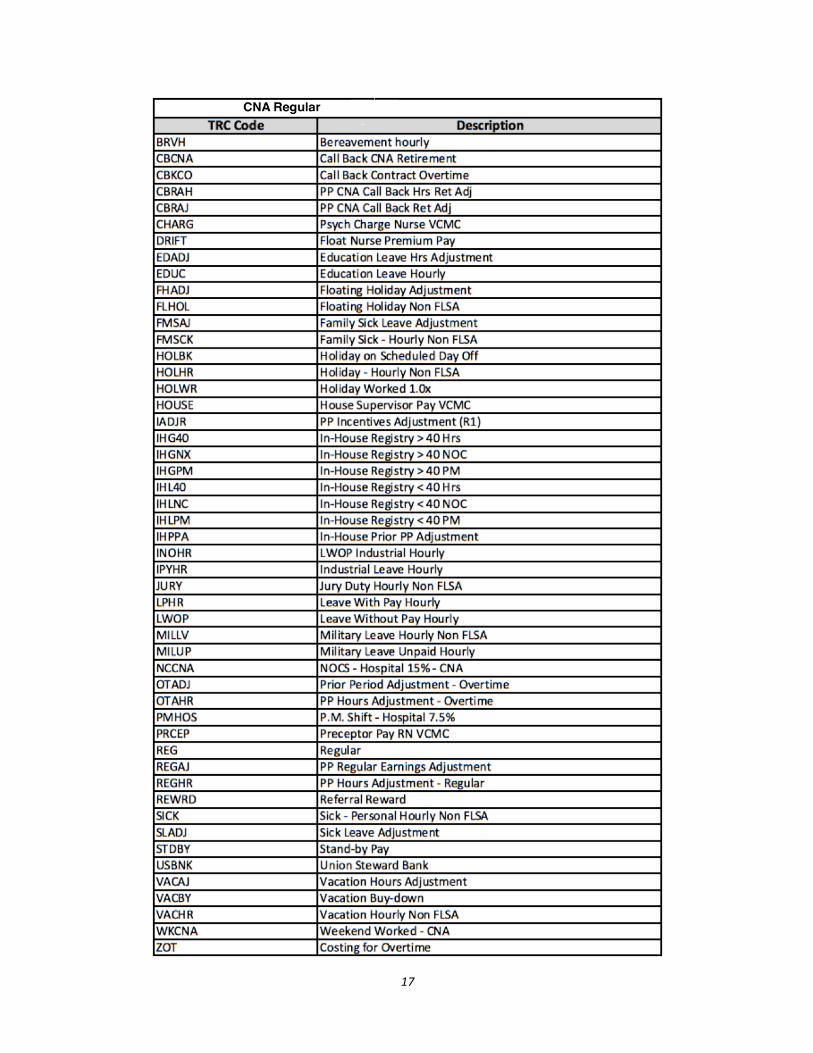
TimeCardsandCodes
Timecardsarecurrentlydonemanually.Yourunitpreceptorcanhelpyouwithyourfirsttimecard.Inthebackofthismanualyouwillfindactivitycodesspecifictoyourunitaswellastimereportingcodes(TRC)necessarytofillingoutyourtimecard(AppendixA).
Certificationpaywillautomaticallybeaddedtoyourtimecardonceyouhavefilledouttherequestform.Certificationsmustbejobrelated.Regularemployeescanbecompensated$0.813foreachcertificationuptofive,perdiememployeesuptothree.Youwillfindacopyofthisforminthebackofthismanual(AppendixB).
TimeAdjustmentForms–IfyoufindthatthereisanerroronyourtimecardpleasefillouttheTimeCardAdjustmentformandhaveitsignedbyyourmanager.Youwillfindacopyoftheforminthebackofthismanual.(AppendixC).
RegularemployeesarealsoeligibleforTextbookandTuitionReimbursement.Youwillfindinformationonthisinthebackofthismanual(AppendixD).
Competencies
Competenciesmaybedeliveredinavarietyofmethods.Competencieswillconsistofhospitalwidecompetenciesandunitspecificcompetencies.
TargetSolutionsisouronlinetrainingcenter.Youwillreceiveinstructionstosetthisuponceyouactivateyourcountyemail.
ReportinganInjury
Ifyouareinjuredonthejobpleasereporttheinjuryimmediatelytoyournursemanagerandthenursingsupervisor.Theywillassistyouinfillingouttheappropriatepaperworkandyoushouldseekmedicalcareasappropriate.
HIPAAPatientPrivacyandConfidentiality
Everypatientwithinoursystemhastherighttoexpectabsoluteconfidentialityoftheirmedicalrecordandhealthcareinformation.VCMC/SPHhasazerotoleranceforunauthorizedentryintoapatientsoryourownchart.Theonlyacceptablereasonstoaccessamedicalrecordareasfollows:youareateammemberprovidingcare,peerrevieworchartaudit,billingorinsurancepractices,partofalegal,regulatoryorlitigationmatter,reviewingaspartofastudentnursingassignment.Anyotherreasonsmustbeapprovedbyadministrationinwriting.IfyouwouldliketolookupyourownmedicalrecordpleasefillouttheappropriateforminMedicalRecordsandtheywillbehappytoassistyou.RefertoPolicy109.001

5
Professionalism
Weexpectallemployeestoconductthemselvesinaprofessionalmannerwhileatworkorwhenrepresentingouragency.
SocialMedia–theuseofpersonaldevicesshouldbelimitedtowork-relateduseonly.Pleasedonotdiscusspatientrelatedsituationsonsocialmediaandpleaserefrainfrompostingonsocialmediawhileatwork.Alsorefrainfrompostingphotographsofyourselfand/orcoworkersinthesettingoftheworkplace.Ifyouneedtomakeaphonecallorcheckyouremail,pleasedosoonyourbreak.
DressCode–PictureIDmustbewornabovethewaist.Pleasereporttoworkcleanandwellgroomedandfreeofstrongfragrances.Professionalattireshouldbeworn,nojeans.Ifyouareprovidingdirectpatientcare,pleasewearauniformandappropriatefootwear.Noartificialnailsandnaturalnailsmust¼”orshorterinlength.
HealthyWorkEnvironment
Wewantallemployeestoworkinanenvironmentthatissafe,empowering,supportiveandsatisfying.TheCountyofVenturahasaZeroTolerancepolicyforbullying,violent,ordisrespectfulbehaviorandweencourageyoutoreportanysuchbehaviortoyourdirectsupervisor.
Bullying–canbeanyverbal,non-verbalorphysicalbehaviorthatdiminishesanotherperson’sneeds,concerns,orcontributions.PleasedoyourpartinhelpinguscreateaHealthyWorkEnvironment.
SickCalls
Pleasedoyourpatientsandyourco-workersafavoranddon’tcometoworksick.Ifyouneedtocallinsick,youmustnotifyyourmanagerand/orthenursingsupervisoratleast2hourspriortothestartofyourshiftsothatyourshiftcanbecovered.Annualflushotsareofferedtoallemployees,freeofchargethroughEmployeeHealthServices.Ifyouchoosenottoreceivetheflushot,youwillwearamaskforeveryshiftduringfluseason,asrecommendedbytheCDCinordertoprotectco-workersandpatientsfromillness.
SafePatientHandlingandLifting
TheSafePatientHandlingandLiftingpolicyhasbeenimplementedtoimprovethesafetyofourpatientsandhealthcareworkforce.Itprovidesformethodsoracombinationofmethodstoreplacemanualliftingandtransferring.Staffwilluseappropriatehandlingandmobilitytechniques,mechanical,non-mechanical,andtransferaidsordevicesinaccordancewitheducation,training,andmanufacturer’sinstructionsandguidelines.Staffwillrefrainfrommanualliftingmethodsforsafepatienthandlingtasksandmobilityinallbutexceptionalorlifethreateningsituations.Policy100.099

6
“Liftteam”isdefinedasanyhospitalemployeesspecificallytrainedtohandlepatientlifts,repositioningandtransfersusingpatienttransfer,repositioningorliftingdevicesasappropriateforthespecificpatient.
PalliativeCare
• PalliativeCareTeamincludes:Physician,Nurses,aPsychologist,andaChaplainwhosegoalistoimprovequalityoflifeforboththepatientandthefamily.
o PhysicalWell-Beingo PsychologicalWell-Beingo SocialWell-Beingo SpiritualWell-Being
• PalliativeCareisappropriateatanyageandatanystageinaseriousillness,andcanbeprovidedtogetherwithcurativetreatment.
BloodTransfusion
• RNandanotherlicensedstaff(RN,LVNorPhysician)verifybloodagainstunittagandagainstpatientbandsatbedside
o Nameo MRNo Bloodbando ABO/Rho Unit#o Verifyexpirationdateandtime
• Bothmustsignunittagandco-signinCerner• Tagmustremainattachedtoblooduntilcompletion• Verifyingpersonmustremainatbedsideuntiltransfusionisconnectedtopatientandinfusionisstarted• Starttransfusionslow(75ml/hr)andincreasetoprescribedrateafter15minutesifpatienttoleratingwell.• Bloodtransfusionmustbecompletedwithin4hours• Tubinglifefortransfusionis4hours• Vitalsigns
o Upto30minutespriortotransfusiono 15minutesafterstartingtransfusiono Atcompletionoftransfusion
• WatchforsignsoftransfusionreactionincludingTRALI–mostcommonisfevero Stoptransfusionimmediatelyo StartNormalSalinetokeepveinopeno NotifyPhysiciano ReturnBloodtothebloodblankwithtubing,completedbloodtransfusionreactionform,andurine
specimeno MonitorVSo Enterlaborderfor“TransfusionReactionInitial”

7
o DocumentinCerner(note)o CompleteNotificationForm
• RefertoPolicyE.1
OneLegacy
• OneLegacyisthenon-profitorganizationdedicatedtosavinglivesthroughorgan,eyeandtissuedonationintheseven-countygreaterLosAngelesarea.
• AsrequiredbyCMS,VCMCandSPHwillreferALLDEATHStotheappropriateOrganandtissueProcurementOrganProcurementOrganization,whichisOneLegacy.
• Donationshouldnotbediscussedwithfamily,insteadanypotentialdeath,imminentdeathoractualdeathshouldbereferredtoOneLegacyat800-338-6112.Theywillreviewthecaseanddetermineifandwhentoapproachfamily.
• RefertoPolicy100.048
QualityAssessmentandPerformanceImprovement
• HospitalAcquiredinfections(HAI)o Greatestprevention–WashyourHands
• CatheterAssociatedUrinaryTractInfections(CAUTI)o Assesseveryshiftfornecessity,removeassoonaspossibleo Bedsidebladderscanningo FollowUrinaryCatheterAssessment,MaintenanceandBestPracticesBundleo FollowNurse-DrivenFoleyRemovalProtocolo Policy1.3
• CentralLineAssociatedBloodStreamInfections(CLABSI)o Assesseveryshiftfornecessity,removeassoonaspossibleo CentralLineInsertionProcess(CLIP)formoneverycentrallineinsertionattempto PolicyE.10,E.9,E.5o FollowCVCCareandMaintenanceBestPracticeBundleo Capsandtubingchangedevery96hoursorafterblooddrawsortransfusionso Dressingchangewithin24hoursofinsertionandatleastevery7dayso AllportsofCentralLinesshouldbecoveredwithone-timeuseCurosProtectivePortandtip
protectors.Theseshouldbechangedanytimetheyareremovedforanyreasonorevery7days• SurgicalSiteInfections(SSIs)
o Pre-operativeChlorhexidineGluconatebathingo Smokingcessationo Glucosecontrolpre,postandintraoperativeo ObservanceofAsepticTechnique
• NotificationandIncidentReportingo ReportallsafetyrelatedeventsandsentineleventstoManager/NursingSupervisoro SubmitElectronicNotificationFormfoundPolicies&Proceduresandicononeverydesktop

8
• PatientExperiences–NursingRelatedSurvey o Listencarefully,communicatewithcourtesyandrespecto Answercallbellspromptlyandattendtopatientsneedso Makeeveryattempttoprovideappropriatepaincontrolo Educateyourpatientsonnewmedications,diagnosis,anddischargeinstructionso Rememberpatientsneedaquietenvironment
• ComplaintsandGrievanceso VCMC/SPHgoalisearlycomplaintresolution.o Anystaffmembercanreportthepatientcomplainttomanagementorthepatientadvocateto
expediteresolutiono Anycomplaintthatcannotberesolvedimmediatelybecomesagrievanceandwillbehandedoff
tothepatientadvocatewhowillformalizetheprocess
VCMC/SPHCoreMeasures2016
• HospitalBasedInpatientPsychiatricCareReportingMeasureso HBIPS-1Admissionscreeningforviolencerisk,substanceuse,psychologicaltraumahistoryand
patientstrengthsiscompletedo HBIPS-2Hoursofphysicalrestraintuseo HBIPS-3Hoursofseclusionuseo HBIPS-5Patientsdischargedonmultipleantipsychoticmedicationswithappropriatejustification
• HospitalInpatientQualityReportingMeasureso Sepsis(SEP)
§ SEP-1EarlyManagementBundle(63dataelements)inadults18yearsandolderwithadiagnosisofsepsis,severesepsisorsepticshock
o AcuteMyocardialInfarction(AMI)§ AMI-7aFibrinolytictherapyreceivedwithin30minutesofhospitalarrival
o Stroke(STK)§ STK-1VTEprophylaxis§ STK-4Thrombolytictherapy§ STK-6Dischargedonastatinmedication§ STK-8Strokeeducation
o VenousThrombusEmbolism(VTE)§ VTE-1VTEprophylaxis§ VTE-2ICUVTE § VTE-3VTEpatientswithanticoagulationoverlaptherapy§ VTE-5VTEwarfarintherapydischargeinstructions§ VTE-6HospitalacquiredpotentiallypreventableVTE
o EmergencyDepartment(ED)§ ED-1MediantimefromEDarrivaltoEDdepartureforadmittedEDpatients§ ED-2AdmitdecisiontimetoEDdeparturetimeforadmittedpatients
o Immunization(IMM)§ IMM-2Screenallinpatientsforinfluenzaimmunizationstatus

9
o PerinatalCare(PC)§ PC-01Numberofpatientswithelectivedeliverypriorto39weeks
Stroke
• Stroke
Patientswithsuddenstroke-likesymptoms,andlastknownwelltimeiswithin6hoursofpresentingintheEmergencydepartmentorinpatients,willbetriagedandconsideredforeligibilityintheadministrationofIVt-PA,standardizedtreatmentfortransientischemicattack,ischemic,orhemorrhagicstroke,neurosurgicalservices,admissionasanobservationorin-patienttoadesignatedunit,and/orinter-hospitaltransferforneuro-interventionalservices.Physiciansutilize/accessneurologicalexpertisetoexpeditecareofthestrokepatient.Neurologicalexpertise(asdefinedbyVCMC/SPHmedicalpolicies)isavailablewithin15minutes,eitherbytelephoneand/ortelemedicine.Amultidisciplinaryapproachisintegratedinthestrokesystemtopromotethoroughcommunicationanddecisionmakingforbestoutcomes.RefertohandoutsinAppendixE
• SwallowScreen
Thenurse,competentinswallowscreening,willaccuratelyidentifypotentialpatientsatriskforaspirationandperforma“Threestepswallowscreen”.First,thepatients’presentationandpastmedicalhistorywillbereviewedtoidentifythepredispositionforaspiration.Second,asimple3ouncewatertestwillbeconductedandthenursewillproceedtothethirdstepifthepatienttolerates3ouncesofwater.Third,3sipsofwaterwillbegivenandadeterminationwillbemadeforapassorfailstatus.The“Threestepscreenwillbeconductedtodetermineifpatientsareatriskforclinicallysignificantaspirationorrequireaspeechreferralforadefinitiveswallowevaluation.RefertohandoutsinAppendixE
MedicationSafety
RefertohandoutsprovidedbyTorriBoghossian,MedicationSafetyOfficer
Glucostabilizer
RefertohandoutsprovidedbyClaireRithner,DiabeticEducator
Restraints
Restraintisanymanualmethod,physicalormechanicaldevice,materialorequipmentthatimmobilizesorreducestheabilityofapatienttomovehisorherarms,legs,bodyorheadfreely.Physicalrestraintsaretheonlytypeofrestraintsusedhere,VCMCdoesnotusemedicationrestraints.
• Typeso Non-violent–formanagementofbehaviorthatdisruptsorinterfereswiththepatients’abilitytoheal

10
o Violent–forthemanagementofviolentorself-destructivebehaviorthatjeopardizestheimmediatephysicalsafetyofthepatient,staff,orothers.
o Seclusion–involuntaryconfinement,usedonlyforthemanagementofviolentorself-destructivebehavior
• Alwaysattemptalternativemethodsfirsto Diversiono FamilyInvolvemento Sitteratbedside
• Whenrestraintsarenecessary,chooseleastrestrictive,optionsincludeo Handmittso Vesto Limbrestraints
• Ordersarerequiredassoonaspossibleforallrestraintso Emergencyinitiationo TemporaryPhysicalHoldo ViolentorSeclusion–
§ agebaseddurationorsoonerifable§ In-personre-orderifneeded>24hours
o Non-violent§ Re-ordereachcalendarday
• Properapplicationo Useonlyhospitalapprovedrestraintso UseQuickreleaseslipknotso Assuredeviceislooseenoughtoprovideadequatecirculationandbodyalignment
• Documentation• PlanofCare• RefertoPolicy100.075
CrashCart
• Crashcartshouldbekeptlockedatalltimeswhennotinuse.• Everynurseshouldbecomefamiliarwiththecrashcartanditscontents.• Crashcartshouldbecheckedasperunitpolicy.• RefertoPolicy100.055
CodeBlue&RapidResponse
Anycodeshouldbecalledusingthefollowingemergencynumbers
• VCMC7-6666• SPH7-8666
11
CodeBlue–CardiacArrest(alongwithcallingtheabovenumber,thein-roomcodebuttonshouldbeactivated,whereavailable).Refertopolicy100.055
RapidResponse–Calledforanypatientwhoexhibitshemodynamic,respiratoryorneurologicalinstability/deteriorationorwhenthenurseisotherwiseconcernedaboutapatientandisunabletoreachphysician.Refertopolicy100.086
Sepsis
Sepsisisanewcoremeasureandeveryadultpatientmusthaveadocumentedscreen–• Intriage• Uponadmission• Atleastevery12hours• Anychangeorworseningofconditionoranytimeyouareconcerned
UnderstandingSepsis-Firstyoueitherhaveaninfectionorsomesortofphysiologicaltraumaorevent.• SIRS–systemicinflammatoryresponsesyndrome.Canbecausedbyinfectionorotherinsult.• Sepsis–systemicresponsetoinfection,youhavetohaveaninfectiontohavesepsis.Thatwould
beSIRSplusdocumentedorpresumedinfection.• SevereSepsis–sepsisplussepsis-inducedorgandysfunctionortissuehypo-perfusion.• SepticShock-severesepsisplushypotensionnotreversedwithfluidresuscitation.
WhatisaPositiveSepsisScreen?• Apatientscreenspositiveforsepsisiftheymeet2ormoreofthecriteriafromQuestion1AND1or
moreofthecriteriafromQuestion2oftheSepsisClock(AppendixF)• IfbothcriteriaaremetthenaLactatemustbedrawn,followSepsisProtocol(AppendixG)
WhodrawstheLactate?• Drawingalactateisasharedresponsibility• RT,RN,Physician,phlebotomist• MUSTberunbyRT,DONOTsendtolab• MUSTbeplacedonice,MUSTbetoanalyzerandprocessedwithin15minutes
LactateResults• Lactate<2mmol/L–Assessforseveresepsisasnotedonsepsisclock• Lactate>2but<4mmol/L(2.1to3.9)–RNtonotifythephysicianofresultsandcontinuewithsepsisclock• Lactate>4mmol/L–
o EmergencyDepartment-RN(ordelegate)callsaCODESEPSIS,notifiesphysicianstatandcontinueswithSepsisClock
o Inpatient-RN(ordelegate)overheadpagesCODESEPSISandnotifiesphysicianandcontinueswithSepsisClock
SepsisCare� Obtainurineculture(beforeantibioticsifpossible)� TwosetofBloodculturesbeforeantibiotics� Antibioticswithin3hourofseveresepsis� A30ml/kgcrystalloidinfusionforhypotensionand/orLactate>4.Documentfluidstartandcompletion
time.

12
� Norepinephrineifhypotensiondoesnotrespondtoinitialfluidresuscitationwithin1hour� Repeatlactatewithin4hoursofseveresepsisifinitiallactate>2
RefertoPolicy100.201
WoundCare
• GoalistoPreventpressureulcersinsteadoftreat• RiskAssessmentusingtheBradenScoring
o Score<18callsforearlyinterventiono AtleastQ2hrturnso Offloading
• Accuratedocumentationandpicturesuponadmission• Documentation
o Shiftassessmento Turnso Ofwoundifpresento Notificationformfilledoutandmanagernotified
• PlanofCareenteredasappropriate• Appropriatebedorbedsurface• RefertoAppendixH
Age&CulturalSpecificPatientCenteredCare
• CulturalCompetencyo WevaluethediversepopulationthatweserveinVenturaCounty.Allpatientsandlovedones
mustbetreatedwithdignity,respectandwithculturalsensitivity.Refertopolicy100.053• AgeSpecificgroupsforphysiologicalandpsychologicalcare.Refertopolicy108.017
o Neonate–first4weeksoflifeo Infants–upto1yearo Toddler–1-3yearso Preschool–3-5yearso SchoolAge–6-12yearso Adolescent–13-18yearso YoungAdult–19-44yearso Adult/MiddleAge–45-65yearso OlderAdults/Geriatrics–over65years
AddressingPain&Sedation
• Painmustbedocumentedwitheverysetofvitalsigns.Painisdocumentedbeforeand30minutesafteradministrationofpainmedications.

13
• Sedationlevelmustbedocumentedanytimeapatientisonmedicationsforsedationandorwhenthatmedicationistitrated.
• Treatmentofpainandsedationmayvarydependinguponage,sizeandpatients’individualperceptionofpain.
• PainScalesusedatVCMC/SPH(AppendixI)o VisualAnaloguePainScale–askpatienttoratepainonscaleof0-10o FacesRatingPainScale–askpatienttoratepainonscaleof0-10usingpicturesoffaceso VenturaObservationalPainScale(VOPS)–ascoringsystemusedtoratepaininthenon-verbal
adultpatiento Face,Legs,Arms,CryandConsolability(FLACC)–ascoringsystemusedtomeasurepainin
infantsandchildrenwhoareunabletocommunicatetheirpaino NeonatalPain,AgitationandSedationScale(N-PASS)–ascoringsystemusedtodeterminepain,
agitationandsedationleveloftheneonate• AgitationScale(AppendixJ)
o RichmondAgitationandSedationScale(RASS)–ascoringsystemusedtomeasureagitationorsedationlevelofapatient
o NeonatalPain,AgitationandSedationScale(N-PASS)–ascoringsystemusedtodeterminepain,agitationandsedationleveloftheneonate
• RefertoPolicy100.076
InterpretationServices
• VCMC/SPHhasavailableaninterpretationserviceformanydifferentlanguages.Thesedevicesarelocatedineachnursingstation,onthe2ndand5thfloorsofAFMCbuilding,andthreemoredevicesarelocatedinAncillaryservicesandareavailablebycallingDebbieHillinAncillaryServices.
FallPrevention
• FallPreventionProgramo VCMCTraumaincollaborationwithEMSidentifypre-hospitalfallso ElectronicFallFormisfilledout,ahomereferralforsafetycheck,etc.ismadeasappropriateo Fallpreventioneducationalmaterialsaredeliveredtopatientupondischargeo Ifpatientisadmittedareferraltosocialservicesismadeandappropriatereferralsaremade
• InhospitalFallPreventiono Goal–Reducefallsbyidentifypatientsatriskandinitiateinterventionsthatpreventaperson
fromfallingo Fallisdefinedasalossofuprightpositionthatresultsinlandingonthefloor,groundoranobject
offurnitureorsuddenuncontrolled,unintentional,non-purposeful,downwarddisplacementofthebodytothefloor.
o Completefallassessmentonadmissionandevery12hours,atchangeofcondition,attransfertoanewunitorafterafall.
§ MorseFallScale(Adult)(AppendixK)

14
§ HumptyDumptyFallScale(Pediatric)(AppendixL)o Highrisk>45onMorseFallScale
§ Yellowwristband§ Re-assessenvironmentandre-orientpatientasneeded§ Assuresupervisionandassistance§ Notifyphysician(iffalloccurs)§ Notificationform(iffalloccurs)
o Educatepatient&familyonfallriskreduction–callbutton,footwear,etc.o Bedsinlowpositiono Answercalllightspromptly
• RefertopoliciesA.24and107
SBAR
• Therecommendedmodeofcommunicationbetweenhealthcareproviderstodiscusspatients,patientneedsandpatientrelatedeventsatVCMC/SPH
• WhatisSBARo S=Situation–Whatisgoingonwiththepatient?Aconcisestatementoftheproblem.o B=Background–Whatistheclinicalbackgroundinformationthatispertinenttothesituation?o A=Assessment–Whatdidyoufind?Analysisandconsiderationsofoptions.o R=Recommendation–Whatactionorrecommendationisneededtocorrectthe
problem?Whatdoyouwanttohappenforthispatient?• WhySBAR
o Asimplemethodtohelpstandardizecommunicationo SBARallowsallpartiestohavecommonexpectations:
§ Whatisgoingtobecommunicated§ Howthecommunicationisstructured?§ Requiredelements
o Focusesontheproblem,notthepeopleo TheformatofSBARallowsprofessionalstodelivershort,organizedandpredictableinformation
inaneasytounderstandformat.• ImplementingSBARforpatienthandoffs
o Handoffsincludeverbalcommunicationo Face-to-faceinteractiono Opportunitytoaskandanswerquestionso Documentation

15
APPENDIXA-ActivityCodes–UnitSpecific
VCMC
6010 Intensive Care - ICU 6020 Definitive Observation - DOU 6050 PICU 6070 NICU 6171 Med Surg - 3 North 6173 Med Surg - 3 West 6174 Med Surg - 4 North (OB) 6177 Med Surg - 2W 6290 Pediatric Acute 6340 Psychiatric Acute - IPU 6380 Obstetrics Acute - OB 6381 Obstetrics Acute - OB 6530 Nursery Acute - TCN 7010 Emergency Services - ER 7400 Labor and Delivery - L&D 7421 Surgery (General) - OR 7425 Surgery - Pre-Op 7426 Surgery - GI Lab 7427 Surgery - PACU
SPH
6011 Intensive Care - ICU 6131 Definitive Observation - DOU 6180 Med Surg - M/S 6385 Obstetrics Acute - OB 6535 Nursery Acute - TCN 7015 Emergency Services - ER 7405 Labor and Delivery - L&D 7423 Surgery - Pre-Op 7424 Surgery - GI Lab 7428 Surgery - PACU 7429 Surgery (General) - OR 7435 Surgery - SDS

16
17

18
APPENDIXB–PerDiem

19
APPENDIXB–regularfulltime

20
APPENDIXC

21
APPENDIXD
Textbook & Tuition Reimbursement
All Regular full and part time employees are eligible for textbook & tuition reimbursement for job related courses, workshops and seminars. Courses must be taken on employees own time with proof of successful completion.
How much?
x $600 per fiscal year for lower division courses x $900 per fiscal year for upper division or graduate coursework x $900 Nurse certification testing fee reimbursement x $2000 RN to BSN coursework with pre-approval (40 employee slots available)
Did you know...
x All courses need pre-approval for guaranteed reimbursement (Pink T&T sheet) x Per our contract, "Reimbursement will be made to the employee within 2 weeks after the grade cards and
receipts have been received by the Agency head" x New employees must work 1040 hours to be eligible x Part time employees will be reimbursed on a pro rata basis
What's the Process?
Before Class
x Prior to class fill out the pink "Textbook & Tuition Reimbursement Application" and turn it in to your manager for signature. It will be sent to Nursing Administration for processing.
x A copy will be returned to you with instructions on how to fill out the "Textbook & Tuition Claim" form.
After Class
x Fill out the "Textbook & Tuition Claim" form x Attach proof of payment AND proof of satisfactory completion x Sign the claim form and return it to your manager for their signature. The form then goes to Nursing
Administration x Reimbursement check will be mailed to your home address

22
APPENDIXE

23

24

25

26

27

28

29

30

31

32

33

34
APPENDIXF

35
APPENDIXG

36

37
SIRS SEPSIS SEVERE SEPSIS SEPTIC SHOCK
DEFINITIONS
SystemicInflammatoryRespons
eSyndrome(SIRS)Musthaveatleast2ofthefollowing:• Temp<
96.8F• Temp>
100.4• HR>90• RR>20• WBC<
4,000• WBC>
12,000• Bands>
10%
SIRS
+ Infection
/ Suspect
ed Infection
16% Mortality
Rate
SIRS +
Infection/ Suspected Infection
+ Organ Dysfunction
Musthaveatleast1ofthefollowing:• Lactate>2• SBP<90• SBPdecrease>40mmHgfrombaseline**• MAP<65• Bilirubin>2*• Creatinine>2*• Platelets<100*• INR>1.5*• PTT>60seconds*• UO<0.5ml/kg/hourfor2hours*• Respiratoryfailure(requiringCPAP/BIPAP)*
*newforpatient**ReasonforrequiredfromMD>20%MortalityRate
SIRS +
Infection/ Suspected Infection
+ Organ Dysfunction
+ LA > 4
and/or
Persistent Hypotension In The 1 Hour After 30ml/Kg IVF Bolus Completion
What is hypotension?
• SBP<90• SBPdecreaseofmorethan40mmHGfrompatientsbaseline
• MAP<65>46%MortalityRate
TO D
O L
IST
Recognize & Assess for infection
Order & draw lactate within 30 minutes of recognition
w/in 3 hours of meeting severe sepsis: 1. Initial Lactate level 2. Blood cultures before antibiotics 3. Broad Spectrum Antibiotics
o If C-diff suspected then ORAL Vancomycin to be started w/in 3hrs.
4. *IF initial hypotension START LR/NS 30ml/kg bolus (rate no less than 126ml/hr)
w/in 4 hours of initial lactate: 1. Repeat Lactate Level
o Only required if initial LA>2 (Cerner automatically orders)
2. IF patient received bolus: assess & document BP x2 w/in hour bolus completes. *done to assess if patient is in Septic Shock
w/in 3 hours of meeting septic shock: 1. Initial Lactate level & repeat w/in 4hr
when ≥ 4 2. Blood cultures before antibiotics start 3. Broad Spectrum Antibiotics o If C-diff suspected then ORAL
Vancomycin to be started w/in 3hrs. 4. START LR or NS 30ml/kg. Assess &
document BPx2. w/in 6 hours of meeting septic shock 1. Start Vasopressors within 6 hours post IVF
bolus completion for persistent hypotension 2. MD/PA/NP Need to document bolus status &
tissue perfusion assessment from either option below: a. Focus assessment doc by MD/PA/NP:
1.All 4 Vitals: HR, B/P, Temp & RR 2.Cardiopulmonary assessment 3.Capillary refill 4.Skin color exam
b. MD/PA/NP to document on 2 options below: 1.CVP 2.ScvO2 or SvO2 3.Bedside CV ultrasound 4.Passive leg raise OR Fluid Challenge

38
APPENDIXH

39

40

41

42

43

44

45

46

47

48

49

50
APPENDIXI–PainScales
VisualAnalogue&Faces
FLACC–Face,Legs,Activity,CryandConsolability

51
VOPS–VenturaObservationalPainScale

52
N-PASSNeonatalPain,AgitationandSedationScale

53
APPENDIXJ–AgitationScale

54
APPENDIXK
MorseFallScale

55
APPENDIXL
HumptyDumptyFallScale
Parameter Criteria ScoreAge Lessthan3yearsold 4
3tolessthan7yearsold 37tolessthan13yearsold 213yearsandabove 1
Gender Male 2Female 1
Diagnosis NeurologicalDiagnosis 4Alterationsinoxygenation(respiratorydiagnosis,dehydration,anemia,Anorexia,syncope,dizziness,etc.)
3
Psych/BehavioralDisorders 2OtherDiagnosis 1
CognitiveImpairments Notawareoflimitations 3Forgetslimitations 2Orientedtoownability 1
EnvironmentalFactors Historyoffallsorinfant–toddlerplacesinAdultbed 4Patientusesassistivedevicesorinfant–toddlerincriborfurniture/lighting
3
Patientplacedinbed 2Outpatientarea 1
ResponsetoSurgery/Sedation/Anesthesia
Within24hours 3Within48hours 2Morethan48hours/None 1
MedicationUsage Multipleusageof:Sedatives,hypnotics,barbiturates,phenothiazines,Antidepressants,laxatives,diuretics,narcotics
3
Oneofthemedslistedabove 2Othermedications/None 1

56

57

58

59