welcome to ward e53 - northumbria university welcome to ward e53 ward e53 is primarily a...
TRANSCRIPT

1
Ward E53
Student Nurse Portfolio of Learning Opportunities.
R.L. Layfield (February 2007)
2
WELCOME TO WARD E53
Ward E53 is primarily a gastroenterology medical ward, but occasionally takes
patients from other specialities (e.g. thoracic patients, care of the elderly etc). E53 is a
mixed sex ward, comprising of four, six bedded bays and six side wards (30 beds in
total.) Two the side rooms have special ventilation for barrier nursing patients. We
receive the majority of our patients from the admission units, but we also admit some
from home, clinics or accident and emergency department. The age range of our
patients is sixteen years onwards.
Sunderland City Hospitals has a restricted visiting policy. The daily visiting hours are
as follows:-
2pm – 5pm
6pm – 8pm
Visitors may be also asked to leave the bay for doctor’s rounds and in order to carry
out patient’s personal care requirements. The hospital now promotes a protected
mealtime iniative, which enables the patient to enjoy their meal free from
interruptions.
Due to the nature of ward E53, experience available for students is wide and varied.
We very much hope that you will enjoy your placement with us and we will as a team,
do our utmost to support you during your placement. We will endeavour to help you
develop your knowledge in the understanding of various gastro. conditions as well as
enhancing your clinical skills and where applicable your management skills.

3
A series of competencies will provide you with direction during your placement and
will facilitate your learning. Your mentor will guide you through this process and
provide you with support, advice and expert knowledge. We would be grateful if you
could complete our evaluation form upon completion of your placement.
WARD PHILOSOPHY
The philosophy of care is a statement of professional service offered to patients, and
their families/carers, and hence forms the basis for partnership in care.
Within General Internal Medicine we aim to provide individualised care in a dignified
and confidential manner identifying physical, social and psychological needs of
patients and their families/carers. The patients right to privacy will be respected and
every effort will be made to maintain this.
We will do this by working in a safe and secure environment where care needs are
assessed, planned and implemented in partnership with all concerned – whilst at the
same time respecting patients rights as an individual, acknowledging individual
beliefs and values, and supporting individual choices made.
Patients will be cared for by a skilled team of professional staff, who are competent in
their roles, are approachable, and able to provide information, support and advice.

4
By using evidence based practice we aim to offer the highest standard of care in an
environment that is conducive to learning where we support learners to acquire the
necessary skills and competencies to carry out high quality patient care.
Teaching and education for staff, patients and carers is an integral part of care
delivery in all clinical areas in General Internal Medicine. Our aim is to help patients
attain, maintain and restore health via problem solving, goal/objective setting,
leadership and decision making.
Discharge planning will commence on admission where appropriate, ongoing care
and support arranged for patients requiring terminal care, and all care will be co-
ordinated and facilitated by the patients Named Nurse.
We value and welcome patients and relatives views and comments, which helps us to
monitor satisfaction of the service that we provide.
WARD LAYOUT AND FACILITIES
Ward E53 has 30 beds arranged in four six bedded bays and six single side rooms.
The four bays and side rooms are serviced with piped oxygen and wall suction. Side
room 5 and 6 have special ventilation systems for barrier nursing as well as ensuite
washing facilities. E53 is a mixed sex ward: the six bedded bays are allocated
male/female as required. There are clearly marked male and female toilet and shower
rooms on the ward allowing for the privacy of sexes. There are also two bathrooms on
5
the ward. Each bed has the patient line available. We also have a quiet relative’s room
outside of side room 4.
Each day both a vendor delivering newspapers and magazines and the WRVS trolley
shop visit the ward.
Patient education is encouraged and there are fully stocked information racks as well
as having poster displays.
E53 actively encourages the Trusts No Smoking policy.
THE DIRECTORATE
E53 comes under the directorate of General Internal Medicine.
DIRECTORATE STAFF
Clinical Director
Business Manager Mr Tom Dodds
Matron Mrs G Wright
Practice Development Nurse Miss L Downey
MEDICAL STAFF
Consultants :-
Dr D Hobday
Dr H Mitchinson
Dr J Painter
Dr D Nylander
Dr D Oliver
6
Registrars (Reg):- x 2
Senior house Officer (SHO):- x 2
House Officer (HO):- x 2
NURSING STAFF
Ward Manager (Band 7) Mrs R Layfield
Junior Sister (Band 6) Mrs C McGill
Staff Nurses (Band 5)
Health Care Assistants (Band 2)
Ward Clark Mrs M Finkle

7
OTHER MEMBERS OF STAFF YOU MAY MEET ON THE WARD
Domestics
Springboard
Pharmacist (ward based)
Pharmacist Technician
Occupational Therapist
Physiotherapist
Physiotherapist Assistant
Speech and Language Therapist
Dietician
Medical Social Workers
PEG Specialist Nurse
Palliative Specialist Nurses
Ward Hostess
Radiographer

8
Who's Who On E53
WARD SISTER JUNIOR SISTER
Navy Uniform. Navy Uniform
STAFF AUXILLARY NURSES. NURSES.
Pale Blue Uniform. Beige Uniform. White Tunic. White Tunic. (With Pale Blue Epaulettes) (With Beige Epaulettes)
STUDENT NURSES. SPRINGBOARD.
White Tunic. Pale Green Uniform Black Trousers.
DOMESTIC STAFF. PHYSIOTHERAPISTS.
Yellow Tunic/Dress. Navy Trousers. Navy Trousers/ Top White Tunic.
OCCUPATIONAL RADIOGRAPHER. THERAPISTS.
Green Trousers. Burgundy Trousers White Tunics. White Tunics.
9
OFF DUTY / MENTORS
You will be allocated a mentor prior to commencement of your placement. Your
mentor will help co-ordinate your experience during your time with us. All mentors
have been prepared for their role and will be familiar with your training requirements.
If you are unhappy with your mentor or any other aspect regarding this placement,
please speak to the Ward Manager.
Your off duty should be negotiated with your mentor or Ward Manager (please note
we expect you to work a minimum of 50% of your off duty with your mentor.) It is
your responsibility to be flexible, working as many shifts as possible alongside your
mentor, thus making the most of your placement. To enable you to gain insight into
different aspects of holistic patient care you should try and work a variety of shifts.
OFF DUTY TIMES
Early 7:30 am – 4
Early half 7:30 am - 1pm
Late 12.00pm - 8.30 pm
Night duty 8: 15pm – 7.45 am
Off duty where possible is completed four weeks in advance.

10
PRACTICE PLACEMENT FACILITATOR
(Joint appointment between City hospitals Sunderland and Northumbria University.)
The practise placement facilitator is available to support your learning experience.
Her contact details are:-
Sonia Malt
City Hospitals Sunderland: - 0191 5656256 Ext 47210
Bleep: - 52273
Mobile: - 0776982053
Email: - [email protected] < mailto:[email protected]>
Direct Post to :-
Sonia Malt
Room 1510
Education and Training Centre
Sunderland Royal Hospital
Kayll Road
Tyne and Wear
Office
Room 1510
1st floor (opposite the Learning Resource Centre)

11
EMERGENCY ALARM CALLS AND NUMBERS
Fire Alarm
Each Thursday morning the fire alarms will sound an intermittent tone. This is a test
procedure only. In the event of the same tome sounding at any time this indicates that
the alarms have been activated and that action must be taken. When this occurs it is
everyone’s responsibility to ensure that all doors and windows are closed and remain
closed until the stand down is given. Visitors and patients should not leave the ward
during this time. In the event of a continuous unbroken tone, this indicates that the fire
alarms have been activated in your area and requires urgent investigation and possible
evacuation of all patients, relatives and staff. The nurse in charge will give you full
directions if this was to occur.
Cardiac Arrest/ Crash Call
In the event of a cardiac arrest on the ward your first line of action is to activate the
emergency buzzer and shout for assistance. The crash trolley and portable suction
machine is located in the centre of the ward, outside side room 6.
CARDIAC ARREST 2222
FIRE 333
SECURITY 777
12
TEAM NURSING
Staffs upon E53 are divided into two teams of nursing:
Team 1:- Bay 1 and 2 and side rooms 1, 2 and 3
Team 2:- Bay 3 and 4 and side rooms 4, 5 and 6
You will be allocated into the team where your mentor works on the first day of your
placement.
Within the team you will be allocated patients whose care you will be responsible for,
delivering the care under the supervision of your mentor. Your mentor will orientate
you to the wards layout and supervise you throughout your placement. All members
of staff upon the ward are available for support and advice – please use us!
Team nursing involves the Team Leader (staff nurse) dividing the workload fairly and
equally between the team members, delegating responsibilities for specific patients to
the staffs skill mix.
All members of the team should be aware of the patients’ medical conditions and
needs from the verbal handover received from the staff nurse at the start of each shift.
A team usually consists of 2 staff nurses and 2 health care assistants, and possible a
student nurse.
The organizational method of Team Nursing was devised primarily to provide the
non-professional nursing personnel with more supervision from the Registered Nurses
to allow them to give planned care rather than task orientation.
An important feature of Team Nursing is communication between members,
informing the Team Leader of any problems identified or changes in a patient’s status
will allow prompt action, revise goals so that all team members can learn to
participate in planning and evaluate care, whilst also at the same time having learning
and teaching opportunities.

13
The Health Care Assistants on the ward all undergo assessments for various
competencies and relevant forms signed to state that they are competent in a particular
task, e.g. blood pressure monitoring or blood glucose monitoring. Most of our health
care assistants have undertaken and completed the NVQ level 2 and are currently
working towards NVQ level 3. All health care assistants upon E53 are very skilled
and will be able to assist you with certain tasks.
TRANSFER OF PATIENTS
When a patient is transferred onto the ward, we aim to introduce the named Nurse
almost immediately. Ward leaflets will be given with details of visiting times, named
nurse and the ward telephone numbers. We also maintain a safe environment for the
patient to stay in whilst they are under our care. Patients’ modesty, privacy and
confidentiality are of utmost importance. The nurse should also when appropriate act
as the patients advocate.
WARD ROUNDS
The gastroenterology Consultants rotate from ward work , endoscopy unit and out -
patient clinics. They are usually ward based for approximately four weeks. They have
a ward round twice weekly – Monday afternoons and Thursday mornings.
The House Officers are on the ward each day and review their patients regularly.
We also work with all other general medical consultants and their own teams
including renal medicine, endocrinology, respiratory, cardiology, neurology and
oncology.

14
INFORMATION AND RESEARCH
We encourage giving research and evidence based nursing care. We have regular
teaching sessions on the ward for all grades of nurses. We also have a Health
Education / Information board which is changed on a monthly basis.
We also have link nurses to make it easier to identify whom to approach for various
problems. There are information files set up by the link nurses and a variety of
journals and medical books in the staff resource room. Please feel free to read them
but DO NOT remove them from the ward.
LIST OF LINK NURSES ON E53
Infection Control--------------------------- S/R C McGill HCA Donaldson
Diabetes------------------------------------- S/N Fox HCA Corner
CPR------------------------------------------ S/N Martin S/N Gilmore
Manual Handling------------------- --------S/N Dolman HCA Lay
Education-------------------------- S/N De Los Reyes S/N Chan
Oncology and palliative care- ------------S/N Rooks S/N Vizcarra
Critical care------------------------ S/N Nair S/N Chan
H+S/COSHH----------------------- SR Layfield S/N Yap
Clinical Governance ----------- SR Layfield
HISS---------------------- S/N Rooks S/N Gilmore
Equipment --------------- S/N Nair HCA Nelson
Discharge----------------- S/N Martin S/N Narayankurup
Tissue Viability/ Wound Care---------- S/N Miraflares HCA Stephenson

15
ESSENCE OF CARE LINK NURSES
PRESSURE ULCERS S/N MCGILL HCA STEPHENSON
PRIVACY AND DIGNITY S/N YAP HCA CORNER
RECORD KEEPING S/N DOLMAN HCA DONALDSON
HYGIENE S/N MOULD HCA NELSON
NUTRITION S/N VIZCARRA HCA BROOKES
CONTINENCE S/N NAIR HCA LAY
SELF CARE S/N ROBIN HCA LYNCH
SAFETY S/N FOX HCA WALTON
COMMUNICATION S/N DE LOS REYES HCA SHICKLE

16
LEARNING OPPORTUNITIES
The following opportunities may be available to you during your placement:
To observe and participate in essential nursing care relevant to a variety of
medical conditions e g. assessing , planning, implementing and evaluating care
using the adapted Roper, Logan and Tierney model of activities of daily living
and the computerized HISS system.
Care of patients in need of pain control, care of the terminally ill and dying
patients
Care of newly diagnosed conditions e.g. cancers.
You will be able to take part in the care and management of patients with
varying causes of liver disease, especially relating to alcohol cirrhosis and
further complications.
Detoxification of alcohol dependent and drug dependent patients, providing
support, advice and self help referral.
Patients requiring investigations into jaundice.
Patients with forms of inflammatory bowel disease (IBD) e.g. Ulcerative
Colitis/ Crohns Disease
Patients with gastro-intestinal cancer and associated problems e.g. weight loss,
dyspepsia
Opportunities to nurse patients with respiratory, renal, cardiology and
endocrinology problems.
Patients requiring insulin treatment and blood glucose monitoring

17
There may be also opportunities to insert and remove urinary catheters,
preparation and administration of medicines and intravenous medication under
supervision of your mentor
Participation in organising the safe transfer of a patient to another ward or
hospital following relevant guidelines
Participation in organising the patients safe discharge home from hospital
Referral to Medical Social Workers, Occupational therapist and other
members of the Multidisciplinary team.
Common test and investigations you may wish to observe include:-
Electrocardiogram (ECG)
Phlebotomy
X-Ray
Ultra sound scan ( USS)
Endoscopy
Colonoscopy
ERCP
Central Venous Pressure Line Insertion/removal
Paracentesis
Medical Physics scans
Liver biopsy
And many more
18
Remember – it is your responsibility to approach your mentor and arrange to observe
these procedures. During your placement with us it is your responsibility to fulfil your
objectives, remembering that your mentor and all members of staff are there to help
you and answer any questions you may have.
If you experience any problems during your placement please see your mentor or the
Ward Manager during your placement – problems cannot be rectified after you have
left the ward.

19
Be on time for your shift.
To make the most of the Educational Opportunities the ward has to offer.
Inform the ward as soon as possible if you are sick and give a date for your return.
Report for duty clean and tidy with minimum jewellery. Long hair should be tired back.
Wear an identification badge.
Remember that we can also learn from you.
We encourage the use of up to date practices and welcome the sharing of the new information.
Responsibility for the maintenance of confidentiality within the patient / nurse relationship, and within the Multi – disciplinary team.
To ask if you are not sure of anything
To be an active member of the ward team.
WHAT
WE EXPECT FROM
YOU

20
LEARNING OPPORTUNITES E53
Interpersonal Skills
Clinical Nursing Skills
Health Development Opportunities
Anatomy, Physiology and
pathology
Management of Care
Managerial and Organisation
Skills
21
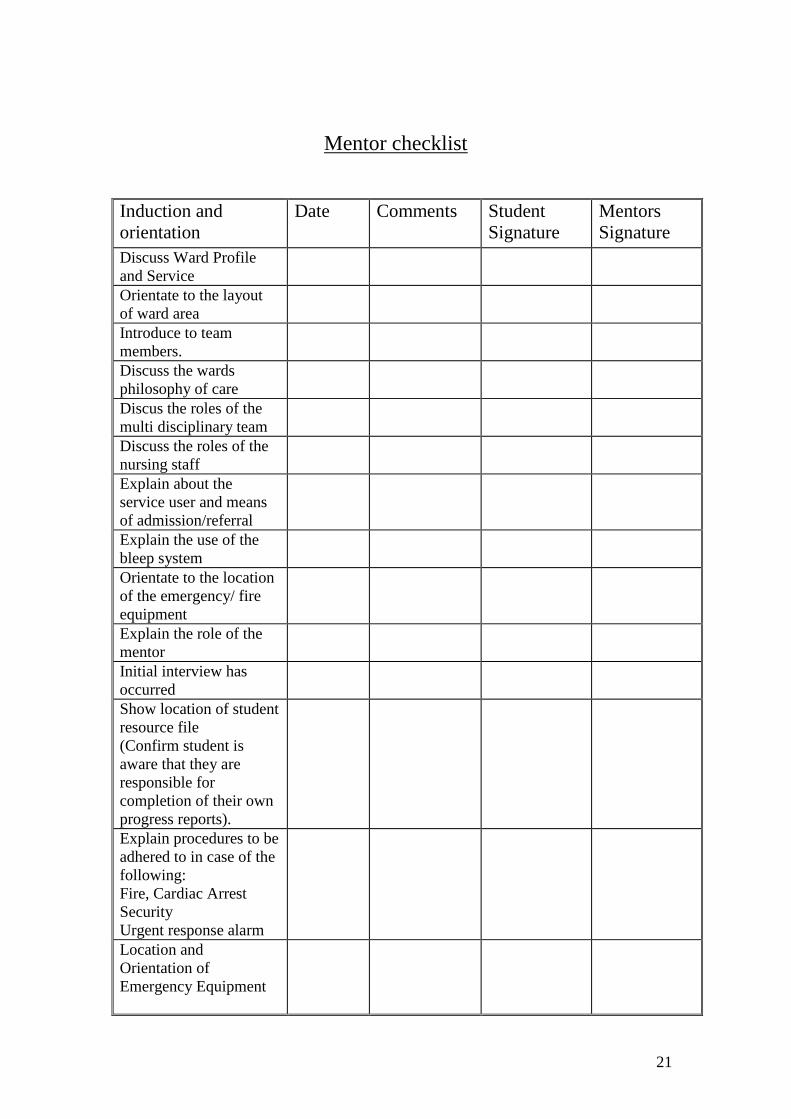
Mentor checklist
Induction and
orientation
Date Comments Student
Signature
Mentors
Signature
Discuss Ward Profile
and Service
Orientate to the layout
of ward area
Introduce to team
members.
Discuss the wards
philosophy of care
Discus the roles of the
multi disciplinary team
Discuss the roles of the
nursing staff
Explain about the
service user and means
of admission/referral
Explain the use of the
bleep system
Orientate to the location
of the emergency/ fire
equipment
Explain the role of the
mentor
Initial interview has
occurred
Show location of student
resource file
(Confirm student is
aware that they are
responsible for
completion of their own
progress reports).
Explain procedures to be
adhered to in case of the
following:
Fire, Cardiac Arrest
Security
Urgent response alarm
Location and
Orientation of
Emergency Equipment

22
Students
Responsibilities in
regard to :
Professionalism
Confidentiality
Conduct
Attire
Procedure for disposal
of
Sharps
Bodily Fluids
Glass
Drugs
Blood Products
Discuss levels of
education in relation to:
Manual Handling
Infection Control
CPR
Location of Manual
Handling equipment
Hoist
Pat slide
Hours of Duty
Sickness Procedure
An appropriate
Knowledge and
Understanding of The
HISS system in:
Nursing Module
Evaluation
Discharge/Transfer
Location of
Policy/Procedure Files
in:-
Nursing Policies File
Health and Safety File
Infection Control
Manual
Standards File
Complaints Procedure
(discussed)
Sickness Policy
Blood Product’s File
COSHH
Drug Administration
23
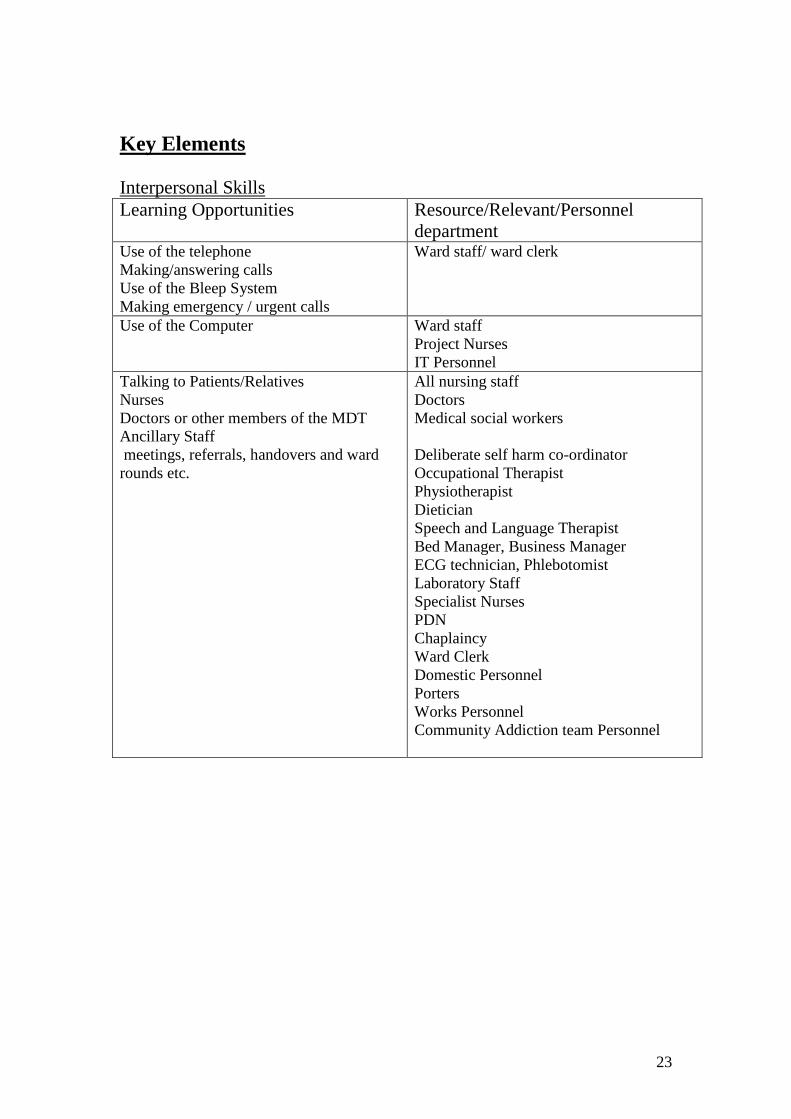
Key Elements
Interpersonal Skills
Learning Opportunities Resource/Relevant/Personnel
department Use of the telephone
Making/answering calls
Use of the Bleep System
Making emergency / urgent calls
Ward staff/ ward clerk
Use of the Computer Ward staff
Project Nurses
IT Personnel
Talking to Patients/Relatives
Nurses
Doctors or other members of the MDT
Ancillary Staff
meetings, referrals, handovers and ward
rounds etc.
All nursing staff
Doctors
Medical social workers
Deliberate self harm co-ordinator
Occupational Therapist
Physiotherapist
Dietician
Speech and Language Therapist
Bed Manager, Business Manager
ECG technician, Phlebotomist
Laboratory Staff
Specialist Nurses
PDN
Chaplaincy
Ward Clerk
Domestic Personnel
Porters
Works Personnel
Community Addiction team Personnel

24
Key Elements
Clinical Skills
Learning Opportunities Resource/Relevant/Personnel
department Patient Hygiene
Mouth Care
Skin Care
Nail Care
Hair Care
Bed Bathing
Physiological Observations
Neurological Observations
Blood Pressure
Temperature, Pulse, Respirations
Blood Glucose Monitoring (BM)
Fluid Balance
Peak Flow Measurement
Weight
Pulse Oximetry
Maintaining accurate charts
Drug Administration
Intramuscular Injections
Intravenous Drugs
Oral
Rectal
Subcutaneous
Intravenous Fusions
Moving and Handling
Use of Aids and Hoists
Correct procedures
Infection Control
Isolation/ Barrier Nursing
Hand washing
Aseptic technique
Nutritional Assessment
Recording Intake
Nutritional Supplements
Procedures
Cannulation/ care of the cannulae
Catheter insertion and care of.
ECG recording
Care of IV infusions
Administration Blood/ Blood products
Phlebotomy
Preparation of investigations and
procedures eg endoscopy
Care of central lines
All Nursing Staff
Occupational Therapist
Registered Nursing Staff
Diabetic Link Nurse
All registered Nurses
Pharmacist
Doctors
Manual handling link
All qualified nurses
Manual Handling Advisor
All registered Nurses
Control of Infection Link
Infection Control Nurses
All registered Nurses
Nutritional Link Nurse
Dietician
Registered Nurses
Registered Nurses, doctors,
Registered nurses, doctors,

25
Key Elements
Anatomy, Physiology and Pathology
Learning Opportunities Resource/Relevant/Personnel
department Nervous system
Head injury
Epilepsy
CVA
Infection
Headache
Infection/immunology
Causes
Spread
Prevention
Antigens
Immune system
Mental Health
Deliberate Self harm
Overdose
Psychiatric emergency’s
Psychosis
Drug addiction
Alcohol Addiction
Infection
Degenerative diseases
Respiratory system
Pnuemothorax
Pneumonia
Asthma
Pulmonary embolism
COPD
Chest infection
Pleural effusions
Lung canceers
Disorders of the Cardiovascular system
Cardiac Arrest
Congestive Heart Failure
Left Ventricular Failure
Myocardial Infarction
Hypertension
Registered nurses
Specialist nurses, physio, OT, MSW
Doctors, CVA team/unit X-ray
Registered nurses, doctors, infection
control nurses, infection control policies.
Registered nurses, Doctors, CAT
team, Deliberate Self Harm co-
ordinator, PSW, CPN’s, crisis teams, Support workers, Pharmacist
Registered nurses
Specialist nurses
Doctors, X-ray
Dietician, doctors, Specialist nurses
Registered nurses
ECG technician
26
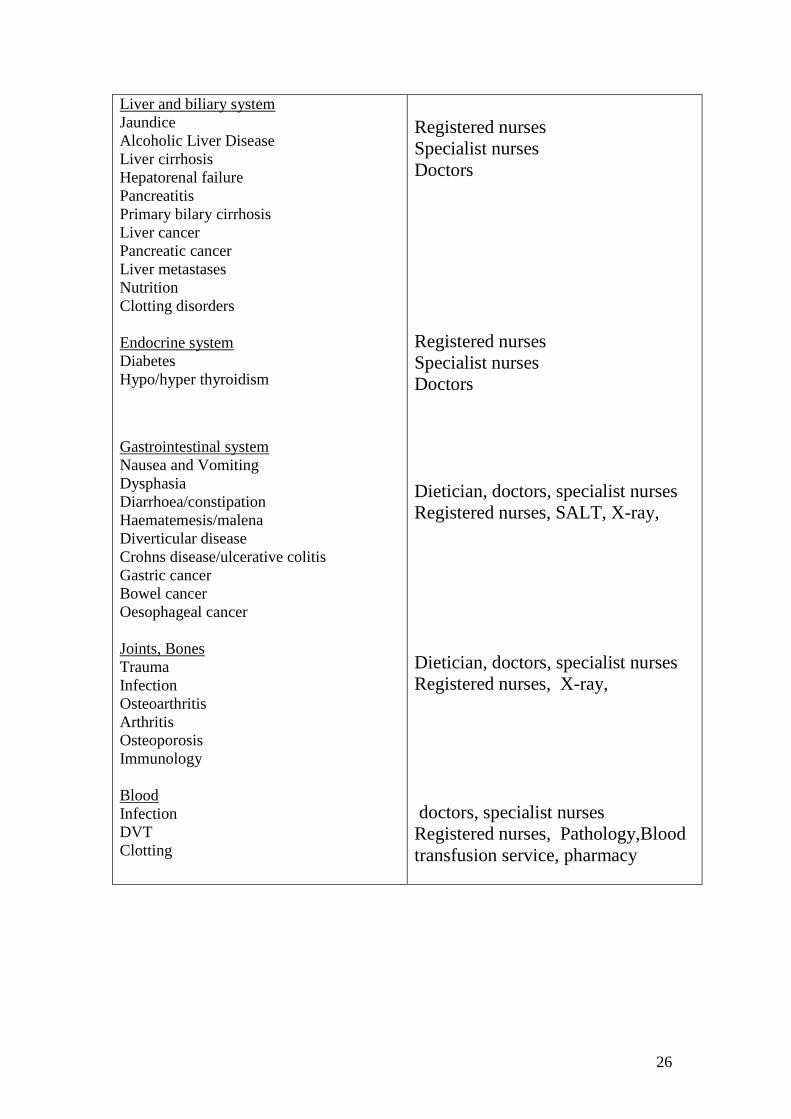
Liver and biliary system
Jaundice
Alcoholic Liver Disease
Liver cirrhosis
Hepatorenal failure
Pancreatitis
Primary bilary cirrhosis
Liver cancer
Pancreatic cancer
Liver metastases
Nutrition
Clotting disorders
Endocrine system
Diabetes
Hypo/hyper thyroidism
Gastrointestinal system
Nausea and Vomiting
Dysphasia
Diarrhoea/constipation
Haematemesis/malena
Diverticular disease
Crohns disease/ulcerative colitis
Gastric cancer
Bowel cancer
Oesophageal cancer
Joints, Bones
Trauma
Infection
Osteoarthritis
Arthritis
Osteoporosis
Immunology
Blood
Infection
DVT
Clotting
Registered nurses
Specialist nurses
Doctors
Registered nurses
Specialist nurses
Doctors
Dietician, doctors, specialist nurses
Registered nurses, SALT, X-ray,
Dietician, doctors, specialist nurses
Registered nurses, X-ray,
doctors, specialist nurses
Registered nurses, Pathology,Blood
transfusion service, pharmacy
27
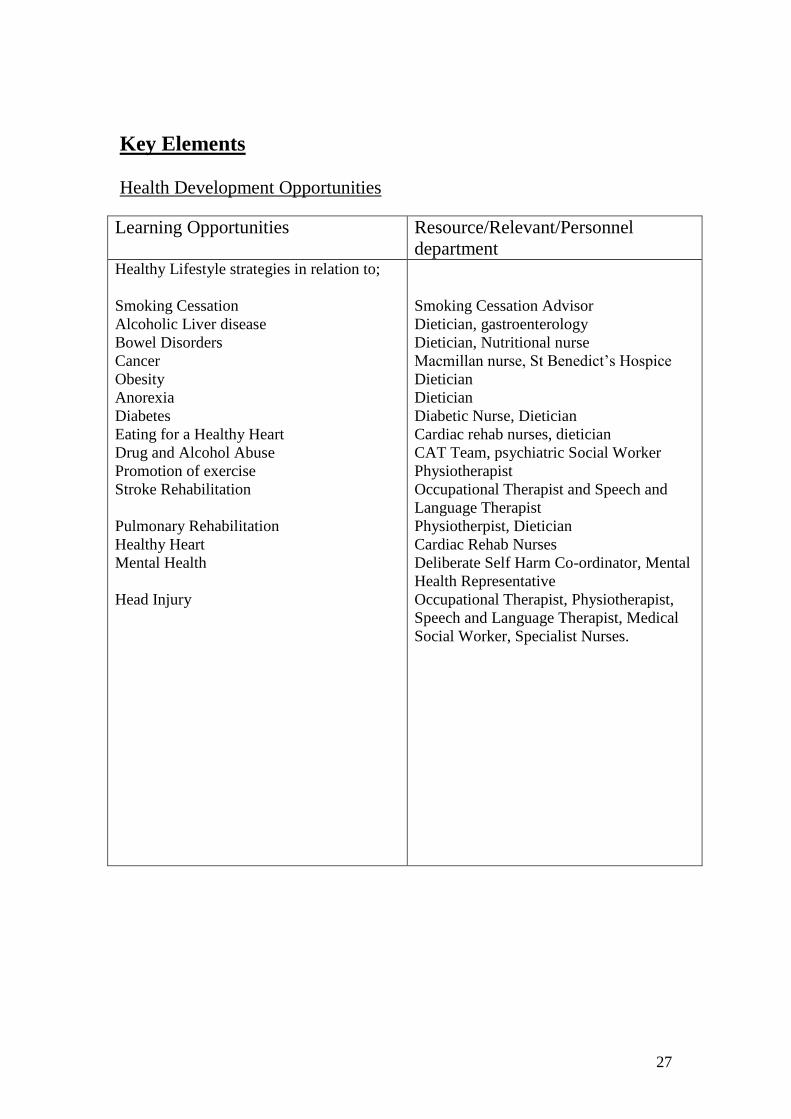
Key Elements
Health Development Opportunities
Learning Opportunities Resource/Relevant/Personnel
department Healthy Lifestyle strategies in relation to;
Smoking Cessation
Alcoholic Liver disease
Bowel Disorders
Cancer
Obesity
Anorexia
Diabetes
Eating for a Healthy Heart
Drug and Alcohol Abuse
Promotion of exercise
Stroke Rehabilitation
Pulmonary Rehabilitation
Healthy Heart
Mental Health
Head Injury
Smoking Cessation Advisor
Dietician, gastroenterology
Dietician, Nutritional nurse
Macmillan nurse, St Benedict’s Hospice
Dietician
Dietician
Diabetic Nurse, Dietician
Cardiac rehab nurses, dietician
CAT Team, psychiatric Social Worker
Physiotherapist
Occupational Therapist and Speech and
Language Therapist
Physiotherpist, Dietician
Cardiac Rehab Nurses
Deliberate Self Harm Co-ordinator, Mental
Health Representative
Occupational Therapist, Physiotherapist,
Speech and Language Therapist, Medical
Social Worker, Specialist Nurses.

28
Key Elements
Management of Care
Learning Opportunities Resource/Relevant/Personnel
department Nursing Process
Use of the Nursing Model
Philosophy of Care
Documentation Used
Assessment
Who assesses
How is it carried out
What is assessed
Where does it take place
Planning
Care plans
Care pathways
Multi- disciplinary team plans
Discharge Planning
Risk Assessment
Referrals to other agencies:
Physio, OT, SALT, Social Worker, District
Nurse, Specialist Nurse, Macmillan Nurse.
Discharge Liaison
24/7 Team
Relevant Departments
Implementation/ Evaluation
Ward Rounds
MDT/ TDT Meetings
Documentation
Standards
Protocols
Communication to relatives and Patients
Time Management
Planning Priorities
Dealing with difficult situations
Deceased patients
Patients property/valuables
Self Discharge
Religious needs
Registered Nurses
Registered Nurses
Patient, relatives, doctors notes, district
nurses
Registered Nurses
Specialist Nurses
MDT
Registered Nurses
Discharge liaison
Registered Nurses
Registered Nurses, Ward Sister, Doctors
Registered Nurses
Registered Nurses
Registered Nurses
Registered Nurses
Registered Nurses
Registered Nurses
Registered Nurses
Registered Nurses
Registered Nurses
Registered Nurses
Registered Nurses, doctor
Registered Nurses, Chaplaincy

29
Key Elements
Organisational and Managerial Issues
Learning Opportunities Resource/Relevant/Personnel
department Managing a Team
Organisational Skills
Delegation Skills
Prioritising Skills
Time management
Leadership
Off Duty
Managing patient workload
Quality
Standards of Care
Implementing Change
Managing Risk
Policies and Procedures
Equipment and Safety Checks
Quality Control
Infection Control
Moving and Handling
Emergency Situations
Cardiac Arrest
Fire
Violent incidents
Bed alerts
Patient Falls
Fast Bleep system
Missing Persons
Resources
Stock Control
Drugs
Material Management
Non-Stock
Stationary
Establishment and Skill Mix
Budget Control
Staff Development
IPR/ Appraisal
Clinical Supervision
Reflective Practice
Communication
Staff, doctors, patients, relatives
Other members of MDT/ TDT
Other Departments
Registered Nurses
Registered Nurses
Registered Nurses/doctors
Registered Nurses
Ward Sister
Ward Sister
Registered Nurses
Registered Nurses
Registered Nurses
Registered Nurses
Ward Sister/ Registered Nurses
Health and safety officer/ Electronics/Sister
Infection Control
Manual Handling Officer
Registered Nurses
Fire Officer
Security
Bed Manager
Switchboard
Security
Registered Nurses/ stores Department
Pharmacy
Stores department
Ward Sister, ward clark
Ward Sister
Ward Sister
Registered Nurses
Registered Nurses
Registered Nurse/ doctors

30
Learning Zones N.B. it is important that when considering a visit to a Learning Zone that the
competencies a student will have achieved will have been clearly identified and
discussed with the assessor and student. The student must follow the visit, compile a
Testimony of Witness and must have this countersigned by the practitioner with whom
the competencies have been undertaken in order for the assessor to verify the
competencies have been achieved.
Palliative Specialist Nurses Chiropodist Liver Unit Freeman Hospital Hospice Gastro. Specialist Nurse Community 24/7 Addiction Team Pathology Labs Radiology Farnborough Chaplaincy Court District Nurses Smoking Cessation Team Diabetic Rapid Specialist Response Team Porters Gastro Specialist Nurse Control of Infection
Occupation Therapist Discharge liaison
Team
Pharmacist Bed Management Team
Medical Social Endoscopy Unit
Worker
Physiotherapist PEG Specialist Nurse
Dietician Speech & Language Therapist
Medical Staff Discharge Lounge
E53
31
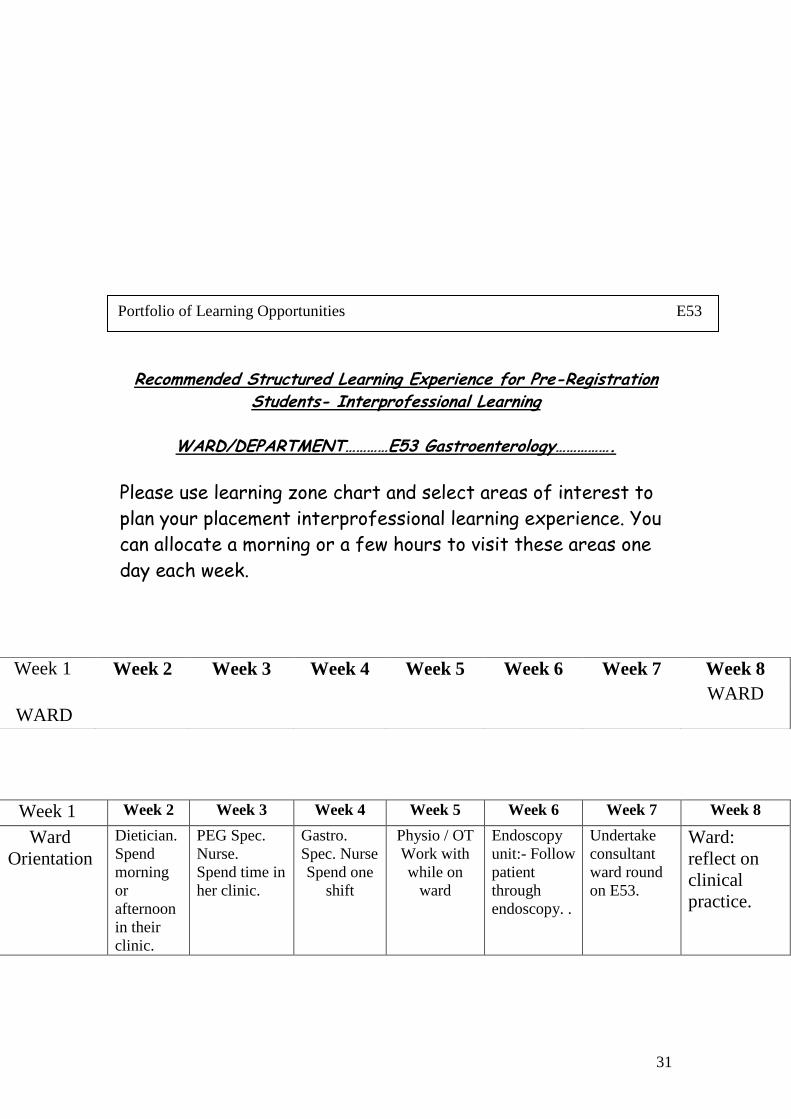
Recommended Structured Learning Experience for Pre-Registration Students- Interprofessional Learning
WARD/DEPARTMENT…………E53 Gastroenterology…………….
Please use learning zone chart and select areas of interest to
plan your placement interprofessional learning experience. You
can allocate a morning or a few hours to visit these areas one
day each week.
Week 1 Week 2 Week 3 Week 4 Week 5 Week 6 Week 7 Week 8
Ward
Orientation
Dietician.
Spend
morning
or
afternoon
in their
clinic.
PEG Spec.
Nurse.
Spend time in
her clinic.
Gastro.
Spec. Nurse
Spend one
shift
Physio / OT
Work with
while on
ward
Endoscopy
unit:- Follow
patient
through
endoscopy. .
Undertake
consultant
ward round
on E53.
Ward:
reflect on
clinical
practice.
Week 1 Week 2 Week 3 Week 4 Week 5 Week 6 Week 7 Week 8
WARD
WARD
Portfolio of Learning Opportunities E53

32
The Heart
Portfolio Of Learning Opportunities E53

33
The Circulatory System
Portfolio of Learning Opportunities E53

34
The Respiratory System
Portfolio of Learning Opportunities E53

35
The Skeleton System
Portfolio of Learning Opportunities E53
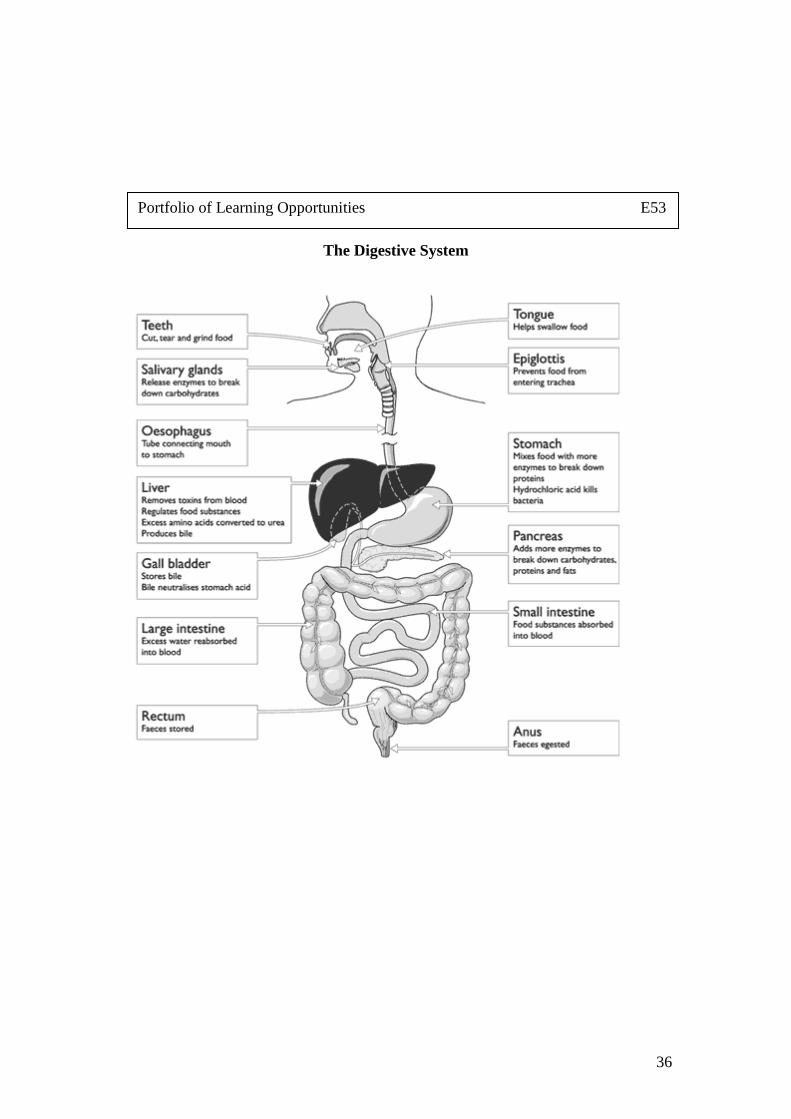
36
The Digestive System
Portfolio of Learning Opportunities E53

37
The Nervous System
Portfolio of Learning Opportunities E53

38
Portfolio of Learning Opportunities E53
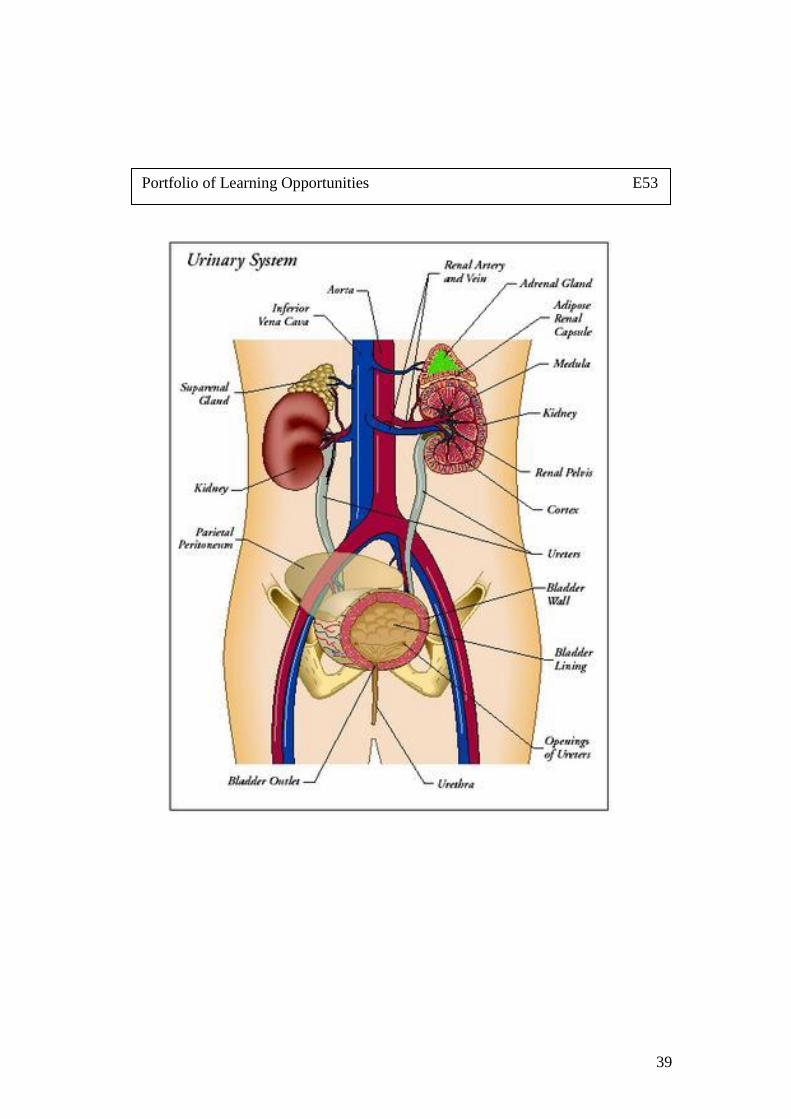
39
Portfolio of Learning Opportunities E53

40
Abbreviations
A A&E Accident &Emergency A/W Awaiting ABG Arterial Blood Gases ACLS Advanced Cardiac Life Support AF Atrial Fibrillation AFB Acid Fast Bacilli ALS Advanced Life Support ALD Alcoholic Liver Disease ANT LAT MI Anterior Lateral Myocardial Infarction ANT MI Anterior Myocardial Infarction AP Anteroposterior APTT Activated Partial Thromboplast In Time ARDS Adult Respiratory Distress Syndrome AVF,AVL,AVR Augmented Limb Leads
B BD Twice Daily BM Boehringer Mannheim (Blood Glucose) BNO Bowels Not Opened BO Bowels Opened BP Blood Pressure BPM Beats Per Minute BSA Body Surface Area
C C&S Culture & Sensitivity CA Cancer CAT Computer Aided Tomography CABG Coronary Artery Bypass Graft CBD Catheter Bag Drainage CCF Congestive Cardiac Failure CCU Coronary Care Unit CE Cardiac Enzymes CHB Complete Heart Block CHEMO Chemotherapy CK Creatine Kinase
41
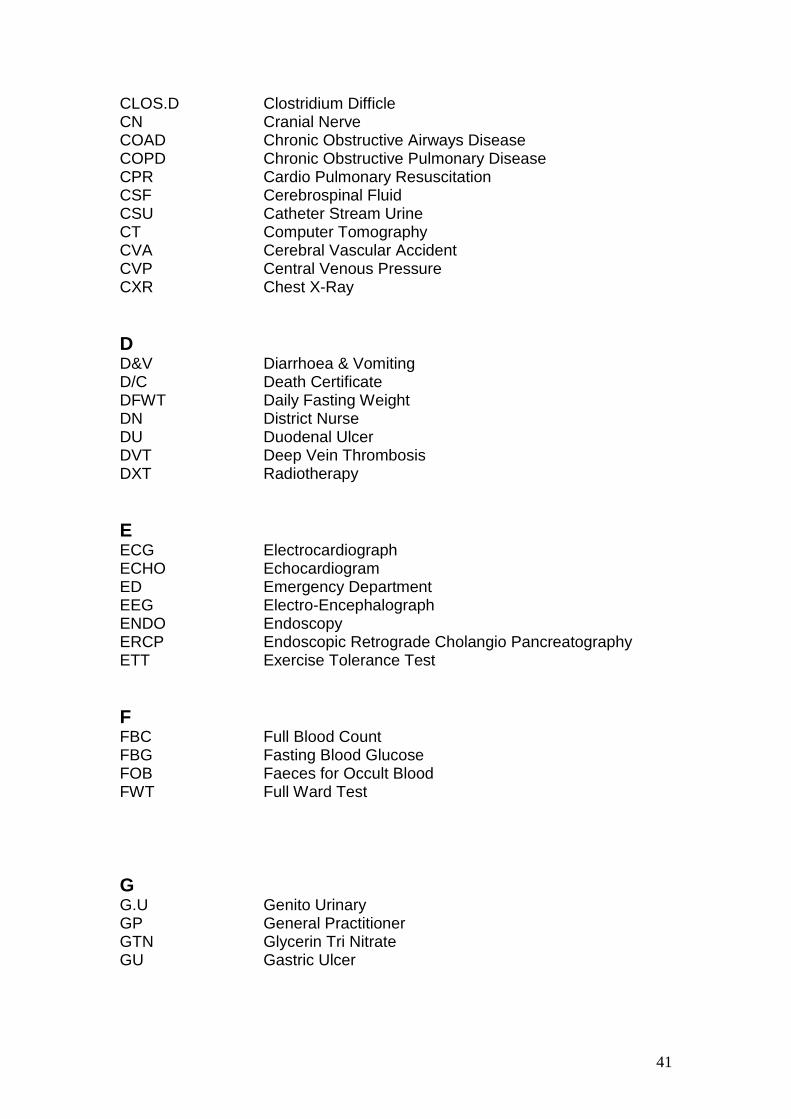
CLOS.D Clostridium Difficle CN Cranial Nerve COAD Chronic Obstructive Airways Disease COPD Chronic Obstructive Pulmonary Disease CPR Cardio Pulmonary Resuscitation CSF Cerebrospinal Fluid CSU Catheter Stream Urine CT Computer Tomography CVA Cerebral Vascular Accident CVP Central Venous Pressure CXR Chest X-Ray
D D&V Diarrhoea & Vomiting D/C Death Certificate DFWT Daily Fasting Weight DN District Nurse DU Duodenal Ulcer DVT Deep Vein Thrombosis DXT Radiotherapy
E ECG Electrocardiograph ECHO Echocardiogram ED Emergency Department EEG Electro-Encephalograph ENDO Endoscopy ERCP Endoscopic Retrograde Cholangio Pancreatography ETT Exercise Tolerance Test
F FBC Full Blood Count FBG Fasting Blood Glucose FOB Faeces for Occult Blood FWT Full Ward Test
G G.U Genito Urinary GP General Practitioner GTN Glycerin Tri Nitrate GU Gastric Ulcer
42
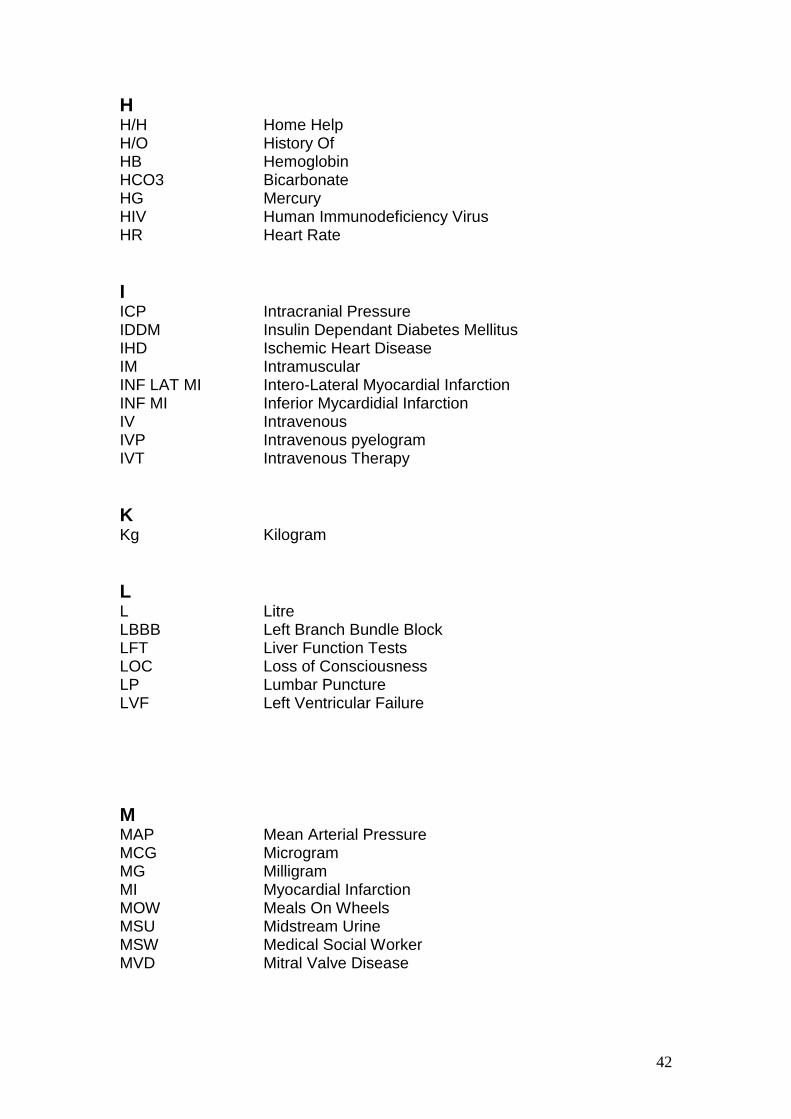
H H/H Home Help H/O History Of HB Hemoglobin HCO3 Bicarbonate HG Mercury HIV Human Immunodeficiency Virus HR Heart Rate
I ICP Intracranial Pressure IDDM Insulin Dependant Diabetes Mellitus IHD Ischemic Heart Disease IM Intramuscular INF LAT MI Intero-Lateral Myocardial Infarction INF MI Inferior Mycardidial Infarction IV Intravenous IVP Intravenous pyelogram IVT Intravenous Therapy
K Kg Kilogram
L L Litre LBBB Left Branch Bundle Block LFT Liver Function Tests LOC Loss of Consciousness LP Lumbar Puncture LVF Left Ventricular Failure
M MAP Mean Arterial Pressure MCG Microgram MG Milligram MI Myocardial Infarction MOW Meals On Wheels MSU Midstream Urine MSW Medical Social Worker MVD Mitral Valve Disease

43
N NAD No Abnormalities Detected NBM Nil By Mouth NIDDM Non Insulin Dependent Diabetes Mellitus NGT Nasal Gastric Tube NPU Not Passed Urine NS Normal saline (solution) NSAID Nonsteroidal Anti-inflammatory Drug
O O/A On Admission O/D Overdose O2 Oxygen OBS Observations OGD Oesophageal Dilation OPST Older Person's Support Team OT Occupational Therapist
P P Pulse PBC Primary Biliary Cirrhosis PE Pulmonary Embolism Peds Pediatrics PEFR Peak Expiratory Flow Rate PEG Percutaneous Endoscopic Gastrostomy Physio Physiotherapist PID Pelvic Inflammatory Disease PO By Mouth POST MI Posterior Myocardial Infarction PR Per Rectum PRN As Required PT Prothrombin Time PTT Partial Thromboplastin Time PU Passed Urine PUT Passed Urine in Toilet PX Prescribed
Q QDS Four Times a Day
R RBBB Right Bundle Branch Block RBC Red Blood Count
44
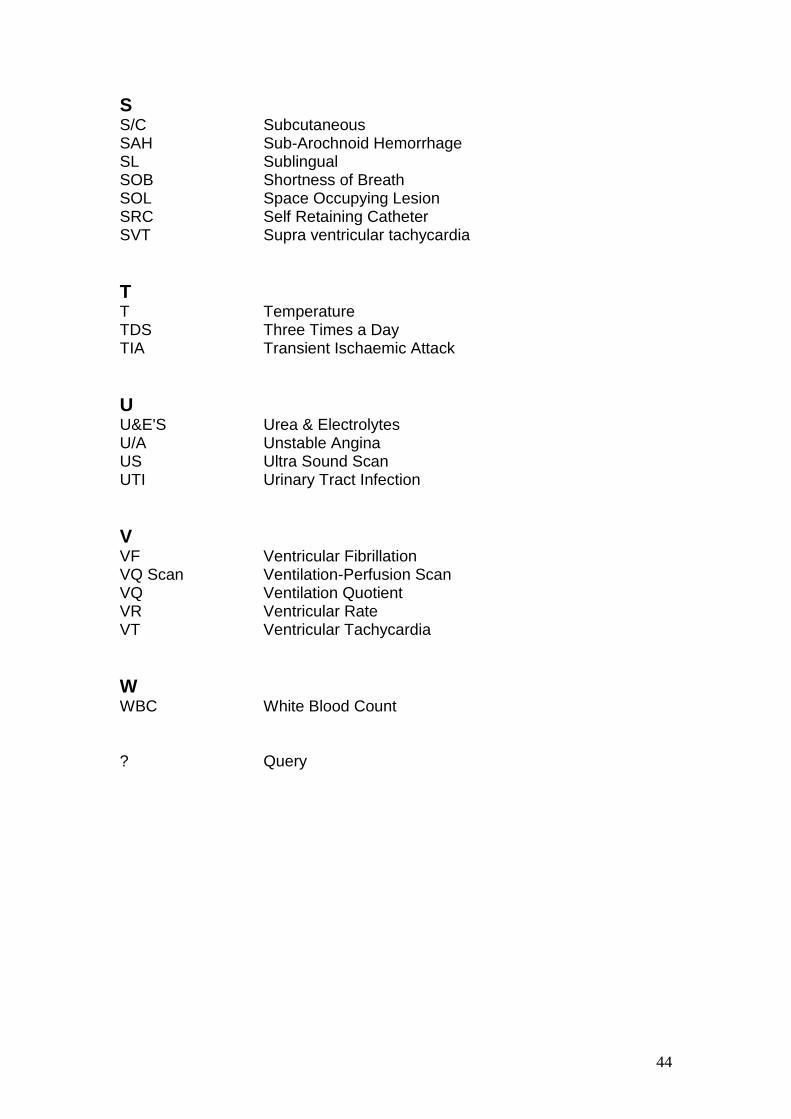
S S/C Subcutaneous SAH Sub-Arochnoid Hemorrhage SL Sublingual SOB Shortness of Breath SOL Space Occupying Lesion SRC Self Retaining Catheter SVT Supra ventricular tachycardia
T T Temperature TDS Three Times a Day TIA Transient Ischaemic Attack
U U&E'S Urea & Electrolytes U/A Unstable Angina US Ultra Sound Scan UTI Urinary Tract Infection
V VF Ventricular Fibrillation VQ Scan Ventilation-Perfusion Scan VQ Ventilation Quotient VR Ventricular Rate VT Ventricular Tachycardia
W WBC White Blood Count ? Query
45
Glossary of Useful Terms
AMNESIA: Failure of memory. Hence, POST-TRAUMATIC AMNESIA (PTA)
which is the lapse of time after the injury until continuous recall, and
retrograde amnesia (see RETROGRADE AMNESIA).
ANOSMIA: Loss of sense of smell.
ANEURISM: Swelling or dilation of an artery due to a weakened wall.
ANOXIA: A term applied to that state in which the body tissues have an
inadequate supply of oxygen. This may be because the blood in the lungs
does not receive enough oxygen, or because there is not enough blood to
receive oxygen, or because the blood stagnates in the body.
APATHY: A direct result of brain injury to frontal lobe structures which
concern emotion, motivation and forward planning.
APHASIA/DYSPHASIA: Difficulty understanding or expressing language as a
result of damage to the brain.
APRAXIA/DYSPRAXIA: Inability to plan and perform purposeful movements,
while still having the ability to move and be aware of movements.
ARTERIAL LINE: A very thin tube (catheter) inserted into an artery to allow
direct measurement of the blood pressure, the amount of oxygen and carbon
dioxide in the blood.
ARACHNOID: One of the three membranes holding the brain together within
the skull.
ATAXIA: Abnormal movements due to loss of co-ordination of the muscles.
46
AXON/DENDRITES: Nerve cells in the brain that look like small hair-like
tentacles. The cells communicate with each other by passing electrical and
chemical impulses between the tentacles.
BRAIN STEM: The lower extension of the brain where it connects to the
spinal cord. Neurological functions located in the brain stem include those
necessary for survival (breathing, heart rate) and for arousal (being awake
and alert).
BRAIN PLASTICITY: The ability of intact brain cells to take over functions of
damaged cells. Plasticity diminishes as a person gets older.
CARPEL TUNNEL SYNDROME: Condition in which compression of the
median (middle) nerve in the wrist, causes numbing and tingling in the fingers.
CELLULITUS: Streptococcal inflammation of tissues which cause an
oesematous appearance.
CEREBRAL: Concerning the brain.
CEREBRAL CORTEX: The largest part of the brain. It controls thought
processes (such as memory and learning) and motor functions (such as
walking).
CEREBRO-SPINAL FLUID (CSF): Liquid which fills the ventricles of the brain
and surrounds the brain and spinal cord.
COMA: The state of not being responsive or able to be aroused. The person
does not open their eyes, follow commands or speak.
COLONOSCOPE: a fibreoptic instrument, passed through the anus, for
examining the interior of the colon.
CONTRACTURES: Joints and muscles which are not used regularly quickly
becoming stiff, and rendering them resistant to stretching.
47
CRANIOTOMY: Surgical removal of the skull in small pieces.
CRANIUM: The bony skull which completely engulfs the brain to protect it.
CT SCAN/CAT SCAN: Computerised tomography. A series of X-rays at
different levels of the brain. (Tomography is a technique using X-rays to build
up a focused image of a "slice" through the body at a given level).
DENDRITE: (See AXON).
DIPLOPIA: Double vision.
DISINHIBITION: Difficulty in controlling urges and impulses to speak, act or
show emotions.
DURA: One of the three membranes holding the brain together within the
skull.
DYSARTHRIA: Difficulty speaking because of weakness and lack of co-
ordination of the muscles for speech.
DYSPHAGIA: Difficulty with swallowing.
DYSPRAXIA: Inability to plan and perform purposeful movements, while still
having the ability to move and be aware of the movement.
ELECTROENCEPHALOGRAM (EEG): EEG is a test used to record any
changes of electrical activity in the brain by placing electrodes on the scalp.
EMOTIONAL LABILITY: Rapid and drastic changes in emotional state (such
as laughing, crying or anger) that are inappropriate.
EPILEPSY: There are many varied presentations. Seizure or fit activity
involving parts of or the complete body.
FOCAL BRAIN INJURY: Injury restricted to one region (as opposed to
diffuse).
48
FRONTAL LOBES: Part of the brain involved with planning, organising,
problem solving, selective attention, personality and a variety of "higher
cognitive functions".
GASTRALIGA: Pain in the stomach.
GASTRECTOMY: excision of part or whole of the stomach.
GASTRIC: pertaining to the stomach.
GASTRITIS: inflammation of the lining of the stomach.
GASTROENTERITIS: inflammation of the lining of the stomach and intestine.
GASTROENTEROLOGY: the study of diseases of the intestinal tract.
GASTROSCOPE: an endoscope especially designed for passage into the
stomach to permit examination of the interior.
GASTROSTOMY: The creation of an opening into the stomach for the
administration of foods and fluids when swallowing is impossible.
GLASGOW COMA SCALE: A score given to head injured patients starting
immediately after the head injury to measure the degree of unconsciousness.
A score of 7 or less indicates that the person is in a coma. A maximum score
of 15 indicates that the person can speak coherently, obey commands to
move, and can spontaneously open their eyes.
HAEMATOLOGY: the science dealing with the nature, functions and diseases
of the blood.
HAEMATOMA: A collection of blood forming a definite swelling which
compresses and damages the brain around it.
HAEMORRHAGE: Blood loss, bleeding.

49
HEMIANOPIA: Blindness in the same side of both eyes which can follow
damage to the brain. This can cause an inability to see things on the left or
right side.
HEMIPLEGIA: Loss of power in one side of the body.
HEPATIC: relating to the liver.
HEPATITUS: inflammation of the liver.
HEPATOCIRRHOSIS: cirrhosis of the liver.
HEPATOMA: a primary malignant tumour arising in the liver cells.
HEPATOMEGALY: an enlargement of the liver.
HYPOTHALAMUS: A nerve centre deep in the diencephalon area which
controls the automatic nervous system, food intake, sexual rhythms, emotions
and memory.
HYDOCEPHALUS: Enlargement of the ventricles due to an increase of
cerebrospinal fluid (CSF) on the brain.
HYPOXIA: Diminished availability of oxygen to body tissues.
IMPULSIVITY: A tendency to rush into something without reflecting or thinking
first.
INTRACRANIAL PRESSURE (ICP) MONITOR: A monitoring device to
determine the pressure within the brain. It consists of a small tube (catheter)
in contact with the pulsing brain or the fluid cavity within it. ICP is measured
by means of a metal screw or a plastic catheter connected to an electronic
measuring device.
MAGNETIC RESONANCE IMAGING (MRI): Enables detailed pictures of the
brain to be acquired using a scanning machine. It uses a strong magnet rather
than X-rays.

50
MANNITOL: A solution which removes water from the brain by accelerating
urinary excretion and thus reduces raised intracranial pressure.
MOTOR CORTEX: The part of the brain around which mental activity is
centred.
NASOGASTRIC TUBE: This is the very thin tube that is threaded through the
nose and throat into the stomach for giving liquid food and pureed meals.
Used if there are swallowing difficulties.
NEURON: This is a nerve cell.
NEURO-TRANSMITTERS: Chemicals made in the nervous system that serve
as messengers, aiding or interfering with the functions of the nerve cells.
OEDEMA: Increased water content in the brain, causing brain swelling.
OCCIPITAL LOBES: A region in the back of the brain which processes visual
information.
PARIETAL LOBES: The part of each cerebral hemisphere primarily
concerned with the perception and interpretation of sensation and movement.
PERSISTENT VEGETATIVE STATE (PVS): A long-standing condition in
which the patients utters no words and does not follow commands or make
any response that is meaningful.
PIA: One of the three membranes holding the brain together.
PROPRIOCEPTION: The sensory awareness of the position of body parts
with or without movement.
RIGIDITY: This simply means stiffness, resistance to movement.
SENSORY CORTEX: The sensory cortex is situated in the cerebrum.
Different parts of the sensory cortex deal with the sensations experienced in
different parts of the body.
51
SHUNT: A devise to draw off excess fluid in the brain. A surgically placed
tube runs from the ventricles and deposits fluid into the abdominal cavity,
heart or large veins in the neck.
SPASTICITY: An involuntary increase in muscle tone (tension).
TEMPORAL LOBES: The part of each cerebral hemisphere concerned with
sound and language interpretation, and important in memory function.
TRACHEOSTOMY: An operation to insert a plastic tube in the neck just below
the Adam's apple. Through this tube, an adequate air passage can be
maintained. It may be necessary to leave the tube in the windpipe for a
prolonged period.
TREMOR: Regular repetitive movements which may be worse either at rest or
on attempted movement.
ULCER: an erosion or loss of continuity of the skin or of a mucous membrane.
ULTRASOUND: ultrasonic waves used to examine the interior organs of the
body.
VENTILATOR: A machine that does the breathing work for the unresponsive
patient. It delivers moistened (humidified) air with the appropriate percentage
of oxygen and at the appropriate rate and pressure.
VENTRICLES: Cavities (spaces) inside the brain which contain cerebro-spinal
fluid.
VESTIBULAR: System in the middle of the ear which senses movement.
Injury can lead to dizziness.
WERNICKE'S AREA: An area of the brain concerned with producing speech.
WITHDRAWAL: abstention from drugs or alcohol which one is addicted to.
52
USEFUL WEB SITES
www.doh.gov.uk
www.haznet.org.uk
www.nice.org.uk
www.nhsia.nhs.uk
www.modernnhs.nhs.uk
www.nmc.org.uk
53
STUDENT EVALUATION FORM
WARD E53
1. Were you introduced to staff on the ward on your first
day?............................................................................................................................
....................................................................................................................................
...................................................................................................................................
2. Were you introduced to the ward environment on your first
day?............................................................................................................................
....................................................................................................................................
....................................................................................................................................
3. Were you allocated a
mentor?.......................................................................................................................
....................................................................................................................................
....................................................................................................................................
4. Were you allocated an Associate Mentor in your mentors
absence?......................................................................................................................
....................................................................................................................................
....................................................................................................................................
5. Have your worked alongside your mentor throughout your placement with
us?...............................................................................................................................
....................................................................................................................................
....................................................................................................................................
6. Were you given the Student Information Pack at the commencement of your
placement?..................................................................................................................
....................................................................................................................................
....................................................................................................................................
7. Were you made aware of the POLO file and learning
zones?.........................................................................................................................
....................................................................................................................................
....................................................................................................................................
8. Were you made welcome throughout your
placement?..................................................................................................................
....................................................................................................................................
....................................................................................................................................
9. Did you gain enough learning
experiences?...............................................................................................................
....................................................................................................................................
....................................................................................................................................
54
10. What could we do to improve learning opportunities for
students?.....................................................................................................................
....................................................................................................................................
....................................................................................................................................
11. Have you gained the competencies which you set out to
achieve?......................................................................................................................
....................................................................................................................................
....................................................................................................................................
12. If not, can you explain
why?...........................................................................................................................
....................................................................................................................................
....................................................................................................................................
13. Have you enjoyed your placement here with
us?...............................................................................................................................
....................................................................................................................................
....................................................................................................................................
14. If not can you tell us
why?...........................................................................................................................
....................................................................................................................................
...................................................................................................................................
15. What do we on E53 do the best for the students coming onto our
ward?..........................................................................................................................
....................................................................................................................................
....................................................................................................................................
16. What do we on E53 do worst for the students coming onto our
ward?..........................................................................................................................
....................................................................................................................................
....................................................................................................................................
17. Is there anything else you could suggest to improve learning for students coming
onto our
ward?..........................................................................................................................
....................................................................................................................................
....................................................................................................................................
18. What year Student are
you?............................................................................................................................
....................................................................................................................................
...................................................................................................................................
Thank you for taking the time to complete this evaluation form.
Your thoughts and opinions are very valuable to us.

55