welfare to work convention 30 th june, 2011 developing and sustaining a healthy workforce &...
TRANSCRIPT

Welfare to Work Convention Welfare to Work Convention 3030thth June, 2011 June, 2011
Developing and Sustaining a Healthy Developing and Sustaining a Healthy Workforce & Delivering Employment Workforce & Delivering Employment Outcomes Through Health Related Outcomes Through Health Related
Group WorkGroup Work
Lucy Goodwin & Nicky ThomasLucy Goodwin & Nicky Thomas
(Occupational Therapists)(Occupational Therapists)

Aims of SessionAims of Session
To cover the following themes:To cover the following themes:
Into work and staying there: what works?Into work and staying there: what works?
Delivering fairness: Opportunities for allDelivering fairness: Opportunities for all

History of the Condition History of the Condition Management Programme (CMP)Management Programme (CMP)
Green Paper (published November 2002) Green Paper (published November 2002) set out a strategy for set out a strategy for enabling people with health conditions to move into and remain enabling people with health conditions to move into and remain in workin work
Department for Work and Pensions (2003) Department for Work and Pensions (2003) Pathways to Work: Helping Pathways to Work: Helping People into Employment, The Governments response and Action PlanPeople into Employment, The Governments response and Action Plan D.W.P. London D.W.P. London
2.7 million people 2.7 million people receiving Incapacity Benefit (IB) in May 2002receiving Incapacity Benefit (IB) in May 2002
The duration on IB was increasing – averaged 9 years The duration on IB was increasing – averaged 9 years compared to 3 years in 1985 compared to 3 years in 1985
Once people have been on IB for 1 year, their chances of Once people have been on IB for 1 year, their chances of returning to work diminish significantlyreturning to work diminish significantly

Aims of the CMPAims of the CMP To promote self care and use of self help To promote self care and use of self help
techniquestechniques Explore and overcome barriers to recoveryExplore and overcome barriers to recovery Assist customers to achieve a work life balanceAssist customers to achieve a work life balance Reinforce the health benefits of workReinforce the health benefits of work
(Waddell & Burton 2006)(Waddell & Burton 2006)
N.B Medical treatment and diagnosis not offeredN.B Medical treatment and diagnosis not offered

Long term health impacts
Chronic Pain
Depression
Reduced Self Esteem
Anxiety / Fear
Low Motivation
Social Exclusion
Stigma
DebtLow Confidence
Fatigue

CMP
Solutions focused
Groups and 1:1
Community Delivery
Motivational Interviewing Approaches
Partnership with JCP
Signposting
Increased social inclusion
Increased quality of life
CBT based interventions
Education and
advice

EvaluationEvaluation
An evaluation of CMP An evaluation of CMP revealed successful revealed successful outcomes in relation tooutcomes in relation to
Return to work/training Return to work/training and educationand education
VolunteeringVolunteering Re-engagement with Re-engagement with
the communitythe community Positive customer Positive customer
experienceexperience

Research QuestionResearch Question
‘‘To what extent do CMPs To what extent do CMPs enable customers to manage enable customers to manage their health conditions & move their health conditions & move closer to closer to work/education/training?’work/education/training?’
Dr Carly Reagon and Chris Vincent Dr Carly Reagon and Chris Vincent

Data CollectionData Collection N=244 (122 non-responses)N=244 (122 non-responses) Qualitative interviews with customers Qualitative interviews with customers
(N=15) & staff (N=12)(N=15) & staff (N=12) Customers represent broad range of Customers represent broad range of
ages, but cluster in 36-55 yr bracketages, but cluster in 36-55 yr bracket Primary health conditions: Mental health Primary health conditions: Mental health
& musculoskeletal& musculoskeletal Quantitative data collection over 12 Quantitative data collection over 12
months: SF36v2, GSES, HADS plus months: SF36v2, GSES, HADS plus demographic datademographic data

Short Form 36 Outcome MeasureShort Form 36 Outcome Measure
Health-related quality of life measure Health-related quality of life measure
Produces two scores:Produces two scores: Physical Component Summary (PCS)Physical Component Summary (PCS) Mental Component Summary (MCS)Mental Component Summary (MCS)
A score of between 45 and 55 is deemed A score of between 45 and 55 is deemed the norm for the general populationthe norm for the general population

Changes in SF36v2 Component Changes in SF36v2 Component Scores (%)Scores (%)
16.610.5
20.6
47.4
68.9
36
PCS MCS
worse same better

The Hospital Anxiety and The Hospital Anxiety and Depression ScaleDepression Scale
Provides scores of Generalised Anxiety & Provides scores of Generalised Anxiety & Depression Depression
Interpreted as: Interpreted as: • Normal Normal (0 - 7)(0 - 7)
• Mild Mild (8 - 10)(8 - 10)
• Moderate (11 - 14)Moderate (11 - 14)
• Severe Severe (15 - 21) (15 - 21)

HADS Depression Scores Pre/Post HADS Depression Scores Pre/Post CMP (%)CMP (%)
26.5
17.8
37.4
18.3
normal mild moderate severe
5.3
18.4
47.4
28.9
normal mild moderate severe
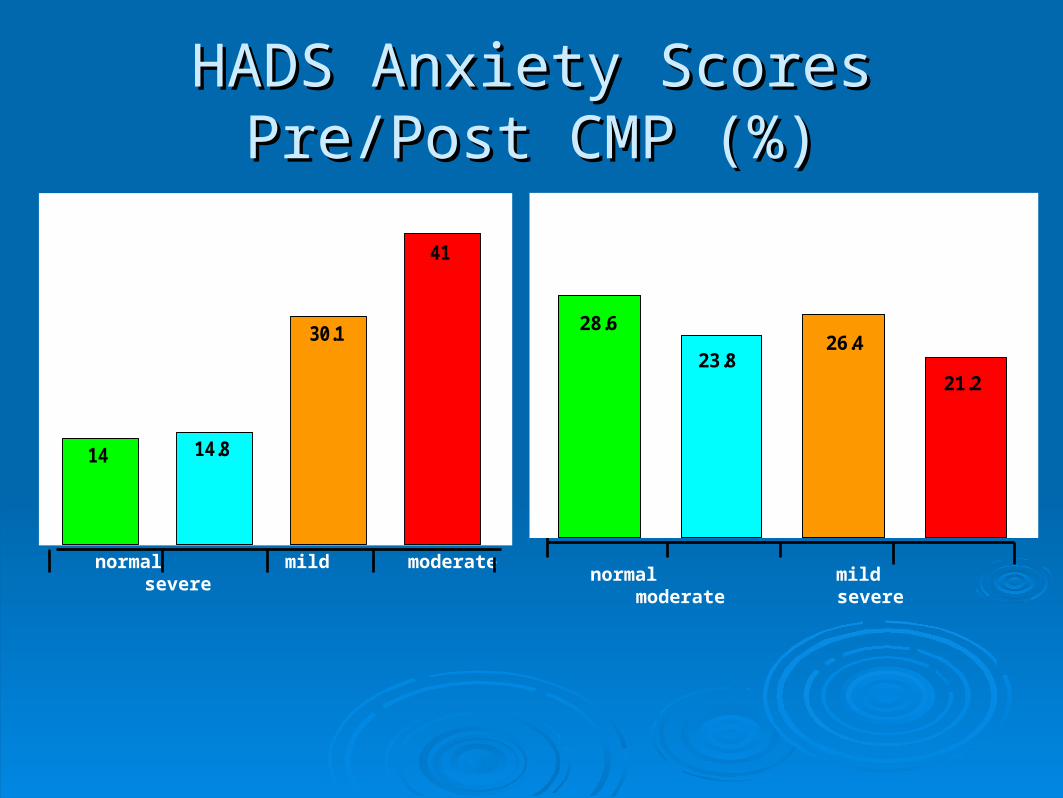
HADS Anxiety Scores Pre/Post HADS Anxiety Scores Pre/Post CMP (%)CMP (%)
normal mild moderate severe normal mild moderate severe
41
30.1
14.814
21.2
26.423.8
28.6
General Self Efficacy Outcome General Self Efficacy Outcome MeasureMeasure
Self belief to cope with life demandsSelf belief to cope with life demands
Produces a score of between 10 & 40Produces a score of between 10 & 40
A score of 29 is deemed the average A score of 29 is deemed the average score for the general healthy populationscore for the general healthy population

GSES ScoresGSES ScoresM
ean
10
20
30
GSES Post Score
GSES Pre Score
0

Work OutcomesWork Outcomes

Work OutcomesWork Outcomes During the 2009/10 operational year During the 2009/10 operational year 250 250 clients clients
completed the Pathways to Work CMP. Of those, completed the Pathways to Work CMP. Of those, 112 112 (45%)(45%) reported positive work related outcomes: reported positive work related outcomes:
Paid employment 62 (25%)Paid employment 62 (25%) Voluntary work 25 (10%)Voluntary work 25 (10%) Training/education courses 25 (10%)Training/education courses 25 (10%)
A further 23 (9%) clients were referred or signposted A further 23 (9%) clients were referred or signposted to other services/organisations which is considered to other services/organisations which is considered to be a positive outcome as a result of accessing to be a positive outcome as a result of accessing the CMPthe CMP

Qualitative AnalysisQualitative Analysis
Main Themes – CMP staffMain Themes – CMP staff The bio-psycho-social approach meets the complex The bio-psycho-social approach meets the complex
needs of CMP customersneeds of CMP customers Work and unemployment linked to personal identity Work and unemployment linked to personal identity
and social inclusionand social inclusion Link between being out of work and deteriorating Link between being out of work and deteriorating
mental healthmental health Personal motivation related to successful outcomesPersonal motivation related to successful outcomes Therapeutic relationship dependant on Therapeutic relationship dependant on
collaborative working, openness and honesty, and collaborative working, openness and honesty, and professional behavioursprofessional behaviours

““Our programme is entirely tailored to individual Our programme is entirely tailored to individual needs, it is not standardised. it is clinician led needs, it is not standardised. it is clinician led
which means that the clinician has the skills and which means that the clinician has the skills and professional competence to [act upon] what the professional competence to [act upon] what the
individuals are telling them.”individuals are telling them.” (M1:298-301) (M1:298-301)
“ “we don’t work from an expert model, the clients we don’t work from an expert model, the clients are the experts and we have the skills, so we work are the experts and we have the skills, so we work
with them”with them” (OT2 415-416) (OT2 415-416)

Qualitative AnalysisQualitative Analysis
Main Themes – CustomersMain Themes – Customers Association between CMP and Job Association between CMP and Job
Centre plus created anxiety for some:Centre plus created anxiety for some:
““[The Job Centre] [The Job Centre] just want people off just want people off their books…I’d like to be off their books their books…I’d like to be off their books but you can’t magically say you haven’t but you can’t magically say you haven’t got pain, get a job.” (C7:33-35)got pain, get a job.” (C7:33-35)

Main Themes –Customers cont’dMain Themes –Customers cont’d
Health practitioners seen as prime facilitators of Health practitioners seen as prime facilitators of change.change.
Benefits of seeing the same health practitioner Benefits of seeing the same health practitioner throughoutthroughout
Intervention plans tailored to suit their needsIntervention plans tailored to suit their needs
““It’s helped me to deal with my physical It’s helped me to deal with my physical problems and I emphasise that: my particular problems and I emphasise that: my particular physical problems, because mine are not the physical problems, because mine are not the same as anyone else’s.”same as anyone else’s.”
(C15: 407-409)(C15: 407-409)

Common ThemesCommon Themes Benefits of CMPBenefits of CMP Education about health condition/sEducation about health condition/s Learning to manage health conditionLearning to manage health condition Learning to manage painLearning to manage pain Social interaction with other participantsSocial interaction with other participants Increased confidence & self esteemIncreased confidence & self esteem Being listened to by healthcare Being listened to by healthcare
practitionerpractitioner Referral/signposting to other servicesReferral/signposting to other services Increasing activity & routineIncreasing activity & routine

Common ThemesCommon Themes
•Referrals from employers/early intervention:Referrals from employers/early intervention:
““If I had been picked up earlier by my employer and gone If I had been picked up earlier by my employer and gone through [the CMP then] I would not have become ill. It would through [the CMP then] I would not have become ill. It would have been caught and sorted earlier.”(C2:250-5)have been caught and sorted earlier.”(C2:250-5)
•Renewed sense of hope:Renewed sense of hope:•Physiological & psychological problems often co-existPhysiological & psychological problems often co-exist
““On the last session [at the CMP] I was a different person, a On the last session [at the CMP] I was a different person, a totally different person … I felt positive for the first time in totally different person … I felt positive for the first time in years … I [was] more like the person I wanted to be, not the years … I [was] more like the person I wanted to be, not the person I was when I became ill. I don’t want to be that person I was when I became ill. I don’t want to be that person again.” (C2:159-165)person again.” (C2:159-165)
Benefits of Group workBenefits of Group work Provided a structured day in the Provided a structured day in the
weekweek Interactive media –opportunity Interactive media –opportunity
for group discussionfor group discussion Building confidence through Building confidence through
Social interactionSocial interaction Solutions focused approachSolutions focused approach Venue choice e.g. raising Venue choice e.g. raising
awareness of local servicesawareness of local services Focus on exploring and Focus on exploring and
overcoming barriers to returning overcoming barriers to returning to workto work
Previous customers talk about Previous customers talk about their experience of the coursetheir experience of the course

Added Value and UnintendedAdded Value and Unintended ConsequencesConsequences
Use of non clinical Use of non clinical venuesvenues
Job Centre plus funding Job Centre plus funding benefitsbenefits 3 month gym pass3 month gym pass Equipment to deliver Equipment to deliver
coursescourses Staff training i.e Staff training i.e
motivational interviewing, motivational interviewing, solution focus, solution focus, transactional analysis, transactional analysis, mindfulnessmindfulness

SustainabilitySustainability
Raising Political Awareness/SupportRaising Political Awareness/Support Customer stories ( influenced ABMU Executive Customer stories ( influenced ABMU Executive
Team)Team) Argued the case for cost effectivenessArgued the case for cost effectiveness Demonstrable outcomesDemonstrable outcomes NHS Award for ‘Working Seamlessly Across NHS Award for ‘Working Seamlessly Across
Organisations’Organisations’ Publications in local media, professional Publications in local media, professional
magazines & research journalmagazines & research journal

The FutureThe Future NHS Staff Health & NHS Staff Health &
Well-being AgendaWell-being Agenda Well-being through WorkWell-being through Work Developing NHS Pain Developing NHS Pain
Management Management ProgrammeProgramme
Developing Chronic Developing Chronic Fatigue ProgrammeFatigue Programme
Providing services to Providing services to local private & voluntary local private & voluntary sectorsector
Work ProgrammeWork Programme

Debate: Opportunities & Debate: Opportunities & ChallengesChallenges
Further service development to ensure fit Further service development to ensure fit for purposefor purpose
Explore use of telephone support & e-Explore use of telephone support & e-resources to deliver health interventionsresources to deliver health interventions
Involvement of participants in deliveryInvolvement of participants in delivery ‘ ‘ DOES HEALTH RELATED SUPPORT DOES HEALTH RELATED SUPPORT
HAVE HAVE TO BE DELIVERED BY TO BE DELIVERED BY HEALTHCARE PROFESSIONALS’HEALTHCARE PROFESSIONALS’

Contact DetailsContact Details
Nicky Thomas and Lucy Goodwin - Occupational Nicky Thomas and Lucy Goodwin - Occupational Therapists Therapists
Condition Management Programme, Condition Management Programme, ABMU Health Board, ABMU Health Board, Britannic House, Britannic House, Llandarcy SA10 6JQ. Llandarcy SA10 6JQ. Telephone: 01792 326568Telephone: 01792 326568
Email: Email: [email protected]@wales.nhs.uk [email protected]@wales.nhs.uk

ReferencesReferences Department for Work and Pensions (2002) Department for Work and Pensions (2002)
Pathways to Work: Helping People into Pathways to Work: Helping People into EmploymentEmployment
Department for Work and Pensions (2003) Department for Work and Pensions (2003) Pathways to Work: Helping People into Pathways to Work: Helping People into Employment, The Governments response and Employment, The Governments response and Action PlanAction Plan D.W.P. London D.W.P. London
Reagon, C & Vincent C (2010) Reagon, C & Vincent C (2010) An Evaluation of An Evaluation of Three NHS-led Condition Management Three NHS-led Condition Management programmes in Walesprogrammes in Wales Cardiff: Cardiff University Cardiff: Cardiff University
Waddell, G & Burton, A.K. (2006) Waddell, G & Burton, A.K. (2006) Is Work Good Is Work Good for Your Health and Well-being?for Your Health and Well-being? London: TSO London: TSO