what are we treating? - west coast hand therapy...
TRANSCRIPT

1
The use of EPAs
In the management of Inflammation/edema/swelling
Hand therapists Feb 2016
Alison M HoensPhysical Therapy Knowledge Broker,
UBC, PABC, VCHRI, PHCRI
Clinical Professor, UBC
Research, Education & Practice Coordinator, PHC
With content from Dr. J AnthonyClinical Associate Professor 1
What are we treating?
� Inflammation
� Edema
� Swelling
� Are these synonymous terms? Is the treatment the same?
� Is trauma induced inflammation the same as immune-mediated inflammation?
2
3

2
4
ELECTRICAL STIMULATION
5
HVPC
Intensity
Duration
Interpulse interval
9900 microsec100 microsec
Pulse duration
6

3
ESTIM FOR INFLAMMATION, EDEMA,
SWELLING - HVPC
� Waveform: Twin peak monophasic
� Frequency: ~ 1-200 Hz
� Pulse Width: ~ 5-65 microsec (fixed)
� Peak Current: High
� Interpulse Interval: Long
� Total Current: Very low (~ 1.5 mA)
� Polarity: Yes
7
ESTIM FOR INFLAMMATION, EDEMA, SWELLING - PHYSIOLOGICAL RATIONALE
� Critical to apply early in inflammation
� Temporary effect (Dolan, 2003)
� Negative polarity (*if monophasic)� Postulated mechanisms
� Repulsion of serum proteins
� Reduction in blood flow *microvessel constriction
� Reduction in pore size
8
ESTIM FOR INFLAMMATION, EDEMA, SWELLING - CLINICAL APPLICATION
� Caution with acute inflammation (redness/heat)
� Contraindications
� Sensation testing
� Skin preparation
� Explanation
� Twitch to cause mm pump
� 10 Hz
� Intensity to muscle twitch
� 20-30 min
� *For extraarticular
� Combine with elevation, compression, exercise, positioning
9

4
ESTIM FOR INFLAMMATION, EDEMA, SWELLING - CLINICAL APPPLICATION
MONOPOLAR
BIPOLAR
or
10
ESTIM FOR INFLAMMATION, EDEMA, SWELLING - CLINICAL APPLICATION
CLOSER = More superficial
11
IFC – electrode placement
Beattie et al, 2011 12
5
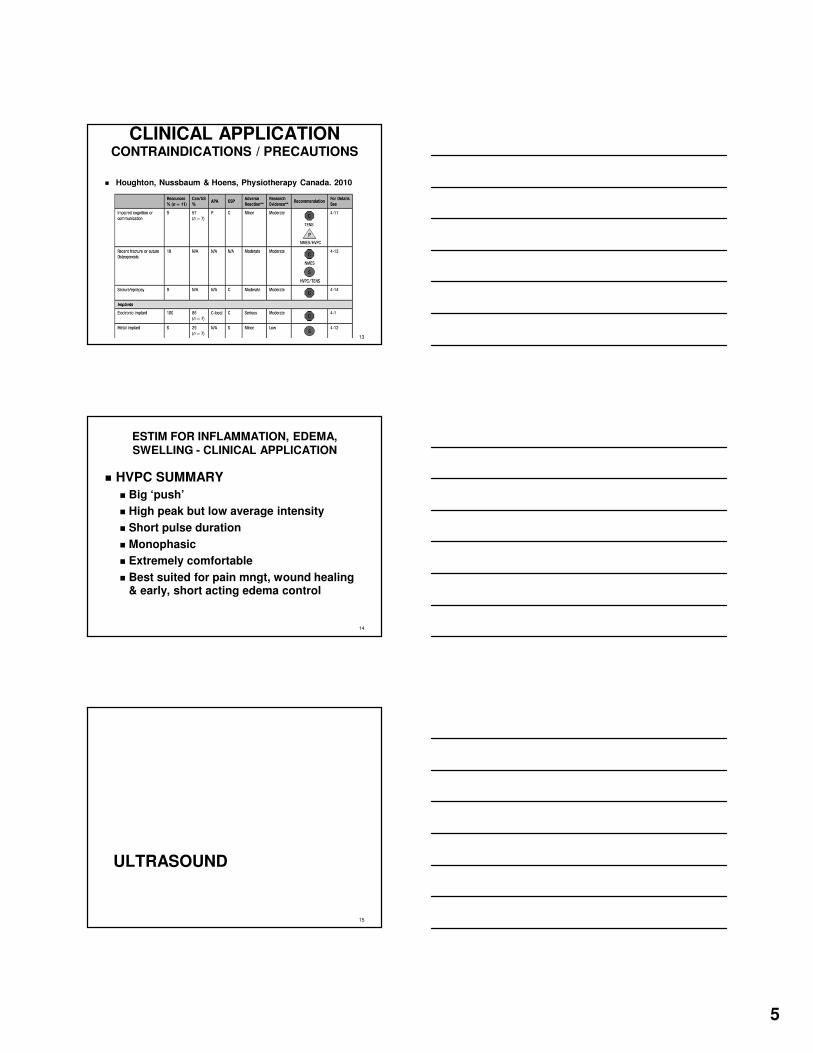
CLINICAL APPLICATIONCONTRAINDICATIONS / PRECAUTIONS
� Houghton, Nussbaum & Hoens, Physiotherapy Canada. 2010
13
ESTIM FOR INFLAMMATION, EDEMA, SWELLING - CLINICAL APPLICATION
� HVPC SUMMARY
� Big ‘push’
� High peak but low average intensity
� Short pulse duration
� Monophasic
� Extremely comfortable
� Best suited for pain mngt, wound healing & early, short acting edema control
14
ULTRASOUND
15

6
ULTRASOUND
For Inflammation, Edema, Swelling
� Physiological Rationale
� US is ‘pro-inflammatory’� Mechanical effects – leading to signalling
events
� Acoustic streaming
� Micro-massage
� Stable cavitation*
� Standing waves*
� Thermal effects
• *It is now believed that unstable cavitation does not occur in mammalian tissue at
therapeutic intensities.• *Stable cavitation and standing waves are
of minimal clinical relevance.
16
Slide courtesy
Dr J Anthony
US Non-thermal effects - molecular
� Increased membrane permeability
� Degranulation of mast cells & histamine release
� Increased transport of Ca++ across cell membrane� Stimulation of protein synthesis
� Release of growth factors & other cytokines
� Stimulus of collagen synthesis (fibroblast proliferation)
17
Slide courtesy
Dr J Anthony
US Absorption
� US is preferentially absorbed by tissues
with a higher protein content.
Figure 12.2 Ranking of musculoskeletal tissues according to their relative absorption of ultrasound energy.
Copyright © 2008 Churchill Livingstone, an imprint of Elsevier Ltd
18
Slide courtesy
Dr J Anthony

7
Ultrasound
� Release of “wound-healing” factors –histamine from mast cells; serotonin from platelets (Fyfe & Chahl 1982, 1984; Williams 1974; Williams et. al. 1976), leading to vasodilation & activation of adhesion molecules
� Probably by altering membrane permeability to Ca++ and other ions (e.g. Mortimer & Dyson 1988, Dinno et. al. 1989)
� This effect may be mechanical in part (Schilcher, 2006)
� Appears to accelerate inflammatory stage to make it as efficient as possible
� Encourages edema to occur more rapidly, then subside more rapidly (Fyfe & Chahl 1985, Hustler 1978)
Slide
courtesyDr J Anthony
US for inflammation/ edema/swelling: Summary
� US works best in tissue that has high
protein (collagen) content
� In early phase of repair, low dose is
effective (eg. Larsen et al, 2005), higher dose can be
counter-productive (Roberts et al, 1982)
� In long-standing STIs, higher US dose
shown to be effective
20
Slide courtesy
Dr J Anthony
Injury Bleeding Inflammatory Phase Proliferation Remodelling
<--------------->
No U/S
<--------------->
Low dose, pulsed, for effect on mast
cells, platelets, phagocytic
leukocytes, macrophages. “Pro-
inflammatory”, but optimizes the
process.e.g. SATA up to
~0.5 Wcm-2
Low dose, pulsed, for effect
on fibroblasts, endothelial cells,
myofibroblasts. “Pro-
proliferative”, but maximizes the
efficiency of the proliferative
phase. e.g. SATA up to ~ 1.5 Wcm-
2
<-----------> <----------->
Higher dose, pulsed -
becoming continuous.
Affects orientation of
collagen fibres in developing
scar. Changes collagen type III
to type I. Up to 2.5 - 3 Wcm-2.
Min. 720 J/session
after Watson, T (2008) Ultrasonics 48; 321-329 and Robertson, Ward, Low & Reed (2006) “Electrotherapy
Explained”, 4th ed. p 288., Alexander LD et al (2010)
Ultrasound is valuable not because it changes the sequence of the healing events, but because it has the capacity to stimulate or enhance normal events
and increase the efficiency of repair phases. (Watson)
21
Slide courtesy
Dr J Anthony

8
US Technique Tips
� Size of area: not greater than 2x sound head� Duration of Rx: 5 – 10 minutes for twice the area of the
treatment head face (= 2.5 – 5 mins for every ERA)
� Calibration of equipment!� studies show that ultrasound equipment is
frequently delivering less energy than expected (see, e.g. Kollmann 2005, Artho 2002, Pye 1996, Rivest 1987)
� US devices should be calibrated at least once per year –more frequently if in constant use
� Calibration is not the same as electrical safety check
22
Contraindications & Precautions
Physiotherapy Canada 62(5), 2010.
Special Issue on Electrophysical Agents.
Houghton PE, Nussbaum EL, Hoens, AM.
23
LOW LEVEL LASER THERAPY
24

9
LASER: Mechanisms
� Photo-biomodulation:� Photo-biostimulation
� Photo-bioinhibition
� Laser photons are absorbed by photosensitive organic molecules (chromophores)
� Chromophores are molecules which absorb light:
� respiratory chain enzymes (e.g. cytochrome-c oxidase; red -near IR)
� hemoglobin, myoglobin; visible red
� water; infra-red
� also non-mitochondrial photoacceptors (e.g. NADPH-oxidase, NO-synthase)
25
Slide modified
fromDr J Anthony
LASER – Mechanism of Action
Photobiomodulation
26
Chung H, et al. Annals of Biomedical Engineering, 2011Slide modified from
Dr J Anthony
LASER Reduces Inflammation
� Reduces prostaglandin E2 concentrations
� Inhibits cyclooxygenase-2 (COX-2) in vitro
� Reduces TNFα
� Enhances local hemodynamics
� Increases cellular oxygenation and mitochondrial ATP
Fulop A, et. al (2010))
27
Slide courtesy
Dr J Anthony

10
LASER: Mechanism cont’d
� Light in the green to red / near IR wavelengths catalyzes the ability of nitric oxide synthase to generate NO, leading to:
� Vasodilation (relaxes vascular smooth muscle)
� Modulation of inflammatory & immune response by inhibiting T- and B-cell diversification and leukocyte recruitment
� Production & regulation of several cytokines, chemokines and growth factors regulating the pro-and anti-inflammatory response (next slide)
� Modulation of angiogenesis (upregulates VEGF)
28
Slide courtesy
Dr J Anthony
Why is NO modulation important?Because of the effect on cytokines & growth factors
Prindeze, 2012
29
Slide modified from
Dr J Anthony
LASER For Inflammation, Edema, Swelling
Clinical Application
� CI/Ps; Goggles for patient and therapist
� Clean lens - check with manufacturer
� Contact is better than non-contact � Apply some pressure on contact
� 904 nm LASER 1-4 J min total dose
� 820 nm LASER 4-16 J min total dose
� Increase dosage for increased pigmentation of skin
30
Slide courtesy
Dr J Anthony

11
LASER Reduces Inflammation
“Red and near infrared LLLT administered
with mean laser output of 2.5–100 mW, irradiation times of 16–600 sec and doses of
0.6–9.6 J reduces inflammation significantly,
and is equally effective as NSAIDs in animal laboratory studies.”
Bjordal J, et al, (2010)
31
Slide courtesy
Dr J Anthony
Contraindications & Precautions
Physiotherapy Canada 62(5), 2010.
Special Issue on Electrophysical Agents.
Houghton PE, Nussbaum EL, Hoens, AM.
32
Therapeutic Application
� Colour
� Red vs. Infra-red
� Dose
� J / point*
� # of points
� Technique
* See handout for calculating Joules if your LASER does not do so automatically
33

12
Further details available: www.walt.nu
34
Further details available: www.walt.nu
35
LASER Technique
� Contact
� Grid
� Point
� Non-contact
� Grid
� Scanning
http://www.lasermedix.com
36

13
LASER Technique Tips
� Contact (with pressure) is preferable to
non-contact
� Clinical relevance of frequency of pulsed
output still unclear
� Current guidelines are < 1 kHz for acute, > 1 kHz for chronic
37
BC LASER Safety GuidelinesHigher Power Laser Safeguards
Higher power health care and industrial lasers, classes 3b (i.e. 5 – 500 mW) and Class 4 (now seen clinically)
• Use in a controlled area.
• Laser eye protection is required.
• Only authorized personnel must occupy the area.
• The area must have an appropriate warning sign.
• Any windows, doorways, openings, etc. must be either covered or restricted
See full details at:
http://www.bccdc.ca/healthenv/Radiation/Lasers/Gnrl_Laser_Guide.htm
38
In Summary
� Evidence to support the use of LASER in
� Pain management
� Wound healing / Scar management
� Inflammation
� Tendinopathy
� Current dosage guidelines appear adequate
39

14
Cryotherapy
40
Take home message: strong evidence that it is effective for pain & mod evidence that it attenuates secondary cell death d/t reducing cell metabolism & neutrophil activity
COLD FOR INFLAMMATION, EDEMA, SWELLING - PHYSIOLOGICAL RATIONALE
� To decrease local metabolism (McAuley, 2001; Merrick, 2002)
*prevent secondary cell death
� Vasoconstriction of cutaneous bvs� Hunting reaction ears, eyes, hands, feet; increase viscosity
& decrease flow but if too intense cooling, increases clotting time (Robertson et al, 2006)
� Decrease blood flow deeper� If cooled sufficiently; bone (Ho et al, 1995); depends on
adipose layer (Myrer et al, 2001)
� Peripheral NS� Immed sensation of cold, then numb then deep ache; decreased
conduction
Up to 48-72 hrs
41
COLD FOR INFLAMMATION, EDEMA, SWELLING - CLINICAL EVIDENCE
� Intermittent applications [10 minutes] may enhance therapeutic effect (Bleakley, 2006)
� excessive cooling can cause greater damage (Collins,
2008) & potentially increase deposition of more fibroblasts -> scar tissue
� NOT WITH CRPS!!!
42

15
COLD FOR INFLAMMATION, EDEMA, SWELLING - CLINICAL APPLICATION
� Ice packs
� layer of warmth within ~ 1 minute. Moving them increases risk of ice burn
� To increase cooling effect
� Immersion > frozen peas & damp towel > ice massage > ice pack > gel pack (Kennet, 2007)
� Caution with compression (Barlas et al, 1996)
� Inspect skin at 1 and 5 minutes
� To decrease cooling effect:
� Layer of insulation (eg. paper towel)
43
COLD FOR INFLAMMATION, EDEMA, SWELLING - CLINICAL APPLICATION
44
COLD FOR INFLAMMATION, EDEMA, SWELLING - CLINICAL APPLICATION
� Cooling for acute inflammation
� Think ‘movement’/ compression/traction for intraarticular swelling
� If there is restricted ROM, after treatment to increase ROM, cool in the lengthened position
� Caution with skilled motor tasks immediately post cooling
45

16
www.electrotherapy.org
Therapeutic Windows for EPAs
Dr. Watson, WCPT 2007
Effective doses
46
What’s happening in RA?
47
T-cells activated & secrete cytokines
T-cells activated & secrete cytokines
B-cells activated & produce cytokines & drive other inflammatory mediators
B-cells activated & produce cytokines & drive other inflammatory mediators
�macrophages in synovium cause damage & produce more pro-inflammatory mediators
�macrophages in synovium cause damage & produce more pro-inflammatory mediators
�bloodflow to joint leaking inflamm mediators into joint
tissues
�bloodflow to joint leaking inflamm mediators into joint
tissues
Redness, tenderness, effusion & heat
Redness, tenderness, effusion & heat
Systemic & local inflammation
Prostaglandins, nitric oxide, matrix metallo.
IL-2, TNF, IL-4
48
PROPOSED MODEL
Mast cell
Macrophage
Efferent sympathetic nerve
Synovial microvessel

17
Clinical Tips
� Swelling� Intraarticular
� Traction/compression
� Extraarticular� Muscle pump / exercise / compression / elevation
� Ice: 10 minute intervals
� US: see chart
� LASER: 904 nm 3.6-4.0 J/cm2
� HVPC: 10 Hz, 20 min, motor intensity
� NMES: 10 Hz 10:10 sec 20 min, motor intensity
� IFC: 10-20 Hz, 20 min, motor intensity
� Caution with suction electrodes
� Quadrapolar set up difficult to justify
� Sponges: dry completely between patients 49
Clinical Tips
� Consider
� Adv of each modality
� Disadv of each modality
� Evidence
� Clinical experience
� Patient preference
50
How do you know that
the Rx worked?
MDC MCID
Pain - NRPS 3 3
Pain - VAS - 13mm for initial scores of </=34mm
- 28mm for initial scores of >/=67mm
Edema/ Swelling –Circumferential measures
>0.5 cm
Edema/ Swelling –Volume
150 mL*
HAQ -0.22
DASH 8-17 (mean 13)
10.2

18
Take Home Messages
52
� Patient-appropriate clinical application
� Use appropriate outcome measures to
monitor effectiveness
� Evidence-informed practice = evidence +
clinical experience + patient values