what’s new for 2008? healthcare engineering consultants does the joint commission manual have...
TRANSCRIPT

What’s New for 2008?
Healthcare Engineering Consultants
Does the Joint Commission Manual Have Major Changes
for 2008?

Organization of the 2008 Accreditation Manual
Healthcare Engineering Consultants
Section 1 - Patient Focused Functions
Ethics, Rights and Responsibilities (RI)
Provision of Care, Treatment and Services (PC)
Medication Management (MM)
Surveillance, Prevention and Control of Infection (IC)
Section 2 - Organization-Focused Functions
Improving Organization Performance (PI)
Leadership (LD) - (includes previous governing body)
Management of the Environment of Care (EC)
Management of Human Resources (HR)
Management of Information (IM)
Section 3 - Clinical Functions
Medical Staff (MS)
Nursing (NR)
No Major Change!Note: Standards rewrite in 2009

What’s New for 2008?
Healthcare Engineering Consultants
What Will the Survey Process be Like in
2008?

Unannounced Surveys in 2008
Healthcare Engineering Consultants
Typical Surveys Include:
Two to five days “on-site”
Two, three or more surveyors (usually nurses
and physicians - includes a “Life Safety Specialist”
for all hospitals in 2008; multiple days for >750K
square feet
Review of documents (survey planning meeting)
Life safety-focused facility tour
Three-part “EC” interview
Questions to staff based on tracer methodology
Summary conference to present tentative findings

Unannounced Surveys in 2008
Healthcare Engineering Consultants
Can Occur Due To:
Regular unannounced survey
Random off-cycle selection (5%)
Sentinel event follow-up
Adverse media coverage of specific issue
Complaint from the public
Note: All new applicants for the accreditation process as well as changes to a new classification (example: critical access designation) will now have unscheduled surveys

What’s New for 2008?
Healthcare Engineering Consultants
What Scoring Rules Apply for 2008?

Joint Commission Scoring Guidelines
Healthcare Engineering Consultants
No major scoring changes for 2008, except SOC:
“EP’s” scored 0, 1 or 2
0 = insufficient compliance
1 = partial compliance
2 = satisfactory compliance
Scoring categories have been continued for each
EP: A, B or C (B may be eliminated later!)
Standards are scored “compliant” or “non-
compliant”
No grid score calculation
Rationale is not scored

Joint Commission Scoring for EP’s
Healthcare Engineering Consultants
Category A: usually used for policies and procedures
or the presence or absence of a requirement
Scored either “0” or “2”
A “2” may become a “1” or “0” if the track record is
insufficient
Category B: used for process requirements
If requirement exists, then process design and
track record is scored (may be eliminated during 2008!)
Category C: instances of non-compliance
Score “2”: 1 or no instances of non-compliance
Score “1”: 2 instances of non-compliance
Score “0”: 3 or more instances of non-compliance

Joint Commission Scoring for EP’s
Healthcare Engineering Consultants
If any “EP” is scored “0”, the standard is
not compliant
If 65% of the EP’s are scored “2”, then
the standard is considered “compliant”,
unless any other EP is scored “0” (up to
35% of the EP’s may be scored a “1”!)

Special Scoring for SOC Deficiencies
Healthcare Engineering Consultants
“X” is considered a minor deficiency Example: a fire door does not latch properly (item 1C2) – Score 1
“Y” is considered a midrange deficiency Example: the same fire door above is missing hardware (item 1C2) – Score 2
“Z” is considered a major deficiency Example: the building is not of an allowable type of construction (item 1A1) or each floor does not have at least two approved exits (item 5A) – Score 4
Note 1: Use the scoring grid and key to determine the X, Y and Z scores; 1-5 total score is partial compliance; 6 or greater is non-compliance, or a “Z” score!
Note 2: Use of the BMP “caps” scores for each category at “1”

Joint Commission Scoring Decisions
Healthcare Engineering Consultants
Accreditation Decision Rules for 2008
Accredited (same)
Provisional Accreditation (same)
Conditional Accreditation (change)
10 or more non-compliant standards (< 100 ADC)
14 or more non-compliant standards (>100 ADC)
Preliminary Denial of Accreditation (change)
14 or more non-compliant standards (<100 ADC)
18 or more non-compliant standards (>100 ADC)
Denial of Accreditation (same)
Preliminary Accreditation (same)

“EC”-Related Scoring Rules
Healthcare Engineering Consultants
Preliminary Denial of Accreditation (PDA)
PDA01 - Immediate threat to health or safety
PDA03 - Falsification of documentation
PDA06 - Non-compliant standards 3 standard
deviations above the mean (14 or 18 RFI’s)
Conditional Accreditation (CON)
CON01 - Non-compliant standards count 2 standard
deviations above the mean (10 or 14 RFI’s)
Note: In 2008, will be 1.5 deviations above the mean
CON03 - Failure to clear repeat non-compliant
standards
CON04 - Delayed PFI or no ILSM’s when required

What’s New for 2008?
Healthcare Engineering Consultants
Which Areas Have Historically Been the
Lowest Scoring?

Lowest Scoring JC Areas
Healthcare Engineering Consultants
Percent Scored Not Compliant for Hospitals
IM.3.10 (44%) – Information management
MM.2.20 (36%) – Medications storage
PC.13.20 (29%) – Operative procedure planning
EC.5.20 (19%) – Compliance with the Life Safety Code
MM.3.20 (19%) – Clear medication orders
IM.6.50 (15%) – Transcription of verbal orders
IM.6.10 (15%) – Complete and accurate medical record
PC.8.10 (14%) – Pain assessment and treatment
PC.2.120 (13%) – Definition of initial assessment time frame
EC1.10 (12%) – Safety management risk assessment

Lowest Scoring “EC” Areas
Healthcare Engineering Consultants
Percent Scored Not Compliant for Other Facilities
Assisted Living – EC.1.5 (33%) Fire prevention planning
Assisted Living – EC.2.2 (33%) Security planning
Assisted Living – EC.2.5 (33%) Fire prevention implementation
Assisted Living – EC.1.4 (33%) Emergency planning
Ambulatory Care – EC.4.10 (19%) Emergency management
Behavioral Health Care – EC.4.10 (10%) Emergency management
Behavioral Health Care – EC.4.20 (5%) Emergency drills
Critical Access Hospital – EC.1.10 (10%) Safety risk management
Critical Access Hospital – EC.7.10 (4%) Utility management
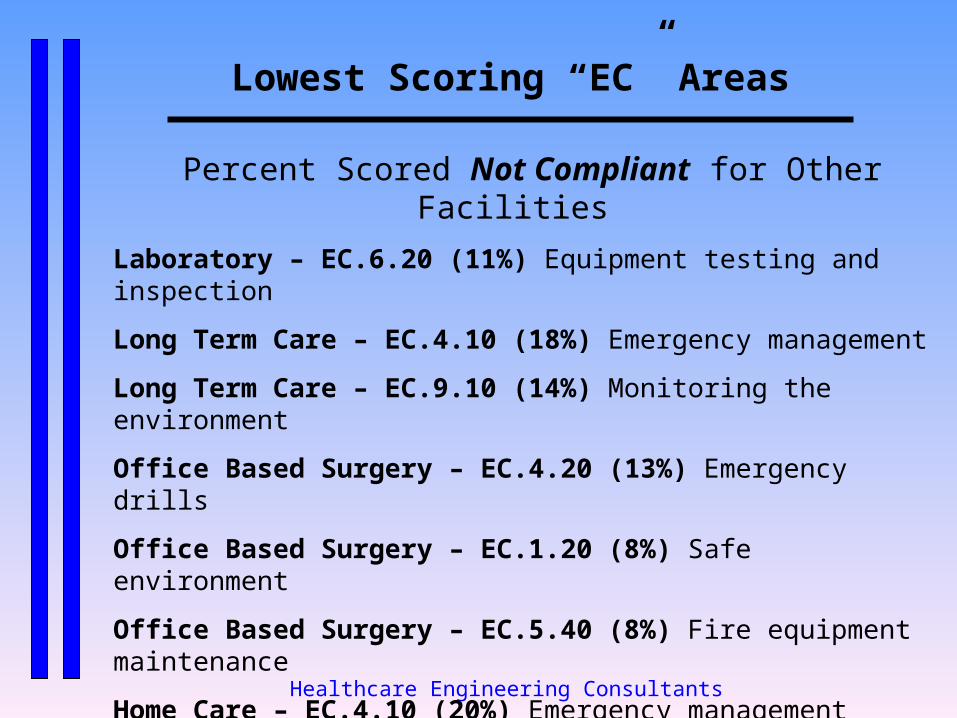
Lowest Scoring “EC” Areas
Healthcare Engineering Consultants
Percent Scored Not Compliant for Other Facilities
Laboratory – EC.6.20 (11%) Equipment testing and inspection
Long Term Care – EC.4.10 (18%) Emergency management
Long Term Care – EC.9.10 (14%) Monitoring the environment
Office Based Surgery – EC.4.20 (13%) Emergency drills
Office Based Surgery – EC.1.20 (8%) Safe environment
Office Based Surgery – EC.5.40 (8%) Fire equipment maintenance
Home Care – EC.4.10 (20%) Emergency management
Home Care – EC.4.20 (10%) Emergency management drills
Home Care – EC.6.60 (7%) Medical equipment testing

What’s New for 2008?
Healthcare Engineering Consultants
What will be the Other Major EC
Changes for 2008?

Possible Change for 2008
Healthcare Engineering Consultants
2006 AIA Document:
Approval voted June, 2005
May be adopted by JCAHO in the future
Available for purchase now! (AIA.org or ASHE.org)
Multiple changes for single rooms, expanded
ICRA, space revisions, HVAC changes, patient
safety language, surge capacity information in
Appendix

Other Changes for 2008
Healthcare Engineering Consultants
Electronic SOC Document
All BBI’s and PFI’s must be electronically entered into
the Joint Commission Connect site
Deadlines: BBI’s: 1/1/07 PFI’s: 9/1/07
Annual submission of SOC with PPR delayed!
Entered data will be “frozen” after approval by surveyor
PFI entries should be continuous
Password for organization will be required for data entry
Actual completion dates must be entered as they occur
Be sure to fill out forms, even if “No Deficiencies” on PFI
Download the data and put “hard copy” in notebook

Other Changes Continued for 2008
Healthcare Engineering Consultants
Electronic SOC Document PPR process will now include questions about the e-SOC
No longer “busted plan” – now termed “Non-Compliant”
e-SOC will track when completion dates are changed prior
to approval by surveyor
PFI’s completed beyond 6 months of intended date may be
cited under: EC.5.20, LD.2.20, LD.3.80 or LD.4.50
Can delete buildings on BBI, but not sites!
PFI summary uses the following colors:
- Yellow for 4 months beyond intended completion date
- Orange when beyond the 6-month grace period
- Salmon when PFI completed after 6 months of intended date

Other Changes Continued for 2008
Healthcare Engineering Consultants
Generator Run Tests (EC.7.40) 4-hour run at greater than 30% of nameplate load every three years; first due 7/1/07
Load test should be dynamic (actual hospital load), although the Joint Commission will accept load bank tests
Any 4-hour @ 30% load test since July 1, 2004 will count and the next test will not be required until the 3-year anniversary date
Test failure requires interim measures until repairs are completed; successful retest is required after initial failure
All other existing generator tests still required; reference NFPA 110, 2005 edition
Simultaneous monthly, annual load bank and trienniel tests will count, as long as first 30 minutes are at 30%, rather than 25% of load (NFPA 70 panel does not yet agree!)

Expectations for 2008
Healthcare Engineering Consultants
Sentinel Event Alert #37 Recommendations
Perform emergency power system gap analysis
Maintain complete, labeled, accurate inventory of loads served by the emergency power system (EPS)
Ensure competency training of staff who are responsible for the testing and maintenance of the EPS
Test generator fuel oil on an annual basis and filter or replace, as necessary
Communicate EPS capabilities and limitations to clinical staff and hospital management
Establish clinical contingency plans in the event of brief or prolonged failure of the EPS

Other Changes for 2008
Healthcare Engineering Consultants
Operational Damper Tests
Re-inspection now every six rather than four years in hospitals; other occupancies still four years per NFPA
Change effective January 1, 2008
Result of move from NFPA 90A to NFPA 80 (fire dampers) and NFPA 105 (smoke dampers), the 2007 editions
For smoke dampers, the inspection shall occur one year after installation and then on a six-year basis
Inaccessible dampers should be placed on the PFI form and given a 6-year time period for completion; completion date can be extended after the 6-year period has expired
Emergency ManagementEMERGENCY
Healthcare Engineering Consultants
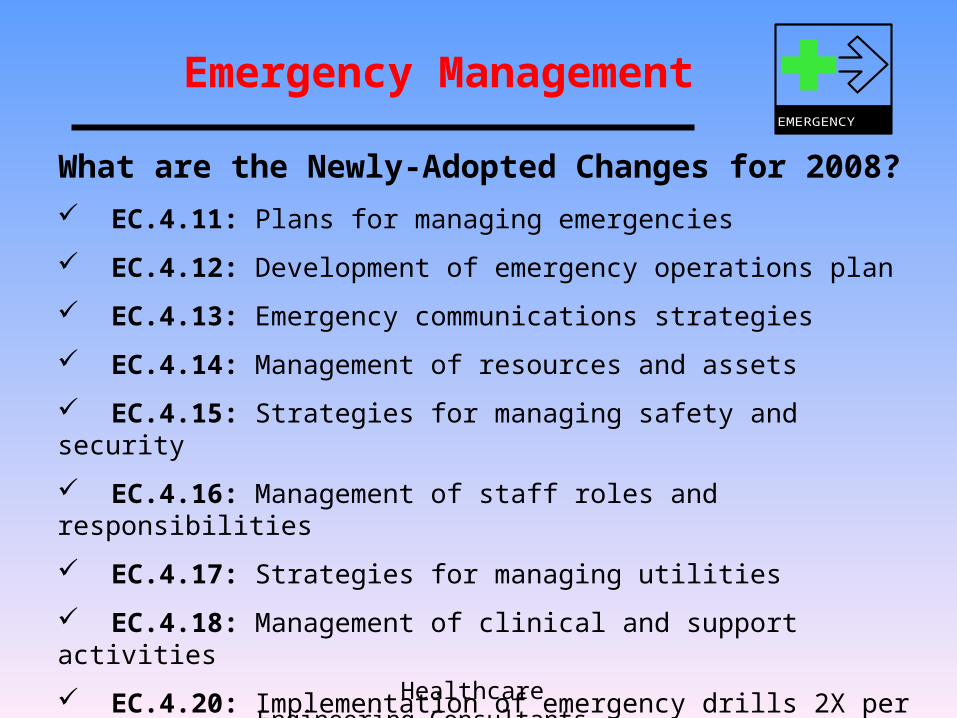
What are the Newly-Adopted Changes for 2008? EC.4.11: Plans for managing emergencies
EC.4.12: Development of emergency operations plan
EC.4.13: Emergency communications strategies
EC.4.14: Management of resources and assets
EC.4.15: Strategies for managing safety and security
EC.4.16: Management of staff roles and responsibilities
EC.4.17: Strategies for managing utilities
EC.4.18: Management of clinical and support activities
EC.4.20: Implementation of emergency drills 2X per year
Note: One drill requires external “non-support” simulation

Top “EC” Focus Areas for 2008
Healthcare Engineering Consultants
Patient Safety
Infection Control
Emergency Management
(Katrina impact – 2008 changes)
Life Safety (life safety specialist
surveyor change)
Risk Assessment

“EC”-Related Patient Safety Goals for 2008
Healthcare Engineering Consultants
For Ambulatory, Behavioral Health, Home Care and Hospital Facilities
Add Goal #13: Encourage patient’s active involvement in their own care as a patient safety strategy (define and communicate the means for patients and families to report safety concerns)
Add Goal #15: The organization identifies safety risks inherent in its patient population (identify suicide risk – relates to patients being treated for emotional and behavioral disorders)
What’s New for 2008?
Healthcare Engineering Consultants
What Other Chapters in the Manual Will Impact
EC in 2008?

Organizational Function Overview
Healthcare Engineering Consultants
Human Resources (HR)
Staff training, competency and performance
Leadership (LD)
Compliance, resources, patient safety (LD.3.50,
oversight of contracts/ services; 7/1/07)
Performance Improvement (PI)
Data collection, aggregation, analysis , action
Information Management (IM)
Data collection, aggregation, security
Infection Control (IC)
Measurement and reduction of infections

What’s New for 2009?
Healthcare Engineering Consultants
What will the EC Chapter look like
in 2009?

The 2009 EC Chapter
Healthcare Engineering Consultants
What will be the major EC changes?
Mostly editorial changes
Emergency management and life safety (not fire safety) will have their own chapters
Staff competency (including for clinical staff) will be returned to the EC chapter
Safety and security will be combined into one standard
An entirely new numbering system will be used

Numbering the EC Standards
Healthcare Engineering Consultants
EC.1.01 – Management Plan Requirements
EC.2.01, 2.03 – Safety and Security
EC.3.01 – Hazardous Materials and Wastes
EC.4.01 through 4.04 – Fire Safety
EC.5.01, 5.02 – Medical Equipment
EC.6.01 through 6.05 – Utilities Management
EC.7.01, 7.03 – Other Physical Environment
EC.8.01 – Staff Competency
EC.9.01 through 9.03 – Monitoring, Improvement

Understanding the Four “EC” Vulnerabilities
Healthcare Engineering Consultants
What are the Four Survey Points of EC
Vulnerability for 2008?

The Four Survey Points of Vulnerability
Healthcare Engineering Consultants
The Survey Planning Session
LSC Facility Tour
The “EC” Interview Session
Involves all seven EC areas
Documents and staff must be available
Consists of three phases
“EC” Tracers
The Four “EC” Vulnerabilities
Healthcare Engineering Consultants
What is the Expectation Triad?

The Expectation Triad
Healthcare Engineering Consultants
Regulatory Compliance
Performance
ImprovementRisk Assessment

The Expectation Triad
Healthcare Engineering Consultants
Regulatory Compliance:
“Ensuring that all of the required
standards are being met”

The Expectation Triad
Healthcare Engineering Consultants
Performance Improvement:
“Attempting to measure and
improve performance on an
ongoing basis in the
Environment of Care”

The Expectation Triad
Healthcare Engineering Consultants
Risk Assessment:
“Prioritization and management
of resources through an
assessment of probability
and impact”