what's new in the 2nd edition?
TRANSCRIPT
What's New In The 2nd Edition?

Disclosure Statement• Faculty:
• Jill Boulton• Kevin Coughlin• Deepak Manhas
We have no affiliation (financial or otherwise) with a pharmaceutical, medical device or communications organization

Our Thanks To:
• Co Editors ACoRN 2021:• Jill Boulton• Kevin Coughlin• Debra O’Flaherty• Alfonso Solimano
• Major Contributors:• Debbie Aylward• Deepak Manhas• Elene Vanderpas
• French Edition Contributors:• Ahmed Moussa• Genevieve Piuze
• ACoRN Steering and Education Committee Members
• Many many other contributors and reviewers
• Tireless ACoRN instructors in Canada and around the world
• CPS Staff• Jackie Millette• Keisha Powell• Jennifer Strickland

Agenda
• The history of ACoRN• Highlight what’s new in the second edition• Present the ACoRN educational approach• Discuss what’s next?
• Provincial and regional launches• CPS Practice Point

The historyof ACoRN
Jill Boulton, MD

From NRP Steering Committee breakfastat CPS annual meeting, Winnipeg 1999…
X 3
2015

I think I get it
Explain How that works again ?
Huntsville 1999
Calgary 2003

Problem List Respiratory Cardiovascular Neurology Surgical conditions Fluid & glucose Thermoregulation Infection
Support
Respiratory Laboured respiration* Respiratory rate > 60/min* Receiving respiratory support*
Surgical Conditions Anterior abdominal wall defect Vomiting or inability to swallow Abdominal distension Delayed passage of meconium or imperforate anus
Thermoregulation T < 36.3 or > 37.2ºC axillary* Increased risk for temperature instability
Fluid & Glucose Management Blood glucose < 2.6 mmol/L At risk for hypoglycemia Not feeding or should not be fed
Neurology Abnormal tone* Jitteriness Seizures*
Cardiovascular Pale, mottled, or grey* Weak pulses or low BP* Cyanosis unresponsive to O2 Heart rate > 220 bpm
Baby at risk Unwell Risk factors Post-resuscitation requiring stabilization
Sequences
Resuscitation Ineffective breathing Heart rate < 100 bpm Central cyanosis
Infection Risk factor for infection ACoRN alerting sign with * Clinical deterioration
Consider transport
7
2012 2021

• Remains prioritized based around Primary Survey
• Updates to clarify, add missing information asked for (i.e. HIE management, neural tube defects and jaundice)
• Sequences maintain same structure ‘ACORNS’
• Two new chapters:• Transition• Jaundice
*
**
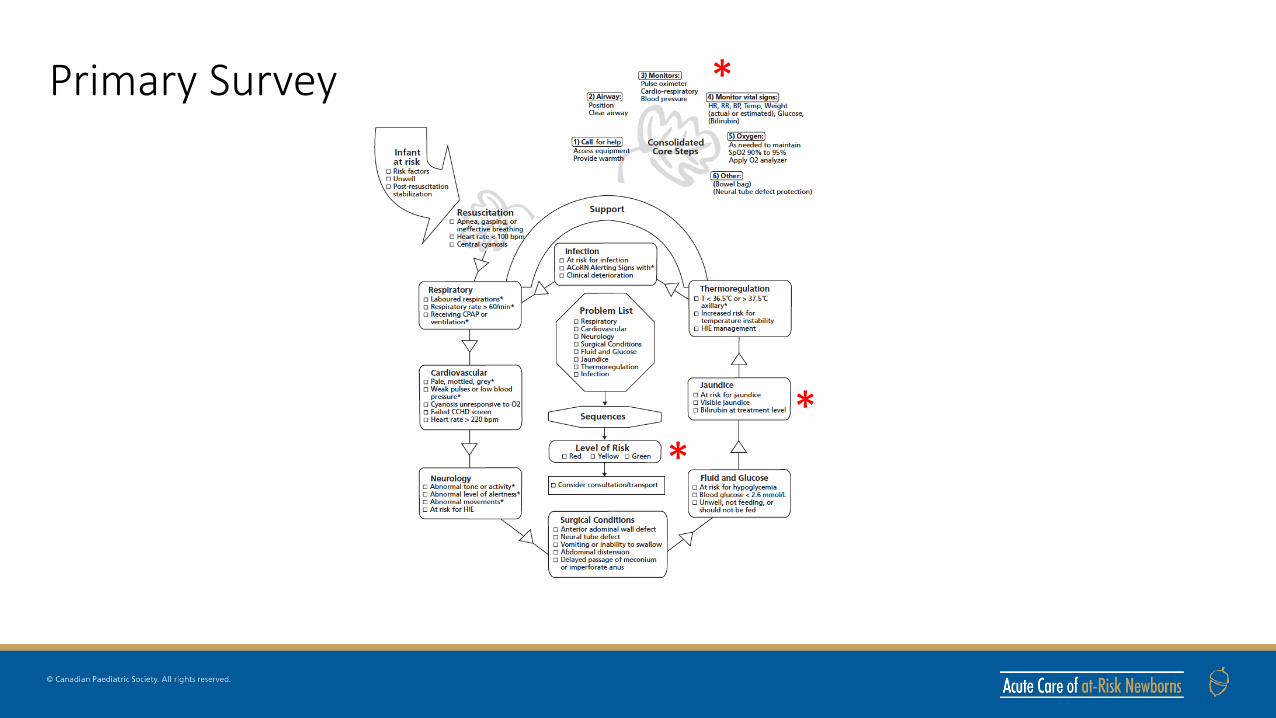
Primary Survey

Consolidated Core Steps
• Creation of the Consolidated Core Steps (CCS) to better fit with actual practice and decrease repetition between sequences
• CCS are now performed in parallel with the Primary Survey by a second ACoRN provider

• Level of Risk identification:
• Consider consultation/transport

*
*
*
*
**
*
*
Alerting Signs

• 7 new, 7 altered Alerting Signs:Sequence New Alerting Sign ReplacesResuscitation Apnea, gasping or ineffective
breathingIneffective breathing
Respiratory Receiving CPAP or ventilation* Receiving respiratory support
Cardiovascular Failed CCHD screen
Neurology Abnormal tone or activity*Abnormal level of alertness*Abnormal movements*At risk for HIE
Abnormal tone*
Jitteriness/ Seizures*
Surgical Conditions Neural tube defect
Fluid & Glucose Unwell, not feeding, or should not be fed
Not feeding or should not be fed
Jaundice At risk for jaundiceVisible jaundiceBilirubin at treatment level
Thermoregulation T<36.5℃ or > 37.5℃ axillary*HIE management
T<36.3℃ or > 37.2℃ axillary*

Chapters
• Critical knowledge and physiology points at start of each chapter rather than presented in cases
• Useful tools for many of the sequences • Cases continue to illustrate flow through the ACoRN Process and
Level of Risk determination

• Reorganized with most acute/serious condition on the far left
• Some additional qualifiers to alter Organization of Care after Core Steps (e.g. glucose level in Neurology Sequence)
Sequences

• No significant change to Next Steps• Still point where you exit the
sequence on first run through to address next item on Problem List
• Consider the Level of Risk for each sequence
• Patients final level of risk is highest achieved in any sequence
Sequences

What's new in the 2nd edition?
Kevin Coughlin, MD

Orientation to ACoRN Sequences
• Overall flow and structure of the sequences has not changed
• Streamlined the Core Steps• Re-organized Organization of Care so
most urgent is to the left of the sequence
• First exit still at Next Steps• Addition of Level of Risk assessment for
each sequence

Resuscitation
• Simplified• In line with ILCOR/NRP

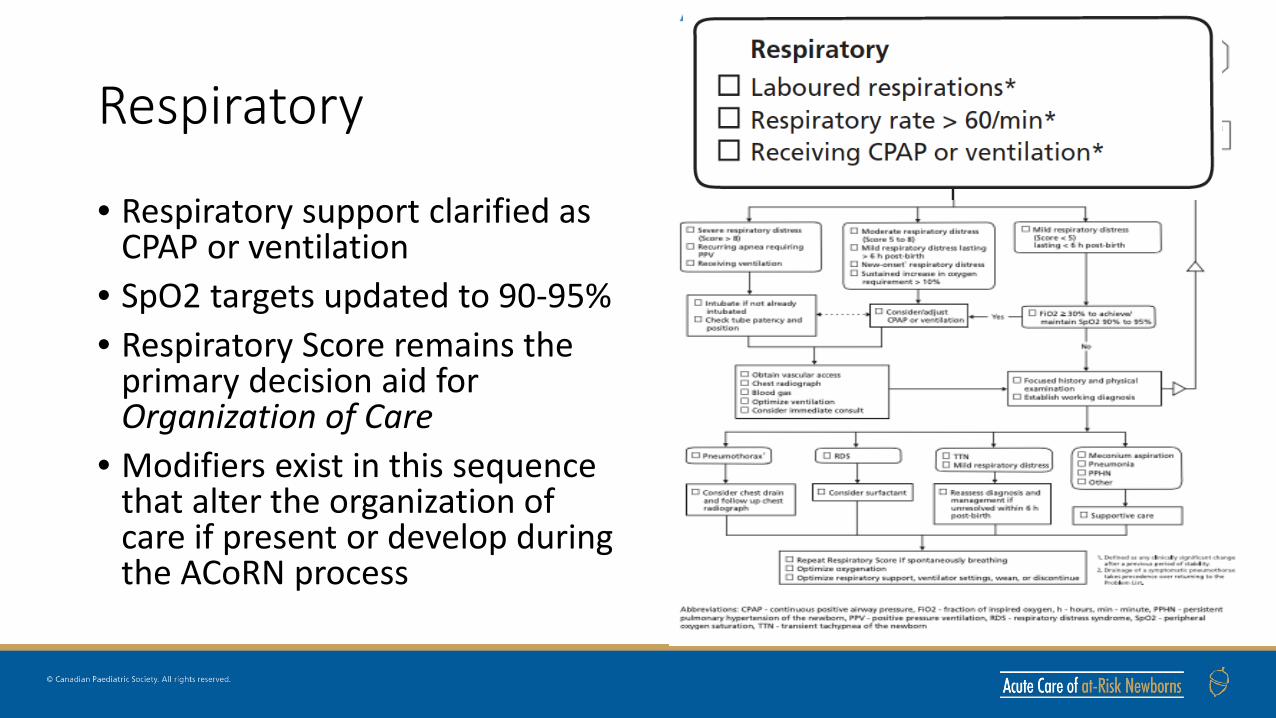
Respiratory
• Respiratory support clarified as CPAP or ventilation
• SpO2 targets updated to 90-95%• Respiratory Score remains the
primary decision aid for Organization of Care
• Modifiers exist in this sequence that alter the organization of care if present or develop during the ACoRN process
Respiratory
• Respiratory support clarified as CPAP or ventilation
• SpO2 targets updated to 90-95%• Respiratory Score remains the
primary decision aid for Organization of Care
• Modifiers exist in this sequence that alter the organization of care if present or develop during the ACoRN process

Respiratory
• Respiratory support clarified as CPAP or ventilation
• SpO2 targets updated to 90-95%• Respiratory Score remains the
primary decision aid for Organization of Care
• Modifiers exist in this sequence that alter the organization of care if present or develop during the ACoRN process

Respiratory
• Respiratory support clarified as CPAP or ventilation
• SpO2 targets updated to 90-95%• Respiratory Score remains the
primary decision aid for Organization of Care
• Modifiers exist in this sequence that alter the organization of care if present or develop during the ACoRN process

Core Steps: Respiratory Score
• No major changes to previous respiratory score

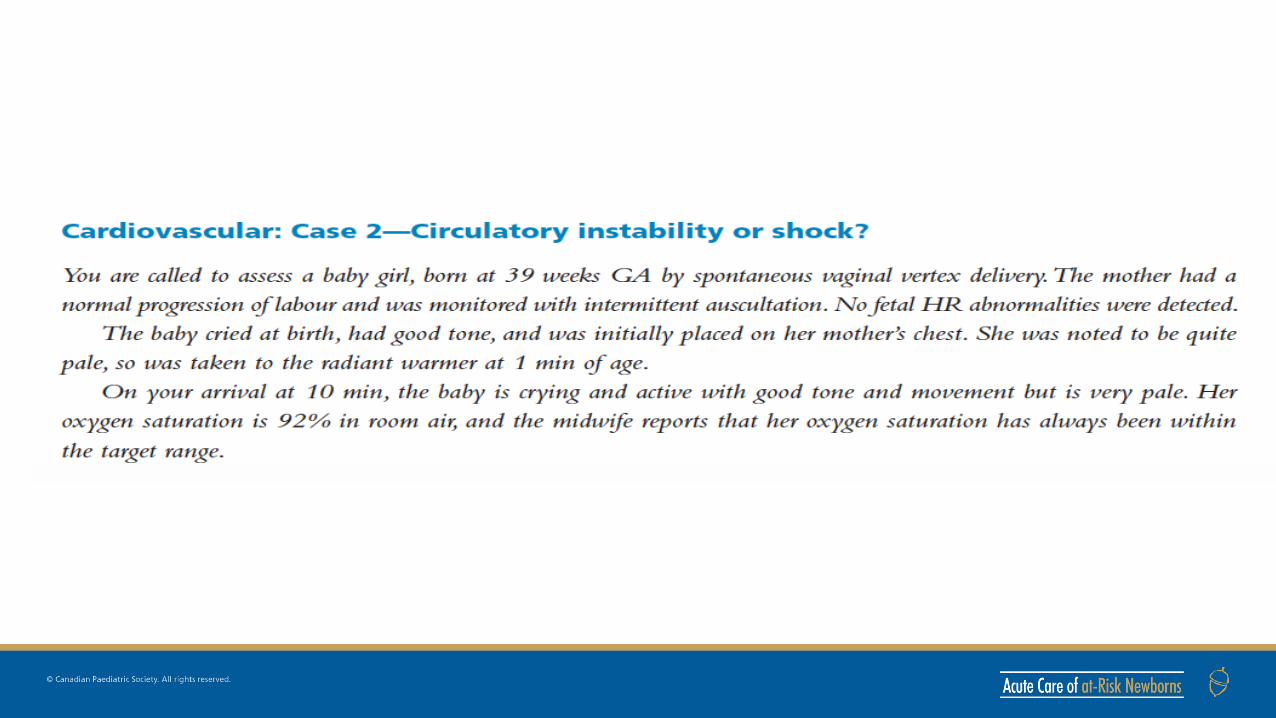
Cardiovascular
• Added failed CCHD screen• Clinical Assessment of Circulation
table is primary decision aid for Organization of Care
• Differentiation of shock vs circulatory instability without shock

Cardiovascular
• Added failed CCHD screen• Clinical Assessment of Circulation
table is primary decision aid for Organization of Care
• Differentiation of shock vs circulatory instability without shock

Cardiovascular
• Added failed CCHD screen• Clinical Assessment of Circulation
table is primary decision aid for Organization of Care
• Differentiation of shock vs circulatory instability without shock

Cardiovascular
• Added failed CCHD screen• Clinical Assessment of Circulation
table is primary decision aid for Organization of Care
• Differentiation of shock vs circulatory instability without shock

Core Steps: Clinical Assessment of Circulation

Neurology• Updated Alerting Signs including
abnormal level of consciousness and ‘At risk for HIE’
• Encephalopathy Assessment table and initial glucose level are primary decision aids for Organization of Care
• Goals: early recognition and treatment of symptomatic hypoglycemia, seizures and HIE
• Includes direction for HIE management

Neurology• Updated Alerting Signs including
abnormal level of consciousness and ‘At risk for HIE’
• Encephalopathy Assessment table and initial glucose level are primary decision aids for Organization of Care
• Goals: early recognition and treatment of symptomatic hypoglycemia, seizures and HIE
• Includes direction for HIE management

Neurology• Updated Alerting Signs including
abnormal level of consciousness and ‘At risk for HIE’
• Encephalopathy Assessment table and initial glucose level are primary decision aids for Organization of Care
• Goals: early recognition and treatment of symptomatic hypoglycemia, seizures and HIE
• Includes direction for HIE management

Neurology• Updated Alerting Signs including
abnormal level of consciousness and ‘At risk for HIE’
• Encephalopathy Assessment table and initial glucose level are primary decision aids for Organization of Care
• Goals: early recognition and treatment of symptomatic hypoglycemia, seizures and HIE
• Includes direction for HIE management

Core Steps: Encephalopathy Assessment Table

Surgical Conditions
• Addition of open neural tube defect to

Fluid & Glucose
• Sequence is harmonized with CPS statement on hypoglycemia management
• Balanced between appropriate treatment and maintaining breast feeding

Fluid & Glucose
• Introduces simplified GIR calculation and maximal recommended fluid intakes to avoid dilutional hyponatremia
• Stepwise treatment recommendations

Fluid & Glucose
• Introduces simplified GIR calculation and maximal recommended fluid intakes to avoid dilutional hyponatremia
• Stepwise treatment recommendations

Jaundice Sequence
• New sequence to ACoRNintroduced at providers’ request
• 3 new Alerting Signs• Core Step involved plotting
bilirubin values on standardized curves
• Organization of Care depends on plotted results

Jaundice Sequence
• New sequence to ACoRNintroduced at providers’ request
• 3 new Alerting Signs• Core Step involved plotting
bilirubin values on standardized curves
• Organization of Care depends on plotted results

Jaundice Sequence
• New sequence to ACoRNintroduced at providers’ request
• 3 new Alerting Signs• Core Step involved plotting
bilirubin values on standardized curves
• Organization of Care depends on plotted results

Jaundice Sequence
• New sequence to ACoRNintroduced at providers’ request
• 3 new Alerting Signs• Core Step involved plotting
bilirubin values on standardized curves
• Organization of Care depends on plotted results

Thermoregulation
• Updated temperature range: 36.5-37.5℃
• Added HIE management as both an Alerting Sign and Response

Thermoregulation
• Updated temperature range: 36.5-37.5℃
• Added HIE management as both an Alerting Sign and Response

Infection Sequence
• Alerting Signs remain the same• Reorganized based on the
Infection Assessment Table• Additional information in the
chapter on common organisms causing EOS and LOS, biomarkers, non-bacterial causes of infection

Core Steps: Infection Assessment Table

The ACoRN ProgramAdditional Tools & Resources:• Additional resource and tables
in the textbook & appendices• ACoRN: The Essential Guide• The ACoRN Workbook• ACoRN Simulations• ACoRN Key Concepts• ACoRN Skills

Resources for the ACoRN Instructor/Provider
• ACoRN: The Essential Guide• ’coles notes’ version of the text• forms essential materials in the
reading lists we used to provide to those coming to an ACoRN course
• meant to supplement the textbook
• option for those providers who use an institutional library copy of the textbook

Resources for the ACoRN Instructor/Provider
• The ACoRN Workbook• Replaces the laminates used
in the past• Useful in the moment
• Include primary survey & consolidated core steps, sequences, core steps and useful tools to navigate the ACoRN process
Resources for the ACoRN Instructor/Provider
• ACoRN Key Concepts• Brief 30 min talks• Outline key learning concepts• Developed/used based on need• Anchors within the course agenda
• Examples:• ACoRN 2nd Edition Updates• Key Concepts of Transition• Key Concepts of Neurology Sequence• Key Concepts of Fluid & Glucose
Sequence

Resources for the ACoRN Instructor/Provider
• ACoRN Simulations• Key component of the ACoRN
program• Series of purpose-built simulation
scenarios to help instructor navigate ACoRN providers through learning the process
• 9-10 developed to date• Template will be available to
instructors to develop your own

Resources for the ACoRN Instructor/Provider
• ACoRN Skills • Yet to be developed• Many can be reused from past
edition• Targeted to course/provider based
on need• Chest Radiograph Interpretation• Vascular Access (IO/UVC)• Needle Thoracocentesis• Chest Tube Insertion• Blood Gas Interpretation• CBCD Interpretation

ACoRN educational approachDeepak Manhas, MD

Educational Supplements
• Updated Textbook Cases• Pre-Test• Draft Agenda• Workbook• Laminates• Simulation Scenarios
• Case• Equipment and Images• Debriefing
• Demo Video














ACoRN Workbook
• ACoRN Algorithms• ACoRN Tables• Level of Risk






Demo simulation video coming soon to [email protected]

Administration of ACoRN in Canada
Kevin Coughlin, MD

ACoRN Providers and Instructors
• Will follow a process similar to NRP• 3-year renewal process• Online exam prior to attending a course• Requirement for teaching to maintain status as Instructor
• ACoRN is meant to be taught in a multidisciplinary team• Within the teaching team, the content knowledge and skills must be present
to teach the entire core content of the ACoRN course
• Current ACoRN Instructors who have taught within the last 3 years (before COVID) will be eligible for update and renewal of status
ACoRN Courses
• Flexibility in how ACoRN is taught• There will be clearly identified core content that is necessary for a
complete course• Additional materials will be provided for Instructors to use as add on
modules based on a site/provider groups’ needs
• Instructor resources including “Key Concepts” videos, Simulation and Debrief guides etc will be on the Instructor side of the ACoRN website

Newborn Stabilization in Canada
• It is recognized that newborn stabilization skills are variable across the country.
• CPS Practice Point in process identifying the need for a standard stabilization program (similar to NRP) across the country.
ACoRN: The Vision
• ACoRN 2nd Edition is an update of the already fabulous ACoRN Program• Move to more of a simulation-based content delivery• Increased interactive nature with participant driven learning through
simulation, debrief and reflection• Standardization and support of educational quality through the Key
Concepts anchoring talks and Simulation Scenarios• Increased flexibility in design and delivery of the content
• Modular components with identified ‘Core Content’ and additional resources available to Instructors as needed based on site/learners needs
• Evaluation and assessment through online pretest and participation in simulations
Implementation Across the Country
• Rolling out the new edition has been complicated by COVID• The change to increase the hands on, intensively simulation-based
group learning nature of the 2nd edition pedagogy in this environment is further complicating things
• Plan to reach out to each Regional/Provincial body to see how we can best support Instructor updates and roll out of the 2nd edition in the early fall.
• We welcome your thoughts on how this can best be done
ACoRN: The Vision• Goal today: to highlight the newly developed content for you, a group
of experienced ACoRN Instructors/Providers
• We welcome feedback on things that you think will work and opportunities for improvement
• We thank you, in advance, for your participation!
Questions and Comments?