what’s the big idea? harvey skinner dean, faculty of health, york university university of calgary...
Post on 19-Dec-2015
213 views
TRANSCRIPT

What’s The BIG Idea?What’s The BIG Idea?Harvey SkinnerHarvey Skinner
Dean, Faculty of Health, York Dean, Faculty of Health, York UniversityUniversity
University of Calgary April 16, 2008
local
global

Today’s Dialogue ObjectivesToday’s Dialogue Objectives
1.1. The ChallengeThe Challenge Designing for after the health care system Designing for after the health care system
implodesimplodes
2.2. The BIG Idea: The BIG Idea: “first Health, then Medicine”“first Health, then Medicine” keeping more people healthier longerkeeping more people healthier longer
3.3. The OpportunityThe Opportunity your fresh thinking for changeyour fresh thinking for change
What is the BIG idea?What is the BIG idea?


The BIG IdeaThe BIG Idea““first Health, then Medicine”first Health, then Medicine”
Fresh thinking and action
for
Keeping more people healthier longer
by
Co-Creating the Total Health System

Planning Quagmire

Ten Great Achievements of Ten Great Achievements of Public Health in 20th CenturyPublic Health in 20th Century
vaccinationvaccination motor-vehicle safetymotor-vehicle safety safer work placessafer work places control of infectious diseasescontrol of infectious diseases prevention of heart disease and strokeprevention of heart disease and stroke

Ten Great Achievements of Ten Great Achievements of Public Health in 20th CenturyPublic Health in 20th Century
safer and healthier foodssafer and healthier foods healthier mothers and babieshealthier mothers and babies family planningfamily planning fluoridation of drinking waterfluoridation of drinking water tobacco recognition and preventiontobacco recognition and prevention

Policies and Components

Ten Great Achievements of Ten Great Achievements of Public Health in 20th Public Health in 20th CenturyCentury
Added Added 25 Years+25 Years+ to Life to Life Expectancy of People in North Expectancy of People in North AmericaAmerica
BUT

Obesity Trends* Among U.S. AdultsBRFSS, 1990
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14%
Behavioral Risk Factor Surveillance System (BRFSS)

Obesity Trends* Among U.S. AdultsBRFSS, 1991
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19%

Obesity Trends* Among U.S. AdultsBRFSS, 1993
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19%

Obesity Trends* Among U.S. AdultsBRFSS, 1992
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19%

Obesity Trends* Among U.S. AdultsBRFSS, 1994
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19%
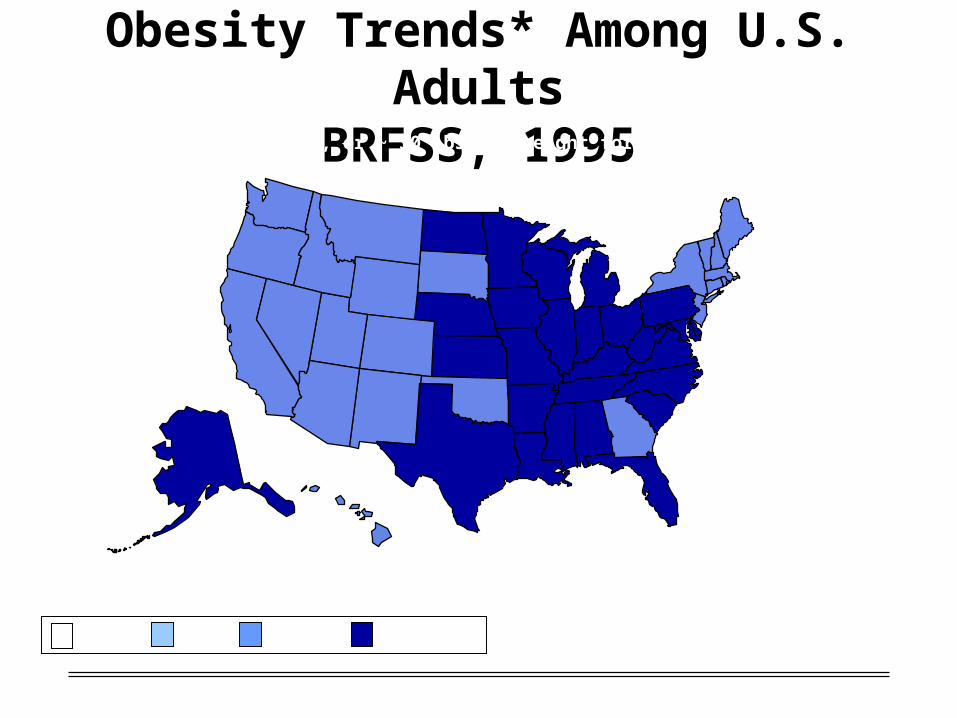
Obesity Trends* Among U.S. AdultsBRFSS, 1995
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19%

Obesity Trends* Among U.S. AdultsBRFSS, 1996
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19%

Obesity Trends* Among U.S. AdultsBRFSS, 1997
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% ≥20%

Obesity Trends* Among U.S. AdultsBRFSS, 1998
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% ≥20%

Obesity Trends* Among U.S. AdultsBRFSS, 1999
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% ≥20%

Obesity Trends* Among U.S. AdultsBRFSS, 2000
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% ≥20%

Obesity Trends* Among U.S. AdultsBRFSS, 2001
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% 20%–24% ≥25%

(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
Obesity Trends* Among U.S. AdultsBRFSS, 2002
No Data <10% 10%–14% 15%–19% 20%–24% ≥25%

Obesity Trends* Among U.S. AdultsBRFSS, 2003
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% 20%–24% ≥25%
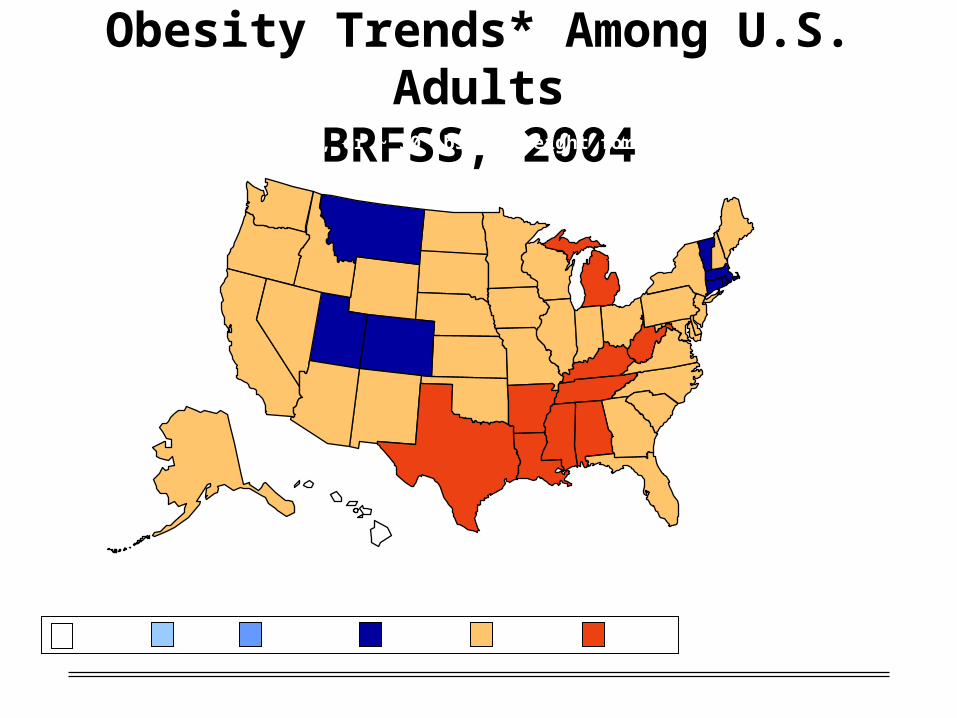
Obesity Trends* Among U.S. AdultsBRFSS, 2004
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% 20%–24% ≥25%

Obesity Trends* Among U.S. AdultsBRFSS, 2005
(*BMI ≥30, or ~ 30 lbs overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%

Obesity Trends* Among U.S. AdultsBRFSS, 2006
(*BMI ≥30, or ~ 30 lbs. overweight for 5’ 4” person)
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%
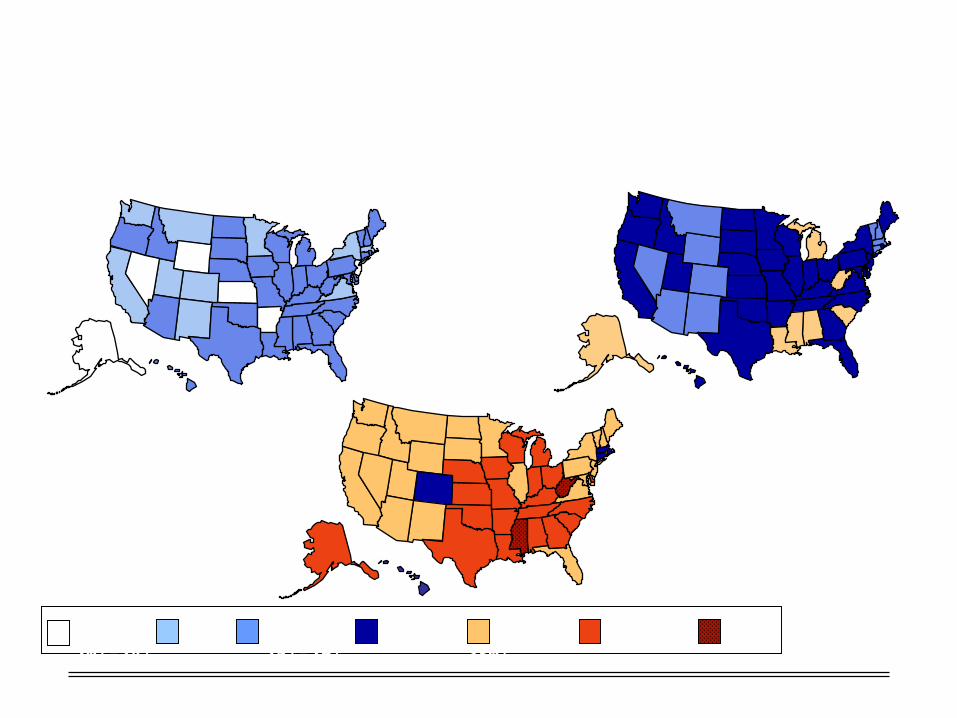
1998
Obesity Trends* Among U.S. AdultsBRFSS 1990 - 1998 - 2006
(*BMI 30, or about 30 lbs. overweight for 5’4” person)
2006
1990
No Data <10% 10%–14% 15%–19% 20%–24% 25%–29% ≥30%

Obesity in Canadian AdultsCCHS 2004 (measured data)

Excess weight (BMI 25) in youth (2-17)Canada, 2004 (measured data)(% Obesity)
(7%) (8%)
(10%)(9%)
(9%)(7%)
(17%)
(13%)(9%)
(8%)

Childhood ObesityChildhood Obesity

25-3435-44
45-5455-64
65+
Can-M
Can-F
FN-M
FN-F
0
5
10
15
20
25
30
35
40
45
%
Age
Diabetes: First Nations to the Canadian Population,Age-gender-specific prevalence (%)
(Source: RHS 2002/03 & CCHS 2001)
Can-M
Can-F
FN-M
FN-F

Cuba’s ‘Natural Experiment’
Cuba’s economic crisis of 1989-2000 resulted in reduced energy intake, increased physical activity, population wide weight loss and reduction in chronic diseases
Reduced daily energy intake from 2,899 to 1,863 calories Physical activity in adults increased from 30% to 67% 1.5 unit shift down in body mass – obesity declined from 14% to 7% Decline in deaths attributed to
Diabetes: 51% Coronary heart disease: 35% Stroke: 20% All causes: 18%
Franco et al. Am J Epidemiology, 2007

Ontario Budget ExpenditureOntario Budget Expenditureon Health Careon Health Care
32 % of Ontario budget ten years ago32 % of Ontario budget ten years ago
46% today46% today
75% by 202375% by 2023
100% by mid-2030s100% by mid-2030s
Based on 2004 budget projections

Ontario Government Ontario Government ExpendituresExpenditures
$$79.3 billion in fiscal year ending March 31, 79.3 billion in fiscal year ending March 31, 20072007
35.7 billion: Health35.7 billion: Health
12.1 billion: Education12.1 billion: Education
10.4 billion: Children & Social Services10.4 billion: Children & Social Services
9.8 billion: Environment9.8 billion: Environment
5.4 billion: Post-Secondary5.4 billion: Post-Secondary
3.2 billion: Justice3.2 billion: Justice
2.7 billion: Transportation2.7 billion: Transportation

Globe and Mail headlineApril 7, 2008
B.C. intent on tackling issue of funding in health care
Province to defy Ottawa by enshrining fiscal sustainability in medicare laws
Health Minister struggling
B.C. Health Minister George Abbott wants to make fiscal sustainability a founding principle of health-care delivery, a measure flatly rejected by his federal counterpart, Tony Clement.
"We will continue to embrace the five principles of the Canada Health Act," Mr. Abbott said in an interview. "We believe we should enshrine sustainability as a principle as well."

a framed statement of values
Mr. Abbott said the province has to grapple with escalating costs that are threatening program spending in other areas
Health-care spending currently consumes about 44 per cent of the provincial budget. He said that by 2013 it is expected to chomp through fully half of all B.C. government spending. "Government needs to be conscious of the fact that we have 20 other areas of ministerial responsibility and service delivery besides health care"

Critics worry that the sustainability principle will push B.C. toward more privatized health-care services
"Adding a sixth principle to the Canada Health Act is opening the door to look at health care through a financial lens for the first time in history," said Leslie Dickout, a campaigner for the B.C. Health Coalition, a group that champions the protection and expansion of universal health care.

The Challenges are The Challenges are LargeLargebut not Insurmountablebut not Insurmountable

The BIG IdeaThe BIG Idea““first Health, then Medicine”first Health, then Medicine”
Keeping more people healthier longer Preparedness: public health threats … Prevention: tobacco control … Promotion: active living …
50% premature mortality is preventable Up to 70% of conditions that patients present in hospitals
and clinics are preventable
Co-Creating the Total Health System Access: reducing disparities Quality, Safety and Effectiveness (outcomes) Utilization (waste; integration; eHealth) Global Health: integrated services and delivery

first Health then Medicine

Fresh Thinking and Action
Reframing: first Health then MedicineReframing: first Health then Medicine Bottom of the Pyramid (Prahalad) Bottom of the Pyramid (Prahalad) Co-creation PPP: people, private, Co-creation PPP: people, private,
publicpublic Global – Local integrationGlobal – Local integration TechnologyTechnology ?????? ??????

Road to Fresh Thinking
The Road to Quality ...
I f everything's under control,
you're not going fast enough.
- Mario Andretti

1. What is the Worst Thing we could do?
Please identify really Please identify really bad ideasbad ideas for for keeping people healthier longerkeeping people healthier longer

2. Now flip the Bad Ideas into good ones?
Pick several bad ideas and transform Pick several bad ideas and transform them into good but still outrageous – them into good but still outrageous – way out there -way out there -

3. Convergence
Review the good ideas and propose Review the good ideas and propose several practical directions and several practical directions and solutions for the BIG Ideasolutions for the BIG Idea
Your Take Home Your Take Home Message?Message?

Dr. Ida S. Scudder, Founder, Christian Medical College & Hospital, Vellore, India, 1900

An Apple a Day: Strategies for Change
Penelope Hawe and Alan Shiell
1. Create demand for prevention by measuring, mapping and communicating the distribution of preventive policies & programs
2. Make new investments in evaluation and quality improvement in prevention
3. Open pathways to enable the switch from ineffective programs to effective ones with new customized decision-support tools
4. Create ‘healthy strings attached’ economic incentives to provide prevention policies and supportive environments for health