whitehorse continuing care facility: business case analysis
TRANSCRIPT

Primary Contact:Tim Turner-Davis
T-Square ArchitecturePO Box 31623Whitehorse, YT
t. 867.633.6030 [email protected]
New Whitehorse Continuing Care FacilityBusiness Case Analysis
Submitted by:
In Asssociation with:
M. Saar ArchitectureCornerstone Planning Group
LCVM ConsultantsResearch Northwest
Jon Schmidt
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 1
Whitehorse Continuing Care Facility DRAFT July 29, 2014
TABLE OF CONTENTS
A. INTRODUCTION .................................................................................................................................. 3 PROJECT CONTEXT ...................................................................................................................................... 3 INFORMATION SOURCES .............................................................................................................................. 3
B. DEMAND PROJECTIONS ................................................................................................................... 4 YUKON POPULATION ................................................................................................................................... 4 SENIOR/ELDER POPULATION ..................................................................................................................... 5 CONTINUING CARE DEMAND ...................................................................................................................... 6
C. EXISTING FACILITIES ........................................................................................................................ 8 MACAULAY LODGE ...................................................................................................................................... 8 THOMSON CENTRE ...................................................................................................................................... 9 COPPER RIDGE .......................................................................................................................................... 10 MCDONALD LODGE .................................................................................................................................. 10
D. FACILITY PLAN ................................................................................................................................ 10 PHASED CONSTRUCTION ........................................................................................................................... 10 FACILITY CLOSURES .................................................................................................................................. 10 FACILITIES PLAN ...................................................................................................................................... 12
E. DEVELOPMENT OPTIONS ............................................................................................................. 13 OPTION 1: PHASED 300 BED FACILITY ................................................................................................. 13 OPTION 2: TWO STAND-‐ ALONE 150 BED FACILITIES ............................................................................ 14 OPTION 3: PHASED 300 BED FACILITY WITH SUPPORT FOR 450 ...................................................... 15 PREFERRED OPTION ................................................................................................................................ 16
F. CARE MIX ........................................................................................................................................... 16
G. FUNCTIONAL PROGRAM ............................................................................................................... 17 BUILDING AREA REQUIREMENTS ............................................................................................................ 18 PARKING REQUIREMENTS ........................................................................................................................ 20 COMPONENT PROFILES ............................................................................................................................ 20 A: SHARED PUBLIC AND RESIDENT SUPPORT ........................................................................................................ 20 B: ADMINISTRATIVE SUPPORT .................................................................................................................................. 21 C: FACILITY AND OPERATIONS SUPPORT ................................................................................................................ 21 D: STANDARD RESIDENCE CARE PODS .................................................................................................................... 21 E: MENTAL HEALTH RESIDENT POD ....................................................................................................................... 22 F: PALLIATIVE CARE POD ........................................................................................................................................... 23 G: HIGH ACUITY CARE POD ........................................................................................................................................ 23 H: SHARED RESIDENCE SUPPORT PODS .................................................................................................................. 23 I: RESPITE CARE AND DAY PROGRAM SERVICES .................................................................................................... 24 COMPONENT RELATIONSHIPS .................................................................................................................. 24

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 2
CONCEPT DESIGN GUIDELINES ................................................................................................................ 30 SITE SELECTION GUIDELINES .................................................................................................................................... 30 MASSING AND IMAGE GUIDELINES ........................................................................................................................... 30 PATIOS AND GARDEN AREAS GUIDELINES .............................................................................................................. 31 PARKING AREA GUIDELINES ...................................................................................................................................... 31 PHASING GUIDELINES ................................................................................................................................................. 31 ENERGY AND SUSTAINABILITY STRATEGY .......................................................................................... 31
H. SITE SELECTION .............................................................................................................................. 32 PORTER CREEK ......................................................................................................................................... 33 LOCATION ...................................................................................................................................................................... 33 SITE ................................................................................................................................................................................. 33 TEST FIT ........................................................................................................................................................................ 35 COMMENTARY .............................................................................................................................................................. 37 WHISTLE BEND ........................................................................................................................................ 37 OWNERSHIP .................................................................................................................................................................. 37 LOCATION ...................................................................................................................................................................... 38 SITE ................................................................................................................................................................................. 40 TEST FIT ........................................................................................................................................................................ 42 COMMENTARY .............................................................................................................................................................. 44 RANGE ROAD NORTH ............................................................................................................................... 44 RECOMMENDED SITE ................................................................................................................................ 45
I. CAPITAL AND LIFE CYCLE COST ESTIMATES .......................................................................... 46 CAPITAL COSTS ......................................................................................................................................... 46 LIFE CYCLE COSTS .................................................................................................................................... 47
J. RISK ASSESSMENT ........................................................................................................................... 48 RISK ASSESSMENT FOR DEVELOPMENT OPTION .................................................................................... 49 RISK ASSESSMENT FOR SITE SELECTION ................................................................................................... 49
K. PROCUREMENT STRATEGY ......................................................................................................... 50 SWOT ANALYSIS ...................................................................................................................................... 51 RECOMMENDATION .................................................................................................................................. 52 Appendix A: Standards Review Appendix B: Desktop Geotechnical Study by Tetra Tech EBA Appendix C: Detailed Risk Assessment Appendix D: Capital and Life Cycle Cost Estimates – Development Options and Site
Selection Appendix E: 6-Year Cumulative Cost Estimate – Thomson Centre and Macaulay Lodge Appendix F: Planning Assumptions Document
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 3
A. Introduction Continuing Care, a division in the Department of Health and Social Services (HSS) of the Yukon Government (YG), administers senior/elder care, including all home care, respite services, and residential care. The Yukon population presents unique challenges for senior/elder care: much of the population is spread into remote communities, complicating the provision of services; also, due to a number of lifestyle-related factors, care utilization rates tend to be higher than in other parts of Canada. While the continuing care population is mostly comprised of senior/elder citizens, continuing care is also provided to pediatric and adult clients with chronic illness, as well as long-term mental health clients. Because the Yukon’s population is not large enough to support numerous specialized facilities, these clients share facilities with the rest of the continuing care population, albeit with some segregation within facilities.
PROJECT CONTEXT HSS currently operates four continuing care facilities. There is currently a waiting list for permanent continuing care beds. Additionally, the demand for beds is expected to continue to grow for the foreseeable future. To this end, HSS and YG’s Department of Highways and Public Works (HPW) has begun a project to plan for the expansion of continuing care capacity. In 2012, HSS, HPW, and Kobayashi Zedda Architects (KZA) produced a Functional Program for a 300-bed continuing care facility. It provided a needs analysis, an assessment of the existing Whitehorse continuing care facilities, and a functional program for the new facility. The current Business Case was commissioned to confirm the needs analysis and functional program, make recommendations for the development strategy of the new facility, and recommend a site based on pre-established site selection criteria.
INFORMATION SOURCES Information for this report was gathered from the following sources:
• Tours of the three existing Whitehorse Continuing Care Facilities • Planning conference with HSS staff • 2012 Functional Program by Kobayashi Zedda Architects • Tours of potential sites
Standards for continuing care facilities were gathered from the following sources:
• Vancouver Coastal Health Design Guidelines Complex Residential Care Developments (2007)
• Alberta Government Design Guidelines for Continuing Care Facilities in Alberta (2012)
• New Brunswick, Department of Social Development Design Standards for Nursing Homes (2012)
• Nova Scotia, Department of Health Long Term Care Facility Requirements (Space and Design) Appendix B (2007)
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 4
• Ontario Ministry of Health and Long Term Care – Long Term Care Home Design Manual (2009)
• BC Ministry of Health and Ministry Responsible for Seniors – Multilevel Care Design Guidelines (1994 reviewed in 1998)
Additionally, a preliminary geotechnical desktop evaluation was performed by Tetra Tech EBA to determine anticipated soil conditions at each site. The report is attached in Appendix B.
B. Demand Projections Predicting demand for Continuing Care beds was performed as a three-step process. First, the Yukon’s overall population was extrapolated to 2035. Next, these overall estimates were used to estimate the senior/elder population. Finally, the senior/elder population was used to create an estimate for the total demand for Continuing Care.
YUKON POPULATION Yukon Bureau of Statistics population projections were selected as a starting point for projection. The Bureau of Statistics numbers were selected over Statistics Canada projections for being locally generated and based on up-to-date understanding of demographic influences and trends. Since this population projection ends in 2021, the data needed to be extrapolated a further 14 years. A non-linear extrapolation was used to project to 2035, reflecting the trend of diminishing growth identified in the Bureau of Statistics data. The projection was then compared to Statistics Canada’s projections for the same period for confirmation. The above methodology produced a population projection that is 1.6% higher than the Statistics Canada projections which, considering the length of the projection, is quite close, lending credibility to the above methodology. The table below shows the extrapolated Bureau of Statistics projections in comparison to Statistic’s Canada’s projections for the same period.
Yukon Population Senior/Elder Population
Continuing Care Demand

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 5
Figure 1: Yukon 20-year Population Projections
SENIOR/ELDER POPULATION Seniors/elders currently make up 9.9% of the Yukon’s population, which is a lower proportion than the Canadian average of 15.3%. The projection methodology took into account baseline data from recent years, and assumed that the proportion of seniors/elders would grow at an increasing rate, as is expected for the Canadian population at large. It was expected, however, that growth in the proportion of seniors/elders would continue to lag behind national statistics. The projections estimated that seniors/elders would make up 13.1% of the population in 2021 and would grow to 23% of the population by 2031, which is the lower end of Statistics Canada’s projection for the country as a whole.
SOURCE'DATA:'Yukon'Bureau'of'Statistics,'
"Projections'Based'on'June'2001'C'2011'Reference'
Period"'for'the'years'2012'through'2021'(Note:'
Numbers'appearing'in'blue'font'were'extrapolated'by'the'Consultant'Team)
SOURCE'DATA:'Statistics'Canada,'"Population'
Projections'for'Canada,'Provinces'and'Territories,"'2009'C'Projection'Based'on'"MediumCGrowthC1988'to'1996'Trends'Scenario"
YEAR
2011 35&175 34&1002012 35&691 34&5002013 36&204 35&0002014 36&716 35&4002015 37&225 35&8002016 37&729 36&3002017 38&227 36&7002018 38&717 37&1002019 39&199 37&5002020 39&671 37&9002021 40&130 38&3002022 40'576 38&7002023 41'008 39&2002024 41'424 39&6002025 41'822 40&0002026 42'201 40&4002027 42'558 40&8002028 42'892 41&2002029 43'202 41&5002030 43'488 41&9002031 43'748 42&3002032 43'981 42&7002033 44'186 43&1002034 44'361 43&4002035 44'504 43&800
PROJECTED'POPULATION
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 6
Use of the forecasted senior/elder population data relied on the principle of “all else equal.” For planning purposes it was assumed that the following conditions would prevail for the planning period:
• Historical and current referral patterns would continue • Historical and current patterns of immigration and emigration would continue • No known or anticipated technologies or therapies will change demand for
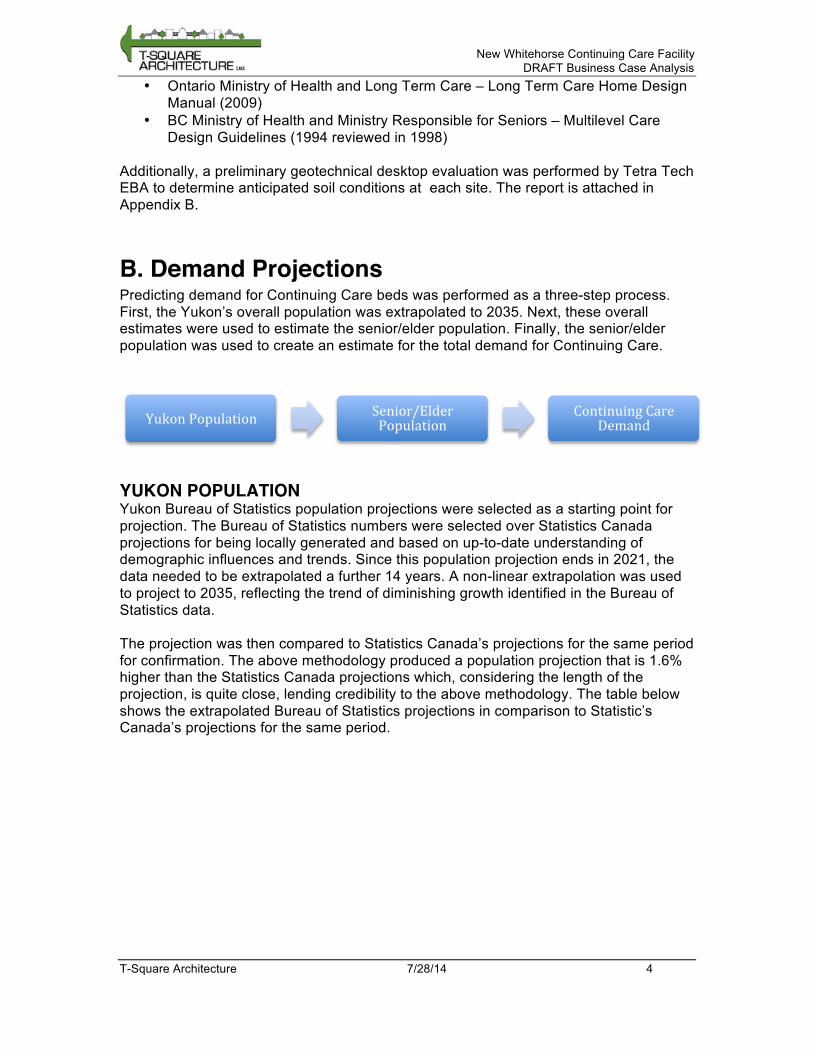
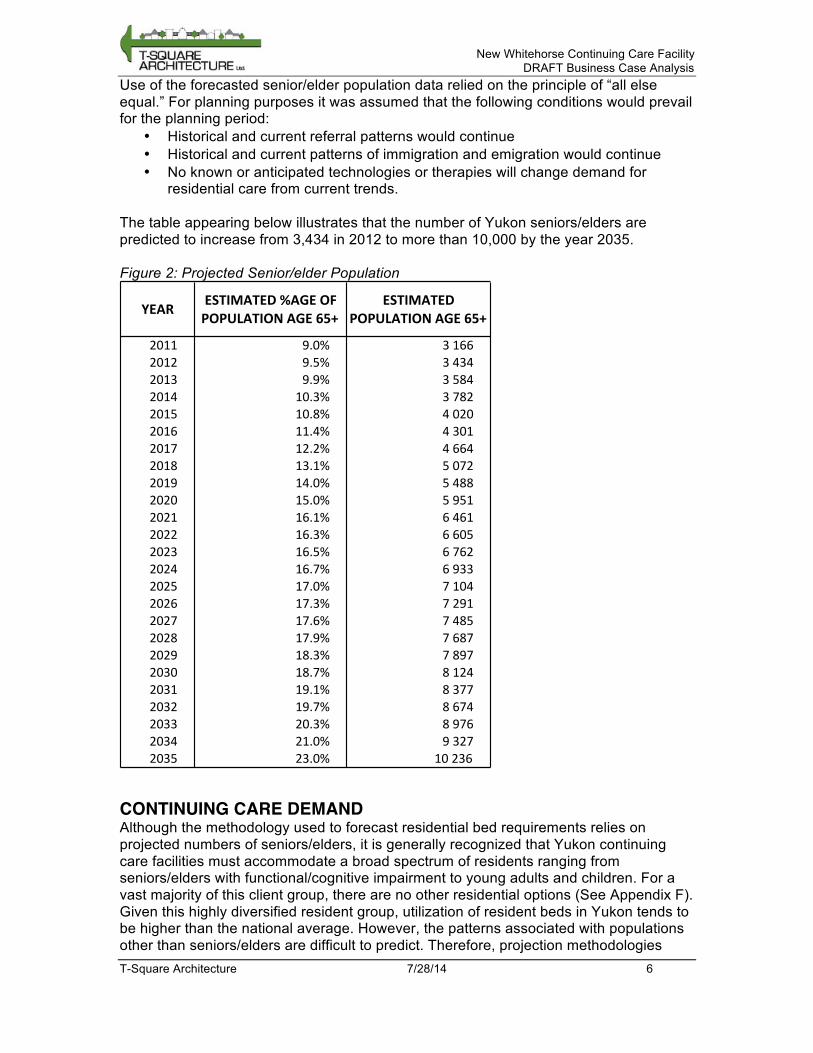
residential care from current trends. The table appearing below illustrates that the number of Yukon seniors/elders are predicted to increase from 3,434 in 2012 to more than 10,000 by the year 2035. Figure 2: Projected Senior/elder Population
CONTINUING CARE DEMAND Although the methodology used to forecast residential bed requirements relies on projected numbers of seniors/elders, it is generally recognized that Yukon continuing care facilities must accommodate a broad spectrum of residents ranging from seniors/elders with functional/cognitive impairment to young adults and children. For a vast majority of this client group, there are no other residential options (See Appendix F). Given this highly diversified resident group, utilization of resident beds in Yukon tends to be higher than the national average. However, the patterns associated with populations other than seniors/elders are difficult to predict. Therefore, projection methodologies
YEAR ESTIMATED*%AGE*OF*POPULATION*AGE*65+*
ESTIMATED*POPULATION*AGE*65+*
2011 9.0% 3(1662012 9.5% 3(4342013 9.9% 3(5842014 10.3% 3(7822015 10.8% 4(0202016 11.4% 4(3012017 12.2% 4(6642018 13.1% 5(0722019 14.0% 5(4882020 15.0% 5(9512021 16.1% 6(4612022 16.3% 6(6052023 16.5% 6(7622024 16.7% 6(9332025 17.0% 7(1042026 17.3% 7(2912027 17.6% 7(4852028 17.9% 7(6872029 18.3% 7(8972030 18.7% 8(1242031 19.1% 8(3772032 19.7% 8(6742033 20.3% 8(9762034 21.0% 9(3272035 23.0% 10(236
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 7
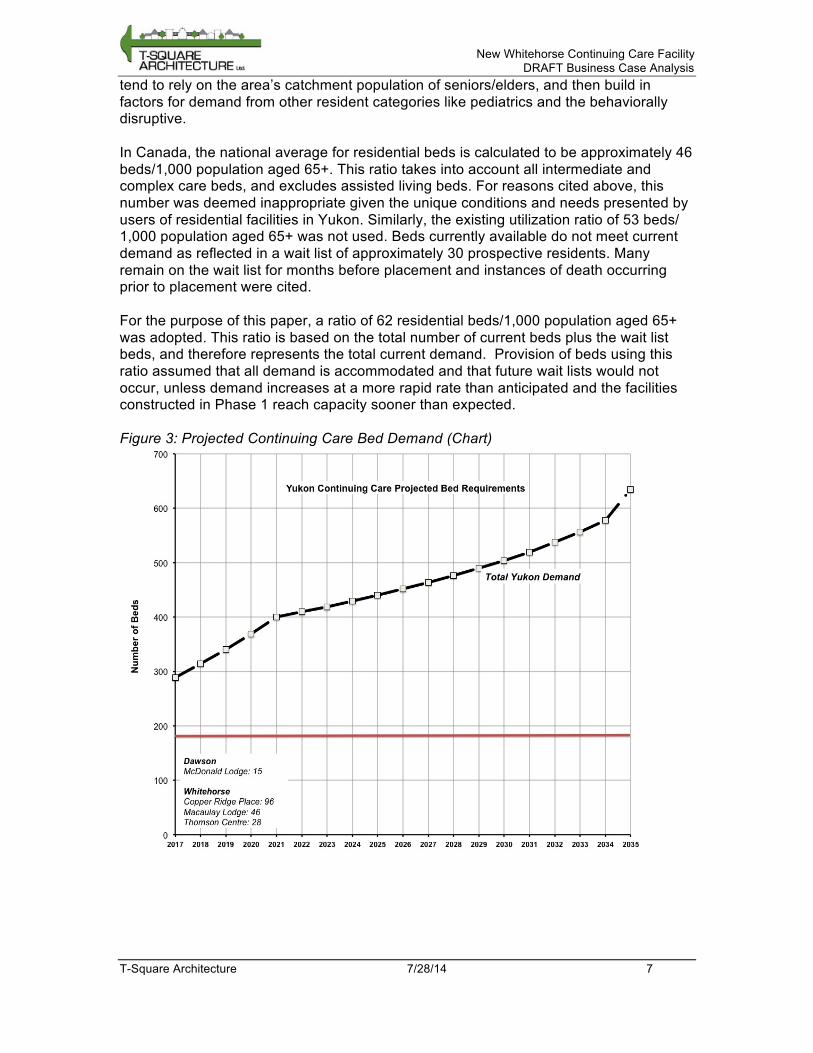
tend to rely on the area’s catchment population of seniors/elders, and then build in factors for demand from other resident categories like pediatrics and the behaviorally disruptive. In Canada, the national average for residential beds is calculated to be approximately 46 beds/1,000 population aged 65+. This ratio takes into account all intermediate and complex care beds, and excludes assisted living beds. For reasons cited above, this number was deemed inappropriate given the unique conditions and needs presented by users of residential facilities in Yukon. Similarly, the existing utilization ratio of 53 beds/ 1,000 population aged 65+ was not used. Beds currently available do not meet current demand as reflected in a wait list of approximately 30 prospective residents. Many remain on the wait list for months before placement and instances of death occurring prior to placement were cited. For the purpose of this paper, a ratio of 62 residential beds/1,000 population aged 65+ was adopted. This ratio is based on the total number of current beds plus the wait list beds, and therefore represents the total current demand. Provision of beds using this ratio assumed that all demand is accommodated and that future wait lists would not occur, unless demand increases at a more rapid rate than anticipated and the facilities constructed in Phase 1 reach capacity sooner than expected. Figure 3: Projected Continuing Care Bed Demand (Chart)
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 8
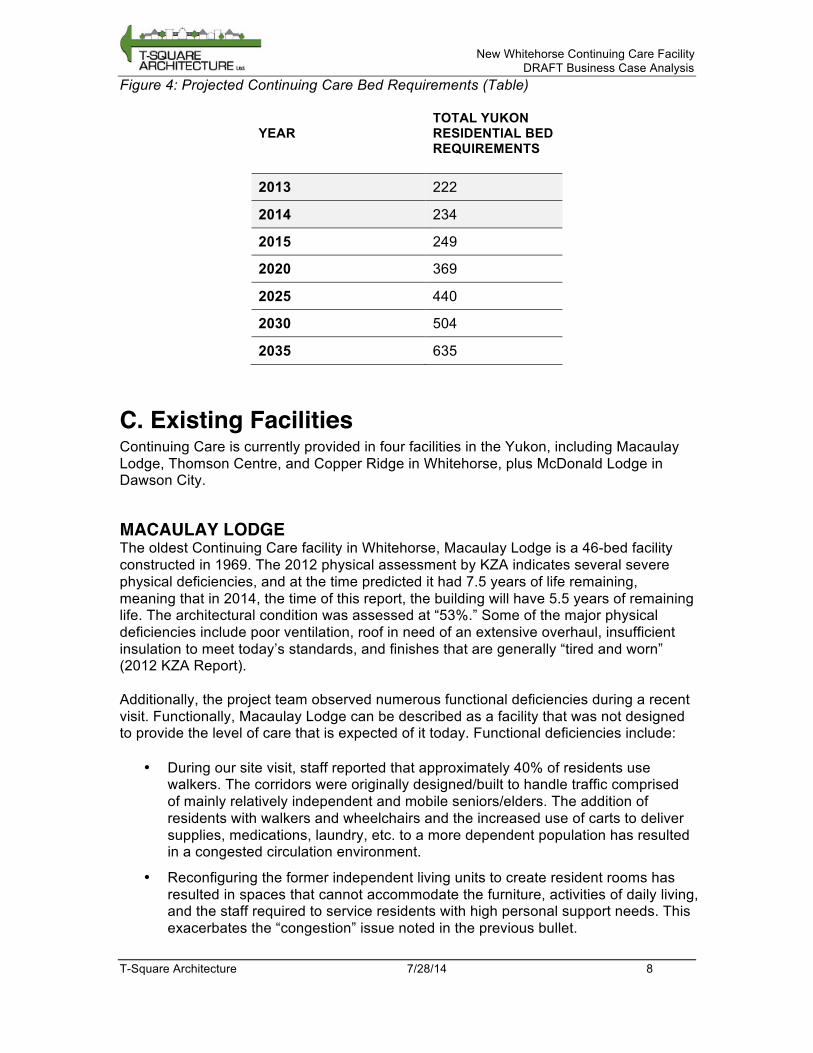
Figure 4: Projected Continuing Care Bed Requirements (Table)
YEAR TOTAL YUKON RESIDENTIAL BED REQUIREMENTS
2013 222
2014 234
2015 249
2020 369
2025 440
2030 504
2035 635
C. Existing Facilities Continuing Care is currently provided in four facilities in the Yukon, including Macaulay Lodge, Thomson Centre, and Copper Ridge in Whitehorse, plus McDonald Lodge in Dawson City.
MACAULAY LODGE The oldest Continuing Care facility in Whitehorse, Macaulay Lodge is a 46-bed facility constructed in 1969. The 2012 physical assessment by KZA indicates several severe physical deficiencies, and at the time predicted it had 7.5 years of life remaining, meaning that in 2014, the time of this report, the building will have 5.5 years of remaining life. The architectural condition was assessed at “53%.” Some of the major physical deficiencies include poor ventilation, roof in need of an extensive overhaul, insufficient insulation to meet today’s standards, and finishes that are generally “tired and worn” (2012 KZA Report). Additionally, the project team observed numerous functional deficiencies during a recent visit. Functionally, Macaulay Lodge can be described as a facility that was not designed to provide the level of care that is expected of it today. Functional deficiencies include:
• During our site visit, staff reported that approximately 40% of residents use walkers. The corridors were originally designed/built to handle traffic comprised of mainly relatively independent and mobile seniors/elders. The addition of residents with walkers and wheelchairs and the increased use of carts to deliver supplies, medications, laundry, etc. to a more dependent population has resulted in a congested circulation environment.
• Reconfiguring the former independent living units to create resident rooms has resulted in spaces that cannot accommodate the furniture, activities of daily living, and the staff required to service residents with high personal support needs. This exacerbates the “congestion” issue noted in the previous bullet.
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 9
• Resident rooms do not have ceiling lifts, which is a significant cause of staff injuries.
• The KZA Report alluded to a 1997/98 renovation that “…eliminated potentially dangerous dead end corridors.” In spite of this renovation, residents are isolated from external environmental cues due to the lack of exterior views and way finding and orienteering remain issues for today’s residents.
• The building is a 2-storey structure, and with the acceptance of “higher level” residents there are instances of residents being moved from the second level to a ground floor unit due to difficulty in using stairs. In an acute care setting, it is generally accepted that transferring clients from room-to-room is not a good practice as this has been shown to have a negative impact on general health and recovery. There are no studies to suggest that inter-room transfers in the continuing care setting do not have similar effects, especially when a resident’s room essentially becomes their home.
While residents praise Macaulay Lodge and staff for its ‘homey,’ non-institutional feel, the facility is nearing the end of its life. The building would require extensive renovations to alleviate its physical and functional deficiencies, which would be very expensive and would likely require that the building be vacated.
THOMSON CENTRE Thomson Centre was opened as a 46-bed facility in 1991. The building was vacated in 2002, then later partially reinstated as a 28-bed facility. The rest of the facility is now used by the Hospital, which owns the building and leases the space to HSS. A 2012 condition assessment by KZA noted that the facility appeared to be functionally adequate with some problems. There are also a number of functional deficiencies:
• Support space for staff is inadequate (break areas, cloak rooms, lockers, meeting rooms)
• Space is not available to provide recreational therapy, physiotherapy or occupational therapy, examination/treatment, quiet space
• Support space for the units are inadequate – there is only one clean utility room and only one dirty utility room for the two units
• No large gathering space - originally the building was designed to accommodate a large great room with a fireplace. This has been taken over by the Hospital Corporation for staff training and is not available to the residents. There is no space to offer chapel services
Based on discussions with YG staff, there has been speculation regarding the possibility of returning a portion of the facility currently used by the Hospital for use by Continuing Care. However, no commitment or formal offer for such an arrangement exists at this time. Should the opportunity arise, YG will need to evaluate the life cycle costs and functional benefits of renovating and operating a re-expanded Continuing Care operation at Thomson Centre against that of a new facility. With continued maintenance and renovations, the facility could be kept in service for an extended period of time. However, a preliminary analysis of staffing and operating costs indicates that Thomson Centre has a higher operating cost per bed than both Macaulay Lodge and McDonald Lodge. It is less costly than Copper Ridge Place, but this may be a

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 10
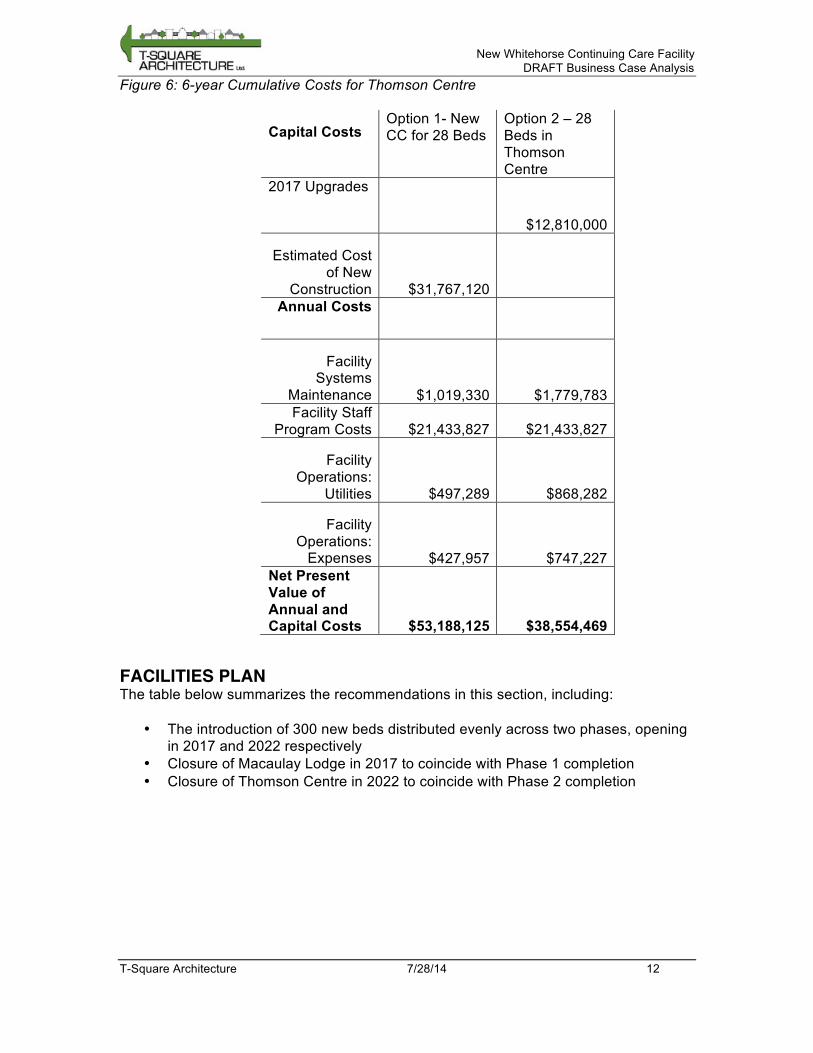
function of the difference in the type of care delivered at Copper Ridge (i.e. Copper Ridge accommodates Extended and Special Care, while Thomson Centre accommodates Intermediate and Extended Care). If a new facility with more beds than at Thomson Centre were available to accommodate the same level of Intermediate and extended care, the operating cost per bed would likely be less than the costs at Thomson Centre. Figure 6 in Section D indicates that while operating costs of this new facility are lower, the high capital cost of building new capacity means that cost savings would not be realized in the short-term. As a result, the decision to continue to operate Thomson Centre will need to take into account the strategic context of continuing care in the Yukon as a whole. This is discussed in further detail in section D: Facility Plan.
COPPER RIDGE Copper Ridge, a 97-bed site, is the newest continuing care facility in the Yukon. As it was constructed in 1999, the facility is considered to be in good shape and fit for continued use. The facility includes six units providing continuing care for seniors/elders, plus an adult unit and a pediatric unit.
MCDONALD LODGE McDonald Lodge currently provides 11 care beds in Dawson City, and is being replaced by a 15-bed facility, which is expected to open in January 2016. As the only facility located outside of Whitehorse, McDonald Lodge provides continuing care and respite to some of the Yukon’s most remote communities. McDonald Lodge is currently being replaced, with its replacement expected to last the duration of the planning period.
D. Facility Plan The facility plan provides a framework for meeting the projected demand, given the current supply. It includes two parts: the timing for bringing new capacity online, and the retirement of older facilities as they age or become not cost-effective to operate. The former is set out by the terms of reference in this project, while the latter will need to be determined based on building condition and operational costs.
PHASED CONSTRUCTION The terms of reference for the study are based on a two Phase development concept that has been reiterated in the recent budget announcements - “$6.9 million in 2014-2015 for phase one of a new 300 bed continuing care facility which will include an initial 150 beds with the capacity to expand by an additional 150 beds as required in the future.” It was therefore considered extremely important to not exceed 150 beds for Phase 1. Planning and design for the first phase will begin immediately, with construction expected to commence in 2016. Planning and design for Phase 2 is expected to begin shortly after, with completion targeted for 2022.
FACILITY CLOSURES Copper Ridge Place is in good condition and is expected to remain in operation for the duration of the planning period. The replacement for McDonald Lodge will be a new facility, and also expected to remain in operation for the duration of the planning period.
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 11
Macaulay Lodge, however, has physical and functional deficiencies (as detailed in Section C), and should be replaced within 5 years. The opening of Phase 1 presents the soonest opportunity to retire Macaulay Lodge without incurring a large wait list. In preparation for the decommissioning of Macaulay Lodge, a decanting plan should be developed immediately to ensure a smooth and safe transition for residents.
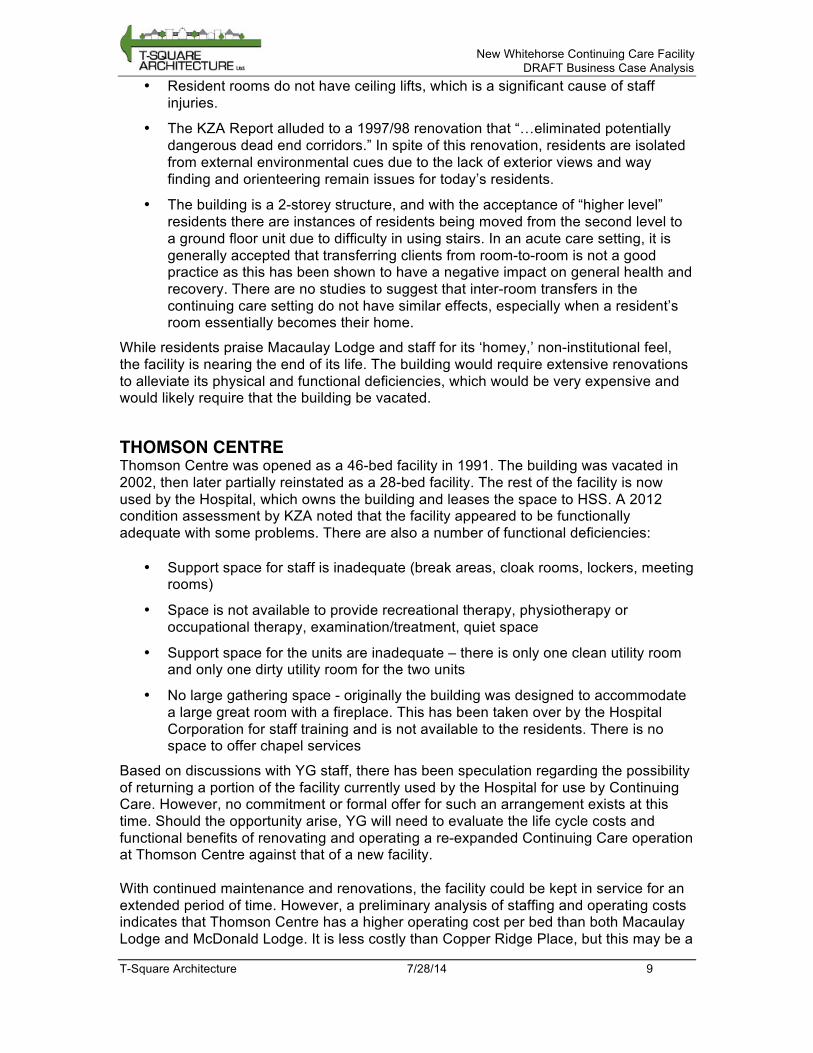
Thomson Centre is in reasonable condition, but is potentially an uneconomical size for a continuing care facility. As shown below, staffing costs per bed for Thomson are higher than McDonald or Macaulay Lodge. Staffing costs for Copper Ridge are higher than Thomson, but this is presumably because Copper Ridge provides a higher level of care to a more diverse population. Non-salary operating costs per bed are also highest at Thomson Centre, due mostly to the cost of leasing the facility from the Hospital. Further analysis is needed to determine whether the beds accommodated in Thomson Centre would be more economically accommodated in a larger facility. Figure 5: Comparison of Operating Costs for Existing Facilities
2012-2013 (Actual) Copper
Ridge Place Macaulay
Lodge Thomson
Centre McDonald
Lodge Total Actual Operating $2,538,903 $656,460 $1,289,005 $230,115 Total Actual Salary & Benefits $14,832,381 $4,405,511 $3,022,589 $887,567
Number of Beds 96 46 28 11
Cost per Bed $180,951 $110,042 $153,985 $101,607
Types of Care Extended
and Special Care
Intermediate Care
Intermediate and
Extended Care
Personal Care
It is recommended that Thomson Centre continue to operate to alleviate wait list conditions, particularly as Macaulay Lodge will be closing soon. However, it is recommended that during Phase 2 planning, the situation be reviewed with the goal of creating a long-term, cost-effective plan that does not create excessive wait lists. 6-year cumulative operating costs were prepared for Thomson Centre, to determine the short-term cost implications of closing the facility compared to the cost of renovations and continued use. Shown below, Figure 6 indicates that while operation costs for Thomson are higher than that of a new facility, the high capital cost associated with building a new replacement facility is not economical in the short-term. More detailed analysis of Thomson Centre’s cost-effectiveness should be performed in planning for the Phase 2 facility.
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 12
Figure 6: 6-year Cumulative Costs for Thomson Centre
Capital Costs Option 1- New CC for 28 Beds
Option 2 – 28 Beds in Thomson Centre
2017 Upgrades
$12,810,000
Estimated Cost of New
Construction $31,767,120
Annual Costs
Facility Systems
Maintenance $1,019,330 $1,779,783 Facility Staff
Program Costs $21,433,827 $21,433,827
Facility Operations:
Utilities $497,289 $868,282
Facility Operations:
Expenses $427,957 $747,227 Net Present Value of Annual and Capital Costs $53,188,125 $38,554,469
FACILITIES PLAN The table below summarizes the recommendations in this section, including:
• The introduction of 300 new beds distributed evenly across two phases, opening in 2017 and 2022 respectively
• Closure of Macaulay Lodge in 2017 to coincide with Phase 1 completion • Closure of Thomson Centre in 2022 to coincide with Phase 2 completion

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 13
Figure 7: Projected Surplus/Wait List for recommended Facilities Plan
2017 2021 2022 2026
Total Yukon Beds Required 289 401 409 452
Beds Available
McDonald Lodge (Dawson) 15 15 15 15
Copper Ridge Place 96 96 96 96
Macaulay Lodge 46 0 0 0
Thomson Centre 28 28 0* 0*
New 150 150 300 300 Total Yukon Beds Available 335 289 411 411
Surplus (Wait List) 46 (112) 2 (41) *Note: The figure shows an option where Thomson Centre is closed in 2022. It is recommended that the decision to close or maintain Thomson Centre be examined more closely in the planning stages of Phase 2.
E. Development Options The development strategy details the means of producing the capacity described in the previous section. All three options listed below involve the creation of 150 beds in Phase 1, with another 150 beds in Phase 2. However, Option 3 includes sufficient support space in Phase 1 to accommodate a total of 450 beds and therefore assumes a third phase of another 150 beds at a separate timing that is yet to be determined. The options explore the cost and functional implications of placing both phases in the same facility or in separate facilities. For the case of standalone facilities, the options also examine the implications of concentrating support space (such as laundry and kitchen) into one facility for potential cost savings.
OPTION 1: PHASED 300 BED FACILITY Strategy 1 involves building a new 300-bed facility in two phases. The Phase 1 facility will have 150 beds and enough support space (offices, common areas, loading, kitchen, laundry, etc.) to sustain a 300-bed facility. In the second phase, a 150-bed addition will be built to complete the facility. The first phase should be designed such that the second phase addition can be built simply and with the least disruption to residents. The area table shows that the first phase is a larger project than a stand-alone 150-bed facility with no allowance for future expansion. However, by building a larger facility in Phase 1, the size of Phase 2 is reduced. In addition, the overall construction area is less than it would be if two separate 150-bed care facilities were constructed, as shown in Phase 2.

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 14
Figure 8: Area Required for Development Option 1
This Strategy has the advantage of requiring less construction than the other Strategies, and therefore will have the lowest capital cost. This is a result of the operational synergies that are realized by housing all 300 beds under one roof. However, the major disadvantages of this strategy also stem from the concentration of all 300 beds in one facility. The stated goal of building a continuing care facility with a non-institutional feel will be more difficult with a larger facility. Additionally, the size of the building demands a larger site than the other two options, which will influence the site selection process.
OPTION 2: TWO STAND- ALONE 150 BED FACILITIES In this strategy, two identical standalone facilities are constructed in the sequence. Each facility operates independently and is built with its own administration offices, kitchen, and laundry facilities. The two facilities could be located on the same site but it would also be feasible to locate them on different sites. The area table shows that while the construction outlay is equal for both phases, this plan requires a larger overall construction area than Strategy 1. This increased area is due to the duplication of kitchen, laundry, and other support facilities in both facilities, as well as the loss of economy of scale associated with larger buildings.
PHASE ONE150 Bed Facility (with
support for 300)
PHASE TWO150 Bed Addition
TOTAL300 Bed Facility
NetComponent
Gross NetComponent
Gross NetComponent
GrossA Shared Public and Resident Support 631.0 757.0 0.0 0.0 631.0 757.0B Administrative Support 559.0 671.0 0.0 0.0 559.0 671.0C Facility and Operations Support 918.5 1,102.0 0.0 0.0 918.5 1,102.0D Standard Resident Care Pods 4,742.5 6,023.0 6,123.5 7,776.5 10,866.0 13,799.5E Mental Health Resident Pod 576.0 731.5 0.0 0.0 576.0 731.5F Palliative Care Pod 552.0 701.0 0.0 0.0 552.0 701.0G High Acuity Care Pod 282.0 358.0 0.0 0.0 282.0 358.0H Shared Residence Support Pods 234.0 297.0 234.0 297.0 468.0 594.0I Respite Care and Day Programs/Services 234.0 297.0 0.0 0.0 234.0 297.0TOTALS 8,729.0 10,937.5 6,357.5 8,073.5 15,086.5 19,011.0
TOTAL Building Gross 13,442.7 9,790.6 23,233.2PARKINGStaff 120 100 220Visitors 41 45 86Maintenance Vehicles 6 2 8Handybus 2 2 4Total Stalls 169 149 318OUTDOOR PATIOS AND GARDEN AREAS (s.m.) 225 225 450
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 15
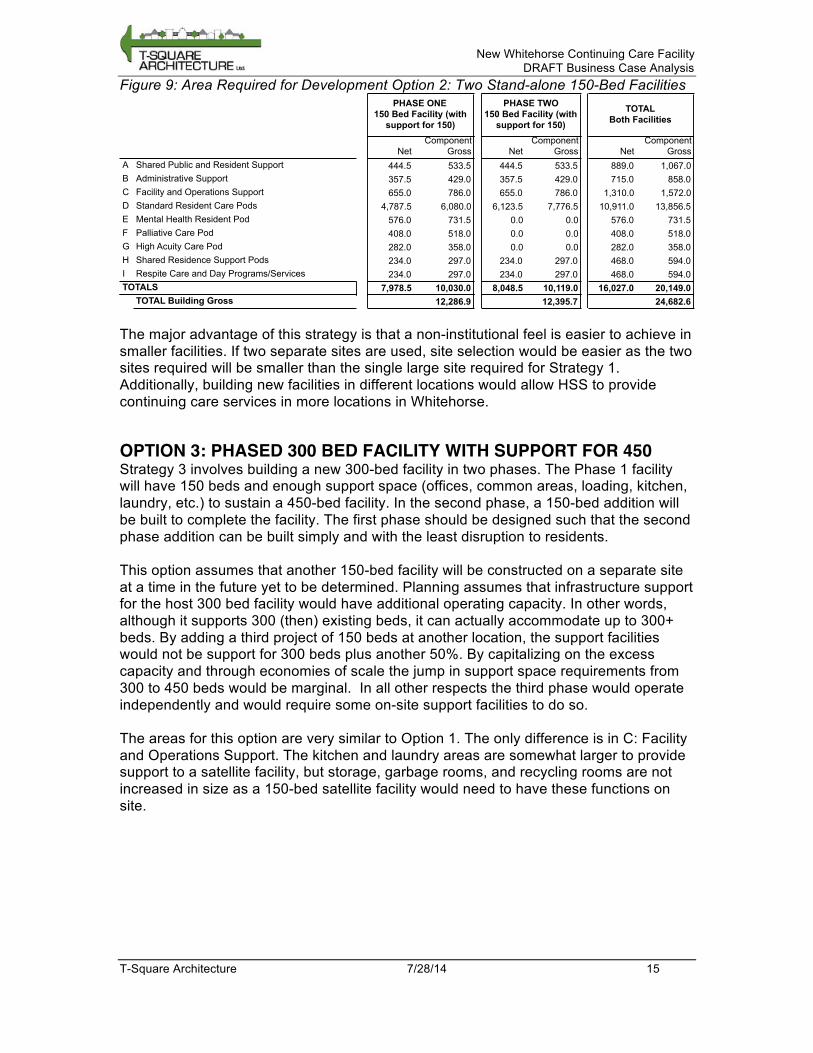
Figure 9: Area Required for Development Option 2: Two Stand-alone 150-Bed Facilities
The major advantage of this strategy is that a non-institutional feel is easier to achieve in smaller facilities. If two separate sites are used, site selection would be easier as the two sites required will be smaller than the single large site required for Strategy 1. Additionally, building new facilities in different locations would allow HSS to provide continuing care services in more locations in Whitehorse.
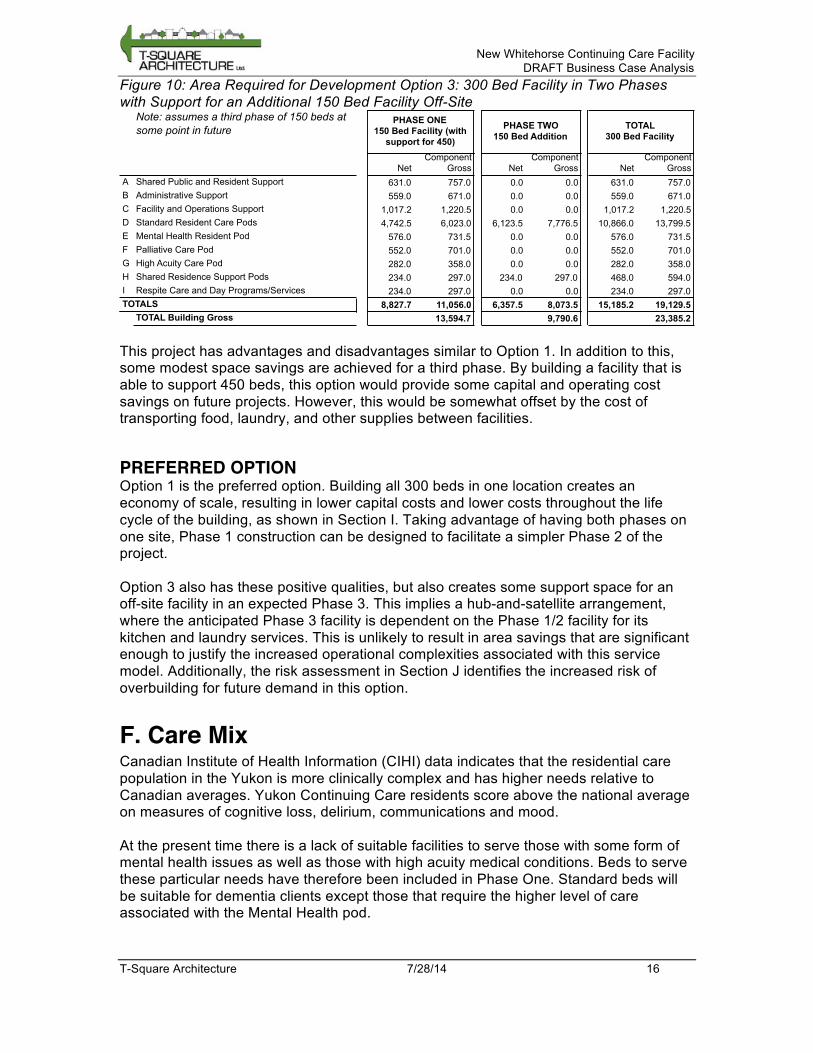
OPTION 3: PHASED 300 BED FACILITY WITH SUPPORT FOR 450 Strategy 3 involves building a new 300-bed facility in two phases. The Phase 1 facility will have 150 beds and enough support space (offices, common areas, loading, kitchen, laundry, etc.) to sustain a 450-bed facility. In the second phase, a 150-bed addition will be built to complete the facility. The first phase should be designed such that the second phase addition can be built simply and with the least disruption to residents. This option assumes that another 150-bed facility will be constructed on a separate site at a time in the future yet to be determined. Planning assumes that infrastructure support for the host 300 bed facility would have additional operating capacity. In other words, although it supports 300 (then) existing beds, it can actually accommodate up to 300+ beds. By adding a third project of 150 beds at another location, the support facilities would not be support for 300 beds plus another 50%. By capitalizing on the excess capacity and through economies of scale the jump in support space requirements from 300 to 450 beds would be marginal. In all other respects the third phase would operate independently and would require some on-site support facilities to do so. The areas for this option are very similar to Option 1. The only difference is in C: Facility and Operations Support. The kitchen and laundry areas are somewhat larger to provide support to a satellite facility, but storage, garbage rooms, and recycling rooms are not increased in size as a 150-bed satellite facility would need to have these functions on site.
PHASE ONE150 Bed Facility (with
support for 150)
PHASE TWO150 Bed Facility (with
support for 150)
TOTALBoth Facilities
NetComponent
Gross NetComponent
Gross NetComponent
GrossA Shared Public and Resident Support 444.5 533.5 444.5 533.5 889.0 1,067.0B Administrative Support 357.5 429.0 357.5 429.0 715.0 858.0C Facility and Operations Support 655.0 786.0 655.0 786.0 1,310.0 1,572.0D Standard Resident Care Pods 4,787.5 6,080.0 6,123.5 7,776.5 10,911.0 13,856.5E Mental Health Resident Pod 576.0 731.5 0.0 0.0 576.0 731.5F Palliative Care Pod 408.0 518.0 0.0 0.0 408.0 518.0G High Acuity Care Pod 282.0 358.0 0.0 0.0 282.0 358.0H Shared Residence Support Pods 234.0 297.0 234.0 297.0 468.0 594.0I Respite Care and Day Programs/Services 234.0 297.0 234.0 297.0 468.0 594.0TOTALS 7,978.5 10,030.0 8,048.5 10,119.0 16,027.0 20,149.0
TOTAL Building Gross 12,286.9 12,395.7 24,682.6
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 16
Figure 10: Area Required for Development Option 3: 300 Bed Facility in Two Phases with Support for an Additional 150 Bed Facility Off-Site
This project has advantages and disadvantages similar to Option 1. In addition to this, some modest space savings are achieved for a third phase. By building a facility that is able to support 450 beds, this option would provide some capital and operating cost savings on future projects. However, this would be somewhat offset by the cost of transporting food, laundry, and other supplies between facilities.
PREFERRED OPTION Option 1 is the preferred option. Building all 300 beds in one location creates an economy of scale, resulting in lower capital costs and lower costs throughout the life cycle of the building, as shown in Section I. Taking advantage of having both phases on one site, Phase 1 construction can be designed to facilitate a simpler Phase 2 of the project. Option 3 also has these positive qualities, but also creates some support space for an off-site facility in an expected Phase 3. This implies a hub-and-satellite arrangement, where the anticipated Phase 3 facility is dependent on the Phase 1/2 facility for its kitchen and laundry services. This is unlikely to result in area savings that are significant enough to justify the increased operational complexities associated with this service model. Additionally, the risk assessment in Section J identifies the increased risk of overbuilding for future demand in this option.
F. Care Mix Canadian Institute of Health Information (CIHI) data indicates that the residential care population in the Yukon is more clinically complex and has higher needs relative to Canadian averages. Yukon Continuing Care residents score above the national average on measures of cognitive loss, delirium, communications and mood. At the present time there is a lack of suitable facilities to serve those with some form of mental health issues as well as those with high acuity medical conditions. Beds to serve these particular needs have therefore been included in Phase One. Standard beds will be suitable for dementia clients except those that require the higher level of care associated with the Mental Health pod.
Note: assumes a third phase of 150 beds at some point in future
PHASE ONE150 Bed Facility (with
support for 450)
PHASE TWO150 Bed Addition
TOTAL300 Bed Facility
NetComponent
Gross NetComponent
Gross NetComponent
GrossA Shared Public and Resident Support 631.0 757.0 0.0 0.0 631.0 757.0B Administrative Support 559.0 671.0 0.0 0.0 559.0 671.0C Facility and Operations Support 1,017.2 1,220.5 0.0 0.0 1,017.2 1,220.5D Standard Resident Care Pods 4,742.5 6,023.0 6,123.5 7,776.5 10,866.0 13,799.5E Mental Health Resident Pod 576.0 731.5 0.0 0.0 576.0 731.5F Palliative Care Pod 552.0 701.0 0.0 0.0 552.0 701.0G High Acuity Care Pod 282.0 358.0 0.0 0.0 282.0 358.0H Shared Residence Support Pods 234.0 297.0 234.0 297.0 468.0 594.0I Respite Care and Day Programs/Services 234.0 297.0 0.0 0.0 234.0 297.0TOTALS 8,827.7 11,056.0 6,357.5 8,073.5 15,185.2 19,129.5
TOTAL Building Gross 13,594.7 9,790.6 23,385.2

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 17
Palliative beds and High Acuity beds both require gases and the facility program proposes that they be located in close proximity to facilitate flexible use. To augment the flexible use potential of the facilities, a portion of beds in one of the Standard Resident pods is to be also equipped with medical gases. The following table illustrates the proposed care mix for both phases.
Figure 11: Care Mix
G. Functional Program A Functional Program for a 300-bed Continuing Care Facility in Whitehorse was prepared and submitted in July 2013 by Kobayashi + Zedda Architects (KZA). The terms of reference for the current Business Case and Pre-Concept Planning study specified that this program be reviewed, verified, modified and refined to reflect an analysis of a preferred location for a new facility as well as the optimal type, size, organization and configuration of spaces within it to accommodate all functions that support the needs of residents, visitors and staff. A review of the KZA Program was undertaken with the objective of making adjustments as required to produce an updated space list that would provide reliable basis for exploring development options, undertaking site fit tests and estimating development and life cycle costs. Our review indicated that the net areas in the KZA program were generally appropriate for the care mix described in the document. Minor modification were made to the area allowances in a few selected spaces to better reflect current practices, but these changes did not significantly affect the overall net space. Of particular note were the areas specified for the resident rooms. The areas indicated in the KZA program met or exceeded the Continuing Care Standards that were reviewed as part of this phase (see Appendix A). The net areas indicated in our updated Functional Program refer to “useable” space within the room and do not include an entrance or vestibule into the room (this will be covered under the gross up factor of 1.5. Rsident rooms have been programmed at 24 nsm which allows for at least 18 nsm of useable space and ensures clearances of 1.5 meters around the bed on all 3 sides, plus a washroom with an area of at least 5.5 nsm. A bariatric resident room at 37 nsm allows
Whitehorse Continuing Care Facility Care MixStandard
(incl dementia)
Mental Health Bariatric
Palliative (gases) High Acuity Totals
Phase one Beds 114 12 6 12 6 150Percentage Distribution 76% 8% 4% 8% 4% 100%
Phase Two Beds 143 0 7 0 0 150Percentage Distribution 95% 0% 5% 0% 0% 100%Total Beds 257 12 13 12 6 300Percentage Distribution 86% 4% 4% 4% 2% 100%

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 18
for at least 25 nsm of useable space assuming a 2490 mm x 1574 mm bariatric bed and clearances of 1.5 meters on all three sides of the bed. The Palliative Care room has been programmed at 28 nsm to allow for extra space for family to room in if necessary. The 6 High Acuity beds collocated with Palliative Care have also been programmed at 28 nsm to allow for flexible use of this space. The High Acuity rooms, which are part of the Standard Residential Unit, have been programmed at the typical size of 24 nsm. To accommodate the updated care mix, as described in Section F, a Mental Health Unit and a High Acuity Unit were incorporated into the 300-bed program requirements in addition to the Intermediate, Extended, Special, Respite/Day Care, and Palliative Care services identified in the KZA program. The building gross area in the KZA program appeared to be lower than would be anticipated using typical planning standards. It was difficult to isolate the rationale for grossing up factors. For example, mechanical and electrical spaces were originally included in the net area and grossed up. This is not normal facility planning practice, which more typically includes an overall grossing factor for such space, given that the net areas for M&E space cannot be prescribed at the time of planning. We therefore applied a methodology based on established facility planning practices that more explicitly differentiates allowances for internal component circulation, major circulation, and building systems. Although there are no widely accepted standards for Net to Building Gross multipliers for Continuing Care facilities, the generally accepted range is 1.50 to 1.60. In the updated Program a “mid-range” ratio of 1.54 was adopted for planning purposes. To provide the required net area within the total gross area the building design will have to be efficient, but there is enough leeway to achieve the quality of environment necessary for this type of facility. The Functional Program describes the requirements for the preferred 300-bed Development Option (see Section E) that involves building a new 300-bed facility in two phases. The Phase 1 facility will have 150 beds and enough support spaces or infrastructure (offices, common areas, loading, kitchen, laundry, etc.) to sustain a 300-bed facility. In the second phase, a 150-bed addition will be built to complete the facility.
BUILDING AREA REQUIREMENTS In Phase One the first three Components will be built to the scale required for a 300-bed facility – A. Shared Pubic and Resident Support; B. Administrative Support; and C. Facility and Operational Support. Three special purpose resident pods will also be built to their full scale in Phase 1 – the E. Mental Health, F. Palliative, and G. High Acuity Care components. The Respite Care/Day Program Unit (I) constructed in Phase One will not be expanded further in Phase Two. The Phase Two addition is therefore primarily another 150 Standard Resident Beds plus additional Shared Residence Support (H).

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 19
Figure 12: Requirements Summary for Two Phase 300-bed Facility
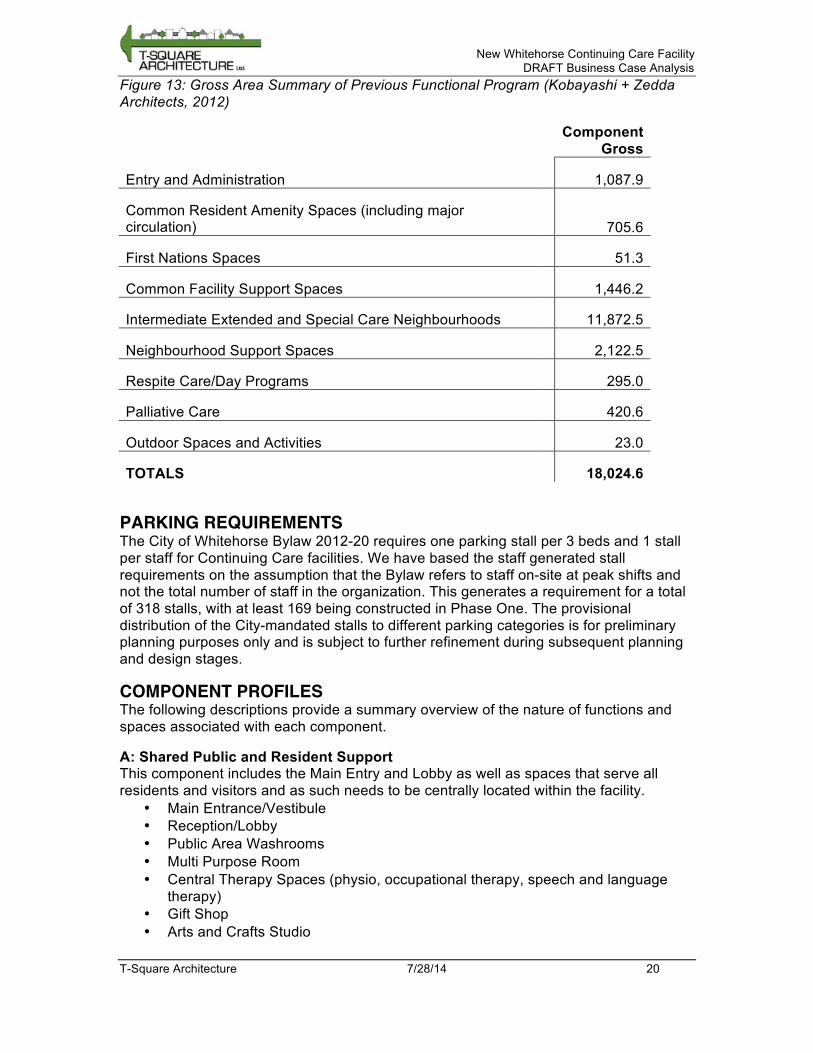
The functional program developed in this report was a refinement of the previous program produced by Kobayashi + Zedda Architects (KZA) in 2012. The current functional program uses a different methodology for applying building grossing factors and grouping spaces into components. These differences make a space-by-space comparison difficult. However, as shown in the table below, the current functional program has a gross building area of 23,233 sm where the KZA program had an overall area of 18,025 sm. The major area of increase is in the resident pods themselves. Smaller specialty units (Mental Health, Palliative Care, and High Acuity pods) require a greater overall area. The KZA program does not contain these specialty pods. Additionally, differences in building grossing factors and methodology may account for some of the difference in gross areas.
PHASE ONE150 Bed Facility (with
support for 300)
PHASE TWO150 Bed Addition
TOTAL300 Bed Facility
NetComponent
Gross NetComponent
Gross NetComponent
GrossA Shared Public and Resident Support 631.0 757.0 0.0 0.0 631.0 757.0B Administrative Support 559.0 671.0 0.0 0.0 559.0 671.0C Facility and Operations Support 918.5 1,102.0 0.0 0.0 918.5 1,102.0D Standard Resident Care Pods 4,742.5 6,023.0 6,123.5 7,776.5 10,866.0 13,799.5E Mental Health Resident Pod 576.0 731.5 0.0 0.0 576.0 731.5F Palliative Care Pod 552.0 701.0 0.0 0.0 552.0 701.0G High Acuity Care Pod 282.0 358.0 0.0 0.0 282.0 358.0H Shared Residence Support Pods 234.0 297.0 234.0 297.0 468.0 594.0I Respite Care and Day Programs/Services 234.0 297.0 0.0 0.0 234.0 297.0TOTALS 8,729.0 10,937.5 6,357.5 8,073.5 15,086.5 19,011.0
TOTAL Building Gross 13,442.7 9,790.6 23,233.2
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 20
Figure 13: Gross Area Summary of Previous Functional Program (Kobayashi + Zedda Architects, 2012)
Component Gross
Entry and Administration 1,087.9
Common Resident Amenity Spaces (including major circulation) 705.6
First Nations Spaces 51.3
Common Facility Support Spaces 1,446.2
Intermediate Extended and Special Care Neighbourhoods 11,872.5
Neighbourhood Support Spaces 2,122.5
Respite Care/Day Programs 295.0
Palliative Care 420.6
Outdoor Spaces and Activities 23.0
TOTALS 18,024.6
PARKING REQUIREMENTS The City of Whitehorse Bylaw 2012-20 requires one parking stall per 3 beds and 1 stall per staff for Continuing Care facilities. We have based the staff generated stall requirements on the assumption that the Bylaw refers to staff on-site at peak shifts and not the total number of staff in the organization. This generates a requirement for a total of 318 stalls, with at least 169 being constructed in Phase One. The provisional distribution of the City-mandated stalls to different parking categories is for preliminary planning purposes only and is subject to further refinement during subsequent planning and design stages.
COMPONENT PROFILES The following descriptions provide a summary overview of the nature of functions and spaces associated with each component.
A: Shared Public and Resident Support This component includes the Main Entry and Lobby as well as spaces that serve all residents and visitors and as such needs to be centrally located within the facility.
• Main Entrance/Vestibule • Reception/Lobby • Public Area Washrooms • Multi Purpose Room • Central Therapy Spaces (physio, occupational therapy, speech and language
therapy) • Gift Shop • Arts and Crafts Studio

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 21
• Hair and Podiatry Salon • Religious/Devotional Space • Gardening Rooms • FN Healing Room • Family Visitor's Accommodation
B: Administrative Support The reception functions of the Administrative Support Component will be located close to the main entrance. The remainder of the administrative functions and spaces can be located in other parts of the facility, but must be easily accessible by major circulation.
• Administration- General Office • Copier, Mail, and Supplies Room • Medical Records and Storage Room • Administration-Management Offices • Volunteer Room • Multiple Use Office Spaces • Other Office Spaces • Systems Training • Central Staff Room • Staff Lockers and Showers M&F
C: Facility and Operations Support This component is often referred to as “back-of-house” support functions that are usually considered a “staff” zone. Convenient access to a service entry is important, as materials transfer is one of the major activities. Transfer of food to and from the residential units is a high frequency activity and travel distances between the kitchen and residential units is an important planning consideration.
• Woodworking Shop • Kitchen (including First Nations space) • Food Services Office • Dry Storage • Freezer and Cooler • Shipping and Receiving • Oxygen Storage Room • Family Storage • Maintenance Workshop • Facility Laundry • Materials Management and Storage • Continuing Care Equipment Storage (including room to clean equipment) • General Storage Incl. Power Scooters • Central Autoclave Room • IT/Communications Room • Garbage • Recycling • Landscape Equipment Storage
D: Standard Residence Care Pods For planning purposes, a grouping of 24 beds in Phase One has been considered a “house”. In Phase Two, the groupings 4 houses of 21 beds and 3 houses of 22 beds. This is at the upper end of the number of beds considered suitable for a residence grouping. Our review of Continuing Care standards indicated that the preferred pattern is

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 22
small groupings of resident rooms co-located with living, dining, kitchen areas, resident laundry, quiet room, and bathing facilities. The Standards Review in Appendix A found that for this type of facility, the number of rooms in each pod ranges from a low of 12 to high of 32, with an average between 12 and 20. For larger pods, it is suggested that they be to broken down into smaller sub-groupings of 10 – 12. While smaller pods have a positive effect on the home-like atmosphere, they also tend to increase the per-patient cost of the overall facility. Half of one pod (12 beds) will be serviced with medical gases so that it can accommodate high acuity residents in the event that the High Acuity pod is at capacity. All pods will be designed to support the Dementia population through the use of lockable doors to prevent wandering. Each Standard pod includes resident rooms and support functions associated directly with that group of rooms.
• Resident Rooms and Bathrooms • Bariatric Resident Room and Bathroom • Janitor/Housekeeping Rooms (Plus elsewhere) • Resident Living Room • Resident Dining Room • Servery/Kitchen • Resident Activity Room • Quiet Room/Space • Care Station & Nurse Manager's Office • Medication Room • Clean Utility Room(s) • Dirty Utility Room • Staff Washroom • Resident Washroom • Wheelchair Shower and Residential Tub • Spa Washroom • Spa/Tub Room • Storage incl. Power Wheelchairs • Staff Room • Meeting Room
E: Mental Health Resident Pod This set of 12 resident beds is intended to provide a secure environment for residents who may harm themselves or represent a potential danger to other residents due to medical/behavioral issues. This may include residents with some form of dementia as well as those with mental health and substance abuse issues. The design of surfaces, fittings, and furniture must meet special standards. Two groups of 6 beds are required to provide sufficient flexibility in accommodating residents with varying conditions.
• Resident Rooms / Bathrooms (Group 1) • Secure/ Ante Room (Group 1) • Resident Rooms / Bathrooms (Group 2) • Secure/ Ante Room (Group 2) • Janitor/Housekeeping Rooms • Resident Living Room • Resident Dining Room

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 23
• Servery/Kitchen • Family Gathering Room • Assessment/Interview/Treatment Room • Care Station & Nurse Manager's Office • Staff Room • Meeting Room • Medication Room • Clean Utility Room(s) • Dirty Utility Room • Staff Washroom • Resident Washroom • Wheelchair Shower and Residential Tub • Public Washroom • Spa/Tub Room • Personal Effects Storage
F: Palliative Care Pod This set of 12 resident beds is subdivided into two sub groups of 6 beds. This component accommodates those that require a high level of care and often require medical gases. These beds should be associated with the High Acuity Pod that also requires medical gases. This proximity will facilitate use of the beds for both palliative and high acuity situations while providing suitable separation between residents with different conditions. Family members may have extended visits and convenient access to an outside entrance is therefore highly desirable.
• Palliative Care Resident Room • Family Room • Common Space • Washrooms • Care Station and Medications • Office and Meeting Room
G: High Acuity Care Pod This set of 6 resident beds accommodates those that require a high level of medical care on an urgent but temporary basis due to illness. As noted above, close proximity to Palliative Care beds is required. Similar to Palliative Care, family members may have extended visits and convenient access to an outside entrance is therefore highly desirable. One bariatric bed has been included.
• High Acuity Care Resident Rooms • Bariatric Resident Room and Bathroom • Family Room • Common Space • Washrooms • Care Station and Medications • Office and Meeting Room
H: Shared Residence Support Pods Although each resident bed pod has integral support spaces and functions, there are a number of functions that are not within the pods but rather are shared among residential

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 24
pods. These are functions that need to be close to the residential pods and are therefore not suitable for the centralized support functions that serve the full facility. The Support Pods will be located to best serve groups of Residential Pods.
• Family Meeting Rooms • Family Dining and Kitchen • Physiotherapy Spaces • Pantry/Servery • Physician Office/Exam Rooms • Social Worker Space • RAI Assessors
A single subset of this component services the joint needs of the Palliative Care and High Acuity Care Pods. Planning assumes a very high affinity between these latter 2 components to enable sharing of commonly required spaces, and subsequent planning and design initiatives may consider collapsing the 2 care pods plus the following support facilities into a single component.
• Housekeeping • Staff room • Clean Utility • Dirty Utility • Staff WR • Shower Room • Spa WR • Tub Room • Storage
I: Respite Care and Day Program Services These services support families and caregivers who reside in their own homes and not at the Care Facility. Respite clients may use available beds in Standard Residential Units if needed. The following spaces accommodate recreational, physiotherapy, and occupational therapy functions associated with the Day Program. Convenient access from drop-off points and parking are important considerations.
• Day Program/Respite Entry Vestibule • Day Program Room • Kitchen/Servery • Day Program Storage • Day Program Nap Room • Respite and Day Program Spa Bathing • Day Program Office • Washrooms
COMPONENT RELATIONSHIPS Figure 12: Component Relationship Diagram (below) should not be viewed as a floor plan but rather as a two dimensional diagram that illustrates a number of important relationships among the components and major circulation.
• The Main Entry should be clearly identifiable from main avenues of approach and from visitor parking.
• Staff Parking should be located to provide convenient access to a building entrance.

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 25
• Shared Public Functions (A) should be located at a central point within the facility and provide equitable access for residents in both phases and be conveniently accessible from the main entrance.
• Shared Residence Support Pods should be located with Residential Pods to provide equitable access from the pods served.
• Palliative and High Acuity Care Pods to be located in close proximity and near a secondary entry
• Convenient connections from ground level Residential Pods to outdoor spaces are desirable
• All pedestrian entries and exits must be barrier free and have appropriate secure access controls.
Figure 14: Component Relationship Diagram
A
B
C
I
MAIN ENTRY
Loading Entry
F
H
Secondary Entry
E
Legend
patio / garden area
A: Shared Public and Resident Support B: Administrative Support
C: Facility and Operations Support
D: Standard Resident Care Pods
H: Shared Residence Support Pods E: Mental Health Pod
I: Respite Care & Day Programs
G: High Acuity Care Pod
F: Palliative Care Pod
G
D
D
D
D
D
Phase 2
H
H
H
D
B
A
A
Secondary Entry
D
D D
D
D
D

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 26
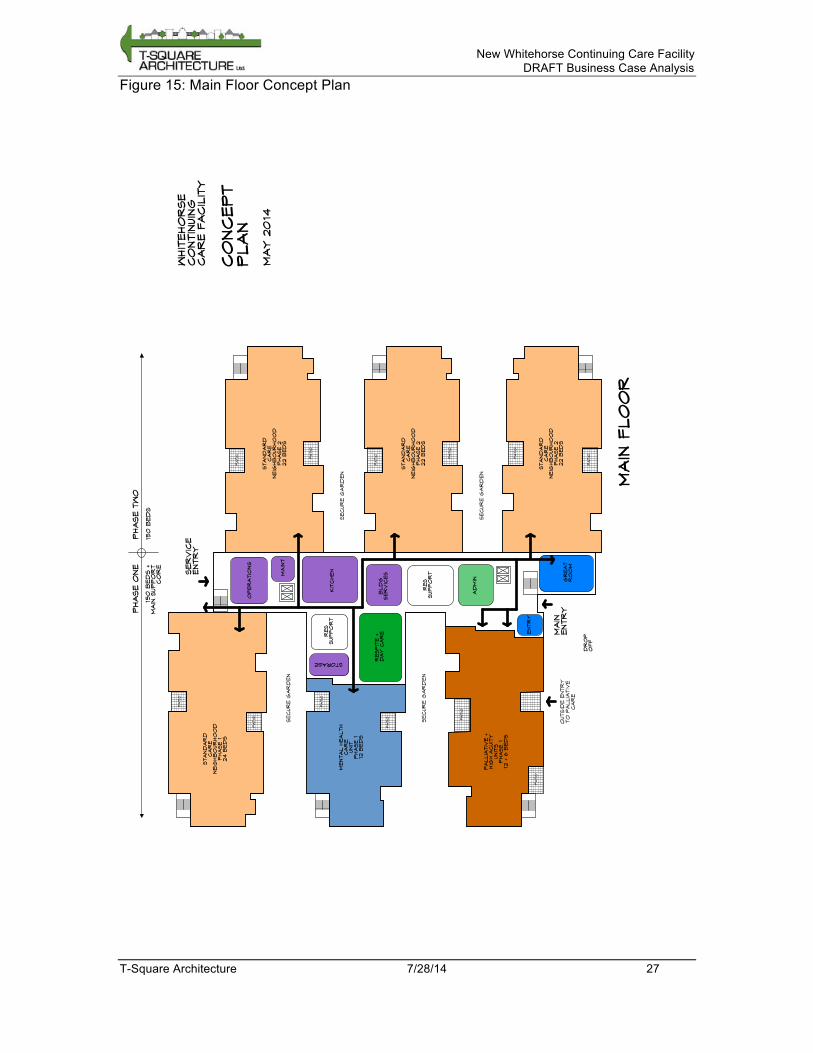
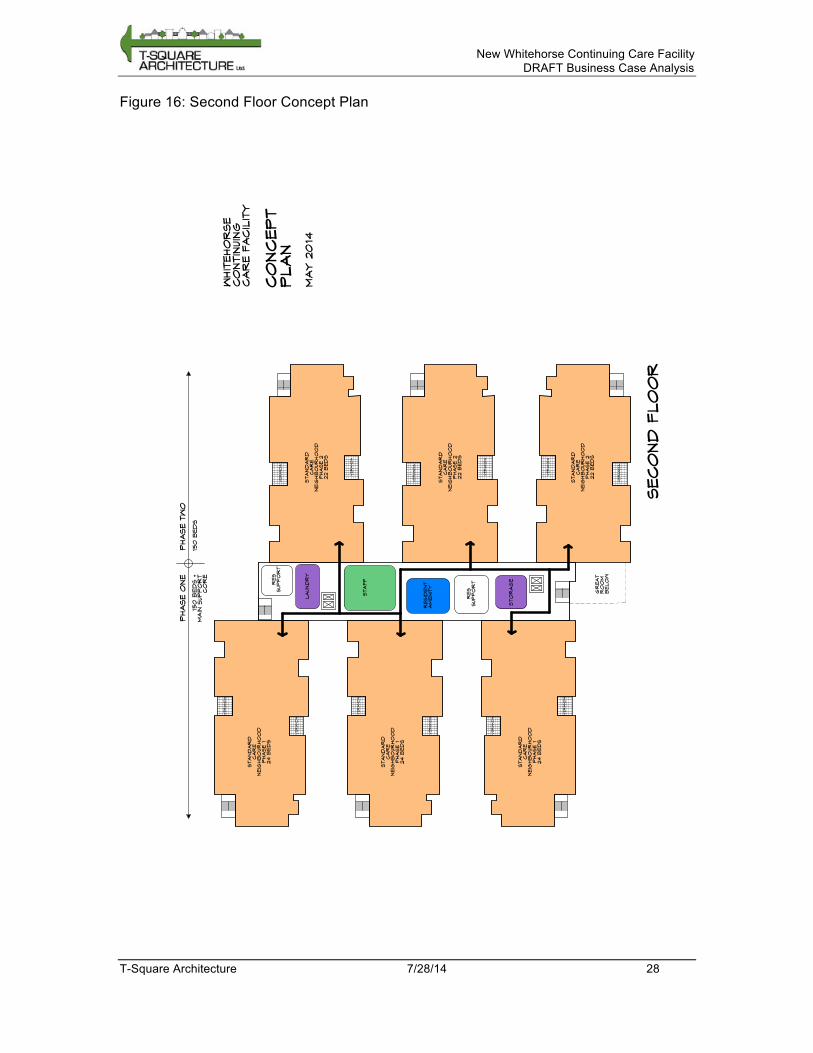
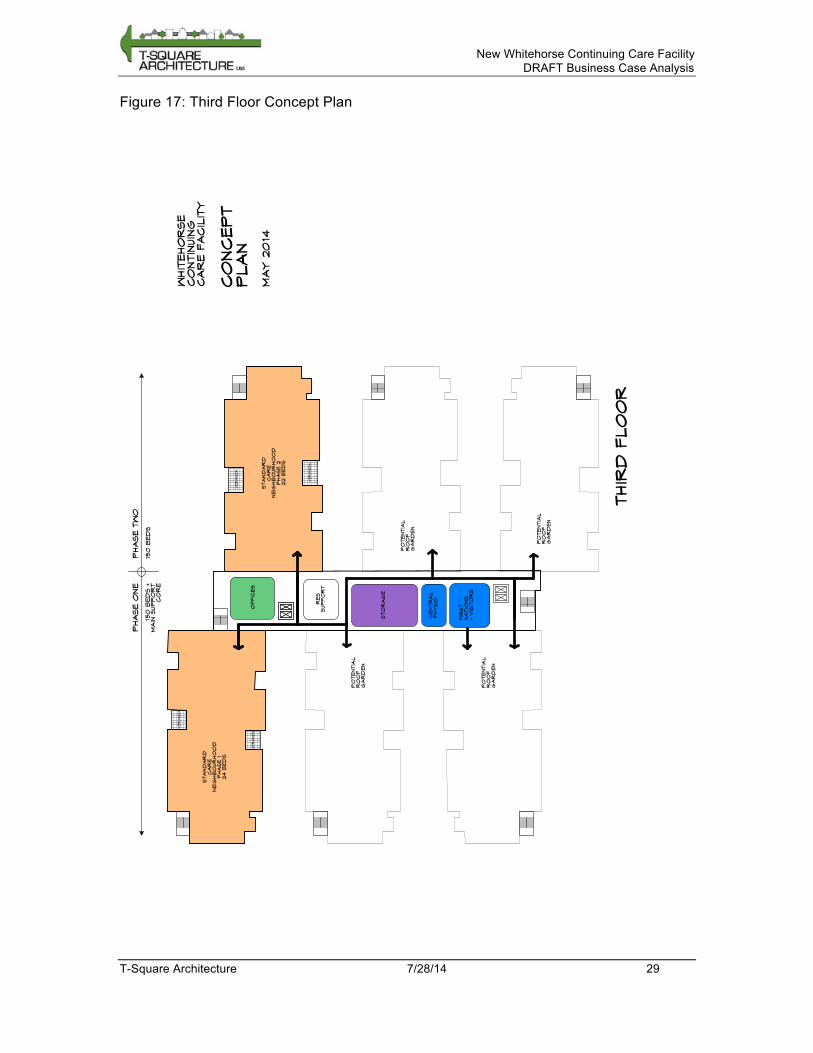
The following concept plans show a hypothetical three-floor layout for the building based on the above relationship diagram. While these diagrams are not intended to represent the final floor plan for the facility, they do serve to illustrate the viability of the concepts developed above and provide a basis for estimating the building footprint, which will be used to test potential sites in Section H: Site Selection.
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 27
Figure 15: Main Floor Concept Plan
WHIT
EHO
RSE
CO
NTIN
UIN
G
CAR
E FACIL
ITY
CO
NCEPT
PLAN
MAY 20
14
PHASE TW
OPHASE O
NE
150
B
ED
S150
B
ED
S +
MAIN
SUPPO
RT
CO
RE
PATIO
PATIO
STAND
AR
D
CAR
E
NEIG
HB
OUR
HO
OD
PHASE 1
24 B
ED
S
PATIO
PATIO
MENTAL HEALTH
CAR
E
UNIT
PHASE 1
12 B
ED
S
PATIO
PATIO
PALLIA
TIV
E +
HIG
H ACUIT
Y
UNIT
S
PHASE 1
12 + 6 B
ED
S
OUTSID
E ENTR
Y
TO
PALLIA
TIV
E
CAR
E
STAND
AR
D
CAR
E
NEIG
HB
OUR
HO
OD
PHASE 2
22 B
ED
S
PATIO
PATIO
STAND
AR
D
CAR
E
NEIG
HB
OUR
HO
OD
PHASE 2
22 B
ED
S
PATIO
PATIO
STAND
AR
D
CAR
E
NEIG
HB
OUR
HO
OD
PHASE 2
22 B
ED
S
PATIO
PATIO
MAIN
ENTR
Y
DR
OP
OFF
SER
VIC
E
ENTR
Y
GR
EAT
RO
OM
MAIN
FLO
OR
RES
SUPPO
RT
RES
SUPPO
RT
OPER
ATIO
NS
BLD
G
SER
VIC
ES
KIT
CHEN
AD
MIN
ENTR
Y
STORAGE
SECUR
E G
AR
DEN
SECUR
E G
AR
DEN
SECUR
E G
AR
DEN
SECUR
E G
AR
DEN
MAIN
T
RESPIT
E +
DAY CAR
E
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 28
Figure 16: Second Floor Concept Plan
WHIT
EHO
RSE
CO
NTIN
UIN
G
CAR
E FACIL
ITY
CO
NCEPT
PLAN
MAY 20
14
SECO
ND
FLO
OR
PHASE TW
OPHASE O
NE
150
B
ED
S150
B
ED
S +
MAIN
SUPPO
RT
CO
RE
RES
SUPPO
RTRES
SUPPO
RT
STAND
AR
D
CAR
E
NEIG
HB
OUR
HO
OD
PHASE 2
22 B
ED
S
VERANDA
VERANDA
VERANDA
VERANDA
STAND
AR
D
CAR
E
NEIG
HB
OUR
HO
OD
PHASE 1
24 B
ED
S
VERANDA
VERANDA
STAND
AR
D
CAR
E
NEIG
HB
OUR
HO
OD
PHASE 1
24 B
ED
S
VERANDA
VERANDA
STAND
AR
D
CAR
E
NEIG
HB
OUR
HO
OD
PHASE 1
24 B
ED
S
STAND
AR
D
CAR
E
NEIG
HB
OUR
HO
OD
PHASE 2
22 B
ED
S
VERANDA
VERANDA
STAND
AR
D
CAR
E
NEIG
HB
OUR
HO
OD
PHASE 2
22 B
ED
S
VERANDA
VERANDA
GR
EAT
RO
OM
B
ELO
W
LAUND
RY
STAFF
STO
RAG
E
RESID
ENT
AM
ENIT
Y
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 29
Figure 17: Third Floor Concept Plan
WHIT
EHO
RSE
CO
NTIN
UIN
G
CAR
E FACIL
ITY
CO
NCEPT
PLAN
MAY 20
14
PHASE TW
OPHASE O
NE
150
B
ED
S150
B
ED
S +
MAIN
SUPPO
RT
CO
RE
RES
SUPPO
RT
OFFIC
ES
STO
RAG
E
CENTR
AL
PHYSIO
THIR
D FLO
OR
VERANDA
VERANDA
STAND
AR
D
CAR
E
NEIG
HB
OUR
HO
OD
PHASE 1
24 B
ED
S
STAND
AR
D
CAR
E
NEIG
HB
OUR
HO
OD
PHASE 2
22 B
ED
S
VERANDA
VERANDA
FIR
ST
NATIO
NS
+ V
ISIT
OR
S
PO
TENTIA
L
RO
OF
GAR
DEN
PO
TENTIA
L
RO
OF
GAR
DEN
PO
TENTIA
L
RO
OF
GAR
DEN
PO
TENTIA
L
RO
OF
GAR
DEN

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 30
CONCEPT DESIGN GUIDELINES The following guidelines are intended to inform pre-concept test fit analyses and deal with site selection, massing and image, patios and gardens, parking, and phasing.
Site Selection Guidelines The following guidelines were established as planning assumptions through discussions with the Steering Committee. The site:
• Must have sufficient land to accommodate the 20-year projected requirements for new beds.
• Must have immediate access to public transportation. • Must have opportunities for resident ambulatory activities like neighbourhood
walking. • Should provide opportunities to integrate with local primary/secondary schools for
learning and community programs. • Must provide continuity between indoor space and outdoor space, subject to
seasonal restrictions. Activities compatible with the current season must be accommodated.
• Must have low likelihood of encountering project delays due to zoning or community issues as time is of the essence for this project.
• Should be in an established community with public amenities such as parks, commercial spaces.
• Should not be in a community under development because of the disruption that would occur with on-going construction and noise.
The following site features were frequently noted as desirable in the Community Care Standards that were reviewed during the study (See Appendix A).
• Close to community services, residential, public transport, shopping • Provides active observable interest such as schools or parks • Easy access to other services - doctors, dentists, therapists • Safe for pedestrians
Massing and Image Guidelines Based on a review of relevant standards (Appendix A) the preferred arrangement for continuing care facilities is a single-story building solution with ample outdoor space for residents at grade or a 2 story building solution with grade level entry for both levels. This arrangement appears to be generally associated with facilities that are in the 50 to 100-bed range. In larger facilities, such as that being proposed for Whitehorse (300 beds in two phases), a single story approach can make it challenging to provide reasonable travel distances for residents to access centrally shared services and for the transporting of food and supplies to and from residential pods. A multi-story building of two or three levels will shorten travel distances, however, this arrangement can reduce the homelike setting that is considered a necessary feature and present a more institutional image inside the facility and in the external appearance. One of the determinants of the number of levels is the number of functions for which a ground level location is either imperative or highly desirable. This will establish the ground level configuration and building footprint. The remainder of the functions that do
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 31
not require ground level access can then be located on upper levels. The optimal number of levels is a function of access and proximity grouping factors. For the Whitehorse Continuing Care Facility a ground level location is required for all entrances and is considered imperative or highly desirable for the following components:
• A Shared Public and Resident Support (includes reception functions) • C Facility and Operations Support • D Standard Resident Care Pods (critical to have as many pods as possible) • E Mental Health Resident Pod • F Palliative Care Pod (possibly with own entrance) • G High Acuity Care Pod
Patios and Garden Areas Guidelines Convenient access to outdoor areas should be provided from within each Residential and Care Pod, preferably from the common area associated with that “house” or grouping. Access from within the residence pod should be barrier free. At ground level, some form of perimeter control should be provided. Wind and weather protection will be required on above ground patios and possibly on ground level garden areas. Conventional community care facility standards typically allow 2 square meters per bed for outdoor patios and garden spaces. In the estimates for the Whitehorse facility we have allowed 3 square meters per bed to reflect the emphasis placed on the importance of this type of space in a northern context. However, it is recognized that this is a provisional allowance subject to further refinement.
Parking Area Guidelines Surface parking should be organized so that it is not all centralized in one large lot. Visitor parking should be close to the main entry and drop off. Staff Parking should be located convenient to staff entrances. Maintenance vehicles and Handybus parking should be close to the loading entry. Landscaping will be required to mitigate the visual impact of large paved parking areas.
Phasing Guidelines The configuration of Phase 1 should facilitate the construction of Phase 2 and minimize disruption for Phase One environment and operations. This will include consideration of the location of vehicle and equipment access routes during construction of Phase 1.
ENERGY AND SUSTAINABILITY STRATEGY The development of a sustainable building requires a multi-step approach, and should begin long before the decision to build a new building has been made. At the building program stage, also known as a pre-design or conceptual phase of planning, sustainability goals and considerations are important to identify. YG does have some very strong commitments to energy and greenhouse gas emission reductions that should be reviewed and reflected in the phased development of this continuing care facility. Through the Climate Change Action Plan (2009) YG has committed to reducing greenhouse gas emissions by 20% by 2015 and becoming
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 32
carbon neutral by 2020. Setting a high standard for energy performance in this new facility is beneficial to contributing toward meeting these targets. The following generic guiding principles should be considered in application to the building of this continuing care facility in the Yukon.
• Site: Low-emitting and fuel efficient vehicles through provision of vehicle charging stations and light pollution reduction (both interior and exterior)
• Energy: Optimum energy performance (compared to conventional construction),
renewable energy (solar) and an ability to measure and verify energy consumption.
• Materials and Resources: Storage and Collection of recyclables, space
requirements as well as flow of materials should reflect strategic planning and resourcing for deliberate minimizing of construction waste through careful management.
• Indoor Environmental Quality: Use low-emitting materials and incorporate
lighting and building controls (thermal).
• Innovation in Design: Optimal opportunities in these basic principles based on general climate conditions and Canadian North location.
These basic guidelines are preliminary in nature and should be culminated in a more detailed process as the building moves into the design stage. Establishing individual responsibilities and timelines for all project partners to ensure the realization of the projects energy and sustainability goals is important to achieving above average performance outcomes.
H. Site Selection Selection of sites is based on a number of criteria, both functional and financial. Functional criteria include:
• Compatibility of surrounding area: Is the site embedded within a pre-existing community?
• Adequacy of space: Is the site large enough to support the building, parking lot, and landscaped areas without significant restrictions to the design or layout?
• Adequate access: Is the site located on suitable collector road, and does the shape of the site allow for good access?
Since the facility is expected to have a 50-year service life, it is important that potential sites be evaluated with a view towards this time frame. The evaluation must not look only at the site itself, and its ability to support the proposed facility, but at the surrounding environment as well. Future anticipated uses of surrounding areas, especially in the case of currently undeveloped land, can change, often substantially. What is suitable in the context of current plans may be totally unsuitable relative to future plans.
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 33
The financial evaluation involves a comparison of capital costs. Some major cost differences will arise from the soil conditions of each site (which may require more robust and expensive foundations), and the need for blasting. The following commentary describes the vital details of each site, including a description of the zoning status, an overview of the surrounding area, and a description of the site itself. It was found that all three sites would require zoning to PS (Public Services) zoning, and would also require an additional variance to allow for a Floor Area Ratio (FAR) of greater than 0.5.
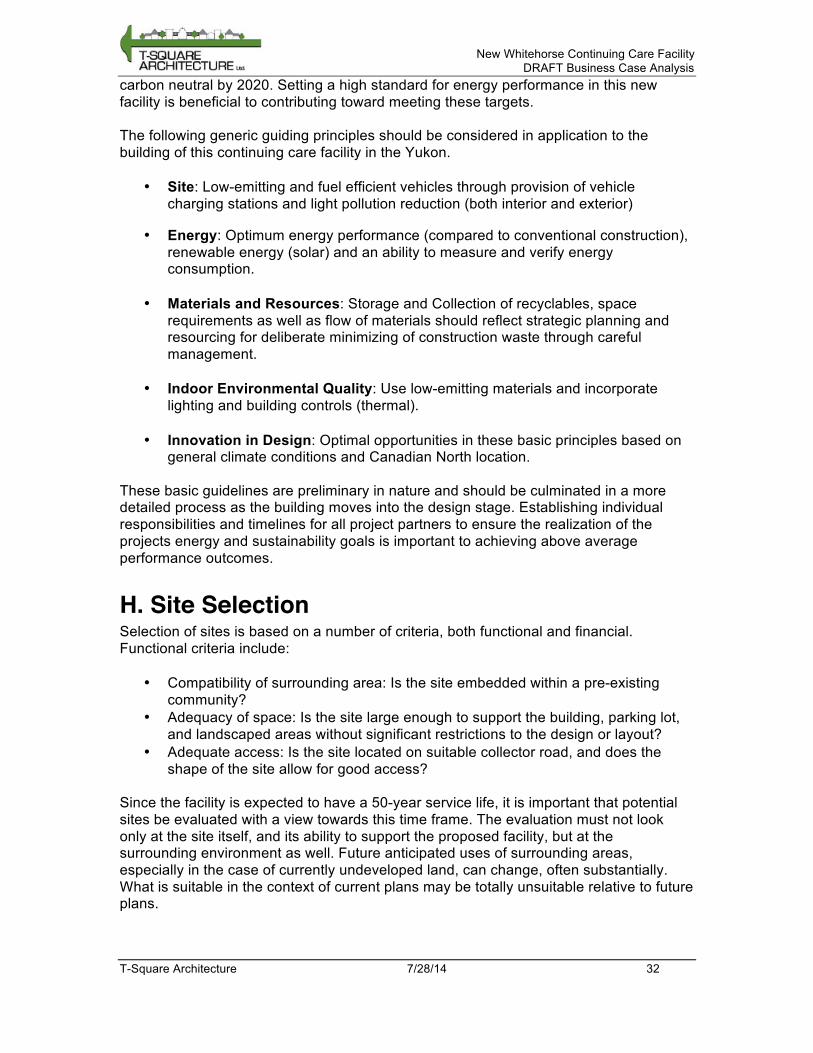
PORTER CREEK Figure 18: Aerial View of Porter Creek Site
Area: 4.16 Ha (Lot 1: 2.22 Ha, Lot 2: 1.94 Ha) Rezoning: Required for Lot 2 from RS (Residential Single Detached) to PS (Public Services), including rezoning for Floor Area Ratio (FAR) OCP Amendment: Not required
Location The site is located adjacent to Porter Creek Secondary School, within an existing sub-division of mostly single-family residential development. Porter Creek Centre is the closest commercial area to the north on Wann Road, though at 2km away it is not a walkable distance. Bus service to the area is excellent, owing to the high school and established residential neighbourhood.
Site The site has varied, original topography including organic ground cover, original trees (mostly coniferous) and some significant rock outcrops. To accommodate both Phases I and II on this site it is anticipated that selective blasting of the rock outcrops with associated rock removal would be required. In addition, clearing and grubbing will be necessary along with a blend of cutting and filling to establish a level grade for both building and parking. For the purpose of evaluation, it was assumed that the site would be graded approximately two meters above Hickory Street, allowing for an efficient cut
Porter Creek Site
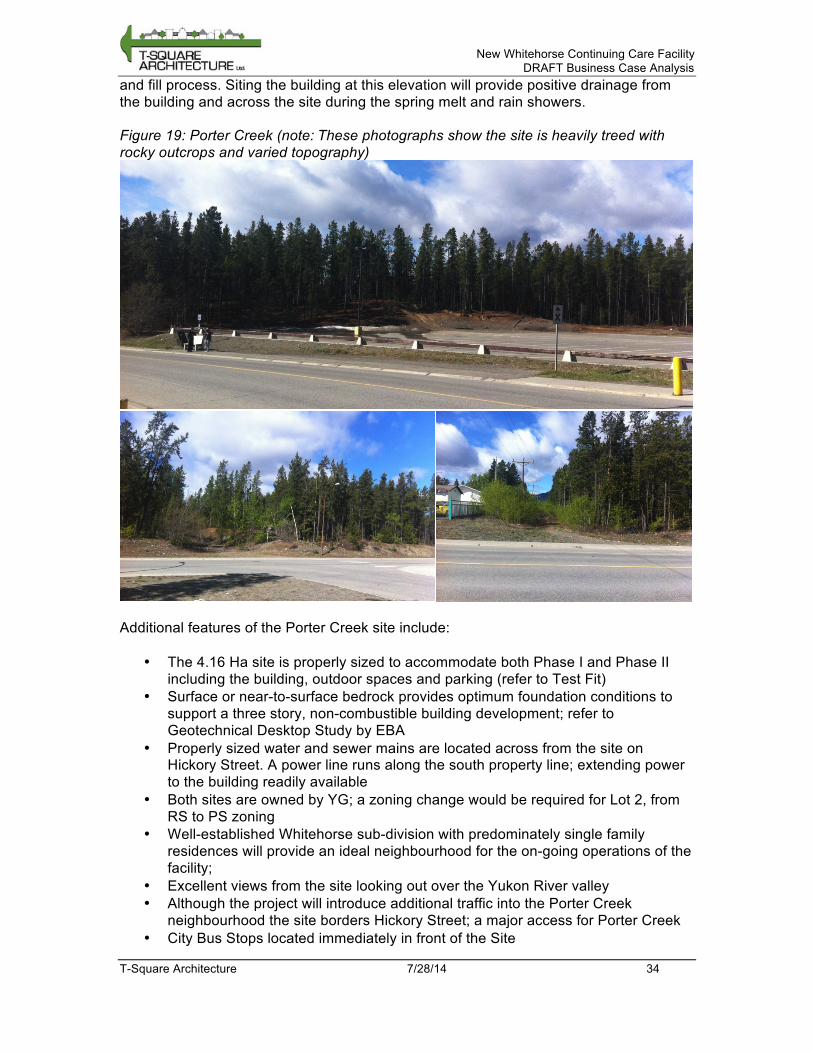
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 34
and fill process. Siting the building at this elevation will provide positive drainage from the building and across the site during the spring melt and rain showers. Figure 19: Porter Creek (note: These photographs show the site is heavily treed with rocky outcrops and varied topography)
Additional features of the Porter Creek site include:
• The 4.16 Ha site is properly sized to accommodate both Phase I and Phase II including the building, outdoor spaces and parking (refer to Test Fit)
• Surface or near-to-surface bedrock provides optimum foundation conditions to support a three story, non-combustible building development; refer to Geotechnical Desktop Study by EBA
• Properly sized water and sewer mains are located across from the site on Hickory Street. A power line runs along the south property line; extending power to the building readily available
• Both sites are owned by YG; a zoning change would be required for Lot 2, from RS to PS zoning
• Well-established Whitehorse sub-division with predominately single family residences will provide an ideal neighbourhood for the on-going operations of the facility;
• Excellent views from the site looking out over the Yukon River valley • Although the project will introduce additional traffic into the Porter Creek
neighbourhood the site borders Hickory Street; a major access for Porter Creek • City Bus Stops located immediately in front of the Site

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 35
• Building can be located on the site as close to PCSS as possible with a pedestrian connector path; also, Jack Hulland Elementary School is located a short bus ride from the site
• Green spaces and neighbourhood parks located in close proximity to the site • With the introduction of a traffic circle at the intersection of Hickory and Tamarack
the smooth flow of traffic to and from the site will be minimized • A treed buffer zone between the existing single family residences and the new
Whitehorse Continuing Care Facility can be provided
Test Fit The test fit below shows a potential layout for the site to demonstrate feasibility. In this test fit, access is provided with the introduction of a traffic circle at the intersection of Hickory and Tamarack, with secondary access from Hemlock Street. From this test fit, we can see that the site is large enough for the building, parking lot, and landscaped areas.

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 36
Figure 20: Porter Creek Test Fit
1
2
Are
a=
1.9
4 h
a
Are
a=
2.2
2 h
a
405
420
422
429
296
421
P I N E
428
427
S P R
U C
E
401
402
403
404
419
418
423
1298
1299
426
417-2
417-1
400
399
398
397
396
LA
NE
S T R
E E
T
476
E L
E V
E N
T H
A
V E
N U
E
456
451-2
451-1
477
455
454
453
452
465
464
463
T A M
A R
A C
K
GR
EEN
BELT
1082
415518
H E M
L O C
K
406
468
467414
413
412
411
410
409
408
407
519
520
521
522
523
1249
532
531
530
529
1250
526
525
524
RE
M
527
RE
M
H I C K O R Y
471
470
469
472
473
474
416
1062A
1038
1039
1040
1041
1042
1043
1113
1128
1129
1130
1131
1132
1133
1134
1136
1135
1081
1080
1079
1078
1063
1064
1065
1066
1068
1069
1070
1071
1072
1073
1074
1075
1076
1077
1037
1251
1551
1550
1143
1137
D R
I V E
1060
1059
1058
1057
GR
EEN
BELT
1044
1056
1045
1046
1055
1047
1048
1049
1088
1085
1084
1108
1109
1110
1111
1112
1114
1083
T A M
A R
A C
K
1115
A V
E N
U E
T W
E L
F T
H
S T R
E E
T
1623
16
71
140.5m
201m
109.7m
Hickory St
Tam
ara
ck
Drive
PED
ESTR
IAN
ACCESS
TO
SCHO
OL
PR
OPO
SED
TR
AFFIC
CIR
CLE
PO
RTER
CR
EEK
SIT
E
LO
TS 1 + 2
4.16 HA
DELIV
ER
Y
SER
VIC
E
NORTH
MAY 20
14
PAR
KIN
G
SITE
ENTRY
PO
TENTIA
L
SECO
ND
ENTRY
POTENTIA
L
LANE
ENTR
Y
MAIN
ENTR
ANCE
SIT
ING
O
PTIO
N
3 S
TOREY
SUPPORT
CORE
3 STO
REY
CARE WIN
G
PHASE 2
2 STO
REY
CARE WIN
G
PHASE 2
3 STO
REY
CARE WIN
G
2 STO
REY
CARE WIN
G
2 STO
REY
CARE WIN
G
PHASE 2
2 STO
REY
CARE WIN
G
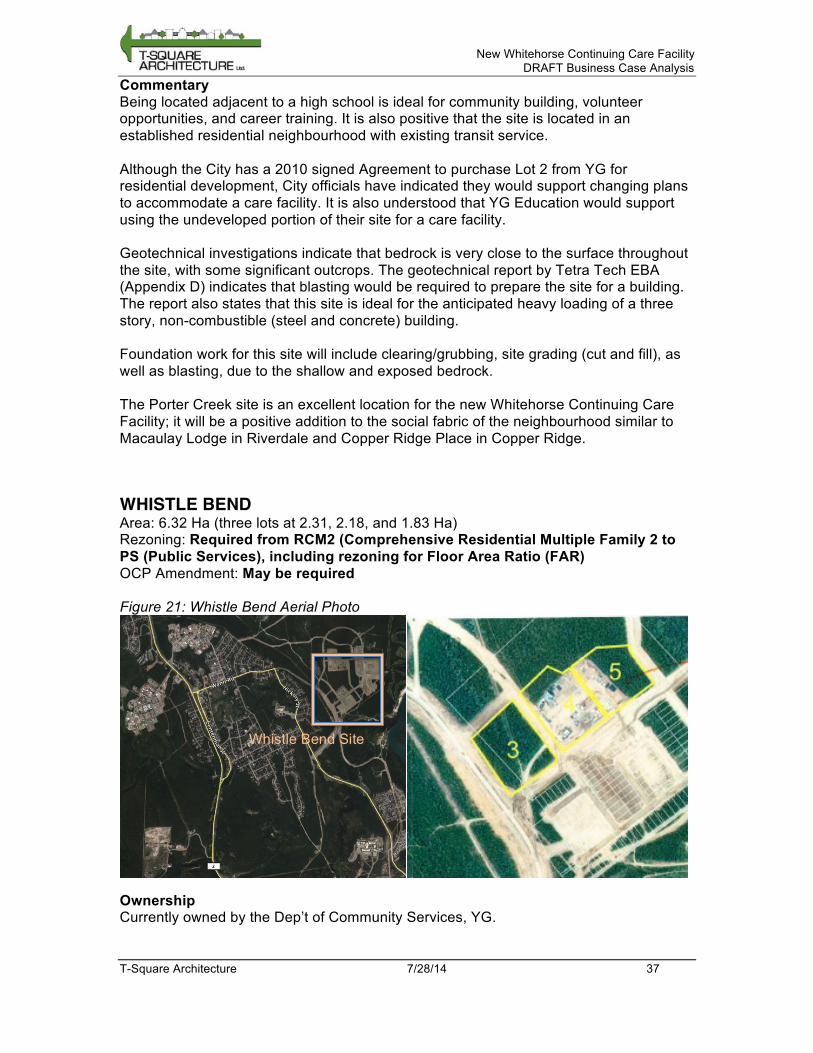
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 37
Commentary Being located adjacent to a high school is ideal for community building, volunteer opportunities, and career training. It is also positive that the site is located in an established residential neighbourhood with existing transit service. Although the City has a 2010 signed Agreement to purchase Lot 2 from YG for residential development, City officials have indicated they would support changing plans to accommodate a care facility. It is also understood that YG Education would support using the undeveloped portion of their site for a care facility. Geotechnical investigations indicate that bedrock is very close to the surface throughout the site, with some significant outcrops. The geotechnical report by Tetra Tech EBA (Appendix D) indicates that blasting would be required to prepare the site for a building. The report also states that this site is ideal for the anticipated heavy loading of a three story, non-combustible (steel and concrete) building. Foundation work for this site will include clearing/grubbing, site grading (cut and fill), as well as blasting, due to the shallow and exposed bedrock. The Porter Creek site is an excellent location for the new Whitehorse Continuing Care Facility; it will be a positive addition to the social fabric of the neighbourhood similar to Macaulay Lodge in Riverdale and Copper Ridge Place in Copper Ridge.
WHISTLE BEND Area: 6.32 Ha (three lots at 2.31, 2.18, and 1.83 Ha) Rezoning: Required from RCM2 (Comprehensive Residential Multiple Family 2 to PS (Public Services), including rezoning for Floor Area Ratio (FAR) OCP Amendment: May be required Figure 21: Whistle Bend Aerial Photo
Ownership Currently owned by the Dep’t of Community Services, YG.
Whistle Bend Site
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 38
Location The Whistle Bend Subdivision is currently in the design and development stages for a residential community of up to 8,000 residents over the next 15 to 20 years with Phases I and II well underway. Design and Development are taking place under the Land Development Protocol, 2006 between City of Whitehorse and the Yukon Government.

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 39
Figure 22: Whistle Bend Subdivision Plan
Whi
stle
B
end
Site
Site
of
Futu
re
Ele
men
tary
S
choo
l
Site
of
Futu
re
Hig
h S
choo
l

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 40
Site The site consists of three lots. All are flat. Lot 3, the westernmost lot, has total tree cover, while the other two lots are mostly clear. Figure 23: Whistle Bend Site (note: the entire site is flat, while most of the site is clear of trees)
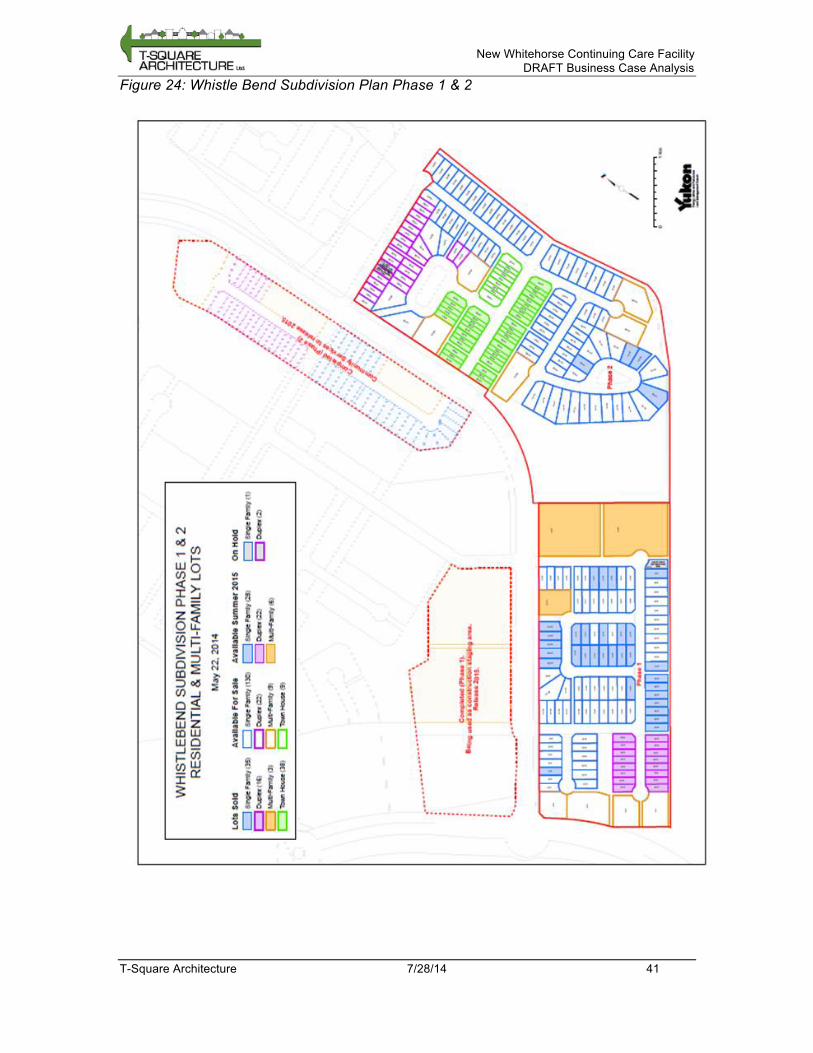
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 41
Figure 24: Whistle Bend Subdivision Plan Phase 1 & 2
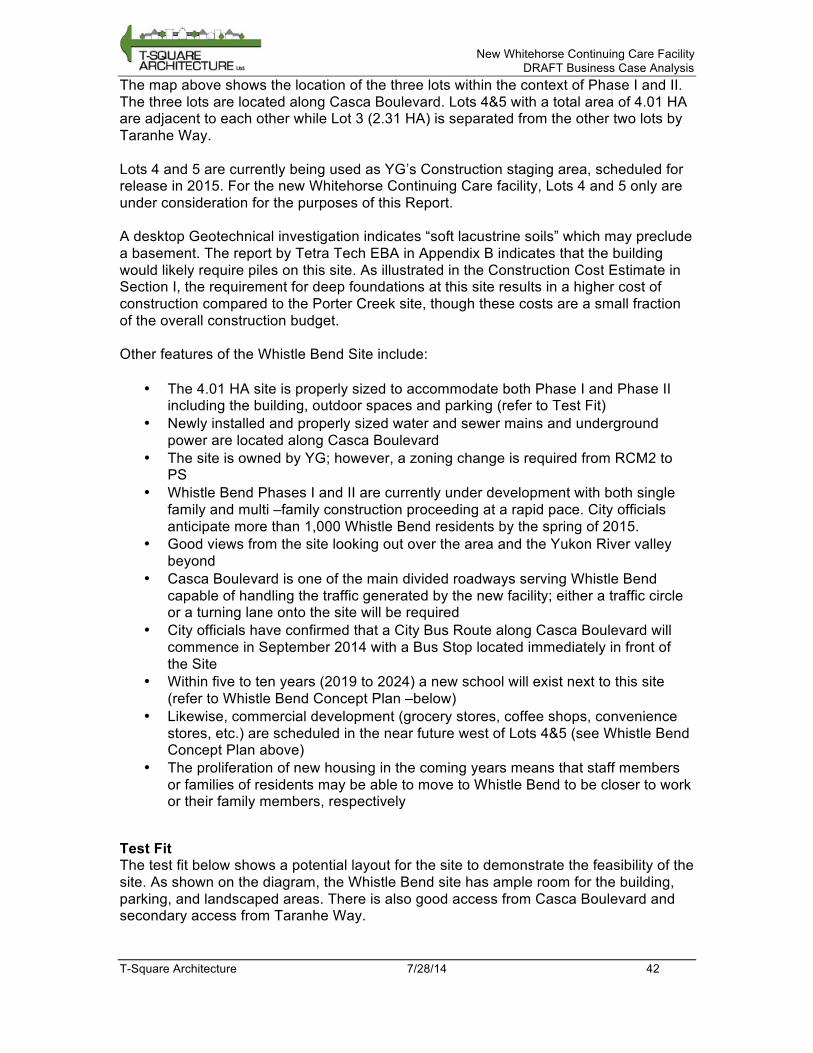
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 42
The map above shows the location of the three lots within the context of Phase I and II. The three lots are located along Casca Boulevard. Lots 4&5 with a total area of 4.01 HA are adjacent to each other while Lot 3 (2.31 HA) is separated from the other two lots by Taranhe Way. Lots 4 and 5 are currently being used as YG’s Construction staging area, scheduled for release in 2015. For the new Whitehorse Continuing Care facility, Lots 4 and 5 only are under consideration for the purposes of this Report. A desktop Geotechnical investigation indicates “soft lacustrine soils” which may preclude a basement. The report by Tetra Tech EBA in Appendix B indicates that the building would likely require piles on this site. As illustrated in the Construction Cost Estimate in Section I, the requirement for deep foundations at this site results in a higher cost of construction compared to the Porter Creek site, though these costs are a small fraction of the overall construction budget. Other features of the Whistle Bend Site include:
• The 4.01 HA site is properly sized to accommodate both Phase I and Phase II including the building, outdoor spaces and parking (refer to Test Fit)
• Newly installed and properly sized water and sewer mains and underground power are located along Casca Boulevard
• The site is owned by YG; however, a zoning change is required from RCM2 to PS
• Whistle Bend Phases I and II are currently under development with both single family and multi –family construction proceeding at a rapid pace. City officials anticipate more than 1,000 Whistle Bend residents by the spring of 2015.
• Good views from the site looking out over the area and the Yukon River valley beyond
• Casca Boulevard is one of the main divided roadways serving Whistle Bend capable of handling the traffic generated by the new facility; either a traffic circle or a turning lane onto the site will be required
• City officials have confirmed that a City Bus Route along Casca Boulevard will commence in September 2014 with a Bus Stop located immediately in front of the Site
• Within five to ten years (2019 to 2024) a new school will exist next to this site (refer to Whistle Bend Concept Plan –below)
• Likewise, commercial development (grocery stores, coffee shops, convenience stores, etc.) are scheduled in the near future west of Lots 4&5 (see Whistle Bend Concept Plan above)
• The proliferation of new housing in the coming years means that staff members or families of residents may be able to move to Whistle Bend to be closer to work or their family members, respectively
Test Fit The test fit below shows a potential layout for the site to demonstrate the feasibility of the site. As shown on the diagram, the Whistle Bend site has ample room for the building, parking, and landscaped areas. There is also good access from Casca Boulevard and secondary access from Taranhe Way.
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 43
Figure 25: Whistle Bend Test Fit
3
4
5
Are
a=
2.3
1 h
a
Are
a=
2.1
7 h
a
Are
a=
1.8
3 h
a
2
3
4
5
6
7
8
9
13
14
15
16
17
18
19
20
21
22
23
24
25
11
6 (
Park
)
27
28
29
30
31
32
33
34
35
36
37
38
39
40
41
93
92
91
94
95
96
97
98
99
10
0
10
1
10
2
10
3
10
4
10
7
10
6
10
5
87
88
89
90
80
81
82
83
84
85
86
73
74
75
76
77
78
79 42
44
45
46
47
48
49
50
51
66
67
52
G8
04
RO
AD
R/W
68
69
70
71
72
11
4
11
2
11
1
11
0
10
9
10
8
RO
AD
6
RO
AD
7
RO
AD
8
BAIL
EY P
LAC
E
ATLI
N P
LAC
EAKSALA
DR
IVE
RO
AD
9
DO
RA C
RESC
EN
T
43
10
11
12
55
56
57
58
336(
PU
L)59
60
61
62
63
64
65
337(PUL)
53
54
LAN
E 1
158(
PU
L)
159(PUL)
115(PUL)
289(
PU
L)
268(PUL)
287(PUL)
113(PUL)
338(
TR
AIL
)
46
5 R
EM
RO
AD
15 (B
ELLIN
GH
AM
CO
UR
T)
17
9
17
8
17
6
19
6
33
9 (
Park
)
33
2 (
Park
)
19
5
18
4
18
1
19
417
7
19
7
18
3
18
2
17
5
18
0
359
(TR
AIL
)
128.4m
169.7m
MAIN
ENTR
ANCE
DELIV
ER
Y
SER
VIC
E
WHIS
TLE B
END
SIT
E
LO
TS 4 + 5
4.0
0 HA
LO
T 3
2.3
1 HA
NORTH
VIS
ITO
R
PAR
KIN
G
STAFF
PAR
KIN
G
SITE
MAIN
ENTRY
SITE
SERVIC
E
ENTR
Y
MAY 20
14
3 S
TOREY
SUPPORT
CORE
3 S
TOREY
CARE
WING
PHASE
2
2 S
TOREY
CARE
WING
PHASE
23 S
TOREY
CARE
WING
2 S
TOREY
CARE
WING
2 S
TOREY
CARE
WING
PHASE
2 2 S
TOREY
CARE
WING
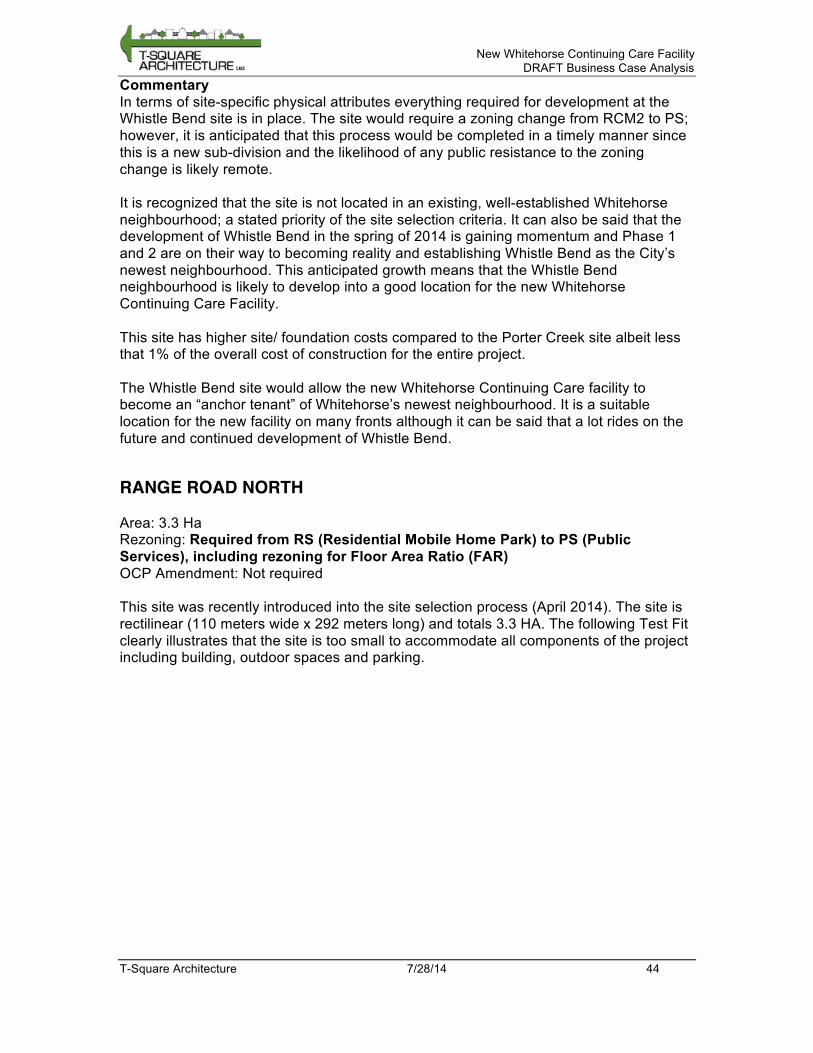
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 44
Commentary In terms of site-specific physical attributes everything required for development at the Whistle Bend site is in place. The site would require a zoning change from RCM2 to PS; however, it is anticipated that this process would be completed in a timely manner since this is a new sub-division and the likelihood of any public resistance to the zoning change is likely remote. It is recognized that the site is not located in an existing, well-established Whitehorse neighbourhood; a stated priority of the site selection criteria. It can also be said that the development of Whistle Bend in the spring of 2014 is gaining momentum and Phase 1 and 2 are on their way to becoming reality and establishing Whistle Bend as the City’s newest neighbourhood. This anticipated growth means that the Whistle Bend neighbourhood is likely to develop into a good location for the new Whitehorse Continuing Care Facility. This site has higher site/ foundation costs compared to the Porter Creek site albeit less that 1% of the overall cost of construction for the entire project. The Whistle Bend site would allow the new Whitehorse Continuing Care facility to become an “anchor tenant” of Whitehorse’s newest neighbourhood. It is a suitable location for the new facility on many fronts although it can be said that a lot rides on the future and continued development of Whistle Bend.
RANGE ROAD NORTH Area: 3.3 Ha Rezoning: Required from RS (Residential Mobile Home Park) to PS (Public Services), including rezoning for Floor Area Ratio (FAR) OCP Amendment: Not required This site was recently introduced into the site selection process (April 2014). The site is rectilinear (110 meters wide x 292 meters long) and totals 3.3 HA. The following Test Fit clearly illustrates that the site is too small to accommodate all components of the project including building, outdoor spaces and parking.
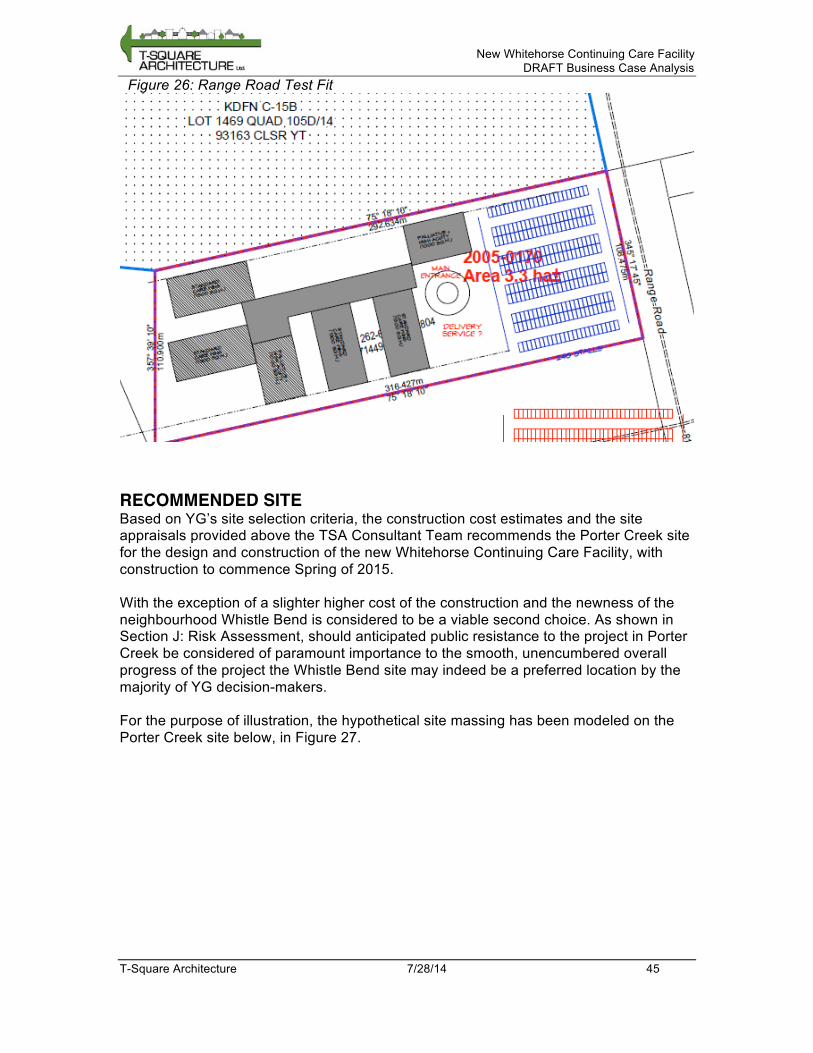
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 45
Figure 26: Range Road Test Fit
RECOMMENDED SITE Based on YG’s site selection criteria, the construction cost estimates and the site appraisals provided above the TSA Consultant Team recommends the Porter Creek site for the design and construction of the new Whitehorse Continuing Care Facility, with construction to commence Spring of 2015. With the exception of a slighter higher cost of the construction and the newness of the neighbourhood Whistle Bend is considered to be a viable second choice. As shown in Section J: Risk Assessment, should anticipated public resistance to the project in Porter Creek be considered of paramount importance to the smooth, unencumbered overall progress of the project the Whistle Bend site may indeed be a preferred location by the majority of YG decision-makers. For the purpose of illustration, the hypothetical site massing has been modeled on the Porter Creek site below, in Figure 27.
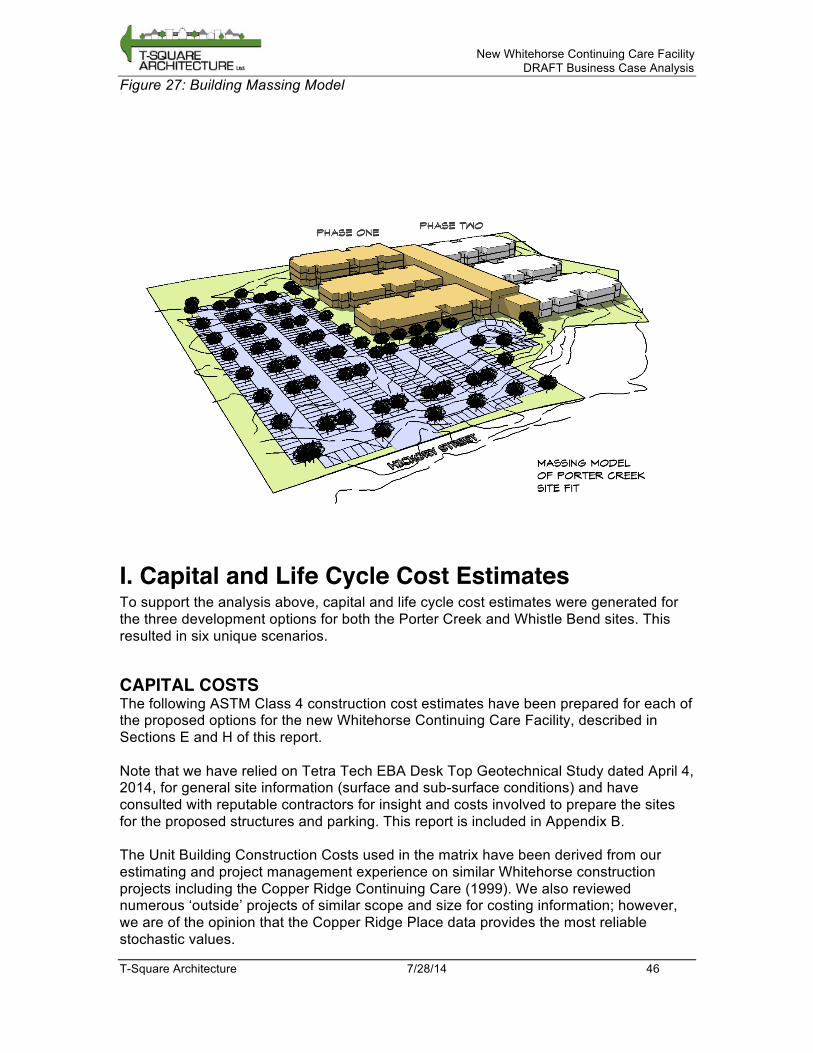
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 46
Figure 27: Building Massing Model
I. Capital and Life Cycle Cost Estimates To support the analysis above, capital and life cycle cost estimates were generated for the three development options for both the Porter Creek and Whistle Bend sites. This resulted in six unique scenarios.
CAPITAL COSTS The following ASTM Class 4 construction cost estimates have been prepared for each of the proposed options for the new Whitehorse Continuing Care Facility, described in Sections E and H of this report. Note that we have relied on Tetra Tech EBA Desk Top Geotechnical Study dated April 4, 2014, for general site information (surface and sub-surface conditions) and have consulted with reputable contractors for insight and costs involved to prepare the sites for the proposed structures and parking. This report is included in Appendix B. The Unit Building Construction Costs used in the matrix have been derived from our estimating and project management experience on similar Whitehorse construction projects including the Copper Ridge Continuing Care (1999). We also reviewed numerous ‘outside’ projects of similar scope and size for costing information; however, we are of the opinion that the Copper Ridge Place data provides the most reliable stochastic values.

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 47
All values are stated in 2014 dollars and we rely on the LCC program to index costs to the actual start date. In general, Option 1 is the least expensive development option, largely because it has the least construction area of the three options. Porter Creek is expected to be a less expensive site to build on, largely because Whistle Bend’s soil conditions will require a more expensive foundation.
LIFE CYCLE COSTS Life cycle costs were projected over a 20-year period for all six options. These costs take into account the capital costs as listed above, as well as facility systems maintenance, utility expenses, facility operations expenses, and program expenses. The life cycle cost analyses use the following key assumptions:
1. All construction capital costs include escalation to completion. There are different assumptions for design and construction scheduling for each alternative. The approval milestone for the building occupancies to start is estimated to be April 2017.
2. Program Staff Costs are escalated at 3% per Annum. 3. The Discount rate of 3.5% is used over the 20-year study period. 4. An annual escalation factor of 4% is used for operating costs. 5. An annual escalation of 4.5% is applied to utility costs. 6. An annual escalation of 4 % is used for Capital Construction and 4.25 for cyclical
renewals. 7. Market value (residual values) is not included with this study.
The life cycle costs for the six scenarios are summarized in the figure below. For more details on the methodology, as well as a breakdown of the costs listed below, see Appendix D. In terms of ongoing operation and maintenance costs, Option 1 is the least expensive. This is due mainly to the slightly lower operating and maintenance costs anticipated for a single facility. No significant O&M cost difference is expected between the two different sites. In terms of overall life cycle costs, Option 1 and Porter Creek are the cheapest development option and site respectively, due to lower construction and ongoing costs associated with both. However, the difference between the largest and smallest 20-year net present value cost is 3%. Given the preliminary nature of this estimate, and the small difference in cost between options, cost is not a major driver in the choice of development option or site.

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 48
Figure 28: Life Cycle Cost Estimate Matrix – 20-year cumulative investment (all costs $million)
J. Risk Assessment A risk assessment was prepared, considering two decisions: the choice between three development options as described in Section E, and the choice of two sites as described in Section H. For site selection, this risk assessment only considers the Porter Creek and Whistle Bend sites. Range road is excluded from the risk assessment, as it is not considered functionally suitable for this facility. The assessment identifies the following for each option:
• Description of each risk • Category of risk • Likelihood; and • Consequences
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 49
The assessment creates a numerical risk score based on the formula:
Risk score = (Likelihood × Consequences) Likelihood and Consequences are scored from 0 to 5, with 0 being impossible or inconsequential, and 5 being certain or catastrophic, respectively. This creates a range of risk scores from 0 to 25, across the following range: Score 0 No risk Score 1-5 Low Score 6-10 Medium Score 12-16 High Score 20-25 Extreme
RISK ASSESSMENT FOR DEVELOPMENT OPTION The risk assessment for development options included the three options listed in Section E: a single 300-bed facility built in two 150-bed phases, two standalone 150-bed facilities built in two phases, and a single 300-bed facility built in two phases with the capability to provide support to a third 150-bed facility built in a future phase. The total risk scores are shown below. A full breakdown of each option’s risk score is shown in Appendix E. Figure 29: Risk Assessment Scores for Development Option
Risk Score
Option1: Single 300-bed facility built in two 150-bed phases 81
Option 2: Two stand-alone 150-bed facilities 71
Option 3: Total of 450 beds, one 300-bed facility built in two 150-bed phases and separate 150-bed facility built in future phase. 85
Option 2 is considered to have the lowest risk. This is mostly associated with the flexibility of building two standalone facilities. The risk that future building code changes would make the second phase more expensive is mitigated by the fact that the design of the second-phase facility is not restricted by the first-phase facility. Additionally, building two smaller facilities mitigates the risk associated with potential public opposition to a large facility approach to care. Option 3 has the highest risk, owing mainly to a high risk of over-building in relation to demand. This risk had the highest risk score for all options, with Option 3 being particularly exposed to this risk because it builds support facilities for a third phase before the demand is fully realized.
RISK ASSESSMENT FOR SITE SELECTION The risk assessment for site selection compares the risk associated with the Whistle Bend and Porter Creek sites. The Range Road site was not considered in the risk assessment, as it is considered too small for the project. This decision is justified in Section H. A detailed breakdown of the risk assessment is shown in Appendix E.
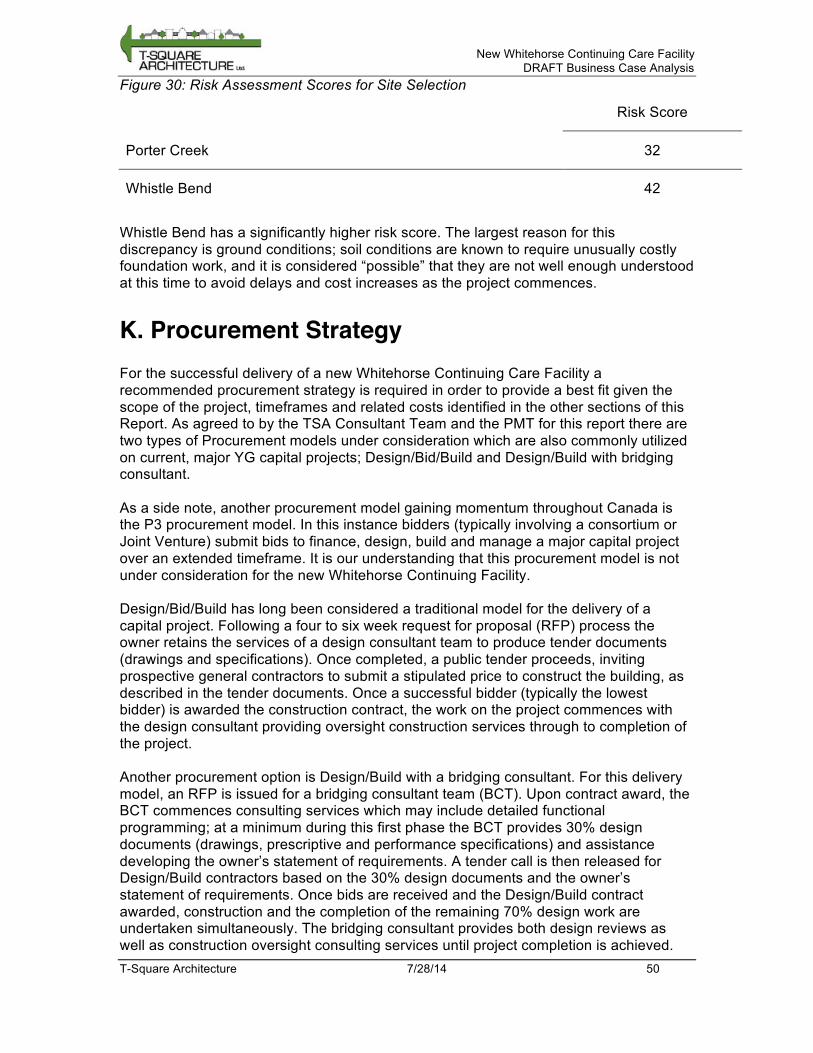
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 50
Figure 30: Risk Assessment Scores for Site Selection
Risk Score
Porter Creek 32
Whistle Bend 42
Whistle Bend has a significantly higher risk score. The largest reason for this discrepancy is ground conditions; soil conditions are known to require unusually costly foundation work, and it is considered “possible” that they are not well enough understood at this time to avoid delays and cost increases as the project commences.
K. Procurement Strategy For the successful delivery of a new Whitehorse Continuing Care Facility a recommended procurement strategy is required in order to provide a best fit given the scope of the project, timeframes and related costs identified in the other sections of this Report. As agreed to by the TSA Consultant Team and the PMT for this report there are two types of Procurement models under consideration which are also commonly utilized on current, major YG capital projects; Design/Bid/Build and Design/Build with bridging consultant. As a side note, another procurement model gaining momentum throughout Canada is the P3 procurement model. In this instance bidders (typically involving a consortium or Joint Venture) submit bids to finance, design, build and manage a major capital project over an extended timeframe. It is our understanding that this procurement model is not under consideration for the new Whitehorse Continuing Facility. Design/Bid/Build has long been considered a traditional model for the delivery of a capital project. Following a four to six week request for proposal (RFP) process the owner retains the services of a design consultant team to produce tender documents (drawings and specifications). Once completed, a public tender proceeds, inviting prospective general contractors to submit a stipulated price to construct the building, as described in the tender documents. Once a successful bidder (typically the lowest bidder) is awarded the construction contract, the work on the project commences with the design consultant providing oversight construction services through to completion of the project. Another procurement option is Design/Build with a bridging consultant. For this delivery model, an RFP is issued for a bridging consultant team (BCT). Upon contract award, the BCT commences consulting services which may include detailed functional programming; at a minimum during this first phase the BCT provides 30% design documents (drawings, prescriptive and performance specifications) and assistance developing the owner’s statement of requirements. A tender call is then released for Design/Build contractors based on the 30% design documents and the owner’s statement of requirements. Once bids are received and the Design/Build contract awarded, construction and the completion of the remaining 70% design work are undertaken simultaneously. The bridging consultant provides both design reviews as well as construction oversight consulting services until project completion is achieved.

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 51
SWOT ANALYSIS The following SWOT Analysis has been assembled to highlight the Strengths, Weaknesses, Opportunities and Threats for both procurement models: Figure 31: SWOT Analysis – Design/ Bid /Build Strengths Weaknesses
• Industry-wide familiarity with this process; including roles and responsibilities
• Well defined scope of work for bidding purposes
• Owner controls quality of the work throughout
• Design changes can be made before work begins
• Best suited for projects that are budget sensitive but not extremely schedule sensitive
• Requires sequential scheduling of each phase resulting in lengthy overall design and construction process
• Contractor brought into project post-design; effective alternates cannot be entertained
• Requires considerable owner expertise
• No fast –tracking available if needed
• High potential for costly change orders if design documents are lacking
• Undue pressure on designer to estimate and make educated guesses in the absence of GC’s experience and relationships in the construction industry
Opportunities Threats • Separate competitive processes for
both designer and contractor that can improve efficiencies and quality of work for the owner
• Designer can remain impartial; always looks out for owner’s best interests
• If project overdesigned delays may occur
• Potential for disputes and delays since design & construction team may have opposite goals; cost effectiveness vs. acceptable quality.
• Relationships can be adversarial • Owner at risk to contractor for
design errors
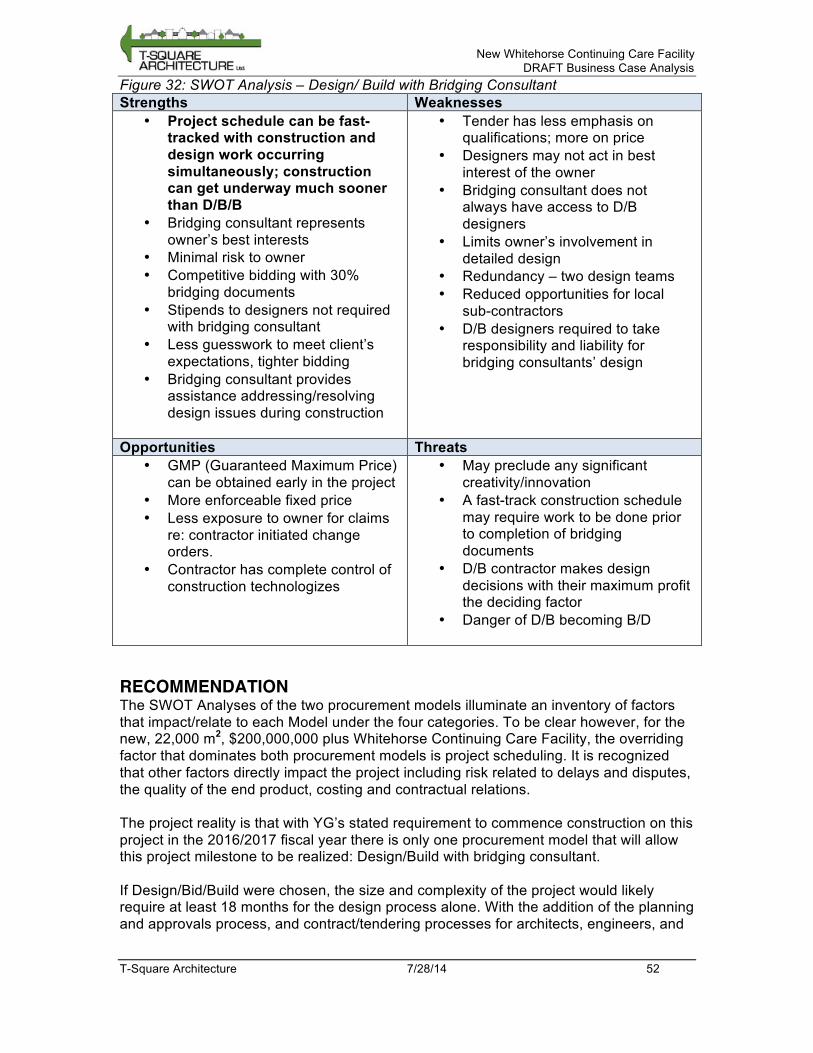
New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 52
Figure 32: SWOT Analysis – Design/ Build with Bridging Consultant Strengths Weaknesses
• Project schedule can be fast-tracked with construction and design work occurring simultaneously; construction can get underway much sooner than D/B/B
• Bridging consultant represents owner’s best interests
• Minimal risk to owner • Competitive bidding with 30%
bridging documents • Stipends to designers not required
with bridging consultant • Less guesswork to meet client’s
expectations, tighter bidding • Bridging consultant provides
assistance addressing/resolving design issues during construction
• Tender has less emphasis on qualifications; more on price
• Designers may not act in best interest of the owner
• Bridging consultant does not always have access to D/B designers
• Limits owner’s involvement in detailed design
• Redundancy – two design teams • Reduced opportunities for local
sub-contractors • D/B designers required to take
responsibility and liability for bridging consultants’ design
Opportunities Threats • GMP (Guaranteed Maximum Price)
can be obtained early in the project • More enforceable fixed price • Less exposure to owner for claims
re: contractor initiated change orders.
• Contractor has complete control of construction technologizes
• May preclude any significant creativity/innovation
• A fast-track construction schedule may require work to be done prior to completion of bridging documents
• D/B contractor makes design decisions with their maximum profit the deciding factor
• Danger of D/B becoming B/D
RECOMMENDATION The SWOT Analyses of the two procurement models illuminate an inventory of factors that impact/relate to each Model under the four categories. To be clear however, for the new, 22,000 m2, $200,000,000 plus Whitehorse Continuing Care Facility, the overriding factor that dominates both procurement models is project scheduling. It is recognized that other factors directly impact the project including risk related to delays and disputes, the quality of the end product, costing and contractual relations. The project reality is that with YG’s stated requirement to commence construction on this project in the 2016/2017 fiscal year there is only one procurement model that will allow this project milestone to be realized: Design/Build with bridging consultant. If Design/Bid/Build were chosen, the size and complexity of the project would likely require at least 18 months for the design process alone. With the addition of the planning and approvals process, and contract/tendering processes for architects, engineers, and

New Whitehorse Continuing Care Facility DRAFT Business Case Analysis
T-Square Architecture 7/28/14 53
contractors, it would be unlikely that construction would be able to begin in the 2016/2017 fiscal year. With the recommended Design/Build process, a bridging consultant should be retained as soon as this report is accepted. To elaborating on the recommended Design/Build with bridging consultant procurement model: once the business case analysis and pre-concept planning final report is released in July 2014, it is recommended that YG issue an RFP to retain the services of a bridging consultant team. It is anticipated that the bridging consultant RFP process would be completed and a contract award in place by August 2014. Allowing for seven months to produce 30% design documents and the statement of requirements the D/B contract can in turn be tendered and awarded by May 2015.