why are we redesigning the long- term care system?
TRANSCRIPT

Why are we redesigning the long-term care system?

2
Concerns and issues... ACCESS--Can people get the services they need,
when they need them?
CHOICE--Do people who need long-term care have a choice, or are they just ‘slotted in’ to what is available in their community?
QUALITY--Do long-term care services work to support a good quality of life?
ECONOMY--Are we spending more money than is necessary?
3
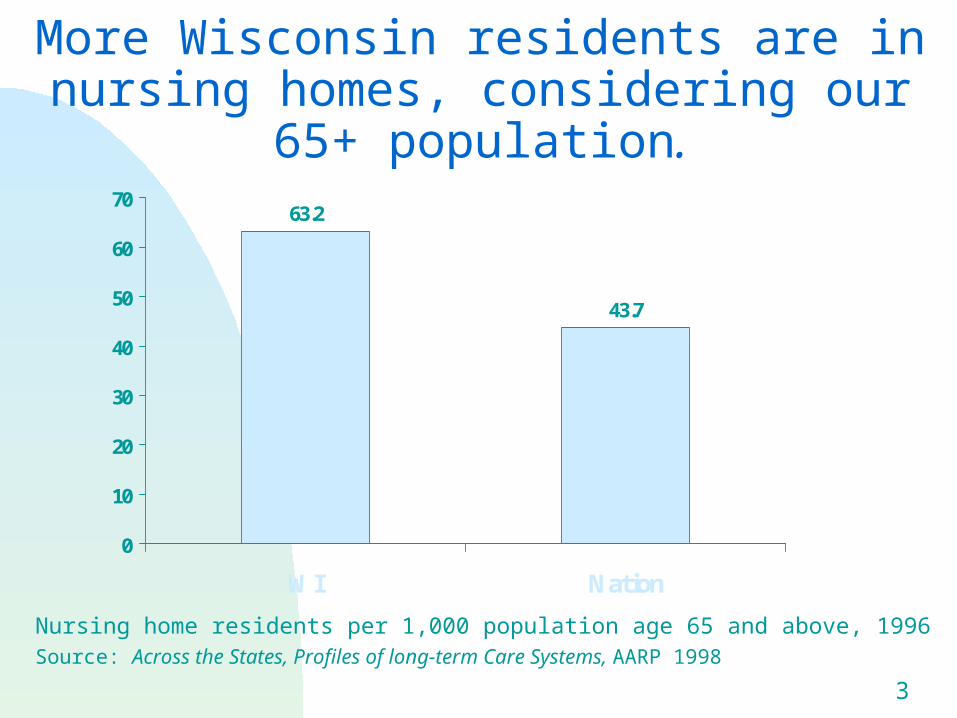
More Wisconsin residents are in nursing homes, considering our 65+
population.
Nursing home residents per 1,000 population age 65 and above, 1996Source: Across the States, Profiles of long-term Care Systems, AARP 1998
63.2
43.7
0
10
20
30
40
50
60
70
WI Nation

4
WI Medicaid spends more per capita on long-term care than the
national average.
$167
$47
$105
$320
$141
$35
$65
$241
$0
$50
$100
$150
$200
$250
$300
$350
WIU.S.
Nursing Homes
ICF-MR Home Care
Total LTC
Per capita Medicaid expenditures for long-term care services, 2000
5
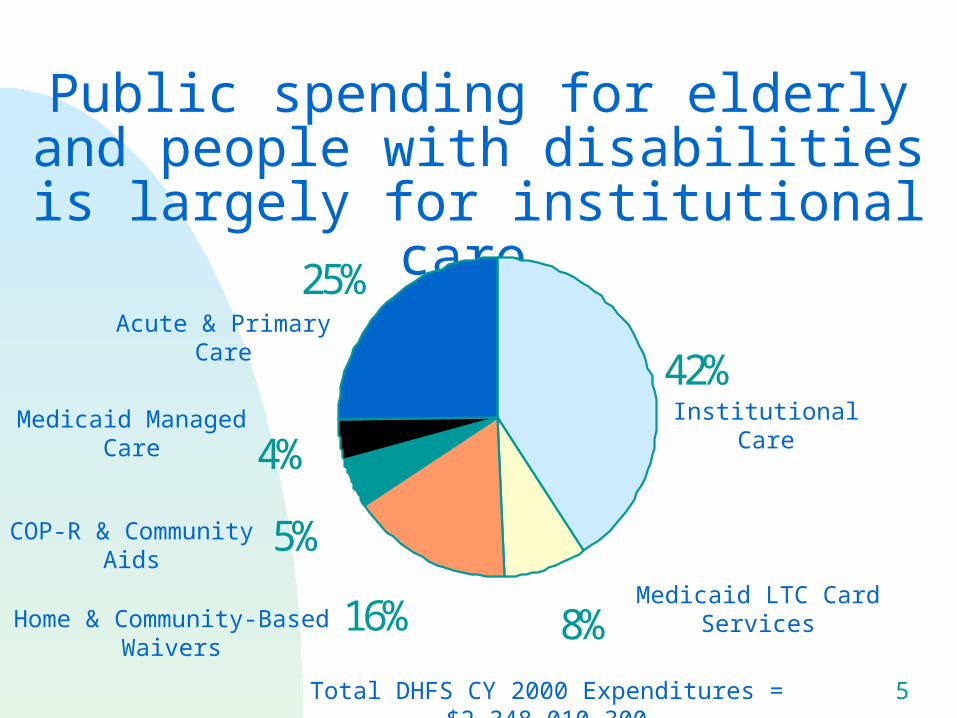
Public spending for elderly and people with disabilities is largely for institutional care.
42%
8%16%
5%
4%
25%
Institutional Care
Acute & Primary Care
Home & Community-Based Waivers
Medicaid LTC Card Services
COP-R & Community Aids
Medicaid Managed Care
Total DHFS CY 2000 Expenditures = $2,348,010,300
6
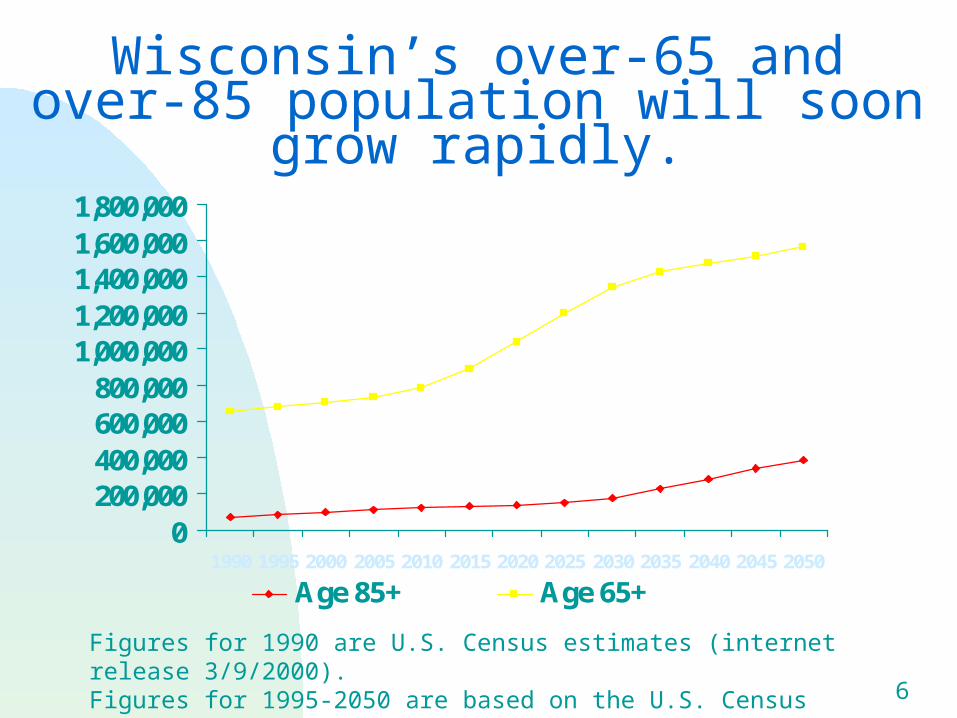
Wisconsin’s over-65 and over-85 population will soon grow rapidly.
0200,000400,000600,000800,000
1,000,0001,200,0001,400,0001,600,0001,800,000
1990 1995 2000 2005 2010 2015 2020 2025 2030 2035 2040 2045 2050
Age 85+ Age 65+
Figures for 1990 are U.S. Census estimates (internet release 3/9/2000). Figures for 1995-2050 are based on the U.S. Census population projections.
7
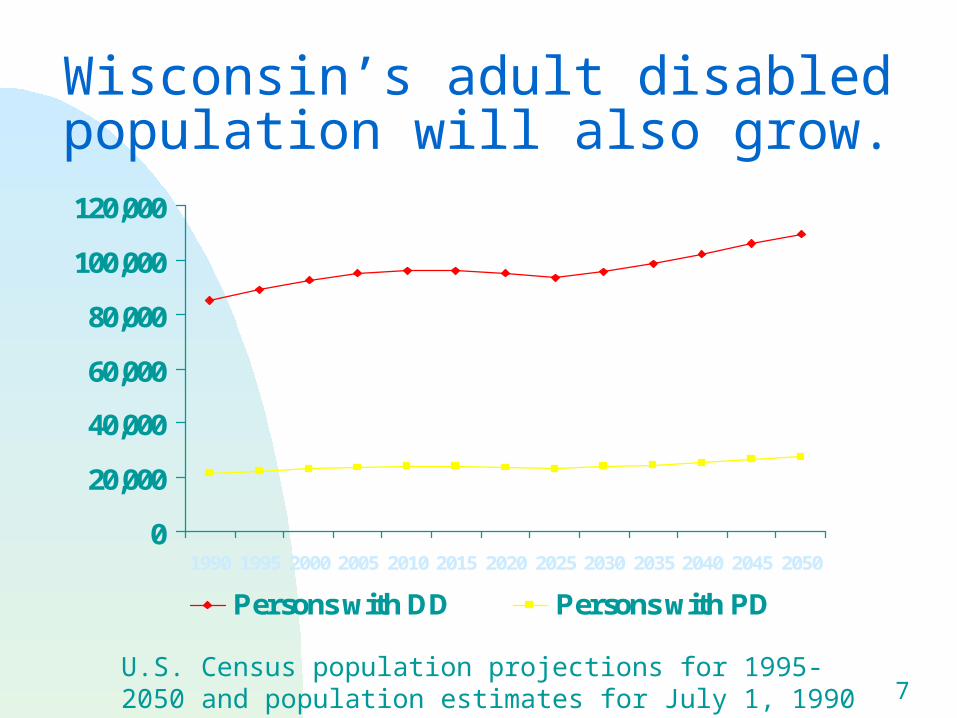
Wisconsin’s adult disabled population will also grow.
0
20,000
40,000
60,000
80,000
100,000
120,000
1990 1995 2000 2005 2010 2015 2020 2025 2030 2035 2040 2045 2050
Persons with DD Persons with PD
U.S. Census population projections for 1995-2050 and population estimates for July 1, 1990 based on 1990 Census.

8
Community Options Program (COP)
Make funding available to counties to provide community-based long-term care services
Piloted in 1981; open to all target groups
In 2001, provided services to 2,254 Wisconsin residents
9
C O P
Provides for comprehensive assessments and encourages the use of appropriate professionals
Provides for the development of Comprehensive Service Plans Aids in the relocation of people from
institutional settings Diverts people from institutional
settings

10
C O P
Encourages the maintenance of existing relationships with natural supports
Encourages the maintenance of and/or improvement of the Quality of Life of the people served
11
1980s - Medicaid Home and Community Based Waivers (HCBWs)
Federal Medicaid funds and state match made available to provide community-based services in place of institutional care
Similar to COP but not as flexible
Includes expanded eligibility for Medicaid
In 2001, provided services to 22,000 Wisconsin residents.

12
H C B Ws
CIP 1A - Relocation of people from State Centers for the Developmentally Disabled Required bed de-certification
CIP 1B - Relocation and Diversion of people from ICF-MRs No bed de-certification required
13
H C B Ws
CIP II - Relocates people from nursing facilities Bed de-certification required
COP-W - Diverts people from nursing home admissions No bed de-certification required
BIW - Relocates people with Traumatic Brain Injury from rehabilitation facilities
14
Goals of Family CareACCESS--Improve people’s access to services.
CHOICE--Give people better choices about the services and supports available to meet their needs.
ECONOMY--Create incentives and ability for providing and purchasing cost-effective alternatives.
QUALITY--Improve the overall quality of the long-term care system by focusing on achieving people’s health and social outcomes.
15
A Pilot Program
The Legislature directed DHFS to test a partially integrated* managed-care model for the delivery of long-term care services, which includes both community-based and institutional care, for possible expansion statewide.
Currently, nine Wisconsin counties have implemented aspects of Family Care.
16
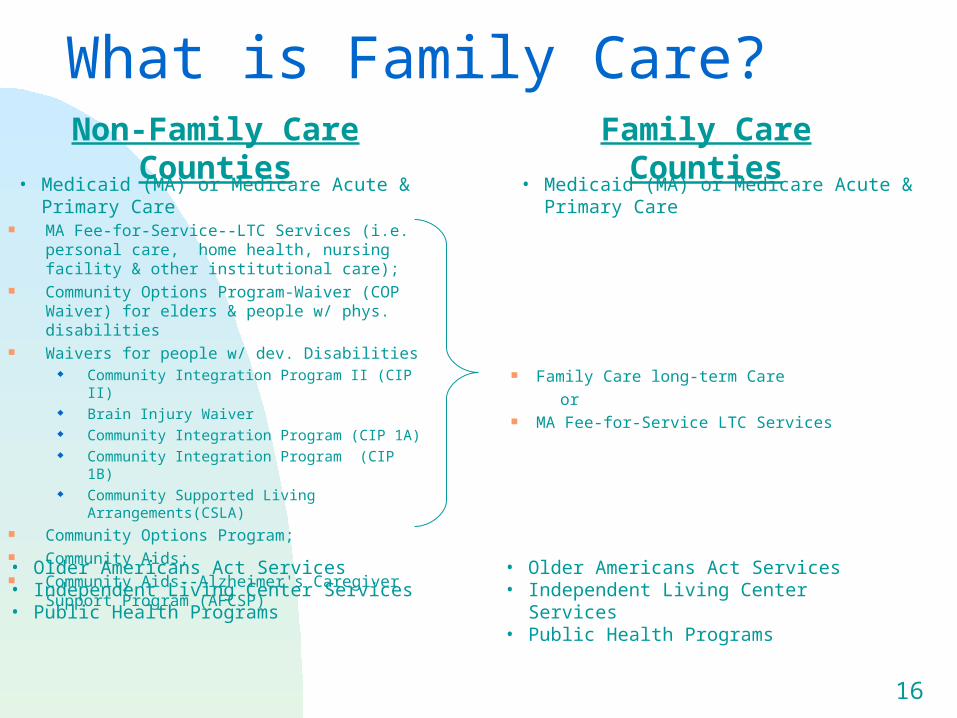
What is Family Care?
MA Fee-for-Service--LTC Services (i.e. personal care, home health, nursing facility & other institutional care);
Community Options Program-Waiver (COP Waiver) for elders & people w/ phys. disabilities
Waivers for people w/ dev. Disabilities Community Integration Program II (CIP II) Brain Injury Waiver Community Integration Program (CIP 1A) Community Integration Program (CIP 1B) Community Supported Living Arrangements(CSLA)
Community Options Program; Community Aids; Community Aids--Alzheimer's Caregiver Support Program
(AFCSP)
Family Care long-term Care
or MA Fee-for-Service LTC Services
Non-Family Care Counties Family Care Counties
• Medicaid (MA) or Medicare Acute & Primary Care • Medicaid (MA) or Medicare Acute & Primary Care
• Older Americans Act Services• Independent Living Center Services• Public Health Programs
• Older Americans Act Services• Independent Living Center Services• Public Health Programs
17
Why are we redesigning the long-term care system?
Family Care goal:
Improve consumer access and choice….

18
Old/current system Uncoordinated fee-
for-service care, with no safeguards against gaps & overlaps
Immediate entitlement to nursing home care; wait list for community care
In NH, certain services regardless of need; in waiver, a limited benefit package.
Family Care Managed care, with
focus of responsibility for quality and cost.
Immediate entitlement to long-term care suitable for individual needs
Single, expanded, flexible benefit package
19
Old/current system Waiver care
management has social work expertise.
Waiver assessment limited to need for waiver services
Acute/primary care rarely coordinated with waiver services.
LTC ‘card services’ not coordinated with waiver services.
Family Care Interdisciplinary care
management: social work and nursing.
Holistic approach to care planning
Mandatory contacts with primary health providers.
Control, responsibility for all MA-funded LTC services under one local agency.
20
Old/current system No local incentive for
intervention & prevention. Person leaves the waiver if condition deteriorates.
Service authorization limited by available funds, State approval
Family Care Intervention &
prevention in care plans; CMO on the hook if condition deteriorates.
Service authorization by local teams, asking ‘what is cost-effective?’

21
Federal Issues about Access to LTC Services Olmstead vs. L.C., U. S. Supreme Court Decision ruled
that--”unjustified isolation is properly regarded as discrimination based on disability” under ADA Title II.
Federal CMS staff have noted that Family Care provides key components that would help assure state compliance: Resource Centers offer Pre-Admission Consultation & Options
Counseling for all who enter institutional & residential services. Enrollees have access to a range of long-term care services,
including home and community based care based options--based on need. It ends the institutional bias of Medicaid.
Family Care CMOs are required to develop the services needed by their enrollees. They are monitored to assure individual outcomes are met.
22
Why are we redesigning the long-term care system?
Family Care goal:
Ensure quality for consumers….

23
Quality: Consumer Perspective
Person-centered, consumer-focused
Measuring outcomes from the perspective of the consumer
24
Family Care Outcomes Self-determination and Choice
People are treated fairly People have privacy People have personal dignity and respect People choose their services People choose their daily routine People achieve their employment objectives People are satisfied with services
25
Family Care Outcomes, cont’d
Community Integration People choose where and with
whom they live People participate in the life of
the community People remain connected to
informal support networks
26
Family Care Outcomes, cont’d
Health and Safety People are free from abuse and
neglect People have the best possible
health People are safe People experience continuity and
security

27
Why are we redesigning the long-term care system?
Family Care goal:
Provide services economically….

28
Cost-Effectiveness=Quality and Economy
CMOs Avoid Unnecessary Costs by: Coordinating benefits and services, including
primary health care Enabling member’s reliance on friends and
family Focusing on prevention of disability
29
0
250
500
750
1000
1250
1500
1750
2000
2250
Without Family Care Family Care
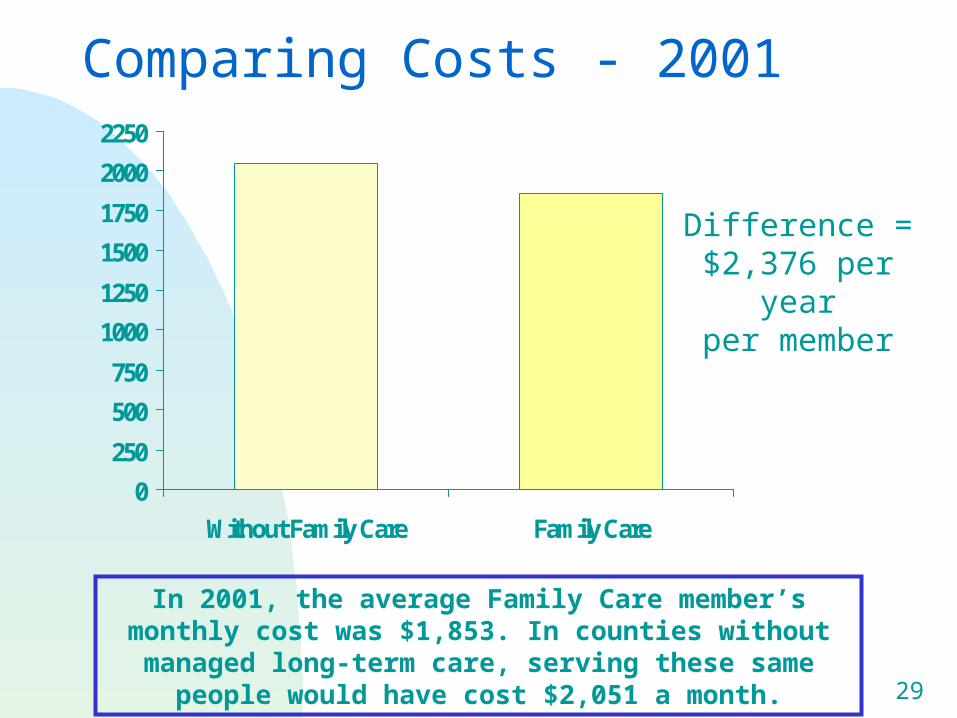
In 2001, the average Family Care member’s monthly cost was $1,853. In counties without managed long-term care, serving
these same people would have cost $2,051 a month.
Difference = $2,376 per year
per member
Comparing Costs - 2001

The Organizations of Family Care

31
32
The organizations of Family Care
The Aging and Disability Resource Centers….

33
Resource Centers: Goals
Reach a broad base of consumers, regardless of income or condition
Delay or prevent the need for LTC services Enable people to make informed, cost-effective
decisions about LTC Identify people at risk and with urgent needs and
connect them to services Serve as the single entry point for publicly-funded
long-term care

34
Resource Centers: Services Outreach and public education Information and assistance Benefits counseling & screening for eligibility Emergency response Transitional services Prevention and early intervention activities Enroll recipients in CMO, in those counties with
CMOs. Provide services over the telephone or in visits to
an individual’s home.

35
Where are the Resource Centers?
Fond du Lac Jackson Kenosha
(One for developmental disabilities; one for elderly and physical disabilities)
La Crosse Marathon Milwaukee
(elderly only)
Portage Richland Trempealeau

36
The organizations of Family Care
The Enrollment Consultants….

37
Enrollment Consultants: Purposes
Make sure potential CMO members know their options.
Address federal and state concerns Cherry-picking and hot potatoes
Conflict of interest County governments operate both RCs and
CMOs.

38
Enrollment Consultants: Services
Enrollment consultants provide unbiased information and advice about long-term care.
Communicate with potential enrollees
Explain managed care
Help with enrollment
The Southeastern Wisconsin Area Agency on Aging, under contract with the Department of Health and Family Services, provides enrollment consultation.
39
The organizations of Family Care
The Care Management Organizations….
40
Care Management Organizations:
Purpose
To support long-term care consumers in achieving their personal outcomes in a cost-effective system of long-term care.
41
Care Management Organizations:
Services Assess clients’ personal outcomes Involve consumer in decision-making
and creating member-centered plan to support outcomes
Provide services, directly or by contract
Coordinate other services not included in the Family Care benefit
Assure quality
42
The Family Care Benefit Adaptive aids, communication aids, medical supplies,
home modifications Home health, therapies, nursing services, personal care,
supportive home care Residential services, nursing facility services Transportation, daily living skills training, supportive
employment Meals: home delivered and congregate, Emergency response system services Respite Care, adult day care, day services
Case Management

43
Where are the CMOs?
Fond du Lac …...899 members
La Crosse ……1,399 members
Milwaukee……4,363 members (elderly only)
Portage…………655 members
Richland………..292 members
Membership as of September 1, 2003

44
PACE and Partnership
Integrates all Medicare, Medicaid and HCBW services
Benefits are capitated and paid to small, community-based organizations
Contractors are at full risk for all health and long-term care outcomes
Care management is team-based

45
PACE
Most services are provided in an adult day center
Primary care physician and most services providers are PACE employees
Serves frail elderly age 55 and older
Participants must be Medicaid eligible and in need of a nursing home level of care
46
Partnership
Most services are provided in the community
Primary care is provided by an independent physician panel
Serves frail elderly age 55 and older, and adults with physical disabilities
Must be Medicaid eligible and in need of a nursing home level of care

47
PACE/Partnership Enrollment
CCO/CCE (Milwaukee, Racine)
PACE 445
Partnership 324 CHP (Eau Claire,
Dunn, Chippewa) 485 CLA (Dane) 260 Eldercare (Dane) 453
August 31, 2003

48
Goals of Reform:ACCESS--Improve people’s access to services.
CHOICE--Give people better choices about the services and supports available to meet their needs.
QUALITY--Improve the overall quality of the long-term care system by focusing on achieving people’s health and social outcomes.
ECONOMY--Create incentives and ability for providing and purchasing cost-effective alternatives.
49
Council Role
Advise on: What concerns and issues need to be
addressed What should the implementation
strategy be regarding such issues as: timing? providers/partners? target populations?

50
Council Role : Today’s Question
What do we want to request in a waiver regarding our goal to: assure adequate nursing home care and
expand community capacity? improve quality in the existing waiver
programs? pursue steps toward managed care such
as pre-Family Care? diversify the nursing home industry by
regulatory change and other strategies?