within reach ending preventable child...
TRANSCRIPT
WITHIN REACH Ending preventable child deaths
A Child Health Now policy briefing

© World Vision International 2013ISBN 978-0-918261-35-9
All rights reserved. No portion of this publication may be reproduced inany form, except for brief excerpts in reviews, without prior permission of the publisher.
Published by World Vision International.
For further information about this publication or World Vision International publications, or for additional copies of this publication, please contact [email protected].
World Vision International would appreciate receiving details of any use made of this material in training, research or programme design, implementation or evaluation.
This report has been written by Rachel Coghlan drawing on research by Helene Cunat (consultant). Significant contributions were made by Kate Eardley, Marie Durling and Lisa O’Shea. We are grateful for comments and input from staff across World Vision. Additional thanks are due to a number of experts around the globe who graciously gave time for interviews.
Senior Editor: Heather Elliott. Production Management: Katie Klopman, Daniel Mason.Copyediting: Debbie Johnson. Proofreading: Audrey Dorsch.Cover Design and Interior Layout: Siefert/Irwin, Inc.Cover photo © World Vision/Justin DouglassInside photos © World Vision staffpage 3: Bangladesh / Xavier Skupage 4: Cambodia / Sopheak Kongpage 9: Mali / Justin Douglasspage 10: Myanmar / Khaing Min Htoopage 11: Bolivia / Jon Warrenpage 12: Zambia / Collins Kaumbapage 14: Ethiopia / Paul Bettingspage 15: Uganda / Simon Peter Esakupage 17: Mali / Justin Douglasspage 19: Nepal / Alina Shresthapage 23: Bangladesh / Amio Ascension
www.childhealthnow.org

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
1
present concreteopportunities to put
children,familiescommunitiesat the centre.
survivalCurrent child
initiatives
Executive summaryThe world is at a critical juncture in the effort to achieve lasting progress on child mortality. The number of children dying each year under the age of 5 has fallen from 12 million to fewer than 7 million in the past two decades – a dramatic 42 per cent reduction.1 But there is still a long way to go. A staggering 4.4 million children died in 2011 from conditions which are preventable or treatable: pneumonia, diarrhoea, malaria, birth complications and newborn infections.
Solutions are known and cost effective. The recent Lancet series on childhood pneumonia and diarrhoea shows that by 2025, key solutions for these top two killers of children under 5 could virtually eliminate child deaths from diarrhoea and reduce by almost two-thirds child deaths from pneumonia. These reductions would be possible if the solutions were scaled up to reach at least 80 per cent of the people who need them.2
The majority of children dying of preventable causes are concentrated in the poorest and most marginalised communities. This report argues that these children are not beyond reach. It highlights an often overlooked strategy that is key to keeping children healthy: engaging and empowering families and communities in taking control of their own health. Mothers, caregivers and families need to know how to prevent and treat sickness. They need to have a sense of ownership over their child’s health by being able to take responsibility for it. Families and communities act as front-line health workers for child health and survival.
The Millennium Development Goals (MDGs) and a range of other recent and upcoming initiatives for child survival present concrete opportunities to put children, families and communities at the centre of efforts to reduce child deaths amongst those once thought to be out of reach. Amongst these initiatives are the UN Secretary-General’s Every Woman Every Child initiative, A Promise Renewed, the UN Commission on Life-Saving Commodities for Women and Children, the Integrated Global Action Plan for the Prevention and Control of Pneumonia and Diarrhoea and the Global Newborn Action Plan. These initiatives should support and align with national policies. The success of these initiatives should be measured not only by the supply of medicines or by policy change at the national level, but also by families’ capacity to, amongst other things, prevent illness and get the medicines they need to treat their sick child at home.
At the community level, preventing and treating the major childhood diseases needs to include:
• care and attention provided to women and children by their own informed families and communities
• knowledge and experience of skilled front-line health workers
• availability of adequate local health facilities and community health posts, essential medicines, and emergency care when needed.
Expanding coverage of essential child health interventions to children most in need requires a strong partnership between families, communities, the health system, governments and donors (Figure 1).
and

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
2
Figure 1. The right environment for child survival
World Vision proposes the following critical community-based strategies to effectively engage and empower families and communities for improved child health outcomes:
• community health worker home visits to provide information and education to promote healthy behaviours
• community case management of childhood pneumonia, diarrhoea, malaria and neonatal infections
• mothers’ groups focused on support and education for pregnant women and new mothers
• accountability and collective community action for better health services.
World Vision recommends the following:1. National and sub-national governments should demonstrate leadership and commitment to ending preventable child deaths by:
• reviewing and revising national health policies to ensure adequate focus on children most in need
• ensuring community health workers are integrated into the health system and appropriately trained, supervised and equipped
• increasing investment for the implementation of proven community-based strategies, including community health workers, community case management and mothers’ groups
• engaging and empowering families and communities as partners in the planning, delivery and review of health services.
HealthService
Providers
Timely referral and health information, including pregnancies and births
Supervision, training and commodities
Prom
otin
g ke
y fa
mili
y
prac
tices
crit
ical
for c
hild
hea
lth
Accountable to fam
ilies
and comm
unities
Seek
ing
timel
y
care
for
child
hood
ill
ness
es
Seeking timely
care for
childhood
illnesses
CommunityHealth
Workers
Families
National Policy Environment
Donors and Global Initiatives

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
3
donors,multilateralsand civil society
choosethe right waysto target them.
within reachwho are most in needare
if governments,
The children
2. Current and upcoming initiatives, such as the UN Commission on Life-Saving Commodities for Women and Children, the Integrated Global Action Plan for the Prevention and Control of Pneumonia and Diarrhoea, the Global Newborn Action Plan, and the post-2015 development framework, should:
• respect principles of country ownership for national policies to reach children most in need
• reflect a greater focus on engaging and empowering families and communities through proven strategies, including community health workers, community case management and mothers’ groups
• enhance accountability by involving communities in the planning, monitoring and review of these initiatives
• include metrics of measurement that reflect a focus on family and community strategies and impact on children most in need.
As the 2015 deadline of the MDGs looms near and preparations for the post-2015 agenda intensify, the pressure is on. Maintaining momentum is the minimum required to reduce child mortality by two-thirds. Increasing momentum is necessary to go beyond this target and end all preventable child deaths. The children who are most in need are within reach if governments, donors, multilaterals and civil society choose the right ways to target them. These methods include rebalancing efforts to ensure that engaging and empowering families and communities is a foundation for better child health.

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
4
1. Increasing momentum to reach all childrenThe world is at a critical juncture in the effort to achieve lasting progress on child mortality. The number of children dying each year under the age of 5 has fallen from 12 million to fewer than 7 million in the past two decades – a dramatic 42 per cent reduction.3 But there is still a long way to go. A staggering 4.4 million children died in 2011 from conditions which are preventable or treatable: pneumonia, diarrhoea, malaria, birth complications and newborn infections. These conditions accounted for 64 per cent of the total number of child deaths in 2011.
Solutions are known and cost effective. The recent Lancet series on childhood pneumonia and diarrhoea shows that by 2025, key solutions for these top two killers of children under-five could virtually eliminate child deaths from diarrhoea and reduce by almost two-thirds child deaths from pneumonia. These reductions would be possible if the solutions were scaled up to reach at least 80 per cent of the people who need them.4
The majority of the children dying of preventable causes are concentrated in the poorest and most marginalised communities. This report argues that these children are not beyond reach. It highlights an often overlooked strategy that is key to keeping children healthy: engaging and empowering families and communities in taking control of their own health.
The MDGs and a range of other recent and upcoming initiatives for child survival present concrete opportunities to put children, families and communities at the centre of efforts to reduce child deaths amongst those once thought to be out of reach.
As the 2015 deadline of the MDGs looms near and preparations for the post-2015 agenda intensify, the pressure is on. Maintaining momentum is the minimum required to reduce child mortality by two-thirds.5 Increasing momentum is necessary to go beyond this target and end all preventable child deaths.
2. A critical stumbling block in reaching the MDGsThe challenge of meeting the child survival targets is increasingly found in the poorest countries and communities. Countries that are fragile or affected by conflict have seen the least progress, with no fragile state having achieved any of the MDGs. Eighteen of 26 countries with the largest decreases in under-five mortality show a widening of the gap between the richest and poorest groups.6 This is in part because the MDGs have been equity-blind: the focus on global aggregates and ‘one-size-fits-all’ global targets has allowed some states to meet their MDG targets without addressing the needs of the most vulnerable.
The burden of child mortality remains with families living in the most remote areas on the lowest incomes. In low-income countries, children born in the poorest 20 per cent of households are almost twice as likely to die before age 5 as those in the wealthiest 20 per cent of households.7 They often have the least access to health services, the poorest diets, the most crowded living conditions and the highest exposure to illness. Both pneumonia and diarrhoea are closely associated with risk factors related to poverty, such as undernutrition, poor hygiene and deprived home environments.8

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
5
informed
community members.
mothers,caregivers andcommunities,
threatsMany of
to newbornand child healthcan be prevented by
Poverty is not the only underlying factor. Children born in rural areas are at a greater risk of dying compared to children in urban areas, and the under-five mortality rate for children born to mothers with no education is almost three times higher than for children whose mothers have secondary education. The environment in which children are born and raised is a critical determinant of their health and survival.
Estimates show that many of the 6.9 million deaths in 2011 of newborns, infants and children could have been averted by increasing coverage of proven and cost-effective interventions which target the main causes of post-neonatal deaths (pneumonia, diarrhoea and malaria) and the most vulnerable babies.9 Interventions include education about breastfeeding, good nutrition, hygiene and early identification of symptoms as well as treatment of diseases with simple antibiotics or medicines.
Scaling up these interventions could have a dramatic impact on child mortality. However, failing to ensure that the poorest and most marginalised children, families and communities can benefit from such interventions is putting in jeopardy child health initiatives which aim to reach and go beyond MDG 4 to end preventable child deaths.
3. Preventing and treating the major killers of children In many high-mortality settings where inequities are greatest, health services are frequently too far away and too poor in quality to respond to the needs of families and communities, particularly in potential emergencies (for example, childbirth or severe pneumonia). In these contexts, many of the major threats to newborn and child health can be prevented by informed mothers, caregivers and communities, or treated by community members. Actions by families and communities can help to prevent disease and stop children from dying at home when they do become sick.
Community-based strategies to deliver preventive and basic treatment interventions have shown significant impact on reducing child mortality in high-mortality, resource-poor settings.10 Some community members may be trained as lay health workers – often referred to as community health workers (CHWs) – to provide such care. Research by World Vision and the Burnet Institute focusing on care delivered to families and communities in Papua New Guinea suggests that up to one-third of maternal deaths, over two-thirds of newborn deaths and half of child deaths could be prevented through near universal coverage of community-based interventions.11
At the community level, the right environment to prevent and treat the major childhood diseases needs to include:
• care and attention provided to women and children by their own informed families and communities
• knowledge and experience of skilled front-line health workers
• availability of adequate local health facilities and community health posts, essential medicines, and emergency care when needed.
This report reinforces an often overlooked strategy for extending the fight against preventable deaths to children most in need and overcoming bottlenecks: engaging and empowering communities to understand and participate in their own health.
the major
or treated by

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
6
Engaging and empowering families and communities should not be viewed as auxiliary to essential child health interventions but as primary for child survival. Mothers, caregivers and families act as front-line health workers. CHWs provide a vital link between the family and community and the primary health-care system. Communities need to know their rights and the services available, and they need to trust that health service providers will provide quality services.
Family and community empowerment is defined as ‘the process and outcome of those without power gaining information, skills and confidence and thus control over decisions about their own lives’.12
Figure 1 describes the relationships between families, communities and health services. Each of these elements is critical and interrelated, and it is important that health investments find the right balance amongst them. Expanding coverage of essential child health interventions to children most in need requires a strong partnership between families, communities, the health system, governments and donors.
Figure 1. The right environment for child survival
HealthService
Providers
Timely referral and health information, including pregnancies and births
Supervision, training and commodities
Prom
otin
g ke
y fa
mili
y
prac
tices
crit
ical
for c
hild
hea
lth
Accountable to fam
ilies
and comm
unities
Seek
ing
timel
y
care
for
child
hood
ill
ness
es
Seeking timely
care for
childhood
illnesses
CommunityHealth
Workers
Families
National Policy Environment
Donors and Global Initiatives
requires a strong partnershipbetween families, communities,
governmentsand donors.the health system,
interventionsessential
Expandingcoverage of

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
7
4. Overcoming barriers: targeting children most in needWorld Vision supports growing international momentum to target children most in need as central to accelerating efforts to end preventable child deaths.13 Children are continuing to die because of limitations on preventive and curative health services. There are, however, also gaps at the family level, including knowledge on disease prevention and management and delayed care-seeking.14
There are many reasons why families and communities will not seek health care when they need it:
• lack of education and information on the most effective ways to prevent and treat disease
• poor and uneven quality of health services
• gender norms, including lack of power for mothers to make decisions at home
• community and cultural preferences and norms
• time and distance required to reach essential health services
• cost of health care and time spent away from work.
At the moment, the path for many countries and donors in tackling child mortality is to focus on removing barriers to service provision. Actions to this end include increasing the training and deployment of professional health workers, expanding building infrastructure and ensuring the availability and supply of essential medicines and commodities. This approach tends to focus on the ‘supply’ side of health care. Some investment has been made to overcome barriers which stop families and communities from accessing and using the provided services. Improving this ‘demand’ side of health care is often accomplished through the use of mass communication and social marketing to encourage the poorest communities to seek care.15
It is important to find the right balance of investments between service delivery and quality, and the access to and use of services. On the one hand, focusing exclusively on service delivery often fails to reach the poorest communities, because wealthier populations tend to capture much of any public subsidy delivered. On the other hand, investing solely in creating demand for services when health systems are too weak to respond to the increased demand is also doomed to failure.
The focus on promoting care-seeking through mass media and social marketing approaches, whilst important, neglects the role of families and communities as active participants in their own health and the personal contact made possible by relationships with front-line health workers, volunteers and other community members. Without this balance, we will still fail to reach children most in need.
WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
8
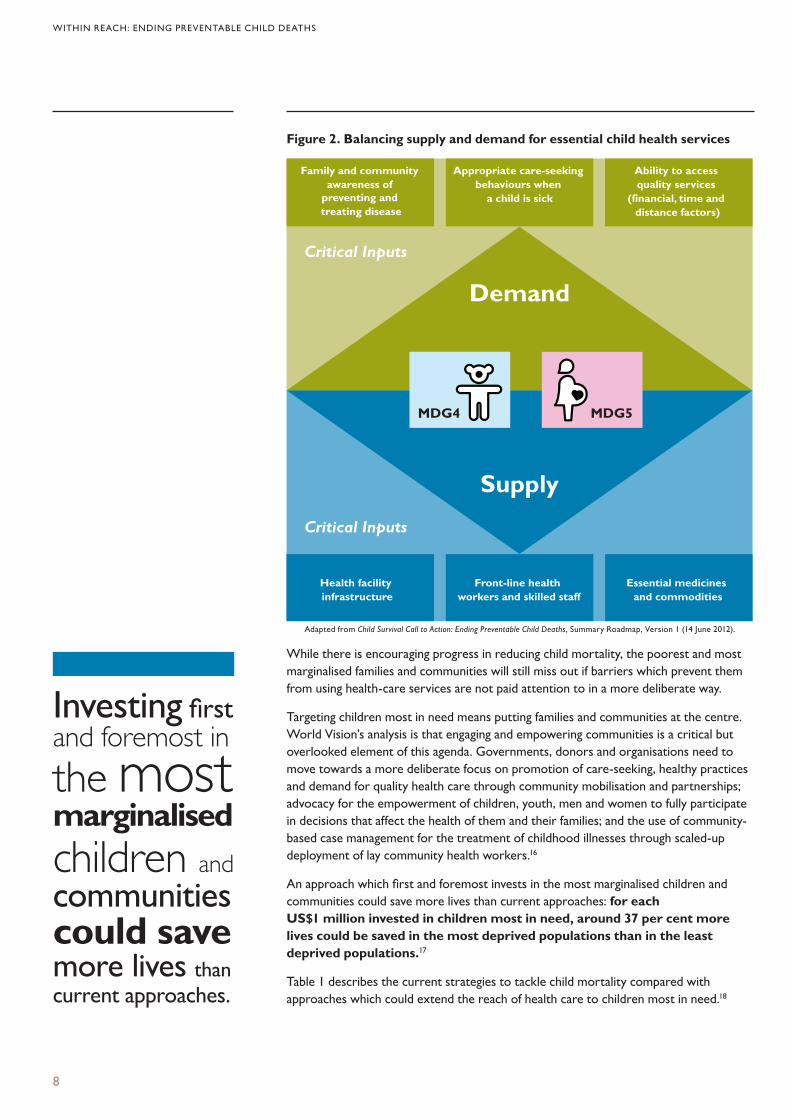
Figure 2. Balancing supply and demand for essential child health services
\
While there is encouraging progress in reducing child mortality, the poorest and most marginalised families and communities will still miss out if barriers which prevent them from using health-care services are not paid attention to in a more deliberate way.
Targeting children most in need means putting families and communities at the centre. World Vision’s analysis is that engaging and empowering communities is a critical but overlooked element of this agenda. Governments, donors and organisations need to move towards a more deliberate focus on promotion of care-seeking, healthy practices and demand for quality health care through community mobilisation and partnerships; advocacy for the empowerment of children, youth, men and women to fully participate in decisions that affect the health of them and their families; and the use of community-based case management for the treatment of childhood illnesses through scaled-up deployment of lay community health workers.16
An approach which first and foremost invests in the most marginalised children and communities could save more lives than current approaches: for each US$1 million invested in children most in need, around 37 per cent more lives could be saved in the most deprived populations than in the least deprived populations.17
Table 1 describes the current strategies to tackle child mortality compared with approaches which could extend the reach of health care to children most in need.18
Family and community awareness of
preventing and treating disease
Appropriate care-seeking behaviours when
a child is sick
Ability to access quality services
(financial, time and distance factors)
Health facility infrastructure
Front-line health workers and skilled staff
Essential medicines and commodities
Critical Inputs
Critical Inputs
Demand
Supply
MDG4 MDG5
children and
could savecommunities
current approaches.more lives than
marginalised
Investing firstand foremost in
the most
Adapted from Child Survival Call to Action: Ending Preventable Child Deaths, Summary Roadmap, Version 1 (14 June 2012).

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
9
Table 1. Child health services: comparison of approaches
Level of health service delivery Current strategies Strategies to target children
most in need
Family and community-based care
Moderate focus on maintaining services at the current level.
Strong focus on deploying community health workers to reach per cent of villages; allowing lay health workers to deliver integrated maternal, newborn and childhood community-based management of illness; and improving performance and retention of community health workers.
Scheduled services at the population level
Strong focus on universal access to services through outreach (such as child health days) and salaries, training and supplies for outreach.
Strong focus on universal access to services through campaigns and social mobilisation; targeted cash transfers and fee waivers; and enhanced supervision and monitoring of lay health workers.
Health facility services
Strong focus on increasing infrastructure, universally expanding professional health workers, training and supervising all health workers, and strengthening supply and logistics services.
Moderate focus on infrastructure investment, mostly through maintaining or upgrading facilities, and upgrading one hospital per district for complicated emergency obstetric care.Strong focus on universal access to skilled birth attendants and full maternity services at primary levels, including waiting homes.
Reducing direct and indirect financial costs
Strong focus on elimination of user fees for all. Weak focus on conditional cash transfers.
Strong focus on targeted elimination of user fees for the poorest families and communities and targeted conditional cash transfers.
Information, communication and education approaches
Strong focus on mass media and social marketing to increase awareness and demand for services and healthy behaviours.
Strong focus on engaging and empowering families and communities and promoting demand for essential health services in partnership with community members.

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
10
5. Power in their hands: communities key to saving livesThere are a number of proven community-based strategies which can address many of the barriers that keep families and communities from accessing and using health services. World Vision proposes the following critical community-based strategies to effectively engage and empower families and communities for improved child health outcomes:
• community health worker home visits to provide information and education to promote healthy behaviours
• community-based case management of childhood pneumonia, malaria, diarrhoea and neonatal infections
• women’s groups focused on education and support for pregnant women and new mothers
• accountability and collective community action for better health services.
Table 2 summarises the barriers discussed in Section 4 and the community-based strategies which can help prevent them.19
Table 2. Key community-based interventions to address barriers to health care-seeking
Type of demand-side barrier Description Community-based
intervention
Lack of information and education on the most effective ways to prevent and treat disease
Families in high-mortality, resource-poor settings often lack knowledge to: • practise healthy behaviours at home to
prevent disease• identify early signs of childhood illness • understand the importance of timely
care-seeking• know available service providers from
whom to seek care.
CHW home visitsWomen’s groups Community case management of childhood illness
Poor and inconsistent quality of health services
Families may be reluctant to seek care if they have to face poor-quality health services, such as:• long wait times at the health clinic or
hospital • staff absenteeism or shortage of skilled
and professional staff• unfriendly or discriminatory staff
attitudes towards patients • misdiagnosis and inappropriate
prescription of medicines • lack of commodities and essential
medicines at the clinic or hospital.
Demand, take collective action and advocate at the local level for better services Supply-led subsidiesStaff training and other capacity building approaches (mentoring)Improved health staff supervisionAddress human resource shortages

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
11
Type of demand-side barrier Description Community-based
intervention
Gender norms, including lack of power for mothers to make decisions at home
In some contexts and cultures, women may have limited power in the decision-making process to seek health care for themselves and their children. Examples include: • cultural unacceptability to travel outside
her village alone or leave home for a long period
• lack of authority to see a doctor when she is sick
• reduced access to household resources to pay for health centre fees, medicines or transport when she or her child is sick
• men or senior household members (e.g. mother-in-law) make the final decision to take a child to the health facility or not
• heavy burden of multiple responsibilities, including childcare, domestic tasks and other paid work, negatively affects care-seeking for child illnesses
• perception that receiving assistance with childbirth shows weakness.
Women’s groupsMen’s groupsGrandmothers’ groups
Community and cultural preferences and norms
Social and cultural norms which can delay or prevent appropriate care-seeking include:• belief and trust in traditional medicine
over western medicine• favouring of home care due to
prohibition of important cultural practices in health facilities
• families seek treatment through unregistered providers, such as drug sellers, that are inappropriate for their condition.
Women’s groups for education and supportMen’s groupsGrandmothers’ groups
Cost of health care and time spent away from work
In many resource-poor contexts, much of health care is financed through out-of-pocket payments, making price an important determinant of demand for care. Costs include:• health services and medicines • long, slow and costly travel to health
facilities• income lost due to the time spent
travelling and at the health centre • informal payments to the health centre
for commodities or staff.
Removal of user fees to health servicesConditional cash transfer programmesVoucher schemesCommunity insurance schemes
Table 2. (continued)

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
12
Community health worker home visits to provide information and education and to promote healthy behaviours
Community health workers (CHWs) are an effective strategy for getting health care to the poorest children where health systems are weak and workforce resources are limited. They are an influential force for promoting healthy behaviours and improving child health outcomes.20 Appropriately trained and supervised CHWs provide a critical link between families, communities and professionals in the formal health-care system.
Many countries on track to achieve MDG 4 to reduce child mortality have shown remarkable progress, largely attributed to their nationwide CHW programmes that reach the poorest children. Critical elements for successfully improving child survival are government ownership of national CHW programmes, a formal role in the health system afforded to CHWs, partnerships between the health system and communities, and adequate policy and regulatory frameworks.
Another important success factor is community awareness and support for CHWs:
The literature is unanimous . . .CHW programmes should be owned and driven by communities, and CHWs should be accountable to their communities.21
Community leaders, committees and groups, including women’s groups, play an important role in the selection of CHWs and in providing guidance, support and oversight. CHW programmes are more effective when combined with strong community engagement and participation in their design, implementation, monitoring and evaluation.22 In this way, CHWs are more likely to deliver culturally sensitive education messages and the community is more likely to listen to and accept CHWs.
CHW programmes are an important investment where the formal health system is not able to respond to the needs of the most marginalised communities. The harsh alternative is no health care at all for those living on the fringes.
Case study 1 on changing health and nutrition practices in Ethiopia describes the importance of targeted personal contact from health workers and peer mothers.
‘The literatureis unanimous
communities
to their communities.’
should be owned. . .CHW programmes
and CHWs should
and driven by
be accountable

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
13
CASE STUDY 1: ETHIOPIA CHANGING HEALTH AND NUTRITION PRACTICES THROUGH PEER MOTHER SUPPORT
Problem
Ethiopia has the second highest rate of malnutrition in sub-Saharan Africa. At least 53 per cent of the country’s mortality is attributed to malnutrition, particularly amongst women and children.23 Approximately 47 per cent of all children under 5 are stunted.24
The Timed and Targeted Counselling approach
World Vision has been implementing the Timed and Targeted Counselling (ttC) project, funded by the Bill and Melinda Gates Foundation and implemented by a consortium of agencies25 in three countries.26 The project aims to reduce child deaths, illness and malnutrition caused by sub-optimal feeding practices by increasing demand for, and uptake of, good infant and young child feeding (IYCF) practices. World Vision project staff train Ministry of Health officials and health extension workers (HEWs) in ttC methodology. They in turn train, deploy and supervise mothers selected as peer educators from targeted communities. The female peer educators provide household-level counselling to mothers in their community on key IYCF practices, hygiene and care practices for newborns and children, and encouragement to seek preventive and curative health care. Messages are appropriately timed for when the behaviour is needed during pregnancy and after birth, and appropriately targeted to those who would practise these behaviours or influence the decision to adopt them. The ttC approach covers 10 visits per mother starting in the third trimester of pregnancy and continuing until 18 months after birth.
Outcomes
An evaluation survey of eight hundred women, completed two years after the ttC project started, showed that women’s knowledge and uptake of key IYCF practices had significantly improved in the areas where mothers received peer educator visits compared to a control area:27
• Increased uptake of services: 20.9 per cent of women reported they had received four or more antenatal care visits during their previous pregnancy in the intervention area compared with 14.7 per cent in the control area.
• Improved knowledge: 89.1 per cent of women who received four or more visits knew the importance of colostrum feeding, compared with 84.9 per cent of women who received one to three visits, and 74 per cent amongst women who did not receive any visits.
• Improved care-seeking behaviours: (particularly for immunisations and vitamin A supplements) 44 per cent of children aged 6 to 23 months in the intervention area received vitamin A during the previous six months, compared to 28 per cent in the control area.

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
14
• Health and nutrition outcomes: There was a significant reduction in undernutrition amongst children between 6 and 23 months in the intervention area. Wasting prevalence reduced from 9.7 per cent to 4 per cent between 2010 and 2012, and the number of underweight children reduced from 15.6 per cent to 10.7 per cent in the same period.
Key success factors and lessons learnt from the ttC project
Community acceptance of the female peer educators and the advice they provided was high, as the peer educators came from the same village and understood and shared the community’s experiences and concerns. The counselling and dialogue-based approach used by peer educators helped to address traditional and sociocultural barriers that may impede improved health practices.
The government-run Health Extension Programme (HEP) has played a key role in the success of the ttC project. HEWs trained and supervised peers educators and created a link between families, communities and formal health services. HEWs are members of their local government cabinets and participate in health management committees, where they are accountable to communities and the government for improved maternal and child health and nutrition. The HEP has educated and deployed 34,000 salaried female HEWs since 2004, extending primary health-care services to rural communities.28
National leadership and supportive policy environment
Strong political commitment and a conducive national policy environment have helped bring significant health improvements to women and children. The Government of Ethiopia has provided dynamic leadership, including doubling the budget for health over the past five years and developing an ambitious national health plan.29 The Federal Ministry of Health (FMOH) has been focusing on cost-effective preventive and basic curative health services, with a high priority on both women and children, and on disadvantaged rural and pastoralist populations. Ethiopia has seen marked falls in child mortality, from 198 per one thousand births in 1990 to 77 in 2011.30
The Health Sector Development Plan IV (HSDP IV 2010–2015) translates Ethiopia’s national health policy into concrete action.31 One of the key objectives of the HSDP IV is to ‘increase communities’ empowerment and ownership to take responsibility for improving their own health’. Commitment to this approach comes from the highest level. In the recent Global Campaign for the Health Millennium Development Goals report, Ethiopian Prime Minister Hailemariam Desalegn wrote: ‘Ethiopia’s health policy focuses on disease prevention and health promotion. For this purpose, ensuring community ownership is paramount’.32
full participation

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
15
Critical success factors at the national level include:
• Adoption of a multi-pronged national strategy addressing ‘supply’ (provision and training of HEWs and supervision staff, and setting up and equipping health posts) and ‘demand’ interventions (strengthening community empowerment and ownership) that engage all governance levels – national, regional, district and village levels.
• Effective inter-sectoral collaboration at all administrative levels, including the FMOH and the Ministry of Education for the training of HEWs, and the Ministry of Work and Urban Development for the construction and rehabilitation of health posts.
• Integration of HEWs in the government health system, making them part of the salaried government staff.
• Strengthening of sub-national-level decision-making and accountability mechanisms.
• Significant increase in national-level expenditure allocated to the HEP with the commitment of regional and district governments in covering some of the costs of the programme (HEW salaries and construction of health posts).
• Significant rise in national health expenditure over the last two decades. Between 1989 and 2010, health expenditures rose from 2.8 per cent to 13 per cent of total government expenditure.33
Community-based case management of childhood pneumonia, malaria, diarrhoea and neonatal infections
Community-based management of childhood pneumonia, malaria, diarrhoea and neonatal infections requires a community-based worker who has training to diagnose these conditions and medicines to treat them, and who knows when to refer a child to a health facility. Community-based case management has the potential to achieve significant reductions in child mortality from preventable causes amongst children most in need. For example, achieving 90 per cent breastfeeding promotion, scaling up treatment for diarrhoea and providing case management of pneumonia through CHWs could avert 64 per cent of diarrhoeal deaths and 74 per cent of pneumonia deaths amongst the poorest children in Pakistan, Bangladesh and Ethiopia.34
CHWs can help mothers and caregivers understand when and how they can safely treat children at home. Bangladesh provides a good illustration. The country has seen huge reductions in child deaths from diarrhoea due to substantial demand for and use of oral rehydration solution (ORS) to treat diarrhoea at home. Overall, 81 per cent of children with acute diarrhoea receive ORS, including 76 per cent in rural areas.35 This remedy has placed the power to treat children in the hands of their mothers.
Women’s groups focused on education and support of pregnant women and new mothers
The mobilisation and empowerment of families and communities through women’s groups has been an important vehicle to address maternal and child health over the past 20 years. A review of seven trials published in The Lancet in May 2013, together with programme monitoring and evaluation of participatory women’s groups, shows positive outcomes for maternal, newborn and child health, especially in poor rural populations with limited access to health services. In four trials where at least 30 per cent of

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
16
pregnant women participated in groups, there was a 55 per cent reduction in maternal mortality and a 33 per cent reduction in neonatal mortality.36 Grandmothers’ groups and men’s groups are also valuable peer education platforms.
The importance of engaging communities through women’s groups has prompted the development of a global report on community mobilisation through this platform, due to be released in late 2013.
TWO APPROACHES TO ENGAGING COMMUNITIES THROUGH WOMEN’S GROUPS
Women’s groups using the Participatory and Learning Action model
The Participatory and Learning Action (PLA) model involves groups of women meeting with a paid educator to discuss health issues in their own community, build understanding of the causes of sickness, develop practical solutions and provide a trusting environment for information sharing.37 The model has been successful in improving health outcomes for mothers and newborns in remote areas. In an area of Nepal where setting up and sustaining CHW home visits was a challenge, women’s groups using a PLA approach were able to reduce newborn mortality by 30 per cent.38 In Ethiopia, mobilising women’s groups to identify and treat malaria at home led to a 40 per cent reduction in newborn mortality.39 In Bolivia, mobilising women’s groups through a PLA cycle showed a 62 per cent reduction in perinatal mortality. The project has since been expanded nationally.40
Women’s groups using the Care group model
The Care group model is a peer-to-peer education approach involving groups of volunteer health educators, supervised by CHWs, who learn a new health education message and share that message with mothers in surrounding households. They meet one-on-one or in groups. In rural Mozambique, 2,300 volunteers contributed to a 66 per cent decline in infant mortality and 62 per cent reduction in under-five mortality over three years.41 During this time, seeking treatment for pneumonia in children under 5 years with rapid breathing increased from 2 per cent to 60 per cent. Care groups have helped transform the attitudes of clinical workers and the quality of services, as proactive and informed families seek assistance from them.42
Accountability and collective community action for better health services
Families and communities should feel empowered to raise their voices about their right to quality health care and to hold health service providers and governments to account for their ability to provide such services. Social accountability, an approach which seeks to create community demand and accountability for improved health services, is emerging as a priority in resource-poor, high-mortality settings.43
There are clear examples where the social accountability approach has led to improve-ments in maternal, newborn and child health and well-being. Experiences show that:44
• Strengthening relationships between communities and health service providers and governments is an important element of social accountability. Relationships need not be adversarial. All sets of community members can find ways to act
element of social
Strengthening
communities,
governmentsis an important
health service
between
accountability.
relationships
providers and

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
17
collectively to solve critical child health challenges.
• When communities have access to information and are aware of their entitlements, they become active advocates for the provision of essential services.
• Social accountability encourages governments and local communities to take ownership of health services. Women and children can become active participants in the services that are so essential to their health and well-being.
A randomised control trial of community-based monitoring in Uganda showed that social accountability is an effective approach that can be used for significant and measurable improvements in the delivery of essential health services.45 The study aimed to find a mechanism of accountability which enabled poor people to scrutinize whether or not those in authority had fulfilled their health responsibilities. Community-based monitoring of public primary health-care providers resulted in improved quantity and quality of care, including a 20 per cent increase in utilisation of outpatient services and a 33 per cent reduction in under-five mortality. Treatment practices, including immunisation of children, wait times and staff absenteeism, improved significantly. These health outcomes have been sustained, even though communities received minimal support beyond the initial intervention.46
CASE STUDY 2: UGANDA CITIZEN VOICE AND ACTION: COMMUNITY DEMAND FOR BETTER HEALTH SERVICES
The Citizen Voice and Action modelCitizen Voice and Action (CVA) is an approach that transforms the dialogue between communities and government in order to improve services like health and education that impact the daily lives of children and their families.47 Using a simple set of tools, citizens (including children) monitor health facilities in their communities and measure the reality against government commitments. The approach combines several elements of social accountability into one package:
• Communities are provided with information on their entitlements for health, education or other public services and the standards to which their governments have committed.
• Communities are introduced to a scorecard that allows them to compare the reality of services against national standards. Communities generate their own performance measures for monitoring improvements.
• All stakeholders are invited to participate in an interface meeting. CVA acts as a ‘quality audit system’ and helps the community, health service staff, politicians and bureaucrats respond to critical issues which prevent women and children from using essential services.
• CVA encourages collective action. When politicians support their local communities and health staff, the united pressure can have an effect on the decisions of sub-national governments.
• Once communities see the success they can have through local advocacy, they will usually begin the monitoring process again and focus on increasingly complex and challenging issues.
WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
18
World Vision has found CVA to be transformative in the areas in which it operates. In 2005, World Vision began piloting CVA in Uganda. The tool has since been implemented in 29 countries across the world.
Outcomes of CVA in Uganda
CVA has significantly improved the relationship between health staff and communities, reduced staff absenteeism, and increased staff numbers at the clinics. These have, in turn, contributed to increased utilisation of services, particularly by pregnant women who attend antenatal care and birth delivery, and mothers who bring their children for immunisation. In some clinics, the number of women attending antenatal services and giving birth in facilities has more than doubled.
Critical success factors
• Collective action of lobbying, mobilising, assessing and decision-making that is stimulated by CVA.
• Increased capacity and confidence of local politicians to effectively lobby for resources on behalf of their constituents. Local political representatives in very different contexts are sharing similar stories on what they have learnt about local-level governance through CVA and how they have grown to become leaders. The strengthened relationship between communities and local political representatives on health service priorities has led to more effective lobbying and improved service quality.
• Strengthened planning skills of district technical staff. This has improved the relationship of technical staff with local politicians and communities.
CVA – a potential vehicle to drive higher level policy change
Although the power of CVA lies primarily at the local level, increasingly communities are using CVA to identify patterns of government failure across entire regions and countries. These patterns tend to indicate systemic failures by governments that are ripe for policy change. During the 2013 national health budget decision-making process in Uganda, testimonies and field evidence raised from CVA processes supported an advocacy agenda on community-level maternal, newborn and child health issues targeting Members of Parliament (MPs). A village health team member and member of a local CVA working group presented a moving testimony during a high-level policy dialogue with MPs to advocate for additional community-level health budget allocation. The testimony prompted MPs to block the budget-approval process until additional resources were allocated to the health sector. At the same time, communities from four districts where CVA is operating raised their voices through a text-message campaign targeting their MPs. This added pressure to the national advocacy campaign, resulting in the approval of a US$20 million increase for the health sector in Uganda.
Communities
across entire
patterns of
regionsand countries.
are usingCitizen Voiceand Actionto identify
government failure

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
19
6. Context mattersThe requirements to best support community empowerment for maternal, newborn and child health vary, and the national context of politics and policy is important. Case study 3 describes the importance of high-level leadership and national policies to support community-based health efforts in Nepal. Nepal is on track to meet MDGs 4 and 5, and it has been a global leader in the implementation of community-based programming for child health. The case study reviews the critical success factors for improving child survival in this country.
CASE STUDY 3: NEPAL TRANSLATING GOVERNMENT COMMITMENTS TO ACTION
Maternal, newborn and child health in Nepal
Between 1990 and 2011, the under-five mortality rate in Nepal fell from 141 to 48 per 1,000 live births, a rate of decline of 64 per cent.48 The maternal mortality ratio plummeted between 1990 and 2010 from 770 to 170 per 100,000 live births.49 No other low-income country in the world with a child mortality rate greater than one hundred in 1990 has made more rapid progress in reducing its child mortality. The Government of Nepal and its partners recognise that sustaining progress on child health will require greater effort to tackle neonatal mortality. Evidence from operational research and field trials in Nepal indicates that a substantial proportion of mortality decline can be attributed to child survival programmes.50
National health policies and programmes supporting families and communities most in need
The Government of Nepal has been resolutely committed to tackling maternal and child mortality. The national Female Community Health Volunteer (FCHV) programme was introduced in 1988 under the leadership of a female health minister with strong commitment to women’s empowerment and political participation. The FCHV initiative allowed adult women into the health system and established ‘local expert’ links with households and communities. The programme aimed to promote the active involvement of women in maternal and child health and family planning services to reduce mortality and fertility. The FCHV provided personal and more frequent contact between community members and the health system.
FCHV roles were later expanded to include service-provision tasks, namely distribution of vitamin A and the treatment of childhood pneumonia through community case management. Today, 48,549 FCHVs assist with primary health-care services and act as a bridge between the community and health services.51 The intervention has been estimated to save 6,000 lives per year in Nepal and is expected to save 10,200 lives per year when national scale-up is complete.52

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
20
The Nepal Family Health Programme (NFHP) included a specific focus on improving the relationship between health facility staff and communities. This was accomplished through meaningful participation in meetings of women and marginalised groups and by coaching women to help them understand their roles.53 The Nepal Family Health Programme II (NFHP II) supports mothers’ groups as a platform for FCHVs. In some districts, FCHVs participate in Health Facility Operations and Management committees, which improves the functioning of the committee, serves to empower FCHVs, further strengthens their ties to the community and increases representation of marginalised groups.54
Critical success factors
• Strong leadership at the ministerial level.
• A government-led family health programme with a specific focus on strengthening the relationship between communities, lay health workers and health facilities.
• Carefully monitored, phased introduction of community interventions. Nepal has focused on documenting programme effectiveness from pilot studies to influence high-level decision makers to shape national policies and support scalable programmes.
• Formal policies or guidelines have in some cases followed early implementation, allowing for rapid scale-up.
• Non-monetary incentives for FCHVs. FCHVs receive the standard government allowance for time spent in training and meetings and no more compensation other than in-kind community support. Nonfinancial incentives, such as increased social status and recognition by their community, remain the most important motivators. FCHVs were initially compensated for their work, which created a challenging dynamic with their communities. In response, the National Vitamin A Programme developed a system to generate endowment funds for FCHVs managed by the Village Health Committee.55
• Programme success made ‘visible’ to communities and providers contributed to more rapid results. Communities quickly recognised that FCHVs provided timely treatment of pneumonia, which rapidly increased the proportion of expected cases receiving treatment.
• Increased levels of funding were devoted to health services, and more of that funding was given to primary health care than it was in peer countries.
• Effective donor coordination. The Nepal Health Development Partnership has made a commitment to advance citizens’ rights through participation: ‘Citizen participation, both as health system users and as active monitors to ensure systems strengthening, is crucial to meeting the MDGs. . . .Civil society and particularly community-based health organisations have an important role to play in the design and implementation and review of national health plans’.56

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
21
7. Time for change: the opportunitiesThe MDGs and other recent and upcoming commitments to child survival, such as the UN Secretary-General’s Every Woman Every Child initiative, A Promise Renewed, the UN Commission on Life-Saving Commodities for Women and Children, the Integrated Global Action Plan for the Prevention and Control of Pneumonia and Diarrhoea and the Global Newborn Action Plan present the opportunity to put children, families and communities at the centre of efforts to reduce child deaths amongst those once thought out of reach.
Throughout such initiatives, communities are often positioned as passive recipients of services or as the target of mass marketing campaigns. There is much less emphasis on engaging communities as active participants in their own health care. However, there is an opportunity to include strategies which strengthen partnerships between families, communities and front-line health workers through personal contact (such as mothers’ groups) or by targeting the collective needs and expectations of communities, where the community provides the resources.57
This section provides a review of some of the most relevant global child survival initiatives and offers suggestions for how these initiatives could better put families and communities at the centre as a means of reaching more children most in need. Putting families at the centre must be reflected in coordinated country plans.
Commitments to the Every Woman Every Child initiative and A Promise Renewed
In commitments made to advance the UN Secretary-General’s Every Woman Every Child initiative,58 there is increasing recognition of the importance of ‘demand’ for high-quality services, but the ‘supply’ side of service delivery has received more attention from stakeholders.59 However, some commitments do highlight increasing demand and directly address strengthening community systems. Their approaches range from large-scale communication and marketing to mobilising local women’s networks for political participation. World Vision has committed to a primary focus on empowering communities to raise their voices about their right to quality health care and to hold their governments accountable for delivery. The Government of Côte d’Ivoire refers to ‘community involvement in health management’ in its commitment. The Government of Zambia commits to scaling up ‘implementation of integrated community case-management of common diseases for women and children, and to bring health services closer to families and communities to ensure prompt care and treatment’.60 Yet, there remains significant room to strengthen accountability mechanisms at national and local levels by ensuring the meaningful participation of all key stakeholders and, in particular, communities.61
must bePutting families
reflectedcountry plans.
at the centre
in coordinated

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
22
The Child Survival Call to Action convened in June 2012 saw a revitalised commitment to ending child deaths under the banner of A Promise Renewed.62 It sees empowerment as a shift that would accelerate progress on ending preventable child deaths globally and within countries, and recognises that scaling up and sustaining high impact interventions depends on strengthening both supply and demand. In this regard, demand encompasses accelerating behaviour change through community action groups and decreasing financial and geographic barriers. A Promise Renewed focuses on priorities which strongly support family and community engagement:
• evidence-based country plans, including support for the families and communities whose decisions profoundly influence prospects for maternal and child survival
• transparency and mutual accountability across global, national and local levels
• global communication and social mobilisation, including encouragement of private citizens, especially women and young people, to participate in the search for innovative approaches to health.
United Nations Commission on Life-Saving Commodities for Women and Children
The UN Commission on Life-Saving Commodities for Women and Children (UN CoLSC) aims to increase access to 10 overlooked life-saving medicines and health supplies in 50 of the world’s poorest countries.63 The UN CoLSC’s report identifies a key barrier resulting in limited demand: a lack of access to and awareness of how, why and when to use these commodities.64 Ten recommendations aim to deliver on the promise of saving the lives of women and children. Recommendation 7 aims to increase demand and utilisation of health services and products, particularly amongst under-served populations by:
• reviewing and collating evidence of supply and commodity-related communications, including Social and Behavioural Change Communication (SBCC) and commercialisation, social networking, franchising and marketing
• establishing innovative public-private partnerships to address SBCC needs and develop materials and messages to enhance demand
• supporting government agencies in Every Woman Every Child countries to establish a road map and build capacity to develop, monitor and sustain SBCC and mass-media activities.
‘Demand creation’ strategies as identified by UN CoLSC centre on information, education and social marketing for uptake of essential commodities, for example, through partnerships with media and entertainment industries to support the inclusion of health messaging in commercial productions, or partnerships with businesses for workplace-based health care.
If these commodities are going to reach the poorest and most underserved communities, it will be critical that country-level plans recognise communities as active stakeholders. The working group established to develop toolkits and a roadmap for demand creation to support national-level implementation should include strategies that reflect the importance of family and community engagement and empowerment.
Integrated Global Action Plan for the Prevention and Control of Pneumonia and Diarrhoea
The recent Lancet series on childhood diarrhoea and pneumonia identifies low uptake and poor quality of services as being amongst the top five barriers for reducing deaths from these conditions. It recommends social marketing to promote desired behaviours and CHWs as ‘health messengers’ to promote the use of life-saving commodities, such as ORS, zinc and antibiotics.
communities
has committedto empowering
their voicesabout their right to
World Vision
to raise
qualityhealth care.

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
23
The Integrated Global Action Plan for the Prevention and Control of Pneumonia and Diarrhoea (GAPPD) highlights the need to generate demand and ensure supply-side interventions in order to reach all children at risk of death from pneumonia and diarrhoea.65 Like those of the UN CoLSC, the GAPPD ‘demand creation’ interventions occur mainly through information, education and communication strategies in which communities are perceived as recipients of education and as users of health services rather than active stakeholders.
Recommendations for country action in the GAPPD refer to community engagement to strengthen family and community knowledge on essential preventive practices and basic treatments for diarrhoea and pneumonia. However, the GAPPD-recommended strategies to generate demand do not include support for communities to become actively engaged in decisions that affect their health and to use their own capacities to address health needs.
The development or revision of country plans to tackle childhood pneumonia and diarrhoea provides opportunity to focus on strategies to increase utilisation of preventive and curative interventions for these diseases through family and community engagement and empowerment. Countries should include community representatives and people with extensive experience in working with communities so that interventions are culturally sensitive and build on community structures.
Global Newborn Action Plan
A Global Newborn Action Plan is due for release in late 2013. It recognises the need for specific attention to be focused on the neonatal period, an important but neglected part of the health continuum of care, particularly in high-mortality countries. Focus on newborn survival is essential for the attainment of MDG 4 and for addressing preventable child deaths beyond 2015.
Highly cost-effective interventions at the family and community level can play a major role in reducing newborn deaths, especially those due to low birthweight or premature delivery and neonatal infections. Much of this can be achieved through better maternal care in pregnancy,66 through early postnatal home visits from a lay health worker to promote healthy behaviours and treat neonatal infections, and through the support of mothers’ groups. The central role of families and communities should be considered in the forthcoming action plan and subsequent country implementation.
8. Need for actionWorld Vision welcomes the great strides already made in tackling child survival through concerted efforts by leaders, governments, organisations and civil society. But we believe there is opportunity to go further – to scale up efforts to end preventable child deaths and target children most in need. To do this, existing initiatives must expand their focus to deliberately engage and empower families and communities and put them at the centre of efforts to improve child health. The community-based strategies we have described illustrate how this can be done.

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
24
National and sub-national governments should demonstrate leadership and commitment to ending preventable child deaths by:
• reviewing and revising national health policies to ensure adequate focus on children most in need
• ensuring community health workers are integrated into the health system, and are appropriately trained, supervised and equipped
• increasing investment for the implementation of proven community-based strategies, including community health workers, community case management and mothers’ groups
• engaging and empowering families and communities as partners in the planning, delivery and review of health services.
Current and upcoming initiatives, such as the UN Commission on Life-Saving Commodities for Women and Children, the Integrated Global Action Plan for the Prevention and Control of Pneumonia and Diarrhoea, the Global Newborn Action Plan, and the post-2015 development framework, should:
• respect principles of country ownership for national policies to reach children most in need
• reflect a greater focus on engaging and empowering families and communities through proven strategies, including community health workers, community case management and mothers’ groups
• enhance accountability by involving communities in the planning, monitoring and review of these initiatives
• include metrics of measurement that reflect a focus on family and community strategies and impact on children most in need.
9. The final pushIn the final push to meet the MDGs, we cannot leave the poorest and most marginalised communities until last. The simple truth is that the MDGs and other recent and upcoming international commitments to child survival – Every Woman Every Child, A Promise Renewed, the UN Commission on Life-Saving Commodities for Women and Children, the Integrated Global Action Plan for the Prevention and Control of Pneumonia and Diarrhoea, the Global Newborn Action Plan – will only be realised through greater focus on the world’s poorest children. As all involved work towards the fulfilment of these initiatives and what comes next in the post-2015 framework, they must recommit to ending preventable child deaths. The children who are most in need are within reach if the right ways to target them are chosen. This includes rebalancing efforts to ensure that engaging and empowering families and communities is a foundation for better child health.
The children
target them
are withinreachwho are most in need
are chosen.
if the right ways to

WITHIN REACH: ENDING PREVENTABLE CHILD DEATHS
25
Endnotes 1 Interagency Group for Child Mortality Estimation (UNICEF et al.), Levels and
Trends in Child Mortality: Report 2012 (New York: UNICEF, 2012). 2 Z. Bhutta, J. Das, N. Walker, A. Rizvi, H. Campbell, I. Rudan and R. Black,
‘Childhood Pneumonia and Diarrhoea 2: Interventions to address deaths from childhood pneumonia and diarrhoea equitably: what works and at what cost?’ The Lancet (published online 12 April 2013) <http://dx.doi.org/10.1016/ S0140-6736(13)60648-0>.
3 UNICEF et al (2012). 4 Bhutta et al. 5 MDG 4 is to reduce child mortality by two-thirds. MDG 5 is to improve
maternal health. 6 UNICEF, Progress for Children: Achieving the MDGs with Equity (New York:
UNICEF, 2010). 7 Interagency Group for Child Mortality Estimation (UNICEF et al.), Levels and
Trends in Child Mortality: Report 2011 (New York: UNICEF, 2011). 8 Bhutta et al. 9 UNICEF et al (2012).10 P. Freeman, H. Perry, S. Gupta and G. Rassekh, ‘Accelerating progress in
achieving the millennium development goal for children through community-based approaches’, Global Public Health, 7 (4) (2012), 400–419; H. Perry and R. Zulliger, How Effective Are Community Health Workers? An overview of current evidence with recommendations for strengthening community health worker programs to accelerate progress in achieving the health-related millennium development goals, (Johns Hopkins Bloomberg School of Public Health, 2012); Bhutta et al.; A. Byrne and C. Morgan for Burnet Institute, COMPASS and World Vision, Improving Maternal, Newborn and Child Health in Papua New Guinea through Family and Community Care, (Melbourne: World Vision Australia, 2011).
11 Byrne and Morgan.12 M. Rosato, G. Laverack, L. Howard, P. Tripathy, N. Nair, C. Mwansambo, K.
Azad, J. Morrison, Z. Bhutta, H. Perry, S. Rifkin, A. Costello, ‘Community participation: lessons for maternal, newborn and child health’, The Lancet, 372 (2008), 962–71.
13 World Vision understands that ‘children most in need’ includes children in the bottom quintile, those from rural or minority ethnic communities, disadvantaged groups (such as disabled children) and those outside family care.
14 Byrne and Morgan.15 C. Carrera, A. Azrack, G. Begkoyian, J. Pfaffmann, E. Ribaira, T. O’Connell,
P. Doughty, K.M. Aung, L. Prieto, K. Rasanathan, A. Sharkey, M. Chopra, R. Knippenberg, Equity in Child Survival, Health and Nutrition 2: ‘The comparative cost-effectiveness of an equity-focused approach to child survival, health, and nutrition: a modelling approach’, The Lancet (published online 20 September 2012) <http://www.thelancet.com>; UNICEF, Narrowing the Gaps to Meet the Goals (New York: UNICEF, 2010).
16 Carrera et al. 17 Carrera et al. 18 Adapted from Carrera et al.19 T. Ensor and S. Cooper, ‘Overcoming barriers to health service access:
influencing the demand side’, Health Policy and Planning, 19 (2) (2004), 69–79; O. O’Donnell, ‘Access to health care in developing countries: breaking down demand-side barriers’, Cadernos de Saude Publica, Rio de Janeiro, 23 (12) (2007), 2820–2834; E. Richards, ‘Gender Influences on Child Survival, Health and Nutrition: A Narrative Review’ (UNICEF and Liverpool School of Tropical Medicine: New York, 2011); M. Chopra, A. Sharkey, N. Dalmiya, D. Anthony and D. Binkin, ‘Equity in Child Survival, Health and Nutrition 1: Strategies to improve health coverage and narrow the equity gap in child survival, health and nutrition’, The Lancet (2010; published online 20 September 2012) <http://dx.doi.org/10.1016/ S0140-6736(12)61423-8>.
20 Freeman et al.; Perry and Zulliger; Bhutta et al.; U. Lehmann and D. Sanders, Community health workers: What do we know about them? The state of the evidence on programmes, activities, costs and impact on health outcomes of using community health workers (Geneva: World Health Organization, 2007).
21 Lehmann and Sanders.22 Rosato et al; N. Nair, P. Tripathy, A. Prost, A. Costello and D. Osrin, ‘Improving
Newborn Survival in Low-Income Countries: Community-based Approaches and Lessons from South Asia’, PLoS Medicine, 7 (4) e1000246 (2010).
23 L. Caulfield, M. de Onis, M. Blössner and R. Black, ‘Undernutrition as an underlying cause of child deaths associated with diarrhoea, pneumonia, malaria and measles’, American Journal of Clinical Nutrition, 80 (2004), 195.
24 Government of the Federal Republic of Ethiopia, ‘Program implementation manual of national nutrition program July 2008–June 2013’ (Federal Ministry of Health, 1 July 2008).
25 Family Health International 360 (FHI360), the International Food Policy Research Institute (IFPRI), GMMB, Save the Children, BRAC, UC Davis and World Vision.
26 Ethiopia, Bangladesh and Vietnam.27 Baseline September 2010, Endline September 2012. World Vision, Final Report:
Outcome Evaluation of the World Vision Alive & Thrive Operations Research Project in SNNPR, Ethiopia (Addis Ababa: World Vision, 2012).
28 W. Wakabi, ‘Extension workers drive Ethiopia’s primary health care’, The Lancet, 372 (9642) (13 September 2008), 880.
29 ‘Ethiopia’, US Global Health Initiative <http://www.ghi.gov/country/ethiopia/index.htm> accessed 1 April 2013.
30 UNICEF et al (2012).31 Government of the Federal Republic of Ethiopia, Health Sector Development
Program IV In line with GTP 2010/11 – 2014/15 (2010) <http://www.phe-ethiopia.org/HEALTH%20CHAPTER%20OF%20GTP%20English.pdf>.
32 H. Desalegn, ‘Federal Democratic Republic of Ethiopia, MDGs 4 and 5: Towards eliminating preventable deaths’, The Global Campaign for the Health Millennium Development Goals – Report 2013: Accelerating progress in saving the lives of women and children (Ministry of Foreign Affairs, Norway, 2013).
33 ‘Fact sheets’, FDRE Ministry of Health <http://www.moh.gov.et/English/Information/Pages/Fact%20Sheets.aspx >; Countdown to 2015, Building a Future for Women and Children: The 2012 Report (Washington DC: World Health Organization and UNICEF, 2012).
34 Bhutta et al.35 Bhutta et al.36 The Lancet – forthcoming publication.37 M. Morrow, et al, Reducing Maternal, Newborn and Child Death in the Asia Pacific:
Strategies that Work (Melbourne: World Vision and The Nossal Institute for Global Health, 2008).
38 D. Manandhar, D. Osrin, B.P. Shrestha, N. Mesko, J. Morrison, K.M. Tumbahangphe, S. Tamang, S. Thapa, D. Shrestha, B. Thapa, J.R. Shrestha, A. Wade, J. Borghi, H. Standing, M. Manandhar, A. Costello, ‘Effect of a participatory intervention with women’s groups on birth outcomes in Nepal: cluster-randomised controlled trial’, The Lancet, 364 (2004), 970–79.
39 G. Kidane and R. Morrow, ‘Teaching mothers to provide home treatment of malaria in Tigray, Ethiopia: a randomised trial’, The Lancet, 356 (2000), 550–55.
40 K. O’Rourke, L. Howard-Grabman and G. Seoane, ‘Impact of Community Organization of Women on Perinatal Outcomes in Rural Bolivia’, Pan American Journal of Public Health, 3 (9) (1998), 9–14.
41 A. Edward, P. Ernst, C. Taylor, S. Becker, E. Mazive and H. Perry, ‘Examining the evidence of under-five mortality reduction in a community-based programme in Gaza, Mozambique’, Trans R Soc Trop Med Hyg., 101 (8) (2007), 814–22.
42 World Relief, The Care Group Difference: A Guide to Mobilizing Volunteer Community-Based Volunteer Health Educators (Baltimore: World Relief, 2004) <http://www.coregroup.org/>.
43 S. Molyneux, M. Atela, V. Angwenyi and C. Goodman, ‘Community accountability at peripheral health facilities: a review of the empirical literature and development of a conceptual framework’, Health Policy and Planning, 27 (2012), 541–554.
44 D. Booth, Development as a Collective Action Problem: Addressing the real challenges of African governance (London: Africa Power and Politics Programme, Overseas Development Institute, 2012); M. Björkman, D. de Walque and J. Svensson, Community Based Monitoring: When does it work (even in the long run)? Experimental evidence from Uganda (2012); M. Ghazala and R. Vijayendra, Localizing Development: Does participation work? (Washington DC: World Bank, 2012); World Vision, Citizen Voice and Action in Uganda: Civic demand for better health and education services (London: World Vision, 2012); The World Bank, World Development Report 2004: Making Services Work for Poor People (Washington DC: World Bank, 2004).
45 M. Björkman and J. Svensson, ‘Power to the People: Evidence from a randomized field experiment on community-based monitoring in Uganda’, Quarterly Journal of Economics (May 2009).
46 Björkman, de Walque and Svensson.47 World Vision, Citizen Voice and Action: civic demand for better services, (London:
World Vision, 2012).48 UNICEF et al (2012).49 Countdown to 2015.50 BASICS II, The MOST Project and USAID, Nepal Child Survival Case Study: Technical
report (Arlington, VA: Basic Support for Institutionalising Child Survival Project for USAID, 2004).
51 Nepal Family Health Program II, Technical Brief #1 (revised February 2012), <http://www.nfhp.org.np/> accessed 1 April 2013.
52 Perry and Zulliger.53 USAID and Nepal Family Health Program, Review of Activities Undertaken by NFHP
and Its Partners to Strengthen the Partnership between Community and Health Facilities (Sanepa, Kathmandu: Nepal Family Health Program, 2007).
54 Nepal Family Health Program II.55 BASICS II, The MOST Project and USAID.56 Nepal Health Development Partnership, International Health Partnership National
‘Compact’ between Ministry of Health and Population, Federal Democratic Republic of Nepal and External Development Partners (February 2009) <http://www.mohp.gov.np/>.
57 Rosato et al.58 ‘Commitments’, Every Woman Every Child <http://www.everywomaneverychild.org/
commitments>.59 Partnership for Maternal, Newborn and Child Health, The PMNCH Report 2011:
Analysing Commitments to Advance the Global Strategy for Women’s and Children’s Health (Geneva: World Health Organization, 2011).
60 Partnership for Maternal, Newborn and Child Health, The PMNCH Report 2012: Analysing Progress on Commitments to the Global Strategy for Women’s and Children’s Health (Geneva: World Health Organisation 2012).
61 Every Woman Every Child, Commitments to the Global Strategy for Women’s and Children’s Health: As of February 23, 2012 (2012) <http://www.everywomaneverychild.org/images/Every_Woman_Every_Child_Commitments_Cumulative_3.22.2012.pdf>.
62 UNICEF, Committing to Child Survival: A Promise Renewed, progress report 2012 (2012) <http://www.apromiserenewed.org>.
63 United Nations Foundation, ‘UN Commission on Life-Saving Commodities’, Every Woman Every Child <http://www.everywomaneverychild.org/resources/un-commission-on-life-saving-commodities>.
64 Every Woman Every Child, UN Commission on Life-Saving Commodities for Women and Children: Commissioners’ Report (September 2012).
65 WHO and UNICEF, Integrated Global Action Plan for the Prevention and Control of Pneumonia and Diarrhoea (Geneva: World Health Organization, 2013).
66 Byrne and Morgan.

WORLD VISION IS A CHRISTIAN RELIEF, DEVELOPMENT AND
ADVOCACY ORGANISATION DEDICATED TO WORKING WITH
CHILDREN, FAMILIES AND COMMUNITIES WORLD-WIDE TO
REACH THEIR FULL POTENTIAL BY TACKLING THE CAUSES OF
POVERTY AND INJUSTICE. WORLD VISION IS DEDICATED TO
WORKING WITH THE WORLD’S MOST VULNERABLE PEOPLE.
WORLD VISION SERVES ALL PEOPLE REGARDLESS OF RELIGION,
RACE, ETHNICITY OR GENDER.
World Vision International Executive OfficeWaterview House 1 Roundwood AvenueStockley ParkUxbridge, MiddlesexUB11 1FG, UK
World Vision Brussels & EURepresentation ivzw18, Square de Meeûs1st floor, Box 2B- 1050 Brussels, Belgium+32.2.230.1621
World Vision International Liaison Office7-9 Chemin de Balexert Case Postale 545 CH-1219 Châtelaine Switzerland+41.22.798.4183
World Vision International United Nations Liaison Office919, 2nd Avenue, 2nd FloorNew York, NY 10017, USA+1.212.355.1779
www.wvi.org
www.childhealthnow.org
INTERNATIONAL OFFICES