working with a disability in california world institute on disability copyright © 2006
TRANSCRIPT

working with a disability in California
World Institute on DisabilityCopyright © 2006

2
“Medicare, the Parts and the Players”
And Medicare Part D
3
Medicare Training1. Medicare Parts and Supplements
2. New Prescription Drug Benefit 2006
3. Financial Subsidy for New Drug Plan Costs
4. What’s in a Medicare Prescription Drug Plan?
5. Special Needs Plans
6. Beneficiary Protections and Appeals
7. State of California Involvement
8. Resources and References

4
Medicare >Caution Ahead<New rules and new programs …
The Gold Standard: know your customer. What is their current benefits status, their needs,
their plans? Work from this vantage point when explaining
new rules and new options. Avoid information overload, if possible. Share practical info for customer needs, wants,
plans.
5
Medicare Training
1. Medicare Parts and Supplements
6
Medicare
• Covers most age 65 or older• Some younger than 65 with disabilities,
mostly Social Security Disability Insurance (SSDI) beneficiaries
• People with end stage renal diseases (ESRD)
7
Medicare Today
The Parts
Not full coverage or comprehensive insurance by itself
New parts and supplements make for many new rules
Leave your logic and common sense at the door.

8
MedicareKey Terms, or Terms of Art• Part A, Part B, Part C, and Part D• Medicare Supplements
• Medigap Plans, or Medigap: private insurance plans• Medicare Savings Programs: government support to supplement
Medicare costs for low income beneficiaries• Medicare Advantage Plans (HMOs, were called Medicare
+ Choice), what is now Medicare Part C• Premiums, Deductibles, Coinsurance, Co-payments (co-
pays)• Dual eligible(s), or Medi-Medi(s)• Formulary
9
MedicareKey Terms or Terms of ArtCourtesy: California Legislative Analyst Office, www.lao.ca.gov
Key Insurance Terms — Definitions• Premium
• An amount paid often in monthly installments to purchase an insurance policy
• Deductible• An initial specified amount that an enrollee has to pay before the insurer
begins to contribute towards medical costs• Coinsurance
• A set percentage of medical costs that enrollees must pay towards the cost of their medical care
• Co-payment• A fixed fee that enrollees of a medical insurance plan must pay for their
use of specific medical services provided by the plan, for example, prescription drugs
10
Medicare Eligibility
For most SSDI beneficiaries:• Eligibility begins in the 25th month of SSDI
cash benefits, which is 29 months after the date Social Security determines that the disability began.

11
Medicare in 2006
• Part A: Hospital Insurance• Part B: Medical Insurance• Part C: Medicare Advantage (HMOs)
formerly Medicare + Choice,in some but not all CA
counties• Part D: Prescription Drug Benefit

12
Medicare Part A
• Pays for most inpatient hospital care• some inpatient skilled nursing home care• some home health care, and hospice care, blood
transfusions
• SSDI qualify automatically for Medicare, no monthly premium for Part A coverage
13
Medicare Part A
• Has deductibles and copayments
14
Medicare Part B
• Pays for doctors' services • Outpatient hospital care• Outpatient physical and speech therapy• Some home health care but not long term
services• Ambulance services, and some medical
equipment and supplies
15
Medicare Part B• Part B coverage is voluntary, about 95 percent of
Part A folks voluntarily stay enrolled in Part B. • Monthly premium ($88.50 in 2006) automatically
deducted from Social Security benefit check every month, higher premiums with incomes above $80,000/yr. starting in 2007
• If you don't receive Social Security benefits, you are billed for Part B.

16
Medigap Insurance
Private insurance Covers co-payments, deductibles, and some
services for Original Medicare beneficiaries only
Details at www.calmedicare.org
17
Medicare Savings Programs
Government help with Medicare deductibles, premiums, copays, or coinsurance.Apply for at CA county welfare offices.
Details at www.calmedicare.org1. Qualified Medicare Beneficiary-QMB 2. Specified Low-Income Medicare Beneficiary-SLMB 3. Qualified Individual-QI-14. Qualified Disabled Working Individual-QDWI Also see Medi-Cal on www.db101.org and in training
manual
18
MMA
The Medicare Prescription Drug, Improvement, and Modernization Act
of 2003
19
Medicare Training
1. Medicare Parts and Supplements
2. New Prescription Drug Benefit 2006

20
New Drug Benefit Overview Standard and enhanced benefits delivered through
private plans, Prescription Drug Plans, PDPs, Medicare’s new Part D, and Medicare Advantage Prescription Drug Plans, MA-PD, to be found in Medicare’s Part C
Market driven model of competing private plans in terms of benefits and costs, with a minimum choice of at least two plans for every Medicare beneficiary, one of which must be a stand-alone Prescription Drug Plan, a PDP
Each PDP negotiates with drug makers for drug prices, not Medicare or the government.
Drug Benefit Cost slides with permission the Kaiser Family Foundation, 2004

21
New Drug Benefit Overview Most dual eligibles now get most of their drug
benefits from Medicare or other insurance, not Medi-Cal drug services which use federal funds, effective January 1, 2006.
Monthly penalty for late enrollment, which is 1% of base premium for each month of delay
Important exception applies for those who already have prescription drug coverage at least as good as Medicare Part D drug plans (CMS 3/05). This is called “creditable” coverage.
Drug Benefit Cost slides with permission the Kaiser Family Foundation, 2004
22
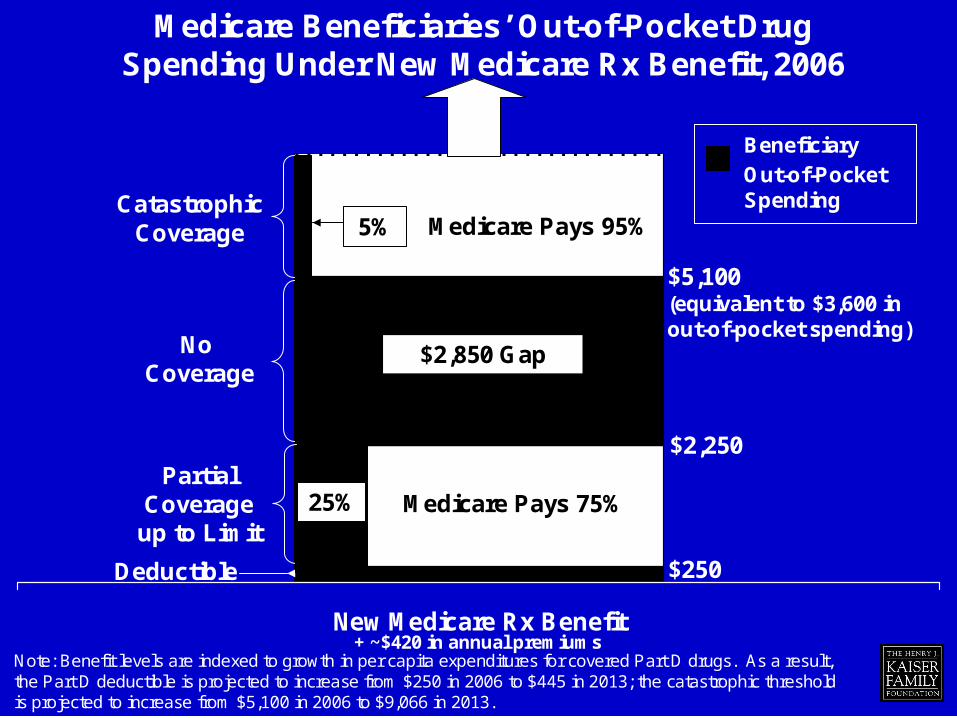
Medicare Beneficiaries’ Out-of-Pocket Drug Spending Under New Medicare Rx Benefit, 2006
+ ~$420 in annual premiumsNew Medicare Rx Benefit
Deductible $250
No Coverage
CatastrophicCoverage
PartialCoverage
up to Limit
$2,250
$5,100 (equivalent to $3,600 inout-of-pocket spending)
25%
5%
$2,850 Gap
Beneficiary Out-of-Pocket Spending
Note: Benefit levels are indexed to growth in per capita expenditures for covered Part D drugs. As a result, the Part D deductible is projected to increase from $250 in 2006 to $445 in 2013; the catastrophic threshold is projected to increase from $5,100 in 2006 to $9,066 in 2013.
Medicare Pays 75%
Medicare Pays 95%
23
2006 Prescription Drug Benefit
Important General InformationEntitled to Part A or enrolled in Part B =
eligible for a Medicare PDPEntitled to Part A and enrolled in Part B = also
eligible for a Medicare Advantage PD planVoluntary benefit, for all except duals and with
an understanding of the late enrollment rules

24
Medicare Training
1. Medicare Parts and Supplements
2. New Prescription Drug Benefit 2006
3. Financial Subsidy for New Drug Plan Costs
25
The Players
• 43 million Medicare beneficiaries nationwide
• 6.8 million are dual eligible for Medicaid and Medicare
• California Players
Statewide and Select Counties

26
CA Migration January 2006California Department of Health Services, andLegislative Analyst Office Data
Medicare
Part D
July 2004 duals: 1.1 million, at least 689,895 are age 65
and over,
273,214 under 65
Medicare Savings Program
individuals
Medicare only (They have Medicare A or B)
3.5 million over 65
500,000 under 65

27
CA Migration January 2006California Department of Health Services, andLegislative Analyst Office Data
Medicare
Part D
937,000 in
Medi-Cal fee for service
More than twice as likely to be in fair or poor health,
25% are in long-term care facilities, 40% have a cognitive impairment
137,00 in Medi-Cal managed care
28
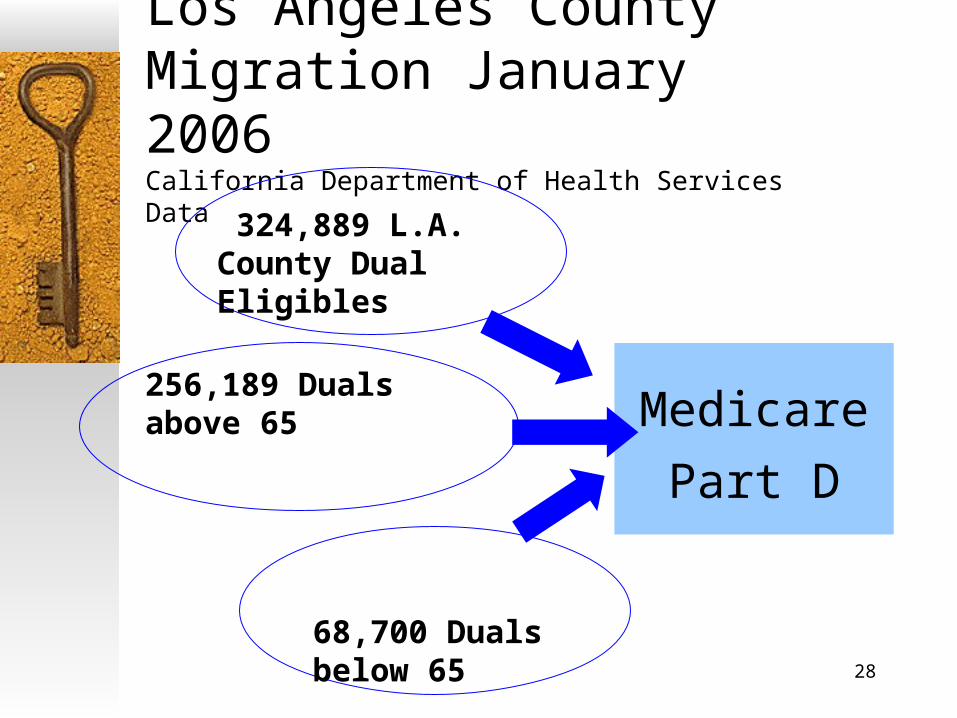
Los Angeles CountyMigration January 2006California Department of Health Services Data
Medicare
Part D
324,889 L.A. County Dual Eligibles
256,189 Duals above 65
68,700 Duals below 65
29
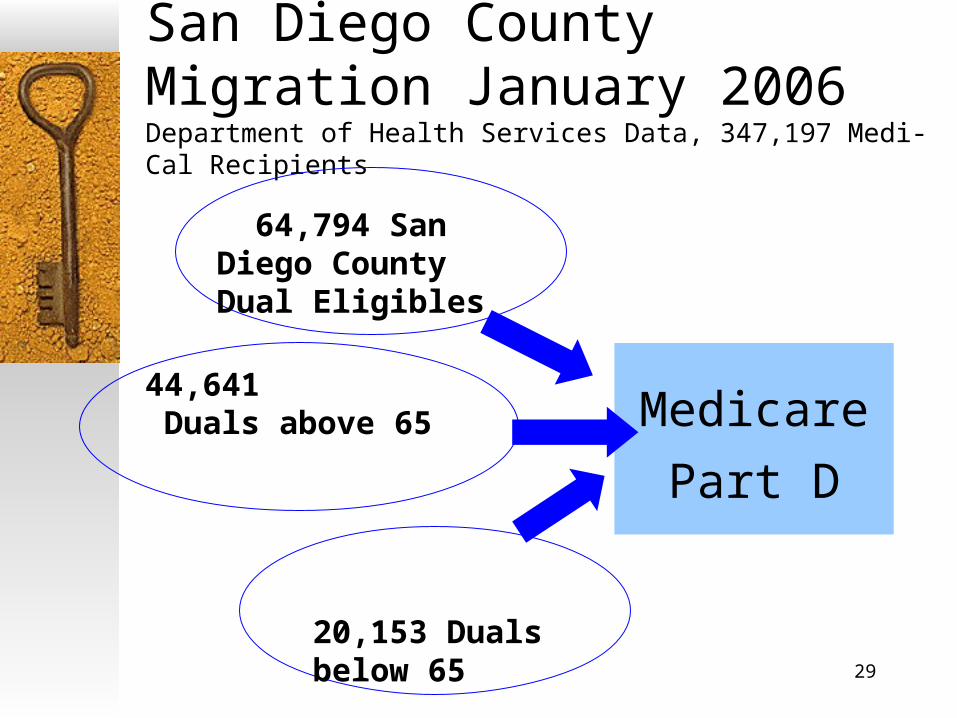
San Diego CountyMigration January 2006Department of Health Services Data, 347,197 Medi-Cal Recipients
Medicare
Part D
64,794 San Diego County Dual Eligibles
44,641 Duals above 65
20,153 Duals below 65
30
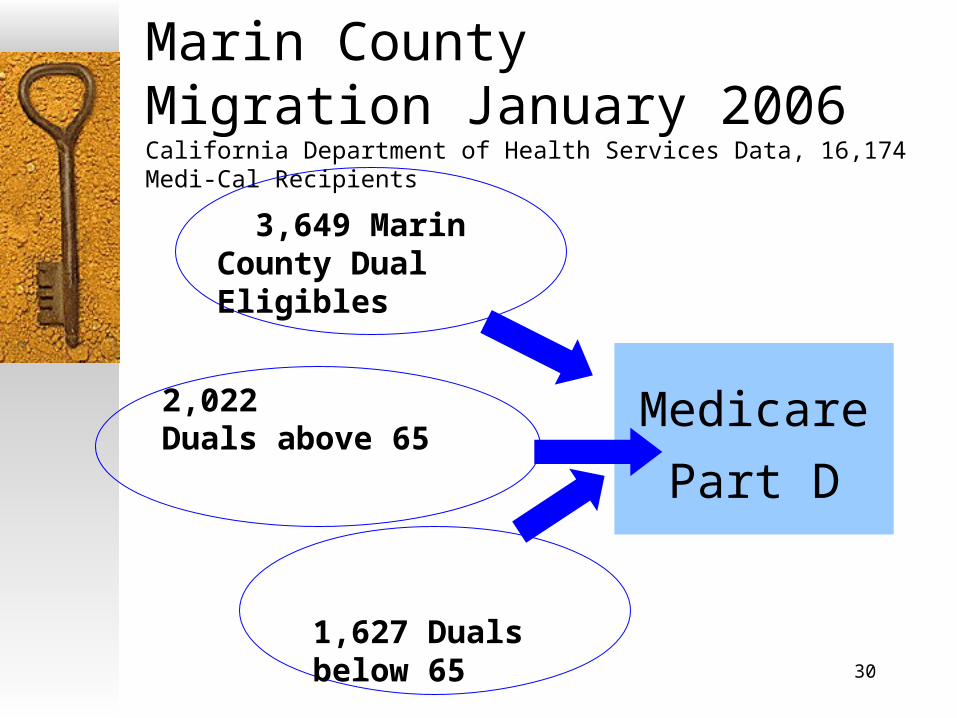
Marin CountyMigration January 2006California Department of Health Services Data, 16,174 Medi-Cal Recipients
Medicare
Part D
3,649 Marin County Dual Eligibles
2,022Duals above 65
1,627 Duals below 65

31
San Francisco CountyMigration January 2006California Department of Health Services Data, 123,293 Medi-Cal Recipients
Medicare
Part D
41,298 SF County Dual Eligibles
32,612Duals above 65
8,686 Duals below 65
32
Full Benefit Dual Eligibles
• Medicare offers better premium and cost-sharing rates for certain “subsidy eligible” individuals.
• Eligibility for a subsidy depends on an enrollee’s Medi-Cal status and income.
33
Full Benefit Dual Eligibles
Medicare enrollees eligible for Medicaid “under any eligibility category covered under the State Plan” are deemed “FULL BENEFIT DUAL ELIGIBLE” individuals (MMA/CMS regulation Section 423.772), or Section 1860D and 1935C-6, Social Security Act.
Includes 2,400 Medi-Cal Working Disabled Program enrollees.
88% today are employed dual eligibles (November 2006)
Medically Needy categories, special rules apply here.Home and community based waiver folks who are
eligible for some services in a Medicaid state plan

34
Low Income Subsidy, or LIS
For those with limited income For those with limited assets or resources Medicare Part D LIS rules are based on
SSI income and asset rules, not identical to all of them
POMS Citations, updated regularly HI 03000.000: Eligibility for Subsidized Medicare Prescription Drug Coverage

35
LIS Application in English and Spanish: How to apply: LIS Application via the Internet,
www.socialsecurity.gov Social Security Field Office application LIS phone application with Social
Security 1-800-772-1213 LIS paper application via the US Mail,
scannable, do not photo copy State Welfare or Medi-Cal Office will
take application for the LIS

36
LIS Benefit Analysis, Frank Is Frank on Medicare? YES Is Frank on Medi-Cal? NO Is Frank in a Medicare Savings Program,
an MSP? NO Does Frank have limited income? YES Does Frank have limited assets? YES Explain the LIS and assist with LIS if
Frank chooses to apply.

37
LIS Benefit Analysis, Frank Does Frank have all the information needed for the
LIS? NOConsider using and mailing the paper application, the SSA-1020 form, Social Security will contact Frank.
Does Frank have all the information needed for the LIS? YES
Consider the Internet Application Is Frank working and not on Medi-Cal? YES
Consider Medi-Cal Working Disabled Program.Explain Medi-Cal estate recovery rules if Frank is 55 and does not know about these Medi-Cal rules.

38
LIS Benefit Analysis, Frank Is Frank on Medi-Cal using the Medically Needy
category, with a Share of Cost (SOC)? YESExplain the special LIS rules for this situation and that he can be eligible for the LIS.
Is Frank married? Are they living together? YES
SSI deeming rules apply, as in SSI or Medi-Cal. LIS information is checked against the data Social Security has on file for the spouse.
Frank’s exempt assets: The house he lives in, his car, $1,500 in savings for burial

39
LIS Benefit Analysis, Frank If Frank appears to be eligible for MSP or
Medi-Cal, or both, explain the differences between applying for the LIS with Social Security, or with the local welfare or Medi-Cal offices.Social Security will not screen and enroll for MSP
and Medi-Cal.
CA welfare and Medi-Cal offices will screen and enroll for MSP and Medi-Cal.
40
Common Medi-Cal Categories Eligible forLow Income Subsidy (LIS)
41
Medi-Cal Working Disabled ProgramEligible person:• Can be working when applying for Medi-Cal• Social Security disability rules apply• Does not need to be on SSI or SSDI• IHSS personal assistance services available:
• In the program• At the workplace
• Dual status rules apply with respect to Medicare Part D eligibility
42
Medi-Cal Working Disabled Program
• Individual can earn $48,870 in 2005• Affordable premiums, $20 - $175.00 for
a single person• Any IRS approved retirement products,
Individual Retirement Accounts are allowed, “IRAs”
• Disability income not counted• See Medi-Cal on www.db101.org or in
training manual
43
Medically Needy Medi-Cal, MNCommon name: Share of Cost (SOC) Medi-Cal• Apply for Low Income Subsidy (LIS). Result:• In the first month the share of cost is met, the
recipient is eligible for the LIS in the Group 2 levels of cost sharing.
• Eligible for LIS for remainder of that calendar year.
• See Medi-Cal on www.db101.org and in training manual

44
Other Subsidy Eligible Folks
Medicare Savings Program Eligibles• Qualified Medicare Beneficiary, QMB • Specified Low Income Medicare
Beneficiary, SLMB • Qualified Individual, QI 1• Qualified Disabled Working Individual,
QDWI, • QDWI must apply for subsidy

45
Subsidy Eligibles Medicare Benefits Planning Tips Assess if a Medicare only beneficiary may be eligible for
Medi Cal, or a Medicare Savings Program (MSP). If so, Medicare, and Medicare drug benefit may become more
affordable.File Subsidy application at CA Medi-Cal for
processing, not at Social Security.Counties encouraged to take Medi-Cal and MSP
applicationsSubsidy application filed with Social Security will
not be screened for MSP or Medi-Cal eligibility.CA All County Welfare Directors Letter ACWDL
05-23 (August 4, 2005)Medicare Part D Prescription Drug Program
46
Other Subsidy Eligibles
Duals living in institutions have no cost sharing or copays during those months.Special rules apply for these plans and
their participating pharmacies
47
Subsidy Help Groups• Group 1
• Full-benefit dual eligibles with incomes at or below 100% of the Federal Poverty Level (FPL), $9,570
• Group 2• Full-benefit dual eligibles above 100% of FPL, $9,570• Medicare Savings Programs eligibles or enrollees: QMB, SLMB,
QI, or non-dual eligible beneficiaries with incomes below 135% FPL, $12,920 and limited resources ($6,000 per individual and $9,000 for a married couple)
• Group 3• Medicare beneficiaries with incomes below 150% FPL, $14,355
and limited resources ($10,000 individual and $20,000 married couple) (CMS March 2005)

48
Subsidy Levels Courtesy: The Health Strategies Consultancy
Group 1, 2, 3 Premium Deductible CopaysCoverage
Gap
#1-Up to 100% FPLand a dual eligible
None None $1 / $3 None
#2-Up to 135% FPL or all other duals None None $2 / $5 None
#3-135 - 150% FPLand not dual-eligible
Sliding Scale $50
15% of drug cost None
49
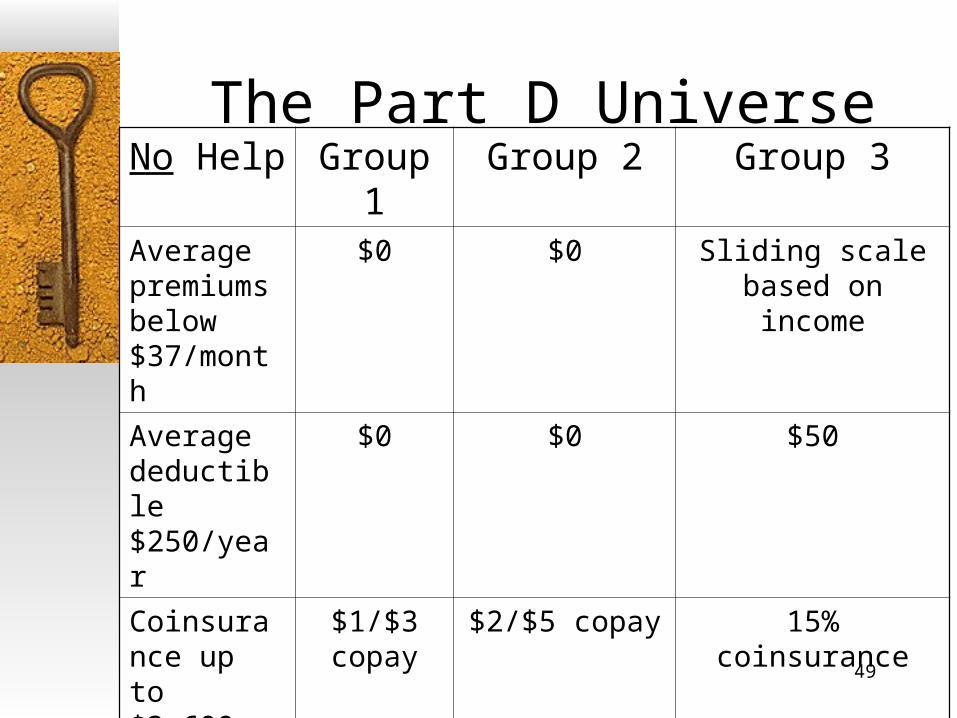
The Part D UniverseNo Help Group 1 Group 2 Group 3
Average premiums below $37/month
$0 $0 Sliding scale based on income
Average deductible $250/year
$0 $0 $50
Coinsurance up to $3,600 out of pocket
$1/$3 copay
$2/$5 copay 15% coinsurance
Catastrophic 5% or $2/$5 copay
$0 $0 $2/$5 copay

50
Lower Subsidies for Medicare Enrollees who are not Medi-Cal Eligible
• Medicare only enrollees are eligible for a subsidy based on income levels• Individuals with income below 135% FPL and resources at or
below $6,000 ($9,000 couple) receive full subsidy with $2/$5 co-pays, or Group 2
• Individuals with income below 150% FPL and resources at or below $10,000 ($20,000 couple), or Group 3:
• Sliding scale premium
• $50 deductible
• 15% cost-sharing up to $3,600 out-of-pocket limit (OOP)
• $2/$5 co-pay after OOP limit is reached

51
Subsidy Eligibility DataCourtesy: ©The Health Strategies Consultancy
The Federal Poverty Level, or “the FPL”
2005 - 100% of FPL: $9,570 for one-person household, $12,830 for two-person household;
135% of FPL: $12,920, and $17,321 respectively;
150% of FPL: $14,355, and $19,245 respectivelySliding scale premium defined for individuals between 135-150% FPL
• 135%-140% FPL, CMS will cover 75% of premium • 140%-145% FPL, CMS will cover 50% of premium • 145%-150% FPL, CMS will cover 25% of premium
Subsidy Income and Resource Calculations generally based on SSI countable income and asset rules, with some changes.
Note: Institutionalized dual eligibles pay NO cost-sharing.
52
Medicare Training
1. Medicare Parts and Supplements
2. New Prescription Drug Benefit 2006
3. Financial Subsidy for New Drug Plan Costs
4. What’s in a Medicare Prescription Drug Plan?
53
2006 Prescription Drug BenefitDrug Plan FormulariesContain:
1. Broad categories, for example, drugs for depression
2. With classes of drugs in each category grouped according to chemical nature of the drugs, for example antineoplastics (cancer drugs)

54
2006 Prescription Drug BenefitDrug Plan Formularies• Must provide 2 drugs for each of 146 drug
therapy categories. Brand name and generic drugs will be in each formulary (CMS 3/05).
• Provide prescription drugs, biologicals, insulin and medical supplies for injection of insulin
• Allowed to change drug formulary at any time with 60 days written notice to doctors, pharmacists and beneficiaries using that drug
55
2006 Prescription Drug BenefitDrug Plan Formularies• Cannot provide Barbiturates, Benzodiazepines, valium,
xanax, non prescription drugs, or agents used for anorexia, weight loss, fertility, hair loss
• Cannot provide drugs available in Medicare Part A or Part B regardless of whether beneficiary has Part A or Part B.
• CMS will ensure formularies do not discourage enrollment among certain groups of people (CMS 3/05).
• The PDP not Medicare makes the determination of what is medically necessary.
• Formulary review requirements are posted on www.cms.hhs.gov/pdps
56
2006 Prescription Drug BenefitDrug Plan FormulariesCMS Administrator Mark McClellan recently announced that
there will be 6 categories of drugs for which all Part D plans must provide a: 1. Majority of antidepressants 2. Majority of antipsychotics 3. Majority of anticonvulsants 4. Majority of antiretrovirals 5. Majority of immunosuppressants 6. Majority of antineoplastics (cancer drugs)
If a Part D plan does not cover “all or substantially all” of the drugs in each class, the plan must provide justification to CMS why not.
57
Plans can have tiered formulariesPreferred Drug Levels
• Tier 1 has the lowest cost sharing.• Subsequent tiers have higher cost sharing in
ascending order.• CMS will review to identify drug categories that
may discourage enrollment of certain people with Medicare by placing drugs in non-preferred tiers
• Plan must have procedures so beneficiaries can request exceptions for tiered formularies
(CMS March 2005)
58
Drug TransitionPlanning – Plan “Requirements”423.120 (b)(3)) CMS MMA regulation
Prescription Drug Plans are required to have an approved drug "transition process" for new enrollees. http://www.cms.hhs.gov/medicarereform/issuepapers/title1and2/
Expected to have procedures for medical review of non-formulary drug requests by the beneficiary
59
2006 Prescription Drug BenefitCA Dual Eligible LIS covered Drug Plans
Stand-Alone Drug Plans10 PDPs approved statewide with LIS coverage
(CMS as of 10/10/05)
Medicare Advantage Drug PlansMA-PDs approved and with LIS coverage are
listed county by county
Keep Checking www.Medicare.gov Landscape of Local Plans 1-800-MEDICARE will mail detailed responses to caller
inquiries

60
Drug TransitionPlanning Requirements423.120 (b)(3)) CMS MMA regulation
Special Enrollment PeriodAllows a full-benefit dual eligible individual to change PD plans to better accommodate his/her pharmaceutical needs and pharmacy affiliations at any time because of a Special Enrollment Period afforded to them. (SEP)
Special Enrollment Period allows full benefit dual eligibles to switch from one MA-PD plan to another, from one PD plan to another, or from original Medicare and a PD plan into an MA-PD plan and vice versa.
Special Enrollment Period extends beyond December 31st indefinitely. There is no known termination date for duals eligible for the SEP.
61
Medicare Training1. Medicare Today, Parts and Supplements
2. Temporary Prescription Drug Discount Card
3. New Prescription Drug Benefit 2006
4. Financial Subsidy for New Drug Plan Costs
5. What’s in a Medicare Prescription Drug Plan?
6. Special Needs Plans
62
Special Needs Plans - SNPs
• SNPs by design cover all services for SNP enrolled beneficiaries
• SNPs running now or soon: • Evercare • Cal Optima OneCare, Orange County: 55,000
Orange County duals would be eligible to enroll.
63
Cal Optima OneCareDiscussionA single system responsible for providing
access to a full continuum of services • Primary and specialty physician care• Acute inpatient care• Prescription drugs• Medical supplies and equipment• Home and community based care (future)• Long-term care
• Coordinate care and help members get the services they need

64
Medicare Training1. Medicare Parts and Supplements
2. New Prescription Drug Benefit 2006
3. Financial Subsidy for New Drug Plan Costs4. What’s in a Medicare Prescription Drug Plan?
5. Special Needs Plans
6. Beneficiary Protections, Appeals and Exceptions in New Drug Plans
65
Plan Information Dissemination
• Plans must provide information about• Service areas• Benefits• Cost sharing• Formulary• Pharmacy access• Other aspects of coverage available through the
plan

66
Exceptions Process
• Ensures access to medically necessary Medicare covered prescription drugs
• Provides process for enrollee to • Obtain a covered Medicare prescription drug at
a more favorable cost-sharing level• Obtain a covered Medicare prescription drug
not on the formulary

67
Protections and Appeal Process
• ALL beneficiaries protected by the same process, no population receives special or different formulary access
• Some protections: • CMS oversight of formularies to prevent
discrimination to Medicare sub-populations• PDP drug transition process

68
A Coverage DeterminationThe Appeals and Exceptions Process5 steps for an exception or an appeal to a PDPAppeal rights are provided to beneficiaries by all PDPs. The beneficiary, not others, appeals or files an exception to the plan, not to
the pharmacy. A Coverage Determination comes from the PDP or MA-PDP to the beneficiary.
Beneficiary files a Redetermination request of an unfavorable Coverage Determination to the PDP using this process.A Redetermination is performed by the PDP. If a negative result:
1. Beneficiary files a Request for Reconsideration to an Independent Review Entity, IRE, a CMS contractor. IRE decisions based on and have capacity for medical appropriateness. Unfavorable PDP Redeterminations above are not auto referred to an IRE.
2. Further appeal allowable to an Administrative Law Judge (ALJ)3. Further appeal allowable to the Medicare Appeals Council (MAC),
and finally to4. Federal Court
Process builds on the current Medicare Part C (MA) Appeals Process
69
Coverage Determination and the Appeals www.medicareadvocacy.org Appeals Process Resource
Expedited Review (faster) is available when and if Medicare Part C (MA) due process standards are in place and being met.
Continued drug coverage pending an appeal (as in current Medi-Cal protections) is not included.
Pharmacy is allowed to not fill a prescription if beneficiary does not have the copay, but is also allowed to waive the copay.
70
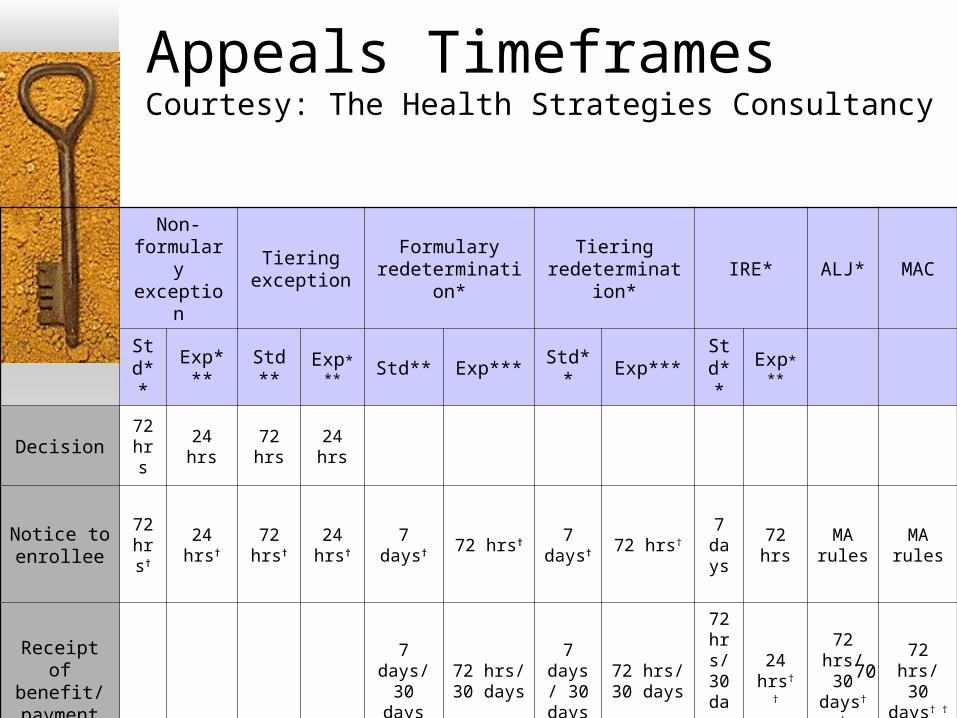
Appeals Timeframes Courtesy: The Health Strategies Consultancy
Non-formulary exception
Tiering exception
Formulary redetermination*
Tiering redetermination*
IRE* ALJ* MAC
Std**
Exp***
Std** Exp***
Std** Exp*** Std** Exp***Std**
Exp***
Decision72 hrs
24 hrs 72 hrs 24 hrs
Notice to enrollee
72 hrs† 24 hrs† 72
hrs†
24 hrs† 7 days† 72 hrs† 7
days† 72 hrs† 7
days
72 hrsMA rules
MA rules
Receipt of benefit/ payment
7 days/ 30 days
72 hrs/ 30 days
7 days/
30 days
72 hrs/ 30 days
72 hrs/ 30 days † †
24 hrs† †
72 hrs/ 30
days† †
72 hrs/ 30 days†
†
71
Due Process
PDPs are required to send written Notice of a formulary change or cost sharing change at least 60 days in advance of the changes to those enrolled using that drug; and,
The Notice must be sent to CMS, SPAPs, pharmacies and prescribing providers. http://www.cms.hhs.gov/medicarereform/issuepapers/title1and2/ - Issue Paper #33
72
Medicare Training1. Medicare Parts and Supplements2. New Prescription Drug Benefit 20063. Financial Subsidy for New Drug Plan Costs4. What’s in a Medicare Prescription Drug
Plan?5. Special Needs Plans6. Beneficiary Protections and Appeals7. State of California Involvement

73
Medi-Cal, Dept. of Health Services• Medi-Cal “wrap-around” coverage to Part D
• CA new budget contains $94 million for current Medi-Cal drugs not available in Medicare Part D and which will continue to receive federal match funds
• No CA funds available for Part D covered drugs, co-pay assistance, or premium assistance for higher cost plans.
• CA is required to help CMS identify duals.• State is required to take subsidy applications, along
with Social Security, the lead agency for subsidy applications for those who must apply for a subsidy
• Those who are not already deemed and/or notified by CMS.

74
Medicare Training1. Medicare Today, Parts and Supplements
2. New Prescription Drug Benefit 2006
3. Financial Subsidy for New Drug Plan Costs
4. What’s in a Medicare Prescription Drug Plan?
5. Special Needs Plans
6. Beneficiary Protections and Appeals
7. State of California Involvement
8. Resources, Citations and References
75
www.Medicare.gov
Landscape of Local Plans Compare Medicare Prescription Drug
Plans Formulary Finder Medicare & You 2007

76
ResourcesFor individual counseling and assistance
HICAP: Health Insurance Counseling and Advocacy ProgramStatewide program, state and federally funded counseling
Call 1-800-434-0222 for individual appointments
For technical information and assistance California Health Advocates 916-231-5110 (Sacramento office)
Medicare fact sheets, updated information for CAwww.cahealthadvocates.org and
www.calmedicare.org
California Benefits Plannerswww.db101.orgworking with a disability in California
77
Resources Center for Medicare and Medicaid Services,
CMSwww.medicare.gov1-800-MEDICARE, TTY 1-877-486-2048
www.cms.hhs.gov/medicarereform/Center for Medicare Advocacy, Inc.
www.medicareadvocacy.orgKaiser Family Foundation
www.kff.orgFamilies USA
http://www.familiesusa.org/site/PageServer?pagename=Medicare_Drug_Law_Materials
78
Citations and Legal References• Medicare Part D Statute and Regulation(s)
• 42 USC § 1395, Tit. XVIII.• 70 Fed. Reg. 4194 (January 28, 2005).• 42 CFR Parts 400,403,411,417 and 423.• www.cms.gov
• Low Income Subsidy• 70 Fed Reg 10558 (March 4, 2005).• 20 CFR Part 418.• POMS Section HI 03001.000 et seq
• Dept. of Health Services Index: All County Welfare Director Letters: • http://www.dhs.ca.gov/mcs/mcpd/MEB/ACLs/
© Copyright 2006 by World Institute on Disability, permission to copy will be granted to non profit entities with appropriate acknowledgement of credit.