world bank document - documents & reports - all...
TRANSCRIPT

Document of
The World Bank
Report No. 13947-SL
STAFF APPRAISAL REPORT
REPUBLIC OF SIERRA LEONE
INTEGRATED HEALTH SECTOR INVESTMENT PROJECT
FEBRUARY 6, 1996
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized

CURRENCY EQUIVALENTS(as of January 5, 1996)
Currency Unit = LeonesUS$1.00 = 948 Leones
ACRONYMS AND ABBREVIATIONS
AfDB African Development BankDHMT District Health Management TeamDOF Department of FinanceDOH Department of HealthEU European UnionFP Family PlanningFY Fiscal YearGDP Gross Domestic ProductGOSL Government of Sierra LeoneI-RV Human Immunodeficiency VirusICB International Competitive BiddingIDA International Development AssociationtMF International Monetary FundIPAM Institute of Public Administration and ManagementMCH Maternal Child HealthNHAP National Health Action PlanNCB National Competitive BiddingNGO Non-Governmental OrganizationPHC Primary Health CarePHU Peripheral Health UnitPHRD Policy and Human Resources Development (Japanese Grant)PMISU Planning, Monitoring, Information and Statistics UnitPER Public Expenditure ReviewPIP Public Investment ProgramSAP Structural Adjustment ProgramSDR Special Drawing RightSIP Sector Investment ProjectSOE Statement of ExpenditureUNDP United Nations Development PrograrnmeUNFPA United Nations Fund for Population ActivitiesUNICEF United Nations Children's FundWFP World Food ProgramWHO World Health Organization
BORROWER'S FISCAL YEAR
January 1 - December 31 (from January 1, 1996)July 1 - June 30 (until December 31, 1995)

REPUBLIC OF SIERRA LEONEINTEGRATED HEALTH SECTOR INVESTMENT PROJECT,
Contents
CREDIT AND PROGRAM SUMMARY .......................................................... iii
L INTRODUCTION ........................................................... 1
HI. THE HEALTH SECTOR .......................................................... _2
A. SECTOR BACKGROUND ........................................................................... _2
B. CURRENT STATE OF THE HEALTH SECTOR ..................................................................... 3Organization of the health care system ............................. 3..............................3Status of health facilities ........................................................... 4Health personnel ........................................................... 5Health financing ........................................................... 5
C. PREVIOUS BANK OPERATIONS IN THE HEALTH SECTOR AND LESSONS LEARNED ............. 8D. DONOR ASSISTANCE IN THE SECTOR ............................................................................ 8
E. KEY ISSUES ............................................................................ 9Poor access to health care ........................................................... 9Poor quality of services .......................................................... 10Poor management, with inadequate community involvement and accountability ....... 10Insufficient financing and misallocation of scarce resources ................ ...................... 11
IM. THE HEALTH SECTOR DEVELOPMENT STRATEGY .. 11
A. THE GOVERNMENT REFORM PROGRAM ...................................................................... 11B. RATIONALE FOR IDA INVOLVEMENT ........................................................................... 12C. BANK ROLE IN THE HEALTH REFORM PROGRAM .......................................................... 13D. FUTURE DONOR SUPPORT FOR THE HEALTH REFORM PROGRAM ........... ....................... 14
IV. THE PROGRAM .......................................................... 15
A. PROGRAM SCOPE AND OBJECTIVES ........................................................................... 15B. PROGRAM DESCRIPTION ........................................................................... 16
iThis report is based upon the findings of missions which visited Sierra Leone in February, May and August, 1994,and February and October, 1995. The mission members consisted of Messrs./Mmes. D. Peters (MissionLeader/Public Health Physician, AF4PH), S. Luculescu (Mission Leader/Senior Public Health Specialist, AF5PH), J.Angers (Operations Analyst, AF4PH), S. Ben-Halima (Implementation Specialist, AF5PH), A. E. Elmendorf (LeadAdvisor/Principal Management Specialist, AFTHR), F. Fichtl (Economist, AF5PH), D. Harris (Economist, AF4PH),G. Raheem (Project Management Specialist, AFTCB), 0. Ransome-Kuti (Professional Education/PHC Specialist,AFTHR), K. Bhattacharyya (Beneficiary Assessment, Consultant), K. Brown (Human Resource ManagementSpecialist, Consultant), S. Cunningham (Financial Management Specialist, Consultant), B. Siegel (Health PolicyAdvisor, Consultant), and S. Bradley, J-P. Manshande, and P. Bachrach (Health Planning Consultants). TheTechnical Review team includes Ms. H. Saxenian (PHN), Ms. D. Vaillancourt (PHN), and Mr. J. Roome (AFIEI).Ms. J. Christiansen assisted in the preparation of the report. Messrs. 0. Pannenborg and J-L. Sarbib are themanaging Division Chief and Department Director, respectively, for the operation.
- ii -
Definition of NHAP technical programs and support services . .................................. 17Health facilities rehabilitation and re-tooling .................................................... 18Institutional development .................................................... 19The first year program .................................................... 22
C. PROGRAM COSTS AND FNANCING ................................................................. 24
V. PROGRAM IMPLEMENTATION .................................................... 29
A. STATUS OF PROGRAM PREPARATION ........................................................ ......... 29B. PROGRAM IMPLEMENTATION (MANAGEMENT AND COORDINATION) ........... ................ 31C. PROGRAM SUSTAINABILiTY AND RECURRENT COST IMPLICATIONS .............................. 32D. PROGRAM MONITORING AND REPORTING ................................................................. 33E. ANNUAL AND MID-TERM REVIEWS .................................... ............................. 35F. ENVIRONMENTAL ASPECTS ................................................................. 35G. PROCUREMENT ................................................................. 35H. DISBURSEMENTS ................................................................. 39I. ACCOUNTING, AUDITING, AND REPORTING ................................................................. 40
VL PROGRAM BENEFITS AND RISKS .................................................... 41
A. PROGRAM BENEFITS ................................................................. 41B. PROGRAM RISKS ................................................................. 41
VLL AGREEMENTS, CONDITIONS, AND RECOMMENDATION .. 42
ANNEXES
1. Socio-Economic Indicators2. Letter of Health Sector Development Policy3. Causes of Mortality in Western Area4. Distribution of Health Facilities and Public Sector Health Workers5. Historical Health Sector Expenditures in Sierra Leone6. Communique of the Social Sectors Round Table Consultations7. Framework for Prioritization of the Core Program of the National Health Action Plan8. Detailed Description of Technical and Support Programs9. Proposed Training Plan10. Detailed Program Cost Estimates and Financing Plan11. Draft of Key Health Sector Performance Indicators12. Department of Health Organogram13. Summary Program Implementation Schedule14. Operational Manual Draft Table of Contents15. Supervision Plan16. Disbursement Forecast
Map

- iii -
REPUBLIC OF SIERRA LEONE
INTEGRATED HEALTH SECTOR INVESTMENT PROJECT
CREDIT AND PROGRAM SUMMARY
Borrower: Republic of Sierra Leone
Beneficiary: Department of Health (DOH)
Poverty: Not included in the Program of Targeted Interventions
Credit amount: SDR 13.6 Million (US$20.0 Million equivalent)
Terms: Standard IDA terms, with 40 years maturity
Commitment Fee: 0.50 percent on undisbursed Credit balances, beginning 60days after signing, less any waiver.
Financing Plan: See paragraph 4.20 on page 27
Net Present Value: Not applicable
Staff Appraisal Report: 13947-SL
Map: IBRD 26923
Project ID No.: SL-PA-2422


Republic of Sierra LeoneINTEGRATED HEALTH SECTOR INVESTMENT PROJECT
I. INTRODUCTION
1.1 The Government of Sierra Leone, in its effort to improve the health of its people, hasrequested IDA assistance of SDR 13.6 million (US$20 million equivalent) to finance a Creditaimed at supporting the Government's reform of the health sector based on its National HealthAction Plan (NHAP).
1.2 With an annual GNP/per capita of only US$150 (1993), Sierra Leone is classified asone of the poorest and "least-developed" countries in the world. After negligible growth in the1970s, the economic situation sharply deteriorated in the 1980s, coinciding with the Bank'sfive-year suspension of activities in the country. By 1990, over two-thirds of the populationlived in absolute poverty, a situation exacerbated by the influx of refugees from Liberia and,more recently, the displacement of large segments of the population due to rebel attacks onmining sites and small towns (see Box 1). Although measures taken by Government,particularly during the last months, seem to bear positive results, the future remains difficult topredict, and the country is faced with new economic problems such as inflation caused by thedecline of export revenue, particularly of rutile and diamond mining industry. This situationis being compounded by the fact that social services and human resources have been largelyneglected during the past decade. At present, the infrastructure in the social sector hasdeteriorated significantly because of the absence of maintenance systems, the erosion of publicsector management and underfunding.
1.3 Faced with limited resources, the Government of Sierra Leone (GOSL), with assistancefrom the Bank and the IMF, embarked on an ambitious structural adjustment program in late1989, aimed at economic stabilization and creation of conditions for sustained economicgrowth and reduction of poverty. As stated in its Policy Framework Paper, increased publicinvestment in social sectors, particularly for basic education and health care, is a central part ofthe GOSL adjustment program and development strategy. Substantial progress had been madein achieving macroeconomic and fiscal management targets: growth rates are recovering, andinflation, which reached a peak of 170 percent in 1986-87, stabilized at around 15 percent in1993-94. Since the resurgence of rebel activities, macroeconomic performance has begun tosuffer as a result of decreasing revenues from the productive areas of the country, anddeviations of public expenditures, largely for military purposes. Government has maintainedits fiscal commitments to the health sector, though without external support to implement itsproposed plan, it will be difficult to maintain these efforts in the medium term. Rehabilitationof social infrastructure has begun with the resumption of donor assistance and IDA projectactivities, yet there remains an enormous challenge to assure the provision of basic socialservices and to develop the institutional capacity needed to maintain them. The proposedinvestment credit would help the Government's sector reforms lay the foundation for asustainable, equitable and efficient health system, while addressing the new demandsexacerbated by the rebel activities.

II. THE HEALTH SECTOR
A. SECTOR BACKGROUND
2.1 Sierra Leone has hardly begun the health BOX 1 The Security Situation in Sierra
transition, as evidenced by its dire health Leone
indicators. The population of 4.7 million (1995)' Since January, 1995, rebels (assumed to be nois growing at an approximately 2.6 percent per more than 500-600) have mounted a "hit andyear. The total fertility rate is very high, estimated run" campaign against the public. Villages,at 6.5. Little change in fertility can be expected road convoys, construction sites, and minesuntil substantial improvements are made in have been attacked, in some cases taking
cvilians in custody. Many vilagers (perhapsmortality conditions, which are among the worst up to 1 million) have moved to safer areas inin the world. High fertility also contributes the main towns and in neighboring Guinea.significantly to high mortality. Life expectancy, Aid workers have relocated to Freetown, andafter improving during the 1 960s and 1 970s, most development efforts outside Freetowns4tagnated during the 1980s, and is currently only have ceased. For years, the rebels did not
specify a political or military agenda, though39 years,' the lowest in the world. More than one in the last few months, one leader haschild in four dies before the age of five, and adults expressed his intention to become presidethave the second highest rate of mortality in the The initial attempts of the government toworld (World Development Report, 1995). The resolve the conflict by increasing the size ofmain causes of mortality and morbidity are the army were lagely unsuccessful andcontributed to a loss of discipline in the army.infectious diseases, largely related to the childhood In June, 1995, the Government hired a privatecomplex of pneumonia, diarrhea, measles and mercenary force, which has mounted anmalnutrition (see Annex 3). Other infectious intense coumter-offensive against allegeddiseases, such as malaria, tuberculosis, rebel targets. In paralel with the militaryonchocerciasis and schistosomiasis, are highly approach, the Govement ha also takenseveral initiatives to reach a negotiatedprevalent in all age groups, and the human solution and to foster democracy byimmunodeficiency virus (HIV) poses a new threat announcing general elections for early 1996.to youth and adults (HIV prevalence is estimated At Government's request, a special UN envoyat nearly five percent among low risk groups in is trying to broker a settlement with rebel
leaders, while the Commonwealth SecretariatFreetown). Maternal mortality rate IS also and the Organization of African Unity areexceptionally high, estimated at 800 deaths per also actively supporting negotiated solutions.100,000 deliveries. Foreign representatives are firm in their
assessment of the Government's commitment2.2 The nutritional situation has changed to end the war. To date, the outcomes oflittle over the last decade. In 1978, a national these measures look promising but not yetsurvey revealed that 30.5% of children under five conclusive.years were underweight; the most recent estimate in 1989-90 showed a prevalence of 33.4%in the same age group. The data show similar trends for stunting and wasting. The dailysupply of calories is only about 1,800 - less than 80% of estimated requirements; about the
Department of Health figures differ, estimating the population to 4.2 million and life expectancy at 43 years and 45years.

same level as ten years ago. Micronutrient deficiencies are also common. For example, iron-deficiency anemia is found in about two-thirds of pregnant women and nearly 60% of allchildren. Among other causes, this can be attributed to chronic or recurrent illness (especiallymalaria), worm infestation, poor feeding practices (e.g. late addition of supplemental foods forinfants), and short birth spacing.
2.3 There are a number of factors contributing to the poor levels of health statusindicators in Sierra Leone. There is a high burden of disease exposure due to crowded andunsanitary living conditions. For example, less than half the population has access to safedrinking water or sanitation facilities, with conditions being much worse in rural areas. Toomany children, spaced too closely, by mothers that are too young, increase health risks tomothers and their children. Extremely low levels of literacy and basic education leave manypeople ignorant about good health practices, limit the ability of women to make healthychoices for their families, and perpetuate the cycle of poverty and illness. These areaggravated by the social disruption and disorganization that has afflicted Sierra Leone.Traditional practices and cultural norms also may impose additional health risks or may limitaccess to modem health care.
B. CURRENT STATE OF THE HEALTH SECTOR
2.4 According to the Government, health services have "reached an appalling state ofdeterioration both in quality and scope" (NHAP). Because of this, health care services aredoing little to respond to the huge health needs of the population. A lack of sustained politicalwill, grossly inadequate funding, and the near absence of responsibility and accountabilitywithin the health sector in the past contributed to the breakdown in public services. Theprivate sector has compensated to a small degree for failings of the public system, but mostprivate services are inaccessible to the majority of the population and are of variable quality.
Organization of the health care system
2.5 Health care is provided through a network of about 550 primary, secondary, andtertiary government health facilities, and another 35 hospitals and 84 clinics operated by themission and private sectors (see Annex 4). There are two main types of public facilities, asoutlined below.
(a) Peripheral Health Units (PHUs). Over 500 PHUs are supposed to provideprimary health care services: predominantly antenatal care, family planning,immunizations, and simple curative care. There are currently three types of PHUswhich differ, at least in concept, by the level of staffing, equipment, and the size of thecommunities in which they serve. In order of decreasing size, these PHUs are locatedat chiefdom headquarters (Community Health Centers, catchment population of 10,000- 20,000), small towns (Community Health Posts, catchment population of 5,000), andvillage level (Maternal and Child Health Posts). The latter facilities may not be formalclinics, as they are often based in the homes of local health workers (MCH Aides).
- 4 -
(b) Hospitals. There are 24 public hospitals currently open, which mostly providethe services of a first referral hospital. The Govemment defines hospitals with lessthan 40 beds as secondary care facilities, and larger hospitals as tertiary care facilities.The larger hospitals are usually located in major towns (e.g. provincial headquarters)and are supposed to have more specialized curative care services. Connaught hospitalin Freetown is the main referral hospital in the country.
2.6 Prior to the sector reforms of 1994, the organizational structure of the Department ofHealth (DOH) was convoluted, and inconsistent with the health care delivery system. Healthactivities in the DOH were separated between "clinical" and "public health" services, and therewas no clear responsibility for or authority over health service delivery. There was very littlesharing of information or coordination of the different "programs" that existed, partly becauseof a lack of joint planning and the separate funding arrangements with different donors. Theheadquarters of the DOH did not have a single executive head, and the administrative authoritywas divided between the Permanent Secretary and the Chief Medical Officer, who handlednearly all paperwork and decisions in the DOH. The vast majority of decisions regardingbudgets, expenditures, appointments, discipline and pay were still referred to other CentralGovernment Departments. In the DOH, the major services needed to operate a GovernmentDepartment, such as those for budgeting, accounting, personnel and management informationwere at best extensions of Central Departments, with little autonomy, capacity, or directionfrom the DOH.
2.7 Below the headquarters level, the Provincial management tier is being eliminated,opening up a direct link between headquarters and the district level (there are 12 rural districtsand 2 administrative divisions in Western Area-Freetown). A District Medical Officer (usuallya "public health" physician) heads the district management team, and the district hospital isusually headed by another District Medical Officer (a "clinical" physician). The district teamis responsible for both primary and secondary care facilities, but in practice, hospital planningand management have been quite separate from other district health activities. District teamslack the management structures and authority to plan, make expenditures, or monitor healthservices in their districts. Few district teams provide training, supervision or other support totheir PHUs, much less interface with their communities in a meaningful manner. For example,community health or development committees are rarely functional. There is no effectivereferral system, and hospitals spend much of their resources providing primary curative care.Many of the services that are to be delivered at PHUs are being done poorly, and someservices, in particular health education, family planning, and community nutrition, arefrequently not delivered at all.
Status of health facilities
2.8 Except for a few projects earmarked by donors, specific data on the physical status onmost health facilities are not yet available. The physical state of most hospitals and clinics isdeplorable, since virtually no attention has been paid to maintenance and repairs in decadepreceding 1992. Basic infrastructure (water, electrical power, and access roads) is oftenlacking. Furthermore, in a 1994 DOH/WHO survey of district health care, it was determinedthat there are not enough PHUs, and also noted that many of the clinics that were expected to

exist were no longer in operation. There was no functional ambulance or communicationssystems to connect PHUs to hospitals until 1994, when a small ambulance service was started.Although the situation has improved in the last two years, shortages of essential drugs(including contraceptives and vaccines), medical equipment, and supplies are commonplace,seriously undermining the capability of facilities to deliver services.
Health personnel
2.9 The 1994 DOH/WHO survey of district health care revealed that there are widevariations in the numbers and levels of qualified staff in PHUs. In general, health personnelare unevenly distributed, inadequately trained, badly supervised, poorly supported, and under-compensated. Consequently, staff performance is poor and morale is low. It is estimated thatcurrently nearly two-thirds of all health personnel are deployed in hospitals, including allclinical doctors in the public sector. To establish the basis for forward looking manpowerplanning, the DOH has initiated the set up of a manpower database to monitor the actualnumbers of health personnel, their qualifications, and location (see Annex 4 for the estimateddistribution of health personnel). In its preliminary estimates, the NHAP indicated that thereare major shortages of community health workers, pharmacy technicians, nurses, midwives,and doctors. At the same time, the DOH has been hampered with a large number of dailywage earners, which has consumed much of the wage bill and prevented the recruitment ofmuch needed health staff. By mid-1991, more than half of the DOH's staff consisted of dailywage workers (6,100). Since then, however, the number of daily workers has been reduced tounder 2,200, and the number of staff given temporary appointments has dropped by 27 percent(see Figure 2.1).
2.10 In the past, training of health workers has been inconsistent, and has suffered fromchronic under-funding, ad hoc development of training programs, out-dated and redundantcurricula, and poor competing local training institutions. Government recognized theseproblems and, despite prevailing constraints, developed well-designed training programs forMCH Aides and other mid-level staff as well as a physician training program. As part of itsnew manpower plan, the DOH has decided to rationalize the composition and training ofhealth workers according to the types of skills needed at various levels of the health system.The implementation of this plan is part of the NHAP core program.
Health financing
2.11 During the past decade, the health sector has been grossly under-funded. In FY90/91,the share of health expenditures in the total Government expenditures was about 2 percent, andthe share of the recurrent health expenditures in the total Government recurrent expenditureswas about 2.8 percent, both in sharp decline as compared to the previous years, e.g., in1980/81, these shares were 6 percent and 7 percent, respectively. This situation is graduallybeing reversed under the current structural adjustment program. As a result, in FY95/96 thehealth sector's share in the total Government's expenditures increased to about 6 percent (seeFigure 2.2). In real terms (constant 1986/87 Le), health expenditures per capita increased fromabout Le2O in FY90/91 to Le33 in FY 95/96, and as a share of GDP, the public sector's healthbudget increased from 0.4 percent to about 1 percent over the same period (see Annex 5). The

- 6 -
Government, at the Social Sector Consultation with donors and NGOs in October 1995,reiterated its commitment to further increase the financial allocation to the health sector.Although this might be hampered by slow economic growth and a high population growth rate,it appears reasonable to attempt to maintain, or slightly increase, the share of financialresources allocated to the health sector at the current level of more than 6 percent of theGovernment budget (not including public debt service). In US Dollar terms, per capitaexpenditures for health in the public sector in 1995/1996 amounted to approximately $3.1($1.5 contributed by GOSL and $1.6 by donors). Based on the household survey conducted in1989/1990, it can also be estimated that some other $4 were spent by the population in theprivate formal and informal health sector. Under the new project, the Government's allocationfor the provision of health services in FY 1996 will amount to approximately $2.1 per capita,while donor assistance to the health sector from bilateral and multilateral sources, as well asfrom NGOs, will exceed current Government contribution, and will amount to approximately$3.2 per capita. This will represent an increase of funding to the public health services ofabout 70%.
Fizure 2.1
DOH Employment Trends 1991 - 1995
7000 - Pernn Staff6000 -i ---- Temp. Staff
6000 - - - * - -Daily Workers4000 -
2 000 IL-
1000
0Jun491 Jun492 Jun493 Jun-94 Sep496
Source: Government of Sierra Leone--Accountan Gyeneral's Office
2.12 Government financed development expenditures in the health sector were negligibleduring since the beginning of the 1990s. The only notable exception has been theestablishment of a new College of Medicine and Allied Health Sciences in 1988, financed asan educational institution from funds allocated to the Department of Education. A proposal tobuild a new tertiary hospital near Freetown has been on the drawing board for nearly 10 years.However, in the process of setting the priorities for the NHAP, Goverinment has made aconscious and commendable decision to postpone the building of a tertiary care hospital and toconcentrate its infrastructure development efforts on primary health care and on rehabilitatingexisting facilities.

-7 -
Figure 2.2
Govemment Expenditure in the Health Sector(Percertages of Total Expenditue)
7.00%
OO00% Total Exp. in Heafthrrotal5.00%y Exp.
4.00% - - -- -- Recuwrert Exp ./Total
3.00y. . . . - * - ~ i / Recwrert Exp.
2.00Y / - - - Investmert Exp.lotal2.00Y. - , -lrw ~ ~ ~ _s X Investment Exp.1.00%Y -O
O.0. ___S' II s_I I
90191 91192 92193 93194 94J96 95196*
Source:Govemment of Sierra Leone--Department of Finance
* Budget Allocation
2.13 Since the inception of its health sector reform, the DOH has achieved a stunning turn-around in the economic composition of its recurrent expenditures by reducing the share ofpersonnel expenditures and, conversely, increasing the share for other operating expenditures.In 1992/93, the DOH used more than 63 percent of all recurrent expenditures for salary andwage related expenses. This share has been reduced, within two years, to only 30 percent in1994/95 (see figure 2.3). The underlying basis for this change has been the above mentionedreduction in DOH staff, in particular of daily wage workers (see para. 2.9), and the increase ofthe budgetary allocations to the health sector. Indications are that this change has impactedpositively on service delivery, improving the funding for critical recurrent expenditures such asdrugs, contraceptives, supplies, maintenance and repair, while the laid-off staff - consisting ofeither "ghost workers" or of relatively inefficient custodial and clerical workers - hardlycontributed to service delivery.
Fieure 2.3
Economic Composition of DOH Expenditures
100% -r- -- - --- _ - -- a- - - - - - a
80%~~~~~~~~~~~~~~~~~~~~ - - ----- Persnnel
60% -'~ Goods and Services
40%. TOW....................
20%
0%1992/93 1993/94 1994/95 1995/96
Source:Govemment of Sierra Leone--Department of Finance
2.14 While this is a remarkable success, unprecedented in any other West African country,personnel expenditures remain distorted towards hospital services: it isestimated that 27% of personnel expenditures are paid to PHU workers, 72% to hospitalworkers, and the remainder to central DOH staff. Non-personnel recurrent costs also show a
- 8 -
hospital bias; 19% of these expenditures went to PHC services, and 53% went to hospitals, theremainder to central DOH operations. Salaries are still severely distorted, so that a physicianentering Govemment service receives virtually the same gross pay as a low-skilled dailyworker doing menial cleaning. However, physicians and other health providers supplementillegally their incomes through charging additional fees, allegedly enabling some of them toeam ten times their official salaries. Other health workers often demand two to four times theamount of their official salaries to augment their incomes. In January 1995, an ad-hoccommittee has been set up with support from WHO to assess the situation and to coordinatehealth care financing issues, initially focusing on tertiary level hospitals.
2.15 User fees for drugs and services were commonly applied in public facilities. However,during the last years, the sharp increase in the number of displaced people and the decliningeconomy have impoverished a large proportion of the population. The government wastherefore forced, in 1994, to temporarily suspend cost recovery for drugs and, to a large part,the collection of user fees for services.
C. PREVIOUS BANK OPERATIONS IN THE HEALTH SECTOR AND LESSONS LEARNED
2.16 The resumption in 1992 of project activities under the Health and Population Project(CR 1695-SL) has demonstrated the severe institutional weakness of the DOH. A limitednumber of very capable staff are over-stretched with responsibilities, and there are fewfunctioning management systems to support them. While much of 1992-93 was needed to re-establish the project, with increased supervision and technical assistance, project performancehas progressively improved. The project is expected to fully disburse its funds by the closingdate at the end of 1995. The experience reinforces the need for an investment operation thatconcentrates on human resource development and the establishment of management systems.It also suggests that health system investment requires a long-term commitment to effectsustainable change. Lessons from two World Bank studies have been instrumental in thedevelopment of the program. The World Development Report 1993: Investing in Health wasused as a resource in the prioritization of activities, particularly to identify the more cost-effective services. The comprehensive review of African experience, Better Health in Africa,outlines processes for change in health policy and strategy development, governmentcommitment and collaboration with the private sector, cost-effective approaches to the deliveryof care, managerial development and institutional reform, and donor support to a singlecountry reform program. These have all been adopted by the Government of Sierra Leone inthe development of the NHAP. The program is thus becoming an example of how to apply theBetter Health in Africa study.
D. DONOR ASSISTANCE IN THE SECTOR
2.17 There is a wide number of donors involved in the Sierra Leone health sector, whoseactivities have increased over the last ten years as the public system's needs have increased.The main bilateral donors have included France, Germany, the United States, the UnitedKingdom, and others, while the multilateral agencies have included, African DevelopmentBank, IDA, UNDP, UNFPA, UNICEF, and WHO. The number of non-governmental
organizations (NGOs) has also increased, and includes AFRICARE, CARE, Christian ChildrenFund, Christian Health Association of Sierra Leone, Sierra Leone Muslim Mission, PlanInternational, Plan Parenthood Association, Sierra Leone Red Cross, Marie Stopes and others.Many agencies are involved in emergency relief operations for refugees and war victims, thelargest of which is the World Food Program. Otherwise, the main activities have includedsupport for maternal child health and family planning, hospital services, and variouspreventive programs. The total amount of external assistance in the health sector wasestimated at US$8.4 million in 1992 (see Annex 5). By comparison, donor assistance for theentire period from 1989 to 1992 amounted to US$38.5 million. Most donors have bypassedGovernment structures as much as possible in the planning and implementation of theirprograms, largely because of the limited administrative and operational capacity and lack ofaccountability in the Government system, and the need to achieve short term performancecriteria by which project implementation is usually judged. The lack of coordination amongparticipants in the health sector has led to a fractionated health system. At one point in 1994,the DOH estimated that it had at least 47 different "project implementing units" aligned withthe various donors. The failure of such a divisive approach is one of the major reasons thatGovernment and donors have opted for an integrated sector-wide approach. Implementation ofthe NHAP provides the means for the DOH to develop as a Department of Health rather than aDepot for Health Projects; the DOH will become the true coordinator of the sector and guidedonor efforts, rather than the other way around.
E. KEY ISSUES
2.18 The security situation has been a central concern for the health sector in recent years,and has taken up much of the energy of the DOH and other health agencies (see Box 2). Oneof the functions of a health system is to respond to emergency needs caused by man-madecrisis or natural disasters. Government has taken the position that emergency responses andrehabilitation efforts will be wasted in Sierra Leone unless underlying reform in the healthsector also takes place. In this respect, the Government's program addresses four underlyingproblems of the health sector.
Poor access to health care
2.19 Physical access is limited by the insufficient number of functional health facilities toserve the vast majority of the population who live in rural areas. Only about 65% of thepopulation live within a 10 km radius of a health facility, and the proportion is lower in theNorthern and Southern Provinces. Many of the facilities provide poor quality services, due tolack of diagnostic equipment, drugs, contraceptives, vaccines and supplies, or because of a lackof qualified and motivated staff. Inadequate knowledge about the need for health care, highfees charged by health workers, and the poor quality of care also diminish the access to and theuse of health care services, particularly for the poor.

- 10-
Box 2 The Effects of the Security Crisis on the Health Sector
The deteriorating security situation has put additional strain on an already weakened public health system. Nearly all healthpersonnel in the most affected districts (4 out of 13) have been moved to larger towns, a number of public and private hospitalsandi clinics have closed, and the provision of health services in these districts have been disrupted severely. Supply and logisticsupport to district hospitals and PHUs have been hampered. At the same time, the large scale movement of the population hascaused increased demand for health services in the remaining districts not affected by the conflict, particularly in Freetown andthe Westem Area.
Despite the ongoing strife, the DOH is conducting more district outreach activities than in 1992, even after the events ofJanuary, 1995. Partly because of the influx of refugees, and also because of the improved quality of care, utilization of healthseivices in Freetown and other urban areas appears to have increased in the last years. In the last month, some of the drugs andsupplies that were planned for peripheral distribution are being used to meet the emergency needs of refugees in Freetown. Asthe security situation improves, they will be distributed to peripheral clinics and hospitals as necessary.
The current uncertainty about the security situation has affected much of the physical planning for the health sector. There ismutch need for repair and retooling of clinics and hospitals throughout the country. However, these activities will now need tobelin in the Westem Area and the safe districts until security is completely restored in the outlying areas. Much of the ongoingand1 planned training activities in the health sector will be able to continue, though the development and upgrading of somesupport systems may well have to be delayed or phased in because of the uncertainty in the countryside. For example, thedevelopment of better cost-recovery systems for drugs will probably need to be delayed as Govermment is planning to subsidizedrugs for hospitalized refugees and displaced persons.
The management of the DOH has reacted flexibly and quickly to the current crisis. Even more remarkable is that while underthis increased strain, the DOH has mustered the energy and taken major steps to reform the health system. The security crisishaa put additional pressure on the Govemment's budget by reducing income and increasing military expenditures.Nevertheless, the DOH was able to maintain the support of central Govemment, and allocations for the health sector actuallyincreased for the FY1995/1996.
The uncertainty caused by the deteriorating security situation has increased the need for a comprehensive and flexible approach.The sector-wide approach and the implementation and monitoring modalities require that each year's financing is based onreview of past performance and a plan for the coming year approved by IDA. This will allow maximum flexibility forGcvernment and donors to begin the upgrading of the health system in the most safe areas, and to react quickly to any changesin he security situation. To restore the provision of quality health care in the district - as soon as the security situation allows -wil be a necessary precondition for the return of the rual population, and for the recovery of agricultural production, and thusimprovement of the prospects for a lasting peace in the country.
Poor quality of services
2.20 There are a number of immediate factors which contribute to poor quality of care, inaddition to the basic problems of under-funding of health services and poor management.Anong them, insufficient attention to in-service training and to supportive supervision ofhealth workers is a major factor, particularly for those in the outreach, such as MCH aides,community health officers, and other mid-level staff.
Poor management, with inadequate community involvement and accountability
2.21 This situation is partly a result of insufficient training, a lack of investment inmanagement systems such as management information, and an organizational structure that ishighly centralized and dominated by a power culture where decisions are not linked to thelevel of operations. This has led to a disconnection between peripheral and central levels ofhealth care delivery, inadequate planning, and an inability to regulate the defacto parallel

-11 -
private health care system. The lack of community involvement is partly due to insufficientattention to this matter by an administration currently confronted with war and low economicperformance, no clear accountability of health providers to the communities they serve,insufficient skills in community relations and development, and the absence of incentives forhealth workers to involve communities.
Insufricient financing and misallocation of scarce resources
2.22 There has been inadequate fumding for critical support programs such as maintenanceand essential drugs systems, resulting in physical decay of health facilities, shortages of drugs,and loss of confidence in public sector health services. The use of the scarce resources has beenbiased to urban, hospital based curative care, at the expense of more cost-effective primarycurative and preventive measures aimed at those most at risk. There was a heavy payroll with alarge proportion going to daily wage workers who contributed little to the sector, while mosthealth professionals are paid well below a living wage, forcing many to take on other jobs orcharge patients extra fees. To improve financial management, Government has introduced -beginning FY 94/95 - a program budgeting system to better match resources with stated priorityprograms and activities; and it is also in the process of establishing a comprehensive accountingsystem which would more closely monitor the appropriate allocation of financial resources.
III. THE HEALTH SECTOR DEVELOPMENT STRATEGY
A. THE GOVERNMENT REFORM PROGRAM
3.1 As part of its structural adjustment program, the Government of Sierra Leone isdemonstrating a greater commitment to reforming the health sector by increasing the share ofits resources allocated to health, though public expenditures on health are yet to reach the 1980levels. Following the change in Government in April 1992, the Government began a series ofpublic discussions on the problems of the health sector. This led to the development of aNational Health Policy in 1993, which outlined its main intentions for reform in terms ofimproving the health of its population through comprehensive and systemic reform. Again,using widespread consultation, a National Health Action Plan (NHAP) was developed in 1994to provide the framework for health sector reform, and outline its overall costs. Since then, theDOH has undertaken a series of steps to further advance their reforms, including a publicinformation campaign about the NHAP, an assessment of health services and priorities fromthe viewpoint of beneficiaries, a prioritization exercise to develop a core program of theNHAP, a reorganization of the DOH based on a institutional self-assessment, a comprehensivemanpower plan, and a financial management plan. The DOH is also developing proceduresfor district health planning, and has begun the formulation of operational plans by the newunits of the DOH and the districts. It has outlined its plan for infrastructure investment, and isfurther studying its financing options for the health sector.
3.2 In the National Health Policy, the Government declares its intention to seek economicgrowth and social justice by improving the quality and distribution of services, including

- 12 -
health care. The National Health Policy states that the focus of efforts in health care will be onthe development of preventive services, while strengthening the existing delivery system. Themain agenda for Government as described in the National Health Policy is that:
(a) a network of sound primary, secondary, and tertiary health facilities will bestrengthened through rehabilitation, appropriate staffing and logistical support;
(b) environmental health and communicable disease control will be promoted;(c) community participation and intersectoral cooperation will be fostered;(d) health care delivery will be decentralized to the district level;(e) Government financing of health care will increase;(f) certain services will be privatized, where appropriate; and(g) cooperation with international agencies and NGOs will be promoted.
3.3 The NHAP builds on the National Health Policy by providing a framework for healthsector actions, and proposes systematic improvement in the delivery of priority health servicesand the support services that maintain them. The NHAP was developed through a participativeworkshop involving a wide variety of stakeholders using an adaptation of the ZOPP(objectives oriented project planning) methodology developed by the German technicalassistance agency (GTZ). This resulted in an unconstrained "total" program costing aboutUS$270 million over five years, and an agreed set of criteria for prioritization: (a) need; (b)cost-effectiveness; (c) cultural acceptability; (d) operational feasibility; and (e) equitypromotion. A series of highly participative consultations were used to analyze the totalprogram according to these criteria (see para. 4.3, and Box 3). Given the anticipated limitationson financing, the central planning team applied the findings on priorities to the total program,to end up with a core program costing about US$138 million, comprising the most essentialelements of the sector plan which need to be financed before other elements of the program.The core program of the NHAP is intended to guide sector activities for the next five years andprovide a focal point for donor assistance. It is the basis for the sector investment credit.
3.4 The process of reform has done much to energize the Department of Health, districtstaff and the people associated with it. DOH staff have learned to work in teams to identifyand solve problems, and therefore communication and the effectiveness of the work of theDOH has improved. The reform process has brought Department staff much closer to theusers of the health system and to other providers. This is one of the main reasons why theDOH was selected Government's most productive Department (see Box 4).
B. RATIONALE FOR IDA INVOLVEMENT
3.5 There are compelling reasons for IDA to continue to support the Government'sreform initiatives in the health sector which started with assistance from a first project, i.e.,Health and Population Project, which will be closed at the end of 1995: (a) the Bank hasinvested heavily in sector work to promote health system reform (notably the above-mentioned, 1993 World Development Report and Better Health in Africa) to foster rationalpriority setting and selection of cost-effective interventions. The sector reform process in

- 13 -
Sierra Leone follows the same objectives and will benefit from IDA financial and technicalsupport; (b) the policy and type of program developed in Sierra Leone, and the agreement withdonors and NGOs makes possible a more comprehensive and integrated approach to which theBank is committed and which will ensure a sustainable development impact; (c) the healthsystem in Sierra Leone has deteriorated to such an extent that there is a large financial andtechnical gap between what is currently available (and provided by Govemment, donors andNGOs) and what is needed to begin making the health system work in Sierra Leone; (d) at thispoint in time, IDA is in a decisive position. Its contribution as a donor of last resort, fillingthe gap after other donors have adjusted their support to meet specific requirements andrestrictions, will enable the Government to address the basic health needs of a very poorpopulation, carry out a fundamental sector reform, and help the economic and societalrecovery.
Box 3 Stakeholders Set Priorities
At the first Bintumani conference in November, 1993, a large group of health professionals, officials and otherinterested parties was charged with outlining a National Health Action Plan, based on recently developedNational Health Policy. The result was an ideal health program estimated to cost over $270 million for the next5 years. The participants recognized that the draft NHAP was not a program that could be feasibly financed orimplemented at this time, so they worked out a set of criteria to choose priorities. The main criteria were: (a)need; (b) cost-effectiveness; (c) cultural acceptability; (d) operational feasibility; and (e) equity promotion. Anexternal consultant was hired to operationalize these criteria, to help the DOH choose among the nearly 60 mainactivities outlined in the draft National Health Action Plan.
A number of tools were used for priority setting, including structured interviews with officials in variousGovernment Departments and non-governmental organizations; a written survey for DOH staff from all levels;focus group meetings with opinion leaders from key groups, such as with women's organizations, healthproviders, and health care consumers; and town meetings with 150 male and female chiefs located throughoutthe country. At each stage, the results were discussed with the participants. A detailed beneficiary assessmentwas also conducted by Department staff and local consultants, to obtain in-depth feedback on priorities andconcerns about health care. A central team of DOH staff went through an exercise to use this information,along with data on cost-effectiveness of interventions from the World Development Report, to rank the priorityprograms and activities. These results were then systematically applied against the first draft of the NHAP todetermine the most essential services and activities.
The core program of the NHAP that resulted from this exercise cost around one half the original NHAP, andincluded activities for incremental financing. The most critical programs identified were in the areas ofprimary health care, particularly for maternal and child health, clean water and sanitation, and health education.Difficult decisions were also made to freeze public investment on tertiary care. Equally important is theconsultative processes that were established within Government, between Goverunent and the public, and withother health agencies. As a result, there is a great deal of public support for the health reforms, and a high levelof ownership and enthusiasm within Govermnent for the NHAP.
C. BANK ROLE IN THE HEALTH REFORM PROGRAM
3.6 In response to a Govemment request, the Bank has assisted the Government inpromoting the sector-wide investment approach among the donors and has been a key partnerin the Government's efforts to design its reform program. Through a Japanese PHRD Grant,IDA has helped Government with much of the technical preparatory work and consensus-

- 14 -
building for the NHAP and the development of the core program. IDA has supported theassessment and reorganization of the DOH and its training programs, and has providedtechnical assistance in design and facilitation of the planning, budgeting, and prioritizationprocesses. This has included a formal beneficiary assessment, the development of healthplanning tools, a human resources plan, and design of its technical and support programs,(such as nutrition, health information and education, essential drugs and contraceptives,laboratory services, maintenance and repair services), and support to strengthen sectorfinancial management. Last, but not least, IDA-together with the other donors and NGOs-participated actively in the social sectors consultations held in 1994 and 1995, and supportedDOH to become a true coordinator of the donor community in both health and educationsectors.
D. FUTURE DONOR SUPPORT FOR THE HEALTH REFORM PROGRAM
3.7 In 1993 Government launched its new policy for the sector and declared that its maingoals were improvement in social conditions and poverty alleviation, along with sustainedeconomic growth, which were reflected in its Public Investment Program (PIP). AConsultative Group (CG) meeting held in March, 1994, was carried out to serve as a vehicle tobring the needs of Sierra Leone before the donor community and encourage donor support tothe human resources sectors (Health, Education, and Poverty Alleviation). The CG wasfollowed by two Social Sectors Round Tables in May, 1994, and in October 1995, to mobilizeexternal assistance and coordinate donor interventions around the core program of the NHAP.The donor and NGO community responded with full endorsement of the NHAP and theintegrated sector approach, as described in the Communiques of the Round Table Meetings(Annex 6). Aside from IDA, donors made pledges for over US$55 million in support of thecore program of the NHAP, with additional support for technical assistance. The donorsoffering support include the Africa Development Bank, the European Union, the IslamicDevelopment Bank, the Saudi Fund for Development, UNDP, UNFPA, UNICEF, and WHO,with potential for additional donor assistance. As agreed at the Round Table Meetings, theGovernment would play the lead role in coordination, and would commit to regularly (i.)discuss with donors and NGOs sector plans and budgets, and (ii.) jointly review theirimplementation.
- 15 -
Box 4 Heroes Day Award to DOH
As part of the 1994 Sierra Leone Star Awards, the following citation was given to the Department of Health:
DEPARTMENTAL AWARD FOR HIGH PERFORMANCE IN THE CIVIL SERVICE
CITATION
I, Hilton Fyle, Convener and Coordinator of the 1994 Awards, declare that from votes sent in by the SierraLeone Public, the Departmental Award for High Performance in the Civil Service goes to the DEPARTMENTOF HEALTH, for the following reasons:
- The success of the National Cleaning Exercise- The efficient clearing of rubbish in the capital- The introduction of an Ambulance Service- The rehabilitation of Hospitals- The provision of affordable medicines for the poor- The launching of a New Blood Bank- And the pursuit of pioneering Health Policy and Action Plan
This is the people's choice. This is the people's voice.
IV. THE PROGRAM
A. PROGRAM SCOPE AND OBJECTIVES
4.1 The proposed IDA Credit would support the Government's NHAP core program, withthe intention of improving the health status of the people of Sierra Leone by increasing accessto and improving the quality of a basic package of health services that would be bettermanaged and delivered through an increasingly decentralized system. In the prioritizationexercise which led to the definition of the NHAP core program, the DOH identified thefollowing general development objectives: (i) improve key health status indicators; (ii)increase access to health care and family planning, particularly in the rural areas; (iii) improvethe quality of service through training, supervision and improved logistic support; (iv)strengthen management, accountability and community involvement at central and peripherallevels, and; (v) increase efficiency and improve the financing for health care. The NHAP coreprogram also identifies the following program priorities: (a) improve child health; (b) improvematernal health; (c) reduce fertility; (d) reduce the incidence and prevalence of communicablediseases and other common ailments, including HIV; (e) reduce mental illness; (f) reduceinjury and handicaps; (g) assure satisfactory nutritional status; (h) reduce drug abuse; (i)improve living conditions; and (j) improve food hygiene. Specific indicators to monitorprogress in the achievement of these objectives have been developed and will be used duringsupervision. Successfully laying the foundation for a sustainable, equitable and efficient healthsystem will also contribute to the attainment of more general societal goals, such as social

- 16-
sustainability of the adjustment program, improvement of prospects for a lasting peace in thecountry, and the strengthening of the human resource base needed for a sustainable economicdevelopment.
4.2 The credit is designed as an integrated sector investment operation, such as thetransport sector projects in Tanzania and Mozambique, and the credits approved to the healthsector of Bangladesh and, more recently, of Pakistan and Zambia. Government has taken thelead to design a common framework for action in the entire sector, under which IDA and otherdonors will provide support. The credit thus supports Government in its continualdevelopment of policy and on-going operations, even as reforms and rehabilitation proceed.The number of reforms needed are vast, and often there are no clear-cut answers to theproblems they seek to address. The changes will require considerable financial and technicalsupport for in-country testing and discussion, requiring maximum flexibility in the type ofsupport needed by Government. Accordingly, the specific items for financing will beidentified throughout implementation of the NHAP, based on regular review, re-planning andclient consultation.
4.3 Priorities. The prioritization of health needs and services has been a major part ofthe preparation process, leading to the definition of the core program from an initialdescription of a total or desired sector program. As discussed above, a comprehensiveapproach was used to develop priorities within Sierra Leone (see para. 3.3 and Box 3). Abroad consensus was reached on a number of key areas, which formed the basis for thedevelopment of the core program. As described in the NHAP, the programs of highest priorityare: (a) maternal and child health, including family planning; (b) communicable diseasecontrol; (c) sanitation and clean water; and (d) health education. The lack of awareness aboutthe emerging threat of HIV infection and the relatively low priority accorded to HIVprevention is a concern that will need to be addressed as a major challenge for the DOH andthe Disease Prevention and Control and Health Education units in particular. There are alsofour cross-cutting issues of the reform program that DOH has recognized as needing urgentattention: (a) expanding and strengthening peripheral health units; (b) confronting theproblems of high health service fees and drug pricing; (c) increasing community involvementin health service planning, execution and oversight; and (d) planning for decentralization.Although there are many concerns about the need to build a new tertiary care facility, adifficult decision was made to exclude it from the core program for the next three years.Annex 7 demonstrates how decisions were taken on the core program, and how it compares tothe initial total program, and the essential packages of care described in the Better Health inAfrica study, and the World Development Report 1993: Investing in Health.
B. PROGRAM DESCRIPTION
4.4 In the NHAP, the Government is proposing a major reform and restructuring of thehealth sector. In addition to radical organizational changes and substantial human resourcesdevelopment, the program proposes a substantial rehabilitation of health services, primarily inrural areas, by soliciting community involvement, repairing or constructing health facilities,training health personnel for clinical and managerial responsibilities, and investing in support

- 17-
services and systems that are needed to sustain operations. In summary, implementation of theNHAP is intended to:
(a) Increase access to health care by:
(i) rehabilitating existing health facilities to make them functional;(ii) creating new health posts and health centers;(iii) increasing access to health workers trained and equipped for midwifery
and family planning;(iv) enhancing the community health skills of health workers; and(v) implementing EEC strategies to increase demand for health and family
planning services and to improve healthy behaviors, including theprevention of HIV transmission.
(b) Improve the quality of health care by:
(i) training, retraining and supervising health workers;(ii) providing drugs, contraceptives, vaccines, materials and logistic support;(iii) rehabilitating existing clinics and hospitals; and(iv) making health services responsive to community needs.
(c) Strengthen the management of health care by:
(i) involving communities in health care management;(ii) developing management skills and establishing management systems;(iii) decentralizing the management of health service delivery to the district
level;(iv) reorganizing and strengthening the central Department of Health; and(v) defining and implementing a core set of technical programs and support
services.
(d) Improve the financing for health care by:
(i) increasing Government expenditures on health care;(ii) involving donors and non-governmental organizations; and(iii) attracting more household health expenditures to an improved public
sector health service.
Definition of NHAP technical programs and support services
4.5 The NHAP organizes the overall sector program into eight technical programs andsix support services. Technical programs are the elements of the system which directly deliverhealth services to the public. The technical programs include six Primary Health Care (PHC)services: (a) Maternal-Child Health, including Family Planning; (b) Treatment of CommonAilments; (c) Communicable Disease Control; (d) Sanitation and Water; (e) Nutrition; and (f)Information, Education and Communications; along with (g) Secondary Health Care; and (h)

- 18 -
Tertiary Health Care. Support services are those functions which are needed to support thetechnical programs, and include: (a) Drugs and Medical Supplies; (b) Laboratory Services; (c)Infrastructure, Equipment, Transport and Maintenance; (d) Human Resources; (e) Planningand Information Systems; and (f) Central Administration. Consideration is also given to legalaspects and private practice, though no funding has been allocated to them at this time. Adescription of the proposed activities under each of the technical programs and supportservices is outlined in Annex 8; a further description of the initial total program is provided inthe NHAP, while the core program is detailed in the Government paper: Better Health inSierra Leone: A Proposalfor Donor Funding (it has subsequently been revised to improveconsistency and to integrate a number of sub-services at the operational level).
4.6 The on-going programs are designed so that they will not be implemented as verticalprograms, but as part of a package of essential health services. The 13 districts will becomethe focus of operational planning and implementation. Following general guidance of thecentral DOH, the District Health Management Teams (DHMT) will be responsible forplanning and delivery of most elements of the six PHC services in their own district. Theoperational details of how the specific services will be provided in each area will be workedout m each district as part of their annual planning exercise, with the PHUs expected to delivermuch of the preventive and primary curative services. Each PHU will be linked to a districtlevel hospital which will provide first referral services. Larger hospitals will provide more ofthe same services as the district hospitals, and also function as referral points for morespecialized services (tertiary health care services). The larger hospitals will be under theadministration of newly created hospital management committees.
Health facilities rehabilitation and re-tooling
4.7 In the NHAP, the Government not only redefines the type of services that are to beprovided in Sierra Leone, but points out that a substantial increase in access to services isneeded if the health goals are to be met. This will entail a substantial investment inrehabilitation of PHUs and hospitals, and an expansion of new PHUs to under-serviced areas.In early 1994, a DOH survey found that there were 504 Government-run PHUs in the country.Most of them are ill equipped and in dire need of repair, and many are not operational due tothe poor state of the facility or because of civil conflict in the area. The DOH is currentlyrehabilitating 17 PHUs and 3 hospitals. It has prioritized another 44 PHUs and 10 hospitalsfor the next stage of repairs, and identified the next 7 of 57 locations in under-served areaswhere it intends to build new PHUs. The bidding documents have already been prepared forthe next 15 PHUs and 3 hospitals. Based on criteria of populations served by health facilities,it was estimated that the country will need about 600 PHUs by the end of the century (400health posts, each serving about 5,000 people, and 200 health centers, covering populations of10,000 to 20,000 inhabitants). The long range plans are to replace the health posts with healthcenters, but there are not sufficient physical or manpower resources at this time. The maincriteria for initial selection for rehabilitation or construction are the distance to anotherworking clinic (either public or private) and the size of the population served. Functionalwater and power supply are pre-requisites to any building repair or re-equipping. The selectedPHUs will need to be in locations where the civil situation is secure for rehabilitation to beconsidered. Because of the security situation, the specific sites and the volume of operations

- 19-
will be revised and adjusted with each annual plan, or more often if required. In the future, theDistrict Management Team's ability to plan and implement health plans will also beconsidered. The DOH also has specific plans for repairing and re-equipping the existingGovemment hospitals, so that they will be able to better serve as first referral facilities.Government spending on tertiary care services will be held constant in the next years of theNHAP, though hospitals may open private wings which may provide such services, to befinanced out of private sources. Part of the DOH plan to make the clinical and public healthlaboratory services functional includes reconstruction of laboratory space to consolidate thecentral laboratories, and rehabilitation of peripheral laboratories. As part of the preparation forthis work, and in order to take advantage of economies of scale, the DOH is standardizing thecivil works designs and equipment requirements for each level of facility. In addition todeveloping a database of major repair and equipment needs, the central DOH is spearheadingthe development of an asset registry for all new buildings and equipment, and of maintenanceschedules as part of an effort to upgrade its maintenance and repair unit.
Institutional development
4.8 In order to achieve the sectoral goals and implement the technical programs andsupport services, the DOH is currently being strengthened at both headquarters and districtlevels to manage a more effective health service for Sierra Leone. The focus of these changeswill be in four key interlocking areas:
(a) enhancing the authority of the DOH on key financial and personnel decisions inrelation to Central Government;
(b) strengthening the role of the DOH headquarters in policy and strategyformulation, planning, budgeting and health financing, and problem solving andsupport for district management teams;
(c) building the capacity of district management teams to plan, manage andsupervise health services delivered by hospitals and PHUs; and
(d) developing the skills and experience of personnel deployed in both healthservice delivery and support services.
4.9 DOH authority over finance and personnel. Decision-making in Government onpersonnel and financial matters is highly centralized, thereby affecting the health service byimpairing the quality of decisions and undermining the DOH's accountability for health sectorperformance. Accordingly, the GOSL has indicated that the DOH has obtained from theDepartment of Finance and the Establishment Secretary:
(a) authority to decide manpower and line item budgets, in relation to the coreprogram, and within an overall departmental and program ceilings agreed with theDepartment of Finance;

- 20 -
(b) real influence over the recruitment and selection process, and the application ofemployment practices for staff promotions, discipline and transfers; and
(c) authority to determine the numbers, categories, and skill mix of staff required inline with an overall departmental manpower plan, as well as some discretion overindividual's pay within established salary structures.
4.10 Steps to delegate authority to the DOH will be carefully coordinated with parallelmeasures to introduce improved central accounting and budgeting systems, rationalizedmanpower levels and revised salary scales. Both financial and personnel management withinthe DOH will be strengthened in terms of upgraded skills and improved systems to enabledelegated authority to be fully effective.
4.11 Strengthened DOH headquarters. Currently the DOH headquarters plays an activerole both in authorizing expenditure and the management of health programs, throughmonitoring and direct supervision. The DOH intends to "decentralize" the health systemwhich will shift health program management (and expenditure authorization) to the districtlevel. Accordingly, the role of headquarters will be strengthened to concentrate on:
(a) policy and strategy formulation, planning, budgeting, evaluation and theestablishment of norms, and developing alternative strategies and mechanisms forfinancing health care;
(b) providing technical assistance in the form of support and problem solving fordistrict management teams, rather than direct program management, and by means ofmonitoring and direct supervision;
(c) the analysis and processing of management information for use by head officeand district managers; and
(d) the provision of central services, such as laboratory and pharmaceutical servicesand management support services.
4.12 The DOH has begun to implement its institutional reform plans to enable it toeffectively fulfill its new role. This will necessitate:
(a) complete transition to its recently revised organization structure which is moreservice-oriented and matches NHAP objectives. As a condition for effectiveness, theDOH would staff the following key positions: Director of Management Support,Director of Financial Resources, Chief Procurement Officer, and a supporting positionat the Donor Relations Office to monitor and coordinate donor programs and budgets(para. 7.3(h));

- 21 -
(b) the adaptation of the organization culture to one which is more decentralizedand formalized to enable "decentralization" to be effective;
(c) the development of management control strategies and systems moreappropriate for a "decentralized" health service;
(d) building systems and developing professional competence in personnel andfinancial management, procurement and management information; and
(e) improvements in personnel and reward systems, and in training.
4.13 District management. District Health Management Teams will gradually be givengreater authority over operational, financial and personnel decisions, and responsibility toprepare district health plans. Guidelines for developing district health plans are beingdeveloped and field tested in a number of districts. These plans are to play an increasinglyprominent role in the determination of DOH activities and budgets. Since few people at thedistrict level have experience in planning and management, technical assistance and training isplanned in the areas of health planning, as well as in community health care, team building,financial management and accounting, so that the district teams will be able to plan,implement, and monitor health care, family planning and nutrition activities in their districts.As a condition for negotiations, guidelines for district health planning to make DistrictHealth Management Teams functional, and indicating decentralization of decision-making inthe sector were submitted to IDA. At negotiations, assurances were provided that the GOSLwill give budgetary authority to implement a prepared district health plan to at least oneadditional district in each year of the operation (para. 7. I(a)). Community representation andaccountability is expected to play a prominent role in these plans. The pace of decentralizationwill be quite cautious, and will depend on the security situation in the country and on theprogress made in the first districts with decentralized authority.
4.14 Strengthening district management will involve the following changes in bothorganization structure and culture in line with the spirit of "decentralization."
(a) The Provincial level of management will be removed, thereby providing thedistricts with direct reporting to headquarters.
(b) The DHMT will exercise managerial authority over the PHUs, namely thehealth centers and health posts. Members of this team would also provide technicalsupervision over the activities of the health centers, and the health posts would bedirectly supervised from the health centers.
(c) District health planning will be conducted and mechanisms established forinvolving communities in the planning process. District Development Committees andHealth Committees will be set up to enable key stakeholders to influence and reviewthese plans.

- 22 -
(d) The DHMT will coordinate the activities of NGOs and the private sector inorder to improve the coverage of health services.
4.15 Human resource development. Significant changes are proposed in nearly allfacets of manpower development. Enhancing institutional capacity will involve considerabletraining and management development across the DOH. This will involve managerial,professional and technical personnel drawn from support service as well as health servicefunctions. The DOH manpower plan was developed on the basis of a reappraisal of the type ofhealth personnel needed at each level of the system, compared with its existing resources basedon a 1994 census of health personnel (though three of the districts were not included due to theongoing conflict). Analysis of the personnel census revealed that there are nearly 2,000workers being paid by the Establishments Department who were no longer working in theDOH. As a condition for Board presentation, the Government submitted to IDA a detailedplan and timetable for reconciling the DOH payroll and the actual DOH staff census (para.7.2(a)). The priority areas of training are shown below in Table 4.1, whereas Annex 9summarizes the proposed training plan for the sector. One of the most significant changes isthat the wide variety of PHC staff and training programs will be simplified, phasing out single-purpose workers and developing a cadre of PHC workers with polyvalent skills and greaterability to deal with communities. Large gaps in job categories (especially for hospital nurses,community health assistants, and community health aides) would mostly be met byredeployment and retraining of existing workers, and substantial training of new recruits.Existing training institutions, namely the School of Hygiene and the Paramedical School,would be merged and strengthened in terms of improved and revised curricula, and upgradedskills in training design and delivery. It is still likely that shortages of skilled personnel willexist five years from now, although guidelines have been drafted to improve the utilization ofthe manpower to achieve the most efficient and equitable service coverage. A managementtraining program is a major component of the manpower plan, and is designed for developingnew skills and practices of senior managers, middle managers, and a critical mass from eachDHMT. Most of the training will be conducted in Sierra Leone (using local institutions wherepossible), although it will also include other countries in the region and outside the continent,where appropriate. The substantial investments in training (estimated at US$5.2 million) willbe closely coordinated with actions taken to improve the working environment, pay andincentives, and performance appraisal systems.
The first year program
4.16 The first year of the prograrn has been designed to set the foundation for the NHAPimplementation while addressing the current security situation. Detailed activities and budgetsfor the first 12 months were prepared by the DOH staff for the entire program, and areincluded in the DOH Operational Manual. Since many of the districts are currentlyinaccessible, more central level activities are programmed for the first year. The emphasis onimproving the ongoing service delivery will focus on the Western Area and the towns wherethe populations have concentrated. It is estimated that 1.5 million people are now living inWestern area. Physical project supervision in these areas is currently going on, and should bepossible during the coming years. Maternal and child health services, including familyplanning, obstetrics, and well-child care, along with communicable disease control, water and

- 23 -
sanitation services, and nutrition take the majority of inputs for service delivery. Emergencyassistance for refugees is being handled separately from routine DOH activities, under anumbrella organization in the Government. Implementation of the institutional changes in theDOH is another highlight of the first year's plan. Staff have been reassigned to the new unitsof the Department, but further work and support is planned for 1996 to get them fullyfunctional. The key areas include Management, Financial Management, Procurement, andMaintenance and Repair. Human resources development will comprise a major part of the firstyear: curricula at the training institutions will be revised, and the first year of the new cadres ofperipheral health staff is expected this year, while personnel systems will be set up. Revisingthe health information system is also planned during the first year. Decentralization will beimplemented slowly during this year. The Western Area District Health Management Teamhas developed its district plan, and will be given authority to implement the plan, includingbudgetary allocations for non-wage recurrent expenditures. Physical rehabilitation willconcentrate in the Western Area. Three hospitals, 17 PHUs, a maintenance facility, and a drugwarehouse, all in the Western Area, are scheduled for rehabilitation in 1996. A healthfacilities infrastructure and equipment survey will be extended in a phased manner to cover theremainder of the country, and it will form the basis for specific rehabilitation plans in thesubsequent years. Essential drugs, contraceptives, vaccines and laboratory reagents for PHUsand hospitals will also be purchased and distributed.
Table 4.1 Traidng Priorities for the Sierra Leone Department of HealthFunction Sldfls needed
PHUs Community health, nursing, midwifery, family planning, healtheducation and communications, nutrition, counseling for sexuallytransmitted diseases (particularly H1V)
Medical service management Management, team building, training design and delivery
Accounts and internal au&t Financial management and audit
Personnel Personnel management
Planning and management information Management information
Purchasing and stores Procurement management
District hospitals Internal medicine, surgery, obstetrics and gynecology,pediatrics, hospital administration
DOH and district management Public health, epidemiology, health services administration,planning budgeting, human resources management, maintenance

- 24 -
C. PROGRAM COSTS AND FINANCING
4.17 Health sector budget. The Government funding for the health sector is, at present,limited mainly by the economy's capacity to generate income, and the Government's ability tocollect taxes. Therefore, only a conservative projection-to be reviewed annually-of healthsector budget increases has been made. This is based on the assumption-in line with theongoing structural adjustment program-that total Government expenditures remain limited toabout 20 percent of GDP and that the share of allocation to the health sector steadily increasesfrom about five percent in 1995 to about seven percent of total Government budget in 2000(see Annex 10). The most critical part of most Government financing is the non-salaryrecurrent component of the budget. In Sierra Leone the share of the non-salary recurrentbudget in the total recurrent health budget is exceptionally high (about 70%) but expected tofall somewhat in the future as critical health personnel will be recruited and salaries might beadjusted in the context of a Civil Service Reform. However, Government ought to endeavor tomaintain the share of its non-salary expenditures in the sector at low levels, should anyimprovements in health services be achieved in the following years.
4.18 Costs. The total cost for the core program for fiscal year 1996-2000 is aboutUS$138 million, or about US$5.5 per capita per annum, with the breakdown shown in detail inAnnex 10 (see also para. 3.3). Technical programs would receive 55 percent of the totalprogram funds, of which primary health care would receive about 60 percent, and secondaryand tertiary care about 40 percent. The support services, which cut across the technicalprograms, would receive about 45 percent of the total funds, including the rehabilitation ofhealth facilities (17% of total funds).
4.19 Detailed costs are determined on an annual basis in the NHAP, to coordinateGovernment and donor budget preparation. The total cost for the first year of the program isUS$25.6 million equivalent, with foreign exchange costs estimated at US$11 million, or 43percent of the total costs. Table 4.2 summarizes the costs of the first year of the program,according to component, and Table 4.3 summarizes the costs according to expenditurecategory.
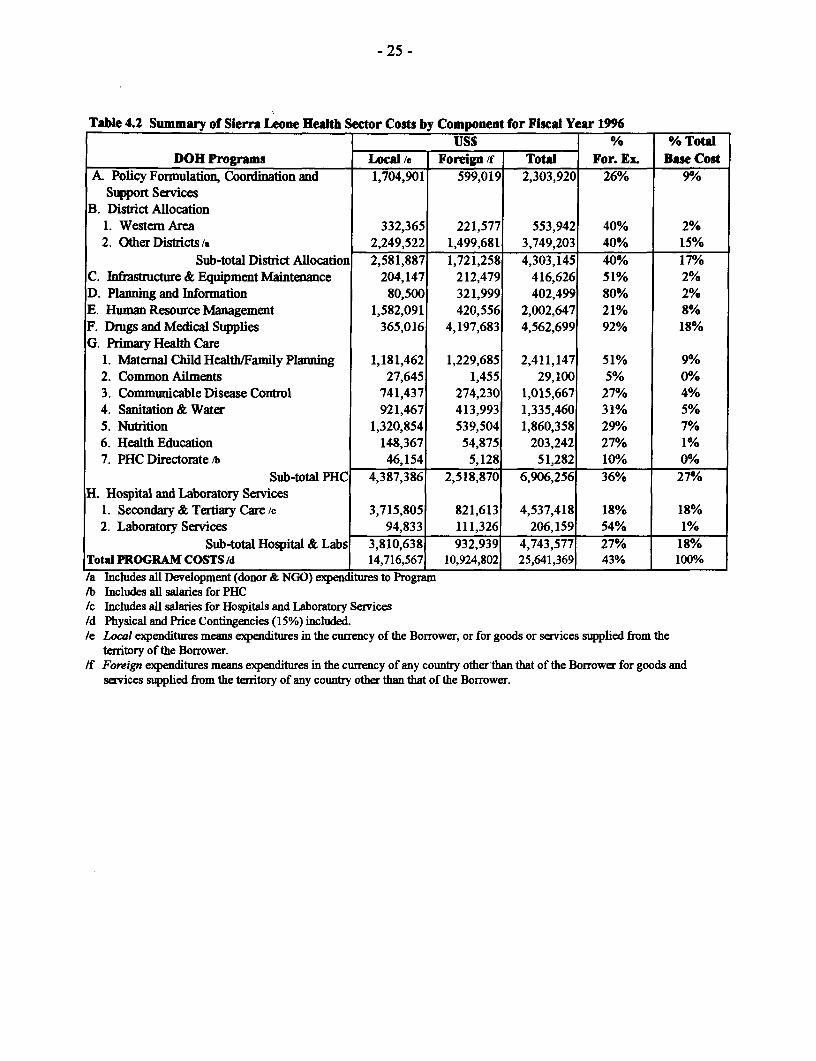
- 25 -
Table 4.2 Summary of Sierra Leone Health Sector Costs by Component for Fiscal Year 1996USS __ _ % Total
DOH Programs Local /e Foreign /f Total For. ExL Base CostA. Policy Formulation, Coordination and 1,704,901 599,019 2,303,920 26% 90/o
Support ServicesB. District Allocation
1. Westem Area 332,365 221,577 553,942 40% 2%2. Other Districts /a 2,249,522 1,499,681 3,749,203 40% 15%
Sub-total District Allocation 2,581,887 1,721,258 4,303,145 40% 17%C. Infiastructure & Equipment Maintenance 204,147 212,479 416,626 51% 2%D. Planning and Information 80,500 321,999 402,499 80% 2%E. Human Resource Management 1,582,091 420,556 2,002,647 21% 8%F. Drugs and Medical Supplies 365,016 4,197,683 4,562,699 92% 18%G. Primary Health Care
1. Maternal Child Health/Family Planning 1,181,462 1,229,685 2,411,147 51% 9%2. Common Ailments 27,645 1,455 29,100 5% 0%3. Communicable Disease Control 741,437 274,230 1,015,667 27% 4%4. Sanitation & Water 921,467 413,993 1,335,460 31% 5%5. Nutrition 1,320,854 539,504 1,860,358 29% 7%6. Health Education 148,367 54,875 203,242 27% 1%7. PHC Directorate /b 46,154 5,128 51,282 10% 00/0
Sub-total PHC 4,387,386 2,518,870 6,906,256 36% 27%H. Hospital and Laboratory Services
1. Secondary & Tertiary Care /c 3,715,805 821,613 4,537,418 18% 18%2. Laboratory Services 94,833 111,326 206,159 54% 1%
Sub-total Hospital & Labs 3,810,638 932,939 4,743,577 27% 18%Total PROGRAM COSTS /d 14,716,567 10,924,802 25,641,369 43% 100%/a Includes all Development (donor & NGO) expenditures to Program/b Includes all salaries for PHC/c Includes all salaries for Hospitals and Laboratory Services/d Physical and Price Contingencies (15%) included./e Local expenditures means expenditures in the currency of the Borrower, or for goods or services supplied from the
tenitory of the Borrower./f Foreign expenditures means expenditures in the cunrency of any country other than that of the Borrower for goods and
services supplied from the territory of any country other than that of the Borrower.

- 26 -
Table 4.3 Summary of NHIAP Core Program Costs by Expenditure Category for Fiscal Year 1996US S % % Total
Descripton of Expenditure Local /c Foreign /d Total For. Ex Base CostL INVESTMENTA. Civil Works 1,147,230 1,720,845 2,868,075 60% 11%B. Goods and Equipment
1. Medical equipment 749,643 749,643 100% 3%2. Lab Equipment (District Hospitals) 869,688 869,688 1000/% 3%3. Furniture 255,756 383,633 639,389 600/o 2%4. Vehicles 1,599,765 1,599,765 100% 6%
Sub-total Goods and Equipment 255,756 3,602,729 3,858,485 93% 15%C. Materials 1,222,649 1,222,649 1000/a 5%D. Drugs, Contraceptives, Vaccines & 3,042,120 3,042,120 1000/% 12%
Supplies /aE. Services
1. Technical Assistance 1,139,329 1,139,329 100% 4%2. Training/Workshops 2,207,728 2,207,728 0% 90/0
Sub-total Services 2,207,728 1,139,329 3,347,057 34% 13%IL RECURRENT
A. Personnel Recurrent Expenditures1. Salaries 1,171,896 1,171,896 0% 5%2. Allowances 549,603 549,603 0% 2%3. Wages 608,041 608,041 0% 2%
Sub-total Personnel Recurrent Expenditures 2,329,540 0 2,329,540 0% 90/0B. Other Recurrent Expenditures
1. Traveling Oocal) 153,937 153,937 0% 0%2. Traveling (overseas) 156,783 156,783 100% 0%3. Office and generd 83,000 83,000 0% 0%4. Recruitment and training expenses 726,956 726,956 0% 3%5. Professional fees, honoraria, other 116,846 116,846 00/a 0%
allowances6. Transport, fuel and oil 190,488 190,488 00/a 0%7. Electricity and water charges 156,339 156,339 0% 0%8. Telephone and other communication 217,986 217,986 0% 0%9. Printing, publicity and advertising 56,447 56,447 0% 0%10. Stores and other supplies 1,257,771 1,257,771 0% 5%11. Freight and port charges 189,474 189,474 0% 0%12. Repairs & Maintenance 176,541 176,541 0% 0%13. Public relations expenses 6,947 6,947 0% 0%14. Miscellaneous /b 3,239,088 3,239,088 0% 13%15. Subscriptions and membership dues 632,368 632,368 0% 2%16. Donations, grants and other 981,063 981,063 0% 4%
contributions17. Diets 270,009 40,346 310,356 13% 1%18. Uniforms 39,474 39,474 0% 0%19. National oncho development program 28,947 28,947 0% 0%20. Medical expenses 252,632 252,632 0% 0%
Sub-total Other Recurrent 8,776,313 197,129 8,973,443 2% 35%Total Recurrent 11,105,853 197,129 11,302,983 2% 44%
Total 14,716,567 10,924,802 25,641,369 43% 100%/a Including freight and port charges/b Includes all operating costs inputs from donors and NGOs active in health sector/c Local expenditures means expenditures in the currency of the Borrower, or for goods or services supplied from the
territory of the Borrower./d Foreign expenditures means expenditures in the currency of any country other than that of the Borrower for goods and
services supplied from the territory of any country other than that of the Borrower.

- 27 -
4.20 Financing. It is expected that Government will contribute about US$63 million (46%)to the core program over the next five years. The IDA credit is estimated to be about US$20million, covering about 14 percent of the program costs. It is also expected that the remainder,US$55 million, will be made up through donor contributions, an amount well within the statedintentions of donors attending the Social Sectors Round Tables. Table 4.4 provides asummary of donor commitment to the NHAP (FY96 - FY00) based on pledges made at theSecond Social Sectors Donor's Meeting and subsequent discussions held with GOSL anddevelopment partners. Table 4.5 shows the donor financing to various progran areas. TheIDA credit would represent initial support for IDA's long term commitment to rehabilitation ofthe sector. The credit would fund a "time slice" of sub-sectors of the health budget-bothoperational and developmental-to support the core program, and would be eligible for anyforeign exchange or local costs net of duties and taxes, with the exception of the followingitems: land acquisition; donations; salaries of non-imcremental personnel; subscriptions andmembership fees; and overseas medical expenses.
Table 4.4 Financing Plan (US$ million) FY96 - FY00
Financier Local Foreign TotalGOSL 63.2 0.0 63.2
AfDB 3.0 12.0 15.0EU 0.0 4.0 4.0Saudi Fund forDevelopment 5.0 11.0 16.0UNDP 0.6 1.4 2.0UNICEF 1.3 3.6 4.9UNFPA 1.2 2.8 4.0WHO 1.0 3.0 4.0NGOs and Others 1.5 3.0 5.0
IDA 4.0 16.0 20.0
Total 81.1 57.0 138.1"I Estimated, final arnount may vary depending on annual negotiations with donors.

- 28 -
Table 4.5 Areas of Financial Support to the NHAP According to Agency InvolvedCentral District Support Planning Human Drugs & Primazy Hospital SalariesAdmnin. Allocation Services & Info. Resource Medical Health & Lab &
Mgmt. Supplies Care WagesMudilaterals:African Development X X X X X XBankEuropean Union X XIDA X X X X X X X XIslamic Development X XBankUNDP XUNFPA X XUNICEF X X XWFP x xWHO X X X X X X XBflbterab:ODA(UK) X XSnudi Fund for X X XDevelopmentU.S.A. X XNon-Govermmental Organizations:Action Aid X XAfricare X XAhmaddiya Mission X XAICF X XBaptist Convention XCare XCause Canada X XChristian Health X XAssociation of SierraLeoneCatbolic Relief Service XGerman TB/Leprosy X X XMarie Stopes X XPlan Internat'l XRotasy Internat'l xSierra Leone Family XPlanning AssociationSierra Leone Red Cross X XHousehold X X XContribuotbnGOSL X X X X X X X X X
4.21 A detailed determination of all investment items for the program would be done foreach year through the annual planning processes. A traditional investment would not besupportive of the Sierra Leone program, particularly as it hopes to decentralize responsibilityto district teams and hospitals, and to institutionalize the annual planning and budgetingprocess. IDA's role will be to help ensure that all agreed and vital elements of the annual plansare funded. Therefore, financing through the credit would be phased to coincide with theannual budgets and workplans of the DOH, as agreed with IDA and other donors. Fundingwill be dependent on coordinated planning processes with Government, local stakeholders, andother donors, to ensure an appropriate sequence and pace of action, and to avoid thecontinuation of small, disparate, donor-driven projects. External financing would be madeavailable as progress is made on the specific annual workplans of the sector. As shown inTable 4.6, Government input is expected to increase over the program period while donorcontributions are declining as a proportion of total expenditures.
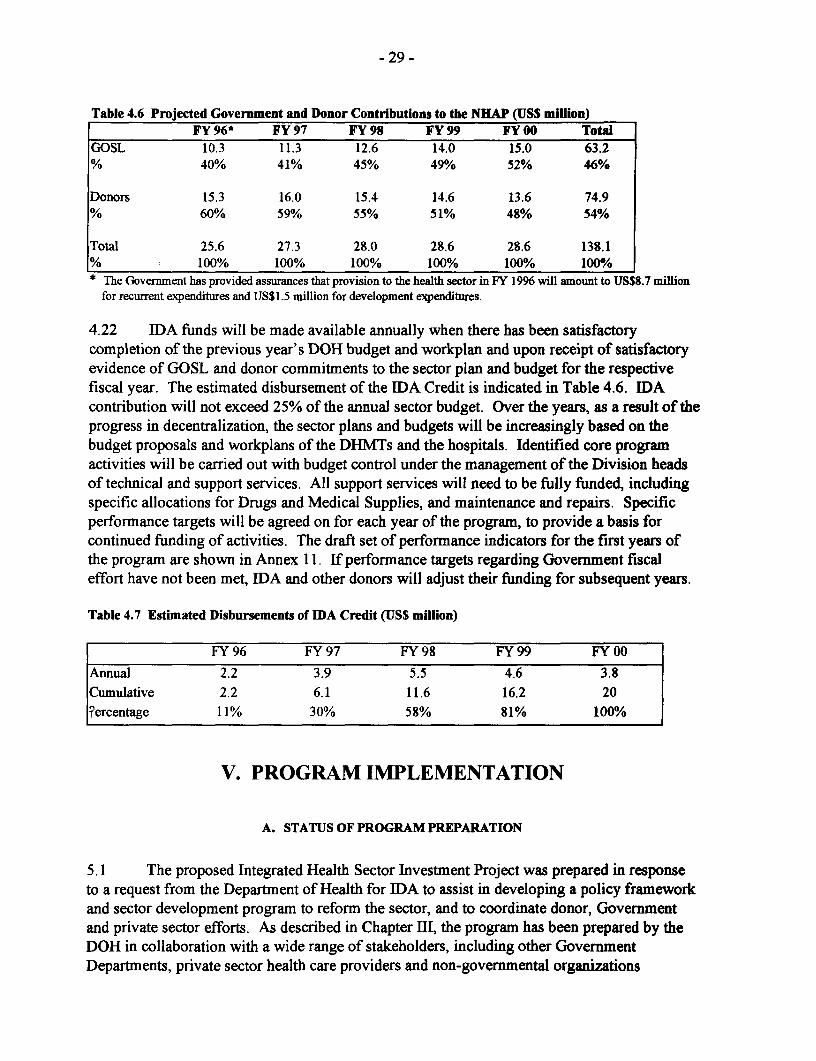
- 29 -
Table 4.6 Projected Government and Donor Contributions to the NHAP (USS million)FY 96* FY 97 FY 98 FY 99 FY 00 Total
GOSL 10.3 11.3 12.6 14.0 15.0 63.2% 40% 41% 45% 49% 52% 46%
Donors 15.3 16.0 15.4 14.6 13.6 74.9% 60% 59% 55% 51% 48% 54%
Total 25.6 27.3 28.0 28.6 28.6 138.1-% l 100% 100% 100% 100% 100% 100%* The Govermment has provided assurances that provision to the health sector in FY 1996 will amount to USS8.7 million
for recurrent expenditures and USS1.5 million for development expenditures.
4.22 IDA funds will be made available annually when there has been satisfactorycompletion of the previous year's DOH budget and workplan and upon receipt of satisfactoryevidence of GOSL and donor commitments to the sector plan and budget for the respectivefiscal year. The estimated disbursement of the IDA Credit is indicated in Table 4.6. IDAcontribution will not exceed 25% of the annual sector budget. Over the years, as a result of theprogress in decentralization, the sector plans and budgets will be increasingly based on thebudget proposals and workplans of the DHMTs and the hospitals. Identified core programactivities will be carried out with budget control under the management of the Division headsof technical and support services. All support services will need to be fully funded, includingspecific allocations for Drugs and Medical Supplies, and maintenance and repairs. Specificperformance targets will be agreed on for each year of the program, to provide a basis forcontinued funding of activities. The draft set of performance indicators for the first years ofthe program are shown in Annex 11. If performance targets regarding Government fiscaleffort have not been met, IDA and other donors will adjust their funding for subsequent years.
Table 4.7 Estimated Disbursements of IDA Credit (US$ million)
FY 96 FY 97 FY 98 FY 99 FY 00
Annual 2.2 3.9 5.5 4.6 3.8
Cumulative 2.2 6.1 11.6 16.2 20
Fercentage 11% 30% 58% 81% 100%
V. PROGRAM IMPLEMENTATION
A. STATUS OF PROGRAM PREPARATION
5.1 The proposed Integrated Health Sector Investment Project was prepared in responseto a request from the Department of Health for IDA to assist in developing a policy frameworkand sector development program to reform the sector, and to coordinate donor, Governmentand private sector efforts. As described in Chapter III, the program has been prepared by theDOH in collaboration with a wide range of stakeholders, including other GovernmentDepartments, private sector health care providers and non-governmental organizations
- 30 -
(NGOs), community representatives, and multilateral agencies, including among others, WHO,UNICEF, UNDP, UNFPA, and IDA.
5.2 The Government's reform program is an ongoing effort that needs to occur at thesame time that it is attempting to restore basic services. Some of the critical areas underpreparation include: (a) institutional arrangements to implement the program; (b) the programcontent itself, and (c) costs and financing.
(a) Institutional arrangements and capacity. An institutional assessment of theDOH and an analysis of job tasks have been done, resulting in reformed organizationalstructure of the central DOH, and a decision to successively decentralize authority forimplementation of health care delivery to districts and hospitals. It has already beendecided that the program will operate through the permanent DOH structure, and thatthere will be no separate project implementation units for individual donor programs.Departmental Units have been established, and staff assigned to the new units.Program coordination and donor liaison functions have been incorporated into the neworganizational structure of the DOH. As a condition for negotiations, the DOHsubmitted to IDA the detailed description of the finalized re-organization of the DOH,including terms of reference for key offices for NHAP implementation, including theDOH Management Team, the Management Support Office, and a FinancialManagement Team. Submission to IDA of a draft Operational Manual, detailing theroles, responsibilities, and implementation procedures under the program for theDepartment of Health was a condition for negotiations. To strengthen the DOH sothat it will be able to perform its new roles, considerable training and technicalassistance will be needed, particularly in the areas of financial management,procurement and general management. Plans to set up the systems are currently beingdeveloped. As a condition of effectiveness, technical assistance agreements with afinancial management consultant firm and a procurement technical assistance agencyfor at least 12 months each, for support services to be provided during the first twoyears of the project, and an agency to conduct the in-house management training (theSierra Leone Institute for Public Administration and Management) would be signedunder terms and conditions satisfactory to IDA (para. 7.2 (a & b)).
(b) The program. After the planning workshops and extensive priority-settingexercises, the NHAP core program clearly identifies priorities of sector programs andactivities. Submission to IDA of a draft Letter of Health Sector Development Policy,outlining the specific policy commitments of Government to the NHAP, the prioritiesfor Government, private and donor funding, and indicating that the DOH is givenauthority to decide manpower and line item budgets within the program resourceceilings agreed with the DOF, and the authority over staff numbers, selection,promotions, discipline and pay within the established salary structure was a conditionfor negotiations (also outlined in para. 4.9). Submission of a draft Letter of HealthSector Development Policy, satisfactory to IDA, was a condition for negotiations, andwas signed as a condition of Board presentation (para. 7.2(b)). Work in the followingareas needs has been submitted to IDA as a condition for negotiations: (i) the finaldetailed first year implementation plan and budget for the program; (ii) a finalized

- 31 -
human resources plan showing commitment to rationalizing health personnel anddecentralizing service delivery; and (iii) completion of the formal beneficiaryassessment. As a condition for effectiveness, the Government would submit to IDA (i)the training plan and (ii) the plan for recruitment and redeployment of staff for thosehealth facilities of the Western Region where rehabilitation and construction works isto take place during the first year of the project (para 7.3(c)).
(c) Costs and financing. At the Social Sectors Round Table meetings in May1994, Government reconfirmed its commitment to increase allocation to the healthsector during the program period in line with the SAP. Other donors pledged aboutUS$55 million to the NHAP, but actual commitments need to be reconfirmed regularly.At the Donors Conference, in October 1995, donors and NGOs pledges to the sector forFY 1996 were over US$12 million. Government is confident to obtain additionalfunding in the amount of US$3.3 million from donors not represented at theConference, thereby closing the financing gap for FY 1996. Because little is knownabout how much the private sector and households contribute to the sector, a study isbeing conducted to describe the financing options and mechanisms to optimize thepublic/private mix of financing and service provision.
B. PROGRAM IMLEMENTATION (MANAGEMENT AND COORDINATION)
5.3 The DOH, through its staff working within its permanent organization structure(shown in Annex 12), will be responsible for implementation of the NHAP. The variousmultilateral and bilateral donors have agreed to adopt this consistent and common managementand implementation approach for all financing agencies and for all components under theprogram. A new organization structure has been adapted by the DOH to facilitate this, andmanagement systems of the DOH are being established, particularly in accounting andbudgeting arrangements, and district planning.
5.4 At the head of the new DOH is a DOH Management Team, comprised of theDirectors General, key heads of units of the DOH, and led by the Secretary of State.Responsible managers within the strengthened structure, at both headquarters and districtlevels, will be given the authority and resources to implement specific interventions andservices in the NHAP. Coordination of those interventions and services will be achievedlargely through the newly adopted organization structure and any special coordinatingmechanisms such as improved annual planning procedures, identified as part of theinstitutional development component of the program.
5.5 As the implementation of the program will require new relationships to be built withdonors, a clear focal point is needed in the organization structure of the DOH to manage theserelations effectively. This will become one of the functions of the Donor Relations Office,which reports to the DOH Management Team. The Director of Donor Relations is responsiblefor managing and coordinating external relations. More importantly he/she will also beresponsible for monitoring donor programs and inputs to the sector; hence the need tostrengthen this office.

- 32 -
5.6 A Management Support Office, led by a technical officer providing support to theDOH Management Team, will also be recruited to oversee the coordination of work of DOHstaff on the physical and technical program implementation activities as well as the monitoringand reporting element of implementation. He/she will also provide and obtain information andsupport to and from those managers responsible for implementation of the DOH program.
5.7 Management support services will be largely the responsibility the FinancialManagemtent Unit (i.e., accounting and disbursement), the Procurement Unit, and the FacilitiesManagement Unit (i.e., maintenance and repairs). These divisions will be strengthened byupgrading the number of staff and their skills and by introducing improved systems whichwould meet the different procurement and accounting requirements of both the Governmentand individual donors. In addition, as an aid to more decentralized financial management, asystem of district level warrants will be introduced. The Planning, Monitoring, Informationand Statistics Unit (PMISU) will play a key role in the design and implementation of healthand management information, and in providing support to district planning, monitoring andevaluation.
5.8 While the District Medical Officers would be responsible for program execution forthose areas within their jurisdiction, communities would be involved in both the planning andmanagement of health services and their periodic review. It is anticipated that sucharrangements will strengthen accountability and improve the quality of services. Conditions ofeffectiveness have been designed to strengthen the DOH's implementation capacity inpreparation of Program implementation (para. 7.3). A summary of the implementationprogram is shown in Annex 13, with a outline of an Operational Manual shown in Annex 14.The Operational Manual would be finalized as a condition for effectiveness (para. 7.3(d)).
C. PROGRAM SUSTAINABILITY AND RECURRENT COST IMPLICATIONS
5.9 In response to the current state of collapse and fragmentation in the health caresystem, sustainability is an integral part of the sector goals. The reform program seeks toachieve social sustainability by soliciting community support in the preparation of theprogram, and by ensuring an important role for the community in the operation andmaintenance of health services, so that the health system becomes more accountable to thecommunities that they serve. The program currently enjoys considerable political support, asevidenced by the involvement of the President and cabinet in the launching of the NationalHealth Policy and NHAP, and by the eagerness to make major policy decisions. Efforts willbe made to maintain the political support through continued involvement of key decision-makers in the planning and evaluation of health services. A major challenge of the program isto develop managerial and technical capacity to ensure sustainability of the health caredelivery. This is why the program intends to put heavy investments in training (both formaland on-the-job), technical assistance, and the establishment of management systems to developthe necessary cadre of appropriately trained people to meet local needs and to plan for servicesthat respond to these needs. To build up local capacity, local technical assistance and trainingwill be used as much as possible, and the modalities for long term technical assistance, where

- 33 -
required, will be designed to maximize local capacity and control. For example, long termassistance may be done through twinning arrangements with external public health andmedical organizations, and use and development of local consultancy capacity.
5.10 Financial sustainability. The program aims to be financially sustainable in the longrun, but will be dependent on considerable donor investment in the short and medium term.Government health expenditures are expected to increase from US$10.3 million in FY 1996 toUS$15.0 million in FY 2000 over the next five years. Government financing will cover anincreasing proportion of the core program (40% in 1996 to 52% in 1999). The increases arebased on commitments to increasing Government allocations to health, and on projections foreconomic growth. On a per capita basis, the total program expects to spend about US$5.5 percapita per annum at the end of the program, double the current public and donor expenditures.According to Better Health In AJrica, a well-run system would cost, in low revenue countries,around US$9 per capita (1993). Thus, it is likely that continued increase in health financingwill be needed in Sierra Leone, and that additional financing will be needed from privatesector sources and households. Increased household expenditures on more effective public andprivate services is anticipated as the quality of these services improve. As mentioned, theprogram foresees external financing by donors on a declining basis.
D. PROGRAM MONITORING AND REPORTING
5.11 Program monitoring, that is measuring, evaluating and reporting progress, would bethe responsibility of the DOH and those line managers responsible for specific interventionsand services. The Management Support Office will coordinate this effort in the central DOH,and will bring together all parties involved so that key issues are dealt with through discussionsamong those concerned. The line managers would be, in turn, responsible for taking anynecessary corrective action, as indicated by the monitoring information. The PMISU willundertake to coordinate program monitoring and reporting on health services performancefrom the districts. In order to do this, the DOH will establish its own approach, acceptable tothe Bank and other donors, for developing annual workplans and reviewing progress on aperiodic basis. The annual workplans, to be agreed on by all donors, would form the basis forreviewing progress on a regular basis. At negotiations, assurances were provided thatGovernment will submit a three-year rolling plan, an annual progress report, and a draftdetailed implementation plan and budget at least three months prior to the beginning of eachfiscal year, and prior to an annual Government-led meeting with donors where progress on theprevious year's health program would be reviewed and specific financing commitments madefor the next year in advance of the submission of the Government's annual budget (para.7. 1(b)).
5.12 Progress reports will be made available to donors and the recently-established AidCoordination Unit at the Department of Development and Planning, which is charged, amongother things, with coordinating donor assistance to the Government's Public Health SectorInvestment Program. The Donor Liaison Officer would be responsible for collating theperiodic reports for submission to Government and donors. The program reporting system tobe developed would establish short-term targets and indicators as appropriate for each

- 34 -
component of the program, regardless of the funding source. These measures will enable theresponsible line managers to check whether program components are on track, in termns ofachieving the desired outputs spelled out in the NHAP for the different technical programs andsupport services. Therefore, there is need for clear conceptual linkages between theintermediate reporting measures and the long-term output and impact indicators used for theprogram.
5.13 Specific targets are given for involvement of communities in districts and hospitalboards, development of standards for quality, outputs targets for training and rehabilitation offacilities and utilization of facilities, and impact targets for mortality, fertility, and disease ratereduction (Annex 11). For example, the impact targets for the year 2000 include: infantmortality at 70 deaths per 1000 live births; under 5 mortality at 160 deaths per 1000 live births;and total fertility rate at 6.0 children. During negotiations, assurances were provided thatGovernment will meet the key time-bound performance indicators agreed on for the program,as shown in Annex 11 (para. 7.4(c)). In addition, assurances were provided by Governmentduring negotiations that it will undertake the following measures in support of the NHAP: (a)develop a health sector financing plan by the end of 1997 to identify the public and privatefinancing mix of health services; (b) institutionalize feedback of health service users byconducting formal beneficiary assessments in 1998 and 2000; (c) conduct a national householdsurvey on health behaviors, health status and health expenditures in 1999; and (d) initiate acertificate of need process whereby all capital investments above US$25,000 must obtainformal approval from the DOH Management Team to justify investments according to priority,based on the criteria of: (i) meeting community needs; (ii) addressing program goals; and (iii)the affordability of the proposal. (para. 7.1(d)).
5.14 The Monitoring cycle. A regular program planning and monitoring cycle would beestablished under the NHAP, based on the Government's financial calendar. A progress reportand draft rolling implementation plan and budget, covering activities, training, andprocurement would be circulated to donors at least three months before the beginning of thenext fiscal year. Two months before the beginning of the next fiscal year, Government wouldconvene a joint meeting with donors to review progress made during the previous year, andfinalize specific financial commitments for the coming year, based on the draft plans.Eventually, the national plan would be a consolidation of previously prepared District andcentral DOH plans. One month before the end of the fiscal year, the annual implementationplan and budget for the next FY would be agreed upon for Government and donordisbursement. Government would produce an annual progress report, summarizing reportsfrom the Districts and the DOH programs, for distribution among donors, prior to supervisionmission. These reports would not only indicate progress in relation to the plans from thecentral DOH and the districts, they would also report actions taken to resolve problems. TheManagement Support Officer would liaise with the respective line managers to ensure that theysubmit timely written progress reports on the specific program interventions and services forwhich they are responsible. Formal Bank supervision missions-to be carried out incollaboration with donors and NGOs-would take place at least twice a year, and one of thesewill be scheduled to follow the receipt of the annual report from the DOH, and will continuewith the program annual review and the donor consultation meeting on sector plan and budgetfor the next fiscal year (see Annex 15 and also 5.15 below). The primary objective of

- 35 -
supervision would be to provide support and guidance to the DOH to solve those problemswhich it is unable to resolve by itself. The program has budgeted for the DOH to hireadditional technical assistance for the preparation of sector plans and budgets. This approachto supervision places the responsibility firmly with the DOH, so that the Borrower would takeits own necessary corrective action on the basis of monitoring information available before thearrival of a donor supervision mission. The DOH will also provide Part II of the ProgramCompletion Report to IDA within six months of the closing date.
E. ANNUAL AND MID-TERM REVIEWS
5.15 A comprehensive annual review of the program conducted jointly with theGovernment and other donors is an important feature of the operation. These reviews wouldfocus on the achievement of the intermediate targets and indicators in the agreed upon annualworkplan and the reasons for any variation. The approach to the reviews would be forward-looking, endeavoring to identify factors which are likely to impede progress in the followingyear, and taking necessary steps to overcome these constraints in a timely manner or to amendobjectives in the light of changing circumstances. The reviews would also assess progress onthe indicators of the NHAP and decide whether financial resources from the Credit would bemade available for the implementation of program activities. The implications of the findingsof the annual review for the current year's workplan would also be examined, and the workplanwould subsequently be amended as appropriate.
5.16 Assurances were provided at negotiations, that in the third year of the program, amid-term review will be carried out jointly with the Government and other donors to assess theprogram achievement toward meeting its original objectives (para. 4.1) and targets (Annex11), and on that basis make necessary adjustments in program objectives, inputs andperformance indicators prior to starting the second phase of the program (para. 7.1(e)). TheGovernment will prepare, two months ahead of time, a report required for a comprehensivemid-term review covering all aspects of the program being implemented (both at headquartersand district levels). Based on the outcome of the review, the Government and other donorswill agree on whether to alter program objectives and/or to reduce or increase the scope of theprogram. Government will then prepare a revised NHAP that will reflect any agreed changesfor improving program implementation.
F. ENVIRONMENTAL ASPECTS
5.17 This project is classified as category C in view of its negligible environmental effects.Because the program includes improvements in sanitation, food hygiene, and medical waste,the net effects of the program are expected to be beneficial to the environment.
G. PROCUREMENT
5.18 As is the case for other sector investment credits, the credit is undetermined forprocurement purposes. The exact mix of civil works, goods and services to be financed by theCredit will depend on the results of the annual planning process that will be reflected in the

- 36 -
annually agreed upon plans. The proposed totals for the procurement (and disbursement)categories are thus expected to change during implementation. The initial estimates are shownin Table 5. 1. National competitive bidding (NCB) procedures will include: (a) explicitstatement to bidders of the evaluation and award criteria; (b) local advertising with public bidopening; (c) award to lowest evaluated bidder; and (d) foreign bidders would not be precludedfrom participating in NCB. Government confirmed the above NCB principles duringnegotiations.
5.19 Government's overall procedures for procurement are being developed with IDAassistance to ensure that they are economic, efficient, fair and acceptable to other contributorsto the NHAP. For the use of Government funds, the thresholds 2 for goods, works, andservices are currently as follows: purchases exceeding Le5 million require public tenderingthrough the Central Tenders Board (which meets at least every two weeks); purchasesbetween Le700,000 and Le5 million require public tendering through a Departmental TenderBoard; purchases between Le200,000 and Le700,000 require at least three price quotations;and purchases under Le200,000 may be made at the discretion of the Vote Controller.National bidding requires publication of invitations to tender in at least two local newspapers,and a bidding period of at least one month. For international competition, the invitations arealso published in overseas newspapers and international trade journals, and disseminated tolocal embassies, and a bidding period of at least nine weeks is required. A technical committeemakes recommendations for award based on the lowest evaluated bid, based on criteria clearlydescribed in the bidding documents. A register for contractors for works and services is beingmaintained to classify them according to their financial standing and value of contracts forworks and services for which they are normally capable of carrying out satisfactorily. Furtherdetails are outlined in the DOH Operations Manual. Procurement staff from the ManagementServices Division will be trained in the new procedures, and assisted by a procurement agency.
5.20 Civil works. The programn's civil works include the construction of 57 health centers,and the rehabilitation of 61 PHUs and 13 hospitals. For the use of IDA funds for civil works,contracts for construction and rehabilitation estimated at more than US$500,000 per contractwould be awarded on the basis of international competitive bidding (ICB) in accordance with theGuidelinesfor Procurement under IBRD Loans and IDA Credits (January 1995). The majority ofcivil works are small and scattered, and unlikely to attract international bidders. The constructionof health centers and rehabilitation of clinics that cannot be grouped into large contracts or are lessthan US$500,000 per contract and US$4.5 million in aggregate would be awarded on the basis ofcompetitive bidding advertised nationally (NCB) in accordance with procedures acceptable toIDA. Minor rehabilitation and repairs works that are estimated to cost less than US$25,000equivalent per contract, up to an aggregate of US$0.5 million, would be procured underprocedures acceptable to IDA on the basis of price quotations obtained from at least three localreliable contractors who use local labor and materials, including participation of communities, tothe extent practical.
2 Government is currently revising thresholds in the light of new exchange rates and inflation.

- 37 -
Table 5.1 Summary of Proposed Procurement Arrangements (US$ million)Procurement Category ICB NCB OTHER N.F.A. TOTAL
1 Civil Works1.1 Construction/Rehabilitation of health centers 2.2 4.5 0.5 13.8 22.0
and hospitals (2.2) (4.5) (0.5) (-) (7.2)
2. Goods2.1 Essential drugs, equipment and materials 2.0 0.5 2.5 3.5 8.5
(2.0) (0.5) (2.5) (-.-) (5.0)3 Consultancies3.1 Institutional development, studies, monitoring -.- -.- 2.5 1.4 3.9
& supervision (-) (-.-) (2.5) (-) (2.5)
4 Training4.1 Training and workshops -.- -.- 3.4 2.0 5.4
( ) ( ) ~(3.4) (-.-) (3.4)
5 Operating costs . -.- 2.0 97.5 99.5( ) ( ) ~(2.0) (- -) (2.0)
TOTA1L 4.2 5.0 10.9 118.2 138.1IDA Financing (4.2) (5.0) (10.9) (0.0) (20.0)
Note: Totals may not add up due to rounding. Figures in parentheses are the estimated amounts to be financed by the IDAcredit. Final totals may vary significantly since only the first year of the Sector Investment Credit has been programmedin detail.N.F-A. = Not Financed by the Association
5.21 Goods. Goods financed by IDA under the program would include: essential drugs,medical equipment and materials, vehicles, and office equipment and furniture for a total valueof US$5 million equivalent. Because of the current need to use drug kits for PHUs,procurement of essential drugs for primary health care would be procured from UNICEF, fordrugs stocked by them, up to an aggregate of US$2 million. Approximately US$1.5 millionequivalent in pharmaceuticals would be procured through ICB, and another US$250,000through international shopping for drugs estimated to cost less than US$25,000 equivalent percontract in accordance with Bank Guidelines. In general, goods valued at US$250,000 ormore per contract would be procured through ICB. Goods estimated at less than US$250,000per contract, and US$0.5 million in the aggregate, would be procured through nationalcompetitive bidding (NCB) under procedures acceptable to IDA. The remaining goods whichcannot be grouped into bid packages of at least US$25,000 equivalent up to an aggregate ofUS$250,000 would be procured by national shopping up to an aggregate of US$100,00equivalent, or by international shopping up to an aggregate of US$150,000 according to BankGuidelines.
5.22 Services. Consultants financed by IDA would be contracted in accordance with IDA's,Guidelines for the Use of Consultants (August 1981). The consultancy services required under theproject would be mostly for project management, supervision and implementation, architecturaland engineering services, and for training activities. It would include, specifically, the services oflocally recruited consultants and training institutions to carry out activities such as: (a)
- 38 -
procurement agents; (b) quantity surveyors and building technicians; (c) annual program audits;(d) training of DOH and District staff; and (e) preparation of training and [EC materials. Traininginstitutions would be selected on the basis of a short-list and submitted proposals. Where specificarea of expertise is required intermittently over an extended period, contracts with internationaluniversities or training institutions will be considered.
5.23 Procurement arrangements. The procurement activities of the program financedby IDA will be straightforward. The construction and rehabilitation works will be supervisedby project engineers and final payment will be made to contractors only when the work iscomplete according to specifications. The procurement will be carried out by staff who haveprocurement experience under the ongoing IDA-assisted project, who will be assigned to thenew Procurement Services Unit of the DOH (under the Management Services Division), withadditional technical assistance support. The Unit will be staffed with professional purchasingand stores personnel and utilize improved procurement management systems, covering bothGovemment and donor procurement procedures. Although the DOH Management Team willbe responsible for the oversight of the administrative and contractual arrangements of theprogram, the Management Support Officer will liaise closely with the Procurement ServicesUnit for handling all matters related to the preparation, implementation and monitoring ofwork plans for the smooth execution of procurement of all works, goods, and services,including the preparation of bidding documents, launching of tenders, evaluation, andreporting the results to the Government and to IDA for review. In addition, adequate recordson procurement progress, including staff reports on site visits, the timing of works and goodsprocurement; and compliance with agreed methods of procurement will be maintained by theProcurement Services Unit. These will be used in DOH's program monitoring system.Commitment to following a generic timetable for the detailed steps of the differentprocurement activities were agreed at negotiations (para. 7.1 (f)).
5.24 Bank review. Prior review by IDA would be required for procurement of packagesof works and goods which exceed US$100,000. Procurement documentation andarrangements for each consultant contract valued at US$100,000 or more for firms andUS$50,000 or more for individuals would be subject to prior review by IDA. However, theexceptions to prior IDA review would not apply to (a) the terms of reference for suchcontracts; (b) single-source selection of consulting firms; (c) assignments of a critical nature,as reasonably determined by the Association; (d) amendments to contracts for the employmentof consulting firms raising the contracts value to US$100,000 equivalent or above; or (e)amendments to contracts for the employment of individual consultants raising the contractvalue to US$50,000 equivalent or above. All bidding documents will be prepared using theBank's Standard Bidding Documents for each type of ICB procurement which will besubmitted to IDA for review and approval. Submission to IDA of finalized first year biddingdocuments for civil works and goods for the Western Region-to be financed by IDA-to beprocured through international competitive bidding would be a condition of effectiveness(para. 7.3 (e)).

- 39 -
H. DISBURSEMENTS
5.25 In accordance with the NHAP, the Credit is expected to be completed within a five-year period by December 31, 2000 (completion date), with all disbursements made by June 30,2001 (closing date). Although the program is expected to be implemented with considerabledifficulty because of the enormous challenges faced by the DOH, successful disbursement isanticipated because of (a) the considerable time and resources invested in preparation andplanning; (b) the high degree of Government ownership and commitment to the programdeveloped through the preparation process; (c) the strengthening of DOH capacity by staffingof key positions and support by local and international consultants; and (d) the use of trainingand technical assistance in financial management. There is limited Regional experience in thedisbursement of integrated sector-wide programs. The funds for this operation are forecast todisburse at a faster rate than the Regional profile because the operation is equivalent to theDOH program, and cannot be marginalized, and because of the up-front preparation andsystematic review of program implementation. The estimated disbursement schedule is givenin Annex 16.
5.26 The following table gives the categories and amounts to be financed out of the IDACredit, and the percentage to be financed in each category.
Table 5.2 Allocation and Disbursement of the IDA Credit (US$ million)1. Civil works 6.3 100% of foreign expenditures
90% of local expenditures2. Drugs, furniture, equipment, vehicles, supplies 4.3 100% of foreign expenditures
and spare parts 90% of local expenditures3. Technical assistance and studies 2.1 100% of expenditures4. Training, including training materials 3.0 100% of expenditures5. Incremental operating costs' 1.7 100% of foreign expenditures;
90% of local expenditures untilDecember 31, 1998; then, 75%of local expenditures
6. Refunding of Project Preparation Advance 0.3 100%7. Unallocated 2.3
Total credit amount 20.0These include: incremental administrative and rnnning costs of districts, the DOH Management Team, the PMISU,
the Management Support Office, the Financial Management Unit, and the Procurement Unit, such as salaries forincremental staff positions, per diems, travel costs, general office supplies, fuel, vehicle and equipment maintenance costs,and other administrative expenses.
5.27 Disbursement and withdrawal procedures are detailed in The World BankDisbursementHandbook (1992 edition). All disbursements are subject to the conditions of theDevelopment Credit Agreement and the procedures defined in the Disbursement Letter. TheOperational Manual will further outline what individual managers need to do to spend andaccount for money under their authority.
5.28 Special Account. To facilitate disbursements of eligible expenditures for works,goods and services, the Government would open a Special Account in a commercial bank tocover part of IDA's share of eligible expenditures to be managed and administered by the

- 40 -
DOH. The authorized allocation for the Special Account would be US$1 million covering anestimated four months of eligible expenditures financed by IDA. Upon effectiveness, 500/o ofthe authorized allocations amounting to US$500,000 would be deposited to the SpecialAccount. The remaining balance will be made available as needed. Monthly replenishmentrequests would be fully documented except for contracts for civil works, goods and consultingfirms below US$100,000 equivalent, and for contracts for services from individuals belowUS$50,000, and all incremental operating costs, which may be claimed on the basis ofStatements of Expenditure (SOEs). Documentation would be retained by DOH for review byregular IDA supervision missions and the external auditors. Replenishment requests would beaccompanied by up-to-date bank statements and reconciliations of the Special Account. Allpayments under US$50,000 equivalent must be made through the Special Account; paymentsabove that amount may be made through direct payment or special commitment procedures.All direct-IDA payments must be according to the procedures set out in The World BankDisbursement Handbook (1992 edition). Funds in the Special Account cannot be mixed withother funds (such as funds from Government sources or other donors).
5.29 Government financing. Government financial contribution to the health sectorwould be monitored through the accounting system being established with the assistance of anauditor and with the Department of Finance (DOF). As a condition of effectiveness, theGovernment would sign a contract for (i) the installation in the system of an accountingsoftware for the DOH's programs, and (ii) the training of DOH's staff in the use of the saidsystem (para. 7.3(f)). The DOF would be required to make quarterly allocations to the DOHon the basis of an agreed budget for the program, proposed by Government, and accepted byIDA one month before the beginning of each fiscal year.
L. ACCOUNTING, AUDITING, AND REPORTING
5.30 Overall responsibility for the project's financial management would rest with theFinancial Management Division of the DOH, which would maintain the consolidated ProgramAccounts for the entire program. To improve Government's coordination of donor funds andto ensure transparency for the entire program, accounting for all transactions of the ProgramAccounts, including Government funds, the IDA Special Account, and funds from otherdonors, would be maintained in accordance with international accounting standards. Annualfinancial statements of Government and all donor finances would be prepared and audited inaccordance with international auditing guidelines. By June 30th of each year, theimplementing agency would submit to IDA and other donors an auditor's report, managementreport and audited financial statements for the Program Accounts, the Special Account, andStatement of Expenditures (SOEs) for the preceding fiscal year, audited by an independentexpert under terms and conditions acceptable to IDA. Therefore, the appointment of anindependent auditor will be crucial,and it would be a condition of credit effectiveness (para.7.3(g)), the Government will have issued the letter of invitation satisfactory to IDA for theemployment of an independent auditor to audit the expenditures financed from proceeds of theproposed Credit. The audit of Credit 1695-SL implemented by the DOH is current.

- 41 -
VI. PROGRAM BENEFITS AND RISKS
A. PROGRAM BENEFITS
6.1 Implementation of the program will enable the Government to attain its sector goals,offering Sierra Leoneans more access to health services of better quality, and will ultimatelylead to, through its emphasis on primary health care, improved health status of the populationwith emphasis on the poor, women and children. The main benefits of the project would be to:(a) reduce excessive morbidity, mortality, and fertility through extension of basic qualityhealth and family planning services to those most in need; (b) implement a comprehensivereform of the health sector aiming at directing resources to those priority health problems forwhich cost-effective intervention strategies are available; (c) strengthen the capacity of centralDOH to use resources in an efficient manner; (d) develop sector capacity in areas such asmanagement, financial management, human resources development and planning; (e)decentralize decision-making, and enable communities and districts to make decisions and tohave greater control over budget and service delivery; and (f) diversify the financing of healthservices and help establish a more equitable and affordable basis for it.
B. PROGRAM RISKS
6.2 There are a number of potential risks, most notably: (a) the persistence of-or latesolution to-the security situation, which multiplies health emergencies, makes rehabilitationin parts of the country untenable, and increases the possibility of not obtaining sufficientdomestic resources to implement the NHAP; (b) an over-ambitious program, which over-stretches the implementation capacity of the DOH, could lead to weak efficiency gains anddonor skepticism concerning GOSL potential to coordinate and implement its policy, and; (c)moving too quickly, before the reorganization of the DOH and the strengthening of its keyunits are completed, could lead to a decline in efficiency, further dysfunction and distortions inthe provision of health services, and the inability to use national- and donor-contributed funds.
6.3 The risks are minimized by implementing the program in phases, starting physicalrehabilitation in areas free from civil unrest (e.g., Western Area). The sector investmentapproach is also appropriate in these circumstances, as it allows a greater deal of flexibility inprogram planning, enabling quick response to changing situations. The development phasesare also planned according to the growing capacity of Govemment, investing heavily ontraining, support systems, and studies, using pilot initiatives, and reviewing progressfrequently, to minimize the risk of moving too quickly with institutional reform. Particularemphasis on financial management, accounting and controls will help to ensure that allocatedfunds are used for intended purposes in the health sector. The risks are further diminishedbecause there has been a comprehensive effort to examine organizational needs andcapabilities, incentives, and institutional culture, and to involve a wide number of Governmentparticipants in the reform process. Decentralization of authority will be accompanied byappropriate financial support and intensive training in management systems. Annual reviewsundertaken jointly by the Government, IDA, and other donors will enable Government to

- 42 -
make required changes in programming strategies on a frequent basis. A mid-term review willprovide an opportunity for major restructuring, and cancellation, if necessary. Efforts toincrease participation with other Government Departments and stakeholders outside of theGovemment should help to assure domestic support, and will diminish the risks due to politicalinstability, by developing a broad approval for the program and for the process of programdevelopment and management. Finally, through the Bank's assistance by means of thestructural adjustment program, there is a consistent effort to maintain the commitment of theGovernment to invest in social sectors.
VII. AGREEMENTS, CONDITIONS, AND RECOMMENDATION
7.1 During negotiations, the Government provided assurances that it will:
(a) give budgetary authority to implement a prepared district health plan to at least oneadditional district in each year of the operation (para. 4.13);
(b) submit a three year rolling plan, an annual progress report, and a draft annual detailedimplementation plan and budget at least three months prior to the beginning of eachfiscal year, and prior to an annual Government-led meeting with donors, whereprogress on the previous year's health program would be reviewed and specificfinancing commitments made for the next year in advance of the submission of theGovernment's annual budget (para. 5.11);
(c) make all efforts to meet the key time-bound performance indicators agreed on for theprogram (para. 5.13);
(d) undertake the following measures in support of the NHAP: (a) develop a healthsector financing plan by the end of 1997; (b) institutionalize feedback of healthservice users by conducting formal beneficiary assessments in 1998 and 2000; (c)conduct a national household survey on health behaviors, health status and healthexpenditures in 1999, and (d) initiate a certificate of need process whereby all capitalinvestments above US$25,000 must obtain formal approval from the DOHManagement Team to justify investments according to priority, based on the criteriaof: (i) meeting community needs; (ii) addressing program goals; and (iii) theaffordability of the proposal. (para. 5.13).
(e) carry out jointly with other donors a mid-term review to assess the programachievement toward meeting its original objectives (para. 4.1) and targets (Annex 11)in the third year of the program, and on that basis make necessary adjustments inprogram objectives, inputs and performance indicators prior to starting the secondphase of the program (para. 5.16).
- 43 -
(f) upgrade procurement procedures to meet IDA standards (para. 5.18); and follow anagreed generic timetable for the detailed steps of the different procurement activities(para. 5.23).
7.2 As a condition for Board presentation, the Government submitted:
(a) a detailed plan and timetable for reconciling the DOH payroll and the actual DOHstaff census (para. 4.15); and
(b) a signed Letter of Health Sector Development Policy satisfactory to IDA (para.5.2(b)).
7.3 As a condition of effectiveness, the Government would:
(a) sign two technical assistance agreements, for at least twelve man months each, forsupport services to be provided during the first two years of the project, with (i) afinancial management consulting firm, and (ii) a procurement technical assistanceagency, under terms and conditions satisfactory to IDA;(para. 5.2(a));
(b) sign a technical assistance agreement to conduct in-house training with the SierraLeone Institute for Public Administration and Management (IPAM), under terms andconditions satisfactory to IDA (para. 5.2(a));
(c) submit to IDA for the Western Region district: (i) the training plans and (ii) the planfor recruitment and redeployment of staff for those health facilities whererehabilitation and construction works will take place during the first year of theproject (para. 5.2(b));
(d) finalize the Operational Manual (para. 5.8);
(e) prepare and finalize the first year bidding documents for civil works and goods forthe Western Region district to be procured through International Competitive Bidding(ICB) and to be funded by IDA; (para. 5.24);
(f) sign a contract for: (i) the installation in the system of an accounting software forDOH's programs, and (ii) the training of DOH's staff in the use of the said system(para. 5.29);
(g) issue the letter of invitation to recruit an independent auditor to audit the expendituresfinanced from proceeds of the Credit (para 5.30); and
(h) staff the following key positions: Director of Management Support, Director ofFinancial Resources, Chief Procurement Officer, and a professional supportingposition at the Donor Relations Office to monitor and coordinate donor programs andbudgets, under terms and conditions satisfactory to IDA (para 4.12(a)).
- 44 -
Recommendation
7.4 Subject to agreement to the above, the proposed program will constitute a suitablebasis for an IDA credit of SDR 13.6 million (US$20 million equivalent) to the Republic ofSierra Leone on standard IDA terms with a maturity of 40 years.

ANNEX 1
REPUBLIC OF SIERRA LEONE
INTEGRATED HEALTH SECTOR INVESTMENT PROJECT
Sodo-Economic Indicators
Most SameRecent Region Income Groups
Unit of Estimate Sub-Sah. Low- Middle-Measure (mre) Africa Income Income
Income IndicatorsGNP per capita USS 150 520 380 2480
Social IndicatorsPublic Expenditures on Basic Social Services % of GDP 3.1 - - -
Gross Enrollment Ratio: % school age groupPrimary: Total 48 67 101 104
Femals 39 60 93Secondary: Total 16 42
Female 12 34 -
Mortality per '000 live birthsInfant Mortality Rate 164 93 64 39Under-5 Mortality Rate 284 172 103 57
Immunization (under 12 months) % age groupMeasles 74 49 44 65DPT 75 38 43 67
Child malnutrition (<5) 23 28 38Life Expectancy at birth years
Overall 39 52 62 68Female advantage 3.2 3.4 2.4 6.4
Total Fertility Rate births per woman 6.5 6.1 3.4 3.1Matemal Mortality Rate 100.000 live births 800 - -
Sources: Social Indicators of Development, 1993-1994, The World Bank, 1994.World Development Report 1995: Workers in an Integrating World, The World Bank, 1995.


ANNEX 2Page I of 6
SECRETARY OF ST7ATE FOR HEALTHAND SOCUL SERVICES
DEPARTMENT OF HEALTH 4TH FLOORTOUTIBUILDING
FREETOWN, SIERRA LEONE
Februazy 5, 1996
Mr. James D. WolfensobnPresidentThe World BankWashington, D.C.
Dear Mr. Wolfensohn:
Sector Development Policy
I wish, on behalf of the Govemment and people of Sierra Leone, to thank the World Bank,through you, for the assistance it has provided right from the start of the development of our NationalHealth Action Plan to tbis stage.
Over the last three years, our health sector in Sierra Leone has developed a policy, details ofwhich will be spelt out below.
Strting September 21-25, 1992, the Department convened a week-long seminar involving allstakeholders in the health sector in Sierra Leone. It provided an open forum for a dialogue, assessmentof needs, people-centred prioritizafion, and for the creation of an atmosphere of cooperation between thepublic, private and the private non-profit sectors, the health consumers and the international community.
The National Health Policy, which was the outcome of this exercise, was closely scrutinized andfinally accepted by Government in June 1993.
The policy mapped out a new direction for the health care system, focussing on the developmentof preventive services whilst simultaneously strengthening the existing deivery system. The mainagenda for Government described in the National Health Policy is that:
(a) a network of sound primaiy, secondary, and tertiary health facilities will be strengthenedthrough rehabilitation, appropriate staffing and logistical support;
(b) environmental health and communicable disease control will be promoted;
(c) community participation and intersectoral cooperation will be fostered;

ANNEX 2Page 2 of 6
(d) health care delivery will be decentralized to the district level;
(e) Govemment financing of health care will increase;
(f) certain services will be privatized, where appropriate; and
(g) cooperation with international agencies and NGOs will be promoted.
The Government's main health objectives and indicators for the nation are clearly stated in theNHAP. In brief the main objectives are to: (a) improve child health; (b) improve matemal health; (c)reduce fertility; (d) reduce the incidence and prevalence of communicable diseases and other commonailments, including H1V; (e) reduce mental illness; (f) reduce injury and handicaps; (g) assuresatisfactory nutritional status; (h) reduce drug abuse; (i) improve living conditions; and 0) improve foodhygiene. The NHAP defines the main functions of the health sector, and identifies how each of itsprogrammes are designed to fulfill these functions and contribute to one or more of the nine populationimpact objectives. Each programme within the NHAP has clear operational targets to be attained duringthe next five years, which will contribute to achieving its main objectives. Fulfilling these objectiveswould contribute to the social sustainability of the adjustment programme, and strengthen the humanresource base needed for the future growth of Sierra Leone.
In order to transform the Health Policy into action, the Department organized a participativeworkshop, held from October 27-November 5, 1993, involving various stakeholders, including the othersectoral Departments, non-governmental organizations and donor agencies. This analysed healthproblems, determined objectives and formulated both technical and support programmes (Annex 1), inan effort to develop a consensus around an effective health policy and planning process as a criticalmeans of increasing effectiveness and efficiency. The National Health Action Plan (NHAP) wasdeveloped at the workshop.
The Action Plan (NHAP) envisaged a major reform and restructuring of the health sector,resulting in: (1) a radical organizational change (2) substantial human resource development andmanagement; (3) rehabilitation of the health infrastructure, particularly in the rural areas; (4)enhancement of community participation, as well as investment in support services and systems thatsustain operations; (5) district level decentralization, and; (6) integration of vertical health serviceprogrammes to make public health care more responsive to community needs.
The following four, related issues are recognized as critical in the establishment of a foundationfor a sustainable, equitable, and efficient health care: (a) poor access to health care; (b) poor quality ofservices; (c) poor management, inadequate community involvement and accountability; and (d)insufficient health care financing. The net effect of the reform programme is expected to improve thehealth status of the people of Sierra Leone, by increasing access to healthcare and improving quality of anational package of health services that is better managed and financed through a progressivelydecentralized system.
The total cost of these programmes is estimated at US$270 million over the period 19941999.Comparing these estimates with projected Government and donor expenditure at current levels gives afinancing gap of US$184 million.

ANNEX 2Page 3 of 6
In view of the magnitude of the fimding gap for the NHAP, the Department prepared a coreprogramme of high priority interventions and services for discussion with donors.
The core programme was developed by considering the highest priority programmes and,therefore, represents a more modest version or subset of the NHAP. The total estimated cost of the coreprogramme is US$138.2 million (adjusted for physical and price contingencies). After taking account ofthe current Govemment and donor support of US$86 million for the Health Sector, the financing gap isestimated at US$52 million.
Of the funding gap for the core programme of US$52 million, it is estimated that an additionalUS$26 million will be contributed by the Government and household sectors. The core programme wilLtherefore, require an incremental donor contribution of US$26 million.
It is recognised that the cost and financing totals are preliminary estimates requiring furtherrefinement through discussion with donors and other major stakeholders. In particular, the costs oftraining, improved staff remuneration and decentralization need considerable further analysis. Periodicreview of programme expenditures and donor commitments is therefore envisaged.
It is recognized that the cost and financing totals are preliminary estimates, requiring furtherrefinement through discussion with donors and other major stakeholders. In particular, the costs oftraining improved staff remuneration and decentralization need considerable further analysis. Periodicreview of program expenditures and donor commitments is therefore envisaged.
The provision of a more comprehensive, integrated and sustainable health care system is centralto the country's development strategy. The health system had deteriorated to such an extent that there isa large financial and technical gap between what is currently available and what is needed to make itwork.
At the Social Sectors Round Table Consultations (May, 1994) the Department presented itsplans for the reform and restructuring of the health care system, with the objective of promoting dialogueand fostering consensus among Govermnent, NGOS, the donor community and other key stakeholders,and of generating support for the health sector reforms. Government was encouraged to make greateruse of NGOs and the enhanced role of the private sector in financing and health care delivery. NGO'sagreed to work fully within the framework of the NHAP and share their information and technicalcapabilities with Govermment.
Participants applauded government's determination to decentralize the health care services atdistrict level and enhance accountability at both Headquarters and at the periphery.
Donors and NGOs agreed-inter alia-to: work exclusively within the framework of the NationalHealth Action Plan as much as possible, using common implementation modalities; participate withGovermment in the joint review and planning process; provide financial and/or technical assistance insupport of the NHAP; meet the estimated funding gap in the NHAP; mobilize their resourcecommitments for the NHAP; prepare their information requirements for discussion with Government;adapt the scope and modalities of their development assistance to accord with the needs of the NHAP,and; offer to redirect some existing projects' funds to finance some sharply-focussed, technicalassistance-both to yield demonstrable progress in the field and improve the efficiency of the Department.

ANNEX 2Page 4 of 6
At the October 1995 Social Sectors Donors Meeting, donors and NGOs agreed to support theincremental core program activities with an additional US$5.75 million for 1996.
Governmenfs commitment to the NHAP has been demonstrated by its acceptance of thedocument, and its commitment to increase expenditure in the health sector by at least 5% per annum inreal terms over the duration of the NHAP. More recently, Govemment has agreed in principle toauthorize the Department of Health to have:
(a) authority to decide programme, manpower and line item budgets, in relation to the coreprogramme, and wihiin an overall departmental ceiling provided by the Department ofFinance;
(b) real influence over the recruitment and selection process, and the application ofemployment practices for staff promotions, discipline and transfers, and;
(c) authority to determine the numbers, categories, and skill mix of staff required in line withan overall departmental manpower plan, as well as some discretion over individual's paywithin established salary structures.
An improved organizational structure of the Department has been developed and jobdescriptions have been prepared to delegate authority from the Secretary of State to the central anddistrict levels of management as follows:
1. Top Management Team2. Director-General of Medical Services3 . Director-General of Management Services4. Donor Relations5. Intemal Auditor6. Management Support Office7. Division Directors8. Unit Managers9. District Health Management Teams10. National Health Councils, District Health Boards and Hospital Management Committees
The process of reform has done much to energize the Department of Health and the peopleassociated with it. DOH staff have learned to work in teams to identify and solve problems, andtherefore communication and the effectiveness of the work of the DOH has improved. The reformprocess has brought Department staff much closer to the users of the health system and to otherproviders. Much of this is due to the preparation of the NHAP and the confidence they have gained fromthe experience. This is one of the main reasons why the DOH was selected Governments mostproductive Department.
The beneficiaries have been involved in the development of the National Health Policy and theNational Health Action Plan. They participated in a programme prioritization exercise, which identifiedthe core programmes of the NHAP, and they have indicated their commitment to the NHAP throughtheir willingness to pay for the improved services through user fees and the Bamako Initiative. A

ANNEX 2Page 5 of 6
beneficiary assessment was carried out to establish a baseline for the future analysis of the impact ofGovernment actions on health care. The finding that was specifically relevant and important to theDepartment of Health was the thought that Government could help by providing roads, basic servicessuch as water, and improving literacy and increased economic activity.
The programmes are designed so that they will not be implemented vertically, but as part of apackage of essential health services. The district will become the focus of operational planning andimplementation. Following general guidance of the central DOH, the District Health ManagementTeams (DHNT) will be responsible for planning and delivery of most elements of the six PHC servicesin their own district. The operational details of how the specific services will be provided in each areawill be worked out in each district as part of their annual planning exercise, with the PHUs expected todeliver much of the preventive and primary curative services. Each PHU will be linked to a district levelhospital which will provide first referral services. Larger hospitals will provide more of the sameservices as the district hospitals, and also function as referral points for more specialized services(tertiary health care services). The larger hospitals will be under the administration of newly createdhospital management committees.
The first year of the programme has been designed to set the foundation for the NHAPimplementation while addressing the current security situation. Detailed activities and budgets for thefirst 18 months were prepared by the DOH staff for the entire programme, and are included in the DOHOperational Manual. Since many of the districts are currently inaccessible, more central level planningand irnplementation occurs in the first year. The emphasis on improving the ongoing service deliverywill focus on the Westem Area and the towns where the populations have concentrated. Matemal andchild health services, including family planning, obstetric, and well-child care, along with communicabledisease control, water and sanitation services, and nutrition take the majority of inputs for servicedelivery. Emergency assistance for refugees is being handled separately from routine DOH activities,under an umbrella organization in the Govemment. Implementation of the institutional changes in theDOH is another highlight of the first year's plan. Staff have been reassigned to the new units of theDepartment, but further work and support is planned for 1995/96 to get them fully functional. The keyareas include the establishment of the Financial Management Team, the Procurement Unit, theMaintenance and Repair Unit, and a Donor Relations Secretariat. Human resources development willcomprise a major part of the first year: curricula at the training institutions will be revised, and the firstyear of the new cadres of peripheral health staff is expected this year, while personnel systems will be setup. Revising the health information system is also planned during the first year. Decentralization will beimplemented slowly during this year. The Western Area District Health Management Team hasdeveloped its district plan, and will be given authority to implement the plan, including budgetaryallocations for non-wage recurrent expenditures. Rehabilitation will concentrate in the Westem Area.Hospitals and PHUS, a maintenance facility, and a drug warehouse, all in the Westem Area, arescheduled for rehabilitation in 1995/96. A health facilities infrastructure and equipment survey will beextended in a phased manner to cover the remainder of the country, which will form the basis for specificrehabilitation plans in the subsequent years. Pharmaceutical seed stocks (essential drugs, contraceptives,vaccines, laboratory reagents) for PHUs and hospitals will also be purchased and distributed.
An annual review of the programme will be conducted jointly with the Govermment and the otherdonors. This review will focus on the achievement of the immediate targets and indicators in the agreedannual workplan, and the reasons for any under-achievement or variation. The approach of the reviewwould be forward looking, endeavouring to identify factors which are likely to affect progress in the

ANNEX 2Page 6 of 6
following year, and taking necessary steps to overcome these constraints in a timely manner or to amendobjectives in the light of changing circumstances.
The implementation of the findings of the annual review for the current years workplans wouldalso be examined. This workplan would subsequently be amended as appropriate, demonstrating theflexibility of the NHAP implementation process.
The World Bank has funded the Health and Population Project (HPP) from which lessons havebeen leamed. These will be useful in the implementation of the National Health Action Plan. One of thechallenges of the NHAP implementation will be to recognize, develop and apply local capacity to solvehealth problems of the country.
The lack of coordination in the Health Sector has led to a fractionalised health system. TheNational Health Action Plan seeks to ensure that donor support is focussed on the enhancement of theobjectives of the plan and so obviate the tendency to run separate projects.
Additional recent information about our programme, is provided in the draft ImplementationManual, a copy of which is being transmitted to you.
We thank you profoundly for the Bank's cooperation in our efforts to provide better health carefor our people.
With best regards.
Yours sincerely,
Dr. S.U.M. JahSecretary of State for Health and Social Services

REPUBLIC OF SIERRA LEONEINTEGRATED HEALTH SECTOR INVESTMENT PROJECT
Causes Of Mortality in Western Area
C e _hd dc m -utky 65 yr. md wr 4544 yr# 1S44 yn 5-14 yr 1-4 yr. Ud.r I yr TOTALNumber % N14_r % NH_r * N_or % Nu.er % _mer % Nmewr s
b.edilm d _ dms_ 175 2 Is 29 179 44 75 66 259 7i 416 67 11" 46Pimania (lowu mrpirmloty tmd ifecliona) 94 12 33 11 53 13 13 12 73 22 151 24 417 16Malaria 14 2 13 4 30 7 26 23 60 18 110 18 253 10ln1o.em jectim dieoase (diarthe) 31 4 11 4 28 7 13 12 60 I8 81 13 224 9Meale 10 9 57 17 47 8 114 4TuhouJosi 24 3 10 3 37 9 8 7 1 0 80 3Smoke *mia 5 1 19 5 5 1 12 2 41 2Maili. 2 0 3 1 10 2 3 3 3 1 6 1 27 1Tetanus I 0 7 2 1 0 8 1 17 1Hqepdlis 2 0 6 2 1 1 9 0Olibr infaclious Caum 2 0 2 1 1 0 1 1 1 0 7 0
Me ?EaegP ( _seUe4) 14 2 13 4 6 1 1 1 34 1
e, Nd,ks._ i Mde D_a _wrw I .rs 17 2 a 3 4 1 19 6 30 5 73 3Nulsutlasa manimea & otw prlzei-calori malnulrilion 19 6 30 5 49 2DIat meitiu 17 2 8 3 4 1 29 1
D _lemew E_Bbed d BEmdJe n (ldm6 esC l_I 1 a 9 2 5 4 2 1 17 1
D_ d 6k Cfr1q4y Syg4W 345 43 3 44 o 20 555 Csrilov.cular dimeas 292 36 83 29 66 16 443 17Cereeovaoular dimee 53 7 43 13 14 3 112 4
D_ *f y 8y b ah_-) 12 1 2 1 6 I 2 2 11 3 1i 2 43 3
Dimmew d 6k Digedive Sydm 20 2 13 4 22 5 2 2 57 2Chron lice, disa d cinbodi 7 1 1 0 3 1 1 1 0O gfSi"oiateaisal trat clIne 13 2 12 4 19 5 2 2 46 2
D _w d 6ke G dmkmwy Sydm __eEu re_ tll e 10 1 9 3 20 5 1 1 1 0 41 2
C.ingedIlm Es m, - rh1h * an pampa (rddde _ dine 7 2 7 t
c _m O, W bg ham p,,w. P4.d I 0 no 19 121 5ProiuriIy m bmw ww&ghl 1 0 74 12 75 3Bi.&L tomum 46 7 46 2
ki-7 -a PWNNbg 2 0 1 0 14 3 1 1 5 1 23 1
0o , Nmp.le I Cd_wd Ca 214 24 33 1 i 14 26 23 36 11 49 3 466 16
TOTAL Ole 1a 294 1 45 139 113 139 336 139 as 13 2381 li
Soue Wetm Arwa Vitl Ragitb, 1993
N.W Th ashmt ta m bl ofdaat u t1 W..t.m Alma Ia 1993a qrm f4iy 2211000 XM,000 - 19.36D death;: trbuer& the PmesDftle of death d ia tem Vibl R*glt" ilo"wi_lumal 13%.


REPUBLIC OF SIERRA LEONE
INTEGRATED HEALTH SECTOR INVEHrMENT PROJECT
DIHrUBUrION OF HEALTH FACILITIES AND PUBLIC SECTOR HEALTH WORKERS
DISTRIBUNION OF HEALTTH FACILITIES - 1994
Est Mhoa IndEud &i 0th.rAdmnistrdiv. POp. G ovt. HOoD Mision Hop. Private HOs itd. Total Pop.
Dbtriots 1994 Pr. No. bd No. Bed No. Bed No. B.d pe HOap('000) CHC CHP MCHP TotW CUrnlo Totes Comd. Comdn. Comdn. Compi. Bed
1. Eaastrn ProvinceKailahun 289 14 30 6 50 9 59 2 87 16 1 172 12 1 closed 4 259 28 1,116Kenema 408 13 31 24 6s 2 70 1 132 10 2 40 -1 3 123 21 6 295 31 1,383Kono 446 13 11 5 35 6 41 1 45 10 - - 6 144 34 7 198 44 2,370
Sub-total 1,143 40 78 35 153 17 170 4 264 36 3 212 12 10 267 55 17 743 103 1,541
2. Northern PrvvnceBombali 409 19 11 20 48 9 57 1 50 10 3 108 16 1 30 5 5 199 31 2,178Kambia 217 13 11 4 28 5 33 1 37 5 1 30 5 * - 2 67 10 3,238Koinadugu 206 5 13 5 23 2 25 1 65 10 - - - 1 25 5 2 90 15 2,289Port Loko 352 10 23 1S 52 9 el 2 83 19 2 100 10 1 50 S 5 233 36 1,554Tonkolili 278 10 17 35 62 4 66 1 85 16 2 340 10 - 3 425 26 654
Sub-total 1,462 56 75 93 214 28 242 6 320 59 9 578 41 3 105 19 17 1,003 119 1,489
3. Southern ProvinceBO 319 14 15 30 59 10 6s 1 185 16 1 closed - - 2 185 le 1,724Bonthe 122 7 12 1 20 2 22 1 44 5 1 64 11 1 50 10 3 158 26 772Moyamba 316 14 15 13 42 6 48 3 122 20 - - - 1 64 10 4 le9 30 1,699Pujehun 129 8 7 15 30 - 30 1 closed - - - - - - 1 closed
Sub-total s99 35 42 44 121 19 169 6 351 41 2 64 11 2 114 20 10 529 72 1,674
4. Western AreaRural Area 156 a 1 3 12 9 12 2 50 - - * - - 2 50 - 3,120Urban Area 726 4 - - 4 12 4 7 979 135 1 25 - 6 236 55 14 1,240 190 585
Sub-total 982 12 1 3 16 21 16 9 1,029 135 1 25 - 6 236 55 16 1290 190 3,705
TOTAL 4,373 143 196 166 504 84 597 25 1,964 271 14 879 64 21 722 148 60 3,566 483 1,230
I-
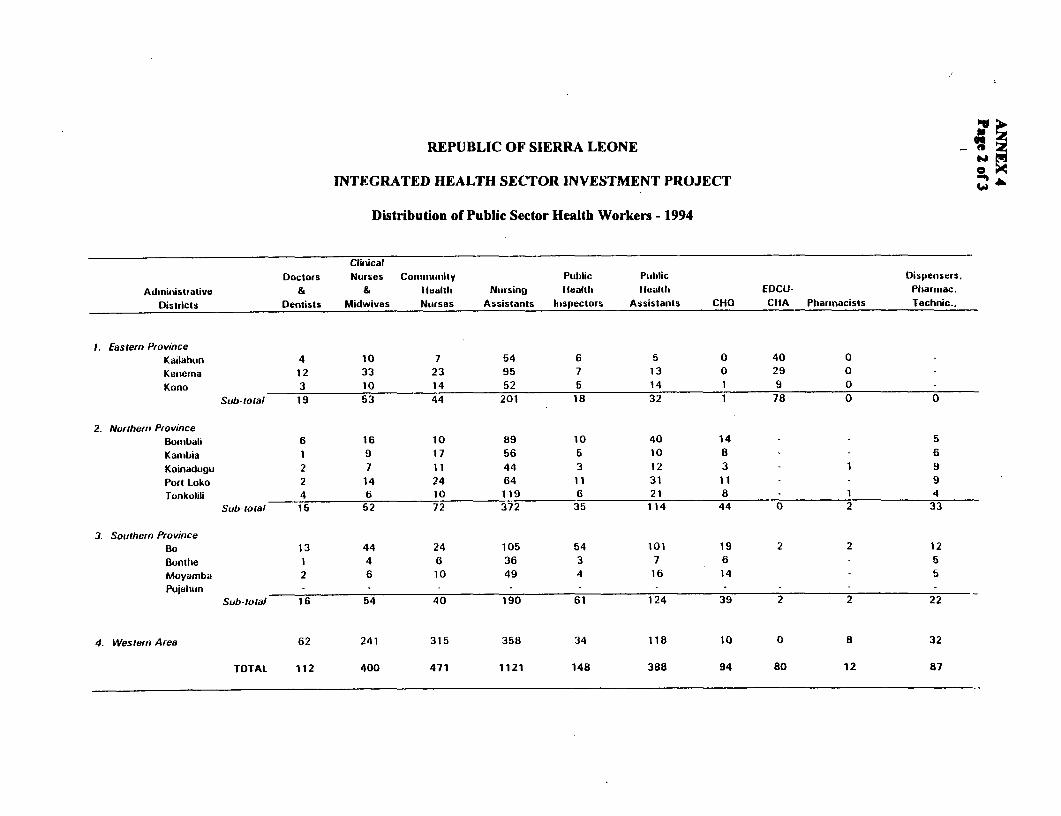
REPUBLIC OF SIERRA LEONE
INTEGRATED HEALTH SECTOR INVESTMENT PROJECT
Distribution of Public Sector Health Workers - 1994
ClinicalDoctors Nurses Conii,irtnity Public Ptiblic Dispensers.
Adinillistrative & & lealth Nursing Healtil Heal(ii EDCU- Pharmac.
Districts Dentists Midwives Nurses Assistants hispectors Assistants CHO CIIA Pharinacists Technic..
I. Easrern ProvinceKailalhun 4 10 7 54 6 5 0 40 0
Kenerna 12 33 23 95 7 13 0 29 0
Kono 3 10 14 52 5 14 1 9 0 -
Sub-total 19 53 44 201 18 32 1 78 0 0
2. Northern ProvinceBomibali 6 16 10 89 10 40 14 - 5
Kamibia 1 9 17 56 5 1 0 8 - - 6Koinadtigu 2 7 11 44 3 12 3 1 9
Port Loko 2 14 24 64 11 31 11 - 9
Tonkolili 4 6 10 119 6 21 8 1 4Sub-toral 15 52 72 372 35 114 44 0 2 33
3. Sotuthern ProvinceBo 13 44 24 105 54 101 19 2 2 12
Buntlie 1 4 6 36 3 7 6 - 5
Moyamba 2 6 10 49 4 16 14 - 5
Pujehun -Sub-rota) 16 54 40 190 61 124 39 2 2 22
4. Western Area 62 241 315 358 34 118 10 0 8 32
TOTAL 112 400 471 1121 148 388 94 80 12 87

REPUBLIC OF SIERRA LEONE
INTEGRATED HEALTH SECTOR IVESTMENT PROJECT
DISTRIBUTION OF PUBLIC HEALTH WORKERS - 1994
Non- Nurses/Administrative Stat. Lab. Maint. Support Staff Clinical Population/ Doctor
Districts Officers Staff Techn. Drivers Admin. Clerical Minor Specialists Physians Nurses Ratio
1. Eastern ProvinceKailahun - - - - - - - - 72,300 17,000 4Kenema - - - - - - - - 34,000 7,300 5Kono - - - - - - - - 149,000 18,600 8
Sub-total - - - - - - - - 60,000 11,800 5
2. Northern ProvinceBombali 21 2 8 18 4 21 78 - 68,100 15,800 4Kambia 3 1 5 5 5 65 - 217,000 8,300 26Koinedugu 1 1 - 5 0 5 65 - 103,000 11,400 9Port Loko 1 1 1 9 0 10 316 - 176,500 9,300 19Tonkolili 2 5 5 7 1 9 84 - 69,500 17,400 4
Sub-total 28 9 15 44 10 50 808 0 97,500 11,800 8
3. Southern ProvinceBo 10 14 38 32 13 10 130 1 24,500 4,800 5Bonthe 3 7 2 2 - 2 27 - 122,000 12,200 10Moyamba 2 14 2 6 - 6 59 - 158,000 19,800 8Pujehun - 8 - - - - - - closed
Sub-total 15 35 42 40 13 18 216 1 47,300 8,100 6
4. Western Area 52 4 - 84 23 309 1105 12 9,500 1,200 8
TOTAL 95 48 57 18 46 377 1929 13 25,100 4,200 6 ov
Onx
(ann4b.xls)


REPUBLIC OF SIERRA LEONEINTEGRATED HEALTH SECTOR INVESTMENT PROJECT
Government Financed Health Sector Expenditures in Sierra Leone (1990/91-1995/96)(millions of Leones)
90/91 91/92 92/93 93/94 94/95 95/96*Nominal ExpendituresRecurrent Expenditures in Health 769.9 1545.3 2479.5 4406.5 5342.9 5417.4Investment Expenditures in Health 12.5 17.0 291.0 384.0 69.0 773.2Total Expenditures in Health 782.4 1562.3 2770.5 4790.5 5411.9 6190.6
Recurrent Exp ./Total Recurrent Exp. 2.80% 3.30% 3.90% 5.84% 6.47% 6.21%Investment Exp./Total Investment Exp. 0.20% 0.10% 1.66% 1.72% 0.35% 4.75%Total Exp. in Health/Total Exp. 2.30% 2.50% 3.41% 4.90% 5.29% 5.98%
Recurrent Health Expenditure/GDP 0.42% 0.52% 0.63% 0.92% 0.96% 0.84%Investment Health Expenditure/GDP 0.01% 0.01% 0.07% 0.08% 0.01% 0.12%Total Health Expenditure/GDP 0.43% 0.53% 0.70% 1.00% 0.97% 0.96%
Per Capita Expenditure in Health (1986/87 Le)
Real ExpendituresReal Recurrent Expenditure inHealth 19.17 18.87 21.99 32.29 33.06 29.28Real Investment Expenditure in Health 0.31 0.21 2.58 2.81 0.43 4.18Real Total HealthExpenditures 19.48 19.08 24.58 35.10 33.49 33.46
Memorandum Items:
GDP (millions of Leones) 181624 295259 395057 480113 558006 645400DomesticInflation(Index1986/87= 100) 957 1901 2551 3010 3473 3876 :Population (Millions) 4.2 4.3 4.4 4.5 4.7 4.8 M
Allocations for FY 1995/96. AU other yas a1c l expeidiur. Sources: Deparbines of Fnance; World Bank Repoit No. 1261 8-SL
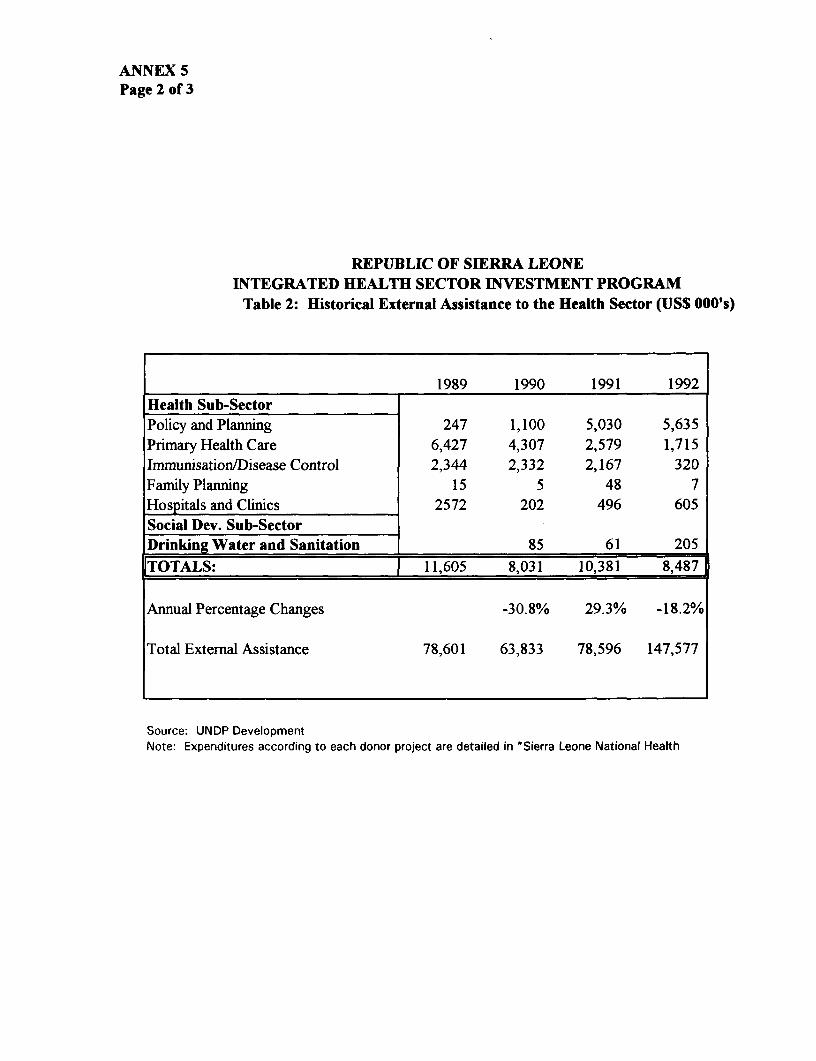
ANNEX 5Page 2 of 3
REPUBLIC OF SIERRA LEONEINTEGRATED HEALTH SECTOR INVESTMENT PROGRAM
Table 2: Historical External Assistance to the Health Sector (US$ 000's)
1989 1990 1991 1992Health Sub-SectorPolicy and Planning 247 1,100 5,030 5,635Primary Health Care 6,427 4,307 2,579 1,715Immunisation/Disease Control 2,344 2,332 2,167 320Family Planning 15 5 48 7Hospitals and Clinics 2572 202 496 605Social Dev. Sub-SectorDrinking Water and Sanitation 85 61 205
|TOTALS: | 11,605 8,031 10,381 8,487
Annual Percentage Changes -30.8% 29.3% -18.2%
Total External Assistance 78,601 63,833 78,596 147,577
Source: UNDP DevelopmentNote: Expenditures according to each donor project are detailed in "Sierra Leone National Health

ANNEX 5Page 3 of 3
REPUBLIC OF SIERRA LEONE
INTEGRATED HEALTH SECTOR INVESTMENT PROJECT
Estimates of 1989/90 Household Expenditures on Health Care
Household Expenditure Leone US$ Percent
Monthly household expenditureFood 6,839 37.8 60.0%Beverages & tobacco 430 2.4 3.8%Medicine & medical care 359 2.0 3.1%Other non-food expenditure 3,769 20.8 33.1%
Total 11,398 63.0 100.0%
Annual household expenditure 136,774 756Total national household expenditure 86,840,933,168 485,765,266Total household expenditure on health (3.1%) 2,766,456,035 15,298,656
Per Ca ita Ex enditure
Monthly per capita expenditure 1770 9.8Monthly per capita expenditure on health (3.1 %) 56 0.31Annual per capita expenditure 21,238 117.4Annual per capita expenditure on health (3.1%) 669 3.7
Notes: - The average household size was 6.44 persons.- The 1990 population estimate was 4.1 million persons.- Parallel market exchange rate (1990 ann.av.) US$1=Lel81.- These estimates are likely understatements of true private expenditures, since other sources of
private health expenditure are not included, e.g. industry, personal loans).
Source: Report on Survey of Household Expenditure and Household Economic Activity.Central Statistics Office. Government of Sierra Leone. December, 1993.

ANNEX 6Page 1 of 9
REPUBLIC OF SIERRA LEONEINTEGRATED HEALTH SECTOR INVESTMENT PROJECT
Communique of theSocial Sectors Round Table Consultations
Freetown, Sierra LeoneMay 17 to 20, 1994
1. The Social Sectors Round Table was officially opened by His Excellency the Chairman,National Provisional Ruling Council (NPRC) and Head of State, Captain Valentine E M Strasserthereby demonstrating Government's firm commitment to social sector reform with the objectiveof raising the level of human development.
The National Action Plans
2. The Government of Sierra Leone (GOSL) presented National Action Plans for theEducation and Health Sectors at a UNDP sponsored Social Sectors Round Table convened inFreetown from May 17 to 20, 1994. Its purpose was to promote dialogue and to fosterconsensus among Government, NGOs, the donor community and other key stakeholders, and togenerate support for the Government's health and education sectors reform programmes.
3. The National Education Action Plan (NEAP), underpinning the recently introduced 6-3-3-4 Education Reform, is to improve quality and quantity of basic education and technical trainingsystem. NEAP focuses on three main priorities: primary and junior secondary level education,both formal and non-formal; enhancing the management and administration of the educationsystem, especially increasing decision making powers at the local level; and training of educationsector personnel.
4. The core program of the National Health Action Plan (NHAP) is a comprehensiveframework of technical and support services emphasizing primary health and supportive hospitalservices to improve access and quality of care. The main priorities are maternal and child healthcare, water and sanitation, and health education, whilst strengthening the sector's management,human resources and maintenance functions.
5. Taking into account likely financial constraints and implementation capacity, these six-yearplans aim for effective, efficient, and sustainable provision of services. Equitable treatment forunder-served groups - notably women, girls and the rural poor - are hallmarks of the plans. Thespecial needs of education and health services in the war affected areas were recognized and willbe addressed as soon as the security situation allows.
6. The compelling economic and humanitarian rationale for immediate implementation of thesocial sector reform agenda has led GOSL to move boldly on two fronts: delivering benefits to
ANNEX 6Page 2 of 9
individuals and communities while at the same time building institutional capacity to implement,absorb and sustain massive reform.
Discussions
7. Donors responded by congratulating Government on its initiative in requesting the firstever Round Table on the social sectors. Endorsement was given to the highly participatoryprocess used to formulate and prioritize the Action Plans, which has resulted in strong localownership and commitment.
8. The sector program approach - the conceptual framework for the Plans - was commendedfor its potential to: harmonize sectoral development with macro-economic policy adjustment;integrate ongoing and projected activities whether domestically or externally financed; respond tounforeseen circumstances while maintaining direction and cohesiveness; facilitate Governmentcoordination of donor and NGO assistance; and generally maximize developmental impact. Italso enables donors to provide their assistance to specific components, geographic areas, as wellas to broader program support.
9. The importance of increasing authority and responsibility for delivering education andhealth services at district level was a central feature of both plans. Donors applaudedGovernment's determination to decentralize operations and to enhance accountability at bothheadquarters and in the field.
10. Emphasis was placed on the need for enhanced coordination within each Department, andbetween these line departments and the central coordinating agencies of Government. Thisincludes the establishment of an aid coordination unit in the Department of Development andEconomic Planning (DODEP).
11. Donors concurred with Government that achievement of ultimate objectives would be bestassured through periodic review and updating.
12. Donors responded enthusiastically and practically to GOSL's courageous strategy ofsimultaneously getting results on the ground and strengthening the institutional base.
13. Donors and NGOs offered to redirect some existing project funds and to finance somesharply focused technical assistance both to yield demonstrable progress in the field and toimprove the efficiency of Department of Education (DOE) and Department of Health and SocialServices (DOHSS) headquarters and district administrations.
14. Government was also encouraged to investigate greater use of NGOs and enhanced rolefor the private sector in financing and delivery of education and health care.
ANNEX 6Page 3 of 9
Understandings Reached
15. GOSL agreed to:
* increase the financial allocation to health and education by at least 5% per annumin real terms over the life of the plans;
* focus DOE and DOHSS activities and resources on planning, implementing,monitoring and evaluating the agreed sector programmes;
* review the progress and content of the programmes in collaboration with donorsand other stakeholders on a regular basis; and
* reorganize both Departments at central and district levels to facilitateimplementation of their programmes. These changes would include:
* development of implementation and monitoring arrangements to preclude the needfor separate project implementation units;
a coordination of information flow with NGOs and donors, in collaboration with theDODEP;
decentralization of responsibility and authority to enhance local management,accountability and sustainability of service delivery.
16. NGOs agreed to:
work fully within the framework of NEAP and NHAP; and
share their information and technical capabilities with Government.
17. Donors agreed to:
* work exclusively within the framework of NEAP and NHAP, as much as possible,using common implementation modalities;
* participate with Government in joint review and planning processes;
* provide financial and/or technical assistance in support of NEAP and NHAP;

ANNEX 6Page 4 of 9
* meet the estimated financing gaps in both sectors ($25 million for the initial threeyears in education; $37 million for the next five years of the health program).
Next Steps
18. GOSL will:
* prepare detailed implementation plans for each of the components of the sectorprogrammes, including organizational change, financial management and humanresources policies and incentives by the end of 1994;
* develop guidelines on the use of technical assistance to best promote local capacitydevelopment and utilization and program sustainability;
* follow up with donors to ascertain what is needed to realize their full support;
* develop a detailed schedule for preparation of the sector programmes, and distributethis to donors within the next month; and
* produce a status report on the programmes, including donor commitment, by the nextConsultative Group Meeting in 1995.
19. NGOs will:
* provide information to Government on their current and proposed activities; and
* adapt their existing development assistance to accord with NEAP and NHAP.
20. Donors will:
prepare their information requirements to discuss with Government;
adapt the scope and modalities of their development assistance to accord with theneeds of the NEAP and NHAP; and
* mobilize their resource commitments for the NEAP and NHAP.
21. In light of the success of this meeting, it was proposed to reconvene a follow-up RoundTable Consultation on the Social Sectors in 18 months, within the wider context of povertyalleviation.

ANNEX 6Page 5 of 9
22. The meeting was attended by representatives from France, the United Kingdom, theUnited States of America, the European Union, Food and Agriculture Organization, IslamicDevelopment Bank, United Nations Children's Fund, United Nations Population Fund, UnitedNations Education Scientific and Cultural Organization, World Food Program, World HealthOrganization, World Bank, International Monetary Fund, United Nations Development Program,the Government of Sierra Leone - Departments of Health and Social Services, Education,Development and Economic Planning, Finance, and also international and national NGOs andother organizations.

ANNEX 6Page 6 of 9
COMMUNIQUE
SOCIAL SECTOR DONORS MEETINGBINTUMANI HOTEL16 - 18 OCTOBER, 1995
1. The Social Sectors Donors Meeting, a follow up of the May, 1994, Social Sectors RoundTable Consultations was officially opened by His Excellency Captain Valentine E.M. Strasser,Head of State and Chairman of the National Provisional Ruling Council thereby giving credenceto Governments strong commitment to Social Sectors reform.
2. Sierra Leone Government reported on progress, in the Education and Health Sectors, onthe understandings and agreements reached at the May, 1994, Consultations.
3. The National Education Sector Policy and Priorities were presented:
4.The Health Sector Priority activities and incremental costs for Fiscal Year 1996 (For WesternArea District and Central Level Program) activities; budgets; implementation arrangements andmonitoring indicators.
5.Government of Sierra Leone is strongly committed to Social Sectors reform including theprocess of democratization already started and which will be leading to the reactivation, of thedistrict councils, which will give the districts the authority to plan, implement and monitor theirrespective Health and Education programmes.
6.Government increased its financial allocation to the Health and Education Sectors by at least5% per annum in real terms, with effect from the 1994/95 fiscal year; the increases will besustained over the life span of the Health and Education Action Plans.
7.The Education and Health Sector have benefited from the Social Action and Poverty Alleviation(SAPA) activities; School rehabilitation; pedagogical material and equipment; hospital and healthcenter refurbishment; supply of essential drugs on a cost recovery basis and the supply of basicequipment.
8. Government highlighted its commitment to address the special and dire needs of theeducation and health sectors affected by the rebel war which has a devastating effect on thesources of Government revenue through the disruption of economic activities.
9. Government agrees to convene a similar Social Sector Donors Meeting each year ofNHAP and NEAP Implementation to appraise Donors and NGOs of progress made to presentsector plans and Budgets for the following year, and to encourage continued commitment andsupport to the implementation of the two national plans.

ANNEX 6Page 7 of 9
IN THE EDUCATION SECTOR
Donors and NGOs:
1. Commended the DOE on progress made since the last Donors Round Table for the socialsector in May 1994. They recognized the significant effort involved in the production ofthe new education sector policy and the difficulties the DOE has faced over the last 18months in responding to the emergency needs of the displaced school-aged population.
2. Appreciate the steps which have been taken thus far towards the restructuring the centraladministration of the DOE, and recognize that initial steps have been taken to review theNational Education Plan and Policy and to improve efficiency in the tertiary sector.
3. Also appreciate that further work is needed in relation to prioritization, phasing anddetailed costing in order to operationalize the new education policy. A master plan whichwill be completed by 1996 will serve as the basis for medium-term coordination andcooperation with donors.
4. Are in full agreement with the priority for improving both the quality of, and access to,basic education, (formal and non-formal) paying particular attention to the needs of girls'disabled and disadvantaged and gifted. They would wish to emphasize the importance ofquality primary education as a prerequisite for the successful development of qualityeducation thereafter.
5. Recognized the positive role of the DOE during the last 18 months in ensuringcoordination of donor contributions but would stress the need for further attention todeveloping this partnership.
6. Recognized that central to the implementation of the whole new education policy is theefficient management of the teacher resource; donors support the establishment of ateaching service commission, the continuing professional development of teachers, andcontrol of the payroll.
IN THE HEALTH SECTOR
Donors and NGOs commended the Department of Health on the progress made on theinitiative in convening this Meeting as a follow up to the Social Sectors Roundtable Consultationsof May 1994. The participants congratulated the DOH on the quality of work which has goneinto the preparation of the working documents including the detailed plans and budgets forWestern Area District activities, Central Program support activities, and the Estimates ofResource Requirements for 1996, as well as other supporting documentation.
ANNEX 6Page 8 of 9
Donors and NGOs praised the efforts of the Government in restructuring the Department,strengthening management capabilities, and in the progress made in the decentralization of healthcare management and delivery. Participants also applauded Government in setting up a central aidcoordination unit in the Department of Development and Economic Planning and also theDepartment of Health for putting in place a Donor Coordination Secretariat.
Donors and NGOs:
1. agreed with the Government's efforts to continue health care throughout the country, withspecial emphasis on districts with influx of the displaced, while emphasizing keyinvestment at central level and in the Western Area as the foundation for extension intothe areas of the country in subsequent years.
2. restated their commitment to work within the framework of the NHAP, and recognizedthe important role of DOH in managing the process of overall planning for the sector.Notwithstanding this, participants also encouraged the Department to continue with itsefforts build capacity at both central and district levels needed for the efficientimplementation of the NHAP.
3. noted the excellent working relationship enjoyed with the Department and suggested thatcontinued dialogue and consultations between DOH and partners in the health sector beheld periodically.
During discussions, donors and NGOs also highlighted the need for information sharingand joint program review with a view to maximize use of resources.
Recognizing the health needs of the country and the commitment on the part ofGovernment to share the cost of implementing the NHAP, donors and NGOs indicated that, theywould continue their current support to the overall health sector prograrn including the emergencyactivities, at the minimum amount of US$6.9 million. An additional US$5.75 million minimumwas committed in support of the incremental core program activities for 1996. Assuming that theoverall core NHAP Program will cost approximately US$24 million for 1996 and thatGovernment will contribute approximately US$7 million; a projected gap of at least US$4.5million still exists. Government will take steps to fill this financing gap through discussion withdonors, NGOs and its other partners in the health sector. To this end, those unable to quantifytheir organizations' contributions to NHAP implementation, committed themselves to provide thefinical information to the DOH as soon as available.
In conclusion, the donors and NGOs reiterated their support for the Departments effortsand in the implementation of the NHAP.
The meeting was attended by representatives from the United Kingdom, United States ofAmerica, European Union, United Nations Development Program, United Nations Children's

ANNEX 6Page 9 of 9
Fund, United Nations Population Fund, United Nations Education, Scientific and CulturalOrganization, United Nations High Commission for Refugees, World Health Organization,African Development Bank, Islamic Development Bank, World Bank; the NGOs - AFRICARE,Choithram Charitable Trust, Christian Children's Fund, Sierra Leone Red Cross, Action Aid, PlanInternational, AICF, Christian Health Association Sierra Leone, German Leprosy ReliefAssociation, Marie Stopes, Plan Parenthood Association; the Sierra Leone Government -Departments of Health and Social Services, Education, Development and Economic Planning,Finance, Audit, State Law Office and the University of Sierra Leone.


ANNEX 7Page 1 of 7
REPUBLIC OF SIERRA LEONE
INTEGRATED HEALTH SECTOR INVESTMENT PROJECT
Economic Analysis and Framework for Prioritization of the Core Program of the NationalHealth Action Plan (NHAP)
This analysis of the Integrated Health Sector Investment Project (IHSIP) is based on thepublic expenditure reviewl and the health sector policy (NHAP core program), and takes intoaccount existing resource constraints.
The Sector Investment Approach (SIP) does not lend itself to assessing the rate of returnof the IHSIP because: (i) the IDA level of funding and the breakdown by expenditure categoriesare to be determined on an annual basis; and (ii) IDA funds are fungible and will be used as alast resort source of financing. It is therefore not feasible to prospectively quantify project costsand benefits. For this reason, a detailed analysis of the soundness of the entire national sectorinvestment program, as presented in the sector policy (NHAP core program), was carried out.
Sector-wide review of public expenditures
Focus on service provision. The review of public expenditures has focused on restoringthe GOSL's capacity to provide basic services, specifically in the health and education sectors.2
Consequently, DOH has developed its health sector strategy-as presented in the NHAP-in thegeneral frame and constraints offered by the review. As a result, the sector refocused its plansgiving greater emphasis to cost-effective interventions, such as preventive and curative primaryhealth services, and abandoned efforts to establish a new tertiary facility in the form of ateaching hospital at Jui near the capital Freetown. Efforts have been stepped up to diversify thefunding of the public health sector and to increase private health care provision by activelyfacilitating NGO activities3 and by starting privatization of tertiary services4.
The status-quo alternative (i.e. no change in Government intervention and donorsupport). Regarding the provision of preventive services, such as immunization or vector
I Sierra Leone: Public Expenditure Policiesfor Sustained Economic Growth and Poverty Alleviation. February 16, 1994.Cf. Report No. 12618-SL.
2 Sierra Leone: Policiesfor Sustained Economic Growth and Poverty Alleviation. May 14, 1993. Cf. World Bank Report No.11371-SL.
3 In early 1995, the DOH established a donor liaison office. It is now actively assisting a local foundation in the constructionof a new 56-bed hospital near Freetown by facilitating duty-free status and expediting customs and other administrativeprocedures. DOH is liaising with all NGOs in order to avoid overlap and duplication by the public sector in the provisionof health care services.
4 A portion of the Connaught Hospital, termed the "Annex," is providing above-standard services (higher staff/client ratio,air-conditioning, better food, etc.) and is now financed by collecting increased fees.

ANNEX 7Page 2 of 7
recognized. With regard to primary health care and related referral services, a good case can bemade for the public provision of these services, especially at the outreach, on the basis of marketfailures. It is reasonable to assume that maintaining the status quo in the sector would result in afurther deterioration of the already poor provision of health services to the general public: (a)consumers in rural areas would not gain access to acceptable health services; (b) the overallquality of health services, particularly at primary level, would remain low; (c) the lack ofinformation would continue to hamper rational decision-making by consumers; (d) expendituresby private households on traditional healers and drug peddlers could not be recouped in favor ofbetter services; and (e) preventive services such as immunization or vector control would continueto be supplied below optimal levels.
Macroeconomic environment
Budgetary impact. The Project's program evaluation and programming cycleincorporates a mechanism, on an annual basis, to review together with Government of SierraLeone (GOSL) and other donors not only the IHSIP performance but the entire sector program-under the leadership of GOSL- and to coordinate both recurrent and investment healthexpenditures with the Government's overall budget. The project therefore will facilitate macro-economic stability while at the same time contributing to the gains in the sector and to theachievement of a reasonable level and composition of health expenditures (see figures 2.2 and 2.3in the SAR).
Marginal cost of funds. No country-specific estimate for the marginal cost of publicfunds is available. However, to overcome existing data limitations, the GOSL has committeditself during Negotiations to conduct a national survey on household expenditures and householdeconomic activities, and to develop a comprehensive health sector financing plan latest by the endof 1997, addressing the question of the public/private mix of services and diversification of sectorfinancing. Given that there is a premium on public income (since, generally speaking,governments resort to distortionary taxation for revenue) and in order to ensure sustainability ofthe health sector reform, the GOSL in the context of the IHSIP intends to upgrade and streamlinevarious existing cost recovery measures into a more coherent and efficient system.
Cost effectiveness
No specific data are available for Sierra Leone regarding the distribution of deaths byspecific cause, age and sex. However, it can be assumed that the country's mortality patternfollows the model used for sub-Saharan Africa, as it is the case in neighboring Guinea for whichpreliminary data exist from an ongoing study. Similarly, intervention costs have been estimatedfrom NHAP costs, literature and ongoing studies.

ANNEX 7Page 3 of 7
NHAP Program: Unit cost by level of intervention (1996-2000)
Estimated % of Five-yearCost Total Beneficiaries Unit cost(US$ (million) (US$/beneficiary)
million)
PRMARY HEALTH CARE 77.1 55.8 5.0 15.3
Public Health ServicesMaternal and Child Health 14.2 10.3 2.0 7.0Control of Communicable Diseases 15.4 11.2 5.0 3.1
Sanitation and Safe Water 12.0 8.7 5.0 2.4Nutrition 9.0 6.5 1.0 9.1Health Education/Communication 7.0 5.1 5.0 1.4
Essential Clinical ServicesTreatmentofCommonAilments 19.5 14.1 5.0 3.9
SEcoNDARY HEALTH CARE 25.1 18.2 5.0 5.0
TERTiARY HEALTH CARE 13.1 9.5 5.0 2.6
ADMINISTRATION 22.8 16.5 5.0 4.5
TOTAL 138.1 100 5.0 27.4
The NHAP activities were compared with activities of the minimum package of care,
selected on the basis of demonstrated favorable cost-effectiveness ratios, and presented by the
World Bank in two major publications, i.e., Better Health in Africa (1994) and World
Development Report (1993). The table below demonstrates that NHAP activities concur with the
Bank's recommendations and are economically justified.

ANNEX 7Page 4 of 7
Health system level/NHAP Program/ In NHAP in In BHA Package In WDR93 PackageIntervention or Service (Y/N) NHAP and/or Priorities (Y/N)
Core Y/N Y-C ClinProgram Y-P Pub
(Y/N) and/or WDR PrioritiesTECHNICAL PROGRAMSA. PRIPMARY CARE _
1. Maternal and child healthAnti-natal Y Y Y Y-CDelivery Y Y Y Y-CPost-natal y y y Y-CMicro-nutrient supply Y Y Y Y-PFamily planning Y Y Y Y-CSchool health Y Y Y Y-PORT Y Y y Y-CGrowth monitoring & promotion Y Y Y NBreast feeding Y Y Y Y-P
2. Common ailmentsTreatmentVReferral Yr-2 y 2
Drugs/Supplies Y Y Y YFirst Aid/Referral YY-2 2 __
Education on food selection & Y Y Y Y-PpreparationPublic and patient info. Y Y Y Y-P
3. Communicable disease controlImmunization
BCG Y Y Y YEPI Y Y Y YYellow Fever Y Y N YHepatitis B N N3 N Y
Preventive servicesOnchocerciasis spray Y y4 Y NTB Chemo. Y Y ? ?Blood bank safety Y Y' Y5 NAlDS/STDs N Y Y N
Curative services
TB_ Y Y Y YLeprosy __N6_N N
STD Y _ Y Y YARI Y Y Y YHelminths _ _ Y
1 Basic trauma, maaa, diarrhea, local infection.2 Assessment, advice, alleviation of pain, treatment of infection and minor trauma.3 Cost and feasibility in Sierra Leone to be reviewed.4 Maintenance after devolution.5 Not to imply 100% testing.6 To be further reviewed for relative cost-effectiveness; not clear whether costs included in NHAP.

ANNEX 7Page 5 of 7
Health system level/NHAP Program/ In NHAP In In BHA Package In WDR93 PackageIntervention or Service (Y/N) NHAP and/or Priorities (Y/N)
Core Y/N Y-C ClinProgram Y-P Pub
(YIN) and/or WDR Priorities4. Water sanitation
Well digging Y Y Y NLatrine construction Y Y Y NPiped water system y7 N N NSewage system y6 N N NSolid waste y__2 N N N
5. Nutrition & dieteticsNutrition education Y Y Y Y-PNutrition rehabilitation Y Y Y Y-C (0-5 wrs.)Diet therapy y N8 N NMicro-nutrients
Vitamin A N N9 Y Y-PIodine Y Y Y Y-P
6. Health education & communication _
Community health education Y Y Y Y-PIOPrinted materials Y Y ? ?Drama and songs Y Y ? ?Mass media Y Y Y YSchool health education Y Y Y Y
B. SECONDARY CAREGeneral in-patient services Y Y" Y yl2
Mental health care Y y13 N NLimited care for chronic diseases Y N Y YTB treatment Y Y Y Y
C. TERTIARY CARE
Various specialist care Y N14 N NPsychiatric care Y N15 N NClinical lab Y Y N NResearch & data collection Y N y6Y
SUPPORT PROGRAMSA. DRUGS AND SUPPLIES
Selection/Quantification Y Y Y y-p17
7 Responsibility of Department of Works.8 Dietetics & diet therapy to be moved to secondary care, as non-care interventions.9 To be reviewed for relevance in Sierra Leone.10 Health education and communication interventions were included in the WDR interventions for alcohol,
tobacco, and school health11 Resources unlikely to permit more than 12 below.12 Assessment, advice, alleviation of pain, treatment of infection and minor trauma, other treatment as resources
permit.13 Mental health services at all levels merit further reflection; there is no consensus in the NHAP Task Force on
them.14 Future needs for specialist staff merit careful review, as many existing staff are soon to retire.15 Mental health services at all levels merit review.16 Public health monitoring and surveillance, provided outside tertiary care.

ANNEX 7Page 6 of 7
Health system level/NHAP Program/ In NHAP in In BHA Package In WDR93 PackageIntervention or Service (Y/N) NHAP and/or Priorities (Y/N)
Core Y/N Y-C ClinProgram Y-P Pub
(Y/N) and/or WDR PrioritiesProcurement Y Y Y Y-PStorage/Inventory Y Y Y Y-PDistribution Y Y Y Y PRational drug prescription & use Y Y Y Y-PCost recovery/Pricing Y Y Y Y-PQuality control Y y y y.pDrug regulation/Control Y Y Y Y-PNGO, private sector N Y18 y Y-P
B. NATIONAL FOOD, ENVIRONMENT, &
CLINICAL LAB SERVICE
Advice to clinicians & policy makers Y N N NAnalysis of lab samples Y N N NTraining lab staff Y Y N NQuality control of lab services Y N N NPromotion of safe blood Y yN9 y20 NForensic analysis Y N N NRegulation and enforcement Y N N N
C. MAINTENANCE & REPAIR (M&R)
DOH-level unit Y Y Y NDistrict units Y Y Y NNorms for M&R/Equipment N Y Y YPlanning & M&R skills N Y Y N
D. HuMAN RESOURCE MANAGEMENT
Long-term planning Y Y Y NTraining plans Y Y N NCoordinating mechanism for Y Y Y Ntraining/management developmentDevelop HRM capacity Y Y Y NEmployee relations strategy/pay Y Y Y NComputerized PMIS Y Y N NChanging mix of staff N y21 y yRedeploying staff N Y Y YChanging training curricula N Y Y YLeadership/Supervision N Y Y N
E. PMISU
Training staff in info. management Y Y Y NEstablish district M&E capacity, Y Y Y Nincludin at hospitalsOperational research Y Y Y Y
17 Drugs and supply services were included implicitly as part of the WDR essential care package.18 Private sector roles in marketing and distribution of drugs merit review.19 Quality control under lab services; promotion belongs under health education.20 May not be a lab service; NHAP foresees provision of safe blood. BHA encourages promotion of safe blood, but
does not see provision of safe blood as a priority intervention.21 Task Force endorsed a Y, but urges that the subject be approached with care.

ANNEX 7Page 7 of 7
Health system level/RAP Program/ In NELA in In BRA Package In WDR93 PackageIntervention or Service (Y/N) NLAP and/or Prioritis (Y/N)
Core YIN Y-C CInProgram Y-P Pub
(Y/N) and/or WDR PrioritiesCollection/dissemination of Y N N Ninfo./reportsAsdst in distict health plans Y Y Y YEvidemiological data N Y Y YMonitoring/health finance N _ Y YSupport community management N Y Y Y
22 Organizational locus in DOH merits serious consideration.


ANNEX 8Page 1 of 11
REPUBLIC OF SIERRA LEONE
INTEGRATED HEALTH SECTOR INVESTMENT PROJECT
Detailed Description of Technical and Support Programs
1. This description of the technical and support programs of the National Health Action Plan(NHAP) is adapted from the Social Sectors Round Table document "Towards Better Health inSierra Leone: A Proposal for Financial Assistance from The International Community". Thisdescription identifies differences between the total NHAP and the core program developed inMarch 1994, and projects costs for the first five years of implementation. Further detaileddescriptions are found in an Annex to the Social Sectors Round Table document, and in theNHAP itself The programs are as follow:
Technical Programs
Primary Health Care
1 - Maternal and Child Health2 - Treatment of Common Ailments3 - Control of Communicable Diseases4 - Sanitation and Safe Water5 - Nutrition6 - Health Education/Communication7 - Secondary Health Care8 - Tertiary Health Care
Support Programs
1 - Drugs and Medical Supplies2 - National Food, Environment and Clinical Laboratory Service3 - Maintenance and Repair4 - Human Resource Management5 - Planning, Monitoring, Information and Statistics Unit6 - Central Administration
Primary Health Care Programs
2. The objectives and services for each of the six primary health care programs are describedin paragraphs 5-23 below. These programs will be implemented through a strengthened primaryhealth care delivery system. There may appear to be some overlap in the definition of programs;this does not occur in practice at the district level, since the package of services will be deliveredthrough the same personnel. Successful implementation will depend on an implementationstrategy which emphasizes the:

ANNEX 8Page 2 of 11
(a) revitalization of health centers and district hospitals, and the effective operation ofDistrict Health Management Teams;
(b) gradual conversion of PHU staff to more multi-skilled health care personnel;
(c) effective coordination with the private voluntary sector in respect to the design ofPHU staff training, the establishment of service standards, and monitoring servicedelivery throughout the country;
(d) establishment of guidelines for specific services and staff training;
(e) elimination of "vertical" programs; and
(f) sensitization and mobilization of communities for improved health care.
3. Successful implementation also depends upon the effective integration of health educationwith the other technical programs and the establishment of close links with the Department ofEducation to expand school health education.
4. The key elements of improved primary health care delivery are:
(a) improved performance of front-line staff, in particular, TBAs, midwives, MCHAides, through training and the provision of drugs, equipment and supportservices;
(b) increased service coverage and improved service quality; and
(c) behavioral change at the community level.
Technical Program 1: Maternal and Child Health
5. Deplorable child health and poor maternal health are amongst the most pressing healthproblems facing Sierra Leone. The Maternal and Child Health (MCH) program addresses theobjectives of reducing maternal and child morbidity and mortality, and focuses on six key servicesas follow:
(a) antenatal care, safe delivery, post-natal care;(b) family planning;(c) school health services;(d) oral rehydration therapy (diarrhea control);(e) growth monitoring and promotion; and(f) breast feeding.

ANNEX 8Page 3 of 11
6. All of these services are incorporated in the core program which is estimated to cost $10.0million before contingencies. Given existing Government and donor commitments to MCH, theincremental costs of the MCH core program are estimated at $3.2 million.
7. The key weaknesses in the current MCH program which need to be addressed relate topoor service coverage at community level, in particular growth monitoring, family planning andschool health services.
Technical Program 2: Treatment of Common Ailments
8. Common ailments in Sierra Leone include those with high prevalence, such as malaria,helminths, STDs and injuries. The objective is to reduce the general levels of illness and death byimproving diagnosis and treatment at PHUs. Although there is no specific technical program,there are a number of services which contribute to this objective as follow:
(a) clinical diagnosis, treatment and referral;(b) the provision of essential drugs;(c) first aid for injuries;(e) education on food selection and drug abuse;(f) distribution of food supplements;(g) programs to reduce drug abuse; and(h) public and patient information services.
9. The core program includes:
(a) the treatment and referral of basic trauma, malaria, diarrhea and local infections;(b) assessment and advice on the alleviation of pain, and the treatment of infection and
minor trauma;(c) the provision of drugs and supplies;(d) education on food selection and preparation; and(e) public and patient information services.
10. The total cost of the core program for common ailments is estimnated at $15.6 millionbefore contingencies. The incremental costs requiring funding are estimated at $8.8 million.
11. One key issue is the potential overlap with other programs, such as nutrition and healtheducation, which could result in a waste of resources.
Technical Program 3: Control of Communicable Diseases
12. The control of communicable diseases covers some of the most severe health problems inSierra Leone, specifically, tuberculosis, measles, polio, tetanus and pertussis. The overallobjective of this program is to reduce morbidity and mortality rates, particularly in infants and

ANNEX SPage 4 of 11
children under-five. In order to achieve this objective, the NHAP envisages a comprehensiveapproach to CDC which incorporates immunization, curative and preventive services.
13. All preventive services in the NHAP are included in the core program, all immunizationservices except rabies and meningitis, and all curative services excluding leprosy. In addition, thecore program explicitly adds AIDS and other STDs to the priority preventive services. The totalcost of the core CDC program is estimated at $11.6 million (before contingencies), withincremental costs to be funded estimated at $3.0 million.
14. Outstanding issues to be addressed include weaknesses in cold chain management andcoordination with NGOs active in CDC programs.
Technical Program 4: Sanitation and Safe Water
15. Access to safe water and sanitation in Sierra Leone is very low, representing only 22%and 35% of the rural population respectively. The overall objective of this program is to alleviatethe current unsanitary living conditions and reduce food contamination by improving access tolatrines and safe water.
16. The NHAP sets out a comprehensive program for sanitation and safe water whichcomprises well digging, latrine and toilet construction, and the extension and improvement ofpiped water and sewage/solid waste disposal. Of these services, only well digging and latrineconstruction are included in the priority core program as the remainder are the responsibility ofthe Department of Works. The total costs of the core program are estimated at US$10.0 million(before contingencies) and, of this amount, the incremental costs to be funded are estimated atUS$1.1 million.
17. A key element of the program is the cooperation of various agencies, including NGOs, andcommunities in expanded programs of well and latrine construction. The NHAP recognizes thekey role of communities in both the construction and maintenance of wells and latrines.Accordingly, provision has been made to train village residents in well maintenance.
Technical Program 5: Nutrition and Dietetics
18. The poor nutritional status of the population, particularly children, has been identified as amajor health problem in Sierra Leone. Studies show that malnutrition is a factor in more than onethird of infant and child deaths. Further, the poor quality and low quantity of food intake,including breast milk, retards growth, reduces immunity, creates learning disabilities anddepresses work productivity. In order to address these problems, the main objective of theoverall NHAP program is to reduce the prevalence of childhood malnutrition by providing acomprehensive range of services comprising:
(a) nutrition education and rehabilitation;(b) food supplementation and fortification;

ANNEX 8Page 5 of 11
(c) diet therapy;(d) research; and(e) food control.
19. The emphasis in the core program will be on nutrition education and rehabilitation, andthe provision of iodine micro-nutrients. The total cost of the core program is estimated at US$6.2million (before contingencies), of which incremental costs to be financed amount to an estimatedUS$1.0 million.
20. Nutrition services will be provided through the PHU network and integrated with otherservices at this level. One key element of this program, therefore, will be to increase theperformance of PHU staff to provide counseling, supplements and support services. Finally, oneoutstanding issue is the need to develop a nutrition policy and convert this into a detailed plan.
Technical Program 6: Health Education and Communication
21. Weaknesses in health education and communication are a key factor in many healthproblems in Sierra Leone. This program, therefore, contributes to the effectiveness of the othertechnical programs, although it currently lacks focus. The objective in the NHAP is to develop anationwide health education program which underpins the other technical programs. The NHAPoutlines a number of services in order to achieve this objective, as follow:
(a) community health education;(b) production of printed materials;(c) drama presentations and songs;(d) mass media; and(e) school health education.
22. All of these services have been included as a priority in the core program. The total costsof the core program are estimated at US$4.0 million (before contingencies), of which US$0.5million represents incremental expenditure to be funded.
23. Outstanding issues which require urgent attention include the development of an IECstrategy and the effective mobilization of community motivators and the communities with whomthey work.
Technical Program 7: Secondary Health Care
24. Currently, district hospitals are providing very limited specialized care because of grosslyinadequate facilities, equipment, materials and inappropriately trained personnel. As a result,hospitals have tended to focus on primary health care services. The main objective of secondaryhealth care, therefore, is to provide a referral service for the peripheral health units centered on

ANNEX SPage 6 of 11
the district hospitals. The intention is for district hospitals also to play a role in monitoring andfollowing up patients who have been referred back to the PHUs after treatment.
25. This program involves four health services under the NHAP, as follow:
(a) hospital services;(b) mental health care;(c) drug information and poisoning services; and(d) disaster preparedness.
26. The core program includes only the first of these services: emphasizing the provision ofbasic in-patient care, some limited chronic care and curative care, and the treatment oftuberculosis. The estimated cost of the core program is US$18.6 million (before contingencies),with incremental costs to be financed estimated at US$3.5 million.
27. The key elements of improved secondary health care include:
(a) improved staff performance through training, better infrastructure, equipment andsupport services;
(b) the rehabilitation of district hospitals; and(c) strengthened district management.
28. The secondary health care delivery system will be based on and around the district hospitalwith a capacity of 40 beds or more, manned by at least 3 doctors. Each hospital wili be equippedto handle basic medical and surgical emergencies and all routine clinical work. The districthospital is also expected to improve the skills and services of the PHUs by referring patients homefor outpatient care.
29. Successful implementation will depend on the rehabilitation of district hospitals, thedeployment of appropriate staff and improved management to ensure quality standards areestablished and maintained.
30. There are many outstanding issues which need to be resolved under secondary health care,in particular:
(a) attracting and retaining skilled personnel;(b) improved cost recovery through user fees and drug charges; and(c) the control of intra-mural private practice.
Technical Program 8: Tertiary Health Care
31. Tertiary health care provides a higher level of specialized care and referrals fromsecondary health care. Currently, however, the range of services offered is restricted by the lackof working equipment and trained specialists. The NHAP set out plans to establish specialist
ANNEX 8Page 7 of 11
departments for pediatrics, surgery, opthalmology, cardiology and dentistry in the larger Districthospitals.
32. None of the proposed services for tertiary care have been included under the priority coreprogram in order to ensure that additional resources are geared initially towards the basic healthneeds of the population. Existing levels of expenditure will be maintained, but no incrementalexpenditure is envisaged over the period of the plan.
33. Nonetheless, it remains a priority to analyze the cost-benefit of different tertiary careservices to determine where existing resources are best allocated. In addition, because of therelatively high costs of tertiary care, the potential for cost recovery needs to be urgentlyaddressed.
Support Program 1: Drugs and Medical Supplies
34. The majority of the technical programs rely heavily on the provision of drugs and medicalsupplies. However, the establishment of an efficient supply system is threatened by shortages ofessential drugs and a low cash recovery rate. The overall objective of this support program willbe to ensure that both essential and specialized drugs are widely available. In this regard, theGovernment has established a list of essential drugs. Specialist drugs and supplies will be suppliedto secondary and tertiary care hospitals.
35. The NHAP sets out a comprehensive approach to drugs and medical supplies including:
(a) selection and quantification;(b) procurement, storage and distribution;(c) rational drug usage;(d) improved cost recovery;(e) quality control; and(f) drug regulation.
36. All of these services are included in the core program, as well as a review of the potentialinvolvement of the private sector in marketing and distribution. The estimated cost of the coreprogram is US$11.8 million (before contingencies), giving an incremental cost to be financed ofUS$5.3 million.
37. The key elements of this support program are better availability of essential drugs,improved cost recovery and the provision of trained staff at all levels. The successfulimplementation of the drugs and medical supplies support program will require:
(a) a revitalized procurement, storage and distribution system;(b) improved monitoring and supervision at district level;(c) the appointment of specialized procurement staff, and(d) an efficient cost recovery system.

ANNEX SPage 8 of 11
38. There are a number of outstanding issues which require urgent attention, in particular, theerratic supply of essential drugs, the shortage of foreign exchange, the role of the private sector indistribution, and solutions to the poorly functioning cost recovery system. These issues should beaddressed through the development of an essential drugs policy.
Support Program 2: National Food, Environmental and Clinical Laboratory Service
39. The country has no national laboratory service despite a perceived requirement to maintainquality standards for drugs, food supply, water and the environment. Currently, analyses areperformed by separate organizations, such as the central medical stores and the district hospitals.The objective of this support program is to set up a national laboratory to monitor and teststandards in drugs prescribed, water quality, the environment and food. The program wilH providea public health laboratory service as well as services to secondary and tertiary clinical care.
40. The NHAP sets out a comprehensive set of services as follow:
(a) advice to clinicians and policy makers;(b) routine analysis of laboratory samples;(c) training of laboratory staff;(d) quality control of public and non-Government laboratories;(e) provision of safe blood;(f) provision of forensic analysis; and(g) preparation and enforcement of laws.
41. The core program includes two of these services: laboratory staff training and theprovision of safe blood. The cost of the core program is estimated at US$1.5 million (beforecontingencies), all of which is incremental expenditure to be financed.
42. Outstanding issues to be resolved include the training and acquisition of specialist staff andthe potential for laboratory services to generate revenue.
Support Program 3: Maintenance and Repair
43. Maintenance and repair is the most neglected area of all the technical and supportprograms. Physical infrastructure is dilapidated and equipment non-functional. Yet no currentexpenditure is budgeted for maintenance and repair. Accordingly, the NHAP plans to establishan ongoing maintenance program to carry out the enormous rehabilitation work required. Bothdistrict hospitals and peripheral health units will be renovated and re-equipped.
44. The services envisaged are mainly concemed with strengthening the organization,management and staffing of the maintenance and repair function. Specifically, the NHAP involvesthe establishment of:
ANNEX $Page 9 of 11
(a) a central Facilities Management and Maintenance Unit providing services inmedical electronics, civil works and transport maintenance;
(b) regional maintenance and repair departments based at the larger hospitals; and(c) district maintenance units at the district hospitals.
45. The core program covers the establishment of organizational units and facilities at thecentral and district level. The estimated cost of the core program is US$13.0 million (beforecontingencies), all of which are incremental costs.
46. The successful implementation of the maintenance and repair program under the NHAPwill require the reorganization and expansion of the maintenance and repair function, supportedby the installation of management information and control systems. At the district level, a Districtmaintenance Officer would be responsible for planning and budgeting, and monitoring contractwork.
47. Outstanding issues to be resolved include the need to develop sound maintenance policiesand procedures and to complete the construction of maintenance facilities quickly to enable themassive rehabilitation program to proceed. In addition, a skilled staffing plan needs to beprepared as this program will place major demands on staff capability.
Support Program 4: Human Resource Management
48. The human resource management function is headed by a Personnel Manager who is thesole personnel professional employed in the DOH. The scope of this function is presently limitedto recruitment and promotion services, leave and retirement administration, staff transfers andsalary administration. Pre-service training is managed separately under the various traininginstitutions.
49. The most urgent issues facing this support service are:
(a) very low remuneration in relation to both a "living" wage and compensation in theprivate and parastatal sectors. This has contributed significantly to the low moralein the health service;
(b) deficiencies in the manual personnel records system, so that there is no accurateinformation for manpower planning purposes; and
(c) weaknesses in pre-service training. There are only 11 full-time trainers in theentire DOH.
50. The NHAP intends to establish a comprehensive Human Resource Management functionresponsible for all activities related to the resourcing and development of personnel, and employeerelations. Key actions to be carried out are the:
(a) preparation of a long-term manpower plan;(b) development of managerial and technical training plans;

ANNEX SPage 10 of 11
(c) establishment of effective mechanisms for coordinating training and managementdevelopment;
(d) development of a HRM capability at head office;(e) establishment of effective employee relations strategies, with an emphasis on pay;
and(f) establishment of a computerized personnel information system.
51. With the exception of a computerized personnel information system, all of these activitiesare included in the core program. In addition, the development of leadership and supervisoryskills has been explicitly added. The cost of the core program is estimated at US$1.7 million(before contingencies), of which US$0.3 million are incremental costs to be financed (At thisstage, the costs of the overall training program for the DOH have yet to be determined, althoughsome provisional estimates for training, of US$4 million, have been incorporated under thedifferent technical and support programs).
52. The key elements of the HRM component are the development of a manpower andtraining plan, management and clinical training, and strengthening the capability of local traininginstitutions.
53. Successful implementation of the Human Resource Management program will requireacceptance of a new approach to managing staff which shifts responsibility from theEstablishments Department towards the DOH and line managers. Outstanding issues to beresolved include:
(a) the extent to which the HRM function should be "decentralized" to district level;and
(b) enhancing staff morale by taking steps to improve the working environment, staffremuneration, and attitudes towards employees.
Support Program 5: Planning, Monitoring, Information and Statistics Unit
54. The Planning, Monitoring, Information and Statistics Unit (PMISU) is the basic researchand data collection center of the health delivery system. The PMISU currently provides servicesin:
(a) training district staff in data collection;(b) operating the health management information system;(c) conducting base line surveys; and(d) managing and coordinating development projects.
55. Of these services, the management information function is currently in most need ofimprovement because of deficiencies in data collection, analysis and use both at head office anddistrict levels. This support program will involve the following services:

ANNEX 8Page 11 of 11
(a) training health staff in health and management information;(b) the establishment of district monitoring and evaluation offices;(c) setting up hospital medical records systems;(d) the design and conduct of research studies;(e) the collection and distribution of health information; and(f) support for developing district work plans.
56. Of these services, the core program includes the establishment of a district monitoring andevaluation capacity, operational research, and support for district work plans. It also includes thecollection of epidemiological data and support for community management. The estimated costof the core program US$4.8 million (before contingencies), of which US$1.5 million representincremental costs to be financed.
57. Key elements of this support program are better trained and equipped staff, strengtheneddistrict health planning and improved management information systems. In respect of the latter,the NHAP seeks to improve the gathering and dissemination of health care information at alllevels, improve understanding and help professional program managers make better qualitydecisions.
58. Successful implementation of this support program will depend crucially on the ability ofPMISU to train health staff and managers. Outstanding issues are how to ensure that theinformation is both useful for and used by management, and that all divisions cooperate in regulardata collection.
Support Program 6: Central Administration
59. This support service comprises the central administrative support services, including:
(a) financial management, including accounting(b) procurement management(c) transport administration
60. The key element of the plan are to develop and implement these systems in the mostefficient manner. Purchasing and stores management functions will be kept separate fromfinancial management and pay functions in the Department to increase transparency and hastenimplementation. The estimated cost is US$7 million before contingencies.

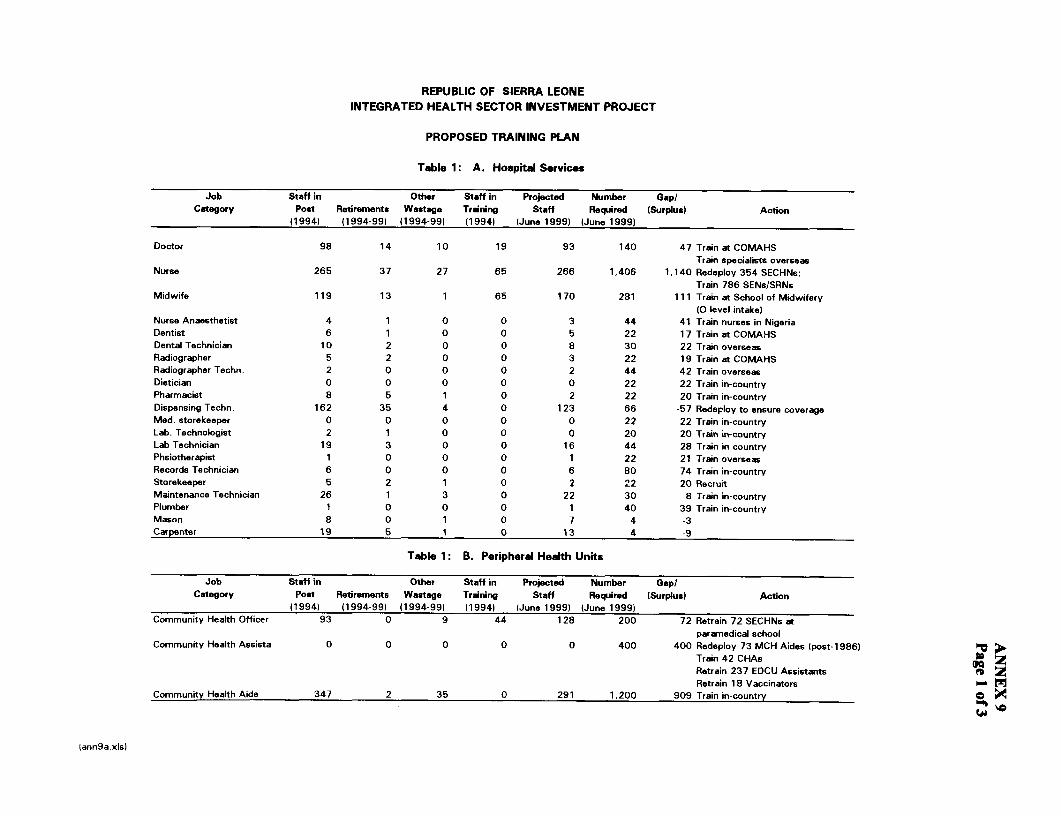
REPUBLIC OF SIERRA LEONEINTEGRATED HEALTH SECTOR INVESTMENT PROJECT
PROPOSED TRAINING PLAN
Table 1: A. Hospital Services
Job Staff in Other Staff in Projected Number Gap/Category Post Retirements Wastage Training Staff Required (Surplus) Action
( 994) (1994-99) (1994-99) (1994) (June 1999) (June 1999)
Doctor 98 14 10 19 93 140 47 Train at COMAHSTrain specialists overseas
Nurse 265 37 27 65 266 1,406 1,140 Redeploy 354 SECHNs;Train 786 SENs/SRNs
Midwife 119 13 1 65 170 281 111 Train at School of Midwifery(O level intake)
Nurse Anaesthetist 4 1 0 0 3 44 41 Train nurses in NigeriaDentist 6 1 0 0 5 22 17 Train at COMAHSDental Technician 10 2 0 0 8 30 22 Train overseasRadiographer 5 2 0 0 3 22 19 Train at COMAHSRadiographer Techn. 2 0 0 0 2 44 42 Train overseasDietician 0 0 0 0 0 22 22 Train in-countryPharmacist 8 5 1 0 2 22 20 Train in-countryDispensing Techn. 162 35 4 0 123 66 -57 Redeploy to ensure coverageMed. storekeeper 0 0 0 0 0 22 22 Train in-countryLab. Technologist 2 1 0 0 0 20 20 Train in-countryLab Technician 19 3 0 0 16 44 28 Train in-countryPhsiotherapist 1 0 0 0 1 22 21 Train overseasRecords Technician 6 0 0 0 6 80 74 Train in-countryStorekeeper 5 2 1 0 2 22 20 RecruitMaintenance Technician 26 1 3 0 22 30 8 Train in-countryPlumber 1 0 0 0 1 40 39 Train in-countryMason 8 0 1 0 7 4 -3Carpenter 19 5 1 0 13 4 -9
Table 1 B. Peripheral Health Units
Job Staff in Other Staff in Projected Number Gap/Category Post Retirements Wastage Training Staff Required (Surplus) Action
(1994) (1994-99) (1994-99) (1994) (June 1999) (June 1999)Community Heafth Officer 93 0 9 44 128 200 72 Retrain 72 SECHNs at
paramedical schoolCommunity Health Assista 0 0 0 0 0 400 400 Redeploy 73 MCH Aides (post-1986) h ;,
Train 42 CHAsRetrain 237 EDCU Assistants D
Retrain 18 Vaccinators -Community Heafth Aide 347 2 35 0 291 1,200 909 Train in-country
lann9a.xis)
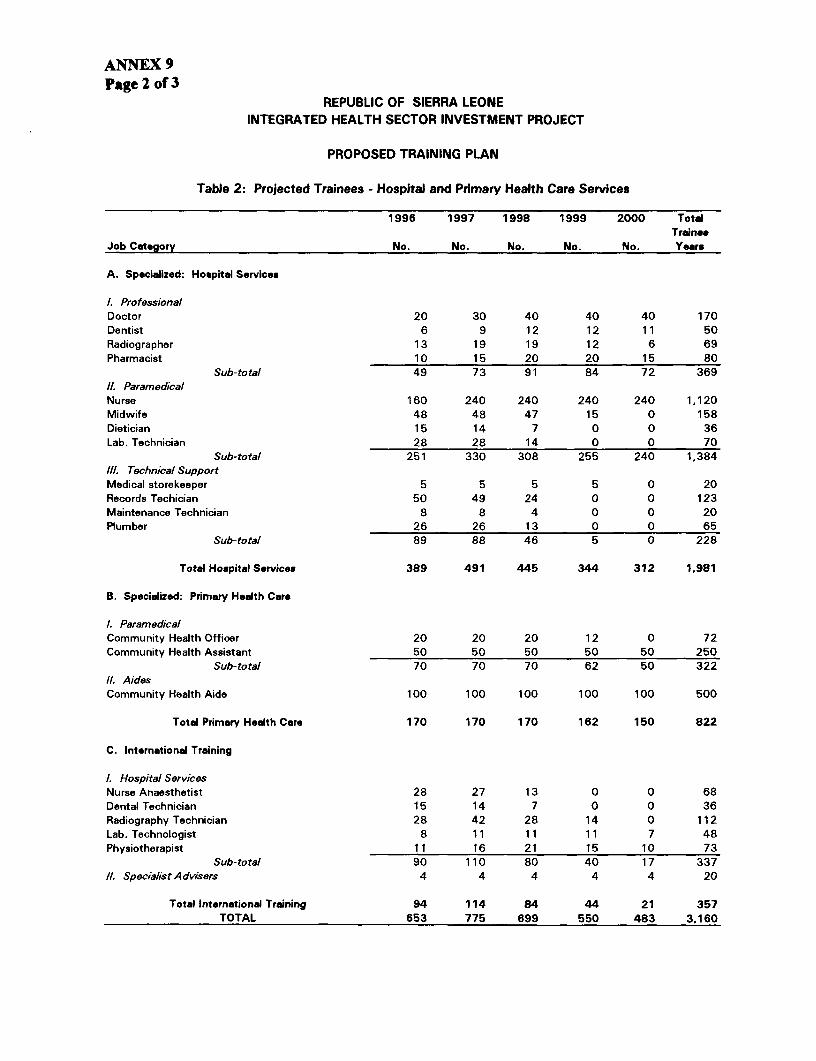
ANNEX 9Page 2 of 3
REPUBLIC OF SIERRA LEONEINTEGRATED HEALTH SECTOR INVESTMENT PROJECT
PROPOSED TRAINING PLAN
Table 2: Projected Trainees - Hospital and Primary Health Care Services
1996 1997 1998 1999 2000 TotalTrain"
Job Category No. No. No. No. No. Years
A. Specialized: Hospital Services
1. ProfessionalDoctor 20 30 40 40 40 170Dentist 6 9 12 12 11 50Radiographer 13 19 19 12 6 69Pharmacist 10 15 20 20 15 80
Sub-total 49 73 91 84 72 36911. ParamedicalNurse 160 240 240 240 240 1,120Midwife 48 48 47 15 0 158Dietician 15 14 7 0 0 36Lab. Technician 28 28 14 0 0 70
Sub-total 251 330 308 255 240 1,384l1l. Technical SupportMedical storekeeper 5 5 5 5 0 20Records Techician 50 49 24 0 0 123Maintenance Technician 8 8 4 0 0 20Plumber 26 26 13 0 0 65
Sub-total 89 88 46 5 0 228
Total Hoapital Service. 389 491 445 344 312 1,981
B. Specialized: Primary Health Care
1. ParamedicalCommunity Health Officer 20 20 20 12 0 72Community Health Assistant 50 50 50 50 50 250
Sub-total 70 70 70 62 50 32211. AidesCommunity Health Aide 100 100 100 100 100 500
Total Primary Health Care 170 170 170 162 150 822
C. International Training
1. Hospital ServicesNurse Anaesthetist 28 27 13 0 0 68Dental Technician 15 14 7 0 0 36Radiography Technician 28 42 28 14 0 112Lab. Technologist 8 11 11 11 7 48Physiotherapist 11 16 21 15 10 73
Sub-total 90 110 80 40 17 337/1. Specialist Advisers 4 4 4 4 4 20
Total International Training 94 114 84 44 21 357TOTAL 653 775 699 550 483 3.160

REPUBLIC OF SIERRA LEONE
INTEGRATED HEALTH SECTOR INVESTMENT PROJECT
PROPOSED TRAINING PLAN
Table 3: Management Training Plan
1996 1997 1998 1999 2000 TotalTraining No.Days No. No. No. No. No. Trainees
ProgramManagement Skills 3 55 20 20 20 115Future Performance 15 10 10Better Service 15 45 20 20 20 105Planning & Organizing 10 55 20 20 20 115Implementing Plans 10 55 20 20 20 115Coaching Skills 5 20 10 10 40Trainer Skills 5 30 30 30 30 120Computer Skills 10 40 40 40 120
Total Trainees 130 190 160 150 110 740Total Staff-days 1,090 1,660 1,360 1,310 950 6,370
(ann9c.xls)


ANNEX 10Page 1 of 3
REPUBLIC OF SIERRA LEONEINTEGRATED HEALTH SECTOR INVESTMENT PROJECT
Detailed Program Estimates(USS '000)
Fiscal Years1996 1997 1998 1999 2000 TOTAL
INVESTMENT COSTS
A TECHNICAL PROGRAMS
1.0 PRIMARY HEALTH CARE SERVICES 3,236 4,500 4,850 4,000 4,000 20,586
2.0 Hospital and Laboratory Services1. Secondary & Tertiary Health Care 497 1,500 2,000 2,000 1,966 7,9632. Laboratory Services 344 846 550 250 250 2,240SUBTOTAL TECHNICAL PROGRAMS 4,077 6,846 7,400 6,250 6,216 30,789
B SUPPORT SERVICES1.0 Policy Formulation I Central Administration 459 600 600 700 200 2,5592.0 District Allocation 1,000 1,000 1,300 1,300 1,500 6,1003.0 Support Services (maintenance & repair) 204 615 543 482 480 2,3244.0 PlanningandInformationSystems 52 311 710 18 100 1,1915.0 Human Resources /a 1,052 100 100 100 100 1,4526.0 Drugs and Medical Supplies/b 4,303 1,159 0 220 220 5,902
SUBTOTAL SUPPORTSER7VICES 7,070 3,785 3,253 2,820 2,600 19,528
TOTAL INVESTMENT COSTS /c 11,147 10,632 10,653 9,070 8,816 50,318
OPERATING COSTS
A TECHNICAL PROGRAMS
1.0 PRIMARY HFALTH CARE SERVICES 3,670 4,290 4,881 5,364 5,605 23,810
2.0 Hospital and Laboratory Services1. Secondary & Tertiaiy Health Care 3,799 4,318 4,318 4,377 4,410 21,2222. Laboratory Services 104 123 130 190 188 735SUBTOTAL TECHNICAL PROGRAMS 7,573 8,731 9,329 9,931 10,203 45,767
B SUPPORT SERVICES1.0 Policy Formulation / Central Administration 1,845 1,249 1,248 1,248 1,248 6,8372.0 District Allocation 3,303 4,046 4,130 4,173 4,218 19,8703.0 Support Services (maintenance & repair) 212 118 227 335 335 1,2274.0 Planning and Information Systems 350 529 559 577 577 2,5935.0 Human Resources 951 372 237 257 237 2,0546.0 Drugs and Medical Supplies 260 1,624 1,623 3,013 2,923 9,443
SUBTOTAL SUPPORTSERVICES 6,921 7,938 8,024 9,603 9,538 42,023
TOTAL OPERATING COSTS /c 14,494 16,669 17,353 19,534 19,741 87,790
TOTAL PROGRAM COSTS 25,641 27,300 28,006 28,604 28,557 138,108
/a Most of the training for the FY 95/96 is allocated to Human Resources; in subsequent years it is divided accross the respective services./b The initial year budgets drug seedstock under capital costs; in subsequent years replenishments are budgeted under operating costs to beconsistent with government budget headings./c Physical and Price Contingencies 115%) included.
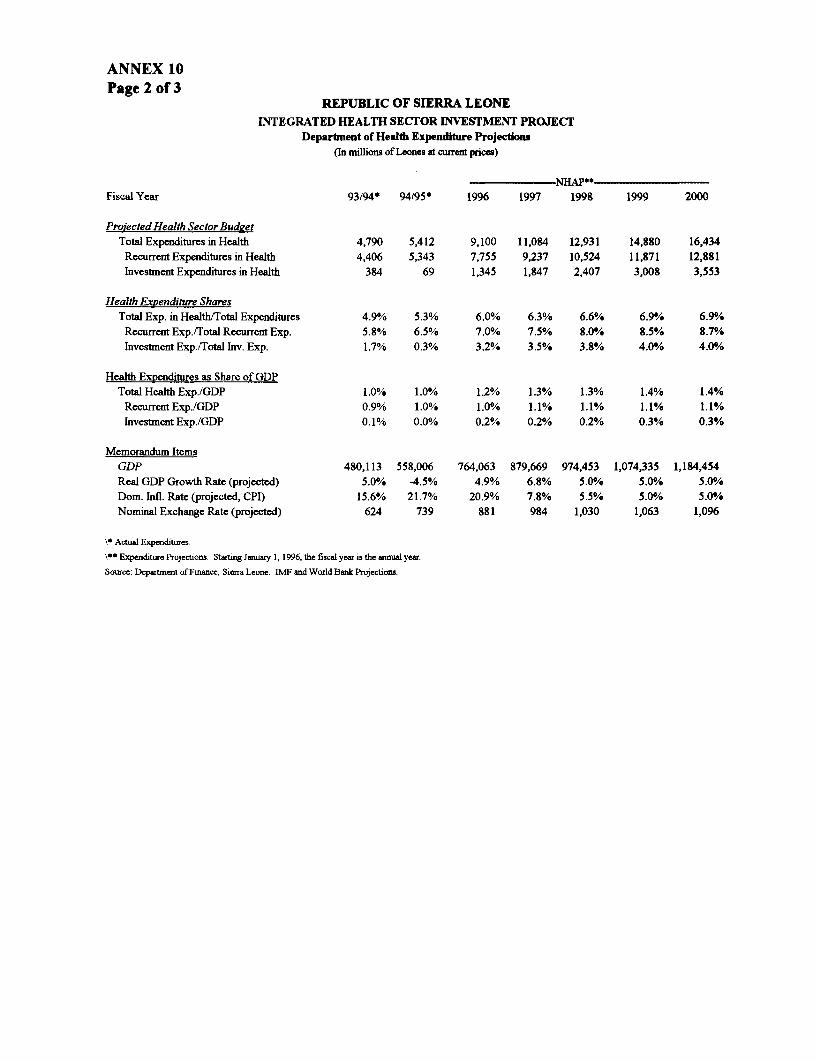
ANNEX 10Page 2 of 3
REPUBLIC OF SIERRA LEONEINTEGRATED HEALTH SECTOR INVESTMENT PROJECT
Department of Health Expenditure Projections(In millions of Leones at current prices)
NHAP**Fisca Year 93194* 94/95* 1996 1997 1998 1999 2000
Proiected Health Sector BudgetTotal Expenditures in Health 4,790 5,412 9,100 11,084 12,931 14,880 16,434Recurrent Expenditures in Health 4,406 5,343 7,755 9,237 10,524 11,871 12,881Investment Expenditures in Health 384 69 1,345 1,847 2,407 3,008 3,553
Health Expenditure SharesTotal Exp. in Health/Total Expenditures 4.9% 5.3% 6.0% 6.3% 6.6% 6.9% 6.90/o
Recurrent Exp./Total Recurrent Exp. 5.8% 6.5% 7.0% 7.5% 8.0/ 8.5% 8.7%Investment Exp./Total Inv. Exp. 1.7% 0.3% 3.2% 3.5% 3.8% 4.0% 4.0%
Health Expenditures as Share of GDPTotal Health Exp./GDP 1.0% 1.0% 1.2% 1.3% 1.3% 1.4% 1.4%
Recurrent Exp./GDP 0.9% 1.0% 1.0% 1.1% 1.1% 1.1% 1.1%Investment Exp./GDP 0.1% 0.0% 0.2% 0.2% 0.2% 0.3% 0.3%
Memorandum ItemsGDP 480,113 558,006 764,063 879,669 974,453 1,074,335 1,184,454Real GDP Growth Rate (projected) 5.0% -4.5% 4.9% 6.8% 5.0% 5.0% 5.0/oDom. Infl. Rate (projected, CPI) 15.6% 21.7% 20.9% 7.8% 5.5% 5.0% 5.0/eNominal Exchange Rate (projected) 624 739 881 984 1,030 1,063 1,096
\* Actual Expenditures.
\00 Expenditure Projections. Stating January 1, 1996, the fiscal year is the annual year.
Source: Department of Finance, Sierra Leone. IMF and World Bank Projections.

REPUBLIC OF SIERRA LEONEINTEGRATED HEALTH SECTOR INVESTMENT PROJECT
NEAP Components by Finander (USS)FY 1996
IDA GOSL ADB IDB BU UNICBF UNDP UNFPA WHO SFD NGOs & Othes TowlNHAP Components Amount % Amnunt % Amount % Amount % Amount % Amount % Amount % Amount I % Amou| %I Amount %I Amount i % Amount I %
A Policy Formaoion 146,480 6.4% 1,713,621 74% 257,090 11% 2,876 0'/% 60,000 3% 123,853 5% 2.303.920 100'%
B District Opeations 0 0% 1,252,562 29% 156,354 4% 396,000 9%1. 105,263 2% 27,550 1% 2,365,415 55% 4,303,145 100%!
C hifrastructure & Eqwpment Maintnance 139,647 33 5% 175,047 42% 50,009 12% 51,923 12% 416,626 100'%
D Planning and information 0 0/ 321,433 80% 14,993 4% 66,074 16% 402,499 100'/.
E Human Resource Management 348,721 174% 764,982 38% 183,009 9% I 36,863 2% 480,264 24% 188,807 91/. 2,002,647 100%
F Dru and Medical Supplies 1,061,865 23 3% 1,769,046 39% 15,400 0%/ 148,463 3% 240,000 5% 135,000 3% 1,192,925 26% 4,562,699 100%,.
G Primary Health Care 387,788 5 6% 1,029,041 15% 550,010 8 520,000 8% 430,200 6% 3,989,217 58% 6,906,256 100%!
H Hospital and Laboratory Servces 71,701 1.5% 3,308,122 70/. 715,016 15% 202,895 4% 41,400 1% 404,443 9V1. 4,743,577 100N%
Total Disbursements 2,156,203 8.4% 10,333,854 40% 1,376,471 5% 411,400 2%1 308,158 1% 738,212 3% 480.264 2% 760,000 3% 694,150 3% 0 0%!. 8.382,657 33% 25,641,369 100'!.


REPUBLIC OF SIERRA LEONEINTEGRATED HEALTH SECTOR INVESTMENT PROJECT
Key Health Sector Performance IndicatorsA
Indicator Baseline Level When Measured How Measured(year)
96 97 98 99 00Inputs __ Govermnent Health Budget/Expendimurs:(i) Budget allocation at least 6% of Govt. Budget (current (i) 5.2% (94/95) 6.0% 6.3% 6.6% 6.9% 6.9% (i) Annual budget submissionand investment), not including public debt service andexclusive of funds generated by cost recovery andcontributed by donors(ii) % annual health budget expended (iii) 96% (93-94) >96% >95% >95% >95% >95% (ii) Annual audit report; public
expenditure reviewDonor Health Budgets/Expenditures:(i) # of donors contributing to NHAP (i) 22 (95-96) X X X X X (i) & (ii) Annual budget commitments(ii) Amounts donors budgeted for NHAP (ii) $15.3m (96) X X X X X with GOSL(iii) Prop. of annual budgets disbursed through GOSL (iii) no baseline X X X X X (iii) Annual external audit(iv) Prop. of annul budgets disbursed through NGOs (iv) no baseline X X X X X (iv) Donor Relations ReportsProcesses _ _ __ X _<XCommunity Participation:(i) # of districts decentralized (i) 0 (95) 1 2 3 4 5 (i) & (ii) Annual District Health Team(ii) # of functional chiefdom health development (iu) 0 (95) 10 X Reportscommittees with community representatives indecentralized districts(iii) # of functional hospital management committees with (iii) 0 (95) 1 2 X X X (iii) Hospital Reports (HMIS)community representatives(iv) Community feedback on quality, relevance of health (iv) 3 sites (94) 2 per de- 2 per (vi) Beneficiary Assessmentservices, and ability to pay centr. de-centr.
district districtClinical Quality: (i) Annual Report(i) Development of case management protocols for clinical not developed Yesworkers (ii) Annual Report (HMIS - HRD)(ii) # of workers trained in case management protocols X X X X(iii) % of workers properly using case management in (iii) Supervision Reports (HMIS -decentralized districts X X X X HRD)Quality of Financial Management:(i) Satisfactory audits of GOSL (i) no baseline Yes Yes Yes Yes Yes (i) Annual internal audit(ii) Satisfactory audits of donor expenditures (ii) no baseline Yes Yes Yes Yes Yes (u) Annual external audit s z
okm
Key performance indicators have been developed to monitor programs' progress in inputs, processes, outputs, and outcomes and project impact. These indicators will be usedyearly at the evaluation sections with donors and NGOs to assess the achievement of program objectives, and when and if necessary, will be updated to keep abreast of anychanges in the sector.

Indicator Baseline Level When Measured How Measured(year) 1:
_ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ 96 97 98 99 00 Outputs _ m
Staff Training at Training Institutions: Current level: (i) 70 (i) 70 (i) 70 (i) 70 (i) 70(i) # staff retrained & redeployed (total, SECHNs, MCH 93 CHOs; SECHNs; SECHNs; SECHNs; SECHNs; SECHNs; DOH Semi-annual Report (HMIS -Aides) 0 CHAss; (i) (ii) (i) 6) () HRD)(ii) # new staff trained & employed in Sierra Leone (total, 347 CHAides; 50HAs 50CHAs 20CHOs 20CHOs (iCK Rs
CHOs, CHAs, CHAides) 471 SECHNs; 100CHAi IOCi CHAi lOOCHAi IOOCHAides; des; des; des; des;
Facilities: DOH Semi-annual Report (HMIS -(i) # of PHUs rehabilitated no baseline 11 X X X X Support Services)(ii) # of hospitals rehabilitated 4 X X X X(iii) # of PHUs built X X X X X(iv) # of PHUs equipped 11 X X X X(v) # of hospitals equipped 4 X X X X
Utilization: (i) - (iv) Facilities reports (HMIS)(i) # of outpatients seen at PHUs (i) _ (94) X X X X X(ii) # of inpatients at hospitals (ii) _ (94) X X X X X NB: rehabilitated and non-rehabilitated(iii) o f outpatients at hospitals (iii) _ (94) X X X X X facilities are to be distinguished(iv) bed occupancy rate at District hospitals (distinguish (iv) no baseline X X X X Xdecentralized District hospitals) ICoverage: (i) Clinic reports (HMIS); cluster(i) % of 1 year olds fully immunized (i) 35% (94) X X X X 85% survey (96, 98, 2000)(ii) # of women with 3 antenatal visits (ii) no baseline X X X X 60% (ii) Clinic reports (HMIS)
Outcomes/ImpactChild Health:(i) Infant mortality rate (i) 135 (92) X X X X 70 (i), (u) & (iv) National Household(ii) Under 5 mortality rate (ii) 240 (90) X X X X 160 Survey(iii) Low birthweight (iii) 17% (90) X X X X 8.5 (iu) Hospital Reports (HMIS)(iv) Childhood prevalence of low wt/age (iv) 33 % (89-90) X X X X 25%
Maternal Health:(i) Maternal mortality rate (i) 630 (92) X X X X 400 (i) & (iu) National Household Survey(iu) Contraceptive prevalence rate (ii) 4% (93) X X X X 10%(iii) Total fertility rate (iii) 6.5 (91) X X X X 6.0 (u) Reports from FP clinics (HMIS)
Communicable Diseases:(i) HIV prevalence among blood donors in Western Area (i) 2.1 % (94) X X X X X (i) Blood Bank data (HMIS)(ii) # of measles cases (ii) 674 (92) X X X X X (ii)-(i) Clinic reports (HMIS)(iii) # of neonatal tetanus cases (iii) 61 (92) X X X X X(iv) # new cases sputum positive tuberculosis (iv) (94) X X X X X (iv) CDD program reports (HMIS)
Notes:- Most targets assume full operation of health programs in the country.- Information should be broken down by district level where appropriate.

ANNEX 12Page I of 2
DEPARTMENT OF HEALTH ORGANIGRAM(CENTRAL LEVEL)
i S.O.S.
FD.G. MED. SRVCS. ... DnDeRn. Audit. GT RVS
D.D.M.S.
I~~~~~~~D Inem Audi
HOSPE DRUS XFIN. SUPT.PHC & P NL ED. NURS. RES. SRVCS,
MCH HOSP. PH. HA RECT.FIN.
PREV. L LAB, PLFAN.NMPLYSTORES]
_ FOOD |AMGT. WLFRE
_ TRANSP.
_ CFACILMGNT.
BLTH. SEE
LEGEND; SEE v

ANNEX 12Page 2 of 2
KEY STAFF FOR THE DEPARTMENT OF HEALTH ORGANIGRAM
TITLE ABBREVIATION
SECRETARY OF STATE S.O.S.
DIRECTOR GENERAL OF MEDICAL SERVICES D.G. MED. SRVCS.
DIRECTOR GENERAL OF MANAGEMENT SERVICES D.G. MGT. SRVCS.
DIRECTOR OF DONOR RELATIONS D.D.R.
DIRECTOR OF MANAGEMENT SUPPORT D.M.S.
DIRECTOR OF INTERNAL AUDIT D.INTERN. AUDIT
DIRECTOR OF PLANNING AND INFORMATION P&I
DIRECTOR OF PRIMARY HEALTH CARE P.H.C.
DIRECTOR OF HOSPITAL AND LAB SYSTEM HOSP. & LAB.
DIRECTOR OF NURSING NURS.
DIRECTOR OF RESOURCES (FINANCE) FIN. RES. 1ASSISTANT DIRECTOR OF RESOURCES (FINANCE) FIN. RES. 2DIRECTOR OF SUPPORT SERVICES SUPT. SRVCS.
DIRECTOR OF DRUGS AND MEDICAL SUPPLIES DRUGS MED. SUPPL.
DIRECTOR, HUMAN RESOURCES HRM
HOSPITAL CARE MANAGER HOSP.
MATERNAL AND CHILD HEALTH MANAGER MCH
DISEASE PREVENTION AND CONTROL MANAGER DIS. PREV. CONT.
FOOD AND NUTRITION MANAGER FOOD NUTR.
ENVIRONMENTAL HEALTH MANAGER ENV. LTH.
HEALTH EDUCATION MANAGER HLTH. EDUC.
LABORATORY SERVICES MANAGER LAB.
PLANNING MANAGER PLAN
PUBLIC HEALTH AND MEDICAL STATISTICS MANAGER P.H. MED. STATS.
MANAGEMENT INFORMATION MANAGER MGT. INFO
ARCHITECTURAL SERVICES MANAGER ARCH
FINANCIAL ACCOUNTANT FIN. ACCT.
HEALTH CARE FINANCING MANAGER HCARE FIN.
RECRUITMENT AND TRAINING MANAGER RECT. TRN.
STORES MANAGER STORES
PROCUREMENT MANAGER PROC.
TRANSPORTATION MANAGER TRNSP.
FACILITIES AND MAINTENANCE MANAGER FACIL. MGNT.
EMPLOYEE WELFARE MANAGER EMPLY. WLFRE.

}~~h [ -t -lii&|!tI I l
I ~ IF.....................
.......................................................... .... ..................................................................... ....... .................... ...................................................... ..... ....................11ii --- -I I -.. ....I' ... Mi
mm *~mI- l - x
,,:ID4.~~~~~~~~~~~~~~~~~~~~~~. 0. ........................................... .. ........... ........................................................................ .................... ..............
4................... ............
.................................................. ...................................................................................................... ........................... ...............................
.......................... ............................................................................................................. ........................ ...........................
.......................................................................................................................... .....................

-i-- F- - - - - - - - - - -- - - -
I~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~fr X yX......
.. .... . . . . . . .. [ 11 . . ... ........
U~~~~~ U
..... ... .............. ...... ........ ...... ............ ..... .. ............... ........... ........ .......... ..... .. ............. .......... ........... ......... ............ ........... ....... .... ..... ..... ........... ........... ........ ... .........
. .. . .. .. . .. .. . .. . .. . . . . .. . . .. .. . . . .. . . . . ... . . .. . . . . .. .. .. . . . . . .. . .. . .. . . . .. . .-.. . . . . .. . . . .. . . . . .. . . .. .. . . . . .. . . . . .. . . .. . . . . ..
. ................................. .................................................. .....................................................

ANNEX 14Page 1 of 3
REPUBLIC OF SIERRA LEONE
INTEGRATED HIEALTH SECTOR INVESTMNENT PROJECT
Operational Manual - Draft Table of Contents
Preface .................................
Introduction to the Operational Manual ............................... ii
Terms of Reference ................ iii-v
1. SITUATION ANALYSIS IN THE HEALTH SECTOR ................................ 1
2. THE NATIONAL HEALTH POLICY AND OBJECTIVES .......................... 2
3. THE NATIONAL HEALTH ACTION PLAN .............................................. 23 .1 rna-oa ucn o rl ...................................................................... ........... I. Descr on . .2......................................................... 2
'Scze for . '=dh= Care 3e iverv ......................................................... 53.4 E maced 7oim md C regor Costs ......................................................... 53 5 Finarc= ? . .......................................................... S3.6 Donor C rdi oa ......................................................... 83.7 MfuanL Dooor Cocdicons ......................................................... 83. Ke: Lmvic3cn=ou And O eratona4 PoLic4es .................................................... 8
4. MANAGEMENT ARRANGEMENTS..........................................................
4.1 -ad.quzr-ters O isaion Sauc ................................................... 4.' Roles nd Resronsibihaes: ................................................. 8
a) ToO Mmagenant TG .................................................. ao) S r ! of Sr . ................ .... .. 9........................ ....... 9c! Du*c:or CGenral - fedical Se-vices ................................................. 9d) D:ecor Gc -aI .Mm emnt Sa4vices ................................................. 9e) Director of Donor Reaos ................................................. 9t) Dira: -or of inteaW Aucit .................................................. 9g Dur-,or o tM a entSupport ................................................. 10h Division D c:ors ................................................. 10
t) t rnit M!aage S ................................................. 10j) Dis ct Heaida M oeme t Tms ................................................. 10k) Nanoaal Health CoLmcT ad dHospimi Managent Co rimem .................. 10
4.3 Dec=n-aliain ,., 104.4 4M.anpower D3c e±opment .................... 104 5 Nanonal Co-:rdin.roa nd Monitoring ................................ 114 6 Discict Co-reiinanon and Momitoi ng . ................................. i I

.................................................. ioany T~s -nx3t.................................................o:Pnv TU uf l HOG o02 a3 0 SC= 1 .1
Ll v1 - * OTpnV 7=zq i=m AoC posodoLd 11
91 ==;;zz~~~~~~~~~~lr;rS. I25s t 01
9 1 - - -... -........ -......... = SAS fi lSno Pv C=Y2rf1`fAO3 :1 * 0191- ----- -- ........................... mmasAs kr;;#ne pm Srm=c-rncv =DLIT1) I ol9. ............................................... -- NLNnofQ Vl 0o
9.l -d-almO t 6
cl ~~~~~~~~~~~~~~~~~~~~~~~~~~- .--D! 0o3=zs mcsLC - 6s- - ---- *== 2zrV = CsIQ 6
......................... SQNfl .40 1N3W NVVy 6
................................ ..- .O.O. ... ...1-. A .C v : S'=X ,-g^ ] .......... --............... -( AC 'pzimn; -'1 l= -
.IN- l3WflZnOUd *8.. . .. . . .. . . .. . . .......................... ..........-----..--'.'''-'''.ZL1i-in:
c1''' ' '..........''.''''....................................................n,_ 1.J......... . --- J I d NLLm l :3 I
... n-- ...... --- =O0it U 'a== = 9
_a ....................................................... ............... C
................ . 1OlNO ON NLLVn7A3 'NNOiINO 9
I ........................ . IsJ03C ;po P M ] C q UCISL,0nS -,.n -0 - Is lL LLOTES =L I 1 NOLLIIN3WB3dWI i03L Obd 20 NOISIAN3dnfS S
LiJ Z atINXIV

ANNEX 14Page 3 of 3
Annexes
Annex 1 Detailed Description of NHAP .............................................. 20
Annex 2 Organisation Structure - Organogram ....................................... 21
Annex 3 Organisation Structure - Detailed Post Analysis ...................... 22
Annex 4.. Terms of Reference for Key Technical Assistance .23
Annex 5 Annual Planning and Budgeting Cycle ..................................... 37
Annex 6 Annual Implementation Plan .. . .................................... 42
Annex 7 NHAP Budget and Financing Plan .................................... 43
Annex 8 Annual Financing Plan and Budget .................................... 44
Annex 9 Procurement Arrangements .................................... 45
Annex 10 Financial Management Guidelines .................................... 47
Annex 11 Internal Audit Guidelines from Auditor General's Dept ......... 52
Annex 12 Performance/ Progress Indicators .......................................... 57
Annex 13 Outline of Contents of Progress Reports ............................... 58
Annex 14 List of Key Addresses and Telephone Numbers .................... 62
Annex 15 Main Donor Conditions ............................,.,.,,,.,,,,. 63
Annex 16 List of Relevant Documents .. ,,. 64
Annex 17 Pro forma Documents (eg letter of invitation to tender).......67


ANNEX 15REPUBLIC OF SIERRA LEONE
INTEGRATED HEALTH SECTOR INVESTMENT PROJECT
Supervision Plan
1. Due to the sector reform nature of the Project, supervision missions will be done jointly with theDepartment of Health and Social Services and other donor agencies based on progress reports with a commonformat. Currently the Department is planning to invite donors for two reviews per year. One in the first half of theyear to review progress during the previous year and present a revised strategic plan, and one late in the year topresent the budget and work program for the following year. It is the Department's intention to collapse these twoworkshops into one later in the program. This schedule, however is based on the current thinking, and thus reflectstwo annual workshops.
2. Other implementation support will be provided by Bank staff and consultants on mission to Sierra Leone asnecessary.
Bank Supervision Inputs into Key ActivitiesApproximate Date Activity Expected Skills Required Staff inputs(Month/Year) _ (in staff weeks)
3/% Project Launch Mission Procurement, disbursement, 10financial management, publichealth
10/96 FY 96 Activity Plan Public health, health 10Implementation Review and economics, financing, donorFY97 Budget and Activity coordinationPlan Review
4/97 FY97 Budget and Activity Public health, health 6Plan Review economics, financing, donor
coordination10/97 FY 97 Activity Plan Public health, health 0
Implementation Review and economics, financing, donorLaunching of FY98 Plan and coordinationBudget
4/98 FY98 Budget and Activity Public health, health 6Plan Review economics, financing, donor
coordination10/98 FY98 Activity Plan Public health, health 10
Implementation Review and economics, financing, donorLaunching of FY99 Plan and coordinationBudget
4/99 Mid-term Review and FY99 Public health, health 14Activity Plan Implementation economics, EEC, humanReview resources, evaluation
10/99 FY99 Activity Plan Public health, health 10Implementation Review and economics, financing, donorFY2000 Activity Plan and coordinationBudget Launching
4/00 FY00 Budget and Activity Public health, health 6Plan Review economics, financing, donor
coordination12/00 FY00 Activity Plan Public health, health 0
Implementation Review and economics, financing, donorPreparation for Final coordinationEvaluation
4/01 Final Evaluation Procurement, disbursement, 10financial management, publichealth


ANNEX 16Page 1 of 2
REPUBLIC OF SIERRA LEONEINTEGRATED HEALTH SECTOR INVESTMENT PROJECT
Disbursement Forecast
PHN Sector Disbursement Profiles(% Cumulative Disbursements)
Quat&s from Approval Date 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30 32 34 36 38
All Regions 0 3 6 10 14 18 26 34 42 50 62 70 78 86 90 98 100Afiica 0 3 6 10 14 18 22 30 38 50 58 66 74 82 90 98 98 100Siera Leone (All Selors) 0 14 18 22 26 38 46 54 66 74 82 82 86 86 90 94 98 98 100Integrated HealthSectorInv.Project 0 6 11 21 31 44 58 70 81 91 100
Disbunsement Proflles
100 - - -
70
%50 j' / -'_~~~~~~~~~~~~~~~~~~~~Integraed Healthi Sector Inv. Projec
2468112 14 16 18 20 22 24 26 28 30 32 34 36 38
% ~ ~ ~ u~ 50 h

ANNEX 16Page 2 of 2
REPUBLIC OF SIERRA LEONEINTEGRATED HEALTH SECTOR PROJECT
Disbursement Forecast(US$ million)
Program Costs Other Donors IDA Fhncing Government Contributfo]DA Fisal Yearsand Semesters Semester Cumulative Semester Cumlative Semester Cumulative Semester Cumuative
1996 1, 0 0 0 0 0 0 0 02 12.8 12.8 6.6 6.6 1.1 1.1 5.2 5.2
1997 3 12.8 25.6 6.6 13.1 1.1 2.2 5.2 10.34 13.7 39.3 6.0 19.1 2.0 4.2 5.7 16.0
1998 5 13.7 52.9 6.0 25.1 2.0 6.1 5.7 21.76 14.0 66.9 5.0 30.1 2.8 8.9 6.3 28.0
1999 7 14.0 80.9 5.0 35.0 2.8 11.6 6.3 34.38 14.3 95.2 5.1 40.1 2.3 13.9 6.9 41.2
2000 9 14.3 109.5 5.1 45.2 2.3 16.2 6.9 48.110 14.3 123.8 4.9 50.1 1.9 18.1 7.6 55.7
2001 11 14.3 138.1 4.9 54.9 1.9 20.0 7.6 63.2Total 138.1 138.1 54.9 54.9 20.0 20.0 63.2 63.2
Disbursement Schedule140-
130-
120
110
100 -
90
0 ~~~~~~~~~~~~~~~~~~~~Program70 - Cods
(Cumuiative)50 -~ / ,, ' ,, .(Cumufaive)
, , . -IDA Financing
00 - / _ _ - (CumutibHve)
10- ' ' Fh
1 2 3 4 5 6 7 8 9 10 11Semester

MAP SECTION


IBRD 26923
I cf~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~' LKN
Folobo / T
\A~~~~!' ,,ZTI e
t;' ; J ~~~~~~KABALA 3'
Z ' l Komakwie '
Fadugu 1. Kamaron >o
/ KAMBIA r ~Pendembu ,,_._0 D.~4t ,.0 °')/
K.AMBIA 0mBumbuna
M6nboloO , E - MAKENI Worodu
lrb PORT LOKO SlonKonoktidee ° ° ' .akidu 0
0 Marom KoIn.ordu \Lungi ) , Lu 24 l 0 M BURAKA> Matotoko Mosingbe 0 N O
or ~~~~~~~~~~~e1- -~ ~ ~ ~ ~~~Kinod
REETgtWN Pepe P- O SEFADU
Yele. Jalama0" 0
AREA [10a t ON 6Makonkor, O Yonibono
W ES T f RR' Nwcterr ,,<i,
O' wtaima/Kent Ml O Y A M B A 0 oSenehur OP KAILAHUN j
MOYAMBA Dodo
Pond mbu0 IG)BO
-Sembabun s
Gbongbotok
. 2O6
Nitti_ malig JJoru
' . E , ° ; O---'Matru . -BONTHE(iL L ' A
C) C B O K F,o SIERRA LEONE)'Tormobum HEALTH SECTOR
":' Z -- <t0K,, < INVESTMENT CREDIT4~ / < PFiro :j/ PAVED ROADS
7' C * NATIONAL CAPITAL
8 Sulima -®t () DISTRICT CAPITALS 7
All \ (i) INTERNATIONAL AIRPORT
DISTRICT BOUNDARIES
\ ~ Zt RIVERS
INTERNATIONAL BOUNDARIES
The boundones, colors, denominations and any other informationshown on this map do not imply, on the part of The World Bank 0 10 20 30 40Group, any judgment on the legol status of any territory, or any K LOMETERSendorsement or acceptance of such boundaries. M LES
13 12 '21
DECFMBER 1995



IMAGING
Report No: 13947 SLType: SAR