world universities network presentation dr heather mckenzie professor kate white dr lillian hayes mr...
TRANSCRIPT

World Universities Network World Universities Network PresentationPresentation
Dr Heather McKenzie
Professor Kate White
Dr Lillian Hayes
Mr Keith Cox
Associate Professor Maureen Boughton
Ms Judith Fethney
Ms Jo Dunn
1

Introduction
• Overview of program of research
• Introduction to this presentation
• Background: Study One

Exploratory research• To explore the nature of nurse-
patient encounters and relationships in the context of community care of cancer patients
• Research focus was on particular nurse-patient encounters & involved interviews with nurses and patients and observation of each encounter

Research findings
• Sense of security for patients and their families about the ‘immediate situation’
• A pivotal role for community nurses• Education of patients and their families
about managing self care• Potential for reduction in unplanned
presentations to hospital for cancer patients

Publications• McKenzie H, Hayes S, Forsyth S & , Boughton
M (2008) Explaining the Complexities and Value of Nursing Practice and Knowledge. In Crouch M & Morley I (Eds) Illumination Through Critical Prisms, Rodopi, Amsterdam
• McKenzie H, Boughton M, Hayes L, Forsyth S, McVey P, Davies M, Underwood E (2007) A sense of security for cancer patients at home: the role of community nurses, Journal of Health and Social Care in the Community, 15(4): 352-359

Study Two

Chemotherapy Chemotherapy outpatients’ outpatients’ unplanned unplanned
presentations to presentations to hospital: hospital:
A retrospective studyA retrospective study
Funding: Merck Sharp & Dohme

Aims• To identify and analyse the nature and
magnitude of chemotherapy outpatients unplanned presentations (and admissions) to the emergency department or cancer centre at a large metropolitan hospital
• To explore the antecedents to these visits

BackgroundBackgroundNSW (2006):
• 600 outpatient chemotherapy chairs
• 125,000 outpatient chemotherapy visits annually
• Research demonstrates side effects of chemotherapy can be distressing and debilitating

What is Known?• Chemotherapy-related
serious adverse effects may be more common than reported in clinical trials
• Cancer patients receiving chemotherapy are more likely than those who are not to visit the emergency room or be hospitalised
• Chemotherapy patients incur significant costs
(Hassett et al 2006)

Methodology• Retrospective study
– October 1, 2006 - September 30, 2007
– Data bases, medical records from ED & Sydney Cancer Centre
– All patients on chemotherapy within 6 months of their unplanned presentation to RPAH
– Variables: cancer diagnosis, reason for presentation, chemotherapy regimen, position in the treatment trajectory, whether or not they were admitted & if so for how long, and a range of demographics.
• Interviews (2008)– To explore antecedents to the unplanned presentations to
hospital

Between October 2006 - September 2007:
316 people469 unplanned presentations
Between October 2006 - September 2007:
316 people469 unplanned presentations
Chemotherapysix months prior to
unplanned presentation(s)
Visits = 363 (77.4%)People = 233 (73.7%)
Chemotherapysix months prior to
unplanned presentation(s)
Visits = 363 (77.4%)People = 233 (73.7%)
No Chemotherapysix months prior to
unplanned presentation(s)
Visits = 106 (22.6%)People = 83 (26.3%)
No Chemotherapysix months prior to
unplanned presentation(s)
Visits = 106 (22.6%)People = 83 (26.3%)
0
10
20
30
40
50
60
70
80
90
< 19 20 - 29 30 - 39 40 - 49 50 - 59 60 - 69 70 - 79 80 - 89
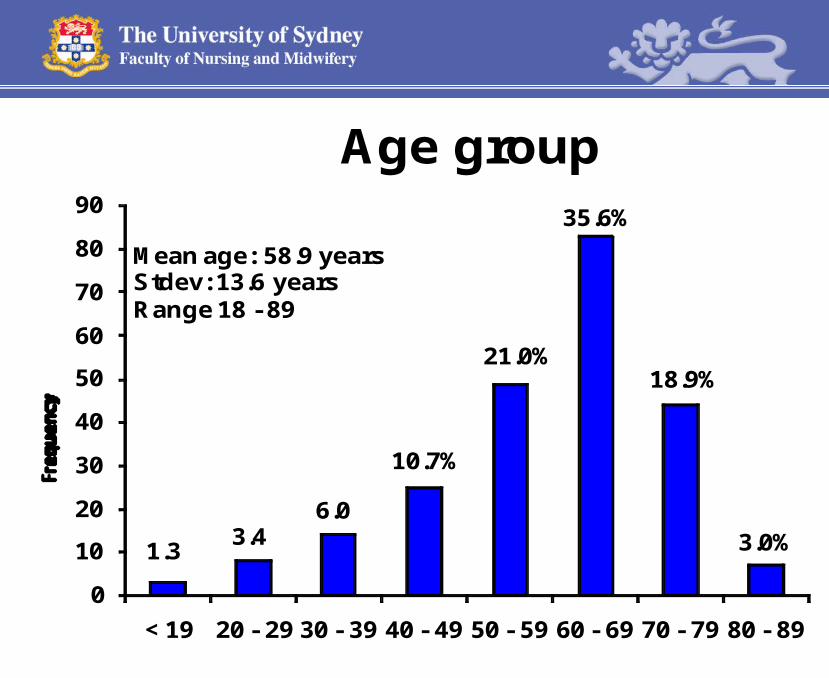
Age group
1.33.4
6.0
10.7%
21.0%
35.6%
18.9%
3.0%
Mean age: 58.9 yearsStdev: 13.6 yearsRange 18 - 89

0
10
20
30
40
50
60
Individuals on chemotherapy in last 6 months who made an unplanned presentation: Principal diagnosis
21.0% 19.7%
8.2%6.9%
5.6%4.7% 4.7% 3.4%

Admissions 317 of 363 visits (87.3%) resulted in a hospital
admission
Length of stay Median = 5 days
Range 1 – 70 days
Total bed days over the study period
2,622
Cost (estimated bed day $886)
$2,323,092

363 Presentations233 People
chemotherapy within 6 months
Chemotherapy in last 4 weeks
prior to visit
253 visits (53.9%)188 people (59.5%)
Chemotherapy in last 4 weeks
prior to visit
253 visits (53.9%)188 people (59.5%)
No Chemotherapyin last 4 weeks
prior to visit
110 visits (23.4%)45 people (14.2%)
No Chemotherapyin last 4 weeks
prior to visit
110 visits (23.4%)45 people (14.2%)
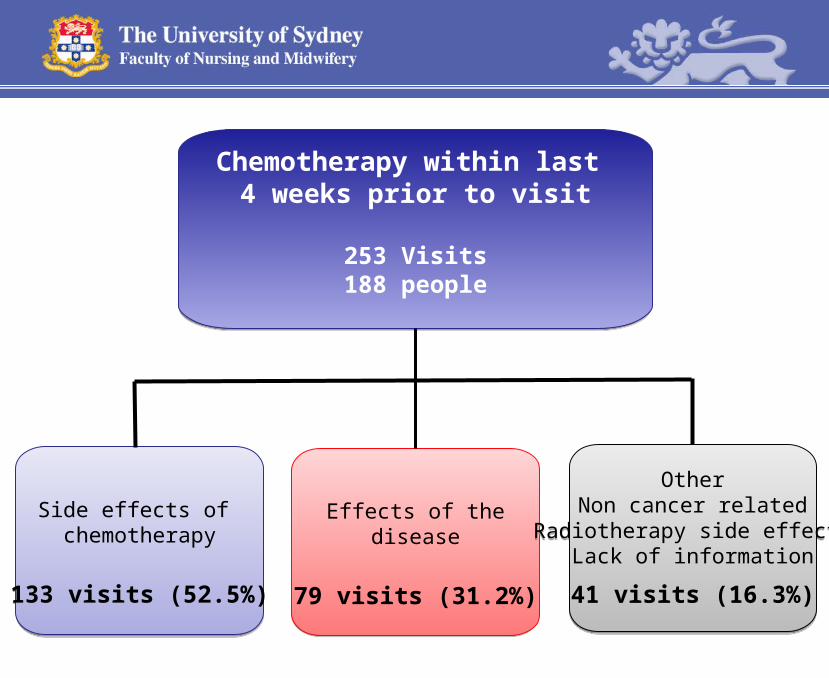
Chemotherapy within last 4 weeks prior to visit
253 Visits188 people
Chemotherapy within last 4 weeks prior to visit
253 Visits188 people
Side effects of chemotherapy
133 visits (52.5%)
Side effects of chemotherapy
133 visits (52.5%)
Effects of thedisease
79 visits (31.2%)
Effects of thedisease
79 visits (31.2%)
OtherNon cancer related
Radiotherapy side effectsLack of information
41 visits (16.3%)
OtherNon cancer related
Radiotherapy side effectsLack of information
41 visits (16.3%)

0
10
20
30
40
50
60
70
80
1 - 7 8 - 14 15 - 21 22 - 28
Visits made within 4 weeks of chemotherapy (n=253): day in cycle
33.3%
29.6%
20.7%
16.4%
Day in cycle
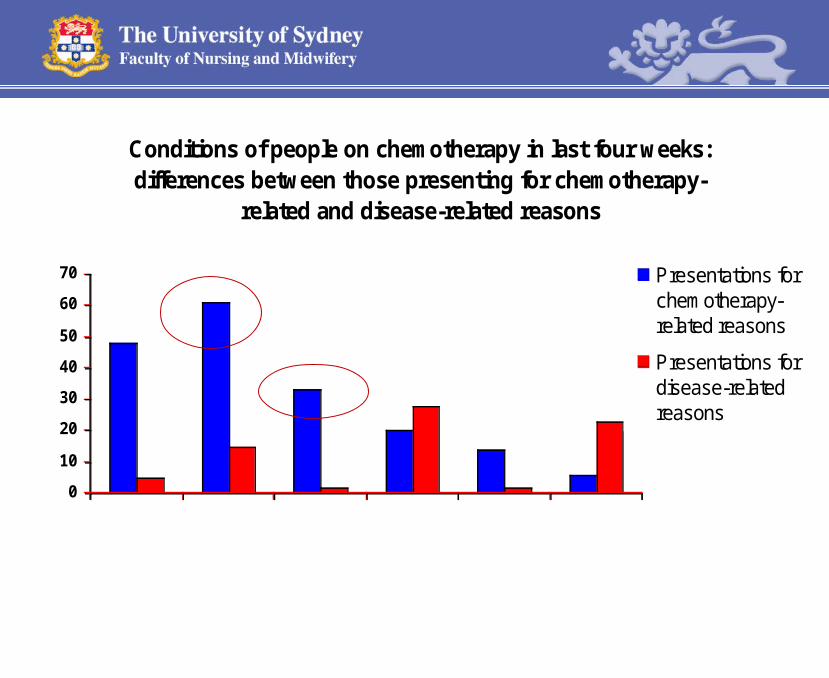
Conditions of people on chemotherapy in last four weeks: differences between those presenting for chemotherapy-
related and disease-related reasons
0
10
20
30
40
50
60
70
Fever and/or
febrileneutropenia
Nauseaand/orvomiting
Dehydration
Pain
AnaemiaShortnessof breath
Presentations forchemotherapy-related reasons
Presentations fordisease-relatedreasons

“My GP has seen me and she says, 'you're pretty awful again today, if you need support
then go back to your chemo people’… I’d rather do without it … and not overload the
resources.
But I just feel that I need it sometimes cause I’m really very shaky and there is nothing that we can do at home, that we can think of…I have
absolutely no coping skills...I felt awful coming up but at the same time I felt I needed support
in my struggle. And how do I get that at home?”
“My GP has seen me and she says, 'you're pretty awful again today, if you need support
then go back to your chemo people’… I’d rather do without it … and not overload the
resources.
But I just feel that I need it sometimes cause I’m really very shaky and there is nothing that we can do at home, that we can think of…I have
absolutely no coping skills...I felt awful coming up but at the same time I felt I needed support
in my struggle. And how do I get that at home?”
Woman (60 yrs) describes why she chose to come to the Cancer Centre(September 2008)

21
Wife, and main carer, of man (59 years) with Gastric Carcinoma. Unplanned visit to cancer centre 3 days after treatment (October 2008)
“I am a small person and he was barely able to walk.
It was hard to put him in the car ... It’s a lot for his
body because he is so weak. He is not able to walk
properly and he is not feeling well.
And that is why he doesn’t want to come here. You
wait and wait and you get to the point where it is
more and more.
There should be a way to avoid this situation. It
should be easier.”
“I am a small person and he was barely able to walk.
It was hard to put him in the car ... It’s a lot for his
body because he is so weak. He is not able to walk
properly and he is not feeling well.
And that is why he doesn’t want to come here. You
wait and wait and you get to the point where it is
more and more.
There should be a way to avoid this situation. It
should be easier.”
ConclusionConclusion• Chemotherapy
outpatients have significant unmet needs
• Increasing trend towards outpatient care
• Improved integration of tertiary and community care is needed to address the burden of chemotherapy side effects
22
Study ThreeStudy Three
Closing the circle of care:
Evaluating a shared care clinical pathway intervention for
chemotherapy outpatients
• RCT of community/hospital shared care clinical pathway intervention for patients receiving outpatient chemotherapy.
• H1 There is a statistically significant reduction in the number of unplanned presentations to hospital between the control and intervention groups
Aim• Determine if the intervention reduces the
number of unplanned presentations to hospital for chemotherapy outpatients; and
• Improve physical and psychosocial health outcomes.
• To explore the cost-effectiveness of the intervention, focusing on the potential reduction in hospital costs and improved quality of life.

Study Design• Multi-centre RCT of chemotherapy
outpatients undergoing chemotherapy cycles 1, 2 & 3
• Standard Treatment versus Clinical Pathway
• Target Recruitment : 300 patients
Intervention• Structured Community Nurse
Assessment and follow up post chemotherapy
• Clinical Pathway Guided Care
• Feedback to Cancer Centre

Community Nurse Education• Two Day Education Program:
– Trends in cancer– Chemotherapy – Symptom assessment– Supportive Care– Clinical Assessment– Study protocol– Patient education


Intervention: The CN Visit• The standardised visits will focus on:
– Assessment of the patient (physical and psychosocial and knowledge)
– Referral , provide care and advice as needed
– Electronic documentation Chemotherapy Symptom Assessment Scale (C-SAS)
Brown et al
2001
• C-SAS transferred (via palm pilot technology) to the patient’s specialist cancer centre and GP

Data Collection 4 time points• Baseline: demographic & treatment information• SF36 and time point 4
All time points:• Unplanned presentations to hospital• Patient participant quality of life measures;
• Hospital Anxiety and Depression Scale (HADS),
• Functional Assessment of Cancer Therapy – General (FACT-G)
• Cancer Behaviour Inventory – Long version (CBI-L).
• Individual and focus group interviews with HCT

Outcomes• Primary: A reduction in the proportion of
chemotherapy outpatients on cycles 1, 2 & 3 making an unplanned presentation to hospital.
• Secondary: Chemotherapy outpatients in the intervention group will have statistically significantly improved scores QoL measures compared with the control group.

Data Analysis Quantitative Data:• Poisson regression analysis • Repeated Measures Analysis of Variance
Economic Analysis:• Data linkage • Cost weights for DRG• Clinical outcomes: test for differences into index
of overall health-related quality of life using algorithms to convert response of the SF-36.

• Facilitating patient and carer education
• Coordinating the interface between community and cancer centre settings