wound ca re ad visor€¦ · woc, wcc, dwc, oms co-founder, wound care education institute...
TRANSCRIPT
November/December 2016 • Volume 5 • Number 6
WoundCareAdvisor.com
A Publication
Official journal of
WoundCareADVISOR
PRACTICAL ISSUES IN WOUND, SKIN, AND OSTOMY MANAGEMENT®
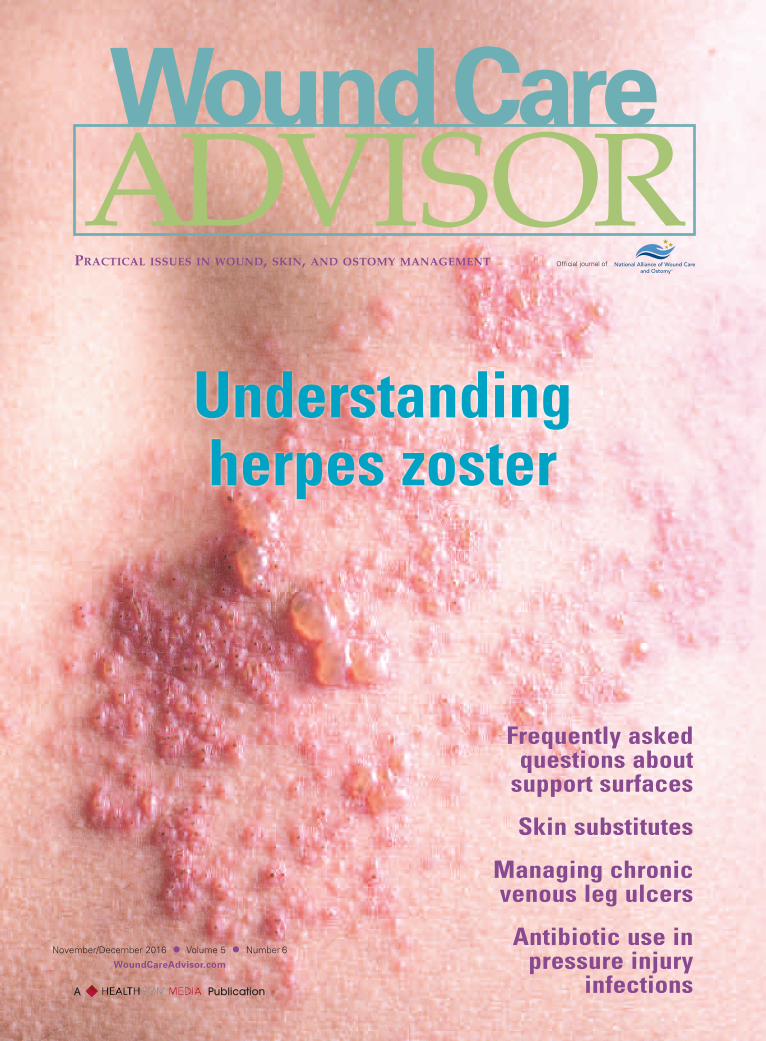
Understanding herpes zoster
Frequently askedquestions aboutsupport surfaces
Skin substitutes
Managing chronicvenous leg ulcers
Antibiotic use inpressure injury
infections

Reduce risk through proven clinical outcomes:
(study available upon request)
• Up to 4.4x faster healing of pressure ulcers which may
mean cost savings/decreased expense to the facility1
• Up to 2.6x lower hospital and emergency room visits1
Improve caregiver efficiency with Clinitron® Rite Hite® System
• Fully electric with an adjustable bed height
• Head of bed articulation (with HOB angle indicator)
Clinitron® Air Fluidized Therapy BedTried, Tested, and Trusted: Provide the highest quality of care for your higher-acuity patients
©2015 Hill-Rom Services, Inc. ALL RIGHTS RESERVED. 191289 rev 2 26-FEB-2015 ENG – US
For a free patient evaluation or for more information, contact your local Hill-Rom Account Manager by calling 800-638-2546.
1. Ochs RF, Horn SD, et al. Comparison of Air-Fluidized Therapy with Other Support Surfaces Used to Treat Pressure Ulcers in Nursing Home Residents. Ostomy Wound Management, 2005, 51(2):38-68.
The comforts of homeWe offer home care equipment solutions that meet the unique needs of patients dealing with spinal cord injuries, cerebral palsy, and other severe mobility-limiting conditions
• Talk directly to a Hill-Rom patient advocate
about our home care beds and patient lifts
• Learn about payment and payer options
• Ask about free delivery and set up
©2014 Hill-Rom Services, Inc. ALL RIGHTS RESERVED.189531 rev 1 15-OCT-2014 ENG – US
Contact Us Today 800.833.4291 [email protected] www.hill-rom.com

Wound Care Advisor • November/December 2016 • Volume 5, Number 6 WoundCareAdvisor.com 1
EDITOR-IN-CHIEFDonna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
Co-Founder, Wound Care Education InstituteLake Geneva, WI
EDITORIAL ADVISORY BOARD
Nenette L. Brown, RN, PHN,MSN/FNP, WCC
Wound Care Program CoordinatorSheriff’s Medical Services Division
San Diego, CA
Debra Clair, PhD, APN, RN, WOCN,WCC, DWC
Wound Care ProviderAlliance Community Hospital
Alliance, OH
Kulbir Dhillon, NP, WCCWound Care SpecialistSkilled Wound CareSacramento, CA
Fred BergVice President, Marketing/Business
DevelopmentNational Alliance of Wound Care and
OstomySt. Joseph, MI
Cindy Broadus, RN, BSHA, LNHA,CLNC, CLNI, CHCRM, WCC,
DWC, OMSExecutive Director
National Alliance of Wound Care and OstomySt. Joseph, MI
Gail Hebert, MS, RN, CWCN, WCC,DWC, OMS
Clinical instructorWound Care Education Institute
Plainfield, IL
Joy Hooper, BSN, RN, CWOCN,OMS, WCC
Owner and manager of MedicalCraft, LLCTifton, GA
Catherine Jackson, RN, MSN, WCCClinical Nurse Manager
Inpatient and Outpatient Wound CareMacNeal Hospital
Berwyn, IL
Jeffrey Jensen, DPM, FACFASDean and Professor of Podiatric
Medicine & SurgeryBarry University School of Podiatric
MedicineMiami Shores, FL
Rosalyn S. Jordan, RN, BSN, MSc,CWOCN, WCC
Director of Clinical EducationRecoverCare, LLCLouisville, KY
Jeff Kingery, RNVice President of Professional
DevelopmentRestorixHealthTarrytown, NY
Jeri Lundgren, RN, BSN, PHN, CWS,CWCN
Vice President of Clinical ConsultingJoerns
Charlotte, NC
Nancy Morgan, RN, BSN, MBA,WOC, WCC, DWC, OMS
Co-Founder, Wound Care EducationInstitute
Plainfield, IL
Steve Norton, CDT, CLT-LANACo-founder, Lymphedema & Wound Care
Education, LLCPresident, Lymphedema Products, LLC
Matawan, NJ
Bill Richlen, PT, WCC, CWS, DWCOwner
Infinitus, LLCChippewa Falls, WI
Lu Ann Reed, RN, MSN, CRRN,RNC, LNHA, WCC
Adjunct Clinical InstructorUniversity of Cincinnati
Cincinnati, OH
Stanley A. Rynkiewicz III, RN, MSN,WCC, DWC, CCS
AdministratorDeer Meadows Home Health and
Support Services, LLCBHP Services
Philadelphia, PA
Cheryl Robillard, PT, WCC, CLTClinical SpecialistAegis TherapiesMilwaukee WI
Donald A. Wollheim, MD, WCC,DWC, FAPWCA
Owner and Clinician, IMPLEXUS WoundCare Service, LLC Watertown, WI
Instructor, Wound Care EducationInstitute
Plainfield, IL
STAFFGroup Publisher
Gregory P. OsborneVice President of Publishing & Sales
Sofia GollerDirector, Marketing & Program Mgmt.
Tyra LondonEditor-in-Chief
Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMS
Editorial DirectorCynthia Saver, RN, MS
EditorKathy E. Goldberg
Copy EditorJulie CullenArt Director
David BeverageProduction Director
Christian Evans GartleyAccount Managers
Susan Schmidt, Renee Artuso,John Travaline, Stanley Anton
PUBLISHED BYHealthCom Media
259 Veterans Lane, Doylestown, PA 18901Tel: 215/489-7000 • Fax: 215/230-6931
Chief Executive OfficerGregory P. Osborne
Digital Design Manager Michelle Welliver
Finance Director/OperationsMaryAnn Fosbenner
Finance Manager/OperationsNancy J. Dengler
Wound Care Advisor (ISSN 2168-4421) is published byHealthCom Media, 259 Veterans Lane, Doylestown, PA18901. Printed in the USA. Copyright © 2016 by Health-Com Media. All rights reserved. No part of this publica-tion may be reproduced, stored, or transmitted in anyform or by any means, electronic or mechanical, includ-ing photocopy, recording, or any information storageand retrieval system, without permission in writing fromthe copyright holder. Send communication to Health-Com Media, 259 Veterans Lane, Doyles town, PA 18901.
The opinions expressed in the editorial and advertis-ing material in this issue are those of the authorsand advertisers and do not necessarily reflect theopinions or recommendations of the National Al-liance of Wound Care and Ostomy®; the EditorialAdvisory Board members; or the Publisher, Editors,and the staff of Wound Care Advisor.
Editorial Mission: Wound Care Advisor providesmultidisciplinary wound care professionals withpractical, evidence-based information on theclinical management of wounds. As the officialjournal of the National Alliance of Wound Careand Ostomy®, we are dedicated to deliveringsuccinct insights and information that our read-ers can immediately apply in practice and useto advance their professional growth.
Wound Care Advisor is written by skin and woundcare experts and presented in a reader-friendly elec-tronic format. Clinical content is peer reviewed.
The publication attempts to select authors who are knowl-edgeable in their fields; however, it does not warrant theexpertise of any author, nor is it responsible for any state-ments made by any author. Certain statements about theuse, dosage, efficacy, and characteristic of some drugsmentioned here reflect the opinions or investigational ex-perience of the author. Any procedures, medications, orother courses of diagnosis or treatment discussed or sug-gested by authors should not be used by clinicians with-out evaluations of their patients’ conditions and possiblecontraindications or danger in use, review of any applica-ble manufacturer’s prescribing information, and compari-son with the recommendations of other authorities.
2 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor
November/December 2016 • Volume 5 • Number 6WoundCareAdvisor.comCONTENTS
page 9
page 27
page 17
FEATURES
9 Herpes zoster: Understanding the disease, its treatment, and prevention By DeSales Foster DNP, CWOCN, CRNP, GNP-BC, AGACNP-BC Learn how to assess shingles and who should get the vaccine to prevent it.
21 Frequently asked questions about support surfaces By Armi S. Earlam, DNP, MPA, BSN, RN, CWOCN Support surfaces are a valuable tool in preventing pressure injuries. Here are answers to some commonly asked questions about them.
DEPARTMENTS
4 From the Editor Knowing when to ask for help
5 Clinical Notes
13 Best Practices Managing chronic venous leg ulcers — what’s the latest evidence?
Antibiotic use in pressure injury infections
19 Apple Bites Ostomy documentation tips
27 Business Consult What the mirror doesn’t tell you Skin substitutes: Understanding product differences
33 Clinician Resources
35 NAWCO News


4 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor
From theEDITOR
As a wound care expert, you’re proba-bly consulted for every eruption,scrape, and opening in a patient’s
skin. Occasionally during a patient assess-ment, you may scratch your head and askyourself, “What is this? I’ve never seen any-thing like it.” Most wound care experts want to help heal
everyone, and most of us love a challenge.But when should we step back and considerreferring the patient to another clinician? In a recent conversation, a healthcare cli-
nician told me about the “magic” protocolshe uses at the outpatient wound clinicwhere she works. A patient came to theclinic complaining that the current ostomyskin barrier kept leaking and wouldn’t stayin place longer than 2 days. The clinicianstarted the patient on her protocol, whichinvolves multiple ostomy products, some ofthem off-label, along with a heating pad toachieve an ostomy skin barrier that stays inplace for at least 3 weeks with no changerequired.For 3 weeks? Wow! The clinician was so
proud she was saving the patient money.But by asking a few questions, I found outthat:• the skin barrier manufacturer recom-mends a maximum 7-day wear time forthe product
• the clinician learned about the protocolfrom another clinician, who’d heardabout it from a patient
• none of the clinicians involved had osto-my management training
• the patient now has severe denudedskin around the stoma.
Moral of the story: Even though this clini-cian had good intentions, she should havereferred her patient to an ostomy specialist.She still would have saved her patient mon-ey and time and would most likely haveprevented the peristomal skin breakdown.When encountering a skin or wound
problem for the first time, we need to lookbeyond just the local wound bed and com-plete a holistic, detailed review of the pa-tient’s clinical history, including systemic, local, and psychosocial factors that affectwound healing. If you can’t determine anobvious cause or you lack the knowledgeor experience to deal with the patient’sproblem, initiate a referral immediately. Forwounds on the lower extremities, refer thepatient to a vascular surgeon or specialist orto another wound specialist; for a diabeticwound or toenail complications, refer thepatient to a diabetic specialist, podiatrist, oranother wound specialist; for an unknownrash, skin eruption, or allergic reaction, referthe patient to a dermatologist; and for osto-my or stoma-related problems, refer the pa-tient to an ostomy specialist or surgeon.Don’t let pride get in the way of doing
what’s best for your patients. To paraphraseKaren Marie Moning, author of Dreamfever,Strength isn’t about being able to do every-thing alone. Strength is knowing when to askfor help and not being too proud to do it.
Donna Sardina, RN, MHA, WCC, CWCMS, DWC, OMSEditor-in-Chief, Wound Care Advisor
Cofounder, Wound Care Education InstitutePlainfield, Illinois
Knowing when to ask for help

Prevalence of ostomy-relatedcomplications identified
One or more complications occur in 35%of patients by 1 year after ostomy surgery,according to a study in Ostomy WoundManagement. “The prevalence of ostomy-related com-
plications 1 year after ostomy surgery: Aprospective, descriptive, clinical studyA” reports that the most common surgicalcomplication is a colostomy hernia. Theuse of convexity is more common amongpatients with a stoma height ≤ 5 mm thanin patients with a stoma height > 5 mmand among patients who have emer-gency, as opposed to elective, surgery.
Braden Scale in long-term care
“A meta-analysis to evaluate the predictivevalidity of the Braden Scale for pressure ulcerrisk assessment in long-term careB,” pub-lished in Ostomy Wound Management,concludes that the scale has only moder-ate predictive validity and low predictivespecificity for pressure injuries in long-term care residents.
The researchers examined eight studieswith 1,489 residents meeting the criteria tobe included in the analysis.
TMA as an option for diabeticfoot gangrene
Transmetatarsal amputation (TMA) is oftena valuable option for patients with diabet-ic foot gangrene who need an amputation,concludes a study in International WoundJournal.The authors of “The care of trans-
metatarsal amputation in diabetic foot gan-greneC” reviewed 51 articles and note thatTMA can prevent “major limb loss andminimise loss of function.”
CNA education improves pressureinjury care
A 1-hour education program for certified
Wound Care Advisor • November/December 2016 • Volume 5, Number 6 WoundCareAdvisor.com 5
ClinicalNOTES

nursing assistants (CNAs) reduces pressureinjury and increases reporting of skinbreakdown, according to “Exploring the ef-fect of educating certified nursing assistantson pressure ulcer knowledge and incidencein a nursing home settingD,” published inOstomy Wound Management. The program, completed by 33 CNAs in
a care facility for residents age 55 yearsand older, included early identification,treatment, and prevention. From 3 monthsbefore the intervention to 3 months after,the number of pressure ulcers decreased12.3%, from 5 to 0, while CNA reports ofskin breakdown increased by 68%, from 8to 17.
Exercise and diabetes
Exercise interventions can improve staticbalance, lower-limb strength, and gait inolder adults with diabetes, reports astudy in the Journal of Diabetes and ItsComplications. “Exercise interventions for the improve-
ment of falls-related outcomes among olderadults with diabetes mellitus: A systematicreview and meta-analysesE” included 10randomized clinical trials.
Depressive symptoms common inpatients with chronic wounds
Symptoms of depression are common inpatients with wounds, particularly thosewith wounds of 90 days or longer in dura-
tion and with pain related to the woundsat initial examination, according to a studyin Wound Repair and Regeneration. “Depressive symptoms in patients with
wounds: A cross-sectional studyF” reportsthat 81.5% of the 260 patients had minimalto severe depressive symptoms, with 22.1%having moderate to severe symptoms.
Pioglitazone and diabetesprevention
“Pioglitazone prevents diabetes in patientswith insulin resistance and cerebrovasculardiseaseG” examined 3,876 patients with re-cent ischemic stroke or transient ischemicattack (TIA), no history of diabetes, fastingplasma glucose < 126 mg/dL, and insulinresistance by homeostasis model assess-ment of insulin resistance score > 3.0. Pa-tients were randomly assigned to pioglita-zone or placebo.The study in Diabetes Care concludes
that in patients with insulin resistance butwithout diabetes who have had a recentischemic stroke or TIA, pioglitazone de-creases both the risk of diabetes and therisk of subsequent ischemic events.
6 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor

Identifying risk of lymphedema
According to a study presented at the Amer-ican Society for Radiation Oncology 2016Annual Meeting, among patients who haveundergone radiation therapy after breastcancer, the risk for lymphedema is highest 2to 3 years after treatment. Results from the study, reportedI by Med-
scape, could affect when clinicians have pa-tients return for lymphedema monitoring.
Multidisciplinary team improvesvenous ulcer care
A multidisciplinary team approach to man-aging chronic venous ulcers increaseswound healing, according to an article inthe International Journal of Surgery.
“Management of venous ulcers: State of theartH” also concludes that a multidisciplinaryteam helps reduce wound-associated painand required daily wound treatments. n
Online ResourcesA. o-wm.com/article/prevalence-ostomy-related-complications-1-year-after-ostomy-surgery-prospective-descriptive
B. o-wm.com/article/meta-analysis-evaluate-predictive-validity-braden-scale-pressure-ulcer-risk-assessment-long
C. onlinelibrary.wiley.com/doi/10.1111/iwj.12682/full
D. o-wm.com/article/exploring-effect-educating-certified-nursing-assistants-pressure-ulcer-knowledge-and
E. jdcjournal.com/article/S1056-8727(16)30637-7/fulltext
F. onlinelibrary.wiley.com/doi/10.1111/wrr.12484/full
G. care.diabetesjournals.org/content/39/10/1684
H. sciencedirect.com/science/article/pii/S174391911630173X
I. medscape.com/viewarticle/869873
Present Your Wound Care CredentialsWith Distinction.
The NAWCO online Print Shop offers custom business materials that you can order online. Each piece is professionally designed to visually promote you and all your active NAWCO credentials.
Business CardsNote CardsPost Cards
To browse the print shop and order 24 hours a day, 7 days a week.
CLICK HERE

Wound Care Advisor • November/December 2016 • Volume 5, Number 6 WoundCareAdvisor.com 9
Herpes zoster (HZ, also calledshingles) is a painful conditionthat produces a maculopapularand vesicular rash. Usually,
the rash appears along a single der-matome (band) around one side of thebody or face. In most cases, pain, tingling, burning,
or itching occurs a few days before therash. Next, blisters form, scabbing over in7 to 10 days. In rare cases, the rash iswidespread, resembling varicella zoster(VZ, or chickenpox) rash. Pain can rangefrom mild to severe and may be dull,burning, or gnawing. It may last weeks,months, or even years after the blistersheal. Shingles on the face may impair vi-sion or hearing. According to the Centers for Disease
Control and Prevention (CDC), nearly 1 million Americans get shingles eachyear and one in three have it duringtheir lifetime. Caused by the same virusthat causes chickenpox, shingles can oc-cur in anyone who has had chickenpox.Most people who develop shingles havejust one lifetime episode, but a smallpercentage have second or even thirdepisodes.Risk increases with age. Nearly half of
shingles cases occur in people ages 60and older; about half of those older thanage 85 develop shingles. Immunocom-promised persons also are at higher risk.About 100 Americans die of shingles-re-
lated causes each year, nearly all of themelderly or immunocompromised.
How shingles developsAfter a person recovers from chickenpox,the VZ virus (VZV) lies dormant in the cra-nial nerves, dorsal roots, and sensory gan-glionic neurons. If this latent virus reacti-vates, it moves down the nerve fibers to theskin, where it multiplies to cause the rash.VZV can spread through direct contact withthe rash to someone who has never hadchickenpox—typically a child, who mightthen get chickenpox, not shingles.
Complications Shingles complications are more common
Herpes zoster: Understanding the disease, its treatment, and prevention Learn how to assess shingles and who should get the vaccine to prevent it. By DeSales Foster DNP, CWOCN, CRNP, GNP-BC, AGACNP-BC
10 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor
in elderly and immunocompromised pa-tients. One in five people with shinglesdevelops postherpetic neuralgia (PHN)—apainful, chronic condition in the area af-fected by VZV. Typically, PHN lasts longerthan 90 days after the shingles rash heals.Pain can be debilitating, leading to activitylimitations and decreased quality of life.(See Shingles complications.)
Signs and symptoms Signs and symptoms of shingles occur inthree stages.• Prodromal stage. Before the rash ap-
pears, patients may have pain, acuteneuritis, burning, itching, numbness, tin-gling, a stabbing sensation, fever, chills,headache, malaise, fatigue, and extremesensitivity on one side of body. Depres-sion and stomach upset may occur, too.
• Active stage. A unilateral erythematousand maculopapular rash arises in one tothree dermatomes, along with malaise,headache, nausea, and fever. Vesiclesform within 12 to 24 hours, pustulesappear in 1 to 7 days, and crusting oc-curs in 2 to 3 weeks. Once the crustsfall off, the skin remains erythematousand hyperpigmented or hypopigmentedwith scars.
• Chronic stage. After the rash resolves,PHN may occur. The pain may be con-stant, brief, or sharp. Pain from constantPHN usually is described as deep; briefpain as shooting or stabbing pain, pos-sibly tic-like. Sharp pain may radiateand can be triggered by light touch.
Diagnosis Differential diagnosis includes impetigo,contact dermatitis, folliculitis, scabies, in-sect bites, candidiasis, dermatitis herpeti-formis, and drug eruptions. If clinical di-agnosis isn’t possible, laboratory tests maybe done. The gold standard for diagnos-ing shingles is a tissue culture, but resultsmay take 3 to 7 days, delaying treatment.The enzyme-linked immune-sorbent assayand additional tests confirm diagnosis.Rapid diagnosis also may be obtained us-ing polymerase chain reaction. Laboratoryconfirmation is mandatory for pregnantwomen, newborns, immunocompromisedpatients, and those with atypical rashes.
TreatmentThe goal of treatment is to reduce painand complications, expedite rash healing,and decrease new lesions. Treatment de-creases viral shedding and risk to othersin contact with the patient. It should startimmediately to avoid cutaneous dissemi-
Besides postherpetic neuralgia, shingles complica-tions may include:• secondary bacterial skin infection• vasculopathy• myelopathy• meningoencephalitis• cerebellitis• viral dissemination • organ or visceral infection• meningitis• skin scarring• Hutchinson’s sign or herpes zoster (HZ)
ophthalmicus associated with lesions on the nose.
Immunosuppressed patients may develop a cuta-neous disseminated rash similar to that of a drug-re-lated eruption, as well as pneumonia, hepatitis, orencephalitis with or without rash. Shingles rash onthe face or head may cause vision or hearing prob-lems, eye infection and inflammation with pain,uveitis, keratitis, acute retinal necrosis, and progres-sive outer retinal necrosis, which may threaten vi-sion. An ophthalmologist should assess the patientimmediately and start antiviral therapy as soon asshingles is confirmed to help prevent hearing or vi-sion impairments.
Rare complicationsRamsay Hunt syndrome (RHS, or HZ oticus) is a rareneurologic disorder that can result from shingles af-fecting the facial nerve. Marked by facial palsy andan ear or mouth rash, RHS also can cause ear pain,ringing in the ears, hearing loss, nystagmus, vertigo,and vesicles in the ear canal. Zoster sine herpete,another rare complication, is marked by chronic low-er-extremity pain without a rash.
Shingles complications

Wound Care Advisor • November/December 2016 • Volume 5, Number 6 WoundCareAdvisor.com 11
nation, PHN, and other serious complica-tions. Starting antiviral therapy within 72hours of rash onset reduces PHN risk. Inelderly and immunocompromised patients,clinicians must act quickly to reduce therisk of cutaneous or visceral rash dissemi-nation, prevent secondary bacterial infec-tions, and decrease time to healing.Up to 4% of people with shingles need
to be hospitalized for I.V. antiviral thera-py (acyclovir or valacyclovir) to treat orhelp avoid complications related to ad-vanced age, immunosuppression, super-infection, and ocular or visceral involve-ment. All immunocompromised patientsshould receive treatment; those with or-gan transplants or disseminated shinglesshould be hospitalized for immediate I.V.antiviral therapy. Patients with neurologiccomplications typically receive 10 to 14days of I.V. acyclovir therapy and aremonitored closely for signs and symp-toms of stroke.In a double-blind study comparing vala-
cyclovir therapy (1,000 mg three timesdaily for 7 to 14 days) to acyclovir therapy(800 mg five times daily for 7 days), thetwo regimens yielded similar resolution ofcutaneous lesions. Valacyclovir produced aslight reduction in acute neuritis. Cranial neuropathies should be verified
by testing for VZV DNA or antiviral IgGantibody in cerebrospinal fluid. Patientsmay be treated with oral acyclovir, butthose who are immunocompromised orhave ophthalmic rash distribution requireI.V. acyclovir 10 to 15 mg/kg three timesdaily for 5 to 7 days.Supportive care includes use of nonadher-
ent dressings, soothing emollients, cleansing,and compresses to reduce the risk of bacteri-al superinfection. (See Home care.)
Treating PHN PHN treatment isn’t definitive. Medicationsused to manage shingles pain also can beused for PHN. They include antidepres-sants, analgesics, topical lidocaine or cap-
saicin, anticonvulsants, gabapentin, dival-proex sodium, tramadol, and opioids. Ab-lation and nerve blocks or stimulators alsomay be given.
Preventing shingles The shingles vaccine (Zostavax®) decreas-es the risk and severity of shingles, aswell as the risk and severity of PHN inpeople who develop shingles after vacci-nation. It reduces shingles incidence by64% in persons ages 60 to 69 and by 38%in those ages 70 and older. In personsages 70 and older, it reduces PHN inci-dence by 67%.A live attenuated vaccine, the vaccine is
approved to prevent shingles in adultsages 50 and older and is recommendedfor those ages 60 and older. Studies showit’s safe and effective, with no adverseside effects except headache and minordiscomfort at the injection site. In 2015, Marin et al studied the impact
of shingles vaccine in a matched case-con-trol study. Results showed a 58% reduc-tion in prodromal symptoms and a 61%reduction in PHN. This was the first studyto show reductions in pain severity anddiscomfort after vaccination. Further stud-ies are underway to determine if a shin-gles vaccine can be developed that willmaintain its efficacy as the adult ages. Anew HZ subunit vaccine (a vaccine free
Home care for patients with shingles may includeacyclovir topical cream, with or without antibioticointment, for those with signs of secondary bacterialinfection. Cool compresses may reduce itching,which can lead to secondary infections.
Teach home caregivers to protect themselvesfrom contact with the patient’s vesicles, especially ifthey haven’t received the shingles vaccine, and toavoid contact until the vesicles crust over. Urgethem to use protective gear. Encourage both pa-tients and caregivers to wash their hands frequentlyand avoid contact with pregnant or immunocompro-mised persons.
Home care

12 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor
from viral nucleic acid that contains onlyspecific protein subunits of the HZ virus)looks promising in maintaining efficacy at97% and doesn’t diminish with age.
Contraindications Contraindications for the shingles vaccineinclude:• AIDS or other clinical indications of hu-man immunodeficiency virus
• immunosuppressive therapy (includinghigh-dose corticosteroids)
• hematopoietic stem cell transplantation• recombinant human immune mediatorsand immune modulators
• current cancer treatment with radiationor chemotherapy
• bone marrow or lymphatic cancer (suchas lymphoma)
• congenital or hereditary immunodeficiency• pregnancy.
Women should avoid getting pregnantfor 3 months after receiving the vaccine.Also, persons with moderate or severeacute illness (including those with a tem-perature of 101.3° F [38.5 ° C] or higher)should wait until they recover before get-ting the vaccine.
How to help patients with shinglesSingles can be extremely painful and de-bilitating, even decreasing quality of life.By understanding the disease, its treat-ment, and complications, you can helpthose who have this illness. To help pre-vent shingles, teach patients about theshingles vaccine and urge those ages 60and older to get it. n
DeSales Foster is a wound care nurse practition-er at Riddle Memorial Hospital in Media, Penn-sylvania.
Selected referencesAlbrecht MA. Clinical manifestations of varicella-zoster virus infection: herpes zoster. UpToDate, Inc.;2016. uptodate.com/contents/clinical-manifestations-of-varicella-zoster-virus-infection-herpes-zoster?source=search_result&search=varicella-zoster+virus&selectedTitle=1%7E150
Bader MS. Herpes zoster: diagnostic, therapeutic,and preventive approaches. Postgrad Med. 2013;125(5):78-91.
Centers for Disease Control and Prevention. Shinglessurveillance. August 19, 2016. cdc.gov/shingles/surveillance.html.
Cohen JI. A new vaccine to prevent herpes zoster. N Engl J Med. 2015;372(22):2149-50.
Cunningham AL, Lal H, Kovac M, et al; ZOE-70Study Group. Efficacy of the herpes zoster subunitvaccine in adults 70 years of age or older. N Engl JMed. 2016;375(11):1019-32.
Devi MR, Haribabu Y, Velayudhankutty S, et al. Re-view on: shingles, its complications & management.Pharma Innov J. 2013;2(4):21-7.
Gilden D, Nagel M, Cohrs R, Mahalingam R, BairdN. Varicella zoster virus in the nervous system.F1000Res. 2015;4:pii.
Harpaz R, Ortega-Sanchez IR, Seward JF; AdvisoryCommittee on Immunization Practices, Centers forDisease Control and Prevention. Prevention of her-pes zoster: recommendations of the Advisory Com-mittee on Immunization Practices (ACIP). MMWRRecomm Rep. 2008;57(RR-5):1-30.
Johnson BH, Palmer L, Gatwood J, et al. Annual in-cidence rates of herpes zoster among an immuno-competent population in the United States. BMC In-fect Dis. 2015;15:502.
Lal H, Cunningham AL, Godeaux O, et al; ZOE-50Study Group. Efficacy of an adjuvanted herpeszoster subunit vaccine in older adults. N Engl J Med.2015;372(22):2087-96.
Marin M, Yawn BP, Hales CM, et al. Herpes zostervaccine effectiveness and manifestations of herpeszoster and associated pain by vaccination status.Hum Vaccin Immunother. 2015;11(5):1157-64.
Nagel MA, Gilden D. Neurological complications ofvaricella zoster virus reactivation. Curr Opin Neurol.2014;27(3):356-60.
Nagel MA, Gilden D. Update on varicella virus vas-culopathy. Curr Infect Dis Rep. 2014;16(6):407.
Oxman MN, Levin MJ, Johnson GR, et al; ShinglesPrevention Study Group. A vaccine to prevent her-pes zoster and postherpetic neuralgia in olderadults. N Engl J Med. 2005;352(22):2271-84.
The shingles vaccinedecreases the risk andseverity of shingles.

Managing chronicvenous leg ulcers— what’s thelatest evidence?By Jodi McDaniel, PhD, RN
Chronic venous leg ulcers (CVLUs) af-fect nearly 2.2 million Americans an-
nually, including an estimated 3.6% ofpeople over the age of 65. Given thatCVLU risk increases with age, the globalincidence is predicted to escalate dramati-cally because of the growing population ofolder adults. Annual CVLU treatment-relat-ed costs to the U.S. healthcare systemalone are upwards of $3.5 billion, whichare directly related to long healing timesand recurrence rates of over 50%. CVLUs are not only challenging and
costly to treat, but the associated morbiditysignificantly reduces quality of life. Thatmakes it critical for clinicians to chooseevidence-based treatment strategies toachieve maximum healing outcomes andminimize recurrence rates of these com-mon debilitating conditions. These strate-gies, which include compression therapy,specialized dressings, topical and oralmedications, and surgery, are used to re-duce edema, facilitate healing, and avertrecurrence. In 2006, the Wound Healing Society
(WHS) developed guidelines for treatingCVLUs based on human and animal stud-ies; the guidelines were updated in 2015by an advisory panel of academicians,clinicians, and researchers, all with ex-pertise in wound healing. The guidelinesare organized by categories: diagnosis,compression, infection control, wound
bed preparation, dressings, surgery, useof adjuvant agents (topical, device, andsystemic), and long-term maintenance.Each recommendation is evaluated ac-cording to strength of evidence. (See Lev-els of evidence.)WHS guidelines provide clinicians with
evidence-based treatment recommenda-tions for caring for patients with CVLUs. Asummary of the guidelines regarding com-pression, infection control, wound bedpreparation, dressings, and long-termmaintenance, is provided in this article.You can access the full guidelines athttp://onlinelibrary.wiley.com/doi/10.1111/wrr.12394/full.
Lower extremity compressionExternal compression has long been thegold standard for treating venous hyperten-sion and the associated edema and ulcera-tions of the lower extremities. Level 1 rec-ommendations from WHS state to use: • a class 3 (most supportive) high-com-pression system to enhance healing ofCVLUs. Methods of compression in-clude multilayered elastic compression,inelastic compression, Unna’s boot, andcompression stockings. Consider patientcost and comfort when choosing themethod.
• intermittent pneumatic pressure with orwithout compression dressings to stimu-late venous return.
Wound Care Advisor • November/December 2016 • Volume 5, Number 6 WoundCareAdvisor.com 13
BestPRACTICES
Infection controlPreventing or treating infections as soon aspossible are important because overgrowthof bacteria in the wound bed impedeswound healing. The only level I recom-mendation from WHS in this category is todebride (using sharp, enzymatic, mechani-cal, biological, or autolytic methods)necrotic or devitalized tissue that can be asource of bacterial growth. Level II recommendations:
• Collect a tissue biopsy or use a quantita-tive swab technique to determine thetype and level of infection in the CVLU.
• Prescribe an appropriate topical or sys-temic antimicrobial therapy based onthe findings from tissue biopsy or cul-ture and discontinue the antimicrobialagent when the bacteria is “in balance”(defined as ≤1 × 105 CFU/g of tissue withno beta-hemolytic streptococci) to re-duce the chances of cytotoxic effects orbacterial resistance.
• Use systemic gram-positive bactericidalantibiotics to treat cellulitis around theCVLU site.
• Reduce bacteria levels in CVLU tissuebefore trying surgical closure (≤1 × 105
CFU/g of tissue with no beta-hemolyticstreptococci).
Wound bed preparation Wound bed preparation is used to accel-erate healing or to facilitate the effective-ness of other therapeutic measures. Toachieve these goals, the level I recom-mendation from WHS is to document thehistory, recurrence, characteristics (loca-tion, size, exudate, staging, condition ofsurrounding skin, pain), and healing rateof CVLUs on a regular and ongoing basisto determine if care plans need reassess-ment.Level II recommendations:
• Complete a comprehensive history andphysical examination to assess for fac-tors that may be contributing to tissuedamage. These factors include systemicdiseases, medications, nutritional sta-tus, and potential causes of inadequatetissue perfusion and oxygenation, suchas dehydration and cigarette smoking.
• Perform maintenance debridement toremove cellular debris, necrotic tissue,excessive levels of bacteria, and senes-cent cells, which will help create anoptimal healing environment.
WHS also makes one level III recom-mendation, which is to cleanse thewound with sterile water or saline initial-
14 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor
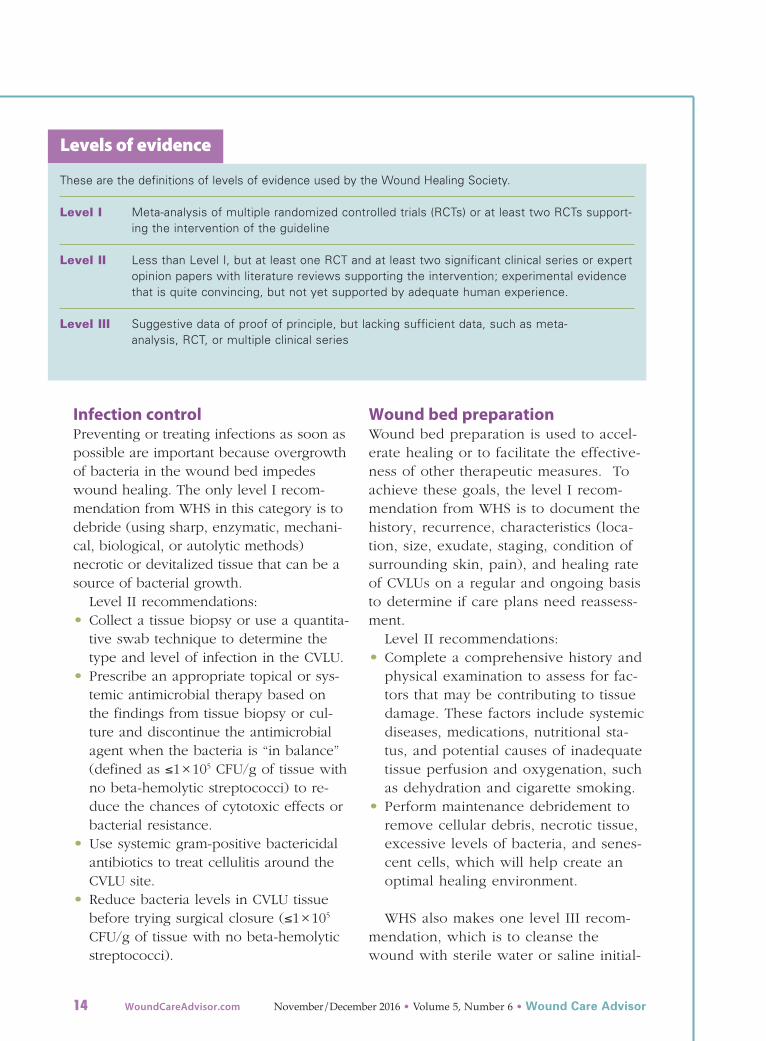
These are the definitions of levels of evidence used by the Wound Healing Society.
Level I Meta-analysis of multiple randomized controlled trials (RCTs) or at least two RCTs support-ing the intervention of the guideline
Level II Less than Level I, but at least one RCT and at least two significant clinical series or expertopinion papers with literature reviews supporting the intervention; experimental evidencethat is quite convincing, but not yet supported by adequate human experience.
Level III Suggestive data of proof of principle, but lacking sufficient data, such as meta-analysis, RCT, or multiple clinical series
Levels of evidence

KILLSSUPERBUGS
Pathogenic Bacteria:Acinetobacter baumannii
Carbapenem Resistant E. coli (CRE) Clostridium difficile (including spores)
Escherichia coliMethicillin Resistant Staphylococcus aureus (MRSA)
Proteus mirabilisPseudomonas aeruginosa
Serratia marcescensStaphylococcus aureus
Vancomycin Resistant Enterococcus faecalis (VRE)Pathogenic Fungi:
Aspergillus nigerCandida albicans
Pathogenic Virus:HIV
Anasept® Antimicrobial Skin & Wound Products• No known bacterial, fungal or viral
resistance to Anasept. • Safe, non-cytotoxic and tissue
compatible, • Clinically Tested* • 18 month to 2- year shelf life• Anasept Gel is Medicare reimbursed
HCPCS # A6248Anasept is a registered trademark of Anacapa Technologies, Inc*J. Lindfors, Ostomy/Wound Management. 2004; 50 (8): 28-41.
® 800-489-2591*www.anacapa-tech.net

ly and at dressing changes to remove de-bris. Using increased intermittent pres-sure to deliver the water or saline solu-tion is acceptable.Dressings WHS recommendations are to considerpatient activity, wound location, andperi-wound skin quality when choosing adressing that:• sustains a moist wound environment(for example, a continuously moistsaline gauze dressing), which promotescell migration, matrix formation, anddebridement and helps reduce CVLU-associated pain.
• diminishes wound exudate and there-fore protects skin around the CVLUfrom maceration.
• is cost effective (factor in cliniciantime, application time, healing rate,and unit cost).
• remains in place, reduces shear andfriction, and does not cause further tis-sue damage; adhesives are not requiredwhen using compression systems.(Note: This is the only level II recom-mendation; the others are level I.)
Another level I recommendation is toconsider using adjuvant therapies (topi-cal, device, or systemic) if there is nohealing progression within 3 to 6 weeksof beginning a treatment plan.
Long-term maintenance CVLUs are considered long-term prob-lems because of their high recurrencerates, so long-term maintenance is re-quired even after ulcers have healed.WHS guidelines for long-term mainte-
nance and prevention of CVLUs state thatpatients:• with healed CVLUs should wear com-
pression stockings continually and in-definitely to help reduce venous hy-pertension—the underlying cause ofCVLUs. (Level I recommendation.)
• should perform exercises that increasecalf muscle pump function on a regu-lar basis. (Level III recommendation.)
A patient-centered care plan developedby a multidisciplinary team that includesevidence-based treatment strategies forCVLUs will produce the best possible heal-ing outcomes and help prevent recur-rences of these recalcitrant wounds. n
Jodi McDaniel is an associate professor and direc-tor of the Honors Program at The Ohio State Uni-versity, Columbus, Ohio.
Selected referencesAlavi A, Sibbald RG, Phillips TJ, et al. What's new:Management of venous leg ulcers: treating venousleg ulcers. J Am Acad Dermatol. 2016;74(4):643-64;quiz 665-6.
Ashby RL, Gabe R, Ali S, et al. Clinical and cost-ef-fectiveness of compression hosiery versus compres-sion bandages in treatment of venous leg ulcers (Ve-nous leg Ulcer Study IV, VenUS IV): a randomisedcontrolled trial. Lancet. 2014;383(9920):871-9.
Beidler S, Douillet C, Berndt D, et al. Inflammatorycytokine levels in chronic venous insufficiency ulcertissue before and after compression therapy. J VascSurg. 2009;49(4):1013-20.
Bergan JJ, Pascarella L, Schmid-Schonbein GW.Pathogenesis of primary chronic venous disease: in-sights from animal models of venous hypertension.J Vasc Surg. 2008;47(1):183-92.
Marola S, Ferrarese A, Solej M, et al. Management ofvenous ulcers: state of the art. [published onlineahead of print June 21, 2016]. Int J Surg.doi:10.1016/j.ijsu.2016.06.015.
Marston W, Tang J, Kirsner RS, et al. Wound HealingSociety 2015 update on guidelines for venous ulcers.Wound Repair Regen. 2016;24(1):136-44.
Raffetto JD. Dermal pathology, cellular biology, andinflammation in chronic venous disease. ThrombRes. 2009;123(Supplement 4):S66-S71.
Rice JB, Desai U, Cummings AK, et al. Burden ofvenous leg ulcers in the United States. J Med Econ.2014;17(5):347-56.
16 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor

Antibiotic use inpressure injuryinfectionsBy Jeri Lundgren, BSN, RN, PHN, CWS, CWCN
Antibiotic overuse contributes to theproblems of antibiotic resistance and
healthcare acquired infections, such asClo stridium difficile. Antibiotic steward-ship programs improve patient outcomes,reduce antimicrobial resistance, and savemoney. These programs are designed toensure patients receive the right antibi-otic, at the right dose, at the right time,and for the right duration. Clinicians need to understand the
proper role of antibiotics in patients withpressure injuries (PIs) so optimal benefitsare achieved. Here are a few considera-tions to keep in mind.
First steps Before starting an antibiotic, culture thePI and use the results to choose the ap-propriate drug. Debride devitalized tissueto decrease bacterial growth. Support thepatient by addressing nutritional deficits,stabilizing glycemic control, improvingarterial blood flow, and reducing im-munosuppressant therapy, if possible.These actions will enhance antibiotic re-sponse and wound healing.
Role of antiseptics Antiseptics are agents that inhibit or de-stroy the development and growth of mi-croorganisms in or on living tissue. Theseagents have multiple targets and a broadspectrum of activity that includes bacteria,fungi, viruses, protozoa, and even prions.Antiseptics may be considered when
PIs are not expected to heal, but clini-cians want to control bacterial bioburden.Consider nontoxic topical antiseptics atthe appropriate strength for a limitedtime until bioburden is controlled. Commonly used antiseptics for PIs are
iodine compounds (slow-release cadex-omer iodine); silver compounds, includ-ing silver sulfadiazine; polyhexanide andpolyaminopropyl biguanide; chlorhexi-dine; sodium hypochlorite; and aceticacid. Discontinue the antiseptic once thePI is clean and the surrounding inflam-mation is reduced.
Role of topical antibioticsThe use of topical antibiotics for a locallyinfected PI is limited because of side ef-fects, resistance, and hypersensitivity re-actions. However, a short (2-week)course of topical antibiotics may be con-sidered in the following situations: • The PI is not healing despite properwound management.
• The PI appears clean, but continues tohave a bacterial bioburden. After thebioburden has decreased, discontinuethe topical antibiotic.
Silver and honey dressings are an optionfor PIs infected with multiple organismsbecause they offer broad antimicrobial cov-erage. Silver sulfadiazine may be helpfulfor heavily contaminated or infected PIs.Ensure the patient is not allergic to
honey or has silver or sulfur sensitivities.Silver may has toxic properties, so limitthe length of time it’s used.
Role of systemic antibioticsSystemic antibiotics are indicated for man-aging PIs with evidence of systemic infec-tion, such as positive blood cultures, sys-
Wound Care Advisor • November/December 2016 • Volume 5, Number 6 WoundCareAdvisor.com 17
temic inflammatory response syndrome,sepsis, advancing cellulitis, fasciitis, or os-teomyelitis. In the presence of ischemictissue, topical antibiotics may be used inconjunction with systemic antibiotics. Unlike topically applied agents, sys-
temic antibiotics can reach the base ofthe infected tissue. Antibiotics should bechosen based on confirmed antibioticsusceptibilities of the known pathogens.For life-threatening infections, empiricantibiotics should be based on local an-timicrobial susceptibility patterns andreevaluated when definitive cultures be-come available.Grossly infected or abscessed PIs
should be drained and debrided to treatrelated sepsis or advancing cellulitis be-fore starting systemic antibiotics.
Appropriate interventionInfected PIs can lead to sepsis. If usedappropriately, antiseptics and antibioticscan help reduce the risk of sepsis andantibiotic resistance. n
Jeri Lundgren is the president of Senior ProvidersResource in Cape Coral, Florida. She can be con-tacted at [email protected].
Selected referencesCenters for Disease Control and Prevention. Why In-patient Stewardship?. 2010. http://www.cdc.gov/getsmart/healthcare/inpatient-stewardship.html
National Pressure Ulcer Advisory Panel, European Pres-sure Ulcer Advisory Panel and Pan Pacific Pressure UlcerInjury Alliance. Prevention and Treatment of Pressure Ul-cers: Clinical Practice Guideline. Emily Haesler, ed. Os-borne Park, Western Australia: Cambridge Media; 2014.
Wound Ostomy and Continence Nurses Society.Guideline for Prevention and Management of Pres-sure Ulcers (Injuries). Mount Laurel, NJ: Wound, Os-tomy, and Continence Nurses Society; 2016.
Wound Care Advisor • November/December 2016 • Volume 5, Number 6 WoundCareAdvisor.com 19
Ostomydocumentationtips By Nancy Morgan, RN, BSN, MBA, WOC, WCC, DWC, OMS
In each issue of Wound Care Advisor,Apple Bites brings you a tool you canapply in your daily practice. In this issue,we’ll focus on documenting ostomy care.
General characteristics• Document if the diversion is an intestin-al or urinary ostomy, whether it’s tem-porary or permanent, and the loca-tion—abdominal quadrant, skin fold,umbilicus. (See Descriptor reference.)
• Describe the type of ostomy:• colostomy (colon)—sigmoid or de-scending colostomy, transversecolostomy, loop colostomy, ascend-ing colostomy
• ileostomy (small bowel)—ileoanalreservoir (J-pouch), continent ileosto-my (Kock pouch)
• urostomy (bladder)—continenturostomy, Indiana pouch, orthotopicneobladder.
• Document the presence and location ofbowel sounds.
Stoma information• Note the type:• loop (two openings through one stoma)• end (one stoma)
• double barrel (two distinct stomas).• Document the overall appearance(shiny, taut, edematous, dry, moist,pale, textured, smooth, bloody) and thepresence of stents, rods, drains (includetype and location).
• Describe the color (red, beefy red,pink, pale pink, purple, blue, black)and shape (round, oval, budded).
• Note the height:• flush—at skin level• prolapsed—telescoped out from theabdominal surface.
• Document the size in millimeters:• Round stomas are measured by diameter.
• Oval stomas are measured by widestlength and width.
• Describe the lumen:• location—straight up, side, level withskin, or centrally located
• number of lumens, stenosis, or stricture.
• Note: Document the location of thelumen by using the clock system,with the patient’s head at 12:00.
• Describe the odor—presence or ab-sence of odor, strong, foul, pungent, fe-cal, musty, sweet.
• Note whether the stoma and peristomalskin junction is intact or separated.
EffluentFor a fecal stoma, describe the amount,consistency, and overall appearance of ef-fluent—thick, viscous, liquid, pasty, oily,formed, soft, thin, tarry.
AppleBITESBITES
Dose from WCEI

For a urinary diversion, describe urinecharacteristics, volume, presence of odor(musty, fishy, fecal, acid), color (clear,cloudy, amber, straw, colored, bloodtinged), and presence of substances otherthan fluid (grit, crystals, mucous strands).
Peristomal skin• Describe the characteristics of peristom-al skin—color, edema, firmness, intact-ness, induration, pallor, lesions, texture,scar, incision, rash, staining, moisture.
• Assess a minimum of 2 inches out fromaround the stoma.
Appliance and accessories • Document the type of ostomy applianceand accessories. Include the pouchingsystem product, size, and product num-ber. Note the presence of a spout, theconvexity, and whether it’s a one-pieceor two-piece system,
• Observe and document proper functionand adhesion, and complications expe-rienced with appliance systems. Docu-ment any modifications to the care
plan, implementation of new orders,and referrals.
Other important information• Document pain—location, causative fac-tors, intensity, quality, duration, alleviatingfactors, patterns, variations, interventions.
• Note stoma or peristomal skin compli-cations—mucocutaneous separation,stenosis, necrosis, bleeding, dermatitis,folliculitis, peristomal hernia, caputmedusae, peristomal hyperplasia,pseudoverrucous lesions, allergic der-matitis, contact dermatitis, pouch leak-age, infection.
• Document patient and caregiver educa-tion—topics covered, level of understand-ing, and education materials distributed.n
Nancy Morgan, cofounder of the Wound Care
Education Institute, combines her expertise as a
Certified Wound Care Nurse with an extensive
background in wound care education and pro-
gram development as a nurse entrepreneur.
Information in Apple Bites is courtesy of the WoundCare Education Institute (WCEI), © 2016.
20 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor
It’s important to be precise in describing locations. The image below identifies terminology you can use; directional information is located to the right.
Descriptor reference
Righthypochondriac
region
Umbilical region
Right lateralor lumbar
region (flank)
Right iliacor inguinal
region
Right lowerquadrant
(RLQ)
Fixed anatomical directionsSuperior – up Inferior – down Anterior – front Posterior – backMedial – towards middle Lateral – away from middle
Directions attached to specimenCephal – towards head Caudal – towards tailVentral – towards belly Dorsal – towards back
Specialized directions for limbs Proximal – towards body Distal – away from body
Lefthypochondriacregion
Epigastric region
Left lateralor lumbarregion (flank)
Left iliacor inguinalregion
Left lowerquadrant(LLQ)
Right upperquadrant(RUQ)
Left upperquadrant(LUQ)
Suprapubic (pelvic) or hypogastric region
Wound Care Advisor • November/December 2016 • Volume 5, Number 6 WoundCareAdvisor.com 21
The National Pressure Ulcer Adviso-ry Panel (NPUAP) describes sup-port surfaces as “specialized de-vices for pressure redistribution
designed for management of tissue loads,microclimate, and/or other therapeutic func-tions.” These devices include specializedmattresses, mattress overlays, chair cushions,and pads used on transport stretchers, oper-ating room (OR) tables, examination or pro-cedure tables, and gurneys. Some supportsurfaces are part of an integrated bed sys-tem, which combines the bed frame andsupport surface into a single unit. Support surfaces must be used in con-
junction with other interventions, such asnutritional support, skin care, repositioning,pressure redistribution, risk identification,and patient and caregiver education. Al-though studies have shown that supportsurfaces can help decrease the incidence ofpressure injuries (PIs), there is no evidenceshowing one brand or type of support sur-face is better than another.
What does it mean when a supportsurface is described as reactive oractive? Reactive surfaces, also called reactive/con-tinuous low pressure, may be powered ornot powered and can adjust pressure redis-tribution only when a load (such as theweight of a patient) is applied to it. An active surface is always powered.
Pressure distribution is adjusted mechani-
cally, even when there is no patient on thesurface.
What materials are used in supportsurfaces? Materials include foam, gel, fluid, and sili-cone beads. Australian medical-grade sheep-skin is also used, but has limited availabilityin the United States. Some support surfaceshave covers made of Gore-Tex® or anothermaterial that helps reduce friction.
What do the terms immersion,envelopment, and bottoming outmean? Pressure redistribution with support sur-faces is achieved through immersion andenvelopment.Immersion refers to the fact that as the
body sinks into the surface, pressure is re-distributed over the entire area of contactand not just the bony prominences. Envel-opment is the ability of the support surfaceto conform evenly to irregularities, such asbody contours, linens, and the patient’s
Frequently asked questions about support surfaces Support surfaces are a valuable tool in preventing pressure injuries. Here are answers to some commonly asked questions about them. By Armi S. Earlam, DNP, MPA, BSN, RN, CWOCN

22 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor
clothing, without causing excessive pressureon the body.Bottoming out refers to the patient’s body
sinking in so deeply on the support surfacethat it rests against the bed frame or anothersurface, such as a gurney, that lacks suffi-cient cushioning.
What is microclimate control? Microclimate control (control of temperatureand moisture) is achieved by: • controlling the airflow against the skin bypumping air through minute perforationsin the surface cover
• increasing the exchange of air betweenthe skin and the surface through the useof porous covers that allow moistureevaporation and body heat dissipation.
This feature keeps the skin cool and dry.Microclimate control is beneficial for pa-
tients who are constantly moist (for exam-ple, diaphoretic or incontinent). Excessmoisture raises the risk of friction and shear,which can result in skin breakdown. Thecoolness feature helps avoid higher skintemperature, a risk factor for PIs.
What do the features lateralrotation, alternating pressure, lowair loss, and air fluidized mean? These features are the functional or thera-peutic components of a support surface.They can be used singly or in combination. With continuous lateral rotation, or simply
lateral rotation, the surface provides rota-tion longitudinally (head-to-toe), turning thepatient to a set degree, in a set duration,and at a set frequency. Rotation is limited to40 degrees or less to each side. Lateral rota-tion does not replace repositioning the pa-tient to address skin issues, nor does it pro-vide pressure redistribution or offloading.Instead, surfaces with this feature help facili-tate pulmonary hygiene among patientswith acute respiratory conditions. NPUAP defines alternating pressure as “a
feature of a support surface that provides
pressure redistribution via cyclic changes inloading and unloading as characterized byfrequency, duration, amplitude, and rate ofchange parameters.” Surfaces with alternat-ing pressure may be mattresses or overlaysand are always powered. They can changedistribution of load with or without appliedload—even when no patient is in the bed.These surfaces have air cells that cyclicallyinflate and deflate, thus changing the areasof the body under pressure. Low air loss means that the surface pro-
vides flow of air to help manage the micro-climate of the patient’s skin. Air-fluidized surfaces provide pressure re-
distribution by immersion and envelopment,using a fluid-like medium created by forcingair through silicone beads. Air-fluidized sur-faces are expensive and difficult to maintain;beds with these surfaces are usually rentedinstead of purchased. They are heavier thana standard bed, so are not always suitableto place in older homes.Air-fluidized beds are often used for pa-
tients with multiple full-thickness wounds orwho have undergone myocutaneous proce-dures. They are not typically recommendedfor a patient with an unstable spine or pul-monary disease. The fluid-like surface does-n’t provide sufficient support for a patientwith an unstable spine, and for patientswith pulmonary disease, the lack of firmsupport makes it difficult for patients tocough effectively.
What are general considerations formatching patients to appropriatesupport surfaces? It’s important to base the choice of supportsurface on individual patient needs. (SeeDetermining type of support surface.) For ex-ample, consider the patient’s weight, height,and shape. (Bariatric patients must usebariatric surfaces; be aware of the weightlimitation of the surfaces.)Other considerations include:
• risk for new PIs• number of current PIs, including severity

24 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor
and location• patient’s activity, mobility (for example,avoid surfaces that might make it difficultto get a patient out of bed), and moisture
• risk for falls and entrapment in the bed• appropriateness for the setting (for exam-ple, powered surfaces can’t be used in ahome without a reliable power source).
Consider contraindications when choos-ing a support surface. For example, reac-tive/constant low pressure, reactive/constantlow pressure with low air loss, active sur-faces with alternating pressure feature, andair-fluidized surfaces are contraindicated forpatients with unstable cervical, thoracic, andlumbar spines, and patients with cervical orskeletal traction.Assess the appropriateness of the choice
on a regular basis. For example, a patientwith multiple stage 3 PIs that have healedmay no longer need the surface with lowair loss but can now be placed on a reac-tive/constant low pressure surface. If a pa-tient experiences pain or discomfort with aparticular surface, consider alternatives.
What are important points toremember when using supportsurfaces? Education is key to promote optimal use ofthese surfaces. Staff such as nurses, certifiednursing assistants, and other team memberswho handle the surfaces, including house-keeping and maintenance staff, all need in-formation on how to use the support sur-face correctly. Education should extend tofamilies, caregivers, and patients in thehome setting. Although the manufacturer may state an
expected lifespan for a product, staff mustbe taught that the lifespan can be shorter,depending on use. Staff need to be awareof indicators of wear and tear; discoloration;any change in height or thickness of thesurface; any break in the seams, cover, zip-pers, flaps; breakdown of internal compo-nents; or presence of foul odor. Deficientproducts must be repaired or replaced. Other important points related to using
support surfaces include the following:• Ensure the appropriate type and numberof linens or liners are used with the sur-faces. For example, a liner with a plasticbottom is not ideal with low air loss sur-faces because the non-breathable featureof the plastic will not allow the air fromthe support surface to go through.
• Clean surfaces as specified by the manu-facturers. If the correct cleaning process isnot used, the surface poses an infectionrisk. Incorrect use of agents, for exampleusing products that destroy the integrityof the cover, also increases the risk ofcross-infection.
Most importantly, remember that patientsmust still be repositioned even if they are ina support surface. An active support surfaceshould be used when frequent manualrepositioning is not possible. When possi-ble, avoid positioning a patient with an ex-isting PI on the affected area.
What should facilities use as supportsurfaces in the OR, ED, andprocedure areas? Support surface options for the OR includeair, gel, and high-specification foam mat-tresses. Consider the patient position re-
The Wound, Ostomy and Continence Nurses Society developed an evidence- and consensus-based supportsurface algorithm, which is available at http://algorithm.wocn.org/#home. The algorithm notes that patientswith large, or multiple stage 2, 3, or 4 pressure injuries on the trunk or pelvis involving more than one turn-ing surface should be placed on a support surface with a low air loss or an air-fluidized feature. The algo-rithm also suggests that among patients with Braden moisture subscale scores of 2 or 1 (very moist or con-stantly moist), surfaces with a low air loss feature should be considered.
Determining type of support surface

Wound Care Advisor • November/December 2016 • Volume 5, Number 6 WoundCareAdvisor.com 25
quired for the procedure when making aselection. There are also pads with pres-sure redistribution properties that can beused for transport and on ED beds. Moreresearch is needed to determine the effec-tiveness and proper use of these supportsurfaces. When selecting products to usein these special situations, consider safety,care, and costs.
Understanding support surfaces Support surfaces are an integral part ofPI prevention and treatment. When se-lecting a surface, the patient’s individualneeds, including past experiences withthe surfaces, must be taken into consider-ation. It’s important for clinicians to con-tinuously assess patients for the appropri-ateness and the functionality of thesurface. n
Armi S. Earlam is the lead certified wound, osto-my, and continence nurse at Lutheran MedicalCenter in Wheat Ridge, Colorado.
Selected referencesCenters for Medicare and Medicaid Services. NationalCoverage Determination (NCD) for air-fluidized bed(280.8). cms.gov/medicare-coverage-database/de-tails/ncd-details.aspx?NCDId=228&ncdver=1&bc=AAAAgAAAAAAA&.
Mackey D, Watts C. Therapeutic surfaces for bedand chair. In Doughty D, McNichol L, eds. CoreCurriculum: Wound Management. Philadelphia, PA:Wolster Klower; 2016:362-83.
McNichol L, Watts C, Mackey D, et al. Identifyingthe right surface for the right patient at the righttime: generation and content validation of an algo-rithm for support surface selection. J Wound OstomyContinence Nurs. 2015;42(1):19-37.
Moore Z, Stephen Haynes J, Callaghan R. Preventionand management of pressure ulcers: support sur-faces. Br J Nurs. 2014;23(6):S36-S43.
National Pressure Advisory Panel. Terms and definitionsrelated to support surfaces.npuap.org/wp-content/uploads/2012/03/NPUAP_S3I_TD.pdf. 2007.
National Pressure Ulcer Advisory Panel, EuropeanPressure Ulcer Advisory Panel, & Pan Pacific Pres-sure Injury Alliance. Prevention and treatment ofpressure ulcers: clinical practice guidelines. OsbornePark, Australia: Cambridge Media; 2014.

Presented By
2017October 4-7, 2017 | www.woundseminar.com
www.wcei.net | 1-888-318-8536
National Conference
Experience what wound care education is all about. Wild on Wounds™ (WOW) is the national wound conference designed for healthcare professionals that are interested in enhancing their knowledge in skin and wound management. Clinicians come from all over the US to see, touch and participate in our hands-on workshops. Join us and learn about all the new and advanced wound care treatments and technologies to better help care for your patients.
Attend WOW for Free!Wound, Diabetic & Ostomy Certi cation Course.Attend one of these certi cation courses o ered in Las Vegas the week of October 2, 2017 and get a FREE ticket to the Wild On Wounds Conference!
Save the Date
This Wound Care Certi ed (WCC®) course o ers and an evidence-based approach to wound management with current standards of care practices to keep clinicians legally defensible at bedside.
This Diabetic Wound Certi ed (DWC®) course takes you through the science of the disease process, focuses on limb salvage and prevention, and covers the unique needs of a diabetic patient. This course is taught by a board certi ed DWC physician who is passionate about caring for diabetic patients.
This Ostomy Management Specialist (OMS) course will take you through the anatomy and physiology of the systems involved in fecal/urinary diversions. The course includes online pre-class modules followed by hands-on classroom sessions.

What the mirrordoesn’t tell you The amazing work andwonder within you
By Tracey Long, PhD, RN, MS, MSN, CDE, CNE,CHUC, CCRN
“Ihate my body.” “I’m such a fat, worth-less cow.” “Where did all these grayhairs and wrinkles come from?” “I have to-tal thunder thighs.” “How could anyonefind me attractive when I look like this?”“My body is such a burden.”If you’re like 97% of the American pop-
ulation, you’ve probably had thoughts likethese at some point. According to a sur-vey by Glamour magazine 30 years agoand updated in 2014, 54% of women areunhappy with their body and 80% claimthe mirror makes them feel bad aboutthemselves. Unhappiness about body im-age has been reported in girls as young asage 6. Even men admit to body-imageangst; from 1997 to 2001, the number ofmen who had cosmetic surgery increased256%. Clearly, we need to evaluate themessages the mirror is telling us. (SeeCampaigning for real beauty.)
Mirror, mirror, on the wall Although many of us rely on the messagesin the mirror as the absolute truth, weneed to be aware of the inherent distor-tions it may hold. Ever since 8,000 B.C.,when the mirror made its first appearance,people have been evaluating their person-al worth based on their physical appear-ance. Two opposite attitudes exist: Somepeople are fixated by their own faces, asshown by an obsession with “selfies.” Oth-
ers declare their body hatred throughoutthe day. We have a love-hate relationship with
the mirror—but the mirror may not alwaystell the truth. People with anorexia nervosasee a distorted view in the mirror; someview themselves as fat even though they’rescarily thin. The mere act of focusing onsomething, such as a nose or a mole, maymake it look larger in the mirror. Evenyour mood may affect the way you seeyourself. When you’re tired, angry, or anx-ious, the mirror may reflect your emotionsmore than your true physical image.
Wound Care Advisor • November/December 2016 • Volume 5, Number 6 WoundCareAdvisor.com 27
BusinessCONSULT
In 2004, Dove® commissioned a global study,called The Real Truth about Beauty, to further glob-al understanding of women, beauty, and well-be-ing—and the relationships among them. The studyfound only 2% of women would describe them-selves as beautiful.
Subsequently, Dove launched its Campaign forReal Beauty, which triggered a global discussionabout the need to define beauty more broadly. It us-es various vehicles, including media messages,partnerships, and training with the Girl Scouts ofAmerica and Boys and Girls Clubs, to promoteawareness and education for women and girls of allages. Its video “EvolutionA” shows how profession-al makeup artists, photo enhancement, and comput-er manipulation can make an average-lookingwoman look beautiful.
Campaigning for real beauty
28 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor
What the mirror tells youRelying on the mirror to tell you “who isthe fairest of them all” may not give youthe honest truth. But despite potentiallynegative messages people get from themirror, it can provide helpful information.It can tell you a lot about the outside andthe inside of your body. Although we focuson our exterior image, the mirror offersclues to the internal health of your body. Using your critical thinking assessment
skills, take an objective look at your skinand hair. The skin, the body’s largest or-gan, can provide feedback on your sleep(or lack thereof) and nutrition. Without ad-equate vitamin intake or sun, your skinmay look pale and flaccid; without ade-quate essential fatty acids, it may be dullor dry. Stress, overwork, and lack of pur-pose in your life may reflect in the eyesthat stare back at you. Your hair textureand natural color also can hint at the stateof your nutrition, exercise, and rest.
What the mirror doesn’t tell youThe mirror doesn’t tell you about the amaz-ing functions of your body systems, or thatyou and your body are the most brilliant
creations in the universe. As Shakespeare’sHamlet exclaimed, “What a piece of workis man! How noble in reason, how infinitein faculty! In form and moving how ex-press and admirable!” Your endocrine system, for instance, is
an amazing creation of numerous autonom-ic functions working through a negativefeedback loop of chemicals to regulatemany systems. It also balances your energylevels through the thyroid gland. And whenis the last time your thanked your adrenalglands for helping regulate your bloodpressure via cortisol and aldosterone? Thanks to auto-regulation, your body
can keep its temperature within the samegeneral range even when the environmentaround it changes constantly. Breathing iscontrolled by tissues in your carotid arter-ies that track carbon dioxide (CO2) concen-tration and send messages to the brain’srespiratory center. Your body breathesfaster or slower to eliminate CO2 as need-ed, all without your conscious awareness. Your pancreas produces both insulin and
glucagon, which naturally oppose each oth-er but work in harmony to balance bloodglucose levels. These levels affect the func-
The more you know about yourbody, the more you can appreci-ate it.
• The 60,000 miles of bloodvessels inside the averageadult are enough to travelaround the earth 2.5 times.
• Nerve impulses travel 250miles per hour.
• The body contains 70 octil-lion atoms—23 times morethan the 300 billion stars inour galaxy.
• The combined hair of a hu-man's head can support theweight of two elephants.
• Human bone is as strong asgranite and concrete. A blockof bone the size of a matchboxcan support 9 tons.
• The human brain can perform38 thousand trillion operationsper second, compared to the92 trillion performed by theworld’s most powerful super-computer.
• Your body creates 7 miles ofnew blood vessels for everypound of fat or muscle yougain to perfuse it.
• Each second, 25 million newbody cells are created.
• Your outer skin is replacedevery month.
• Besides the classic five sens-es, you also have a sense ofbalance, temperature, pain,emotions, air, hunger, thirst,and fullness.
• A red blood cell can travelthroughout your whole bodyin 20 seconds.
• The surface of one lung’scapillaries is as large as oneside of a tennis court.
• Your body makes about 1.5 Lof saliva each day.
Amazing body facts the mirror doesn’t tell you
Wound Care Advisor • November/December 2016 • Volume 5, Number 6 WoundCareAdvisor.com 29
tion of all three trillion cells in your body.Your glucose level rises in the morning toawaken you and give your cells energy tostart the day automatically. Somatostatinregulates the endocrine system, balancinginsulin and glucagon to work in completebalance without your attention.The mirror doesn’t tell you how well
your liver detoxifies drugs and chemicalsand maintains your blood glucose levelwhen you’re asleep. Nor does it revealthat your immune system constantly moni-tors and patrols your blood for foreignpatho gens, which it then kills through acomplex chemical cascade. Does it tellyou that your spleen has been workinghard to store white blood cells and recy-cle red blood cells?What the mirror doesn’t tell you about
your magnificent self is far more interest-ing and exciting than the cellulite you mayglimpse in your reflection. It doesn’t let onthat your body has innate abilities, such asauto-regulation, self-defense, and self-heal-ing. Even the guy who cut you off on thefreeway yesterday has an amazing physicalorchestra playing within him. (See Amaz-ing body facts the mirror doesn’t tell you.)
The clinician reflectionIronically, some clinicians who care for sickpatients and help promote health and heal-ing are unhealthy themselves. For example,research shows that occupational stress,poor coping behaviors, and lack of support
cause anxiety and depression in nurses.The longitudinal Nurses Health Study,which began in 1988, examines relation-ships among hormone replacement ther-apy, diet, exercise, and other lifestyle prac-tices and chronic illnesses. It found femalenurses’ health was no better than that of thegeneral populace. Ideally, clinicians’ healthshould mirror their knowledge about thehuman body, health, and illness. Unfortu-nately, knowledge alone doesn’t create vi-brant health. We should sing along with theDisney character Mulan, who asks, “Whenwill my reflection show who I truly am?” As clinicians, we can do better to reflect
the true inner beauty of our bodies—andproject that beauty in our lifestyles. Bal-ancing the mirror’s messages is the key.What the mirror doesn’t tell you can in-spire you to honor your body. What itdoes tell you can motivate you to care foryourself so you can better model healthybehaviors for patients.
Fixing the mirror’s reflectionIn our society of quick fixes and limitedwarranties, it’s easy—and often neces-sary—to replace just about everything. Wecan replace most material objects whenthey’re worn out. The only thing that can’tbe replaced is the human body. We canmisuse and abuse it, or treat it with lovingcare. (See Learning to love your reflection.) Despite the wondrous advances of med-
ical science (and plastic surgery), your
Here are some ways to changewhat you see in the mirror.
• When looking in the mirror, fo-cus on what you love.
• Stop comparing yourself to thecelebrities you see in fake air-brushed photos.
• Look past your face and hair soyou can pick up on health cues.
• Honor your body by giving itsome TLC.
• Take time to care for your body.
• Be grateful for your body sys-tems that are working well.
• Pay compliments to your inter-nal organs.
• Focus on your energy level, notyour weight.
Learning to love your reflection
30 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor
body is still your very essence. Although itcomes with a lifetime warranty, its qualityisn’t guaranteed; that’s up to you. So what does your mirror say to you?
And will you listen? n
Tracey Long is a professor of nursing for KaplanUniversity and International Service Learning in LasVegas, Nevada. As an identical twin, she some-times uses her twin sister as her mirror.
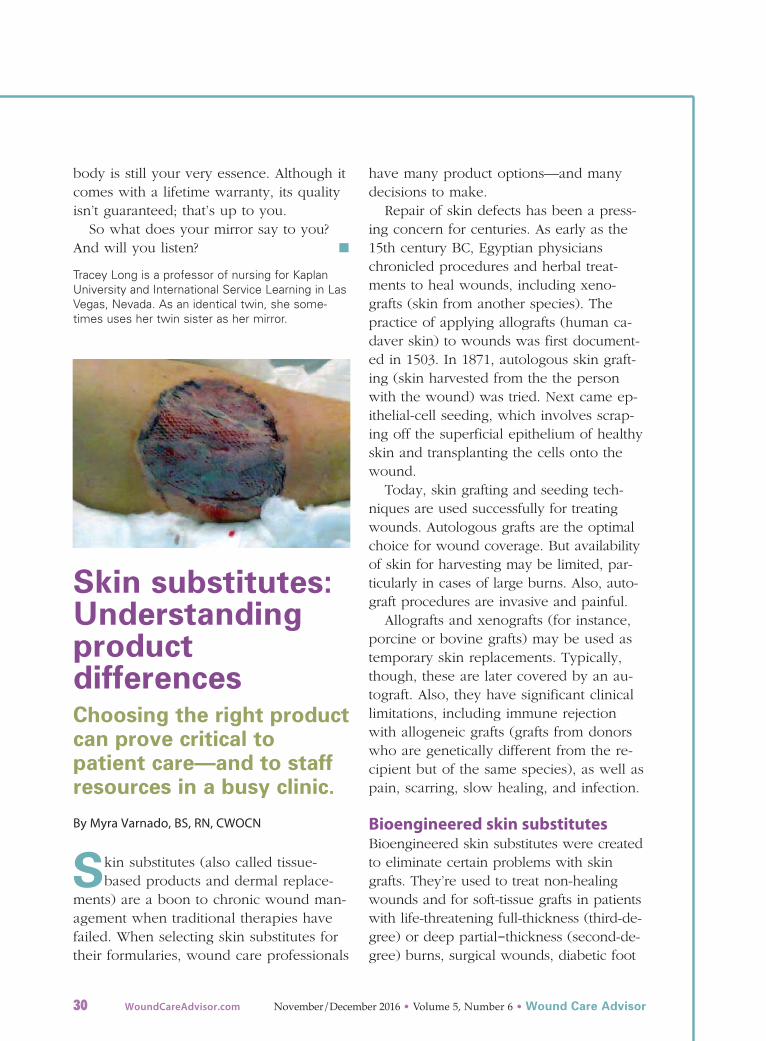
Skin substitutes:Understandingproductdifferences Choosing the right productcan prove critical topatient care—and to staffresources in a busy clinic.
By Myra Varnado, BS, RN, CWOCN
Skin substitutes (also called tissue-based products and dermal replace-
ments) are a boon to chronic wound man-agement when traditional therapies havefailed. When selecting skin substitutes fortheir formularies, wound care professionals
have many product options—and manydecisions to make. Repair of skin defects has been a press-
ing concern for centuries. As early as the15th century BC, Egyptian physicianschronicled procedures and herbal treat-ments to heal wounds, including xeno -grafts (skin from another species). Thepractice of applying allografts (human ca-daver skin) to wounds was first document-ed in 1503. In 1871, autologous skin graft-ing (skin harvested from the the personwith the wound) was tried. Next came ep-ithelial-cell seeding, which involves scrap-ing off the superficial epithelium of healthyskin and transplanting the cells onto thewound.Today, skin grafting and seeding tech-
niques are used successfully for treatingwounds. Autologous grafts are the optimalchoice for wound coverage. But availabilityof skin for harvesting may be limited, par-ticularly in cases of large burns. Also, auto-graft procedures are invasive and painful. Allografts and xenografts (for instance,
porcine or bovine grafts) may be used astemporary skin replacements. Typically,though, these are later covered by an au-tograft. Also, they have significant clinicallimitations, including immune rejectionwith allogeneic grafts (grafts from donorswho are genetically different from the re-cipient but of the same species), as well aspain, scarring, slow healing, and infection.
Bioengineered skin substitutesBioengineered skin substitutes were createdto eliminate certain problems with skingrafts. They’re used to treat non-healingwounds and for soft-tissue grafts in patientswith life-threatening full-thickness (third-de-gree) or deep partial-thickness (second-de-gree) burns, surgical wounds, diabetic foot

Wound Care Advisor • November/December 2016 • Volume 5, Number 6 WoundCareAdvisor.com 31
ulcers, venous ulcers, and certain otherconditions, including epidermolysis bullosa.(See Skin substitutes for chronic wounds.) Bioengineered skin substitutes contain
live human cells that are seeded onto amatrix and provided with the proteins andgrowth factors needed to grow and multi-ply into the desired tissue. Various biosyn-thetic and tissue-engineered human skinequivalents are manufactured under an ar-ray of trade names and marketed for vari-ous purposes. Because these products areprocured, produced, manufactured, orprocessed in different ways, they can’t beevaluated as equivalent. Bioengineered skin substitutes fall into
five classifications: • cultured epithelial autografts • human skin allografts derived from do-nated human cadaver tissue
• allogenic matrices derived from humanneonatal fibroblasts
• composite matrices derived from humankeratinocytes, fibroblasts, and bovine orporcine collagen
• acellular matrices derived from porcineor bovine collagen.
Some skin substitutes also possessunique regenerative properties. For in-stance, an allograft made of amniotic mem-brane and umbilical cord (NEOX®, madeby Amniox Medical) exhibits the same biol-ogy responsible for propagating fetal re-generative and scarless wound healing.When transplanted into the adult woundenvironment, these placental tissues modu-late inflammation and promote healing. In a 2016 study of 32 diabetic foot ulcers
by Raphael, an average of 1.68 NEOX appli-cations resulted in a healing rate of 87.5%. A2016 study by Caputo et al found that anamniotic membrane/umbilical cord allograft
proved effective in treating complex diabeticfoot ulcers with osteomyelitis; patients hada 78.8% healing rate after an average of 1.2applications. In contrast, a 2002 study byMargolis et al found that only 32% of dia-betic foot ulcers healed within 20 weeks ofstandard-of-care therapy (debridement,dressings, and topical ointment).
Choosing skin substitutesEfficacy of skin substitutes varies widely interms of the number of applications need-ed to close a wound, healing rates, andhealing times. Dehydrated amniotic skinsubstitutes are convenient to store and use,but are less potent than cryopreserved am-niotic/umbilical cord skin substitutes,which better preserve the structure and keybiological signaling of fetal tissues toquickly promote revascularization in theadult wound bed. Choosing the skin substi-tute to match the desired clinical outcomeis crucial. In addition, Medicare coveragevaries considerably by region. (See HowMedicare reimburses for skin substitutes.)
Ease of use and storage Some skin substitutes require more mainte-nance than others, potentially leading toproduct waste if storage conditions aren’t
Typically, chronic wounds (those that don’t re-spond to initial treatment despite appropriatecare) require advanced wound-healing interven-tions. A wound is considered chronic if it resistshealing after 4 to 12 weeks of treatment, depend-ing on wound type. The most common examplesof chronic wounds are those with complicatedetiologies, such as diabetic foot ulcers, venousleg ulcers, pressure injuries, and surgical wounds.Diabetic foot ulcers, venous leg ulcers, burns,and pressure injuries are most commonly treatedwith a tissue-based product.
Skin substitutes for chronic wounds

32 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor
optimal. For example, tissue-based productscontaining live cells have stringent shippingand application requirements; they’reshipped on dry ice and the patient must re-ceive the graft within hours after the productarrives at the wound center. During an icestorm in Dallas, a truck delivering a tissue-based skin substitute for one of our patientshad to wait out the storm on the side of theroad; the patient cancelled his appointmentdue to impassable roads. By the time the pa-tient rescheduled and the truck arrived withthe skin substitute, the product was nolonger usable and had to be thrown out. In contrast, a skin substitute that re-
mains stable in a wound center’s refrigera-tion unit is available when the patientneeds it, so treatment can start sooner thanwith a product that has a narrow windowfor use. For instance, NEOX can be refrig-erated safely at temperatures ranging from-112° to 39° F (-80° to 3.8° C) for up to 2years without structural or functional com-promise. If the product isn’t opened, it canbe exposed to room temperatures of 68°to 77° F (20° to 25° C) for up to 6 hours
and safely returned to cold storage. NEOXis the only cryopreserved amniotic mem-brane product that doesn’t need to bestored in a deep freezer.Also, skin substitutes that require exten-
sive preparation consume precious staff re-sources. One product, for example, needs tobe washed in water at a temperature not ex-ceeding 43° F (6.1 °C) before it can be ap-plied to a patient’s wound. This requires anextraordinary effort for personnel in a busywound clinic. Skin substitutes that can beexposed to room temperature before useare much more convenient and eliminatethe need for special equipment, such asthawing tubs.
Disadvantages of skin substitutesAs an advanced tissue treatment modality,skin substitutes are more expensive thanconventional wound dressings and mayhave more complex storage and preparationrequirements. To prevent waste, cliniciansshould choose a product that can be stockedin a range of sizes. Some substitutes areavailable only in small or very large sizes,which don’t conform to most wounds; thismeans the wound center ends up payingfor the excess product it must throw away.Also consider how many times a skin
substitute will need to be placed on a pa-tient’s wound before it closes. One thatneeds to be applied only twice is morecost effective than a less expensive onethat requires multiple applications. n
Myra Varnado is director of Clinical Wound andOstomy Services for Corstrata, a nationaltelemedicine company in Savannah, Georgia.Since 2000, she has been a member of theWound Guidelines Task Force for the Wound,Ostomy and Continence Nurses Society (WOCN).
Wound centers need to select efficacious and cost-effective skin substitutes that are reimbursable.The Medicare Local Coverage Determination (LCD)for each region determines which skin substitutesMedicare reimburses for, as well as the criteria pa-tients must meet for the skin substitute to be ap-plied. When I was chief nursing officer for a com-pany with many wound centers across the UnitedStates, I dealt with multiple LCDs, each with differ-ent requirements for applying skin substitutes. OneLCD might allow a particular skin substitute to beapplied anywhere on the body, while another limit-ed that product to the foot. In determining whichadvanced tissue products to place on the formularyfor our wound centers, we chose those with thewidest applicability to the most patients.
How Medicare reimburses for skin substitutes
(continued on page 34)
Here are a variety of resources for you toapply in your practice.
Pressure injury prevention in the OR
The perioperative environment can pose arisk for pressure injuries, particularly forpatients who are older or undergoinglengthy procedures. The Association ofPeriOperative Nurses developed a toolkitclinicians can use to help prevent injuries.The toolkit includes• an educational slide program on patientpositioning
• a sample pressure injury worksheet• a sample checklist for preventing pres-sure injuries
• instructions on how to use the MunroPressure Ulcer Risk Assessment Scalefor Perioperative Patients (for adults)
• sample case studies.
Workforce violence preventionportal
You can access a wealth of information atthe website portal Workplace Violence Pre-
vention ResourcesA from The Joint Commis-sion. The portal is dedicated to broadeningawareness of the problem and providing in-formation and resources, such as: • slides from presentations• past newsletters• sample policies• links to relevant resources from the feder-al government, states, and organizations
• how facilities are taking steps to pre-vent violence and responding effective-ly should it occur.
Influenza resources
Stay abreast of influenza activity in theUnited States at the Centers for DiseaseControl and Prevention (CDC) websiteB.Topics for clinicians include vaccination,antiviral drugs, infection prevention, anddiagnostic testing. You also can access free resources,
such as fact sheets, posters, stickers, pod-casts, and videos, to help educate yourpatients and the general public, anddownload an app so you can look up in-fluenza content on your mobile device.The CDC recommends a yearly flu vaccinefor everyone 6 months and older.
Opioid use disorder webinars
The American Psychiatric Nurses Associa-
Wound Care Advisor • November/December 2016 • Volume 5, Number 6 WoundCareAdvisor.com 33
ClinicianRESOURCES
tion is offering free webinarsC on effectivetreatments for opioid use disorders. Targetaudiences include registered nurses andadvanced practice nurses. The webinarsare available for nursing education contacthours.
The Joint Commission and pres-sure injuries
Access an advisory on preventing pressure
injuriesD from The Joint Commission. Theadvisory discusses the recent change interminology and tips for prevention. n
Online ResourcesA. jointcommission.org/workplace_violence.aspx
B. cdc.gov/flu/index.htm
C. apna.org/i4a/pages/index.cfm?pageID=6088
D. https://www.jointcommission.org/assets/1/23/Quick_Safety_Is-sue_25_July_20161.PDF
34 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor
Varnado is a primary author of WOCN’s guidelinefor management of wounds in patients withlower-extremity neuropathic disease. She is also aspeaker and consultant for Amniox Medical, Inc.,which markets the NEOX line of products.
Selected referencesAmin N, Doupis J. Diabetic foot disease: from theevaluation of the “foot at risk” to the novel diabeticulcer treatment modalities. World J Diabetes.2016;7(7):153-64.
Calota DR, Nitescu C, Florescu IP, et al. Surgicalmanagement of extensive burns treatment using al-lografts. J Med Life. 2012;5(4):486-90.
Caputo WJ, Vaquero C, Monterosa, A et al. A retro-spective study of cryopreserved umbilical cord as anadjunctive therapy to promote the healing of chron-ic, complex foot ulcers with underlying os-teomyelitis. Wound Repair Regen. 2016;24(5):885-93.
Cooke M, Tan EK, Mandrycky C, et al. Comparisonof cryopreserved amniotic membrane and umbilicalcord tissue with dehydrated amniotic membrane/chorion tissue. J Wound Care. 2014;23(10):465-74, 476.
Doughty DB, McNichol LL, eds. Wound, Ostomyand Continence Nurses Society® Core Curriculum:
Wound Management. Philadelphia, PA: Wound, Os-tomy and Continence Nurses Society; 2015.
Halim AS, Khoo TL, Mohd, et al. Biologic and syn-thetic skin substitutes: an overview. Indian J PlastSurg. 2010;43(Suppl):S23-8.
Hill-Rom. 2016 International Pressure Ulcer Preva-lence (IPUP) Survey. 2016. hill-rom.com/ipup/
Margolis DJ, Allen-Taylor L, Hoffstad O, et al. Dia-betic neuropathic foot ulcers. Diabetes Care. 2002;25(10):1835-9.
Nathoo R, Howe N, Cohen G. Skin substitutes: anoverview of the key players in wound management.J Clin Aesthet Dermatol. 2014;7(10):44-8.
National Pressure Ulcer Advisory Panel. NPUAPPressure Injury Stages. 2016. npuap.org/resources/educational-and-clinical-resources/npuap-pressure-injury-stages/
Raphael A. A single-centre, retrospective study ofcryopreserved umbilical cord/amniotic membranetissue for the treatment of diabetic foot ulcers. JWound Care. 2016;25(Suppl 7):S10-7.
Online ResourceA. youtube.com/watch?v=iYhCn0jf46U
(continued from page 32)

Wound Care Advisor • November/December 2016 • Volume 5, Number 6 WoundCareAdvisor.com 35
NAWCONEWS
Note from Executive Director
By Cindy Broadus, RN, BSHA, LNHA,CLNC, CLNI, CHCRM, WCC, DWC, OMS
This is the final article in the seriesabout certification. I’m not going totake up your time explaining or com-
paring the different wound certifications thatexist. If you have taken the steps to furtheryour education, enhance your knowledge,and obtain certification, then more than like-ly you have already performed your owndue diligence about what’s available. In-stead, I want to write about the benefits andmeaning of certification. After going through years of schooling
and extensive training to become a health-care professional, you may become physi-cally ill at the idea of attending more class-es or training. You’re definitely not the onlyone! As a clinician, you have experienced agrueling training period, so you may scoffat the idea of additional training to becomecertified. But there are significant benefitsto taking this step—not just for you, but al-so for your patients and coworkers.When you specialize in an area of health
care, such as wound care, you become aunique asset to your employer. You aretrained extensively, and your knowledgeand resources can be used in very specificsituations. As a certified healthcare profes-sional, your knowledge and experience canmake you difficult to replace, and yourservices become exceptionally valuable.Other additional personal benefits of certifi-cation include:• improving earning potential• expanding your opportunities for careeradvancement
• making yourself in demand, whichmeans career moves to other locationsmay be easier to make
• providing leadership opportunitiesamong your peers
• creating a sense of pride and accom-plishment.
Completing certification also shows youremployer that you’re willing to go that extramile to learn and contribute to the organiza-tion and to your patients. This speaks vol-umes about your commitment and the qual-ity of your work.Employers look for certified healthcare
professionals because those individuals gen-erally offer higher quality services. Manyemployers see you as a safe bet when youare certified. Those who are certified aremuch less likely to be involved in danger-ous or unsafe clinical practice, which re-duces legal risks for your employer. Thatnot only makes the employer happy, itmakes their insurance carrier happy as well.Of course, your employer also can brag a
little about your skills to their customers.Patients will feel safer and more comfort-able knowing that they are in the hands ofa certified healthcare professional. Thatcould increase the number of patients whoreceive care at your healthcare facility, andkeep them coming back—both things thatyour employer loves.You receive specialty training and access
to unique resources when you become certi-fied. This knowledge helps you provide bet-

36 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor
ter services to your patients. One of the ma-jor reasons that you became a clinician mayhave been because you love giving back toother people in need; certification offers youa unique way to give back that increases thequality of your services. Your patients cantake comfort knowing that they are in yourwell-trained hands. Consider the following:• You may be able to recognize potentialproblems before they happen andknow how to prevent them.
• Certification provides you with up-to-date knowledge and skills that you maynot have otherwise obtained.
• Studies indicate that the higher thenumber of certified nurses in an inten-sive care unit, the fewer serious injuries
occurred that were only distantly relat-ed to the patient’s condition (includingfalls and related injuries).
• Those certified in wound care score sig-nificantly higher in areas like classifica-tion of pressure injuries and specificwound closure procedures.
With more knowledge, you’re simply ableto provide better care to your patients, al-lowing them to recover faster and more fully.There is no better way to provide qualitycare than making sure your skills and knowl-edge are as complete and up to date as pos-sible. Certification means a lot of things to alot of people, so let me ask you this: Whatdoes certification mean to you? n
Beverly AbcedeVictor AbdelsayedRhonda AccardoKrystal AdamsJennifer AdamsCindy AdamsKelly AhrensRose AkamnonuCarrie AlbertIlene AlexanderDebora AllenAmanda AlmeidaEmilie AlonzoLeonel AltemaSolomon AlukoBetsy AlversonTammy AlversonAntonio Ambrosio, Jr.
Marvia AndersonEditha AndradaAlexis AningalanJeane AnthonyYolanda ApedaileKimberly ArchibaldGabriela ArguelloAshley ArmentiWilma ArnoldSharon ArvinSandra AstucuriTrisha AtkinsonColleen AubryGina AukerRebecca AxeBrent BabcockCherry BaileyMilan Bajmoczi
Parmalee BakerAaron BallSharon BaroniMiriam BarrettoDeborah BartmannSummer BatesValerie BeckErin BellMarianne BennettArlene BerdijoFrancesca BerrimanSherry BerryAnnemarie Bianchetto
Jose Joey BienvenidaAdrienne BiunnoAmy BlakeShannon BlakeNatacha BlanchetMelissa BlankenshipElizabeth BlondeauKaren BondarKarla Bonilla Carmona
Michael BonnerJeffrey BoppMeghan Boulmay-Cuevas
Cassandra BraderTammy BradleyLisa BradleyCari BranshawLisa BrattonAllison BraunJennifer BraunlichChristina BrechtelAaron BremnerMichelle BrewingtonSheila BrigoliMary BroemmelsickTraci BrownMegan BrownMelody BrownlieAmy BucholtzJewell BuettnerSarah BullardBrittany BurclTheodore Burge
New certificants
Below are WCC, DWC, and OMS certifi-cants who were certified from July 2016to September 2016.

Rachel BurnettShannyn BurnsDana ButtsHannah CainChristine CainBrandi CampbellTammie CamptonRebecca CanizalesWendy CardenasEdgar Cardona Traverzo
Cynthia CarlsonDeborah CarpenitoAmber CarpenterHeather CarpenterDanielle CarrMichelle CaswellBeena ChackoCynthia Chavooshian
Jessica ChenDana ClantonEugenio ClarkeStephanie ClineLisa CollinsSusanne CollinsSharmaine CollinsChristy CollomAmanda CongerShandra CooperCosmarie Cortes-Rivera
Samantha Cournoyer
Sarah CourvilleJoseph CovelliJeffrey CoxLaura CoxJennifer CoxRandi CoxBetty CraigMia CrawfordSarah Crawford
Kimberly CrawfordMorgan CrawfordClinton CrawfordLeigh CromerRobin CroninJennifer CurtissTonye Dakoru-Oruene
Amy DalzielTracy DanielsChelsea DannerSue DarizVanessa DarnellKeith DavidsonValerie DavidsonTina DavisVickie DavisRebecca DeaneNorma DennisBrandi DennyDana DeroskyMyrna DiazSarah DiDomenicoJenell DixonDeborah DodsonHillery DolfordNancee DroneVernon Drummond, Jr.
Callie DunbarJennifer DunivantTerri DunnLatisha EdgarAngel EisnaugleJanet EngelLori EngenMary-Jane EspereDebra EspositoGladys EstolasJenifer EubanksCindy EvansVanessa FadulChristina Falcone
Marybeth FanningMary FargoJulie FarmerTracy FarranAshlea FennerAmy FentonKimberlee FerrellKatherine FerrellPaula FerronMitzi FinnKendra FlingBernadine FloresAmanda FlorianJean FolchettiJessica FoxVictoria FoxellAmanda FranciscoHeather FranklinKurt FrauenpreisJenny FriedmanCarla FrymierCinquella FullertonDiana FurmanNeyhoney GalangKimberlee GalipeauJanice Galvin-GarciaTiffany GamabLisa GanekoBrittany GanoRobin GarofaloTiffany GarrettMichelle GazdakMeskerem Ge-bremedhinDiana GedamkeDeborah GeigerTonya GeiseSara GeislerMaria Victoria Geminiano Gatt
Debbie GentryYolanda GeorgeRandal Gerber
Maria Theresa Gerona
Renee GibbsAnn GillespieLisa GinappJillian GivensCrystal GlassburnTamesa GolstonVelia GonzalezRobin GoodRobin GoodingTyler GoodmanJennifer GoodpasterHeather GrantAfton GrapCrystal GreakColin GreenwoodJennifer GregorNerio GregorioDavid GriffithAmie GroceJennifer GroomJulie GrossNeelam GuptaSandra GutierrezPatricia GuzikLori GyldenvandLouis GyovaiMichelle HackerBrandy HairrellErin HalbachApril HallCharissa HambrockMelissa HammondKellee HaniganSandra HardinDiana HarlessPamala HarnessRecel HarrisRoberta HarrisRachael HartBrittany HaynesJennifer Held
Wound Care Advisor • November/December 2016 • Volume 5, Number 6 WoundCareAdvisor.com 37

Megan HellisKevin HelmondollarDemetria HendersonAndrea HenningsenTammy HeringMaria HeslerLonna HessCourtney HiceLaurie HigbeeTara HigginsAmy HillDiHuyen HoStephanie HoffmanNatalie HoganHope HolbenGregg HolcombTanya HolcombEvangeline HolleranTiffany HollingerJune HoodLesa HowardMandy HughesCynthia HunterLori HuntzingerJovan HussTracy InemanShelly InskoFrances IrbyKayleen IrwinBrian IscrupeSusan JacksonChandrasheneJackson
Stacy JamesonHeidi JanzRose JelinekJanatha JettersMary JirlesRenee JoderMarylyn JohnsBrittany JohnsonKelley JohnsonKristy Jones
Tonya JonesTracy JordanAmy JoryRodrigue JosephNatasa JurichRafael Justiniano Ramirez
Whitney KandelBeth KarnsSukhbir KaurCathy KavejonMeagan KeithLacey KellerLaura KellyChristina KernsDena KerschnerColleen KeyesMichele KirkJonathan KlingbeilLeah KnaggsAlison KnepperSara KobersteinShannon KoppertDorian KorzJulie KovachDiania KuftaKathy KulenichRamesh KumarDori LacapJennifer LadnerChristine LaGrangeClare LarsonKarla LathamRebecca LavenderTara LawlessRobin LawsonRanka LazicJanet LeeDoreen LeeMikyung LeeRenee LehrRinalda LeiteKeona Lemons
Elaine LendallBrenda LenegarCharles LesterBarbara LewisAmanda LewisSharlotte LewisAmanda LewisSamantha LeyClaudette LibanKristi LiebKevin Liebel IIJeanine Linehan-Burack
Monica LiptonPatricia LisakaGeorgianna LittleWendy LizakJessica LoriaLisa LoringTayana LouisJohn LubranoAundrea LudlowKatelin LyonsYuying MaLaura MaceCharlotte MacKnightJanelle MacSwainJeanne MafokouJoab MagaraLauren MahoneyKristen ManleyDavid MarciniecVicki MaritDiana MarkleJoelle MartinJanice MartinJanet MartinezMary MartinezRuth Martinez Camacho
Debra MasseyHannah MathesonKristin Mathewson
Sandra MathisCarrie MattixChristine MaustTamula MaxwellAndrea MayRita McBrideAmber McCaffertyTanya McCaffreyKaitlyn McCarthyMichelle McCarthyPatricia McCleesJaqueline McClenithan-Bland
Kelly McCoyDeanna McCoyMichele McCreightJeanne McCullenElizabeth McCurleyLori McGrathSandra McGuireKimberly McKevittAlan McMahanShalanda McNeilAlisha McVayKristin MelbournAmber MelunJose-Clemente Mendez
Lilia MercadoAnna MichelMai MilanMichael MillerShanella MillerMelanie MillerMelinda MillerJames Miller IIIKelly MilliganLori MinerLala MinerValerie MitchellClaudia MolinaCathleen MondfransValerie Moore
38 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor
Angela MooreShellie Moore-Hernandez
Mary Anne Moraleda
Lisa MoralesSalvador MoralesIrma Morales LopezRachel MorganRachelle MorganNicole MorinErin MorrowMary MorseMagdalena MorseOma MullinsRobin MurrayAmanda MyersRosa NaniaDebra NegleyGuy Nelson, Jr.Pamela NewlunLorna Nichols-Turner
Noelle NikasPamela NodleyDiana NoreGeorge NormoyleEverlyne Nyamwange
Mary OakesTabitha ObenourIsabelle OforiWemimo OlagbajuTiwalade OlawuyiImelda OrdonezAaron OrtegoAlma Ortiz NievesAraseli OssonDorothy OwsleyZeferina PadillaRemuel PadlanSuzzane Paguia-Patigas
Stephanie Papacostas
Jill ParrottMary ParsonsSondra PassmoreAngela PattersonLamika PattonDebra PautzMagdalena PawelekAmie PenningtonJomala PerkinsAmanda PerrionPatricia PetersenErin PetrySamantha PettigrewJane PhamAmy PhillipsIngrid PiedrahitaMaureen PilatiMyriam Pinchinat-Vassor
Karen PitchfordElizabeth PlataSonja PoseyLana PotocnjakJill PoupartJohn PreeceWanda PrinceSabine Prince-Bataille
Melissa PritchardFely PulaCrystal QuinnAngela RabuckColleen RaderAnna RakJocelyn RamseyChristopher RedilLori ReeseSandra ReisJustine RelosLaurie ReserGayle Rex
Joan RexfordJillian ReynoldsDavid RichardsKathleen RichesJimmy RicottoneLori RileyKacy RileyFiona RippleJolene RitcheyMarie Rivera Polanco
Janese RixDana RoachKristin RobbinsLisa RobertsMargaret RobertsonMaritza Rodriguez, MD
Wendy RoesslerStaci RogersCynthia RogersJessica RoisumCatherine RoseJennifer RosierIla RoskeRobert RossYael RothJennifer RothacherKimberly RoyerKayli RozelleRheannon Rundstrom
Mallory RusichJaime RyanMelissa SalazarLeah SalterLisa SalvatoreHolly SamuelsWinnie SandersRuth Santiago MarinMarcus SantiniPamela SardyDaniel Satterfield
Laura ScalfLeah SchellenbergJutta SchimmollerTamara SchirtzingerNicole SchmidtKimberly Schuch-Estep
Melissa ScottSharon Scott-Bellinger
Redmond SeeJeanette SeidofCrystal SeyboldFransesca ShannonAngela SharpLois ShawCynthia ShawMichelle SheetsDeborah SherronShelby ShipleyKatie ShoemakerLinda Lee Showerman
Kyle SimmsValerie SingletonNannette Sinigaglia Orengo
Laura SizemoreTerrill SkawMichele SmithKristina SmithRita Smith-ShawPamela SnelgroveNorma SolisHeather SosbyDavid SpenceTabitha SpinelliKatherine SprysJennifer StacyMarsha StechschulteJuliet SteinhoffDiana StetlerMelissa Stone
Wound Care Advisor • November/December 2016 • Volume 5, Number 6 WoundCareAdvisor.com 39
Suzanne StosichThomasina StoutJade StoverKatherine StrandJennifer StricklandTroy StrubingKyndall StuckyRonda StumpLadina SuberKristi SuchPamela SulekAlysia SweeneyRose SweeneyHeather SwinkPatricia TarawaliMaria TarkirShannon TateVeronica TautgesLindsay TaylorCharise TaylorKimberly TealAutumn TeaterGloria TercyakJoan TerlisnerZachary ThomasonJennifer ThompsonTommie ThorntonKimberly ThurmanLinda TillmanGenevieve TipsonAurora TiptonAndrea TorokCheryl TraceyDeala TrahanKimyen TranKaren TrifonoffMichelle TroutmanTracy TurnerCrystal UlbrightBrandi UrbanZofia UscinskiTheresa ValentDonald Van Boxel
Douglas Van HornMary VargasBillie VarnerMarcel VasquezWendy VeitchFreddie Velazquez Feliciano
Duane VerhasseltEliasib Vias CorderoSheila VillaceranJo Anna Villegas Marquez
Laura VinesMichele VingiaDenise ViningElena VolkovPamela Von BuschAmy WagnerAleisha WalburnJamey WalkerMikel WalkerMichelle WalkerChristine WalmsleyStacy WaltersDeborah WarfeAmanda WarnerHayley WarnerKathryn WatfordCooper WattElaine WelchDanielle WellerKelly WelshLisa WentzellLisa WepkingLena WheatAngela WheatonAngela WhiteKaren WhiteWendy WhitkanackAmy WhitlowCarrie WiegingJoshua WilliamsDeloria Williams
Dianna WillisErik WilsonCharlotte WilsonStefanie WinklerSusan WiseJennifer WoodRebecca WoodsLisa WooldridgePaul WrubelConnie WymanDeanna WymanJaymark YapeChristiana YeboahAudrey YoungbloodGrace ZamoranoJamie ZnidarsichAngela ZookJoni Zoz
Phyllis AbrahamsonAdelfa AcideraJanice AdawayPamela AdkinsJames AkindunbiVilma AlbertoDina Almeida-McGlotten
Robert AndersenSarah AndersonBarbara AndersonGabriela Andrade-Lopez
Ann AndruszkoJesi ArcherElizabeth ArityRaymund ArzadonJackie AtkinsonRenata BaieveSandy BaileyWendy BakerJacquelyn BakerLynn BarryStephanie BattaglinoRachael Beauchemin
Kelli BennettSanjeev BhatiaMarlene BilelloAnita BirdHeather BogdanovTeresa BowenThomas BoyesLinda BradenTanya Braunschweig
Kathleen BrighamWallace Brinkman, Jr.
Antonio BrownAyana BrownKendra BrownTracey BruceSarah BrunnerShelia BuffordLisa BurlisonKristian BurnhamTracy BuxtonRebecca CampbellEgbert CaoRosangela CarmonaAlana Carver Labrum
Deborah Casagrande
Sandy Castaneda
40 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor
Recertified certificants Below are WCC,DWC, and OMS certificants whowere recertifiedfrom July 2016 toSeptember 2016.

Katherine CastilloMichelle CepedaCatherine ChunDebra CingariLynne ClarkJane ClarryElizabeth CloverMichele ConeMargarita CoreasBertha CorralMarcilla CouittAndrea CrnkoMary CummingsDiane CurrenSusan CurryTeresa DanielsMiriam de SouzaFred DeanMaria DeBruyneChristina DeckerBrandi Deitrich Erickson
Eliud Del ToroRivera MDDeanna DelaraNatalie DeLongMelanie DominguezKrzysztof DraganLucinda DriggersKaren DumkeMildred DunnPaula DyerRoxanne EarleTracie EastDianne EdwardsCharles EricksonJulio EsquivelMaribel FalzoneAmy FannMadeline FiorelloDana FitzhenryJoan FloydSarah Fourman
Deborah FoxAndrea FranceJean FrankCatherine Friel-Dombeck
Jennifer FullenKaren FungKimberly GagnonKathy GardAngelita GarlitosPatricia GartlandLeena GeevargheseJoseph GiglioJolyne GilesNataliya GillilandMary GlattCathleen GohlikeLiberty Gonzales-Cabebe
Kimberly GoolsbyKathryne GorbyMarianneGorzkowskiMichelle GrattonJoAnne GreenePaige GregarRebecca Gurule-Lovato
Aireen Gutierrez, MD
Miriam GuzmanJennifer HaleRose HammondShadine HarveyJoshua HaynesKelly HaywardErin HebertHoli HeffronAlexander HellingerSilvia HinderliterSusan HofstetterRona HolandezJenna Hollinger
Debra HoneycuttSukhyune HongSheila HonlSusan HookerMonte HooverGeorgeta IacobBrian IscrupeJacqueline JacksonCarol JaconettiManish JainAshly JarrettAlicia JeromeColinda JonesMary JonesRhonda JonesSandra JonjoChristene JosephJanice KastnerSusan KennerlyJulia KhanShahida KhattakDosun KimWendy KinsmanAndrea KleessJanice KleinAnn KlinkusoomLinda KluthTammy KubeckaJoseph LachPatricia LarsonJohn LautenschlagerLacie LeBlancLinda LeblondJosephine LedesmaJelene LedesmaRobin LeeShannon LienLisa LindseyKimberly LinseJeanne LipelyFaith LoiselleJennifer LosheYolanda Loveless
Carole LowensteinPatricia LutzKaye LynchEmily MahnenMisty MartinLeanne MathisJoi McMillonSonny MeekLandon MetcalfLinda MichaudFay Micner-WeissKaren MillsCatrina Mitchell-Smith
Carla MitschGertrudes MonroeTina MooreMaria MoralesSandra MorenoBelma MorenoLinda MorganDonna MorrowPhyllis MulletTracie NakamuraSheryl NewmanDawn NimtzJuanita OlingerBonnie PannillLisa ParisiSeema PatelMaria PerezMa Teresa PerezJanet PerhachJoan PerroneMary PerryJuzell PettisLana PortRamona PratherTyla Pratt-WildmanCristina PresbiteroSusan PtacekCherry RavaloJoshua Richardson
Wound Care Advisor • November/December 2016 • Volume 5, Number 6 WoundCareAdvisor.com 41

Heather RichardsonJillian RiveraEduardo RiveraJoan RobertsRita Roberts SlackVictor Robles PadroJohn RogersKimberly RosatiRoxanne RoseKristina RushJaime RussellDonna RussoNatalie SaemmerGina SalernoEla SaludJoanne SalyarsCarla SalzerBonnie SchwartzMargery Seidel
Isabelle SerapionNikelle SevereKimberly SheridanJulia ShillingfordTina ShurleyJennifer SiwekChristina SlivkanchAmanda SmalleyPamela SmithSusan SmithMaria Jesusa Soriano
Pamela SpadePhyllis SpeirSharon StermerDawn StoneDeborah StormsCatherine Sudduth Wallbank
Michele SwainDebra SwansonJulie TallmanLee TerrillKelly TherrienYvonne Thornton-Headley
Sara ThurlowPaula TimpanaroAndrew TingueElizabeth TokunbohErlinda TomHongxia TongAndrea TorokJulie TorresMariah TumbarelloJune TurnerMarcia TurnerLaura Usher
Michael VaccaTiffany VaughnGuillermo VicencioErma VillarrealCarrie VincentJulie WagnerGwendolyn WassellAmanda WeissShawna WesselsPamela WestElizabeth WestonAlicia WilliamsConnie WinterlingRoberta WrightAmber YanesAlla YusupovaJohn ZachmanKaren ZanelliVera Zlotin n
1 in 3 women dies of heart disease and stroke. It’s not just a man’s disease. You can prevent it.BLAZE A NEW ONE FOR 43 MILLION WOMEN.
MAKE A CHANGE AT GoRedForWomen.org
TM G
o Re
d tr
adem
ark
of A
HA,
Red
Dre
ss tr
adem
ark
of D
HH
S.
42 WoundCareAdvisor.com November/December 2016 • Volume 5, Number 6 • Wound Care Advisor