wound care in the community: infection, exudate and … · 2014-10-20 · jcn 2014, vol 28, no 5 43...
TRANSCRIPT

JCN 2014, Vol 28, No 5 43
WOUND CARE
Unlike in the hospital setting where nurses are often able to draw on a number of fellow
expert professionals when presented with a particular clinical problem, in the community, nurses are more isolated and may be forced to make clinical decisions alone and without access to specialist opinion (Queen’s Nursing Institute [QNI), 2009).
Nowhere is this truer than in the realm of wound care, where treatment choice can have a serious effect on healing and nurses often have to make ‘on-the-spot’ decisions (Hallett et al, 2000). Whereas the inpatient nurse may have access to onsite infection control teams, tissue viability specialist nurses, link nurses and various medical specialties such as vascular, plastic surgery, surgical, etc, the community practitioner may have to act alone to identify and commence treatment in a range of wound complications — infection; excess
Wound care in the community: infection, exudate and conformability
exudate; correct dressing choice, to name but a few — without immediate recourse to wound care specialists. This was backed up by research from Drew et al (2007), which found that over 70% of wound care was carried out in the community.
Similarly, while the inpatient nurse may have an in-depth knowledge of a particular specialty, the community nurse is required to have a wide understanding of many subjects — including different wound types and their treatments, ranging from burns, the compression therapy required in leg ulcers, through to the intensive techniques involved in managing diabetic foot ulcers, for example (Mahoney, 2014).
This article examines some of the common wound issues that the community nurse may have to assess and diagnose such as excess exudate, infection and patient concordance (Mahoney, 2014). The author also looks at a versatile wound dressing (Durafiber® Ag; Smith & Nephew), which has a variety of applications in
primary care and can form a useful part of the community nurses’ wound care toolkit (Table 1; Figure 1).
WOUND CARE IN THE COMMUNITY
Due to the wide range of wound types seen in the community, it is important that community nurses have a working knowledge of some of the more common symptoms and/or problems that they are likely to encounter. However, with wound care being just one element of the extensive knowledge base required by community nurses, it can be hard to keep abreast of the latest developments and techniques (Nash Greally and Wardick, 2013). It is, therefore, crucial that community nurses have access to clear and concise wound care information, which will not only improve their knowledge of innovative equipment and techniques (Dowsett, 2009), but also make sure that patients continue to receive evidence-based care in order to prevent and manage complications.
Tracey Morgan, clinical nurse specialist, tissue viability, Aneurin Bevan University Health Board, Wales
Community nurses require a wide skill set to deal with the variety of clinical presentations they meet in any given day. This includes wound care, which can present nurses with a range of management challenges, i.e. how to combat infection, which kind of dressings to use to control exudate volume and how to ensure that dressings provide patient comfort and do not further damage the wound or skin on removal. It is important, therefore, that community nurses have access to a range of versatile products that can be used in a variety of clinical situations and which are also cost-effective. This article examines some of the common wound care issues that community nurses can face, as well as looking at how a versatile wound dressing (Durafiber® Ag; Smith & Nephew) — which has a variety of applications in primary care — can help with some of these issues.
KEYWORDS:Wound care Infection Wound coverage Exudate
Tracey Morgan
THE SCIENCE — INFECTION AND EXUDATE
Community nurses can use wound exudate to glean important information on a wound’s condition. The properties of wound exudate such as volume, colour, viscosity and odour all provide clues to the state of the wound, such as its bacterial load and infection status (WUWHS, 2007), for example, a wound infected with bacteria may have a ‘green’ colour or tinge.
© 2014
Wou
nd C
are P
eople
Ltd

44 JCN 2014, Vol 28, No 5
Wound pain Swelling Feeling of ‘warmth’ in the tissues Purulent wound discharge Malodour Fever.
There are a number of stages that
lead to a wound becoming infected, which involve a delicate balance between the amount of bacteria present and the ability of the patient’s defenses to fight off infection (Butcher, 2013): Contamination: the presence in
the wound of low numbers of bacteria
Colonisation: the absence of effective patient defenses, which means bacteria can multiply
Critical colonisation: where the numbers of bacteria begin to impact on wound healing.
Many bacterial species can be involved in wound infection, with one study of 676 post surgical patients who had clear signs and symptoms of wound infection identifying a number of different bacterial strains, the most common being (Giacometti, 2000): Staphylococcus aureus
(191 patients) Pseudomonas aeruginosa
(170 patients) Escherichia coli (53 patients) Staphylococcus epidermidis
(48 patients) Enterococcus faecalis
(38 patients).
WOUND CARE
contaminated with a certain number of organisms and most wounds go on to heal despite this (Butcher, 2013). However, understanding when a wound is about to become infected is not easy, as there is no ‘set’ number of bacteria for a wound to become infected. A diagnosis of wound infection is usually based on the presence of ‘classic’ signs and symptoms (Butcher, 2013; Cutting and Harding, 1994; World Union of Wound Healing Societies [WUWHS], 2008): Erythema (red skin colouration,
resulting from capillary congestion and often due to inflammation)
WOUND TYPES COMMONLY FOUND IN THE COMMUNITY
Community nurses may be called upon to deal with a range of wounds in the community, including: Leg ulcers Pressure ulcers Diabetic foot ulcers Surgical wounds Traumatic wounds Donor sites Partial thickness burns Fungating wounds.
However, by far the most common wounds seen by community nurses will be chronic wounds that are struggling to heal, particularly, pressure ulcers, diabetic foot ulcers and venous leg ulcers (Health Service Executive, 2009). These wounds can involve ongoing treatment, and, while they all have their own particular treatment requirements, for example, leg ulcers require compression bandaging, pressure ulcers require regular repositioning etc, there are some issues that are common to all which community nurses need to identify and address, including: Infection risk Excess exudate production Ensuring that dressing choice is
conformable and does not cause trauma or pain at dressing change.
INFECTION
It is normal for a wound to be
Figure 1.Durafiber Ag is available in a range of sizes..
Table 1: What is Durafiber Ag?Durafiber Ag is an absorbent, non-woven, silver-containing antimicrobial gelling dressing designed for use in a range of wounds, including chronic and acute, full thickness, partial thickness, or shallow granulating exuding wounds. For the community nurse who has to deal with a wide range of wounds, Durafiber Ag’s versatility is an asset, particularly as it can be used on the following: Leg ulcers Pressure ulcers Diabetic ulcers Surgical wounds Traumatic wounds Donor sites Partial thickness burns Tunnelling and fistulae wounds Wounds left to heal by secondary intention Wounds prone to bleeding, such as those that have been surgically or mechanically debrided Fungating wounds.
While Durafiber Ag assists in the management of wounds prone to minor bleeding, it is not intended to be used as a surgical sponge in heavily bleeding wounds.
© 2014
Wou
nd C
are P
eople
Ltd

JCN 2014, Vol 28, No 5 45
‘The use of silver in the manufacture of Durafiber Ag means that it provides antimicrobial action for up to seven days (in vitro) against a broad spectrum of common wound pathogens’
Many dressings are designed specifically to deal with exudate, for example, some form a gel on contact with wound fluid that absorbs excess fluid, locks exudate away from the wound and provides a moist environment to support autolytic debridement.
Any dressing required to absorb exudate requires some of the following characteristics (Adderley, 2008; Stephen-Haynes, 2011): High absorbency, thereby reducing
dressing frequency The ability to ‘lock away’ exudate
within its structure Ability to be used under
compression bandaging Easy to remove, thereby
minimising trauma and pain at dressing changes
Conformity to the wound site.
Durafiber Ag is specifically designed to form a gel on contact with wound fluid, absorbing excess exudate, and ‘locking’ it away from the wound (Dowler, 2010). This provides a moist environment to support autolytic debridement (Myers, 2012) and means that the dressing conforms to the wound bed (Forlee et al, 2014).
ADDITIONAL DRESSING CHARACTERISTICS
The following factors need to be considered by community nurses when choosing a dressing that will protect the full extent of the wound area.
Conformability The conformability of a dressing — or how well it ‘fits’ the wound site and is able to deal with elements such as pain on removal, leakage, patient positioning and ‘wear and tear’ — is crucial, particularly as no one wound is the same. Wounds can be a range of sizes, depths, in different anatomical positions, as well as forming cavities or skin flaps where exudate and bacteria can collect, greatly increasing the risk of infection (Bowler et al, 2010).
Coverage Dressings also need to provide adequate coverage of the wound bed, both to promote a moist wound healing environment, and prevent
When a wound becomes infected, this not only affects the patient negatively, but also has a deleterious effect on healthcare budgets, leading to higher treatment costs and rising numbers of inpatients (Cook and Ousey, 2011).
Antimicrobial dressingsButcher (2013) points to guidelines on the management of wound infection (European Wound Management Association [EWMA], 2006; WUWHS, 2008), which suggest that topical antimicrobial dressings are useful in reducing wound bioburden. These dressings work in a variety of ways — some incorporate ingredients that interrupt the ability of bacteria to thrive; some are poisonous to cells; others ‘bind’ bacteria to the dressing, which is then removed at dressing change.
Studies have recommended antimicrobial agents such as iodine, silver, honey and polyhexamethylene biguanide (PHMB) and these are considered to be the first line of treatment in wound infection (Cooper, 2004), particularly as they act against multiresistant organisms such as meticillin-resistant Staphylococcus aureus (MRSA) (Sibbald et al, 2001) and do not effect the ‘healthy’ bacteria in other parts of the body, such as the gut.
Silver Studies have shown the positive effects of silver as an antimicrobial in wound care (Gottrup et al, 2013). Essentially, silver destroys bacterial cells by disrupting the cell wall and causing cell leakage (Butcher, 2013). It also eliminates a wide range of bacteria, including antibiotic-resistant species such as MRSA and vancomycin-resistant Enterococci (VRE) (Parsons et al, 2005).
The use of silver in the manufacture of Durafiber Ag means that it provides antimicrobial action for up to seven days (in vitro) against a broad spectrum of common wound pathogens, helping to reduce bacterial bioburden and the risk of infection (Woodmansey, 2010; Vaughan et al, 2010).
EXUDATE
Wound exudate is the fluid that oozes from the blood vessels in a wound as a response to inflammation (Wolcott, 2012). For something that causes so many issues in wound care, exudate is both a natural and necessary part of healing, preventing the wound bed from becoming too dry and providing the much-needed nutrients that enable healing to progress, such as electrolytes, proteins and growth factors, as well as various cells including neutrophils, platelets, leukocytes and macrophages (White and Cutting, 2006; World Union of Wound Healing Societies [WUWHS], 2007).
However, if the wound produces too much exudate it can begin to cause problems, chiefly maceration (softening and breaking down of skin) around the wound (Beldon, 2014). Exudate can be a management problem for the community nurse — causing leaking and ‘heavy’ dressings — as well as discomfort and malodour for patients (Beldon, 2014).
Exudate also provides clues to the condition of the wound. Factors like the volume, colour, viscosity and odour of the exudate indicate potential problems such as bacterial load and infection (WUWHS, 2007). Dressings that have just been removed can also be examined for their level of saturation, which provides clues to how well the chosen dressing is managing and if healing is progressing — for example, an infected wound will leave a purulent residue in the dressing (WUWHS, 2007).
Community nurses should also discuss the state of exudate with patients, as they may be anxious about the volume or smell (Beldon, 2014).
© 2014
Wou
nd C
are P
eople
Ltd
46 JCN 2014, Vol 28, No 5
room and it was decided to use an absorbent dressing (UrgoTM Clean; Urgo Medical) and a crepe bandage to manage the wound.
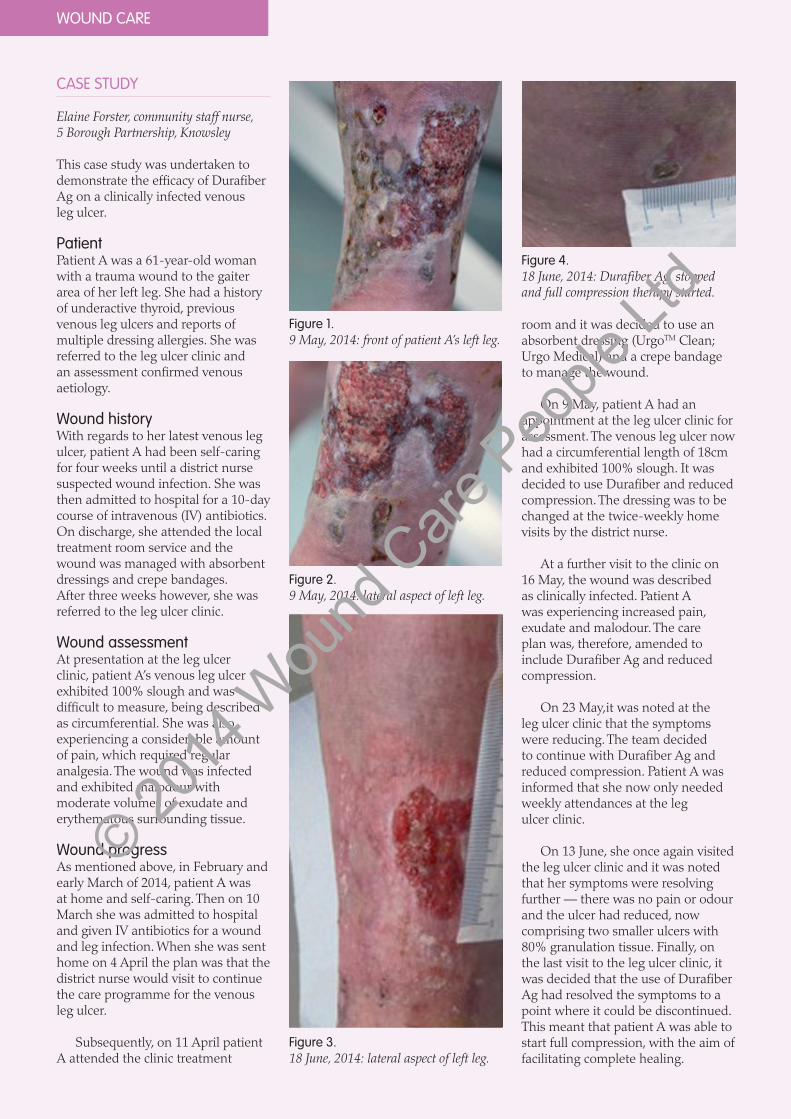
On 9 May, patient A had an appointment at the leg ulcer clinic for assessment. The venous leg ulcer now had a circumferential length of 18cm and exhibited 100% slough. It was decided to use Durafiber and reduced compression. The dressing was to be changed at the twice-weekly home visits by the district nurse.
At a further visit to the clinic on 16 May, the wound was described as clinically infected. Patient A was experiencing increased pain, exudate and malodour. The care plan was, therefore, amended to include Durafiber Ag and reduced compression.
On 23 May,it was noted at the leg ulcer clinic that the symptoms were reducing. The team decided to continue with Durafiber Ag and reduced compression. Patient A was informed that she now only needed weekly attendances at the leg ulcer clinic.
On 13 June, she once again visited the leg ulcer clinic and it was noted that her symptoms were resolving further — there was no pain or odour and the ulcer had reduced, now comprising two smaller ulcers with 80% granulation tissue. Finally, on the last visit to the leg ulcer clinic, it was decided that the use of Durafiber Ag had resolved the symptoms to a point where it could be discontinued. This meant that patient A was able to start full compression, with the aim of facilitating complete healing.
CASE STUDY
Elaine Forster, community staff nurse, 5 Borough Partnership, Knowsley
This case study was undertaken to demonstrate the efficacy of Durafiber Ag on a clinically infected venous leg ulcer.
PatientPatient A was a 61-year-old woman with a trauma wound to the gaiter area of her left leg. She had a history of underactive thyroid, previous venous leg ulcers and reports of multiple dressing allergies. She was referred to the leg ulcer clinic and an assessment confirmed venous aetiology.
Wound historyWith regards to her latest venous leg ulcer, patient A had been self-caring for four weeks until a district nurse suspected wound infection. She was then admitted to hospital for a 10-day course of intravenous (IV) antibiotics. On discharge, she attended the local treatment room service and the wound was managed with absorbent dressings and crepe bandages. After three weeks however, she was referred to the leg ulcer clinic.
Wound assessmentAt presentation at the leg ulcer clinic, patient A’s venous leg ulcer exhibited 100% slough and was difficult to measure, being described as circumferential. She was also experiencing a considerable amount of pain, which required regular analgesia. The wound was infected and exhibited malodour with moderate volumes of exudate and erythematous surrounding tissue.
Wound progressAs mentioned above, in February and early March of 2014, patient A was at home and self-caring. Then on 10 March she was admitted to hospital and given IV antibiotics for a wound and leg infection. When she was sent home on 4 April the plan was that the district nurse would visit to continue the care programme for the venous leg ulcer.
Subsequently, on 11 April patient A attended the clinic treatment
Figure 1.9 May, 2014: front of patient A’s left leg.
Figure 2.9 May, 2014: lateral aspect of left leg.
Figure 3.18 June, 2014: lateral aspect of left leg.
Figure 4.18 June, 2014: Durafiber Ag stopped and full compression therapy started.
WOUND CARE
© 2014
Wou
nd C
are P
eople
Ltd

JCN 2014, Vol 28, No 5 47
WOUND CARE
leakage of exudate from the wound bed onto the surrounding skin (Davies and Rippon, 2010). Coverage can be an issue with some dressings, which shrink or expand when they come into contact with moisture such as wound exudate (Aramwit et al, 2010).
Pain and trauma at dressing changeApplication and removal of dressings are also important considerations, both for ease of use for the nurse and to avoid unnecessary trauma to the wound bed and periwound skin.
Pain and damage to the fragile periwound skin are both considerations for the community nurse at dressing change (Hollinworth, 2002). Exudate can soak into a dressing and then cause trauma when it dries out and ‘binds’ to the dressing, causing problems on removal (Edwards, 2013). Dressings that have dried out while in place are one of the most common causes of wound pain (Bell and McCarthy, 2010). Other researchers have agreed with this, citing the most widespread causes of wound pain as dressings that have adhered to the wound bed, skin stripping through the use of dressings with adhesive borders, and maceration of the periwound skin through exudate leakage (Davies and Rippon, 2008).
Dressings with a variety of wound contact layers have been designed to reduce the amount of adherence to a drying wound (Thomas, 2003). These include soft silicones (Edwards, 2013) and gelling fibres, which retain moisture and lock in exudate on
treatment, Durafiber Ag can be left in place for up to seven days (Dowler, 2012; Forlee at al, 2014).
See Table 2 for guidelines on how to apply Durafiber Ag (Dowler, 2012; Forlee at al, 2014).
CONCLUSION
Community nurses require a wide skill set in order to deal with the variety of clinical presentations that they may encounter in any given day. This includes wound care, which can present nurses with a range of management challenges, including how to combat infection, which kind of dressings to use to manage exudate and how to ensure that any dressing provides patient comfort and does not further damage the wound or skin on removal. It is important, therefore, that community nurses have access to versatile products that can be used in different clinical situations, while also being cost-effective.
Durafiber Ag has a range of applications, including the ability to manage excess exudate and a composition that helps to ensure conformability and patient comfort (Dowler, 2010). Durafiber Ag also provides the ability to manage infection. It can also be left in place for a significant amount of time, crucial to the community nurse (Dowler, 2012). This means that for the busy nurse with a range of patients and clinical presentations, Durafiber Ag represents a useful addition to the clinical armoury.
REFERENCES
Adderley, U (2008) Wound Exudate: What it is and How to Manage it. Wounds Essentials 3: 8–13
Aramwit P, Muangman P, Srichana T (2010) In Vitro Evaluation of the Antimicrobial Effectiveness and Moisture Binding Properties of Wound Dressings. Int J Mol Sci 11(8): 2864–74
Bell C, McCarthy G (2010) The assessment and treatment of wound pain at dressing changes. Br J Nurs 19(11 suppl): S7–S10
Beldon P (2014) How to recognise, assess and control wound exudate. Wound Care Today 1(1): 38–44
contact, thereby reducing the amount of trauma on removal (Greenwood and Grothier, 2012). Community nurses should consider any option that will improve the quality of life and reduce pain and trauma for the patient.
Similarly, a dressing that is easy to apply and remove will involve less nursing time than one that is more difficult to use (Davies and Rippon, 2010). Ease of removal and application, therefore, can have significant time and budgetary benefits and these, factors that community nurses should also consider when choosing a dressing.
With regards to patient comfort, the high integral wet strength of Durafiber Ag also means that it can be removed from moist wound beds and cavity wounds in one piece, thereby reducing trauma and pain (Dowler, 2010).
USING DURAFIBER AG IN THE COMMUNITY SETTING Like any other wound dressing, Durafiber Ag should be changed when clinically indicated, for example, where there is leakage or excessive bleeding. Community nurses should exercise professional judgement in assessing this.
Similarly, in the first stages of treatment, the dressing should be frequently inspected.
However, crucially for the time management of community nurses is the fact that once established as a
Table 2: How to apply Durafiber Ag
Cleanse the wound according to local clinical protocol
Select appropriate dressing size
Remove the Durafiber Ag dressing from pack, using a clean technique. Cut to shape if necessary.
Apply the dressing to the wound and allow for a 1cm / 1/3in. dressing overlap onto the skin surrounding the wound.
When using Durafiber Ag in deep cavity wounds, use whole dressings where possible and leave at least 2.5cm/1in. of each piece outside the wound for easy retrieval
Loosely pack deep wounds up to 80% capacity, as Durafiber Ag will expand on contact with wound fluid
Secure Durafiber Ag with a moisture-retentive dressing or other appropriate secondary retention
The dressing can be removed in one piece using sterile tweezers, forceps or a gloved hand
The dressing may adhere if used on lightly exuding wounds. If the dressing is not easily removed, moisten or soak the dressing in sterile saline to assist removal and avoid disruption of the healing wound
JCN
© 2014
Wou
nd C
are P
eople
Ltd

48 JCN 2014, Vol 28, No 5
WOUND CARE
Bowler P, Jones S, Towers V, Booth R, Parsons D, Walker M (2010) Dressing conformability and silver-containing wound dressings. Wounds UK 6(2): 14–20
Butcher M (2013) Assessment, management and prevention of infected wounds. J Comm Nurs 27(4): 25–34
Cook L, Ousey K (2011) Demystifying wound infection: identification and management. Pract Nurs 22(8): 424–28
Cooper RA (2004) A review of the evidence for the use of topical antimicrobial agents in wound care. World Wide Wounds Available at: http://www.worldwidewounds.com/2004/february/Cooper/Topical-Antimicrobial-Agents.html (accessed 9 August, 2014)
Cutting KF, Harding KG (1994) Criteria for identifying wound infection. J Wound Care 3(4): 198–201
Davies P, Rippon M (2008) Evidence review: the clinical benefits of safetac technology in wound care. J Wound Care 17(11 Suppl): 3–31
Davies P, Rippon M (2010) Comparison of foam and hydrocolloid dressings in the management of wounds: a review of the published literature. World Wide Wounds Available at: http://www.worldwidewounds.com/2010/July/DaviesRippon/DaviesRippon.html (accessed 9 August, 2014)
Drew P, Posnett J, Rusling L, Wound Care Audit Team (2007) The cost of wound care for a local population in England. Int Wound J 4(2): 149–55
Dowler A (2010) DURAFIBER Ag dressing physical properties (in vitro). Smith & Nephew, data on file. Number:DS/10/60/R1
Dowler A (2012) Integrity testing of DURAFIBER Ag in horse serum and ionic solution (in vitro). Smith & Nephew, data on file. Number: DS/12/093/DOF
Dowsett C (2009) Use of TIME to improve community nurses’ wound care knowledge and practice. Wounds UK 5(3): 14–21
Edwards J (2013) Dealing with wound-related pain at dressing change. J Comm Nurs 27(4): 63–42
EWMA (2006) Position Document: management of wound infection. MEP Ltd, London
Forlee M, Rossington A, Searle R (2014) A prospective, open, multicentre study to evaluate a new gelling fibre dressing containing silver in the management of venous leg ulcers. International Wound Journal Available at: http://onlinelibrary.wiley.com/doi/10.1111/iwj.12239/full (accessed 27 September, 2014)
Greenwood M1, Grothier L (2012) Effective patient outcomes using a gelling fibre dressing. Br J Community Nurs March (42 Suppl): S44–S47
Giacometti A , Cirioni O, Schimizzi AM, et al (2000) Epidemiology and microbiology of surgical wound infections. J Clin Microbiol 38(2): 918–22
Gottrup F, Apelqvist J, Bjansholt T, et al (2013) EWMA document: antimicrobials and non-healing wounds — evidence, controversies and suggestions. J Wound Care 22(5 Suppl): S1–S92
Hallett CE, Austin L, Caress A, Luker KA (2000) Wound care in the community setting: clinical decision making in context. J Adv Nurs 31(4): 783–93
Health Service Executive (2009) National Best Practice and Evidence-based Guidelines for Wound Management. Health Service Executive, Dublin
Hollinworth H (2002) How to alleviate pain at wound dressing changes. Nurs Times 98(44): 51
Mahoney K (2014) Understanding the basics of wound care in the community setting. J Comm Nurs 27(3): 66–75
Myers D (2012) The clinical and physical properties of DURAFIBER Ag, the moist wound environment and the autolytic debridement. Smith & Nephew, data on file
Nash Greally J, Wardick K (2013) Learn to heal. World of Irish Nursing 20(10): 58
Parsons D, Bowler PG, Myles V, Jones S (2005) Silver antimicrobial dressings in wound management: a comparison of antibacterial, physical, and chemical characteristics. Wounds 17(8): 222–32
QNI (2009) 2020 Vision: focusing on the future of district nursing. QNI, London
Sibbald RG, Browne AC, Coutts P, Queen D (2001) Screening evaluation of ionised nanocrystalline silver dressing in chronic wound care. Ostomy Wound Manage 47: 38–43
Stephen-Haynes J (2011) Managing exudate and the key requirements of absorbent dressings. Br J Community Nurs 16(3 Suppl): S44-49.
Thomas (2003) Atraumatic wounds. World Wide Wounds Available at: http://www.worldwidewounds.com/2003/january/Thomas/Atraumatic-Dressings.html (accessed 27 February, 2014)
Vaughan KL, McMillan J, Lumb H, Woodmansey E (2010) Antimicrobial activity of DURAFIBER Ag against bacteria, yeast and fungi commonly found in wounds over a seven-day period (in vitro). Smith & Nephew, data on file. Number: 1009012
White R, Cutting KC (2006) Modern exudate management: a review of wound treatments. World Wide Wounds Available at: http://www.worldwidewounds.com/2006/september/White/Modern-Exudate-Mgt.html (accessed 27 September, 2014)
Wolcott RD (2012) The effects of a hydroconductive dressing on the suppression of wound biofilm. Wounds 24(5): 132–37
WUWHS (2007) Principles of Best Practice; Wound Exudate and the Role of Dressings. A Consensus Document. MEP Ltd, London
WUWHS (2008) Wound Infection in Clinical Practice: an International Consensus. Medical Education Partnership Ltd, London
Woodmansey E (2010) Antimicrobial activity of DURAFIBER Ag against bacteria, yeast and fungi commonly found in wounds over a seven-day period (in vitro). Smith & Nephew, data on file. Number: 1004007
Answer the following questions about this article, either to test the new knowledge you have gained or to form part of your ongoing practice development portfolio.
1 – What types of wounds are commonly found in the community?
2 – What constitutes an infected wound?
3 – What are some of the properties of wound exudate?
4 – Why is conformability important in a wound dressing?
5 – Can you explain why some dressings contain silver?
Five-minute test
© 2014
Wou
nd C
are P
eople
Ltd