wound healing and wound care. - university of medical ...oer.unimed.edu.ng/lecture...
TRANSCRIPT

Wound healing andWound care.
Odunayo M. Oluwatosin, FMCS (Nig)Department of Surgery
Learning outcomeby the end of this presentation, you should be able to:
• Describe the process of wound healing.
• Discuss complications of wounds healing.
2
Learning outcomeby the end of this presentation, you should be able to:
• Discuss the total care of a patient whopresents with a wound / ulcer
• Compare the present mode of wound carewith the past
• Contrast the present mode of wound carewith the past
3
A wound is an area of thebody whose normal integrity
has been compromised
4
Wound can be found in:• Skin,• Mucosa,• Bone,• Brain
Can be:• Acute• Chronic
5
Acute wound• Trauma• Surgery• Infection• Inflammation
Chronic wound• Poorly treated trauma• Vascular disease• Haematological disease• Pressure• Infection• Endocrine• Malignancy
6
Aetiology

Traumatic wounds on the face
7
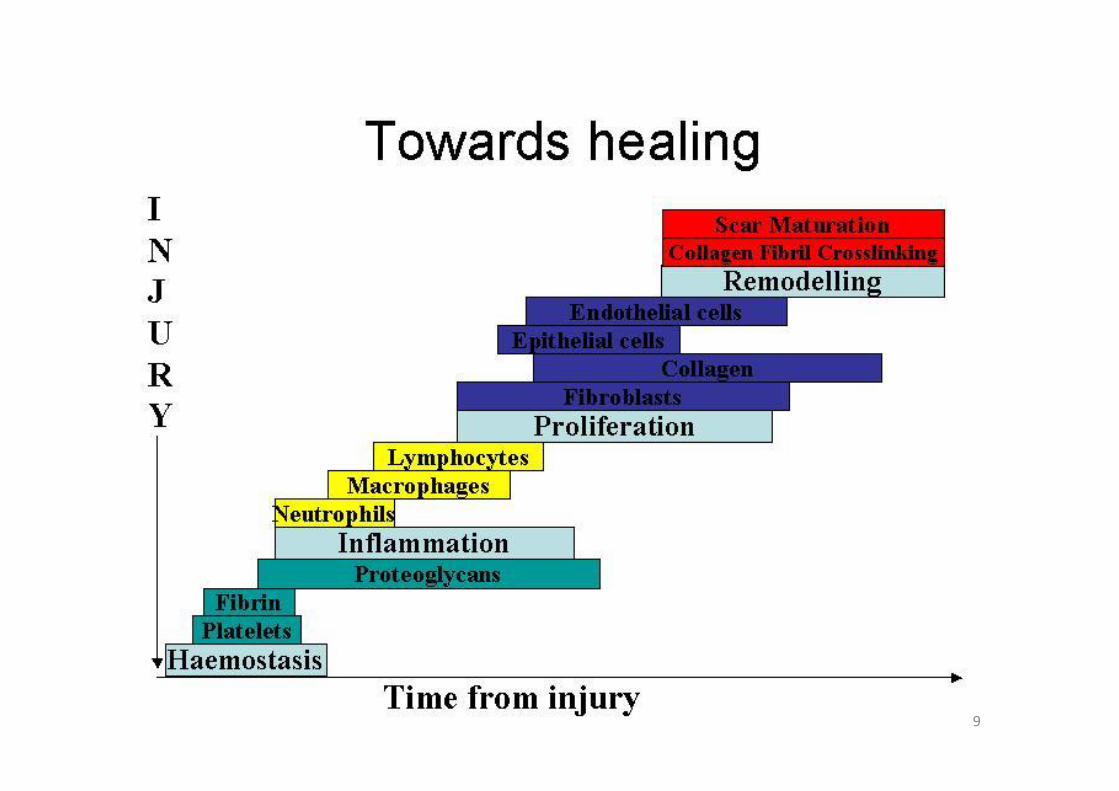
Phases of wound healing
• haemostasis• inflammation• proliferation• maturation
8
9
Haemostasis• microvascular injury leads to extravasation of
blood,• activation of coagulation cascade,• constriction of injured vessels,• clot formation,• platelet aggregation.• Fibrin, fibronectin, vW (von Willibrandt) factor,
and thrombospondin, provide initial matrix forcellular migration
10
Inflammation
• Initial inflammatory exudate contains mainlypolymorphs that later gets replaced bymonocytes and lymphocytes.
• Monocytes must be present to trigger offfibroblast invasion of the wound as well asproliferation
11
Proliferation
• Fibroplasia• Epithelialisation• Angiogenesis
• commences 3 days into wound healing• lasts weeks depending on the size of wound, and type
of tissue involved.• replacement of provisional fibrin/fibronectin matrix by
a more definitive framework comprises
12
Fibroplasia
• commences 2-4 days after wounding.• fibroblasts are attracted to site by PDGF and
TGF-β• they proliferate and construct new
extracellular matrix (ECM) which initiallycomprises fibronectin and hyaluronan butlater, collagen and proteoglycan.
13
Fibroplasia
• During the first three weeks, all wounds gainstrength at the same rate
• thereafter the gain in strength becomesvariable depending on the tissue.
• for the skin, peak tensile strength is achieved60 days after injury.
14
Epithelialisation
• Epithelial mobilisation, migration, division,and differentiation are stimulated by anapparent loss of contact inhibition.
• EGF stimulates mitogenesis and chemotaxis
• β-FGF and keratinocyte growth factor (KGF)stimulate epithelial proliferation.
15
Epithelialisation
• Advancing cells bridge the wound
• Cellular differentiation from the base to thesurface occurs.
• The rate of epithelialisation increases if:the wound does not require debridement,the basal lamina is intactthe wound is kept moist.
16
Angiogenesis• Stimulated by:
TGF-β and PDGF from plateletsTNF-α and β-FGF from macrophages.
• The capillary sprouts invade fibrin to formgranulation tissue network
• With time, blood vessel density reduces andscar tissue develops.
17
Maturation orremodelling
• Balance develops between collagenformation and degradation
• This reaches a steady state at 21 days afterwounding.
• The eventual tensile strength achieved is only80% of normal.
18
Maturation• Collagen degradation is by matrix
metalloproteinases (MMPs)
• Produced by: fibroblasts, granulocytes,macrophages.
• Tissue inhibitors of MMP (TIMP) deactivateMMPs.
19
MMP TIMP
• While early collagen deposition isdisorganised, local forces cause the laiddown collagen to orientate in an organisedfashion.
• Subsequently, activity of MMPs decreases
• Tissue inhibitors of MMP (TIMP) activityincrease.
20
Maturation
• macrophage, and fibroblast density becomesreduced by apoptosis
• capillary outgrowth stops
• acellular and avascular scar results
21
Maturation
Complications of wound healing
• Wound infection• Systemic infections• Chronic wounds and ulcers
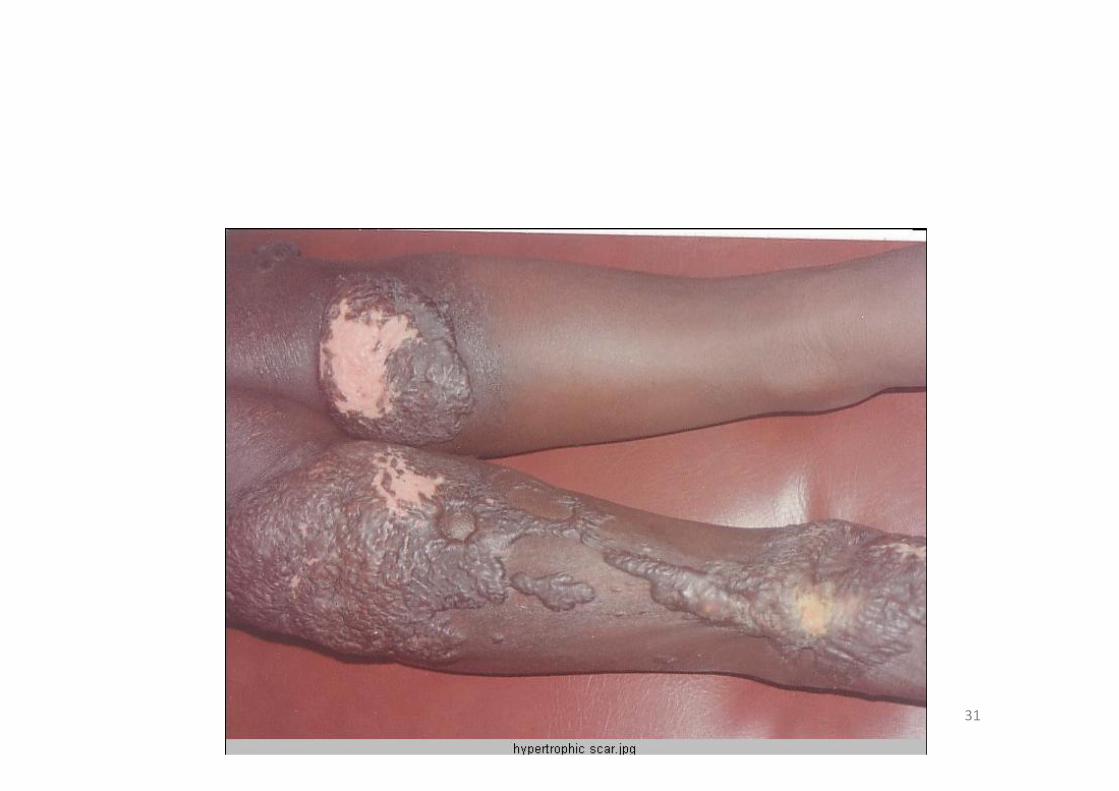
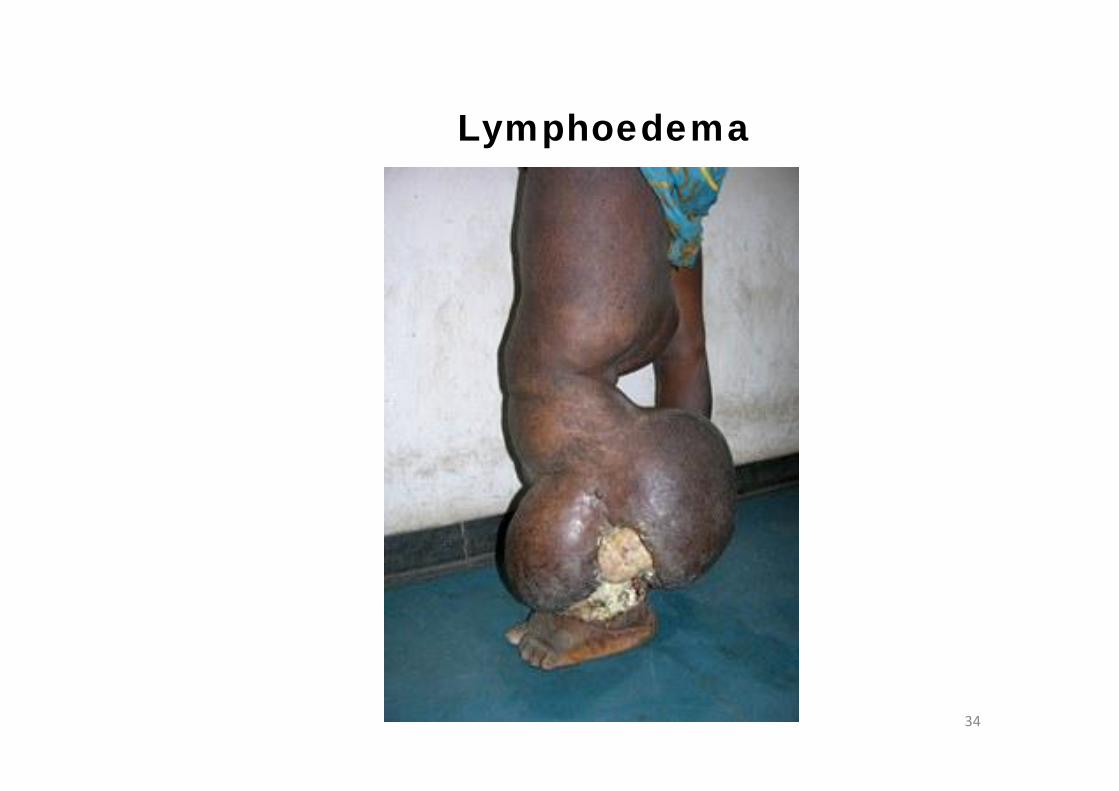
Scars and contractureskeloidsLymphoedemaBone complications: osteitis, osteomyelitis
Marjolin’s ulcer• Tetanus• Pressure ulcers
22
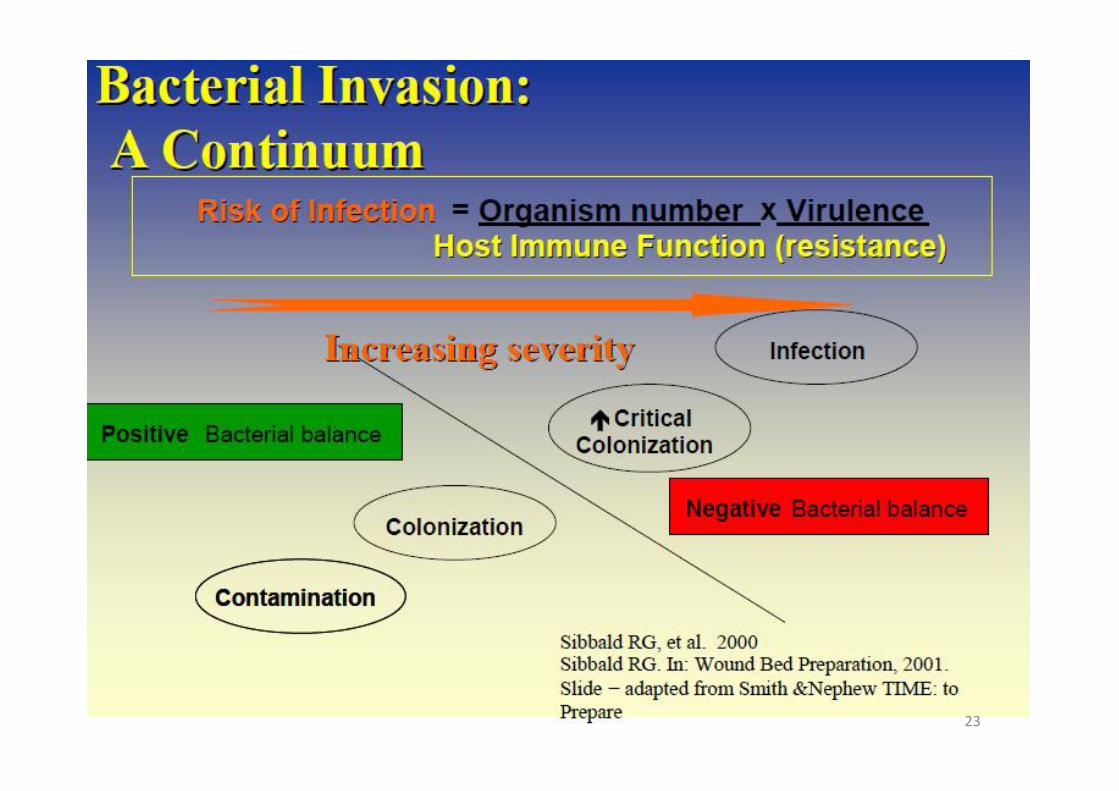
23
24
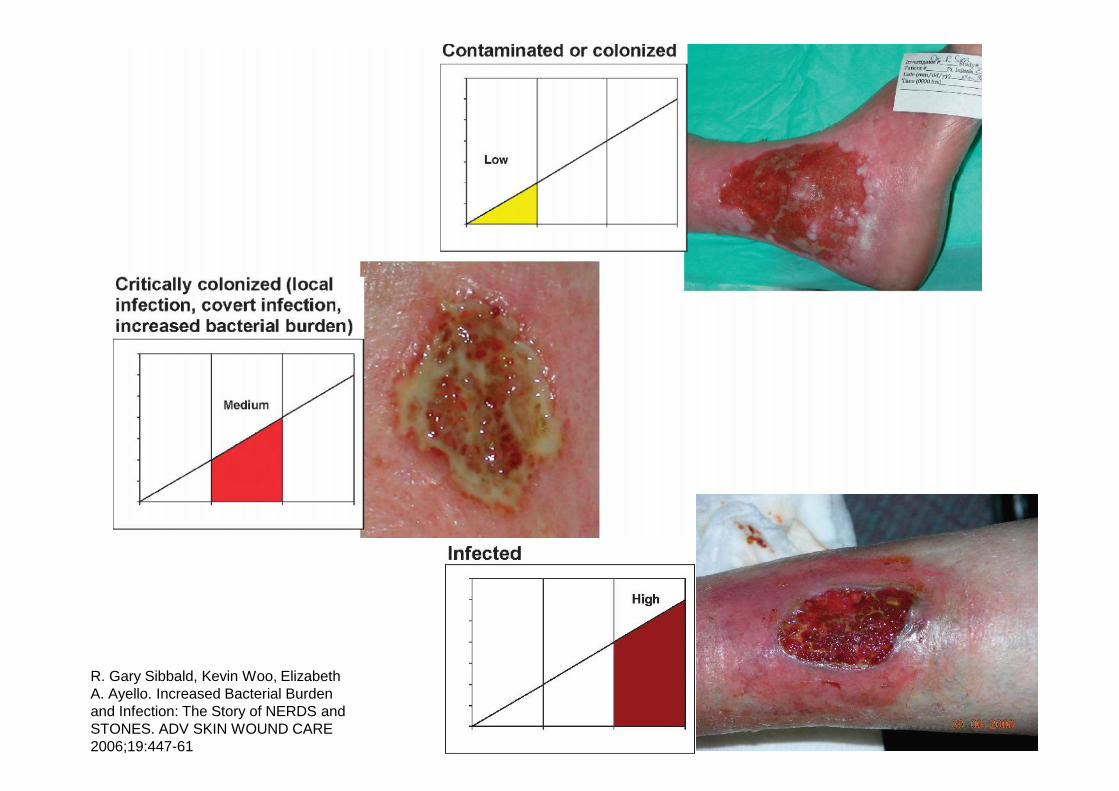
R. Gary Sibbald, Kevin Woo, ElizabethA. Ayello. Increased Bacterial Burdenand Infection: The Story of NERDS andSTONES. ADV SKIN WOUND CARE2006;19:447-61

25
Acutewound
Chronicwound
Repetitive traumaLocal tissue ischaemia
Necrotic tissueHeavy bacterial burden
Tissue breakdown

Differences between acute andchronic wound healing
• In a chronic wound, the timely and orderlymanner of acute wound healing enumeratedpreviously is disrupted.
• This disruption occurs in most cases in theinflammatory and the proliferative phases
26
Differences between acute andchronic wound healing
The disruption manifests in:• alterations in protease activity,• alteration in cytokine profile and
inflammatory response,• changes in cellular profile and activity,• changes in the composition of extracellular
matrix and environment,
27
28
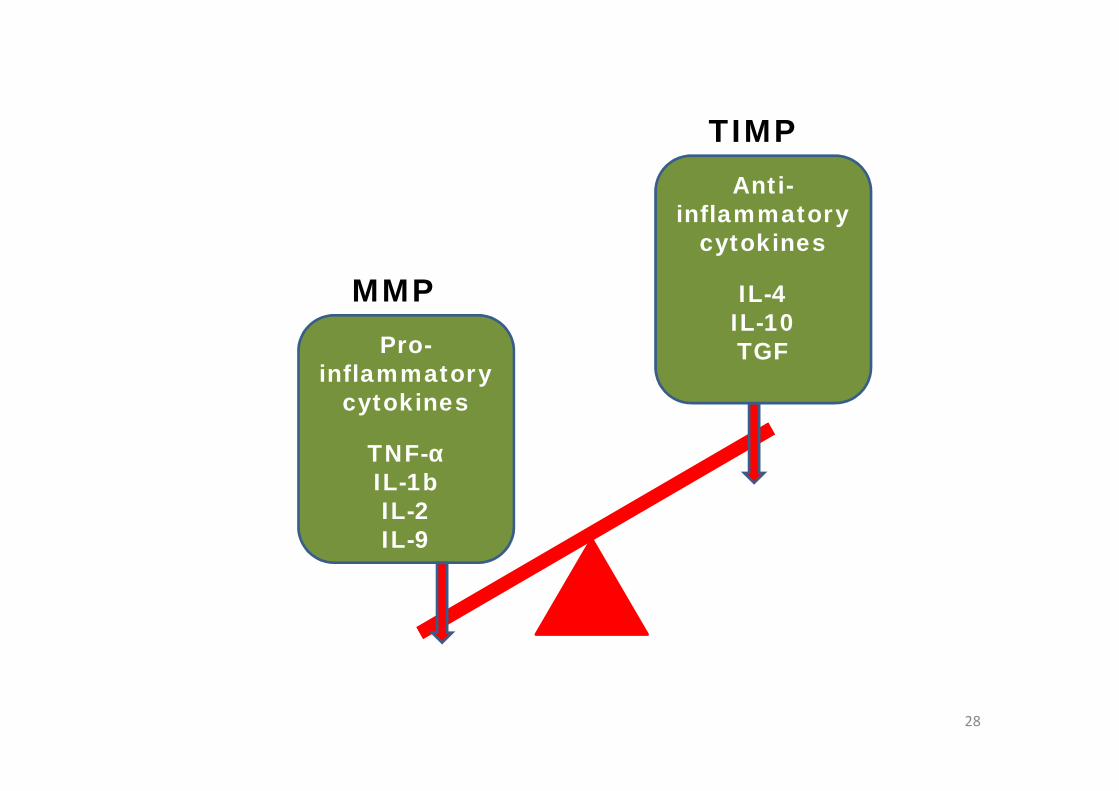
Pro-inflammatory
cytokines
TNF-αIL-1bIL-2IL-9
MMP
TIMPAnti-
inflammatorycytokines
IL-4IL-10TGF
Differences between acute andchronic wound healing
The disruption manifests in:• presence of free radicals and role of nitric
oxide,• accumulation of necrotic tissue and slough,• presence of micro organisms,• disease specific pathological change.
29

30
31
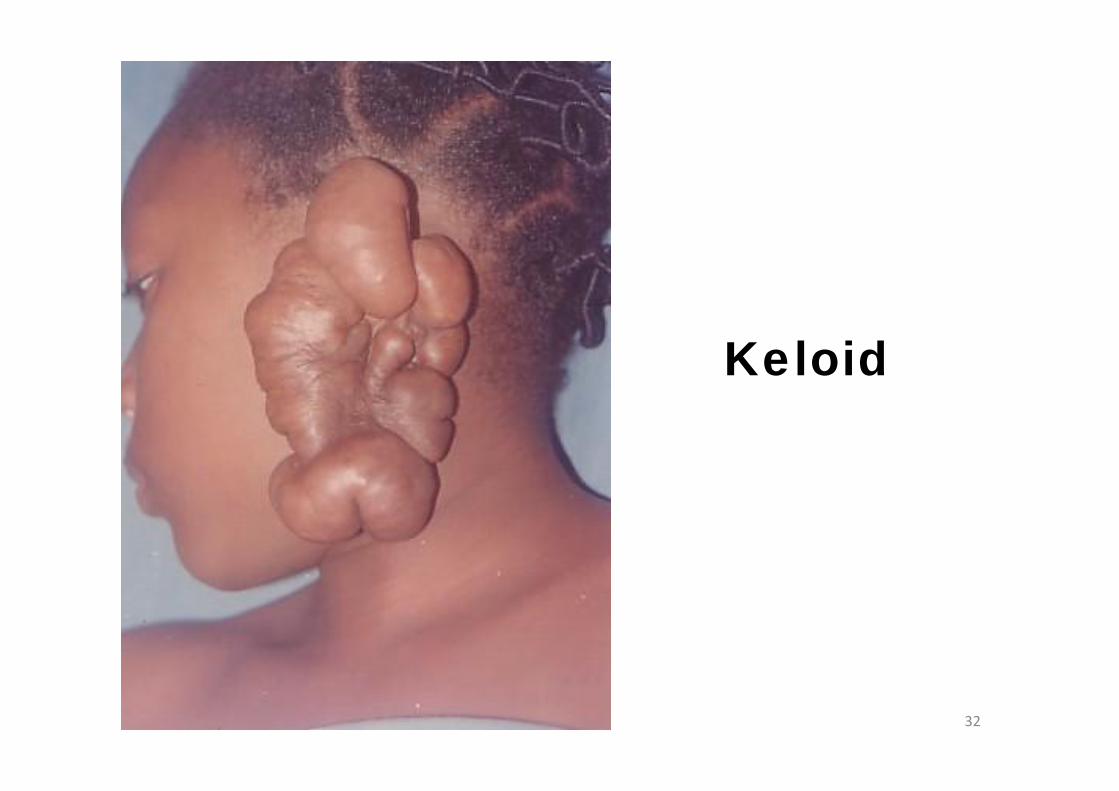
Keloid
32

33
Bone complications
34
Lymphoedema
Total care of a patient who presentswith a wound / ulcer
• Identify and treat the cause
• Address patient-centeredconcerns
• Provide local wound care
• Denis Okan, Kevin Woo, Elizabeth A. Ayello, R. Gary Sibbald. The Role of Moisture Balance inWound Healing. Adv Skin Wound Care 2007; 20: 39-53 35
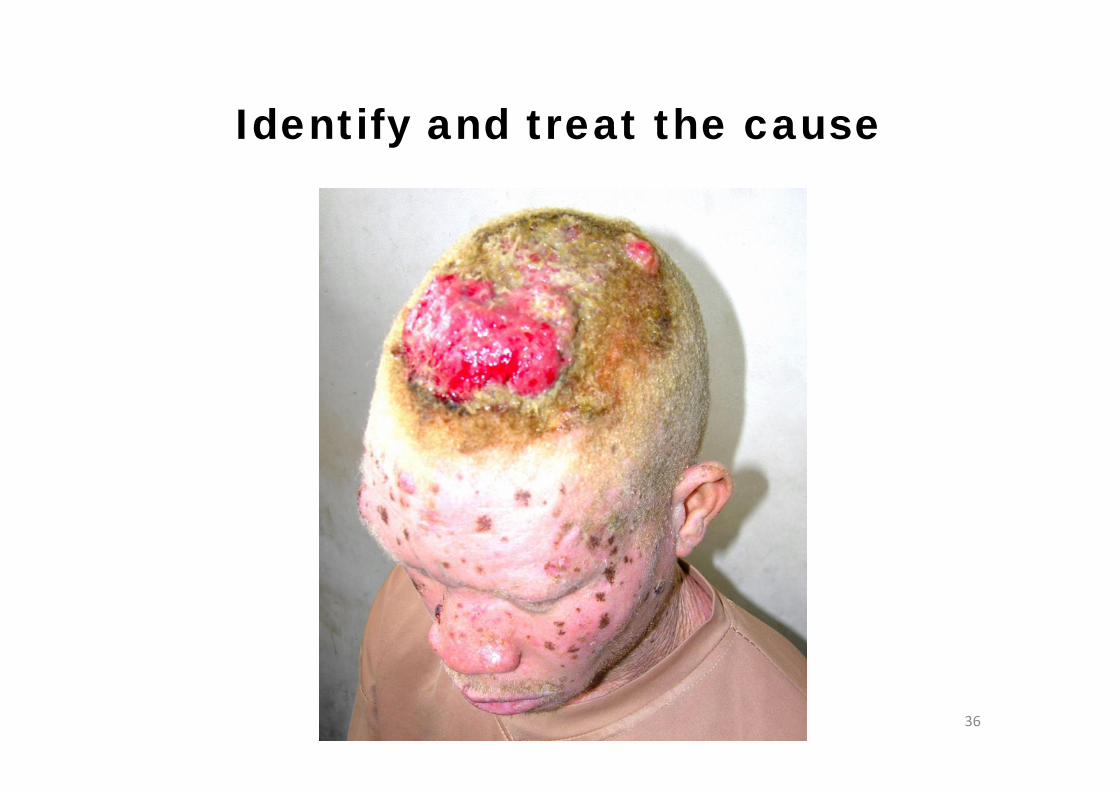
Identify and treat the cause
36
• Venous leg ulcers• Arterial ulcers• Pressure ulcers• Diabetic foot ulcers• Malignant ulcers and Marjolin’s ulcer
37
Identify and treat the cause
Address patient-centered concerns
• Provide emotional support• Assess and consider financial situation• Provide patient and family education• Assess and provide/facilitate optimum
health care
38
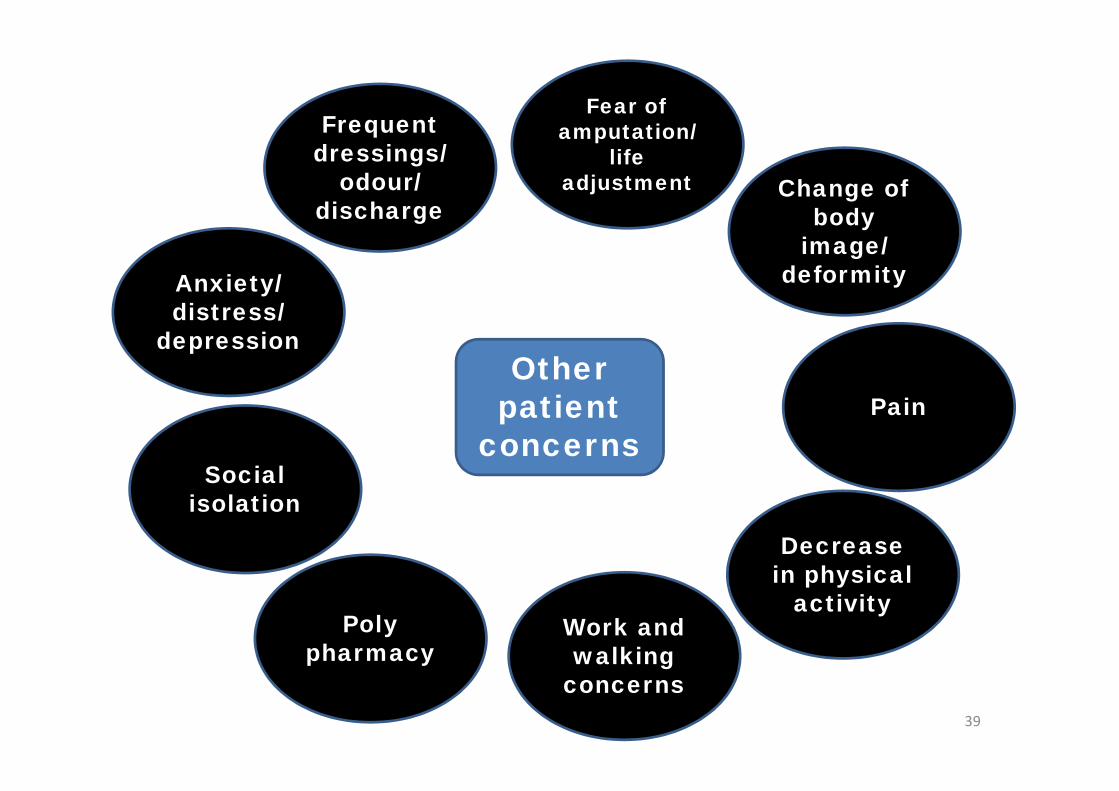
39
Otherpatient
concerns
Frequentdressings/
odour/discharge
Anxiety/distress/
depression
Socialisolation
Polypharmacy
Work andwalking
concerns
Decreasein physical
activity
Fear ofamputation/
lifeadjustment Change of
bodyimage/
deformity
Pain
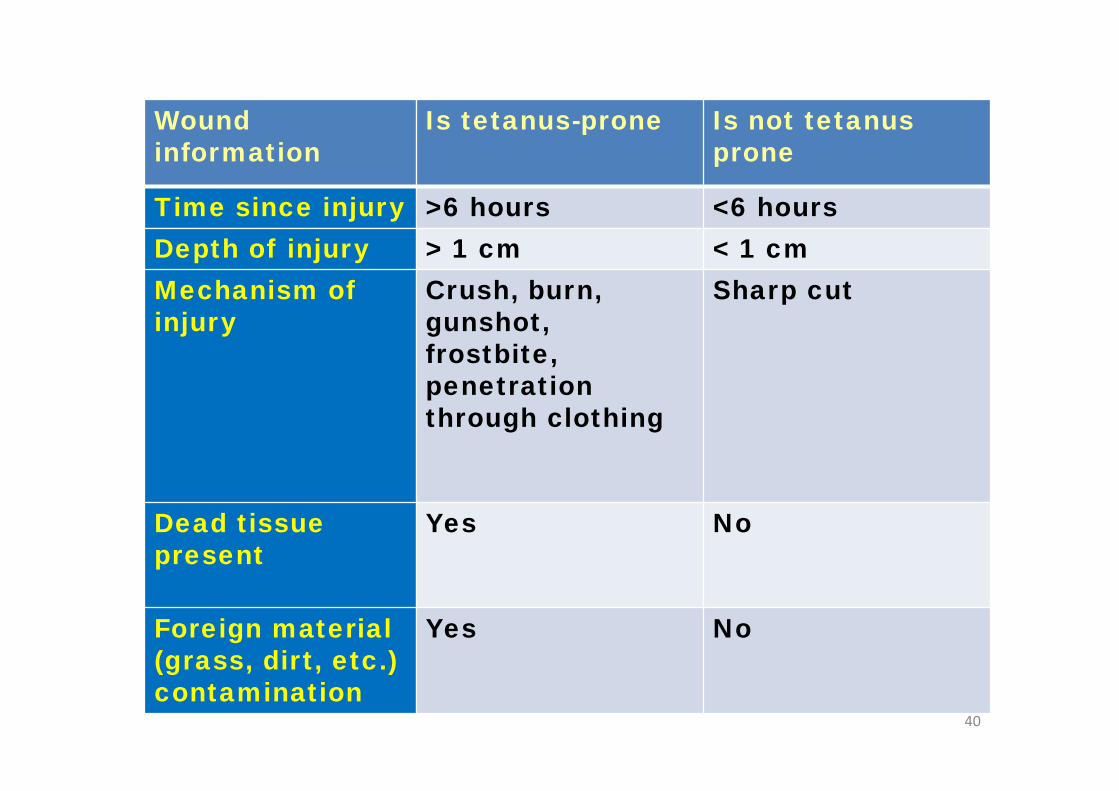
Woundinformation
Is tetanus-prone Is not tetanusprone
Time since injury >6 hours <6 hoursDepth of injury > 1 cm < 1 cmMechanism ofinjury
Crush, burn,gunshot,frostbite,penetrationthrough clothing
Sharp cut
Dead tissuepresent
Yes No
Foreign material(grass, dirt, etc.)contamination
Yes No
40
Pain management
• Injury pain (immediate, severe, regressive),background pain which is prolonged untilwounds are healed
• Procedural pain (dressing changes,physiotherapy, post operative) which issevere and repetitive.
• WHO pain ladder• Appropriate timing
41
Total care of a patient who presentswith a wound / ulcer
• Identify and treat the cause
• Address patient-centeredconcerns
• Provide local wound care
• Denis Okan, Kevin Woo, Elizabeth A. Ayello, R. Gary Sibbald. The Role of Moisture Balance inWound Healing. Adv Skin Wound Care 2007; 20: 39-53 42
Provide local wound care
Determine the potential for healing
Assess the wounda) Obtain the wound historyb) Assess and monitor the physical characteristics of
the woundc) Assess and manage wound pain
43
Local Wound Carea) Tissue concernsb) Infection/Inflammation concernsc) Moisture concernsd) Edge concerns

Determine the potential for healing
Blood supply
44
Determine the potential for healing
Risk factors and co-morbidities that mayaffect wound healing:a) Drugs i.e. immunosuppressive agents and systemic
steroidsb) Periwound edema in a chronic woundc) Serum albumin: <30g/L delays healing, <20g/L very
hard to heal or non-healing woundsd) Hemoglobin: <100g/L delayed healing, < 70-80g/L very
hard to heal or non-healing woundse) Diseases or treatments that impair immunity such as
rheumatoid arthritis and collagen vascular diseases (lupus,scleroderma, dermatomyositis), chemotherapy and radiationtherapy
f) Chronic diseases such as uncontrolled diabetes,hepatic/renal/lung disease and vascular disease
45
Treat the wound
Determine the potential for healing
Assess the wounda) Obtain the wound historyb) Assess and monitor the physical characteristics of
the woundc) Assess and manage wound pain
46
Local Wound Carea) Tissue concernsb) Infection/Inflammation concernsc) Moisture concernsd) Edge concerns
Local Wound CareWound Bed Preparation:
47
To accelerate endogenous healing
To facilitate the effectiveness ofother therapeutic measures
TIME principles of Wound BedPreparation
TIME
TISSUE
INFECTIONINFLAMMATION MOISTURE
EDGEOF
WOUND
Wound cleansing(from page 12 of UK policy doc.)
• Normal saline• High quality pure water• Chlorhexidine gluconate 0.015 - 0.05% w/v
• Povidone-iodine 10%
• Cetrimide 0.15%
49
The effects of water compared withother solutions for wound cleansing
• Water is frequently used for cleaning wounds toprevent infection. This can be tap water, distilledwater, cooled boiled water or saline.
• Using tap water to cleanse acute wounds inadults does not increase the infection rate,however, there is no strong evidence
• That cleansing per se is better than not cleansing.The reviewers concluded that where tap water ishigh quality (drinkable), it may be as good asother methods such as sterile water or saline (andmore cost-effective),
• But more research is needed.
50
24/03/03 Reconstructive surgery 51
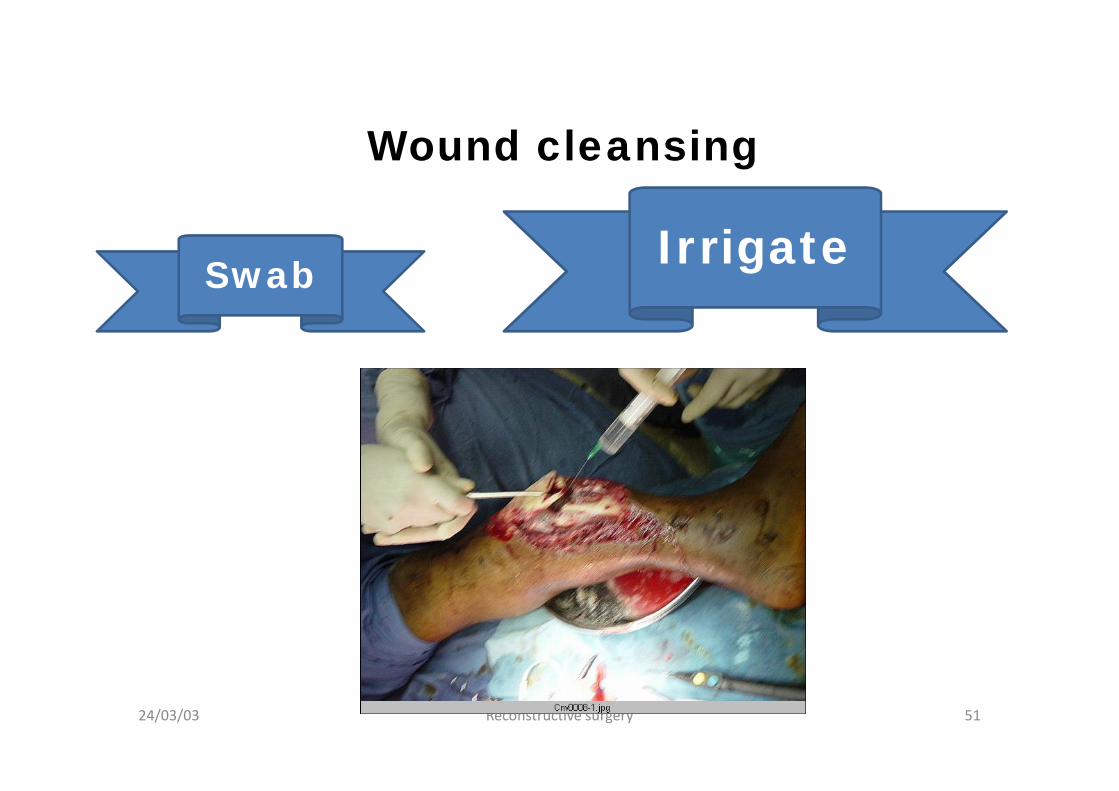
Wound cleansing
Swab Irrigate
52
TISSUE
For clean wounds, no raw surface:Gauze dressing
For raw surface like skin graft donorsite, partial thickness burn, abrasion:Non-adherent dressingsOpsite, Tulle gras, Jelonet, Sofratulle,Vaseline gauze, Bactigras, Melolin,Mepitel,
Temporary biosynthetic skin
24/03/03 Reconstructive surgery 53
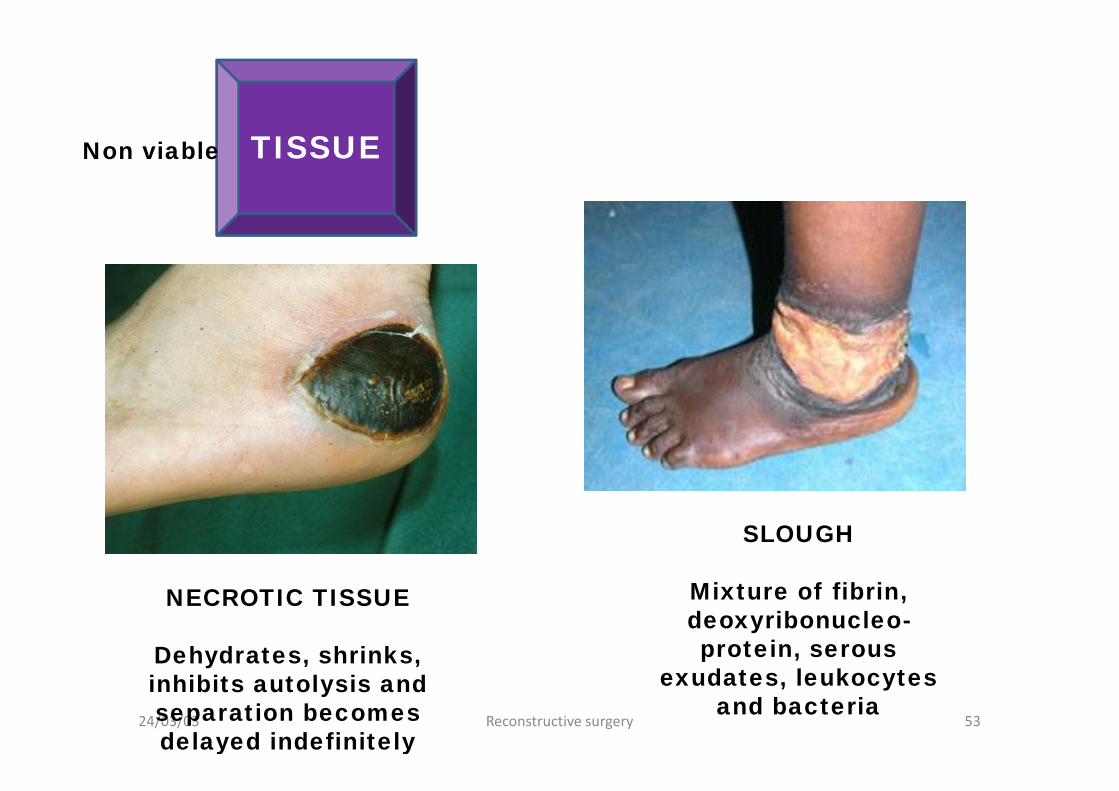
TISSUE
NECROTIC TISSUE
Dehydrates, shrinks,inhibits autolysis andseparation becomesdelayed indefinitely
SLOUGH
Mixture of fibrin,deoxyribonucleo-protein, serous
exudates, leukocytesand bacteria
Non viable
54
Methods ofdebridement ofnon-viable tissue:
•surgical•mechanical•autolytic•chemical•biological•enzymatic
TISSUE

24/03/03 Reconstructive surgery 55
TISSUE
Sharp debridement and wound excision must be thorough

24/03/03 Reconstructive surgery 56
Beware of the closed degloving wound
57
Methods ofdebridement ofnon-viable tissue:
•surgical•mechanical•autolytic•chemical•biological•enzymatic
TISSUE
58
Methods ofdebridement ofnon-viable tissue:
•surgical•mechanical•autolytic•chemical•biological•enzymatic
TISSUE
Hydrocolloids, Hydrogels,Films, Honey:
• Absorb fluid andprogressively movebacteria and cellulardebris away from thesurface of the wound
• Facilitate tissue digestionand separation of theslough

59
Methods ofdebridement ofnon-viable tissue:
•surgical•mechanical•autolytic•chemical•biological•enzymatic
TISSUE
Hypochlorite solutionAserbine
60
Methods ofdebridement ofnon-viable tissue:
•surgical•mechanical•autolytic•chemical•biological•enzymatic
TISSUE
Larvae of Luciliasericata (greenbottlefly) digest necrotictissue and pathogens
61
Methods ofdebridement ofnon-viable tissue:
•surgical•mechanical•autolytic•chemical•biological•enzymatic
TISSUE
VaridaseIruxol
62
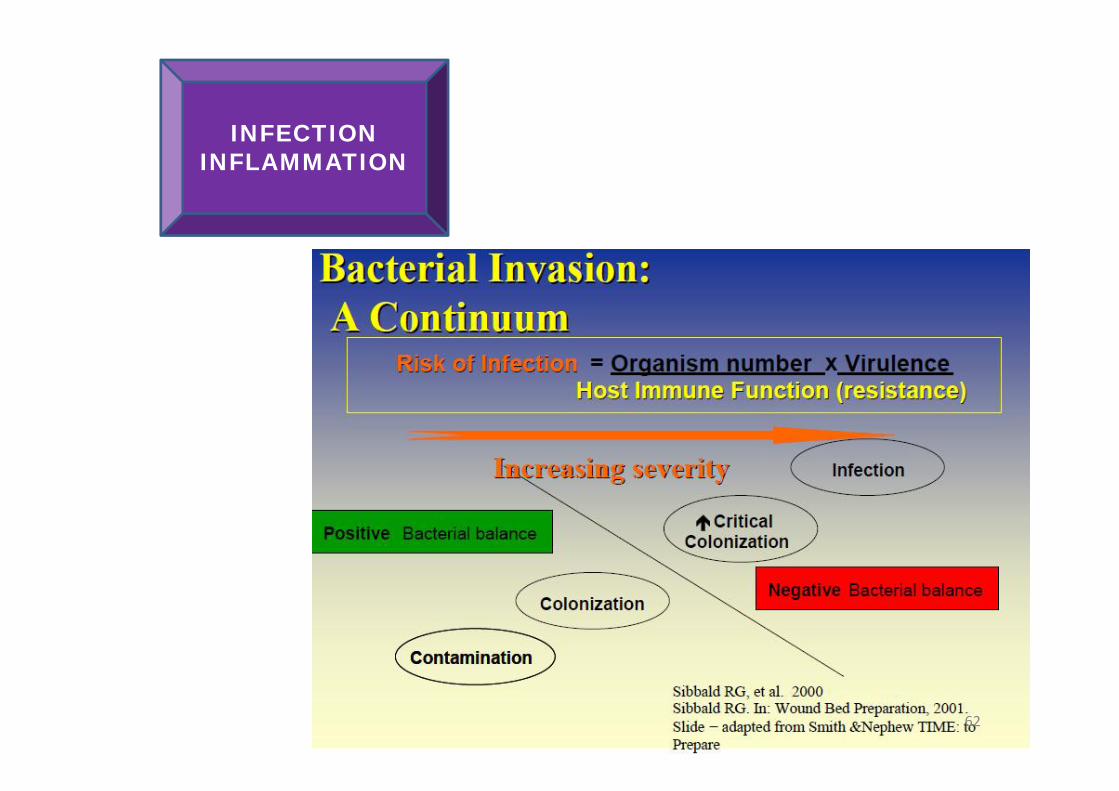
INFECTIONINFLAMMATION

24/03/03 Reconstructive surgery 63
INFECTIONINFLAMMATION
64
INFECTIONINFLAMMATION
Topical antibiotics and antiseptics:
• Honey• Silver sulphadiazine• Impregnated gauze – sofratulle, bactigras,• Inadene• Iodine based polysaccharide bead
dressings e.g. Iodosorb, Iodoflex• Metronidazole gel,• Mupirocin (Bactroban), fusidic acid
(Fucidin)• Nanocrystalline silver
“A moist wound healingenvironment enhances re-epithelialization in open wounds,but excessive wound fluid can slowdown wound healing and causemaceration”
(Bishop et al 2003)65
MOISTURE
66
MOISTURE
Absorbent dressings:
FoamHydrofibreCalcium alginateCrystalline salineHydropolymer foamAcrylic dressing
Proper moisture balance produces:
• Decreased healing time• Decreased rate of infection• Reduced wound trauma• Fewer dressing changes• Reduced pain• Increased cost effectiveness
67
MOISTURE

Dressing Water Absorbed (grams)Gauze 6” x 9” 4-ply 28.0
ABD Pad 5” x 9” 111.9EXU-DRY 6” x 9” 214.8
Absorbency
Low Moderate High
Films
Replicare / hydrocolloids
AlgiSite* M / alginates
Allevyn and other Foams
EXU-DRY
Gauze
RELATIVE MOISTURE MANAGEMENT
• 20 to 40% reduction in two and fourweeks is likely to be a reliablepredictor of healing
• Non-healing edge is cliff like; healingedge is sloppy and bluish tinged
• Consider removal of hyper-keratoticand fibrotic rim
• Use growth factors
69
EDGEOF
WOUND

70
WOUND MANAGEMENT PRODUCTSFOR TYPES OF WOUNDS
(page 8 of UK policy paper)
71
• Healing is a matter of time, but it is sometimes also amatter of opportunity.Read more:http://www.brainyquote.com/quotes/authors/h/hippocrates.html#ixzz1kM4R2jiv
• Make a habit of two things: to help; or at least to do noharm.Read more:http://www.brainyquote.com/quotes/authors/h/hippocrates.html#ixzz1kM4fNvM0
• Science is the father of knowledge, but opinion breedsignorance.Read more:http://www.brainyquote.com/quotes/authors/h/hippocrates.html#ixzz1kM4xMqEj
72