(wp)hin/icp/hst/005-e english only - world health …
TRANSCRIPT

(WP)HIN/ICP/HST/005-E ENGLISH ONLY
~SHOPS ON THE ASSESSMENT AND DEVELOPMENT OF NATIONAL HEALTH
INFORMATION SYSTEMS (NHIS) AND EPIDEMIOLOGICAL SURVEILLANCE
Convened by the
REGIONAL OFFICE FOR THE WESTERN PACIFIC
OF THE
WORLD HEALTH ORGANIZATION
Manila, Philippines 23-27 September 1985
and
Suva, Fiji 21-25 October 1985
Not for sale
Printed and distributed
by the
Regional Office for the Western Pacific of the World Health Organi&ation
Manila, Philippines February 1986

N~E
The views expressed in this report are those of the participants in the workshops on the aasessment and development of national health inforaation ayate .. (NRIS) and epidemiological surveillance and do not necessarily reflect the policies of the Organization.
This report has been prepared by the Regional Office for the Western Pacific of the World Health Organization for governments of Member States in the Region and for those who participated in the Workshops on the Assessment and Development of National Health Information Systems (NRIS) and Epidemiological Surveillance, which were held in Manila, Philippines, from 23 to 27 September 1985 and in Suva, Fiji, from 21 to 25 October 1985.
I,
II
"

1.
2.
3.
4.
5.
6.
CONTENTS
BACKGROUND AND OBJECTIVES •• ,.,.." ... " ... '"".,. ..... ,." •••••• ,. •• ,.",. '",..
ASSESSMENT OF NATIONAL HEALTH INFO~~TION SYSTEMS (NHIS) AND EPIDEMIOLOGICAL SURVEILLANCE •••••••••••••••••••••••••••••
2.1 2.2 2.3
General object ives .... ,..,. .... ",. ..... ,. ..... ,..,." ,"". '" .. " .... ,." .. '" .. '" As.e • .-ent protocols ••••••••••••...•••••••••.•••••.•.••• Result. of che 8.8essment •••••••••.••••••••••••••.••••••
NATIONAL HEALTH INFORMATION SYSTEM CONCEPTS AND PRINCIPLES •••
3.1 3.2 3.3
Introduction.,." .• '". '" '". '",.,." •• ,..",. ....... ",. •.. ,." •••• " .. " .. ,. ..... Conceptual framework and background .•••••••••••••••••••• Basic principles" .••• ,""" '" '" ....... '" '". '" '" ..•• '". '" •.. '" ...•• '" ..
COMPONENT ANALYSIS: AN EXAMPLE '" .. '" '" " " ......... '" '" " . '" . '" '" " . '" . '" .. . TOWARDS A MODEL NATIONAL HEALTH INFORMATION SYSTEM •••••••••••
5.1 5.2 5.3
Introduction'",. .. '" •••• '" '". '". '".,. ••• " '"" ..... '" '" '" '" '" ,""" '" '" '" .. '" '" •• '" ,"" The Core system • '" ,"" ..... ,. •• ,." '" • '" ......... '" ••••••••••••••••••• The Support system •••••••••.•••••.••••••••••••••••••••••
CONCLUSIONS AND RECOMMENDATIONS . ............................ . ANNEXES
ANNEX 1 LIST OF PARTICIPANTS, OBSERVERS, CONSULTANTS AND SECRETARIAT ••••••••••••..•••••••••••••.••••••
ANNEX 2 AGENDA •••••••••••••••••••••••••••••••••••••••••••
ANNEX 3 PROGRAKME OF ACTIVITIES .......................... ANNEX 4 REFERENCES •••••••••••••••••••••••••••••••••••••••
1
2
2 2 7
18
18 18 21
23
28
28 28 33
37
39
47/48
49
S5

1. BACKGROUND AND OBJECTIVES
Within the concept of the strategies of health for all by the year 2000, many of the countries/areas are attempting to reorient their delivery of health care towards an emphasis on, and extension of, primary health care (PHC). For the planning, monitoring and evaluation of that reorientation process. accurate and timely information relevant to primary health care is vital. An essential first step is the determination of where the countries are today in their information system development.
To answer this need, the WHO Regional Office for the Western Pacific conducted two workshops on the assessment and development of national health information systems (NHIS) and epidemiological surveillance in selected countries in the Western Pacific. The overall objective of the project was to enable countries or areas of the Western Pacific Region to develop national plans for the collection and use of information in support of health management.
The project had two phases. The first one involved the conduct of an assessment of the present status of national health information systems and epidemiological surveillance in the countries of the Region, and the preparation of an analytical report of the results. The specific objectives of the first phase of the project were as follows:
(1) to review the current status of national health information system development in the countries of the Region in order to form a more comprehensive baseline for support programme planning;
(2) to determine the availability of information in the countries in four selected areas of the health services; maternal and child health services at the PHC level, reportable communicable diseases, with special attention to EPI target diseases, diarrhoeal diseases, noncommunicable diseases and human resource development;
(3) to obtain detailed data on surveillance procedure and systems in the country and in their relationship to overall national health information system activities;
(4) to determine the extent to which data are available and used for monitoring and evaluation of health services and their goals;
(5) to determine the availability of needed data, their reliability, completeness and timeliness;
(6) to determine the level of analysis and methods of presentation of data;
(7) to determine the flow of data in the reporting system;
(8) to determine the level and types of data collected and relevant processing methods and equipment.
The second phase consisted of two workshops - one for the larger developing countries of the Region, and one for the islands of the South Pacific - in which the analysis of results as assessed against a reference presentation of a "model" national health infonnation system, for discussion of comparative differences between what is available and what is desired. Specifically, the objectives of the second phase were as follows;
- 2 -
(1) to provide a forum for discussion on national health information systems (NUIS) development in support of health systems management;
(2) to review the results of the assessment of the current status of NHIS development in relation to a model NHIS, and to discuss the comparative differences between these;
(3) to prepare a plan for further development of existing NHIS to overcome the problem. faced by countries, as determined by the assessment.
The first workshop was held in Manila on 23 to 27 had fifteen participants representing eight countries. was held in Suva, Fiji, from 21 to 25 October 1985 and participants from eleven countries. Annex 1 gives the of the two workshops while the agenda and programme of Annex 2 and Annex 3, respectively.
September 1985 and The second workshop
had twenty-five list of participants activities are in
2. ASSESSMENT OF NATIONAL HEALTH INFORMATION SYSTEMS (NHIS) AND EPIDEMIOLOGICAL SURVEILLANCE
2.1 General objective.
The main objective in the development of the protocols for the assessment wa. to gather baaeline information to be used for the NUtS workshops to be conducted in Manila in September and in Suva in October. In addition, it was deemed that the assessment of national health information system that would be done in preparation for the workshops would also be a good opportunity to collect data that would provide a sound basis for evaluating requests for WHO support and planning of programmes related to health information system. In view of these underlying objectives, the protocols were developed so as to provide a more detailed picture of the health information system of Member States than what one would get by doing an intensive review of documents currently available at WHO/WPRO. While it is recognized that a number of such documents already exist, most of them deal with general observations and do not adequately describe the specific components and processes that comprise the health information system of the countries. Moreover, since it was earlier decided by the short-term consultants for the project that the ultimate aim of the protocols should be to permit an objective assessment of the current status of the Member States' health information systems, the specific objectives defined by the project proponents (e.g. determine availability, accuracy, timeliness of data) were expressed in measurable and observable terms as far as possible in order to minimize subjective biases on the part of the data collectors. As a consequence, the interview schedules were relatively long.
2.2 Assessment protocols
The protocols that were developed were designed for two kinds of respondents: the data providers and the data users. The data providers are those actually involved in or at least supervising the collection and processing of statistical d,ata generated from the various record systems. Included in this category are the epidemiologists/biostatisticians or equivalent positions at the intermediate and the central/national levels,

- 3 -
a9 well as the health personnel or data collectors at the peripheral level, directly recording information from patients or from the general population. Data users, in the context of the assessment, pertain to the programme and service managers, who are expected to utilize data produced by the providers for the planning and monitoring of their respective programmea.
In view of the heterogeneity of the nature of the different components of a health information system, it was decided to categorize data providers into four sub-groups, according to the kind of data being produced, namely, census data, vital statistics, morbidity and .. ternal and child health, and manpower. A separate protocol was developed for each of these sub-groups. While it is recognized that morbidity and maternal and child health statistics may have several co.ponents defining a number of independent data systems, only one protocol was developed to cover the different areas within morbidity and maternal and child health statistics, since the same variables are being investigated (e.g. data flow, data elements collected, etc.) irrespective of the source of data, the kind of disease investigated, or the type of maternal and child health service rendered.
A protocol was also developed for the hospital and clinic visit, which was considered an integral part of the assessment. Unlike the protocols for the data uaers and data providers, however, the hospital and clinic visit protocol was shorter and more subjective, since a large part of it dealt with the general impression(s) of some aspects of the hospital/clinic related to the collection and recording of information, such as the forms used, the data filing system, record linkage and the like. The impressions thst were gathered during the hospital and clinic visits are regarded more as supporting information than as conclusive evidence since it was recognized that observations made during the site visit may not be representative of conditions prevailing throughout the country.
Overall, seven interview schedules were developed as follows:
Form I
2A
2B
3
4
5
6
Protocol for data users
Protocol for providers of census data (for countries with an organized census)
Protocol for providers of census data (for countries without an organized census)
Protocol for providers of vital statistics
Protocol for providers of morbidity and/or MeH service statistics
Protocol for providers of manpower statistics
General observation guidelines for the clinic and hospital visit

- 4 -
2.2.1 Content
Each type of protocol that was developed had a number of sub-components or blocka, consisting of related questions on specific issues.
Form 1 for data users has 13 questions, sub-divided into six blocks as follows!
A. Data utilization B. Data source C. User involvement in information systems D. Linkages E. Assessment of data quality F. Problems perceived
Forms 2A to 5 differed in the number and kind of questions asked. However, they all have the same blocks of questions, namely:
A. Background information B. Data elements C. Data quality D. Data flow E. Data processing/analysis F. Dissemination G. Sample survey capability H. Problems encountered
An exception to the above is Form 2A, where the section on sample survey capability was excluded. This was done since it was deemed unlikely that a country without an organized census up to the present time would have any form of sample survey capability.
Form 6 has an entirely different format as it merely consists of a listing of items to be observed during the clinic and hospital visit, rather than a series of structured questions. Items covered included the following:
A. Patient flow
B. General impression
1. Forms used
1.1 Quality of forms 1.2 Quantity of forms
2. Data filing system
2.1 Sorting system used for filing of patient's records 2.2 Record linkage

- 5 -
3. Data atorage
3.1 Phyaical facilitiea for data atorage 3.2 Length of atorage of forma
4. Referral system
5. Other comments/observations
since it is recognized that the data collector may have been faced with several data aystems, especially with respect to morbidity and maternal and child health statistics, it was agreed that the focus of the assessment should be on data which are collected routinely on a nationwide basis.
2.2.2 Respondents
The following were the intended respondents for each of the forms developed:
Form
1
2A
28
3
4
Respondent(s)
Director of planning office or equivalent
Director of health services or equivalent
Director of human resource development office or equivalent
Programme director for the following areas:
Ca) Diarrhoeal diseases Cb) EPI target diseases Cc) Noncommunicable diaeases Cd) Haternal and child health programme
Statistician at national census office or equivalent
Statistician at m.nlatry of health in-charge of collecting population data
Statistician at civil regiatrar's office or equivalent, or,
Statistician at ministry of health in-charge of collecting data on births and deaths (if the country does not have an established vital registration ayatem)
Central/national level personnel in-charge of collecting/collating data for each of the following prosraa.ea:

5
- 6 -
(a) Diarrhoeal diseases (b) EPI target diseases (c) Noncommunicable diseases (d) Manpower (e) Maternal and child health
Personnel in charge of collecting and collating morbidity and maternal and child health statistics at the intermediate level
Health personnel involved in data collection at health centre and hospital visited
statistician at human resource development office or equivalent
Personnel involved in collecting and collating manpower statistics at the intermediate level
No specific respondent; data collector to record general impressions after talking to personnel during clinic and hospital visits
It was expected that in smaller countries especially a single person may be holding several responsibilities or positions and hence may be the only respondent for several of the questionnaires.
2.2.3 Limitation
The main limitation faced by the assessment team with the use of the protocols was the fact that the accuracy and completeness of the data that were collected were highly dependent on the respondent's position, qualifications and awareness of existing procedures and problems facing their health information system. To minimize this problem, the following measures were adopted in the course of the data collection:
(1) Each completed protocol was regarded as a conglomeration of the responses of several respondents from different levels, rather than from one individual respondent. For example, it was observed that, in general, higher level officials based at the central office of the Ministry of Health can give detailed information on dissemination of data, sample survey capability and problems encountered, but have difficulty identifying data elements being collected and describing the data flow. These latter set of information were best supplied by the peripheral level workers. It was then possible for a protocol to be filled up by having different sources for each section, depending on who was in the best position to supply the information.
(2) The respondents' anawers were validated by counter-checking the given information with existing documents and publications. Samples of forma and publications were always requeated whenever they were available.

- 7 -
(3) For some questions like those pertaining to the assessment of the quality of data being produced, it was indicated whether the respondent's answer' were based on available data, special studies or a personal guess of the respondent.
2.3 Results of the assessment
Thirteen countries were included in the assessment, namely, Brunei Darussalam, Cook Islands, Fiji, Kiribati, Lao People's Democratic Republic, Malaysia, Papua New Guinea, Philippines, Republic of Korea, Samoa, Solomon Islands, Tonga and Vanuatu. The results of the preliminary analysis done on the data collected from these thirteen countries are presented in the following sections. A more in-depth analysis of the dsta from the same survey will be presented in another report.
2.3.1 Background information
2.3.1.1 Census
All the 13 countries visited for the assessment had undertaken at least one census. Three of the countries had their last census in 1976, while four had it in 1979. The remaining six had it in the early 19808, with one (Lao People's Democratic Republic) having its first census only 1n March 1985.
Six of the countries conduct their census every ten years, while two countries have it every five years. Four countries have been conducting their censuses at irregulsr intervals.
2.3.1.2 Vital statistics
Two of the thirteen countries visited do not have an organized vital registration system. The Ministry of Health is the source of vital statistical data for four of them, while the General Registry Office or its equivalent (e.g. Census, Home Affairs) is the main source for five other countries. Both the Ministry of Health and the Department of Justice or the Registry General are the dats source for four countries. The registration of births and deaths is promulgated by law in only ten out of the thirteen countries.
2.3.1.3 Morbidity/maternal and child health
All the thirteen countries visited have government clinics and hospitals as their source of morbidity and maternal and child health service statistics. Only one country reported the inclusion of data from semi-government clinics and hospitals. Two countries reported the inclusion of data from the private sector.
In eight of the countries visited, the reporting of notifiable diseases is promulgated by law. However, in five of these eight countries, no penalties are imposed on health personnel/facilities who fail to report the incidence of notifiable diseases. Even in countries where such penalties theoretically exist, its imposition have been very lenient.

- 8 -
2.1.3.4 Manpower
Interviews regarding the collection of manpower statistics were done in only twelve countries. A manpower data system exists in only nine of these countries, with all of them having data only for health manpower employed by the government.
2.3.2 Data elements
2.3.2.1 Census
Of the data elements collected during the census, age is one of the most important in relation to health statistics, since its distribution is used as the denominator for most morbidity and mortality rates.
Table 1 shows the distribution of countries according to the type of age distribution that they routinely generate from census reaults, and the lowest level of detail for which data are available. Of the ten countries for which data are available, only seven generate age distributions by single years of age, while nine present it by 5-year age-groups. For most of the countries, these data are available for geographic subdivisions of the popUlation (e.g. regions, provincea, etc.).
Table 1. Distribution of countries according to type of age distribution routinely generated from census results and lowest level of detail for which data are available
TYPE OF AGE LOWEST LEVEL OF DETAIL DISTRIBUTION NATIONAL GEOGRAPHIC DOES NOT TOTAL
SUBDIVISION COMPUTE
Single years 2 5 3 10
5-year ap groupe 2 7 1 10
Data not available for three (3) countries.
Another question asked during the assessment was the availability of intercensal estimates. Of the eleven countries who responded to the question, nine indicated that they compute intercensal estimates on a yearly basis, while one country reported that such estimates are computed only at five-year intervals. The respondent for one country was simply aware that intercensal estimates were being computed but did not know the frequency of the computation.
Nine of the countries who compute intercensal estimates generate age-distributions by geographic subdivisions. Of these, four present their intercensal age distributions by five-year age groups while two present it by single years of age. The respondents of three countries did not know the specific type of age distribution being generated. Only one country indicated that their intercensal age-distributions are computed only at the national level, by five-year age groups.

- 9 -
Another question of interest i. the extent of the Ministry of Health's involvement in census activities. Any degree of collaboration between the two agencies opens the potential for the inclusion of health-related questions during the census, Which is a very rich data source.
Nine countries indicated the collaboration of the Census Office and the Ministry of Health (among other agencies) in the conduct of the census. No data are available for the other four countries. Of the nine countries Where such collaboration exists, seven indicated involvement in the formulation of health and health-related questions to be included in the census.
2.3.2.2 Vital statistics
A review of the birth and death certificates used by the countries included in the assessment showed that the number of variables/data elements asked for in the birth certificate ranges from 3 to 18, While that of the death certificate ranges from 6 to 11. The specific variables included in the country with a birth certificate of only three variables are the date of occurrence of the event, the place of occurrence and the sex of the child.
2.3.2.3 Morbidity/maternal and child health
The number and the kind of data elements collected for morbidity and maternal and child health statistics are the most difficult to track due to the gross proliferation of forms, the lack of uniformity and the large heterogeneity in the kind and quantity of data being collected, both within and across countries. For this reason, only some highlights of the findings are presented in these preliminary results. These findings are purposively chosen to emphasize the current state of the countries with respect to the type and quantity of data elements routinely collected by the various components of the health system. Among these highlights are:
(1) One of the sample forms that was collected during the assessment had 48 columns. This form was to be filled up by a peripheral level worker.
(2) One nurse interviewed at the peripheral level had to fill up the following forms regularly:
Monthly forms:
8 different forms for immunization; 2 other forms on deliveries and immunization; 1 form for caseload by midwife; 1 form for manpower report (posts filled; number of vacancies); 1 form for full-cream milk inventory; 5 different forms for family planning (1 each for defaulters, follow-ups, etc.).
Quarterly forms:
2 forms for pap smear returns; 4 different forms for births and deaths; I form for oral rehydration.

- 10 -
All of the above forms had to be collated at end of each year to derive annual summaries.
(3) In another country. the interviewer got a sample of 42 different forms to be filled up at the peripheral level.
(4) In still another country. the interviewer noted 75 different forms being used; she had to use a microcomputer to record them all down.
2.3.2.4 Manpower
Generally. there was no manpower data system in the countries visited. Where it exists. the data consisted of the distribution of health manpower employed by the government. according to type of personnel (e.g. doctors, nurses. etc.).
2.3.3 Data flow
2.3.3.1 Census
In general. census data flows from the interviewer to an intermediate level office. and then on to the National Censua Office. where data are processed, analysed. disseminated and stored. For most countries, no processing and analysis of data are done at the peripheral and intermediate levels.
2.3.3.2 Vital statistics
The data flow for vital statistical data for most countries follows the following pattern: every birth and death is reported by an informant to the local civil registrar. the police or the village head based either at the peripheral or at an intermediate level. A copy of the birth or death certificate is maintained at this level for administrative and legal purposes. A duplicate copy of the certificate is sent to the national level for statistical purposes.
2.3.3.3 Morbidity/maternal and child health
The general pathway followed by morbidity/maternal and child health statistics was observed to be as follows:
Patient
1 Fundamental record maintained at peripheral level
1 Data from fundamental records summarized
for all cases seen at peripheral level and submitted to intermediate level
1 Data for different intermediate levels
summarized at national level

- 11 -
The number of times the data are summarized depends on the number of intermediate levels they need to go through before reaching the national level.
2.3.3.4 Manpower
There is no specific pathway for manpower statistics. The flow of data generally depends on the office to which the data are being submitted.
2.3.4 Data quality
To assess the quality of data being collected, questions were asked on three aspects: timeliness, extent of coverage and accuracy. Each of these aspects was measured in terms of questions which allowed their objective assessment.
2.3.4.1 Timeliness
To measure the timelinesa of the data being collected, the respondents during the assessment were asked to estimate the average time gap between the reference date of data being collected and selected end points. Specific end points considered were the time the information is received for final processing at the central unit (i.e. at the national office of the Ministry of Health), a8 well as the time the results are disseminated. The results are shown in Table 2.
Table 2. Average time gap between reference data of different types of health statistics and selected end points
AVERAGE TIME GAP BETWEEN REFERENCE DATE AND TYPE OF RECEIPT OF INFORMATION FOR FINAL DISSEMINATION DATA PROCESSING AT CENTRAL UNIT
MINIMUM MAX1I'IUM MINIMUM MAXIMUM
Census - - 6 weeks 5 years
Vital statistics 10 days 1 year 2 weeks 5 years
Morbidity/MCH 2 weeks I year 2 weeks 5 years
Manpower - - 1 month 2 years
Table 2 shows the large heterogeneity in the average time gap reported by countries, between the occurrence of events and the final processing and dissemination of data. In the case of the census for instance, the results are disseminated as early as six weeks after data collection for some countries and are delayed as much as five years for others. In the case of vital, morbidity, and maternal and child health statistics, the problem seems to lie in the disseminition of results. While the maximum average
- 12 -
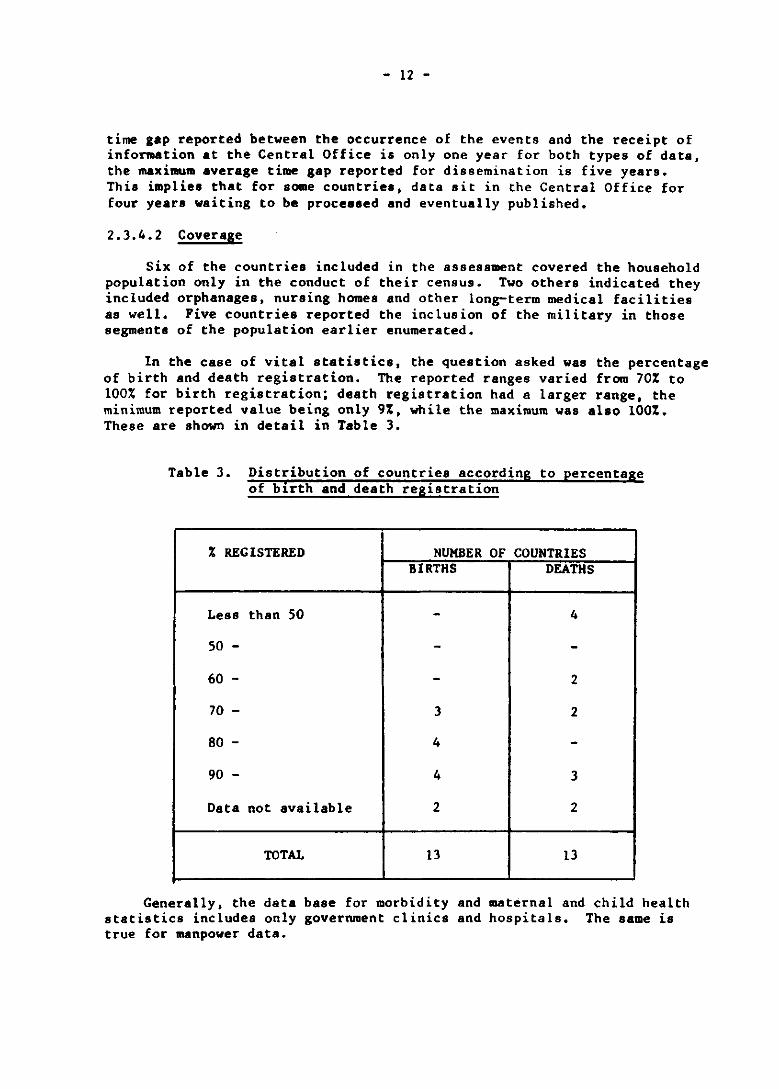
time gap reported between the occurrence of the events and the receipt of information at the Central Office is only one year for both types of data, the maximum average time gap reported for dissemination is five yearo. This implies that for some countries, data sit in the Central Office for four years waiting to be procesaed and eventually published.
2.3.4.2 Coverage
Six of the countriea included in the assessment covered the household population only in the conduct of their census. Two others indicated they included orphanages, nursing homes and other long-term medical facilities as well. Five countries reported the inclusion of the military in those segments of the population earlier enumerated.
In the Case of vital statistics, the question asked was the percentage of birth and death registration. The reported ranges varied from 70% to 100% for birth registration; death registration had a larger range, the minimum reported value being only 9%, while the maximum was also 100%. These are shown in detail in Table 3.
Table 3. Distribution of countries according to percentage of birth and death registration
% REGISTERED NUMBER OF COUNTRIES BIRTHS DEATHS
Less than 50 - 4
50 - - -60 - - 2
70 - 3 2
80 - 4 -90 - 4 3
Data not available 2 2
roT~ 13 13
Generally, the data base for morbidity and maternal and child health statistics includes only government clinics and hospitals. The same is true for manpower data.

- 13 -
2.3.4.3 Accuracy
To measure the accuracy of census data, respondents were asked whether they measure the extent of their content and coverage errors, these being the most common errors committed in the conduct of the census. Of the thirteen countries, nine answered in the affirmative, while two ssid no. The respondents of the two other countries could not provide any information.
Of the nine countries where these errors are messured, seven indicated doing post-enumeration surveys as their means of detecting and estimating these errors. One country reported doing it by record matching, while one other did not know the specific method used. Seven of these countries make corresponding adjustments for such errors in their official estimates of the population.
In the case of vital statistics, the measures of accuracy used were the reported percentage of deaths medically certified and the percentage of births medically attended. For both types of data, information was provided only by eight of the thirteen countries. Of these, four reported the percentage of medically certified deaths to be at most only 50%. The figures for the proportion of medically attended births are relatively higher; five of the countries reported this figure to be between 51% and 75% while the three other countries reported higher figures. Theae are shown in detail in Table 4.
Table 4. Distribution of countries according to percentage of deaths medically certified and percentage of births medically attended
% NUMBER OF COUNTRIES DEATHS MEDICALLY BIRTHS MEDICALLY
CERTIFIED ATTENDED
o - 25 1 -26 - 50 3 -51 - 75 2 5
76 - 100 2 3
No data available 5 5
roTll 13 13
Another indirect measure of the accuracy of the vital statistical data being generated is the existence of training programmes for peripheral level personnel responsible for the registration of vital events. Of the twelve countries who answered this question, seven indicated the absence of such training programmes.
- 14 -
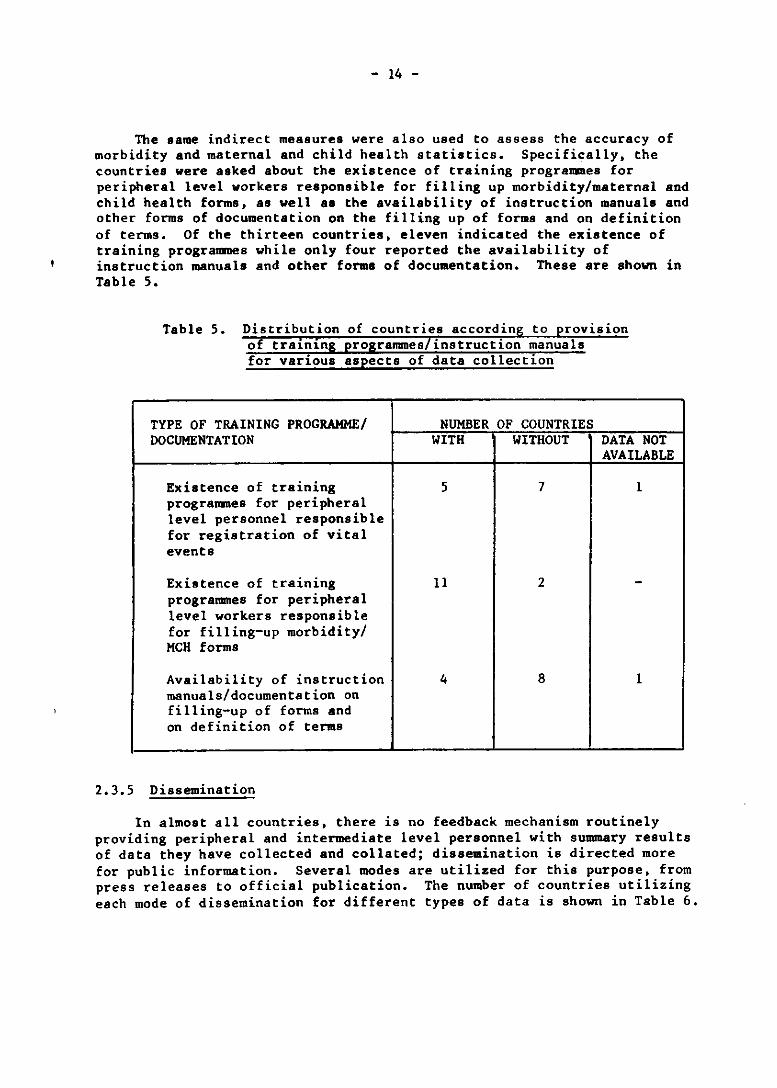
The same indirect measures were also used to assess the accuracy of morbidity and maternal and child health statistics. Specifically. the countries were asked about the existence of training programmes for peripheral level workers responsible for filling up morbidity/maternal and child health forms. as well aa the availability of instruction manuals and other forms of documentation on the filling up of forms and on definition of terms. Of the thirteen countries. eleven indicated the existence of training programmes while only four reported the availsbility of instruction manuals and other forms of documentation. These are shown in Table 5.
Table 5. Distribution of countries accordin rovision of training programmes instruction manuals for various aspects of data collection
TYPE OF TRAINING PROGRAMME/ DOCUMENTATION
Existence of training programmes for peripheral level personnel responsible for registration of vital events
Existence of training programmes for peripheral level workers responsible for filling-up morbidity/ MCH forms
Availability of instruction manuals/documentation on filling-up of forms and on definition of terms
2.3.5 Dissemination
NUMBER OF COUNTRIES WITH WITHOUT
5 7
11 2
4 8
DATA NOT AVAILABLE
1
1
In almost all countries. there is no feedback mechanism routinely providing peripheral and intermediate level personnel with summary results of data they have collected and collated; dissemination is directed more for public information. Several modes are utilized for this purpose. from press releases to official publication. The number of countries utilizing each mode of dissemination for different types of data is shown in Table 6.

- 15 -
Table 6. Number of countries utilizing each mode of dissemination for different types of data
MODE OF TYPE OF DATA DISSEMINATION CENSUS VITAL MORBIDITYI
STATISTICS MCH
Official publication 11 9 10
Occasional newsletter 6 I -Press releases 5 - -Upon request 7 4 4
Data not disseminated - 3 4 I
2.3.6 Sample survey capability
MANPOWER
3
--3
3
One area of interest in the assessment is the capability of the Ministry of Health to conduct sample surveys. This facility is complementary to the routine statistical system, and is important because it covers information on the general population rather than information on patients presenting themselve8 to health facilities for services, something no clinic ba8ed facility can easily provide. In addition, such capability need to be developed first before one can mOve on to a system where only the most basic information needed for the operation snd management of health services will be routinely collected and transmitted to higher levels, while other supporting information and those dealing with specialized topics will be collected by sample surveys.
One of the questions asked regarding sample survey capability is whether they have actually undertaken sample surveys in the past on specific areas of interest, for different types of health statistics. Eleven of the respondents representing the census indicated that their agency has conducted sample surveys in the past. Seven of the countries indicated that they have done sample surveys in the area of morbidity, while only two reported the same for both vital statistics and manpower. These findings support the general observation that sample survey capability often rests with the Census Bureau.
2.3.7 Problems encountered
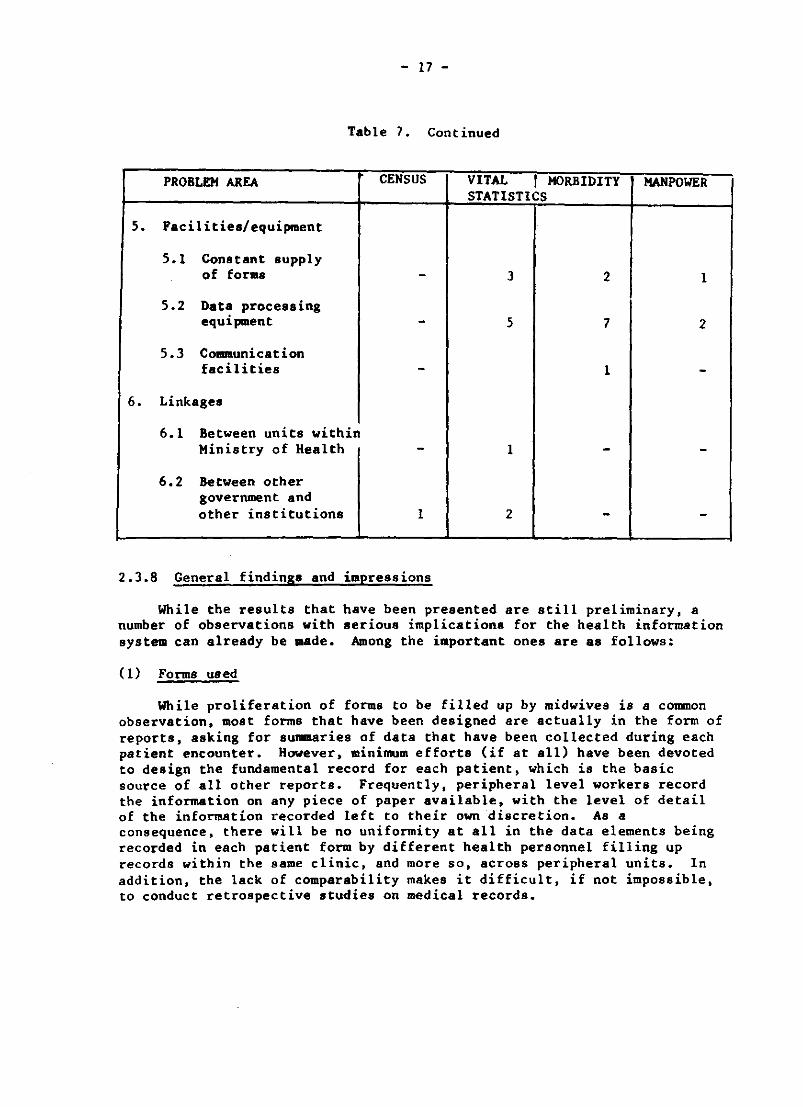
The final section in the assessment protocols dealt with the problems encountered by the different countries in the areas of data quality, manpower, training, technical capability, facilities/equipment and establishment of linkages. Among the problems frequently mentioned were the completeness of coverage of vital statistics, the lack of funds to create new positions, the conduct of in-service training programmes, and lack of data processing equipment. The actual number of countries indicating each type of problem is shown in Table 7.

1.
2.
3.
4.
- 16 -
Table 7. Number of countries who have indicated specific problem areas for different kinds of health statistics
PROBLEM AREA CENSUS VITAL , MORBIDITY MANPOWER STATISTICS
Data quality
1.1 Completeness of coverage 2 6 4 1
1.2 Accuracy 1 3 3 3
1.3 Timeliness 3 2 3 1
Manpower
2.1 Difficulty of recruitment 1 2 2 -
2.2 Lack of funds for new position - 2 6 1
2.3 Lack of funds to offer competitive salary - 2 2 1
2.4 Availabil ity of qualified personnel
- to be trained 3 3 2 1 - already trained - 2 4 -
Training
3.1 In-service training 3 - - -- peripheral level - 4 7 -- intermediate leve - 4 5 -- national level - 3 6 1
3.2 Post-graduate training programmes 2 1 2
Lack of local technical capability
4.1 Development/design of forms 2 1 3 -
4.2 Data management 1 - 2 -4.3 Data analysis/
interpretation 3 2 4 -
i
i
- 17 -
Table 7. Continued
PROBLEM AREA CENSUS VITAL r MORBIDITY MANPOWER STATISTICS
5. Facilities/equipment
5.1 Constant supply of forms - 3 2 I
5.2 Data processing equipment - 5 7 2
5.3 C OIIIIIIuni cat ion facilities - 1 -
6. Linksges
6.1 Between units within Ministry of Health - I - -
6.2 Between other government and other institutions I 2 - -
2.3.8 General findings and impressions
While the results that number of observations with system can already be made.
(1) Forms used
have been presented are still preliminary, a serious implications for the health information
Among the important ones are as follows:
While proliferation of forms to be filled up by midwives is a common observation, most forms that have been designed are actually in the form of reports, asking for summaries of data that have been collected during each patient encounter. However, minimum efforts (if at all) have been devoted to design the fundamental record for each patient, which is the basic source of all other reports. Frequently, peripheral level workers record the information on any piece of paper available, with the level of detail of the information recorded left to their own discretion. As a consequence, there will be no uniformity at all in the data elements being recorded in each patient form by different health personnel filling up records within the same clinic. and more so, across peripheral units. In addition, the lack of comparability makes it difficult, if not impossible, to conduct retrospective studies on medical records.

- 18 -
(2) Data processing
The summary forms that have been designed are actually complicated cross-tabulations involving several variables. It is not uncommon to find 4-way tables in some of these forms. It may be too presumptuous to expect peripheral level workers, most of whom ha~e.only a high ~chool educa~ion, to fill up these forms correctly. In addltl0n, the multlple processlng of data, as it flows from the peripheral level to the national level, immensely increases the potential for errors.
(3) Data analysis
A common observation made with respect to data flow is the progressive compilation of data, resulting in the lack of geographic detail of the information maintained at the national level. This limits the utility of the indicators generated.
(4) Dissemination of data
The most notable observation made with respect to data dissemination is the complete absence of a feedback mechanism to peripheral and intermediate level personnel regarding data that they have collected and collated. As a consequence, most of these workers do not understand and appreciate at all the uses for which the data are generated. This will have repercusssions on the quality of data that they will produce and the amount of time they are willing to put into it.
3. NATIONAL HEALTH INFORMATION SYSTEM CONCEPTS AND PRINCIPLES
3.1 Introduction
A national health information system may be defined in terms of its purposes and objectives, sources of information, primary users of information, producers of information, system design, organizational structure, data flow, outputs and products. In almost every instance, the system, as defined and developed, will be complex and unique to the characteristics and needs of each country. To facilitate the further development and improvement of existing information systems, it is useful to identify certain concepts and principles which are COmmon and important to all national systems. These will assist in developing alternative models and in providing guidance and technical cooperation to assure the production of timely, accurate and relevant information to meet priority needs in health.
3.2 Conceptual framework and background
The hasic sources of information and data regarding health are:
The Population - information directly obtained, usually by interview or sample survey
Health manpower - information directly obtained by query to trained personnel

- 19 -
Re~lth fac~lities - information directly obtained from institutions wh1ch prov1de care or meet other responsibilities in the health arena
Recorda - adminiatrative, health care and other record and reporting systems
In the instance particularly of information systems based on records it must be acknowledged that such systems are developed usually to serve ~ primary purpose as, for example, patient care and management, vital registration or licensing of manpower. Increasingly. these systems are serving multiple purposes: their primary purpose for which they were designed; programme management; programme monitoring and evaluation; surveillance; planning; and assessment of health status are some examples. Their incorporation into a national health information system requires recognition of these multiple purposes and a design and structure for the system that assures that all priority needs for information are met with efficiency, minimal duplication and without encumbrance of the basic system beyond its capability to produce relatively accurate and timely data.
For any identified component of a national health information system. emphasis must be placed on the basic collection mechanism and process. What information is collected, by whom, for what purposes? Row is the information requested or obtained? Row is it recorded? Row is it transcribed and transmitted? Row are the basic records maintained? Secondary uses of the data cannot be met with any reliability without a basic understanding of this aspect of the system or without an adequate programme of data collection snd quality control at the source.
As any component of the system is identified, developed, expanded or modified, it is essential that the primary USers and uses of the data be identified, that required data elements be defined, that purposes and dsta elements be rejected that are not relevant to the source and that decisions are made that best accommodate the priority needs for data and the capacity of the basic design of any given component of the system.
The system must be designed and modified to facilitate the recording and collection of accurate information at the source. The capacity of individuals or institutions to provide accurate and relevant information must be considered. The capacity of those who collect and record must be considered. Flexibility should be permitted to best accommodate these needs in the collection and storage of basic records from which data may be abstracted on a current or retrospective bases for mUltiple purposes.
Those involved in data collection at the source should understand the purposes for which data are collected. To the extent possible, data elements are best excluded from the system that have little utility for the primary purpose for which a system was developed. Health personnel will adhere to the requir~ments of data systems when the utility of the information is clear and important to their primary function.
As a component of the national health information system is identified and defined, it is paramount that the decision-making process regarding its design, structure and function be based on input from the primary users of the data'and the producers of the data. Unilateral decisions should not be

- 20 -
permitted, placing, for example, demands on the syste~ by users withou~ . consideration of the problema of the producers or having producers modif~ basic data elements without agreement with those users who are dependent on those particulsr data elements.
The greatest volume of data will be collected and maintained at the source of the information. At that level, to meet the primary functions of most components of an information system, it is necessary to have detailed information regarding individuals and/or events. For most other purposes, summary or sample data may be abstracted to be forwarded to other agencies and personnel. Requirements should be reviewed critically to assure that only data that are absolutely essential be summarized and reported. Samplea should be used when complete coverage is not essential. In this manner, limited resources can best be used to meet priority objectives.
Rigidity in requirements and guidelines for any component of the system should be kept to a minimum. Whenever feasible, opportunities to adapt to local purposes, variations and characteristics should be facilitated. However, certain requirements are essential, for example, to assure comparability of data over time between geographic areas and between population groups. While, for example, patient care may not require rigidity in data requirements from one clinic to the next, it becomes essential to have comparability when a major objective may be to evaluate trends over time or to compare health care as delivered in different communities within a country. For any given component, flexibility can be met by defining minimum data sets, developing standard definitions and guidelines, and recommending basic quality control procedures which serve as technical resources for countries to use as they develop and refine their information systems over time.
Minimum data sets can be defined as a core set of items that serve a variety of uses such as patient care, institutional management, programme management, evaluation, policy-making at all levels, and research. The word "minimum" should be stressed. The data sets should be restricted to the smallest core of data elements which are essential to meet the requirements of the principal users and purposes of the system. Criteria for inclusion in the data set should include utility of the item, feasibility of collecting the item with reasonable accuracy, reliability and economy and an assessment that the item is best collected from the particular component of the system under study. Data sets between various components of sn overall national syatem must, however, be coordinated in many instances. For example, if socioeconomic descriptions of patients do not correspond to those used in a census activity, accurate population-based rates will not be feasible.
Precise definition of the components of a national syatem, identification of priority uses, development of core data elements, specification of standards and definitions, effective design for collection, processing and transmission will contribute significantly to building and improving an information system which can respond to meet needs. However, each component of the system, to perform in an efficient and precise manner, is most dependent on well-trained staff who understand the purposes of the data collection and have relevant knowledge of the

- 21 -
des~g~ and speci~i~ations of the.sys~em. The selection of qualified s~aff, tralni~g, supervlslon and communication become essen~ial elemen~s of an ~ffectively operated system. These efforts must be ongoing and designed lnto the support structure for the system.
3.3 Basic principles
(1) Each country has a responsibility to design and ensure the operation of health information systems which permit identification of health problems, monitoring the status of ~he health of the population and planning and evaluating a wide variety of health programmes and activities. These information aystems should and will differ in design as they reflect the variations in legal authorities, organizational struc~ure, health care practices, cultural environment and the current heal~h problems.
(2) The development of a specific model therefore, has limited utility in collaborating with countries in this enterprise. It is more important to recognize the features that all national health information systems will have in common and to think in terms of alternative models which build upon sound principles in their design and operation. Examples, guidelines and other technical materials can be developed and shared which will greatly accommodate countries in developing, modifying and improving a system which, while it builds upon ~heir own needs and structure, can nevertheless provide comparstive statistics for national and international purposes.
(3) The basic components of a national health information system are usually best defined in terms of the source of the information and data flow. For example, components may be identified in terms of vital statistics, hospital care, clinic care, etc. Even in the instance of vital statistics, the design characteristics will be different for the birth and death records as the initiation of the basic record occurs in different settings.
(4) It should be the goal of each country to develop over time a fully comprehensive health information system which will permit continuing with periodic access to information from all of the basic sources: the population, health personnel, health institutions and relevant health reCOrds. There are many data elements, critical to some assessments, that can only be obtained through one particular source. Increasingly, the effective study snd resolution of most health problems require data from multiple sources that are collected in a precise and timely manner to permit appropriate analysis.
(5) A broad conceptualization of a national health information system is necessary to ensure that fundamental objectives can be defined and met, such a8 ongoing assessments of the health status of ~he population and monitoring changes in health as related to new programmatic efforts. As priority objectives are defined,

- 22 -
necessary indicators can be identified, data elements outlined and decisions made as to the most relevant sources of an overall set of information. A cooperative enterprise in this effort should function to critically review all proposals and ensure that only the most important data are integrated into the system, that inappropriate sources are not used and that the total system operates to produce relevant, accurate data as they are needed on a timely basis.
(6) An organizational structure must exist or be developed to identify major components of the system and to ensure management of the system through involvement. cooperation and commitment of the primary users and producers of dats. Typically. this structure will be complex and involve various units of government snd the health community. The complexity of the design of an overall health information system requires a structure which assures that all relevant organizations are involved and share in the commitment to design and operate the system. Nevertheless. it is critical in moving to improved structures to ensure leadership by an agency or unit of an agency where authority is provided to facilitate the development and growth of the system. and where there exists access to all relevant technical and scientific expertise.
(7) In many countries. it will be necessary to consider legal authority for the operation of the system and the collection of dsta. In addition. legis 1st ion and/or guidelines will be required to assure the appropriate balance between legitimate access to data and. when necessary. protection of privacy and the confidentiality of data.
(8) As each component of the system is identified. cooperative efforts involving both primary users and producers of data should define and approve the primary objectives of the system. the necessary core data elements. appropriate definitions and standards. data collection and processing protocols. reporting requirements. and data flow, quality-control procedures and necessary training materisls.
(9) Detailed data should be maintained at the sOurce and reporting requirements kept to a minimum of only elsential seta of information. The cooperative definition and management of the system should provide for a review and decision-making to ensure that reporting requirements are precisely defined. and that the system operates to produce data of acceptable quality for specific purposes. Reporting fr~ one level to another should be handled with optimum efficiency over time. For example. it may be possible to combine reporting for several programme areas of concern such as the many programme. of care provided in a primary care clinic in order to avoid repeated and varying classifications of patient characteristics. Where possible. more detailed reporting may be transmitted through the system when overall volume and resources permit computerization close to the source. This will typically be characteristic only for the larger, more developed countries.

- 23 -
(10) ~s the system is de~ined, developed and modified over time, it is lmportant to communlcate well and on a timely basis between all those involved, users and producers of data and others who have a responsibility to the system. It should be a responsibility of the lead agency to assure such communication, using the relevant resources and products of the jointly developed system and the cooperating units, organizations and personnel. Descriptions, guidelines and supportive technical materials should be developed and routinely made available. Changes, modifications of the system and updated materials should be disseminated on a timely basis. Host importantly, analytical products and outputs of innovative new analytical methodologies should be emphasized. It is these products demonstrating the utility of the system to programme managers and personnel in management and decision-making that will result in improving the system and operate to retain official commitment to the system.
4. OOMPONENT ANALYSIS - AN EXAKPLE
National health information systems are typically complex, involving a variety of data collection and other related activities conducted by mUltiple agencies and organizations within government as well as in the private sector. Historically, health information has tended to flow from local to provincial, to national to international organizations as related to particular health problems or programmes. Increasingly, as information requirements become more complex, it is necessary to examine and evaluate statistical systems as they operate to make data available from identified, unique sources: medical care records; health care clinics, hospitals and other institutions; vital records; health care personnel: surveys of populations; as well as other sources. This is necessry to maximize effficiency and quality, avoid duplication of effort, provide Some flexibility in adjusting to new priorities and ensure response to major health policies and strategies.
Some examples of components within the Iletilth informtition system, as defined by source of information, tire as follows:
(a) Vital statistics
Births Deaths
(b) Health manpower inventories and surveys
Physicians Nurses Psramedical
(e) Health facilities inventories and surveys
Hospitals Clinics

- 24 -
(d) Hospital care statistics
Patient discharge-inpatient care Outpatient
(e) Clinic care statistics
Maternal and child health Communicable disease Noncommunicable disease
(f) Population ststistics
Census information Household interview survey
Each of these components must have certain specifications, in line with the basic principle earlier presented. These are!
(i) Statement of prLmary objectives - identification of major users and identification of those responsible for data collection, training, etc.
(ii) Minimum data set
(iii) Definitions and standards
(iv) Description of data flow
(v) Manual for data collection and processing
(vi) Specification of reporting requirements
(vii) Specification of quality control procedures
(viii) Plans for analysis, tabulation and reports
(ix) Training materials
(x) Plans and management protocols to ensure required trained manpower and other resources
One can take the prLmary care clinic data as an illustrative example of how a single component functions in the light of these principles. Figure I shows the data flow requirements of such a component. From the figure, one can see that among the bases for the identification of data elements in the bssic data record are the existing standards and norms for care and goals in prevention. Another important feature of such a record is that it should be accessible for special studies inVOlving variables not included in routine reports. From the basic data records, summary reports are abstracted for multi-purpose use. Such reports are then transmitted to higher levels like the district, the province, and eventually the Ministry of Health. Analysed data should be fed back not only to routine users but also to the clinics at the peripheral level.

- 26 -
The data requirements at different levels within the system are best exemplified by the Hayan temple diagram shown in Figure 2. The most comprehensive data are collected and maintained at the clinic level, to meetrequirements for patient care and clinic management. Within this data set is a minimum subset of elements which are maintained uniformly by health diatricts and provinces to permit valid comparisons between these geographic subdivisions. The smallest aubset which should be developed cooperatively is the one which is transmitted through all the levels, including the international health organizations. This minimum data set is maintained to permit valid national and international comparisons.
The need for multiple data sources to meet the requirements even of a single component can be appreciated by looking at the regional indicators set by WHO for maternal and child health care. There are nine such indicators, the computation of which necessitates the collection of eighteen different data elements. These data elements with their corresponding sources are enumerated below.
Population
No. of women of child bearing age
By age, race, residence, economic status
No. of pregnant women not seen for antenatal care
No. of children 0-4 not attending clinic
No. of children not immunized
Birth records
No. of births by weight of child
No. of births with trained attendant
No. of infants less than 2500 grams birth weight
Mortality records
Maternal mortality No. of infant deaths Deaths of children by cause
Clinics
No. of visits for antenatal care
No. of women with 3 or more antenatal visits
No. of children 0-4 under routine care
No. of children below standard height/weight measurements
Reportable disease for children Immunizations for children
Hospitals
No. of children discharged with
treatment for malnutrition or related problems
No. of women treated for complications of pregnancy
Discharges of children by cause

LEV E L
WHO/wpRO
NATlOIIAL
PRO'.INCE
IlEALTH DISTRICT
CLINIC
Figure 2. Data requirements at different levels - Example - Single component -Primary care clinic data
. ," ",;-.,
NUTRITIONAL STATUS-CHILDREN 0-4
NO. or PRECHANT WOKEN UNDER CAllE NO. or CHILDREN UNDl!Il CAll!
[ Internst ional indicators to measure progres.
[
National indicator. Health atatu. indicators Priorities and policies
~"':-:' , ' ~ ~, ~
TOTAL NO. or CLINIC VISITS NO. or tMMUNlZATIONS, ETC [
Prolra....., Hanagement Surveillance Programme Planning
~ ~ I
~ . ,
~
MOST DETAILED DATA ARE REQUIRED AT THE CLINIC LEVEL
GProgramme Hanagement Surve i Uance
rogramme Planning
[
Data requirements for patient care and clinic manaaement
JIIf Minimum data set should be developed cooperatively to PERMIT VALID NATIOIIAL AND INTl!IlNATIONAL COMPARISONS
~ Minimum data set expanded at national level to PERMIT VALID COMPARISONS BETWEEN PROVINCES
N .....

- 28 -
5. TOWARDS A MODEL NATIONAL HEALTH INFORMATION SYSTEM
5.1 Introduction
The World Health Organization has, over several decades, been collaborating with countries in the develop~ent of their health information systems. These efforts at collaboration have met with varying degrees of success and were mostly concentrated on technological inputs into development efforts, sometimes under conditions when the health infrastructure could not support these inputs into the system.
Weakness of health infrastructures is therefore a common problem of developing countries and this haa to be tackled in any attempt to develop national health information systems. Since the tool used to evaluate health services and programmes requires itself to be monitored and evaluated, and both facilities are hounded by common infrastructure problems, the problem becomes particularly difficult to solve - especially when the development needs of the health information system have to come into competition with the more immediate demands of the health services.
It would be a useful exercise for every country to construct its own model system in order to meet its particular information needs. The models will provide standards of excellence against which countries can evaluate the systems actually in operation; thus, to enable them to more easily identify their strengths and weaknesses, and so to more effectively direct government and WHO collaborative efforts to more productive ends.
In terms of the regional workshop objective, which was to facilitate the further develop~ent of existing national health information systems, perhaps the best approach is to describe a model national health information system in two parts (see Figure 3).
(a) the core system, which consists of the basic components necessary for an operationally effective health information system; and
(b) the support sy.te~, which is defined by a series of components designed to enhance, extend, and to facilitate activities related to the core system.
The two parts of the model reflect, respectively, the two following major concerns in NHIS development:
(i) Technological, which aims to enable countries to build on the existing information structurea and to constantly review and adapt their information needs according to Changing situations.
(ii) Managerial, which seeks to improve the administrative and management environment in which the health information system operates.
5.2 The core system
The core syst~ has seven components, reflecting the different steps involved from the time the data sets to be collected are identified to the dissemination and utilization of results. Specific concerns for each of these components are discussed in detail in the following sections.

- Zq -
Figure 3. The core and support systems
SYSTEM DESIGN. DEVELOPMENT AND
MANAGEMENT
MULTIPLE COMPONENTS
DATA J::LEMENTS DATA QUALITY DATA COLLECTION. TIMlNG .-.ND FLOW DATA PROCESSING DATA ANALYSIS DATA DISSEMINATION SURVEY/SPEClAL STUDY CAPABILITY

- 30 -
5.2.1 Data elements
The identification of the specific data elements to be collected is one of the most crucial steps in the development of the NHIS. All other activities revolve around it; the utility of the system is highly dependent on it.
A common observation among countries with respect to the collection of data elements is the proliferation of data sets. Different health programmes organized vertically within the Ministry of Health have traditionally been collecting their own data, independent of, and with very little coordination with other health programmes. This has brought about the proliferation of forms to be accomplished by peripheral level workers, hence significantly increasing the time and cost of data collection and recording. The high degree of duplication of data elements across forms and the problems arising from the absence of uniform and standard definitions muddle the system even further with serious repercussions on the quality and utility of the data being generated. These problems call for the need for a coordinated effort to establish a record system from which minimum and uniform data can be obtained.
The concept of a "uniform minimum basic data set" is not new. It started as early as 1880 when the National Board of Health of the United States convened the State and local registrars to deliberate on the best methods for collecting and publishing vital statistics. Since then the concept has greatly expanded, having been applied to many additional areas of health statistics.
The basic principle behind the concept of minimum basic data sets is for various users to agree on the content, terms and classification of the elements in the data set deemed to be the most necessary for planning, providing, monitoring and evaluatinf health care. To meet its ends, it must have the following properties:
(1) A minimum basic data set should refer to some comprehensive class of persons, places or events that are common to a broad category of health care settings. As an example, the data set can refer to patient visits in out-patient settings in general, rather than to patient visits in specialized clinics like family planning, well-baby or sexually-transmitted disease clinics. The generalization of the data set to out-patient settings covers both the specialty clinics and the general out-patient departments.
(2) A minimum basic data set is a core of items that serve a wide variety of uses such as institutional management, patient care, programme management, billing, evaluation, policy-making at all levels, and research. A data set designed for a single purpose, i.e. billing, would not qualify as a minimum basic data set.
lRice, D.P., "Uniform minimum basic data sets and their implications". Paper presented at the 7th International Congress on Medical Records Meeting, Canadian Association of Medical Record Librarians, Toronto, Canada, 15 September 1976.
- 31 -
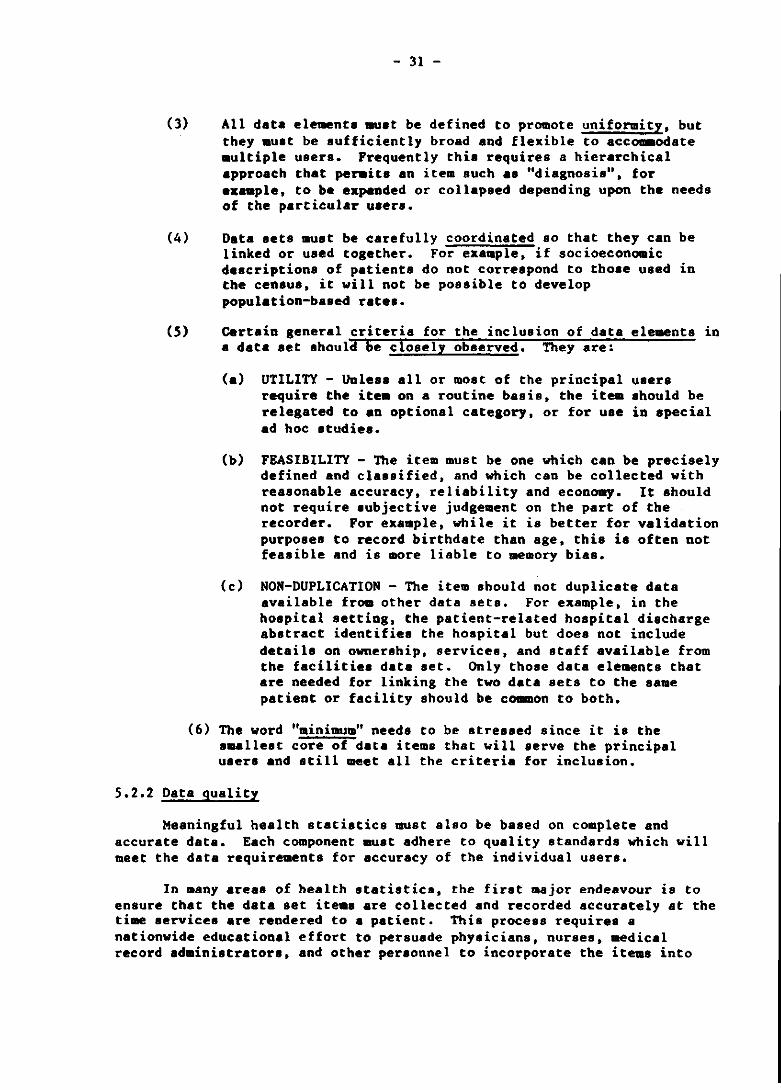
(3) All data eleuenta ~at be defined to promote uniformity, but they muat be aufficiently broad and flexible to accommodate aultiple users. Frequently thia requires a hierarchical approach that penita an item such as "diagnosis", for example, to be expanded or collapsed depending upon the needs of the particular uaers.
(4) Data aets auat be carefully coordinated so that they can be linked or used together. For example, if socioeconomic descriptiona of patienta do not correspond to thoae uaed in the censua, it will not be possible to develop population-based rate ••
(5) Certain general criteria for the inclusion of data elements in a data set ahould be closely obaerved. They are:
(a) UTILITY - Unless all or moat of the principal users require the ite. on a routine basis, the it .. ahould be relegated to an optional category, or for uae in special ad hoc studies.
(b) FBASIBILITY - The item must be one which can be precisely defined and classified. and which can be collected with reasonable accuracy, reliability and econo.y. It ahould not require aubjective judgement on the part of the recorder. For example, while it ia better for validation purposes to record birthdate than age. this is often not feasible and is more liable to memory bias.
(c) NON-DUPLICATION - The item should not duplicate data available from other data sets. For example, in the hoapital setting. the patient-related hospital diacharge abstract identifies the hospital but doea not include details on ownership. services. and staff available from the facilities data set. Only those data elements that are needed for linking the two data sets to the same patient or facility should be common to both.
(6) The word "minimum" needs to be stressed since it is the smallest core of data items that will serve the principal uaers and still meet all the criteria for inclusion.
5.2.2 Data quality
Meaningful health statistics IIlUst also be based on complete and accurate data. Each component IIlUSt adhere to quality standards which will meet the data requirements for accuracy of the individual users.
In .any areas of health atatistica, the firat .ajor endeavour is to ensure that the data set ite.a are collected and recorded accurately at the time services are rendered to a patient. Thia process requirea a nationwide educational effort to persuade phyaicians, nurses. medical record adminiatrators, and other personnel to incorporate the iteaa into

- 32 -
existing record-keeping procedures, which should be standardized nationwide. This may involve the conduct of periodic training programmes, especially for peripheral level workers, on the proper collection, recording and processing of data, as well as the development of manuals, guides and other forms of documentation for such procedures. There should be continuing efforts for the evaluation and monitoring of existing quality control procedures. as well as for the testing of new ones.
5.2.3 Data collection, timing and flow
The component management operates the collection process using appropriate methods (e.g. sample of records or encounters, complete or partial abstract of information from a total number of records, etc.) within a timeframe permitting the user with the earliest need for the finished data product to be satisfied. The appropriate flow of data from the site of collection to the site of processing and analysis varies with the urgency and nature of the information to be transmitted, and the kind of data processing availsble.
In the traditional pathways where data are manually processed, information flows, step-by-step, upward through the different echelons of the health services. At each level, data are collated, processed, used by line management and passed up to the next higher level.
With modern electronic data processing methods, data may be captured at the base of the health information system, processed locally and passed to the top of the hierarchy.
For notifiable and other diseases requ1r1ng special public health action and/or investigation, special information pathways may need to be developed. These, however, should be kept to a minimum and only the pathway should be changed, not the recording nor the collection process.
Other relevant activities under this component of the core system are the development, implementation and monitoring of appropriate methods for data collection, the design, testing and introduction of necessary forms, the development and implementation of manuals and guidelines for data collection as well as the ongoing monitoring and evaluation of data collection activities.
5.2.4 Data processing
Much of the "processing" of data within the Region has been on a manual basis. With the advent of the microcomputer, the extent of automation of data processing with the components of an NHIS has been greatly increased. At the component level in this "model", however, we must accommodate for both manual and automated data processing.
A major phase of data processing is the generation of statistical tables for analysis. In places where processing is done on a manual basis, tabulation may be done directly from the forma. In the case of automated systems, the data must undergo a reduction process from a paper/writing medium like a questionnaire or 8 fo~, to a tape. card, disc or some other
- 33 -
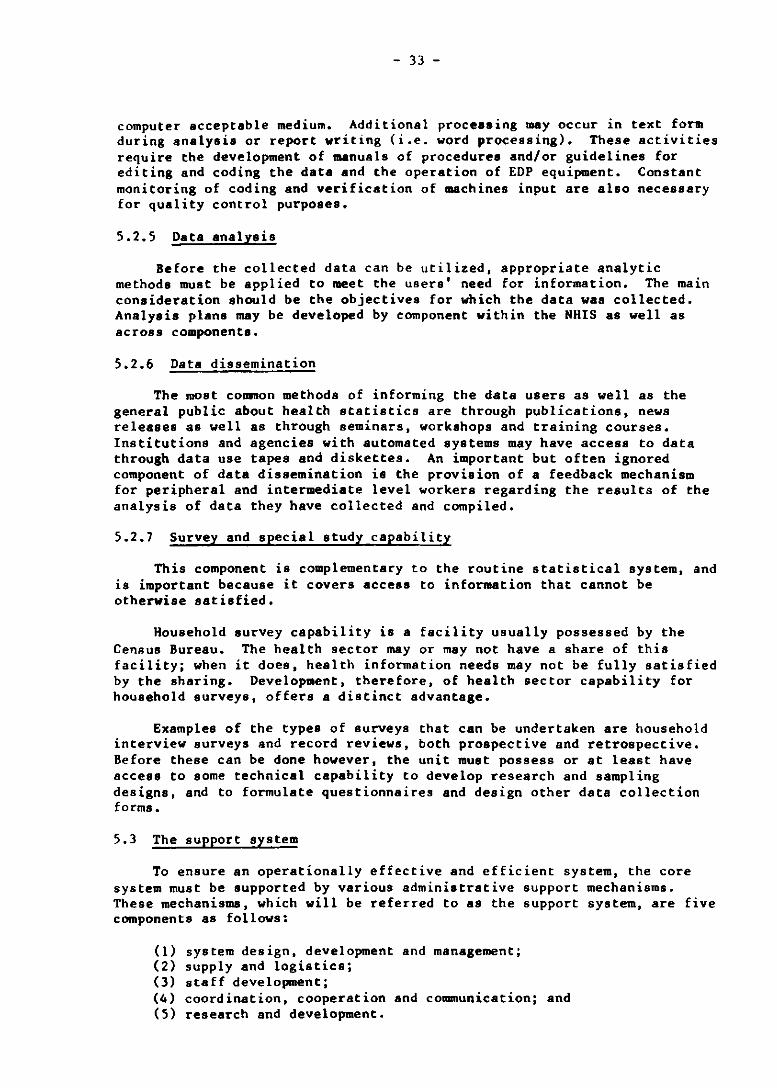
computer acceptable medium. Additional processing msy occur in text form during analysis or report writing (i.e. word processing). These activities require the development of manuals of procedures and/or guidelines for editing and coding the data and the operation of EDP equipment. Constant monitoring of coding and verification of machines input are also necessary for quality control purposes.
5.2.5 Data analysis
Before the collected data can be utilized, appropriate analytic methods must be applied to meet the users' need for information. The main consideration should be the objectives for which the data was collected. Analysis plans may be developed by component within the NHIS as well as across components.
5.2.6 Data dissemination
The most common methods of informing the data users as well as the general public about health statistics are through publications, news releases as well as through seminars, workshops and training courses. Institutions and agencies with automated systems may have access to data through data use tapes and diskettes. An important but often ignored component of data dissemination is the provision of a feedback mechanism for peripheral and intermediate level workers regarding the results of the analysis of data they have collected and compiled.
5.2.7 Survey and special study capability
This component is complementary to the routine statistical system, and is important because it covers access to information that cannot be otherwise satisfied.
Household survey capability is a facility usually possessed by the Census Bureau. The health sector mayor may not have a share of this facility; when it does, health information needs may not be fully satisfied by the sharing. Development, therefore, of health sector capability for household surveys, offers a distinct advantage.
Examples of the types of surveys that can be undertaken are household interview surveys and record reviews, both prospective and retrospective. Before these can be done however, the unit must possess or at least have access to some technical capability to develop research and sampling designs, and to formulate questionnaires and design other data collection forms.
5.3 The support system
To ensure an operationally effective and efficient system, the core system must be supported by various administrative support mechanisms. These mechanisms, which will be referred to as the support system, are five components as follows:
(1) system design, development and management; (2) supply and logistics; (3) staff development; (4) coordination, cooperation and communication; and (5) research and development.

- 34 -
Each component must be designed to facilitate the activities and to enhance and extend the functions of the core system.
5.3.1 System design, development and management
Activities related to system design, development and management are integrated at the highest management level to produce the type of system and system products amenable to meeting mUltiple needs for data, both within and outside the health sector. There are four areas of concern under this subcomponent of the support system, namely (1) the organizational element, (2) authorities, regulations and guidelines, (3) project development, piloting and evaluation, and (4) communication within the system.
5.3.1.1 Organizational elements
The responsibility for the overall definition, development and management of a national health information .ystem should be placed at a focal point located at a high level of the organization, to ensure that information requirements are articulated and understood a. part of the overall management process for health development. Its leadership function is critical both within the system and in a coordinative, cooperative, or collaborative role with other sectors - both at the management level and the information system level.
A prilllllry function of this "focal agency" is to provide a process or forum for the development of minimum basic data sets and definitions, levels of quality, methods of collecting, legitimacy of users, data flow, priorities for component operations and similar activities. It must also establish mechanisms for the periodic revision of existing procedures, including the identification of elements in the minimum data set. The time interval between revisions can vary widely, depending on the subject matter area. An important point to consider is that revisions must not be made unilaterally by any particular group, including the Hinistry of Health, if a consensus among all interested parties is to be maintained. In addition, an implementation plan must be made, allowing sufficient lead time for change-over by pre-existing system., which may require additional data items, redesign of forms, new editing and coding procedures, retraining of data recorders, and modification of existing computer files and programs.
In general, system planning for the NHIS must be carried out at three levela;
(a) integration with the overall Hinistry of Health programme;
(b) coordination with other sector plans; and
(c) within the Hinistry.
Activities emanating from such plans can be expensive and must be carefully budgeted for. The support system should be a direct budget item. In the case of the core system, the coat can either be shared by the users, or the user. can support the syste. by paying for data and data services.
- 35 -
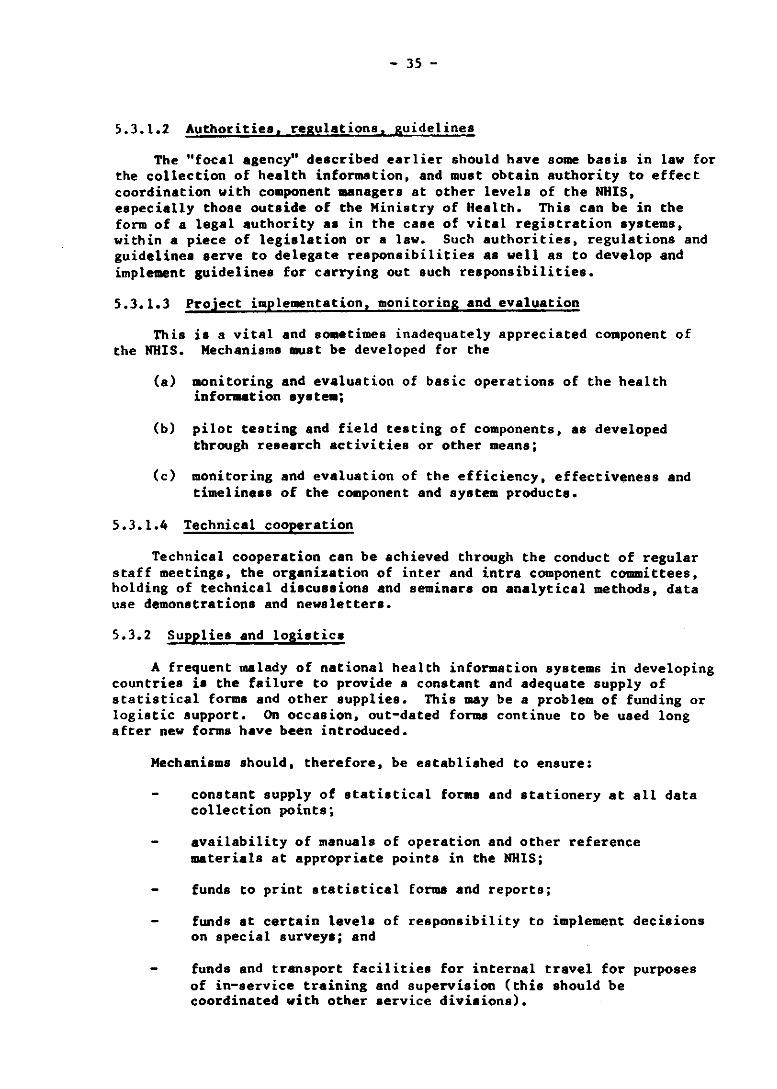
5.3.1.2 Authorities. regulations. guidelines
The "focal agency" described earlier should have some basis in law for the collection of health information. and must obtain authority to effect coordination with component managers at other levels of the NUIS, especially those outside of the Ministry of Health. This can be in the form of a legal authority as in the case of vital registration systems, within a piece of legislation or a law. Such authorities, regulations and guidelines serve to delegate responsibilities as well as to develop and implement guidelines for carrying out such responsibilities.
5.3.1.3 Project implementation, monitoring and evaluation
This is a vital and sometimes inadequately appreciated component of the NUIS. Mechanisms must be developed for the
(a) monitoring and evaluation of basic operations of the health information system;
(b) pilot testing and field testing of components, as developed through research activities or other means;
(c) monitoring and evaluation of the efficiency, effectiveness and timeliness of the component and system products.
5.3.1.4 Technical cooperation
Technical cooperation can be achieved through the conduct of regular staff meetings, the organization of inter and intra component committees, holding of technical discussions and seminars on analytical methods, data use demonstrations and newsletters.
5.3.2 Supplies and logistics
A frequent malady of national health information systems in developing countries is the failure to provide s constant and adequate supply of statistical forms and other supplies. This may be a problem of funding or logistic support. On occasion, out-dated forma continue to be used long after new forms have been introduced.
Mechanisms should, therefore, be established to ensure:
constant supply of statistical forms and stationery at all data collection points;
availability of manuals of operation and other reference materials at appropriate points in the NUlS;
funds to print statistical forma and reports;
funds at certain levels of responsibility to implement decisions on special surveys; and
funds and transport facilities for internal travel for purposes of in-service training and supervision (this should be coordinated with other service divisions).

- 36 -
5.3.3 Staff development
In order to maintain at all times an adequate level of knowledge, understanding and appreciation of the operation of the health information system, it is necessary to develop:
(1) programmes for high level training of selected health personnel in health statistics, health planning and epidemiology;
(2) mechanisms for continuing training of supervisors;
(3) mechanisms for continuing supervision and in-service training of peripheral data collectors;
(4) the upgrading, through training, of managerial skills at national, regional, district and community levels in order to instil a greater appreciation of the use of statistics for management, planning and evaluation; and
(5) the appropriate roles, tasks and functions required at different levels of care, and training and reorientation of staff to carry them out effectively.
Other issues related to staff development are the recruibnent and retention of personnel. Problems of retention may be lessened if a career ladder exists, especially for those who have undergone advanced training. Giving assignments across components and/or across functions, and assigning tasks which will develop the staff's full potential may help make positions more interesting and challenging.
5.3.4 Research and develOpment
Research and development activities are essential for the growth of the system. Examples of potential areas for research and development are:
(1) Data sets and classifications
The process for development of a minimum basic data sets varies according to the specific needs of the users. The most common approach is to convene a working group of experts representing data users and data provider. to think broadly about the problems and come up with preliminary recommendations. The recommendations are then transmitted to the Committee on Minimum Basic Data Sets of the Ministry of Health (expanded) for refinement, testing, solicitation of advice from other interested parties, and eventual promulgation. Another approach would be for a small Ministry of Health staff involved in a specific component area to develop a proposed data set and then circulate it widely for written comment to data providers, users and other interested persons. (Minimum basic data sets are always a compromise.)
(2) Data use and analysis
A data use and analysis function would serve as a clearing house regarding effective techniques for using data generated by the system. Innovative uses of data could be identified, documented and disseminated through published materials, meetings and training programmes.

- 37 -
(3) Improved processinl and automation
Automation reaearch and development functions are in three areae' (1) nev hardvare and their place in the system: (2) innovative softvare for component or syetem applications; and (3) improved data reduction equipment such as key-to-disk or optical character recognition devicea.
Improvement in data processing overlaps the automation function somewhat but collection methods and data editing and coding techniques are in need of experimentation to develop new approaches and techniques.
(4) SYstem exteneion
System extenaion activities would centre around a focal point activity to stay abreast with nev health programme development and priorities, to attempt to forecast nev inforaation requirements, and to interface vith the component managers, other R&D staff and coordination staff to front-end load the planning and system design functions of the support structure.
5.3.5 Coordination, cooperation and communication
No activities described earlier in both the core and support systems will vork unless a certain degree of inter and intrasectoral coordination, cooperation and communication is obtained.
Cooperating units/agencies still have control of their own staff and budget and assume full responsibility for their respective areas. The decision to join hands and pull together reaources for a common end is well-intentioned and is based only on merit.
Coordination on the other hand must be done with authority. Without such authority the linkage becomes only cooperation.
Both cooperation and coordination necessitate an effective communication system to be effective. This can be attained through the formstion of advisory groups, the conduct of technical discussions, workshops and seminars, the assignment of staff across agencies, and the exchange of newsletter. or technical note ••
6. CONCLUSIONS AND RECOMMENDATIONS
The following recommendations are given based on the results of the assessment and the discussions during the workshops:
(1) Assessments should be completed on all Hember States of the Region as feasible. It is also recommended that a mechanism should be developed to update the information contained in the assessments on a periodic basi.. A protocol should be developed to ensure that the periodic updates are conducted in such a manner as to ensure the collection of appropriate information in a uniform manner with coverage of all relevant items.

- 38 -
(2) At the minimum, an analysis of the assessment documents should include the countries' capability to produce minimally defined indicators in the areas of maternal and child health, manpower, communicable and noncommunicable disease. Next in priority would be a review of the assessment results as related to priorities regarding primary health care.
(3) Time permitting, there would be merit in an evaluation of the protocols and procedures used in the assessments and revision for future use.
(4) Summaries of the country reports and plans should focus on categorization of priorities and defined areas of need as related to mechanisms that may be appropriate to meet these needs.
(5) It might prove useful to summarize results of the assessments on a component-by-component basis. Additional interest might be generated in other relevant agencies, for example, by a comprehensive analysis of the status of census data in the Region.
(6) It is recommended that other Regional Office staff should be encouraged to use the assessment documents as relevant to their needs.
(7) Results of the assessments and the workshops should be formally communicated to the regional advisers and other appropriate staff with analysis of the results presented regarding the availability and gaps in information required in programme areas of need.
(8) Depending on the level of interest, two or more programme areas might be selected to jointly pursue appropriate follow-up activities related to the country plans ensuring an integrated approach in working toward effective health information systems which will have the strength and flexibility to meet multiple areas of need.
(9) Appropriate results of analysis should be provided to all country participants, observers, staff and consultants involved in the assessments and workshops.
(10) Programme plans impacting on health information systems should be reviewed periodically to ensure consideration of the priorities and plans of the countries.
(11) Follow-up on the assessments should encompass documentation of modifications in the plans and priorities of the countries.
(12) All follow-up projects and activities, including those supported by other agencies, should be documented and encompassed in an overall evaluation of the activity within the next budget cycles of WPRO.

- 39 -
ANNEX 1
LIST OF PARTICIPANTS, OBSERVERS, CONSULTANTS, AND SECRETARIAT
A. Manila, 23-27 September 1985
BRUNEI DARUSSALAM
CHINA
HONG KONG
MACAU
1. PARTICIPANTS
Dr P. Durayappah Senior Medical Officer Medical and Health Headquarters Miniatry of Education and Health Bandar Seri Begawan
Mr Pg Mohiddin Tajuddin Senior Medical Records Officer Ministry of Education and Health Bandar Seri Begawan
Dr Li Biying Aaaociate Professor Inatitute of Medical Information Chineae Academy of Medical Sciences Beijing
Dr Jiang Feng Assistant Researcher The Research Centre for Health Planning and Statistic. Miniatry of Public Health Bei jing
Dr Susan Chan Principal Medical and Health Officer Medical and Health Department Hon& Kong
Dr Mario Manuel de Jesus Pinho da Silva Director Medical and Health Services Direc~ao do. Servi~os de Saude Macau
Dr Haria Helena V.F. da Silva Gon~alves Vieira Technician, Planning Sector Direc~lo dos Servi~o8 de Saude Macau

Annex I
HALAYSIA
PHILIPPINES
REPUBLIC OF KOREA
SINGAPORE
- 40 -
Hr Chong Yok Ching Mathema t ician Planning and Development Division Ministry of Health Kuala Lumpur
Dr Ismail Hohd. Noor Deputy Director Department of Hedical and Health Services Kedah
Dr Ahmad Tajudin Jaafar Deputy Director (Medical) General Hospital Pahang Road Kuala Lumpur
Dr Conrado Galsim Jr. Chief Medical Division Ministry of Health Regional Health Office No. I San Fernando La Union
Dr Zenaida Ludovice Chief Division of Health Statistics Health Intelligence Service Ministry of Health Hanila
Hr Jong Hwa Byun Senior Researcher Korea Institute of Population and Health Seoul
Dr Young-Soo Park Associate Profe.aor The Korea National University of Education Chung-Bug
Hr Khoo Jin Hoe Senior Statistician Ministry of Health Singapore
Dr Ling Hun Kin Deputy Head Quarantine and Epidemiology Department Hinistry of Environment Singapore
- 41 -
2. OBSERVERS
Mr Hiroichi Hagivara Manager Service Division
Annex 1
Southeast Asian Medical Information Centre/ International Medical Foundation of Japan Tokyo Japan
Dr Hakoto Ohashi Director Department of Microbiology Tokyo Metropolitan Research Laboratory of Public Health Tokyo Japan
3. CONSULTANTS
Dr Gail F. Fisher Associate Director Programme Planning, Evaluation and Coordination National Centre for Health Statistics Maryland
Dr Ophelia M. Mendoza Assistant Professor and Chairman Department of Epidemiology and Biostatistics Institute of Public Health University of the Philippines Manila
4. SECRETARIAT
Mr H.S. Dhillon Chief Human Resource Development WHO Regional Office for the Western Pacific P.O. Box 2932 Manila

Annex I
- 42 -
Dr Hu Ch ing-Ii Regional Adviser in Maternal and Child Health WHO Regional Office for the Western Pacific P.O. Box 2932 Manila
Dr T. IlIIBi Computer Systems Analyst WHO Regional Office for the Western Pacific P.O. Box 2932 Manila
Dr R.D. Mercado Director Health Services Development and Planning WHO Regional Office for the Western Pacific P.O. Box 2932 Manila
Dr A. Reyes Acting Regional Adviser in Communicable Diseases WHO Regional Office for the Weatern Pacific P.O. Box 2932 Manila
Dr J.M. Robey (Operational Officer) Regional Adviser in Health Information WHO Regional Office for the Western Pacific P.O. Box 2932 Manila
Mr Y. Sato Information AnalYlt WHO Regional Office for the Weatern Pacific P.O. Box 2932 Manila
Dr Y. Terao Regional Adviser in Noncommunicable Diseases WHO Regional Office for the Western Pacific P.O. Box 2932 Manila
Mr K. Uemura Director Epidemiological Surveillance and Health Situation and Trend Asa.88ment WHO Headquarters Geneva

.43 -
Annex 1
B. Suva, Fiji, 21-15 October 1985
AllEUCAN SAMOA
roOK ISLANDS
FIJI
GUAM
1. PAKTICIPANTS
Dr Bernard N. Killner Deputy Director of ijealth L.B.J. Tropical Kedical Center Tutuila
Kr Anetere'a Andy Puletasi Deputy Director Health Planning Agency L.J.B. Medical Centre Tutuila
Dr George Koteka Director-General of Health Hinistry of Health Rarotonga
Hr Ngari Munokoa Tini Health Statistics Officer Ministry of Health Rarotonga
Mrs Vilimaina Naroba Medical Statistician Medical Statistics Ministry of Health and Social Welfare Suva
Dr Sakio 1. Varea Acting Divisional Medical Officer Miniatry of Health and Social Welfare Suva
Hr David Chandra City Heal th Officer Suva City Council Suva
Mr Michael Duenas Administrator Health Planning and Development Agency Government of Guam Agana
Mrs Ann H. Untalan Director Office of Planning, Evaluation and Grants Management Department of Public Health and Social Services "'ana

Annex 1
KIRIBATI
PAPUA NEW GUINEA
SArfOA
SOLOMON ISLANDS
TONGA
- 44 -
Mrs Atu Moaniba Health Information Officer Ministry of ~ealth and Family Planning Tarawa
Dr Terenganuea Taaram Senior Medical Officer Ministry of Health and Family Planning
. Tarawa
rfr Raka Guma Coordinator Policy, Planning and Evaluation Division Department of Health Boroko
Dr John Sa i rere Provincial Health Officer Division of Health East Sepik Province
Dr Likei Theo Acting Assistant Secretary of Health Division of Health Department of Morobe Morobe Provine e
Dr John Ah Ching Registrar Obstetrics and Gynaecology Unit Western Samoa National Hospital ~
Dr Tipasa Me Health Planning and Information Officer Health Department Apia
Ms Terira Eria Statistics Clerk Statistics Division rfinistry of Health and Medical Services Honiara
Dr N. Kere Undersecretary/Health Improvement Ministry of Health and Medical Services Honiara
Mr S.B. Kautoke Assistant Secretary for Health Ministry of Health Nuku'alofa
Dr S.T. Puloka Senior Medical Officer Vaiola Hospital Ministry of Health Nuku'alofa
TRUST TERRITORY OF THE PACIFIC ISLANDS
VANUATU
- 45 -
118 Lynnette Araki Chief Health Planner Division of Health Services Federated States of Micronesia Ponape
Ma Julita Meyar Heal th Planner Bureau of Health Services Koror Pa'i8u
IIr Tamic Romson Health Service Administrator Ar.er Ishoda Memorial Hospital Majuro Marshall Islands
Dr Selwyn Leodoro
Annex'
First Secretary to Minister of Health Ministry of Health Vila
Dr Bernard Montaville Medical Superintendent Vila Central Hospital Ministry of Health
Yi!!
2. OBSERVERS
Ma Pat Monahan Peace Corps Volunteer
~ S....,a
Dr Richard Taylor Epidemiologist South Pacific commission Noumea Cedex New Csledonia
3. OONSULTANTS
Dr Gail F. Fisher Associate Director Programme Planning, Evaluation and Coordination National Centre tor Healtn Statistics Maryland

Annex 1
- 46 -
Dr Opnelia M. Mendoza Assistant Professor and Chairman Department of Epidemiology and Biostatistics Institute of Public Healtn University of tne Philippines Manila
4. SECRETARIAT
Dr R.W.K. Gee Medical Officer ICP/CVD/OOl Suva
Mr P. Hedrick Statistician ICP/PHC/002 Suva
Dr H. Mehta Medical Officer ICP/HST/OOl Suva
Dr J .M. Robey (Operational Officer) Regional Adviser in Healtn Information WHO Regional Office for the Western Pacific P.O. Box 2932 Manila
Hr M. Subramanian Scientist Development of Epidemiological and Health Statistical Services \IRO Headquarters Geneva

- 47/48 -
AGENDA
1 Introduction and orientation
Welcome address Introduction of partlclpants and secretariat Hiatory and background of the workshop Objective. of the workshop Review of agenda and atructure of workshop
ANNEX 2
2 Presentation of results of .ssessment of national health information systems (HHIS)
The framework for the assessment Country visi ts Highlights of findings Diacussion of findings
3 Presentation of country reports
Recent developments in each country's national health information systems Problems and/or constraints in development Future plans Discussion of country reports
4 Presentation of a "model" national health information system
Conceptual framework Guiding principles Component structure Specifications Health indicator development
5 Towards the model NHIS
The core sys tem The support structure Implementation of the model
6 Work groups I, II, III - Discussion of the Core System
7 Work groups by country - Development of Plan: The Core System
8 Plenary: General discussion of core issues, problems and approaches
9 Work groups I, II, III - Discussion of the Support Structure
10 Work groups by country - Development of Plan: The Support Structure
11 Plenary: General discussion of the support structure issues, problems and approaches
12 Work groups by country - Development of Plan: Implementation
13 Development plans presented by country
14 Closing ceremony and Adoption of group reports
- 49 -
ANNEX 3
PROGRAMME OF ACTIVITIES
A. Manila, 23-27 September 1985
Monday, 23 September
A.M. 0830-0900
0900-1000
1000-1030
1030-1200 1
NOON 1200-1400
P.M. 1400-1530 2
1530-1600
1600-1700
Tuesday, 24 September
A.M. 0830-1000 3
Registration - Conference Room A-208/209 Second Floor, Annex Bldg.
Opening ceremony (Moderator: Dr J.M. Robey)
WelCOme Address by the Regional Director Introduction of Participants and Secretariat
COFFEE BREAK AND GROUP PICTURE-TAKING
Introduction and orientation (Presentor: Dr J.M. Robey)
History and background of the workshop Objectives of the workshop Review of provisional agenda and structure of the workshop
LUNCH BREAK
Preaentation of results of assessment of national health information systems (MHIS) (Presentor: Dr O. Mendoza)
The framework for the asseSSment Country visits Highlights of findings Discussion of findings
COFFE! BREAK
Agenda item 2 continued
Presentation of country reports
Recent developments in each country's health information systems Problems and/or conetraints 1n development Future plans Discussion of country reports

- 50 -
Annex 3
Tuesday, 24 September (cont'd)
1000-10)0
10)0-1200
NOON 1200-1400
P.M. 1400-15)0 4
15)0-1600
1600-1700
Wednesday, 25 September
A.M. 0830-1000 5
1000-1030
1030-1200
NOON 1200-1400
P.M. 1400-1530 7
15)0-1600
1600-1700 8
Tnursday, 26 September
A.M. 0830-1000 9
1000-1030
CDFYEE 6REAl<.
Agenda item 3 continued
LUNCH BREAK
Presentation of a "model" national health intormation system (Presentor: Dr G. Fisner)
•
Conceptual framework Guiding principles Component structure Specifications Health indicator development
CDrrE! BREAK
Agenda item 4 continued
Towards the model NHIS (Presentor: Dr J.M. Rooey)
The core system The support structure Implementation of the model
CDPPEE aREAK
Work groups I, II, III - Discussion of the core system
LUNCH BREAK
Work groups by country - Development of plan: The core system
CDrFEE BREAK
Plenary: General discussion of core system issues, problems and approaches
Work groups I, II, III - Discussion of the support structure
CDrr!! BREAK

- 51 -
Annex 3
Tnureday, 26 September (cont'd)
1030-1200 10 Work groupe by country - Development of plan: The aupport structure
NOON 1200-1400 LUNCH BREAK
P.M. 1400-1530 11 Plenary: General diBcussion of the support structure i.aues, problems and approaches
1530-1600 OOFFEE BREAK
1600-1700 12 Work groups by country: Development of plan: Implementation
Friday, 27 September
A.M. 0830-1000 13 Development plans presented by country
1000-1030 OOFFEE BREAK
1030-1200 Agenda item 13 continued
NOON 1200-1400 LUNCH BREAK
P.M. 1400-1530 14 Closing ceremony and adoption of group reports
- 52 -
Annex 3
B. Suva, Fiji, 21-25 October 1985
Monday, 21 October
A.M. 0830-0900
0900-0945
0945-1030
1030-1100 1
1100-1200 2
MOON 1200-1400
P.M. 1400-1530
1530-1600
1600-1700 3
Registration
Opening ceremony (Moderator: Dr J.M. Robey)
~elcome Addres8 by Dr M. Fel~ser,
WIlO Representative and Programme Coordinator Message from Dr H. Nakajima, Regional Director, ~orld Health Organization Introduction of Participants and Secretariat
COFFEE BREAK AND GROUP PICTURE-TAKING
Introduction and orientation (Presentor: Dr J.M. Robey)
•
•
History and background of the workshop Objectives of the workshop Review of provisional agenda and structure of the workshop
Presentation of results of assessment of national health information systems (NHIS) (Preaentor: Dr O. Mendoza)
• The framework for the assessment Country visiu Highlights of findings Discu8sion of findings
LUNCH BREAK
Agenda Item 2 continued
COFFU BREAK
Presentation of country reports (Moderator: Mr P. Hedrick)
• Recent developments in each country's health information aystems Problems and/or constraints in development Future plana Discussion of country reports

Annex 3
Tueaday, 22 October
A.M.
NOON
P.M.
0830-1000
1000-1030
1030-1130
1130-1200
1200-1400
1400-1530
1530-1600
1600-1700
Wednesday, 23 October
A.M. 0830-1000
1000-1030
1030-1200
NOON 1200-1400
P.M. 1400-1530
1530-1600
1600-1730
4
5
6
8
9
- 53 -
Annex 3
Alenda Item 3 continued
OOFnE BREAK
Alenda item 3 continued
• Review of the family health information .yatem in Samoa
• PRe evaluation in Fiji: lnforaation aspects (Presentor: Hr P. Hedrick)
LUNCH B REAIt
Presentation of a "mOdel" national health information system (Presentorl Dr G. Fisher)
Conceptual framework Guiding principles Component structure Specifications Health indicator development
ooFFEE BREAK
Towards the model NHIS (Presentor: Dr J.M. Robey)
The core system
Alenda Item 6 continued The support system
ool'l'EE BREAK
Work groups I, 11, 111, IV - Discussion of the core system
LUNCH BREAK
Plenary: General discussion of the core and support systems - Issues, problems and approaches
ooFFEE BREAK
Work groups by country - Development of plans for the core system and the support structure

Annex 3
Thursday, 24 October
A.M. 0830-1000
1000-1030
1030-1200 10
11
NOON 1200-1400
P.M. 1400-1530 12
1530-1600
1600-1700
Friday, 25 October
A.M. 0830-1000 13
1000-1030
1030-1200
NOON 1200-1400
P.M. 1400-1530 14
- 54 -
Agenda Item 9 continued
OOFP'EE BREAK
Implementation of the model (Presentor: Dr J.M. Robey)
Role of the other agencies in NKIS development (Presentor: Representative of otber agencies>
LUNCK BREAK
Finalization of country reports
OOFFEE BREAK
Agenda Item 12 continued Submission of country worksheets and development plans
Development plans presented by country
OOFFEg BREAK
Agenda item 13 continued
LUNCH BREAK
Closin~ ceremony and adoption of group reports

- 55 -
ANNEX 4
REFERENCES
0) Diehr, P. "Small area atatistics: Large statistical problems", American journal of public health, Vol. 74, No.4 (April 1984)
(2) Rice, D. "Uniform mini .. m basic data sets: Their implications", Presented at the 7th International Congress on Medical Records Meeting, Canadian Association of Medical Record Librarians, Toronto, Canada (15 September 1976)
(3) Robey, J.M. and Anderson, J. "Developllent of a total health information syst_", Proceedings of the 107th Meeting of the American Public Health Association, New York, New York (November 1979)
(4) Wennberg, J. and Gittl •• ohn, A. "Small area variations in health care delivery". Science, 18:1102-1108 (1973)
(5) White, Kerr L. "A new look at health information", World health forua, 4:368-373 (1983)