writing with purpose - school of medicine | university of
TRANSCRIPT

Writing with purpose
Make IT real and simple
2017-2018
Omar S. Darwish, MS, DO Health Science Assistant Professor Coordinator of the M&M Dept of Med Hospitalist University of California, Irvine
On the Medicine Wards for Medical Students, Interns, and Residents

2
Objectives
• History and Physical Medicine Admission Note
• Progress Note
• Discharge Note
Department of Medicine

3
Objectives
(I) For the H/P notes…
• In the history section, focus your documentation on the elements of the complaint
• in addition to providing a comprehensive exam, also documenting pertinent positives and negatives in your exam
• providing a problem lists that reflects the active issues and the stability of the comorbidities and providing an “active” plan
Department of Medicine
4
Writing notes…
Tiresome, Monotonous, Boring
Time Consuming
No one reads it anyway
Gets in the way of patient care
Department of Medicine
Tell us how you really feel

5 Department of Medicine
Problem
Failure to Communicate Active Plans of the Day
Failure to Keep up with the Note
Failure to Reflect The Amount of Work Done
Barriers
High Turnover High Census Academic commitments and too
many necessary/unnecessary Interruptions
6 Department of Medicine
READ MY NOTES
I WANT TO SHOW OFF MY KNOWLEDGE & ACTIVITY
Change of attitude

7
History Section of the H/P and Progress Note
Department of Medicine
H&P Document (Comprehensive History)
• Focus on the Elements of the Chief Complaint
or the reason for admission. (Stop Writing the
List of Past Medical Problems)
• PMH Connection
• Are there prior Hospitalization
• 10 System ROS: A few needs to be
documented, but then the statement ”all other
systems are negative” needs to follow.
• PMH/Surgical History, Family History (CANNOT
WRITE NONCONTRIBUTORY), Social History
Progress Note (Detailed History)
• Daily assessment of how their chief complaint
is doing. Great place to ask the patient if they
are in pain (rate it, where is it, associated
symptoms) and are pain meds helping
• ROS: At least 2 are needed
Detailed Hx: 4 HPI elements or the status of 3 chronic medical problems + 2 ROS Comprehensive Hx: Same as above except + 10 ROS + Complete PFSH

8
EXAM Section of the H/P and Progress Note
Department of Medicine
H&P Document (Comprehensive Exam)
• 1 bullet from each of the organ systems (8 pts)
• Example: • Vitals: BP 120/80, HR 60, RR 23, T 98.6
General: NAD, alert and oriented x 3
Constitutional System
1 bullet for vital signs, 1 bullet for general appearance
Progress Note (Detailed Exam)
• 5 bullets from any organ system
Progress Note (Expanded Problem Focused Exam)
• 2-4 bullets from any organ system
Vital signs: 120/80, P 67, RR 18, T 38 (constitutional +1) Gen: NAD (psycho +1) and A&O x 3 (neuro + 1) Heart: RRR no m (cardio + 1) Lungs: CTAB (pulm + 1)

9
Imaging and EKG
Department of Medicine
Cutting and Pasting Imaging Findings & Impressions are Discouraged. Best thing to write is your interpretation, then if you are in agreement or question radiologist impression
Why? Clutters the progress notes & for Discharge Summaries abnormalities listed maybe become a LIABILITY
Example: CXR: my interpretation R large pleural effusion consistent with radiology impression
10 Department of Medicine
Assessment/Plans
• By far the most difficult section to write

11
Medical Decision Making (MDM)
Overall MDM Problem Points Data Points Risks
Straightforward 1 1 Minimal
Low 2 2 Low
Moderate 3 3 Moderate
High 4 4 High
Department of Medicine
For High MDM; Requires 2 out of the 3 of the following 1) Four Problem Points 2) Four Data Points 3) High Risk

12 Department of Medicine
Problem Points
Problems Points
Self-limited or minor 1
Established problem, stable or improving 1
Established problem, worsening 2
New problem, with no additional workup- planned 3
New problem, with additional workup planned 4
Example: 1. Atrial Fibrillation with RVR- etiology from HTN, hemodynamically stable, new diagnosis 2. Type 2 Diabetes with peripheral neuropathy – stable, at hospitalized blood sugar goal on Lantus 30 U/day and Neurontin 300 bid. 3. Hypertension with cardiac disease- controlled on Norvasc 5 mg qday 4. Moderate Risk for DVT on Lovenox 40 SQ day. Overall Plan/ For new Atrial Fibrillation, start Metoprolol 25 bid, check thyroid panel, obtain echocardiogram, start NOAC
6 pts
13
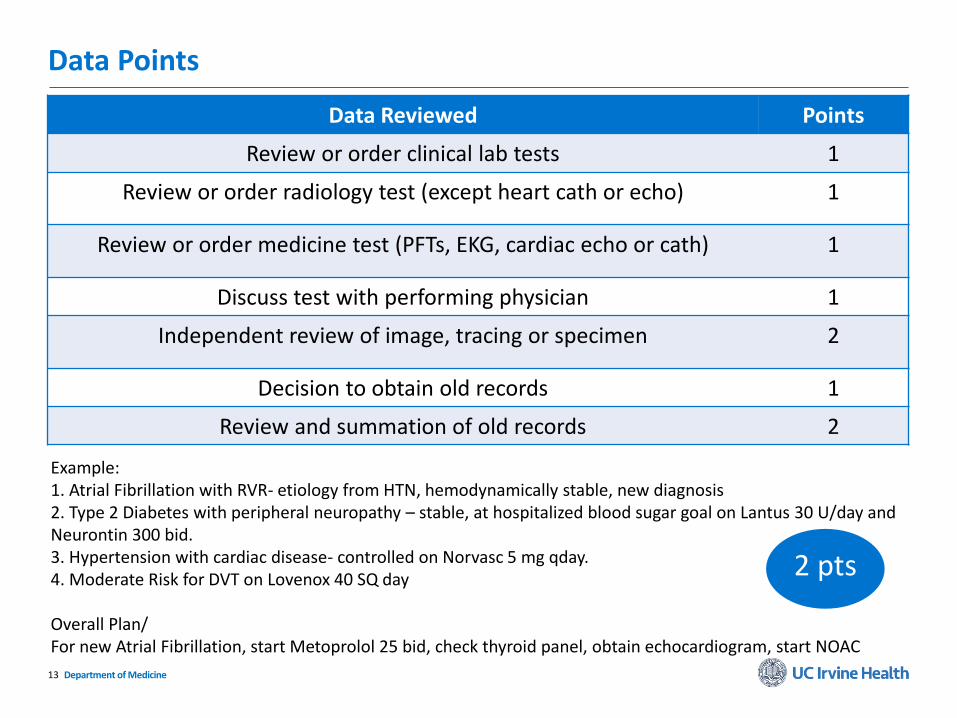
Data Points
Department of Medicine
Data Reviewed Points
Review or order clinical lab tests 1
Review or order radiology test (except heart cath or echo) 1
Review or order medicine test (PFTs, EKG, cardiac echo or cath) 1
Discuss test with performing physician 1
Independent review of image, tracing or specimen 2
Decision to obtain old records 1
Review and summation of old records 2
Example: 1. Atrial Fibrillation with RVR- etiology from HTN, hemodynamically stable, new diagnosis 2. Type 2 Diabetes with peripheral neuropathy – stable, at hospitalized blood sugar goal on Lantus 30 U/day and Neurontin 300 bid. 3. Hypertension with cardiac disease- controlled on Norvasc 5 mg qday. 4. Moderate Risk for DVT on Lovenox 40 SQ day Overall Plan/ For new Atrial Fibrillation, start Metoprolol 25 bid, check thyroid panel, obtain echocardiogram, start NOAC
2 pts

14
Risk: Requires ONE element in ANY of the following three categories
1. Type of Presenting Problem (MODERATE: e.g. mild COPD exacerbation; HIGH: acute hypoxic hypercapnic respiratory failure due to COPD)
2. Type of Diagnostic Procedure (MODERATE: EGD without risk factors; HIGH: EGD with risk factors)
3. Type of Management Options (MODERATE: Prescriptions; HIGH: Prescriptions requiring close monitoring
Department of Medicine

15
So How Should We Write the Note?
• An integrated problem lists with or without a line plan
• Adding a Discussion paragraph maybe needed to explain a complicated case
• Ending with an overall plan that shows current activity for that day
Department of Medicine

16
Example 1: of a Note on Day 30
Department of Medicine

17
Example 1 of a Note Day 31
Department of Medicine

18
Example 1: Apply the New Way of Writing
Department of Medicine

19
Example 2
Department of Medicine
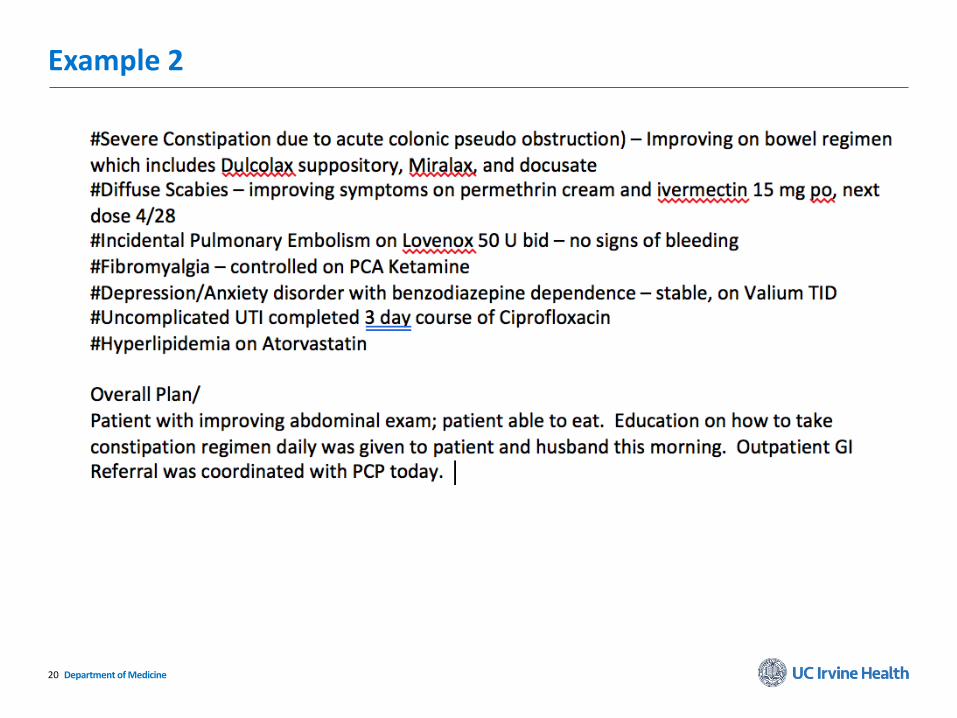
20
Example 2
Department of Medicine

21
Example 3. How To Apply from Day to Day
Department of Medicine

22
Do NOT Write
DM2 or DM
HTN
Anemia
Malnutrition
Hypokalemia
CHF
Cellulitis
Assessment of Common Medical Conditions (Degree, Complications). Be Specific (Location Matters)
Please Write (e.g.)
Type 2 diabetes with peripheral neuropathy
Hypertension with heart disease and CKD stage III
Microcytic Anemia with blood loss
Severe Protein Calorie Malnutrition (MCC*)
Severe Hyperkalemia due to urine loss
Acute on Chronic Systolic Heart Failure (MCC*)
R foot cellulitis
Department of Medicine
*MCC: Major complication or comorbidity; others include Acute Renal Failure, Acute Respiratory Failure, Acute CHF, hyponatremia, functional quadriplegia Protein Calorie Malnutrition

23
Use Non-Definitive Words
• Apply words like Presumed, Probable, or Possible when treating conditions you are not sure about.
• Example: Presumed Gram negative and MRSA Pneumonia – on Vancomycin and Zosyn. The following day you could say Pneumonia Ruled Out – stop antibiotics
Department of Medicine

24
Choose the Diagnosis that Best Reflects Severity
A. Cellulitis
B. Sepsis
C. Septic Shock
Department of Medicine
Answer: Sepsis Sepsis due Cellulitis
25
Choose the Diagnosis that Best Reflects Severity
A. Pneumonia
B. Severe Sepsis
C. Acute Hypoxic Respiratory Failure
Department of Medicine
Answer: Acute Hypoxic Respiratory Failure due to Severe Sepsis from presumed Gram Neg. Pneumonia

26
Choose the Diagnosis that Best Reflects Severity
A. Diabetes
B. Type 2 Diabetes
C. Type 2 Diabetes with peripheral neuropathy
D. Type 2 Diabetes with CKD stage III and peripheral neuropathy, retinopathy, and history of R toe amputation
Department of Medicine
Answer: D Make connections

27 Department of Medicine
READ MY NOTES
I WANT TO SHOW OFF MY KNOWLEDGE & ACTIVITY
Change of attitude

28 Department of Medicine
Assessment/Plans
• Reflect your knowledge • Reflect your activity for that day • Overall show that you are committed in
providing the best care