www.ias2011.org long term side effects of art in africa: third millenium dr cissy kityo mutuluuza...
TRANSCRIPT

www.ias2011.org
Long Term Side Effects of ART in Africa: Third Millenium
Dr Cissy Kityo Mutuluuza
Joint Clinical Research Centre
IAS Conference 17-20 July 2011- Rome, Italy

www.ias2011.org
Number of people receiving ART in low and middle income countries by region 2002–2009
5,25 million on ART by end of 2009 30% rise from end of 2008
13 fold increase in six years
5,25 million on ART by end of 2009 30% rise from end of 2008
13 fold increase in six years
Source: WHO, 2010

www.ias2011.org
"Treatment 2.0": Re-energizing the Public Health Approach to ART
TREATMENT2.0
Strengthen delivery systems
Mobilize communities
Provide point of care diagnostics
Optimize drug
regimens
Reduce costs
TREATMENT2.0
Strengthen delivery systems
Mobilize communities
Provide point of care diagnostics
Optimize drug
regimens
Reduce costs
www.ias2011.org
Benefits of ART
A. voluntary testing/counselingB. awareness of HIVC. motivation of health care workersD. expenses for palliative and OI careE. number of orphansF. Keeps households and businesses intactG. access to health facilitiesH. Potential to enhance prevention
a. Behavioral: access to prevention education during care encounters
b. Biological: decreased transmission due to lowered viral load

www.ias2011.org
Impact of ART on mortality in
Impact of ART on mortality in
Northwest Province, South Africa
Northwest Province, South Africa
Data source: Ministry of Health, South Africa
0
2000
4000
6000
8000
10000
12000
1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
dea
ths
0
5000
10000
15000
20000
25000
30000
35000
40000
Eve
r o
n A
RT
cum on
ART15-24
25-34
35-44
45-54
65+
data sources: Stats SA: SA
MOH South Africa
Impact of ART on TB incidence in
Impact of ART on TB incidence in Botswana Botswana
0
100
200
300
400
500
600
700
1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
inci
den
ce/1
00,0
00
0
10000
20000
30000
40000
50000
60000
70000
80000
90000
100000
ARTTB
Sources: NASA data reported to WHO and UNAIDS by Ministry of Health, Botswana;
TB Program, Ministry of Health, Botswana
Impact of ART in Resource-Limited Settings

www.ias2011.org
Relative rate of MI according to PI exposure
D:A:D NEJM 2007
Adjusted RR* per year of PI: 1.16 [1.10-1.23]
None <1 1-2 2-3 3-4 4-5 5-6 >60.5
1
2
4
8
PI-exposure (yrs)
RR
(95
% C
I)
However, there are complications: no such a thing as a free lunch….

www.ias2011.org
Many organ systems are affected by ART
• Cardivascular system• Kidneys• Liver• Pancreas• Bone• Perpheral Nervous System• Muco-cutaneous membranes• Lypodystrophy• Lactiacidosis

www.ias2011.org
0.1 1 10
Are you better off with ART : Serious Non-AIDS Outcomes in SMART
No. of Patients with EventsEndpoints
Major CVD+, hepatic or renal disease 104 1.8 1.1CVD+ 79 1.3 0.8
Relative Risk (95% CI)
RateDC VS
Renal (ESRD) 11 0.2 0.1
1.4Hepatic (Cirrhosis) 17 0.3 0.2
1.4
4.5
1.7
NADM++ 47 0.8 0.5
1.8
1.6
Favors DC Favors VS
Other non-OD death 51 0.9 0.5
Any of the above 186 3.2 2.0
1.6
+ MI (clinical or silent), stroke, surgery for CAD++ Except non-melanoma skin
NEJM 2006; 355:22838-96

www.ias2011.org
SMART Results for START Endpoints
No. of Patients with EventsEndpoint
Serious AIDS 59 1.3 0.4
Favors VS ►
►
Favors DC
Hazard Ratio (DC/VS) (95% CI)Rate*
DC VS
3.6
1.9
Serious non-AIDS 186 3.2 2.01.6
* Per 100 person-years
Serious AIDS or 239 4.4 2.4non-AIDS
Curr Opin HIV AIDS 2008;3:112-117
0.1 1 10

www.ias2011.org
ART Treatment for AfricaWhere are we now?
• Priorities now:– Roll-out to rural areas, near health centres where
most people live– Integrate with other services– Strengthen systems
• WHO 2010 Guidelines?:– Alternative first-line ART (replacing stavudine)– Moving CD4 threshold for ART initiation up– Increased efficacy (CD4? Viral load?) monitoring

www.ias2011.org
Monitoring Long Term Side Effects• Few studies conducted to optimise long term ART
outcomes in adults and children
• Data from African ART programs and cohorts is mainly limited to initial short term utility of ART
• Data from Developed countries cannot always be extrapolated to Africa
• Factors in Africa that may affect long term effects of ART include:– Prevalence of co-infections is high– Nutritional status is poor– Use of herbal medicines is widespread– Treatment is started in advanced stage of disease

www.ias2011.org
The Development of AntiRetroviral Therapy in
Africa(DART) trial
Routine vs clinically driven laboratory monitoring of HIV antiretroviral therapy in Africa:
a randomised non-inferiority trial
(www.ctu.mrc.ac.uk/dart)
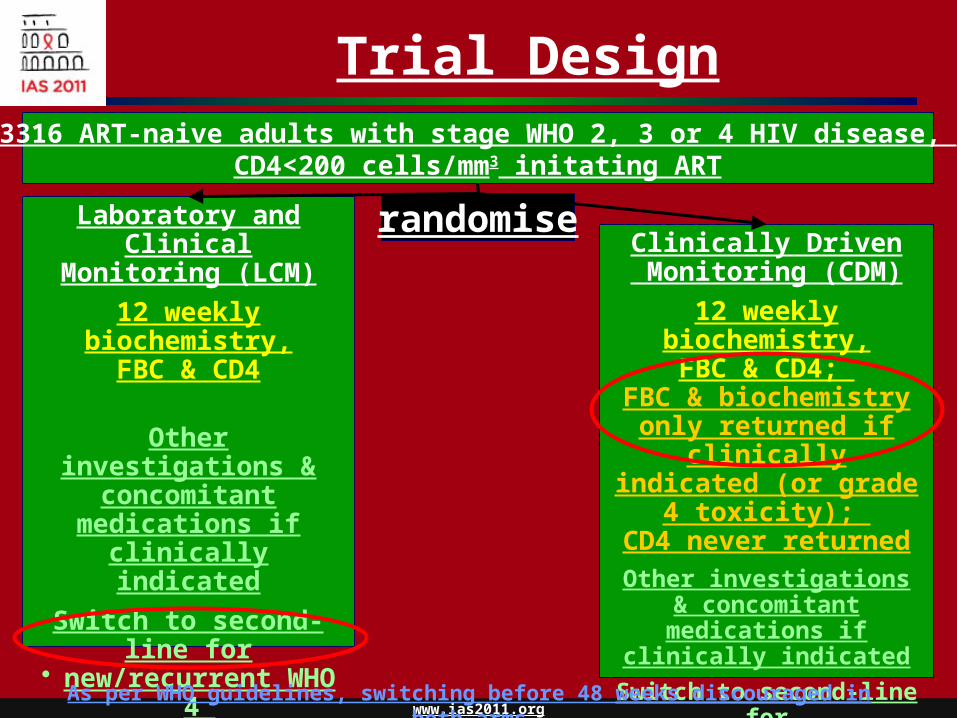
Trial Design3316 ART-naive adults with stage WHO 2, 3 or 4 HIV disease,
CD4<200 cells/mm3 initating ART
Laboratory and ClinicalMonitoring (LCM)
12 weekly biochemistry,FBC & CD4
Other investigations & concomitant
medications if clinically indicated
Switch to second-line for
• new/recurrent WHO 4 (or multiple WHO 3)
• CD4<100 cells/mm3
Clinically Driven Monitoring (CDM)
12 weekly biochemistry,FBC & CD4;
FBC & biochemistry only returned if clinically
indicated (or grade 4 toxicity);
CD4 never returnedOther investigations &
concomitant medications if clinically indicated
Switch to second-line for• new/recurrent WHO 4
(or multiple WHO 3)
randomise
As per WHO guidelines, switching before 48 weeks discouraged in both arms

Main objectives of DART
• To evaluate the need for routine laboratory monitoring of ART in African adults starting ART having fulfilled clinical and CD4 criteria for ART initiation
• To evaluate 12 week cycles of structured treatment interruptions (STIs) in patients with CD4 300 cells/mm3 at 48/72 weeks (stopped March 20061)
• Primary endpoints
– Efficacy: new WHO stage 4 HIV event (AIDS) or death
– Safety: any Serious Adverse Event which is not only HIV-related
• Cost-effectiveness analysis1 DART Trial Team AIDS 2008;22(2):237-47

www.ias2011.org
Toxicity monitoring
Routine laboratory monitoring for toxicity did not impact adverse events or substitutions in first-line
• Differences between arms are driven by HIV events
• More tests done in LCM
– routine monitoring does not prevent extra tests being requested
• Routine laboratory tests for toxicity were the most costly part of ART provision in DART
• Laboratories are still needed– eg screening; diagnosis and management of acute
illnesses

www.ias2011.org
0.0
0.2
0.4
0.6
0.8
1.0
Pro
po
rtio
n e
ve
nt-
fre
e
0 1 2 3 4 5
Years from randomisation (ART initiation)
LCM CDM
Grade 4 AEp=0.18
SAE p=0.20
ART-modifying AE
p=0.85
Adverse events
Grade 3/4 AEp=0.52

www.ias2011.org
Data on longer term toxicities of ART
• Needed to understand how to prevent, diagnose and manage these complications in order to provide optimal long-term care in Africa
• Use of existing good quality cohorts in Africa to obtain data
• Targeted lower intensity monitoring approaches – non-invasive portable techniques for measuring cardiac
and vascular function– Bioelectrical Impedance Analysis (BIA)– ? Role of immune activation markers (D Dimer, IL-6, CRP)

www.ias2011.org
Need to invest in ART Pharmacovigilance
• Long-term use of ARTon such a large scale, could potentially lead to a significant number of adverse drug reactions especially for highly-vulnerable groups like pregnant women and young children
• Few countries have an effectively functioning pharmacovigilance system for monitoring the appropriate use and collection of drug safety data.
• Establishing