www.pspbc.ca pain management module learning session 1
TRANSCRIPT
2
Agenda
1. Welcome/Introductions (15 mins)
2. What are we trying to accomplish? (45 mins)
• The Biopsychosocial Approach
• Patient Voice
3. The 7 Pain Tools (45 mins)
Break (15 mins)4. Case Study Application (60mins)
5. Wrap up (30 mins)
• Action Period Planning
• Session Assessment
3
Faculty/Presenter Disclosure
Faculty’s Name: Speaker’s Name
Relationship with commercial interest:
-Grants/Research Support: PharmaCorp ABC
-Speakers Bureau/Honoraria: XYZ Biopharmaceuticals Ltd
-Consulting Fees: MedX Group Inc.
-Other: Employee of XYZ Hospital Group
4
Disclosure of Commercial Support
This program has received financial support from [organization name] in the form
of [desribe support here – e.g. educational grant]
This program has received in-kind support from [organization name] in the form
of [describe the support here – e.g. logistical support]
Potential for conflicts(s) of interest:
-[Speaker/Faculty name] has received [payment/funding, etc.] from
[organization supporting this program AND/OR organization whose products are
being discussed in this program].
-[Supporting organization name] [developed/licenses/distributes/benefits from
the sale of, etc.] a product that will be discussed in this program. [Enter generic
and brand name here].
5
Mitigating Potential Bias
[Explain how potential sources of bias identified in slides 1 and 2 have been
mitigated].
Refer to “Quick Tips” document
6
The aim of this module is to improve the quality of patient care available in non-pain specialized physician practices for patients living with chronic pain. This will be measured by an increase in function, or reduced decline in function, as indicated by a change in the Brief Pain Inventory Scores.
Through this work we expect: The experiences of patients and their families to improve
through better management of chronic pain Improve physician experience through increased
confidence in identifying and managing patients with persistent pain
Reduced health care utilization costs to the system through optimal use of general and specialist services.
Aim
7
Describe a rationale for using a bio-psychosocial approach to assessing and managing pain
Identify the 10 Pain tools available through the EMR template
Select the appropriate tool(s) for addressing a pain scenario
Report increased confidence in supporting patients that experience chronic pain
Learning Objectives
8
The Heartsink Patient
The Situation
9
17-31% of Canadians report chronic pain (Canadian Pain coalition)
18% of Canadians suffer from severe chronic pain –more than diabetes or heart disease. (Chronic pain association of Canada)
Chronic pain prevalence is approximately 33% in those over 55 years old (Moulin et al)
38% of institutionalized seniors experience pain on a regular basis (Stats. Can. 2008)
The Situation
10
The single biggest cause of disability in Canada
It affects the elderly the most
The elderly are about to become the largest cohort of patients
The Situation
11
70% of cancer patients experience moderate to severe pain during their illness
The majority reported that they had not been asked about their pain by doctors or nurses (Chronic pain association of Canada)
The Situation
12
Chronic pain is a strong independent predictor of health resource use
“There was a strong association between pain-related disability and greater use of services” (Blyth et al. Pain 2004)
The Situation
13
The cost of pain to the Canadian economy is estimated at $6 Billion annually (Jovey)
Pain is almost unmentioned in medical schools (Chronic pain association of Canada)
“Funding for research, training and treatment of pain in Canada is woefully inadequate” (Jovey)
The Situation
14
CHRONIC PAIN IS AN EPIDEMIC THAT AFFECTS UP TO A THIRD OF ALL
CANADIANS
WE ARE NOT ASKING ABOUT IT
WE DON’T KNOW HOW TO TREAT IT
15
People with chronic pain have a three times the average risk of developing psychiatric symptoms, mainly depression
Depressed people have three times the average risk of developing chronic pain
Nearly all medications for depression also help reduce chronic pain (Harvard Health Publications 2004)
Chronic Pain and Depression
16
Women with chronic pain are three times more likely to commit suicide than matches in the general population without chronic pain (Fishbain et al)
Chronic Pain and Suicide
CHRONIC PAIN IS A DISEASE THAT WILL
LARGELY BE TREATED BY FAMILY DOCTORS
18
Denial
Lack of time
Lack of resources
Lack of knowledge
Lack of effective “cures”
Not wanting to open a “Pandora's Box”
Barriers for GPs
19
So what do I do with my chronic pain patients?
20
Shift paradigm:
Sole pursuit of tissue pathology…
….to reasonable attempt to exclude pathology and reach diagnosis.
What are we trying to accomplish?
21
Shift paradigm:
Sole pursuit of pain reduction…
….to whole person centered approach aiming at functional gain and pain reduction.
What are we trying to accomplish?
22
Shift paradigm
“There’s nothing that I can do”…
….to “we can together work as a team to reduce the alarm (pain) in your nervous system and increase your function.”
What are we trying to accomplish?
freedigitalimages.net
23
Shift paradigm
“I only have one tool (prescriptions)”…
….to “there are a toolbox of options we can use to help reduce your pain and increase your function.”
What are we trying to accomplish?
24
Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.
- International Association for the Study of Pain(1979)
What is Pain?
25
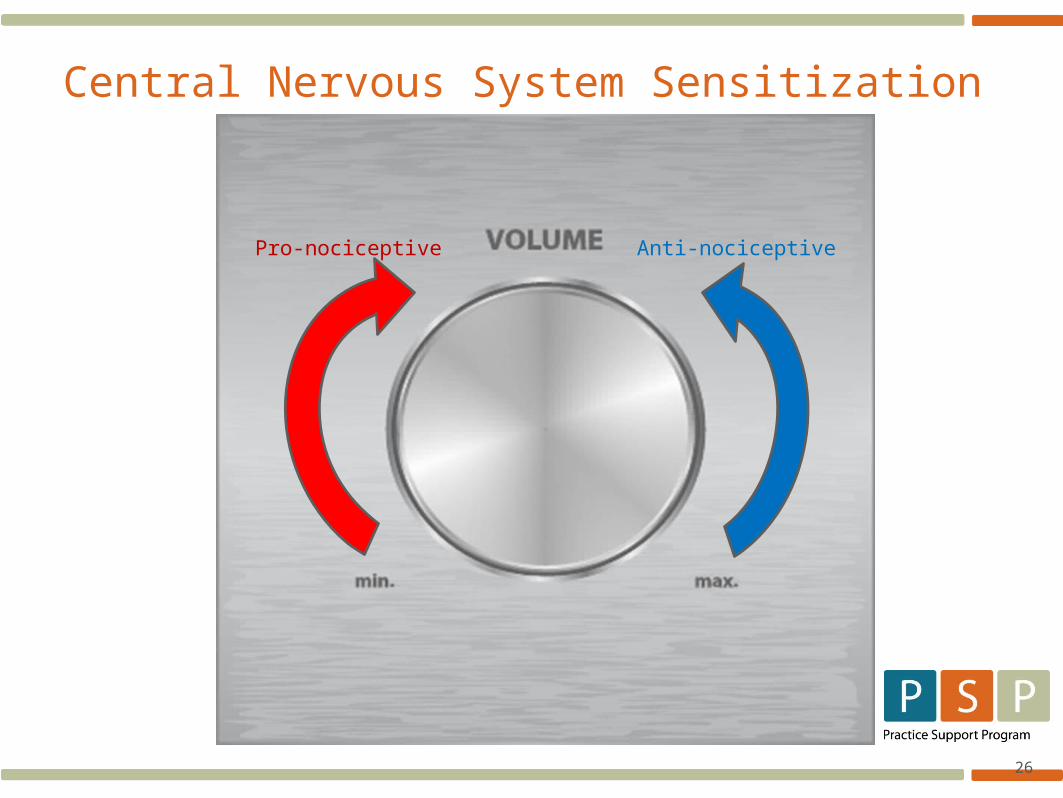
26
Central Nervous System Sensitization
Pro-nociceptive Anti-nociceptive
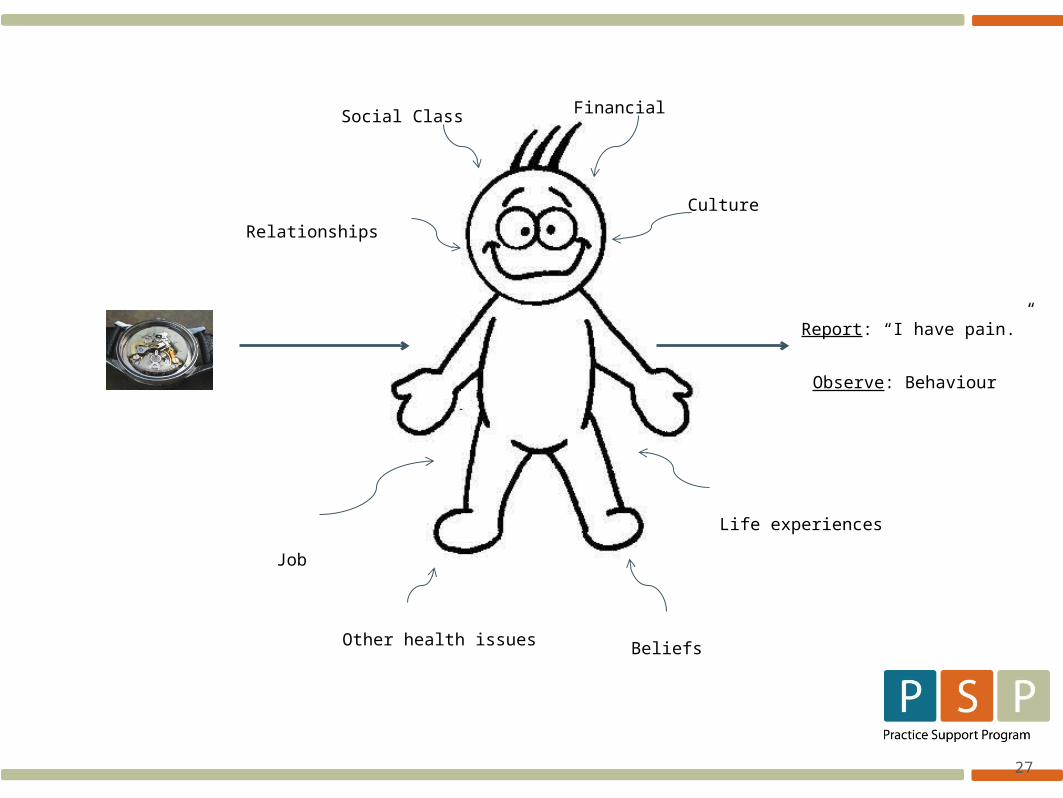
27
Social Class Financial
Relationships
Job
Culture
Beliefs
Life experiences
Other health issues
Report: “I have pain.”
Observe: Behaviour
28
Pain in not a “thing”
Pain is not in the tissues
No pain receptors No pain pathways No pain centres
It’s a multidimensional, lived, experience constructed by the brain.
What is Pain?
29
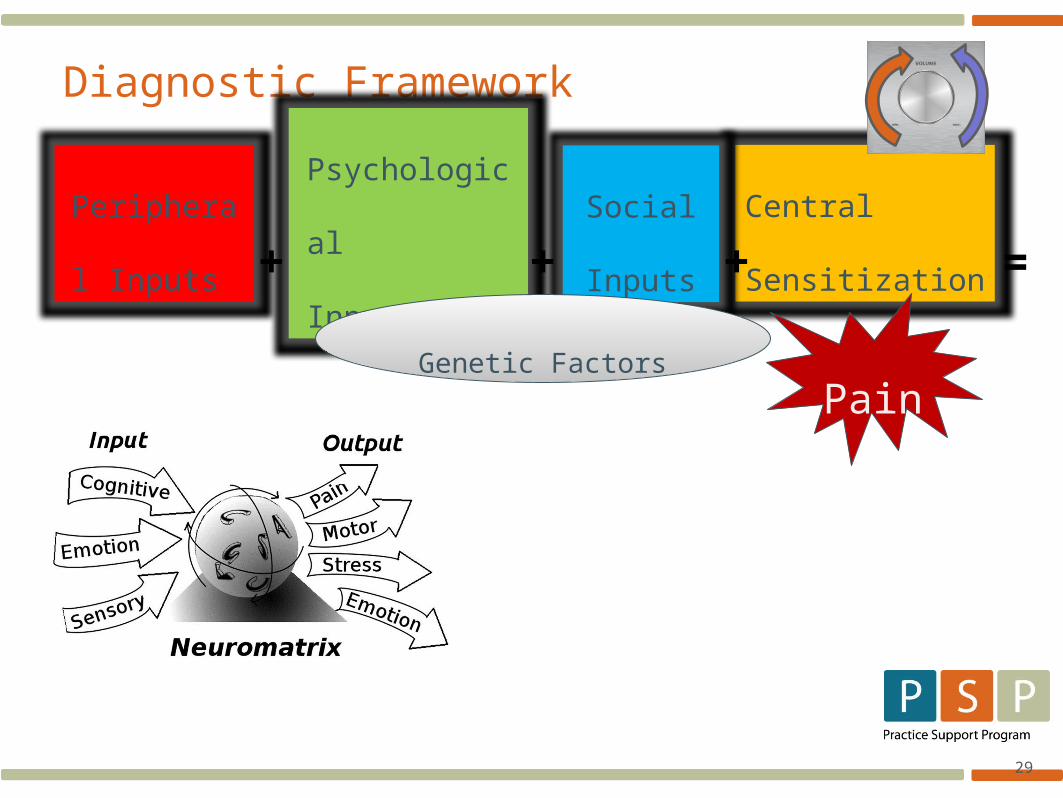
Diagnostic Framework
Peripheral
Inputs
Central
Sensitization
Psychological
Inputs
Social
Inputs+ + + =
PainGenetic Factors
30
Ac
tiv
ity
• Gen
tle
• Prog
ressi
ve
• Paci
ng
• Goa
ls
Mo
od
• Coa
chin
g
• Bou
nce
Bac
k
• Copi
ng
• Resi
lien
ce
Sl
ee
p
• Slee
p
hygi
ene
• Aids
• Med
icati
on
Toolbox of Supports
31
Mi
nd
ful
ne
ss
• Med
itati
on
• Yog
a
• Tai
Chi
• Bre
athi
ng
Me
dic
ati
on
s
• TCA
s
• Anti
-
con
vuls
ants
• Opi
oids
• Oth
er…
Int
er
ve
nti
on
s
• Inje
ctio
ns
• Sur
gery
• Man
ipul
atio
n
Toolbox of Supports
32
Kn
ow
le
dg
e
• Pain
• Bod
y
• Self
awa
rene
ss
• Con
cept
s
Su
pp
ort
• Fam
ily
• Frie
nds
• Wor
k
• SM
gro
ups
• Sup
port
gro
ups
Ps
yc
ho
lo
gy
• CBT
• ACT
• BAP
• Coa
chin
g
• Gro
up
Med
ical
Visit
s
Toolbox of Supports