yellow fever training programme - microsoft · yellow fever is currently the only disease for which...
TRANSCRIPT

Yellow Fever Training Programme.
Training for Registered Yellow Fever Vaccination Centres in ScotlandHealth Protection Scotland and NHS Education for Scotland
April 2019
Click anywhere to continue

WelcomeWelcome to the yellow fever training programme produced by Health Protection Scotland (HPS) and NHS Education for Scotland (NES).
The programme is aimed at healthcare practitioners who work within registered Yellow Fever Vaccination Centres (YFVCs) in Scotland. Practitioners who work within YFVCs in Scotland, should be fully aware of all aspects of Designation status which can be found in the HPS Designation Information Pack.
This learning programme may be undertaken to fulfil the biennial update training requirement of Scottish YFVCs. Practitioners undertaking the training for this purpose must complete the entire programme and submit the Confirmation of Completion Form to HPS. This will ensure that your training record is updated on the HPS YFVC database.
You will be promted to go to the Confirmation of Completion Form at the end of the programme.
The programme will be of interest to other practitioners wishing to update their knowledge of yellow fever. Completion of the Confirmation of Completion Form is not necessary for such individuals.
Practitioners undertaking training as a newly registered YFVC, should attend the HPS face-to-face training in the first instance. Details of the face-to-face training for new centres are available on the Yellow fever vaccination centres registration and training requirements page on the HPS website.

Programme summaryThe training programme focuses on the subject of yellow fever and does not cover other aspects of travel health in any depth. Individuals providing yellow fever services should be competent in conducting a travel health risk assessment and should undertake general travel health training. Participants should consult RCN Travel Health Competencies1 in this respect.
The programme takes approximately 1.5 hours to complete, depending on individual learning needs. Participants need not complete the programme in one session, and can opt to stop and save their work at any time, allowing the individual to dip in and out of the programme.
Please click on on the ‘Save programme’ button to save the programme as and when required.
When using Adobe Reader® or Adobe Acrobat® to complete the programme users can enable the application to open documents at the last page viewed. Instructions how to enable this function can be found on the next page.
Please note: this function may not be possible if completing the programme in other PDF viewers e.g. Preview on Apple Mac.
1 RCN. Travel health nursing: career and competence development. RCN guidance, 2018. Available at: https://www.rcn.org.uk/professional-development/publications.
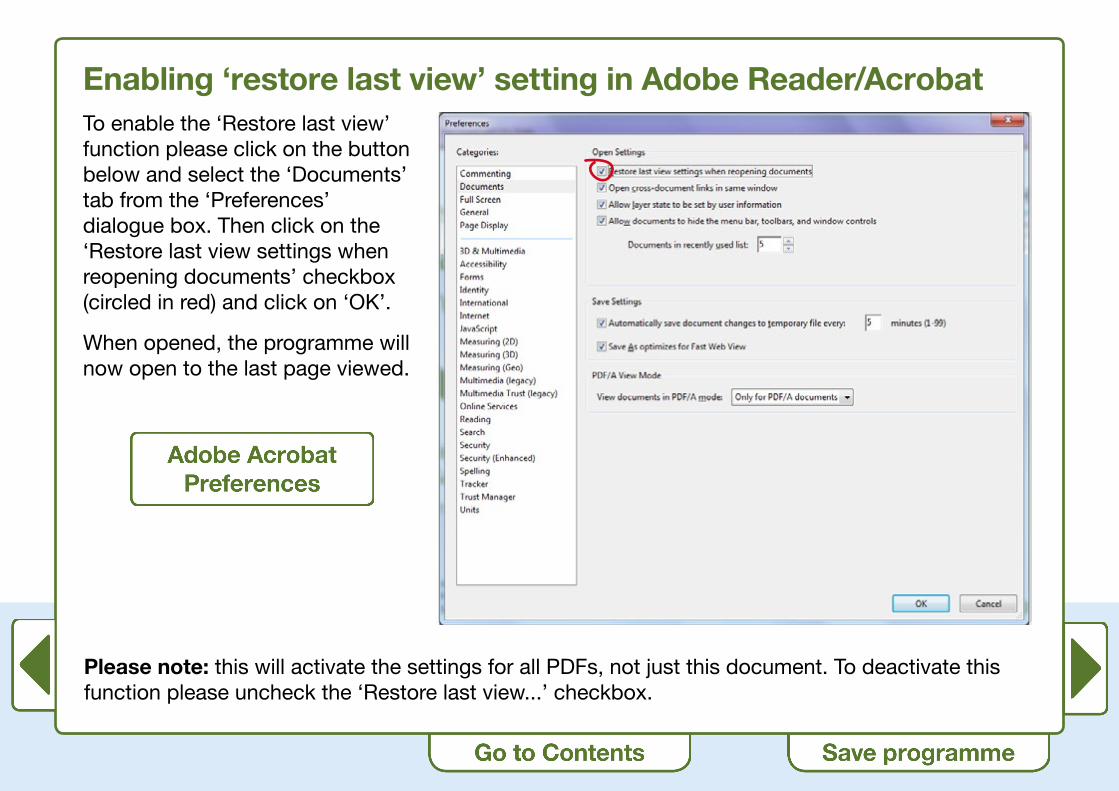
Enabling ‘restore last view’ setting in Adobe Reader/AcrobatTo enable the ‘Restore last view’ function please click on the button below and select the ‘Documents’ tab from the ‘Preferences’ dialogue box. Then click on the ‘Restore last view settings when reopening documents’ checkbox (circled in red) and click on ‘OK’.
When opened, the programme will now open to the last page viewed.
Please note: this will activate the settings for all PDFs, not just this document. To deactivate this function please uncheck the ‘Restore last view...’ checkbox.

ContentsThe programme has three parts. If this is the first time you have undertaken the programme, we recommend that you complete the three parts in order.
Part 1: Introduction to yellow fever
Part 2: Yellow fever – the disease and vaccine
Part 3: Administrative issues for Yellow Fever Vaccination Centres
During the programme there are several interactive activities, including case studies, to enhance learning. The activities are not time consuming to complete.
Continue to the next page for the programme Learning Outcomes.

Learning outcomesAt the end of the programme, participants should:
1. Describe the role of Health Protection Scotland (HPS) with regard to Yellow Fever Vaccination Centres (YFVCs) in Scotland
2. Know how to find information on the HPS website
3. Understand yellow fever in relation to:
• The disease
• The vaccine
• International Certificates of Vaccination or Prophylaxis (ICVP)
4. Be able to identify travellers who:
• Are at risk of yellow fever
• Require a yellow fever ICVP
• Should be issued with a yellow fever exemption certificate
5. Be able to undertake administrative issues relevant to YFVCs, including legal aspects and accountability
6. Understand the Conditions of Registration for YFVCs
7. Know when and where to seek specialist advice

Part 1.
Introduction to yellow feverAt the end of this section, participants should:
• Describe the role of Health Protection Scotland (HPS) with regard to Yellow Fever Vaccination Centres (YFVCs) in Scotland
• Know how to find information on the HPS website
Click anywhere to continue

International Health Regulations and administration of yellow fever vaccineThe administration of yellow fever vaccine is regulated by the World Health Organization (WHO) International Health Regulations (IHR).
The aim of the IHR is to help prevent the international spread of disease. When originally established in 1969, the IHR were primarily intended to monitor diseases like smallpox, cholera, plague and yellow fever. However, the revised IHR2 have a broader scope and encompasses new and re-emerging disease threats like SARS and pandemic influenza, as well as non-infectious diseases which have potential international health concerns.
Yellow fever is currently the only disease for which vaccination may be required under IHR and is the reason why an International Certificate of Vaccination or Prophylaxis may be requested from individuals entering certain countries.
Under the IHR, yellow fever vaccine can only be administered at centres that have Yellow Fever Vaccination Centre designation status.
2 World Health Assembly. Revision of International Health Regulations WHA 58:3. Fifty-eighth World Health Assembly. 23 May 2005. Annex 6 and 7.

The role of HPS in designating yellow fever vaccination centresHPS is a centre of excellence in the provision of travel health advice and services including the TRAVAX website which provides travel health advice for healthcare practitioners (further information to follow) and fitfortravel website which provides travel health information for the general public. The International Travel and Health team at HPS is therefore well placed to oversee the yellow fever centre programme in Scotland. In December 2006, responsibility for designating centres in Scotland was passed from the Scottish Government Health Directorate to HPS under the National Health Service Amendment Order.
In order to become, and to remain a YFVC, certain criteria and conditions must be met. These criteria and conditions are clearly set out in the Conditions of Registration for YFVCs. The full Conditions of Registration can be found in the Designation of Yellow Fever Vaccination Centres Information pack. These conditions will be explained more fully during this training programme.
HPS has a statutory responsibility on behalf of the Scottish Government, to ensure that designated YFVCs continue to meet conditions of registration, and HPS has the authority to de-designate a YFVC that does not comply with those conditions.

The conditions of registration for YFVCsThe Conditions of Registration for YFVCs will be considered more fully in Parts 2 and 3 of this learning programme. In summary the conditions are as follows:
1. A centre will administer only yellow fever vaccines approved by WHO.
2. All yellow fever vaccinations will be performed by a responsible medical practitioner, or by a suitably qualified person (doctor, nurse, pharmacist) acting under his/her control.
3. Facilities for ordering and storing vaccines will be of an acceptable standard.
4. Appropriate policies for safe administration of yellow fever vaccine will be in place, and all staff involved in administration of vaccine be appropriately trained. Such knowledge and training must include: risk assessment for travel; requirements for vaccination as a condition for entry to a country; the safe administration of yellow fever vaccine; yellow fever disease prevention measures; potential vaccine-associated adverse events.
5. The centre will comply with staff training as required by HPS.
6. The centre will keep appropriate records of all vaccinations administered. Records will be maintained for 10 years.
7. International Certificates of Vaccination or Prophylaxis (ICVP) against yellow fever will be completed and signed by the vaccinator in accordance with IHR.

The conditions of registration for YFVCs (continued)8. Vaccine associated adverse events will be reported to the Medicines and Healthcare Products
Regulatory Agency (MHRA) via the yellow card reporting system.
9. Annual returns of vaccine utilisation will be returned to HPS on the Annual Returns form provided.
10. HPS will be notified immediately of any changes which may affect the centre’s registration status.
11. If requested HPS will be given access to the centre or receive copies of YFVC records to ensure the centre is complying with the conditions of registration.
12. The centre’s status will be reviewed biennially.

Information for YFVCsAll information required by YFVCs can be accessed directly from the HPS website. Information includes: necessary documentation for YFVC registration and training, links to useful resources, and relevant contact details at HPS.
Activity
Go into the HPS website and access the section for Yellow Fever Vaccination Centres.
Ensure that you can find all of the information on the check list on the right. Use the check boxes to tick off the infomation as you find it.
How to register as a new YFVC
Other resources for YFVCs
How to order YF ICVPs
Training requirements for YFVCs
How to make payments
How to locate the nearest YFVC
Contact details at HPS for any aspect of YFVC registration.

Information for YFVCsFor clinical and country-specific information relating to yellow fever, we recommend that, where possible, practitioners use TRAVAX.
TRAVAX is available free of charge within the NHS in Scotland and you can register online. If you do not work within the NHS, or if you use another information resource, it is essential that it is up-to-date and reliable.
Provision of yellow fever vaccine is only part of the provision of Travel Medicine services. Healthcare practitioners who provide yellow fever vaccine should be aware of the wider issues around Travel Health including carrying out a comprehensive risk assessment, provision of other vaccinations, general travel health advice and malaria advice. If you have not already done so, you should refer to the RCN Travel Health Competencies3 previously mentioned. The RCN competencies, though written primarily for nurses, are also useful for other healthcare practitioners.
An additional resource for healthcare practitioners is ‘Protecting the health of travellers from UK and Ireland’ from the Royal College of Physicians and Surgeons Glasgow.4
3 RCN. Travel health nursing: career and competence development. RCN guidance, 2018. Available at: https://www.rcn.org.uk/professional-development/publications.
4 Faculty of Travel Medicine Executive Board, RCPSG. Position paper: Protecting the health of travellers from UK and Ireland. 2014. Available at: https://rcpsg.ac.uk/documents/agm-and-elections/ftm/255-health-of-travellers/file. [Accessed July 2018]

Summary: Part 1Introduction to yellow feverThis concludes Part 1 of the training programme about the role of HPS in YFVC designation and making use of the HPS website.
Please continue on to Part 2.
Part 2.
Yellow fever – the disease and vaccineAt the end of this section participants should:
• Understand yellow fever in relation to:
- The disease
- The vaccine
- International Certificates of Vaccination or Prophylaxis (ICVP)
• Be able to identify travellers who:
- Are at risk of yellow fever
- Need a yellow fever ICVP
- Should be issued a yellow fever exemption certificate
Click anywhere to continue

What is yellow fever?Yellow fever is a zoonotic flavivirus infection.
Terminology
• Zoonosis – any infectious disease that can be transmitted from animals to humans.
• Flavivirus – a family of viruses that can be transmitted by mosquitoes and/or ticks.
In simple terms, yellow fever is a viral infection, harboured in monkeys and spread by mosquitoes.
These key facts are relevant when learning about the epidemiology of yellow fever and when considering ways to prevent disease transmission.

Transmission of yellow fever Yellow fever is transmitted from monkeys and humans to other monkeys and humans principally by the Aedes Aegypti mosquito.
The Aedes Aegypti mosquito is synonymous with the disease and is sometimes called the yellow fever mosquito. However, several other species of Aedes also transmit the yellow fever virus.
This mosquito bites predominantly during the day, which is important when considering preventive measures.

Yellow fever transmission cyclesThere are three yellow fever transmission cycles:
• Jungle (or sylvatic) yellow fever – found in both Africa and South America
• Intermediate yellow fever – found in Africa only
• Urban yellow fever – found in both Africa and South America

Jungle (or sylvatic) yellow feverIn this cycle, transmission occurs mainly between mosquitoes and monkeys in jungle/rural areas. Transmission to humans occurs when a human inhabits this environment e.g. for the purposes of work (such as loggers) or for adventure travel.
► Start
An infected mosquitoes (Aedes Aegypti) bites a monkey in the jungle.
Other mosquitoes bite the infected monkey and become infected themselves.
These mosquitoes then transmit infection to other monkeys or humans who visit the jungle.
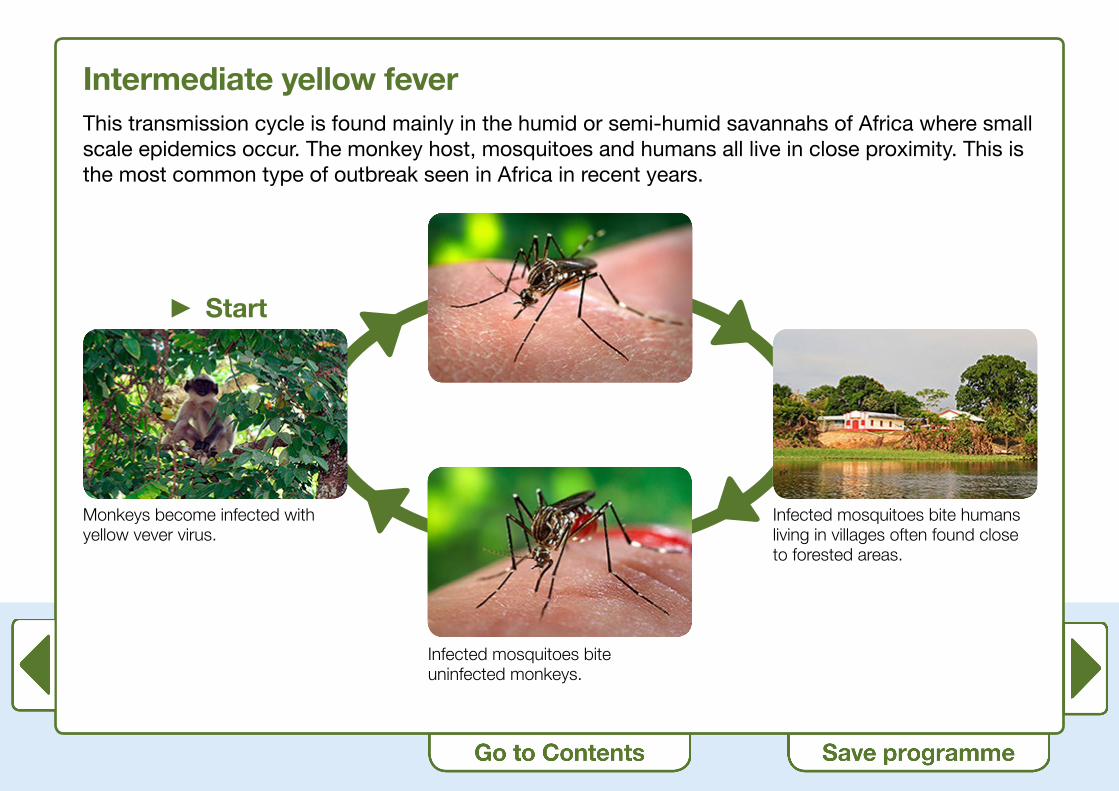
Intermediate yellow feverThis transmission cycle is found mainly in the humid or semi-humid savannahs of Africa where small scale epidemics occur. The monkey host, mosquitoes and humans all live in close proximity. This is the most common type of outbreak seen in Africa in recent years.
► Start
Monkeys become infected with yellow vever virus.
Infected mosquitoes bite humans living in villages often found close to forested areas.
Infected mosquitoes bite uninfected monkeys.
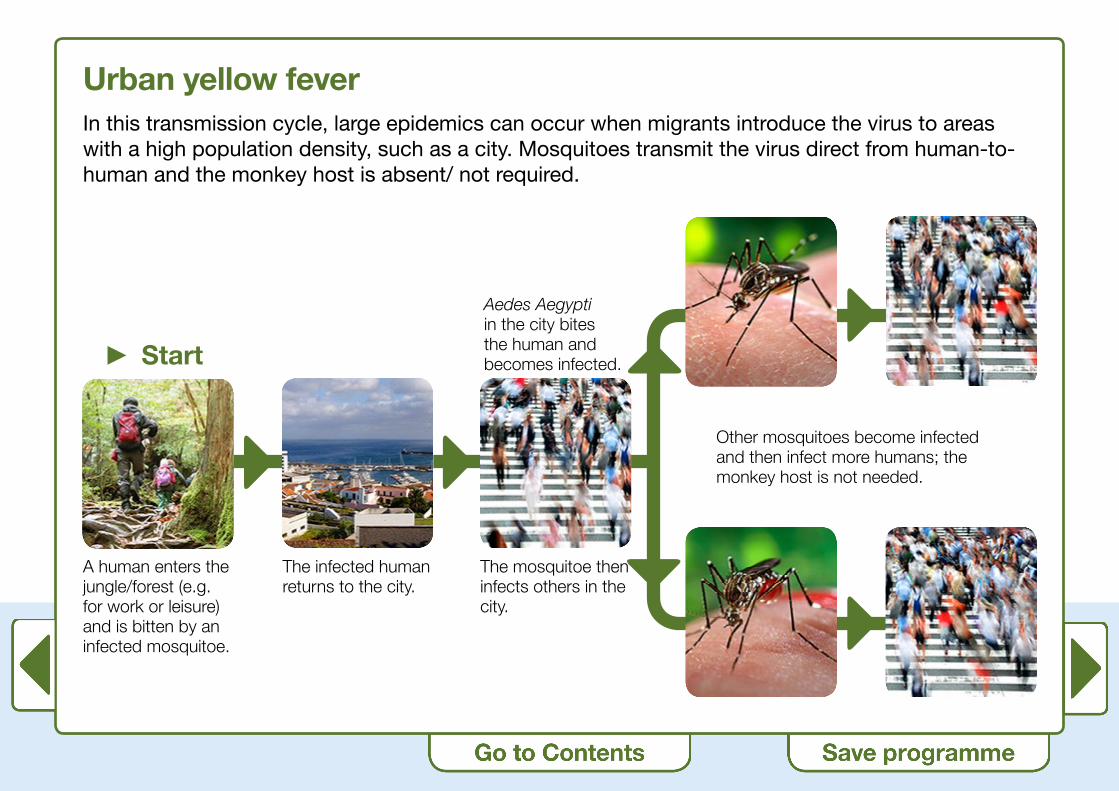
Urban yellow feverIn this transmission cycle, large epidemics can occur when migrants introduce the virus to areas with a high population density, such as a city. Mosquitoes transmit the virus direct from human-to-human and the monkey host is absent/ not required.
► Start
A human enters the jungle/forest (e.g. for work or leisure) and is bitten by an infected mosquitoe.
The infected human returns to the city.
Aedes Aegypti in the city bites the human and becomes infected.
The mosquitoe then infects others in the city.
Other mosquitoes become infected and then infect more humans; the monkey host is not needed.

Yellow fever – clinical presentation • The incubation period for yellow fever infection is 3-6 days.
• Most individuals infected with yellow fever virus will be asymptomatic. They will then go on to develop lifelong immunity to the virus.
• Of those who develop symptoms, most will develop a non-specific, ‘flu-like’ illness with fever, headache, chills, backache, malaise, general muscle pain, weakness and nausea.
• These individuals will improve after initial presentation.

Yellow fever – clinical presentation • 15% of those experiencing symptoms will go on to develop the more severe form of the disease
and may demonstrate symptoms including:
- Jaundice (hence yellow fever)
- Liver failure
- Haemorrhagic symptoms (such as petechia, epistaxis, melena, haematemesis)
- Shock
- Complications including secondary bacterial infections and kidney failure
- Multi system organ failure
• The case fatality for those with more severe disease is 20-50%
• Those who recover may experience fatigue and weakness for several months and full recovery may be protracted.

Diagnosis and treatmentDiagnosis is principally through clinical examination. Serological confirmation is possible but may not always be practical in areas where resources are limited.
There is no specific treatment, and therefore is supportive only.
In areas where Aedes Aegypti (the mosquito vector) is present, patients should be nursed in a mosquito screened environment (e.g. with nets), to prevent secondary disease transmission.

The history of yellow feverYellow fever virus originated in Africa around 3000 years ago. The virus and the vector were transferred from Africa to South America, probably by ship.
The first recorded epidemic occurred in Mexico in 1648. There followed many other major outbreaks in America:
• 1793: Philadelphia – 10 000 deaths
• 1853: Louisiana – 7800 deaths
• 1878: Mississippi river valley – 20 000 deaths
• 1878: Memphis – 5000 deaths
In 1882, the disease halted a French company’s attempt to build the Panama Canal due to the number of workers who succumbed to the disease.
In the early days, no-one knew how the disease was transmitted. It was not until 1881 that the mosquito was identified as the possible vector by the Cuban doctor, Carlos Finlay.
This theory was later confirmed by a group of army doctors, keen to determine the cause of the disease which was killing so many soldiers in the Spanish-American war. In 1900, Major Walter Reed demonstrated transmission of yellow fever virus from one individual to another through the bite of the Aedes Aegypti.
Click on the images below to view an enlarged version.

Epidemiology in the 21st centuryYellow fever occurs in Africa and the Americas.
It is estimated that there are approximately 300 000 cases and 20 000 deaths each year, mostly in sub-Saharan Africa. These figures are likely to be under-estimates.
In 2010 a WHO Working Group5 identified the following risk categories:• Endemic
• Transitional
• Low potential for exposure
• No risk
The working group also produced vaccine recommendation maps to aid practitioners. They identified the following 3 categories:
• Vaccination recommended (i.e. for endemic and transitional areas)
• Vaccination generally not recommended (i.e. for low potential for exposure areas, with some exceptions: such as prolonged travel, rural travel, extensive mosquito exposure)
• Vaccination not recommended (for no risk areas)
5 Jentes ES, Poumerol G, Gershman MD, Hill DR, Lemarchand J, Lewis RF, Staples JE, Tomori O, Wilder-Smith A, Monath TP; Informal WHO Working Group on Geographic Risk for Yellow Fever (2010). The revised global yellow fever risk map and recommendations for vaccination, 2010: consensus of the Informal WHO Working Group on Geographic Risk for Yellow Fever.

WHO yellow fever maps
Africa
Below is the WHO yellow fever map for Africa.6
Click on the map to view an enlarged version and the different risk areas and corresponding vaccine recommendation.
6 Centers for Disease Control and Prevention (CDC). Traveler’s Health; Yellow Fever, 2018. Available at: https://wwwnc.cdc.gov/travel/yellowbook/2018/infectious-diseases-related-to-travel/yellow-fever.
Americas
Below is the WHO yellow fever map for the Americas.6
Click on the map to view an enlarged version and the different risk areas and corresponding vaccine recommendation.

Prevention of yellow feverThere are three main ways to prevent the spread of yellow fever in humans:
1. Reduce the number of mosquitoes (Aedes Aegypti)
2. Prevent mosquito bites
3. Vaccinate

Prevention of yellow fever1. Reduce the number of mosquitoes
There are a number of ways to reduce the number of mosquitoes, such as:
• Large scale use of insecticides
• Techniques such as fogging
• Reducing mosquito breeding sites, such as, areas of stagnant water
• Use of bio methods in pools of water to reduce mosquito larvae
These interventions have been shown to have some impact in urban areas, but have much less impact in rural areas.
Click on the images below to see examples of insecticide spraying, fogging and example of mosquito breeding sites/stagnant water.

Prevention of yellow fever2. Prevent mosquito bites
There are a number of ways that an individual can prevent mosquito bites. Although the Aedes Aegypti mainly bites during the day, other mosquitoes bite at night, so preventive measures are advised at all times, where possible.
Measures that that have been shown to be effective include:
• Reducing skin exposure to mosquitoes by covering up with clothing, such as long-sleeved shirts and trousers and socks
• Using an effective insect repellent, such as one containing DEET, and following the product directions for application
• Where possible, sleeping in an air-conditioned environment where the numbers of mosquitoes is reduced (or ensuring sleeping quarters are well-screened where air-conditioning is not present)
• Sleeping under a an impregnated bed-net (mosquitoes are killed on impact with a pyrethroid impregnated net, so these are far more effective)
• Avoiding areas where mosquitoes breed, such as areas with stagnant water
Click on the images below to see examples of appropriate clothing, insect repellents, mosquito nets.
Prevention of yellow fever 3. Vaccinate
The yellow fever vaccine is highly immunogenic. WHO therefore consider vaccination to be the single most effective way to prevent yellow fever.
For indigenous populations of Africa and South America, vaccination is normally included as part of the routine national vaccination schedule for that country (although vaccine coverage will not always be 100%).
Vaccination is the most practical way to prevent jungle yellow fever where other interventions have limited success.
Large scale vaccination is the most effective way to prevent the spread of urban yellow fever during outbreaks.
Yellow fever vaccination for travellersYellow fever vaccination may be indicated for a traveller:
• Where the individual is at personal risk
• Where the individual requires a yellow fever International Certificate of Vaccination or Prophylaxis (ICVP)
• Both of the above
Healthcare practitioners advising travellers must undertake a thorough risk assessment so that they can identify those who need to be vaccinated and/or require an ICVP.
For clinical and country-specific information relating to yellow fever, we recommend that, where possible, practitioners use TRAVAX.
TRAVAX is available free of charge within the NHS in Scotland and you can register online. If you do not work within the NHS, or if you use another information resource, it is essential that it is up to date and reliable.
TRAVAX yellow fever advice is an interpretation of guidance including the WHO IHRs. Each country record gives a recommendation based on whether there is a yellow fever risk and vaccine recommendation and whether there is a yellow fever ICVP requirement.

What is the risk of yellow fever to travellers?A traveller’s risk for acquiring yellow fever is determined by various factors including:
• Location of travel – are they travelling to a risk area?
• Local rate of virus transmission at the time of travel – is there active disease transmission or is there an outbreak?
• Duration of exposure – the longer duration the higher potential for exposure.
• Occupational and recreational activities – the more time spent outdoors the higher potential for exposure.
• Immunisation status – is the individual already immune?
All of the above can be determined by carrying out a thorough risk assessment.7
7 RCN. Travel health nursing: career and competence development. RCN guidance, 2018. Available at: https://www.rcn.org.uk/professional-development/publications.
Risk of yellow fever to travellersFrom 1970-2010 there were 9 cases of yellow fever in unvaccinated travellers from the United States and Europe:
• 5 cases occurred in travellers to West Africa
• 4 cases occurred in travellers to South America
• 8 out of 9 of the cases were fatal
The vaccine is found to be highly effective and there has only ever been one documented case of yellow fever in a vaccinated traveller. This case (in a traveller from Spain who visited West Africa) turned out to be non-fatal.
While the local rate of transmission of yellow fever at a destination at the time of travel can be helpful to highlight areas of higher risk, the absence of disease at a destination does not mean that there is no risk of yellow fever.
This is because in areas where a high proportion of the local population is already vaccinated against yellow fever, human cases may be rare or absent. However, if the monkey host is present, there is the potential for transmission of the yellow fever virus from an infected monkey (via the mosquito) to an unvaccinated/non-immune individual.
Travellers going into such areas are therefore still advised to be vaccinated.

Case study 1The need for Yellow Fever Vaccine (YFV) and International Certificate of Vaccination or Prophylaxis (ICVP)
George is referred to your YFVC by a neighbouring GP practice for yellow fever vaccination.
He is travelling to Kenya.
► Question: What other risk assessment information do you require about George?
Use the ‘My Notes’ textbox to record any information required for a risk assessment for George.
At this point, we are only asking about George himself; we will ask about his trip later.
My Notes

Case study 1The need for YFV and ICVP
Risk assessment information about George:
• Age
• Current health status
• Past medical history
• Current medications
• Any allergies
• Previous immunisations
• Previous travel experience
• Any special needs?
► Question: What other risk assessment information do you require about George’s trip?
My Notes

Case study 1The need for YFV and ICVP
Risk assessment information about George’s trip:
• Where in Kenya is he going? Is he going to any other countries or will he have any stopovers in transit?
• When does he leave?
• How long is he going for?
• What activities will he be undertaking?
• Will he be in rural/urban areas or both?
• What will his accommodation be like? Will he have air-conditioning?
• Financial budget
• Does he have insurance?

Case study 1The need for YFV and ICVP
Further information:
• George is 30 years old. He is well and has no recent or previous medical history of note. He takes no medications and has no allergies. He has not had yellow fever vaccine before.
• He has travelled across Europe in the past but has never been to Africa.
• His trip is an organised two week tour, staying in a coastal resort close to Mombasa but including a 4 day safari to the Masai Mara Reserve. He flies directly to Kenya (Nairobi) from London, and takes a second flight to Mombasa.
• He will spend time relaxing at the beach while in the resort and will be outdoors while on safari.
• He will stay in an air-conditioned hotel in the resort and luxury tents during the safari.

Case study 1The need for YFV and ICVP
► Question: Is yellow fever vaccine advised and is there an International Certificate of Vaccination of Prophylaxis requirement?
Activity
Access TRAVAX and look at the country specific advice for Kenya.
If you do not use TRAVAX, access your normal resource for clinical/country-specific information.
My Notes

Case study 1The need for YFV and ICVP
► Answer: Yes - yellow fever vaccine is recommended for the safari part of the trip. An ICVP is needed, but only if travelling through a yellow fever infected area.
► Questions for further consideration:
• This patient has been referred to you by his GP practice for YFV – where does your duty of care start and end?
• Will you ensure that he has had all other recommended vaccines and advice?
• Whose responsibility is it to advise this patient about the risk of malaria and malaria prevention?
My Notes

Case study 1The need for YFV and ICVP – answers
► Question: This patient has been referred to you by his GP practice for YFV – where does your duty of care start and end?
► Answer: Healthcare practitioners who work within YFVCs need to give this careful consideration. It is essential that you ensure that other appropriate health advice is given to travellers who attend for YFV, and not just advice around yellow fever.
► Question: Will you ensure that he has had all other recommended vaccines and advice?
► Answer: There is a duty of care not just around YFV requirements, but for those other vaccinations that the traveller may need. If you are not supplying and administering the other vaccinations at the YFV, then you need to be sure that the traveller knows where other vaccinations can be obtained.
► Question: Whose responsibility is it to advise this patient about the risk of malaria and malaria prevention?
► Answer: It is the responsibility of all healthcare practitioners who advise travellers to give comprehensive advice on malaria risk and prevention.

Yellow fever International Certificate of Vaccination and Prophylaxis (ICVP) requirementsOutwith the risk of yellow fever to the individual traveller, where there is an International Health Regulation (IHR) regarding yellow fever, the individual may need to be vaccinated for certificate purposes.
Countries set their own requirements for yellow fever vaccination and certificates and inform WHO of their requirements.
• The aim of IHRs is primarily to protect the receiving countries (i.e. those countries that have the mosquito vector but do not have the disease).
• Each country informs WHO if it has yellow fever cases.
• Each country informs WHO if it has any International Certificate requirement.
This information is published annually in the WHO publication International Travel and Health.8
This information is also incorporated into country specific advice for every country on TRAVAX and is updated at least once per year. This ensures that the correct and most recent information about yellow fever risk and any ICVP requirement is available to healthcare practitioners advising travellers.
8 WHO. International Travel and Health. Geneva. World Health Organization, 2018. Available from: http://www.who.int/ith/en/

Case study 1 The need for YFV and ICVP
► Question: Consider George again – is there an ICVP requirement for his trip?
Activity
Access TRAVAX and look at the country specific advice for Kenya.
If you do not use TRAVAX, access your normal resource for clinical/country-specific information.
My Notes

Case study 1 The need for YFV and ICVP
► Answer: As George is travelling directly from London to Kenya with no stop over, there is no ICVP requirement. A YF ICVP will still be issued however, as he is having YFV administered for his own protection against yellow fever.

Yellow fever International Certificate of Vaccination and Prophylaxis (ICVP) requirementsA yellow fever vaccination certificate is always issued when the vaccine is given, whether there is a certificate requirement or not.
Only registered YFVCs can administer the vaccine and issue the ICVP.
Further administrative issues around vaccine certification are addressed in Part 3 of the training programme.

Case study 1 The need for YFV and ICVP
► Question: Imagine that George now changes his plans and decides that he also wants to visit Tanzania after visiting Kenya. Will he need an ICVP now?
Activity
Access TRAVAX and look at the country specific advice for Tanzania.
If you do not use TRAVAX, access your normal resource for clinical/country-specific information.
My Notes

Case study 1 The need for YFV and ICVP
► Answer: Yes. Tanzania has an ICVP requirement for travellers coming from YF infected areas and Kenya is a YF infected area.

Yellow fever exemption certificatesOccasionally, it may be in the best interest of the patient not to administer yellow fever vaccine (see vaccine exclusions and cautions).
Where there is a certificate requirement from the country to be visited, and it is deemed in the best interest of the individual not to vaccinate, an exemption certificate may be issued. When an exemption certificate is issued, the traveller should be made aware that destination countries are under no obligation to accept exemptions in place of the yellow fever vaccination certificate and that there is a small chance that entry could be denied.
Any healthcare professional can issue an exemption certificate – it need not be a practitioner within a YFVC. Further information on completing the exemption certificate can be found in Part 3 of the training programme.

Yellow fever vaccine The first yellow fever vaccine (still in use today) was developed at the Rockefeller Laboratories in New York 1937. It was developed in the 1930s by Max Theiler, who was later awarded the Nobel Prize for his work.9
The live attenuated vaccine was produced using the 17D strain of virus; the virus is grown in embryonated chicken eggs and goes through a sequential passage of various substrates until the virulence of the virus is decreased.
All subsequent vaccine sub strains are derived from the original 17D strain.
Production of the vaccine is under control of the WHO.
9 Encyclopaedia Britanica. Yellow Fever,2015. Available at: http://www.britannica.com/EBchecked/topic/652578/yellow-fever.

Yellow fever vaccine The current yellow fever vaccine contains 17D-204 virus strain (live attenuated) not less than 1000 units per 0.5ml dose.
Dosage is 0.5mls of reconstituted vaccine and administration is by deep subcutaneous injection.
The vaccine is highly immunogenic. Protective antibodies take 7-10 days to develop, consequently, the vaccine should be given at least 10 days before the traveller visits an area with risk of yellow fever transmission.
Re-immunisation every 10 years has been recommended until recently. In 2013, the WHO Strategic Advisory Group of Experts (SAGE) on Immunization10 stated, that with some exceptions, protection from yellow fever vaccination is considered to be lifelong for immunocompetent individuals. Boosters are therefore no longer routinely advised, except as below:
• Those individuals who may not retain long term immunity if vaccinated when: < 2 years of age; while pregnant; before undergoing a bonemarrow transplant; while infected with HIV; when immune suppressed.11
10 WHO Strategic Advisory Group of Experts on Immunization. World Health Organization, 2013. Available at: http://www.who.int/immunization/policy/sage/en/.
11 Public Health England. Immunisation Against Infectious Diseases: Yellow Fever (The Green Book). Available at: https://www.gov.uk/government/collections/immunisation-against-infectious-disease-the-green-book.

Case study 2The need for YFV boosters
Susan is 46 years old. She is well and has no recent or previous medical history of note. She takes no medications and has no allergies.
She had yellow fever vaccine 16 years before. She was completely well when she had the vaccine.
She is travelling to Gambia for a beach holiday.
She will be staying in an air-conditioned hotel.
She leaves in 4 weeks time and will be there for one week.
Case study 2The need for YFV boosters
► Question: Is yellow fever vaccine advised and should Susan have it? Is there an ICVP requirement?
Activity
Access TRAVAX and look at the country specific advice for Gambia.
If you do not use TRAVAX, access your normal resource for clinical/country-specific information.
My Notes

Case study 2 The need for YFV boosters
► Answer: There is a risk of yellow fever in Gambia but this traveller does not need to be re-vaccinated as she is still protected by the YFV she had 16 years ago. She does not need a ICVP unless travelling through an infected area.
If she was going to a country where all travellers required an ICVP (e.g. Cameroon), her original certificate would still be valid as the ICVP lasts the duration of the life of the person vaccinated.

Vaccine exclusionsThe following are absolute exclusions to yellow fever vaccination:
• Anyone with an acute febrile illness at the time of presentation for vaccination
• Anyone aged 6 months or under
• History of confirmed anaphylactic reaction to previous yellow fever vaccine or any of its components
• History of confirmed anaphylactic reaction to eggs or chicken protein
• Anyone with thymus disorder (see following pages)
• Anyone who is immunocompromised due to a congenital condition, disease process or treatment (see following pages)

Vaccine exclusions – Thymus disorderThere is an increased risk of serious adverse event if YFV is given to an individual with thymus disease. For this reason, YFV should not be given to anyone with thymus disorder.
The thymus gland (not to be confused with the thyroid gland) is found in the upper chest behind the sternum and forms part of the immune system.
Examples of thymus disease include thymoma and myasthenia gravis.*
The following paper11 describes a fatal adverse event in an individual with undiagnosed thymic disease who received YFV. Though tragic, such events are rare.
*Please note that there is no evidence that incidental removal of the thymus, e.g. during cardiac surgery, or indirect radiation leads to an increased risk.
11 Centers for Disease Control (CDC). Notes from the Field: Fatal Yellow Fever Vaccine-Associated Viscerotropic Disease – Oregon, September 2014. MMWR, 2015 / 64 (10); 279-281. Available at: http://www.cdc.gov/mmwr/preview/mmwrhtml/mm6410a5.htm?s_cid=mm6410a5_e

The Thymus GlandThyroid
• 2 lobes: ‘butterfly’
• Sits against and in front of the larynx and trachea
• Produces three hormones: T3/T4/calcitonin
• Influences the metabolic rate and protein synthesis
• Lasts for life
Thymus• 2 identical lobes
• Located in front of the heart and behind the sternum
• Matures T-cells
• Most active as neonate and pre-adolescent
• Continues for lifetime

Vaccine exclusions – ImmunocompromisedBeing immunocompromised is an exclusion for yellow fever vaccination in some instances and a caution in others. A careful and thorough risk assessment is essential, and likely risk of exposure to yellow fever virus must be considered.
Where an individual is immunocompromised due to an underlying medical condition or treatment, further information and advice should be sought from the medical consultant who attends the individual for that condition and/or treatment.
For those who are HIV positive, vaccination is contraindicated where HIV infection is symptomatic, or where the individual is asymptomatic, but there is evidence of an impaired immune function. Where the CD4 count is greater than 200 and the viral load is suppressed, vaccination may be considered, but specialist advice should be sought.

Vaccine cautionsThe following are cautions to yellow fever vaccination; specialist advice should be sought:
• Babies aged 6-9 months* – vaccination may be considered for this age but only if the risk of yellow fever infection is considered to be high and if travel is unavoidable.
• Individuals aged over 60 years – a thorough risk assessment is required due to the increased risk of serious side effects in this age group and in some instances specialist advice may be needed (see following pages).
• During pregnancy and breastfeeding - vaccination may be considered only if the risk of yellow fever infection is considered to be high and if travel is unavoidable.
• Individuals who are immunocompromised (see previous pages).
*Vaccine is not generally advised to children aged < 9 months – this is because of the risk of post-vaccine encephalitis in this group. In rare circumstances (e.g. during and outbreak and where travel is unavoidable) vaccine may be considered for children aged 6-9 months. Specialist advice should be sought.

Case study 3YFV cautions
Carolyn is 26 years old. She is well and has no recent or previous medical history of note. She takes no medications and has no allergies.
She is 12 weeks pregnant.
She has not had yellow fever vaccine before.
She is an experienced traveller.
She is travelling to Central African Republic for work purposes. She works in an administrative role with an international charity. During the trip, she will be office based, in the capital Bangui.
She will be staying in an air-conditioned hotel.
She leaves in 4 weeks time and will be there for one week.

Case study 3YFV cautions
► Question: Is yellow fever vaccine advised and is there an ICVP requirement?
Activity
Access TRAVAX and look at the country specific advice for Central African Republic.
If you do not use TRAVAX, access your normal resource for clinical/country-specific information.
My Notes

Case study 3 YFV cautions
► Questions for further consideration
• What is the risk of yellow fever in the Central African Republic?
• How do her intended activities, accommodation etc. impact on her risk of acquiring yellow fever?
• What are the concerns regarding yellow fever and Carolyn being pregnant?
• What are the options and how will you advise Carolyn about: YF the disease; YF the vaccine; YF ICVP?
My Notes

Case study 3 YFV cautions – answers
► Question: What is the risk of yellow fever in the Central African Republic?
► Answer: Yellow Fever is endemic in this country so there is a risk.
► Question: How do her intended activities, accommodation etc. impact on her risk of acquiring yellow fever?
► Answer: Being office based (therefore indoors) and based in the capital city mean that the risk is less than if she were in a rural area and undertaking outdoor activities. Having air-conditioned accommodation also reduces the risk of exposure.
► Question: What are the concerns regarding yellow fever and her being pregnant?
► Answer: Pregnancy is not an absolute contraindication to vaccination with YFV, but it is a caution. This means that we would prefer not to give the vaccine, but we can give it where the risk of acquiring yellow fever outweighs any risk to the foetus from the vaccine. This is a decision that needs to be made by the pregnant woman following discussion with the healthcare practitioner.

Case study 3 YFV cautions
► Question: What are the options and how will you advise Carolyn about: YF the disease; YF the vaccine; YF ICVP?
My Notes
Case study 3 YFV cautions
► Answer
• The first option may be to advise the traveller not to travel.
• If this is not possible, then the traveller needs to decide whether to have the vaccine or not.
• If she decides to travel but not to have the vaccine, then there is a risk of acquiring yellow fever. In addition, a YF ICVP is required by all travellers over 9 months, for entry into Central African Republic. In the absence of YF ICVP she takes the chance of being refused entry into the country even if she has an exemption certificate.
• If she chooses to have the vaccine, we cannot guarantee no adverse effects to the foetus, although limited data available suggest no adverse effects.12
12 STAMARIL SPC, 2018 . Available at: http://www.medicines.org.uk/EMC/medicine/9846/SPC/Stamaril/

Case study 3 YFV cautions
► Questions for further consideration:
• This patient has been referred to you by her GP practice for YFV – where does your duty of care start and end?
• Will you ensure that she has had all other recommended vaccines and advice?
• Whose responsibility is it to advise this patient about the risk of malaria and malaria prevention?
• In this scenario you may wish to seek specialist advice – where would you get this?
My Notes

Case study 3 YFV cautions – answers
► Question: This patient has been referred to you by her GP practice for YFV – where does your duty of care start and end?
► Answer: Healthcare practitioners who work within YFVCs need to give this careful consideration. It is essential that you ensure that other appropriate health advice is given to travellers who attend for YFV, and not just advice around yellow fever.
► Question: Will you ensure that she has had all other recommended vaccines and advice?
► Answer: There is a duty of care not just around YFV requirements, but for those other vaccinations that the traveller may need. If you are not supplying and administering the other vaccinations at the YFVC, then you need to be sure that the traveller knows where other vaccinations can be obtained.

► Question: Whose responsibility is it to advise this patient about the risk of malaria and malaria prevention?
► Answer: It is the responsibility of all healthcare practitioners who advise travellers to give comprehensive advice on malaria risk and prevention.
► Question: In this scenario you may wish to seek specialist advice – where would you get this?
► Answer: It is essential to know where you should refer for specialist advice should it be required.

Vaccine adverse eventsAs with all vaccinations there is the risk for adverse events to occur. Full detail of these may be found in the vaccine Summary of Product Characteristics (SPC), but they can be summarised as follows:
• Very common adverse events – headache, local reaction at vaccination site
• Common adverse events – nausea, pyrexia, myalgia, nausea, vomiting
• Uncommon adverse events – abdominal pain, arthralgia
• Rare, but serious adverse events – viscerotropic and neurotropic reactions (see further notes)
Vaccine adverse eventsAdministration of yellow fever vaccine is associated with rare, but serious adverse events. These are classified as viscerotropic and neurotropic reactions:
• The viscerotropic reaction, also known as YEL-AVD, closely resembles fulminant infection with wild yellow fever virus where the vaccine virus proliferates in multiple organs
• The neurotropic reaction, also known as YEL-AND, affects the central nervous system and may manifest as meningoencephalitis, Guillian-Barre syndrome, and acute disseminated encephalomyelitis

Yellow fever vaccine Associated Viscerotropic Reaction (YEL-AVD)YEL-AVD closely resembles fulminant infection with wild yellow fever virus where the vaccine virus proliferates in multiple organs.
• The average onset is 4 days post vaccination (range 0-8 days)
• Initial symptoms include: fever, malaise, headache, myalgia, vomiting and diahorrea
• More severe symptoms include: hypotension, thrombocytopaenia, coagulopathy, hepatic, renal or respiratory insufficiency or failure. Multi-organ failure and death occurs in 60% of those affected by YEL-AVD
• Since this complication was first recognised in 2001, more than 65 cases have been reported throughout the world.13 The risk of YEL-AVD is estimated to be 0.4 per 100 000 doses administered
• There is no specific treatment for YEL-AVD and treatment is supportive only once other diagnosis have been excluded. Diagnosis can be made by detecting yellow fever vaccine virus by PCR in serum or tissues
13 Centers for Disease Control and Prevention (CDC). Traveler’s Health; Yellow Fever, 2018. Available at: https://wwwnc.cdc.gov/travel/yellowbook/2018/infectious-diseases-related-to-travel/yellow-fever.
Yellow fever vaccine Associated Neurotropic Reaction (YEL-AND)YEL-AND is a serious but rarely fatal reaction. The vaccine virus infects the central nervous system and meningoencephalitis is the most common presentation. Other manifestations include Guillian-Barre syndrome and acute disseminated encephalomyelitis.
• The average onset is 14 days post vaccination (range 3-28 days).
• The risk of YEL-AND is estimated to be 0.8 per 100 000 doses administered.
• The treatment for YEL-AND depends on the symptoms. A neurological consultation should be sought and cerebrospinal fluid should be tested for the presence of yellow fever virus or yellow fever virus-specific antibodies.
• Most individuals recover fully.

Risk of YEL-AVD and YEL-AND in those aged over 60 yearsAnalysis of adverse events reports suggest that the risk of a serious adverse events is greater in those aged 60 and over, especially if it is the first time receiving yellow fever vaccine.
Based on the most recent analysis of YEL-AVD in the United States, the risk of YEL-AVD is 0.4 per 100 000 doses of vaccine given overall. This increases to 1.0 per 100 000 doses in those aged 60-69 yrs and further increases to 2.3 per 100 000 doses in those aged over 70yrs. Similar increases in age-related risks are seen for YEL-AND.14
Age in itself is not a contraindication to yellow fever vaccination, but careful risk assessment is essential. Vaccination may not be suitable for those aged 60 and over if there is an additional underlying medical conditions and/or medications (particularly immune-suppressants), are being taken.
The likely exposure to yellow fever virus at the destination needs to be carefully considered and if the risk is deemed to be high, the individual may be advised not to travel. If travel is unavoidable, the traveller needs to be made aware of the risk of travelling unvaccinated, and mosquito bite prevention advice should be given. Where a certificate of vaccination is required, an exemption certificate may be given (see Part 3).
14 Centers for Disease Control and Prevention (CDC). Yellow Fever History, Epidemiology and Vaccination Information. 2015. Available at: http://www.cdc.gov/travel-training/local/HistoryEpidemiologyandVaccination/page27254.html.
Case study 4 YFV cautions / ICVP requirements
Mr and Mrs Anderson are 75 and 70 years old respectively.
Mr Anderson is currently well. He had bowel cancer 10 years ago but is now fully recovered. Mrs Anderson is generally well although she has type 2 diabetes and takes an alpha glucosidase inhibitor. Neither has any allergies.
Neither has had yellow fever vaccine before.
They are going on a 15 day cruise and their itinerary is as follows: Puerto Vallarta (Mexico); Puerto Quepos, (Costa Rica); Panama Canal transit (Panama); Aruba; Florida (disembark). At each destination there will be daytime excursions.
They have been advised by the cruise company that they need YF ICVPs. They leave in 5 weeks time.

Case study 4 YFV cautions / ICVP requirements
Activity
Access TRAVAX and look at the country specific advice for Mexico, Costa Rica, Panama, Aruba and the USA.
If you do not use TRAVAX, access your normal resource for clinical/country-specific information.
My Notes

Case study 4 YFV cautions / ICVP requirements
► Questions for further consideration
• What is the risk of yellow fever in each of the destinations?
• How do their intended activities, accommodation etc. impact on their risk of acquiring yellow fever?
• What are the concerns regarding YFV and their ages?
• What are the options and how will you advise them about: YF the disease; YF the vaccine; YF ICVP?
My Notes

Case study 4 YFV cautions / ICVP requirements – answers
► Question: What is the risk of yellow fever in each of the destinations?
► Answer: When there are multiple destinations, such as with a cruise, each destination must be considered in turn. The order in which countries are visited is relevant as this can affect the ICVP requirements.
Although YF is present in Panama, the Andersons are not going into a YF risk areas. However, Aruba requires a YF ICVP because they have been to Panama, which is considered an infected country (even though they do not visit a risk area).
► Question: How do their intended activities, accommodation etc. impact on their risk of acquiring yellow fever?
► Answer: Most of their time will be spent onboard the ship, with daytime excursions only. Most cruise liners are air-conditioned. If their itinerary did take them into a YF risk area – we could not entirely rule out the risk of YF exposure as the YF mosquito bites during the day.

Case study 4 YFV cautions / ICVP requirements – answers
► Question: What are the concerns regarding YFV and their ages?
► Answer: Both travellers are in their 70s and therefore in the age group where there is a higher risk or serious adverse event (YEL-AVD and YEL-AND) following administration of YFV when given for the first time.
Case study 4 YFV cautions / ICVP requirements
► Question: What are the options and how will you advise them about: YF the disease; YF the vaccine; YF ICVP?
My Notes
Case study 4 YFV cautions / ICVP requirements
► Answer:
• They are not at risk of acquiring YF, the disease.*
• There is a YF ICVP requirement. In addition, the cruise company have advised them that they need ICVPs.
• Age alone is not a contraindication to vaccination, however Mrs Anderson does have a chronic medical condition.
• A full discussion around risk versus benefit should take place.
• In this instance, it may be in the best interests of the travellers to issue yellow fever exemption certificates (see Part 3).
* This scenario does not take into account any recent yellow fever outbreaks. Outbreaks need to be checked regularly e.g. using TRAVAX.
Summary: Part 2Yellow fever – the disease and vaccine This part of the learning programme has covered key aspects of learning regarding yellow fever, the disease, the vaccine and the ICVP.
The next part of the programme will cover aspects relating to administrative issues relevant to yellow fever vaccination centres.

Part 3
Administrative Issues for Yellow Fever Vaccination CentresAt the end of this section, participants should:
• Be able to undertake administrative issues relevant to YFVCs, including legal aspects and accountability
• Understand the Conditions of Registration for YFVCs
• Know when and where to seek specialist advice
Click anywhere to continue

Providing yellow fever servicesIn Part 1 of the training programme, we established that the administration of yellow fever vaccine is regulated under the World Health Organization (WHO) International Health Regulations (IHR) and that in Scotland, HPS has a statutory responsibility for Scottish YFVC registration.
Any centre with a Registered Medical Practitioner (RMP) can become a YFVC. The RMP must agree to, and sign, the Conditions of Registration. The RMP has overall responsibility for that YFVC and must ensure that all terms and conditions of registration are adhered to.
In this part of the learning programme, we will highlight some key aspects of the Conditions of Registration, and some other factors for consideration for YFVCs.
YFVCs should administer only yellow fever vaccines approved by WHOA key aspect of YFVC registration is that yellow fever vaccine procured for use in the YFVC is only that approved for use by WHO. This is to ensure that the safety and effectiveness of the vaccine used throughout the world is of a required standard.
In the UK there is currently only one WHO approved vaccine manufacturer for yellow fever vaccine:
Stamaril™ available from:
Sanofi UKOne Onslow StreetGuildfordSurrey
General Information tel: 01483 505 515 Medical Information tel: 0845 372 7101
Website: www.sanofi.co.uk
In Scotland, YFVCs purchase the vaccine directly from the vaccine manufacturer.

Facilities for ordering and storing vaccines will be of an acceptable standardIt is essential that YFVCs are responsible for all aspects of correct vaccine storage and handling.
HPS has published guidance on Vaccine Storage and Handling.
This document sets out a framework outlining the minimum standards that are required for effective storage and handling of vaccines thereby minimising the risk of compromising the effectiveness of vaccines given to patients and supplements the recommendations in Chapter 3 of Immunisation against Infectious Disease 2006 (the Green Book).
In order to meet the objectives of the yellow fever learning programme, please complete the storage and handling of vaccines programme which has been produced by NHS Education Scotland (NES).
The Storage and Handling of Vaccines programme takes approximately 10-15 minutes to complete.

Yellow fever vaccine will be administered by a responsible Healthcare PractitionerThe Registered Medical Practitioner (RMP) responsible for the YFVC can administer the vaccinations and complete the ICVPs. More often, the RMP may choose to delegate this to another suitably qualified healthcare practitioner within the practice (e.g. other doctor, nurse or pharmacist).
The Royal College of Nursing (RCN) considers that the prescription, provision and administration of yellow fever vaccine are part of a more specialist travel health service.15 In addition they say that those involved in provision of more specialist travel health services should undertake specific travel health education.
The RCN have published a career and competence framework16 aimed at nurses working in the field of travel medicine from level 5 (the competent nurse) through to level 7 (the senior practitioner / expert nurse). Though aimed primarily at nurses, this is also a useful resource for other healthcare practitioners as it gives detailed information on conducting the travel health risk assessment. If you do not already have a copy of the career and competence framework, you can download it from the RCN website.
15 RCN. Delivering travel health services. RCN guidance for nursing staff, 2005. RCN Publishing, London Code: 002 757.
16 RCN. Travel health nursing: career and competence development. RCN guidance, 2018. Available at: https://www.rcn.org.uk/professional-development/publications.

YFVCs must comply with staff training as required by HPSHPS stipulates that when a new YFVC registers, at least one individual from that practice must undertake the HPS yellow fever face-to-face training before they can practice as a YFVC. Thereafter, at least one person from the YFVC must undertake yellow fever training (either face-to-face or online) at least once every two years.
As the online training is available free of charge and can be completed at any time, it is recommended that all practitioners undertake this training, even if they have not attended the face-to-face training. In addition, the online training can be undertaken at any time should an individual feel there is a learning or training need.
These training requirements are the minimal requirements. Given that the RCN considers that provision of yellow fever vaccine is a more specialist service, additional training is recommended for all practitioners delivering YFV services.

Appropriate policies for safe administration of yellow fever vaccine should be in placeThe RCN also advocates the use of protocols within the clinic environment.17 A protocol is an agreed framework outlining the care that will be provided to patients in a designated area of practice and are very useful in establishing areas of responsibility. Protocols should be written and agreed by all those involved in the service and should be updated regularly.
The following aspects could be included in a YFVC clinic protocol (this list is not exhaustive and each centre will have its own priority areas).
17 RCN. Using protocols, standards, policies and guidelines to enhance confidence and career development, 2008. Available at: www.rcn.org.uk/publications.

Aspects for inclusion in a YFVC protocol• When the clinic will operate (set times or ad hoc as patients attend).
• Whether appointments will be offered at weekends / evenings.
• Who will see travel patients e.g. are all clinical staff capable of seeing patients who require YFV.
• Who should provide the service when a key staff member is on leave.
• Whether the clinic will be advertised and if so who should be targeted.
• Whether appointments will be offered to patients outwith the surgery list.
• What training is required for staff initially and ongoing continuous professional development (CPD).
• Who will order and manage stock including vaccines.
• Who will monitor and record the vaccine fridge temperature.
• Who will check any emergency equipment.
• How will YFV be prescribed.
• Charging for vaccines and who will handle payments / money.
• Who will be responsible for maintenance of vaccine administration records and YFV audit (required by HPS).

Prescribing yellow fever vaccineYFV is normally prescribed using a Patient Specific Direction (PSD). This can be issued by any independent prescriber such as a doctor, nurse or pharmacist. A PSD is a written instruction by the independent prescriber for a medicine to be supplied or administered to a specific, named individual.
In primary care, the PSD may be a simple instruction in the patient’s notes.
In a clinic setting this could be a list of named patients to be prescribed a medication signed by the prescriber.
YFV can be supplied and administered under a Patient Group Directive (PGD) under special circumstances as follows:
• Some community pharmacies offer private travel vaccines using a PGD. This is possible if the pharmacy is part of a UK-wide organisation and the PGD has been authorised in England, where the law is different
• Special arrangements can be set up between pharmacies and their own regional health-boards whereby YFV can be prescribed using a PGD
• From April 2017, a change in the law in Scotland means that private clinics registered with Health Improvement Scotland can develop and authorise their own PGDs
Further information on the use of PGDs can be found at the Medicines and Healthcare Products Regulatory Agency.
Charging for YFVYFV is not remunerated by the NHS, therefore the patient pays for the vaccine.
In this instance, the process of administration of the vaccine is also chargeable. In addition, YFVCS can also charge for issuing the YF ICVP. Most clinics round this up for one payment.
An FP10 (or equivalent NHS prescription) must not be used to provide YFV.18
The British Medical Association (BMA) has further information on charging for travel vaccines.
18 British Medical Association (BMA). BMA Focus on Travel Immunisation (GPC guidance) 2016. Available at: https://www.bma.org.uk/advice/employment/gp-practices/service-provision/prescribing/vaccination/travel-immunisation.
YF International Certificates of Vaccination (ICVP) will be completed in accordance with IHRThe YF ICVP is an individual certificate and one should be issued for each person vaccinated, including children. The ICVP is valid for the duration of the life of the person vaccinated, beginning 10 days after the date of vaccination.
The person who administers the YFV should issue the ICVP (either the registered medical practitioner responsible for the YFVC or the designated person), and must sign the certificate. The certificate should bear the official stamp of the administering centre.
The date of vaccination must be recorded as follows: the day placed first in numerals, the month second in letters and the year last in numerals, for example, 10 August 2007.
The individual being vaccinated must also sign the certificate. Where the person being vaccinated is a child and is unable to sign their own name, the signature should be that of the parent or guardian.
Full details of all aspects of certificate completion can be found within the HPS Designation Information Pack.

Completion of the ICVP
Activity
On the next page is an example of an ICVP that has 9 errors in completion.
Click on the certificate where you think there may be an error or use the ‘Show all errors’ button to show all the errors on the form.
Errors in completion are highlighed with a
Correctly completed sections with a
You can also view a sample of a correctly completed IVCP by clicking on the ‘Show corrected ICVP’ button.
Please note: the next page may take a moment to load, please be patient and do not click the forward or back buttons until the activity has loaded.


Reissuing a YF ICVPIn the case of a lost certificate, the original YFVC administering the ICVP should ideally re-issue it. A certificate need not be signed by the original vaccinator and can be signed instead by a person authorised to sign at the time of re-issue. In these circumstances, the name of the original vaccinator should be noted in the records where possible. The date on the certificate should be the date of the original vaccination.
If the original administering YFVC is no longer a designated centre, or the patient is unable to attend the original administering YFVC, any designated YFVC may reissue a certificate. In order to do this they must be satisfied that the individual has been vaccinated and that sufficient information is available to complete another certificate e.g. date of vaccination, manufacturer and batch number of vaccine.
The YFVC is entitled to charge for reissuing an ICVP.
In the event that a record of vaccination could not be accessed, the individual would need to be revaccinated in order to ensure that they are protected against yellow fever.

Issuing an exemption from vaccination certificateIn Part 2 of the programme, we identified that there are some instances where an ICVP is required, but for health reasons, it may not be in the best interests of the individual to receive YFV.
In such circumstances, it is appropriate to issue an exemption from vaccination certificate. Any healthcare professional can issue an exemption certificate, they do not have to work within a YFVC.
The most recent ICVP booklets, contain a page specifically for this purpose.

Issuing an exemption from vaccination certificateIf the healthcare professional does not have copies of the ICVP, they can issue an exemption certificate using headed notepaper as long as they include all of the relevant information including:
• The patient’s name and date of birth
• A statement of explanation for exemption such as:This is to certify that on medical grounds I advise that Yellow Fever vaccine is contraindicated in the above named person and should not be given
• Date that the exemption begins
• Date that exemption expires (normally the duration of the impending travel – exemption should be reassessed for subsequent travel and a new certificate issued)
• Printed name and signature of healthcare practitioner issuing the certificate
• Relevant professional qualifications (MD, RN etc.)
• Ensure name and address of the practice is included in the headed paper, and stamp with clinic stamp

The Centre will keep appropriate records of all vaccinations administeredDetails of YFV administration must be clearly recorded in individual patient records.
Under the Conditions of Registration, there is a requirement for YFVCs to keep records of all yellow fever vaccinations administered. Records should be maintained for 10 years after vaccination. This also applies for any patients seen for YFV who are not registered patients within that practice.
Maintaining records for the first year is essential to fulfil the HPS annual audit/ annual returns requirement (to follow).YFVCs are required to maintain a record of the number of YFVCs given each year and any adverse events experienced by patients.
Thereafter, reasons for keeping the records of vaccination for 10 years, are in part, to ensure that the ICVP can be re-issued in the event that a certificate is lost.
In addition, YFVCs should keep a separate record of YFVs given, for the purposes of the annual returns. HPS suggest using a form similar to this sample (please click on the thumbnail to view a sample YFV record sheet).

Annual returns utilisation will be returned to HPSThe purpose of the annual returns is for HPS to conduct an audit of Scottish YFVCs around YFV usage and adverse events.
Annual returns of vaccine utilisation may be submitted to HPS using the annual returns form provided. HPS will alert YFVCs initially by email (usually in January) that the annual returns are due for submission. Most centres opt to submit their returns electronically; if the form is used it can be sent by email. HPS provide the annual return form and it can also be downloaded from the website.
YFVCs must enter the number of doses of vaccine given by the centre on the previous year and notify whether there were any adverse events. If adverse events are reported, this will be followed up by a member of HPS staff for further information.
Under the Conditions of Registration HPS can request access to a YFVC or copies of YFVC records to ensure the centre is complying with the conditions of Registration. HPS has the authority to de-register any YFVC that does not comply with Conditions of Registration.

Adverse events will be reported to the medicines and healthcare products regulatory agency (MHRA) Any vaccine associated adverse event must be reported to the Medicines and Healthcare Products Regulatory Agency (MHRA) via the Yellow Card reporting system. Any individual can report a possible adverse event using this system including the patient themselves.
In addition, and as already indicated, HPS wish to be informed of any adverse event through the annual return report.

HPS should be notified of any changes which may affect registration statusHPS must be notified immediately of any changes which may affect the centre’s registration status, in particular if the registered medical practitioner (RMP) in charge of the clinic changes.
If the RMP in charge of the clinic moves to another clinic site, he/she must reapply for registration within that new centre (noting that it is the centre that is registered and not the RMP).

All YFVCs status are reviewed bienniallyAll YFVCs must re-register every two years. HPS will inform YFVCs that they are due for re-registration. At that time there is an opportunity to change any clinic details.
Centres who opt to re-register will need to pay a re-registration fee.
Centres can opt to de-register at anytime e.g. they are providing the service for a very small number of clients. The re-registration process offers an opportunity for centres to de-register if they wish to do so.

Useful resources and further adviceFurther information and advice for YFVCs can be accessed through the HPS website.
In addition, YFVCs can contact the HPS YFVC administrator at: [email protected].
Detailed clinical information on yellow fever can be accessed through TRAVAX.
In addition, TRAVAX users can contact the TRAVAX support line to speak with a clinician Monday and Friday from 14.00-16.00 and Friday from 09.30-11.30 at 0141 300 1130.

Summary: Part 3Administrative issues for Yellow Fever Vaccination CentresThis concludes Part 3 of the learning programme which covered administrative issues and conditions of registration for YFVCs.

ConclusionThis concludes the yellow fever training programme provided by Health Protection Scotland and NHS Education for Scotland.
We hope that you have found this programme useful.
If you wish to give us any feedback you can do this via email. Please title your email ‘Yellow fever online programme feedback’ and send it to: [email protected].
If you have completed this learning programme to fulfil your biennial training requirement as a YFVC, please fill in the Confirmation of Completion Form and email it to [email protected].
NB: To ensure full functionality of the pdf form please open in Adobe Reader rather than your web browser.
Alternatively the form can be posted to the address below:
Travel Health (Yellow Fever)Health Protection ScotlandNHS National Services ScotlandMeridian Court5 Cadogan StreetGlasgowG2 6QE

End of Yellow Fever Training Programme

Click anywhere to return to the previous page
Yellow fever vaccine recommendations in Africa1
1 Current as of September 2016. This map, which aligns with recommendations also published by the World Health Organization (WHO), is an updated version of the 2010 map created by the Informal WHO Working Group on the Geographic Risk of Yellow Fever.
2 Yellow fever (YF) vaccination is generally not recommended in areas where there is low potential for YF virus exposure. However, vaccination might be considered for a small subset of travelers to these areas who are at increased risk for exposure to YF virus because of prolonged travel, heavy exposure to mosquitoes, or inability to avoid mosquito bites. Consideration for vaccination of any traveler must take into account the traveler’s risk of being infected with YF virus, country entry requirements, and individual risk factors for serious vaccine-associated adverse events (e.g., age, immune status).

clothingAppropriate clothing to protect skin from mosquito bites
Click anywhere to return to the previous page

repellentsInsect repllents
By Tinton5 (Own work) [CC BY-SA 3.0 (http://creativecommons.org/licenses/by-sa/3.0).
Click anywhere to return to the previous page

netsMosquito nets
Click anywhere to return to the previous page

fogging/sprayingInsect fogging and spraying
Click anywhere to return to the previous page

stagnant waterMosquito breeding sites
Click anywhere to return to the previous page

Vax recordExample yellow fever vaccination record
Click anywhere to return to the previous page

Cutting through the Culebra Mountain, general view looking West, towards Panama.
Credit: Wellcome Library, London. From: Illustrated London News. Published: 1888.
Copyrighted work available under Creative Commons Attribution only licence CC BY 4.0: https://creativecommons.org/licenses/by/4.0/.
Click anywhere to return to the previous page
Juan Carlos Finlay who identified the mosquito as the possible yellow fever vector in 1881.
Credit: Wellcome Library, London. From: Walter Reed and Yellow Fever. By: Kelly, H. A. Published: McClure, Phillips and Company New York 1906.
Copyrighted work available under Creative Commons Attribution only licence CC BY 4.0: https://creativecommons.org/licenses/by/4.0/.
Click anywhere to return to the previous page

Yellow fever memorial marker at Oaklawn Cemetery, Tampa, Florida.
Credit: Marque1313.
Image available under Creative Commons Attribution only licence CC BY 3.0: https://creativecommons.org/licenses/by/3.0/.
Click anywhere to return to the previous page

Plate showing a street plan of New York - taken from ‘An inquiry into the cause of the prevalence of the Yellow-Fever in New York’.
Credit: Wellcome Library, London. From: An inquiry into the cause of the prevalence of the Yellow-Fever in New York. Medical Repository. By: Valentine Seaman. Published: New York 1798.
Copyrighted work available under Creative Commons Attribution only licence CC BY 4.0: https://creativecommons.org/licenses/by/4.0/.
Click anywhere to return to the previous page

Major Walter Reed, who demonstrated that transmission of yellow fever virus from one individual to another through the bite of the Aedes Aegypti mosquito.
Click anywhere to return to the previous page
Horses and carriages, yellow fever prophylaxis team.
Credit: Wellcome Library, London. From: Os serviços de saúde publica no Brasil: especialmente na cidade do Rio de Janeiro: de 1808 a 1907. By: Oswaldo Cruz. Published: Impr. Nacional Rio de Janeiro 1909.
Copyrighted work available under Creative Commons Attribution only licence CC BY 4.0: https://creativecommons.org/licenses/by/4.0/.
Click anywhere to return to the previous page

Spraying roofs to prevent yellow fever.
Credit: Wellcome Library, London. From: Os serviços de saúde publica no Brasil: especialmente na cidade do Rio de Janeiro: de 1808 a 1907. By: Oswaldo Cruz. Published: Impr. Nacional Rio de Janeiro 1909.
Copyrighted work available under Creative Commons Attribution only licence CC BY 4.0: https://creativecommons.org/licenses/by/4.0/.
Click anywhere to return to the previous page

Yellow fever vaccine recommendations in the Americas1 (Updated May 5, 2018)1 This map aligns with recommendations published by the World Health Organization (WHO). It is an updated
version of the 2010 map created by the Informal WHO Working Group on the Geographic Risk of Yellow Fever.2 In 2017, CDC expanded yellow fever vaccination recommendations for travelers to Brazil due to a large
outbreak of yellow fever in multiple states within that country. Please refer to the Yellow Fever in Brazil Travel Notice for more information and updated recommendations.
3 Yellow fever (YF) vaccination is generally not recommended in areas where there is low potential for YF virus exposure. However, vaccination might be considered for a small subset of travelers to these areas who are at increased risk for exposure to YF virus because of prolonged travel, heavy exposure to mosquitoes, or inability to avoid mosquito bites. Consideration for vaccination of any traveler must take into account the traveler’s risk of being infected with YF virus, country entry requirements, and individual risk factors for serious vaccine-associated adverse events (e.g., age, immune status).
Click anywhere to return to the previous page