yorkshire centre for health informatics pct commissioning, business models & pathology dr rick...
Post on 21-Dec-2015
215 views
TRANSCRIPT
Yorkshire Centre for Health Informatics
PCT Commissioning,Business Models & Pathology
Dr Rick Jones
Leeds Teaching Hospitals Trust

A Patient-led NHS requires:
• Informed Patients: – responsibility – choice– tax payers
• Effective Commissioners: – responding to Patients– understanding the evidence base– managing demand
• Responsive providers: – liberated from central control– competing to improve– managing costs

Commissioning
‘the means by which we secure the best value for patients and taxpayers. By ‘best value’ we mean:
– The best possible health outcomes – The best possible healthcare– With the resources made available by the tax payer’
DH 2006

Commissioning
The term “commissioning” is interpreted in different ways by different people. It is often used to denote “contracting” but in reality refers to a much broader process encompassing planning, procurement / contracting and performance management underpinned by partnerships.
Keith Douglas,
Director of Planning and Service Redesign, Eastleigh and Test Valley South Primary Care Trust and New Forest Primary Care Trust

Commissioning:
• ‘the set of linked activities required to assess the health care needs of a population, specify the services required to meet those needs within a strategic framework, secure those services and monitor and evaluate the outcome’
Woodin, 2007

The Commissioning CycleAssess health needs
Decide priorities
Review current service provision
Develop new service model
Procure provider
Award contract
monitor contract

What people want
• Local services there when you need them• Emergency care when you need it• No waiting• The best patient experience• To have a say, to have a choice• More emphasis on prevention• Health and social care working together• Improved health
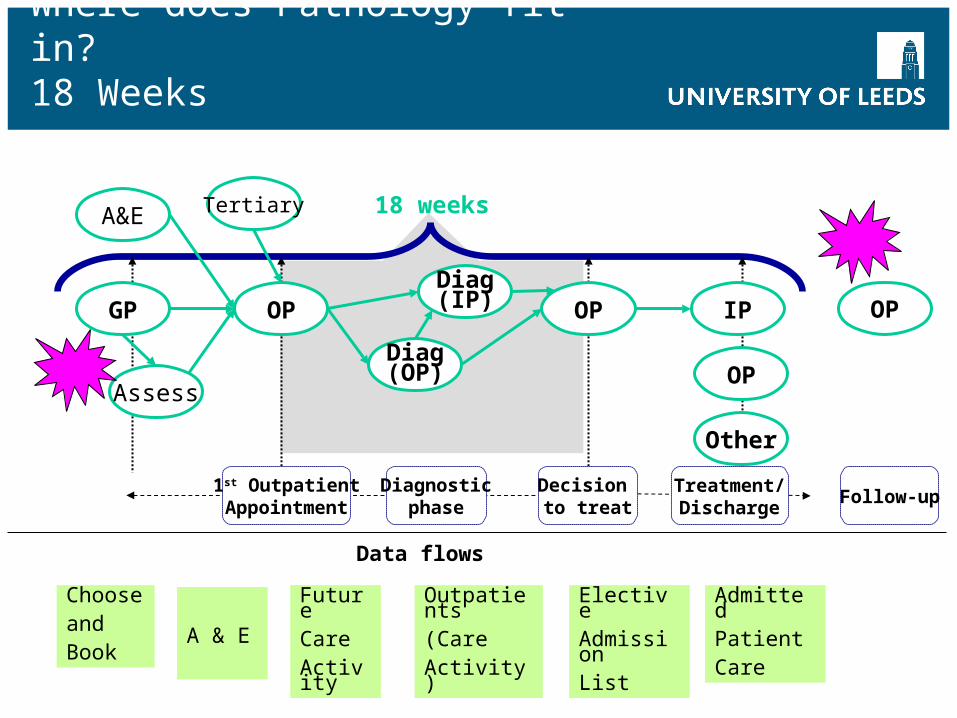
OP
Other
A&E Tertiary
Assess
Diag(OP)
Diag(IP)
Diagnosticphase
OP OP
1st OutpatientAppointment
Decision to treat
GP IP OP
Follow-upTreatment/Discharge
18 weeks
Data flows
ElectiveAdmissionList
AdmittedPatientCare
Outpatients(CareActivity)
FutureCareActivity
A & E
ChooseandBook
Where does Pathology fit in?18 Weeks
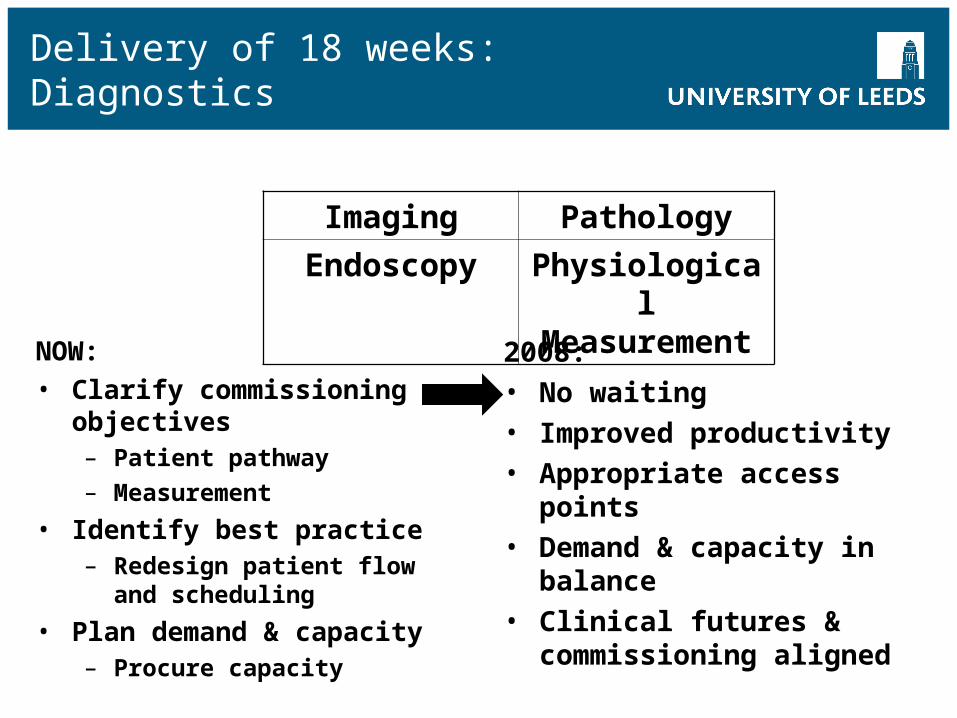
Delivery of 18 weeks: Diagnostics
NOW:• Clarify commissioning
objectives– Patient pathway
– Measurement
• Identify best practice– Redesign patient flow and
scheduling
• Plan demand & capacity– Procure capacity
2008:• No waiting• Improved productivity• Appropriate access points• Demand & capacity in
balance• Clinical futures &
commissioning aligned
Imaging Pathology
Endoscopy Physiological Measurement
Pathways
Pathways need to be focussed on the needs / demands of the population and on resources available: one of the really difficult tasks for commissioning to address is what should and should not be delivered as clearly not everything can be afforded…
Keith Douglas,
Director of Planning and Service Redesign, Eastleigh and Test Valley South Primary Care Trust and New Forest Primary Care Trust

How should pathology engage?
• Who to approach?• By what route?• What type of services to present?• Reactive or pro-active engagement?
First know your customer and your product(s)

From Craftsmen to Service Providers
• Our society has become what it is today through the forces of– Specialization
– Standardization
– Scalability
• It is now almost exclusively “service” oriented– Transportation
– Telecommunication
– Retail
– Healthcare
– Financial services
– …
The IT industry which has many parallels to Pathology – high tech, rapidly developing, knowledge-based, ill understood by majority of users

Tidal Wave of Business Shift
• Classic 1900’s Companies– Control Delivery – Control Services– Control Information– Have expensive acquisition processes and static relationships– Managed pricing and expectations
• Information Age 21st Century– Consumer is empowered by information access– Businesses win by being open– Businesses win by leveraging new mechanisms to drive their own
costs down.– Dramatic lower overall cost potential, higher level of services.

Traditional Pathology Organisation
HaemClin
BiochemHisto Micro Immuno Genetics
Pathology
Local Trust GPs Other TrustsScreening
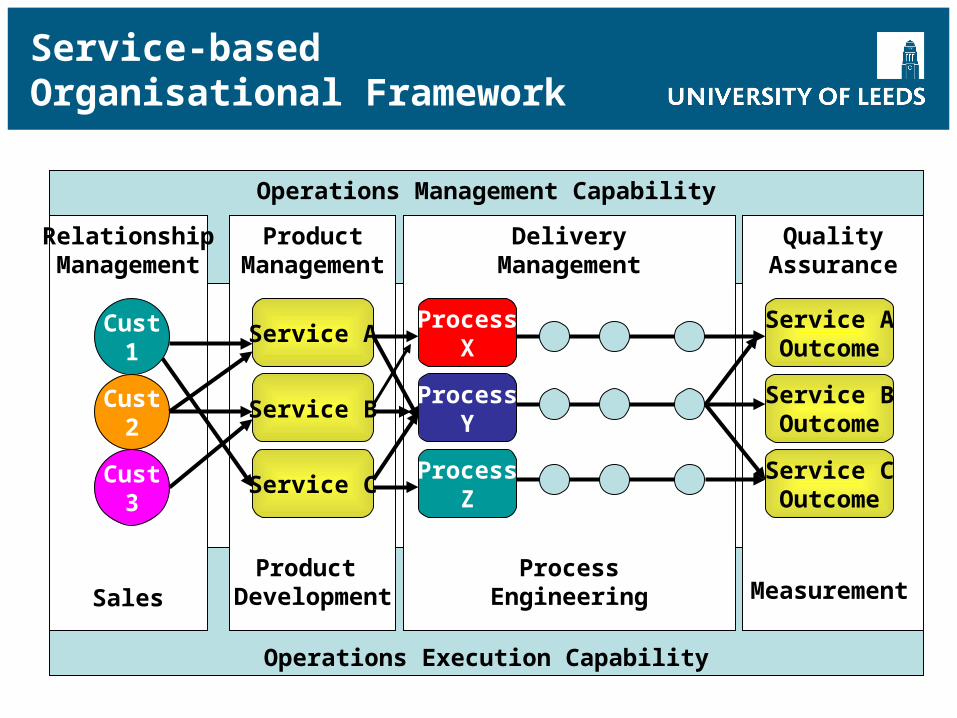
Service-based Organisational Framework
Operations Management Capability
Operations Execution Capability
RelationshipManagement
ProductManagement
DeliveryManagement
QualityAssurance
Cust1
Cust2
Cust3
Service AProcess
XService AOutcome
ProcessY
ProcessZ
Service B
Service C
Service BOutcome
Service COutcome
SalesProduct
DevelopmentProcess
Engineering Measurement
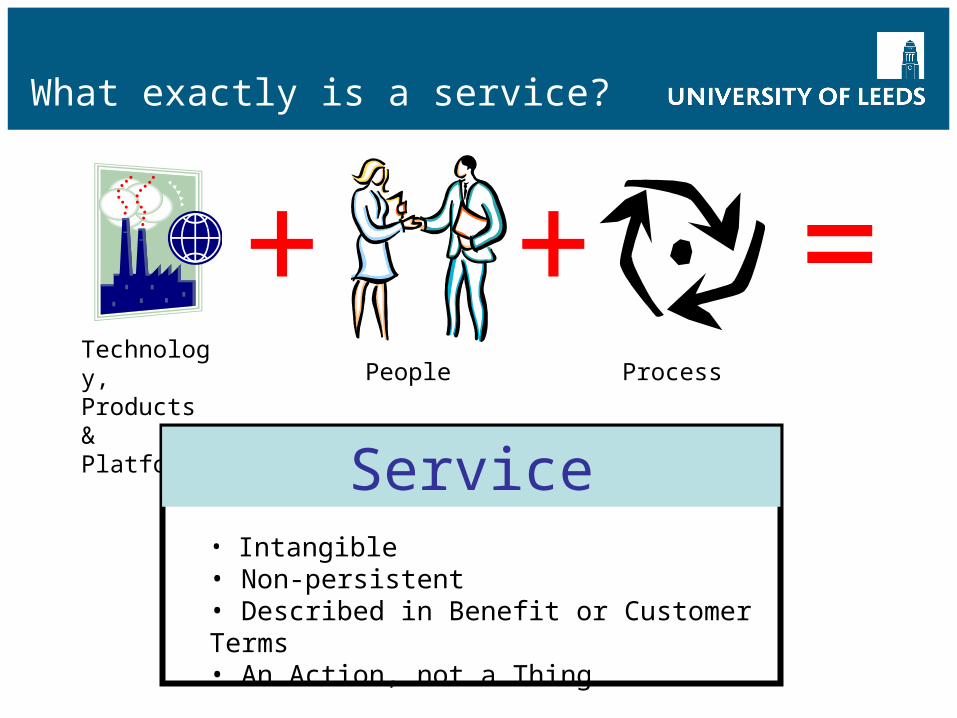
What exactly is a service?
+ + =Technology, Products & Platforms
People Process
Service• Intangible• Non-persistent• Described in Benefit or Customer Terms• An Action, not a Thing

A Service
“Giving assistance or advantage to another”
These are NOT services
What is pathology?
• Laboratory Processing• Near Patient Testing• Clinical Advisory Service• Screening Services• Chronic Disease Management• Direct Clinical Service to Patients• Training and Education• Research and Development• Clinical Audit• Policy support• ………………………….plus other services
What are the key features of good commissioning?
• Not just the responsibility of one organisation - input from wide range of people with different skills
• Strong local partnerships, e.g. – PCT, local authority– Network– local users
• Different types of commissioning, e.g.– PCT commissioning– Joint commissioning– Practice based commissioning– Network commissioning– Specialist commissioning

Supply chain management: The commissioner needs to understand the supplier and aim for mutual success on behalf of local people... understanding the cost base and the problems… the provider needs to understand the commissioners problems, aspirations, targets.
This requires honest and open lines of communication, using the right medium for the right message. Only with this can commissioners and providers deliver in partnership for communities.
Martin Barkley, Chief Executive, Hampshire Partnership NHS Trust

Knowing your place in the Service Fulfilment Chain
A
B
CD
A = ProviderB = Customer
B = ProviderC = Customer
C = ProviderD = Customer
A & B =Pathology
C =Clinician
D =PatientThere are many providers and customers
in a service fulfilment chain, but…
….. services must be expressed in terms of the ultimate end customer,
Examples of PBC Service Redesign
• Chronic obstructive pulmonary disease• Long-term conditions• Ophthalmology• Heart failure
– BNP in community– In-house ECHO
• Urology– Haematuria protocol for diagnostic tests– H.pylori
Knowledge: Commissioners need to know national policy, guidance, standards, targets. They need: a passion (or at least an interest) in the services being commissioned, to understand local needs and priorities, to be able to speak and commit on behalf of the organisation and know the service being commissioned.
Martin Barkley, Chief Executive, Hampshire Partnership NHS Trust
Pathology Commissioning
• Direct Access• Provider / Provider• Clinical contract with Trust• Specialist commissioning
Do commissioners know what to commission?
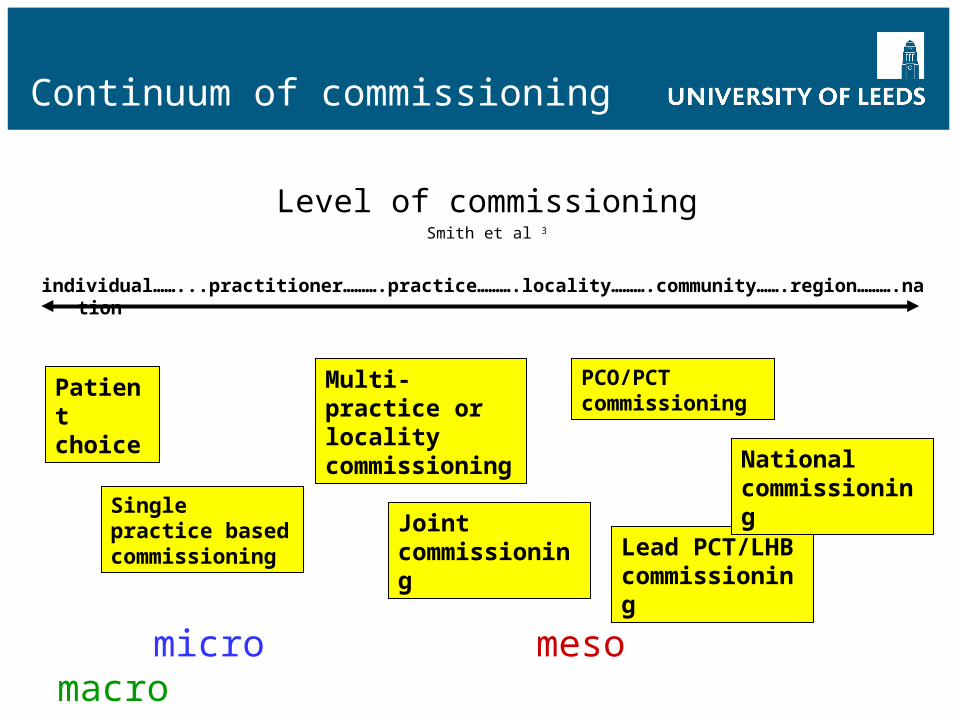
Continuum of commissioning
Level of commissioningSmith et al 3
individual……...practitioner……….practice……….locality……….community…….region……….nation
Single practice based commissioning
Patient choice
PCO/PCT commissioning
Multi-practice or locality commissioning
Joint commissioning Lead PCT/LHB
commissioning
National commissioning
micro meso macro
What SHAs will want
• Strategic Planning (major investment / configuration / workforce)
• Support for research, innovation and education / training• Help in creating new health system• System management with regulators• Performance management of PCTs / market• Possibly some tertiary level via PCT groups & networks

Commissioning Specialist Services
Example: Haemoglobinopathy screening
1. Universal neonatal screening– NHS roll out programme, funded until March 2007
2. Universal antenatal screening funded study for 2 years to screen women in Leeds / Bradford
Post 2007: PCT sign up?

What PCTs will want
• Strategic Commissioning - not short term fixes• Programmes to improve the health of the community• Reduction in inequalities - standard packages• Assurance of safe, high quality services• Managed contracts on behalf of Practices• Performance within budgets• Transparency on costs• Verification of secondary care requirements - checklists• Public engagement - informed choices• May need some community services

Commissioning Cancer Services
Example – leukaemia• Panels of cell markers• Commissioning only from laboratories who meet current
guidelines• Audit of current activity / practice• Need sufficient activity / expertise
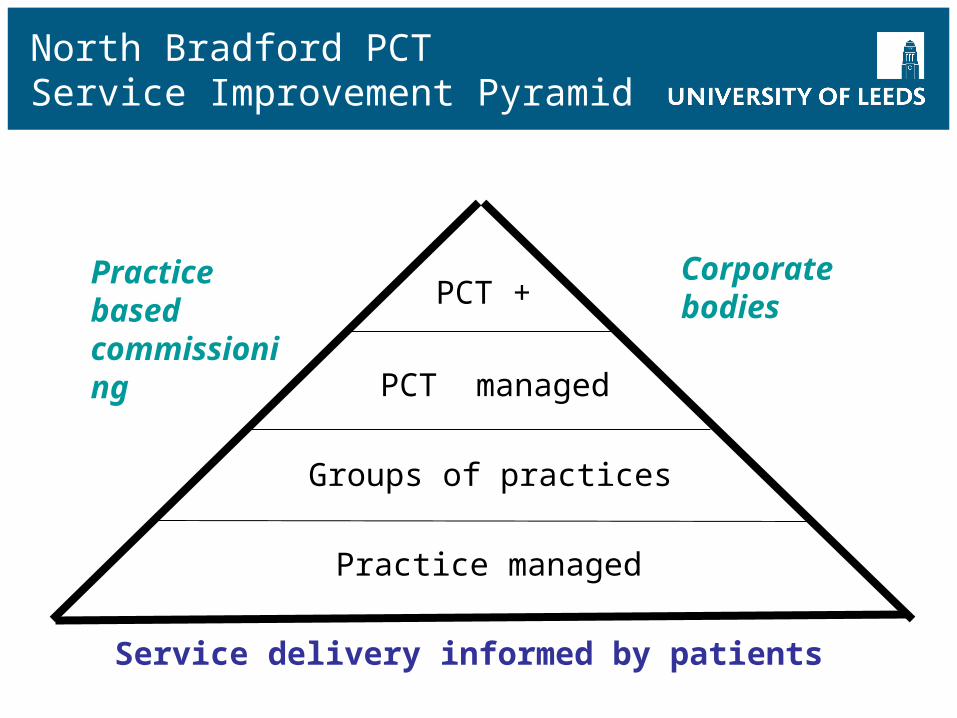
North Bradford PCT Service Improvement Pyramid
Practice managed
Groups of practices
PCT managed
PCT +
Service delivery informed by patients
Corporate bodies Practice based commissioning
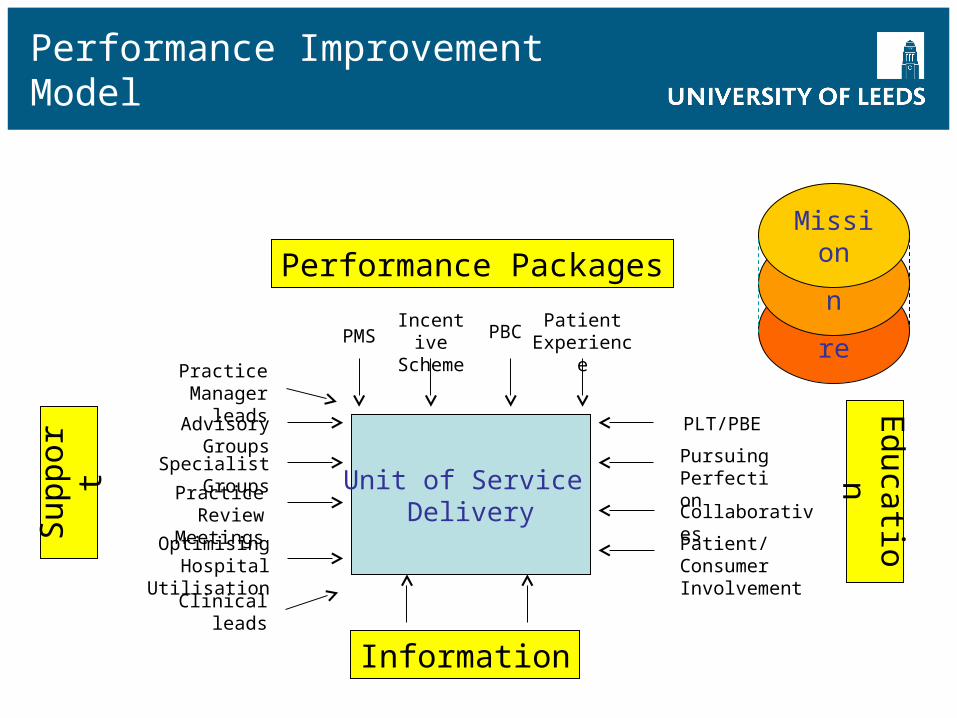
Performance Improvement Model
Unit of Service Delivery
PLT/PBE
Pursuing Perfection
Collaboratives
Educatio
n
Information
Sup
port Advisory Groups
Specialist Groups
Practice Review Meetings
Performance Packages
PMSIncentive Scheme
PBC Culture
Vision
Mission
Patient/Consumer Involvement
Optimising Hospital Utilisation
Patient Experience
Clinical leads
Practice Manager leads
What GPs Want From Pathology
• Benchmarking data (test rates)
• Integration of pathology into care pathway
• Standardised guidance, up-to-date
• Best practice guidelines
• Reduction in inappropriate testing
• Electronic requesting / reporting
• Automatic prompts
• Governance role of laboratories
• Standardisation across the patch
• POCT where appropriate
VALUE ADDED PARTNERSHIP

Must be taken at least 12 hours post chest pain




What patients will want
• Convenient and accessible services• To know why tests are being done• Tests are safe and kept to a minimum• Results in the shortest possible time• Reliable results• Information on meaning and implications of results


Putting it all together
Serv
ice
R
edes
ign
Wor
kfor
ce
Con
nect
ing
for
H
ealth
Faci
litie
s
£ Fi
nanc
ial
im
pact
Strategic commissioning objectives• Long-term conditions• Diagnostics
Enabling projects
• Elective care• Urgent care
How should pathology engage?
• Who to approach?– Trusts– PCTs– SHAs– GPs
• By what route?– Some direct – POCT, INR, DMARDS– Some indirect – clinical bundles, composite services
• What type of services to present?– Coherent - results & evidence & support– Complete – clinical answers not widgets
• Reactive or pro-active engagement?– Pro-active – now or never

Service Orientated Organisation
Users ServiceSupport
Production & Back Office
Regional
AcuteTrusts
&PCTs
National
High Volume Core
Lab
SpecialistFunctions
e.g. MolecularCytologicalScreening
Drugs
LogisticsBusinessSupport
Research / Training / DevelQuality Assurance / Audit
ClinicallyOrientated
ServiceDelivery
PatientCentric
Approach
Knowledge Management
Remember
“ A pessimist sees the difficulty in every opportunity; an optimist sees the opportunity in every difficulty”
Sir Winston Churchill

Yorkshire Centre for Health Informatics
Conclusion
Price & Jones The challenges in commissioning laboratory medicine (pathology) services.Journal of Management & Marketing in Healthcare. VOL. 1 NO. 2. PP 1–13. Jan 2008