© 1999-2013 abbey & abbey, consultants, inc. slide # 1 apc update for cy2013 version 14..0 -...
TRANSCRIPT

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 1
APC Update for CY2013
Version 14..0 - GenericNotes © 1994-2013, Abbey & Abbey, Consultants, Inc.
CPT® Codes – © 2013-2013 AMA
Sponsored By:
AACI Web Sitewww.APCNow.com
Presented By:
Duane C. Abbey, Ph.D., CFPAbbey & Abbey, Consultants, Inc.
[email protected] http://www.aaciweb.comhttp://www.APCNow.com http://www.HIPAAMaster.com

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 2
Presentation Faculty
Duane C. Abbey, Ph.D., CFP – Dr. Abbey is a healthcare consultant and educator with over 20 years of experience. He has worked with hospitals, clinics,physicians in various specialties, home health agencies and other health care providers.
His primary work is with optimizing reimbursement under various Prospective Payment Systems. He also works extensively with various compliance issues and performs chargemaster reviews along with coding and billing audits.
Dr. Abbey is the President of Abbey & Abbey, Consultants, Inc. A wide range of consulting services is provided across the country including charge master reviews, APC compliance reviews, in-service training, physician training, and coding and billing reviews.
Dr. Abbey is the author of fourteen books on health care, including:
•“Non-Physician Providers: Guide to Coding, Billing, and Reimbursement”•“Emergency Department: Coding, Billing and Reimbursement”, and •“Chargemasters: Strategies to Ensure Accurate Reimbursement and Compliance”.
Recent books include: “Compliance for Coding, Billing & Reimbursement A Systematic Approach to Developing a Comprehensive Program”, “Introduction to Healthcare Payment Systems”, “Fee Schedule Payment Systems” and “Prospective Payment Systems” from Taylor and Francis. He has just finished the fourth book in the Healthcare Payment System Series; “Cost-Based, Charge-Based and Contractual Payment Systems”.

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 3
This workshop and other material provided are designed to provide accurate and authoritative information. The authors, presenters and sponsors have made every reasonable effort to ensure the accuracy of the information provided in this workshop material. However, all appropriate sources should be verified for the correct ICD-9-CM Codes, ICD-10-CM Diagnosis Codes, ICD-10-PCS Procedure Codes, CPT/HCPCS Codes and Revenue Center Codes. The user is ultimately responsible for correct coding and billing. The author and presenters are not liable and make no guarantee or warranty; either expressed or implied, that the information compiled or presented is error-free. All users need to verify information with the Fiscal Intermediary, Carriers, other third party payers, and the various directives and memorandums issued by CMS, DOJ, OIG and associated state and federal governmental agencies. The user assumes all risk and liability with the use and/or misuse of this information.
Disclaimer

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 4
To review the 2013 updates to the key features of the APC payment system.
To appreciated the trends in modifications being made to APCs over the years.
To understand the complex nature of APCs and associated compliance issues including RAC concerns.
To appreciate the impact of proper coding and billing on APCs.
To understand the impact of the 2013 changes on the chargemaster, charges and the cost report for APCs.
To review the 2013 update on high impact areas such as observation, the Emergency Department, interventional radiology and associated areas.
To review changes to the Provider-Based Rule (PBR) for 2013.
To discuss anticipated future changes and directions for APCs.
APC Update for CY2013Objectives

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 5
APCs – Ambulatory Payment Classifications APGs – Ambulatory Patient Groups ASC – Ambulatory Surgical Center CAH – Critical Access Hospital CCRs – Cost-to-Charge Ratios CPT – Current Procedural Terminology E/M – Evaluation and Management FFS – Fee-for-Service HCPCS – Healthcare Common Procedure Coding System ICD-9-CM – International Classification of Diseases, Ninth Edition, Clinical MAC – Medicare Administrative Contractor MedPAC – Medicare Advisory Commission MPFS – Medicare Physician Fee Schedule NCCI – National Correct Coding Initiative AWV – Annual Well Visit PPPS – Personalized Preventive Plan Services
APC Update for CY2013Acronyms/Terminology

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 6
NCD/LCD – National/Local Coverage Decision NTIOL –New Technology Intraocular Lens OCE – Outpatient Code Editor OPD – [Hospital] Outpatient Department OPPS – [Hospital] Outpatient Prospective Payment System PHP – Partial Hospitalization Program PM – Program Memorandum PPS – Prospective Payment System QIO – Quality Improvement Organization SI – Status Indicator ASC – Ambulatory Surgical Center RBRVS – Resource Based Relative Value System MPFS – Medicare Physician Fee Schedule Developed through RBRVS VBP – Value Based Purchasing PCR – Payment to Cost Ratio
Note: The Federal Register entry has pages of acronyms!
APC Update for CY2013Acronyms/Terminology

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 7
APC Update for CY2013General Comments
APCs are becoming increasingly complex and more difficult to understand. Enormous Federal Register entries are now the norm.
APCs represent a payment system that is out of control. Significantly increased bundling through packaging is still being added.
APCs appear to be moving back toward APGs. There are wide variations in payments from year to year. Significant compliance concerns exist within the overall APC payment
system. In some cases these compliance concerns result because of lack of
explicit guidance from CMS. At some point the RAC auditors will become more involved in APCs.
APCs and the underlying coding systems (i.e., CPT and HCPCS) generate constant change and the need to update.
Tracking and verifying that correct payment is received is difficult. It is critical to track adjudication and overall payment.
Major issues with hospital charges, CCRs and the cost report are present.
Federal Register Fanatics Look for how many times the word ‘believe’ is used by CMS. What are you allowed to ‘believe’?

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 8
APC Update for CY2013General Comments
Note: All citations to the Federal Register are to the Examination Copy that was released on November 1, 2012. Official publication was on November 15, 2012. Note that implementation is January 1, 2013. Page numbers are provided as reference, again from the Examination Copy.
There are a few references in the notes to the November 1, 2011 Federal Register from last year. Page numbers plus the 1525-FC reference is for last years Federal Register.
This Federal Register entry discusses a number of different topics. Not all the topics discussed necessarily relate to APCs (Ambulatory Payment Classifications). HOPPs ASC – Payment and Quality Reporting Electronic Reporting Pilot Inpatient Rehabilitation Facilities Quality Reporting Revision to Quality Improvement Organization Regulations
Also, there are some hospital related topics discussed in the November 16, 2012 Federal Register for the Medicare Physician Fee Schedule. See new reporting requirements for PT/OT/ST. Technically, these are not part of APCs or HOPPS.

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 9
APC Fundamentals Encounter Driven System
• Some Exceptions – Example: Two separate blood transfusions on the same day or two imaging services at different times on the same day.
CPT/HCPCS Code Driven
• If the service is not coded with a CPT or HCPCS (and/or proper modifiers), then there will be absolutely no payment!
APC Grouper Multiple APCs from Given Claim Inpatient-Only Procedures
• Surgery, if performed outpatient, will not be paid at all! (Patient Liability?)
• How is this list determined? Covered, Non-Covered and Payment System Interfaces
• Example: Self-Administrable Drugs Pass-Through Payments – Directly Based on Charges Made – Covert
Charges to Costs How? (Hint: Cost-to-Charge Ratios)
APC Update for CY2013APC Background Information

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 10
APC Weight, and Thus Payment, Determination Hospital Charges Converted to Costs
• How is this done?
• Do we charge for everything?
• Do we charge correctly for everything? Statistical Process Using the Costs
• Geometric Mean
• Mean Cost for Given APC/Mean Cost for All APCs = the APC Weight Variation of Costs Within a Given APC Category
• 2-Times Rule – “ … if the median cost of the highest cost item or service within an APC group is more than 2 times greater than the median of the lowest cost item or service within that same group.” (Page 368 – CMS-1525-FC)
• 2-Times Rule Exception List Examples:
o 0057 Bunion Procedures
o 0325 – Group Psychotherapy
APC Update for CY2013APC Background Information

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 11
Use of Claims to Statistically Develop the APC Weights
Because outpatient encounters often involve multiple services, the APC grouping process often (if not a majority of the time) generates multiple APCs.
CMS can use only pure claims, that is, claims that group to a single APC. These are called ‘singleton’ claims.
CMS is trying very hard to get around this situation because many of the claims filed by hospitals never get considered when the actual APC weights are determined.
• Small Example: CPT=86891 – Intra- or Post-Operative Blood Salvage
A device is used to save blood, reprocess the blood and generally re-infuse.
Is it possible to have ONLY 86891 on a claim? What kind of payment do we have for 86891? What are the costs involved?
APC Update for CY2013APC Background Information

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 12
APC Cost Outliers Complicated Two-Tiered Formula Based on Excessive Costs - How are costs determined? Nationally, does CMS make full outlier payments?
Provider-Based Rule (42 CFR §413.65) Provider-Based Clinics Provider-Based Clinical Services Potentially, two claim forms filed – CMS-1450 (UB-04) for technical
component and CMS-1500 (1500) for professional component. Reduction in payment for professional component
• Site-of-Service Differential in RBRVS (MPFS)
• Place-of-Service (POS) driven on CMS-1500 Series of Criteria to Meet If to be Provider-Based
• On-Campus versus Off-Campus
• See Physician Supervision Developments Important Changes in rules, regulations and interpretations.
APC Update for CY2013APC Background Information

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 13
APC Update for CY2013APC Background Information
APC Advisory Panel
CMS has developed an ever expanding APC Advisory Panel which they are now extending to a super panel to determine appropriate supervisory levels.
“The Data Subcommittee is responsible for studying the data issues confronting the APC Panel and for recommending options for resolving them. The Visits and Observation Subcommittee reviews and makes recommendations to the APC Panel on all technical issues pertaining to observation services and hospital outpatient visits paid under the OPPS (for example, APC configurations and APC payment weights). The Subcommittee for APC Groups and SI Assignments advises the Panel on the following issues: the appropriate SIs to be assigned to HCPCS codes, including but not limited to whether a HCPCS code or a category of codes should be packaged or separately paid; and the appropriate APCs to be assigned to HCPCS codes regarding services for which separate payment is made.” (Page 47 – CMS-1525-FC)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 14
ASCs – Ambulatory Surgical Centers In CY2008 CMS Started a Hybrid of APCs and RBRVS FR entries for APCs will now also be for ASCs ASC Surgery List
• Regular ASC Surgeries
• Office-Based Surgeries New Additions
• Conditions for Coverage (CfCs) New Acronym
• Additions and Deletions to Lists Payment Formula
• ASC Surgery 65% of APC
• Office-Based Surgeries – Lesser of: 65% of APC or Non-Facility PE RVU from MPFS
• Physician Paid Facility MPFS (As With Hospitals) Separate Payment for Certain Ancillary Services Did all the features of APCs translate over?
APC Update for CY2013APC Background Information
© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 15
APC Update for CY2013By The Numbers
Basically a 1.8% Market Basket Update Several Factors Involved Conversion Factor = $71.313 versus $70.016 for CY2012 (+1.85%) Assumes Quality Reporting Further 2.0% reduction if not. Supposedly 2.60% - 0.70% - 0.10% = 1.80%
Wage Index Changes See IPPS Statewide CCRs See Table 8 – Interesting Just To Peruse SCHs 7.10% Increase on Budget Neutral Basis (Includes EACHs) Cost Outlier
Fixed Threshold from $2,175.00 for CY2010 to $2,025.00 for CY2011 to $1,900.00 for CY2012 to $2,025.00 for CY2013
• This is a fairly significant decrease. What is happening? Labor-Related Calculation Remains the same. Co-Payment Amounts
Still struggling to get to the target of a 20% coinsurance to calculate the copayment amount.
Drug Packaging Threshold $60.00 for CY2009 moved to $65.00 for CY2010 and $70.00 for CY2011
to $75.00 for CY2012 and for CY2013 it is $80.00. Final ASC Conversion Factor - $41.401 ($41.401/$71.313 = 58.05%)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 16
APC Update for CY2013By The Numbers
TOPs – Transitional Outpatient Payment “Effective for services provided on or after March 1, 2012, SCHs
(including EACHs) with greater than 100 beds are no longer eligible for TOPs, in accordance with section 308 of Pub. L. 112-78. Effective for services provided on or after January 1, 2013, a rural hospital with 100 or fewer beds that is not an SCH and an SCH (including an EACH) are no longer eligible for TOPs, in accordance with section 3002 of Pub. L. 112-96. (Page 300)
For SCHs (including EACHs), the 7.1% increase will continue. See also, Children’s Hospitals and Cancer Hospitals
Wage Index “In response to concerns frequently expressed by providers and other
relevant parties that the current wage index system does not effectively reflect the true variation in labor costs for a large cross-section of hospitals, two studies were undertaken by the Department.” (Page 285)
“After consideration of the public comments we received, we are finalizing our policy to adopt the FY 2013 IPPS wage index for the CY 2013 OPPS in its entirety, including the rural floor, geographic reclassifications, and all other wage index adjustments. (Page 287)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 17
APC Update for CY2013By The Numbers
SCH and Rural Hospitals
“After consideration of the public comments we received, we are finalizing our CY 2013 proposal, without modification, to apply the 7.1 percent payment adjustment to rural SCHs, including EACHs, for all services and procedures paid under the OPPS in CY 2013, excluding separately payable drugs and biologicals, devices paid under the pass-through payment policy, and items paid at charges reduced to costs.” (Page 303)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 18
APC Update for CY2013By The Numbers
Statewide Average Default CCRs (Samples)
CY2013 CY2012
ARIZONA RURAL 0.238 0.237
ARIZONA URBAN 0.190 0.190
FLORIDA RURAL 0.182 0.182
FLORIDA URBAN 0.167 0.164
IOWA RURAL 0.296 0.296
IOWA URBAN 0.269 0.269
TEXAS RURAL 0.235 0.236
TEXAS URBAN 0.206 0.196
For chargemaster coordinators these default CCRs can be quite interesting relative to a given hospitals pricing strategies.

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 19
APC Update for CY2013Recalibration of APC Relative Weights
Recalibration and Rebasing Process OPPS Update Federal Registers – Typically Long Discussions Calculation of Geometric Costs Within APC Categories Single Procedure Claims versus Multiple Procedure Claims
• Methodology Carried Over From DRGs – Doesn’t Really Work• Pseudo Single Procedure Claims• Bypass Codes
CCRs – Cost-to-Charge Ratios from Cost Reports• See Revenue Code-to-Cost Center Crosswalk• CT & MRI Equipment – Major Moveable vs. Building Equipment
Device Dependent APCs – Expensive Implant or Supply Item Is Larger than Payment for Service
Blood and Blood Products Still Equalizing Payments Due To Incorrect CCRs
Updated CPT/HCPCS Codes Updated Status Indicators Affecting Packaging
• See Also – Packaged Revenue Codes – Table 2 Payment Variations See 2-Times Rule + Payment Change Limitations Composite APCs Observation, Pulmonary Rehab, Etc.

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 20
APC Update for CY2013Recalibration of APC Relative Weights
For recalibration of the APC weights, the BIGGEST change is that CMS is moving from using the ‘median’ as a measure of central tendency over to the ‘geometric mean’. What is the geometric mean?
• Arithmetic Mean – Add the Data Points and Divide by the Number of Data Points
• Geometric Mean – Multiply the Data Points and Take the Nth Root where N is the number of data points.
Data Set #1: 1, 2, 3, 6, 7, 8, 15 Data Set #2: 1, 1, 2, 4, 6, 9, 11, 18, 21
So what does all this mean? Need to run case-mix models.
Median ArithmeticMean
GeometricMean
Data Set #1 6.0000 6.0000 4.3660
Data Set #2 6.0000 8.1111 4.9537

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 21
APC Update for CY2013Recalibration of APC Relative Weights
Recalibration and Rebasing Process New Codes – CPT and HCPCS
• CMS discusses new codes implemented throughout the year along with addressing new CPT/HCPCS codes.
• See also assignment or reassignment of Status Indicator codes. Multiple Imaging Families – Started in CY2009
• Significant Concerns By Hospitals• Continue with the Composite APCs (8004-8008)
Packaging Services• See SI=“Q1”, “Q2”, and “Q3”• Dependent and Independent Methodology
CMS continues to discuss and apply the concept of dependent services and independent services. Ultimately, dependent services should be bundled (packaged) into independent services.
While this is an adjudication issue for the APC Grouper, it is the same concept as ‘separate procedure’ at the CPT coding level.
© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 22
As usual there are hundreds of changes for both CPT and HCPCS. With the exception of laboratory codes, the rate of change for 2013 is in a fairly normal range.
However, some of the CPT changes have a significant impact on APC grouping and the logic in the I/OCE (Integrated Outpatient Coded Editor).
For new codes and code sets that are not available at the time of the proposed changes to APCs, there is a comment period after the final rule is issues.
Category III Codes 0302T-0307T – Intra-cardiac Ischemia Monitoring 0308T – Ocular Telescope Prosthesis
Psychiatric Services CPT Deleted 28 Psychiatric Codes CPT Added 12 New CPT Codes With Add-On Logic
• See 90791-90840• Timing Issues Relative to Coding
APC Update for CY2013CPT/HCPCS Changes For CY2013

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 23
APC Update for CY2013CPT/HCPCS Changes For CY2013
Partial Hospitalization Billable Codes
RC Description CPT/HCPCS Codes
043X Occupational Therapy G0129
0900 Behavioral Health Tx 90791 or 90792
0904 Activity Therapy G0176
0914 Individual Psychotherapy 90785, 90832, 90833, 90834, 90836, 90837,90838, 90845, 90865,
or 90880
0915 Group Therapy G0410 or G0411
0916 Family Psychotherapy 90846 or 90847
0918 Psychiatric Testing 96101, 96102, 96103, 96116, 96118, 96119,or 96120
0942 Education/Training G0177
• Table 43 Page 719

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 24
APC Update for CY2013CPT/HCPCS Changes For CY2013
Cardiovascular Stenting 92980-92981
• Replaced with a new series of codes – 92928 – Stent + Coronary Angioplasty Major Branch 92933 – Stent + Atherectomy Major Branch 92934 – Stent + Atherectomy Additional Branch 92937 – Bypass Graft – Stent + 92938 - Bypass Graft – Stent + 92941 – Acute Artery Bypass 92943 – Total Occlusion – Single Vessel 92944 – Total Occlusion – Additional Vessel
• Now codes are needed to address drug-eluting stents for APCs G0290 & G0291 are Deleted New Sequence – C9600-C9608
• “The interim APC assignment for CPT codes 92928, 92933, 92929, 92934, 92937, 92938, 92941, 92943, and 92944 is APC 0104 ($6,114.44), and the interim APC assignment for HCPCS codes C9600, C9601, C9602, C9603, C9604, C9605, C9606, C9607, and C9608 is APC 0656 ($7,763.18) for CY 2013.” (Page 113)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 25
APC Update for CY2013CPT/HCPCS Changes For CY2013
Transitional Care Management CPT 99495 APC 0605 - $73.68 (See Also MPFS)
• Communication (direct contact, telephone, electronic) with the �patient and/or caregiver within 2 business days of discharge;
• Medical decision-making of at least moderate complexity during the �service period; and
• Face-to-face visit, within 14 calendar days of discharge.� CPT 99496 APC 0606 - $96.96 (See Also MPFS)
• Communication (direct contact, telephone, electronic) with the patient and/or caregiver within 2 business days of discharge;
• Medical decision-making of high complexity during the service period; and
• Face-to-face visit, within 7 calendar days of discharge. “Transitional care management is comprised of one face-to-face visit
within the specified timeframes, in combination with non-face-to-face services that may be performed by the physician or other qualified health care professional and/or licensed clinical staff under his or her direction.” (Page 681)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 26
APC Update for CY2013Composite APCs – Issues and Changes
Composite APCs Observation – APC=8002 and APC=8003
• See Minor Surgery – Status Indicator “T” Bundling Issue Issue has been presented and noted in the Federal Register.
Next year??• APC 8002 $440.07/$393.15/$394.22/$381.34 • APC 8003 $798.47/$720.64/$714.33/$705.27
LDR Prostate Brachytherapy – APC=8001• CPT=55875+77778• CY2013 $3,254.67 CY2012 $3,339.98; CY2011 $3,229.24
Electrophysiology Studies – APC=8000• APC 8000 $11,145.72/$11,311.28/$10,787.46/$10,118.25• Problematic Area – High variability of services, thus costs.
Mental Health Services – APC=0034• See Payment Limit for APC=0176 (Full Day Partial Hospitalization)• APC 0034 - $191.13/$238.33/$210.89 Wow, significant decrease!
Multiple Imaging – APCs – 8004, 8005, 8006, 8007, 8008• Be certain to check code classifications
Cardiac Resynchronization Therapy Composite APC 0108 - $30,680.01• See Federal Register Discussion Starting on Page .

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 27
APC Update for CY2013On-Going APC Issues
Variation Within APC Categories 2-Times Rule Statistical Measure of Too Much Variation
• “… the median cost of the highest cost item or service within an APC group is more than 2 times greater than the median of the lowest cost item or service within that same group.” (Page 395 – CMS-1504-FC)
• Question: How many years can an APC be repeatedly on the list?
• How is this affecting you? 0057 Bunion Procedures 0045 – Bone/Joint Manipulation under Anesthesia 0060 Manipulation Therapy 0148 – Level I Anal/Rectal Procedures 0272 - Fluoroscopy 0325 – Group Psychotherapy

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 28
APC Update for CY2013On-Going APC Issues
Variation Within APC Categories 0006 Level I Incision & Drainage 0012 Level I Debridement & Destruction 0045 Bone/Joint Manipulation Under Anesthesia 0057 Bunion Procedures 0060 Manipulation Therapy 0105 Repair/Revision/Removal of Pacemakers, AICDs, or Vascular Devices 0148 Level I Anal/Rectal Procedures 0152 Level I Percutaneous Abdominal and Biliary Procedures 0230 Level I Eye Tests & Treatments 0254 Level V ENT Procedures 0272 Fluoroscopy 0325 Group Psychotherapy 0330 Dental Procedures 0340 Minor Ancillary Procedures 0369 Level III Pulmonary Tests 0403 Level I Nervous System Imaging 0409 Red Blood Cell Tests 0688 Revision/Removal of Neurostimulator Pulse Generator Receiver 0690 Level I Electronic Analysis of Devices

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 29
APC Update for CY2013On-Going APC Issues
2 Times Rule
Several APCs No Longer Violate the 2-Times Rule
• APC 0128 (Echocardiogram with Contrast)
• APC 0173 (Level II Partial Hospitalization (4 or more services) for CMHCs)
• APC 0604 (Level 1 Hospital Clinic Visits)
• APC 0655 (Insertion/Replacement/Conversion of a Permanent Dual Chamber Pacemaker or Pacing)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 30
APC Update for CY2013On-Going APC Issues
New Technologies CMS provides a generalized discussion of the goals and objectives for
the new technology payments. CMS makes it fairly clear that they have no intention of paying for expensive capital equipment that may have low utilization during the startup years for a new, high technology, service.
Movement from New Technologies to Clinical APCs• G0417-G0419 Surgical pathology prostate needle saturation
Assign to APC 0661 (Level V Pathology) Device Payment
Pass-Through Expiration Dates See FB and FC Modifiers See Table 29 for Offsets See Table 30 for Listing of Affected Devices Device Dependent APCs No Cost/Full Credit and Partial Credit Hospitals, overall, tend to undercharge for devices. See issues such as
charge compression.

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 31
APC Update for CY2013On-Going APC Issues
Device Payment
“As the commenter noted, the offset reduction may actually be much greater or much less than the credit received by the hospital, depending upon the component that was credited. As we have stated in the past (76 FR 74282), we recognize that, in some cases, the estimated device cost and, therefore, the amount of the payment reduction will be more or less than the cost a hospital would otherwise incur. However, because averaging is inherent in a prospective payment system, we do not believe this is inappropriate.” (Page 535)
See APC 0107 and 0108 Description Changes
• 0107 – Level I Implantation of Cardioverter-Defibrillator
• 0108 – Level II Implantation of Cardioverter-Defibrillator

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 32
APC Update for CY2013On-Going APC Issues
Blood/Blood Products
Question About Pre-Storage Pooled, Leukocyte Reduced Platelets
“Some commenters expressed concern that the proposed APC payment rates for some blood products are less than the acquisition costs of those products, citing a published study of a national survey of blood acquisition and overhead costs. According to the commenters, the safety and availability of blood may be jeopardized without adequate payment. The commenters asked that CMS formally consider and evaluate potential alternative methodologies for setting APC payment rates for blood products, preferably by seeking input from affected stakeholders. The commenters also stated that the use of the geometric mean methodology to calculate blood costs would result in lower payment rates compared to the use of median costs to calculate the payment rates for blood and blood products and urged CMS to use the median cost instead.” (Page 123)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 33
APC Update for CY2013On-Going APC Issues
Blood/Blood Products
“After consideration of the public comments we received, we are finalizing our proposed policy, without modification, to continue to establish payment rates for blood and blood products using our blood-specific CCR methodology, which utilizes actual or simulated CCRs from the most recently available hospital cost reports to convert hospital charges for blood and blood products to costs, for CY 2013. We continue to believe that this methodology in CY 2013 will result in costs for blood and blood products that appropriately reflect the relative estimated costs of these products for hospitals without blood cost centers and, therefore, for these blood products in general.” (Pages 125-126)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 34
APC Update for CY2013On-Going APC Issues
Specific APC Categories – Payment and Code Mappings (Examples) Each year CMS devotes significant discussion to APC assignments and
mapping of codes. Cardiovascular and Vascular Services
• Cardiac Telemetry (APC 0213)• Mechanical Thrombectomy (APC 0653)• Non-Congenital Cardiac Catheterization (APC 0080)• Endovascular Revascularization of the Lower Extremity (APCs
0083, 0229, and 0319)• External Electrocardiographic Monitoring (APC 0097)• Echocardiography (APCs 0177, 0178, 0269, 0270, and 0697)
Gastrointestinal Services• Laparoscopic Adjustable Gastric Band (APC 0132)• Transoral Incisionless Fundoplication (APC 0422)• Gastrointestinal Transit and Pressure Measurement (APC 0361)
Integumentary System Services• Extracorporeal Shock Wave Wound Treatment (APC 0340)• Application of Skin Substitute (APCs 0133 and 0134)• Low Frequency, Non-Contact, Non-Thermal Ultrasound (APC 0015)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 35
APC Update for CY2013On-Going APC Issues
Specific APC Categories – Payment and Code Mappings (Examples) Nervous System Services
• Scrambler Therapy (APC 0275)• Transcranial Magnetic Stimulation Therapy (TMS) (APC 0216)• Paravertebral Neurolytic Agent (APC 0207)• Programmable Implantable Pump (APC 0691)• Revision/Removal of Neurostimulator Electrodes (APC 0687)
Radiation Oncology Services• Proton Beam Therapy (APCs 0664 and 0667)• Device Construction for Intensity Modulated Radiation Therapy
(IMRT) (APC• 0305)• Other Radiation Oncology Services (APCs 0310 and 0412)• Stereotactic Radiosurgery (SRS) Treatment Delivery Services (APCs
0065, 0066, 0067 and 0127)• Intraoperative Radiation Therapy (IORT) (APC 0412)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 36
APC Update for CY2013On-Going APC Issues
Drugs, Biological, and Radiopharmaceuticals Payable Drugs – ASP+6 Transitional Pass-Through Payment Process
• Drugs Expiring• New Drugs on the List• Nuclear Medicine Concerns• Contrast Agent Offset
Packaging Criteria Packaging Threshold - $80.00 CMS Posting Offset Amounts for All Affected APCs Policy-Packaged Drugs and Devices 340B Hospitals – Data Considerations “After consideration of the public comments we received, we are
finalizing our proposals, without modification, to continue to package payment for all nonpass-through diagnostic radiopharmaceuticals and contrast agents, and implantable biologicals that are surgically inserted or implanted into the body through a surgical incision or a natural orifice, regardless of their per day costs.” (Page 268)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 37
APC Update for CY2013On-Going APC Issues
Drugs, Biological, and Radiopharmaceuticals
“We note that although it is CMS’ longstanding policy under the OPPS to refrain from instructing hospitals on the appropriate revenue code to use to charge for specific services, we continue to encourage hospitals to bill all drugs and biologicals with HCPCS codes, regardless of whether they are separately payable or packaged, and to ensure that drug costs are completely reported, using appropriate revenue codes. We also note that we make packaging determinations for drugs and biologicals annually based on cost information reported under HCPCS codes, and the OPPS ratesetting is best served when hospitals report charges for all items and services with HCPCS codes when they are available, whether or not Medicare makes separate payment for the items and services.” (Page 701 – CMS-1525-FC)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 38
APC Update for CY2013On-Going APC Issues
Brachytherapy Sources – See Various A-Codes and C-Codes Congressional Mandate – Pay Separately
• Otherwise CMS would probably package these sources into the associated service.
Pass-Through Payment (Sort Of) Up To CY2009 – SI=“H” “K” “U”• CMS’s interpretation of ‘charges adjusted to cost’ is interesting.
CMS Has Developed a Discrete ‘Mini’ APC System for Sources “After consideration of the public comments we received, we are
finalizing our proposal to pay for brachytherapy sources at prospective payment rates based on their source-specific median costs for CY 2012.” (Page 165 – CMS-1525-FC)
“Consistent with our policy regarding APC payments made on a prospective basis, we are finalizing our proposal to subject the cost of brachytherapy sources to the outlier provision of section 1833(t)(5) of the Act, and also to subject brachytherapy source payment weights to scaling for purposes of budget neutrality.” (Page 165-166 – CMS-1525-FC)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 39
APC Update for CY2013On-Going APC Issues
Brachytherapy Sources – See Various A-Codes and C-Codes Commenter Concerns:
• “First, some commenters claimed that there are longstanding problems with OPPS claims data for brachytherapy source payment.” (Page 129)
• “Second, commenters stated that brachytherapy source payments proposed for CY 2013 are unstable and fluctuate significantly from CY 2012 levels.” (Page 130)
CMS Responses• “ … under the budget neutral provision for the OPPS, it is the
relativity of costs of services, not their absolute costs, that is important, and we believe that brachytherapy sources are appropriately paid according to the standard OPPS payment approach.” (Page 132)
• “After consideration of the public comments we received, we are finalizing our proposal to pay for brachytherapy sources at prospective payment rates based on their source-specific geometric mean costs for CY 2013.” (Page 136)
© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 40
APC Update for CY2013On-Going APC Issues
APC Cost Outliers
“In summary, for CY 2013, we will continue to make an outlier payment that equals 50 percent of the amount by which the cost of furnishing the service exceeds 1.75 times the APC payment amount when both the 1.75 multiple threshold and the final fixed-dollar threshold of $2,025 are met. For CMHCs, if a CMHC’s cost for partial hospitalization services, paid under either APC 0172 or APC 0173, exceeds 3.40 times the payment rate for APC 0173, the outlier payment is calculated as 50 percent of the amount by which the cost exceeds 3.40 times the APC 0173 payment rate. We estimate that this threshold will allocate 0.12 percent of outlier payments to CMHCs for PHP outlier payments. (Page 321)
CMS continues to work toward a 1% overall limitation on cost-outlier payments. Thus the fixed dollar amount will typically change each year based on experience.

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 41
APC Update for CY2013On-Going APC Issues
Drug Administration Services An area of considerable changes over the last several years. Coding and Charge Capture Difficulties APC Panel Recommendation – Pay separately for CPT 96368 and 93676,
that is, concurrent infusion and additional pushes.
• CMS has rejected this recommendation and will continue with the five level APC structure for injections and infusions.
See also slight changes in guidance from CPT.
APC CY2013 CY2012 CY2011 CY2010 CY2009
0436 $27.01 $24.82 $26.35 $25.67 $25.03
0437 $39.13 $34.81 $36.88 $37.44 $36.66
0438 $74.69 $72.73 $75.58 $75.69 $74.32
0439 $146.24 $126.71 $128.44 $126.78 $126.80
0440 $230.50 $207.80 $205.86 $219.96 $191.06

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 42
APC Update for CY2013On-Going APC Issues
Partial Hospitalization Services Hospitals vs. CMHCs
• Two Tiered Costs Structure – Cost Report Data HCRIS• Two Sets of APCs – Status Indicator “P”
APC=0172/0173 Level I and II at CMHC APC=0175/0176 Level I and II at Hospital
“For hospital-based PHPs, the per diem costs would increase from approximately $164 under the current median-based methodology to approximately $183 under the proposed geometric mean-based methodology for Level I services, and from approximately $225 to approximately $233 for Level II services.” (Page 695 – CMS-1589-FC)
APC CY2013 CY2012 CY2011 CY2010
0172 $84.96 $97.63 $129.64 $149.84
0173 $109.67 $113.81 $164.43 $210.89
0175 $180.71 $160.71 $204.89 [$149.84]
0176 $228.26 $191.13 $238.33 [$210.89]

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 43
APC Update for CY2013On-Going APC Issues
Partial Hospitalization Services Cost Report Data for CMHCs Through HCRIS
• Note the significant difference in reimbursement (determined via costs) between hospitals and CMHCs.
• “A few commenters expressed concerns that the technical data on which CMS relies during the rate setting process are fundamentally flawed, in that the data do not reflect the full scope of CMHC costs. These commenters also stated that, due to insufficient cost reporting instructions for CMHCs, they continue to incorrectly exclude owner’s salary costs from their cost reports, contributing to their low median costs.” (Page 797 – CMS-1525-FC)
Separate Cost Outlier Payments to CMHCs• “Specifically, we proposed to establish that if a CMHC's cost for
partial hospitalization services, paid under either APC 0172 or APC 0173, exceeds 3.40 times the payment for APC 0173, the outlier payment would be calculated as 50 percent of the amount by which the cost exceeds 3.40 times the APC 0173 payment rate.” (Pages 800-801 – CMS-1525-FC)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 44
APC Update for CY2013On-Going APC Issues
Partial Hospitalization Services
Significant Coding Changes – See AMA
• “Effective January 1, 2013, CPT codes 90801 and 90802 will be deleted and the E/M services will be billed using the following CPT codes: CPT code 90791 (Psychiatric diagnostic evaluation (no medical services) when completed by a nonphysician) and CPT code 90792 (Psychiatric diagnostic evaluation (with medical services) when completed by a physician).” (Page 713)
See Table 42 For Crosswalks From Old To New CPT Codes
• CPT 90801 CPT 90791 or CPT 90792 (w/o and w Medical Services)
• CPT 90817 E/M Code (Not on Time) + 90833 add-on code
• CPT 90824 E/M Code (Not on Time) + 90833 (30 minute add-on) + 90785 (Interactive Add-On Code w/ patient and/or family)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 45
APC Update for CY2013On-Going APC Issues
Inpatient-Only Procedures “The inpatient list specifies those services for which the hospital will
be paid only when provided in the inpatient setting because of the nature of the procedure, the underlying physical condition of the patient, or the need for at least 24 hours of postoperative recovery time or monitoring before the patient can be safely discharged.” (Page 8902 – CMS-1525-FC)
Commenters continue to recommend doing away with this list.
• “Many commenters suggested that the inpatient only list be eliminated in its entirety. The commenters indicated that hospitals already meet minimum safety standards through Joint Commission accreditation and the Medicare hospital conditions of participation. Commenters suggested that, if the inpatient only list cannot be eliminated in its entirety, an appeals process be developed. Commenters believed that an appeal process would give the hospital the opportunity to submit documentation on the physician’s intent, the patient’s clinical condition, and the circumstances that enabled the patient to be sent home safely without an inpatient stay.” (Page 810 – CMS-1525-FC)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 46
APC Update for CY2013On-Going APC Issues
Inpatient-Only Procedures Deletions from the List
• Only two codes were proposed for removal from the list: CPT 22856 – Total Disc Arthroplasty CPT 27447 – Knee Arthroplasty
• Commenters were significantly opposed to removing CPT 27447 from the list. CMS has conceded and this code will stay on the list.
Note that the procedures on the list are determined in part on a statistical basis and not purely on a clinical basis. This list must be carefully reviewed each year. 39 Codes Were Requested to be Removed.
• Watch for Carotid Stenting – This will probably be removed from the list at some point in the near future. (See CY2010)
“Commenters further noted that performing total knee arthroplasty in the outpatient setting may impact the types of rehabilitation services available to patients upon completion of the surgery, and may make justifying the medical necessity of inpatient rehabilitation more difficult. Furthermore, commenters expressed concern that commercial carriers will change total knee arthroplasty to an outpatient procedure, thereby making it more difficult to get such a procedure authorized.” (Page 727)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 47
APC Update for CY2013On-Going APC Issues
“-CA” Modifier – APC=0375 APC 0375 - Ancillary Outpatient Services When Patient Expires
• Example: Patient rushed to hospital ED, taken to surgery and then expires without being admitted to hospital.
• Blanket payment for various types of procedures. Better Database and Proper Utilization
• CY2013 $6,612.29
• CY2012 $6,038.66
• CY2011 $6,372.10
• CY2010 $5,965.94
• CY2009 $4,770.52 Question: Why don’t we use a process similar to the “-CA” modifier for
inpatient only procedures that are inadvertently performed on an outpatient basis?
• We could do away with the inpatient-only list, and at least there would be a default average payment for such services instead of making then the patient’s liability.

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 48
APC Update for CY2013Physician Supervision Changes
Starting in CY2008 the Issue of Physician Supervision Took On A Life Of Its Own Previous guidance was provided in April 7, 2000 Federal Register
relative to direct physician supervision at off-campus provider-based clinics.
In CY2008 CMS started clarifying their guidance on this requirement as part of the Provider-Based Rule (PBR).
From CY2008 to the present there has been significant discussions in the Federal Registers and changes to the CMS manuals.
Distinguish• Diagnostic vs. Therapeutic Supervision• Off-Campus vs. On-Campus (Out-of-Hospital) vs. In-Hospital• General vs. Direct vs. Personal Supervision
General Application of “Incident-To” From the SSA CAH Issue – Differences in requirement from the CAH CoPs and the
PBR Supervision requirements. Note: At issue is a significant compliance concern. If auditors were to
determine that proper physician supervision was not provided, then recoupments could be demanded.

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 49
APC Update for CY2013Physician Supervision Changes
Physician Supervision Discussions
For 2011: “The definition of direct supervision will be revised simply to require immediate availability, meaning physically present, interruptible, and able to furnish assistance and direction throughout the performance of the procedure but without reference to any particular physical boundary. Since the new definition will now apply equally in the hospital or in on-campus or off-campus PBDs, we are removing paragraphs (a)(1)(iv)(A) and (B) of §410.27 altogether. The new definition of direct supervision under §410.27(a)(1)(iv) will now state, “For services furnished in the hospital or CAH or in an outpatient department of the hospital or CAH, both on- and off-campus, as defined in section 413.65 of this subchapter, ‘direct supervision’ means that the physician or nonphysician practitioner must be immediately available to furnish assistance and direction throughout the performance of the procedure. It does not mean that the physician or nonphysician practitioner must be present in the room when the procedure is performed.” (Page 828, CMS-1504-FC)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 50
APC Update for CY2013Physician Supervision Changes
Physician Supervision Discussions From 2012 Update: “Therefore, in the CY 2009 OPPS/ASC proposed rule
and final rule with comment period (73 FR 41518 through 41519 and 73 FR 68702 through 68704, respectively), we clarified and restated the various supervision requirements for outpatient hospital therapeutic and diagnostic services. We clarified that outpatient therapeutic services furnished in the hospital and in all PBDs of the hospital, specifically both on-campus and off-campus PBDs, must be provided under the direct supervision of physicians. We also reiterated that all outpatient diagnostic services furnished in PBDs, whether on or off the hospital’s main campus, should be supervised according to the levels assigned for the individual tests under the MPFS. (Page 825 – CMS-1525-FC)
Note also that CMS is recognizing all three supervision levels: Personal, Direct and General on the outpatient therapeutic side as well as on the diagnostic side (see MPFS).
• Question: With the above language, do the supervision requirement apply to in the hospital PBDs and well as PBDs on the campus but outside the hospital?

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 51
APC Update for CY2013Physician Supervision Changes
Physician Supervision Discussions “Specifically, for these services we redefined direct supervision to
remove all requirements that the supervisory practitioner remain present within a particular physical boundary, although we continued to require immediate availability. We also established a new category of services, “nonsurgical extended duration therapeutic services” (extended duration services), which have a substantial monitoring component. We specified that direct supervision is required for these services during an initiation period, but once the supervising physician or NPP has determined that the patient is stable, the service can continue under general supervision.” (Page 829 – CMS-1525-FC)
Cardiac Rehabilitation and Pulmonary Rehabilitation – Only physicians may meet the physician supervision requirements.
CAHs and Small Rural Hospitals (Less than 100 beds) have been exempted from the supervision requirements now through 2013.
The key phrase “immediately available” remains undefined.• CMS has given some counterexamples. For instance, a supervising
physician must be interruptible.• How can a physician/practitioner be immediately available and not
on campus??

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 52
APC Update for CY2013Physician Supervision Changes
Physician Supervision Discussions CMS has decided to establishing an independent advisory review
process.• Note: This is a standard bureaucratic approach when difficult
decisions must be made. See ‘share-the-blame’ concept. CMS intends to use the APC Advisory Panel
• But this panel addresses only APCs, that is, HOPPS• Need to include representatives for CAHs and small rural hospitals.• Qualifications of panel members.
Clinicians vs. Non-Clinicians vs. Non-Physician Practitioner vs. Nursing Staff
• Scope of authority limited to supervision issues. Keep in mind that this panel has only advisory capabilities.
CMS can still do whatever they want to do.• Process and criteria for determining which services require what
level of supervision. Subregulatory Process – Not in the manuals.• Services Not Described by CPT Codes• Starting Agenda
Extension Beyond “Incident-To” Services

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 53
APC Update for CY2013Physician Supervision Changes
Physician Supervision Discussions
“We stated in the proposed rule and continue to believe that, while the statute does not explicitly mandate direct supervision, direct supervision is the most appropriate level of supervision for most hospital outpatient services that are authorized for payment as “incident to” physicians’ services. We believe that the “incident to” nature of hospital outpatient therapeutic services under the law permits us to recognize specific circumstances in which general supervision is appropriate, as we have for extended duration services, and that CMS has authority to accept a recommendation by the review entity of general supervision for a given service. However, we continue to believe that direct supervision is the most appropriate level of supervision for the majority of hospital outpatient therapeutic services and, as such, it is the default supervision standard.” (Page 847 – CMS-1525-FC)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 54
APC Update for CY2013Physician Supervision Changes
Clarification for PT/OT/ST – CAHs vs. PPS Hospitals “In this final rule with comment period, we are clarifying that the supervision
and other requirements of the regulation at § 410.27 apply to facility services that are paid to hospitals under the OPPS and to these same services when they are furnished in CAHs and paid on a reasonable cost basis. In OPPS hospitals, the requirements of § 410.27 do not apply to professional services that are separately billed under the MPFS or to PT, SLP, and OT services that are billed by the hospital as therapy services and are paid at the applicable amount based on the MPFS. The requirements of § 410.27 also do not apply to these same professional and PT, SLP, and OT services when they are furnished in CAHs.” (Page 738)
“In OPPS hospitals, a small subset of “sometimes therapy” PT, SLP, and OT services are paid under the OPPS when they are not furnished as therapy, meaning not under a certified therapy plan of care. Because the supervision and other conditions of payment under § 410.27 apply to this subset of “sometimes therapy” services when they are furnished in OPPS hospitals as nontherapy services … those conditions of payment also apply to this subset of “sometimes therapy” services when they are furnished as nontherapy in CAHs.” (Page 738)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 55
APC Update for CY2013Physician Supervision Changes
Enforcement of Physician Supervision Rules (CAHs & Small Rural)
“Regarding the enforcement instruction, as we discussed in the CY 2013 OPPS/ASC proposed rule, we will extend the enforcement instruction one additional year through CY 2013. This additional year, which we expect to be the final year of the extension, will provide additional opportunities for stakeholders to bring their issues to the Panel, and for the Panel to evaluate and provide us with recommendations on those issues.” (Pages 742-743)
• Panel – Special Extended APC Panel – Determine which services require only general supervisions vs. direct supervision (vs. personal supervision).
• See CMS website for additional findings before January 1, 2013.

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 56
APC Update for CY2013Physician Supervision Changes
Physician Supervision Discussions OK, So What Does All This Mean to Hospitals? For 2013 the actual rules and regulations concerning physician
supervision are not being substantively changed.• Some issues are clarified, for example, three levels of supervision
on the therapeutic side. The hold-harmless for CAHs and small rural hospitals is being
continued. However, for most hospitals, the direct physician supervision
requirement will need to be attained for virtually all outpatient services regardless of location. See off-campus vs. on-campus vs. in the hospital.
The advisory panel/committee is being established with all the bureaucratic trappings.
• How long will it take for this panel to actually produce meaningful resutlts?
• And, will CMS accept the recommendations?

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 57
APC Update for CY2013Inpatient vs. Outpatient Observation
In Section XI. – Extended Discussion of the issue of inpatient admissions that are later determined as medically unnecessary. “We received approximately 350 public comments in response to our
solicitation in the CY 2013 OPPS/ASC proposed rule from hospitals and hospital associations, physician associations, rehabilitative and long-term care facilities, beneficiaries, beneficiary advocacy organizations, Quality Improvement Organizations (QIOs), organizations specializing in medical necessity review, and other interested parties. The commenters provided significant input, and the majority requested that CMS not implement a comprehensive solution or set of solutions regarding patient status in the CY 2013 OPPS/ASC final rule with comment period. Instead, many commenters recommended that CMS develop an informed course of action in the upcoming months through a formal, ongoing dialogue with all interested stakeholders (for example, through open door forums or a task force). A few commenters recommended a more immediate course of action to limit beneficiary liability for SNF care and for the difference in beneficiary cost-sharing between hospital inpatient and outpatient services.” (Page 751)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 58
APC Update for CY2013Inpatient vs. Outpatient Observation
Inpatient vs. Outpatient
See AB Rebilling Demonstration
Clarifying Current Admission Instructions or Establishing Specified Clinical Criteria
Hospital Utilization Review
• “Several commenters stated that some hospitals do not have UR staff on hand outside normal business hours or on weekends to assist with patient status determinations, and that this is especially problematic for patients with short inpatient stays.” (Page 759)
Prior Authorizations
Time-Based Criteria for Inpatient Admission
See Also the O’Connor Hospital Ruling

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 59
APC Update for CY2013Inpatient vs. Outpatient Observation
Inpatient vs. Outpatient
Rules for the External Review of Inpatient Claims
Improving Beneficiary Protections
• “These included providing Medicare coverage for self-administered drugs in the hospital outpatient department, waiving beneficiary coinsurance, capping the sum of outpatient services at the inpatient deductible, or establishing annual maximum out-of-pocket costs.” (Page 769)
Revising the Qualifying Criteria for Skilled Nursing Facility (SNF) Coverage
“We [CMS] appreciate all of the public comments that we received on this multi-faceted topic. We will take all of the public comments that we received into consideration as we consider future actions that we could potentially undertake to provide more clarity and consensus regarding patient status for purposes of Medicare payment.” (Page 772)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 60
APC Update for CY2013Hospital Outpatient Visits
Hospital Outpatient Visits – A Continuing Area of Challenge Direct Admits to Observation – G0379
• Changed APC Mapping To APC 0608 – Level 5 (99205/99215) SI=“Q3” Payment $175.79
• Question: When do you receive separate payment for G0379? “We agree with the commenter that we should not move to national
guidelines for visits in CY 2013. As we have in the past (76 FR 74345 through 74346), we acknowledge that it would be desirable to many hospitals to have national guidelines. However, we also understand that it would be disruptive and administratively burdensome to other hospitals that have successfully adopted internal guidelines to implement any new set of national guidelines while we address the problems that would be inevitable in the case of any new set of guidelines that would be applied by thousands of hospitals. As we have also stated in the past (76 FR 74346), if the AMA were to create facility-specific CPT codes for reporting visits provided in HOPDs [based on internally developed guidelines], we would consider such codes for OPPS use.” (Page 673)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 61
APC Update for CY2013Hospital Outpatient Visits
Hospital Visit Coding Guidelines One of the greatest concerns on the part of hospitals is whether or not
their mappings are appropriate. Even with the CY2008 principles, guidance, at best, is very limited and general.
“In contrast, many commenters urged CMS to move forward with the implementation of national guidelines for hospitals to report visits, asserting that CMS has poor data upon which to calculate visit APC payment rates because there are no standard definitions, and citing the challenges of having different guidelines in place by different payers. The commenters recommended that, in the absence of national guidelines for hospital visit reporting, CMS support a request to the American Medical Association CPT Editorial Panel to create unique CPT codes for hospital reporting of emergency department and clinic visits based on internally developed guidelines.” (Page 773 – CMS-1525-FC)
• Coding Issues – Example: Minimal fracture care. Separate code or place in the E/M levels.
• Design Issues: Point System, Narrative System, Hybrid, Diagnoses• What incentive does the AMA have for getting into this area?

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 62
APC Update for CY2013Hospital Outpatient Visits
Hospital Visit Coding Guidelines Commenters are very concerned about contractor audits of the hospital
developed coding guidelines. • “In addition, some commenters expressed their appreciation for CMS’
encouragement of its contractors to use a hospital’s own guidelines when auditing and evaluating the appropriateness of codes assigned, but requested that hospitals be exempt from audits of visit billing until national guidelines are implemented.” (Page 773 – CMS-1525-FC)
• CMS’ Response: “We continue to encourage fiscal intermediaries and MACs to review a hospital’s internal guidelines when an audit occurs, as indicated in the CY 2008 OPPS/ASC final rule with comment period (72 FR 66806).” (Page 774 – CMS-1525-FC)
Exercise: Analyze this response relative to the eventual entry of the RACs (Recovery Audit Contractors) into this area including the use of statistical extrapolation.
Bottom-Line – CMS is making no changes as such for national E/M coding guidelines. They will continue to monitor their national level aggregate data for possible aberrations.
© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 63
APC Update for CY2013Hospital Outpatient Visits
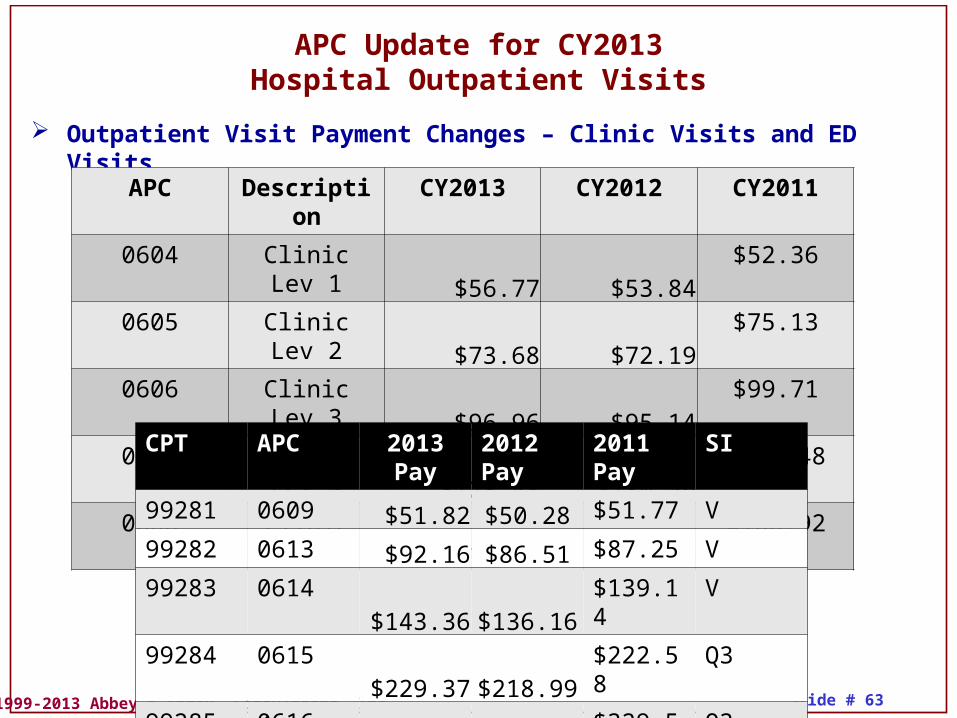
Outpatient Visit Payment Changes – Clinic Visits and ED Visits
APC Description CY2013 CY2012 CY2011
0604 Clinic Lev 1 $56.77 $53.84 $52.36
0605 Clinic Lev 2 $73.68 $72.19 $75.13
0606 Clinic Lev 3 $96.96 $95.14 $99.71
0607 Clinic Lev 4 $128.48 $130.56 $128.48
0608 Clinic Lev 5 $175.79 $176.70 $168.92
CPT APC 2013 Pay
2012Pay
2011Pay
SI
99281 0609 $51.82 $50.28 $51.77 V
99282 0613 $92.16 $86.51 $87.25 V
99283 0614 $143.36 $136.16 $139.14 V
99284 0615 $229.37 $218.99 $222.58 Q3
99285 0616 $344.71 $323.14 $329.54 Q3

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 64
APC Update for CY2013Ambulatory Surgical Centers
ASC Payment Process – See Section XIV. Now a hybrid of APCs and MPFS. Calculation of ASC Payments Depends on Lists of Surgical Procedures
• Office-Based vs. OP Hospital vs. IP Hospital Listings Must Be Updated Each Year
• ASCs Surgical Procedures Include Office-Based and Certain OP Hospital Surgeries The process for determining these lists is all-important for ASCs.
Concerns for excluding surgeries from ASCs. Treatment of new codes. Determination of covered services, drugs, biologics, etc.
Transitional Payment Rate Are No Longer In Use Many issues that are present for OPPS in general (e.g., “-FB” and “-FC”
modifiers, preventive services, etc.) are present for ASCs also.• See NTIOLs relative to cataract surgery.• Significant discussions for cataract surgeries at ASCs.
Update and Cost Data• Conversion Factor to $41.401 from $43.190 in 2012 (-0.4%)
ASC Quality Reporting Program – See Section XVI.

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 65
APC Update for CY2013Reporting Quality Data
Quality Reporting for Hospital Outpatient Services
There is an extensive discussion in the Federal Register addressing Quality Data Reporting.
Quality Reporting In Multiple Settings
• “CMS has implemented quality measure reporting programs for multiple settings of care. These programs promote higher quality, more efficient health care for Medicare beneficiaries. The quality data reporting program for hospital outpatient care, known as the Hospital Outpatient Quality Reporting (Hospital OQR) Program, formerly known as the Hospital Outpatient Quality Data Reporting Program (HOP QDRP), has been generally modeled after the quality data reporting program for hospital inpatient services known as the Hospital Inpatient Quality Reporting (Hospital IQR) Program (formerly known as the Reporting Hospital Quality Data for Annual Payment Update (RHQDAPU) Program).” (Page 1096 – CMS-1525-FC)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 66
APC Update for CY2013Reporting Quality Data
CMS Changes “In the CY 2013 OPPS/ASC proposed rule (77 FR 45178), we did not
propose to retire any measures from the Hospital OQR Program.” (Page 896)
Removal of One Chart-Abstracted Measure for CY2013 and Subsequent Years
• “We emphasize that despite the removal of OP-16 from the Hospital OQR Program, we expect hospitals to continue the timely triage, diagnosis and treatment of cardiac and other patients in the ED according to established clinical guidelines. We also expect that hospitals will continue their efforts to improve communication and throughput in the ED.” (Page 902)
Deferred Data Collection
• Cardiac Rehabilitation (OP-24) “With the inclusion of the abstraction instructions for this
chart-abstracted measure in our July 2013 release of the Specifications Manual, we anticipate that data collection can begin with January 1, 2014 encounters.” (Page 913)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 67
APC Update for CY2013Reporting Quality Data
HOP QDRP Quality Measures – 2014 On OP-1: Median Time to Fibrinolysis OP-2: Fibrinolytic Therapy Received Within 30 Minutes OP-3: Median Time to Transfer to Another Facility for Acute Coronary
Intervention OP-4: Aspirin at Arrival OP-5: Median Time to ECG OP-6: Timing of Antibiotic Prophylaxis OP-7: Prophylactic Antibiotic Selection for Surgical Patients OP-8: MRI Lumbar Spine for Low Back Pain OP-9: Mammography Follow-up Rates OP-10: Abdomen CT – Use of Contrast Material OP-11: Thorax CT – Use of Contrast Material OP-12: The Ability for Providers with HIT to Receive Laboratory Data
Electronically Directly into their Qualified/Certified EHR System as Discrete Searchable Data
OP-13: Cardiac Imaging for Preoperative Risk Assessment for Non-Cardiac Low-Risk Surgery
OP-14: Simultaneous Use of Brain Computed Tomography (CT) and Sinus Computed Tomography (CT)
© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 68
APC Update for CY2013Reporting Quality Data
HOP QDRP Quality Measures – 2014 On• OP-15: Use of Brain Computed Tomography (CT) in the Emergency
Department for Atraumatic Headache• OP-16: Troponin Results for Emergency Department acute
myocardial infarction (AMI) patients or chest pain patients (with Probable Cardiac Chest Pain) Received Within 60 minutes of Arrival
• OP-17: Tracking Clinical Results between Visits• OP-18: Median Time from ED Arrival to ED Departure for Discharged
ED Patients• OP-19: Transition Record with Specified Elements Received by
Discharged Patients• OP-20: Door to Diagnostic Evaluation by a Qualified Medical
Professional• OP-21: ED- Median Time to Pain Management for Long Bone
Fracture• OP-22: ED- Patient Left Before Being Seen• OP-23: ED- Head CT Scan Results for Acute Ischemic Stroke or
Hemorrhagic Stroke who Received Head CT Scan Interpretation Within 45 minutes of Arrival

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 69
APC Update for CY2013Reporting Quality Data
HOP QDRP Quality Measures – 2014 On OP-24: Cardiac Rehabilitation Patient Referral From an Outpatient
Setting (See Additional Comments)
OP-25: Safe Surgery Checklist Use
OP-26: Hospital Outpatient Volume Data on Selected Outpatient Surgical Procedures
See Also Future Auditing for Compliance Relative to Quality Measures
See Also Medicare EHR Incentive Program – Electronic Reporting

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 70
APC Update for CY2013CCRs and Implantable Devices
Charge Compression and Cost-Report Changes “Since the implementation of the OPPS, some commenters have raised
concerns about potential bias in the OPPS cost-based weights due to “charge compression,” which is the practice of applying a lower charge markup to higher cost services and a higher charge markup to lower cost services. As a result, the cost-based weights may reflect some aggregation bias, undervaluing high-cost items and overvaluing low-cost items when an estimate of average markup, embodied in a single CCR, is applied to items of widely varying costs in the same cost center. This issue was evaluated in a report by Research Triangle Institute, International (RTI).” (Page 72)
“Specifically, we created one cost center for “Medical Supplies Charged to Patients” and one cost center for “Implantable Devices Charged to Patients,” essentially splitting the then current cost center for “Medical Supplies Charged to Patients” into one cost center for low-cost medical supplies and another cost center for high-cost implantable devices in order to mitigate some of the effects of charge compression.” (Pages 72-73)

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 71
APC Update for CY2013Proposed Changes to APCs
Other Recommended Changes
MedPAC
GAO
OIG

© 1999-2013 Abbey & Abbey, Consultants, Inc. Slide # 72
APCs Represent CMS’s Most Complex Prospective Payment System The Federal Register Entries Are Becoming Enormous We are into the Twelfth Year (Depending on how you count) of APCs –
The variation in payments continues to be a roller coaster although there appears to be a little more stability. Now CMS is starting to use the geometric mean; how will this affect specific APC payments?
Significant policy changes continue to be developed, specifically increased packaging and more composite APCs.
Apparently there will no national guidelines for technical component E/M coding for the ED and provider-based clinics. (AMA Develop?)
Physician supervision within the Provider-Based Rule has become a major issue due to CMS clarifying guidance.
The cost report and appropriate CCRs have become an issue although this problem has been evident since APCs were implemented.
While there continue to be areas of difficulty (e.g., singleton claims for weight development), CMS is whittling away at issues.
Hospitals should anticipate that APCs will continue to change at a rapid pace during the coming years.
APC Update for CY2013Summary and Conclusions