- pancreas artificial148.206.53.84/tesiuami/uam21322.pdf · y contiene,agua, sales,,acido i...
TRANSCRIPT

- P A N C R E A S A R T I F I C I A L
D 4
/-

R m..
I >+
L
L
r-
L
r i
c
i h-
1 WRCO HEDICO DI GEST ION PANCREAS ANATOkIIA FISIOLOGIA PATOLOGIAS f: IS I OPATOLOG I AS
2 M C O IN6ENIERIL INTRODUCCION METODO DE DIAGNOSTICO POR RAYOS X METODO DE DIAGNOSTICO POR ULTRASONIDO
3 HCIRCO ESPECIFICO PANCREW ARTIFICIAL
INTKODUCCION INVESTIGACIONES SIMULADORES Y MODELOS MRTEMATICOC DISPOSITIVOS EN USO CLINIC0 Y TERAPIA VENTAJAS Y DESVENTAJAS
4 coNcLffi1oNEc
5 REFERENCIAS ART I CULOS RIRLIOGRAFIA
4
6 €I 12 16
20 2c1
21
38
4 o 42
2


DIGEST ION
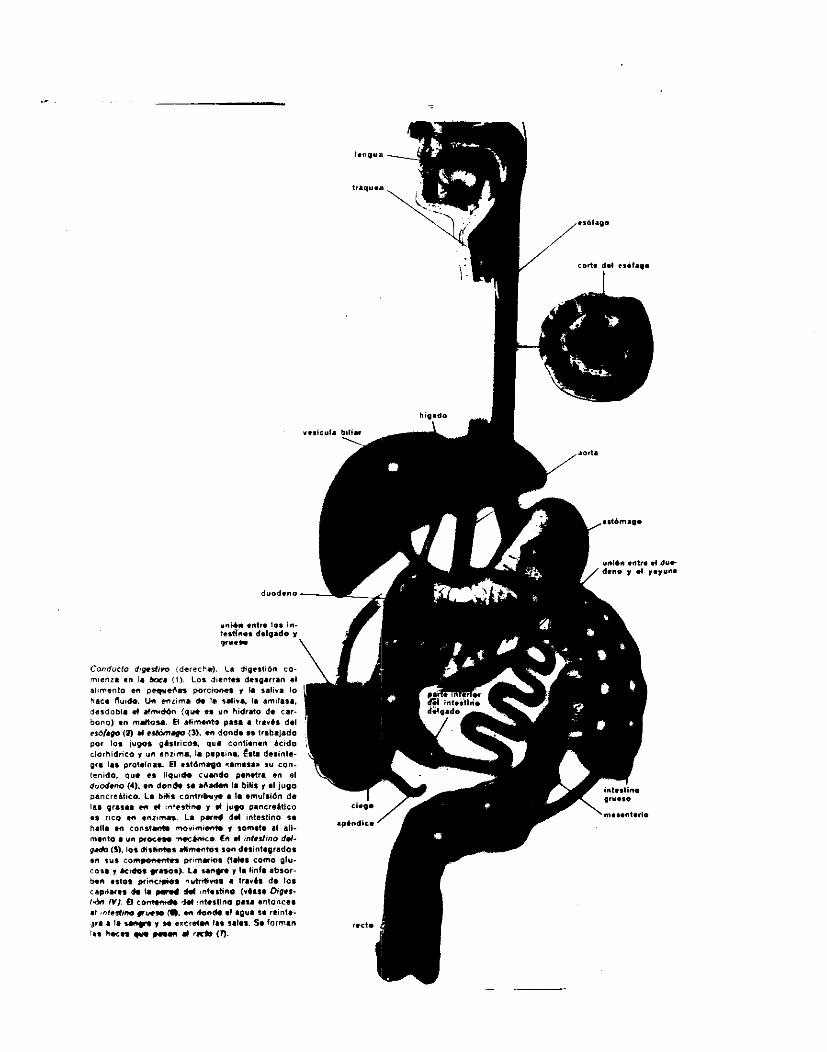
P r o c e s o f i s i o l óg i co q u e t r a t a d e l a d e s i n t e g r a c i ó n d e 19s s u s t a n c i a s c o m p l e j a s c o n t e n i d a s e n los a l i m e n t o s e n s u s t a n c i ? s mas s i m p l e s . E l , s i s t e m a bigest ivo comprende l a boca , q l a n d u l a s s a l i v a l e s , esofago, estomago, i n t e s t i n o s , el h i g a d o , el p a n c r e a s y el recto. Los al imentos c o n t i e n e n h i d r a t o s d e c a rbono , p r o t e i n a s y g r a s a s , as1 como agua, s a l e s y v i t a m i n a s . Los Q i d . r a t o s d e c a r b o n o se convierten e n d i f e r e n t e s c l a s e s de a z u c a r e s y f i na lmente en g l u c o s a , q u e es l a s u s t a n c i a que p r o p F r c i o n a e n e r g i d a l o r gan i smo . Las p r o t e i n a s , s e d e s i n t e g r a n en ,amin?ac idos . L a s g r a s a s s i rven como r e s e r v a e n e r q e t i c a . L a c o n v e r s i o n q u i m i c a se a c e l e r a m e d i a n t e l a s enz imas , q u e son p r o t e i n a s a c t i v a s d i s u e l t a s en los j u g o s d i g e s t i v o s : La d i g e s t i o n se r e a l i z a e n ;tres f a s e s : L a , d e s i n t e g r a c i o n d e l a l i m e n t o en sus componentes b a s i c o s , l a ingestion o a b s o r c i o n d e estos eiementos n u t r i t i v o s p o r el o r g a n i s m o y f i n a l m e n t e , l a excreciori d e 10% p r o d u c t o s d e d e s e cho . En l a r n a s t i c a c i o n el a l i m e n t o rse d e s i n t e g r a en p equeños f r a g m e n t o s y ,se mezcla con ;a s a l i v a p r o c e d e n t e d e tres p a r e s d e g l a n d u l a s : L a s p a r o t i d a s , las s u b m a x i l a r e s y l a s s u b i i n g u a l e s . La s a l i v a consta, p r i n c i p a l m e n t e , d e agua, y cont iene t amb i en moco y e n z i m a , p t i a l i n a ( d i a s t a s a s a : l i v a l ) , una a m i l a s a que d e s i n t e g r a el a lm idon . La p t i a l i n a n o ejerce n ingun efecto s o b r e l a s p r o t e i n a s o l a s g r a s a s . L a s a l i v a c o n t r i b u y e a l r e b l a n d e c i m i e n t o d e l a l i m e n t o y 10 m e z c l a con el moco ( f o rmando el bo lo a l i m e n t i c i o ) , con l o q u e se f a c i l i t a su d e g l u c i o n . LOS, movimientos d e l a l e n g u a h a c i a l a p a r f e p o s t e r i o r d e l p a l a d a r estan g o b e r n a d o s p o r l a v o l u n t , i d , pero ademas in te rv i ene un c e n t r o nervioso e s p e c i a l , h a c i e n d o que se produzcan movimientos incon5cientes d e d e g l u c i o n que emp ie zan a empujar el a l i m e n t o h a c i a el es?fago E l esofago es, un c o n d u c t o d e SO cm d e l o n g i t u d y d e l g r o s o r d e l p u l g a r . Su p a r e d e s t a f o rmada ,po r p l i e g u e s d e una membrana mucosa, r o d e a d a d e muscu los q u e au t oma t i c amen t e impu l san el a l i m e n t o h a c i a a b a j o . E l b o l o t a r d a d e 5 6 seglundos e n a t r a v e z a r el e s o f a y o , desembogando e n e; estomago poir med i o d e l e s f i n t e r ca r -d i aco . E l estomago esta s i t u a d o en l a p a r t e s u p e r i o r i z q u i e r d a d e l abdomen, tiene una c a p a c i d a d aprox imadamente d e 2 a 3 l i t ros , su p a r e d i n t e r n a c o n s t a d e una membrana mucosa d i s p u e s t a eii p l i e g u e s , p o r f u e r a d e esta,existen tres c a p a s d e muscu lo l iso. La p a r t e e x t e r i o r d e l e s t o m a g o e S t a r e c u b i e r t a p o r un > t e j i d o d e l g a d o c o n j u n t i v o , , l a s e r o s a , e s t a es una c o n t i n u a c i o n d e l p e r i t o n e o . E C ~ el es tomago , ei a l i m e n t ? se mezcla i n t imamen t e c on el j u g o g a s t r i c c i ( l i q u i d o f o rmado p o r g l a n d u l a s d e l a membrana mucosa
4
f

I
y c o n t i e n e , a g u a , s a l e s , , a c i d o c l o r h i d r i c o y enzimaE;). La formacion d e l jugo gas t r i c0 e m p i e z a con l a v is ion d e l al imento a p e t i t o s o y continua cuando el a l i m e n t o p e n e t r a en l a , boca . E l c o n t a c t o directo con l a membrana mucosa d e l estomago a c t u a como un nuevo e s t i m u l o . Las c o n t r a c c i o n e s d e los muscu1,os d e l a p a r e d gastr-ica, e n f o rma d e ondas , mez c l an i n t imamen t e el c o n t e n i d o d u r a n t e el , p r o c e s o quirn ico . E l a l imento 5e d e s p l a z a g ~ a d u a l l m e n t e , e n f o rma l i q u i d a h a c i a l a a b e r t u r a i n f e r i o r d e l estomago (el p i l o r o ) q u e p e r m i t e s u p a s o en pequeñas p o r c i o n e s h a c i a el interior d e l duodeno. L a l o n g i t u d d e l duodeno es apro f i imadamente d e 12 a i5 cm, p r e s e n t a f o rma d e h e r r a d u r a y e s t a s i t u a d o e n l a , p a r e d p o s t e r i o r d e l a c a v i d a d abdomina l ; e l p r o c e s o d e d i g e s t i o n , e s mucho mas in tensa , ya qu? el h i g a d o y el p a n c r e a s d e p o s i t a ? a l l i sus jugos. La b i l i s d e l h i g a d o e m u l s i o n a ;as g r a s a s p o r sus a c i d o s b i l i a r e s y c o n t r i b u y e t amb l en a l a a b s o r c i o n d e los componentes de l a s g r a s a s . E l j u g o p a n c r e a t i c o contiene l a s s i g u i e n t e s enzimas: l a t r - i p s i n a , l a q u i motr i p s i na Flmilasa, l i p a s a c a r b o x i p e p t i d a s a , f o s f o l i p a s a Az, r i b o n u c l e a s a , d e s o x i r r i b o n u c l e a s a y col Fstet-i 1 e s t e r - h i d r o l asa. L a b i l i s y el jugo p a n c r e a t i c o se s e c r e t a r ) p o r l a i n f l u e n c i a d e hormonas. Cuando el a l i m e n t o p a r c i a l m e n t e d i g e r i d o a l c a n z a el duodeno se forman d o s hormonas en 5u mocosa! l a c o l e c i s t o q u i n i n a l a c u a l es t r a n 3 p o r t a d a p o r l a sangre a l a y e s i c u l a b i l i a r y p r o d u c e su contraccion y l a c o n s i g u i e n t e s e c r e c i o n , d e b i l i s . Y , l a s e c r e t i n a q u e c i r c u l a con l a s a n g r e y p r o d u c e el e s t i m u l o d e l panc r ea s . Cuando el a l i m e n t o p a s a p o r el i n t e s t i n o d e l g a d o g r a n p a r t e d e l mismo,se ha d e s i n t e g r a d o e n sus componentes b a s i c o s . La p r i n c i p a l f u n c i o n d e l intestino d e l g a d o 1-5 a b s o r b e r los n u t r i e n t e s h a c i a l a sangre y l a l i n f a . E l intestino d e l g a d o t i e n e una ' l o n g i t h d aprox imada d e 4 a 5 mts y p o s e e muchas asas. Empieza en l a p a r t e s u p e r i o r e i z q u i e r d a d e l abdomen y termina e n l a p a r t e i ? fer ior y d e r e c h a , e n donde se a b r e el i n t e s t i n o g r u e s o , ' a t r a . v e s d e l a v a l v u l a i l e o c e c a l . E l c o n t e n i d o i n t e s t i n a l , d e c o n s i ' s t e n c i a p u r i f o r m e , t e ñ i d o d e color o b s c u r o p o r l a b i l i s , se mezch con los jugos i n t e s t i n a l e s ,y se t r a s l a + a l o largo , d e l i i n t e s t i n o m e d i a n t e los movimient .os per i s ta l t i coe d e los muscu los d e su p a r e d l a s h e c e s a d q u i e r e n f o rma y l l e g an a l recto, el clual d e s p u e s d e un corto t r a y e c t o rec t i l ineo , c a l e a l a s u p e r f i c i e d e l c u e r p o p o r el o r i f i c i o ana l o ano. Los intestinos se vaci 'an cuando l a p r e s i ó n e n el recto e s l o s u f i c i e n t e m e n t e in tensa p a r a d e s encadena r un re f l e jo .
.
h.11. ." con,,- mO.im- . ien.1. .I dl.
F t
poncreático menor
Conducto poncreático mayor I

F%8&4 4 i Como glandula de smcreción externa, elabora e1 jugo pamre;tico
iHgregMdo&o,on el duodeno de medio a un l i t r o , diariamente, el cual err un l iquide *cu080 no viscoso, teniendo un contmido de ?gua semejante al de l a Sal iva y qu i l l eva Sierta cantidad da proteinas y otros coinpuestoi wganicos e, inorganfcw, ospscialmentei Na, K, HCO. y C1 . Car Zn, HPOI y $Or ,estan prerqntes en paqueFIas cantidades. .La elevada concmtraciqn de bicarbmato hace qus e1 juga piincreatico 8ea l a recrecion mas a lca l ina del cuerpo, y s ~ a e1 s i s top amr.t;iguador principal para neutral izar el acido clorhidrito p a r t r i p s con un QH de 7 .5 a 8.0 o mayor. Lo ug rec ion y rlt?II)uio del ponceas es debido a l a presencia del quinw)ocido de1 estolgago que act a al duodeno para producir: I9.v*tin*, que estimula horamalhentle e l f lu jo ,de l jugo pancreático y l a Pwiurwtii*ne, que estimula l a produccion de ssnzimar. ñlgu3a6 de l a s enkirhas son sn;ret?d+s como pr8cur*wp% , inactivos (zimogenosi t a l e s c?moiei tripsinogeno y el quisñotripoinagcwto, que son activadoCIel poncw8e en Sontact@ con l a mucoea intest inal . La attivac$on rlel tripsi?o$mno se atribuye a l a enterwinasa que que es produfida p ~ ? + la6 glandirlars intastinalee.
activacion ~utocmtdl i t ica , atliciodal del tripsin&genb y del Una peques Fantidad ge t r ip r ina autiva provoca entonces l a
qui mtri psi nheno.
Enz iM I l Nombre
Tripsi na
Quirotripsina
Nodo de , actrivacim y Gmdic imes optlimas para BU actividad
EI tr ipsinópmo ra convierte en t r ip r ina activa por l a entero- cirtipr del intestirao a r)H 5.2-6.0. Gonvcr- siw autocatal i t ica a pH 7.9.
E8 srcretad? cOin13 qulmotripsincgQno y convet-*ida a la fwma activa por l a t r ips i - na pH 8.0.
8
Substrato Pr odwtos fineles o accion
Pr oteí nas Pal !pÍptidoe Pr ot eosa* Psptonrs
Diprpt i rlor
Proteína8 Polipóptidoo ProteOnas D i p w t i ? h y PaptoW%% CoaguLaci on
para l a leche.

c c c c E c c
c c f [:
c 1 c I:
Car boxi p ~ p t i - dara
.
Lipare
Ribrrtuclerse
-retada C M ~ M procarbox i p&pt.idasa y activada por l a tripsina.
pH 7.1
+tividad por l as sales b i l iue i s? pH B.O.
D I M r irr i bonwcl easa
Cal wtw I i es- Actividad por terni drbi &ma las sa&*%
bi Li we%
Fmsfol i para A.
Pol ipppti- Peptidois dos en el i nf ar ? ores. extremo del Ckninoacidos carbox i 1 o 1 i bree. l i b r e de l a cadena.
~1 m i 40n Maltpa más 01 ucogeno D lucos ido~
r i d w ) mam mal totr i osa.
( 01 i mQ%d%d-
ipipnes ck i dos -ter qPa.io.1 pr i m a t i as de l a s cMOIes, grasas.
monwci 1 g 1 i - di a c i i gl i ce- rol-, p l i - ceral .
k i d 0 MucI&tidas r i bonucf ei - co.
W i d 0 Nucl &ti dos decoxi rr i - bonucleiclos.
Estereme de ~ l w t e ~ o l colm8teVilo. ; ibre mas
ac i d m grasas.
FQsf o1 í p i - doi.. grasos,
Ac i dos
1 5 %Of orf 0- 1 i pi dos.
9

c c c c c c c c c c f c f c c
F:
r La
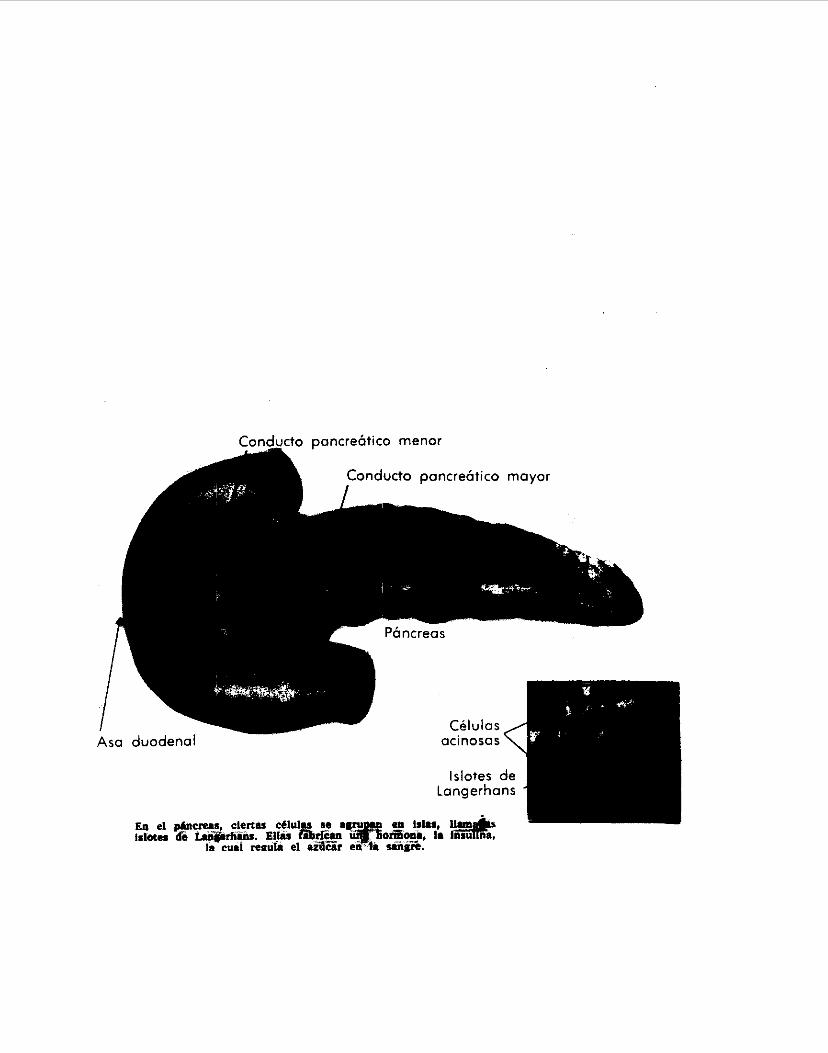
La funci6n e+ocrina del páncrsas está localizada en,loc isloijes de LÍngwihans, ce lu las e j I i te l ia les dispersadas a traves del organ0
hamonas que afectan e1 metabolismo de 105 son producigas por e1 tq j ido insular: La insulina por
las c t lu l a r p y e1 glucagon por , las ce lu las a . TaiAbirn sa ha deturito una r e lu l a A, que almacena y secreta
La inculina desempeña un papel importante en el metabolism gencral, causando awet$o en e; metabolim?o de los carbohitlratoo, al#acenaf!tiento de $lucOgeno, sintesois de acidos qrasos, captacion de ua!noacidos y sintesis de proteinas: Es asi una importante hormona, anabolica que actha sobre una vjr iedrd de te j ido incluyendo el higado, el t e j i do adiposo y el mueculo. La insu l ina~aasa por los capi lares al torrente sanguineo, y cuando l a produccian es insuf ic iente soM=PViene l a Diabetes. La Diabetes os una egfermedad que sw debe a una d e f i c im c i a el funcionamipke del pancreas para s e q e t a r insulina. La causa es deqleneracion o inactivacion de l a s oe lu las p de los islbtes de Langerhans, paro 30 se conoc%n las qausas basics. d e estos s-fectos. En algunos diabeticos, en part icular l o t que l a desarrollan muy a1 principio de , la vida, l a enfermadad es causada por herencia de un padrr (o aigun ancemtrol de ce lu las p muy propmsas a d~q)en?rarse. En otras personas se desarrollen anticuerpor contra lam cq lu las p que l a s destruyen, l o qu9 es uh ejemplo de un proceso patplogico autoinmunitrrio. En otros mas se desarrollan a v%cec anaicuerpos contra l a propia insulina, que l a destruyen antes que puedan actuar en otros sitios del cuerpo, l a cantidad de Snsuliha secretada puede ser t o t a l m t e normal pero nunca l l e ga a SU dert i no. La anomalia primaria de l a Diabetes le5 insuficiencia para u t i l i z a r cantidades suf ic ientes de glucos.* para obtener energia, y por l o tanto el empleo de cantidades excesivas de @ras+ con esta f inal idad. Esto hace que se incrmente l a concentracion sanguinea de glucosa de tras a diez veces de i b normal. 59 pierden grande5 cantidador de glucosa en l a orina porque los tubulos renales no pueden reabswv@r toda l a que l e í llpga en el f i l t r ad o g lmerur?l cad9 minuto. E l exceso d$ glucosa tubular tambien crea una pcesion osmotica enorme en los tubulos, l o qlie disminuye l a resorcion de q u a , crnno resultado l a persona pierde grandes cantidades de aqua l o mismo que de glucoca,pw l a orina. La incapacidad del diabetic0 para utSlizar l a glucosa con objeto de obtener energid l o pr iva de una part? importante de l a energid de sue alimentos. Pierde peso y se debihita a l consumir excesivamente sus reservas de grasa y proteinas. Como resultado de l a def ic iencia de nutrientee l a persona enferma suele estar muy hambrienta. E l mitabolismo extremadamente rapido de l as grasas incrementa a
10
en

f c c c c c t c c 13 c c G c c c c o E
VKRS l a cantibad de cetoacidos en los l iquidos extracelulares. ñ1 pW de lair l jquidos corporales caen hasta 7.0 y algunos casos hasta 6.9, grado de acidosis es incompatible con l a vida duranti mas de unas cuantas horas, l a persona respira con rapidez y gran profundiplad para expulsar todo,el dioxido de carbono, esto l e ayuda a uup#ar l a acidosis metabolica, pero a pesar de este mecaniuno la acidosis se vuelve a menudo de gravedad suficiente para que l a victima caiga en coma. La diabetes prolongada w e l e dar por resultado desarrol lo tempcan0 de a r t ~ r o s c l a r o s i s , que subsecuentamente 6)s causa de cardiopatiac, 1 esi ones renrl es, acci dentes car di ovascul ares. La $rtRro%Cl+PoSiS es debido al m&abolismo de l a glucosa que no reta a un n$vel l o suficiente elevado para prevenir el metabolismo excesivo de $as gra*aa y e l depositd de colesterol en lam paredes de 10% vatmas sanguineor. En wasic$ne ke desarrol la hipyinsulinismo a causa de un sobre trataibiento iye l a persona diabetica con ineulina, , o d r secrecion excesiva de ta m8saa por un tumor de 10s i s lo tes pancreaticos. La émcentracion íangui nea de QlUC05a baja provoca hiperexcitaóifidad del cerebro a1 principio y a continuacik coma.
l i

Eritema palmar
- Infecciones cutlncas

"..
.""
E n d o c r i n o ArJenoma Oe i a i is-- Ca r i l numa de lotes d e Lariqer.riarir; ?os ic;loces
de inr igsrharts

.. , .
....
. .
., ,
-- -~ _ _ 5 _ ..,.. *.-cwII--cI "__^ ......_..,_,,,, ~-.," ..,, . .-,, -.,. . ..* .,,, ... . . ...., .. ,. .. ., , .. ., ..
15



. .-
L ,
I.
..
* -
. .
-...
..
...
I_
, .
F .
. .
, ,.
. .
.
. , . . , / . , , , - " . . , I . , . . * ..-.... *.-<-- __._...,, . . ~ .,,.., , . , . . .# ..,. . , , . , , , ... _ _ ..
.. .. .. ..,- <^ -,.. "llll_- <.-.. I ....... ,," . .... .. . ..

. ..,
.,
.. .
p i e u r a i e s por v i a i i n + á t . i c a c r u z a n d o ei ri iair-aqma. Este ~iquic io c o n t i e n e y r y c a n t i d a d de ami1d.r;a. Cuando el 1 i q u i d o sangu i no1 eritc de or-i g e n p a n c r e $ t i c o esc .apa d e s d e los e s p a c i o s r - e t r o p e r ? t o r i e a l r ? a l t e j i d o subcutar i eo , puede p r o d u c i r ciri camb i o d e rioloracion e q u i m o t i c u r o j i x i > a l r e d e d o r d e l ombligct. La p a n c r e a t i tits aguda puede r-emedar el i r i f a r - t o de mioca rd i c> por- el d o l o r , i ~ t e r i s n a n i v e l d e l ep i ya . s t r - i o . . Tambien s. p r o d u c e i n s u f i c i e r i c i a r e n a l ayuda a c u n s e c u e n c i a ile ia h i p o t e n s i ü n y l a dismirtucion d e l r i e g o s a n g u i n e o r e n a l , ü de la tox I c i dad gentir-al secundar- i a. , Las artomalia!i d e l a c - r ; a g~~ l z . ~ i o r ! d e id sariqre l a s ic~ I . i v idr id p r o t e o l i f i c a de t i p o de t r i p 5 i n a en la zanyi-t. e5 a t r . i u u i d c i a liberacion d e e n z i m a s p r o t e o l i . t . i c a s d e s d e el t e j i d o pancr-eft l .c:o r i ec rusado , ie tia descrito Liii a y m c r i t o d e a c t i v i d a d p r - o t e o l i . t i c : a acompañando a 1 a desí i br i n a c i urlr el coysurriu ace1 e r ado de f i b r i n o g e n 0 y otros factor-es d e c n a y u l a c i o n en p a c i e n t e s c on p a n c r - e a t i t i s ayuda. Las manifestaciones p r o t e i f o r m e s d e l a p a n c r e a t i t i s caguda se comple tar i p o r inarti f e s t a c i o n e s d e psic . c js j i ri aguda, i n c l u y e n d o a l u c i n a c i u n e s pasaieras,, i l u s i o n e s , ayi tacirwi y d e s o r i en t dc i on. b) ~ARClNC)IYFi*.-'- Los si ntoma,s in : i: i a i e5 sori dnurex i < A ? d o l c)i- e p i g a s t r i c 5 1 y de e s p a l d a , vayo, molesto y p e r s i s t e n t e , s,rciedeit:l r a p i d a , p e r d i d a d e p e s o , d i s t e r i a i o i ! abdomi i ia l pra.vc.icadd po r asci t . is , ~ c t e r i c i a y,a veces h ~ : ! c e s gr asosas. pur factores b i o q u i m i c o s ,de~,iroricic:~.tJo5 el par:lw;*..e l l e g a l i a p r e sq r i t a r t ra ! ; torn»s ps iqu i ak r i cos , :i icluyeiitio lsx, rnar i i i .c - i j tac iL , r iE15 p s l c o t i c a s . ir? examer-i f l ~ i c c ) ,puedts dcscubr i r grandes rriasdz tumor-a l es , asiiitis, ictecicia, higado aLtmentadn' !le volumen o r-ciidcjs a r ~ t e r i a l e s poi- c ompre s i on LIE' ejer..;a t ? l t e j i d o tumora l sobre a r t e r - i a s di, ver'sas. c ) f: iERüCiS WIJ1STICR.- Es una a i f e r m e d a d .+ami l iar p y i i i c i p a i i n e n l t ? de
autosomic? . krs uri t r a s t o r - n o dti i a i gianciiii2r+ e:.:m:r-inas L I , L ~ ~ a iec i .a .il ,paricr e a i , pu lmones , i e i ' i ~ i i..ai.aiiosídles, n i gado , v e s i c i i l bi i. i a r . , g l arrdul as j .n t . i s5t ina l es y y 1 antj~tl ~ < s sal i v a l es. Lid c a u y meta1:olica o nioieculnt-. iu:!damei-i¿ai ilc' ¡a +ibro+:l5 qi.~iat i i . :a I E C . est& a c l a r a d a . S i n csmQaugo h a y Uo? d e f e c t o s k.rdnsporte diiorrrsG31 d e elec:tr.o;itiris y a n o m a l i a s $ii;icotju:mica':i da i f i r . . r~ r i c io r i i% r ica-, en y l~ i~ :oprüte I . i ta ! z . c9mo el müco. La i i b r o s i s , qu i s t i c : a cuandii a+ecta a riiñoi 5i.ielr o v i q i n a r c r e c i m i e n t o t :isic:o reduc ido . L.os pacientes t . i r i iden a pr-erxentdr burt-ri a p e t i t c i , y e r o pueden man. i+rs tnr o . iFwI -ea , e j tea tu r - rea f a x u * : . ~ ; r r e , d ~
v i ta in i r i i cas .
,
l a c t a j t e z y rriñus, que se L r a n s m ? t ~ corm t.ar acter . r ' t..' . C.' . L. d i r,i>
distrr;t%ion ,abdominal ~ tono rrwzcu?ar ba JC3 y' de r I il 1 C'I~ic 1 i < 5
18

..
_. .
- -
...
-3 INGENIERIL I

L
Cuando )E s o s p e c h a en+er'rriedad pancr e a t i c a i a inves t i ga .c i c r r i puede requerir , p l aca5 abdom ina l e s , sEr ?es y a s t r o i n test i r i~ l es a l t a s , a n y i oyr-af id, col ar ig iogra .+ i a t r a n s h c p a t i c a , pancr-eat.ogt-aí i a y e s t n d i o s de u l l t r a s o n i d o . Para este t . i p o de e r ; t u d i o s , se n e c e s i t a n bas icament .e d o s , t i p o z . d e a p a r a t o s cuyo + u n c i o ? a m i e n t o SE, explicara b r e v emqn t e , a s i ccmci su utilidad en e:l d i a gnos t i c82 d e en f e rmedades d e l p a n c r e a s .
METODU DE DIAGNOSTICO FOR í1:FiiYOS >:
RAYOS X .---Es una r a d i a c i o r , ~ i l e c t r - o r n a q r i e t i c ~ i de lc!riyit.c!dl de onda muy cor-tia. Se o b t i e n e en tubos Cr-ookes, pero e5 p r e i e r i b l e emp l ea r los t u b o s d e Coolidge, e s p e c i a l m e n t e d i s e ñ a d o s a i e f e c t c i . Se les 1;ama it:ambien rayos be f k e n t g e n , e r i h o n o r d e l m e d i c o t)Lis? los d e a c u b r i o a c c i d e n t a l m e n t e , estcis ciitirnos coristari d e un C ~ C D ~ O y cI@ un anodo; e1 catodo es cin i i Icimerito de tcini igterio o de o.tr o m a t e r i a i , a l ser c a l e n t a d o po r e1 paso de utia coi"r1entc:. elrc:trici.i, emite electr-ones, los que a l chi:jcar con al dnodo se eitat:lrc;i una d i f e r e n c i . r de p o t e n c i a l que a c e l e r a a , l i i s electr.cjii<+sr Los r~ayos X imprec i o r i an p l a c a s fo.tograf 1i:a.j e.ipei:iales y pr-üvotran
tienen qrain pode r p e n e t r a n t e . S i penett-scion depende d 2 l a icir."-' &gi ' It.id de o,-,dj y p a , supuesto, d e ia r;a%:.tir a l e z a del ct.ier-pa que iirs absorbe. 10% mas pene t r a r - ! t e& 5,c:)i; l a s ii(i mci?er i w C y i t i i d d r oi.ida9 iids t i~ieso- ->cm mas o p a s o s íat3scPr beritljs! q c t e 10s m w x u 1 . m " i: 5 i. a d i f f t - e n c i d d e ¿+sor-cion prodLicE! lus tonk.r -aste5 C ) L ~ r egis,ti.,i I o placa r a d i o g r a i i c a . Los rayos poco pfr.netr.a:ii.i-s se 11.arnari blaridcir; 'f
ios ;riiiy per!etif-ante.; se 11 aman cicir 05 .
611 y ? r absorbidos por c u e r p o s f I ~ t o r ecentes, lo.- r a y o s pii)c:ILic.en f enomenos d e f l u o r e s c e n c i a , ec, d e c i r , exc i Lan l a emision de 1t.i-
i v i 5 i b l e i) u l t r - a v i o l e t a ) de 1oriyit.rrd de onda mrrcItio m f ? n o t - quí- i 6 i it ellos, es.ka p r o p i e d a d se u t i l i z a isri l a r . a f l i o s c o p i a , q u e eiriplea:t p a n t a l l a 5 .i:I~mrescente5 par a toi-riat~ v i e , i b l e s las d i 5et-ei.ncirAc de absorczian d f .io5 rayos X en el cuer~pcj Iiurriai.~;~. Ahor ri se t1ab1ar-a d e los compone?n.be=, a d i c i u n ñ l c s a:. i;i!t;o d e r ~ d y c i s ?:, e n c o n t r a d o s ei'i NI equipe r a d i ü g r af I co : .-free t i 4- i c driür. 1-5 d e a 1 t o vo l t a j i:: .--i-rdiisfor-rnaocii.- d e a l t o vo l td j e . - Au.inierita e1 vú1 t a j e nproi:imadaniriii1.e
.-Circuito a, ; t i i>rect i f i c a d o r :- ( i i c ~ i r i t . i i . r t a er i apar atos p o r . t a t i l e s , j d j L i r c . i i i i o di? 1 r e c t i + i c a d o r . U > Ci rcu i t o di? 2 r e c t i t i c a d o r - e s . c j C i r c l i i t o di? 4 r - e c t i f i c a d o r e s . d j C i r c u i t o 0,s & r-ect i f i cadores . e) C i r c u i L o di? 12 r - e c t i í i c a d o i e s .
I
ia flL<Oresciei-nc:i¿i d e ciertos tuerpos. Se! prypagan en iii-tes r-ectii Y
4 O i l ver.c.5 ~;1~!i:)-~x)c! v o l t s a :,o y I'oci i:vol'cs> .
'>Ci L.

...I
I-
. ,. r_
SL
UNIDAD DE RAYOS X BASICA.

La a:iment.acion d e l c i r c u i t o SE' c.at-iecta mediant.e l os i r i t e r v i r p t . o r r s si y c2.
Sz p e r m i t e adaptar - l a un idad a i v o l t k j e d e , l a l i n e a y e l v u i C i m e t r c.i "V", s i r v e para monitor-eos SI esa a d a p t a c i u n f u e c o t - r e c t a . E l i iw t e r rup t o i - Sa s e l e c c i o n a Lir io d e 1 0 % d i + e r ent . es voltajes qus! se a p l i c a n a i t r a n s f o r m a d o r de alto v o l t a j e . i:l v i j lC . imet ro " i . V ' ' . I
deb idamen t e c i a l i b r a d o c on l a r e s i s t e n c i a ñz, mide i r dd i t e c t am fmte el k i l o v o l t a j e aplicado a l tiibo. La re.-. = i = t e r i c i a .- Hi c o n t r o l a l a cur-r,iei..t.e i r p l i r a d a a l t r .a i i s fo r ~ i a d ~ : ~
de f i l a m e n t . o s , 1 u e y o e n t o n c e s , a IC< c o r r - i e n t e d e l í i l amerdc , . E: l inst.i-iimenI.o marcador "mA" i n d i c a d i r e c t a m e n t e , l a carr ieni:.e del tubo d e rayos . X. E l i n t e r v i i l o d e l d i spa r o se i n i c i a a i cer-r-ar el. inter rupI.oi- ~ ~ i ~ i ~ < l
y ter-mina cil ,Final d e l tiernpo p,reselecciona$o. La pisca ab-üriiinal puede demostrar- cal c ~ t l us pan c: t - ~ eat i c o$,, s eña l e s ; dc i i i ?o local en la p a n c r e a t i t i s agrda y u r i a masa titi t . ~ , j i d o ttl ando si e:.: i ste un sew joqc i i 5t.e .voliiriii n o k s t i "
i r i d i t . e c t o 5 de t r a n s t o r n o parir:yeatic:o, ct3mi j in ip i ' es ione i ; i u b r ~ , el duod5no en l a p a n c r e a t i t i s c t - o i i i ca o i i r i el c : . a k ~ c l r i o m a rie :.A i o . b e ~ a de p a n c r e a s , ensanchami en t o del a s c ~ WI ei. =rudoquiste i., z . a r c : i n o m a voluiiiinosu, y p l i e g u e s d i i od e i i a l e s edynatac.stis F'II l d p a n c r e a t i t.is
seudoqui stes !I un p a n c r e a s muy eaemaCo!;o. ,S i lor, siyrti js d ~ o d e i i a I e %
<
La ser ie g a s t r o i n t e s t i n a l , a x , , p;.,edr d e s i u b r i r 551 y!lcl5
ag~ida. ids pr e s z o n y s sobr-e el eiit.omay!:; puederi pv'oduc..ir. I LIS
s o n equi vcicoo~, l a duoc l anoy ra i i a t ? i ~ r . ' i i i j n ~ c a iirele r:xiar'ar i a s l ~ . u a c l o n . , , La angiogr-a+i:s e s , l a deter-miria.triun ,de 1.,3 disposition d e .,asti5 san y i i i neo-, y :l i n f a t i c r ~ 71 n ti i ,=ecc i orb , r:cjmo p u r cap i 1 ar uscc~p >. f l L i r - o s cop i a l o r a d i o g r a f i a . En r a d i u l u g ~ a 5s u. t ; l i -n p a r a ia v ' i s ~ < a l i i a c i o n de? vases saiiqkxineos niedi ai-ite 1 a i !?yecc i on de,,wia i us ta t i c i EA r - a c i i opaca r m i:ux i ca. L.a a n y i o g r a f i a p a n c 7 e a t i c a ,suele poríc-i- d w n ü s ? r ai; NI tumor p a n c r e a t i c o qi.ie n o seria d i a y i i o ~ t i r : a b I e eii otr a .for.md, y e i > j nL~ , c t l o s
casoc, puede d r s f i n q u i r e n t r e ca.r.cirionia y 1.a masa i n d i i r a d a de i.ina p a n c r e a t i t i a ! ;ronica. L.os seuduiqcxiste-rj -re ~ d t - n f i i f i ia i-i t: por- a n g i o y r a f i a : La $ o l a n y i o g r a f i a t ranshapat i c rd . p e u - m i C e c jpac i f ic:ar. 10s coiiductci-. t i e p a t i c o s y 41L c o l e d o c o en presenc r i4 d e i c - ' r . e t IClií, Luanda las. ccs lar ig ioqr-a l i as busalec. e i~i..l'a.veriíis.rs sneleri i -e i? .u l tar inc?+ I C ~ C : E ' S .
t>r. kntrodac :e p y v i a percut.ariea , ~ m o agrtj,~ o uiid sonda er-, l a substanci,t hepat ica , sci pene-t.ro,iriori en ei ccmducCo b i i i a r ~ d i l a t a d o puede cumprubai-se a s p i r a n d o bilis. L y e g o 'x i n y e c t a el rrial.c;r-iai cia cíJr;;raste y st? l o g r a la . , o pac i f icaciori de cündc ic tos tiepa.l. icus y coleduco. L.u o p a c i f i c a c i o n de l os c.oriduc.-os cuciií: lograrse i r i c lusc , cuando no esí:ari d i ;atados. Err -1 p a c i e n t e ictericti i a c , o l arigi iigral: i a t r .;iristiepati c a niu.cti.ts v e c e s ayuil;i a d i s t i n g u i r er!tie u r i $ a l c : d o di- coli:docq c iin t i irnor- de co!id:.tctos s i i i i a r e i , y una c i b s t r u.c.cic!n ext:i.ri,sa del c : o l edoco pur urda
22

masa pancreat icd . J , La te5riir::a mas nueva de ld c u l a r i y i u p a n c r e a t u y r a i i a r e t rug raoa endoscapica, que inF lu f e swidar la ampolla medrarit? un duodenuacopi or parece ,ut 1 1 para <ieniastrar- lesiones panc.reatrcñs in f lamator . ids y neoplasicas. * La pancreatogr;af i a es,la r -ad iogt -a i ia del paric:reas e fectuada durari,t,e la exp la rac ion qu i ru rg i ca , 4.e ?nyectir uri m e d i o cJe ~ u ~ t ~ r a s t e : h id ruso lub l e tin e l c o n d u c t o pancr-elatico y I d p e l l c u l ü se t o m a ccm el abdoniei-1 abi~er-to.
. . . . .^.,..^,...,....-._I- ...-. . ,. . - ~ . . .

La t i t i l i d a d d e l ultra son id c.^, cciiiici het-r-amimita d e d i a g i i u s t i c o , %e basa en el tiecho d e c l u e medios de d:i Fer-ente d e n s i d a d prudu:cari
.. reflexiones Liiarido un t i a i ~.rltrciscsiiicc. i r - i c ide sobre la supe r i i c i e qLte separ,& -ir. med i o d e l o.tr-o, coniiidet-aridi, i a s i g u i e n t e +iclu~-a:
~,
! i
PRINCIPIO DfZ ULTRASONIDO ID4 MSDIOS DE DIFERENTS DENSIDAD.
e n l a -figura " T " es un trarisdur.iior , ~ i i t t - a s o t ~ i c o ~ used, i . t i i
d i s p o s i t i v o c apa z d e g e n e r a r orildas u i1 : raso i i i cas . S i "7. ' ' emte k<n frente d e cinuias u l t r a s u n i c a s 'y d i c h a t r e n t e v i a j a en l a a i r r c c . : i on i n d i c a d a hasta l l e g a r a l a s u p e r f i c ; e I. que separ a al medio I del med i o 2, p a r t e d e l a e n e r g i d u]. i r rasor i i ca co r i t in i i a pr .opayandose t m
l a misma d i r e t r c i o n y p a r t e e% re f l e jeda , y i - e g r ~ s a a:L trai;sduc:t.ür g e n e r a n d o iin "eco". E l prcx-esci 'SE; r-cipit.e, en irada s u p e r , f i F i e d e rrontera, d i sminuyen+ l a e n e r g i a uitrasonrca cada ,vez. mas por f ennmenos d e absorcion en 10s u r s t k i i t o s meUiu5. idotesi- qi.ie. lo supe r f i c i e 1. prod i r ce ref lex~orres que iio r e t o r n a r , a l Crat.isdcict..o~. Los ecos se producen e:icli .tsivo.mente en a q u e l l a s i u p e r f i c : i e c ue iront.era, los C L i l e i son perF>e"dic.ular.-iii. a l eje loi igi t .c i i i i r ir i l del t r ansduc t o r . . Los ecos p r a d ~ : c i d o s pueden r ~ s u a l i r a r 5- e!! , un osc i 1 osc o p i J . P o r e j emp 1 o : , :kip wi g ase q cie itn a i i .en 1. e it .i t. c,. iis)o!i i. i a emite a i n t e r v a l o s r e g u l a r e s , <alr.ed+»i de l(.~f:K) por s,seyi..mc?o, , peqLieKOS "paq~etes" d e enel -g id u1 t t a i , u n i <.aw Ver í i ~ ] u t - O.
.. , . . . . .. .. ..... . ., ... ~" -..., .
\
I I I
I I I
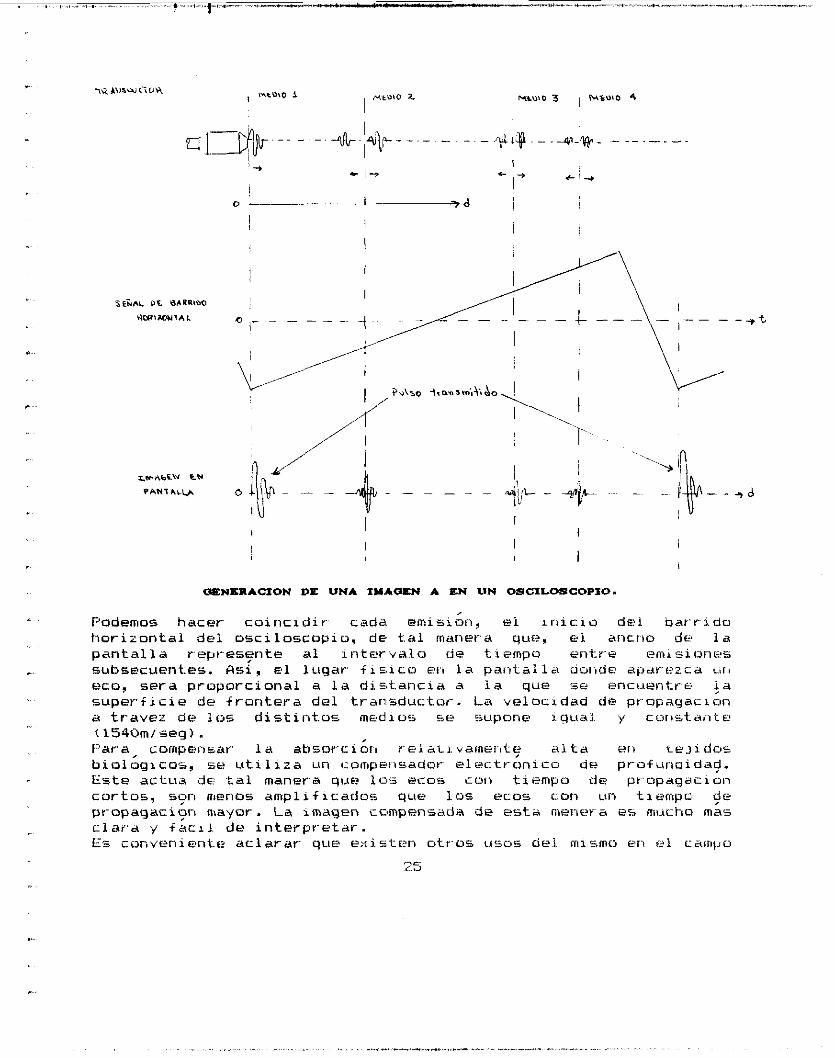
OIENSRACION D E UNA IY.hOIEN A EN IlN OSCILOSCOPIO.
, Podemos hacer coir ic idir cads emisiun, ei i n i c i o d e l ba r r i do hor izonta l d e i osc i l o s cop i o , d e tal rnanera que3 el arictio d e l a p a n t a l l a represente a1 i n t e r v a l o de t.iempo en-tr-e emisiones
.. subsecuent.es. &si, e l lugar f i c . ico eri l a p a n t a l l a oorrde a(,arezca L.%II
eco, s e r a proporcional a l a dio,taricia a l a que i5e encuentre J a s u p e r f i c i e de f r on t e r a d e l transductor-. La velocrdad de propagacicin a t ravez d e 10s d i s t i n t o s m e d i o s sc: i supone xgual. y cor is ta i i te í1540m/seg). f:'ara, compensar l a ahsorciort reiai . i .vamer~~t~ alta e11 teJj .dos b i o l o g i c a s , se u t i l i z a un compeiisador- e l e c t r on i co d e profuriaidag. Este ac tc ia d ~ c -tal manera qt.w 10.;- ~ C G % cor) tiempo de pr-npagacion c a r t u s , s ~ r i menoLj amplif icradoc. que 10% ecos con un tiempos $e pr-opagacion mayor. La imagen cnmpensada de esta mener es mucho, mas c l a r a y íac.11 d e i n t e rp r e t a r . Es conver1ient.e a c l a r a r que existen otr.os LASOS c i d m i s m o en til campo
m c i. -3

".
medico: 1 . -Nebuiizadurrs. u l t rasonicos . - : Eie ricq~1ean en i i iha loterapia y sun importantes porque produ5en neblina.; sumamente f i n a s s go ta s con imas cuantas micras,de diametrcr. L.-Layador,a.;. yJfrasonicas.- St. emplean en l a l impieza de a ~ ~ ~ t j i a s h i poder m i c a5 IZ i n st r umen t a 1 qui r ur g i (I o. 3:-1"era~ia;. 4.-Deteccion mcncvimiento,y- f,~l~i~~:üt.i 1 i:<antio el eTecto Ljoppier de un haz u l t r a son i co continuo. L.a ul t rasonogra f i a suel? poder distiriyuir. L i l t seirdoqui stf? pancr-eatico d e una masa s o l i d a .
,

27

.,..
FAI'ICHEAS A R T I F I C I A L
INTRODUCCION
E l p a n c r e a s a r t i f i c i a l y ¡a. bomba de i n s u i i r i a p o r t a t i l son recientes d e s a r r o l l o s e n d i a i b e t o l o g í a . S i n i m p o r t a r su c0r t .a h i s t o r i a , a p a r e c e n a p r o p i a d o s p a r a l a r e v i s i ó n d e l a s p o s i b i l i d a d e s t e r a p e u t i c a s p r e s e n t e s y fu tura i s o f r e c i d a s p o r es ta nueva t é c n i c a . La t e r a p i a d e i n s u l i n a c o n v e n c i o n a l usada d u r a n t e l a s últ , imcts d é cadas , no e!.tubo d i r i g i d a a l r e e m p l a z o f i s i o l b q i c o d e knsu l i r i a , p r i n c i p a l m e n t e es ta o p t 6 p o r l a compen%ac ión h i p o e hiper -g i sc f :mic .a d e l me t abo l i sino. Por el corit.rai-io, l a t e r a p i a d e i n s u i i n a moderna se basa scjbr-e, el r es tab lec i .mi . e r . i t o d e l a inormog l i cemia . I-lay una d i f e r e n c i a eserTIcia1 entre e s t a s d o s formas d e t r a t a m i e n t u . La primer'ck r e p r e s e n t a una t e r a p i a p r i m i t i v a d e compensac, ión, mientras que :la segunda a vanza e s p e r i z ado ramen t e a una v e r d a d e r a r e h a b i 1 i tación. La h i s t o r i a ati l p á n c r e a s a r t . i . f i c i a 1 esta d i v i d i d a en t r e s -fasei.: ~ ! 1 pasado , cuando este se d e s a r r o l Ió; el pr . eser i t e , c a r a c t e r - i z a d o pcir- l a a p l i c a c i b n d e l a s bombas d e insul : ,na p o r t a k i l y l a i n t e n s i f i c a - c i ón d e l a t e r a p i a d e i r i su l i r i a c o n v e n c i o n a l ; y e l f u t u r o , el c u á l a v a n z a r á a e l pá r i c r eas a r t . i f i c i a ¡ i m p l a n t a b l e í i 3 .
26

INVESTIGACIONES
En l a a c t u a l i d a d se e s t á n d e sa r - r o l i andu p á n c r e a s b i o a r t i f i c l a l e s b a s a d o s en mode l o s teóricos y e x p e r i m e t a i e s con ios cuales SE t r a t a de a l c a n z a r l a s más ce rca r id5 carac.terist.icas + i s i o l o g i c a s p a r a u s o humano. S e hacen i r i v e a t i g a c i o n e s s o b r e l a secreción d e i r r s u l i n a por- med i o s t>asados eri l a a p l i c a c i ó n de c é l u l a s a n i m a l e s , 5e meriii i ona p o r e j e m p l o , el p á n c r e a s a r t i f i c i a l b i o h i b t - i d o , basado i?ii i s1o t c : s c an inos , , en =!;.te d i s p o s i t i v o l a s cé lc i ias b e t a d e 10.5 islstes e s t a n a g rupadas en ! s i e t e ó r g a n o s b i o h i b r i d o s y separadas d e l a cor-r-ieilte sar igui riea por una membrama d e l giada y semi per-meabl e, que permi te el paso d e pcrquel'las mo l&cu l a s t a l e s como l a g l u c o s a e i r i su l i r i a , m i e n t r a s e:<t:Liiye 1 iri+ocitos y a n t i c u e r p o 5 i n v o l u c r - a d o s en el.. inmurtorecliciio,. Es p o r t a n t o p o s i b l e u sa r islotes de ar i ima l es , que están mas f : a ck lmen t e d i s p o n i b l e s que los humanos. Además p u e s t o que 1 a Di. a b e t e 3 . i l ipo I , puede c e r una en f e rmedad a u t o i rimurre, i a membrana sam ipe rmeab l e t amb i en p r o t e g e a 105 i s i c i t e s de posibles ataques ;iut(~ii.nrnunes a l huesped d i a b é t i cu- despc ies del t.r aIisp1 a1t.t.e a este . E l páncrc!as. b i o h i b r i d o p r ~ e s e n t b l i b e r a c i ó n de i n s u ; l i n a e v e n t u a l m e n t e e s t a b l e pur v a r i a . s semanas y i::ontinua r e:spu
Este panci -sa= 7epresen t . a r . i i i a impor tar i te v e n t a j a ya que iio i i i q u i e r e de alimenCacic5n e x t e r n a y no t i e n e macan1smos yue pciedan c a ~ i s ~ ? . r + a l l a s , este s i s t e m a sigue en i n v e s t i g a c i ó n , j a que s o i u e s t a basado en l a s e c r e c i ó n d e i n s u l i n a , po r i o q ~ \ e se r istudii i l a in- f l u e n c i a de ot ras hor-inoiias, como e: giirc.ayori y l a s o m a t o s t a t i i b a e n el pAncrea:; b i o h i b r i d o , $2; é,::itrj us estos es+tudio%, c o n d u c i r í a a l a imp lan t . ac ibn e n el hombre CL3. ütr -as i n v e s t i g a c i o n e s %e han involuirado en l a r e p 1 i . i a c i b n Je i s lo tes t r a n s p i a n t a d o s en i i I~~il i : iOdF'F1i.ridierittcs prw d i a b e t e s m e l l i t u s , er. l o que puede ayudar a ios pán i : r e a s a r C i f i c i a l e s ba sados en i5.l.otes pancreá t i c : o s , f a que aumen ta r í a v i d a di? eskf., d e b i d o a ia r -c iyer ierac ión c e l u l a r - de: 1.0s i:>:ates Cr,Si-i",plai.it.ados, eil
rl Iiurspzdi que se w i c ü n t . r a r i a n en rl párrrireas at t i + i i . i a l
nIcc;:iiiani.idar para estiinular .;.a i e p i i ~ . d c : i & i , ya que cic' o b s e r v ó r.nL.abari eri c a n t i d a d en i c x 5 p . i c . > . e r ~ e i is$! tt.a.ia,niri~~ti, i e r )
ra to i ,ss se hi:.u l a pr-uebai . ULii-ique la n i c o t i r i a m i d a se pr-opmie ñ ii.1~ t t i i rne r i i cdme i i t o squi ii parL, uso t,iimano, p r u e b a s c l í r ~ i c a s tori io5 trorripor-iririt.~~~. ~ i ,
debe rán s i x l l e v a d o s d cabü cur1 yr ñn pret.ai.h:iC>n, a l a 1i.i- d e lc< ohsw v a c i b n , cre que la i i i c ckrnarn ida puede c o n t r . i L s i t i t , ~ a la í i xn iac i t in d e tumore i . ! S i endo estu r.! o b o b i e , y a q u e es ta , puede tzi-ier una inter~+erencifi con el pro1 50 d e repar-acióri del DWi . L Z 3
y1 uc05a.
i inp 1 dii t ad=. p a r a e s t a 'se ci 5. c8 ex p a I ciientdl ii~w it.? 1 CI - ...


..~
I
."
* ..
. .
..
,
" .
.
..".
. ..
I-
.. .
. -
e n t r e otros pa ráme t r o s . E l mode l o iué escr i to e n e? ler i ,yua.je CLAMI tie . j i c i iu lac ión y p r i m e r o c o r - r i d o en una minicomputador-a , l a a .%ubr-utirias de o p t i m i z a c i ó n d e l g r a a i e n t e c:on.jugado, f u e r o n e s c r i t o s en For t ran . La t e o r i a d e c o n t r o l 6 p t i m o puede usarse para mos t r a r que este mode l o mate?mát ico d e un páncrea .s a r t i f i c i a i se c o r i t r o l a 6ptimameiit .e por un cioiit.i-3j. paso--a-paso, s i e m p r e que Liri c o n t r o l ó p t i m o exis.ta. Las suiucici! ie.?s núimericas a t.ai6.s pro¿l~mci?i de cori-tr-o1 ópt imo,pu.eden u s a r s e par~a i o r i s t r u i r l a b a s e d e l cor ioc i i r i i en to para on coritroiaticit r-ealimeri.taclo i . n t e l i g e n t e q u e tu rna r - í a l a i n f u s i ó n a a c t i v a r - s e o desdctrvar-i ,e on un est i lo casi optiinoCLi1 Además dti 105 mode l o s c o m p u t a c i o n a l e s , se d e s a r r u l l a r i utr-os, t.arnbien d e yrtrii i m p o r t a n c i a en los p a n c r e a s or t i f i c i a l e s . 'I es d e como s e r i a 5u f o rma y mater ia les usados p a r a una mejor- Tunc i6n . Como se rrienciorió a r r i b a un páncrea i , t j i o a r t i f i c i a l es uri d i s p o s i t i v o imp ia i - i t ab i e conectado a l d i a b é ' t i c o huesped como una d e r i v a c i c i n a r t e r i o v e n u s a , c o n t i e n e c e l u l a s seyr -egando insu l . i n a , separados UE
la s a n g r e por una membrana s em ipe rmeab l e par-a e v i t a r - - irircictr>c.ir'i-chn-o, esto se modela d e s d e un puritü , d e v i s t a de mecár1:c.a d e f l u i d o s para v c r . y ev ' a lua r l a s cor i .Lr ib i tc i .ones r ~ e s p e c t i v a s d e d i f u s i ó n y ~ i l t r a - f i l tr.ac:ibri a l a t r a n s f e r e n r r i a i i ~ : masa d e l a i n s u i r i i a y 51 ucosa . Lste a n á l i s . i s de t r - a n s f e r e n c i a de masa si- l l e v a a cabo tiacE: p a r a o b t e n e r una, g e o m e t r í a b p t i m a d e l d i s p o s i t i v o , e l cuál uri c a n a l s a n g u i n e 0 en +:orma d e U, r o d e a muy d e c e r c a a un c ompar t imen t o de i5iO'tes muy d e l g a d o f o rmado por- una membr ana p l a n a p l e g a d a . Uri modelo c o m p l e t o d e l i b e r - a c i ó n d e irisu1ic;a pur este . d i s p o s i t i v o se d e s a r r o l l a y se compara con d a t o s i n - - v i t r o ab t . en i do5 c on islotes d e tvata. E s t e m o d e l o i n d i c a ycie l a p e r m e a b i l i d a d de la membrana i- , idr-aci i ica d e b e r i a ser maynr por- un í a c t o r de 1 0 para m e j o r a r el func i onamie r i t o , a p e s a r que l a d e p o i i a c r i i u n i t r i l o d i o buen r e s u l t a d o C 6 1 . S i g u i e n d o c on estos modelos, eii I G S e:;per, imwitüs i e a l i z a d o s se han e n c o n t r a d o comp1icac::ones a lar~gc:, p l a z o a s o c i d d o s con e1 t r a t a m i e n t o de ~3iabet.e.s por i r i y c c c i o i i e 5 de i r isui ina y es d e b i d o a a l c a r e n c i a d e iiori+:rol de insctl. iria y gi.i.ic:ciia f i s i o l 6 g i c a , pero l a r-espuesta de i n s i i l i r i a d l a e s t imu l a c i c i n de g l LlCosa e11 páncrea i , ti ut-, i Lr i ti CJ ar. t i f 1 c i a l p fw m d n C?L e i r iaceptabLemer i t e l e n t a . l o i r . e s u l t a d o 5 d e mode lac i ó r i ile es.te disposi t i v u , e n t r a n s p o r - t e de scili .tto-, arroja que, incremerit i tr ido iii t r - a r i spo r t e c o n e c t i v o m e j o r a í i y r i x f i c a t i v a m e n t r l a i-e.spiresta a iit glucocja, ademas p r o p o r c i o n a c:omprensi6n fundamenta l c f enónienos que yobier-rran el t ransporte . de solutos e n el pAncr-e.:<s u i u a r k r i i c i a i , y a l a hor-a d e Imp1oi?tar- el pAnc.r-eas b i c i h i b r i d o a r - t i i r c i a i . se presentan pi-oblenias a d i c : i o r i a i e s d los d i c : h o s an'tet~ i o r -mente , cuando se inencior;6 este t i p ü d e pánc-r-ea-j, y a que ! a wascular-izacitSri i n t e r n a no rma lmente pr.esririCr :e ( j i e r .de despiier: dc-i a i s l ami en t o, f or z ando a 1 os i s i ,tit ei5 ti depender- p t- i nc i pa I mei'i i.. e d e l a d i + u s i ó r i esterna e i n t e r n a , pd ra pr upor ( i iunar-se ill'i cimlji snte
3 1

donde las células sobrevivan y secreten ~ n s u l i n a , además la Sa1t .a de la pres ión de oxigeno sanyiuiriea demuestra que disminuye la secrecibr; de i n su l i n a , a lo cus.1 los modelos matematicoa pueden diir condic iones de d i seño r eque r idas pard preservar l a c . in l t ic :a
.~ intrinseca de secrecibn d e insuii ina C7lCSl.
..
., . .

DISPOSITIVOS EN USO CLINICCI Y TERAPIA
.. .
En el i n i c i o ije este t r a b a j o se menc ionó d e l p r e s e n t e en pánc ; reas a r t i f i c i a l , ~omo bombas d e i r i s u l i n a p o r t a t . i l , p a r o e s t a s no scm tanto. Estos s i s t e m a s s on e 1 e c : t r ó n i c o s l os c u a l e s r:oriliriuanient.e miden l a r onc . im t r a c i 6n d e i j l u c c ~ a sangu i r i ea e i r i fus i o r i an i n s u l i n a 6 dextrosa según el n i v e l s a n g u i n e o , y es h e c h o i n t r a v enosamen t e c:on una bomba p e r ~ i s t a l t i c a r l a cual i e a c t i v a au t oma t i c amen t e c ada minuto . LijEj algor-i tmoi y c o n s t a n t e s t - e g i s t r a d o a son gua rdados en 1 a memoria C ~ E ? 1,a computadora y SE! usan p a r a p rog ramar e l pánc:r-eas a r t i i i c i a l . Estos d i s p o s i t i v o s se usan e n c ; i r u g i t ~ y C C ~ S D S d e e m e r g e n c i a d e p a c i e n t e s d i a b é t i c o s , as1 como sn e1 c á l c u l o de 5us requer imient . c ) s d e insulinii. iIdemás el p á n c r e a s ar t i f i c i a i es L W I ~ t i e r r am i en t a v a l u a b l e eri l a i n v e s t i g a c i o n c l i i i i c a de la c i iabe t . es m e l l i t u s . De hecho , el ú n i c o p r ob l ema d e este apar-atu es l a m i r i i a t i u r i ~ . a c i 61? per o l a i i i V e s t l g a c i 611 h a c i a este pr&lf?nia iiG l l e v a d c a b o en l a a c t u a l i d a d p o r i n v e s t i g a d o r e s en este campo. C 4 1 Y los t rabch jc6 r e a l i z a d o s par-a t e r a p i a de insL.$ l i r ia convenc ior i c i l conducier .or i para el desar-r,olSi , d e L i r i páncr-eas erii . i6cri: io a r - t i f i c i d l ( F E A ) . Ez1.r' o i i s a r r o l l o c o n t i e n e t.r-s% p a r t e s eserici ales: Liri i e r i s c i r
d~ g i u c o s n , u r , i n y e c t o r de i n s u l i r í a y u n s:stema I ui-i-itt.
Censor- d e q l ~ c o s a . ... E'r¿ 'vee i ni c.)r n i x I di> i n5 i d~ i i. d : ~ e c < ci; oi 8 i 1 ,' 2 i <.!s de ~ i i < i u s ~ i r'ri ia sangre3 i i i , L.A~:. tic.) ~ i l i r ~ I I o ~ i n d l c e d ~ : ':a c ~ l r d a o Ou id'; 3ecr-ec : iones enric!x:r 1 pánc r eds . Las s i s k . e m i i s L I E moni cor izi . icióri del páncr-eas s~):-i itwieroz,c>=$ las keciiiiias eriziniá t i c a s s on ].as más c o t i d i a n a s , ? o ibás rec ier i t . .e tia sidr j eri i d u t i 1 i zdc i 6ri de 1 a s e i i z i mas i n m o v : ~ 1 i 2.ads.s y' d e t-lectr-od05, e s p e c i f i c o s para glucosa. I n y e c t o r . d e i r i su1ina. - Sciminist.ra l a i n s i i I i n a r e q u e r i d a a la c-;irigre para el mariIreiiimierito d e los n i v e l e s de c o n c e r i t r a c i ó n de g l u c o s a s angu inea . Hciy en d ía tiay mucticjs 31sl.fmas de i r iTus iór i a u t o m á t i c o s de i insLi l ina: bombas de h o s p i t a l (pesadas y n o ti--ari%port.ableEi) y bombas por- i ia t i les .Las bombas ;le t-iosk>ital son c.omiirimt.r,.te ri.;addc; í i r l
e l (PEf i ) . a i s t e m a fuen te . - -Se e n c u e n t r a s i tuac2a '.- dltr -e el rrtor-iltor d e q l u c o ~ , a Y e; rinyector- di- i n s u l i n a , p a r o a ~ ~ i s t a r - el + l u j o de Ihciuiiria ioda, ias v e c e s qi:e r e q u i e r a rl F,ac i e r i t e , así ciimü pdt'd 1 Inir-irar las uluccuaciortei-; de azúcar i r , I;ar'.yr L' de:iir' , l ie L . l l l I aiiyc4 p~E5C2iF:CCLcXihUD. La @$6?Ci i v rdad , .5*gi:.l- *dad y aiiapt.acióri d e i P E A i j epende pi imoird ia lmer i te d e l %I kitema Pcierite,ba. jo las modal .idadesi iie cune..:ión da azúcar- sangiuiriec ii d r i t..iernpo dado , y i a direcc i6r i i:ie 10s cambiori dfol a z ú c a r sangu i r i eo a r a z ó n d e l a i n i u c i ó r i tie r r i s i i i i na . Estos son los a1gor i t .mos d e coi-itrol y ion í i i n c i ó n d e 10s i i i . v e l e s d e azi-icor sangu i r i ea que s o r i : menor- que :Xi y 7 0 , e n t r e 7 0 y 1 5 C i , y s o b r e 150 mg/dl. La cant idad d e l f l u j o de i n s u l i n a se d e t e r m i n a pcw el algor- i tmci , de ia azúcar en la s a n g r e proyect.rrda, y c a l c u l a d a iii.rec.tainente por el
P "
d i s p o s i t i v o . E l FEA t amb i en comprende un d i n á m i c o mE'can1smc) d e a l a rma capár d e i n t e r r u m p i r l a i r i y e c c i ó n d e i n s u l i n a si el q r a d i e r i t e es mínimo ( B a j o - - p e l i g r o ) ,ó e s eí.cesiv1.i y a l c a n z a n i ~ ; e l e s d e azílcar s a n g u i n e o , el cual estaii b d j t ~ i .
La c o n t i n u a i n y e c c i 6 n de i t i s u l i n a in t t - avenosa es solo capá z d e l a
dar un p e r f e c t o c o r i o c i m i r n t o ue ios r - equer - im i en tos d e insuiinC-L de cLirso . ~ ,a r - lab l i i s o b r e ei per-iodci del l a s v e i n t i c L i a t r o ho ra s . L.os r equei' i miontos b a s a l e s se i i i c r ementan d u r a n t c l a segunda m i t a d d e i d i d , y er: el t i e m p o de cnmida ,nec :es i ta est.ar proporcioria1nierit .e nias a l t o que i i 1 desayuno , a lmcierzu u c ena . E l FEA es t.ainbién u t i 1 p a r a e.=-t.udiar- y t r a t a r - cri.sis d i a b é t i c a s , además p a r a ayudar- e n el t.rataiiiiento d i f i c u l t a d e s d i a b é t i c a s . t l O 1 . (-ihora i a rieciEz.idad p a r a un PEA por t . a t i 1 , miniatur .c i zado e imp lan t&- b l e es a l t a m e n t e p r i o r i t a r i o y i e ha t r i L i n f a d o cc>n Liri s i s t e m a i . i p o a g u j a , coi'i c i a r - a c t e r i s t i c a s adecuada.; a un s i s t e m a d e contv-o1 p o r t a t i l a l a z o c e r r a d o . E l FEA m i n i a t i i r i z a d o consiste d e &.in 5ensor- t i p o a y u j a con t.iria rnemnrarna de a l c o h o l p o l i v i n i i ico i i i d r o f í l i c o , p a r a aumentar- 1 a t , i o c o r n p a t i b i l i d a d d e l sensor-. uiob bombas par-a martejar- l a unidad¡ de insrrl i í ia y glcicagor; , y i.in s ic , tema cornputari.trAdo basado en LETI
m i i I- op I. oc C-EiaC or , par a 1 u s c ái 1 c. LI 1 os d e I. a i c: cm r~ en t r ai: i one5, d e yli. icosa, g l i c a g o n y l a memc1rizacr6n de l a s medic:ione% ci e i o n c e n t r a i i ori i?s de glucosa. haE. ta por m a s d e ve i r i t i cL ia t . ro iii-iras, además una ba te r i a d e l i t i o para l a a l i m e n t a c i ó n del s5.st.ema. E l mrmitut-eo c o n t i n u o d e g1ucoE.a es 1.m senscv Irr5;ertado en te:,jic¡o subrutaneo de el b r a z o o abdomen Jt? ~ v o l c i n t a r i o s d i a b d t i c o s y ';-.anos r e v s l a r o n que l a s c o n c e n t r - a c i o n e s de g l u c o s a en t s . j . t d o auhcutaneo t u e r o n menores , p e r o a l t a m e n t e c o r r e l a c i o i i a d o s en el i n t e r v a l o Oe 49 a ,358 iny/i?i. 5e h i z o una comparac i ón e n t r e @I conirol q l l c i e m i c o por i r\Cus ión de r n s u l i n a i r , t , ? a v e r ~ o z a y el de subcu taneo a l a z o c e r r a d o F'EH , s i e n n a la s u p e r i o r i z a d d e l s i s t e m a r e a l imen tado i:lar.amente demost rada . Z)Ltr-ant.e l a r a g u l a c i 6 n y l i c i i m i c a coriti .riua, i a s v a r r i a c i o n e s dia tl d i a de los r e q L i e r i m i e n t o s d e i n s u l i n a f u e r o n r e c o n o c i d o s eii c a n t i d a d e s d e i n f u s i ó n dfi i n s u l i n a b a s a l y p o s t a l i m e n t a r - i u s . eii i-.espiiest.a a c om idas y ejercicios i d e n t i c o s . E s t o s da to$ , -;rryieren l a f a c t i b i l i d a d d e l contr-o? cie glucosa en p a c i e n t e s d i a b é t i c o s a l a r g o p l a z o cciri un PEG p o r t a t i l , e i n d i c a que p a r a s u p e r a r l os camb i o s en car a c t e r i s t i c a s m e t a t o l i . c a s i n d i v i d u a l e s r jobre una b a s e de paso a paso, un s i s t e m a d e con t r - c l g l i c e m i c o a l a z o ce r - rado puede ser e s e n c i a l p a r a p a c i eist.es d i a b é t i c o s a m b u l a t o r i o s . C l l i Se tia reportlado que en di v e r s a s a p l icac.ianc-s d e modelos de s i m u l a c i ó n et: p á n c r e a s ; r r t i - i f i c i a l e s l l a s computador-as ji-iegari i i r i
p a p e l a m p l i o , t amb i én se ha i d u e x t e n d i e n d o .n o t r a s ár-ea5 d e e v a l u a c i o n e s p r e c l í n i c a s y t e r a p 6 u t i c a s . En e1 át-ea d e t e r a p i a de l a d i a b e t e s , e x i s t e n r e s u l t a d a s de pr-ogramas que r-eproduceri con
54
n o r m a l i z a r el n i v e l d e l a gi i i i .r isa s angu inea , 'y' ei PEA puede ,cJ1 o
..

gran e x a c t i t u d las r e s p u e s t a s cle d i a b e t o l o g i s t a s en la t e r a p i a de 1 n su 1 i n a C í 2 3 . . .
..
r
,, ,.
.
VENTAJAS Y DESVENTAJAS
En d e s a r r o l l a d e l p b n c r e a s a r . t i C i c i a l i m p l a n t a b l e mues t ra Liri g r a n compromiso , d e b i d o a p r o b l e m a s r e l a c i o n a d o s e n t r e si. Unos son d e b i d o s a l a f a l t a d e c e l u l a s g e n e r a d o r a s d e i n s u l i n e i d e t i p o humano y los r e s u e l v e n con c d l u l a s d e an ima l e s .C27 ,p e rn se e n f r e n t a n a los p r o b l e m a s d e l c o n t r o l d e la i n s u l i n a g e n e r a d o s p o r l a mecan i ca d e f l u i d o s , c l i fus i6r1 t r a n f e r e n c i a d e masaI inniunorect iazo 6 d i s e ñ o 6 p t i m o d e los d i s p o s i t i v o s adecuados en ;.orma geomét r - i ca , m a t e r i a l e 5 , u l a s u p e r v i v e n c i a d e los islotes p r o d u c t o r e s d e i n s u l i n a d en t . r o d e l p a n c r e a s h i b r i d o e tc : . L2lC63C7ILUl. S i e m p r e s a l t a r l a l a pregunta , , P o r q u e n o se hace un e n f o q u e a los es . tud i os de t r a r i s p l a n t e s p a n c r e á t i cos que p r e s e n t a n buenos resultados?, en los c u a l e s se nlotan g r a n d e s mejor-as en me tabo l i smo , n e u r o p a t i a s , r e t i n o p a t i a s o m i c , r o c i r c u l a c i ó n p e r i f e r i c a entre c i t r o s padec im ien t , os . C l 6 1 en los c u a l e s el t . r -ansp lante p a n c r e a t i c u debmeria ser a n t e s de que l a s c o m p l i c a c i o n e s d e l a d i a b e t e s en ie r jan , a1 t i e m p o que i a n s i d e r a n d o e s t a idea no e s t a aun a c e p t a d a p o r q u e no se ha diaqno:s t . i cado c l a r a m e n t e . C131. P e r a un i n c o n v e n i e n t e i inport .ant ,e E ? x i s t e , y e?; e l t e j i d o p a n c r e a t i c o d i s p o n i b l e ( p a n c r e a s tiurnai.ios) , aderaár, d e s e y u i r 1 os pt uti1 e~lirí- gi?rieradof, fmr 1 os si s te ina i d e i'-echazc, i n m u n u l o y i c o a l & g a n o huesped, p o t par-te d e l cuer-po t-iilmaiio, c u m d o se s i e n t e i n ' i a d i c l o p o r otros i ry i rn ismos, que ¡-o +or-man p a r t e d e el mismu, s ean m ic roo r - gan i smos p a t ó y e n i ; ~ ~ 6 t-r-ainspl.antE!5 o ) - ya r i i c os (páncrear í , pulm6n, corazbii etc. i I
La o p c i ó n e n t o n c e s s i g u e e n t r e el p a n c r e a s endocrino b i o h i b r i d o i m p l a n t a b l e , el t r a n s p l a n t e p a n c r e á t i c o I los mé t odos d e infusión de in , z ,u l ina c o n v e n c i o n a i e s 6 d e i n f u s i ó n c i ln t i r iua d e i n s u l i n a sub- cutanea ( I C S I I S i e n d o q u e d e n t r o d e estos d o s irltimos met.odos, e l d e ( I i -51) se obser-<aron mejores c a r a c t e r i s t i c a s contra e1 c o n v e n c i o n a l L i41. Fer-o se inantis'ne l a e s p e c t a t i v a d e que será mas p o s i b l e d e s a r r o l l a r un p a n c r e a s i m p l a n t a b l e 'I q ~ t e seguir e s p e r a n d o siemr~r e l a d i s p o r i i b i I í dac l d e h r g a n o s humaiioc, 6 a i a r . s e s i empr-e a l n ie todos de i n y e c c i 6 n d e i n s u l i n a niuy inolestos p a r a el p a c i e n t e d i a b é t i c o i n d e p e n d i e n t e m e n t e d e su p r o p i a en f e rmedad .

,, ,
..
.-.
E l p á n c r e a s 'se c o n s i d e r a uno de Ins ór-gano5 más i m p o r t a n t e s riel c u e r p o humano, d e b i d o a s u s t r a r a c t e r i s t i c a s e n d ó c r i n a s y e::óc:riria5 p r i n c i p a l r n w v t e . Sus d i s f u n c i c ~ n e s a c a r r e a n una g r a n c a n t i d a d d e en f e rmedades . a l g u n a s POCO comunes, otra:; muy ctiiioci d a s er-i'tr~i l a s q u e se puede menc i onar l a UIAUETES . E5t.a en f e rmedad es s i l e n c i o s a , y e5 causada por d e T i c i e n c : i a ESI'I l a p r o d u c c i ó n de i n s u l i n a , es iJe tectab1.e l a mayor-la d e l a s v e c w cuando y a e s t a dec l a r -add , adeniás d e i ' daño f i s i c n a l a persona , , trae c o m p l i c a c i o n e s p s i c o l o y i a s , s o c i a l e í y e c o n o m i c a s p a r a el p a c i e n t e p o r cu idadws , med icamentos , dietas;, y c o n t r o l medico. El gran coc,l.uii s o c i o e c o n ó m i c o de e s t a d e f i c i e n c i a o r g á n i c a ll.e,#i> a l a n e c e sxdad d e d e 5 a r r . o l l a r una a l t e r n a . t i v a , el páncreas a r t . i i : i c i . a l i p o r t a t i i oie i m p l a n t a b l e ) . UE?sde su i n i c i o , l a s i n v e s t i g a c r i o r i e s han u t i l i z a d o d i f e r e n t e s me t odos y s i s t en i a s , ent.re los c u a l e s están: bombas d e i n f u s i ó n d e i . n s u i i n i , si mu1 a d o r e s matemá.l:i cos, d i s p o s i t i v o s b i o h i b r - i d o s con c é 1 ~ ; l a s d e a n i m a l e s , etc. ,par-a el d i s e ñ o y l a c o n s t r u c c i ó n d e l páriczr-@as a r t i f i c i a l . 'Todo esto hd g e n e r a d o inter& e n el ámb i tu d e l a i n g e r i i e r - i a b i o m e d i c a y m e d i c i n a en g e n e r a l , ya que a pesar' d e los pr-obleinas encunt . rados , la5 n o t i c i a s d e los res~i l tados de es.t as i n v e s t i g a c i o n e s son m a s opt in i i , s tas . E s t e t r a b a j o se p r e s e n t a c on r i ó t o d s l a i n f o r m a c i ó n qite se q u i s i e r . a d e b i d o a q u e ac t .ua lmente e n M d k i c o no se r í i a l i x a n t r a b a j o s sobre este d e s a r r o l l o , o no se han dado a cor~o~:ei-, s a l v o unci ericorit.t-,;rdo e n el I n s t i t d t o N a c i o n a l de l a N i i t r i c i ó n y se i n c l u y e a q u í . N o s o t r o s pensamos que el páncreas a r t i f , i c i a l (por-tat.: 1 (>/e i m p l a n t a b l e ; es ¡.ma g r a n c o n t r i b u c i ó n a l a .salud d e i n i i n i d a d de p e r s o n a s a q u e j a d a s p o r l a d i a b e t e s e n t r e ut.ras en+ermedades , ya que evi t,a grandeis m o l e s t i a s a l pac ie r - , t e , c a ~ i s a d o s p o r met.odris de i n f u s i ó n d e i r i s r r l i na a d o s i s , aunque estas sean nlciy b 1. el-! c a l c u l a d a s , el inargeri d e error es aúi? muy a l t o . S i f u e r a t r ü n s p l a n t e pancrea t . i i co , aunque se a l c a n z a r a e l B x i t o t o t a l ( n o inmunorechazo p o r e : j smplo ) , no , t i a b r i a páncrear j humanos suf icierites 'y se tiene q! ie seguir i n v e s t i g a n d o p a r a resolver este p r o b l e m a . En camb io con el p á n c r e a s a r t i f i c i a l , si s e r l a n estos más f a c i l m e n t e d i s p o n i b l e s , ~ se e v i t a r i a e s t a r esper-ando u r i donador . La d o s i s d e i n s u l i n a e s t a r í a dada i u t o m a t i c a m e n t e según por l a s concen t . rac i óiies d e gl ucosa I En base a l u d i c h o arit.erioririeriCe, se coiic:lLtye que 105 beriefiriI.os r e s u l t a n t e ~ s (de un p á n c r e a s ar t . i + i c i a l , s e r í a n d e t e r m i n a n t e s par a l a salud d e un gran niimero des l a p o b l a c i ó n humana, que padecer¡ d e l pánc r ea s : y con estos, el gran ahorro eCDnblliiC0 y d e a d o r de un t t -anSplar i te 15 i n y e c c i o n e s para l a s d o s i s i n s u l i r i i c a s d e por v i d a .

I_
.
...
'. .
* .
I. .
.,
.. .
...
., .
c..
- ,
1. -
2 . _.
.- 4 . ..-
4. -
c d. -.
6. .-
7:-
a. -
9. -
E. F-. PSr r i . f f e r and W. t::ernsr-. Use of A r t . i i i t . i a 1 P a n c r e a s and F o r - t a b l e I n s u l i n I n f u s i o n Pumps i n D i a b e t e s t h e r a p y : f:'a=-t 2 ' I
F ' resent , and Fu tu r e . A r t i S i c i a l Or-gans. 1985 9 ( L ' ) : 129-137
Yoshinich5ti Araki , etc. . i ? i ohy 'b r id A r - t i f i c i a l P'uricreas. Diabsite.i. 1985 vol. 34, September 850-854
C t e l l a r i C a n d l e r and &-ne Andersson . S t i m u l a t i o n o+ c e l l Rep1 i c a t i on i n T r a n s p l a n t e d Panc r ea t i . c I s 1 ets by N i c o t inlami d e 'Treatment.. T r ansp l an t . a t i on . j.968 VD^. 46, No. 1, J u l y .
B. N. i-iuny and K. W. L i n . Mu l t i -Func t i . on The r . apeu t i c d e v i c e , for D i a b e t e s . IEEE/Eigth annual C o n f e r e n c e riC t h e Eng ine e r - i n y i r M e d i c i n e and H i o l o y y Society. 1986, 912-.915.
R. I _ " Ar r : i e t a . The o p t i m a l control of pancr 'eas : A s i m u l a t i o n s t u d y iEEE/Ninth Annual C o n f e r e n c e of t h e Engineer-¡rig in m e d i c i n e and b i o l o g y Soc1et.y. 1987, pp 3-4
M. Y. J a t f r i n , VTC. Clucose and insulin k i n e t i c s in a b i o a r t i f i c i a l p a n c r e a s . IEE:E/l988 Word C o n g r e s s o n M e d i c a l F ' h y s i c s and B i o m e d i c a l Eng ine e r i r i g . 1988 : 244
M. R. P i l l a r e l l a and A. L. Zydney. S o l u t e t r a n s p o r t i n a h y b r i d b i o a r t i f i c i a l p a n c r e a s IEEE,.~Woi-tl Annual Ccmgrezs i n M e d i c a l P h y s i c s and B i o m e d i c a l E n y i n e e r i n y . 1986 : 237
C l a r k t::. Colton. The e f f e c t of t r ans f r i t 1 i m i C a t i o n s or1 ins.Li1il.i sec r - e t iu r i i n h y b r i d a r t i i i c i a i pmcreas, IEEE/wur-d annual Congress un M e d i c a l f51iysic%. and E<iomed ica l Eny ineer i r - i g . 19813 : 243
S. R a p t i s and G. D i m i t r i a d i z . C w t i f i c i a l b e t a - . - c e l l : pas.f., present. and f u t u r e IEE.E/ E i g h t h Annual Con í e r . enc e of E n g i n e e r i n g i n M e d i c i n e and I c i o l o y y S o c i e t y . 1964 :Y16-916
lO:-J. M i r ouse . A r t i f i c i a l e n d o c r i n e p a n c r e a s (REP) . IEEE iN in th Gnriuai Ccx i f e r enc e of t h e Eng ine e r - i nq i n M e d i c i n e and B i o l o g y S o c i e t y . 1987 : 1384-1:385.
11. .-Motoai:i 5 h i c h i r i , H y u ~ o , Kawuamor- i . Closed-1 o op g l i cemi c ca8ritr-51 with d w e a r a b l e . a r t i i i c i a l e n d o c r i n e panc r ea s . D i a b e t e s . 1984 V o l 31: December .
12. -G. bellorcits, S. Cantuch i A s i m p l e comput.ei. p rog ram í o r i1~5ui1.11 d o s e a d j u s t m e n t i n d i a b e t . i c p a t i e n t . Computer n e t h o d s and p r o g r ams i n b i u m e d i c i n e . 1YE8(2?i) : ;157.,-258
'IC)

”.
1- Y * -.Uav ~d E. f?. Scither- 1 and. Par-icr- cas; tr ar-i-ipi dint J. for- d i abete$,.
‘ rhe Lar i ce t . 1.988 M a y 14.: tli>ci
14. --E. Gar-cia--Rubl Uso de 1ai i n f o c i ó r i c o n t i n u a subcutar iea d e i n s u l i n a cin p a c i e n t e s dia.b&icc>.i con desc io r i t ro l metabmi ico mederado s e c u n d a r i o a i nlf ecc i ones i n t e r c u r r e n t c s . S o c i e d a d I’lexicaria de N u t r i c i o r i y e n u i o c r i n o i o g i a . 1988
15. -A. M. A l b i s s e r - A. C c t i i f f r i r i , I n s u l i n d o s a g e ad justment . u.!<iriy manual methods and computer a l go r - i tms : a compara t . i v e s t u d y M e d i c a l e.: H i 01 o y i c a l Eng i r ieer i r ig K Cíjmputi rrg. J986November : 577-334.
16. -D. Abendr-0th. Fancrcas t r a n s p i aC i un curdtive theraps,ut i c approoch t o d i a b e t i c m i c r oang i opa thy? . T ransp la r i t . a t i on Preceedicgs 1988, v o l X X No. 3 (June) :4.6?--47Ci.
41

. .
".
,.
F i si opat o1 og í a c 1 i n i r. - l r l i l l i am A. Cudeman. J r . , W i l i i a m O Sudemari . ED I n t e r a m e r i cariet. Hex i co, í) ~ F. Dui r i ta e d i c i ó n 197'3 pp 78:3-79:3
l ' e x t o de P a t o l o g í a . i)r Ruy P e r e z 'ramayo. Prer i sa Med i ca Mex i cana México D.F. pp. 688.-hci8
P a t o l o g í a B á s i c a . Rob ins , S t a n l e y i. Ed I r i t e ramer i ca r i a M é x i c c i ü.F. Segunda e d i c i b n . 1974
E l mundo b i o l ó g i c o . A l v i n hiason. Ed Limusa. P r i m e r a E d i c i b n ~ 1980 pp 4S1-441
Di a g n o s t i [IO r a d i o l 6 g i co. D r . G e o r g e T ep l i ck I Dr = Mar-vr n E:. i i a sk in . Ed In t e r ame r i c ana , . Me:.:j.c:» D.F. t e rc . e ra ed i c i o r ; . 1,779
Macrapatuiog ía ; Manual y a t i a s par-a m é d i c o s y e s t u d i a n t e s N. C a n d r i t t e r , C. 'Thomas. Ed. Reve r t e B a r c e l o n a , España l9Bl
Manual de q u i m i c a f i s i o l ó g i c a . Harold A. Harper E.d. Pla!iiral Moderno MBx i co D.F. Sép t ima e d i c i ó n 1900 pp L77;--277
Métodoc. c l i r i i cos . Wa lke r .Ha l1 ,Hur s t Ed. iriteu americac-ia Segunda e d i c i ó n ,
Erici cl uped i a Ved i á t r i ca . Op I z 8,. 5chmi d "Metabol i smo, n u t r i c i ó n y d i g e s t i b n Ed, Nor-ata C . 0 . . P r i m e r a e d i c i ó n 1967. pp 132:5--iZS2
E n c i c l o p e d i a Méd i ca d e l Hogar . LW. Agustiri Pedr-u F:'or-. ,s. Ed. Vargas V e r g a r a S.A. S e x t a e d i c i ó n . i Y 8 2 . pp X6-214.
E l L i b r o d e l a Sali-id Ci. Fernbride;: C r u z . Ed. üanae, B a r c e l o n a España. t e r c e t r a e d i c i 6 n . 1976 pp 10~--20
D i c c i o n a r i o E n c i c l o p e d i cui I1 u s t r a d o d e Med i c i na . Dot-1 and. Ed. Interamer i c a n a . v i g c s i masex ta e d i c i 6 n pp 75--BO
42

mrything e o 3er-
hew and BIT' .ure h t i the m.
:L 193%
Irrfiri«l oryam ~ifZ):i29-l37. Raven Press. New Vork 0 1985 International Smiely for Artificial m n r
VA of Artificial Pancreas and Portable Insulin hfusion Pumps in Diabetes Therapy: Past, Present, and Future
E. E Pfeiffer and W. Kerner
Deparimeni of Iniernal .Medicine I. Universiry of Ulm, Urn, F.R.C.
Abstract: The development of the artificial pancreas (AP) was an important contribution to modern diabetology. The practical and theoretical findings obtained by its ap- plication in type I diabetic patients gave rise to new forms of treatment, ¡.e., portable insulin pumps and intensified conventional insulin therapy. Although these therapies
lead to better results than conventional insulin adminis- tration there ;> no d,*v'-* that the problems of diabetes the ipy can be solved only by an implantable AP or pan. creas transplantation, Key Words: Insulin therapy-Ar- tificial pancreas-Glucose sensor -Insulin pumps-In- tensified insulin therapy.
- .. __
The artificial pancreas (AP) and the portable in- d i n pump are recent developments in diabetology. Despite this short history, it appears appropriate to review the current and future therapeutic possibil- ities offered by this new technique. Conventional insulin therapy used during the last few decades did not aim at ohysiologira! rey!acic-nient cf izsulin; it mainly prevented hypo- and hyperglycemic com- pensation of the metabolism,. On the contrary, modem insulin therapy is based on the reestablish- ment of normoglycemia. There is an essential dif- ferenccbetweeo these two forms of treatment. The firit represents a primitive replacement therapy,' while the second will hopefully lead to true reha- bilitation. This article is divided into three parts: the past, when the AF' was developed; the present, Characterized by the application of portable insulin pumps and intensified conventional insulin therapy; and the future, which will lead to the implant- able AP.
'THE PAST
:!e development of the AP was preceded by two significant technical innovations. The first was the
- Received April IW: accepted April 1984. Address correspoadencc and reprint mquesls lo Dr. E. F.
Heiffer at Department of Internal Medicine 1. University of Ulm, Skinhovelstr. 9, D7WO Ulm. F.R.G.
Resented. in pan. at the Fourth Congressofthe International S N k y for Artificial w n s , Novembcr 14-17. 1983, Kyoto. Japan (Atsumi K. Maekaw M, Ola K. eds. Progress in artiricial ortans-i983. Cleveland ISAO press, 1984).
k '
introduction of the double-lumen catheter, which permitted the continuous withdrawal of blood without systemic heparinization. The second tech- nical innovation was the Technicon Auto-Analyzer, which was modified by the femcyanide method or enzymatic methods !o provide continuous measure- iiiiilt of bluuri yiucost: <¡-6) .
This apparatiis enabled diabetologists for the first time to recognize completely the failure of currently used 'conventional insulin therapy. This therapy consisted of the subcutaneous injection of an inter- mediate-ac '.'. : insulin once daily. Fluctuations in blood glucose concentrations were extremely high. This could not be prevented by two injections of insulin or by the addition of regular insulin (Fig. I ) (7.8). Molnar (9), a pioneer in the field of contin- uous blood glucose monitoring, stressed that inter- mittent determinations of glucose levels never pro- vide a complete determination of glucose metabo- lism. Finally, in the early 1970s, computers were miniaturized so that their application in laboratories became possible.
At the same time, biochemists started to inves- tigate the etiopathology of diabetic microangiop- athy (eye, kidney, and nerves), particularly with respect to the existing hyperglycemia. They discov- ered that glucose nonenzymatically reacts with many proteins such as hemoglobin (10). In addition, glucose may modify proteins by enzyme-catalyzed reactions ( I I) . Both mechanisms were considered the basis for glucose-induced changes in basal mem- branes leading to secondary diabetic complications.
129

.
In 1972, the existing technology was used at the University of Ulm to reestablish the parallelism be- tween insulin and basal glucose concentrations in diabetic patients. The authors' work was similar to the previous studies of Kadish (121, who tried in 1963 to link blood glucose measurement with insulin infusion. The authors combined the Technicon Auto-Analyzer for continuous gLcose irirasure- nient in blood withdrawn with a double-lumen cath- eter, an electronically controlled insulin pump, and a microcomputer. With this system, continuously measured glucose concentrations regulated insulin infusion ri\teo.>mearus of empirically selected al- gorithms.'All data were documented with printbuts (13). At the same time, similar studies were per- formed by Albisser et al. (14) at Toronto.
The combination of all these subsystems led to a rather bulky machine. This first version of the AP used in the authors' initial work was improved in the following years by collaborating with A. H Cle- mens from Life Science Industries, Miles Labora- tories, Inc. (Elkhart, IN, U.S.A.). He developed an electroenzymatic glucose sensor and incorporated all systems into one machinc (glucose-controlled in- sulin infusion system) (Fig. 2). The authors at- tempted to control insulin infusion exclusively via the actual glucose level. Blood giucose curves ob- tained in pancreatectomized dogs after a glucose challenge resembled the results observed in type I1 diabetic patients, who secrete b a d amounts of in- sulin but cannot respond adequately to a glucose
m i l e OiaMea
mm:aA. "w Conlims B(ood-Gl- A-is
27 Y 500
FIG: I . Contirtious blood glu. cose (üG) moi,,.uring in a pa- tient on conventional insulin therapy. B, breakfast, L. lunch; 0, dinner: Sn. snack: E. exer. cis.9.
L.
0 1
E
i i e
h n I D - h 1
- I e I 1 I3 16 17 IS ?I ..'21 1 1 5 7 N h
m : 100 5 L J k ~ 400
300
200
- rn o
d n_ ' 4 i - L 1
stimulus. Glucose tolerance was significantly im- proved when a dynamic component was included in the algorithms for insulin infusion control. This led to increased insulin supply with an increase in glucose concentration resembling the first phase of insulin secretion observed in experiments with per- fused isolated rat pancr~as.
It is now possible to normalize blood glucose con- centratir.is in all type I diabetic patients by contin- uous feedback-controlled administration of insulin (Fig. 3) (616). Basal glucose levels are -80 mgfdl, and increases in blood glucose are immediately fol- lowed oy increased insulin infusion rates. Small quantities of insulin must be administered conti ously because maintenance of basal insulin deliv primarily suppresses hepatic glucose production to normal fasting values.
It is now possible to use the AP to treat different states of hyper- and hypoglycemias (Table I). Pen- operative application in diabetic patients and those suffering from organic hyperinsulinism must be lim- ited. On the other hand. the AP provea to be valuable tool in experimental diabetology (%bl In this regard, experiments on the influence of 'moglycernia induced by feedback-controlled i administration on the concentration of m and counterregulatory hormones appear nificant. The authors were able to demonstrate at least some of those parameters were norm under euglycemic conditions, indicating that phenomena are secondary to the lack of
ArWOwns. Vol. 9. No. 2. 1985 .. .
I 2
tu Ir la;
FIG. 3. System

, .
? , .
. ,..
. ,
. .
' b o ~ l u - rgn pa- 3k in.An ,:L. lunch: ,rE.,wer-
I ,,.
. ,,
. .. P -
. .. r.
:an[-. im- i,included itr&This ncri se in ;bpMse of n.wi,t& per-
LICOL con- by contin- ,.of risulin -8Lnng'dL diately fol- tes,Small :d E itinu- fih deiivery Jducfion ta
at rderenl >k I). Peri. srai--L thc;sf nus_ie l im ,ed to be 5
:ncc )f nor Jilemnsulif metabolite! ir tT>e sig mst-te tha normalize1
g: t M thesi IF. ir ilin.
;Y (Table 2)
~ . .
..~, ,
PERSPECTIVES ON ARTIFICIAL PANCREAS AND INSULIN PUMP 131
INSULIN INFUSION RATC (mu/min)
200i 150
100
50
8- 10- 12- 14- ls- 18- 20- 22- 24- 2- 4- 6- 8- TIME (hwrs)
flQ. 2. Blood glucose (BG) concentrations end insulin infusion rates in type 1 diabetic patients during treatment wlth the artificial pancreas (means 2 CEM, n = i j .
THE PRESENT Tkmain drawback of th- AP is not the minia-
turization of the apparatus to enable implantation. In reality, a permanent, reliable glucose sensor is lacking. The authors' method of continuous blood
system, g~ucose controller, glucose monitor).
glucose determination is based on the formation of hydrogen peroxide by the oxidation of glucose by the immobilized enzyme glucose oxidate. To obta:- this result, either the minimal ele'ctric current gen- erated by the peroxide or the decrease in the ox- ygen measured by a metal electrode (Fig. 4) is eval- uated. Unfortunately, glucose measurement after various periods of time will be disturbed and even- tually inhibited by the deposition of platelets, leu- kocytes, fibrin, etc., as part of the defense reaction of the organism against foreign material. After an interval of 20-800 h, the systems become progres- sively weaker.
TABLE 1. Applications of the artificial pancreas in clinical theram
Diabetic coma Surgery in diabetic patients Total pancreatectomy Delivery (diabetic mothers) Organic hypcnnsulinism Hemodialysis in diabetic patients Induction of the rcmission phase (honeymoon period) Evaluation of insulin doses for subcutaneous therapy
AnBOrgonr. Vol. 9, No. 2, 1985

I I 1 ---I___*
132 E. F. PFEIFFER A N D W. KERNER
TABLE 2. Applicarions of the artificid pancreas This results in unwarranted hopes for the diabetic, in clinical research oatient. a
Blood glucose control applying different insulin u i 4 0 n kinetics Portal venus peripheral insulin infusion
Glucose clamp studies insulin feedback inhibition Insulin sensitivity Absorption kinetics of subcutaneously injected insulin
Hormones, nietabolites, lipids, and blood viscosiiy during Diurnal rhythm of insulin requirement
Effect of drugs on insulin requirement short-term blood glucose normalization
Somatostatin and analogues of somatostatin Sulfonylurras Sugar substitutes Fiber diet
q<
It is well known that this type of programmed? insulin infusion is not as competent at opt insulin delivery to the extent achieved by th back-regulated AP. During the day, significan tuation in the blood glucose concentration be prevented. Hyperglycemic reactions a rectly observed and documentec! if continu blood glucose monitoring is performed and if daily blood glucose profiles obtained by the AP
those obtained under programme reatment. Moreover. it is also n
Disaccharidase inhibitors possible- to &ablish insulin requirements and pr files via the AP and transfer this profile by mean
the profüe of daily insulin delivery, as elaborated by the AP, to establiqh a $0-called "prepro- grammed" insulin infusion via portable pumps. In other words, the use of these simple portable pumps continuously delivering a daily dose of 1-2 U of inculin per hour, ¡.e., 24-4a U/day, was acceptable. This methodology required support of this basal in- sulin infusion by additional insulin supply, the so- called "bolus," during food intake for improved nu- tritional utilization. C?irren!ly, -24 mcdels of there pumps are available commercially (Fig. 5) . Insulin delivery may be dministered by intravenous, sub- cutaneous, or intraperitoneal routes. Evidently, these pumps represent only one-third of the me-
, . o h ¡ d . p s a s - ~ e ? d e d for a completely automatic . AP based on glucose-controlled feedback. Unfor-
tunately, this difference at the present is overlooked in the medical literature as well as in the lay press.
of magnetotape the following day for the same pa
y". ilthough medical science was unwilling to wait ,!ivery by continuous mewurement of blood gluc for the final solution. Instead, varioiis groups used ,./ concentrations. Usually, without continuous a
matic action via the algorithms, uncontrolled poglycemic reactions are obtained during the nor turna1 period, despite continuous ongoing i n s u l i a
This fundamenl.; Zrob , _.has not been solved as tknt without automatic correction of the ...-din .,. Q -
treatment (18). Despite these defects in pump therapy, a nu
of indications have proved valuable. In diab neuropathy, pump treatment has led to considerab improvement by shortening the length of the di ease (19). In children of diabetic mothers wh conditions 'vere carcfiilly con!ro!led with i ! I rently available methods before, during, and pregnancy and who were treated by coTi.tnuous sulin infusions, significant decreases in malfo tions were found (20). On the other hand, no provement in male impotence was obsprrpd du successful treatment of diabetic neuropathy by tinuous insulin infusion.
,
A
ArtfOrg<ii,r. Vol. 9, No. 2. 19&J
O(LUTE0
1"
FiG. 4. A Cross section o zyme membrane. 8: Cross lion of complete glu sensor. C: Bottom view of cell. (From Fogt et al.. ref. GOD. glucose oxidase.

fit .ic
mnr$ed ;iini ng te f-d- rnt fluc- ra''-,ot me .-)r- tinuous d<:if.the :u41 ire wmlned ilso not ind ''-.O-
Ijm,-ns ame pa- irilirle- giu*,se
us auto- blled-hy- the x- ::insulin
nui'-~er dial-tic iiderable t h e i i s -
s w >se aii'Zur-
ind after tuoi in- a l f m a - ,,: no im- d:d""ing "by. o n -
. .
sa siuiif.
I -
I_ .
. , !ion +n en- ^toss sec-
3w c flow I:. rib -17)
2 giwose
w
. -
.. " .
PERSPECTIVES ON ARTIFICIAL PANCREAS AND i N s u L i n PUMP J33
FIG. 5. Typlcal portable insulin pumps (thosyringe ASGC. CPI-Betratron I, Siemens Promedos El).
icant therapeutic effect of infusion therapy on the preproliferative or proliferative retinopathy and ne- phropathy under controlled conditions has bec. -n es- !&!ished to d2to. 13 thio rqxx!, the rcsu!! CF var- ious studies performed and reported in recent years by several CdniSh and British groups was negative (21,22).
It is noteworthy that perhaps this type o f therapy '.vas. stiu@d..+~~~late io be effective, ¡.e., that the "point of no return" had already passed. In 1978, Federlin et ai. (23) at the University o f Ulm dem- onstrated that following a total "cure" o f all symp- toms in diabetic rats by islet transplantation into the liver, improvement in kidney function was evident for only 6 months, as established by histological examination. Beyond this period, no favorable re- sults o f transplantation were observed. In humans, it may be that a "preproliferative" phase of diabetic ritinopathy has to be investigated.
In the interim, the limitations of this type of [.'rerapy compared with conventional treatment by insulin injections have not been overcome. The re- sult of intensified conventional insulin therapy by means o f multiple insulin injections during the day and frequent combinations of short- and long-term acting insulin preparations is more or less de,pen- dent on the cooperation of the individual patient. This is also the case with insulin pump therapy as well. The patient must be put in charge o f deter- mining blood glucose levels by means of the avail-
able apparatus, using reflectometric techniques. With home blood glucose monitoring, the patient is trained to change insulin dosages, ¡.e., mixing short- and long ~teiih sctiiig insulin, accürdizg io ihr immediate requirements (Fig. 6).
It is the patiec:"s task to supplzment blood @u- cose administration as needed by mathematical cai- culation via computer by his or her own activity and intelligence. As it is said in :--fessional lan- guage, it is up to the patient "to close the open loop." In practical terms, it means that the intel- lectual capacity of the individual patient must be evaluated. ih contrast to what one mi the most dific@t patients of this grou those wb.+vf&iept the highest risks, are teachers, nurses, medic#students, and doctors o f both
ese precautions,, the number o f sexes.
is unknown. Of -200 diabetic patients observed by 20 European centers ~
collaborating in a study by the European Diabetes Association on artificial insulin delivery systems 1 and pancreas and islet transplantation, - 10% of the 1 pump-treated patients suffered from hypoglycemic reactions inducing unconsciousness. Frequently, the same patients suffered from several hypogly- cemic attacks. To obtain an unbiased estimate o f the slight symp-
toms of hypoglycemic reaction, self-determination
Despite al reactions caused by this type I
ArI(lOrn<inr, Vol. 9, No. 2. 1985
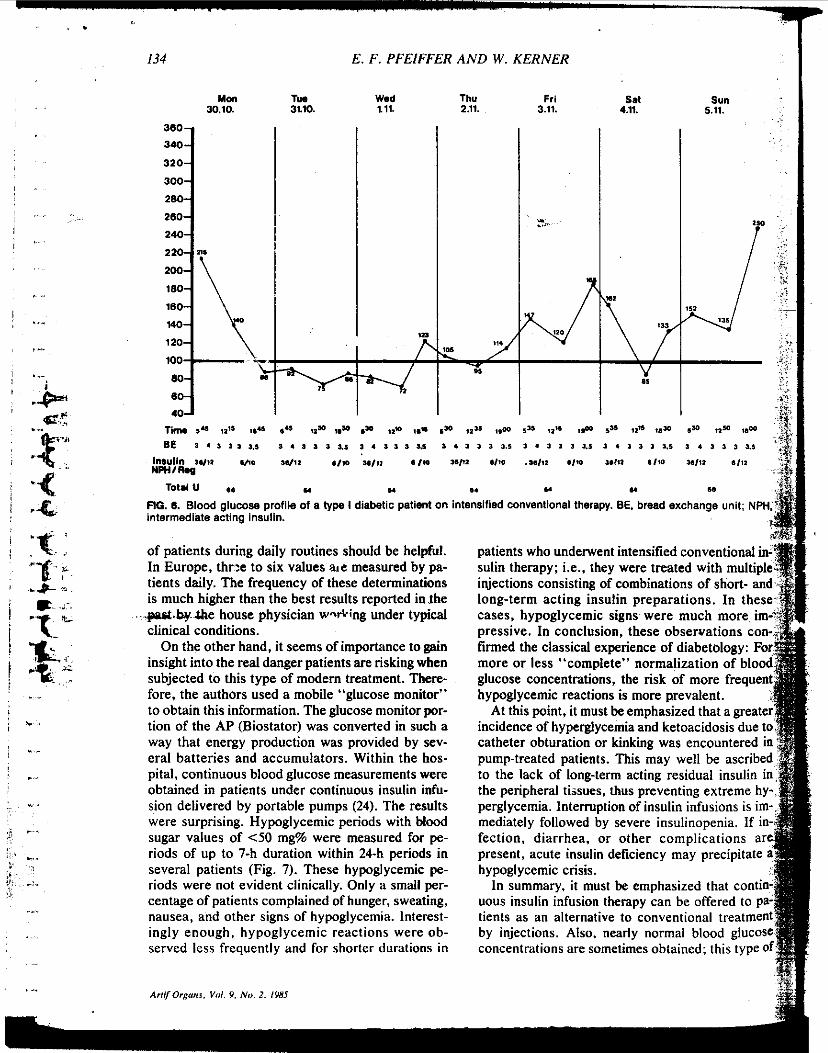
134
Mai 30.10.
E. F. PFEIFFER AND W. KERNER
TW Wid 3110. 1.11.
Thu 2.11.
360
340
320
300
28
180
140
120
100
u
Frl 3.11.
v ... "
Sun 5.11.
. .
intermediate azting insulin.
of patients during daily routines should be helpful. In Europe, thr:e to six values ate measured by pa- tients daily. The frequency of these determinations is much higher than the best results reported in.ihe
&e house physician w d i n g under typical clinical conditions.
On the other hand, it seems of importance to gain insight into the real danger patients are risking when subjected to this type of modem treatment. There- fore, the authors used a mobile "glucose monitor" to obtain this information. The glucose monitor por- tion of the AP (Biostator) was converted in such a way that energy production was provided by sev- eral batteries and accumulators. Within the hos- pital, continuous blood glucose measurements were obtained in patients under continuous insulin infu- sion delivered by portable pumps (24). The results were surprising. Hypoglycemic periods with blood sugar values of <50 mg% were measured for pe- riods of up to 7-h duration within 24-h periods in several patients (Fig. 7). These hypoglycemic pe- riods were not evident clinically. Only a small per- centage o f patients complained of hunger, sweating, nausea, and other signs o f hypoglycemia. Interest- ingly enough, hypoglycemic reactions were ob- served less frequently and for \horter durations in
patients who underwent intensified conventional i sulin therapy; ¡.e., they were treated with multipl injections consisting of combinations of short- an long-term acting insulin preparations. In thes cases, hypoglycemic signs were much more pressive. In conclusion, these observations c firmed the classical experience of diabetology: more or less "complete" normalization of blo glucose concentrations, the risk of more frequen hypoglycemic reactions is more prevalent.
At this point, it must be emphasized that a greate incidence of hyperglycemia and ketoacidosis due t catheter obturation or kinking was encountered i pump-treated patients. This may well be ascribe to the lack of long-term acting residual i the peripheral tissues. thus preventing ext perglycemia. Interruption of insulin infusions IS
mediately followed by severe insulinopenia. I f fection, diarrhea, or other complications present, acute insulin deficiency may precipitate hypoglycemic crisis.
In summary, it must be emphasized that con uous insulin infusion therapy can be offered to tients as an alternative to conventional treat by injections. Also, nearly normal blood gluc concentrations are sometimes obtained; this typ

.
400 - - - P - E
300‘
200
su 5.11.
.. -- ; L
,- .- w w ,sw ,. 1 I 3 L1
r- r*r S l U
L .. ” iiingTwnit; NPH.
.- mventional in- iiww” multiple sof,Jiort- and bns. In these mcb-nore im- =vi ions con- ,%efology: For ,ati<)p of blood imo frequent 4&. :d that a greater mci’ Ilsis due to .enq-intered in !ell be ascribed id& insulin in Og ;treme hy- infiEions is im- iihogenia. If in- rpli itionc are ay ,ecipitate a
zebr ia t contin- )e q , - x e d to pa- tional treatment
iiec this type of ii: bhod glucose
~ ..
PERSPECTIVES ON ARTIFICIAL PANCREAS AND INSULIN PUMP 135
I S i t E FIG. 7. Continuously measbred
blood glucose (BG) Concenlra- tions during pump treatment. 13. brBakf8Jt: L. lunch; C. supper; E, exerciso
I pm 6 9 12 am3 6 9 12 p m 3 6
t : xapy may compete with intensified conventional tieatment of multiple insulin injections of combi- nations of short- and long-term acting insulin prep- arations. The new type of dynamic insulin therapy presents higher risks than conventional treatment based on injections. Hypoglycemia represents only one of these risks. Thcse ccap!ica<?ions will not be overcome until a permanent, implantable “glucose sensor” has been developed. On the other hand, the authors have obtained positive results and fur- ther improvement in diabetic neuropathy and in the p! tventipn of -*’formation, miscarriage, and early death of children of diabetic mothers.
THE FUTURE Obviously, the near future will be under the aus-
pices of continuous improvement of the presently available technology. Experience gained with the automatic AP will be translated to preprogramming of portable insulin pumps. A number of modifica- ti, 11s are indicated. Considerable improvement in d ly blood sugar profiles results from a one-third increase in the early morning injection of insulin before breakfast, or by administering by infusion all of the additional insulin delivered at lunch and dinner under isocaloric conditions (25). Also, pa- tients will be trained to administer the additional insulin infusion 30 min before meals to improve food utilization, particularly glucose, ¡.e., to pre- vent postprandial hyperglycemia (26).
Eventually, basal insulin infusion during the Course of 24 h should be changed quantitatively.
The highest importance must be ascribed to the early morning hours. Under glucose-controlled in- sulin infusion by means of the AP, an increase in the insulin requirement from 8 to 15 mU/min is ob- served between 3 and 4 a.m. in the majority of the patients examined. Comparative determinations of the contraregulatory hormones (growth hormone, glucagon, and cortisol) during this period showed increases predominantly in cortisol level: h e to the circadian rhythms of hormonal secretion, thus re- sulting in increased gluconeogenesis in the liver. These results, of course, demonstrate a close rela- tionship to the “dawn phenomenon .-I).
B y means of manipulation and adjustment to achieve a more physiological mode of insulin ap- plication, the daily blood glucose profile may be improved toward the normal range. However, fun- damental changes in the generally unsatisfactory situation will not be obtained. With the automatic feedback regulation AP. the authors did not achieve more than near normalization of the metabolism in general. Certain parameters, such as pyruvic acid, @-hydroxybutyric acid, and human growth hor- mone, were normalized by means of the AP only if comparatively long periods of precise blood glucose control had elapsed. The fine and ultrafine regula- tion of the metabolically healthy organism ob- viously is based on much more complex mecha- nisms than anticipated.
The only alternative is to return to the original concept of the implantable AP and to develop a per- manent implantable glucose sensor. It should also control the implantable insulin pump via a com-
Arri/Orgnnr. Vol. 9, No. 2. 1985
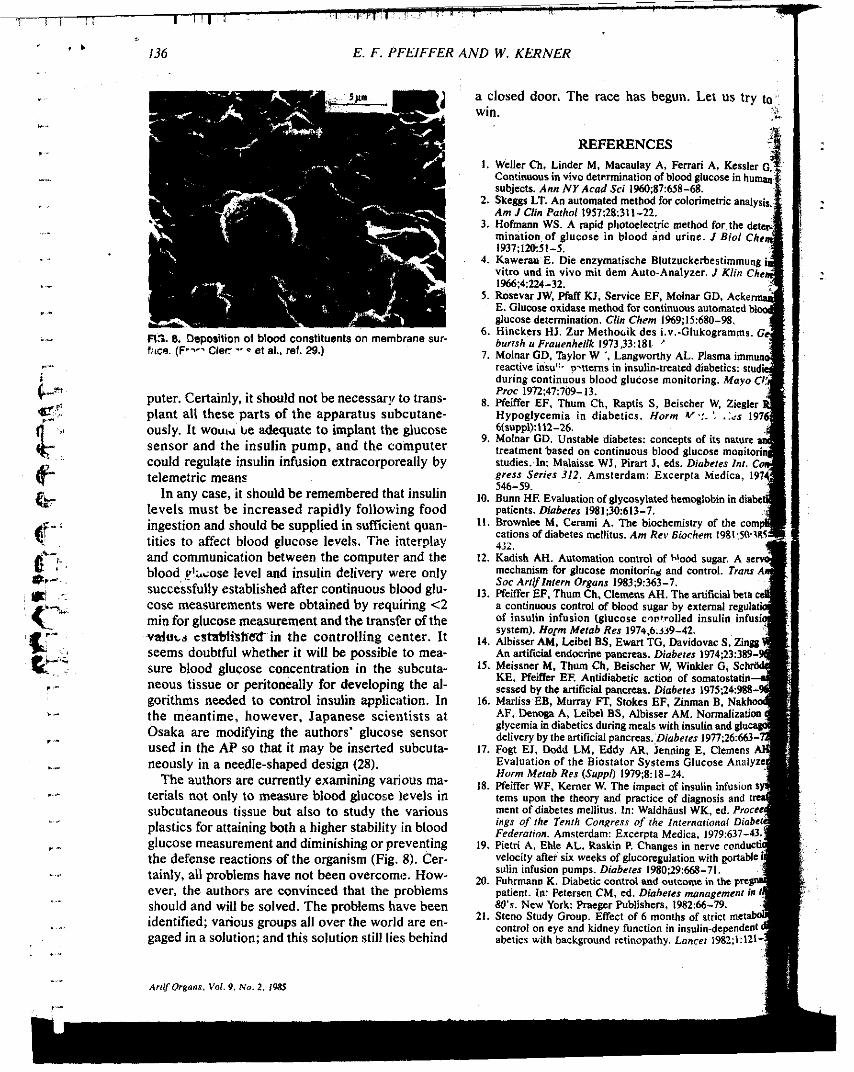
136 E. F. PFEIFFER AND W. KERNER
F13. 8. Deposition of blood constituents on membrane sur- fitce. (F.- Cler -. - et al., ref. 29.)
puter. Certainly, it should not be necessary to trans- plant all these parts of the apparatus sribcutane- ously. It WOUL\L be adequate to implant the glucose sensor and the insulin pump, and the computer could regulate insulin infusion extracorpcireally by telemetric means
In any case, it should be remembered that insulin levels must be increased rapidly following food ingestion and should be supplied in sufficient quan- tities to affect blood glucose levels. The interplay and communication between the computer and the blood &ose level and insulin delivery were only successfully established after continuous blood glu- cose measurements were obtained by requiring <Z min for glucose measurement and the transfer of the d u t s CstaMished- in the controlling center. It seems doubtful whether it will be possible to mea- sure blood glucose concentration in the subcuta- neous tissue or peritoneally for developing the al- gorithms needed to control insulin application. In the meantime, however, Japanese scientists at Osaka are modifying the authors' glucose sensor used in the AP so that it may be inserted subcuta- neously in a needle-shaped design (28).
The authors are currently examining vanous ma- terials not only to measure blood glucose levels in subcutaneous tissue but also to study the various plastics for attaining both a higher stability in blood glucose measurement and diminishing or preventing the defense reactions of the organism (Fig. 8). Cer- tainly, all problems have not been overcome. How- ever, the authors are convinced that the problems should and will be solved. The problems have been identified; vanous groups all over the world are en- gaged in a solution; and this solution still lies behind
ArtilOrgans. Val. 9 , Ne. 2, 1%
a closed door. The race has begun. Let us try t '.
win.
REFERENCES 1.
2.
3.
4. nzymatische Blutzuckerbestimm mit dem Auto-Analyzer. J K/in
tinuous automate 5.
6. i.v.-Glukogramms.
7.
8. h, Raplis S, Beischer W iabetics. Horm v'!. ', .._
9.
io.
II .
ation of glycosylated hemoglobin in d es 1981;30:613-7. erami A . The biochemistry of the es mellitus. Am Rev Eiochern 1981.
12.
13.
14.
IS.
16.
17.
18.
19.
20.
21.
abetics with-background retinopathy. Lancet 1982;1:121-

SUMMARY Long-term insulin secretion was inv biohybrid capillary devices seeded with canine islets. Approximately 50,000 islets could be isolated from a single canine pancreas using collagenase digestion in conjunction with the recently described Velcro tech- nique. Devices were pertused with tissue culture me- dium 199 containing 300 rngidl glucose. Insulin se- cretion fell during the first 1-2 days of culture from approximately 16 to 6 Uiday. After 3-4 wk of perfusion, however, there was a gradual rise in insulin output that reached >15 Wday after 7 wk. Insulin output eventu- ally stabilized at 18-20 Uiday. Two of these devices were studied for 80 and 86 days, respectively, and con- tinued to secrete these same amounts of insulin. Glu- cose-Induced insulin release was studied after 1 and 4 wk of culture and was well preserved. DIABETES 1985; 34:850-54. . ,. , . . ..
- . . . . he biohybrid artificial pancreas offers a potential solution to several .of the major problems involved in iransplantation of insulin-producing tissue in di- T~ abetic'patients. In this device beta cells are sepa-
rated from the blood stream by a thin. semipermeable mem- brane that permits passage of small molecules such as glucose and insulin, while excluding lymphocytes and anti- bodies involved in immune rejection.'z It is therefore possible to use islets from animals that are more readily available than human islets. Moreover, since type I diabetes may be an autoimmune disease. the semipermeable membrane also protects islets from potential autoimmune attack affer trans- plantation in a diabetic host. Recent results of segmental
From lhe Depanmenls of Birchemistry and Medicine R . A , W.L.C ) and Sur- gery (R.M B ), Univarsay of Massachusens Medical Center. Wo~cesler, Mas- SachuCBnS: and lhe Amicon Corwtalim. Lexinalon. Massachusells 1B.A.S.I. Addres reprint requests to ~il iarn L. Chick, MO.. Oepanment o1 Ebche&- istry, Univesniiy of Massachusetts Medical Center. 55 Lake Avenue Nonh. Worcester. Massachwens 01SaS. Received lor Dublicalim 12 December 1984 and in revised form 14 March
pancreatic transplants from nondiabetic to diabetic identical twins suggest that this can occur.'
Devices consist either of bundles of capillary fiber^^^^' or of one or more semipermeable tubes5 sealed into a protective jacket. In the past. devices have generally been seeded with relatively Small numbers of islets from rodents. When per- fused with tissue culture media, these devices show stable insulin output for 1-2 mo, and continued responsiveness to glucose.' For in vivo use, the biohybrid artificial pancreas is implanted as an arteriovenous~shunt in the vascular system. Short-term studies in diabetic rats, and in Small numbers of diabetic dogs and monkeys, demonstrate effective control of blood glucose concentrations and increased circulating insulin levels.)~
Studies in larger animals have been significantly hampered by lack of availability of efficient means for mass isolation 01 islets. Recently. however, Lacy and associates reported an improved method for isolation of islets from beef pancreas using Velcro.'This advance offered the opportunityto extend previous in vitro studies of \he biohybhd pancreas.
The present experiments were undertaken to investgate insulin secretion from capillary devices seeded with large numbers,of canine islets (approximately 50.000 each). The objectives were to determine whether: (1) sufficient numbers of islets,couid be isolated from a single canine pancreas io provide high insulin.aitput from a device (10 Ukr more per day), (2) insulin secretion would continue over extended pe- riods (2 rno or more), and (3) islets remained responsive to glucose.
. .-
MATERIALS AND METHODS Islet Isolation. The procedures used for islet isolation were similar to those reported by Lacy and co-workers for beef pancreas.*Seven male and female dogs weighing 25-40 kg were used as pancreatic tissue donors. Procedures were 'conducted aseptically using Sterile Solutions. Animals were anesthetized by rapid intravenous (¡.v.) injection of Nembutal. The abdomen was opened and the two main pancreatic ducts cannulated with 18-20-gauge catheters. Major blood vessels
. .
OIAEETES VOL 34. SEPTEMBER 1985

i.
y. k *._ $ .̂ . !
; C.. i
supplying the pancreas were ligated."The pancreas was In some cases, the glucose concentraton in the me- quickly removed and transferred to ice-cold Hanks' solution dium was decreased to 100 mgldl to investigate the insulin containing 10% fetal calf serum, 100 Ulml sodium penicillin, secretory response. One hundred millilitefs of medium was and 40 W l m l gentamicin, and then transported to the lab- recirculated through the devices at a rate of 2 3 mllmin. The oratory, The pancreas was distended by injecting 200 mi¡ of perfusion system was maintained at 37°C in a humidified Hanks' solution with the same 'additions.:Extraneous tissue , atmosphere of 5% C0,:95% .air. The 100 ml of perfusion and blood vessels were dissected away and the gland iiut into pieces that were gently pressed down on the spiny sur- face of Velcro (no. 65 hook) with a pair of scissors. This Velcro was previously prepared by sewing together Pio'strips'tlhat were then CUI into 9-cm lengths. The Velcro was boiled in 0.5% NaHCO, for 30 min, washed in double-distilled water for an additional 30 min, and siliconized (Sigmacote, Sigina Chemical Co., St.'Louis, Missouri) before sterilization by ~au- toclaving. Each strip of Velcro with attached pancreas was transferred to a 50-ml, siliconized, round-bottom digestion tube. In most cases, four strips of Velcro were sufficient for a single pancreas. The tissue was dissociated by adding 15 ml of Hanks' solution to each tube. This contained 3 m g h l of collagenase (CLS IV. Cooper Biomedical. Freehold, New Jersey) and 10% fetal bovine serum. The tubes were me- chanically shaken in a water bath at 37°C (üurrell Model 75 shaker). The two initial digestion periods were 2 min ea8rh, followed by consecutive 1-min periods. Total digestion time involved 4 0 min of shaking in the water bath. After each, 1- or 2min digestion period. the solution containing the sus- pended pancreatic fragments was collected in a separ,ate tube and centrifuged. The supernatant fluid containing 'the collagenase was transferred back to the digestion tube lhe cell pellet was suspended in ice-cold medium 199 containing 10% fetal bovine serum. After the pancreatic tissue had been completely dissociated the fragments were collected and redigested for 2-5 min if required.
Islets and exocrine tissue were separated by centrifugation on discontinuws Ficoll gradients containing layers o1 2C8%, 20.5%. and 11% F~COII.B.'~ Canine islet cells concentratea at the interface between the 20.5% and 11% layers after ci?n- trifugation at 800 x g for 10 min. The islets were removed and washed three times with medium 199 containing 10% fetal bovine serum, penicillin. and gentamicin. The islet yiNsld was roughly estimated by diluting a small aliquot of the ¡!;let suspension 1 : 100. and counting the number of islet cell clus- tersin 0.1 ml placed on a slide. The islet isolation procedure averaged 2.5-3 h from the time of pancreatectomy lo transfer to capillary devices. Petri dish cultures. The majority of the.islets were seeded into capillary devices as outlined below. In addition. 1[% 200 islets from each preparation were hand-picked using a braking pipette and transferred to 60-mm plastic Petri dishes not treated for cell attachment (Labtek. Miles Laboratories, NapeNille, Illinois). These were cultured under conditions similar to those used for capillary units. They provided a convenient means for assessing morphology by phase-csm- trast microscopy and for determining insulin output by islets in Petri dish cultures. Perfusion of pancreatic devices. The perfusion deviies were Amicon 3X 50 Vitafiber units (Amicon Corporation, Lex- ington, Massachusetts). The procedures for perfusing these devices have been previously described.' Briefly, devices were perfused with medium 199 containing 10% fetal bovine serum, 1 O0 Ulml sodium penicillin. and 300 mgldl 6-glucose.
~. . * . DIABETES. VOL 34. SEPTEMBER 1?85
medium was changed every 1-2 days, and aliquots frozen at -20°C for subsequent determina#ion of insulin content.' insulin secretion studies. In addition to determining the insulin content of the perfusion medium at 1-2-day intervals. the insulin secretory response to varying concentrations of glucose was investigated. On the sixth and 27th days, the glucose concentratibn in the culture medium was reduced from 300 mgldl to 100 mgldl for 24 h. Short-term insulin secretory response was then investigated by changing the culture medium and perfusing for 2 h at a glucose concen- tration of 100 mgldl. At the end of this 2-h control period, medium containing 300 mgldl glucose was substituted. and perfusion continued for two more hours. Samples were col- lected and stored a¡ -20°C for determination of insulin con- tent. Insulin assay. Insulin concentrations were determined by radioimmunoassay using the alcohol precipitation method." Crystalline porcine insulin was used as the standard, since the. primary amino acid sequences of porcine and canine insulin are reportedly identical." insulin content of isolated islets. Jn !he course of sening up the canine islet isolation techniques in our laboratory, the insulin content of some of the islet preparations was deter- mined. This was done to optimize the digestion and gradient separation procedures. The islet fractions harvested from the Ficoll gradients were weighed and then extracted overnight at 4% in acid-ethanol. The insulin content of whole canine pancreas was similarly determined after homogenization. Re- sults were expressed as units of extractable insulin per gram wet weight of tissue. Morphologic studies. The morphology of freshly isolated islets from each preparation was examined by phase-con- trast microscopy, Unfortunately, it was not feasible to ex- amine in detail the morphologic appearance of islet cells contained within the capillary devices. Therefore, as already outlined, small numbers of Petri dish cultures were prepared from each canine islet. preparation for study by phase-con- trast microscopy during the course of culture. Statistical analysis. Results were expressed as mean of each group f SEM. Comparisons of insulin secretory data were conducted using Student's paired t-test (Minitab com- puter program).
RESULTS Morphology and insulin content of isolated canine islets. Under phase-contrast microscopy. the canine islet prepa- rations consisted mainly of cell clusters with what appeared' to be 'mcasionai intact islets. Clusters ranged in size from approximately 50 to several hundred cells each. These typ- ical endocrine cells appeared slightly gray in appearance and made up the majority of the preparation. In contrast, exocrine cell clusters had a slightly orange appearance un- der phase-contrast using a green interference filter. Individ- ual exocrine cells appeared larger than the endocrine coun- terpart, and contained abundant coarse granules, possibly
851

GLUCOSE 130 im . 3m Lai Im bris floating in the medium, which gradually cleared over
Daily insulin secretion from perfused devices. Insulin con- tent of the perfusate (Figure 1) fell markedly during the first 1-2 days, possibly as the result of release from damaged betacells.Although17.7 2 1.4 U/dayof insulin was released during the initial 24 .h of culture, this subsequently fell to approximately 6 Ulday during the fist week, and remained at a level of 6 9 Ulday for.the subsequent 2 wk. After ap- proximately 3-4 wk of culture, there was a gradual rise in insulin output that reached the initial 24-h level after roughly 60 days of culture. Beyond this point, insulin output appeaied to remain stable in the range of 18-20 Ulday. One of the devices was studied for 86 davs. at which time insulin output
CONC several days. imoiaii
m- . - a z 0 t
z
5 15-
i
-
, o -
> 2 5 - r
! remained at I S 2 0 Ulday.
o 10 n 30 m . 5 0 (o 10 I D A total of seven devices were studied for 52 days or more. Two of the devices were electively terminated after 80 and DUR~TiTIONOFCULTUREld.nl
FIGURE 1. Insulin secretlon hom blohybiid pancreas d a v l m seeded wlih canine isieis. The glucose concentralion in VM medium was 300 mgidl with the arc.ption of Via sixth to seventh and 2nh lo 28th days of culture. Values are mean8 5 SEY. The number oi dwices is lndl. caied by the small numerals.
. ,
representing acinar cell granules. These typical exoc'ine cells were estimated to make up 4 0 % of the population of cells in the interface between the 20.5% and 11% Ficoll lay- ers. In contrast. they constituted the majority of cells pelle1:ing in the 25% Ficoll layer.
Since the majority of islets appeared fragmented,, it was difficult to obtain accurate counts. We estimated, however. that approximately 50,000 islet equivalents (endocrine clus- . ters containing several hundred cells) were isolated from each canine pancreas. The insulin content of the isletben- riched fraction harvested from the Ficoll gradient was 164 * 40 Ulg wet wi of tissue (N = 10 dete!minations) cim- pared with 1.9 U/g wet wi for whole canine pancreas.
On the day after cell isolation, there was some evidence of endocrine cell damage in the Petri dish cultures. Some clusters of cells appeared necrotic. and endocrine cells were swollen and some appeared fragmented. There was cell de-
. .
w
86 days, respectively, for morphologic study. Unfortunately, most 01 the islet cells were lost during fixation of the devices. The remainder of the devices were terminated for a variety of reasons, most notably mechanical failure of the peristaltic pumps that recirculated the perfusate. Insulin secretlon from Petri dish cultures. Insulin secretion from small numbers of Petri dish cultures from each prepa- ration was also studied (Figure 2). The pattern of daily insulin output was similar to that seen with capillary devices. An initial Elecline was followed by a gradual rise. with output eventually reaching a plateau after 50-70 days of culture. Three of the cultures were followed for 120 days, and one for 130 days. Insulin secretion was in the range of 1-1.5 mU/ isletlday. Glucose-stimulated insulin secretion from devices. After six days of culture the glucose concentration in the perfusate was reduced from 300 mgldl to 100 mgldl. Insulin release fell (Figure 1) from 8.07 * 1.59 to 2.94 t 0.80 Ulday (P = 0.015). When the glucose concentration in the perfus- ate was increased back to 300 mg/dl, insulin secretion rose to 7.57 5 1.70 Ulday (P = 0.002). A similar pattern was ob- served when glucose concentration was lowered after 27 days of culture. In this case, insulin secretion decreased from
DIABETES. VOL. 34, SEPTEMBER 1985 852

10.82 2 1.43 -day to 3.10 i 0.62 U/day (P = 0.018). and then rose to’li.15 -t 1.68 Ulday [P = 0.027) when the glu- cose concentration was increased back to 300 mg/dl.
The short-term insulin secretory responses were alsci stud- ied after 1 and 4 wk of culture. Five of the seven units were arbitrarily selected. The data are shown in Fi.gure 3. [luring 2 h of perfusion with medium containing 100 mgldl glucose, total insulin output averaged 0.24 -t 0.09 U. When the glu- cose concentration was increased to 300 mgldl duriiig the subsequent 2 h. total insulin output rose to 0.70 2 0.27 U (P = 0.06). A Similar pattern was seen for glucose respon- siveness after 4 wk of culture.The mean insulin output #during the initial 2 h at 100 mg/dl glucose was 0.35 5.0.09 IJ. This rose to 1.19 2 0.42 U (P = 0.048) during the subsequent 2 h when fresh medium containing 300 mg/dl glucose was used in the perfusion.
DISCUSSION The biohybrid pancreas represents a potentially important future means for treatment of diabetic patients. These de- vices oifer a number of obvious advantages. The trans- planted islet cells are protected from immune rejection. and therefore immunosuppression is not required. Islets from an- imal sources can be employed, thus solving the problem of obtaining large quantities of human islets for transplantation. Because the amount of islet tissue required for transplanta- tion is of the order of 4 g, devices can be sufficiently small so that major surgery should not be required for implantation. Since an increasing body of evidence suggests that type I diabetes may be an autoimmune disease, an added’benefit is that the transplanted islets are protected from potential autoimmune attack by the diabetic host. Furthermore. in con- trast to electromechanical insulin delivery systems. no power supply is required for the biohybrid pancreas. and there are no electrical or moving mechanical parts that can fail
When implanted as arteriovenous shunts in severely dia- betic rats, capillary devices Similar to those used in the pres- ent experiments restore blood glucose homeostasis to nor-
Although implantation studies have also been reported in small numbers of dogs and monkeys.” these have proven extremely diificult because of problems involved in isolating large numbers of viable islet cells for seeding these devices. Because of this, insulin secretion by capillary devices in vitro has been limited to approximately 1-2 U/ day‘ using partially purified neonatal rat islet preparations.
The present study was designed to take advantage of the newly developed Velcro technique for large-scale isi3lation of islets from cattle and dogs.P With this method, it appears that viscous material that normally forms during collagenase digestion of pancreata from larger animals is trapped by Velcro. This permits islet cells to be released into the diges- tion fluid, rather than being enmeshed in a viscous mass.
The present study indicates that large numbers 01 islets can be isolated from canine pancreas using the Velcro tech- nique. It therefore proved possible to demonstrate that bio- hybrid pancreas devices release large quantities of insulin. In the present study. capillary devices seeded vhth the islet cell yield from a single canine pancreas released up to 20 U of insulin per day when perfused with cultute medium containing 300 mg/dl glucose. Furthermore. the d&ta indicate that after an initial fall in insulin content of the peilusate. insulin
0.0
0.4
0.2 P GLUCOSE CONC 100 Jw 100 Jw
Img/dl I 7 DAV za DAY
CULTURES CULTURES
FIGURE 3. Glucose stimulation On insulin secretion from biohybrid pan- creas devices iner 1 and 4 * On cunun. D0vi-s were mainiained wlui phtuiion medium containing I00 mgldl gIucoM) tor 24 h before test- - ing. Th8 medium was then changed and devices p d U d sf 1W mgldl glucoss for 2 h. hiring ihs subsaquinf 2-h pariod, fm8h pariualon mb dium wns subnnuted containing 3W mgldl gluccee. Value6 am, means f SEH for ñve d s v i a
’. -
output subsequently rose, eventually reaching a stable pla- teau. Two of these devices were perfused for 80 days or more and continued to secrete la20 U of insulin per day.
The pattern of daily insulin release from devices was similar to that of Petri dish cultures of canine islets. It is difficult to make direct quantitative comparisons between insulin output of the devices and Petri dish cultures, however, because the number and size of surviving islets during the course of CUI- ture were not known. Studies of these Petri dish cultures suggest that the initial fall in insulin output may be due to beta cell damage produced during the collagenase-Velcro isolation procedure. On the day after isolation, some islet cells appeared swollen, and there was evidence of necrotic debris in the cultures. The highinsulin output during the initial 1-2 days may therefore be the result;+ part, of hormone release from damaged beta cells. The gradual rise in insulin output from both devices and Petri dish cultures after 3 wk could be the result of at least three processes. First, there may be some replication of beta cells with attendant in- creased secretion, reflecting a rise in cell mass. Second, the rise in insulin release may represent gradual recovery of beta cells from the isolation procedure, with an attendant rise in insulin output per cell. Third. the high glucose concentration in the culture medium may cause gradual beta cell hyper- trophy and increased insulin biosynthesis and release during the course of culture.
The present study focuses on insulin, and therefore does not include determinations of glucagon and somatostatin re- lease into the perfusate. The possibility that these hormones
DIABETES, VOL. 34. SEPTEMBER 1985 853

may influence insulim release during the Course 01 ciillure remains to be investigated.
Our data also indicate that thepeta cells in these devices remain responsive to glucose. Lowering the glucose con- centration in the medium results in a significant fall in insulin output that is restored by raising the concentration of the sugar. This result is not surprising, since maintenance of ditferentiation with respect lo glucose responsivenes!; has been previously reported for devices seeded with rat iklets.'
In summary, the present studies suggest that mas!; iso- lation of islets for seeding of biohybrid pancreas devices is feasible. Using this approach, it should prove possible to conduct implantation studies in a variety of diabetic ariimals and, eventually, in man.
ACKNOWLEDGMENTS ' We thank Diane Waice. Erik Larson. and Elizabeth Burns for their skilltul technical assistance.
REFERENCES ' Chick. W. L. Like. A. A., and LaUñS. V: Beta cell Cvllure On s!mthetic capillaries: an allificial endocrine pancreas. Science 1975. 187.84749.
2Chick, W. L.. P e w J. J.. La"%, V.. L w , D.. Galleni. P. M. P m l . G.. Whinemore. A. D.. Like. A A,. Conan. C. K., and Lysaght. M. J.: Artifcial
pancrass using living beta cells eiiects on g l m e hmWStaSiS m diabetic rats Science 1977; 1 9 7 : 7 m .
3Sutheriand. D. L . Presentad at 1984 Meeting of the American Asse ciation of Physicians.
' Knazek. R. A , Gullino. P. M.. KMkr;P. O., and Ded"cl<. R. L.: Cell culture on anificial capillaries> an approach to tissue growth in vnro Science 1972. 178:ffi.
Chick. W. t..Uke. A. A,, Lawis. V.. Galleni. P. M.. Richardm. P. D.. Pam, G.. Mix. 5 w.. and coitm. C. K.: A hybrid artificial pancreas Trans. Am Sac. Anif intern Organs 1975: 21:&14~
'Tze. w. J.. WMIQ. F:c.. Chen. L. M.. and OYwng. S.: ImpiantaM artificial endocrine Dancreas unit used lo restore normaglYCaema in thedi- .
*- .
5 j .~
abet!; rat Nature 1976. 2 € 4 : 4 W 7 'Sun. A. M.. Par~sius. W.. Healy. G M.. Vacek. I.. and Macmorine.
H G.: The use. in diabetic rals and mwikeys. 01 arlificial Capillary Units CMI- taining cultured cstets of Langerhans (anaiciai endocrine pancreas]. Oiabetes 1977; 26 113639.
aTzze, W. J.. Tal. J , Wong. F. C , and Davis. H. R.: Studies with KR plantable artificial capillary units mtaining rat islets MI diabetic dogs. Dig belologia 1980, 19:54145.
Lacy. P E., Lacy. E T., Finks. E. H.. and Yasunami. Y.: An improve0 m e l h d tor the isolation of islets from the beef pancreas Diabetes 1982. 31 (Suppl 4 ) . 1 W l l
'OLindall. A,. Stenes. M.. and Sotenwin. R . Immunoassayable insulin content Otsubcellular tractions 01 rat islets. Endocrinology 1969. 84.21&23.
'* Wrioht. P H.. MakUiU. D. R.. Vichick. D.. and Sussman. K E. insulin immunoassay by back-titration: some Characteristics of the technique and the insulin preipitant action of alcohol Diabetes 1971. 20.33-45.
'2Humbel. A. E., Basshard. H. R.. and Zahn. H.: Chemistry 01 insulin lo Handbwk d Physidogy. Sectim 7: Endocrmn&gy Vol. i. Endocrine Paw cieas. Sleiner. D. F.. and Freinkel. N.. Eds. Banimore. American Ph~siolooical Socieiy. 1972.
'i
OIABEIES, VOL 34, SEPTEMBER 1985
. , - ~ ~~ ~ . . ~ ~ ~ . .

: : I ¡? ior i iea l grafts in rabbits treated with topi- y t ' a a p i : n A: systemic absorption and local im- b c ' effwt. Rr J 0phthalniol 1985; 69: 600. s,p>riti i\: an overview. Trans'plantation 1981; 32
! rlo.;piirin A. Amsterdam: Elsevier Riamedical.
' .\ l.'i<de L>I 1, Grnf E. Speck B. Cyclosporin toxicity in , !42 \ '
, ri8N I . P.ni.,i 196B; 20. 213.
8 : e l ?%7. I:.,< I I :e.i ': .\,.I 6 I te? ! I If:, ,,,1>er 19x7
Vol. 46.30-31. No. 1. July 1988 Ptintrd in U.S.A.
dono. admit posefi glycei 14 pri a sen man !
All itonez aham pencr pI0L-e index leaat Then numb Lble Qmoi Uletc ah (
., . .su ' ~~~
:I *. Tri "3 ~
i *run mK,
STIMIJLATION Ob' CELL REPZlC'ATiON IN TRANSPLANTED PANCREATI(' ISLETS BY NICWI'1UAMTDE TREATMENT' hype1
best, 4.4 r Si ELLAX SANDLER~ AND ARNE ANDERSON
De~:nrtiiim! i,! .+f.!dú.<:l ' r.ll fi&&g, Uppafa Uniuersdy, $-751 W Uppala. Sweden
tuü ir A m a j o r (rl:stacle for i s l i ~ t lr .~~n.;i)lantntion in insulin-
dependent dkahetes mellitit., is t(i obtain a suff ic ient
the cell rep1 ¡<:ation in t h e ~írsftctl islet preparation *:auld be st imulated in the recipiiwt. In i h b , prrsent fitudy udui.t mice were t,reated for 14 <lit>,s w i t h daily injections ( s f nicotina,mirlii (500 mglirs b<,,,r seguent'ly, t,lie autor&dio,:rni;~,ic laheling index in thi: cells of the L,nncreatic i:jl:.ts r a ~ c u l a ~ in ncirm;il mice a n d iih syngeneic isl,.ts trfitm ipkuited into alloxaii- diabet ic micc. Treatment nith nirotinamide c a w e d a m o r e th,an three-fold i n c r e i * w i n the islet cell laheling index in tlri! endogenous p;in<:rixti<: islets, and also a 60% increase in t h e cell reiiliciition r a t e s of t h e trans- planted isle1.s. It thus aiiprars t.hA nicotinamide e n - h a n c e s islet *cell replicai i i in, [mssil>ly through a n inhibi- tion of poly(kDP-ribose) .;ynthetnoe activit ies
ti:.!:iie. I f however, the growth of the grafted isleta, either of ,:jult. could & exwnsively
amount of is'.& tissue. This rii:iy piirtly be overcome i f i,iLli!ants, i ,n this could pogsibly overcome. is in Th thi:3 coni <t ti;il,y
thc'r dia:,ites ( I ) . Nicotinamide treatment also improved the ap'iritaru, us diabei,es of nonobese diabetic mice (2) and a coniibiiiet' treiitmeiit with nicotinamide and desferrioxamine pt,,rentc!! recurrence of the disease in islets transplanted nnriobew diabetic mice (3). In tissue culture experiments with iscil;itecl ,, nii?,tati , , , i 10 m m o l ~ nicotinamide, increased islet ceU
ha\ e lwri , however. no studies on how nicotinamide affects islet cell replication in vivo. We have now investigated whether nicotina iriide influences the replicatory activity of islet cells ioc3ted it the pancreas and in the spleen following transplan-
great interest that long-term treatment of par. mbei Iicre;ltirtd rats with which is a potent olPol
. ileoti * t i *P ama
"TU
or saline. su,>., pol::(Al)i'.rihwe) synthetaseinhibitor, was found toameliorate ' be
pancreatic isle&, we found that me&um supple.
., ~ as by autoradiography (*,, the* ',
Besides the problems with grzi't iejertion, the major obstacle for successfiil islet transplsutation in insulin-dependent din- betes mellit,iis is that of obt,iinitig ti sufficient amount of islet
t,, mice, using autorediographic
MATERIALS AND METHODS
'This work waa supported 'The S.urediih Medical Research Council (12X-109; 12SU2273; 12P-7680). the Swtilish Diabetes h i a t i o n , t he Nordic insulin Fund, Aqe 1,ouis-tIan~~n hiindenfond, the 1ioech:rt Diabetes Pnindatio~ the Siedish k i t t y of Medicine. the Juvenile Dinbetea Foundation Int.rniitii>nal, Msgnnus Bergvills Stiffelse, t.im he Wiberg Foiiniiation, and the Errifor,i Family Fund
'Addnss eornspondeqce to: Dr. Stellan Sardler. Departinent of Medical Cell Biology. Biamcdii:um. P.O Rox 571, S-751 23 Tlppsda, Sweden.
pineniei,ii islets m e a s u d In another series, the mice were diabetic !iy alloxan admimiatration (75 m& body weight, no,iaiy), whereupon 150 islets. mllagenaae isolated from ay
~ - ...._ ~ ~ .-.. ~.

vu. I
"g.
W d topi. I in
1; 32:
dici
'itY in
'ly 19U U.S A
1
SSO@
?We;
her, n
1.4 It i& of pal pov :liar ied kh and
ntea.. ts wit suppJ< ilet .o tb.. affec
vhet' et c nspliii ties.
ram
._ obtain w, ,f o. d i s y lice WI
s in-t reni
iyngen i"tl
e-mm
SANDLER AND ANI)EKSSON 31
,I(
,,ib,,iiti,
nsplanted to itheir spleens, two weeks after aII<ixan The niimher omf transplanted islets chosen was pur-
to Prevent normalization of the animals hyper- es were obtained by retroarhitel puncture on day e serum glucose concentrations were sacayed by
glucose-oxidase method (Glucose Analyzer 2, Beck-
,,r~,rlcjiL,~,~,phy. After 14 days, the animals were injected intrsper- >viti) 'Il~thymidine at B dose of 1 pCi/g body weight (Amer-
~ , , T e r , , r t ~ i ~ ~ d , Amersham, UK) IZO and 60 min before dealh. The S I W " pa.,.rea:.ei (,, the spleens were then fixed in Bouin's solution and
n,~cJsrc[ for aiitoradiowrphy ns described elsewhere ( 5 ) . The latwling P ,n+x deermined by counting the number of labeled nuclei of at i~L)l., ~o(H) islet cells, in the pancreas and in the grafts in each animal.
~ ~ l > , : l i n g index was c!xpressed as 8 percentage of the total lXr of islrt cells counted. No attempts were made to classify the "u::
hkled islet ~ l l s according to twe. A recent study of ours has, however, kn,onstrsted that the islet B cells, which constitute the majority of
equally active in their DNA synthesis BS the other islet cells ( 6 ) -
~inolysis. The resulb are expressed as means f %EM. G~~~~ of data were compared by means of Student's unpaired t ti?st.
RESULTS
,,,, n~,t. l n s i , c , , , ~ ~ ~ ~ t s , Fullerton. CA).
ito,,zaIl?
r e 1 1 6 ,
Treatment with nicotinamide for 2 weeks did not affect the wnlm glucose concentrations at time o f death in the normal ,,,ice (data not shown). Similarly there was no difference in the hyperglycemia of the alloxan-diabetic and transplanted mice mated with saline (25.0+4.7 mmoljl) or nicotinamide (31.11 4.4 mmol/L). However, as shown in Table 1, nicotinamide treatment caused a more than three-fold increase in the islet e l l replicatory rate in the normoglycemic animals. T h e trans- planted islets also showed a marked increase in their rates o f
replication following nicotinamide treatment.
DISCUSSION
The present study thus supports the notion that nicotinaniide enhances islet cell replication, possibly through an inhibition of poly(ADP-rihose) synthetase activities. It cannot, however, be excluded that the increased islet. cell replication in t h e nicotinamide-treated animals merely reflects an increased islet cell turnover rate, and the increased cell replication is only a compensatory effect. On the other band, in the study by Yone- mura et al. ( I ) an increased islet size was reported in the
TABLE 1. Effects of nicotinamide on islet cell replication in mice
Saline Nicotinamide Auuirsdiographie islet cell labeling index 1%)
Pancreatic islets of normogly- 0.20f0.04 (9) 0.7M0.16 (8)"
Islets transplanted into the 1.5f0.25 (IO) 2.4f0.20 (9)" eemic mice
spleen of diabetic mice
Means f SEM for the number of animals given within parentheses. 'PCO.01, unpaired Student's f test. ' PC0.05, unpaired Student's I test.
-
animals treated with nicotinamide, suggestive o f an islet cell regeneration. It is also likely that the prolonged remission phase of the diabetic patients treated with nicotinamide as reported by Vague and colleagues (7) was due to an increased B cell regeneration. The higher cell replicatory rates in the splenic islets of the saline-treated diabetic animals, compared with the islets in the pancreas of the correspondingnormoglycemic mice, probably reflects a stimulation of islet cell replication due to elevated glucose levels ( 5 ) . Even under hyperglycemic condi- tions nicotinamide can further increase the islet cell replicatory rate, as evidenced by the transplantation experiments. This may have implications pertinent in the clinical attempt to transplant isolated islets to diabetics, for which a major obstacle is to obtain a sufficient amount of intact islets. Although nicotinamide is purported to be a safe drug for use in man, clinical trials with the compound should be carried out with great caution in the light o f the observation that nicotinamide may contribute to tumor formation ( 8 ) , probably by an inter- ference with DNA repair processes (9).
Acknowledgments. We thank A-B. Andersson. E. Forsbeek, C. Bitt- kowski. and A. Nordin for their excellent technical assistance and A. Snellman for careful typing of the manuscript.
REFERENCES 1. Yonemura Y , Takashima T. Miws K, Miyazaki I, Yamamoto H,
Okamoto H. Amelioration of diabetes mellitus in partially de- pancreatized rata by poly(ADP-ribose) synthetase inhibitors: evidence of islet B-cell regeneration. Diabetes 19% 3 3 401.
2. Yamada K, Novaka K, Hanahisa T, Miyazaki A, Toyoshima H, Tanú S. Preventive and therapeutic effects of Large-dose nicotin- amide injections on diabetes aasmiated with insuütis: an obser- vation in nonobese diabetic (NOD) mice. Diabetes 1982; 31: 749.
3. Namüm IN, Prowae SJ, Carotenuto P, hfferty KJ. Combined treatment with nicotinamide and desferrioxamine prevents islet allograít destruction in NOD mice. Diabetes 1986; 35: 1302.
4. Sandler S. Andersaon A. Long-term effecta of exposure of pan- creatic islets to nicotinamide in vitro on DNA synthesis, metab- olism and B-cell function. Diabetologia 1986; 29: 199.
5. Swenne I, Andersaon A. Effect of genetic background on the capacity for islet cell replication in mice. Diabetologia 1% 21: 4M.
6. Mellgrea A. SchneU Landstrom AH, Petemson B, Anderasan A. The renal subcapsular site offers better growth conditions for transplanted moue pancreatic islet cells than the Liver or pplan. Diabetologia 1986; 29 670.
7. Vague Ph. Viaiettes B, Lassman-Vague V, Vallo JJ. Nicotinamide may extend remission phase in insulin-dependent diabetes. Lsn- cet 1987; i: 619.
8. Rakieten NBS, Gordon A, Beaty DA, Cwney RD. Davis Rü, Scbein PS. Pancreatic islet cell tumors produced by the combined action of streptozotoein and nicotinamide, Prm Coe Exp Biol Med 1971; 137 280.
9. Ueds K. Hayashi O. ADP-ribosylation. Annu Rev Biochem 1985; 54 73.
Received 10 October 1987. Accepted 11 December 1987.

MULTI-FUNCTION THERAPEUTIC DEVICE FOR DIABETICS
B.N. Hung and K.Y. Lin
Dept. of Biomedical Engineering Chung Yuan Christian University Chungli, Taiwan (32023), R.O.C.
!ABSTRACT
i t ab l e f o r 3-meals uses programnible
i&ODuCTION
chronic disease. The insulin a good treatment f o r , diabeti.cs
there are two major types of ystem. One is close-loo er i s open-loop systea [F-tjP. em uses glucose sensor fo s e value and has a feedback e open-loop system i s only an v i c e that the in ject ion ra t e a patient under doctoii's
instruction.
we chose open-Loop
The ~ e ~ ~ a research has indicated that w i t h precise y con ro l l ed o f the blood plucOSK the diabeticsjcan t bet ter therapy. I n the long term therapy Ifor,d' bet ics , i t i s not enough for a therapeutic e v i c which only o f f e r s meal rate or f i x ed ra t e in ject io , .
In th i s research we change the conven- t i ona l f ixed rate function t o a variable s e t t ing and de l ivery function. In order t o have a simple operation, there are only four functional knobs, that are T,P,L and G knobs. Connecting with se 8-digits monitor we can in j e c t insulin t o dia- betics e f f e c t i v e l y under the doctor's instruction.
SYSTFM STRUCTURE
The system structure i s shorn i n Figure 1 . It contains four major parts.
1. Keyboard ü Display The keyboaid consists o f fourteen knobs
that are ten niimberic knobs and four functional ~~~ ~~~ ~~ ~
knobs.. Those knob and a buffer device were con- nected t o a pin of PCO and Pcl o f the If0 inter- face, I C 8255.
The disp lapcons is ts of two sets o f ADD 5404. They are connected t o CPU from I f 0 device. This system a l so has h o undefining h o b s that can be expanded f o r other use.
Figure 1. system Structure
4

t I I f I I 3 i
i 3
a8 selected as the central as produced by Zilog com- i s 2 MHz that i s osc i l la ted ry has two types, one is AM 6116), the other i s read ). Both of them have 2 K This system can also expand
8 K bytes by adding the ad- dmss l i nes f o memory chip.
Insulin In ject ion Port
PRIBCIPLES 0s INSU i I N INJECTION TRANSFORMATION
of each step o f s t e p K i 3
distance fmm ring to ring of ping motor.
t o t a l steps need to turn one e of stepping motor.
I therebore,
e ateppmg motor turns one cy- tube w i l l I n j e c t Ax distance,
w ve have
1 t
E =A' f A X
Pmm th i s fannula we can calculate t h * t o t a l steps cf stepping motor t o in j e c t t.iie insulin dose to diabetics.
THE SOFTWARE SYSTEM
The main flowchart of software system i s shown i n Figure 2.
Ye used 2-80 assemble language t o run the software system. The micLCJXQCessor development s)tstsm of MICE ( micro i n c i r cu i t emastor ) was used f o r systemic debug and developed o f the Pro- gram.
. . , He also used the EPROM wr i ter t o n r i t e down a l l the systemic program into EPROM memory chip for th i s system.
crc ~viiiylir
MTl TO !/O
E& M T I TO I10
Figure 2 The Hain Flowohart O f ?oft- ware System

I ZX?ERIMEIYTAL !
emining the patient'@ 24-hrs c u m according t o docwr's dieg- re 'insulin dose , tu+ on the the operatina pracedu+s.
T knob : Ye can input the the systo+. by ying the T knob. i 3 from O0 : O0 t o 23 : 59. Cver the rahge the display w i l l be hmn an error signal and we have to key in . the t me once more. I f the Inpiit time is correct , t i s sy9tem w i l l s ta r t t id ine . The 2-80 C X w % l l s t i rt operation.
after keying i n ? knob, va3 can dose rate t o the system i n the
ter completing one set bats, we knob once more and key in ano-
xstem. The i n s u l u dQso rate to 939 mu/min. The bdsal rata include i n this range.
' S knob is used for qxaaiaing F. When we key i n L knqbr"it
w i l l show ths t time and it 's dQse irade. We t w i l l show the nvxt t i d e and
dose rate. knob helps us to examine and
G knob : A e r completing the L knvb, u can key i n tire G $ob. Then the system x i i l e*&
n program. Steppin5 pot8k ulin into the pa t i a i t . , %is be time and shows mrr)nt time. display. When time :re+cb& e and dose rate, the Jtepping
it's CorrespondLng s$s@. ned over 23 : 59 i t w i i l atart
! i ~
R E ~ U L T S
treatment.
Figure 3 The Syetemic Configurat;on
Figure 4 The System Contmi Circuit

t : [':
r r' L
i
Figure 5 ' The
DISC&CIOB
stepping motor
amlog system.
for th is system.!
i
D
- set In d.tl
... <................. aitpuu d i u
1
L 14 16 18 20 22 24
L i n Dose Output Curve
CONCLUCIOA
rcroprocessor t o control >ted an impulse signal to le insulin transfor p i m - le output dose of i n s u l i n Ususlly using microprq- i s more prec ise ly , than
.nt o f th is study i d to f ixed rate method Uo a
.nfusion o f the insulin, inge insulin dobe 'rate ling to t h e i r diigndsia. .abetics w i l l get tneat-
:ated that th is a j s t q is treatment. Furither
I order t o improve tne
! Size and weight. The tis system is small s iae i s more convenient f o r iation, all the functio$s iain the same. Thereflore, iesign an optimal c i m u i t
m e r consumption o f the :est parer cansumptiam of i ject ion port. Hod i o power stepping motor is iign. The ih%& 'rgsiq- ibe has to be nininiized
ACKNOWLEDGEVENTS
This research was supported by the Department o f Health Grant No. DOH75-0303-34. Executive Yuan. the Republic o f China.
REFERENCES
1. J.C.Pickup ** Cl in ica l applications o f infus -ion systems ", J. of Uedical Engineering 8 Technology. vo l . 8. no. 3, pp. 101-107, 1984.
2. A.R.Albisser '* Device for the control of disbetes mell i tus ". Roceedings o f the I E E E , vol. 67, no. 9. pp.1308-1320, 1979.
J.F.Mcmurry " The a r t i f i c i a l pancreas today ** , Henry Ford Hosp Med. J. vol. 31, no. 2, pp. 77-83, 1983-
3.
4. T.G.Marshall, N.Nekhiel. Y.S.Jackman. K.Perlman and A.ü.Albisse " New micmprocessor based insul in contro l ler 'I IEEE Tram. on Biomedical Fagineering, vol . BME-SO, no. 1 1 , pp. 689-695, 1983.
5. P.J.Blackshear I' Insulin infusion pumps i n the treatment o f diabetes '* Medical Instrumentation, vol. 16, no. 1 , pp. 17-19.1982,
6. Y.J.Spencer " For diabet ics . : an e lectronic pancreas I' , IEEE spectrum, pp.38-42, 1978.
I . D.Rothwell. 1.A.Sutherland. J.C.Pickup,J.J.Ben . -ding ,H.Keen and J.A.Parson I' A new miniature , open ioop.ertiacorporeai insulin infusion pump *, J.of Biomedical nigineering, "01.5, pp.178-184, 1983.
8. J.C.Pickup, %Keen, J.A.Parsons. K.G.U.M.Albert and A.S.Rowe "Contiwous sub- cutaneous insulin infueion : irapro*d blood- , g1uco.e and interacdiary metabclite control i n diabetics ", The iancet, v01.51, no. 10,pp. 1255-1261, 1979.
Y.J.Spencer *' A review of programmed insul in de l ivery systems '*, IEEE Trans. on Biomedical Pngineering, vo l . BME-28. no. 3, pp. 237-251,
9.
1981.
10. b .K .H l~y , H.L.Minuk, A.U.Alibisser, S.B.Marliss and B.Zirman " A portable system for continuous intravenous insulin de l i v e r y : characterist ic and results i n diabetic patient ",Diabates Care, vo l . BüE-30, no. 11, pp.689- 695, 1983.

c
THE OPTIUAL CONTROL OF AN ARTIFICIAL PANCREAS: A SIUULATION STUDY
R. T . A r r i e t a
E l e c t r i c a l Engineering Dept. , un ivers i ty o f F l o r i d a C a i n e s v i l l a , FL 32216
glucose r e gu l a t o r y mode l , o f and Uar i I 2 1 was chosen f o r t h i s
9ecause of t h t s ub s t an t i a l amouni.-of r e s e a t ch . a va i l a b l e on t h i s model.
? I t r ~ a d i a b e t i c person under c losed 3ctrOl , the model was modified by 9 the cquat lons represent ing the 'us production and r e l e a s e of ' and . i n s e r t i n g an equation t o p.: the . r p t e o f change o f the
voltagk qutput. The r e s t o f the *i.. equat ion$, !&re l e f t unchanged, 1~"q 'eqGation represent ing the Of re lease o f L: glucagon; there lo re ,
f l e d model + ; e c l o s e l y represents ~ . ~ . a b e t i c pat ient , mer.^, than a
-0' has hadjthe d i s e a s e f o r many
, ImE/Ninth Annual Conference of
~. ~
ABSTRACT
This paper uses optimal cont ro l theory .,,,J d v%ld-<ated. 3&Ko~.-haIELlUnq mode 1 . t o the search f o r a minimum c o s t cont,tol
pancreas. Q u s l i t a t i v e
,&e about the b i o l o g i c a l p a r t o f t&e
;,.,tern vas included a s const ra ints on the olood ' g lucose concentrat ion. , WIU &.eernined t,hat 'aimple on-off n fus ion r i S i r s with t.hq.eqholde that depend on ly on cae bl.aod g ~ u c o s e concentrat ion and the w, @ f i t s , d e r i v a t i v e a r e c l o s e t o
*or ~ Fn ~aft~*fi.ciaT ..
q#ci+.
The f i e l d o f optimal cont ro l d e a l s wick :he maximization o f a perfor--+ m i e i associated with a dynamic system
the equations that q?.v>g-t.he system, atsi any COllS.tt+tiPt. on the v a r i a b l e s of the *ter. ill.
._.
I n medlcine i n p a r t i c u l a r , and app l i ed l n genera l , optimal cont ro l may prove u s e f u l i n determlninq
r:aae,-to-optimal, cont ro l a lgor i thms, n o w %+.: :Simulation modeling has b~ecorne..oMnon- ) i . C Q . The present work is p a r t o f on Oing
into tfie app i ics t ' i on of 09- rrr!c! to the des ign and implementation of *I :c:e?ligent a r t i f i c i a l pancreas. ,~
5
years . The i n su l i n re leased by the pump I s assmmi t o be unmodified ( r e g u l a r ) .
The d iE f e r en t i a1 equation that represents the sensor i s :
11) I t ' a l l ows the introduction o f a l a g between the time that the blood g lucose Concentration (Gbl reaches a c e r t a i n l e v e l and =-time that the g lucose concentrat ion ins ide the sensor c a v i t y IGs) reaches the same l e v e l . The. parameter (Kl respons ib le fo r t h i s l a g depends on the locat ion o f the sensor as w e l l a s the geometry o f the sensor's c a v i t y and the Proper t ies of a scmtpermeable wmbrane which excludes inter fe r ing substances. As a f i r s t approximation, the l a g parameter was set to produce a 1 0 minute l a g in response t o a s tep change i n blood glucose concentration 'i31. Equation 1 i s based on a novel op t i c a l ro ta t ion sensor u t i l i z i n g diode l a s e r s . Within the phys i o l o g i c a l range of g lucose concentration, the response o f t h i s sensor has been shovn t o be l inear 1 4 1 . This l i n e a r i t y i s r e f l e c t e d i n equation 1 .
&Voltage = K(Gb - Gs)
The performance index [ the t o t a l costs that w i l l be minimized by the optimal c on t r o l ) i s g iven by:
f J = L p u d t (21
where p represents the p r i c e of i n su l i n , u i s the i n su l i n in fus ion ra te , and the time interva l O t o T represents 1 day. The search for a minimizing contro l was constrained by the knowledge that c e r t a i n l e v e l s of g lucose a re detrimenLa1 t o the pat ient . To represent qua l i t a t i v e knowledge about the detrimental e f t r cL s uf both very hiyh and very low glucose l e v e l s , a penal ty function was included i n the perfornrnnce index so that var ia t ions i n the blood glucuse l e v e l bryond a certa in a l l owab l e range produced a pronounced increase i n the cost assoc ia ted w i t h that c on t r o l . Exact knowledge of how these glucose l e v e i s are detrimental i s not necessary t o contro l the penetration of the s t a t e trajeCtOKy into these "forbidden** ranges, since the ve iqhts on the qenal ty terms can be chosen s o that the peasetrat ion can be made as small a5 possi b i e .
The r a t e o f glucose dypearancr into

- - . - the bloodstream due t o me!als 15 incorporated into the model a s :
X=A t exp ( -C t ) 0 ) where A and C a r e constants der ived from o r a l glucose to lerance t e s t s and meal du r a t i on s . The inputs in to the model c o n s i s t of three equal -s ized meals which s,um t o a t o t a l g lucose intake o f 2509. S ipce such an input pattern i s a d a i l y event , the optimization of the :system i s constra ined by the need t o have t h e f i n a l d a i l y l e v e l o f blood g lucose equal t o the i n i t i a l d a i l y i c v e l . This const ra int was a l s o included as a pena l ty term i n the performance index.
Even though the insu l in d e l i v e r y system i s not e x p l i c i t l y modeled, the r a t e o f i n su l i n d e l i v e r y into t i s sue s i s assumed to have a maximum va lue that cannot be exceeded.
The model was wr i t ten i n the SLAM11 . , s imulat ion rañguage and run on a Prime
minicomputer. The conjugate g rad ient opt imizat ion subroutines were wr i t ten i n Fo r t r an .
RESULTS ApO DISCUSSION
Using the mi n i mu m p r i n c i p l e of Poyntr iag in i t can be shown that when the rate , equations a r e l i n e a r i n the contro l , and so i s the performance index, the p o s s i b k l i t y e x i s t s Lhal Lhe optimal cont ro l w i l l be a t the boundary o f the contro l r e g i o n (su c a l l e d bang-bang con : ru l ) . For t h i s model, t h i s means an on or o f f cont ro l o f the insu l in d e l i v e r y system, where the d e l i v e r y r a t e i n the on s t a t e i s the Gximum a t t a i nab l e . For the system i n quest ion, so lut ion o f the appropr ia te a d j o i n t equation shows that the Hamiltonian i s always dependent on the contro l , t h i s p rec ludes the ex istence o f a s ingu la r azc, and assures that i f an optimal cont ro l e x i s t s , i t w i l l be bang.-bang ill. This mathematical argument i s I n agreement with r e c en t work that shows decreased i n s u l i n u t i l i z a t i o n f o r a g iven l e v e l of g lucose coritrol vhen the i n su l i n i s in fused i n a p u l s a t i l e manner (51. From the r e s u l t s obta ined from the numerical opt imizat ions it i s apparent that the optimal cont ro l i s
-. v e r y ~ s en s i t i v e to the const ra ints imposed or, the blood g lucose l e v e l . I f the a l l owab l e reg ion i s narrow, say from 80 t o 1 2 0 nig:dl, the optimal contro l can be a s i n g l e long pulse o f insu l in a t the beginning o f the day fo l lowed by smal ler pu l s e s l a t e r un ; whereas, i f the upper bound i s re laxed, the optimal cont ro l produces three s im i l a r pulses, one f o r each iura1 ( the t o t a l amount of insu l in u t i l i z e d i s lower in the l a t t e r c a s e l . The genera l trend discussed above depends heav i l y on the r e l a t i v e k'ights given to the penalty 1.uncLions used for the low and high g lucose concentrat ions .
A given optimal contro l f o r a system such a s this one, where most o f the rate equations a r e coupled, depends on the state Of the system a t every instant. I n the a r t i f i c i a l pancreas, however, only one v a r i a b l e i s measured ---- the glucose con- centrat ion a t the sensor . The s ta te of the system cannot be known from knowledge of j u s t t h i s v a r i a b l e . Even thouqh d i rect u t i l i z a t i o n o f a numerical ly derived opti- mal contro l cannot be car r ied o i t i n this case, optimal cont ro l s derived under a wide v a r i e t y o f simulated conditions a r e being used t o d e r i v e re la t ionsh ips between the sensor g lucose concentration and i t s tim de r i v a t i v e , and the glucose l e v e l s a t which switches in the contro l should occur to approximate optimal cont ro l . T h i s work i n e f f e c t a i m t o c reate an expert system whose knowledge base i s derived from L simulation model. As a prel iminary example o f t h i s approach, blood glucose stayed within the 8O-l4Omg/dl~ range when the knfu- s i on vas t r i g g e r ed by a r i s e i n the sen- sor's g lucose concentration above 13OIcq/dl and was shut o f f by a drop i n the Sensor's glucose concentration below 120mg/dl. A l - ; though such a contro l is not optimal, it behaves s i m i l a r l y t o an optimal Control under s t r i c t s t a t e v a r i a b l e constra ints .
CONCLUSION
Optimal contro l theory can be used to show that this mathematical model o f an ar- t i f i c i a l pancreas i s contro l led o p t i m l l y by a bang-bang contro l whenever an optimal cont ro l e x i s t s . Numerical so lut ions Of such optimal contro l problems can' be used to b u i l d a knowledge Lase lor an i n t e l l i g en t feedback con t r o l l e r that would turn the in fus ion on arid o f f in a quasi--optimal fashion.
REFERENCES
1. Sirye Ap: üutimum Svstemz a L Prent ice -Hal l , Englewood C l i f f s , N . J . , 1968 2 . Cobe l l i C, Mari A: va l idat ion O f mathematircal models o f complex endocrine- metabolic systems. A case study on a nodel o f glucose i e gu i a t i on . a g - ñ i u l . ECL Comout. 21:390-393, 1983 3. March WF, Rabinovitch 0, Adams RL: Noninvasive g lucose monitoring o f the aqueans-humor o f the eye: par t 1 1 . Animal s tudies and the s c l e r a l lens . Diabetes u 5:259-265 , 1982. 4 . A r r i e ta IC, Burk DE, Batich C : The f e a s i b i l i t y o f a semiconductor-lasex glucose-detection system f o r insulin-pump therapy. Presented as abs t ract I 3 0 6 a t tmhe 4 7 t h annual meeting uf the ADA. 1 9 8 7 . 5 . üratusch-Marrain PR, Komlati tI* Waldhausl ww: E f f i c a c y of p u l s a t i l e versUS ,
continuous i n s u l i n administration ! on hepatic glucose production and glU'?Se u t i l i z a t i o n i n type I d i a be t i c h u l n a . I 0 iabe Les 3 5 : 9 2 2 -9 26,19 8 6 . ~~
BEO-H.2 The Medical Device RqJ i i ldt ion i,i the rederal Repub- l i c o f Germany, H. llii?t('?, !ii:!.itute of Ph,ysiJIoqy, Johaniies GutenDErq.-U~,iveiii ty, 0-6500 Maiii.z, RFG
The Medizin~sr.atl.vei^i,rdnung (MedGV) has bcm enac- ted on Jan. l s t , 1986. I t s object,ion i s the protcc- t ion of uscrs, pat.ients and t h i rd persons against any avoidable r i s k s that might Lie iwlated wi,th niedi- Cal devices (iii.ds). In soparate paraariphs,, ' the MedGV speci f ics the regulations both for Iiiiirket ad- mission and employment of m.ds. The rn.ds are clas- s i f i e d iri one of four classes. Tile 1.class consists Of a l i s t with 25 high-risk devices. The ?.c lass compriccs a l l energy-powered.iriiplants. The remaininq energy-powered m.ds belony to the 3.class and a l l other m.ds to the 4.class. The most relevant regu- l a t ions of the MedGV are: (1) mads o f c l ass 1 and 2 need a type-related market admission i n which fur- ther par t i cu la rs are specified. ( 2 ) m.ds of c l ass l and 3 have t o be l i s t e d .in an inventory. (3) Only spec i f i ca l l y t ra ined users are allowed to employ m. ds of c l ass 1 and 3. (4 ) m.ds of c l ass 1 are only f ree f o r the first operation a f te r a complete func- t ional check and operating instruct ion have been Ddde hy tho prodiii:er or ri ippl ícr. ( 5 ) A d:!t.nilcd bol>,: iiiust be kept. f4r each class 1 m.d. ( 6 ) Acci- dents with personal i n ju r i e s must be reported to the author i t ies . ( 7 ) iii.ds supplied before Jan. 'Ist, 1986 had to undergo a safety check by authorized experts within two years i f proper maintenance,in the past could not be proved by the owner.
244 1988 Wor ld Congress on Medlcal Physlcs and Blomedlcal Engineering San Antonlo. Teras

BEB-A.4 !iolutc ~ a m p o r i in a Hybrid Bio-Artificial Piincrcaa, 51.R. Pillarella *. A.L. Zydnry . Department of C!wiiiiraI Engineering, Uiiiwrsity of Delaware. Newark, Delawarr
.
Many of the long-term rornj>lirations ass<- .inted with (he rurreiit treatment of dinhrtes by insulin injrctions hnve bwii l i n k d to the lnrk of physiologic ~lucosc and i n a u l i i i c w t r < ~ I . Ilrrcnc rtiiili* * havi. ~ l ~ ~ i i ~ o i i ~ t r n t ~ ~ ~ l tlic IN>- . . IviitiJil i i C the hybrid bio-iiri!:i<.inl pancreas in controlling blood glucose concentrnrion, hut the insulin response to a
* ~ ! < h o s e stimulation remains unacceptably slow. \Ve hare drveloped a d ¡led theoretical model for
s o l u i r (glucose and insulin) ransport in a hollow fiber riiriiihraiir bio-artificial pancreas. The model explicitly rlrrounts for convective transport arising from Starling
.. ., Bow is the device, inrludiiig the effects of protein and ped crll polarization on tlie flow patterns. Also included is the reduction in solute diffusivity in the porous mem- [irani. M well a.3 the enhancement of solute transport in .:tip liiriien arising froin slivar-induced red cell iiiigrations.
Model prrdictioiis appe well with in uitro dotu taken in Amiron hollow iibr: rwtridges (30,000 54bV cutoff). .. . Rrsulta indicatr that inr:t,asirig convective transport sig- niflcan:ly iinprtivrr thr in<iilin rrsponsr. The model yro-
c m vides R fiiiidniwiitnl iindi~:standing of the important pht%- iioiiiena govrriiing solute transport and can thus be used in t h r &.sign of iriiprovrcl cliriirnl <Iwirrs.
* .
I .,
. ,
.-
.._
..
~ . . BEB-B.2 H<mbranas fur tiasma Fi arc ionat ion. P.S. Hnlchrsky , M. %Ix>rovski, and Y . N o s r . üepartment of A r t i f i c i a l Organs, Cievelan<i C l i n i c Famdat iun, Cleveland, Ohio
c-
I
"Advances i n tho ~ x t r n ~ i o i p o r c a l on-line treatment 3f blood for ther~apeiir irs have madi! i t ai, cffec: ive ti?chtiiqur* i n cl i t> ic .s l ai:plicatiuiis. i t i r lh -r levelopmont t6 increase i t s i'ust e f fert . ivcncss ai:d s impl ic i ty of o p r a t i o n is r equ i r ed . Ncmbrane separarion trt.hnolo#y i s Ldeally su i t ed to meet
. hese needs. l.!unhr.ni<i { t a r l . i o m t i o n of plasma has :,em studied f , ir f hi? sc!Iecr~ivc removal o f macro-
r - mlecules from p la ína . So?iite sclect. ivity niid removal amounts haw bemi ! :how" to be stronp.1y
lilted to thc C I I O ~ C ~ L . : t i i r membrane ami the tmpersture oi ~ p < * r n l ion. l;pt'r;lt ion in t~hr r o l d
em0v.71 of so lu te s formins m i c r o a g g r e g a t e s at. -., >elow pliysioloi<ic t.empi~raturti surh as c r y o i i g ~ r e -
:atatiir. prote ins (;is t > vo~<lciim!ins iiiid immune
.,
cryof i l l r a t i o " ) is p a r t i c u ! a r i y e f f e c t i v e iii t1ic
c,cq> I ex<,:; ) ',,,<I ve ,-y i :il.fip mac i.i,nn Ir r u 1t.s . opera- ; o r 3 "I at>ovi- ~. l iy - . io l I ,wiwrni ure <I Iir~rmoí i 1 - ! a ~ i o i i ) i , ; ~ w r : : e í t I? i n l i p o p r o t c i i i frac- .uristiivi of 'I~P l . w iwii v e r y !iw density i i p i , p r w i n 5 fi-oni fti,. h i s h c1 y I ip"p'">t<', i , , s . <:1ini-- i sl i ,<i i , . : i ti<,\.<. s!:<,,,n lllilt ! h < 1 * . tV<!~:,iq"<.s <ir<,
,e119 i "e p 1as:na L : .f>i:ir c n t pl-udi:cr ?. ai-<! noL
*
- .
-_ ,luired mal. ¡rig m w i ~ r a n c ~ piasma í;.nrt ionst i n n a
r' cferi<.>i a;t! rt t3t ivc t:, p l a s m e,uchiinjic.
h L i E Blomedlral Englnverlng Scientlfic Y a p ~ r s 7
BEE-B. 1 Renal epirhelial cells grown on permeable membranes as a porenrial ulrraflrrarion processor, P. Aebischer:T.K, Ip. Brown University. Providence, RI 02912, USA
Dialysis has dramatically changed the prognosis of renal failure, yet it remains burdened by considerable morbidity because of the non-physiologic manner in which it performs son= of the most critical renal functions. Vie combinntion of nii tiltrufiltriition device with cxchiingers thai nciivcly transpon solutes m y lead to a device that could purify blood in a more physiologic manner. We arc resently studying the transpon capacity of tlie. exchangers. ur approach consists of growing functional kidney epithelial cells in a tight monolayer on permeable membranes. The cell lines LLC-PKI. a proximal tubule-like cell and MDCK, a distal tubule-like cell, can be grown to confluence on nitrocellulose. cellulose. polyacrylonitrile and polysulfone either in hollow fibers or on flat sheet pumcable membranes. Attachment factors must be used in order Io obtain this coverage. Dual label tracer studies reveal that inulin and glucose move across all unseeded membranes with similar rates in either dircction. LLC-PKI cell seeded membranes arc impermcabie to inulin but demonstrate a net apiciil to basolateral glucose flux. Depending on the membrane used this glucose flux varies significantly. The effects of attachment factors, substrate and cell types on the mass transpon capacity of the seeded membrane arc under study. We conclude that renal epithelial cells cnii control the pemicability of a membrane to various solutes, thus opening the way to the development of a biologically controlled ultrafiltration pmess,or.
8
BEE-B. 3 EXTRACORPOREAL IMMbNOAUSORPI ION
Geory~ Buf ta loe : P1t.D. COBE L a b o r a t o r i e s , I n c . 1201 Oak S t .
Lakewood, Co lo rado R0215-4407
E x t r a c o r p o r e a l imnunoadsorp t i on (El) i s d e f i n e d as t h e use o f immab l i zed in imunologic r e a g e n t s f o r t.lX t r e a t m e n t o f b l o o d o i i t s i d c o f t h e body, f o r t h e r a p e u t i c purposes. l a b o r d t o r y and c l i n i c a l s t u d i e s , E1 i s m e r g i n g as a t h e r a p e u t i c m o d a l i t y t h a t t oday can be a p p l - i e d 40 a number o f d i s u r d e r s . Kecen$ advances i n f a b r i c a t i o n e n g i n e e r i n g drid b i o t e c h i i o l o g y a r e b e i n g a p p l i e d t o c r e a t e n w systcins. Thcre a r e c e r t a i n c o r e c r i t e r i a t h a t must br? m e t i n the deve lopmrn t o f E l system5 wh ich i n c l u d e m a t e r i a l s b i o c ~ m p a t a b i l i t y , f l o w / press i i re /vr i Iume pa ramete rs , and c i r c l i i t d c s i g n . Systems can be des igned t o t r e a t wholp b l o o d ,
A f t e r many y e a r s o f
, o r c e l l u l a r f r i i c t i o i i s . o f the h i g h l y s e l e c t i v e n a t u r e o f E l , a
t o t h e a p p l i c a t i o n o f t h i s tech- ology to trmt c u r r e n t m e d i c a l problems. is l a c k o f d e f i n i t i o n of t h e e t i o l o g y o f d s i g n i f i c a n t i i i i i i ibcr o f d i s o r d e r s t o w h i c h E l i n i q h t bP a p p l i e d . 'íiiiis, i n t.lie m d r term, E l w i l l l i k d y p l d v a ro l e ill t h e e l u c i d a t i o n o f d i i e d s e i i iechanises, .ii:d iii thr fu l .ure, E l h.is thP p o t e i i t . i d l o f he- roiiiiiry 'in e l í r v : i i v e for in of t h e r a p y .
c I 1988 World Congress on Medical Dhyslcw and Blomi.dlcal Englrieerlng * San Antonio. Texas 237
'i
I

. Blomedlcal Englneerlng Scientific Papore 8
BE8-G.1 MASS TRANSPOFlT IN PERITCNEAL DlALYSlS J . M. Woll'. M. J. Lysaghl. and J . W. Garber, Baxler Heallhcare Corporalion, Round Lake, It
Peritoneal dialysis is a blooddeansing process widaly applied for Ihe lrealment of palienls with end slage renal disease. Hypertonic diaiysale is periodically infused lnlo the periloneal cavity by gravity lhrough an indwelling cnlholor. Plnsrna walor and 8olules whkh would normally be cleared by Ihe kidney are transported from blood 10 dialysis solution through a rather mmplex series of resislances including capillary endoiheiium. inlerslilial lissue, periloneal membrane and fluid boundary layers. Fluids traverse lhls 'membrane" in response IO osmolic pressure differences: solules are removed by diffusion; both may be relurned Io Ihe bkcdstream via Ihe lymphatic circulation.
Despile ¡Is compiexity, the process may be adequately described by the analogy lo a simplo planar membrane separaiing two well mixed pools, This allow? the calculation of equhaleni irancpoil parameiers wliich characterize lhe system including: hydraulic permeability. sieving coeffidenls and mass iransler coefficients. These lransporl parameters rnay be readily extrapoialed and inlerpolaled so lhal tho behavior of a wide variety of solules rnay be prodicted from a relatively m a i l numbor of experimental maasuremonts.
c '.5 01 Flow Rate on Me Predictmn of
*_ +lw Vaive O d i b Area from Hamo- mic Measurements. R. WoepRoersler'
._<.B. Chadian, Universiiy of Iowa. low8 Iowa. ._ idy was parformed 10 te51 Ihe predicllon biliiies of Iha cilnically used Goriin
8185 tor Ihe effaclive orifice art.n(EOA) o! -- rletic heart valves. Pressure gradient. and valve opening area meosurements
P ., performed on four 27rnm v a l v e heses(Edwards-Duromedics. SI. Jude,
L-. ards-parlcardiai. and a lrlleafiat rethana vahe) each mounted in the aortic on of an In vitro pulse duplicator. Wilh ;nown valve oriflca area, a discharge .- iclenl(Cd) was cornpuled for each of Ihe valves and three EOA formiilas. AH Cd's
rl observed 10 Increase with increasing llic flow rate(CFR). An empirical ._ onship of Cd as a linear fiJncllon of SFR delermined through a regression analysis
~,~ ?ach of the valve geometries which >ved the accuracy of the prediction of the . Further work is needed io le51 for the .IS o i valve size oil the Cd. as well as -mining Cds for prosl1ie:ic hear1 valves O1
'.. .la 03 well ES the Aüslld and Oabbay
._. r- geometries.
P.
c,- G. 2 d kchanical ind Transport Factor. i n Slow Inuous Rana1 Rcplacment Therapies. It i i imci , . , i11 lone., Division N r v h t ~ o iogu. U i i l v . e s i r r , l ioch.+ N V
c -
L.
<,i"OU* ar ter I""e<,"U-. i W ) hemof I 1 ti-at ion .,. '111 and hemod ia l ~ , ~ s l s ,CAL'HPI ,al+? impor tar i t
Ii!ic% f o r treatment o1 hcmndynamical l> u)>- L. le p d t i r n t s w i t h rcndi f i i i l u r s e . Blood t l o w
L I I tticse c i r t i i l t s 1s i p v ~ . ~ n e d by t h e FA' r _ i u i ~ gradient, t o t a l i i i ~ r u i t ie,.;iil.arirc dril?
J r i 5 ~ 0 ; i t y . Dist , i - i t iut i i i , i u t h,.di m I 1 c -,,, W I I P i í goii.in;vi by t h i s \ v l e j t h \ ? I i i i ~ . i t i i , i ,
, , t nPl l I C-, ,.lllj W . r i L I t b y l l i r l i ~ ~ m i > f i l t r i ~ i l i a l ~ ; i i r t 5 L q o b k w ~ m ! hy
m e m b r a n e h y d r a i i l i L and pia%nd i incut ic , i i rc5 and membran<' I i y d r o u l i r permeah) l i t y . nariy variables i i i v o i v e d mdhe c . i r c u l t o p t i - L ion d i f f i r t i l t .
id praficr c i r c u i t c a n s t t u < . l i a n , mathemati-
P,"
*. .
r-
&. mile15 l irive been deve l r i pcd *h:Ciii g i b e i i ,"t and C l r L i l l t Chill~a'tei ::,t.irs a:., I n p ~ I t S , r t system p r r formani 1'. Ii, .r.umpt ,011s i i i r l i i d r , o d c i l i i i g of c<imporiarits o5 Poi5cuille T C ' ~
r!, and n e g l e c t of c o n r e n t i a t i o n polariza- : i f p l a ima p r o t e i r i s . S p a t i d l r a r i a t i o n o f
">*LO.,ty 1 5 co,F.,de,e,j. I ' , cd i c t i ons o f .mancc agree W i t h rezii1t5 o f L" r i t i - i i per $7 elper Imeilta.
c-
.. . r .
... s
L..
BEE-G.3 Tlll: FFFL:CT OF MASS TRANSFER I.IMI'CATI<)NS OM I N!1UI. I N SECH l;T I ON I N flYliR I n ART I F I C I Al . l > A N C H C A : : ( ' l a r k K . Colton, Keith E:. iniorinc, ani1 Martin I , . Yamlush, Departmerit of Chc-miciil ingincerinq , i.?ilss.Ichuse t t .s i n 3 t i t u to of i e c l i n o l e ~ y , Combridge, MP. 02139.
One approach to diabetes therapy i o im- plantation of xenogeneic i s l e t s iminiirioso- ?ate:l by interposit ion of a semiperniedblr r,:embrüne bet.wean the i s l e t i and the blood- itrerim n i t i . - , . sut> . interrial vanciu1oriz.i-
sal ly [pte3erit ifi l o s t d f t e r itio- iilt.iuii, torcing the i:;lct. ta d c p c n d in- s t c a d on external and intcrrial dif tuiioii to provide an environment wh8:rciri ttic hetd cells survive and s c c ~ e t e i n i ü i i n . TWO problcms are doscribed. ( 1 ) The effect of glucose and iiisulin diffusional imi'ations r.n obsc;.ved insulin oecretory dynamics. i:e s II I t s í ram ma t h c ma t i C R I moi le 1 s 1 1 ~ f i t i e (lesion conditions required t:o prelicrvc j.n- t r i ri :I i c ins ti 1 i n seir<- t. i on k i nr t i cs. ( 2 ) The e f f t : c t of p02 an i n t r i n s i c insulin 8"-
i:rc.ti@n. Mcil.suferi!rnt:; iii perifusion atitl s ti, t. i c <'I> 1 tori? deinons 1.ra t c ma r kedly re- <iucr:.l n<.ronri [ h a :;<: ser re t i ori i in d<? r rcrliiced
with R 1 , : w c r is let . c<ir-i, pO7, ,>s predict.e<l hy il m.ittiem.iti<-iil r i ior lc l , f o r ijlur.en<:-stirn- iil.i:i*:i %a>; coiiii>.irr%<l t.o I x i s n l conditions.
*
T O 1 , s ! i t i , . 'rhc::c ri- nix 1 t ~i i o r c c la t,?
F. 1988 World Congress un Medlral Physics and Biomedical Fnglnerrlng San Antonlo. Texas 243
F. mana^- -"I---. -.ll.l..--lly^^-__ -

The A trohLc do ad.&$
Pancreas. N.rgery a pat1mts ot inSUli noreover vaio(ible diabetes niníaturi Pawseas time by
has 23 defsogeiiar a t i w of
BiMtator bet- u1 Life SCieI aad it wii better anc niCter ins mellitus I
I
mc nttifi
me pat i e r w i t h a Bot aerted in1 fWa@ -4
of tbe ai eo **MI %%a way I Catheter <
?UT, BRESWNT AND FüTüRE.
C . Raptis add O. Dimitriadis
'nd Department of -1 n.aiicine-Propaedeutic ithens University dl Schdoi,*EVMGELiSWOS' Hospital
&TRACT
treatrmsPtwith Cn tp normalize the'm
ysioloqical u.
avoided. I
Plgure 1 :
Ria Ar t i f i c ia l Pancrear (~iostatoral
The Biostatozhas the followi g parts:l) A sensktive blood glucose analy er (3 ) . This glucqse analyz has a mebbr e w i t h glum- se oaidaae whia aeanrres'bl d glucose
blood is yithaqrat from the d i n . Blood g%ucoae i s measured 6 t i w s pCr minute (8.640 tima every U hays) 4 An insulin or dutnoee admin.Sotration -.This pump delivers insulin or dextrose into a
concqntrations 3 w i t h i n 14 minu 4 es after

ent than the one awal. Insulin or
..---- LS pdagraiired - $g g p r t a i n a igor i tima 11.2). 4 1 Srint g ace using t h e r m r q
aod glucose conden- of insulin or de%*
trow infu.erl bed every minute.
concentrqtions f a 5) P(e Bi0B-t o an audible signa
belo* 40 ffigldl above 4 0 0 mg/dl.
USE IN C/Lid$d AND RESBAHCH
ne h+s b w n us i@g hemodialysis in and to minta in
mately 70%. The problem consists i n the neutralization of the glucose sensor of the device exposed to the reactive @fforta_ of the body to eliminate the foreign ma- te r ia l present in the peripheral blood circulation ( f i b r in , p latelets etc) ( 2 1 ) .
Figure 2 : Blood glucose concentrations of a patient with diabetes under conven- tional insulin treatment (upper curve) and during connection to BiostatorR(lower curvet.
REFERENCES
1) Pfe i f f e r E, Thum Ch, Clemens A : The a r t i f i c i a l beta c e l l . A continuous con- trol of b l w d sugar by external regu- lation of insulin infusion (Glucose Controlled insulin Infusion System) .
2) Clemens A, Chang P, Myers R : The deve- lopment of BiOstatoC, a glucose con- t ro l led insulin infusion system IGCIIS) Born Xetab xes, Suppl. 7 , 2 2 , 1977.
3) Clarke W, Santiago J : The characteri- s t i cs of a new ulucose sensor for use
Born. Metabol. Fes. 6 , 339, 1974.
in a r t i f i c i a l &creatic beta c e l l . ~ -~ Ar t i f i c i a l organs I , 78. 1977.
4 ) Raptis S and Zoupas Ch : Recent pro3resu in the Therapy of Fiabetes Mellitus.In: The mnaqenent of Genetic Disorders, 299, 1975.
5) P f e i f f e r E, Kerner W, Beischer W e t a l : Insulin treatment during diabetic coma with an A r t i f i c i a l Endocrine Pancreas. tiom MeMb Res SUppl. 8. 150, 1979.

b e t k T i e n t s . Horm. Metab.' Res, Supp 8 , 178, 1979.
iostator GlucoSe Coqtroller.
ice F, Haymand M et al.: ed-loop artificiali $do- s to determine inkutin fo r an open-loop puhuta-
s, Cuppl. 12, 287, 1982. eischer W. Kerner W : The
infusion system.
izza R. Westland R et a l . :
ic activities qf insulin i n health ulin-dependent d i tored by the arti creas. Diabetea C
, Xaraiskos X . Pa olonqed a-qlucasi blood glucose co
rements i n patien dent diabetes qelljims.
I
H O m Metab Rea, 18, 253-55, 1986.
Control of blood suqaiz i n insulin- dependent diabetes : Comparison of an a r t i f i c ia l endocrue pancreas, continuous subcutaneolis insulin infu- sion and intensified conventional insulin therapy. New Enql J Med 303, 1313. 1980
21) Pfeif fer E : The a r t i f i c i a l endocrine pancrean : Past, present and future. Horn Metab Res Suppl 12, 187, 1980
20) Rizza R, Gerich J, Haymond I et a l . :
r' 1, . ? .a
., . I -
%.
w .. " ..
_ ,~ .
* The failUte' of conventional insulin therapy to direction of blood sugar changes, to the rata of
obtain st4ct metabolic control in diabetic insulin infusion: t h e e are the control ~. . algorithm. Rie algorithns are a function of the
levels of blood sugar: lesa than 50 and 70, r". between 70 and 133, and ovar 150 q / d l . "ha rate
of flow of the insulin i a determined by tho algorithm f r m the*projected"blood sugar calculated directly by the device. The t i r projection constant is 4 minutea and the operation i s identical with that defined for the linear blood sugar function. Finally. there is a flash function ~ s u t m a t i c a l l y provided the physician h a
c sought it through a svltch and that the miniam blood sugar gradient is 8 qhll and the ax- 22 mg/mn/l: provide$ the blood sugar is equal to, or greater than, a threaholQ defined by the user.
..
.-.
-.
~.~ ...
The duration of the flash and the flow can be r' manifest. decided in advence. after an insulin
function is inhibited for three hours. L. funtion nvlinly insulin the &'asci% can overrule that inhibition by
poiating the dial for time inhibition to O. There -. is also a m a n u z y operated bolus delivery. ' Thin
AEP also caiprises a dynamic alarm mchsnie capable of interrupting the injection of insulin if the $amwar& gradient is too steep and e bloodsugar levels which are too low. ., AEP i s used in diabetes. F o l l d n g the
n the utiliiation of studieq of BWSON and YAURU, radioimunologiul . .~ 'assays of insulin since 1- have shnm that the pancreas i n the heal subject !mintains the blood ." . sugar at a norma level by the -ai but constant secretion of insulin, w i th an increased rate Of .. secretion dur ineea lg . f u l l control of the
day, there are many systems of blood sugar. such as can be obtained in t,p autmatic i r g u l i n infusion: heavy and non- diabetic on insulin by the AEF', similarly depenb. transportablei pumps said "hospital pumps" and a8 qui- became obvious. 01% a %x+el* level Of portabib pe. The implanted pumgs are not 3 commn. The ospital pump is*currently used in the u. AEP. The f i r s t indication of 4EP i s the study Of
s stem. situated between the brittle diabetes: the intravenous continnOW glucose moni r and the insulin infusor .* intended& insulin eoute'is alone able to normalize the blood
requirebents I of the patient, so as to limit the knowledge of insul in requirements of COW=
essential parts:
._
I.
L to adjust -Y?- t , flow of insulin at a l l tines to the glucose level and the AEP can alone give a perfst
.-.
sugar to *within's variable over the 24-hour period: bad' The effectiveness. the safety requirements are increased during the second half
of the AEP depend primarily of the day end meal time needs ere proportioMll1 and upon the modalities higher during breakfast than at lunch and
a given time, and the dinner.
._ -
r
- .
L.
Canfarence of the Engineering in M i c i n e and Biology Society .. 1384 S1.W c 1987 IEEE
.. 1 , . .. ".., . . ~ ~ ~ __-^ ".

Continwus inaulin in fu ion constitute a explosive dwelopent in the treatment
of diabetics. The calculation of insulin- ,aquirementS my be deduced from observation of the insulin flow brofile'during a 24h. session on the A F ~ . This is the most accurate and mst logical =thod. But the results with sukutansoua route .=e not very good in britt le diabetes.
and
-- - Inter&aádicl or betvaen -1s blood glucose
levels or beMi levela indicate significant differences. Blood glucow is higher i n the afterown than in the morning and in the night than in tha afternoon. The besa1 insulin requirements betwean meals reprasent about 50% of the daily conamuption, amounting in our experience to 1.1 +/- 0.1 ulh. The ma l tiie requir-nts represent the other 50%.
Thus the AEP confirmed a new ecience ariaes: tha chronobtoloni of insulin reauireant. The insulin efficiency i a higher at the beginning than at the end of the day. On the contrary, prandial insulin requiremnts are significantly higher for bresl<fast than for dinner and'supper:* at faating t i r and -1 time. the circadian rythis of insulin requirement are reverse.
Therefore, AEP represent the best method for constant blood glucose control. Thus. as soon as our group developed these technique. We attempted t o induce remission perioda i n caaea of recent
ucute'onset juvenile diabetics with severe insulin deficiency during in i t ia l stages within 6 months of
The AEP is alao useful to atudy and treat diabetic crisis and to help the treatment in difficult diabetics: labour and delivery, renal dialysis, surgical operations and soon in our practice the best use was d u r i n i n c r e a t i c transplantaiton in a terribly britt le diabetic.
The ablation of insulin adenoma was alao _- easi-with a AñP able to arrange intravenous infusion of insulin ur dextroae.
The eua lvcdc clam technique was introduced as a way to quantify i n vivo insulin sensitivity. Since then it has been used to evaluate insulin- stimulated glucoae uptake in a variety of conditions. The technique l a performed after an overnight fast and based on determination of the mount of glucose that must be infused i n order to maintain plasma glucose at constant besal (euglycemic) or elevated (hypprgiycemic) level during a period of .L suatained hyperinsulinemia obtained by conatant insulin infusion. Variable awunts of glucose were infused as a 50% solution. along with a carrier infusion of 0.9% NaCl (0.5 m h n ) containing 0.26 mEq/miK+ and 0.18 mEq/mlFOú I;" Prevent hypokaliemia and hypophosphatemia and to
level. A foream vein was cannulated and used for continuous glucose monitoring with a technicon w i t o r usual17 employed for AEP run. The glucose infusion rate was made by adjusting the percentage "of the pump on the basis of changes in the
OMeti
Clamp'' arterial glucose concentration at choare
plasm glucose concentration observed during continuais glucose monitoring. ühen al l 's M id d done, the AEP was sdjuated at a hyperglycemic 1-1
r a d u l a t e d infvsion of dextrose or insulin and a conatant infusion of the ummderated substance. A ñand vein cannulated in a retrograde manner ms maintained at 55 degrees C in a thermrcgulated box to permit deteirination of plsma giucoae concentrations of arterialized venous samples. Metabolic. h o m o ~ l d b iocha iw l studiea i n patients treated with the AW or wíth Constant insullri infusions have sbam that the majority of the biochemical abnormlitisa so far regarded as aswciated with, and not of necssaity connected with diabetes osllitus. regress in a spectacular fashion wíthin -ya of securing fu l l control ortbe blood sup r over the 24-hour period (lactate, pyruvate free fatty acids, 3- hydroxybutyrate) with the exception of ala$me which remains elevated for a long- time. Adrenaline, noradrenaline, gr>b horwne and glucagon levela are within physiological limits.
To day, the need for a miniaturized portable or implantable AKF' providing continuous control of glucose is clearly mimifeat; t h i s m h a a not yet been fu l f i l l ed but an effective glucose sensor wi l l not become available in the near future.
IEB/Ninth Annul Conference of the Engineering in Medicine and Biology Society-1385
L
c
I 1 - ! ‘ F
i c Control ‘with”a
, , Pancreas , ,
irements to. Glycemic Response MOTOAKI SHICHIRI. RYUZO KAWAMORI NOBUYOSHI HAKUl YOSHIMITSU YAMASAKI AND HlROSHl ABE
1
SUMMARY We succeeded in miniaturizing a needle-type glucose monitoring system wlth characteristics sultable for a p pilcatlon in a wearable, closed-loop control system. A wearable artificial endocrine pancreas (12 x 15 x 6 cm, 400 g) consisting of a sensor, a microcomputer system that calculates insulin and glucagon infusion rates, and two roller pumps was developed.
inserted in the subcutaneous tissue of the forearm or abdomen of healthy and diabetic volunteers revealed that glucose concentrations in subcutaneous tissue were 1ü% lower than, but were highly correlated with, blood glucose concentrations in the range of 49-388 mgldl.
Glycemic control was established in diabetic pa- tients by intravenously infusing insulin in response lo measured glucose concentrations on a moment-to- moment basis for a period of several days. By compar- ing the glycemic control obtained in each patient treated with multiple insulin Injections or open-loop subcutaneous insulin Infusion, the superiority of feed- back control wlth the system was clearly demon- strated.
During continuous glycemic regulation, day-today variations of insulin requirements were recognized in both basal insulin Infusion and postprandial insulln Infusion rates in response to identical meals and exercise.
These data suggest the feasibility of long-term gly- cemic control in diabetic subjects with a wearable arti- ficial endocrine pancreas, and indlcate that to over- come changes in indlvldual metaboilc characteristics on a moment-to-moment basis, a closed-loop glycemic control system may be essential for ambulatory dia-
Continuous glucose monitoring by a glucose sensor
betic patients. DIABETES 1984; 33:lZOO-1202.
This Study ves presenled in pari al lhe 436 and 441h Annual Meetings o1 the American Diabetes Associaliwi. From Ihe First Depailmenl o1 Medicine, Osaka University Medical Scixial, Osaka. Japan. Address reprint requests lo Dr. M. Shichiñ. Erst Deparfmenl d Medicine, Osaka University Medical Schml, 1.150 Fukvshima. Fukushima-ku, Osaka, 553, Japan. Received lor publication 15 July 1984.
1200
e succeeded in miniaturizing a giucose-mon- itoring System into a needle-sized system that preserves sensor characteristics suited to a closed-loop control system. In addition, we
developed a wearable artificial endocrine pancreas that ef- fectively controls glycemia in pancreatectomized dogs for a period of 3 days and with replacement of the sensor for up to 7 days.‘2
Because the subcutaneous needle sensor provides the critical interface between man and machine. we tested its performance, safety. and feasibility in both healthy and di- abetic volunteers. We then attempted glycemic control in diabetic patients with a wearable-artificial pancreas system.
MATERIALS AND MRHODS Needle-type glucose sensor. The characteristics and prep- aration of the needle-type glucose sensor have been previously described.’2 in addition, to augment the bio- compatibility of the sensor, a hydrophilic polyvinylalcohol membrane was appl/ed to the hydrophobic polyurethane membrane. Wearable artificial endocrine’p&creas. The wearable ar- tificial pancreas system, consisting of a needie-type glucose sensor, microcomputer system, Iwo rolier pumps driving the unit for insulin and glucagon infusions. and a lithium battery. was packed into a small unit (12 x 15 x 6 cm) weighing 400 g. The wearable computer system memorizes measured glucose concentrations, insulin infusion rates (IR). and glu- cagon infusion rates (GIR) every minute for more than 24 h. A parameter input4ata output device was connecled to the wearable artificial endocrine pancreas when parame- ters in, the insulin and glucagon infusion algorithms were changW or to record the output from the glucose sensor and the hormone pumps for clinical records. Algorithms for intravenous infusion of insulin and glucagon in the system are the: same as those of our bedside system.”‘ IIR(t) (mu/ kg/min) is expressed as follows: IIR(t) = Kp BG(t) + Kd dBG(t)/dt + Kc. where BG(t) and dBG(t)/dt are glucose
DIABETES, VOL. 33, DECEMBER 1984
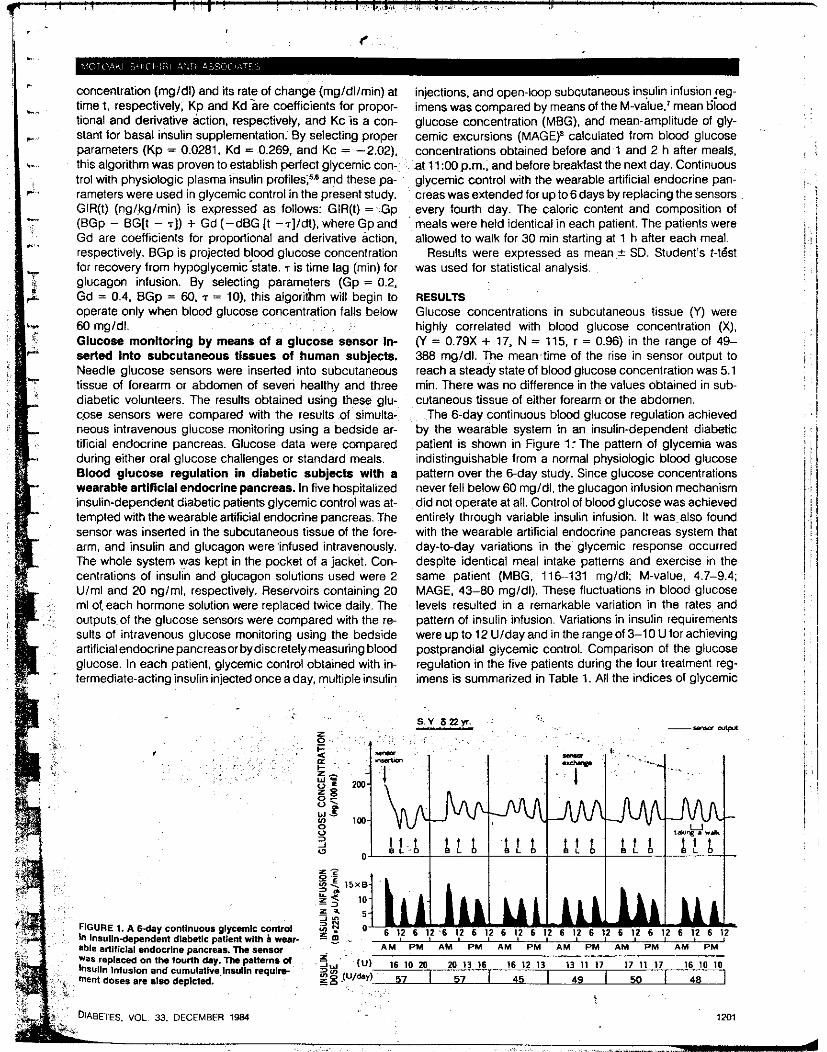
concentration (mgldl) and its rate of change (mgldllmin:) at time t. respectively, Kp and Kd are coefficients for propor- tional and derivative action. respectively. and KC 1s a ci3n- stant for basal insulin supp1ementation:By selecting proper parameters (Kp = 0.0281. Kd = 0.269, and Kc = -2.02). this algorithm was proven to establish perfect glycemic con- trol with physiologic plasma insulin profile^;^^^ and these pa- rameters were used in glycemic control in the present stu8dy. GIR(t) (nglkglmin) is expressed as follows: GIR(t) =' Gp (BGp - BG[t - TI) + Gd (-dBG [I -~]ldt). where Gp and Gd are coefficients for proportional and derivative action. respectively. BGp is projected blood glucose concentration for recovery from hypoglycemicstate. r is time lag (min) for glucagon inlusion. By selecting parameters (Gp = 0.2. Gd = 0.4, BGp = 60. 7 = 10). this algorithm will begin to operate only when blood glucose concentration falls below
Glucose monitoring by means of a glucose sensor in- serted into subcutaneous tissues of human subjecis. Needle glucose sensors were inserted into subcutaneous tissue of forearm or abdomen of seven hea1th.y and th,ree diabetic volunteers. The resulis obtained using these glu- c.ose sensors were compared with the results of simulta- neous intravenous glucose monitoring using a bedside ar- tificial endocrine pancreas. Glucose data were compared during either oral glucose challenges or standard meals. Blood glucose regulation in diabetic subjects with a wearable artificlal endocrine pancreas. In five hospitali2:ed insulin-dependent diabetic patients glycemic control was at- templed with the wearable artificial endocrine pancreas. The sensor was inserted in the subcutaneous tissue of the fa're- arm, and insulin and glucagon were 'infused intravenously. The whole system was kept in the pocket of a jacket. Con- centrations of insulin and glucagon solutions used were 2 Ulml and 20 ng/ml, respectively. Reservoirs containing 20 ml of. each hormone solution were replaced twice daily. The outputs.of the glucose sensors were compared with the re- sults of intravenous glucose monitoring using the bedside artificial endocrine pancreasor by discretely measuring blood glucose. In each patient. glycemic control obtained with in- termediate-acting insulin injected once a day, multiple insulin
60 mgldl. . .
5, . .~ . . .. . .
injections. and open-loop subcutaneous insulin infusion leg- imens was compared by means of the M-value.' mean 6lood glucose concentration (MBG). and mean-amplitude of gly- cemic excursions (MAGE)' calculated from blood glucose concentrations obtained before and 1 and 2 h after meals. .at 1l:Güp.m.. and before breaMastthe next day. Continuous glycemic control with the wearable artificial endocrine pan- creas was extended for up to 6 days by replacing the sensors every fourth day. The caloric content and composition of meals were held identical in each patient. The patients were allowed to walk for 30 min starting at 1 h after each meal.
Results were expressed as mean I SD. Student's ?-test was used for statistical analysis.
RESULTS Glucose concentrations in subcutaneous tissue (Y) were highly correlated with blood glucose concentration (X). (Y = 0.79X + 17, N = 115. r = 0.96) in the range of 49- 388 mgldl. The meawtime of the rise in sensor output to reach a steady state of blood glucose concentration was 5.1 min. There was no difference in the values obtained in sub- cutaneous tissue of either forearm or the abdomen.
The 6-day continuous blood glucose regulation achieved by the wearable system in an insulin-dependent diabetic patient is shown in Figure 1 I The pattern of glycemia was indistinguishable from a normal physiologic blood glucose paiiern over the 6-day study. Since glucose concentrations never fell below 60 mgldl, the glucagon infusion mechanism did not operate at all. Control of blood glucose was achieved entirely through variable insulin infusion. It was~also found with the wearable artificial endocrine pancreas system that day-to-day variations in the glycemic response occurred despite identical meal intake patterns and exercise in the same patient (MBG. 116--131 mg/dl; M-value, 4.7-9.4; MAGE. 43-80 mg/dl). These fluctuations in blood glucose levels resulted in a remarkable variation in the rates and pattern of insulin infusion. Variations in insulin requirements wereupto12UIdayandintherangeof3-10Uforachieving postprandial glycemic control. Comparison of the glucose regulation in the five patients during the four treatment reg- imens is summarized in Table 1. All the indices of glycemic
FIGURE I. A w a y C O ~ I I ~ U O Y S giycmic control h Insullndspendent dhaballc patient wlih ii wear- able aniriclai endocrine mncreas. The smsoi
1 DIABETES. VOL 33. DECEMBkR 1984
= z 0 -
' y o 6 1,Z 6 l,Z 6 1,Z 6 l,Z 6 l,Z 6 12 6 1: 6 I,? 6 1: 6 l,Z 6 I,? 6 12 L m . - AM PM AM PM AM PM AM PM AM PM AM PM
- - - 5, tu)- 16 IO 20 M I3 16 16 I2 13 13 11 17 17 11 17 16 I O IO
a:: LO tu/d.- 57 I 5, I 45 I 4 9 1 5 0 1 4 8
1201

TABLE 1 Blwd glucose regulatory indices in various kinds of insulin treatment regimens in five insulin-dependent diabetic subjects
lieatmen1 N
CSiit 3 13.62 2.6' 126i 12 ' . Y94 235'; WAEP 5 8 . 4 2 2 . 8 1 0 6 ~ 1 1 . 562..13
Data are expressed as mean f SD. 'P c 0.05 versus glycemic control with WAEP. tCSII, continuous subcutaneous-insulin infusion.
regulation (MBG, 106 i 11 mgldl; M-value. 8.14 :e 2.8; MAGE, 56 2 13 mgldl) during application of the wearable closed-loop control system were significantly Smaller than those values obtained by inbrmediate-acting insulin once a day, multiple insulin injection, or open-loop continuous sub- cutaneous insulin infusion regimens. .. respectively (P < 0.05).
With regard to the safety of glucose oxidase used .,in the glucose sensor, we demonstrated that when glucose oxi- dase was immobilized with glutaraldehyde to Cellulose di- acetate, there was no detectable leakage of glucose oxidase from the sensor as judged by measuring glucose oxidase concentration in the perfusate of an in, vitro circulatiori. Fur- thermore, no significant increase in total immunoglobulin concentration bound to glucose oxidase as measured with a double-antibody method was found in sera obtained from human volunteers alter repeated application of the glucose sensor in their'subcutaneous tissue? These data indicate that the glucose sensor in which glucose oxidase is bound to cellulose diacetate is safe and suitable for clinical ap- plication. In the present study we demonstrated that even though sensor outputs might depend on lwal conditions such as extracellular fluid circulation and oxygen availabil- ity. our sensors were rather stable in human subcutaneous tissue. . ' . .
By intravenously infusing insulin in respo'nse to measured glucose concentrations with the aid of a wearable artificial endocrine Dancreas svstem. it was wssible to ClOSelv rea-
DISCUSSION '
removal of the sensor showed a 23%. reduction in output current and prolongation of respase time to 43 s from 29 s. The.biocompatibility of the membrane of sensors kept in subcutaneous tissue for 3 days was examined by electron microscopy. Fixation of protein on me membrane was rec- -0gnized; thus. the decrease in outpui current of sensors alter 3 days of continuous subcutaneous use may be caused by
- the depression of the sensor secondary to protein deposition 'on the membrane. Histologic changes in subcutaneous tis- sue around the sensor-insertion area were examined in nor- mal dogs. Af!er a 3-day application, migration of leukocytes and slight fibrin deposition was recognizable in the insertion area. These changes could result in decreased perfusion of fluid through surrounding tissues and could therefore be one cause of time delay in sensor response. The sensor-related problems will be approached through alterations in mem- brane design such as varying the combination of hydrophilic and hydrophobic components of the sensor membrane. As an explanation for the observed glycemic variability, how- ever, moment-to-moment variation in individual patients' metabolic characteristics seem to be the more important factor. since daily replacement of !he sensor did not prevent daily variations of glycemic excursions. Metabolic charac- teristics that could be changing include variations in meal jngestion and absorption and in insulin sensitivity. Thus, we suggest that a closed-loop glycemic control system suitable for the ambulatory diabetic patient may be necessary to overcome the spontaneou? metabolic changes that seem to characterize the insulin-dependent diabetic subject.
__
ACKNOWLEDGMENTS We are indebted to Dr. M. Kosuga (Director, Medical Sup- plies and System Group, Fujisawa Pharmaceutical Co.. Osaka, Japan) and his staff for their cooperation.
This study was supported in part by a grant from the Re- search Development Corporation of Japan.
REFERENCES Shichiri. M.. Kawamori. R.. Yamasah¡. Y.. Hahui. N., and A h . H.:
Wearable-type artiicial endocrine pancreas with needle-type glucose ~ensoi. Lancet 1w:.2:112931. ,
2Shichiri, M.. Kawamori. R.. Goriya. Y.. Yamasaki. Y., Nomura. M.. Hakitl. N.. and A b . H.: Glycaemic wntrd in cancreatenomized doas with
,,late glyc&,ia even in ambulatory 'diabetic subjects': T& was true despite spontaneous day-to-day variation i l l gly- cemia and insulin requirements in the diabetic subject!; con- trolled with a wearable artificial endocrine pancreas. Three' potential factors could contribute to changes in sensor-
changing rates of perfusion of extracellular fluid through sur- rounding tissues in the region of the sensor, and changing metabolic state of individual patients during the course of the study.
The output characteristics of the needle-type glucose sen- sor were examined during 3 days of continuous tissue glu- cose monitoring and were found to be relatively constant. On the fourth day, sensor,wiput current relative io^ blood glucose determined from discretely obtained blood samples decreased to 74% of the initial value and the relative response time of the Sensor was prolonged 10 13.5 min from 5.1 min, compared with the implanted sen- sor. In vitro characteristics of the sensor determined after
a weirable artificial end?& pancreas Diabetologia 1983: 24:179-84. a Kawanwri. R., Shiihiri. M., Goriya Y., Y a m a d , Y.. Shigela Y., and
A&. H.: imponance 01 illsutin secretiw bared withe rate oi change in blmd glucose wncentration in glucose lokiance. assessed by the artificial beta
'Goriya, Y.. Kawamon. RKShichiri. M.. and A k H.: The development of an aiti~icia~ beta ceii system and itCvalidatia, in depancleatized dags: the physiological restoration of blmd glucose homeostasis. Med Pi=. Technol.
1979: 699-108. 5Shichiri. M.. Kawamori. R.. and Abe. H.: Normaiizatiwi of paradoxic secretiw of giucagw in diabetics who were cwitrotied by the aniiiciai beta cell. Diabetes 1979: 28.272-75.
0 Kawamori. R.. Shichiri. M., Kihuchi. M.. Yamasahi. Y, and Abe. H: P e m mrmalizatim of excessive glucagon responses to intravenous argl- nine in human diabetes mellitus with the artificial beta cell. Diabetes 1980. 29:762-& ' S~hli~htkr~Il. J.. Munk, O., and Jersild, M ' The M-value, an index of blmd-sugar COntrD~ in diabetes. Acta Med %and ~ f f i ; 1m6-102.
.' 'SewlCe,F. J..Molnai.G O..Rosevear.J.W .Ackerman.E..Gatewmd. L~ C.. and Taylor. W. F.: Mean amplitude of glycemic excursions. a measure of diabetic instability Diabetes 1970; 19 644-55.
*Shichiri. M.. and Kawanwri, R.: FeasibilBy of needle-type glucose semor and the wearable artificial endocrine pancreas System in human di- abetes meilitus. In Diabetes Treatment wñh Implantable Insulin Infusion Sys- tems Irrigler. K.. Kri12. H.. and Loven. R.. Eds. Munich. Urban and Schwan- enberg. 1983:224-30.
A*a lS78 07339-51.
measured glycemia: changing function of the sensor per se,
1 m2 DIABETES, VOL 33. DECEMBER 1984
,
i
. .
!
i i
~. " . . ... . . . ~ . _ . . , . _ _ ~ , . . _ . . . I . _ 11" ............I . . .

258
TABLE I
Mean insulin dose change (in units) suggcstcd by four diabetologists (D,, D,, D,, D,) and by the wmputer program. and wrrclations (Pearson’s correlation eoefficimt) between insulin dose suggested by the diabctologists and the wmputer program ( * p c 0.01)
D2 D, D. Program ?1
Cautious Normal
McanfSD . .0.32f2.60 -0.27f2.77 -0.21f3.59 -0.20I3.12 -1.13 * f2.94 0.15f2.44
‘Codations between program and:
D. D, D, D. Ca“ti0US 0.61 * 0.70 ’ 0.42 * 0.63 Normal 0.65 * 0.73 0.46 * 0.65
were compared to those calculated by the com- puter. Statistical analysis was performed using the analysis of vahnce and Scheffe’s test and correla- tions were evaluated by the Pearson’s correlation coefficient 131.
3. Results
The results of the study are shown in Table 1. The mean dose adjustments computed by the program in the ‘normal’ mode did not differ significantly from those suggested by the physicians. In the ‘cautious’ mode however, the program tended (as expected) to underadjust insulin dosage with re- spect to the diabetologists. The changes calculated by the program correlated significantly with those proposed by the four diabetologists, the more so in the ‘normal’ therapeutic mode: Incidentally, the correlation coefficients ‘between’ the M s ranged from 0.46 to 0.73. The insulin dose calcu- lated by the computer was within 2 U of that suggested by the physicians in 95.2% of cases with the ‘ n o d mode, and in 86.3% of cases with the ‘cautious’ mode; and within 1 U in 88.5% in the ‘normal‘ and 71.6% Ui the ‘cautious’ mode.
4. Conclusion
The results of our preiiminary study show that the program described in this paper is capable of
reproducing with sufficient accuracy the responses of expert diabetologists adjusting insulin therapy based on blood glucose profiles. These findings appear encouraging in view of a future clinical application of the program. We feel that this kind of pre-clinical evaluation of ‘therapeutic’ com- puter programs is mandatory, because of the in- creased availability of software, also in the area of diabetes therapy and the I& of standardized methods of medical software evaluation.
5. Availability
The program is available on request from the authors.. .
#’
Acknowiedgements
The assistance of A. Bueti, P. Compagnucci, I. Nicoletti and M. Marcelli in evaluating blood glucose profiles is gratefully acknowledged.
References
(I] Cauo FX-770P p n a l wmputa: user‘s manual ( M a Computer Co. Ltd., 1985).
121 J.S. Skyler, D.L. Skyla and D.E. Siegler, Algorithar lor adjustment of insulin dosagc by patients who monitor blood glucose, Diabetes Care 4 (1981) 311-318.
131 G.W. Sncdsar and W.G. Cochian, Staustical Methods (Iowa State University Refs, Ames IA, 1967).
COmp“, Usev ier
CPB 00
Or:
i I
1. Inn
The I dardi: d iap nine, treat:. pend mark, S t N C !
systrr sella landi: sion 1
to Sb conve A
- COlrtT tioani ford F-
0169-2


."
Y. L o L m P. T. LAsaUrs
s. THOMAS M. HIELM
CAROTUI EMlARTERECTOMY TRIAL: WORD OF CAUíiON

- I ~
USO DE Y INF'IICION CONTINOA SIJKUDdK3 DE 1NSULINA M P A C I W I S I>TAP,XiICOC COH OEAX"%L M T m L l C O HODERMM SEcll1?DL.RIO A IXFFZCIO~ES IWfaaGRF\? FS. Ernestc Garcja-Rubí* IFi esentado por Eerriórdo FErez E.), Ri!>.én C;i:-.Sn-Pi!.r~a*, Enrique qbli~aishi S.*. Francisco J. GÓmez Fíiiez,J.:an A. Rull. D;to. de Diiietes y !i.:C-tcl,olismo de Lípidos. instituto racional de la h t r - i r i 6 n Ti- !tGvTro, D.F.
la efectivioad de la infusión contSnua subcuthca de ir:suiina IICSII en pacientes diabéticos insulinodependientes que CursaSan con un episodio infec sioso intercurrente comparado con un tratamiento convrncicnal intrnsivo i T C I i ~ Los tnfernos fueron pareados en sexo, edad, tiempo de evolucik de la <!ic?-wtes y ti?o de infección. Se evaluó durante el estudio el control glbrímico, l a z p r ? ciin de complicaciones, el impacto sobre el &roces0 infeccioso (medido romo días para lograr la mejoría), y la preferencia por caCa método. Los pacientes asignados a la ICCI la recibieron por una bomba de infusión modelo AS-6C y sistemas Sub-Q-Set con insulina regular bovina U-40 6 U-20, calculhdose la dosis con la fórmula de 0.5 UI/kg peso distribuida el 35 % como infusión basal y el resto en bolos (35 % para el deiayurio, 25 % para la ComiZa y cena, y 15 % pa ra la colaciónl, de 30 a 40' yrrprandiales. A los pacientes asipados al TCI se les calculó la dosis por l a niisma fErmuia distribuida el 30 % c m o insulina into aicdia en dos dosis y el resto de la manera ariotada arriba. Recibieion una dieta calciilada según requerimientos con 45 % de cal-Siiiiidratos, 35 % de gi~asas y 20 % de proteína en tres comidas principales y colación nocturna. Fueron vigilados con qlucemias venosas y capilares pre, postprandiales y nocturnas cada 72 hrs; además 'Eiarimente con glucosurias fraccionadas semicGantitativas tres veces al día. Fue
nienos por dos seniarias y las dosis de insulina modificsdas se$;
Se estudiaron dos grupos de 8 pacientes, cada uno con 4 del sexo n.aiculino y 4 del fensenino. La media de edad y tiempo de evolución de la diabetes para cada grupo fue de 33.7, 6.6 y 33.5 y 7.1 años respectivamente. Los pacientes 3 , 0 y 8 fueron autocontroles. Para el grupo con lCSI las meüias del control glucemico fueron de 178, 189, 190. 190, 193, 166, 182 y 139 m g i mientras que para el coc trol fueron de 189, 198, 180, 211, 178, 194 y 135. Ninguno de estos resultados fueron significativamente diferentes cuando se compraron niediante la prueba de U de Eann-Wnitney La s glucg surjas tuvieron medias de 1.14, 1.05, y 1 .16 gr/L en el grupo con ICSI mientras que fueron de 2.53, 2.63 y 2.91 en el control, siendo signifiratiuaivente diferen tes con la prueba de U íp de 0.007 en los. tres turnos) y la t pareada lp de 0.00007 a 0.0003251. La media de evolución en días del proceso infeccioso fue de 9.75 en la ICCI contra 15.13 en el control siendo significativamente diferentes al compararse con la prueba de t lp de 0.007). Finalmente, la preferencia favors ció a la ICs1 con 5 pacientes contra ninquno en el grupo con TCI qie prefirieron su uso, lo cual resultó significativo al compararse con la prueba exacta de Fisher lp de 0.012). Con estos resultados podemos concluir que el uso de la ICSI no ofrece ventajas reales en cuanto al control glucémico cont.ra el TCI y que puede presentar desveg tajas. Sin embargo, al considerar el control por glucosurias, mejoría en el prg ceso infeccioso y preferencia por el método, l a ICCI puede presentar ventajas contra el TCI. Es posible que en casos bien seleccionados esta modalidad de trs tamiento pueda ser una alternativa ventajosa al tratamiento habitual de pacientes con p-ocesos infecciosos intercurrentes y descontrol moderado, reconociendo que la lCSI no está exenta de desventajas y complicaciones y requiere vigilancia N'
lde p de 0.148 a 0.51 y t pareada lp de 0.08 a 0.581.
dadosa.
. - - Enviar o:

1 Introduction CONTROL IN diabetes is important (CAHILL et af., 1976; SIPERSTEIN et al., 1977). Whether better control will prevent long-term complications is not known (SALANS, 1983), but the clinical benefits of improved control are manifold (JOB et al., 1976). including the potential for delaying certain complications (MAUER et al., 1983; ENGERMANN et al., 1977). Towards this goal, the increasingly frequent and widespread use of self-blood-glucose estimation has pro- vided the diabetic with a new dimension for achieving better control of his or her disease (Diabetes Care, 1980). Interestingly, algorithms to assist the physician and to guide the patient in exploiting these valuable data advan- tageously do exist, and a special-purpose computer device for calculating insulin doses has recently been reported (SCHIFFRIN et af., 1985). Apparently, such a device can in fact provide demonstrable benefit clinically.
Reprint requests should be addresssd to DI Albisser.
First receivsd 18th April and in final form 7th August 1985
@ IFMBE: 1986
We here undertook to study the ability of existing manual treatment methods to improve diabetes control under highly controlled conditions. With this experience as a reference, we also tested the above-mentioned special- purpose device ( S c m N ef of., 1985). the computer algo- rithms of which calculated appropriate adjustments of insulin dosage at each daily injection and thereby achieved and maintained a designated level of control. We here describe the results of this three-way comparison of manual and machine-implemented algorithms adapted for the purpose of improving diabetes control.
2 Materials and methods
2. I Dose-adjusting algorithms Algorithms for adjusting insulin dosages have been
reported (SCHIFFRIN and BELMOME, 1981; SKYLER et al., 1981). We started by choosing the ones described by SKYLER et al. (1981) as a first approach to dosage adjust- ment. For convenience, these have been summarised in Appendix 1. T o test this method of treatment Rgorously,
Medical & Biological Engineering & Computing November 1986 \ 577

Ary -1etabolism (ALBISSER and S<:HULZ, 1986) (Omni et , A ;IWR and SCHULZ, 1986) adapted to the clinical -xm,,tances of meals ar.d injeitions (ALBISSER et al., 85). Some of the details of the simulator are outlined in ,pe ix 2. This simulator is unique because stochastic ri:il ity is introduced to accommodate for the 'fuzzy' rameters of the model. in this way, unpredictable and nerently variable processes such as absorption of food im e gut, absorption of insulin from the subcutaneous pot :ompliance with respect to diet, exercise, and other :tors such as emotions, errors in blood glucose estima- zn, r-ors in drawing up and injecting insulin, all typical hu: i n diabetes and its management, could realistically sindated. The ranges over which the 'fuzzy' parameters
-re allowed to vary depended in part on the compliance el t. We used a value of 3 in a range of O to 10. O rref mds to a patient with4exceedingly poor adherence protocol, who makes large errors in dosage, as well as
:t and even on occasion skips meals or injections. A level c o pliant subject is quite the opposite and shows only
ierc t biological variations consistent with known iges. :Nit+ this simulator of human diabetes, we tested the O l i 5 :d algorithms (SCHIFFRIN et ai., 1985; S C m r N d ~S~LMONTE, 1981; SKYLER et al., 1981) first and then demented proprietary and copyrighted algorithms as .ail below (courtesy BCMC-Better Control Medical mr, ters Inc., Toronto, Ontario, Canada). These were :ctionally a combination of those published but included -efully selected but fixed sensitivity factors so that our -si0 consistently recommended appropriate dosage ing,_ to bring glycaemia to acceptably normal mean 'ues while capable of starting from a broad range of :lor al initial metabolic circumstances in a wide cross- :io of patients. Because a laboratory scientific com- :er was used, many diabetic 'patients' could be iulated before actual clinical trials were conducted. <in ly stated and similar to previously detailed thc s (SKYLER et al., 1981), the present (BCMC) algo- ims were based on the following assumptions. The vni.-g short-acting insulin (SAIB) had major action .we I breakfast and lunch, and its effect was reflected in
b . d d glucose level before lunch. Also, the morning mnediate-acting (NPH or LENTE) insulin (IAIB) had .jor--ction between lunch and dinner, and its effect was ieci I in the blood glucose concentration before dinner. 2 evening short-acting insulin (SAID) had major action ween dinner and bedtime, and its effect was reflected in b' '3d glucose level at bedtime. Finally, the evening
:rn-.,,iiate-acting insulin (IAID) had major action over- nt. and its effect was reflected in the blood glucose test i!lts.on arising the next morning. ~ c c -dingly, the specific insulin dose adjusting algo- imi-Implemented by the computer were as follows. All ;es were in units (U) and blood glucose concentrations T P -mgdl-'.
io' - 5
I d D , = IAID-1 + 1 (BGB - 110), 1 SIC O
= IAID,[9(BGB0 < 50) + lqBGB, > 50>]/10 (1)
ere.JAID, represented the intermediate-acting insulin se dinner on day O, the current day. The '=' sign >ule=-be read as 'is replaced by' and the inequalities umed binary values of I (true) or O (false). IAID-I rep- en?.-{ the intermediate-acting insulin dose taken at ine, the previous day. BGB represented the breakfast
currimt and previous days with i = 0 to -5. SI, were Sensi- tivit:y factors which weighted the summation. BGB, rep- resented the prebreakfast plasma glucose level on day O.
/ - ' - 1 1-1 - 5
I A I B , = IAIB-, + ( B G D - l l O ) ¡ 1 S,,
= IAIB,[9(BGDo < 50)
+ lqBGD, > 50)]/10 (2) wheire IAIB, represented the intermediate-acting insulin dose at breakfast on day O and I A I B . , that of the pre- vious day. BGD was the predinner plasma glucose level and the summation was over the five previous days with i = .- 1 to -5 and S,, were other sensitivity factors. BGD, was the predinper plasma glucose concentration of the current day.
- 5 SAIB, = SAIB. + 1 (BGL - BGB), CSx
- 1 i:: + (BGB - 1 lO)o/Su
= SAIB,[9 (BGL, < 50) + 10 (BGL, Z 50)]/10 (3)
where SAIB, represented the short-acting insulin dose at breakfast on day O and SAIB-, the corresponding dose the previous day. BGL and BGB were, repectively, the pre- lunch and prebreakfast plasma glucose levels on the current and each previous day. S,, and S,, were sensitivity factors.
- 5
SAID, = SAID-, + 1 (BGS - BGD), 1 S,, - 1 i::
+ (BGD - 1 lo), /S6,
= SAID, [9(BGSo < 50) + IqBGS, 50)]/10 (4)
where SAID, was the short-acting insulin dose at dinner on day O and SAID- , the corresponding dose of the pre- vious day. BGS and BGD were, respectively, the presnack and predinner plasma glucose l e v e l d f the current and each previous day. S,, and Sgi were sensitivity factors.
Although a variety of linear or exponential weighting schemes could be implemented in the above general state- ments of these algorithms, in the present simulations the sensitivity factors were constant with Sli = S,, = S,, = S6( == 60 mg d1-I U-' , and S,, = S,, = 50 mg dl-' U-'. These were not specific to the individual simulated here. The prebreakfast and predinner insulin doses were accord- ingly adjusted during the simulations until the prevailing prenieal glucose levels were all essentially within the limits of 60 to 180 mg dl-', regardless of the metabolic control prevailing before starting dosage adjustments by this algo- rithm.
2.2 resting the algorithms T o demonstrate the eficacy of the algorithms, a triple
simulation study was performed, in which the simulator of human diabetes was configured to represent a specific insulin-dependent diabetic patient whose characteristics are detailed in Table 1. A life-like sequence of 150 consecu- tive days was simulated and replayed three times while each of the following three treatment scenarios was explored :
(a) conventional direct intervention by a diabetologist (b) daily dosage adjustment using Skyler's manual algo-
rithm (SKYLER et al., 1981)
I Medical .& Biological Engineering 8 Computing November 1986
(4 d d
To rr Io tn r e p a prese: varia: absor ance ment pel% held accor.
In visits. us (B urina: plasm. lunch. on t h ~ . in ins, until : proce?
In : initial There. intern: plasm. (1981)
In t: initial There:. dosage compu
400
300
ZOO
100
O 1 0
- 1-
E
3 20
O 4 0
3 20
O
Medica

Table 1 Characteristics oJa simulated insulin-dependeni diabetic parienr
Diet Composition Age, Height, Weight, C-peptide, Compliance kcal P/F/C',
Occupation years cm kg per a n t of normal factor per day g 80/100/150 N/A 19 177 65 5 3 1820
* Proteins/fats/carbohydrates, as recommended by the Canadian Diabetes Association. Carbohydrate was taken at break- fast (40 g at 07:30 h), at midmorning snack (25 g at 1O::OO h), at lunch (30 g at 12:30 h), at dinner (30 g at 18:OO h) and at bedtime snack (25 gat 21:30 h).
(c) daily dosage adjustment using the BCMC insulin dosage computer algorithms (SCHIFFRIN et al., 1985).
To make the comparisons between these three approaches to treatment relevant, the 150 day sequence was precisely repeated, a process which could only be done by the present computer simulations. In this way, the sequencc of variations in diet, meal absorption, insulin dosage, insulin absorption kinetics, activity, emotional stress and compli- ance were all exactly replayed. Only the method of treat- ment was different. In all three cases, the first 30 day period was repeated while the initial insulin dosages were held constant. Thereafter, insulin dosage adjustments were according to one of the treatment scenarios.
In the first treatment scenario, the 'patient' made 'oflice visits' every 30 days. He provided the diabetologist. one of us (BSL), with records of four times daily estimates of urinary giucose and Ketone levels, as well as lour premeal plasma glucose levels measured (before breakfast, before lunch, before dinner and before bedtime snack) only once on the day prior to the visit. Based on these data, changes in insulin dosage were prescribed and followed precisely until the next oflice visit 30 days later at which time the process was repeated.
In the second scenario, the same patient rollowed the initial íked insulin dosage schedule for the first 30 days. Thereafter he made daily adjustments to the regular and intermediate-acting insulins precisely in keeping with plasma glucose levels as recommended by SKYLER et al. (1981) and as detailed in Appendix 1.
In the third scenario, the same patient also followed the initial fixed insulin dosage schedule for the first 30 days. Thereafter, daily adjustments to the morning and evening dosages were recommended by the BCMC insulin dosage computer algorithm according to four plasma glucose
levels measured each day before the main meals and the bedtime snack. All the resulting data were accumulated in random access memory and then stored on Hexible mag- netic disks for later comparison and graphic presentation.
2.3 Analytical methods
Statistical methods included the F-test to compare the homogeneity of the variances and the appropriate unpaired t-test to compare the significance of differences in the means resulting from different treatments.
3 Results
3.1 Simulation studies As may be seen in Table 1, the simulated insulin-
dependent diabetic was of average body weight and height. His compliance was assigned to level 3.
For the first 30 days this simulated subject on conven- tional twice daily insulin treatment received 5 U of inter- mediate and 12 U of rapid-acting insulin 30 min before breakfast and 5 U of intermediate and 10 U of rapid- acting insulin 30 min before dinner [see Figs. 1-3 and Table 2). During this interval, the mean ( I SD) before lunch and before bedtime snack plasma glucose concentra- tions were, respectively, 138 I 3 5 and 145 f 35 mg dl-'. However, before breakfast and before dinner the mean SD plasma glucose levels were elevated to 250 _+ 23 and 254 & 21 mg dl-', respectively.
3.1.1 Conventional dire&teruention by a diabetologist. Following a 30-day assessment period during which time urinary glucose and ketones as well as fasting blood glucose levels were measured before each meal and
simulated patient history 6627.506 Fig. 1 Adjusting con- venrional insulin therapy aJter 30 days oJafixed dosage schedule, intervention by a diabetologist. Upper panel: plasma glucose levels measured beJore breakfast, lunch, dinner and bedtime snack
therapy by diabetologist
depot insulins 'O
at - -1 breakfast Jor I50 consecu- rice days MIddk and
2 1"
.^ O - lower oanels:
depot insulins *" II .̂ depot insulins injected at u< bieakfasr and at
dinner 3 20 dinner. Black
- acting insulin
aays actin4 insulin
- - bars are shorr-
O doses: grey bars are- inrermedioie-
- 15 O 15 30 15 60 75 90 I05 120 135 150 165
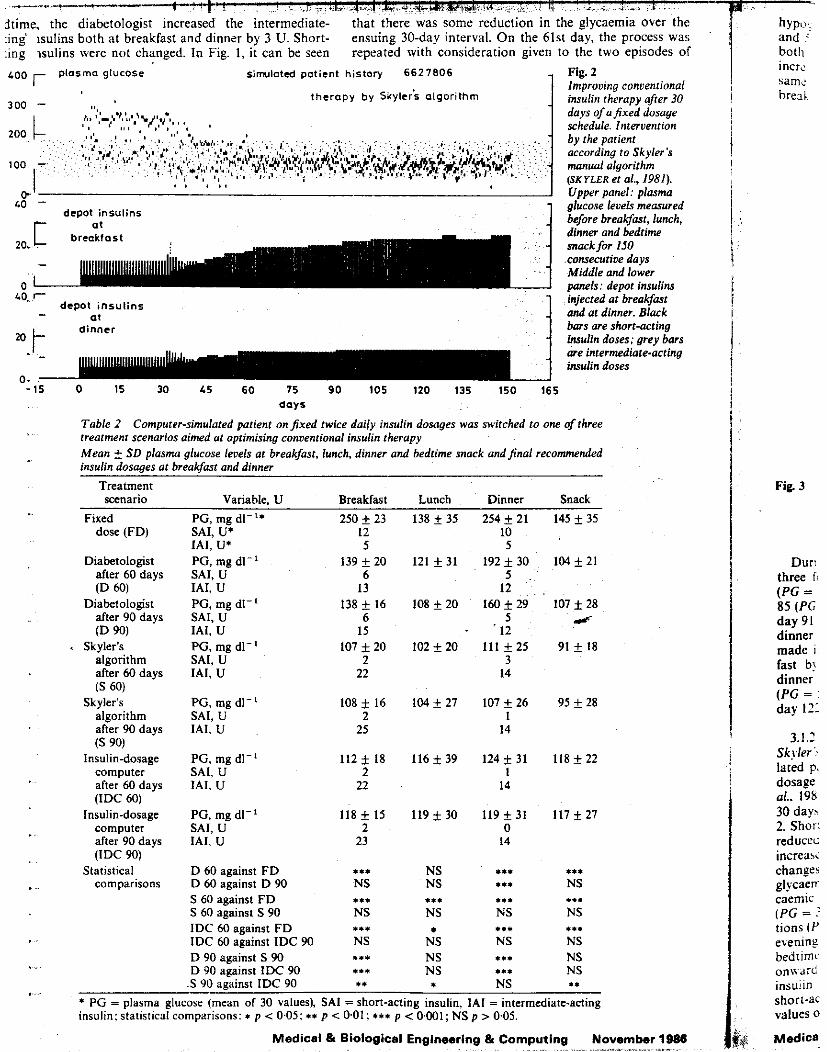
dtime, the diabetologist incr :ing isulins both at breakfast and dinner by 3 U. Short- :ing isulins were not changed. In Fig. 1 , it can be seen LOO plasma glucose simulated patient history 6627806 Fig. 2
ensuing 30-day interval. On the 61st day, the process was repeated with consideration given to the two episodes of
Improving conventional insulin therapy after 30 days of afixed dosage schedule. Intervention by the patient according to Skyler's manual algorithm (SK rLER et al., 1981). Upper panel: plasma
theropy by Ijkylcis algorithm
LO - glucose levels measured 3 before breakfast, lunch, depot insulins
2. Shor: reducei: increas changer glycaen caemic
tions I t ' eienine bedtime o n u d insulin short-ac values o
(PG = .'
&di Medical
40. r- depot insulins
at dinner
- injected a i breakfast and at dinner. Black bars are short-acting Insulin doses: arev bars
- 15
..
..
. ".
. , ,. ..
O 15 30 45 60 75 90 105 120 135 150 165 days
Table 2 Computer-simulated patient onfixed twice daily insulin dosages was switched to one ofthree treatment scenarios aimed at optimising conventional insulin therapy Mean f SD plasma glucose levels at breakJast, lunch, dinner and bedtime snack andfinal recommended insulin dosages at breakfast and dinner
Treatment ~ ~ ~ ~~ ~~~~~ ~~ ~
scenario Variable, U Breakfast Lunch Dinner Snack
Fixed PG, mg dl-" 250 f 23 138 f 35 254 f 21 145 f 35 dose (FD) SAI, U* 12 10
IAI, U* 5 5
~ ~ ~ ~~ ~~~~~ ~~ ~
scenario Variable, U Breakfast Lunch Dinner Snack
Fixed PG, mg dl-" 250 f 23 138 _+ 35 254 _+ 21 145 f 35 dose (FD)
Diabetologist PG. mz dl-' 139+20 121 +31 192+30 104+21 after 6Odays SAI, U- íD 60) IAI, U
Diabetologist PG, mg dl-' 138 f I6 108 + 20 160 I 2 9 107 f 28 after 90 days SAI, U 6 5 i íD 90) IAI. U 15 . '12
Skyler's PG, mg dl-' 107 f 20 102 f 20 111 f 25 91 f 18 algorithm SAI, U 2 3 after 60 days IAl, U 22 14 (S 60)
Skyler's PG, mg dl-' 108 f 16 104f 27 107f26 95 f 2 8 algorithm SAI, U 2 1
(S 90)
computer SAI, U 2 I
after 90 days IAI, U 25 14
Insulin-dosage PG, mg d1-l 112 f 18 116 f 39 I24 f 31 118 f 22
after 60 days IAI. U 22 14 (IDC 60)
Insulin-dosage PG, mg dl-' 118 f 15 119+ 30 119 f 31 I17 * 27 computer SAI, U 2 O after 90 days IAI, U 23 14 (IDC 90)
Statistical D 60 against F D *.* NS .*. *.* comparisons D 60 against D 90 NS NS .*I NS
S 60 against F D *I* til. .I* ... S 60 against S 90 NS NS NS NS IDC 60 against FD ..* *.* I..
IDC 60 against IDC 90 NS NS NS NS D 90 against S 90 *** NS **. NS D 90 against IDC 90 *.I NS .** NS
.S YO against IDC 90 *I * NS *I
* PG = plasma glucose (mean of 30 values), SA1 = short-acting insulin, IAI = intermediate-acting insulin; statistical comparisons: I p < 0.05; it p < 0.01; *** p < 0.001; NS p > 0.05.
Medical & Biological Engineering & Computing November 1988
i i
Fig. 3
Duri 1 three I (PG = 85 (PG day 91 dinner made I
fast b! dinner (PG = day 121
3.1 I
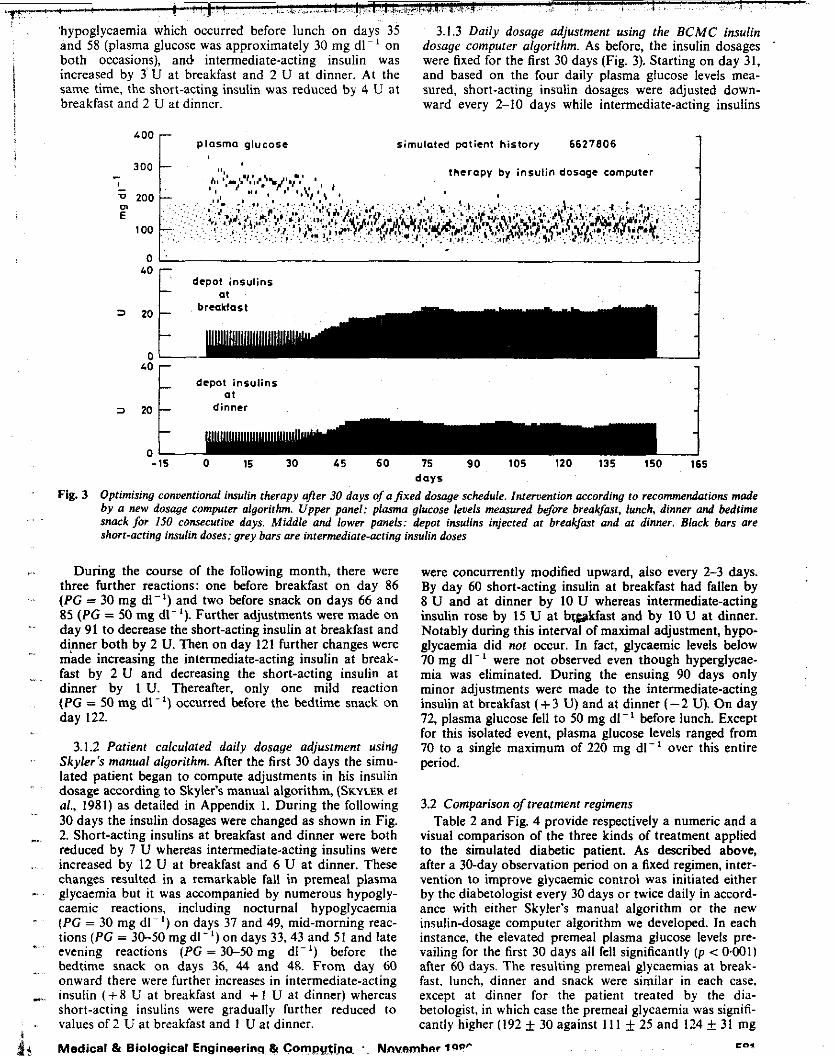
'hypoglycaemia which occurred before lunch on days 35 3.1.3 Daily dosage adjustment using the BCMC insulin and 58 (plasma glucose was approximately 30 mg d1-l on dosage computer algorithm. As before, the insulin dosages both occasions), and intermediate-acting insulin was were fixed for the first 30 days (Fig. 3). Starting on day 31, increased by 3'U at breakfast and 2 U at dinner. At the and based on the four daily plasma glucose levels mea- same time, the short-acting insulin was reduced by 4 U at sured, short-acting insulin dosages were adjusted down- breakfast and 2 U at dinner. ward every 2-10 days while intermediate-acting insulins
¡ j
'Oo r plasma glucose simulated patient history 6627806 1 therapy by insulin dosoqe computer 300
L
0 zoo E
1 O0
' . O '
depot insulins
depot insulins '0E dinner a t
3 20
-15 O I5 30 45 60 75 90 105 120 135 150 165 days
Optimising conventional insulin therapy a/ter 30 days of afired dosage schedule. Intervention according to recommendations made by a new dosage computer algorithm. Upper panel: plasma glucose levels measured before breakfast, lunch, dinner and bedtime snack for IS0 consecutive days. Middle and lower panels: depot insulins injected at breakfast and at dinner. Black bars are short-acting insulin doses; grey bars are intermediate-aciing insulin doses
Fig. 3
. ,
During the course of the following month, there were three further reactions: one before breakfast on day 86 ( P C = 30 mg dl-') and two before snack on days 66 and 85 (PG = 50 mg d1-l). Further adjustments were made on day 91 to decrease the short-acting insulin at breakfast and di.nner both by 2 U. Then on day 121 further changes were made increasing the intermediate-acting insulin at break- fast by 2 U and decreasing the short-acting insulin at dinner by 1 U. Thereafter, only one mild reaction ( P C = 50 mg dl-') occurred before the bedtime snack on day 122.
3.1.2 Patient calculated daily dosage adjustment using Skyler's manual algorithm. After the first 30 days the simu- lated patient began to compute adjustments in his insulin dosage according to Skyler's manual algorithm, (SKYLER et al., 1981) as detailed in Appendix I. During the following 30 days the insulin dosages were changed as shown in Fig. 2. Short-acting insulins at breakfast and dinner were both reduced by 7 U whereas intermediate-acting insulins were increased by 12 U at breakfast and 6 U at dinner. These changes resulted in a remarkable fall in premeal plasma glycaemia but it was accompanied by numerous hypogly- caemic reactions. including nocturnal hypoglycaemia ( P G = 30 mg d1-l) on days 37 and 49, mid-morning reac- tions ( P G = 30-50 mg dl-') on days 33,43 and 51 and late evening reactions (PG = 30-50 mg dl- I ) before the bedtime snack on days 36, 44 and 48. From day (io onward there were further increases in intermediate-acting insulin ( + 8 U at breakfast and + I U at dinner) whereas short-acting insulins were gradually further reduced to values of 2 U at breakfast and 1 U at dinner.
Medical t3 Biological Engineerinq t3 Compy~ins. ' Nnvnr
were concurrently modified upward, also every 2-3 days. By day 60 short-acting insulin at breakfast had fallen by 8 U and at dinner by 10 U whereas intermediate-acting insulin rose by 15 U at brgakfast and by 10 U at dinner. Notably during this interval of maximal adjustment, hypo- glycaemia did not occur. In fact, glycaemic levels below 70 mg dl-' were not observed even though hyperglycae- mia was eliminated. During the ensuing 90 days only minor adjustments were made to the intermediate-acting insulin at breakfast ( + 3 U) and at dinner (-2 U). On day 72, plasma glucose fell to 50 mg dl-' before lunch. Except for this isolated event, plasma glucose levels ranged from 70 to a single maximum of 220 mg dl- ' over this entire period.
3.2 Comparison of treatment regimens Table 2 and Fig. 4 provide respectively a numeric and a
visual comparison of the three kinds of treatment applied to the simulated diabetic patient. As described above, after a 30-day observation period on a fixed regimen, inter- vention to improve glycaemic control was initiated either by the diabetologist every 30 days or twice daily in accord- ance with either Skyler's manual algorithm or the new insulin-dosage computer algorithm we developed. In each instance, the elevated premeal plasma glucose levels pre- vailing for the first 30 days all fell significantly ( p < 0401) after 60 days. The resulting premeal glycaemias at break- fast, lunch, dinner and snack were similar in each case, except at dinner for the patient treated by the dia- betologist, in which case the premeal glycaemia was signifi- cantly higher (192 _+ 30 against 11 1 f 25 and 124 f 31 mg
COI nhnr *QV
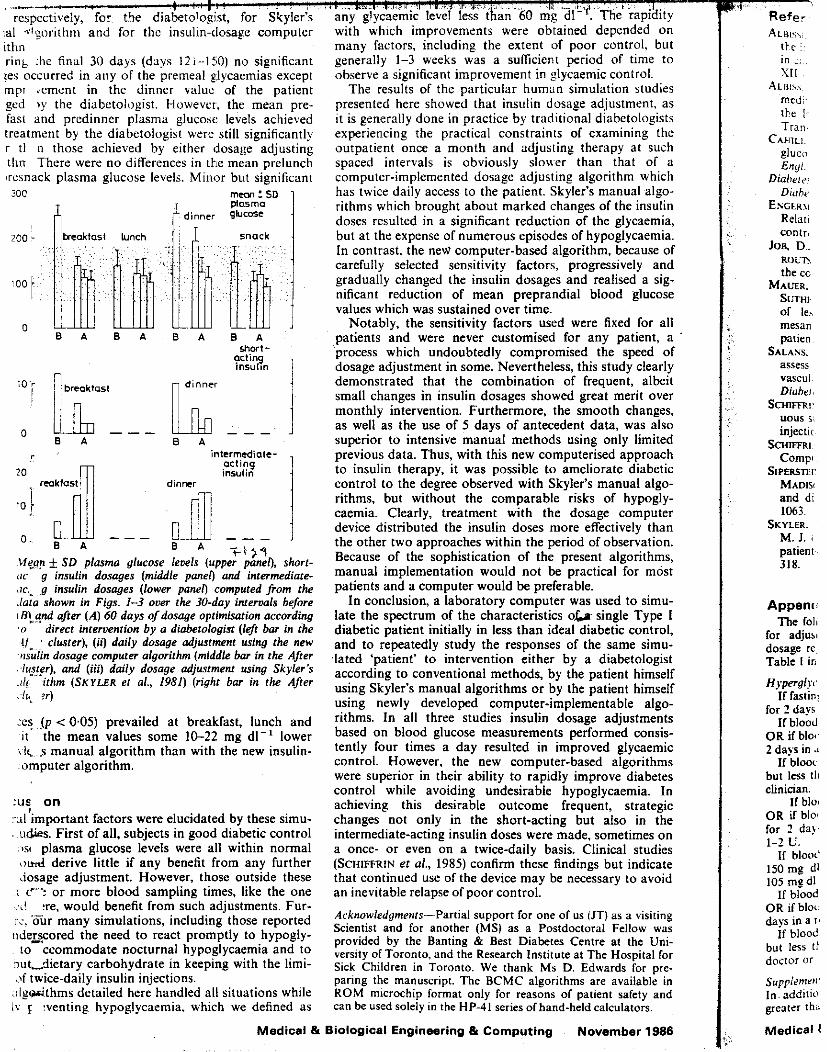
ial ,t"Sorithni and for thc insulin-dosage computer ithn ring :he find 30 days (days I2i--l?iO] no significant ?es occurred in any of the premeal glycaimias except mpi dement in the dinner valui of the patient ged >y the diabetolugist. However, the mean pre- fast and predinner plasma ~ I U C O S C : levels achieved treatment by the diabetologist were still significantly r t l n those achieved by either dosage adjusting tlin There were no differences in the mean prelunch wsnack plasma glucose levels. Minor but significant 3oc rn- : 5D
plosma x r dinncr gbCOSC I
" E A B A B A B A
:o r I
O
20
10 1 O
f i > l
i4q.gn f SD plasma glucose levels (upper panel), short- (IC , g insulin dosages (middle pane0 and intermediate- iic.. ,.g insulin dosages (lower pane0 computed from the ./ata shown in Figs. 1-3 over the 30-day interuals before I B!,Snd after ( A ) 60 days of dosage optimisation according 'o direct intervention by a diabetologist (left bar in the I/-.: cluster), (ii) daily dosage adjustment using the new iisulin dosage computer algorithm (middle bar in the After .Iiwgr), and (iii) daily dosage adjustment using Skyler 5
.ilg ithm (SKYLER et al., 1981) (right bar in the After ~li,, ?r)
' e s .(p < 0.05) prevailed at breakfast, lunch and it the mean values some 10-22 mg dl-' lower !I<, s manual algorithm than with the new insulin- omputer algorithm.
:u$ on XI important factors were elucidated by these simu- , udigs. First of all, subjects in good diabetic control
. ,SI plasma glucose levels were all within normal o d derive little if any benefit from any further dosage adjustment. However, those outside these : f-'? or more blood sampling times, like the one
,..L! :re, would benefit from such adjustments. Fur- i:. our many simulations, including those reported iidezcored the need to react promptly to hypogly-
to ccommodate nocturnal hypoglycaemia and to niit,.dietary carbohydrate in keeping with the limi- i)f twice-daily insulin injections.
.iIg&.thms detailed here handled all situations while I! r :venting hypoglycaemia, which we defined as
!
. _ . with which improvements were obtained depended on many factors, including the extent of poor control, but generall:y 1-3 weeks was a suificient period of time to observe a significant improvement in glycaemic control.
The results of the particular human simulation studies presented here showed that insulin dosage adjustment, as it is generally done in practice by traditional diabetologists experiencing the practical constraints of examining the outpatient once a month and adjusting therapy at such spaced intervals is obviously slower than that of a computer-implemented dosage adjusting algorithm which has twice daily access to the patient. Skyler's manual algo- rithms which brought about marked changes of the insulin doses resulted in a significant reduction of the glycaemia, but at the expense of numerous episodes of hypoglycaemia. in contrast, the nevi computer-based algorithm, because of carefully selected sensitivity factors, progressively and gradually changed the insulin dosages and realised a sig- nificant reduction of mean preprandial blood glucose values which was sustained over time.
Notably, the sensitivity factors used were fixed for all patients and were never customised for any patient, a process which undoubtedly compromised the speed of dosage adjustment in some. Nevertheless, this study clearly demonstrated that the combination of frequent, albeit small changes in insulin dosages showed great merit over monthly intervention. Furthermore, the smooth changes, as well as the use of 5 days of antecedent data, was also superior to intensive manual methods using only limited previous data. Thus, with this new computerised approach to insuliin therapy, it was possible to ameliorate diabetic control to the degree observed with Skyler's manual algo- rithms, but without the comparable risks of hypogly- caemia. Clearly, treatment with the dosage computer device distributed the insulin doses more effectively than the other two approaches within the period of observation. Because of the sophistication of the present algorithms, manual implementation would not be practical for most patients and a computer would be preferable.
In conclusion, a laboratory computer was used to simu- late the spectrum of the characteristics o b - single Type I diabetic patient initially in less than ideal diabetic control, and to repeatedly study the responses of the same simu- .laled 'patient' to intervention either by a diabetologist according to conventional methods, by the patient himself using Skyler's manual algorithms or by the patient himself using newly developed computer-implementable algo- rithms. In all three studies insulin dosage adjustments based on blood glucose measurements performed consis- tently four times a day resulted in improved glycaemic control. However, the new computer-based algorithms were superior in their ability to rapidly improve diabetes control while avoiding undesirable hypoglycaemia. In achieving this desirable outcome frequent, strategic changes not only in the short-acting but also in the intermediate-acting insulin doses were made, sometimes on a once- or even on a twice-daily basis. Clinical studies (SCHIFFRIN et al., 1985) confirm these findings but indicate that continued use of the device may be necessary to avoid an inevitable relapse of poor control.
Acknowledgmenrs-Partial support for one of us (JT) as a visiting Scientist and for another (MS) as a Postdoctoral Fellow was provided by the Banting & Best Diabetes Centre at the Uni- versity of Toronto, and the Research institute at The Hospital for Sick Children in Toronto. We thank Ms D. Edwards for pre- paring the manuscript. The BCMC algorithms are available in ROM microchip format only for reasons of patient safety and can be used solely in the HP-41 series ofhand-held calculators.
Medical & Biological Engineering 8 Computing November 1988
Refer ALIW,,
ttr : ' i n ::. SI1
A L R I ~ ~ medi thc I Trail.
CAHILI. gluco Enyl.
Diahrar: Diuht,
Esmw Relati contri
JOB, D..
the cc MALTR.
SUTHI~ oí le5 mesan patien
SALANS. assess vascui Diuhri
SCwiFfRl.
injectit SCHlFFRl
Compt SiPERsTEi.
MADisr and di 1063.
M. I. , patient 318.
RWlTS
uous si
SKYLER.
Appenu The foli
lor adjus, dosage re. Table I in
If lastini lor 2 days
If blood OR if blo* 2 days in
If blooi but less 111 clinician.
If bioi OR if h l o for 2 da). 1-2 L'.
If blooi' 150mg dl 105 medl
If blood OR if bloc days in a I '
If blood but less 11 doctor or
Supplrrnrii' In. addiiio greirsr tha
Medical I
HyperglR

References ALBISSER, A. M., PERLMAN, K. and SCHULZ, M. (1985) Titrating
the insulin dose by computer: the effects of measurement el-rors in capillary blood glucose estimation. Abstract presented at the XI1 Cong. 01 the IDF, Madrid, Spain, 23rd-28th Sept. 1985.
ALBISSER, A. M. and SCHULZ, M. (1986) Simulating human inter- mediary metabolism: OMNI et al. Proc. Clin. Biocbem. Nearer the Patient I1 Conl.. University of Surrey, Guildford, Surrey, Transmedia Europe Ltd., (in préss).
CAHILL F. G., ETZWILER, D. D. and FREINKEL, N. (1976) Blood glucose control in diabetes. Diabetes, 1976, 25, 237-238, and N . End. Med., 1976. 294, loob1005.
Diobites Core (1980) Symposium on home glucose monitoring.
ENCERMANN. R.. BLOODWORTH. I. M. B. and NELSON. S. (1977) Diabetes Care, 3, 57-139.
. . . ~~ ~
Relationship o1 microvascular disease in diabetes to metabolic control. Diabetes, 26, 7 6 7 6 9 .
JOB, D., ESCHWEG& E., GUYOT, C., AUBRY, J. P. and TCHOB- ROUTSKY, G. (1976) Effect of multiple daily insulin injections On the course of diabetic retinopathy. Ibid., 2 5 , 4 6 3 4 6 9 .
MAUER, S. M., S- M. W., CONNETI, J., NAIARIAN, .I. S., SUTHERLAND, E. R. and BARBOS*, J. J. (1983) The development of lesions in the glomerular basement membrane and mesangium after transplantation 01 normal kidneys to diabetic patients. Ibid., 32, 948-952.
SALANS, L. B. (1983) Proposed protocol for the clinical trial to assess the relationship between metabolic control and the early vascular complications of Type 1 (insulindependent) diabetes. Diabetologia, 24,216.
SCHIFFRIN, A. and BELMONTE, M. M. (1981) Combined contin- uous subcutaneous insulin infusion and multiple subcutaneous injections in type I diabetic patients. Diabetes Care, 4, 595-600.
SCHIFFRIN, A., MIHIC, M., LEIBEL, B. S., ALBISSER, A. M. (1985) Computer assisted insulin dosage adjustment. Ibid., 8,545-552.
SIPERSTEIN, M. D., FOSTER, D. W., KNOWIES, H. C., LEYINF, R., MADISON, L. L. and Row, J. (1977) Control of blood glucose and diabetic vascular disease. N . Engl. J. Med., 296, 1ü6& 1063.
SKYLER, I. S., SKYLER, D. L., SEICLER, D. E. and OSULUVAN, M . J. (1981) Algorithms for adjustment of insulin dosage by patients wbo monitor blood glucose. Diabetes Care, 4, 311- 318.
Appendix 1 The following is a verbatim statement of Skyler's algorithms
for adjusting insulin doses using a 'split-and-mixed' insulin dosage regimen and patient monitoring of blood glucose (from Table 1 in S c " et al., 1985).
Hyperglycaemia not explained by unusual dietíexerciseíinsulin I1 lasting blood glucose on arising is greater than 130 mg dl- '
for 2 days in a row, increase your evening NPH insulin by 1-2 U. I1 blood glucose 2 h alter breaklast is greater than 150 mg d1-l
O R if blood glucose before lunch is greater than 130 mg dl- ' lor 2 days in a row. increase your morning regular insulin by 1-2 U.
I f blood sugar 2 h after breakfast is greater than 150 mg dl- ' , but less than 105 mg dl- ' before lunch, consult your doctor or clinician.
I1 blood glucose 2 h after lunch is greater than 150 mg d1-I. O R il blood glucose before supper is greater than 130 mg dl- ' for 2 days in a row, increase your morning NPH insulin by 1-2 u.
I1 blood glucose 2 h after lunch is consistently greater than 150 mg dl- ' AND blood glucose before supper is less than I05 mg dl- ' , consult your doctor or clinician.
If blood glucose 2 h after supper is greater than 150 mg dl-', O R if blood glucose at bedtime is greater than 130 mg dl- ' for 2 days in a row, increase your evening regular insulin by 1-2 U.
I1 blood glucose 2 h alter supper is greater than 150 mg dl- ' , but less than 105 mg dl- ' belore bedtime snack, consult your doctor or clinician.
Supplements In addition, il blood glucose on arising O R before supper is greater than 140 mg d1-l. take an extra 1-2 U of regular insulin
as a supplement at that time. If blood glucose on arising OR before supper is greater than 200 mg dl- ' , take an extra 2-4 U o1 regular insulin as a supplement at that time. Record the supple- ment in the supplement column so that you do not accidentally change the basal dose of regular insulin.
Hypogljcaernia not expkiinud by unusual dietíexercisejiiisulin Prevent insulin reactions by eating meals and snacks on time. I1 fasting blood glucose on arising is less than 60 mg dl-'. OR
i l there is evidence o f hypoglycaemic reactions occurring over- night, reduce your evening NPH insulin by 1-2 U.
If blood glucose alter breakfast O R before lunch is less than 60 mg dl-', O R if you have a hypoglycaemic reaction between breakfast and lunch, reduce your morning regular insulin by 1-2 u.
If blood glucose after lunch OR before supper is less than 60 mg dl-', OR if you have a hypoglycaemic reaction between lunch and supper, reduce your morning NPH insulin by 1-2 U.
I1 blood glucose after supper O R at bedtime is less than 60 mg dl-', OR if you have a hypoglycaemic reaction between supper and bedtime, reducc your evening regular insulin by 1-2 U.
Appendix 2 Omni is a computer. The computer simulates a presenting indi-
vidual who may be healthy or ill. Vital characteristics of this individual can be redefined by the user either in part or entirely. Those characteristics not assigned by the user are generated by the computer.
The choice in defining an individual is made lrom a population of over IO" different individuals. Interestingly, this represents a population which includes all human beings that have ever existed, and many, many more: hence, Omni . . . et al.!
The unique feature of the computer-simulated individual is that hershe may be ill. For example, he/she may suffer from any one or more of a multitude of disorders characteristic of human epidemiology. Among these, there are metabolic and hormonal diseases, such as Type I or Type I1 diabetes. In all cases, the user can intervene in the care of this 'patient' and define treatment in the lorm of diet, insulin, activity level, compliance etc. Since a day in the lile of Omni lasts only 3 min, the user can rapidly experi- ence the effects of prescribed treatment regimes. The user can also experience the responses of many such patients, each entirely different, but all in a short period oftime.
Omni et al. is rendered realistic by the extensive utilisation 01 stochasm in all metabolic processes, including emotions, diet, exercise, lood absorption, iKulin absorption kinetics, receptor effects, key enzyme activities, and so on.
The user can observe graphically the minute-by-minute trajec- tories of almost any group o1 intermediates of not only carbo- hydrate but also of protein arid lat metabolism. O f course, the main hormones o f metabolic regulation and stress are also acces- sible for study. For example, with improper treatment a Type I diabetic individual simulated by Omni may develop ketoacidosis. convulse or gradually lose weight and even die.
The database for Omni et al. includes the pertinent results from well over 200 publications in the scientific literature.
Authors' biographies
. .
Michael Albisser was born in Johannesburg Union o f South Africa, on the 5th September 1941. He received a B.Eng. degree in Electrical Engineering from McGill University, Mon- treal, Canada in 1964 and the M.A.Sc. degree in Electrical Engineering and the Ph.D. degree in Biomedical Engineering from the University 01 Toronto, in 1966 and 1968, respectively. He is currently a Senior scientist at the depart-
ment of Surgery and Director of the Division of Biomedical Research at The Hospital for Sick Children. Toronto and an Associate Prolessor in the Departments of Medicine. Surgery and Electrical Engineering. University of Toronto. His interests are in the development of biomedical instruments, devices and tech- niques including portable drug delivery systems, and micro- processor devices for the adjustment and optimisation of drug dosage.
M e d i c a l & B i o l o g i c a l Engineer ing & C o m p u t i n g N o v e m b e r 1986 583

'Alicia Schiffrin was born in 1947 and grad- uated with an M.D. in Medicine from the Uni- versity of Buenos Aires in 1971. Since then she has held hospitai posts in Buenos Aires and latterly in Montreal where she was appointed lecturer in 1979. Since 1981 she has been Assistant Professor in the Department of Pae- diatrics of McGill University and has recently been appointed Chief of Diabetes Service. A
list i' :ndocrinology, Dr. Schrillin is active in many learned es, i luding the Canadian and American Diabetes Associ-
Miklos Schulz was born on the 6th May 1951 in Nyiregyhaza, Hungary and received a B.Sc. in Chemical Engineering i n 1973, an M.S. in progress Control Engineering in 1975 and a Ph.D. in 1982 from the University of Vesz- prem. He spent 198&1981 in overseas post- graduate training at The Hospital for Sick Children, Toronto, Canada and is now a per- manent Research Engineer there working on
the development of devices such as the insulin-dosage computer and metabolic simulator.
Bernard S. Leibel studied at the University of Toronto, receiving the B.A., M.A., BSc. and M.D., and in London in 1939-1940, receiving the M.R.C.S. and F.R.C.P. He had 5 years postgraduate training at Guy's Hospital, London. He is a consultant at The Hospital for Sick Children, Toronto, Senior Attending
:, Physician at Mount Sinai Hospital and Associate Professor at the Faculty of Medi-
cine, University of Toronto. In addition he is on the NDRl steer- ing committee at Philadelphia USA, a member of the International Medical Advisory Board of the Juvenile Diabetes Foundation International and on the executive of the Banting & Best Diabetes Centre, Toronto.
Medical O Biological Engineering & Computing November 1986 ., , ~,.. - ~ " ,,... ,.. _._..,..^.,_____l<._l I<___ . . . ~
1 lntro TKE TER ous indi extreme. measurc. of the micropic
The 8:
proposs- BROWS method techniq:: by this I
The !I
arterial pressurt: useful a haemod and PO. and SO' absorpt' can be c' - Fisf m e '
@ IFMBF
Medica

Pancreas Transplantation: Curative Therapeutic Approach to Diabetic Microangiopathy?
D. Abendroth. W-D. lllner, R. Landgraf. and W. Land
HERE IS no doubt that renal transplan- T . tation oñers the optimal treatment for the benefit of pancreas transplanta-
tion must still be proven. The hypothesis that ,,,icrovascular complications of diabetes are partly due to quality of blood glucose control was suggested soon after the introduction of
Patient survival following pancreas trans- plantation has shown a significant improve-
.. ment (40% i n 1977 to 100% in 1986) and the ,' I-year graft survival rate has reached more
than 70% by most experienced groups.' This is indicating that pancreas transplan-
tation is becoming progressively safer and more successful. These results enable us now to evaluate the benefits. especially concerning late diabetic complications. W e want to pre- sent the results of metabolic, opthalmologic, and microcirculatory long-term follow-up data of type I diabetics successfully trans- planted using the method of segmental duct occluded pancreas combined with kidney grafting.
MATERIAL AND METHODS The patient survival rate (n ~ 57) 0184% increased to
100% in a subgroup during the last 33 months. I n this rubgroup since Scptemtw 1987 (n - 26) under a new operative and immunologic management (anticoagula- tion with low-dose heparin and dextran 40; intraperito- neal graft placement together with continuous irrigation: quadruple-drug induction treatment) the )-year graft- survival increased to 74'í .
For registration and quantification of microcirculatory changes alter pancreas and kidney iransplantaiion. we inirduccd a combination of trans~~tane~us oxygen len- sion meawremtnt (tcp0,l and telethermography. as recently published.'.' Both methods are able to detect changes of nutritional flaw, reoxygenation potential after total blwd flow wclusion. and subtle temperature diñer- e m s in sense or micrwirculatory disorder as a timc- dependent spotty underperfusion.
RESULTS
h4etabolic All our patients with functioning graíts
(n = 25) are free of insulin. Fasting blood glucose levels (89 2 3 mg/dL) and HbA, values (7.0 I 0.2%) are in a normal range. Oral glucose tolerance with IO0 g glucose is normal in 65% and impaired in 35%.
Neuropathy Peripheral neuropathy shows a significant
improvement. Subjective signs like hyperaes- thesia, crampi, etc, disappeared in 14 of 16 observed patients within the first 3 to 6 inonths. Peroneal, sural, and median nerve conduction velocities inc-ased significantly (P < .05).
Retinopar hy Visual acuity improved in 56%. stabilized
in 32%. and deterioriated in 12% (n = 4, two patients developed a cataract). The prolifera- tive retinopathy increased only two eyes of all patients.
~
Peripheral Microcirculation Diabetic microangiopathy shows a normal-
ization, strictly correlated to normoglycemia.
From the Division OJ Tronsplontoiion Surgcry. Klirii- kum Grosrhodun. ondthc DepwImmi o/lnlernol Medi- cine "lnnenstodr. '' Univerriry o/ Munich.
Addrerr repprim requests lo DI D. Abrndrorh. Division of Transplmioiion Surgery. Klinikum Grorshodcrn. Morchioninirir /S, 8000 München 70. FRG. O 1988 by Giune di Slrolton. In?. 0041 -I 345l88l2lN34041 S03.OOlO
Tranrplanmfim Proceedings. Vol XX. No 3 IJunel. 1988: pp 469-410 469 I
Tcp0,values rise from 44 t 2 mm Hg to 64 t 5 mmHg (Wilcoxon, P < .Ol), indicating an increase of dermal nutrition, decreased from 203 I I O seconds (normal levels), showing the benefit on thermoregulatory shunt flow behavior. these complications.
CONCLUSION There is accumulating evidence suggesting
that successful pancreatic transplantation can improve severe late complications. Grafting in an earlier stage of the disease might prevent
REFERENCES
1. Waiie JH. Betham W : N Engl J Mcd 212367.
2. McMillan D E Diabelcs. 24:944. 1975 3. Sutherland DER: Transplanl P r w 18:1739. 1986
4. Sunder-Plaismann L, Mcssmcr K. Bccker H ~ :
5. Abcndrath D. lllner W-D. Landgraf R , e t a l : ~ ~ ~ ~ 1935 Angiology 32686. 1981
plant Prw. 192325. 1987
Pancreatic
G. Tyi
LTHOUGH A renal and p: uremic diabetics I in recent years,’ t complications ha\ ing.” It seems i h the secondary c
’ advanced to be ha ,i 1 recipient criteria : institution and I
recently been acc plantation alone.
Fig 1 . Technique with splenic arterial bi
artery and the distal e mosed to the external
rp1einic .rt.ry is anam