01 growth and development
DESCRIPTION
PREPTRANSCRIPT

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 1/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 1
Item 13A 4-year-old girl presents to your office for a health super-vision visit. Her parents arevery worried about the appearance of her ankles. When she is sitting, the feet and anklesappear normal. However, when she walks, the parents observe that her ankles protrudeinward and she seems to have "very flat feet" The child does not report any pain and has
not had difficulty keeping up with her peers at play. The appearance of the girl's feet andankles when standing on her toes is shown (Item Q13). The remainder of the examinationis normal.
ITEM Q13: Feet as descri bed for the gir l in the vignette.
Of the following, the MOST appropriate management is
A. physical therapy for ankle strengtheningB.
reassure the family regarding the physical findingsC.
refer the girl to orthopedic surgery for possible surgical correctionD.
use of rigid 3/ length custom shoe insertsE. use of soft, full-length custom shoe inserts
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 2/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 2
Item 13 Preferred Response: BPhysiologic flat foot, also referred to as flexible flat foot or pes planus, is present inapproximately 45% of preschool-age children. The child described in the vignette hasasymptomatic physiologic flat foot and does not require any treatment. With physiologicflat foot, the arch seems to disappear when the child stands and becomes visible when the
child goes up on his or her toes. Often, the heels deviate outward with standing ("hindfootvalgus") and the ankles appear to protrude medially. For most children, the arch developsspontaneously with growth. Braces, shoes, or shoe inserts have not been shown tofacilitate arch development. As children get older, the fatty tissue over the archdisappears and the ligaments of the foot and ankle become less lax, making the arch moreeasily visible.
In about 1 in 7 people, the arch never develops. Factors that increase the likelihood ofhaving persistent flat foot include obesity, ligamentous laxity, tight calf muscles, and apositive family history. The majority of children and adults with flexible flat foot areasymptomatic.
Children with flexible flat foot generally come to medical attention owing to parents'concerns about the appearance of the foot. Custom shoe inserts are not indicated forasymptomatic or minimally symptomatic patients; inserts are costly and may makechildren less comfortable. For children and teenagers reporting activity-related foot pain,shoe inserts may help alleviate symptoms; however, arch supports do not mold or alterthe shape of the foot. Active children and teenagers often find very rigid insertsuncomfortable; soft, full-length inserts generally are tolerated better. Physical therapy forankle strengthening may be helpful for children with ankle hypermobility and pain orwith symptomatic flat foot associated with poor flexibility; however, physical therapy isnot indicated for children with asymptomatic flat foot.
With pathologic, or rigid, flat foot, the ankles tend to be stiff and standing on one's toesdoes not make the arches visible. Individuals with rigid flat feet are more likely tobecome symptomatic and may require surgical treatment if pain does not resolve with aconservative approach. Tarsal coalition, an abnormal fusion between two of the tarsalbones, is one cause of rigid flat feet. Children with tarsal coalition typically presentbetween the ages of 9 and 13 years with recurrent ankle sprains and activity-related footpain.
PREP Pearls• Flexible flat foot is associated with hindfoot valgus (often referred to as ankle
pronation).•
Asymptomatic flexible flat foot is very common and does not requiretreatment.
• Accommodative shoe inserts ("orthotics") may help alleviate symptoms inchildren with flexible flat foot but will not change the structure of the foot.
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 3/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 3
American Board of Pediatrics Content Specifications:• Know that no treatment for piano valgus is required in childhood• Know that a longitudinal arch support may be helpful if piano valgus is
painful for adolescents
Suggested Reading:
Evans AM, Rome K. A Cochrane review of the evidence for nonsurgicalinterventions for flexible pediatric flat feet. Eur I Phys Rehabil Med.2011;47(1):69-89
Pfeiffer M, Kotz R, Ledl T, Hauser G, Sluga M. Prevalence of flat foot inpreschool-aged children. Pediatrics. 2006;118(2):634-639. doi:10.1542/peds.2005-2126
Rao UB, Joseph B. The influence of footwear on the prevalence of flat foot: asurvey of 2,300 children. J Bone Joint Surg Br. 1992;74(4):525-527
D r _F a q e
7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 4/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 4
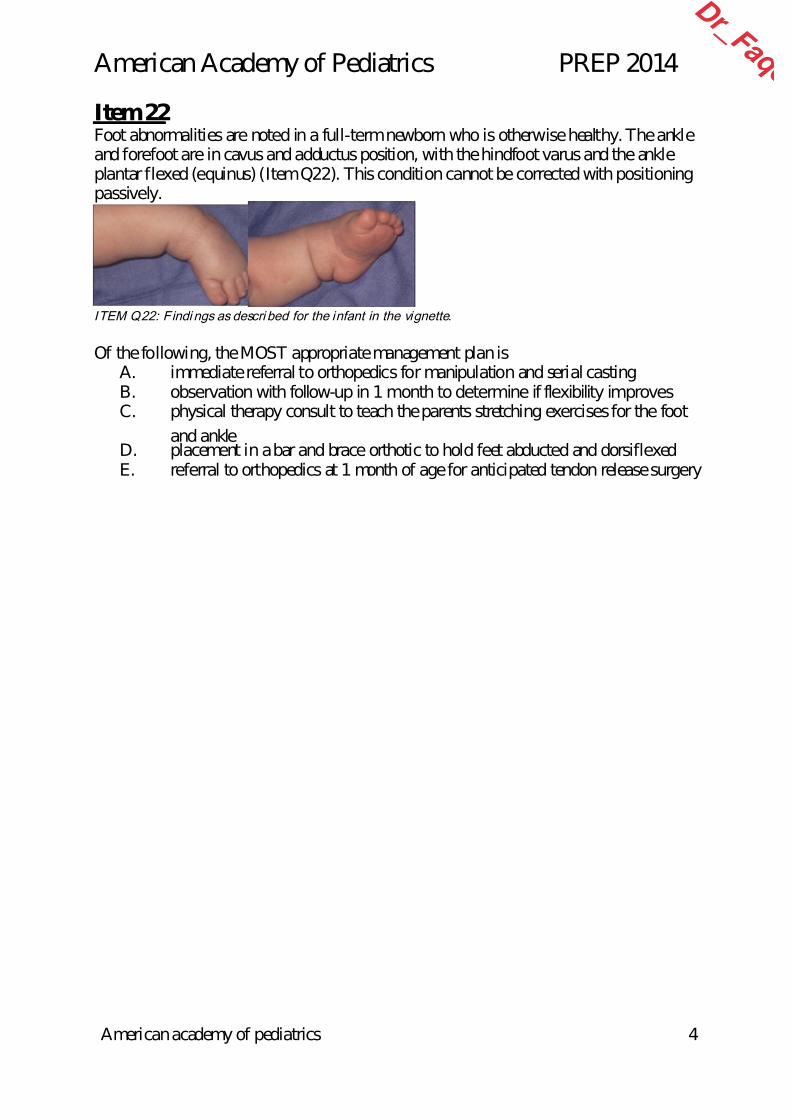
Item 22Foot abnormalities are noted in a full-term newborn who is otherwise healthy. The ankleand forefoot are in cavus and adductus position, with the hindfoot varus and the ankleplantar flexed (equinus) (Item Q22). This condition cannot be corrected with positioningpassively.
ITEM Q22: Findi ngs as descri bed for the infant in the vignette.
Of the following, the MOST appropriate management plan isA.
immediate referral to orthopedics for manipulation and serial castingB.
observation with follow-up in 1 month to determine if flexibility improvesC. physical therapy consult to teach the parents stretching exercises for the foot
and ankleD.
placement in a bar and brace orthotic to hold feet abducted and dorsiflexedE. referral to orthopedics at 1 month of age for anticipated tendon release surgery
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 5/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 5
Item 22 TE I-C Preferred Answer: A The infant described in the vignette has the classic features of talipes equinovarus(clubfoot) and it is recommended that treatment begin immediately after birth. Clubfootor talipes equinovarus is a common congenital deformity affecting approximately 1 per1,000 live births. Boys are affected twice as often as girls, and in half the cases the
deformity is bilateral. A family history of clubfoot increases the risk of subsequentaffected infants, but the inheritance pattern is uncertain. Eighty percent of the deformitiesare isolated whereas 20% are associated with other conditions, including spina bifida,cerebral palsy, and arthrogryposis.
Although talipes equinovarus involves the entire foot, talar anomalies appear to be themajor underlying deformities. On physical examination, the hindfoot is in varus (the heelturning in) and equinus (the foot points downward at the ankle). The forefoot and midfootare adducted whereas the first metatarsal ray is plantar flexed; together this produces thecavus appearance characteristic of the distal foot.
The Ponseti method of weekly manipulation and casting is the most widely usedtreatment in North America. First developed in the 1940s, it involves a specific sequenceof manipulations and stretching of immature collagen into a maximal correction that isthen held in position with a cast. After 6 or more weeks of sequential manipulation andcasting, the midfoot and forefoot are usually corrected. Persistent equinus deformity often(85%) requires Achilles tenotomy, which may be done in the orthopedist's office. This isfollowed by 3 weeks in a final cast. If correction is adequate, the patient is then placed ina "boots and bar" orthotic device that holds the feet externally rotated and dorsiflexed.
For the initial 3 months, the orthosis is used continuously. After 3 months, it is used onlyduring sleep until age 3 to 4 years. Occasionally the deformity may recur, andmanipulation and casting with or without tibialis anterior tendon transfer may bereinstituted. Although some reports indicate that delayed initiation of the Ponseti methodmay still be successful, immediate treatment is still the recommended approach.
Alternatives approaches include early surgical treatment and the French physiotherapymethod. Studies directly com-paring the Ponseti method to early surgery are limited, butoutcomes with surgical management appear to be worse than with the Ponseti method. The French physiotherapy method is very resource intensive, requiring daily treatmentsby a therapist or physician. 'Outcomes are similar to those with the Ponseti method exceptfor the most severely affected children in whom the Ponseti method produces betterresults. More extensive surgical procedures may also be required to achieve the best long-term result after initial treatment with the French method. In a child with a fixeddeformity, passive stretching by the parents at home is unlikely to result in improvement. The brace and bar orthotic, as described above, is used after rather
D r _F a q e
7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 6/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 6
PREP Pearls
Talipes equinovarus is characterized by fixed in-turning of the hindfoot,plantar flexion at the ankle, and cavus appearance of the distal foot (adductionof the fore- and midfoot with first metatarsal ray plantar flexion).
In cases of clubfoot, the Ponseti method of serial manipulation and casting
should be initiated as soon after birth as possible.
Outcomes for serial manipulation and casting appear to be better than those ofa strictly surgical approach.
American Board of Pediatrics Content Specification(s):
Recognize that the treatment for talipes equinovarus is casting or splinting ofthe affected foot
Know that the most common component of clubfoot is equinovarus deformity
Be aware that early treatment of clubfoot is critical
Suggested Reading:
Bridgens J, Kiely N. Current management of clubfoot (congenital talipesequinovarus). BMJ. 2010;340:c355-359. doi:10.1136/bmj.c355
Carroll NC. Clubfoot in the twentieth century: where we were and where wemay be going in the twenty-first century. J Pediatr Orthop B. 2011;21:16. doi:10.1097/BPB.0b013e32834a99f2
Chotel F, Parot R, Seringe R, Berard J, Wicart P. Comparative study: Ponsetimethod versus French physiotherapy for initial treatment of idiopathicclubfood deformity. J Pediatr Orthop. 2011;31:320-325
Van Bosse H. Ponseti treatment for clubfeet: an international perspective.Curr Opin Pediatr. 2011;23:41-45. doi:10.1097/MOP.ObO]3e328342112a
D r _F a q e
7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 7/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 7
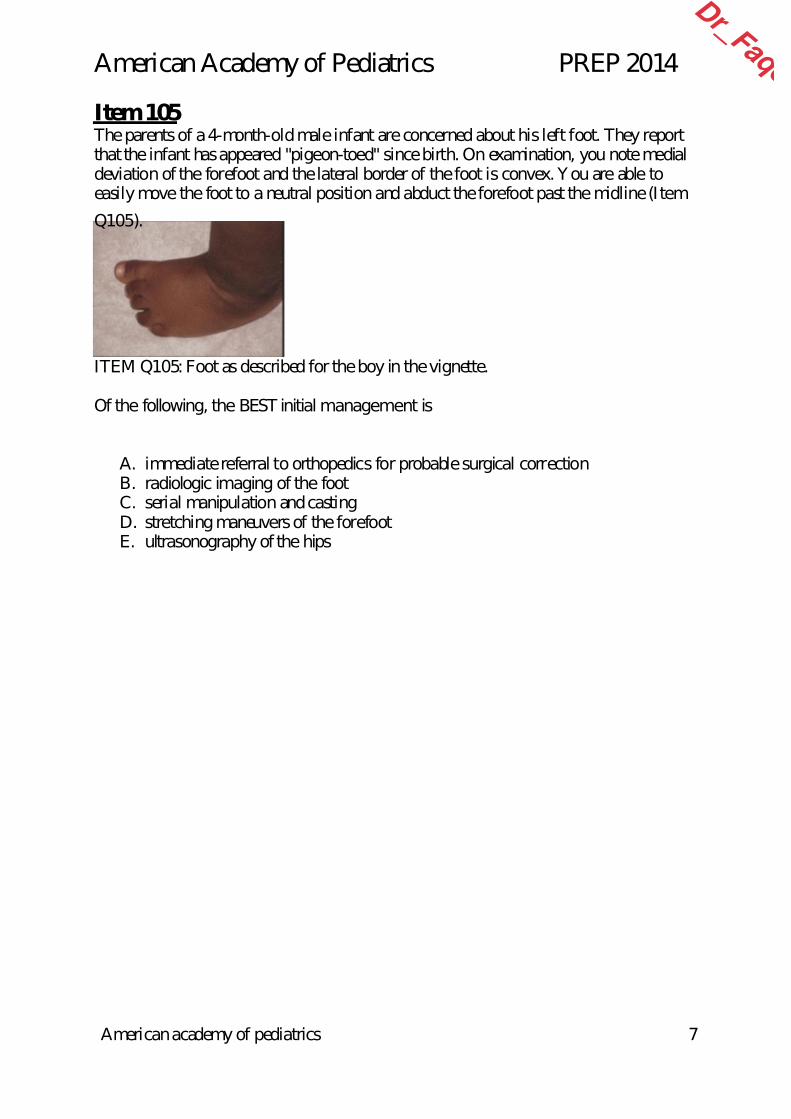
Item 105 The parents of a 4-month-old male infant are concerned about his left foot. They reportthat the infant has appeared "pigeon-toed" since birth. On examination, you note medialdeviation of the forefoot and the lateral border of the foot is convex. You are able toeasily move the foot to a neutral position and abduct the forefoot past the midline (Item
Q105).
ITEM Q105: Foot as described for the boy in the vignette.
Of the following, the BEST initial management is
A.
immediate referral to orthopedics for probable surgical correctionB.
radiologic imaging of the footC.
serial manipulation and castingD.
stretching maneuvers of the forefootE. ultrasonography of the hips
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 8/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 8
Item 105 Preferred Response: D The male infant described in the vignette has the classic features of metatarsus adductus,a congenital foot deformity common in newborns and characterized by adduction ormedial deviation of the forefoot relative to the hindfoot. The incidence is estimated to be1 in 1,000 to 5,000 births, and the most common cause is intrauterine molding. The
incidence is higher in firstborn children and in twin births. Approximately 50% ofaffected infants have bilateral involvement. The diagnosis is made by the physicalexamination. Adduction of the forefoot with the hindfoot remaining in the neutralposition creates the convex shape of the lateral border of the foot. A deep medial crease isoften present, and the base of the fifth metatarsal appears prominent.
Almost all cases of mild to moderate metatarsus adductus will resolve without orthopedicintervention. The need for treatment is based on the rigidity of the deformity. Flexibilityis based on the ability to correct the adduction by providing lateral pressure on theforefoot over the first metatarsal while firmly holding the heel in a neutral position withthe other hand. Mildly affected feet that can be overcorrected into abduction with little
effort may be observed. Passive stretching exercises are recommended for moderate footdeformities that will passively correct only to the neutral position. The outcome in thesepatients is excellent. With this minor manipulation that can be performed by parents,most infants correct by 4 to 6 months of age if the condition is diagnosed and treatedearly.
Surgical correction remains controversial. It may be an option in an older patient (4-6years of age) who have severe persistent metatarsus adductus and exhibit difficulties withphysical function or shoe wear; however, the rate of failure or complications is high.Management with orthotic splints or corrective shoes has been suggested to benefit thosewith moderate deformities but has not been found to be significantly effective.Radiography is not routinely performed but is indicated in toddlers or older children withpersistent deformities. Serial casting is used for patients with more severe or rigiddeformities that cannot be passively abducted to the midline. Results are best whentreatment begins before 8 months of age. Although historically hip dysplasia had beenassociated with metatarsus adductus, more recent data have demonstrated no association. The hips should be examined carefully at every health supervision visit until the child iswalking well as part of the normal physical examination, but ultrasonography of the hipsis not necessary.
PREP Pearls• The diagnosis of metatarsus adductus, a common congenital foot deformity in
newborns, is made by the physical examination.•
The convex lateral border of the foot is due to adduction of the forefoot withthe hindfoot remaining in the neutral position.
• The need for treatment is based on the rigidity of the deformity.• If the forefoot is flexible and can be passively abducted to the midline,
massage and stretching are usually sufficient to treat the deformity.
D r _F a q e
7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 9/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 9
American Board of Pediatrics Content Specification(s):• Understand that if the forefoot can be abducted past the midline, massage and
exercise are usually sufficient to treat metatarsus valgus/varus
Suggested Reading:•
Smith BG. Lower extremity disorders in children and adolescents. PediatrRev. 2009;30:287-294. doi:10.1542/pir.30-8-287• Hosalkar HS. Speigel DA, Davidson RS. Metatarsus adductus. In: Kliegman
RM, Stanton BF, St Geme JW III, Schor NF, Behrman RE, eds. Nelson Textbook of Pediatrics 19th ed. Philadelphia, PA: Saunders Elsevier2011:2335-2336
• McKee-Garrett TM. Lower extremity positional deformations. UptoDate.2012. Available online only for subscription
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 10/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 10
Item 111Parents bring in their 6-year-old daughter because her toes turn in when she walks. Theyare concerned because imaging studies have not been performed and treatment has notbeen prescribed. Examination of this appropriately grown child is notable for moderateintoeing and 90° of internal rotation of both hips when she is in the prone position (Item
Q111). There is no evidence of metatarsus adductus or tibial torsion. Aside from theintoeing, she has a normal gait.
Of the following, the MOST appropriate next step in the care of this child is to
A. counsel the family that a substantial portion of children with this conditionwill require surgical intervention as they grow older
B.
obtain a computed tomography scan to define precisely the femoral neckanatomy
C. prescribe twist cables and corrective shoesD.
reassure the parents that this child has a good prognosis for resolution as the
child maturesE. refer to orthopedics because the intoeing has not corrected by 6 years of age
ITEM Q111: Findings for the girl described in the vignette.
D r _F a q e
7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 11/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 11
Item 111 Preferred Response: DFemoral anteversion occurs when the femoral neck is rotated anteriorly compared withthe transcondylar axis of the knee and the long axis of the femur. It is often the result ofintrauterine positioning and genetic influences and is twice as frequent in girls as in boys.As seen in the patient in the vignette, common characteristics include medially facing
patellae when standing and intoeing, with the patella pointing toward the midline whenwalking. The running gait of a child with femoral anteversion has been described ashaving an "egg-beater" or "windmill" appearance with medial rotation of the thighs andoutward rotation of the feet. Physical examination for femoral anteversion is conductedwith the patient lying prone. With the knees flexed 90°, the lower legs are rotated out,causing the hips to rotate in (Item C111). Children with femoral anteversion havemarkedly increased internal hip rotation up to 90° compared with the normal 35° to 50°.Examination is sufficient to make the diagnosis, and no imaging studies are necessaryunless findings are extreme.
Femoral anteversion is developmentally normal at birth. Typically, the anteversion
decreases by 1° to 2° per year until the adult position is achieved at skeletal maturity.Parents most commonly seek care for their child with this condition when the child isbetween 3 and 6 years old and the normal physiologic external rotation contracture of thehip has resolved. In these children, intoeing may continue to increase until age 6 yearsand then decrease. The condition is not painful and in most cases does not limit function.In about 80% of affected children, femoral anteversion resolves spontaneously, usuallyby age 7 years. However, in some children the final outcome is not seen until age 11years.
In general, referral to an orthopedist is reserved for children who have persistentanteversion beyond age 11 years that causes functional or cosmetic impairment. Ifanteversion is unilateral, the pediatrician should conduct a thorough physical examinationlooking for signs of an underlying neurologic condition such as cerebral palsy. Referral toan orthopedic surgeon may be warranted in this setting. For the few patients requiringtreatment (ie, those with anteversion greater than 50° as seen on radiographic study),femoral derotational osteotomy is effective but has had, in the past, a high rate ofcomplications. Orthotics, twister cables, splinting, bracing, and physiotherapy areineffective in changing the course or degree of intoeing.
Despite reassurance by their primary care practitioner, many parents request anorthopedic evaluation for their child with less significant femoral anteversion. In oneretrospective study, orthopedic specialists in Scotland found that, of 202 patients referredfor intoeing, 86% were discharged after the first visit without a scheduled follow-up andanother 5% were discharged within the next 2 years without intervention. Nine childrenwere re-referred during the study period most commonly because of parental concern.Among parents who completed a questionnaire about their visit, 83% had wanted thereferral but a minority specifically asked for it and only 22% felt their child had a majormedical problem.
D r _F a q e
7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 12/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 12
Long-term consequences of femoral anteversion are some-what controversial. Althoughevidence indicates no substantive link, some practitioners believe there is an increasedincidence of osteoarthritis of the hip and knee, slipped capital femoral epiphysis, andknee and patella instability.
PREP Pearls• Femoral anteversion is diagnosed clinically in a child who has intoeing when
there is increased internal hip rotation (>50°) with the child in the proneposition.
• Besides intoeing, the examiner notes that the patella points medially whenthese children walk.
• The normal course of femoral anteversion is spontaneous improvement by thetime of skeletal maturity.
• Orthopedic referral is indicated when anteversion persists beyond age 11 yearsand causes functional or cosmetic impairment or if the anteversion isunilateral.
American Board of Pediatrics Content Specification(s):• Know that the natural history of femoral anteversion is self-correction• Know that x-ray studies are not necessary for the diagnosis of femoral
anteversion• Know how to evaluate a child with femoral anteversion
Suggested Reading:• Blackmur JP, Murray AW. Do children who in-toe need to be referred to an
orthopaedic clinic. J Pediatr Orthop B. 2010;19:415-417. doi: 10.1097/BPB.0b013e3283339067
•
Hoekelman RA, Chianese MJ. Foot and leg problems. In: Mclnerny TK, ed. Textbook of Pediatric Care. Elk Grove Village, IL: American Academy ofPediatrics; 2009;Chap 183:1541
• Rosenfeld SB. Approach to the child with in-toeing. UptoDate. 2013.Available online only for subscription
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 13/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 13
Item 121 You are examining a female neonate born following an uneventful pregnancy to agravida 3, para 3 woman by repeat cesarean section. The neonate weighs 3.3 kg. A chestradiograph ordered as part of an evaluation for transient tachypnea shows vertebralanomalies and scoliosis. The remainder of the examination is unremarkable. The infant is
breastfeeding well and has no other obvious problems.
Of the following, this neonate is MOST at risk for
A.
cardiopulmonary compromiseB. a connective tissue disorderC.
a cytogenetic abnormalityD.
a genitourinary anomalyE. a neuromuscular disorder
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 14/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 14
Item 121 TE Preferred Response: D The infant described in this vignette has congenital scoliosis secondary to vertebralanomalies. Individuals with congenital scoliosis have high risk for other defects,including an approximate 10% risk of cardiac defects and 25% risk of a concomitantgenitourinary malformation. Conversely, more than 50% of patients with esophageal
atresia have congenital scoliosis. Workup for such infants should include anechocardiogram, renal ultrasound, and magnetic resonance imaging of the spine to assessfor intraspinal anomalies such as lipomas or cord compression resulting from extraduralbony or cartilaginous prominences. Unlike scoliosis that develops after infancy,congenital scoliosis with vertebral defects requires extremely close observation andprompt surgical intervention if any progression occurs. Cardiopulmonary compromise isseen in only the most severe cases but can develop over time if the growth of the thoraciccage is compromised. Therefore, early surgical intervention may assist in maximizingspinal growth and preserving alignment while preventing thoracic restriction.
Children with neuromuscular and connective tissue dis-orders are at increased risk for
secondary scoliosis occurring later in childhood. Cytogenetic abnormalities, while oftenassociated with multiple congenital anomalies, are rarely if ever associated with vertebralmalformations that result in congenital scoliosis.
PREP Pearls• Congenital scoliosis is associated with vertebral anomalies as well as
increased risks for cardiac and genitourinary defects.• Early and aggressive surgical intervention for progressive scoliosis may
preclude compromised spinal growth and respiratory function down the line.
American Board of Pediatrics Content Specification(s):•
Know that congenital scoliosis is associated with other congenitalabnormalities
Suggested Reading:• Scoliosis Research Society. Congenital scoliosis. Scoliosis Research Society
Web site.• Sistonen SJ, Helenius I, Peltonen, Sarna S, Rintala RJ, Pakarinen MP. Natural
history of spinal anomalies and scoliosis associated with esophageal atresia.Pediatrics. 2009;124(6):e1198-e1204. doi:10.1542/ peds.2008-3704
• Zieve D, Ogiela D. Scoliosis. PubMed Health Web site
D r _F a q e
7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 15/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 15
Item 176 The mother of a healthy, 30-month-old girl is concerned because her daughter has begunto run on her toes. She is able to walk with a normal heel – toe gait at times but oftenwalks "on her tip toes.' The birth history is unremarkable, and her developmentalmilestones have been age appropriate. Results of her physical examination, including the
full neuromuscular examination, are normal.
Of the following, your BEST recommendation today is
A.
bracing of the lower extremitiesB. genetic testing for muscular dystrophyC.
magnetic resonance imaging of the spineD.
reassurance that this will likely resolve by 4 years of ageE. referral for botulinum toxin injections
D r _F a q e
7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 16/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 16
Item 176 Preferred Response: D The young age of the girl in this vignette, the parents' report that toe walking is onlyintermittent, and the normal birth and developmental history lead to the most likelydiagnosis of idiopathic toe walking. Importantly, the musculoskeletal and neurologicexamination findings are normal. In this case, toe walking most likely reflects a normal
stage in gait development, and the family can be reassured that it will spontaneouslyresolve by 4 to 5 years of age. Toe walking is more likely to persist beyond 5 years of agein children with neurocognitive disorders.
Children without underlying medical conditions who walk on their toes beyond 3 years ofage are referred to as idiopathic toe walkers. Toddlers may normally experiment withdifferent walking techniques. The heel-toe gait pattern is typically established by 4 yearsof age. Initially, patients with idiopathic toe walking have no specific abnormalities onstatic examination, only on observation of gait. If toe walking persists after 7 to 8 years ofage, heel cord contractures and calf hypertrophy develop. Compensatory external tibialtorsion may occur in the long term. Stretching exercises performed by a physical therapist
or the parents to ensure the child's heel cords remain supple are the first mode oftreatment.
A thorough history and physical examination will help to rule out other causes of toewalking, including neurologic disorders, such as cerebral palsy, muscular dystrophy,tethered spinal cord, or autism. Further evaluation, such as genetic testing for musculardystrophy or magnetic resonance imaging of the spine, should be performed based on thehistory and physical examination. Bracing of the lower extremities may be used toprevent heel cord contractures in older or more impaired children. Interventions, such asserial casting, botulinum toxin injections, or surgery for gastrocnemius or heel-cordlengthening, are sometimes needed in refractory cases.
PREP Pearls• Toe walking may be a normal stage in gait development, especially in children
younger than 4 years.• Pathologic causes of toe walking, such as neuromuscular disorders, should be
ruled out by a thorough history and physical examination.• Toe walking that persists beyond 5 years of age is more common in children with
neurocognitive disorders.
American Board of Pediatrics Content Specification(s):• Know that toe-walking may be a normal stage in gait development or may reflect
underlying pathologic conditions such as neuromuscular disease
Suggested Reading:• Engstrom P, Tedroff K. The prevalence and course of idiopathic toe-walking in 5-
year-old children. Pediatrics. 2012;130:279-284. doi:10.1542/ peds.2012-0225• Smith BG. Lower extremity disorders in children and adolescents. Pediatr Rev.
2009;30:287-294. doi:10.1542/pir.30-8-287
D r _F a q e
7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 17/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 17
Item 253A 6-month-old male infant is seen for his routine health supervision visit. He is doingwell at home, gaining weight, and meeting his milestones. The mother mentions someconcerns about flattening of her son's head posteriorly, and you examine his head fromabove. While he has no evidence of torticollis, he has right-sided flattening of the occiput
as well as flattening above the right orbit, giving a trapezoidal appearance to his head.His mother confirms that they have been placing him in a supine position to sleep atnight. They also have been giving him "tummy time" at home during the day and, sincehis last checkup at 4 months of age, have been alternating his sleeping direction on aweekly basis so that his left and right sides are facing his bedroom door equally.
Of the following, you are MOST likely to recommend
A. continued tummy time and alternating head direction in bed with follow-up inthe pediatric office in 1 month
B.
referral to a pediatric neurosurgeon for evaluation for a possible right coronal
craniosynostosisC. referral to a physical therapist to work with the parents on neck stretching
exercisesD.
referral to the craniofacial team to fit a helmet to correct the positional headdeformity
E.
a switch to a prone sleeping position now that he is capable of rolling over andholding his head up
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 18/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 18
Item 253 Preferred Response: B The infant described in this scenario has evidence of a unilateral lambdoidalcraniosynostosis. Premature closure of a suture (ie, absence of a history and examinationsuggestive of torticollis and presence of a trapezoidal head shape as noted from above)will require neurosurgical evaluation.
Positional skull deformities may be present at birth and can be exacerbated by continuedresting of the head on that side during early infancy. Postnatally acquired positional skulldeformities may also be seen in infants whose cranial contour was normal at birth and insuch instances are often associated with torticollis. Positional skull deformities typi-callyexhibit a parallelogram cranial contour, with the ipsi-lateral ear displaced anteriorly. Incontrast, a deformational defect due to premature fusion of a suture usually shows thetrapezoidal contour, as seen in the infant in the vignette, with no anterior eardisplacement. The differences in the ear position on the ipsilateral side can be comparedand contrasted in Item C253.
Management strategies for positional skull deformities include supine positioning forsleep with the rounded (unaffected) side of the head positioned against the mattress andorienting the crib or sleeping direction so that the infant preferentially gazes away fromthe flattened side. In addition, parents should be encouraged to provide their infants with"tummy time" when they are awake and under observation. For infants with torticollis,parents should be instructed on neck stretching exercises. Most infants with positionalskull deformities will respond to these simple interventions within 3 months. However,deformity progressing by 4 to 6 months of age despite conservative positioning measuresmay also prompt a referral to a neurosurgeon familiar with craniosynostoses.
Whereas some specialists promote skull-molding helmets for positional deformities, thereis little evidence that these devices are more effective than conservative treatment forbabies with mild to moderate deformities. Helmets would be completely ineffective foran infant with a true craniosynostosis, and neck stretching exercises would provide nobenefit in the child in the vignette, who has deformational plagiocephaly and no evidenceof torticollis. Prone positioning for sleep is not recommended for infants at 6 months ofage and would provide no benefit to this child.
PREP Pearls• An infant with plagiocephaly and a trapezoidal head contour is likely to have
a significant craniosynostosis requiring neurosurgical consultation.• If a suspected positional head deformity in an infant is not responding to
conservative measures such as positioning by 4 to 6 months of age, aneurosurgical evaluation may be required.
American Board of Pediatrics Content Specification(s):• Recognize the clinical findings of premature closure of a cranial suture
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 19/47
American Academy of Pediatrics PREP 2014
American academy of pediatrics 19
Suggested Reading:• laughn I. Luerssen 1G, Dias MS; Committee on Practice and Ambulatory
Medicine, Section on Neurological Surgery. Prevention and management ofpositional skull deformities in infants. Pediatrics. 2011;128(6):12361241.doi:10.1542/peds.2011.2220
•
Robin NH. Falk Ml, Haldeman-Englert CR. rGFIL-relatedcraniosynostmissyndromes. In: Pagon RA, Bird TD, Dolan CR, eds. GencRervic". Seattle,Washington: University of Washington; 2013
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 20/47
American Academy of Pediatrics 2013 PREP SA on CD-RO
Copyright 2013 © American Academy of Pediatrics
Question: 158
A father brings his daughter in for a health supervision visit. She skips (alternating feet) into the roomYou give her a piece of paper and a crayon and ask her to draw a person. She proudly draws a personwith 6 body parts. You ask her to take off her shoes and sweater in order to obtain an accurate weightand she quickly complies with your request.
Of the following, the age that BEST describes this childs developmental abilities is A. 2 years old
B. 3 years old
C. 4 years old
D. 5 years old
E. 6 years old
D r _F a
7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 21/47
American Academy of Pediatrics 2013 PREP SA on CD-RO
Copyright 2013 © American Academy of Pediatrics
Preferred ResponseCritique: 158
The girl described in the vignette has reached the normal motor developmental milestones for a 5-year-old. She is able to dress and undress herself, draw a person with 6 body parts, and skip(alternating feet). A 2-year-old can run well, walk up and down steps one step at a time, jump in place,make a tower of seven cubes, scribble in a circular pattern, and imitate a horizontal stroke. At 3 years age, a child is able to pedal a tricycle, draw a circle, and draw a person with a head and 1 other bodypart. A child of 4 years of age is able to copy a cross and a square, catch a bounced ball, and hop onone foot 2 or 3 times. A 6-year-old child can ride a bicycle without training wheels and draw a personwith details of hair, eyes, nose, mouth, and hands with 5 fingers and who is wearing a shirt, pants, andshoes.
Parents typically first report delays in motor development when the infant is between 6 and 12months of age. A childs motor development is assessed using information provided by the parents andby direct observation. A motor quotient may be determined by dividing the developmental age by thechronologic age and multiplying the result by 100. Gross motor quotients below 50 are usually indicativof cerebral palsy. Motor quotients of 50 to 75 may reflect low muscle tone. Children who have mildermotor delays may have comorbid neurodevelopmental disorders, such as learning disorders or attentiodeficit/hyperactivity disorder. SUGGESTED READING:
Accardo PJ, Capute A. A neurodevelomental perspective on the continuum of developmentaldisabilities. In: Accardo PJ. Capute & Accardos Neurodevelopmental Disabilities in Infancy and
Childhood, Volume I: Neurodevelopmental Diagnosis and Treatment. 3rd ed. Baltimore, MD: Paul HBrookes Publishing Co; 2008:3-10
Blasco P. Motor delays. In: Parker SJ, Zukerman BS, Augustyn MC, eds. Developmental andBehavioral Pediatrics: A Handbook for Primary Care. 2nd ed. Philadelphia, PA: Lippincott, Williams &Wilkins; 2005:242-247
Dedrick C. Developmental milestones. Developmental Behavioral Pediatrics Online. 2005
Gerber RJ, Wilks T and Erdie-Lalena C. Developmental milestones: motor developmental. PediatrRev. 2010;31:267-277. doi:10.1542/pir.31-7-267
Schultz M, Blasco P. Motor Development. In: Voight RG, Macias MM, Myers SM, eds. Developmen
D r _F a
7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 22/47
American Academy of Pediatrics 2013 PREP SA on CD-RO
Copyright 2013 © American Academy of Pediatrics
Question: 243
A girl skips (alternating feet) into your examination room for her health supervision visit. She happilyexclaims she is able to tie her shoes and ride her bicycle without training wheels. You give her a blankpiece of paper and ask her to write her name. She proudly writes her first and last name.
Of the following, the age that BEST describes this child is A. 3 years old
B. 4 years old
C. 5 years old
D. 6 years old
E. 7 years old
D r _F a
7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 23/47
American Academy of Pediatrics 2013 PREP SA on CD-RO
Copyright 2013 © American Academy of Pediatrics
Preferred ResponseCritique: 243
The child described in the vignette has reached the normal motor developmental milestones for 6years of age. She can ride a bicycle without training wheels and walk in tandem (skipping). She is alsoable to write both her first and last name. A six-year-old should also be able to draw a diamond and dra person with 12 to 14 parts. A 3-year-old is able to copy a circle and draw a person with a head and one other body part. Theyalso should be able to balance on one foot for 3 seconds and go up stairs alternating feet. A child of 4years of age is able to copy a square, write part of first name, throw a ball overhand, catch a bouncedball and hop on one foot 2 or 3 times. Five-year-olds are able to copy a triangle, write their name, hop one foot 15 times, and skip. A child of 7 years of age can draw an equal-sided diamond and draw a
person with 18 parts. Motor developmental milestones are obtained via parental history and from direct observation. Toascertain if a child has delays in motor milestones, the clinician must take into account history, standarneurodevelopmental milestones, and the presence or absence of primitive reflexes and posturalresponses. A motor quotient (MQ) can be determined by the following: MQ = (motor age/chronologicaage) 100. A MQ above 70 is normal, between 50 and 70 is suspicious and requires monitoring, andbelow 50 is abnormal and requires referral to a specialist.
SUGGESTED READING:
Blasco P. Motor delays In: Parker SJ, Zukerman BS, Augustyn MC, eds. Developmental andBehavioral Pediatrics: A Handbook for Primary Care. 2nd ed. Philadelphia, PA: Lippincott, Williams &
Wilkins; 2005:242-247 Dedrick C. Developmental milestones. Developmental Behavioral Pediatrics Online. 2005
Gerber RJ, Wilks T, Erdie-Lalena C. Developmental milestones: motor developmental. Pediatr Rev
2010;31(7):267-277. doi:10.1542/pir.31-7-267
Perniciaro J. Development, behavior, and mental health. In: Tschudy MM, Arcara KM, ed. The HarrLane Handbook: A Manual for Pediatric House Officers. 19th ed. Philadelphia, PA: Elsevier Mosby;2012:226-242
Schultz M, Blasco P. Motor development in developmental and behavioral pediatrics. In: Voight RG
Macias MM, Myers SM, eds. Developmental and Behavioral Pediatrics. Elk Grove Village, IL: American Academy of Pediatrics; 2011:147-169
D r _F a

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 24/47
merican Academy of Pediatrics 2012 PREP SA on CD-ROM
Copyright 2012 © American Academy of Pediatrics 1
Question: 11
A father brings in his daughter for a routine health supervision visit. The father quietly holds her in hislap while you call to her. She immediately turns toward you and begins to make babbling sounds. Yourespond by saying "dada" while pointing to the father. The girl begins to imitate the "dada" sounds.
Of the following, these developmental milestones are MOST typical for a child whose age is
A. 2 months
B. 4 months
C. 6 months
D. 9 months
E. 12 months
D r _F a
7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 25/47
merican Academy of Pediatrics 2012 PREP SA on CD-ROM
Copyright 2012 © American Academy of Pediatrics 2
Preferred Response: CCritique: 11
The child described in the vignette exhibits the normal cognitive/behavioral developmental milestonesfor 6 months of age: turns directly to sound and voice, babbles consonant sounds, and imitates speechsounds. A 6-month-old child responds to social overtures by displaying an emotional response of pleasure or a negative affect. In addition, the child reaches for familiar persons and displays stranger anxiety with unfamiliar people. Developmental surveillance should be part of every health supervision visit and any concerns shouldbe promptly addressed. A 6-month-old child should turn to a sound or voice, and a child of this age whodoes not respond should be referred for audiologic testing to rule out a hearing deficit. Further neurodevelopmental testing and referral for early intervention also should be considered. The normal cognitive/behavioral developmental milestones for a 2-month-old infant are to smile onsocial contact, listen to voice, and coo. The infant may respond to an adult voice and smile. A 4 month
old laughs out loud, squeals, initiates social interactions, and shows interest in his or her own image in amirror. A 9 month old imitates sounds, babbles, says "mama" nonspecifically, follows a pointed finger,and recognizes familiar people. At 12 months of age, a child shows objects to his or her parents to shareinterest and points for requests. The child uses several gestures while vocalizing.
SUGGESTED READING:
Coplan J. Child development in the first 21 months. In: Parker S, Zuckerman B, Augustyn M, eds.Developmental and Behavioral Pediatrics: A Handbook for Primary Care. 2nd ed. Philadelphia, PA:Lippincott Williams & Wilkins; 2005:445-446
Council on Children with Disabilities, Section on Developmental Behavioral Pediatrics, Bright Futures
Steering Committee, Medical Home Initiatives for Children With Special Needs Project AdvisoryCommittee. Identifying infants and young children with developmental disorders in the medical home: analgorithm for developmental surveillance and screening. Pediatrics. 2006;118:405-420. DOI:10.1542/peds.2006-1231. Accessed December 2010 at:http://pediatrics.aappublications.org/cgi/content/full/118/1/405
Feigelman S. The first year. In: Kliegman RM, Stanton BF, St. Geme JW III, Schor NF, and BehrmanRE, eds. Nelson Textbook of Pediatrics. 19th ed. Philadelphia, PA: Saunders Elsevier; 2011:26-31
Gerber RJ, Wilks T, Erdie-Lalena C. Developmental milestones: motor development. Pediatr Rev.2010;31:267-277. DOI: 10.1542/pir.31-7-267. Accessed December 2010 at:http://pedsinreview.aappublications.org/cgi/content/full/31/7/267
Joint Committee on Infant Hearing. Year 2007 position statement: principles and guideline for earlyhearing detection and intervention programs. Pediatrics. 2007;120: 898-921. DOI: 10.1542/peds.2007-2333. Accessed December 2010 at: http://pediatrics.aappublications.
D r _F a

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 26/47
merican Academy of Pediatrics 2012 PREP SA on CD-ROM
Copyright 2012 © American Academy of Pediatrics 3
org/cgi/content/full/120/4/898
O’Conner Leppert ML. Neurodevelopmental assessment and medical evaluation. In: Voight RG,Macias MM. Myers SM, eds. American Academy of Pediatrics Developmental and Behavioral Pediatrics.Elk Grove Village, IL: American Academy of Pediatrics; 2011:93-120
D r _F a

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 27/47
merican Academy of Pediatrics 2012 PREP SA on CD-ROM
Copyright 2012 © American Academy of Pediatrics 4
Question: 28
During a health supervision visit, a boy calls to his father by saying "dada." His mother enters theroom holding a snack. The child reaches out to her and cries loudly "mama." When the boy notices hismother is holding a banana, he smiles and says "nana." His mother picks him up and offers him thebanana. You inquire if he is saying any other words. His mother replies "not yet."
Of the following, these findings are MOST expected for a typically developing child who is
A. 9 months old
B. 12 months old
C. 15 months old
D. 18 months old
E. 24 months old
D r _F a

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 28/47
merican Academy of Pediatrics 2012 PREP SA on CD-ROM
Copyright 2012 © American Academy of Pediatrics 5
Preferred Response: BCritique: 28
The child described in the vignette exhibits the normal cognitive/behavioral developmental milestonesfor 12 months of age: says "mama" and "dada" with meaning and says at least one additional specificword. A 9-month-old child imitates speech sounds, babbles, says "mama" nonspecifically, follows apointed finger, and recognizes familiar people. At 15 months of age, a child uses three to five words, hasmature jargoning, greets people, and shows empathy. An 18 month old uses 10 to 25 words, names apicture on demand, and engages in pretend play with others. A 24-month-old child has a vocabulary of more than 50 words, speaks in two-word sentences, and engages in parallel play. Early identification of developmental disorders is crucial to a child’s well-being. In addition to routine developmentalsurveillance, a developmental screening tool should be administered regularly at the 9-, 18-, and either the 24- or 30-month health supervision visits.
SUGGESTED READING:
Council on Children with Disabilities, Section on Developmental Behavioral Pediatrics, Bright FuturesSteering Committee, Medical Home Initiatives for Children With Special Needs Project AdvisoryCommittee. Identifying infants and young children with developmental disorders in the medical home: analgorithm for developmental surveillance and screening. Pediatrics. 2006;118:405-420. DOI:10.1542/peds.2006-1231. Accessed December 2010 at:http://pediatrics.aappublications.org/content/118/1/405
Feigelman S. The first year. In: Kliegman RM, Stanton BF, St. Geme JW III, Schor NF, and BehrmanRE, eds. Nelson Textbook of Pediatrics. 19th ed. Philadelphia, PA: Saunders Elsevier; 2011:26-31
First Signs web site. Accessed December 2010 at: http://www.firstsigns.org
O’Conner Leppert ML. Neurodevelopmental assessment and medical evaluation. In: Voight RG,Macias MM. Myers SM, eds. American Academy of Pediatrics Developmental and Behavioral Pediatrics.Elk Grove Village, IL: American Academy of Pediatrics; 2011: 93-120
D r _F a

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 29/47
merican Academy of Pediatrics 2012 PREP SA on CD-ROM
Copyright 2012 © American Academy of Pediatrics 6
Question: 46
When a mother and her child enter the examination room for a health supervision visit, the childquickly states, "I want book." Her mother takes out her picture book, and you ask the girl to find the babyin the story book. She looks through the book and points to a picture of a baby. She then turns andpoints to her doll and says "mine." Her mother proudly states that her daughter has just begun tocombine words.
Of the following, these findings are MOST expected for a typically developing child who is
A. 12 months
B. 18 months
C. 24 months
D. 30 months
E. 36 months
D r _F a
7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 30/47
merican Academy of Pediatrics 2012 PREP SA on CD-ROM
Copyright 2012 © American Academy of Pediatrics 7
Preferred Response: CCritique: 46
The child described in the vignette exhibits the normal cognitive/behavioral developmental milestonesfor a 24-month-old child: combines words into two- or three-word phrases; points to pictures named;uses vocabulary of 50+ words; and uses "I," "me," and "mine" in speech. At 12 months of age, a childsays "mama" and "dada" with meaning and at least one additional specific word. At 18 months of age, achild has a vocabulary of 7 to 10 words. A child of 30 months of age is able to use pronounsappropriately. A child of 36 months of age has a vocabulary of 250 words. Early identification of developmental disorders is crucial to a child’s well-being. Routine developmental surveillance should beundertaken at each health supervision visit. A developmental screening tool should be administered atthe 9-, 18-, and either the 24- or 30-month health supervision visits. An autism spectrum disorder-specific screening tool also should be administered at ages 18 and 24 months of age. Indications for evaluation of language delay are: no babbling, pointing, or gesturing by 12 months; no
single words by 16 months of age; no two-word spontaneous phrases by 24 months of age; and anyregression in language or social skills at any age. A child whose results on screening tools areconcerning should be referred for developmental and medical evaluation as well as early developmentalintervention/early childhood services.
SUGGESTED READING:
Agin MC. The "late talker"-when silence isn’t golden. Contemp Pediatr. 2004;21(Nov):22-34. Accessed December 2010 at:http://www.modernmedicine.com/modernmedicine/article/articleDetail.jsp?id=132720&sk=&date=&pageID=2
Council on Children with Disabilities, Section on Developmental Behavioral Pediatrics, Bright FuturesSteering Committee, Medical Home Initiatives for Children With Special Needs Project AdvisoryCommittee. Identifying infants and young children with developmental disorders in the medical home: analgorithm for developmental surveillance and screening. Pediatrics. 2006;118:405-420. DOI:10.1542/peds.2006-1231. Accessed December 2010 at:http://pediatrics.aappublications.org/content/118/1/405
Johnson CP, Myers SM. Overview of the AAP autism spectrum disorders toolkit and guidelines.Contemp Pediatr. 2008;25(Oct):43-67. Accessed December 2010 at:http://www.modernmedicine.com/modernmedicine/Neurology/Overview-of-the-AAP-autism-spectrum-disorders-tool/ArticleStandard/Article/detail/558616
Leppert MO. Neurodevelopmental Assessment and Medical Evaluation. In: Voight RG, Macias MM,Myers SM, eds. American Academy of Pediatrics Developmental and Behavioral Pediatrics. Elk GroveVillage, IL: American Academy of Pediatrics; 2011:100-102
D r _F a

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 31/47
merican Academy of Pediatrics 2012 PREP SA on CD-ROM
Copyright 2012 © American Academy of Pediatrics 8
Question: 63
A child walks into the examination room, accompanied by his parents. He points to a box of crayonsthat he notices on a nearby shelf. You offer him a paper and the crayons. You then draw a vertical lineand a cross, which he successfully copies. You ask him to draw a person. He draws two circles, one for the head and one for the body. He then stops drawing and says, "Look at me" while he balances on hisfoot for 3 seconds.
Of the following, these developmental milestones are MOST typical for a child whose age is
A. 24 months
B. 30 months
C. 36 months
D. 48 months
E. 60 months
D r _F a

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 32/47
merican Academy of Pediatrics 2012 PREP SA on CD-ROM
Copyright 2012 © American Academy of Pediatrics 9
Preferred Response: DCritique: 63
The child described in the vignette exhibits the normal developmental milestones for 4 years of age.He can copy a cross, draw a simple figure of a person (head plus one other body part), and hop on onefoot two to three times. If asked, it is likely that he also could copy a square. A child of 24 months isable to walk down stars holding a rail, throw a ball overhand, and imitate drawing a horizontal line. A 30-month-old child can alternate feet while walking up stairs with a railing, jump in place, and make aneight-cube tower. A 36 month old can balance on one foot for 3 seconds, pedal a tricycle, and copy acircle. A 60 month old can walk down stairs holding a railing while alternating feet, hop on one foot 15times, skip, copy a triangle, and write his or her name. Motor developmental milestones are obtained via parental history and from observation duringneurodevelopmental examination. To ascertain if a child has delays in motor milestones, the clinicianmust consider the history, standard neurodevelopmental milestones, and the presence or absence of
primitive reflexes and postural responses. A motor quotient (MQ) can be determined by the following:MQ=motor age/chronological age x 100. An MQ of greater than 70 is normal, between 50 and 70 issuspicious and requires monitoring, and less than 50 is abnormal and requires referral to asubspecialist.
SUGGESTED READING:
Gerber RJ, Wilks T, Erdie-Lalena C. Developmental milestones: motor development. Pediatr Rev.2010;31:267-277. DOI: 10.1542/pir.31-7-267. Accessed December 2010 at:http://pedsinreview.aappublications.org/cgi/content/full/31/7/267
Lingam R, Missiuna C, Forsyth K, Emond L. Developmental coordination disorder: a physician’s
guide to assessment and diagnosis. AAP Section on Developmental and Behavioral PediatricsNewsletter. 2009;Fall:4-6. Accessed December 2010 at:http://www.aap.org/sections/dbpeds/pdf/PDFNewContent/ScreeningAssess/Developmental%20Coordination%20Disorder.pdf
D r _F a
7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 33/47
2010 PREP SA on CD-ROM
Question: 10
You are examining a 6-year-old girl at her annual health supervision visit. She has Sexual
Maturity Rating 3 pubic hair, but no axillary hair. Her mother notes that the child has had an adult
body odor for about 6 months. You cannot detect breast tissue, and she does not have
clitoromegaly. You examine her growth chart for height (Item Q10).
Of the following, the MOST important test to perform at this time is
A. bone age radiography
B. magnetic resonance imaging of the head
C. pelvic ultrasonography
D. serum estradiol measurement
E. serum testosterone measurement
Copyright © 2010 by the American Academy of Pediatrics page 1
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 34/47
2010 PREP SA on CD-ROM
Question: 10
Growth chart for height. (Courtesy of L. Levitsky)
Copyright © 2010 by the American Academy of Pediatrics page 2
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 35/47
2010 PREP SA on CD-ROM
Preferred Response: ACritique: 10
Bone age radiographs can offer useful information about the adult height potential of healthy
children who have bone ages of more than 7 years. In addition, a bone age that is advanced, in
contrast to chronologic age, can offer some understanding of the length of time or the severity
of exposure to sex steroids, particularly estrogen, which is responsible for epiphyseal
advancement. Similarly, a bone age that is delayed in relation to chronologic age can offer some
inference as to the length of time of endocrine deficiency disorders such as hypothyroidism or
chronic nutritional disorders such as celiac disease. However, bone age radiographs do not
permit accurate height predictions in children who have bone ages less than 7 years and cannot
offer appropriate height predictions for children who have abnormal growth patterns because of
bone disorders or other growth disorders. Studies have shown that in children who have
isolated premature pubic or axillary hair development (premature pubarche or adrenarche), a
bone age radiograph that is more than 1 year advanced compared with chronologic age
increases the possibility of a serious underlying disorder such as late-onset congenital adrenal
hyperplasia.
The girl described in the vignette has premature adrenarche or pubarche, the early
appearance of the physical signs of adrenal puberty. Her growth chart reveals a small
acceleration in height, which is consistent with this diagnosis (Item C10). She has no evidence
of either ovarian puberty (thelarche or breast tissue) or exposure to potent androgens
(clitoromegaly). An increase in adrenal production of weak androgen precursors
(dehydroepiandrosterone [DHEA] and dehydroepiandrosterone sulfate [DHEA-s]) can be
identified in most children between 4 and 6 years of age. However, the earliest signs of adrenal
puberty (adult body odor, pubic hair) usually occur at the same time or a few months after
thelarche. Rare children may have higher DHEA and DHEA-s values before the age of 7 years or
may be particularly sensitive to low circulating concentrations of these hormones. Such children,
including the girl in the vignette, come to medical attention because of early adult body odor and
pubic and/or axillary hair.
The most likely worrisome possibility in the differential diagnosis for children who have
premature adrenarche is late-onset congenital adrenal hyperplasia. A bone age radiograph
reading within 1 year of the child’s actual age effectively rules out the diagnosis. Magnetic
resonance imaging of the head might be indicated in a female child who has early true sexual
precocity (activation of the hypothalamic gonadotropic axis with thelarche), but there is no
indication for such a study in this child. Pelvic ultrasonography is indicated if there is suspicion
about an androgen-producing ovarian tumor, but the slow progression and lack of clitoromegaly
makes this very unlikely for this girl. Measures of serum estradiol and testosterone are not
useful in this situation. The child’s lack of thelarche or clitoromegaly indicates low estradiol andtestosterone concentrations, respectively, and standard commercial assays do not provide
accurate results at the low concentrations of estrogen and testosterone found in early puberty.
Her growth at a higher percentile is typical of girls who will be slightly early maturers and are
having the mid-childhood growth spurt, sometimes attributed to adrenarche.
References:
Copyright © 2010 by the American Academy of Pediatrics page 3
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 36/47
2010 PREP SA on CD-ROM
Ibánez L, Jiménez R, de Zegher F. Early puberty-menarche after precocious pubarche: relation
to prenatal growth. Pediatrics . 2006;117:117-121. Available at:
http://pediatrics.aappublications.org/cgi/content/full/117/1/117
Kaplowitz P. Clinical characteristics of 104 children referred for evaluation of precocious
puberty. J Clin Endocrinol Metab . 2004;89:3644-3650. Available at:
http://jcem.endojournals.org/cgi/content/full/89/8/3644
Kaplowitz PB. Precocious puberty. eMedicine Specialties, Pediatrics: General Medicine,
Endocrinology . 2007. Available at: http://emedicine.com/ped/TOPIC1882.HTM
Muir A. Precocious puberty. Pediatr Rev . 2006;27:373-381. Available at:
http://pedsinreview.aappublications.org/cgi/content/full/27/10/373
Copyright © 2010 by the American Academy of Pediatrics page 4
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 37/47
2010 PREP SA on CD-ROM
Critique: 10
Copyright © 2010 by the American Academy of Pediatrics page 5
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 38/47
2010 PREP SA on CD-ROM
Question: 11
You are examining a 4-year, 11-month-old child during her health supervision visit. Her mother
has been home with her full time since birth. The friendly, happy child tells you about her trip to
the zoo last week. She asks if you like animals and counts out loud 10 different animals she
saw. When given a crayon, she is able to write her name stating the letters as she writes them.
Her mother expresses concern about her beginning kindergarten next month because she just
meets the age cut-off for kindergarten entry. She inquires about the factors that will help
determine if her child is ready to attend school.
Of the following, the MOST appropriate response is that the girl should
A. be able to maintain attention during story time for at least 20 to 25 minutes
B. be able to state her birthday and address
C. be able to tolerate separations from her parent for several hours at a time
D. identify upper and lower case letters
E. undergo psychoeducational testing to assess kindergarten readiness
Copyright © 2010 by the American Academy of Pediatrics page 6
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 39/47
2010 PREP SA on CD-ROM
Preferred Response: CCritique: 11
Children are socially ready to attend school when they are able to separate from their
parents for several hours at a time. They are expected to pay attention to the teacher, follow the
classroom routine, play well with others, and take turns. During classroom group-based
activities, the young child should be able to pay attention to the teacher for 10 to 15 minutes, sit
quietly, and listen to the teacher without bothering peers or disrupting the activity. Children also
should be able to relate personal experiences and tell stories.
Children entering kindergarten should know color names, be able to count to 10, retell a
story, identify some printed letters, and print their names. Knowing their addresses and birth
dates and being able to identify both upper and lower case letters is expected of children
entering first grade. Because the child described in the vignette has the prerequisite skills for
kindergarten, a psychoeducational evaluation is not indicated at this time.
References:
High PC and the Committee on Early Childhood, Adoption, and Dependent Care and Council on
School Health. School readiness. Pediatrics. 2008;121:e1008-e1015. Available at:
http://pediatrics.aappublications.org/cgi/content/full/121/4/e1008
Kaplan-Sanoff M. School readiness. In: Parker S, Zukerman B, Augustyn M, eds. Developmental
and Behavioral Pediatrics: A Handbook for Primary Care . 2nd ed. Philadelphia, Pa: Lippincott
Williams & Wilkins; 2005:285-288
Copyright © 2010 by the American Academy of Pediatrics page 7
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 40/47
2010 PREP SA on CD-ROM
Question: 203
An infant born at 34 weeks’ gestation comes in for her 1-month-old evaluation. Her neonatal
course was uncomplicated. Her parents ask if she will have delayed development due to her
prematurity.
Of the following, the MOST appropriate response is that healthy preterm infants
A. have age-appropriate language skills by the time they are 12 months of age
B. have an increased risk of mild motor impairment
C. born at 32 to 36 weeks’ gestation have a fourfold increase in intellectual disabilities
D. should have their developmental age corrected for the degree of prematurity until 4 years of
age
E. show hand preference at an earlier age than term infants
Copyright © 2010 by the American Academy of Pediatrics page 8
D r _F a q e
7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 41/47
2010 PREP SA on CD-ROM
Preferred Response: BCritique: 203
Some factors that lead to greater risk of neurological/behavioral problems among preterm
infants (those born at <37 weeks’ gestation) include low birthweight (<2,500 g), intrauterine
growth restriction, and a history of maternal prenatal drug use. Medical complications that could
affect the infant’s development include intraventricular hemorrhage (IVH), cardiac lesions,
bronchopulmonary dysplasia, feeding problems, and retinopathy of prematurity. A preterm infant
who has either a grade 3 or 4 IVH has a 35% to 90% increased risk of a neurodevelopmental
disability.
A 34 weeks’ gestation infant who has an uncomplicated neonatal course, such as the child
described in the vignette, has an increased risk of mild motor impairment, referred to as a
developmental coordination disorder. Most experts agree that preterm infants should have their
developmental ages corrected for the degree of prematurity at least for the first 12 months after
birth; many clinicians continue to use a full correction until 24 months of age. However, age
correction up to 4 years of age is not necessary. Preterm infants born at 32 to 36 weeks’
gestation have a 1.4-fold increased risk of intellectual disabilities over term infants, although the
risk increases to 7-fold for children born prior to 32 weeks’ gestation. Healthy preterm infants
may not develop age-appropriate language skills until they are older than 12 months of age,
which is why their developmental level must be corrected for their level of prematurity. A
preterm infant should not routinely have early hand preference; such a finding may be indicative
of cerebral palsy.
References:
Allen M. Preterm development. In: Accardo PJ, ed. Capute & Accardo’s Neurodevelopmental
Disabilities in Infancy and Childhood. Volume II: The Spectrum of Neurodevelopmental
Disabilities . 3rd ed. Baltimore, Md: Paul H. Brookes Publishing Co; 2008:29-46
Vanderbilt D, Wang CJ, Parker S. The do’s in preemie neurodevelopment. Contemp Pediatr . 2007
September:84-97
Copyright © 2010 by the American Academy of Pediatrics page 9
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 42/47
2010 PREP SA on CD-ROM
Question: 219
A healthy term newborn fails the universal hearing screening. Follow-up testing reveals that he
has a profound hearing loss. His parents inquire about the development of young children who
have congenital hearing loss.
Of the following, the BEST response is that
A. early amplification and developmental services improve overall language outcome
B. hearing aids promote language development only for children who have mild hearing loss
C. lip reading encourages the child to speak and understand language faster
D. prelingual deafness is associated with better cognitive outcome than postlingual deafness
E. severe or profound hearing loss is associated with impaired cognitive skills
Copyright © 2010 by the American Academy of Pediatrics page 10
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 43/47
2010 PREP SA on CD-ROM
Preferred Response: ACritique: 219
Among newborns who have hearing loss, those who receive early amplification and
developmental services fare better than those who receive such services at a later date.
Children who have postlingual deafness have a better cognitive outcome than those who have
prelingual deafness. Quickly developing spoken language is a challenge for the child who solely
uses lip reading. Children who have severe or profound hearing loss do not necessarily have
impaired cognitive skills. The use of hearing aids promotes language development for children
who have varying degrees of hearing loss. Almost all children who have mild and moderate
hearing loss and some who have severe hearing loss can develop spoken language with the
early and consistent use of personal hearing aids.
Children who have a congenital hearing loss may have delays in speech and language
development. One of the early signs of this is a delay in prespeech babble. Children who have
congenital hearing loss also may have decreased attention span and other behavioral difficulties
due to their frustration with their inability to communicate.
References:
Feldman HM. Evaluation and management of language and speech disorders in preschool
children. Pediatr Rev . 2005;26:131-141. Available at:
http://pedsinreview.aappublications.org/cgi/content/full/26/4/131
Gravel JS, O’Gara J. Communication options for children with hearing loss. Ment Retard Dev
Disabil Res Rev . 2003;9:243-251. Available at: http://www.ncbi.nlm.nih.gov/pubmed/14648817
Copyright © 2010 by the American Academy of Pediatrics page 11
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 44/47
2010 PREP SA on CD-ROM
Question: 235
A mother and father bring in their infant for a routine health supervision visit. The mother gently
places the child on the examination table, and the child laughs out loud. As you approach the
child, he squeals and reaches for his father.
Of the following, these developmental milestones are MOST typical for a child whose age is
A. 2 months
B. 4 months
C. 6 months
D. 8 months
E. 10 months
Copyright © 2010 by the American Academy of Pediatrics page 12
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 45/47
2010 PREP SA on CD-ROM
Preferred Response: BCritique: 235
The infant described in the vignette exhibits the normal cognitive/behavioral developmental
milestones for 4 months of age: laughing out loud, squealing, and initiating social interactions.
Infants of this age show interest in the environment by looking at or listening to stimuli for
approximately 3 seconds.
The normal cognitive/behavioral developmental milestones for a 2-month-old infant are to
smile on social contact, listen to voice, and coo. A 6-month-old child responds to social
overtures by displaying an emotional response of pleasure or a negative affect. An 8-month-old
child babbles, enjoys mirrors, and responds to changes in emotional or social content. At 10
months of age, a child responds to the sound of his or her name, plays peek-a-boo or patty-
cake, and waves bye-bye. In addition, the infant may reach up when the parent bends to pick
him or her up and may use hand movements to request a toy or to be picked up.
References:
Coplan, J. Child development in the first 21 months. In: Parker S, Zuckerman B, Augustyn M, eds.
Developmental and Behavioral Pediatrics: A Handbook for Primary Care . 2nd ed. Philadelphia,
Pa: Lippincott Williams & Wilkins; 2005:437-438
Feigelman S. The first year. In: Kliegman RM, Behrman RE, Jenson HB, Stanton BF, eds. Nelson
Textbook of Pediatrics . 18th ed. Philadelphia, Pa: Saunders Elsevier; 2007:43-47
First Signs web site. Available at: http://www.firstsigns.org
Greenspan S. Socioemotional development of infants and children: themes and behaviors. In:
Parker S, Zuckerman B, Augustyn M, eds. Developmental and Behavioral Pediatrics: A
Handbook for Primary Care . 2nd ed. Philadelphia, Pa: Lippincott Williams & Wilkins; 2005:447-450
Copyright © 2010 by the American Academy of Pediatrics page 13
D r _F a q e
7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 46/47
2010 PREP SA on CD-ROM
Question: 250
You observe a child as he walks into the examination room, accompanied by his parents. He is
holding a small ball. When you ask him to let you see the ball, he gives it to you. You hand the ball
back to him, and he throws the ball to you. When you throw him the ball, he reaches to catch it
but almost loses his balance. He stoops to the floor but recovers to a standing position while
laughing and smiling at his parents. You offer him a crayon and a piece of paper, and he draws
a straight line. When he sees a few blocks on the floor, he picks up two and stacks one on top
of the other.
Of the following, these developmental milestones are MOST typical for a child whose age is
A. 9 months
B. 12 months
C. 15 months
D. 18 months
E. 24 months
Copyright © 2010 by the American Academy of Pediatrics page 14
D r _F a q e

7/17/2019 01 Growth and Development
http://slidepdf.com/reader/full/01-growth-and-development 47/47
2010 PREP SA on CD-ROM
Preferred Response: CCritique: 250
Motor developmental milestones are obtained via parental history and from observation
during neurodevelopmental examination. To determine if a child has delays in motor milestones,
the clinician must take into account history, standard neurodevelopmental milestones, and the
presence or absence of primitive reflexes and postural responses. A motor quotient (MQ) can
be determined by the following: MQ = motor age/chronological age x 100. A MQ of above 70 is
normal, between 50 and 70 is suspicious and requires monitoring, and below 50 is abnormal and
requires referral to a subspecialist.
The child described in the vignette shows the normal motor developmental milestones for a
15-month-old, which consist of playing ball, giving and taking a toy, walking independently,
stooping to the floor and recovering to a standing position, making a line with a crayon, and
building a two-cube tower. A 9-month-old child is able to pull to stand and cruise, walk with two
hands held, and employ an immature pincer grasp. Most 12-month-old children are able to walk
alone, use a mature pincer grasp, and release an object to another person on request. An 18-
month-old child is able to run stiffly, walk up steps using a railing, make a tower of four cubes,
and imitate scribbling and a vertical stroke. A 24-month-old child can run well, walk up and down
steps one step at a time, jump in place, make a tower of seven cubes, scribble in a circular
pattern, and imitate a horizontal stroke.
References:
Blasco P. Motor delays. In Parker S, Zukerman B, Augustyn M, eds. Developmental and
Behavioral Pediatrics: A Handbook for Primary Care . 2nd ed. Philadelphia, Pa: Lippincott
Williams & Wilkins; 2005:242-247
Feigelman S. The first year. In: Kliegman RM, Behrman RE, Jenson HB, Stanton BF, eds. Nelson
Textbook of Pediatrics . 18th ed. Philadelphia, Pa: Saunders Elsevier; 2007:43-47
Feigelman S. The second year. In: Kliegman RM, Behrman RE, Jenson HB, Stanton BF, eds.
Nelson Textbook of Pediatrics . 18th ed. Philadelphia, Pa: Saunders Elsevier; 2007:48-53
D r _F a q e