01 - update on general medicine - 1 file download
TRANSCRIPT

01 - Update on General Medicine
1. Which of the following is associated with Lyme disease?
a. The infection is carried by mosquito larvae.
b. The infectious pathogen is Borrelia burgdorferi.
c. Nervous system involvement does not occur.
d. All patients present with a typical rash known as erythema chronicum migrans.
2. In relation to HIV infection, the CCRS receptor gene is important because
a. it is required for attachment of HIV to T lymphocytes
b. a defective CCRS gene allows HIV infection to flourish
c. all long-term survivors of HIV infection have the CCRS gene defect
d. CCRS receptor inhibitors have proven ineffective in clinical trials to treat HIV
infection
3. Which of the following is a risk factor for breast cancer?
a. fibrocystic disease
b. first-degree relative with breast cancer
c. late menarche
d. multiple previous pregnancies
4. What is the most effective screening technique for cervical cancer?
a. Fourier transform infrared
b. PCR assay
c. HPV DNA testing
d. Pap smear
5. Which of the following is a component of the 2009 Recommended
Childhood, Adolescent, and Adult Immunization Schedules?
a. Initial hepatitis B immunization should be given between 3 and 4 years of age.
b. DTP (diphtheria and tetanus toxoids and acellular pertussis vaccine) is first
administered at age 6 weeks or older.
c. The first dose of MMR (measles, mumps, rubella) vaccine is given between 4
and 6 months of age.
d. The varicella vaccine should always be given during pregnancy.

6. What is the most important parameter in predicting anaphylaxis?
a. past use of many antibiotics
b. sensitivity to epinephrine
c. sensitivity to hydrocortisone
d. history of previous allergic reactions
7. In patients with shock, what is the most frequent single cause of death?
a. hemorrhage
b. myocardial infarction
c. ventilatory failure
d. sepsis
8. What is the initial consideration in treating status epilepticus?
a. airway maintenance
b. blood glucose levels
c. blood pressure
d. toxicology status
9. Which of the following is a potential adverse effect of anti cytokine drugs
such as etanercept (Enbrel) and infliximab (Remicade)?
a. disc edema
b. angle-closure glaucoma
c. optic neuropathy
d. increased risk of diabetes
10. Which of the following is most effective for treating Wegener
granulomatosis?
a. acetaminophen
b. non steroidal anti-inflammatory agents
c. cyclophosphamide
d. methotrexate
11. Which of the following is a major ocular manifestation of systemic lupus
erythematosus?
a. retinal and choroidal microvascular lesions
b. heliotrope rash of eyelids
c. recurrent unilateral anterior uveitis
d. conjunctivitis

12. The preferred test for diagnosing type 2 diabetes is
a. hemoglobin A1c
b. fasting plasma glucose
c. oral glucose tolerance test
d. urine glucose and ketones
13. Which of the following classes of oral hypoglycemic agents has been
associated with worsening macular edema?
a. sulfonylureas
b. a-glucosidase inhibitors
c. biguanides
d. thiazolidinediones
14. Patients with multiple endocrine neoplasia syndrome type 2B (MEN 2B)
are likely to have which of the following ophthalmic findings?
a. prominent corneal nerves
b. bitemporal hemianopsia
c. exophthalmos
d. hypertensive retinopathy
15. What is currently the main treatment for Parkinson disease?
a. dopamine
b. pramipexole
c. levodopa
d. benztropine
16. Which of the following ophthalmic findings suggests that a patient is
feigning a grand mal seizure:
a. monocular nystagmus
b. gaze deviation
c. eyelid closure
d. diminished saccades
17. Which of the following types of dementia is more likely to present with
formed visual hallucinations
a. Alzheimer's disease
b. Lewy body dementia
c. vascular dementia
d. dementia associated with Parkinson's disease

18. Which of the following is the leading cause of mortality among women in
the United States?
a. atherosclerotic heart disease
b. breast cancer
c. ovarian cancer
d. stroke
19. The first line of treatment in reducing serum cholesterol should be
a. drug therapy
b. aerobic exercise
c. weight loss
d. dietary therapy
20. When LDL goals are not achieved by lifestyle changes alone in a patient
with hypercholesterolemia, what is the next step?
a. begin nicotinic acid
b. begin bile acid sequestrants
c. begin statin medications
d. change the LDL goal
21. Adverse ocular reactions seen with use of digoxin include which of the
following?
a. glare phenomenon and xanthopsia
b. corneal microdeposits
c. keratoconjunctivitis sicca
d. bull's-eye maculopathy
22. Prophylactic implantable cardioverter-defibrillators are indicated
treatment for which of the following groups?
a. patients with chronic atrial fibrillation
b. survivors of a hemodynamically unstable episode of ventricular tachycardia
c. patients not expected to survive more than 6 months regardless of treatment
d. patients without inducible ventricular arrhythmias on electrophysiologic testing

23. The JUPITER study suggests that
a. statins may be of value in patients with normal serum lipid and an elevated C-
reactive protein level
b. statin use may increase the risk of age-related macular degeneration
c. statin therapy is not indicated in patients whose LDL-C has failed to respond to
therapeutic lifestyle changes
d. statins may rarely cause liver failure, rhabdomyolysis, or polyneuropathy
24. The metabolic syndrome is diagnosed on the basis of the presence of a
constellation of findings, including
a. normal fasting glucose
b. elevated HDL (>50 mg/dL)
c. blood pressure of ll0/70 mmHg
d. increased abdominal obesity
25. You suspect that an older patient who presents with a hyphema has been
abused. What is your first step?
a. Call the patient's primary care physician about the suspected abuse.
b. Treat the suspected eye injury and address the nature of the injury on a follow-up
examination, after obtaining further information from the family.
c. Advise the caregiver to watch the patient for unstable balance and possible falls.
d. Complete a written report promptly, document any suspicious injuries, and
report your suspicions to the appropriate authorities.
26. Two months ago, a 90-year-old patient was informed by her
ophthalmologist that her macular degeneration was progressing. At her
follow-up visit, she seemed withdrawn and thin and talked about having lived
too long. The most likely diagnosis is
a. depression
b. fear of living alone, as her spouse just passed away
c. progressive dementia
d. occult malignancy
27. The severity and frequency of falls increase as we age. Which of the
following is the most likely?
a. The older patient who suffers a fall will most likely develop dementia.
b. Traumatic brain injury in older adults is most commonly caused by falls.
c. Vision loss does not affect the incidence of falls in the older population.
d. An older patient who falls should always be taken to an emergency room.
28. Widespread, cost -effective screening is best for diseases that
a. are not treatable or preventable
b. are difficult to diagnose
c. have a high prevalence
d. are very rare
29. Monitoring for hypertension should begin at what age?
a. 3 years
b. 18 years
c. 35 years
d. 40 years, barring suggestive symptoms or signs
30. Carotid end arterectomy has been proven to be of benefit in reducing
stroke following non disabling symptomatic events in patients with which of
the following:
a. ipsilateral 0%-29% carotid artery stenosis
b. ipsilateral 30%-69% carotid artery stenosis
c. ipsilateral 70%- 99% carotid artery stenosis
d. ipsilateral 100% carotid artery stenosis
31. Magnetic resonance imaging is more sensitive than computed tomography
in the diagnosis of which of the following?
a. intracranial hemorrhage
b. early cerebral infarction
c. ischemic stroke
d. transient ischemic attack
32. The single most effective measure that can be instituted to reduce the risk
of chronic obstructive pulmonary disease is
a. weight loss
b. exercise
c. reduction of respiratory infections by hand washing
d. smoking cessation

33. Which of the following is the best test to monitor heparin therapy?
a. prothrombin time
b. partial thromboplastin time
c. bleeding time
d. platelet count
34. If the risk of endophthalmitis is 1% per year in one hospital and 0.01% in
another over a 1-year period, the risk difference is
a. 0.01% over 1 year
b. 100%
c. 100% over 1 year
d. 0.99% over 1 year
35. In a screening test applied to 250 patients, the sensitivity was estimated to
be 80%. If 100 patients have the disease, then how many patients were false-
negatives?
a. 75
b. 180
c. 20
d. 170

Answers
1. b. The infectious pathogen of Lyme disease is Borrelia burgdorferi. The carrier
is the Ixodes genus of tick. Many patients present with erythema chronicum
migrans but not all.
2. a. CCRS is a surface receptor required for the attachment of HIV to
lymphocytes. Patients with a defective CCRS gene have natural immunity to HIV
infection. Approximately 50% of long-term survivors of HIV infection are
heterozygous for the CCRS defect.
3. b. Nulliparity, early menarche, and history of a first-degree relative with breast
cancer are all risk factors for breast cancer. Fibrocystic disease is not a risk factor
for breast cancer.
4. d. The most effective screening technique remains the Papanicolaou test ("Pap
smear").Fourier transform infrared (FTIR) spectroscopy is a new tool for screening
cervical cancer and has a sensitivity of85% and a specificity of91 %. PCR DNA
techniques can be used to help detect concomitant HPV infection.
5. b. The minimum age for administration of DTaP is 6 weeks. The first hepatitis B
immunization should be given at birth, before discharge from the hospital. If the
mother is HBs Ag positive, the infant should receive hepatitis B immunoglobulin
as well. The first dose of MMR (measles, mumps, rubella) vaccine is given
between 12 and 15 months of age. Pregnancy is a contraindication for the varicella
vaccine.
6. d. The most important parameter for predicting anaphylaxis is a history of a
previous allergic reaction to another drug or antigen. The others are not risk factors
for anaphylaxis.
7. c. Ventilatory failure is the most significant factor in the morbidity and mortality
of shock, with subsequent hypoxemia and metabolic acidosis leading to many
complications.
8. a. The airway must be maintained in the treatment of status epilepticus prior to
any other treatment or diagnostic measures.

9. c. Etanercept and infliximab have been associated with demyelinating disease
and optic neuritis. The antiepileptic medication topiramate (Topamax) has been
associated with acute angle-closure glaucoma.
The newer atypical antipsychotic agents, such as olanzapine (Zyprexa) and
clozapine (Clozaril), may be associated with initiating or worsening diabetes.
Cyclosporine (Neoral, Sandimmune) has been associated with disc edema.
10. c. Aspirin and non steroidal anti-inflammatory agents may be helpful in
managing many forms of arthritis and other inflammatory disorders. Methotrexate
is beneficial as a disease-modifying agent for patients with rheumatoid arthritis and
other autoimmune diseases. Wegener granulomatosis is a potentially fatal systemic
disease and usually requires aggressive treatment, including cyclophosphamide and
prednisone.
11. a. Retinal and choroidal microvascular lesions are one of the more common
manifestations of ocular involvement with systemic lupus erythematosus (SLE).
Discoid lesions of the skin of the eyelids and keratitis sicca from secondary Sjogren
syndrome are also common when the eye is involved.
Recurrent unilateral anterior uveitis would be unusual with SLE; it is much more
common with HLA-B27-associated diseases such as ankylosing spondylitis. A
heliotrope rash of the eyelids, although rare, is almost pathognomonic for
dermatomyositis. Autoimmune conjunctivitis can be a feature of reactive arthritis.
12. b. Fasting plasma glucose (FPG) is the preferred test. The oral glucose
tolerance test may be more sensitive than the FPG, but it is not routinely used
because it is costlier, inconvenient, and difficult to reproduce. The hemoglobin A1c
measurement is not currently recommended for diagnosing diabetes, although this
may change when the test becomes more standardized.
Although measuring urine glucose is much easier than measuring blood glucose, it
is not sensitive, because blood glucose levels need to be quite elevated before
glucose appears in urine. Measurement of urinary ketones is useful during periods
of illness or stress, because any positive value suggests the presence of ketonemia;
however, measurement of urinary ketones is not used for the diagnosis of diabetes.
13. d. The thiazolidinediones (rosiglitazone [Avandia] and pioglitazone [Actos])
have been implicated in contributing to macular edema in some patients. They can
also cause fluid retention, and in 2010 the FDA significantly restricted the use of
rosiglitazone because of increased risk of cardiovascular complications.
The most common side effect of the sulfonylureas is hypoglycemia, especially with
the longer-acting agents. A-Glucosidase inhibitors can cause flatulence, which can

limit compliance. The only available biguanide is metformin (Glucophage), and it
has the potential to cause severe lactic acidosis in the setting of renal insufficiency.
The drug should therefore be avoided in patients with early renal disease and
should not be used concomitantly with intravenous contrast agents that can
precipitate renal failure.
14. a. Prominent corneal nerves are reported to occur in 100% of affected patients.
This finding is significant because almost all affected patients will develop
medullary thyroid cancer; however, because this may not appear until the patient's
second or third decade, the ophthalmic manifestations may be the initial indication
that the syndrome is present. Bitemporal hemianopsia can occur with pituitary
tumors, which are part of multiple endocrine neoplasia syndrome type 1 (MEN 1).
Exophthalmos can occur in Graves’s disease but is not part of the spectrum of the
MEN syndromes. Hypertensive retinopathy can occur in patients with
pheochromocytoma, which can be part of MEN 2A and 2B.
15. c. The main treatment is levodopa (L-dopa), which is generally initiated when
symptoms become significant. Usually patients are given levodopa combined with
carbidopa (Lodosyn), often as a combined pill (Sinemet).
Dopamine itself cannot be given because it does not cross the blood-brain barrier.
Pramipexole (Mirapex) stimulates dopamine receptors in the brain and can be
given alone or in combination with levodopa, but it is less effective than levodopa.
Benztropine (Cogentin), an anticholinergic drug, was a common treatment for
Parkinson disease before the introduction of levodopa.
Anti cholinergics may help control tremor and rigidity, although their benefit is
limited and their effect is usually short-lived.
16. c. It is unusual for patients experiencing a genuine seizure to shut their eyes
during the episode, whereas patients who are feigning a seizure often keep their
eyes closed. Patients who are having seizures may commonly have either
horizontal or vertical gaze deviations.
The gaze tends to be directed away from the site of the cortical lesion during a
seizure and then toward the site of the lesion after the seizure. Monocular
nystagmus can occur during the clonic stage of a seizure. Diminished saccadic
movement is a side effect of the anti seizure medication carbamazepine (Tegretol).
17. b. Lewy body dementia is the second most common form of neurodegenerative
dementia after Alzheimer's disease, and patients with this syndrome often present
with complex, formed visual hallucinations. Although there may be considerable
clinical and neuropathologic overlap among the various types of dementia, visual

hallucinations are not routinely a symptom of vascular dementia, Alzheimer's
disease, or dementia associated with Parkinson disease.
18. a. Atherosclerotic coronary artery disease is by far the number one killer of
women and men, not only in the United States but also in the world. It is estimated
that every minute 1 person in the United States dies of coronary artery disease. The
number of women who die from cardiovascular disease is 10 times that from breast
cancer.
19. d. Dietary therapy should be the first line of treatment in reducing serum
cholesterol. Regular aerobic exercise and limited alcohol intake have a beneficial
effect on serum cholesterol by increasing HDL cholesterol. Medications are used
after other modalities such as diet and exercise have not lowered cholesterol
adequately. Weight loss can be associated with a lowering of cholesterol; however,
in and of itself, it is not the first line of treatment for reducing serum cholesterol.
20. c. Statins are the first choice for medical therapy in virtually all patients whose
LDL goals cannot be achieved by therapeutic lifestyle changes alone.
21. a. The glare phenomenon and disturbances of color vision are the most striking
and the most common adverse ocular reactions seen with the use of digoxin.
Corneal microdeposits occur with use of chloroquine and amiodarone.
Keratoconjunctivitis sicca is not a specific side effect of digoxin but may be
observed in patients using ~-blockers. Bull's-eye maculopathy may be a side effect
of chloroquine.
22. b. If a patient is not expected to survive at least 1 year with good functional
status, an implantable cardioverter-defibrillator (ICD) is not recommended under
current ACC/ AHA guidelines. Survival and functional status are improved with an
ICD in the setting of a previous cardiac arrest, hemodynamically unstable
ventricular tachycardia episode, or inducible ventricular arrhythmias on
electrophysiologic testing. ICDs are not indicated for chronic atrial fibrillation.
23. a. Statins are the first choice for medical therapy in patients who have not
achieved LDL goals through therapeutic lifestyle changes (TLC) alone.
The role of statins in relation to the risk of age-related macular degeneration
(AMD) is unclear, but multiple studies suggest a decreased risk, particularly in late
stages of AMD. The JUPITER study suggests that patients with an elevated C-
reactive protein and no hyperlipidemia have a reduced risk of stroke and coronary
artery disease when statins are used.
24. d. Patients with the metabolic syndrome have 3 or more of the following: a
decreased HDL, increased abdominal obesity, elevated triglycerides, hypertension,
and an elevated fasting glucose. Elevated HDL is generally a protective factor,
reducing the risk of cardiovascular events.
25. d. In many states, reporting suspected elder abuse is mandatory. You should be
aware of your state's rules and regulations. Trauma to the eyes can be seen in elder
abuse. If you suspect elder abuse, you need to report this immediately and not wait
until a follow-up appointment. Sometimes the caregiver may be the abuser, and
examining and interviewing the patient alone may alert you to the abuse situation.
26. a. Depression is a very frequent problem in the older population, and loss of
vision often leads to depression. The role of ophthalmologists is to understand the
effects that loss of vision and blindness will have on patients. Be aware of
community resources, such as a vision rehabilitation center, to which the patient
can be referred. Having a staff member in the office who can help the patient
contact such resources can be an invaluable first step.
27. b. Traumatic brain injury in older adults is commonly caused by falls. Fall-
related direct expenses for those over age 65 totaled over $19 billion in 2000 in the
United States. Vision disorders are responsible for 4% of falls. After a fall in an
older adult, he or she may experience depression and loss of mobility, self-
confidence, and independence.
28. c. Ideal diseases to screen for are the ones that are reliably detectable, treatable,
or preventable, progressive (especially if untreated), and generally asymptomatic.
A high, rather than low, prevalence argues in favor of screening. For a rare disease,
screening may not prove cost -effective.
29. a. Evidence suggests that hypertension in the young is more common than
previously recognized and has substantial long-term health consequences. It is
recommended that children older than 3 years who are seen in a medical setting
have their blood pressure measured.
30. c. Carotid end arterectomy is beneficial for symptomatic patients with recent
non disabling carotid artery ischemic events and ipsilateral 70%-99% carotid artery
stenosis. It is not beneficial for symptomatic patients with 0%-29% or 100%
stenosis, and its potential benefit for symptomatic patients with 30%-69% stenosis
is uncertain.

31. b. All suspected cases of stroke and threatened stroke should prompt computed
tomography (CT) of the brain. Computed tomography is very sensitive to the
presence of intracranial hemorrhage.
Magnetic resonance imaging (MRI), however, is often more sensitive than CT in
detecting an evolving stroke within hours of its onset and an early cerebral
infarction; CT results may be negative for up to several days after an acute cerebral
infarct.
32. d. Smoking cessation is the single most effective intervention to reduce the risk
of chronic obstructive pulmonary disease or slow its progression. Ophthalmologists
should not underestimate the impact of discussing the harmful effects of smoking
with their patients.
33. b. Heparin therapy is monitored by the partial thromboplastin time (PTT).
Prothrombin time, or the international normalized ratio (INR), is used to monitor
oral warfarin therapy. Bleeding time reflects platelet count and function. Platelet
abnormalities do not affect the PTT.
34. d. Risk difference is the difference between 2 risk measures and has
dimensions, so the correct answer is option d because 1% per year minus 0.01% per
year is 0.99% per year.
35. c. Sensitivity refers to the proportion of those who have the disease who screen
positive.
If 80% of the 100 who have the disease screened positive, then 20% of those who
have the disease, or 20 out of 100, screened negative.

02 - Fundamentals and Principles of Ophthalmology
1. If all the nerves passing through the annulus of Zinn were transected,
what nerve would continue to function?
a. superior division of cranial nerve III
b. cranial nerve IV
c. nasociliary branch of cranial nerve V (V1)
d. optic nerve
2. Which extra ocular muscle originates from the annulus of Zinn?
a. levator palpebrae superioris
b. superior oblique
c. lateral rectus
d. inferior oblique
3. What is the ratio of optic nerve axons that cross at the optic chiasm to
those that do not cross at the optic chiasm?
a. 67:33
b. 50:50
c. 30:70
d. 53:47
4. A patient presents with left-sided ophthalmoplegia and forehead
numbness. The lesion is most likely to be located at the
a. brainstem
b. cavernous sinus
c. superior orbit
d. intraconal space
5. The first cells to develop in the embryonic retina are the
a. ganglion cells
b. photoreceptors
c. amacrine cells
d. bipolar cells

6. Which disorder is associated with a defect in a non mitochondrial gene?
a. Leber hereditary optic neuropathy
b. chronic progressive external ophthalmoplegia
c. neuropathy, ataxia, and retinitis pigmentosa
d. retinoblastoma
7. What characteristic of retinoblastoma may facilitate its diagnosis as a
familial condition?
a. It may be associated with chromosome 11 short-arm deletion syndrome and
Wilms tumor.
b. It affects approximately 1 per 100,000 live births in the United States.
c. Approximately 90% of patients with hereditary retinoblastoma have a family
history of the disease.
d. The hereditary pattern in familial retinoblastoma is autosomal dominant, but
the defect is mitochondrial at a cellular level.
8. Mutations in the rhodopsin gene are associated with what inherited
ocular disease?
a. juvenile glaucoma
b. Leber hereditary optic neuropathy
c. retinitis pigmentosa
d. Stargardt disease
9. Mitochondrial inheritance is transmitted by what route?
a. paternal mitochondria
b. maternal mitochondria
c. acquired mitochondria
d. de novo mitochondria
10. Mutations of PAX6 are associated with what disorder?
a. aniridia
b. retinal coloboma
c. renal hypoplasia
d. corneal granular dystrophy

11. An unaffected woman has a brother, maternal uncle, and son affected
with retinitis pigmentosa. What is the most likely mode of inheritance?
a. autosomal dominant
b. X-linked recessive
c. autosomal recessive
d. sporadic
12. What is the basis for complex genetic diseases?
a. a single recessive gene
b. X-linked genes
c. a single spontaneous genetic mutation
d. the resultant effect of many genes, in combination with health habits and
environmental factors
13. What structure, if inflamed, would be considered a sign of uveitis?
a. optic nerve
b. Descemet membrane
c. choroid
d. retinal pigment epithelium
14. What pair accurately matches a cell-type origin with the correct tear-
layer product?
a. goblet cells- lipid layer
b. meibomian glands-mucin layer
c. glands of Krause-aqueous layer
d. glands of Wolfring-mucin layer
15. What option most accurately describes the immunoglobulin(s) that can
be found in the tear film?
a. IgA only
b. IgA and IgG only
c. IgG and IgM only
d. IgA, IgG, IgM, and IgD
16. What intraocular structure is a true basement membrane (basal
lamina)?
a. Bowman layer
b. zonule of Zinn
c. Descemet membrane
d. anterior border layer of iris

17. What is the principal structural protein in the Descemet membrane?
a. type I collagen
b. type II collagen
c. type III collagen
d. type IV collagen
18. What mechanism holds the flap created during laser in situ
keratomileusis (LASIK) in place after surgery?
a. endothelial- Descemet membrane interaction
b. endothelial pump
c. Bowman layer- stromal adhesions
d. Stromal collagen adhesions
19. What property of the retina renders it susceptible to oxidative stress?
a. high content of polyunsaturated fatty acids in photoreceptor outer segments
b. high concentration of carotenoids compared with other intraocular structures
c. presence of vitamin E
d. absence of retinal vessels in the foveal avascular zone
20. What pigment within the retinal pigment epithelium is responsible for
the signal generated in fundus auto fluorescence imaging?
a. melanin
b. lipofuscin
c. rhodopsin
d. lutein
21. The retinal pigment epithelium is the first site of melanogenesis in the
body. Ocular melanin has been shown to participate in what process?
a. pathogenesis of retinitis pigmentosa
b. vitamin A metabolism
c. retinal adhesion
d. retinal development and neuronal migration
22. Age-related loss of type IX collagen has been implicated in what process
related to the vitreous?
a. vitreous hemorrhage
b. angiogenesis
c. increased diffusion of oxygen from the anterior segment into the posterior
segment
d. vitreous liquefaction

23. What vitamin is most critical for the photoreceptor response to light?
a. A
b. B
c. C
d. E
24. In prescribing for elderly patients, what pharmacologic adjustments
must be considered?
a. Hepatic perfusion and enzymatic activity increase with age.
b. Renal function decreases with age.
c. Elderly patients have more albumin relative to weight.
d. Elderly patients have more body water relative to weight.
25. What technique or strategy improves the ocular absorption of eye
drops?
a. rapid instillation of eye drops one after the other without interruption
b. application of digital pressure at the lateral canthus to prevent the eye drop
from escaping
c. keeping the eye open and rolling the eye around after instillation of each drop
d. increasing the viscosity of the delivery vehicle
26. Atropine, 1%, has how many milligrams of drug per drop, assuming 20
drops per milliliter?
a. 1 mg
b. 0.5 mg
c. 0.1 mg
d. 0.05 mg
27. How much epinephrine is present in 1 mL of the 1:10,000 epinephrine
solution?
a. 1 mg of epinephrine
b. same amount of epinephrine as in 1 mL of 0.01% epinephrine
c. same amount of epinephrine as in 1 mL of 1:1000 epinephrine
d. same amount of epinephrine as in 1 mL of 0.1% epinephrine
28. Direct-acting muscarinic agents (miotics) have what clinical effect?
a. hyperopic shift in refraction
b. increased range of accommodation
c. central anterior chamber deepening
d. increased night vision

29. What management strategy has been shown to reduce postsurgical
endophthalmitis?
a. preoperative preparation of the eye with topical povidone-iodine
b. intracameral vancomycin
c. intracameral aminoglycosides
d. subconjunctival fluoroquinolones
30. What property of latanoprost may limit its usefulness?
a. It is a pro drug of prostaglandin E20.
b. It reduces intraocular pressure by increasing trabecular meshwork outflow.
c. It can cause darkening of the iris and periocular skin and hypertrichosis of the
eyelashes.
d. It increases the number of melanocytes.
31. What systemic side effect may result from treatment with oral carbonic
anhydrase inhibitors?
a. insomnia
b. weight gain
c. hyperkalemia
d. aplastic anemia
32. What is a clinically important property of brimonidine?
a. Brimonidine is a selective a 1-adrenergic agonist.
b. Brimonidine is more lipophilic than apraclonidine.
c. Brimonidine has been associated with tachycardia and hyperventilation when
used in infants.
d. Rates of tachyphylaxis and allergic reaction are higher in brimonidine than in
apraclonidine.

Answers
1. b. Cranial nerve IV passes through the superior orbital fissure but not through
the annulus Of Zinn.
2. c. The lateral rectus muscle originates from the annulus of Zinn. The superior,
inferior, medial, and lateral rectus muscles all arise from the annulus of Zinn.
3. d. Anatomical studies demonstrate that more axonal fibers cross at the optic
chiasm than do not cross, in a 53:47 ratio.
4. b. The cavernous sinus is where the trigeminal nerve (ophthalmic branch) and
the nerves controlling eye movement are in proximity to one another.
5. a. The ganglion cells are the first cells to differentiate in the embryonic eye.
6. d. The hereditary pattern in familial retinoblastoma is autosomal dominant and
associated with a mutation in the nuclear tumor-suppressor gene on chromosome
13 (the retinoblastoma, or RBl, gene). The other conditions named have been
associated with mutations in mitochondrial genes.
7. c. The retinoblastoma gene is located on the long arm of chromosome 13. The
aniridia gene, PAX6, and the Wilms tumor gene are adjacent on chromosome 11;
their proximity is important to recognize, as children with aniridia need to be
screened for Wilms tumor.
Retinoblastoma occurs at a rate of approximately 1 per 15,000-20,000 li\e births.
Most cases of retinoblastoma are unilateral and not inherited. Of people who
inherit the gene mutation, 90% will develop retinoblastoma (90% penetrance).
8. c. More than 100 different mutations in the rhodopsin gene are known to cause
retinitis pigmentosa. Juvenile glaucoma is associated with myocilin mutations,
Leber hereditary optic neuropathy is associated with mitochondrial DNA
mutations, and Stargardt disease is associated with ABCA4 gene mutations.
9. b. A significant number of disorders associated with the eye or visual system
involve mitochondrial deletions or mutations. Because a fertilized embryo
receives most of its mitochondria from the egg (maternal side), mitochondrial
disease should be considered whenever the inheritance pattern of a trait suggests
maternal transmission.

10. a. A PAX6 mutation is associated with aniridia. The PAX6 gene product is a
transcription factor that is required for normal development of the eye. Almost
all cases of aniridia are the result of PAX6 mutations.
11. b. Three affected males connected through an unaffected female suggest an
X-linked inheritance. The other modes are possible but much less likely.
12. d. Many common eye diseases are complex genetic diseases involving the
effects of multiple genes. Examples include glaucoma, age-related macular
degeneration, and myopia.
The combined effects of many genes, along with health habits and environmental
factors, result in the disease.
13. c. The optic nerve, cornea, and retinal pigment epithelium are not part of the
uvea. The uveal tract is the main vascular compartment of the eye and consists of
the iris, ciliary body, and choroid.
14. c. Goblet cells produce the mucin layer, and meibomian glands form the lipid
layer. Glands of Krause and Wolfring produce the aqueous layer.
15. d. Proteins in the tear film include immunoglobulin A (IgA) and secretory
IgA (sigA). IgA is formed by plasma cells in interstitial tissues of the main and
accessory lacrimal glands and by the substantia propria of the conjunctiva. The
secretory component is produced within lacrimal gland acini, and sigA is
secreted into the lumen of the main and accessory lacrimal glands. IgA plays a
role in local host -defense mechanisms of the external eye, as shown by
increased levels of IgA and IgG in human tears associated with ocular
Inflammation. Other immunoglobulins in tears are IgM, IgD, and IgE. Vernal
conjunctivitis causes elevated tear and serum levels of IgE, increased IgE-
producing plasma cells in the giant papillae of the superior tarsal conjunctiva,
and elevated histamine levels.
16. c. The Descemet membrane is a true basement membrane produced by the
basolateral surfaces of the basal layer of the corneal endothelium.
17. d. The Descemet membrane is a 10-12-f.Lm-thick basement membrane
between the endothelium and the posterior corneal stroma. Type IV collagen is
the most abundant collagen in the Descemet membrane. Type I collagen,
however, is the major collagen component of the corneal stroma.

18. b. The endothelial pump is responsible for generating the negative
hydrostatic pressure that is necessary for holding the laser in situ keratomileusis
(LASIK) flap in place after surgery.
19. a. polyunsaturated fatty acids have increased numbers of carbon-carbon
double bonds, which enhances their susceptibility to lipid peroxidation.
Other aspects of the retina that increase its susceptibility to oxidative stress
include an increased concentration of mitochondria, a high oxygen tension, and
photo-oxidation triggered by light exposure.
20. b. Lipofuscin molecules are the fine yellow-brown pigment granules of the
retina. They are thought to be "wear-and-tear" deposits resulting from
phagosomal activity. Histologically, lipofuscin stains with Sudan stain and
exhibits auto fluorescence.
21. d. Melanin acts as a neutral-density filter on all wavelengths of light. Patients
with oculo cutaneous albinism have foveal hypoplasia and more contralateral
projections of the retinal ganglion cells, thought to be due to reduced melanin
levels resulting from defects in the tyrosinase gene. Additional functions of
melanin include stabilization of free radicals and detoxification.
22. d. Vitreous liquefaction, also known as syneresis, begins with the breakdown
of collagen fibrils into smaller fragments. This liquefaction is thought to occur
because of a loss of "shielding" of type II collagen by type IX collagen. This
process has no direct effect on the development of vitreous hemorrhage unless it
leads to the development of posterior vitreous detachment (PVD).
A PVD can protect against retinal neovascularization by eliminating the scaffold
for fibrovascular proliferation. Oxygen tension increases in the posterior
chamber in post vitrectomized eyes.
23. a. 11-cis-retinal is a vitamin A derivative. Vitamins C and E play antioxidant
roles in the retina but do not participate in the light response of the retina.
24. b. Compared with younger patients, older patients have less lean body mass
because of decreased muscle bulk, less body water, decreased albumin, and
increased relative adipose tissue. These physiologic differences alter tissue
binding and drug distribution.
Human renal function decreases with age. Hepatic perfusion and enzymatic
activity decrease with age.

25. d. Increased viscosity of the vehicle generally increases drug retention in the
inferior culde-sac, aiding drug penetration.
26. b. A 1% solution has 1 g/ 100 mL, or 1000 mg/ 100 mL, of active ingredient.
Assuming there are 20 drops/mL, 1 drop contains 0.05 mL of drug. Multiplying
1000 mg/100 mL x 0.05 mL yields 0.5 mg per drop of atropine available for
systemic absorption.
27. b. A 1:10,000 dilution has 1 g of drug in 10,000 mL (or 1000 mg/10,000
mL). This concentration is equivalent to a 0.01% solution (0.01 g/100 mL, or 10
mg/100 mL). One milliliter of the 1:10,000 dilution of epinephrine contains 0.1
mg of epinephrine. If the concentration of the solution increases to 1:1000, 0.1
mL of it contains the same amount of epinephrine as in 1 mL of the 1:10,000
solutions.
28. b. Miotic agents constrict the pupillary sphincter and the ciliary muscle.
Ciliary muscle contraction results in increased myopia and a decreased central
anterior chamber. Pupillary constriction causes decreased night vision but
increases the range of accommodation (pinhole effect).
29. a. Topical povidone-iodine solution, 5%, exhibits broad-spectrum
antimicrobial activity when used to prepare the surgical field and rinse the ocular
surface. It has been shown to have a significant effect on postsurgical
endophthalmitis.
30. c. Latanoprost is a prodrug of prostaglandin F2a that reduces the intraocular
pressure primarily by increasing the uveoscleral outflow. It increases the number
of melanosomes (increased melanin content, or melanogenesis) within the
melanocytes but has not been shown to cause melanocytosis (increased number
of melanocytes).
31. d. Use of oral carbonic anhydrase inhibitors can cause paresthesias,
imbalance, anorexia, weight loss, hypokalemia, somnolence, kidney stones,
metabolic acidosis, and aplastic anemia.
32. b. Brimonidine is a selective a2-adrenergic agonist. It is more lipophilic than
apraclonidine and penetrates the blood- brain barrier better. Its use in infants is
contraindicated, and it should be used with caution in small children because of
severe systemic toxicities, in particular bradycardia and apnea. Brimonidine has
lower rates of tachyphylaxis and allergic reaction than apraclonidine.

03 - Clinical Optics
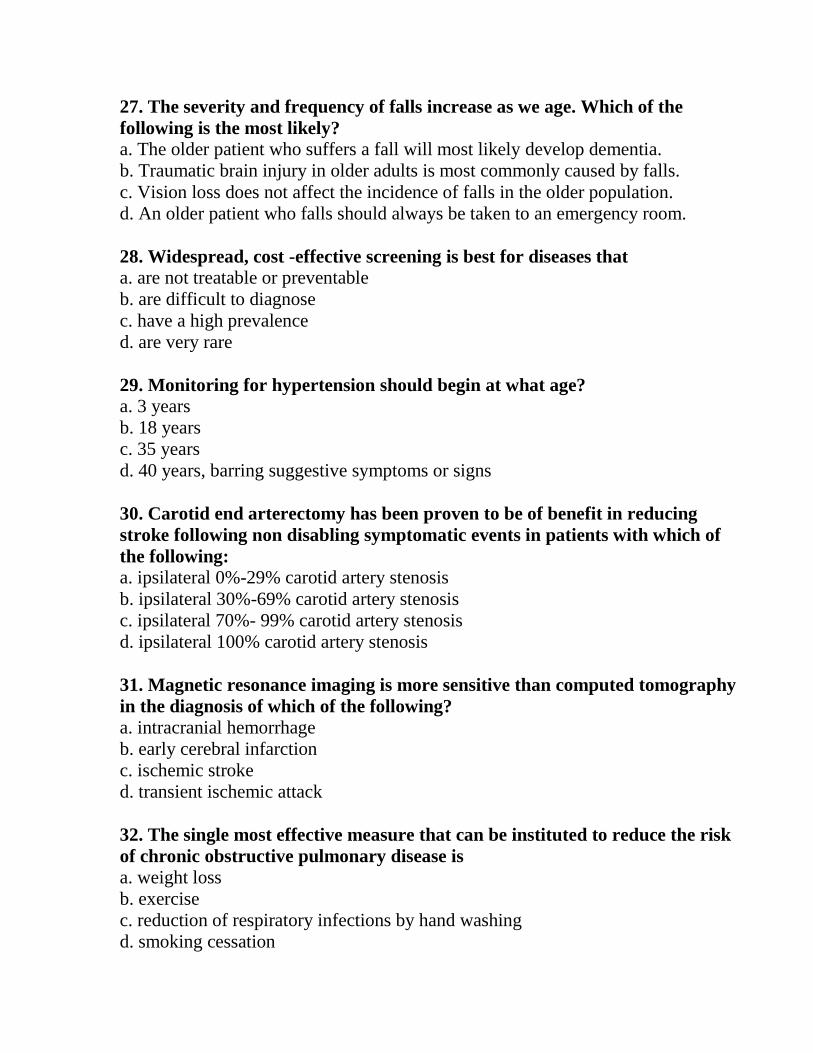
Questions 1-6 refer to the figure above. An object is 1. 0 m to the left of a -1.00
D thin lens.
The -1.00 D lens is, in turn, 1.5 m to the left of a +1.50 D thin lens.
1. Where is the (intermediate) image formed by the first lens?
a. 2.0 m to the right of the lens
b. 0.5 m to the right of the lens
c. 0.5 m to the left of the lens
d. 2.0 m to the left of the lens
2. What are the characteristics (e.g., real or virtual, upright or inverted, and
transverse magnification) of the intermediate image?
a. upright, real, enlarged
b. inverted, real, reduced
c. upright, virtual, enlarged
d. upright, virtual, reduced
3. What is the size of the intermediate image compared with the object?
a. one-fourth the size
b. one-half the size
c. same size
d. twice the size

4. What is the location of the final image?
a. 1.0 m to the left of the second lens
b. 1.0 m to the right of the second lens
c. 4.0 m to the right of the second lens
d. at optical infinity
5. What are the characteristics (e.g., orientation, real or virtual, and
transverse magnification) of the final image compared with the original
object?
a. upright, real, enlarged
b. upright, real, reduced
c. inverted, real, enlarged
d. inverted, real, reduced
6. What is the size of the final image compared with the original object?
a. one-fourth the size
b. one-half the size
c. same size
d. twice the size
7. An object is placed 50 cm in front of a concave spherical mirror with a
radius of curvature of 2.0 m. What is the transverse magnification of the
image, and is it real or virtual?
a. virtual with a transverse magnification of +2X
b. virtual with a transverse magnification of -2x
c. real with a transverse magnification of -0.5x
d. real with a transverse magnification of +0.5x
8. Which of the following statements is true about the derivation of
intraocular lens (IOL) formulas using geometric optics?
a. The index of refraction of the IOL is ignored because it does not differ
significantly from that of the aqueous and vitreous.
b. The refractive contribution of the cornea may be neglected because the light
reaches the IOL plane after it has already passed through the corneal surface.
c. The formula for change of vergence with change in implant location must be
modified because of the index of refraction of the aqueous.
d. The anterior chamber depth may be neglected because studies have shown a
negligible increase in accuracy if it is included in power calculations.

9. Which of the following statements is correct regarding the segment choice
when prescribing bifocals for a patient with hyperopia?
a. The practitioner should leave the choice of the segment type to the optician.
b. A round-top segment is preferred because it lessens image jump.
c. A flat-top segment is preferred because of its thin upper edge, which causes
less prismatic effect.
d. The use of a round-top segment reduces the prismatic displacement effect and
increases image jump.
10. A child has a cycloplegic refraction OD +6.00 D, OS +2.00 D. What is the
best way to manage the anisometropia?
a. full correction
b. partial correction
c. pleoptic therapy
d. occlusion therapy
11. If a cornea has an anterior radius of curvature of 7.7 mm, a posterior
radius of curvature of 6.8 mm, and a center thickness of 0.5 mm, what will
its dioptric power be if it is submerged in water? Assume index of refraction
of water = 1.333; index of refraction of cornea= 1.376; index of refraction of
aqueous= 1.336.
a. -5.89 D
b. -0.30 D
c. +32.00 D
d. +37.60 D
12. Why is there no anterior chamber depth term in the SRK equation?
a. The formula was specifically designed to eliminate the need for this
measurement.
b. Regression analysis did not show increased accuracy when anterior chamber
depth was included in the IOL formula.
c. Modern IOLs are all designed to have about the same anterior chamber depth.
d. The postoperative anterior chamber depth is not necessarily the same as the
measured preoperative anterior chamber depth.

13. The ability of a light wave from a laser to form stable interference
fringes with another wave from the same beam, separated in time, is an
illustration of what property?
a. temporal coherence
b. spatial coherence
c. dispersion
d. intensity
14. Proper medical management of a patient with bilateral dry macular
degeneration and recent visual deterioration to the "legal blindness" level
(20/200) should include which of the following options?
a. a l0x magnifier for reading
b. referral to an orientation and mobility specialist
c. a spectacle prescription for prismatic half-glass readers
d. a 10.00 D magnifier for reading
15. How much does a 15^ prism bend light, in degrees?
a. 5.55°
b. 8.53°
c. 15.00°
d. 30.00°
16. The anterior and posterior focal points of a thin lens are located at
different distances from the lens. Additionally, the nodal points of the lens
do not correspond with the principal points. Which of the following
statements is true?
a. This situation is not possible as described.
b. The optical characteristics described are found only in thick-lens or multi-
element systems.
c. Media of different refractive indices bound the lens.
d. Two separated principal planes must be used to define the lens
mathematically.
17. Which of the following characteristics is a property of all ophthalmic
lasers?
a. a plasma active medium
b. high efficiency
c. stimulated emission
d. continuous wave operation

18. Which of the following properties of light is used by the scanning laser
polarimeter to measure nerve fiber layer thickness?
a. focal spot size
b. power level
c. pulse duration
d. polarization
19. Which of the following statements about dispersion and chromatic
aberration is correct?
a. In the human eye, blue rays focus behind red rays.
b. Red print appears nearer than blue print when both are displayed against a
black background.
c. Image sharpness is improved by chromatic aberration in the eyes of patients
with achromatopsia.
d. Blue-blocking and red-blocking sunglasses improve image sharpness by
eliminating part of the chromatic interval, thereby reducing chromatic aberration.
20. A Snellen visual acuity of20/20 is equivalent to which of the following log
MAR values?
a. 1.00
b. 0.00
c. 10.00
d. 0.10
21. A cycloplegic streak retinoscopy is performed on a nonverbal, adult
patient at a testing distance of 67 cm. The result for the right eye is as
follows: +3D sphere neutralizes the reflex when the streak is horizontal
(180°); +4 D sphere neutralizes the reflex when the streak is vertical (90°).
Which of the following refractions is correct for the right eye?
a. + 1.50 sphere + 1.00 x 90
b. + 1.50 sphere -1.00 x 90
c. +3.00 sphere +1.00 x 90
d. +3 .00 sphere - 1.00 x 90

22. Which of the following statements correctly describes the relationship
between intraocular lens (IOL) implant power, axial length, and corneal
power?
a. The IOL power should be increased as the power of the cornea increases and
the axial length increases.
b. The IOL power should be increased as the power of the cornea decreases and
the axial length increases.
c. The IOL power should be increased as the power of the cornea increases and
the axial length decreases.
d. The IOL power should be increased as the power of the cornea decreases and
the axial length decreases.
23. Which of the following statements about astronomical telescopes is true?
a. The astronomical telescope always produces an inverted image.
b. The principal planes of an astronomical telescope coincide with the objective
lens and eyepiece.
c. The tube length of an astronomical telescope with a +4.00 D objective and a +
10.00 D eyepiece is 35 cm.
d. The angular magnification of an astronomical telescope with +4.00 D
objective and a + 10.00 D eyepiece is 4x.
24. Which of the following statements about keratometers is true?
a. They measure the radius of curvature of the central cornea.
b. The size of the mires depends on the corneal refractive index.
c. They measure the dimensions of a virtual image in specific meridians.
d. They measure the refractive power of the cornea.
25. Which of the following statements about the prescription of visual aids is
true?
a. The Kestenbaum rule provides an endpoint to determine the addition required
to read 1M type.
b. Base-in prisms increase effective magnification for binocular patients using
reading spectacles.
c. Illuminated stand magnifiers help overcome stability and lighting problems
associated with higher-power magnification.
d. Optical magnification is sufficient for patients with severely reduced contrast
sensitivity.

26. Which of the following conditions best characterizes a person with low
vision?
a. a bitemporal hemianopia
b. best -corrected visual acuity of 20/70 or worse
c. myopia greater than -20 D
d. a disability related to visual dysfunction
27. Which of the following components is part of an optical coherence
tomography (OCT) system?
a. laser light source
b. beam splitter
c. double pinhole
d. split prism
28. Which of the following adjustments can improve binocular visualization
when examining an eye with small pupils using a head-mounted, binocular
indirect ophthalmoscope?
a. moving the ophthalmoscope's mirror away from the observer
b. narrowing the observer's effective inter pupillary distance
c. diverging the examiner's eyes slightly
d. reducing the distance between the observer's head and the patient
29. A 92-year-old patient with dry age-related macular degeneration reports
deteriorating vision in l eye. Best-corrected visual acuity 12 months earlier
was 20/30. With the same spectacle correction, it is now 20/100. Attempted
refinement of the manifest refraction using ±0.50 D spherical lenses and a
±0.50 D Jackson cross cylinder elicits no change in the refraction. What is
the next step?
a. Perform a darkroom pinhole test.
b. Repeat the manifest refraction using larger step changes in sphere and cylinder
( e.g., a ±0.75 D or ±1.00 D change in sphere and a ±0.75 D or ±1.00 D Jackson
cross cylinder).
c. Perform a slit-lamp examination for cataract or other media opacity.
d. Dilate the pupil and examine for a choroidal neo vascular membrane.

30. Which of the following statements describes the nodal points of the
reduced schematic eye?
a. They represent the points through which light rays enter or leave the eye
undeviated.
b. They are equivalent to the posterior focal point of the cornea.
c. They allow the size of a retinal image to be calculated if the object height is
known.
d. The nodal points of the reduced schematic eye coincide, and they are located
6.5 mm posterior to the corneal surface.
31. Which of the following statements correctly describes the far point of the
non accommodated -4.00 D myopic eye?
a. The far point and the fovea are conjugate points.
b. The far point is 25 cm posterior to the eye.
c. The far point is 20 cm in front of the eye.
d. The far point is nearer to the eye than is the point of focus of the fully
accommodated eye.
32. Which of the following statements describes the near point of a fully
accommodated young hyperopic eye in which the amplitude of
accommodation is greater than the amount of hyperopia?
a. The near point is beyond plus infinity.
b. The near point is between plus infinity and the cornea.
c. The near point is behind the eye.
d. The near point is beyond minus infinity, optically speaking.
33. Which of the following pairs is matched correctly?
a. diopter-meter
b. prism diopter-meters per centimeter
c. refractive index-meters per second
d. wavelength- nanometers

34. Which of the following statements about irregular astigmatism is true?
a. Manifest refraction and automated refraction rarely differ significantly in the
presence of large amounts of irregular astigmatism.
b. Irregular astigmatism is best treated with soft contact lenses.
c. Irregular astigmatism may be induced by a decentered refractive surgical
procedure, pellucid marginal degeneration, or keratoconus.
d. Best -corrected visual acuity is usually better with spectacles than with rigid
gas-permeable contact lenses in patients with large amounts of irregular corneal
astigmatism.
35. Which of the following factors increases the risk of infection in a patient
using extended wear contact lenses?
a. switching to daily-wear lenses
b. exposure to smoke
c. normal eyelid function
d. intact corneal epithelium
36. Which of the following statements concerning a patient with a central
scotoma is true?
a. Most patients will fixate using the central foveal location, the preferred retinal
locus (PRL) .
b. The location, shape, and number of scotomata variably affect visual function.
c. Eccentric fixation and PRL training are of no value in helping a patient
improve coordination, tracking, and scanning.
d. Reading is usually not possible because central macular function is required to
read.
37. Which of the following conditions typically affects central vision more
than the peripheral visual field?
a. retinitis pigmentosa
b. age-related macular degeneration
c. retinal detachment
d. panretinal photocoagulation
38. Which of the following statements about the entrance pupil of the eye is
true?
a. It is the pupil we see when we look at a patient's eye.
b. It is the image formed by the lens of the anatomic pupil.
c. It is located 0.5 mm posterior to the anatomic pupil.
d. It is 10%-15% smaller than the anatomic pupil.

39. What is the Brewster angle when light travels from air to glass (n =
1.500)?
a. 65.7°
b. 47.6°
c. 56.3°
d. 41.8°
40. What is the critical angle for light traveling from glass (n = 1.500) to air?
a. 65.7°
b. 47.6°
c. 56.7°
d. 41.8°

Answers
1. c. Vergence is the ratio of refractive index, n, divided by the distance from the
object or to the image. Vergence (in diopters) = n/distance (in meters). Vergence
is negative for divergent light and positive for convergent light. In this case, the
lenses are in air, for which the refractive index, n, is 1.000. Light diverges from
the object so the vergence is negative.
The object is 1.0 m from the lens and therefore has a vergence of -1.00 D = -
1.000/ 1.0 m = -1.00 D. The first lens adds an additional -1.00 D of vergence.
Light leaving the lens, therefore, has a vergence of -2.00 D. Light rays with a
vergence of -2.00 D appear to be coming from a point 0.5 m to the left of the
lens.
2. d. The terms anterior focal point and posterior focal point can be confusing
because, for minus lenses, the anterior focal point is actually behind the posterior
focal point. The anterior focal point, F., is always in object space, and the
posterior focal point, FP, is always in image space. By convention, primed letters
indicate image space and unprimed letters, object space. Often, the anterior focal
point is designated F and the posterior focal point, F'. For a -1.00 D thin lens in
air, F is 1.0 m behind the lens, and F' is 1.0 min front of the lens. For all thin
lenses, the principal planes coincide. Likewise, the nodal points coincide.
The image features can be determined graphically, as shown in the figure below.
A ray from the tip of the object directed to F exits the lens parallel to the optical
axis. A ray from the tip of the object parallel to the axis exits the lens divergent,
as if it had come from F'.
A ray from the tip of the object directed to the nodal points exits undeviated and,
in this case, undisplaced, as shown in black below. The image characteristics-
upright, virtual, and reduced-are apparent from this graphical approach
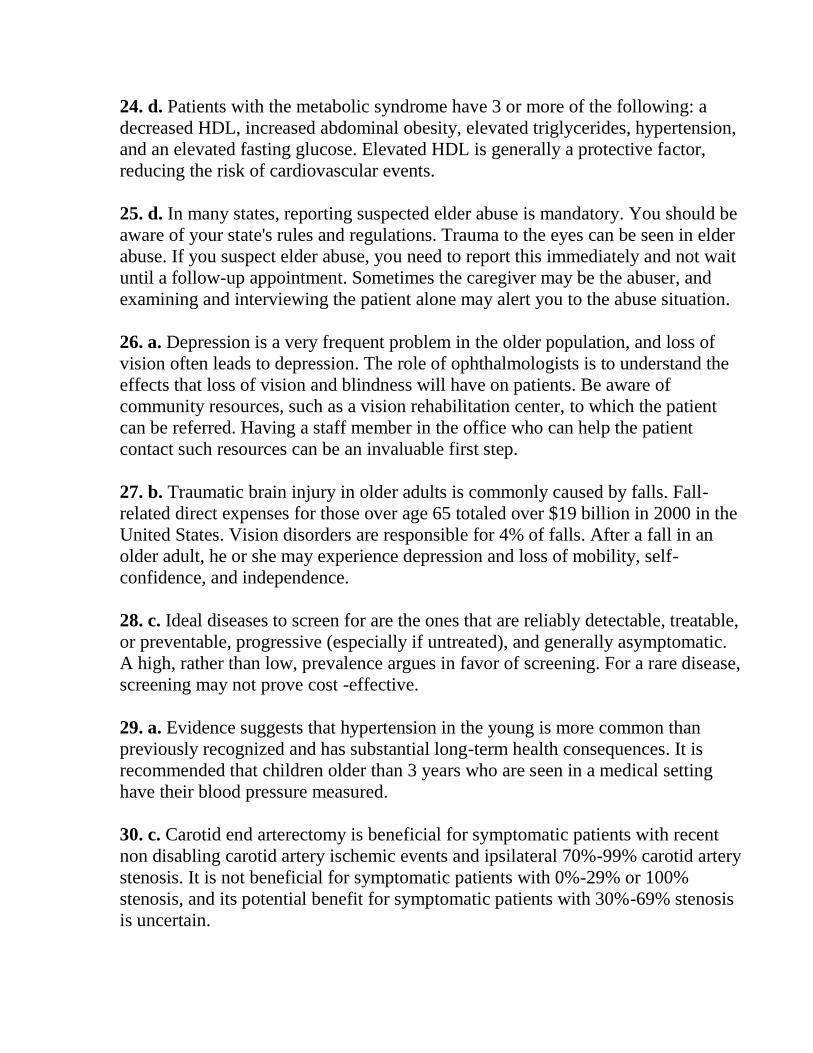
3. b. Using only the ray traversing the nodal points and similar triangles, the
height of the intermediate image is found to be one-half the height of the object
(see figure on the next page). The transverse magnification is +0.5x
4. b. To answer questions 4-6, we treat the intermediate image as the object for
the second lens. From this point on, the first lens can be ignored.
The intermediate image is 2.0 m to the left of the second lens. The vergence of
light entering the second lens is, therefore, -0.50 D. The lens adds+ 1.50 D of
vergence. Therefore, the light exiting the lens has avergence of+ 1.00 D. Light
rays with a vergence of+ 1.00 D come to a focus 1.0 m to the right of the second
lens.
5. d. For the second lens F' is 2/3 m (0.66 m) to the right of the lens, and F is
0.66 m to the left of the lens. Rays can be traced as before. A ray passing from

the object tip parallel to the axis emerges as a ray going through F'. A ray
through F emerges parallel to the axis. A ray through the coincident nodal points
is undeviated and undisplaced.
The image is inverted compared with both the intermediate object and the
original object, is real, and is half the size of the intermediate image and
therefore is also smaller than the original object.
6. a. By similar triangles, the image is half the size of the intermediate image.
The intermediate image is half the size of the object. Consequently, the final
image is (1/2)(1/2) = 1/4 the size of the original object.
7. a. The power of a mirror is 2/r, or in this case, + 1.00 D. The object vergence
is -2.00 D, so the image vergence is -1.00 D. Therefore, the image is virtual and
1.0 m behind the mirror. The image is upright, and the transverse magnification
is + 2x, as shown in the figure

8. c. The intraocular lens (IOL) must, of course, have an index of refraction
different from that of the aqueous and vitreous for it to have any significant
refractive effect. The refractive contribution of the cornea must not be neglected;
in fact, it must be specifically considered. The IOL must provide only the
vergence that is still required at the IOL plane, which is the total vergence
required minus that already provided (at the IOL plane) by the cornea. Although
the anterior chamber depth appears to have little importance in regression-
derived formulas, it is essential in formulas based on geometric optics. The
formula for the change in vergence with change in location is the familiar P/(1-
Pd), where a vergence of power P is moved a distance d. If the refractive index,
n, of the material is not 1, a "reduced distance" of din must be substituted.
9. d. In general, patients perceive image jump as more of a problem than they do
image displacement. Flat-top segments minimize image jump because the optical
center is near the top. In patients with hyperopia, round-top segments reduce
prism displacement because the base-up effect of the distance portion is reduced
by the base-down effect of the segment.
10. a. In children still developing binocularity, a little anisometropia can lead to
a large amblyopia. Anisometropic amblyopia is a fairly common entity and
easily missed because the strabismic cosmetic defect is often absent. Full
correction of the anisometropia may lead to improvement of visual acuity.
Treatment of amblyopia after full correction is total occlusion of the better eye.
Better yet, amblyopia should be prevented by providing the best optical focus for
each eye and the best potential for binocular vision. The younger the child, the
more likely that full correction will prevent amblyopia. In large anisometropia,
particularly in older children, contact lenses are necessary to overcome the large
imagesize difference. Pleoptics has no place in the treatment of anisometropia
per se.
11. b. The power of any rotationally symmetric refracting surface is given by the
equation
Where r is the radius of curvature at the vertex.

For the anterior corneal surface, n2 is 1.376 (cornea) and n1 is 1.333 (water). P1,
the power of the anterior surface under water,
For the posterior corneal surface, n2 is 1.336 (aqueous humor) and n1 is 1.376
(cornea).
The total power of a cornea of thickness t = 0.0005 m submerged in water is
calculated using the equation for the total power of 2 optical systems separated
by distance t:
It is apparent from this calculation that the cornea has a slight diverging
(negative) refracting power under water. In this environment, the crystalline lens
has more converging power than the cornea in the average eye. This explains
why things appear blurry when you open your eyes under water if you are not
wearing goggles.
12. b. No optical principles were used to derive the SRK formula. Rather, it was
derived using only statistical methods, specifically by using linear regression
based on a large number of cases with anterior chamber IOL implants. During
development, the formula included terms for (preoperative) axial length, average
K readings, and anterior chamber depth (ACD). The statistical correlation
between preoperative ACD and IOL power was very weak, so the ACD term did
not significantly enhance accuracy, and it was dropped from the final formula.
The SRK formula was not intended to eliminate the need for an ACD
measurement; the measurement was simply found to be unnecessary. With the
introduction of posterior chamber IOLs, it was found that the SRK formula still
worked well provided that the A constant was modified for different implant

designs. Although adjusting the A constant is perhaps not the best way to adjust
for variations in ACD, it is sufficiently accurate for clinical purposes. Option c is
incorrect because, clearly, all IOLs are not intended to have the same ACD.
Option d is not the best choice for subtle reasons. The preoperative ACD
certainly differs from the postoperative ACD, but the question is not
whether the measurements differ, but rather whether the preoperative ACD
statistically correlates with IOL power. The preoperative and postoperative
ACDs can differ and yet the preoperative ACD may still correlate statistically
with IOL power. The reason the SRK formula contains no ACD term is not
because the preoperative and postoperative ACDs differ but because preoperative
ACD does not correlate with IOL power.
13. a. To observe stable interference patterns, it is necessary for the 2 interfering
wavefronts to have a stable phase relationship. Light consists of a series of wave
trains, and each wave train has a dominant frequency. Stable interference can be
achieved as long as 2 identical wave trains partially overlap. For instance, in the
Michaelson interferometer, light travels slightly different path lengths, and
therefore the 2 interfering wavefronts arise from the same beam but at different
times. If the time difference is small, identical wave trains still partially overlap
and stable interference is observed. If the time difference is too large, different
wave trains overlap and no interference is observable. Spatial coherence refers
to the physical extent of the light source and the presence or absence of a fixed
phase relationship between different parts of a light source. Dispersion refers to
the variation of refractive index with frequency and is unrelated to interference.
Intensity refers, roughly speaking, to the brightness of a source and again is
unrelated to interference
14. d. In the United States and Canada, legal blindness is defined as visual acuity
in the better eye of 20/200 or worse. This level corresponds to severe low vision,
in which the patient's reading speed is slowed despite use of monocular reading
aids (not binocular prismatic glasses). Using the Kestenbaum rule, the dioptric
power of the add is the reciprocal of the visual acuity fraction. Thus, a 10.00 D
lens, not a l0x magnifier (a 40.00 D lens), would be the most appropriate aid.
Referral to an orientation and mobility specialist is usually not needed until the
profound low vision range (20/500-20/100) is reached.
15. b. A useful rule of thumb is that for small angles, a prism diopter produces a
little more than half a degree of deviation. Thus, a 15~ prism produces slightly
more than 7.5° of deviation, so the only reasonable choice is option b.
alternatively, the exact value can be calculated. A 15~ prism deflects light 15 cm

at a distance of 100 cm. The tangent of the angle of the deflection is 15/100; the
angle, therefore, is arctan (0.15) = 8.53°.
16. c. Although a thick-lens or multi-element lens system could have the features
described, the lens in the question is thin. By definition, the principal planes and
nodal points coincide when media with different refractive indices surround a
lens; however, the anterior and posterior focal lengths are different. The nodal
points shift in the direction of the medium with the higher refractive index.
17. c. Laser light is created when atoms of an active medium are exposed to a
source of energy (the pumping source). This introduction of energy causes most
of the active medium's electrons to rise to a higher energy state, a condition
called population inversion. Some of these high-energy electrons undergo
spontaneous emission, generating photons. If these photons first encounter low-
energy electrons, they are merely absorbed. However, if they encounter other
high -energy electrons, stimulated emission occurs. In order to maintain
the chain reaction of stimulated emissions, mirrors are placed at each end of the
cavity, an optical feedback arrangement. One mirror reflects totally and the other
partially. Most of the coherent light generated is reflected back into the ca ity to
produce more stimulated emissions. The relatively small amount of light that is
allowed to pass through the partially reflecting mirror produces the actual laser
beam.
18. d. The nerve fiber layer is birefringent, meaning it polarizes light or changes
the polarization of incident light that passes through it. The scanning laser
polarimeter uses this property to measure nerve fiber layer thickness. The cornea
also polarizes light, so a corneal compensator is necessary to eliminate the
cornea's polarization effects.
19. b. Because red rays focus behind blue rays, the eye must make an
accommodative effort to focus on red print after looking at blue print. It must
relax accommodation to focus on blue print after looking at red print. The brain
therefore perceives that the red print is in front of the blue print when both are
displayed against the same background. Achromatopsia or any other color defect
affects the way the retinal image is converted into nerve impulses but has no
effect on the quality of the retinal image, which is determined solely by the
ocular media.
20. b. Log MAR is calculated by taking the logarithm of the reciprocal of the
Snellen fraction. For instance, if the Snellen visual acuity is 20/200, then the

reciprocal is 200/20, or 10, and the logarithm of 10 is 1. Likewise, for a 20/20
eye, the reciprocal of the Snellen visual acuity is also 20/20, or 1, and the
logarithm of 1 is 0.
21. a. If the retinoscopy streak is horizontal, the axis of the cylindrical lens is
also horizontal (180°). Thus, the sphero cylindrical lens combination for this
patient (before subtracting the working distance adjustment) is + 3.00 + 1.00 x
90. The working distance (67 cm, or 0.67 m) must be subtracted from the final
refraction. Thus, subtracting 1/0.67 m, or 1.50 D, yields the correct answer: +
1.50 + 1.00 x 90. Note that the cylindrical power acts 90° from the axis. If the
retinoscopy streak is horizontal, the axis of the cylindrical lens is 180°, but the
actual power is at 90°. Accordingly, the powers (after subtracting the working
distance) are +1.50 D at 90° and +2.50 D at 180°.
22. d. A certain vergence of light is necessary to focus incoming light on the
retina. As the power of the cornea decreases, a corresponding amount of IOL
vergence power (corrected for the different location of the refractive element)
must be added. Similarly, as the eye becomes shorter, more IOL vergence power
is needed to bring the light into focus on the now-less-distant retina.
23. c. There are basically 2 types of telescopes: the Galilean, or terrestrial,
telescope and the Keplerian, or astronomical, telescope. Each consists of a fairly
low-power, positive objective (front) lens and a high-power eyepiece. The
Galilean telescope has a minus-power eyepiece, and the astronomical telescope
has a plus-power eyepiece. The Galilean telescope produces an upright image
and has a shorter distance between the objective and
Eye piece (tube length) than does an astronomical telescope. The astronomical
telescope produces an inverted image unless prisms or mirrors are incorporated
to invert the image. The image produced by an astronomical telescope is brighter
than the image produced by a Galilean, which is a major advantage. However,
the prisms or mirrors necessary for an astronomical telescope to render an
upright image add weight and expense. Spectacle mounted visual aids utilize the
Galilean design, but other instruments such as hand-held binoculars use the
Keplerian approach. Both telescope designs are a focal. An object ray parallel to
the axis emerges as an image ray parallel to the axis.
Consequently, there are no focal points or principal planes.
The angular magnification is the negative of the ratio of the eyepiece's power
divided by the objective's power. In this case (ignoring the minus sign), the
angular magnification is 10.00 D/4.00 D = 2.5x. Tube length is the sum of the
focal lengths of the eyepiece and objective, so option c is correct.

24. c. Keratometers estimates the refractive power of the cornea. An object of
known size is placed in front of the eye. The tear film-acting as a convex mirror-
produces a virtual image of the object. The keratometer measures the linear
dimensions in a few meridians of the virtual image. The first assumption in the
estimation is that, in the measured meridian, the tear film's cross-section is
circular. In fact, the cross-section is closer to hyperbolic. A hyperbola does not
have a single radius of curvature but rather has a different curvature at each
point. Assuming a circular cross-section greatly simplifies matters because a
circle has a single, constant curvature at each point; however, this assumption
can also introduce inaccuracy. NeYertheless, under the circular assumption, the
"power" can be estimated using the formula r = 2u(I!O), where r is the radius of
curvature of the tear film's assumed circular cross-section, u is the distance from
the object to the cornea, I is the size of the image in a specific meridian, and 0 is
the size of the object. Once the radius of the assumed circular cross-section has
been calculated, the power in the meridian of the assumed circular cross-section
can be calculated using the formula P = (n - 1)/r, where n is the tear-film
refractive index (n = 1.333). Because the tear film is quite thin, the power of the
anterior corneal surface can be calculated by replacing the refractive index of the
tear film with the refractive index of the cornea. The power of the anterior
corneal surface, based on the circular cross-section assumption, is calculated
using the refractive index of the cornea (n = 1.376). The power of the anterior
corneal surface exceeds the power of the entire cornea because the posterior
corneal surface has a negative power of about -6.00 D. Therefore, the power of
the entire cornea can be calculated using a refractive index that is less than the
true refractive index of the cornea. Several modified refractive indices have been
suggested, but most keratometers use n = 1.3375. A reasonable estimate of total
corneal power is produced, not only through use of this value of 1.3375, but also
because a radius of7.5 mm converts to exactly 45.00 D. Clinically, it is important
to remember that the keratometer estimates corneal power based on a series of
assumptions. For certain purposes, such as contact lens fitting, K readings
are sufficiently accurate. However, for other purposes, such as calculating IOL
implant power in patients who have undergone corneal refractive surgery, the
underlying assumptions are invalid and the K readings are unreliable.

25. c. The Kestenbaum rule provides a starting point not an endpoint for the
required add. Base-in prisms should be incorporated into high-power reading
spectacles to assist accommodative convergence in patients who have similar
visual function binocularly, but they do not affect magnification. Magnification
alone does not enhance contrast and therefore would not suffice by itself for
patients with low contrast sensitivity
26. d. A person is considered to have low vision when a visual deficit
significantly affects his or her activities. Visual disability is related to the
interaction of a number of factors, including the complexity of the task, the skill
of the person, the individual's response to reduced vision, and other aspects of
visual function, including contrast sensitivity. A visual field deficit (such as
bitemporal hemianopia) or a specific level of visual acuity (such as less than
20/70) does not in and of itself qualify as low vision if it does not significantly
affect that person's particular activities or if he or she is able to adequately
compensate. Conversely, a patient who performs relatively well on a Snellen test
may be considered to have low vision if he or she is not able to perform
necessary tasks because of loss of vision.
27. d. Optical coherence tomography (OCT) is used to create cross-sectional
images of the living eye. Rays from a light source consisting of a super
luminescent diode-not a laser are split by a beam splitter into a reference beam,
which is directed to a movable mirror, and an object beam, which is directed to
one of the reflective interfaces within the tissue being examined. The 2 reflected
beams are then superimposed by the same beam splitter and transmitted together
to a light detector. By correlating the resulting interference patterns with the
position of the movable mirror, information about the reflectivity of the internal
structure of the cornea, lens, or retina can then be constructed.
28. b. When looking through a small pupil, the observer can improve
visualization by narrowing his or her effective inter pupillary distance. This can
be accomplished by several means. Moving the ophthalmoscope's mirror closer
to the observer (the "small-pupil feature" available on some ophthalmoscopes)
decreases the distance between the light paths to the observer's left and right
eyes, effectively narrowing the observer's inter pupillary distance.
If the examiner can slightly converge, it will narrow the observer's effective inter
pupillary distance. Increasing the distance between the observer and the patient
decreases the angle formed by the observer's 2 eyes and the patient's eye, thereby
allowing the light paths from the observer's eyes to "squeeze through" a smaller
pupil.

29. b. Changes of ±0.25 D and ±0.50 Din sphere and cylinder are likely to be
below the "just noticeable" threshold for a patient with 20/100 visual acuity.
Because the first issue to rule out when vision changes is a change in refraction,
an additional attempt should be made to refine the refraction using larger-step
changes in sphere and cylinder. The darkroom pinhole test is a test of potential
vision. It should be performed after the refraction has been optimized.
30. a. An optical system's nodal points are the points through which light rays
entering or leaving the system are undeviated (but not necessarily undisplaced).
In the reduced schematic eye, the nodal points coincide and are located 5.6 mm
posterior to the corneal surface. Because all light rays passing through this point
are undeviated, a light ray that leaves the tip of an object will pass through the
nodal point and strike the retina undeviated. Retinal image size can be calculated
by similar triangles if both the image height and distance are known.
31. a. The far point of the eye and the fovea are always corresponding points
when accommodation is relaxed. All the other statements are false. The far point
is 25 cm in front of the eye and is farther away from the near point of the fully
accommodated eye.
32. b. The non accommodated hyperopic eye has a far point behind the eye. A
virtual image of the retina forms at this location. As the eye begins to
accommodate, the point of focus recedes to minus infinity. Minus infinity and
plus infinity are essentially the same optically. As the eye continues to
accommodate through optical infinity, the point of focus moves in front of the
eye to a point between plus infinity and the cornea. The near point of the eye, in
diopters, is equal to the far point location, in diopters, plus the amplitude of
accommodation. Because we are told that the amount of hyperopia is less than
the amplitude of accommodation, we conclude that the near point is in front of
the eye (between infinity and the cornea).
33. d. A diopter is the reciprocal of distance in meters. A prism diopter measures
the deviation in centimeters at 1 m, or centimeters per meter. Refractive index is
the ratio of the speed of light in a vacuum to the speed of light in the medium
and, therefore, is dimensionless. Wavelength can be measured in any unit of
length. For optical wavelengths, the nanometer is convenient. Frequency is
measured in cycles per second, or hertz.

34. c. Irregular astigmatism is a general term that encompasses most higher-
order aberrations. Irregular astigmatism caused by an irregular corneal surface is
best corrected by a rigid gas-permeable (RGP) contact lens that replaces the
anterior corneal surface with a smooth air-lens interface. Soft contact lenses are
not as effective in creating a smooth surface because they conform somewhat to
the irregular corneal surface, although they may correct an irregular corneal
surface to some extent. If spectacles could be manufactured to compensate for
higher-order aberrations, they would work in 1 gaze direction only. For this
reason, RGP contact lenses provide the best visual acuity for patients with
irregular astigmatism produced by an irregular cornea.
35. b. There are many risk factors associated with even the most current
extended-wear contact lenses, including swimming with the lenses, previous
history of eye infection, any exposure to smoke, abnormal eyelid function,
severe dry eye, and corneal neovascularization.
36. b. Patients with central scotomata can still read by using eccentric fixation,
along with appropriate magnification and enhanced contrast, if necessary.
Reading speed is usually decreased, but reading ability can often be improved
with training and practice
37. b. Loss of peripheral visual field makes it difficult to navigate unfamiliar
territory and may cause the patient to bump into objects or people. Retinitis
pigmentosa, panretinal photocoagulation, and retinal detachment typically affect
the peripheral visual field, whereas age-related macular degeneration typically
affects central visual acuity.
38. a. The entrance pupil of the eye is the pupil we see when we look at a
patient's eye. For a refractive index of n = 4/3 and a cornea with a power of +43
.00 D, the entrance pupil is the image of the anatomical pupil formed by the
cornea. The crystalline lens does not contributeto the formation of the entrance
pupil. The entrance pupil is located about 0.5 mm in front of the anatomical
pupil and is about 13%- 15% larger.

39. c. The formula is
40. d. The formula is

04 - Ophthalmic Pathology and Intraocular Tumors
1. What is a lesion composed of normal, mature tissue in an abnormal
location?
a. hamartoma
b. choristoma
c. hemangioma
d. granuloma
2. Which of the following cells would most likely be observed on histologic
examination of
a specimen of a bacterial corneal ulcer?
a. eosinophils
b. basophils
c. epithelioid histiocytes
d. neutrophils
3. Which of the following choices is a general histologic sign of malignancy?
a. nuclear/cellular pleomorphism
b. dyskeratosis
c. dysplasia
d. calcification
4. When glaucoma occurs in association with angle recession, it is most
commonly because of which of the following?
a. damage to the trabecular meshwork
b. associated lens subluxation
c. iridodialysis
d. a tear in the ciliary body muscle
5. If a conjunctival biopsy is being performed for suspicion of ocular
cicatricial pemphigoid, then half of the specimen should be submitted in
formalin for routine histology and the other half should be submitted in
what medium for immunofluorescence studies?
a. Michel medium
b. glutaraldehyde
c. saline
d. absolute alcohol
6. What is the first step in preparing a specimen for electron microscopy?
a. glutaraldehyde fixation
b. thick sections
c. thin sections
d. osmification process
7- Frozen sections are appropriate for which one of the following?
a. to surgically control the margins of a neoplasm
b. to interpret a conjunctival lesion
c. to interpret a cutaneous lesion
d. to make a formal diagnosis
8. What is the best way to diagnose orbital hemangiopericytoma?
a. radiologic imaging
b. ultrasound testing
c. fine -needle aspiration or open orbital biopsy
d. clinical symptoms and examination
9. A 40-year-old man has a painless, palpable mass in the right supero
lateral orbit that displaces the globe down and inward. A CT scan shows a
heterogeneous mass in the region of the lacrimal gland with adjacent bone
remodeling. Which biopsy approach is correct?
a. total primary excision through a lateral orbitotomy
b. incisional biopsy through a lateral orbitotomy
c. incisional biopsy through a medial orbitotomy
d. total primary excision through a medial orbitotomy
10. what method can identify infectious agents, neoplastic cells, or
degenerative conditions and distinguish lesions of neuroectodermal origin
from neuroendocrine lesions?
a. Gram stain
b. chromatography
c. routine histologic examination
d. immunohistochemistry
11. Which of the following corneal stromal dystrophies is characterized by
both hyaline and amyloid deposits?
a. granular
b. lattice
c. Avellino
d. macular
12. Which of the following forms of infectious keratitis displays double-
walled cysts in the corneal stroma on histology?
a. pseudomonal ulcer
b. herpetic keratitis
c. Acanthamoeba keratitis
d. Fusarium keratitis
13. A 55-year-old diabetic black female has unilateral elevated intraocular
pressure associated with long-standing intraocular hemorrhage. The
pertinent slit-lamp finding consists of golden brown cells in the anterior
chamber. What is the most likely etiology of her elevated intraocular
pressure?
a. aqueous fluid overproduction
b. artifactual readings due to corneal edema
c. outflow obstruction due to red blood cell membrane rigidity
d. traumatic pupillary block
14. What disease may be diagnosed by finding Heinz bodies on red blood
cell membranes in an anterior chamber aspirate?
a. lymphoma
b. siderosis
c. pseudoexfoliation
d. ghost cell glaucoma

15. A 35-year-old woman, recently diagnosed with rheumatoid arthritis,
presents with a violaceous scleral nodule. The biopsy will most likely reveal
which of the following?
a. palisading arrangement of histiocytes/giant cells around necrotic/necrobiotic
collagen fibers
b. sparse inflammatory infiltrate composed of lymphocytes and plasma cells
c. colonies of gram-negative bacteria associated with acute necrotizing
inflammation
d. circumscribed proliferation of spindle cells in chronically inflamed, richly
vascular, and myxoid stroma
16. The pathophysiology of posterior subcapsular cataract may best be
described by which of the following?
a. posterior migration of lens epithelial cells
b. disorganization of posterior lens fibers
c. infiltration of the posterior lens by inflammatory cells
d. retention of lens fiber nuclei
17. What is the histopathologic appearance of the anterior chamber angle in
a case of phacolytic glaucoma?
a. infiltration by hemosiderin-laden macrophages
b. lack of significant inflammatory cell infiltrate
c. infiltration by neutrophils
d. infiltration by protein-laden macrophages
18. Of the following, which anatomic boundary is not a component of the
vitreous'
a. hyaloid face
b. internal limiting membrane
c. hyaloideocapsular ligament
d. vitreous base
19. Which of the following vitreous degenerations is not age related?
a. vitreous syneresis
b. macular hole
c. posterior vitreous detachment
d. asteroid hyalosis

20. Pathologic examination of cystoid macular edema reveals cysts in which
retinal layer?
a. outer plexiform
b. Bruch membrane
c. internal limiting membrane
d. retinal pigment epithelium
21. A 6-week-old child is brought by his parents because of a 1-cm reddish
mass on the left upper eyelid, which prevents the eye from opening fully. It
has grown rapidly since birth. MRI shows an enhancing vascular lesion.
Which entity is most likely?
a. plexiform neurofibroma
b. acute dacryocystitis
c. capillary hemangioma
d. benign mixed tumor of the lacrimal gland
22. Histopathologically, the uveitis seen in Vogt-Koyanagi-Harada
syndrome most closely resembles the uveitis seen in which one of the
following diseases?
a. juvenile idiopathic arthritis
b. intraocular lymphoma
c. pars planitis
d. sympathetic ophthalmia
23. An asymptomatic, dome-shaped, orange mass is noted in the mid
peripheral fundus of a 30-year-old woman. An overlying exudative retinal
detachment is present. A-scan ultrasonography shows high internal
reflectivity. Which entity is most likely?
a. posterior scleritis
b. central serous retinopathy
c. amelanotic choroidal melanoma
d. circumscribed choroidal hemangioma
24. Which pathologic finding would differentiate between a ruptured
dermoid and ruptured epidermoid cyst?
a. hair follicles
b. lamellated keratin
c. mixed inflammation
d. squamous epithelium

25. What is the most common type of intraocular tumor?
a. melanoma
b. retinoblastoma
c. lymphoma
d. metastatic neoplasm
26. A 25-year-old white male with a history of conjunctivitis presents with a
flesh-colored mass with a central umbilication on the upper eyelid.
Examination of the pathologic specimen reveals invasive lobular acanthosis,
a central umbilication, and eosinophilic and basophilic intracytoplasmic
inclusions. What is the most likely diagnosis?
a. squamous papilloma
b. xanthelasma
c. basal cell carcinoma
d. Molluscum contagiosum
27. A 22-year-old female presents with a painless, non tender, flesh-colored,
hyperkeratotic eyelid mass. Pathologic examination shows acanthotic
epithelium surrounding a fibrovascular core. What is the most likely
etiology?
a. bacterial
b. inflammation
c. sun exposure
d. viral
28. Squamous cell carcinoma in situ is defined as a pathologic anatomic
limitation by which one of the following?
a. superficial epithelium
b. stromal keratocytes
c. basal epithelium
d. basement membrane
29. With which of the following is aniridia most commonly associated?
a. retinal pigment epithelial hyperplasia
b. optic nerve coloboma
c. glaucoma
d. optically empty vitreous

30. What physiologic changes are associated with acquired optic atrophy?
a. increased myelin with thinning of the pial septa
b. shrinkage of the nerve diameter with widening of the subarachnoid space
c. uniform changes across the nerve without variation
d. increased myelin and shrinking of the subarachnoid space
31. What is optic nerve glioma most frequently associated with?
a. Sturge-Weber syndrome
b. neurofibromatosis type 1
c. Peters anomaly
d. neurofibromatosis type 2
32. Which of the following is not a clinical risk factor for metastatic disease
in patients with uveal melanoma?
a. large tumor size
b. ciliary body involvement
c. young age
d. extraocular extension
33. Which of the following is the most important risk factor for the
development of uveal melanoma?
a. dysplastic nevus syndrome
b. light-colored complexion
c. ocular melanocytosis
d. ultraviolet light exposure
34. At the time a choroidal melanoma is diagnosed, which test is
recommended to help rule out metastasis?
a. serum glucose
b. brain MRI
c. bone marrow biopsy
d. abdominal imaging
35. With which of the following organs must the ophthalmologist be most
concerned about in a patient with retinal capillary hemangioblastoma?
a. brain and kidney
b. liver and lung
c. bowel and skin
d. organs of the immune system and central nervous system

36. What association distinguishes von Hippel-Lindau syndrome from von
Hippel disease?
a. intracranial calcifications, ash-leaf spots, retinal astrocytomas
b. cafe-au-lait spots, Lisch nodules, optic pathway gliomas
c. pheochromocytomas, cerebellar hemangioblastomas, renal cell carcinomas
d. limbal dermoids, upper eyelid colobomas, preauricular tags
37. Which of the following is the most important histopathologic risk factor
for mortality in the enucleated globe from a patient with retinoblastoma?
a. the presence of anterior segment involvement
b. the extent of retinal detachment
c. the extent of optic nerve and choroidal invasion
d. the size of the tumor
38. Which of the following clinical characteristics is typical of Coats disease?
a. unilateral
b. associated with HLA-B27
c. found in female patients
d. bilateral
39. Intraocular calcification in the eye of a child is most diagnostic of what
disease?
a. retinoblastoma
b. toxocariasis
c. persistent fetal vasculature
d. Coats disease
40. What is the most common secondary tumor in retinoblastoma patients?
a. fibrosarcoma
b. melanoma
c. pinealoblastoma
d. osteosarcoma
41. When a parent has bilateral retinoblastoma, which risk factors apply to
the affected parent's children?
a. 85% risk of developing retinoblastoma
b. risk of bilateral disease in all affected children
c. risk of developing retinoblastoma in males only
d. 45% risk of developing retinoblastoma

42. What is the primary treatment for a 2-year-old child with unilateral
retinoblastoma classified as International Classification Group E?
a. systemic chemotherapy alone
b. intra-arterial chemotherapy
c. enucleation
d. radiation alone
43. What is the treatment of choice for metastatic carcinoma to the eye?
a. chemotherapy
b. external-beam radiation
c. brachytherapy
d. individually tailored in each case
44. What is the most common finding in ocular involvement in leukemia?
a. retinal hemorrhages
b. aqueous cells
c. retinal perivascular sheathing
d. vitreous cells
45. What tumor frequently occurs in conjunction with central nervous
system involvement?
a. basal cell carcinoma of the eyelid
b. primary intraocular lymphoma
c. retinoblastoma
d. ciliary body melanoma
46. Leukemic retinopathy may cause hemorrhages in which level(s) of the
retina?
a. preretinal (subhyaloidal) and intraretinal
b. subretinal
c. choroidal
d. Leukemic retinopathy does not cause retinal hemorrhages.
Answers
1. b. A choristoma is normal, mature tissue in an abnormal location. A limbal
dermoid is an example of a choristoma- skin that is present at the abnormal
location of the limbus but otherwise normal and mature. The term hamartoma
describes an exaggerated hypertrophy and hyperplasia (abnormal amount) of
mature tissue at a normal location.
An example of a hamartoma is a cavernous hemangioma, an encapsulated mass
of mature venous channels in the orbit. A granuloma is an aggregate of
epithelioid histiocytes within tissue in the setting of chronic granulomatous
inflammation.
2. d. Neutrophils, or polymorphonuclear leukocytes (PMNs), are identified by
their multisegmented nuclei and intracytoplasmic granules, and they
predominate in the acute inflammatory response in bacterial infections.
Eosinophils have bilobed nuclei and prominent eosinophilic intracytoplasmic
granules and are commonly observed in allergic reactions. Basophils contain
basophilic intracytoplasmic granules, circulate in the bloodstream, and play a
role in parasitic infections and allergic responses. Epithelioid histiocytes
have abundant eosinophilic cytoplasm and sharp cell borders and are histologic
markers of granulomatous inflammation.
3. a. Malignant tumor cells are characterized Histologically by cellular and
nuclear pleomorphism (i.e., cells and nuclei of different sizes and shapes).
Premature individual cell keratinization, or dyskeratosis, may be seen in both
benign and malignant epithelial lesions.
Dysplasia (abnormal epithelial maturation) is a premalignant change.
Calcification may be seen in benign and malignant lesions.
4. a. Traumatic recession of the anterior chamber angle is due to a tear in the
ciliary body, between the longitudinal and circular muscles, with posterior
displacement of the iris root. Concurrent damage to the trabecular meshwork
may lead to glaucoma. Lens subluxation and iridodialysis may be observed in
addition to angle recession after blunt ocular trauma; however, the glaucoma that
occurs in association with angle recession is most commonly caused by damage
to the trabecular meshwork.
5. a. Michel (pronounced mee-SHELL) transport medium is used to transport
specimens for immunofluorescence studies. In ocular cicatricial pemphigoid,
immunofluorescence studies demonstrate IgG, IgM, and/or IgA

immunoglobulins, and/or complement (C3) positivity in the epithelial basement
membrane zone. Michel medium is not a fixative.
It should be stored refrigerated (not frozen) until use. Specimens may be kept in
Michel medium for up to 5 days at room temperature. Glutaraldehyde is the
preferred fixative for electron microscopy. Normal saline solution (0 .9% sodium
chloride) and absolute ethyl alcohol may be employed to transport tissue within
24 hours for RNA studies.
6. a. Glutaraldehyde (2.5% solution in phosphate buffered saline) fixation is the
first step in preparing a specimen for electron microscopy. The tissue is then
washed in buffered solution and postfixed in osmium tetroxide (osmification
process). Representative pieces of tissue are processed in graded alcohol baths
for dehydration and embedded in epoxy resin. Thick sections (1 flm in thickness)
are cut to examine the tissue under light microscopy and identify regions of
greatest interest for ultrathin sectioning. The ultrathin sections (50 nm in
thickness) are cut with diamond or glass knives attached to an ultramicrotome
and then mounted on a 3-mm-diameter copper grid. The mounted sections
are then stained with uranyl acetate (or lead citrate) to impart contrast to the
tissue for electron microscopy.
7. a. A frozen section is indicated when the results of the study will affect
management of the patient in the operating room. Two common indications for
frozen section are to determine whether resection margins are free of tumor and
to determine whether the surgeon has obtained a representative biopsy specimen
in the case of metastases. Interpretation or diagnosis of a lesion requires
permanent sections. Permanent sections are always preferred
and are the standard for formal diagnosis based on pathologic findings.
8. c. Hemangiopericytoma is a solid tumor, and radiologic imaging and
ultrasonography would therefore provide only nonspecific features that are of
poor diagnostic value.
Hemangiopericytoma is a primary orbital tumor, and the clinical symptoms will
be the same as the symptoms for any orbital tumor. One can expect proptosis,
pain, and diplopia as presenting features. The diagnosis requires positive
immunohistochemical staining for CD34. The staining can be done on fine-
needle or open orbital biopsy specimen.
9. a. Pleomorphic adenoma (benign mixed tumor) is the most common epithelial
tumor of the lacrimal gland. The tumor is pseudoencapsulated and grows by
expansion. Progressive growth into the bone of the lacrimal fossa may cause

excavation and stimulate new bone (cortication) formation in the area. Total
primary excision through a lateral orbitotomy is the correct approach because
when part of a tumor is left behind, tumor recurrence and, in rare instances,
malignant transformations are possible. A lateral orbitotomy provides the best
surgical exposure and allows for complete removal of the tumor.
10. d. Immunohistochemistry takes advantage of the property that a given cell
can express specific antigens. In immunohistochemistry, a primary antibody
binds to a specific antigen on the surface of or within a cell. The antibody is
linked to a chromogen, whose colored end-product is visualized under a
microscope to determine the cell type. Hundreds of antibodies specific for
cellular products or surface antigens are available, and immunohistochemistry
is the only method capable of distinguishing lesions of neuroendocrine
origin from those of neuroectodermal origin. Chromatography is the collective
term for a set of laboratory techniques used to separate colored chemical
mixtures and is not routinely used in pathologic examination of tissues. A Gram
stain can identify the morphology of an infectious bacterium and the bacterium's
affinity for a specific histological stain, thus distinguishing between gram-
positive and gram-negative bacteria. This information can be used in the
selection of an antibiotic. Routine histologic examination cannot distinguish
neuroendocrine from neuroectodermal lesions because their pathologic
appearance is very similar.
11. c. Avellino dystrophy, or combined granular-lattice dystrophy, displays
features of both granular dystrophy (type 1) and lattice dystrophy (type 1).
Histologically, hyaline deposits (highlighted by the Masson trichrome stain) and
amyloid deposits (highlighted by the Congo red stain) are present within the
corneal stroma, which is characteristic of granular dystrophy and lattice
dystrophy, respectively. Macular dystrophy exhibits mucopolysaccharide
deposits (highlighted by the alcian blue and colloidal iron stains).
12. c. Acanthamoeba protozoa have a double-walled cyst morphology, and these
cysts are difficult to eradicate from the corneal stroma. Less commonly,
trophozoite forms may also be identified. Epithelial cells infected with herpes
virus may display intranuclear inclusions, but these are rarely seen histologically
because corneal grafting is not generally performed during the acute phase of
infection. Pseudomonas is a gram-negative bacterium and is rod shaped
(bacillus).

13. c. Long-standing intraocular hemorrhage leads to degenerative changes in
erythrocytes, which lose intracellular hemoglobin and, clinically, appear golden
brown or "khaki col Answers ored:’ These rigid, spherical ghost cells may
obstruct the trabecular meshwork, leading to ghost cell glaucoma.
14. d. Ghost cells are hemolyzed erythrocytes that have lost most of their
intracellular hemoglobin. Heinz bodies are the remaining denatured, precipitated
hemoglobin particles within the ghost cells.
15. a. The clinical presentation is suggestive of nodular scleritis, related to
rheumatoid arthritis. Choice a describes the histology of a rheumatoid nodule.
16. a. Under normal conditions, the lens epithelial cells terminate at the lens
equator. When the equatorial lens epithelial cells migrate onto the posterior lens
capsule, they swell (referred to as bladder cells of Wedl), resulting in posterior
subcapsular cataract formation.
17. d. In phacolytic glaucoma, denatured lens protein in a hypermature cataract
leaks through microscopic openings in an intact lens capsule. This lens protein is
then phagocytosed by macrophages, which are present in the anterior chamber
angle.
18. b. The internal limiting membrane is the innermost layer of the neurosensory
retina and, though attached to the vitreous, is not considered a component of the
vitreous. The hyaloid face is the outer surface of the vitreous cortex. The
hyaloideocapsular ligament forms the anterior border of the vitreous, which is
attached to the lens capsule. The vitreous base is a firm circumferential
attachment of the vitreous straddling the ora serrata.
19. d. The development of asteroid hyalosis is not known to be a consequence of
age. Vitreous syneresis, macular hole, and posterior vitreous detachment can be
considered age related, as the incidence of these conditions increases with age.
20. a. Nerve fiber layers in the outer plexiform layer (nerve fiber layer of Henle)
run obliquely, allowing for the accumulation of fluid in the macula, which
appears as cysts when there is abnormal permeability of the blood-retina barrier.
21. c. Capillary hemangioma is the most common neoplasm of the eyelid in
childhood and has a bright red appearance clinically. Plexiform Neurofibromas

typically affect the upper eyelid, are not particularly vascular, and do not
typically cause discoloration of the eyelid.
Acute dacryocystitis can occur in children, but it would affect the medial canthal
region of the lower eyelid. Benign mixed tumor of the lacrimal gland is rare in
children. It may cause a mass in the upper outer eyelid, typically without
discoloration. If the eyelid is everted, the mass may be appreciated through the
conjunctiva.
22. d. The inflammation seen in Vogt-Koyanagi-Harada (VKH) syndrome is
very similar to that seen in sympathetic ophthalmia. Both demonstrate the
presence of lymphocytes and epithelioid histiocytes (granulomatous
inflammation) in the posterior uveal tract. VKH involves the choriocapillaris
more often than does sympathetic ophthalmia. Juvenile idiopathic arthritis
typically involves the anterior uveal tract and does not demonstrate
granulomatous inflammation. Pars planitis involves the peripheral retina,
vitreous, and choroid. Typically, the inflammation is not granulomatous.
23. d. Circumscribed choroidal hemangioma typically has a red or orange
appearance clinically, and it is characteristically highly reflective on
ultrasonography. Posterior scleritis may be very difficult to appreciate on fundus
examination but may have an associated exudative retinal detachment. On B-
scan echography, the sclera will appear thickened, and a "T sign" may be seen
around the optic nerve. Central serous retinopathy will have a localized
exudative retinal detachment, typically without significant findings in the
choroid. Amelanotic melanomas usually appear cream colored clinically and
have low to medium internal reflectivity on A-scan echography.
24. a. The correct answer is the presence of hair follicles. An epidermoid cyst is
lined with keratinized stratified squamous epithelium similar to epidermis but
does not have skin adnexal structures such as hair follicles or glands. A dermoid
cyst is lined with epidermal epithelium and has adnexal structures. Both types of
cysts will generate a mixed inflammatory response if they rupture.
25. d. The most common type of intraocular tumor overall is a metastatic
neoplasm. The second most common type in adults is uveal melanoma.
Retinoblastoma is uncommon overall, and lymphomas are rare.
26. d. Molluscum contagiosum is characterized by marked focal acanthosis of
the epidermis with a central umbilication. Viral inclusions are present in most of
the superficial epithelial cells. Squamous papilloma has an upward rather than

downward growth pattern histologically. Xanthelasma consists of aggregates of
foamy macrophages in the dermis.
Basal cell carcinoma has an invasive (downward) growth pattern, with multiple
islands of blue cells with the characteristic peripheral palisading border of tumor
cells. Basal cell carcinoma is more common on the lower eyelid.
27. d. The correct answer is viral. A papilloma, typical of infection of the skin
with human papillomavirus, is defined as acanthotic epithelium with a
fibrovascular core. Bacterial infections typically cause an abscess or cellulitis.
Inflammatory lesions are typically erythematous. Sun exposure may cause
hyperpigmentation, wrinkling, or actinic keratosis (i.e., a flat, red, scaly lesion).
28. d. Squamous cell carcinoma in situ implies that the neoplasm is confined to
the epithelium and does not break through the basement membrane and extend
into the underlying stroma.
29. c. Aniridia is most commonly associated with glaucoma. Foveal hypoplasia,
cataract, and corneal pannus may also be present.
30. b. In acquired optic atrophy, there is loss of axonal fibers, which results in a
decrease in the optic nerve diameter with corresponding widening of the
intermeningeal (subarachnoid) space. Additional changes include gliosis and
thickening of the fibrovascular pial septa.
31. b. Optic nerve glioma is most frequently associated with neurofibromatosis
type 1.
32. c. Old age was found to be a risk factor for metastatic uveal melanoma. The
other choices are also well-established risk factors.
33. b. The risk of developing uveal melanoma is closely related to a person's
complexion.
Uveal melanoma appears mostly in whites, mainly in those of European origin,
and is rare in other races.
34. d. The liver is by far the most frequent site of metastasis from uveal
melanoma, and metastasis to other organs, such as the lungs, skin, and bones, is
rarely found without liver involvement.
35. a. The presence of a retinal capillary hemangioblastoma (previously known
as retinal capillary hemangioma) suggests the possibility of von Hippel- Lindau
(VHL) syndrome resulting from a mutation of the VHL gene on chromosome 3.
Patients with VHL syndrome are at risk for cerebellar hemangioblastomas,
pheochromocytomas, and renal cell carcinomas. Genetic screening of such
patients should be considered.
36. c. Von Hippel disease is limited to a solitary finding, retinal capillary
hemangioblastoma.
VHL syndrome is associated with cerebellar hemangioblastomas. Patients with
this syndrome are also at risk of developing pheochromocytomas and renal cell
carcinomas.
37. c. Invasion of the optic nerve increases the risk of central nervous system
metastasis either by direct access in or along the nerve or by seeding of the
subarachnoid space. Massive, deep invasion of the choroid increases the risk of
hematogenous spread (metastases).
38. a. Coats disease is a unilateral retinal vasculopathy occurring most
commonly in boys younger than 10 years. Some studies have linked Coats
disease to mutations in the Norrie disease gene (NDP). There is no association
with HLA-B27.
39. a. Intraocular calcifications are the hallmark of retinoblastoma and signify
retinoblastoma until proven otherwise. In rare instances, intraocular
calcifications may be seen in toxocariasis, persistent fetal vasculature, and Coats
disease. In these cases, calcifications are usually focal and discrete, occurring
within granulomas (toxocariasis) or a retrolental membrane (persistent fetal
vasculature) or at the level of the retinal pigment epithelium (Coats disease).
40. d. Osteosarcomas represent 40% of tumors arising within the field of
radiation and 36% outside the field of radiation in patients previously treated for
retinoblastoma.
41. d. A parent with retinoblastoma, in theory, has a somatic mutation of at least
1 allele of the retinoblastoma gene (RBl). Thus, there is a 50% chance that the
parent will pass the mutated allele to each of his or her children. There is a 90%
chance of penetrance if the abnormal allele is inherited. Therefore, the child's
risk of developing retinoblastoma is the sum of 0.50 x 0.90, which is 0.45, or
45%.

42. c. A 2-year-old child with unilateral retinoblastoma at diagnosis is unlikely to
develop disease in the other eye. Any tumors that form would most likely be
peripheral to the macula and, with close surveillance, amenable to local
treatment with laser or cryotherapy alone. Eyes classified as International Group
E have the most advanced intraocular disease with limited visual potential.
Tumors may invade the anterior chamber and ciliary body, and there may be
associated neovascular glaucoma. Such eyes are unlikely to respond to
conservative treatment measures.
43. d. Treatment of a patient with a metastasis to the eye should be individually
tailored after consultation with the patient's oncologist. When the patient has
other systemic metastases, systemic chemotherapy- which may also affect the
ocular metastasis- may be considered.
When there are multiple ocular metastases and chemotherapy is not planned,
external-beam radiation may be considered. When the ocular metastasis is
solitary and no other systemic metastases are known, brachytherapy may be the
treatment of choice.
44. a. Retinal hemorrhages, typically white-centered hemorrhages, are the most
common ocular manifestation of leukemia. Patients with leukemia and retinal
hemorrhages typically have anemia and thrombocytopenia. The other findings
are much less common.
45. b. Primary intraocular lymphoma (also known as large cell lymphoma,
vitreoretinal lymphoma, or retinal lymphoma), occurs in 15%-25% of patients
with primary central nervous system lymphoma (PCNSL). On the other hand,
more than half of patients with primary intraocular lymphoma have or will
develop PCNSL.
46. a. Leukemic retinopathy is characterized by intraretinal and preretinal
(subhyaloidal) hemorrhages. The hemorrhages most often result from associated
anemia or thrombocytopenia.
Retinal hemorrhages may have white centers, so-called pseudo-Roth spots.
Additional findings may include hard exudates, cotton-wool spots, and
perivascular Infiltrates

05 - Neuro-Ophthalmology
1. Which of the following structures is the neural integrator for vertical and
torsional gaze?
a. nucleus prepositus hypoglossi
b. interstitial nucleus of Cajal
c. nucleus raphe interpositus
d. rostral interstitial nucleus of the medial longitudinal fasciculus
2. Occlusion of which of the following arteries may result in lateral medullary
syndrome (or Wallenberg syndrome)?
a. posterior inferior cerebellar artery
b. median perforators of the basilar artery
c. posterior cerebral artery
d. anterior inferior cerebellar artery
3. The maxillary division of the trigeminal nerve (V2) enters the skull base
through which foramen?
a. foramen ovale
b. foramen lacerum
c. foramen spinosum
d. foramen rotundum
4. Nephrogenic fibrosing dermopathy occurs in patients with which one of
the following systemic conditions?
a. liver disease
b. kidney disease
c. lung disease
d. autoimmune disease
5. A 29-year-old obese woman notes new headaches for the past year. Which
of the following features would be most consistent with pseudopapilledema?
a. blurring of the disc margins
b. cup- disc ratio of 0.3
c. obscuration of the retinal vessels
d. hyperemia of the disc surface

6. Which of the following signs is more consistent with a retinopathy than an
optic neuropathy?
a. visual acuity of 20/80 in both eyes
b. central scotoma revealed on perimetry
c. Amsler grid testing with missing lines
d. photostress test recovery time of 90 seconds
7. Which of the following is most essential for the diagnosis of idiopathic
intracranial hypertension?
a. obese woman of childbearing age
b. no evidence of mass lesion on magnetic resonance imaging of the brain
c. systolic blood pressure less than 180 mm Hg
d. documented opening pressure of >25 cm H2Oin the prone position
8. What is the most common cause of transient monocular visual loss?
a. papilledema
b. recurrent hyphema
c. retinal ischemia
d. occipital lobe ischemia
9. A history of painless, curtain like visual loss in 1 eye that spontaneously
resolves within 10-15 minutes is most characteristic of what pathologic
entity?
a. retinal embolus
b. complicated migraine
c. drusen of the optic disc
d. occipital lobe seizure
10. Transient visual blurring associated with physical activity or elevation in
body temperature occurs most frequently with which disorder?
a. age-related macular degeneration
b. demyelinating optic neuritis
c. cardiac arrhythmia
d. open-angle glaucoma

11. A patient has a normal eye examination, intact visual fields, and normal
motor function and is able to recognize an object but has difficulties reaching
out to grasp the object. This is characteristic of what entity?
a. ocular motor apraxia
b. optic ataxia
c. prosopagnosia
d. simultanagnosia
12. Following a stroke, a patient can see moving objects in his blind
hemifield; however, static objects are invisible to him. What is the name for
this disorder?
a. Anton syndrome
b. palinopsia
c. Riddoch phenomenon
d. visual anesthesia
13. Which of the following statements characterizes alexia without agraphia?
a. It occurs with damage to the right occipital lobe.
b. It is associated with intact structures anterior to the splenium of the corpus
callosum.
c. It represents a disorder of Yisual-spatial relationship.
d. It is part of Balint syndrome.
14. A 72-year-old man with hypertension and diabetes mellitus frequently
cuts himself while shaving the right side of his face and reports burning his
left hand while cooking. He has trouble tracking moving objects. Visual
acuity and visual field findings are normal; rightward eye movements are
hypermetric. Which of the following examination findings will assist in
localizing the anatomical lesion?
a. see-saw nystagmus
b. eyelid retraction
c. right ptosis and miosis
d. paroxysmal gaze palsy

15. A 68-year-old woman cannot see the food on her dinner plate and is
having trouble reading. Visual acuity is normal, and confrontation fields are
full. She cannot look down when asked to view your fingers but will look
quickly when you toss a ball into her lap. What other clinical findings often
accompany this disorder?
a. light-near dissociation
b. tonic upward ocular deviation
c. reduced blink frequency
d. optic ataxia
16. A 27-year-old man with monthly migraine headache has a dilated left
pupil and blurred vision. He denies diplopia. His last headache was 2 weeks
ago and resolved after 1 day. Visual acuity is 20/20 OU, ocular motility is
normal, and there is no ptosis. The pupils measure 5 mm OD, 6.5 mm OS,
and they constrict to 3 mm OD, 5.5 mm OS with light stimulus. Direct and
consensual reactions are the same in each eye. What is the next step in
managing this patient?
a. urgent noninvasive angiography (magnetic resonance angiography or computed
tomography angiography)
b. hospital admission to a neuro-intensive care unit
c. reassurance and outpatient observation
d. laboratory screening for organophosphate poisoning
17. A 75-year-old woman with long-standing hypertension reports 3 days of
horizontal diplopia worse when looking to the right. It is constant at distance
and bothers her most when driving. It is not present when reading.
Examination shows a deficit of abduction of the right eye. What is the next
step in managing this patient?
a. Obtain a basic metabolic panel, complete blood count with differential,
erythrocytes sedimentation rate, and C-reactive protein determination.
b. Send her to the local emergency department for urgent cranial imaging.
c. Prescribe base-out prism to correct the diplopia.
d. Advise observation and re-examination in 3 months.

18. A 37-year-old woman describes persistent and worsening headache for 2
days and diplopia since yesterday. Visual acuity is normal, and the fundus is
unremarkable. Extraocular movements appear grossly normal; cover testing
shows the following: exotropia 5 prism diopters ^, right hypertropia 4^ in
primary gaze; exotropia 9^, right hypertropia 3^ on right gaze; exotropia 1^,
right hypertropia 7 ^ on left gaze; and exotropia 6^ left hypertropia 4^ on
down gaze.
Both pupils react to light with a less brisk response on the left.
What systemic risk factors are most relevant to this clinical presentation?
a. classic migraine headache since age 16 years
b. smoking 1 pack cigarettes daily for 20 years
c. numbness in both feet
d. diabetes mellitus
19. A 59-year-old woman reports inability to see road signs when driving and
has had 3 minor collisions in the past 6 months. Spontaneous, rapid onjugate
eye movements occur in short bursts both vertically and horizontally. Her
systemic diseases (hypertension, hyperlipidemia) are under good control,
although she has been unable to stop smoking cigarettes. Where would a
mass lesion be most likely present?
a. frontal lobe of brain
b. lower pole of right kidney
c. iliac crest bone marrow
d. middle lobe of lung
20. A 24-year-old woman has had intermittent blurred vision for the past 3
months. Visual acuity is 20/30 in each eye with full fields and normal fundus
appearance. You observe a low-amplitude, moderate-frequency, right-eating
horizontal jerk nystagmus. After documenting your findings, you now
observe a left-beating jerk nystagmus. What findings would you expect on
magnetic resonance imaging of the brain?
a. periventricular white matter lesions on FLAIR sequences
b. empty sella and chiasmal Displacement on sagittal Tl sequences
c. pineal gland enlargement with coronal T1 contrast enhancement
d. clival tumor with midbrain compression on axial Tl contrast-enhanced images

21. Where is the central lesion located that can cause bilateral light- near
dissociation of the pupils?
a. dorsal midbrain
b. nucleus of Budge-Waller in the upper spinal cord
c. hypothalamus
d. occipital lobe
22. Which clinical finding is characteristic of Adie tonic pupil?
a. associated upper lid ptosis
b. sectoral palsy of the iris sphincter
c. iris heterochromia
d. iris supersensitivity to topical apraclonidine
23. A patient presents with facial weakness, diplopia, ataxia, and areflexia.
Which of the following is the most likely cause?
a. Miller Fisher syndrome
b. Ramsay Hunt syndrome
c. Melkersson-Rosenthal syndrome
d. a cerebellopontine angle tumor
24. A patient presents with continuous unilateral undulating contraction of
the orbicularis oculi and most of the facial muscles. Which of the following is
the most likely cause?
a. vascular compression of the seventh nerve
b. pontine glioma
c. excessive caffeine intake
d. aberrant regeneration from prior Bell palsy
25. A 45-year-old man presents with several episodes per day of severe left-
sided orbital and temporal pain lasting 5-10 minutes and occasionally
associated with left ptosis and miosis.
Which of the following is the most likely diagnosis?
a. cluster headache
b. paroxysmal hemicrania
c. hemicrania continua
d. idiopathic stabbing headache

26. A patient receiving prophylactic migraine treatment experiences blurred
vision associated with pain. Which of the following is the most likely migraine
drug used by the patient?
a. gabapentin
b. naproxen
c. topiramate
d. verapamil
27. Which of the following clinical findings is most likely to suggest the need
for additional diagnostic testing in a patient with migraine headache?
a. absence of family history
b. presence of a visual aura with hemianopic distribution
c. presence of a visual field defect
d. pulsating character of headache
28. When the clinician suspects a nonorganic loss of vision in a patient who
claims to see nothing, which of the following test results may be helpful in
establishing the presence of some vision?
a. The eyes do not move during a mirror test.
b. Proprioceptive testing results are normal.
c. The eyes move with rotation of an optokinetic nystagmus drum.
d. There is a normal pupillary reaction to bright light.
29. In a patient with a fixed, dilated pupil, which test result best helps
identify a pharmacologic blockade as opposed to a third nerve palsy or Adie
tonic pupil?
a. normal pupillary light response in the fellow eye
b. minimal pupillary constriction after 0.125% pilocarpine
c. rapid pupillary constriction after 10% phenylephrine
d. absent pupillary constriction after 1% pilocarpine
30. A 68-year-old patient presents with transient visual loss and double
vision. The patient works in telemarketing and has noted recent tongue
discomfort after 1 hour on the job.
Which of the following results supports your suspected diagnosis?
a. erythrocyte sedimentation rate= 10 mm/hr; C-reactive protein= 10 (normal,< 1)
b. negative result on temporal artery biopsy
c. normal platelet count
d. family history of autoimmune disease

31. A 25-year-old woman has a negative past medical history and a 2-week
history of pain on eye movement, a relative afferent pupillary defect, and
decreased color perception.
Which diagnostic study would be most appropriate?
a. fluorescein angiography with attention to the macula
b. screening blood work for human leucocyte antigen A-29 and B-5
c. magnetic resonance imaging of the brain with and without contrast
d. skin biopsy with microscopic dermal evaluation
32. A patient presents acutely with headache, mild ipsilateral ptosis, and
amaurosis fugax. She reports a history of trauma several weeks prior to
presentation.
Which study would you order first? a. computed tomography scan of the brain and orbits
b. bilateral carotid Doppler studies
c. magnetic resonance imaging (MRI) of the brain with and without contrast
d. MRI and magnetic resonance angiography of the neck

Answers
1. b. The interstitial nucleus of Cajal is the neural integrator for vertical and
torsional gaze. The nucleus prepositus hypoglossi is the neural integrator for
horizontal gaze. The nucleus raphe interpositus contains omnipause cells. The
rostral interstitial nucleus of the medial longitudinal fasciculus contains the
excitatory burst neurons for vertical and torsional gaze.
2. a. The posterior inferior cerebellar artery supplies the lateral medulla, where
sympathetic fibers continue from the hypothalamus.
3. d. V2 enters the foramen rotundum, V3 enters the foramen ovale, the middle
meningeal artery enters the foramen spinosum, and the internal carotid artery
passes through the foramen lacerum.
4. b. Nephrogenic fibrosing dermopathy is a potential complication of gadolinium
administration in a patient with renal disease. Many institutions require screening
by determination of serum creatinine levels before administering gadolinium.
5. a. Pseudopapilledema of the optic disc is typically associated with a small to
absent cup disc ratio. Obscuration of the retinal vessels by a thickened and
opacified retinal nerve fiber layer and hyperemia occur only in true edema of the
optic disc (papilledema). Blurring of the disc margins occurs with both
papilledema and Pseudopapilledema.
6. d. The visual acuity can be reduced to any level in 1 or both eyes with either
entity. Central scotomata occur with both maculopathies and optic neuropathies.
Amsler grid testing with missing lines can occur with both entities, whereas
Amsler grid testing with distorted lines is highly suggestive of retinopathy.
Normal eyes recover from a photostress test within 30 seconds.
7. b. Obesity, female sex, and young age are characteristic of idiopathic
intracranial hypertension, but they are not part of the diagnostic criteria. Blood
pressure should be evaluated in patients with papilledema, but it is not part of the
criteria. The opening pressure should be documented in the lateral decubitus
position not the prone position. The criteria specify that no mass lesion should be
apparent on neuroimaging.

8. c. Retinal ischemia is very common and can occur from a variety of
mechanisms. These include emboli, hypotension, vasospasm, and anemia, all of
which can result in decreased perfusion of the retina. Papilledema is one specific
mechanism of visual loss ( e.g., increased intracranial pressure) and thus occurs
less commonly than retinal ischemia. Recurrent hyphema is rare. Occipital lobe
ischemia causes bilateral visual loss.
9. a. Transient visual loss from an embolus typically lasts 10- 15 minutes and is
unilateral.
Migraine typically develops and resolves over a longer time period, 20-30
minutes. Also, migraine and seizure cause bilateral, not monocular, visual
disturbance. Drusen can cause monocular visual loss but the duration is typically
seconds.
10. b. A rise in body temperature does not affect retinal function, cardiac rhythm,
or intraocular pressure. Slowing of neural signals related to a rise in body
temperature occurs when the myelin sheath that contains the synaptic nodes is
damaged, as in optic neuritis.
11. b. Optic ataxia is a disconnection between visual input and the motor system.
Ocular motor apraxia is the loss of voluntary movement of the eyes while fixating
on a target.
Prosopagnosia is the inability to recognize familiar faces. Simultanagnosia is a
failure to integrate multiple elements of a scene.
12. c. This patient is affected by staticokinetic dissociation, also known as the
Riddoch phenomenon. Patients with Anton syndrome are cortically blind but
affirm, often quite adamantly, that they are capable of seeing. Palinopsia refers to
multiple afterimages. With visual allesthesia, patients see their environment
rotated, flipped, or inverted.
13. b. Alexia without agraphia results from interruption of visual information
between the occipital lobe and the dominant angular gyrus, causing a visual-
verbal disconnection (not a form of visual-spatial relationship disruption). It is
usually due to the infarction of the left occipital lobe and to fibers crossing in the
splenium of the corpus callosum. However, because the structures anterior to the
splenium are intact, these patients can produce language and write. Balint
syndrome consists of the triad of simultanagnosia, optic ataxia, and acquired
ocular motor apraxia.

14. c. The patient's symptoms are manifestations of the lateral medullary
syndrome (or Wallenberg syndrome), in which there is loss of ipsilateral facial
and contralateral body sensation. A central (first-order) Horner syndrome, leading
to ptosis and miosis, also may result when the descending neurons are damaged.
15. c. This patient has a supranuclear gaze palsy characteristic of progressive
supranuclear palsy. Patients usually lose down gaze first, and they will often have
exposure keratopathy because of an extremely slow blink rate.
16. c. This patient has a benign episodic pupillary mydriasis and no ocular
motility deficit or ptosis. In such a situation, third nerve palsy is not a
consideration. Many patients with migraine experience intermittent pupillary
mydriasis that does not correspond temporally to the headache itself.
17. a. The patient is likely to have ischemic sixth nerve palsy. Although
neuroimaging may be indicated, her age and medical history require that
unrecognized diabetes mellitus or giant cell arteritis be excluded as potential
causes before obtaining imaging.
18. b. The examination findings are concerning for a partial left third nerve palsy
with pupil involvement. A difference in reactivity, and not marked anisocoria,
may be the only sign.
In a patient of this age, aneurysm at the junction of the posterior communicating
artery and internal carotid artery is the most likely cause, and a major risk factor
for aneurysm formation is cigarette smoking.
19. d. The patient has opsoclonus, and the most likely cause in an adult is
paraneoplastic syndrome from a small cell carcinoma of the lung.
20. a. You are observing periodic alternating nystagmus (PAN). Because the
patient is symptomatic, it is probably acquired rather than congenital. In young
women, the most likely cause of PAN is demyelinating disease such as multiple
sclerosis. Brain magnetic resonance imaging with sagittal FLAIR sequences is
particularly sensitive for locating the typical white matter lesions of this disease.
21. a. Dorsal midbrain damage can result in midsize pupils with poor light
response and preserved near response. A lesion of the nucleus of Budge-Waller
causes Horner syndrome, as does a hypothalamic one. A lesion of the occipital
lobe does not affect the pupils.

22. b. Sectoral palsy of the iris sphincter is one characteristic of Adie tonic pupil.
Isolated unilateral mydriasis from a tonic pupil occurs from injury to the
postganglionic parasympathetic fibers, so there is no alteration of eyelid function.
Iris heterochromia and supersensitivity to apraclonidine are signs associated with
an oculosympathetic deficit.
23. a. Areflexia, ataxia, and ophthalmoplegia characterize Miller Fisher
syndrome, a variant of Guillain-Barre syndrome, and facial diplegia often
accompanies the classic triad. Herpes zoster involving the seventh nerve is called
Ramsay Hunt syndrome. It is diagnosed by the identification of vesicles along the
posterior aspect of the external auditory canal.
Melkersson-Rosenthal syndrome presents as recurrent unilateral or bilateral facial
paralysis and is accompanied by chronic facial swelling. A cerebellopontine angle
tumor may present with facial palsy, diplopia, hearing loss, and nystagmus.
24. b. Facial myokymia typically signifies intramedullary disease of the pons
involving the seventh nerve nucleus or fascicle. It is usually the result of a pontine
glioma or multiple sclerosis. Compression of the seventh nerve root exit zone by
an aberrant vessel has been associated with hemifacial spasm, which is
characterized by unilateral episodic spasm that involves the facial musculature.
Excessive caffeine intake may cause isolated eyelid myokymia. Aberrant
regeneration after facial palsy is typically not continuous.
25. b. This patient has paroxysmal hemicrania, a form of trigeminal autonomic
cephalgia highly responsive to indomethacin. Although cluster headache is also
frequently associated with autonomic features, the bouts of excruciating pain
associated with this disorder are of longer duration (15-180 minutes).
Hemicrania continua is characterized by a continuous unilateral headache.
Idiopathic stabbing headache manifests as episodic, very brief, sharp, jabbing
pains, unassociated with autonomic features.
26. c. Topiramate may result in acute bilateral angle-closure glaucoma and acute
myopic shift, which are usually reversible upon cessation of the drug. The other
agents do not commonly cause visual side effects.

27. c. The presence of a visual field defect requires further evaluation. A patient
with migraine headache and bilateral homonymous visual field deficit needs
neuroimaging study to exclude a structural brain disorder (e.g., mass, vascular
malformation). Pulsating headache is very common in patients with migraine.
Typical visual auras have a hemianopic distribution.
A family history of migraine is often but not always elicited in patients with
migraine headache.
28. c. In complete blindness, the eyes should not move with rotation of the
optokinetic nystagmus (OKN) drum. The OKN system uses smooth pursuit
followed by a saccade when the maximum amplitude of pursuit is exceeded,
eliciting movement. Patients with nonorganic loss of vision may be able to avoid
looking at the OKN by looking away during testing or focusing past the drum and
should be observed carefully during testing. Mirror testing is also very helpful in
establishing nonorganic total visual loss, and the eyes will mo e to follow the
mirror. Proprioceptive testing does not require vision, and pupils will react in the
presence of cortical blindness.
29. d. Administration of 1% pilocarpine does not overcome the pharmacologic
blockade and the pupil remains dilated. Large pupils resulting from either a third
nerve palsy or Adie tonic pupil may constrict following instillation of 0.125%
pilocarpine. Phenylephrine dilates but does not constrict the pupil. The fellow
pupil in a patient with either Adie tonic pupil or third nerve palsy should react
normally.
30. a. The erythrocyte sedimentation rate is normal in up to 16% of biopsy-proven
cases of giant cell arteritis (GCA). Temporal artery biopsy specimens do not
always demonstrate the pathology and may be negative even in cases of GCA.
The constellation of symptoms (jaw/tongue claudication along with transient
visual loss and diplopia) should make the clinician highly suspicious of GCA,
regardless of whether results of ancillary blood studies are normal. The elevated
level of C-reactive protein combined with a normal ESR would be supportive but
not diagnostic of GCA. Whereas certain human leukocyte antigen types may be
more common in GCA, it is not a traditionally inherited disorder.

31. c. The patient's history is consistent with optic neuritis. Magnetic resonance
imaging (MRI) is appropriate to look for risk factors for systemic demyelinating
disease. The presence of a single typical demyelinating lesion on MRI at
presentation increases the risk for developing clinically definite multiple sclerosis
to 72% and helps the patient determine the best course of action in terms of early
use of immune modulators.
32. d. MRI is the best diagnostic test in patients suspected of having carotid artery
dissection, which will not be definitively identified by carotid Doppler studies.
MRI or magnetic resonance angiography has better resolution for soft tissue than
does computed tomography.
Carotid ultrasound is not adequate for detecting arterial dissection.

06 - Pediatric Ophthalmology and Strabismus
1. A pediatrician performs the red reflex examination (Bruckner test) on a
3-month-old infant. What does this test assess?
a. accommodation
b. visual acuity
c. optic nerve function
d. ocular alignment
2. In visual acuity testing, what clinical finding is described by the crowding
phenomenon?
a. increase in performance when the patient's family leaves the examination room
b. increase in performance when reading a single optotype compared to a full line
c. decrease in performance after repeated testing
d. decrease in performance when Teller acuity cards are held too close to the
patient
3. What is the name of the alignment measurement when the paretic or
restricted eye is fixating?
a. primary deviation
b. secondary deviation
c. consecutive deviation
d. comitant deviation
4. What anatomical feature of the inferior oblique muscle differs from that of
the other extraocular muscles?
a. Its origin is on the medial side on the orbit.
b. It is innervated by the inferior division of cranial nerve III.
c. It passes through the trochlea before inserting on the globe.
d. Its primary action is elevation.
5. What is one of the primary components of the extraocular muscle pulleys?
a. elastin
b. striated muscle
c. hyaluronic acid
d. chondroitin sulfate
6. Which form of bilateral, symmetric refractive error at a level of 3.5
diopters would place a child at the greatest risk for isoametropic amblyopia?
a. myopia
b. hyperopia
c. astigmatism
d. no risk of isoametropic amblyopia
7. Which type of amblyopia is most likely to respond to treatment in a
teenager who has had no previous amblyopia therapy?
a. strabismic amblyopia
b. deprivation amblyopia
c. anisometropic amblyopia
d. reverse amblyopia
8. What are the primary synergistic (yoke) muscles that are used for gazing
up and to the right?
a. left inferior oblique and right superior oblique
b. left superior rectus and right inferior oblique
c. left inferior oblique and right superior rectus
d. left superior oblique and right superior rectus
9. What is the term for the positions of gaze in which a single extraocular
muscle is the prime mover of each eye?
a. secondary positions
b. midline positions
c. diagnostic positions
d. cardinal positions
10. What sensory adaptation to manifest strabismus is most commonly seen
in patients?
a. visual confusion
b. diplopia
c. stereopsis
d. peripheral suppression

11. What is the best test for measuring the amount of strabismus in a patient
who has an amblyopic eye with visual acuity of 20/400 and eccentric fixation?
a. simultaneous prism cover test
b. alternate cover test
c. Krimsky test
d. Lancaster red-green test
12. What treatment is most appropriate as initial therapy for high
accommodative convergence/accommodation (AC/ A) esotropia?
a. overminused spectacles
b. alternate occlusion
c. bifocal spectacles
d. base-in prism spectacles
13. What eye motility abnormality is commonly associated with infantile
esotropia?
a. manifest vertical nystagmus
b. dissociated vertical deviation (DVD)
c. symmetric smooth pursuit in horizontal gaze
d. ocular flutter
14. What type of exodeviation is most commonly seen in the general
population?
a. pseudoexotropia
b. infantile exotropia
c. type 2 Duane retraction syndrome
d. intermittent exotropia
15. For which type of exodeviation are orthoptic exercises the most
appropriate initial therapy?
a. Duane retraction syndrome
b. convergence insufficiency
c. dissociated horizontal deviation
d. positive angle kappa

16. A patient is found to have A-pattern exotropia with a compensatory head
posture. What head posture is the clinician most likely to observe?
a. chin up
b. chin down
c. right head tilt
d. right head turn
17. What clinical finding accompanies the upward movement of the eye in
DVD?
a. extorsion of the globe
b. downward movement of the fellow eye on cover testing
c. upbeat nystagmus
d. Esotropia
18. What clinical finding is most suggestive of a bilateral rather than
unilateral superior oblique muscle palsy?
a. extorsion of 5° in downgaze
b. exotropia worse in downgaze
c. large V pattern
d. chin-up head posture
19. What finding on examination of an esotropic patient makes the diagnosis
of type 1 Duane retraction syndrome more likely than the diagnosis of sixth
nerve palsy?
a. limited adduction of the affected eye
b. incomitant esodeviation
c. abnormal head position
d. limited abduction of the affected eye
20. What clinical finding is most helpful in distinguishing congenital motor
nystagmus (infantile nystagmus syndrome) from acquired nystagmus?
a. abnormal head position
b. oscillopsia
c. exponential decrease in velocity of the slow phase
d. change in direction of the fast phase depending on which eye is fixating
21. Four weeks after bilateral medial rectus muscle recession, a patient
presents with a new exotropia of 15 prism diopters. On examination, there is
limited adduction of the right eye. What is the most likely diagnosis?
a. anterior segment ischemia
b. adherence syndrome
c. conjunctival scarring
d. slipped muscle
22. What beneficial effect on the visual field can occur as a result of
strabismus surgery?
a. expansion of the binocular visual field following surgery for exotropia
b. constriction of an overly wide peripheral field following surgery for exotropia
c. expansion of the binocular visual field following surgery for esotropia
d. elimination of monofixation syndrome due to overlapping fields following
surgery for infantile Esotropia
23. What refractive condition is true for most infants during the first year of
life?
a. relatively flat cornea that steepens over time
b. hyperopic refractive error that decreases over time
c. intraocular lens power that increases over time
d. visual acuity of 20/30, measured by preferential looking (PL), that decreases
over time
24. What eye movement abnormality can occur in healthy infants in the first
months of life?
a. intermittent esotropia
b. constant exotropia
c. vertical nystagmus
d. ocular flutter
25. What congenital ocular disorder is most commonly associated with
paradoxical pupils?
a. aniridia
b. anterior segment dysgenesis
c. retinal dystrophy
d. cerebral visual impairment

26. At what age should an infant be able to maintain fixation and react with
facial expressions?
a. at birth
b. 2-3 weeks
c. 6- 8 weeks
d. 3 months
27.An 11-month-old girl presents for evaluation and is found to have
epiblepharon. The child is playful and asymptomatic, and there is no
evidence of corneal involvement. What would be the best initial treatment for
this child's condition?
a. observation
b. artificial tear eye drops every 4 hours
c. surgery to remove a strip of skin and orbicularis muscle from beneath the eyelid
margin
d. Quickert suture repair
28. Which of the following conditions of the affected eye may be associated
with pseudoptosis?
a. hypotropia
b. DVD
c. Duane retraction syndrome
d. infantile esotropia
29. What congenital eyelid malformation would most likely require early
repair?
a. dystopia canthorum
b. eyelid coloboma
c. euryblepharon
d. telecanthus
30. A 2-month-old infant has an enlarging hemangioma of an upper eyelid
and orbit, with anisometropic astigmatism and secondary blepharoptosis.
What is the preferred primary treatment for this patient?
a. topical timolol
b. intralesional corticosteroid injection
c. oral corticosteroid
d. oral propranolol

31. Orbital cellulitis can be distinguished from preseptal cellulitis by what
clinical finding?
a. prominent eyelid swelling
b. presence of sinusitis
c. chemosis
d. fever
32. What is the most common location of blockage in congenital nasolacrimal
obstruction?
a. upper canaliculus
b. valve of Hasner
c. lower punctum
d. valve of Rosenmiiller
33. Curvilinear tears in Descemet membrane are most often seen in what
ocular condition?
a. congenital hereditary endothelial dystrophy (CHED)
b. Peters anomaly
c. primary congenital glaucoma
d. amniocentesis injury
34. Congenital iris ectropion is most commonly seen in what genetic
disorder?
a. incontinentia pigmenti
b. neurofibromatosis 1
c. Marfan syndrome
d. cystinosis
35. What is the most important associated medical condition to exclude in a
patient with sporadic aniridia?
a. neuroblastoma
b. neurofibromatosis
c. Waardenburg syndrome
d. Wilms tumor

36. Which systemic medication is the most appropriate treatment for an
infant with ophthalmia neonatorum secondary to Chlamydia trachoma tis
infection?
a. erythromycin
b. doxycycline
c. ofloxacin
d. azithromycin
37. What is the most severe ocular complication of Stevens-Johnson
syndrome?
a. conjunctival scarring
b. panuveitis
c. acute retinal necrosis
d. corneal ulcer
38. What finding predisposes a child to glaucoma following surgery for
congenital cataract?
a. small corneal diameter
b. optic nerve hypoplasia
c. persistent pupillary membrane
d. posterior subcapsular lens opacity
39. What is the pattern of genetic inheritance in the majority of patients with
primary congenital glaucoma?
a. autosomal dominant
b. sporadic
c. X-linked recessive
d. autosomal recessive
40. In what genetic disorder is pupillary block glaucoma most likely to
occur?
a. ectopia lentis et pupillae
b. Marfan syndrome
c. aniridia
d. Weill-Marchesani syndrome

41. What type of uveitis is most common in children?
a. panuveitis
b. posterior uveitis
c. intermediate uveitis
d. anterior uveitis
42. That is the most significant risk factor for developing retinopathy of
prematurity (ROP)?
a. male sex
b. gestational age
c. white race
d. lung disease
43. Why are magnetic resonance imagings (MRI) and ultrasonography the
preferred imaging modalities instead of a computed tomography (CT) scan in
a pediatric patient with presumed retinoblastoma?
a. .tvlRI and ultrasonography are better at detecting calcium in the tumor.
b. CT scan subjects the child to radiation.
c. MRI and ultrasonography are better at showing bony abnormalities in the orbit.
d. MRI and ultrasonography are easier to obtain in a child.
44. Moyamoya disease is associated with what ophthalmic disorder?
a. CHARGE syndrome
b. morning glory disc anomaly
c. myelinated retinal nerve fibers
d. optic nerve hypoplasia
45. A patient is diagnosed with Pseudopapilledema. What other ophthalmic
finding is frequently seen on examination?
a. hyperopia
b. myopia
c. esotropia
d. exotropia

46. A 5-mm traumatic hyphema, right eye, is diagnosed in a 12-year-old
African American patient. Intraocular pressure is 22 mm Hg OD and 12 mm
Hg OS. What laboratory test is indicated?
a. human leukocyte antigen B27 (HLA-B27)
b. antinuclear antibody (ANA) titer
c. sickle cell
d. B-thalassemia
47. What is the best management of a "white-eyed" blowout fracture in a
child?
a. observation since this injury resolves without treatment
b. observation for 1 month, then surgical repair of the fracture if the injury does
not resolve
c. observation for 6 months, then strabismus surgery if the child still has diplopia
d. early surgical repair of the fracture
48. What is the most common cause of visual impairment in children with
abusive head trauma?
a. cortical or cerebral visual impairment
b. optic atrophy
c. retinal detachment
d. vitreous hemorrhage
49. What is the mode of inheritance of incontinentia pigmenti?
a. autosomal dominant
b. X-linked recessive
c. X -linked dominant
d. mitochondrial DNA defect
50. What is the most common mode of inheritance of neurofibromatosis 1
(NF 1)?
a. autosomal recessive
b. X -linked recessive
c. mitochondrial
d. autosomal dominant

Answers
1. d. The red reflex examination (Bruckner test) evaluates the clarity and
symmetry of the red reflex, identifies significant or asymmetric refractive errors,
and determines the position of the corneal light reflex, which provides an estimate
of ocular misalignment.
2. b. The crowding phenomenon is a characteristic feature of amblyopia in which
letters or symbols of a given size are more difficult to recognize if they are closely
surrounded by similar forms. As a result, the measured "linear" acuity of an
amblyopic eye may be worse than visual acuity measured with isolated optotypes.
For this reason, for the detection of amblyopia, it is best that isolated letters or
pictures not be used to test visual acuity, if possible.
3. b. A secondary deviation is the deviation measured when the paretic or
restricted eye is fixating. It is larger than a primary deviation, which is the
deviation measured when the non paretic eye is fixating. A consecutive deviation
is a strabismus that is in the direction opposite to one that the patient had
originally. A comitant deviation is a strabismus that is the same size in all
positions of gaze.
4. a. The inferior oblique muscle is the only extraocular muscle whose origin is on
the medial orbital wall. The inferior division of the third cranial nerve innervates
the medial rectus, inferior rectus, and inferior oblique muscles. The superior
oblique muscle is the only extraocular muscle that passes through the trochlea.
The primary action of the inferior oblique muscle is extorsion. The primary action
of the superior rectus muscle is elevation.
5. a. Elastin is one component of the pulley; the others are smooth muscle and
collagen. Striated muscle, hyaluronic acid, and chondroitin sulfate are not known
constituents of the pulleys.
6. c. significant levels of astigmatism can lead to isoametropic amblyopia.
Children with moderate degrees of myopia see clearly at near and are not at risk
for bilateral amblyopia. Children with moderate levels of hyperopia are capable of
accommodating to provide clear vision at distance and at near.
7. c. Some cases of anisometropic amblyopia remain responsive to treatment
(optical correction, occlusion therapy, pharmacologic penalization) in the
teenaged years.

8. c. The left inferior oblique and right superior rectus muscles are the prime
agonists for gaze into that position. Options a and dare not correct, because the
superior oblique muscle is a depressor of the eye. Option b is not correct, as the
right inferior oblique muscle has its main elevation action in left gaze.
9. d. By having the patient move the eyes to the 6 cardinal positions, the clinician
can isolate and evaluate the ability of each of the 6 extraocular muscles to move
each eye.
10. d. Peripheral suppression is the sensory adaptation that can develop in
strabismic patients to eliminate diplopia. Visual confusion and diplopia are the
normal consequences of strabismus when there are no sensory adaptations to
prevent them. Although some degree of stereopsis may be present in small-angle
strabismus with monofixation syndrome, good stereopsis indicates that there is no
manifest strabismus and no suppression.
11. c. The Krimsky test does not rely on a sensory or motor response from the
patient. Motor test results will not be accurate if there is eccentric fixation. The
Lancaster test depends on the patient's subjective localization of the targets, which
may not be accurate in the presence of poor vision or anomalous retinal
correspondence.
12. c. Bifocals reduce the need for accommodation at near and thus allow the
potential development of fusion and stereopsis. Overminused glasses increase
accommodation. Alternate occlusion theoretically reduces suppression but has no
role in the treatment of high AC/ A esotropia. Base-in prism would increase the
deviation in a patient with high AC/ A esotropia.
13. b. Dissociated vertical deviation (DVD) is associated with infantile esotropia.
Vertical nystagmus and ocular flutter are not. Patients with infantile esotropia
have asymmetric smooth pursuit, which is better in the temporal to nasal
direction.
14. d. Intermittent exotropia is the most common exodeviation. Infantile exotropia
and type 2 Duane retraction syndromes are uncommon entities. Pseudoexotropia
is the result of certain facial features or a structural abnormality of the retina and
is not a true strabismus disorder.

15. b. Orthoptic training to stimulate convergence may improve the deviation in
patients with convergence insufficiency, a type of convergence weakness
exotropia. Patients with Duane retraction syndrome may present with exotropia
due to decreased adduction. Dissociated strabismus may manifest with an
exodeviation. Both Duane retraction syndrome and dissociated strabismus are
treated surgically. Positive angle kappa is a form of pseudostrabismus, in which
the eyes appear exotropic, but the visual axes are optical!) aligned.
16. b. Since A and V patterns are variations of a primary position horizontal
misalignment, there is no reason for a compensatory head position unless it allows
single binocular vision.
For a patient with A-pattern exotropia, single binocular vision, if achievable, is
attained only with the eyes directed upward; hence, a chin-down head position is
most likely. Head tilting or viewing in lateral gaze does not achieve this result.
17. a. Patients with dissociated strabismus may have accompanying extorsion and
exodeviation (not esodeviation) of the elevating eye. Typically, there is no
hypodeviation of the fellow eye on cover testing, due to an apparent violation of
Hering's law of motor correspondence.
DVD is usually seen in infantile strabismus. In this form of strabismus, any
associated nystagmus is of the latent variety, which has a horizontal vector.
18. c. Bilateral superior oblique muscle dysfunction causes a large difference in
horizontal tropia between downgaze and up gaze. Extorsion in bilateral palsy is
usually well over 10 degree in downgaze. There is usually an esotropic shift in
downgaze, and the head posture would be chin down to avoid the cyclodiplopia in
downgaze.
19. a. Slight limitation of adduction is present in many cases of type 1 Duane
retraction syndrome, if looked for carefully. The features listed in options b, c,
and d can be seen in both disorders.
20. a. Patients with congenital motor nystagmus (CMN; infantile nystagmus
syndrome) often adopt an abnormal head position to take advantage of the better
vision that is possible at a null point. Oscillopsia is characteristic of nystagmus
acquired in adulthood and is rare in CMN. An exponential decrease in velocity of
the slow phase and a fast-phase direction that reverses with a change in fixation
are characteristic of latent nystagmus (fusional development nystagmus
syndrome).

21. d. Limited adduction is evidence that the medial rectus muscle has reattached
too far posteriorly to be effective as an adductor of the eye. Anterior segment
ischemia does not typically limit rotation and would not be expected after
operation on just 1 extraocular muscle per eye. Adherence syndrome causing
restriction would arise from adherence created on the opposite aspect of the globe,
and the lateral rectus muscle was not included in the procedure. Conjunctival
scarring over the medial rectus muscle would, if anything, limit abduction.
22. c. Correction of esotropia can expand the binocular visual field. Surgery for
exotropia constricts the binocular visual field. Monofixation is not eliminated in
patients with infantile strabismus even if the eyes are aligned well.
23. b. In general, eyes are hyperopic at birth, becoming more so until age 7 years,
when they experience a myopic shift toward plano. The newborn has a steeper
cornea and a higher intraocular lens power, both of which decrease over time.
Visual acuity of infants aged 3 months is in the 20/120 range when measured by
preferential looking (PL). Visually evoked potential (VEP) testing estimates
acuity to be 20/20 at 6 months of age.
24. a. In the first few months of life, episodes of intermittent strabismus are
common. Constant strabismus is not normal, even at this early age. Vertical
nystagmus and ocular flutter are also not normal.
25. c. Inherited retinal dystrophies are the most common cause of paradoxical
pupils. Patients with aniridia and anterior segment dysgenesis have abnormal
irises but not paradoxical pupils. Pupillary reactions are normal in cerebral visual
impairment.
26. c. Although there is some variability, the nervous system is typically mature
enough at age 6- 8 weeks for an infant to maintain visual fixation and react with
facial expressions.
27. a. Although epiblepharon may produce an in-turning of the eyelashes, there is
often minimal or no irritation of the cornea. If no significant fluorescein staining
of the cornea is detected, only observation is required. The piblepharon often
resolves spontaneously with time and seldom requires surgical treatment.

28. a. The upper eyelid "follows" the eye in upgaze and downgaze; that is, the
eyelid moves in the same direction as the eye. Therefore, the upper eyelid of a
hypotropic eye will be lower than that of the fellow eye, producing the false
appearance of ptosis. Conditions that cause hypertropia or horizontal strabismus
do not cause pseudoptosis.
29. b. Eyelid coloboma (eyelid cleft, eyelid notch) carries a risk of exposure
keratopathy, and early closure of the eyelid defect is often required.
30. d. Although all the listed treatments may be effective for some hemangiomas,
oral propranolol is now preferred for the treatment of vision-threatening
periocular hemangiomas. Topical timolol may be an effective treatment for
superficial hemangiomas but not for orbital lesions.
31 . c. The presence of chemosis suggests orbital involvement. Eyelid swelling,
sinusitis, and fever may be present with both preseptal cellulitis and orbital
cellulitis.
32. b. Nasolacrimal duct obstruction typically occurs at the most distal portion of
the lacrimal duct, because of incomplete canalization at or around full-term
gestation (40 weeks) of what was a solid structure in the fetus. This blockage
occurs at the valve of Hasner. The canaliculi and puncta and the valve of
Rosenmiiller, which is in the region of the junction of the canaliculi, are more
likely to have canalized normally.
33. c. Tears in Descemet membrane (Haab striae) are seen because of a rapid
stretching of the cornea in primary congenital glaucoma. They are not seen in
congenital hereditary endothelial dystrophy (CHED) or Peter’s anomaly. Trauma
from amniocentesis may result in a penetrating injury of the cornea. Tears in
Descemet membrane may also be seen in a forceps injury sustained during
delivery, but these are usually linear, not curvilinear.
34. b. Congenital iris ectropion may be an isolated finding, or it may be associated
with neurofibromatosis 1, Prader-Willi syndrome, or facial hemihypertrophy.
Retinal abnormalities may be seen in incontinentia pigmenti; dislocated lenses, in
Marfan syndrome; and corneal crystals, in cystinosis.
35. d. In patients with sporadic aniridia, the presence of Wilms tumor must be
excluded with a renal ultrasound scan, which must be repeated until molecular
genetic analysis rules out an llpl3 deletion and confirms an intragenic PAX6

mutation. Iris abnormalities that are associated with systemic abnormalities
include neuroblastoma in patients with Horner syndrome, Lisch nodules in
patients with neurofibromatosis, and heterochromia in patients with Waardenburg
syndrome.
36. a. Infants with Chlamydia trachomatis infection acquired at birth may present
with papillary conjunctivitis during the first week of life. Although the eye disease
is usually selflimited, C trachomatis infection may cause pneumonia and otitis
media in neonates.
Therefore, systemic treatment with oral erythromycin is indicated.
37. d. Conjunctivitis is a common ocular manifestation of Stevens-Johnson
syndrome. In severe cases, progressive scarring of the conjunctiva and eyelids
may lead to corneal complications, including ulceration and perforation.
Panuveitis and acute retinal necrosis are not associated with Stevens-Johnson
syndrome.
38. a. Microcornea is associated with higher incidences of glaucoma following
cataract surgery in children.
39. b. Primary congenital glaucoma usually occurs sporadically, but it may be
inherited as an autosomal recessive trait. Specific genetic mutations have been
identified in some patients.
40. d. Weill-Marchesani syndrome is associated with microspherophakia. The
microspherophakic lens in this syndrome may dislocate into the anterior chamber,
causing pupillary block glaucoma. In the other conditions, dislocation into the
anterior chamber does not usually occur.
41. d. Anterior uveitis is the most common uveitis seen in children. It is most
often idiopathic, related to trauma, or associated with juvenile idiopathic arthritis.
42. b. The 2 strongest risk factors for retinopathy of prematurity (ROP) are
gestational age and birth weight. Although race and lung disease are also risk
factors, they are not as significant as gestational age and birth weight. There is no
difference in the risk of ROP between the sexes.

43. b. Unlike magnetic resonance imaging (MRI) and ultrasonography, a
computed tomography (CT) scan subjects patients to radiation. Children with
heritable retinoblastoma are at high risk for secondary radiation-induced tumors,
so any additional radiation should be avoided, if possible.
44. b. Morning glory disc anomaly has been associated with basal encephalocele
in patients with midfacial anomalies, PHACE syndrome (posterior fossa
malformations, hemangiomas, arterial lesions, cardiac and eye anomalies), and
abnormalities of the carotid circulation, including moyamoya disease.
45. a. Optic discs with small cup- disc ratios that may resemble papilledema are
commonly seen in hyperopic eyes. Optic discs in myopic eyes do not have this
appearance. Strabismus is not associated with pseudopapilledema.
46. c. Sickle cell testing must be performed in all African American patients with
hyphema. Because of sickling of the red blood cells in the anterior chamber,
sickle cell trait or disease may result in elevated intraocular pressure, even in the
presence of a small hyphema.
47. d. "White-eyed" blowout fractures present with marked vertical motility
restriction in both directions with minimal soft-tissue findings. Unless there is
early surgical repair of the fracture, the inferior rectus muscle and its associated
nerve can be permanently damaged.
48. a. The most common cause of visual impairment in children with abusive
head trauma is from cortical or cerebral visual impairment due to neurologic
damage. Optic atrophy and retinal injury may also cause decreased vision, but
they are less common causes.
49. c. Incontinentia pigmenti shows the unusual inheritance pattern of X -linked
dominance with a presumed lethal effect on the hemizygous male fetus.
50. d. Neurofibromatosis 1 shows autosomal dominant inheritance. However,
approximat ly 50% of patients do not have a family history of the disease,
reflecting the high rate of new mutations in the responsible gene.

7 - Orbit_ Eyelids and Lacrimal System
1. When removing bone from the medial wall of the orbit in an orbital
decompression, the surgeon can locate the ethmoidal arteries along the
a. spheno ethmoidal recess
b. superior orbital fissure
c. fronto ethmoidal suture
d. infra orbital canal
2. Orbital computed tomography (CT) scanning of a patient with a dural
cavernous sinus fistula is likely to show enlargement of which one of the
following blood vessels?
a. central retinal vein
b. pterygopalatine venous plexus
c. superior ophthalmic vein
d. inferior ophthalmic vein
3. That disease might be indicated by a salmon- or pink-colored mass in the
conjunctival cul-de-sac?
a. orbital lymphoma
b. systemic lupus erythematosus
c. Lymphangioma
d. xanthogranuloma
4. What condition typically presents with proptosis and axial displacement of
the globe?
a. maxillary sinus tumors invading the orbital floor
b. lacrimal gland tumors
c. frontoethmoidal mucocele
d. intraconal cavernous hemangioma
5. What is the best technique for visualizing the orbitocranial junction?
a. magnetic resonance imaging (MRI)
b. CT scanning
c. ultrasonography
d. plain films

6. A 61-year-old man presents with a 1-week history of redness and pain of
the right eye. He wonders if this is related to his chronic sinus problems. On
examination, his visual acuity is 20/20. His right upper eyelid is swollen. The
right conjunctiva is injected with dilated episcleral vessels inferiorly. The
underlying sclera appears inflamed. His ocular motility is limited, and there
is 2 mm of proptosis in the right eye. A CT scan shows a diffuse infiltrate in
the right inferior orbit. There is also thickening of the left nasal mucosa.
Which of the following tests would be most beneficial in diagnosing this
patient's condition?
a. serum rheumatoid factor
b. conjunctival culture for bacterial and viral pathogens
c. serum erythrocyte sedimentation rate (ESR) and C-reactive protein
d. serum antineutrophil cytoplasmic antibodies (AN CAs)
7. A previously healthy 6-year-old child presents with proptosis of the left
eye.
Family photographs reveal some prominence of the eye for the past year.
One week prior to presentation, the child had a seizure of undetermined
cause. Fundus examination reveals choroidal folds in the left eye. Which one
of the following diagnostic tests is least useful in this case?
a. fluorescein angiography
b. orbital ultrasound
c. MRI
d. CT scan
8. What advantages does CT scanning of the orbit offer over MRI?
a. better view of bone
b. better soft tissue detail
c. better image of the orbital apex
d. more motion artifact
9. Which of the following lesions is most likely to be found in the superonasal
quadrant of the orbit?
a. Wagener granulomatosis
b. mucocele
c. benign mixed tumor
d. meningioma
10. Perineural invasion and pain are associated with which of the following
orbital tumors?
a. esthesioneuroblastoma
b. adenocarcinoma of the lacrimal gland
c. adenoid cystic carcinoma of the lacrimal gland
d. rhabdomyosarcoma
11. All of the following orbital diseases may improve with corticosteroids
except
a. thyroid eye disease
b. orbital mucocele
c. nonspecific orbital inflammation
d. orbital lymphoma
12. A patient presents with a lacrimal fossa lesion. CT scanning shows a
poorly circumscribed lesion with bone destruction.
The most likely diagnosis is
a. lymphoma
b. adenoid cystic carcinoma of the lacrimal gland
c. benign mixed tumor
d. nonspecific orbital inflammation
13. A patient with declining visual acuity has an optic nerve sheath
meningioma that does not extend outside the orbit. Which of the following is
the best treatment?
a. systemic corticosteroid therapy
b. fractionated stereotactic radiation therapy
c. proton beam radiation
d. exenteration
14. The most common cause of unilateral proptosis in adults is
a. lymphoma
b. cavernous hemangioma
c. thyroid eye disease
d. meningioma

15. What is the study of choice for the evaluation of fractures in acute orbital
trauma?
a. MRI
b. CT scanning
c. nerve conduction
d. orbital ultrasound
16. A 30-year-old man is evaluated in the emergency room for trauma to the
right orbit. The patient has marked proptosis and an intraocular pressure of
40 mm Hg on the affected side. A CT scan shows intraorbital hemorrhage.
Which of the following actions would be the least effective in acutely reducing
intraocular pressure?
a. lateral canthotomy and cantholysis
b. administration of topical aqueous suppressants
c. administration of intravenous mannitol
d. administration of high-dose oral corticosteroids
17. Naso-orbital-ethmoidal fractures are most commonly associated with
which one of the following findings?
a. epiphora
b. infraorbital nerve hyposthesia
c. facial nerve palsy
d. trismus
18. The best approach to an intraconal orbital tumor located between the
optic nerve and the lateral rectus is
a. transcaruncular orbitotomy
b. vertical eyelid-splitting orbitotomy
c. medial orbitotomy
d. lateral orbitotomy
19. Dermoid and epidermoid cysts of the orbit are typically located
a. deep in the orbit when seen in young children
b. within the lacrimal gland
c. along the inferior orbital rim
d. in the superior temporal or superior nasal orbital quadrant

20. A biopsy is obtained for a presumed lympho proliferative disorder. The
appropriate way to submit the tissue is
a. alcohol-fixed
b. fresh
c. formalin-fixed
d. frozen
21. During decompression of the orbital floor, diplopia and dystopia can be
minimized by preserving
a. the palatine bone
b. the orbital strut between the medial wall and floor
c. the zygomatic bone
d. the ethmoid bone
22. Which of the following is most important in the management of dermoid
cysts of the orbit?
a. deferring surgery until age 8 to avoid causing bony deformity
b. filling in any bony defects with bone substitute (e.g. hydroxyapatite)
c. early removal to avoid malignant transformation
d. removal of all cyst walls and cyst content
23. The primary advantage of nonporous compared to porous orbital
implants is
a. better orbital volume replacement
b. lower exposure rates
c. increased implant stability
d. better prosthesis motility
24. The principle drawback to using a dermis-fat graft for acquired
anophthalmos in adults is
a. donor site morbidity
b. unpredictable resorption of volume
c. high extrusion rate
d. high infection rate

25. What is the treatment of choice for keratoacanthoma?
a. observation
b. corticosteroid injection
c. incisional biopsy followed by complete surgical excision
d. cryotherapy
26. When planning reconstruction of an eyelid defect, the surgeon should
a. replace both anterior and posterior lamella with grafts
b. avoid undermining adjacent tissue
c. minimize vertical tension
d. allow wounds to granulate prior to reconstruction
27. Appropriate management of multiple or recurrent chalazia includes
a. needle biopsy
b. shave biopsy
c. local injection with triamcinolone
d. full-thickness biopsy
28. The following measurements are obtained bilaterally in a patient with
congenital ptosis: margin- reflex distance (MRD), + 1 mm; eyelid fissure,
5 mm; and eyelid excursion, 4 mm. Which of the following bilateral surgical
procedures is the most appropriate?
a. frontalis suspension
b. maximal external levator resection
c. Fasanella-Servat
d. miillerectomy
29. In a tarsal strip lateral canthoplasty, the strip is sutured to the
a. opposite eyelid margin tarsus
b. opposite limb of the lateral canthal ligament
c. periosteum inside the lateral orbital rim
d. periosteum external to the lateral orbital rim
30. The lacrimal sac is located
a. between the anterior and posterior crura of the medial canthal tendon
b. in the lacrimal gland fossa
c. under the inferior turbinate
d. anterior to the orbicularis muscle

31. A 45-year-old man has a mass medial to the inferior punctum and a
yellow discharge from the punctum. Which of the following is the most
appropriate management option?
a. curettage with possible incision of the punctum
b. aspiration of the mass with a large-bore needle
c. oral steroids
d. Dacryocystorhinostomy (DCR)
32. The cause of congenital nasolacrimal obstruction is
a. maldevelopment of the valve of Rosenmiiller
b. membranous block of the valve of Hasner
c. retention of amniotic fluid in the nasolacrimal sac
d. trauma during delivery

Answers
1. c. The frontoethmoidal suture line defines the junction between the orbit and
sinuses (below) and the anterior cranial fossa (above). This suture line is the
superior-most level reached along the medial orbital wall in orbital decompression
surgery. The anterior and posterior ethmoidal arteries pass through their
respective foramina in this suture line, providing further anatomic clues to define
the location within the orbit.
2. c. The superior ophthalmic vein drains into the cavernous sinus and is typically
seen on neuroimaging studies coursing across the superior orbit. This vein
enlarges in conditions such as dural cavernous sinus fistula that increase venous
pressure within the cavernous sinus, with the superior ophthalmic vein
transmitting this pressure into the orbit.
3. a. Orbital lymphoma primarily affects the anterior orbit and may be seen
protruding beneath the conjunctiva in the cul-de-sac. Systemic lupus
erythematosus may cause telangiectasia and edema of the eyelids. Lymphangioma
has a vascular appearance and may affect the conjunctiva. Necrobiotic
xanthogranuloma is associated with skin lesions with a propensity to ulcerate and
fibrose.
4. d. An enlarging mass in the intraconal space such as a cavernous hemangioma
would mechanically push the globe forward, resulting in axial proptosis.
Maxillary sinus tumors are more likely to cause the globe to move superiorly
(hyperglobus), and frontoethmoidal mucocele will push the globe inferolaterally.
An enlarging lesion in the lacrimal gland fossa will cause inferomedial
displacement and proptosis.
5. a. MRI provides excellent tissue contrast of structures in the orbital apex,
intracanalicular portion of the optic nerve, and orbitocranial processes. CT
provides poor definition of the orbital apex. Ultrasonography is of limited value in
assessing lesions of the posterior orbit because of sound attenuation. Plain films
do not provide the level of definition obtained with CT or MRI.

6. d. The patient has a diffuse orbital inflammatory process with possibly related
sinus disease on the opposite side. Inflammation associated with rheumatoid
disease or an infectious process is unlikely to cause this. Giant cell arteritis
associated with an elevated ESR and C-reactive protein rarely causes an orbital
ischemic syndrome, but the patient is unlikely to retain good vision at that point.
Wegener granulomatosis is associated with elevated serum cytoplasmic ANCAs
and may cause a diffuse orbital inflammation with sinus involvement and small-
vessel vasculitis affecting any organ system.
7. a. Although fluorescein angiography may highlight the choroidal folds, the
pathology most likely to be the primary cause of problems in this patient will
occur in the orbit and brain. CT, MRI, or ultrasound would be useful in the
diagnostic evaluation of an orbital mass or an orbital mass with a possible
intracranial lesion.
8. a. CT scanning offers exquisite detail of bone, which has little or no signal on
MRI. The newest CT scanners have very short image acquisition times, whereas
the physics of MRI demand a longer image acquisition time that makes motion
artifact a potential problem.
MRI generally outdoes CT in soft tissue contrast and imaging of the orbital apex,
where surrounding bone may obscure soft tissue changes on CT.
9. b. Mucoceles, resulting from obstruction of the sinus excretory ducts, most
commonly arise from the frontal or ethmoidal sinuses, thereby producing a
superonasal mass when they expand into the orbit.
10. c. Although also malignant, rhabdomyosarcoma, lacrimal gland
adenocarcinoma, and esthesioneuroblastoma are not associated with the rate of
Perineural invasion that is seen in adenoid cystic carcinoma of the lacrimal gland,
the most common malignant tumor of the lacrimal gland.
11. b. Orbital inflammatory processes would be expected to respond to anti-
inflammatory agents such as steroids. Orbital lymphoma initially improves with
steroids, although it would not be expected to resolve completely and would
generally recur. An orbital mucocele is not an inflammatory process and should
not respond to steroids.

12. b. Orbital bone destruction is most commonly seen in the highly malignant
adenoid cystic carcinoma of the lacrimal gland; however, even aggressive
histologic variants of orbital lymphoproliferative disease have been associated
with bone destruction as well.
13. b. Treatment of optic nerve sheath meningiomas is tailored to the individual
patient based on the amount of visual loss and presence or absence of intracranial
extension. Progressive visual loss with a tumor confined within the orbit is best
treated with stereotactic radiotherapy. Attempts at surgical resection mostly result
in visual loss or spread of tumor.
14. c. Thyroid eye disease is the most common cause of both unilateral and
bilateral proptosis in adults. Proptosis is seen in up to 60% of patients with thyroid
eye disease.
15. b. Excellent bony detail with simultaneous resolution of soft tissues makes CT
scanning the study of choice in the evaluation for fractures with acute orbital
trauma. MRI and orbital ultrasound studies may provide better detail of certain
soft tissues and have greater utility in the evaluation of certain foreign bodies, but
do not provide the bony detail seen in CT.
16. d. The trauma with proptosis suggests extrinsic compression of the globe,
which raises intraocular pressure. A lateral canthotomy and cantholysis will
typically lower intraocular pressure in this situation. Mannitol and topical aqueous
suppressants will lower intraocular pressure arising from intrinsic or extrinsic
factors. High-dose corticosteroids are postulated to have neuroprotective effects,
but also carry numerous risks. They have no direct immediate effect on
intraocular pressure.
17. a. Naso-orbital-ethmoidal fractures frequently involve the bones and soft
tissues around the canthal tendons and lacrimal apparatus, including the
nasolacrimal duct. Tearing due to damage at any of these levels is a frequent
accompaniment to these fractures.
18. d. Lateral orbitotomy provides the most direct route to this lesion located
between the nerve and the lateral rectus muscle. Medial incisions such as the
transcaruncular and medial orbitotomy would lead to the medial orbital space on
the opposite side of orbit compared to the lesion. The eyelid-splitting incision
would also take the surgeon through a less-direct route to the lateral wall.

19. d. These lesions are thought to occur at lines of fetal suture closure. They are
commonly (70%) located around the fronto-zygomatic suture line. They also
occur at other fetal tissue suture lines, especially in the head and neck.
20. b. An essential step in pathologic examination for lymphoproliferative disease
is the use of flow cytometry or other examinations for cell surface markers, to
determine whether there is a monoclonal proliferation suggesting lymphoma. The
specimen may be divided, with a portion submitted in formalin, but studies of
fresh tissue are the most definitive.
21. b. Complete removal of the orbital floor with release of the periosteum may
result in downward displacement of the globe following orbital decompression.
Risks for this are diminished if the anterior portion of the medial orbital strut is
left intact.
22. d. The surgical goal is to remove the entire lesion with the cyst wall intact.
Leaving behind any of the wall of a dermoid cyst will result in recurrence of the
lesion. Leaving any keratin contents behind will result in an acute inflammatory
reaction. Dermoid cysts are often removed when they become clinically apparent
to prevent rupture and an inflammatory reaction. Bone remodeling rarely requires
intervention, and malignant transformation is rare.
23. b. Nonporous implants are an excellent, cost-effective choice for patients not
requiring implant integration and have a lower rate of extrusion when compared to
porous implants.
They transfer motility to the ocular prosthesis only though passive movement.
24. b. Although dermis-fat grafts tend to grow with surrounding orbit in children,
in adults resorption is unpredictable. They are valuable when there is limited
conjunctiva in the socket and can be used as patch grafts in cases of implant
exposure.
25. c. Although gradual involution over months has been observed with
keratoacanthoma, this is regarded as a low-grade squamous cell carcinoma. Thus
complete surgical excision is recommended.
26. c. Vertical tension on the eyelids can cause eyelid retraction or ectropion.
When planning reconstruction of an eyelid defect, the tension of closure should be
directed horizontally.

27. d. Recurrent chalazion may represent an underlying malignancy. Sebaceous
adenocarcinoma may originate in the tarsal plate or the lash margin. A superficial
shave biopsy may reveal chronic inflammation, but miss an underlying tumor.
Thus a full-thickness diagnostic biopsy of the eyelid is recommended.
28. a. Frontalis suspension is correct, because this is a severe, bilateral ptosis with
poor levator function. Mullerectomy and the Fasanella-Servat procedure generally
work better in patients with mild cases of ptosis with better levator function.
Large levator resections can work with in patients with poor levator function but
in a unilateral, not bilateral, case.
29. c. The lateral tarsal strip needs to be attached to the periosteum inside the
orbital rim so that the eyelid will be well-apposed to the globe. Suturing the strip
to the external periosteum would leave the eyelid too distracted from the globe.
Attachment to the opposite eyelid margin and canthal limb would not provide
adequate support or place the eyelid in the proper position with respect to the
globe.
30. a. The lacrimal sac is located in the anterior medial orbit within a bony fossa
that is bordered by the anterior and posterior lacrimal crests, to which the anterior
and posterior crura of the medial canthal tendon attach.
31. a. The initial treatment of canaliculitis is curettage, which may require snip
incision of the puncta to allow access. Some surgeons advocate initial
conservative treatment with warm soaks, digital massage, and topical antibiotic
therapy.
32. b. The most common cause of congenital nasolacrimal obstruction is a
membranous block of the valve of Hasner at the distal end of the duct. Congenital
dacryocystoceles (amniotoceles) are caused by retained amniotic fluid in the
nasolacrimal sac due to proximal and distal obstruction.
08 - External Disease and Cornea
1. From what source does the cornea receive most of its glucose for nutrition?
a. tear film
b. aqueous humor
c. limbal blood vessels
d. corneal epithelium
2. A 72-year-old woman reports experiencing a foreign-body sensation in her
eyes. The referring ophthalmologist thought she had dry eyes, yet her
symptoms have not been relieved by artificial tear supplementation
throughout the day or use of topical cyclosporine.
Which clinical sign would suggest another etiology for her underlying
problem?
a. Schirmer test result <5.5 mm after 5 minutes without anesthetic
b. tear meniscus height of 0.5 mm
c. tear breakup time of 4 seconds
d. redundancy of the inferior bulbar conjunctiva overhanging the lower eyelid
margin
3. Which of the following laboratory test results would be consistent with dry
eye?
a. tear hyperosmolarity
b. decreased level of matrix metalloproteinase-9
c. increased level of tear lactoferrin
d. increased level of tear lysozyme
4. Which of the following treatments is a good therapeutic option for initial
treatment of a neurotrophic corneal ulcer?
a. Gundersen flap placement
b. Boston keratoprosthesis
c. tarsorrhaphy
d. bandage contact lenses

5. What is the most appropriate initial treatment of unilateral stem cell
deficiency with irregularity extending into the visual axis that is secondary to
contact lens use?
a. Boston type I keratoprosthesis
b. corneal debridement
c. discontinuation of contact lens use
d. limbal stem cell allograft transplantation
6. Unlike the human immunodeficiency viruses, viruses of the family
Adenoviridae have a differential ability to survive for weeks on inanimate
surfaces. This ability is best explained by which anatomical feature of the
Adenoviridae?
a. their double-stranded DNA genetic makeup
b. their absence of a surface lipid bilayer envelope
c. the integrin-binding site on their surface
d. the existence of numerous serotypes
7. A healthy 65-year-old man presents with a 2-day history of a painful rash
on the left side of his forehead extending down to his eyelids. A vesicular skin
lesion is also present at the tip of his nose. Which of the following treatment
options would most likely reduce his risk of postherpetic neuralgia?
a. administration of systemic corticosteroids within the first 72 hours
b. use of oral famciclovir 500 mg 3 times daily for 7-10 days after 1 week of
symptoms
c. prior varicella-zoster vaccination
d. use of oral valacyclovir 500 mg 3 times daily, beginning at the time of
presentation
8. A 30-year-old immunocompetent patient presents with a 1-day history of
vesicular lesions on his upper lip and the third recurrence within the past year
of a dendritic epithelial lesion of his right cornea. Which of the following
options would be the most appropriate treatment at this time?
a. topical ophthalmic ganciclovir ointment 0.15% 5 times a day for 1 week
b. topical trifluridine eyedrops 1% 9 times a day for 3 weeks
c. systemic famciclovir 500 mg 3 times daily for 10 days
d. systemic valacyclovir 500 mg 3 times daily for 10 days followed by maintenance
dosing

9. A corneal transplant patient on long-term topical corticosteroid and topical
antibacterial treatment presents with an indolent midperipheral keratitis.
Smear testing shows yeast and pseudohyphae. Which of the following
protocols is the most appropriate initial treatment?
a. topical natamycin 5% every hour
b. intrastromal corneal injection of natamycin
c. topical amphotericin B 0.15% every hour
d. topical moxifloxacin 0.5% every hour
10. What is a typical finding in the early stages of Acanthamoeba keratitis?
a. hypopyon
b. ring infiltrate
c. radial perineuritis
d. corneal neovascularization
11. A 27 -year-old woman who underwent uncomplicated laser in situ
keratomileusis 6 weeks ago presents for routine follow-up examination and is
noted to have a new infiltrate in the interface. There is no improvement after 3
days of hourly administration of fluoroquinolone eyedrops. Which of the
following actions is the most appropriate next step in management?
a. change topical antibiotic to fortified vancomycin
b. lift flap and irrigate with vancomycin
c. lift flap; obtain cultures on blood, chocolate agar, and Sabouraud's agar; change
antibiotic
to fortified vancomycin and gentamicin
d. add topical corticosteroids
12. An SO-year-old nursing home resident presents with a 2-day history of a 6-
mm central corneal infiltrate after accidentally striking the left eye with a
bottle of timolol. What is the best choice for initial management?
a. empiric, topical, fourth -generation fluoroquinolone every hour
b. corneal scraping for culture and sensitivity testing, followed by topical
fourthgeneration
fluoroquinolone every hour
c. emipiric fortified vancomycin and gentamicin every hour
d. corneal scraping for culture and sensitivity testing, followed by fortified topical
vancomycin and gentamicin

13. Which condition is typically associated with keratinized epithelial cells?
a. mucous membrane pemphigoid-associated conjunctivitis
b. herpes keratoconjunctivitis
c. vernal keratoconjunctivitis
d. chlamydia! (inclusion) conjunctivitis
14. How do corneal angiogenesis and lymphangiogenesis affect outcomes after
corneal transplantation?
a. Vascularization of the cornea increases the risk of immune rejection after corneal
transplantation, leading to a frequency of graft rejection greater than 90%. This
may occur even when a strict regimen of topical and systemic immunosuppressive
agents is used.
b. Lymphatic neovessels may grow in parallel with the blood vessels but do not
affect the risk of immune rejection.
c. Blockade of angiogenesis or Iymphangiogenesis decreases the risk of graft
failure in animal models.
d. VEGF inhibitors, including pegaptanib, ranibizumab, and bevacizumab, have
been used for the treatment of corneal neovascularization after corneal
transplantation to improve graft survival in humans.
15. Which of the following treatments is most recommended in the vision
rehabilitation of patients with severe ocular surface disease associated with
chronic Stevens-Johnson syndrome and toxic epidermal necrolysis?
a. osteo-odonto-keratoprosthesis
b. penetrating keratoplasty
c. keratomileusis
d. autologous stem cell transplantation
16. Which statement is more characteristic of atopic keratoconjunctivitis than
of vernal keratoconjunctivitis?
a. Patients with atopic keratoconjunctivitis are younger.
b. The papillae occur in the lower palpebral conjunctiva only.
c. Eosinophils in conjunctival cytology specimens are less numerous and are more
often degranulated.
d. Extensive corneal vascularization and opacification rarely occur secondary to
chronic epithelial disease (likely as the result oflimbal stem cell dysfunction).

17. What percentage of patients with necrotizing scleritis have a detectable
systemic disorder?
a. 5%
b. 33%
c. 66%
d. 90%
18. Which of the following neoplastic lesions of the conjunctiva is most likely
to be associated with a systemic neoplastic disease?
a. ocular surface squamous neoplasia
b. conjunctival papilloma
c. conjunctival lymphoma
d. conjunctival myxoma
19. Which of the following is a risk factor for tumor recurrence after the
successful treatment of ocular surface squamous neoplasia?
a. presence of leukoplakia
b. coexistence of ocular surface squamous neoplasia and pterygium
c. tarsal involvement
d. male sex
20. Which of the following statements characterizes Peters anomaly?
a. a central opacity of the cornea with underlying endothelial defect and iris
adhesions
b. a central opacity of the cornea that is always bilateral
c. a central opacity of the cornea that is never adherent to the lens
d. a central opacity that is always associated with systemic anomalies
21. Which statement best characterizes the corneal injury caused by birth
trauma?
a. a corneal abrasion that heals, leaving no permanent injury
b. a stretching of the corneal stroma leading to a keratoconus-like protrusion
c. a stretching of Descemet membrane that leads to endothelial dysfunction and
corneal edema
d. a vertical break in the corneal endothelium, leaving vertical ruptures in Descemet
membrane that lead to corneal edema; the edema often clears and may produce
high astigmatism

22. Which of the following corneal dystrophies is autosomal recessive?
a. macular dystrophy
b. lattice dystrophy type 1
c. granular dystrophy
d. Fuchs endothelial corneal dystrophy
23. The deposits in Schnyder corneal dystrophy are composed of what
substance?
a. calcium
b. cholesterol
c. amino acids
d. glycosaminoglycans
24. Which of the following metabolic disorders that affect the cornea is X-
linked recessive?
a. Hunter syndrome
b. Hurler syndrome
c. Maroteaux-Lamy syndrome
d. Scheie syndrome
25. Which of the following drugs is associated with cornea verticillata?
a. metoprolol
b. amiodarone
c. erythromycin
d. tetracycline
26. Which of the following features is characteristic of Marfan syndrome?
a. autosomal recessive inheritance
b. spherophakia
c. corneal flattening
d. defect in the elastin gene
27. Which of the following is the most significant risk factor for pterygium
development?
a. peripheral ulcerative keratitis
b. connective tissue disease
c. UV light exposure
d. dry eye

28. Terrien marginal degeneration is characterized by which of the following?
a. a primarily inflammatory condition
b. corneal thinning that usually begins superiorly
c. male predilection
d. spontaneous corneal perforation
29. Which of the following statements characterizes calcific band keratopathy?
a. The condition begins with fine, dustlike, basophilic deposits in Descemet
membrane.
b. The changes are usually first noted peripherally in the 6- and 12-o'clock
positions.
c. A lucid interval is present between the limbus and the peripheral edge of the
keratopathy.
d. The condition is a dystrophy of the superficial cornea.
30. Traumatic hyphema should typically be treated with which medicines?
a. aminocaproic acid to slow clot dissolution and prevent rebleeding
b. topical corticosteroids and cycloplegic agents
c. tissue plasminogen activator to hasten dissolution of the clot
d. intravenous corticosteroids to reduce the inflammation
31. What is the best management of a suspected corneal laceration?
a. Prescribe topical and oral antibiotics and have the patient return for follow-up in
48 hours.
b. To improve exposure, apply 4 rectus sutures in the operating room, usually with
general anesthesia.
c. Perform a thorough, gentle exploration and repair in the operating room, usually
under general anesthesia.
d. Irrigate the fornices to ensure that no particles are left behind.
32. Which clinical finding best supports a diagnosis oflimbal stem cell failure?
a. corneal thinning and melting
b. corneal edema
c. absence of limbal palisades of Vogt with superficial corneal neovascularization
d. corneal opacities with deep corneal neovascularization

33. Which of the following statements is best in relation to corneal surface
healing?
a. Central corneal epithelium is maintained by continued centripetal movement of
central corneal epithelium toward the periphery.
b. The corneal epithelium is entirely regenerated about every 21 days, with the
stem cells serving as the source of this renewal.
c. When there is concurrent damage to the limbal stem cells, the conjunctival cells
do not become involved in repopulating the corneal surface.
d. The limbal basal layer contains the stem cells of the corneal epithelium that
normally repopulate the corneal surface.
34. Eight weeks after undergoing corneal transplantation, a 75-year-old
patient presents with a clear graft and no vascularization to the wound. There
are 8 interrupted and 1 complete continuous sutures. The visual acuity is
20/100 uncorrected and 20/40 best corrected. The corneal topography is 48.40
x 90/42.60 x 180 with clear mires. The refraction is - 2.00 +5 .00 x 90. What is
the best next step at this point?
a. Remove the continuous suture.
b. Remove an interrupted suture at 180°.
c. Perform a relaxing incision at 90°.
d. Remove an interrupted suture at 90°.
35. A 55-year-old patient with Fuchs endothelial corneal dystrophy presents
with visual acuity of 20/200. Slit-lamp examination reveals significant stromal
and epithelial edema but no significant corneal scarring. Which one of the
following procedures would be the most appropriate treatment for this
patient's cornea? a. penetrating keratoplasty
b. endothelial keratoplasty (using Descemet stripping endothelial keratoplasty or
Descemet membrane endothelial keratoplasty)
c. keratomileusis
d. deep anterior lamellar keratoplasty
36. A patient presents 3 weeks after corneal transplantation surgery with a
persistent epithelial defect that has not responded to patching and lubrication.
What is the most appropriate next step in this patient's management?
a. a second corneal transplantation
b. administration of oral acyclovir 400 mg 4 times daily
c. conjunctival flap procedure
d. increased frequency of topical corticosteroids

Answers
l. b. Most of the glucose is transferred into the aqueous humor, from which it then
diffuses through the permeable corneal endothelium and equilibrates in the stroma
for nutritional use. The corneal epithelium has tight junctions that do not allow the
passage of fluid. The limbal blood vessels supply oxygen to the cornea; they are the
source of inflammatory cells in tight lens syndrome but not of nutrition to the
cornea.
2. d. Dry eye is associated with decreases in the Schirmer I test result, tear
meniscus height, and tear breakup time. The symptom of foreign-body sensation
should have improved after artificial tear supplementation or use of topical
cyclosporine. However, redundancy of the inferior bulbar conjunctiva that
overhangs the lower eyelid margin is a clinical sign of conjunctivochalasis, which
typically does not improve with artificial tear supplementation or use of topical
cyclosporine. Patients with this condition may require resection or cautery to
eliminate the redundant conjunctiva.
3. a. Dry eye is associated with tear-film hyperosmolarity, diminished levels of tear
lactoferrin and tear lysozyme, and increased levels of matrix metalloproteinase-9.
4. d. Although a Gundersen flap procedure and tarsorrhaphy are viable options for
the treatment of neurotrophic corneal ulcers, they should be reserved for patients in
whom other interventions have failed. In many cases, patching, increased
lubrication, or placement of bandage contact lenses combined with careful
monitoring will lead to resolution of the ulcer without more invasive therapy. A
Boston keratoprosthesis is indicated for end-stage corneal disease with significant
corneal scarring.
5. c. Unilateral stem cell deficiency secondary to contact lens wear is usually mild
and responds well to discontinuation of contact lens use along with a short course
of topical corticosteroids. If these measures are not effective, then localized corneal
debridement of the superior portion of the irregular epithelium will allow the
healthy inferior corneal epithelium to replace the abnormal epithelium produced by
the stem cell dysfunction.
Limbal stem cell allograft transplantation is reserved for more severe cases of stem
cell dysfunction such as that typically associated with Stevens-Johnson syndrome
or bilateral chemical injuries.

6. b. Human immunodeficiency viruses cannot survive outside the host because
their lipid bilayer envelopes-which are integral to their pathogenicity degrade with
exposure to the environment. Adenoviridae are double-stranded DNA viruses, but
this makeup has no effect on their survival. Numerous individual Adenoviridae
serotypes do exist, but this fact also has no bearing on their ability to survive for
relatively long periods on inanimate surfaces. Non enveloped viruses such as the
Adenoviridae survive and remain infective because their surface structure does not
include degradable lipids.
7. c. Prior varicella-zoster vaccination reduces the incidence of post herpetic
neuralgia (PHN) by 66%. The 500-mg dosing of valacyclovir is below the
recommended dose of 1 g 3 times daily, and the use of any antiviral drug is more
strongly correlated with a reduced duration than with a reduced incidence of PHN.
Corticosteroids have not been shown to reduce the occurrence of PHN, and their
risk outweighs their benefit in uncomplicated herpes zoster.
8. d. None of the topical treatments has been shown to reduce recurrence of
epithelial disease or stromal keratitis, and the topical trifluridine dosing schedule
described is for too long. Patients with repeated recurrences have been shown to
benefit from long-term maintenance dosing of valacyclovir- short-term dosing has
not been shown to reduce recurrence. This patient also has dermatologic lesions
that would benefit from systemic therapy.
9. c. The most common fungal corneal pathogens are Candida species, and the
smear result is suggestive of yeast. The most appropriate initial therapy from the
list of options is amphotericin B, which has broad activity against both yeast and
fungi. Although natamycin has anti yeast activity, it is more effective against
filamentous molds and its poor aqueous solubility restricts its use as an intrastromal
medication. Moxifloxacin is primarily an antibacterial drug with limited antifungal
activity.
10. c. Most studies of large outbreaks of Acanthamoeba keratitis note bilateral
disease in 7%- 11% of patients, unlike for other infectious pathogens. Ring
infiltrates are a later manifestation of disease. The pathognomonic finding of radial
perineuritis does not appear to have prognostic significance for visual outcome.
Although overnight wear of rigid gas-permeable contact lenses may increase the
risk of Acanthamoeba keratitis, overnight wear of soft contact lenses does not do
so.

11. c. Late interface infections (more than 2 weeks after a procedure) are more
commonly the result of slow-growing organisms such as Candida species or
atypical mycobacteria.
Methicillin-resistant Staphylococcus aureus infection is less likely at this juncture,
making empiric vancomycin treatment less appropriate. Patients with late interface
infections require definitive identification of the causative agent, so flap lift and
culture for atypical organisms is the most appropriate next step. In situations of
limited material, preference of cultures should be directed toward the most likely
pathogens, with additional material reserved for other studies.
12. d. The large central ulcer strongly suggests the need for culture, according to
published guidelines. Single-drug therapies have poor in vitro activity against
methicillin-resistant Staphylococcus aureus infection, a likely pathogen in an older
nursing home patient.
13. a. Metaplastic epithelial changes can occur in severe ocular surface diseases,
including mucous membrane pemphigoid, Stevens-Johnson syndrome and toxic
epidermal necrolysis, and ocular graft-vs-host disease.
14. c. Corneal neovascularization increases the risk of graft rejection, but not to
such a severe degree. Lymphatic neovessels increase the risk of graft rejection by
facilitating access of donor and host antigen-presenting cells and antigenic material
to regional lymph nodes, thereby accelerating sensitization to graft antigens.
Several animal studies have demonstrated that blocking angiogenesis and/or
lymphangiogenesis can improve graft survival.
Although VEGF inhibitors have been used for the treatment of corneal
neovascularization, no data are yet available on whether their use improves graft
survival in humans.
15. a. Because of the severe ocular surface disease associated with chronic Stevens-
Johnson syndrome and toxic epidermal necrolysis, outcomes after penetrating
keratoplasty are poor. Boston type II and osteo-odonto-keratoprostheses, though
high risk, have been attempted and are described in the literature. An autologous
stem cell transplant would not be a viable option given the bilateral nature of the
condition, with insufficient stem cells available to transplant from the affected
fellow eye.

16. c. Eosinophils are less numerous in atopic keratoconjunctivitis than in vernal
keratoconjunctivitis.
Patients with atopic disease are typically older, they have papillae involving the
upper eyelid, and they may have extensive corneal neovascularization.
17. c. Scleritis is frequently associated with an underlying systemic immunologic
disease.
About one-third of patients with diffuse or nodular scleritis and two-thirds of
patients with necrotizing scleritis have a detectable connective tissue or
autoimmune disease.
18. c. Conjunctival lymphoma may be a manifestation of systemic lymphoma.
Patients with conjunctival lymphoma should be evaluated by an oncologist to
determine whether there is underlying systemic disease. None of the other lesions
is associated with a systemic neoplastic condition.
19. c. Recurrent ocular surface tumors can be found anywhere on the conjunctiva;
therefore, the entire ocular surface (including the superior fornix) should be
examined at each visit.
Conjunctival melanoma typically spreads to regional lymph nodes, which can be
evaluated by palpation. Squamous cell carcinoma of the conjunctiva results from
sun damage to the ocular surface, which also damages the skin. A dermatologic
evaluation is important for anyone with a diagnosis of an ocular surface tumor.
20. a. Peter’s anomaly is a central corneal opacity with underlying endothelial
defect and iris adhesions. It can be unilateral, may include lenticular corneal
adhesion, and is sometimes associated with systemic anomalies.
21. d. Direct pressure from forceps often causes vertical ruptures in Descemet
membrane that can lead to corneal edema, either transient or permanent, and to
permanent vertical striae in the posterior cornea with resulting high astigmatism.
22. a. Macular corneal dystrophy is autosomal recessive, whereas lattice dystrophy
type 1 and granular dystrophy are autosomal dominant. Fuchs endothelial corneal
dystrophy can show an autosomal dominant inheritance in some families, but in the
majority of cases the pattern of inheritance is yet to be elucidated.

23. b. Schnyder corneal dystrophy is thought to be a local disorder of corneal lipid
metabolism.
Pathologically, the opacities are accumulations of unesterified and esterified
cholesterol and phospholipids.
24. a. Most metabolic disorders that affect the cornea are autosomal recessive. Two
exceptions are Hunter syndrome and Fabry disease, which are both X-linked
recessive.
25. b. Amiodarone, an antiarrhythmic agent, produces lysosomal deposits in the
basal corneal epithelium, creating a whorl-like pattern. A similar pattern can be
found in patients with Fabry disease and its carriers. Other drugs that can cause
verticillata include chloroquine, chlorpromazine, and indomethacin.
26. c. Marfan syndrome, an autosomal dominant disorder associated with a defect
in the fibrillin gene, is commonly associated with lens subluxation (not
spherophakia), scleral thinning (blue sclera), and corneal flattening.
27. c. Pterygia are more common in sunny climates and in people who have spent
significant time outdoors, reflecting exposure to UV light as a significant risk
factor; there is a higher prevalence in men than in women.
28. b. In Terrien marginal degeneration, thinning of the peripheral cornea is a quiet,
essentially non inflammatory process that is unilateral or asymmetrically bilateral
and slowly progressive. Sex prevalence is roughly equal, and cases usually occur in
the second or third decade of life. Terrien marginal degeneration begins superiorly
and spreads circumferentially (in rare cases centrally); it exceptionally involves the
inferior limbus. A line of lipid deposits appears at the leading edge of the pannus.
Spontaneous perforation is rare, although it can easily occur with minor trauma.
29. c. Calcific band keratopathy is a degeneration of the superficial cornea that
begins as fine, dust like, basophilic deposits involving mainly the Bowman layer.
These changes are usually first noted peripherally in the 3- and 9-o'clock positions.
A lucid interval occurs between the limbus and the peripheral edge of the
keratopathy. Eventually, the deposits may coalesce to form a horizontal band of
dense calcific plaques across the inter palpebral zone of the cornea.

30. b. Corticosteroids and cycloplegic drugs are used to reduce inflammation and
put the pupil at rest to reduce the incidence of rebleeding. Oral corticosteroids may
be used to facilitate the resolution of severe inflammation and/or to prevent
rebleeding. Topical anti hypertensive b-blockers and a-agonists) are the mainstay
of therapy, although occasionally intravenous or oral hyperosmotic agents may be
required.
31. c. The initial evaluation of a corneal laceration should be limited, in an attempt
to prevent the extrusion of intraocular contents that could result from unnecessary
pressure on the eye. A computed tomography scan is helpful to rule out an
intraocular foreign body if the history warrants. The evaluation and management
should be done on an urgent basis.
The use of rectus sutures is needed only when the laceration is in the quadrant, in
which case the full extent of the laceration should be explored.
32. c. Destruction of limbal stem cells is characterized by the absence of the limbal
palisades of Vogt, abnormal epithelium on the cornea, and vascularization.
33. d. The corneal epithelium is a highly differentiated cell type that is entirely
regeneratedv approximately every 7 days.
Numerous studies have demonstrated that central corneal epithelium is maintained
by continued centripetal movement of peripheral corneal epithelium toward the
visual axis, as well as by anterior movement from the basal epithelial cells.
The source of the peripheral corneal epithelium is believed to be stem cells that
reside in the basal layer of the limbus.
When there is damage to the limbal stem cells, the conjunctival epithelium
resurfaces the cornea.
34. d. The initial step in treatment of postoperative astigmatism is suture removal,
not a relaxing incision.
Removal of 1 or 2 interrupted sutures can begin starting 4 weeks after
transplantation the suture is removed in the steep axis, which is identified by
manifest refraction and keratometry and is at 90° in this case. Although it is safe to
begin removing interrupted sutures at 4 weeks in the vast majority of cases, the
continuous suture should be left in place for at least 6-12 months before removal.

35. b. Endothelial keratoplasty (EK)- performed with either Descemet stripping
endothelial keratoplasty or Descemet membrane endothelial keratoplasty-is now
the procedure of choice for endothelial dysfunction. Penetrating keratoplasty is a
viable option but is performed less frequently of late because of the advantages of
EK. Keratomileusis and deep anterior lamellar keratoplasty are not indicated for the
treatment of endothelial dysfunction.
36. b. Regardless of the preoperative diagnosis, a patient who presents with a
persistent epithelial defect after transplant surgery may have a herpetic disease;
thus, a trial of oral acyclovir is worthwhile. A second corneal transplant is not
indicated. A conjunctival flap procedure is also premature. If the clinician believes
that patching is not effective, a trial with a bandage lens may be helpful. It may also
be worthwhile to try a temporary tarsorrhaphy.
Increasing the frequency of topical corticosteroids is contraindicated.

09 - Intraocular Inflammation and Uveitis
1. Experimental immune uveitis (EIU) is an animal model in which a
transient anterior uveitis is induced in rodents following foot-pad
administration of lipopolysaccharide (LPS).
What is the likely mechanism of the inflammation induced by LPS?
a. LPS generates a T helper-1 (Th1) response against specific ocular
antigens
b. LPS induces increased B-cell and plasma cell activity with generation
of auto antibodies
c. recognition of lipid A, 0 polysaccharide, and core oligosaccharide by
toll-like receptors triggers up-regulation of cytokines by innate effect or
cells
d. LPS is directly chemotactic for dendritic cells and macrophages
2. What is the principal mechanism of phacolytic glaucoma?
a. granulomatous inflammation occurring around retained cortical lens
fragments
b. lens-protein-laden macrophages populating the anterior chamber and
blocking aqueous outflow in the trabecular meshwork
c. anaphylactic response to previously sequestered lens proteins
d. monocyte cytokine release leading to ciliary body edema with forward
rotation, causing angle closure
3. What is the most likely immune mechanism of Vogt-Koyanagi-
Harada syndrome?
a. Th1 and other T-cell- mediated pathways
b. Th2 and other T-cell-mediated pathways
c. antigen-antibody complexes
d. a complement- and polymorphonuclear-cell-mediated process

4. What is the immune mechanism involved in Toxocara canis-
induced uveitis?
a. molecular mimicry inducing severe inflammation to epitopes shared
by parasite and choroidal cells
b. a Th1 delayed hypersensitivity response resulting in clonal T-cell
proliferation in the choroid
c. basophil and mast cell degranulation leading to increased retinal
vascular permeability
d. a Th2-mediated response resulting in local eosinophilia
5. What is the critical local (ocular) process in anterior chamber-
associated immune deviation (ACAID)?
a. removal of antigen from the anterior chamber
b. use of an adjuvant along with specific antigenic peptide
c. exposure of antigen-presenting cells in the anterior chamber to
transforming growth factor β2 (TGF- β2) results in ultimate suppression
of delayed-type hypersensitivity to specific antigens
d. pharmacologic treatment of preexisting delayed-type hypersensitivity
6. All of the following are thought to increase risk of corneal
allograft rejection except
a. the presence of central corneal vascularization
b. the presence of Fas ligand on corneal endothelium
c. contamination of the graft with donor-derived antigen-presenting cells
at the time of transplantation
d. induction of major histocompatibility complex (MHC) antigens by the
corneal stroma
7. Which of these human leukocyte antigen (HLA) genes confers the
highest relative risk (RR) for its associated disease?
a. Behcet disease and HLA-B51
b. reactive arthritis and HLA-B27
c. tubulointerstitial nephritis and uveitis (TINU) syndrome and HLA-
DRB1 *0102
d. birdshot retinochoroidopathy and HLA-A29

8. A major side effect of systemic cyclosporine is
a. elevated intraocular pressure
b. cataracts
c. osteoporosis
d. systemic hypertension
9. Which statement best applies regarding the use of non steroidal
anti-inflammatory drugs (NSAIDs)?
a. oral NSAIDs may adversely affect renal function and elevate systemic
blood pressure
b. selective cyclooxygenase-2 (COX-2) inhibitors have been
demonstrated to be safer and more effective for treating scleritis than
nonselective inhibitors
c. topical NSAIDs have been demonstrated in controlled studies to be an
effective treatment for uveitic cystoid macular edema (CME)
d. topical NSAIDs are effective in treating scleritis
10. What age group had the highest incidence and prevalence of
uveitis overall in a study population from northern California in the
United States?
a. patients in the first and second decades of life
b. patients in the third and fourth decades of life
c. patients older than age 65 years
d. patients in the fifth decade of life
11. What is the mediator of the anti-inflammatory effects of
Methotrexate?
a. inhibition of folate metabolism
b. nucleotide cross-linking during DNA replication
c. inhibition of calcineurin
d. extracellular release of adenosine

12. A patient has uveitic glaucoma that is not controlled with
maximally tolerated medical therapy. There are extensive posterior
synechiae but 1 clock hour is open and there is no iris bombe. The
uveitis is controlled on antimetabolite medication. What is the next
step in the management of the glaucoma?
a. laser trabeculoplasty
b. laser iridotomy
c. glaucoma implant (aqueous drainage device) or mitomycin
trabeculectomy
d. stop the antimetabolite
13. What is the initial surgical management of a patient with uveitis
and iris bombe?
a. laser iridotomy or surgical iridectomy
b. laser trabeculoplasty
c. trabeculectomy
d. glaucoma implant
14. Florid bilateral CME in a patient with bilateral, chronic,
granulomatous anterior uveitis with 2+ cells in the anterior
chamber, posterior synechiae, and 2+ vitreous cells is most
effectively managed by which of the following?
a. oral acetazolamide
b. topical ketorolac
c. systemic corticosteroids and systemic immunomodulatory therapy
d. pars plana Vitrectomy
15. Which of following is the most appropriate instruction to a
patient beginning daily oral cyclophosphamide therapy?
a. The patient should use 1 mg per day of folic acid supplementation.
b. The patient should undergo annual influenza immunization with an
intranasal live vaccine.
c. The patient should maintain adequate hydration.
d. The patient should avoid taking the medication with a fatty meal.

16. The fluocinolone acetonide implant releases therapeutic levels of
corticosteroids to the vitreous cavity for approximately how many
days?
a. 500
b. 1000
c. 5000
d. 100
17. What is the specific concern about using a tumor necrosis factor
(TNF) inhibitor in a 25-year-old woman with intermediate uveitis
and no evidence of tuberculosis or other systemic disease or
infection?
a. congestive heart failure
b. risk of neoplasia
c. lupus like syndrome
d. demyelinating disease
18. Chronic postoperative endophthalmitis is most commonly caused
by which organism?
a. Candida glabrata
b. Nocardia species
c. Klebsiella pneumoniae
d. Propionibacterium acnes
19. Which of the following findings is most likely to be seen in a
patient with systemic lupus erythematosus?
a. chronic anterior uveitis
b. intraretinal hemorrhages and cotton-wool spots
c. intermediate uveitis
d. acute anterior uveitis

20. A 25-year-old Brazilian man presents with a history of decreased
vision in his left eye for 1 week. Visual acuity is 20/70 and moderate
vitritis is present. On dilated examination, a pigmented scar in the
posterior pole with adjacent focal white chorioretinitis is present.
What is the most appropriate treatment?
a. oral corticosteroids
b. pyrimethamine, sulfadiazine, and prednisone
c. intravenous acyclovir
d. amphotericin B
21. Which of the following statements most likely applies to a patient
newly diagnosed with serpiginous choroiditis?
a. vasculitis is a prominent feature
b. old, scarred lesions may be present in the newly diagnosed eye
c. intense vitritis is common
d. multiple, isolated lesions occur, with recurrences
22. Which clinical finding is associated with acute retinal necrosis?
a. extensive choroidal scarring
b. natural history of rapid progression
c. occlusive vasculopathy mostly involving retinal venules
d. minimal vitritis
23. The white dot lesions of which disease are least apparent on
fluorescein angiography?
a. serpiginous choroiditis
b. punctate inner choroidopathy (PIC)
c. acute posterior multifocal placoid pigment epitheliopathy (APMPPE)
d. birdshot retinochoroidopathy
24. In patients with VKH syndrome, the presence of diffuse
choroiditis is most likely to be found during which stage of the
disease?
a. recurrent
b. prodromal
c. late (chronic)
d. early (acute uveitic)
25. A patient with bilateral anterior and intermediate uveitis is
suspected of having sarcoidosis.
There are no conjunctival or eyelid granulomata. Chest x-ray shows
no abnormalities and serum angiotensin-converting enzyme (ACE)
level is normal. Which of the following is the most appropriate
examination for confirming the diagnosis of sarcoidosis?
a. biopsy of the conjunctiva
b. evaluation ofHLA-B27 status
c. repeat serum ACE test to rule out laboratory error
d. high-resolution computed tomographic scan of the chest
26. Which statement is correct regarding patients with West Nile
virus infection?
a. Ocular involvement is limited to anterior uveitis without chorioretinal
lesions.
b. In the United States, West Nile virus is most commonly acquired in
the winter.
c.West Nile virus is most often contracted via mosquito bites.
d. Ocular involvement requires antiviral therapy.
27. What is the triad of reactive arthritis syndrome?
a. urethritis, polyarthritis, and conjuctival inflammation
b. ulcerative colitis, polyarthritis, and conjunctival inflammation
c. genital ulcers, polyarthritis, and vasculitis
d. palmar rashes, pauciarticular arthritis, and fevers

28. What class of microorganisms has been associated with
glaucomatocyclitic crisis?
a. viruses
b. bacteria
c. fungi
d. parasites
29. What serologic test is most likely to suggest a specific cause of
uveitis, may be curative, and must be considered for all patients with
uveitis?
a. a treponemal-specific serologic test
b. antinuclear antibody (ANA)
c. rheumatoid factor (RF)
d. antineutrophil cytoplasmic antibody (ANCA)
30. What is the most common infectious condition or agent
associated with neuroretinitis?
a. tuberculosis
b. syphilis
c. Bartonella henselae
d. toxoplasmosis
31. What is the most common ocular manifestation of stage 3 Lyme
disease?
a. keratitis
b. anterior uveitis
c. intermediate uveitis
d. panuveitis

32. A patient with uveitis and strongly positive rapid plasma regain
(RPR) and fluorescent treponema antibody absorption (FTA-ABS)
tests has a history of resolved penile chancre, and recently developed
a rash on his palms. What is the most likely diagnosis?
a. primary syphilis
b. false-positive FTA-ABS result
c. secondary syphilis
d. tertiary syphilis
33. When submitting a vitreous biopsy specimen to rule out
intraocular lymphoma, the most important factor that will ensure
the highest chance of obtaining reliable information is
a. preoperative magnetic resonance imaging (MRI) to determine if
central nervous system (CNS) lesions exist
b. preoperative consultation with the ophthalmic pathologist
c. obtaining a large enough specimen to allow vitreous cytokine analyses
d. performance of polymerase chain reaction (PCR) studies to determine
heavy chain rearrangement
34. Which of the following is a common presentation of
CNS/intraocular lymphoma?
a. weight loss and fever
b. decreased vision and floaters
c. pain radiating to jaw or forehead
d. enlarged blind spot
35. Which of the following patients is the most likely to have primary
CNS! Intraocular lymphoma?
a. a 40-year-old man with cotton-wool spots and hard exudates
b. a 59-year-old man with hemorrhagic retinitis and retinal vasculitis
c. a 65-year-old woman with dense vitritis, subretinal infiltrates, and
mental confusion
d. a 29-year-old woman with pars plana exudates and retinal vasculitis

36. An individual infected with the human immunodeficiency virus
(HIV) has a necrotizing retinitis. Which of the following tests would
be most helpful in making the diagnosis?
a. blood and urine cultures for herpes viruses, including CMV
b. vitreous biopsy for polymerase chain reaction evaluation, cultures, and
cytologic testing
c. purified protein derivative testing for tuberculosis
d. serologic testing for herpes viruses, including CMV
37. What is the most common intraocular infection in patients with
AIDS?
a. acute retinal necrosis
b. toxoplasmosis
c. candidiasis
d. CMV retinitis
38. What test may suggest a specific surgical approach to persistent
macular edema in an eye with a long-standing (several years'
duration) intermediate uveitis that has no active inflammation under
treatment with immunosuppressive agents?
a. fluorescein angiography
b. MRI of the head and orbit
c. optical coherence tomography (OCT)
d. Lyme titers

Answers
1. c. Lipopolysaccharide, also known as endotoxin, is a component of the
cell walls of gram-negative bacteria. It is composed of lipid A, 0
polysaccharide, and core oligosaccharide.
Recognition of LPS by cells of the innate and adaptive immune S) stem
leads to up-regulation of immune effector genes including interleukin-1,
interleukin-6, tumor necrosis factor, and chemokines.
LPS can also directly affect vascular permeability and can cause
degranulation of granuolcytes. LPS activity functions through the innate
immune system, and does not induce antigen -specific effects per se.
2. b. In phacolytic glaucoma, soluble lens proteins leak through the
intact capsule, and appear to serve as chemokines for monocytic cells.
Macrophages engulfing this lens protein become swollen and may block
normal aqueous outflow, leading to acute ocular hypertension and,
potentially, glaucoma. This is in contrast to other forms of lens-induced
uveitis, which typically feature zonal granulomatous inflammation.
3. a. Antigen-specific Th1 T cells have been implicated in VKH
syndrome, and more recently Th 17 cells were also shown to possibly
play a role. Th2 T cells are found in parasitic infections, including
toxocariasis. Mucous membrane pemphigoid is thought to result from
antigen -antibody deposition and complement activation in the basement
membrane of mucous membranes including the conjunctiva; some forms
of vasculitis may have similar mechanisms. Polymorphonuclear cells
may be found in acute anterior chamber inflammation, especially in
infectious diseases such as endophthalmitis.
4. d. Toxocara canis is a parasite typically carried by dogs. Ocular
involvement occurs following visceral larval migrans and lodging of the
larvae in the choroid. Like many parasites, T canis induces a strong Th2-
mediated response typified by eosinophil and macrophage infiltration,
immunoglobulin E production, and granuloma formation.

5. c. ACAID is thought to be a major mechanism contributing to immune
privilege in the anterior chamber of the eye. Injection of antigen into the
anterior chamber results in normal B-cell and antibody-mediated
responses but a specific loss of delayed-type hypersensitivity responses.
ACAID is thought to result from aberrant activation of macrophages in
the anterior chamber due to the presence of TGF - B2. Antigen presented
in the spleen then induces a tolerogenic T-cell response rather than
inducing delayed-type sensitivity.
6. b. Corneal allograft enjoys a 90% or greater success rate and uniquely
can be transplanted without histocompatibility matching. The presence
of Fas ligand on the donor graft is thought to lead to apoptosis of
immune effector cells in the anterior chamber, protecting the graft from
rejection.
Corneal vascularization, the presence of donor-derived antigen
presenting cells, and increased expression of MHC genes by donor
stroma all increase the likelihood of T-cell mediated graft rejection.
7. c. Each of these pairs represents a relatively strong association
between a specific HLA allele and disease. HLA-B51 has the weakest
risk conferral of this group, with an RR for Behcet disease of 4-6. HLA-
B27 is strongly associated with reactive arthritis (RR = approximately
60).
Both birdshot retinochoroidopathy and TINU syndrome have among the
strongest HLA associations of any known disease: HLA-A29 confers an
RR of approximately 150 for birdshot disease, and HLA-DRB1 *0102 an
RR of about 167 for TINU syndrome. It is important to remember,
however, that the HLA association for TINU syndrome was based only
on 1 small cohort and the RR is therefore just an estimate. Even the risks
for well-established entities such as birdshot retinochoroidopathy are
estimates that vary in different cohorts.
An important question is whether the HLA associations have sufficient
negative or positive predictive value to be useful clinically. It does
appear that HLA-A29 has sufficient negative predictive value to suggest
that birdshot retinochoroidopathy is less likely than an alternative

diagnosis if the patient is HLA-A29 negative, but in itself HLA-A29-
negative status does not rule out birdshot disease. It is possible that the
negative predictive value of the HLA subtype associated with TINU
syndrome is sufficiently strong to suggest that if it is not present the
diagnosis may be questioned, but there are not sufficient data to verify
that in this rare disease.
8. d. The main potential toxicities of cyclosporine are systemic
hypertension and nephrotoxicity. Additional side effects include
paresthesia, gastrointestinal upset, fatigue, hypertrichosis, and gingival
hyperplasia. Blood pressure measurement, assessment of serum
creatinine levels, and complete blood counts are performed monthly to
monitor patients on cyclosporine.
9. a. Several studies have shown that systemic NSAIDs may be
efficacious in the treatment of chronic iridocyclitis (e.g. juvenile
idiopathic arthritis- associated iridocyclitis) and possibly CME; they may
allow the practitioner to maintain the patient on a lower dose of to pical
corticosteroids. Systemic NSAIDs may be used to treat non necrotizing,
noninfectious scleritis. Potential complications of prolonged systemic
NSAID use include myocardial infarction, hypertension, and stroke
(especially with selective COX-2 inhibitors); gastric ulceration;
gastrointestinal bleeding; nephrotoxicity; and hepatotoxicity. COX-2
inhibitors should only be used with caution and after obtaining detailed
informed consent, if no alternative agents are effective.
10. c. Anterior uveitis is the most common morphologic form of uveitis
worldwide. Men and women appear to be equally affected. In the
epidemiologic study from northern California by Gritz and Wong, the
pediatric age group had the lowest incidence and prevalence and the
group older than age 65 had the highest incidence and prevalence.

11. d. Methotrexate, a folic acid analogue and inhibitor of dihydrofolate
reductase, inhibits DNA replication, but its anti-inflammatory effects
result from extracellular release of adenosine.
12. c. Laser trabeculoplasty in any form (argon, diode, elective) is not
indicated in patients with uveitis and glaucoma. It is ineffective, may
exacerbate intraocular inflammation, and may cause severe intraocular
pressure elevation. Trabeculectomy, use of a glaucoma implant (aqueous
drainage device), and trabeculodialysis have all been successfully used
in the surgical management of these patients.
13. a. The initial management of patients with uveitis and iris bombe
should include laser iridotomy or surgical iridectomy if the laser
procedure is difficult (e.g. due to iris-corneal touch or corneal edema),
glaucoma medications as needed, and intensive application of topical
corticosteroids. Surgical iridectomy may also become necessary if a
patent laser iridotomy cannot be successfully maintained.
A trabeculectomy or glaucoma implant may later become necessary if
there is a patent laser iridotomy and medically uncontrolled intraocular
pressure. Laser trabeculoplasty is of no benefit in uveitic angle closure or
iris bombe.
14. c. Meticulous control of intraocular inflammation with topical,
regional, intraocular, and systemic corticosteroids and, if necessary,
systemic immunomodulatory agents is best for long-term eradication of
uveitic CME. Other ancillary agents may be used when CME persists
despite control of all visible active inflammation or for short-term
management of CME. The severity of CME can but does not necessarily
correspond to the level of inflammatory disease activity, but it is often
slow to respond and clear and often remains even after visible active
inflammation has resolved. Topical NSAIDs and acetazolamide provide
marginal benefits in controlling CME in an eye that is actively inflamed.
Intravitreal triamcinolone shows promise in eliminating CME, at least
temporarily, and is under active investigation. The value of pars plana

vitrectomy in the management of uveitic CME is controversial, although
it may have some role in refractory cases.
15. c. Myelosuppression and hemorrhagic cystitis are the most common
side effects of cyclophosphamide treatment; the latter is more common
when the drug is administered orally.
Complete blood count and urinalysis are performed weekly to monthly.
Patients must be encouraged to drink more than 2 liters of fluid per day
while on this regimen. Microscopic hematuria is a warning to increase
hydration, while gross hematuria warrants discontinuation of therapy. If
white cell counts fall below 2500 cells/µL, cyclophosphamide should be
discontinued until the counts recover. Other toxicities include
teratogenicity, sterility, and reversible alopecia. Opportunistic infections
such as Pneumocystis pneumonia occur more commonly in patients who
are receiving cyclophosphamide; trimethoprimsulfamethoxazole
prophylaxis is recommended.
16. b. The duration of the anti-inflammatory efficacy of the fluocinolone
implant is about 3 years. The implant is effective for a mean of 38
months before first recurrence. At that point, implantation of another
fluocinolone implant or reinstitution of systemic immunomodulatory
therapy must be considered if durable remission has not been achieved.
17. d. While congestive heart failure, malignancy, and lupus like
syndrome are all concerns, the specific controversy in treating
intermediate uveitis, especially in the patient described, is demyelinating
disease. Because women in this age group have a greater likelihood of
developing multiple scelrosis, and intermediate uveitis is associated with
multiple sclerosis in up to 15% of cases, demyelinating disease is a
specific concern in the choice of TNF inhibitor therapy in this instance.
Multiple sclerosis may present years after the onset of the intermediate
uveitis, so even if there was no evidence of demyelinating disease at
onset, that could change while the patient is under therapy.
18. d. Chronic postoperative bacterial endophthalmitis is most
commonly due to Propionibacterium acnes. Many other bacteria and
fungi, such as Staphylococcus epidermidis and Corynebacterium species,
also cause similar chronic endophthalmitis. P acnes, a commensal,
anaerobic, gram-positive, pleomorphic rod, is found on the eyelid skin
and conjunctiva of healthy patients.
19. b. Lupus retinopathy is considered an important marker of systemic
disease activity, and consists of cotton-wool spots with or without
intraretinal hemorrhages occurring independently of hypertension; it is
thought to be due to the underlying microangiopathy of the disease.
Severe retinal vascular occlusive disease (both arterial and venous
thromboses) may result in retinal non perfusion ischemia, secondary
retinal neovascularization, and vitreous hemorrhage and appears to be
associated with central nervous system lupus disease and the presence of
antiphospholipid antibodies. Lupus choroidopathy, characterized by
serous elevation of the neurosensory retina, pigment epithelium, or both;
choroidal infarction; and choroidal neovascularization may be observed
in patients with severe systemic vascular disease due to either
hypertension from lupus nephritis or systemic vasculitis. Uveitis per se is
distinctly uncommon in patients with lupus erythematosus.
20. b. This patient presents with the characteristic lesion of ocular
toxoplasmosis: focal retinochoroiditis with overlying vitreous
inflammation adjacent to a pigmented chorioretinal scar. Moreover, the
patient is from Brazil, an area where toxoplasmosis is endemic. The
presence of significantly reduced visual acuity and vitritis are indications
for treatment.
While numerous agents have been used to treat toxoplasmosis, there is
no single drug or combination that should be applied categorically to
every patient, nor is there consensus as to the most effective regimen.
The classic regimen for the treatment of ocular toxoplasmosis consists of
"triple therapy" with pyrimethamine, sulfadiazine, and prednisone;
because sulfonamides and pyrimethamine inhibit folic acid metabolism,
folinic acid is added to try to prevent the decreases in white blood cells
and platelets that may result from treatment. Some clinicians advocate
adding clindamycin to this regimen as "quadruple" therapy. Alternative
regimens include the use of trimethoprim -sulfamethoxazole,
azithromycin alone or in combination with pyrimethamine, and
atovaquone. Intravitreal clindamycin has been used successfully in
patients in whom systemic therapy is either undesirable or not tolerated.
Oral corticosteroids are frequently added after 24-48 hours of
antimicrobial therapy to treat the inflammatory component of the
disease, but are never used as monotherapy. Similarly, periocular
injections of steroids are contraindicated in patients with ocular
toxoplasmosis. Intravenous acyclovir is the gold standard for the
treatment of herpetic necrotizing retinitis, and amphotericin B is used in
the treatment of fungal endophthalmitis, particularly that caused by
Aspergillus organisms.
21. b. Old, scarred lesions may be present in the newly diagnosed eye.
Funduscopic findings in patients with serpiginous choroidopathy include
characteristic gray-white lesions at the level of the retinal pigment
epithelium (RPE) projecting in pseudopodia! manner from the optic
nerve in the posterior fundus. Less commonly, macular or peripheral
lesions may present without peripapillary involvement. Typically,
disease activity is confined to the leading edge of the advancing lesion; it
may be associated with shallow subretinal fluid. Occasionally, vascular
sheathing has been reported along with RPE detachment and disc
neovascularization. Significant vitritis is distinctly uncommon. Late
findings include atrophy of the choriocapillaris, RPE, and retina, with
extensive RPE hyperpigmentation and subretinal fibrosis; choroidal
neovascularization occurs in some patients at the border of the old scar.

22. b. Acute retinal necrosis presents with a classic triad of retinal
arteriolitis, vitritis, and multifocal yellow-white peripheral retinitis. Early
in the course of the disease, the peripheral retinal lesions are
discontinuous and have a scalloped edge that appears to arise in the
retina. Within days, they coalesce to form a confluent 360° area of
peripheral retinitis that progresses rapidly towards the posterior pole,
leaving full-thickness retinal necrosis in its wake.
23. d. Fluorescein angiography in birdshot retinochoroidopathy reveals
inconsistent findings depending on the age of the lesions and the phase
of the study. Early birdshot lesions may show initial hypofluorescence
with subtle late staining. However, in general, fluorescein angiography
does not typically highlight the birdshot lesions themselves, but rather is
useful in identifying more subtle types of active inflammation such as
retinal vasculitis, CME, and optic nerve head leakage. In contrast, in
patients with APMPPE it shows characteristic early blockage with late
staining of the lesions, and in those with PIC it reveals early
hyperfluorescence with late staining of the lesions. In patients with
serpiginous choroiditis, fluorescein angiography reveals blockage of the
choroidal flush in the early stage of the study and staining of the active
edge of the lesion in the later stage of the angiogram.
Early hyperfluorescence with late leakage is indicative of choroidal
neovascular membranes, which are seen frequently in patients with PIC
and less often in those with serpiginous choroiditis and birdshot
retinochoroidopathy.
24. d. VKH syndrome has been divided into four stages: prodromal,
acute uveitic, convalescent, and chronic recurrent; histologic findings
vary depending upon the stage of the disease. During the acute uveitic
stage, there is a diffuse, non necrotizing, granulomatous inflammation
(virtually identical to that seen in sympathetic ophthalmia) consisting of
lymphocytes and macrophages mixed with epithelioid and multinucleate
giant cells with preservation of the choriocapillaris. The convalescent
stage is characterized by non granulomatous inflammation with uveal
infiltration of lymphocytes and plasma cells and the absence of

epithelioid histiocytes. The number of choroidal melanocytes decreases
with the loss of melanin and pigment, corresponding to the "sunset glow"
fundus seen clinically.
In addition, one sees numerous atrophic depigmented lesions in the
peripheral retina erroneously thought to be Dalen-Fuchs nodules.
The chronic recurrent stage reveals granulomatous choroiditis with
damage to the choriocapillaris.
25. d. The definitive diagnosis of sarcoidosis relies on histologic
confirmation of non caseating granulomata. A chest radiograph is
probably the best single screening test for sarcoidosis, as it reveals
abnormal results in approximately 90% of the patients with active
disease. Thin-cut spiral computed tomographic (CT) imaging is a more
sensitive imaging modality and may be particularly valuable in the
patient with a normal-appearing chest radiograph in whom there remains
a high clinical suspicion for disease. In such cases, parenchymal,
mediastinal, and hilar structures with distinctive CT patterns highly
suggestive for sarcoidosis may lead to the diagnosis. Although serum
ACE and lysozyme levels may be abnormally elevated, neither is
diagnostic or specific.
26. c. The most common ocular manifestation of West Nile virus
infection is a characteristic multifocal chorioretinitis with non
granulomatous anterior uveitis and vitreous cellular inflammation. The
chorioretinal lesions vary in size and number and are distributed
throughout the midperiphery, frequently in linear arrays following the
course of retinal nerve fibers. Active chorioretinal lesions appear whitish
to yellow, are flat and deep, and evolve with varying degrees of
pigmentation and atrophy, not infrequently becoming targetoid in
appearance. West Nile virus is maintained in an enzootic cycle mainly
involving the Culex genus of mosquitoes and birds. Although birds are
the natural host of the virus, it is most often transmitted from them to
humans and other vertebrates through the bite of an infected mosquito.
Peak disease onset occurs in late summer, but the disease can happen
anytime between July and December. There is currently no proven

treatment for West Nile virus infection; in patients with severe disease
therapy is supportive.
27. a. Reactive arthritis syndrome is defined as urethritis, polyarthritis,
and conjunctival inflammation.
28. a. Glaucomatocyclitic crisis has been associated with
cytomegalovirus (CMV) infection and the virus has been isolated from
the eyes of patients with this disease.
Topical corticosteroids and aqueous suppressants are utilized to treat the
acute anterior uveitis and intraocular pressure elevation, respectively,
with which these patients present. Presenting intraocular pressure may be
very high (>40 mm Hg) and should be treated. The inflammation
responds readily to topical corticosteroids.
29. a. Whereas false-positive and false-negative results may occur with
treponemal-specific serologic tests, syphilis is the great imitator and
screening syphilis serologies have an unacceptably high false-negative
rate in patients with uveitis.
ANA and RF testing rarely contribute to uncovering the cause of uveitis
in the absence of scleritis, keratitis, or vasculitis, and then rarely suggest
specific therapy.
ANCA testing is most important when Wegener granulomatosis is
suspected (although patients with other vasculitides may test positive for
ANCA), but again is rarely useful in a patient with isolated uveitis.
Therapy is more directed in a patient with Wegener granulomatosis, but
treatment for this entity is not curative in the sense that appropriate
antibiotic treatment would be for an infectious disease such as syphilis.

30. c. While all of these conditions or agents may be associated with
neuroretinitis, Bartonella henselae is the most common cause (of course,
B henselae may not be the cause of neuroretinitis for an individual from
an area in which a specific disease such as tuberculosis is endemic).
B henselae is a gram-negative rod that causes the anthropozoonosis cat-
scratch disease (CSD); another Bartonella species Bartonella quintana)
is the causative agent in trench fever. Systemic antibiotic treatment for
CSD can be helpful in curtailing the course of systemic disease but may
not be needed, as the illness can be self limiting. The most common
uveitic manifestation of CSD is focal choroiditis, which can look exactly
like Toxoplasma retinochoroiditis.
31. a. Although Lyme disease can be associated with neuro-ophthalmic
abnormalities as well as any of the forms of uveitis (anterior,
intermediate, and panuveitis) in the answers, and is most often thought of
in the context of intermediate uveitis, keratitis that responds to topical
corticosteroids is the most common form of ocular manifestation in stage
3 Lyme disease.
32. c. Uveitis may be seen in any stage of syphilis but most commonly
occurs in the secondary and tertiary stages of the disease. Thus,
laboratory evaluation for syphilis in patients with uveitis should use
treponemal-specific tests such as FTA-ABS or the
microhemagglutination assay for Treponema pallidum antibodies
(MHA-TP) rather than non treponemal screening tests such as the VD
RL or RPR evaluations.
A chancre is seen at the site of inoculation in primary syphilis. In
secondary syphilis a rash may be seen on the palms. This rash may allow
transfer of the spirochete and should not be touched. Tertiary or latent
syphilis is manifested by gummatous inflammation of the viscera and
neurosyphilis.

33. b. Vitrectomy specimens from suspected cases of intraocular
lymphoma must be processed promptly by an experienced ophthalmic
pathologist in order to preserve the cytology for examination. Prolonged
time between obtaining a specimen and its processing by the pathologist
increases the degeneration of the specimen and greatly reduces its value
for obtaining a diagnosis. It is thus important that the surgeon clearly
communicate to the pathologist the clinical suspicion of lymphoma and
indicate that a specimen will be submitted so that arrangements can be
made for timely evaluation. In addition, depending on the clinical
scenario, the pathologist may want special fixatives to be used to allow
special studies, such as flow cytometry, in addition to cytologic
examination.
34. b. Nonspecific symptoms are most common in intraocular lymphoma
and relate to the presence of vitreous cells and debris. Patients with
lymphoma may have extraocular symptoms, but fever is uncommon.
Pain radiating to the jaw or forehead is more consistent with giant cell
arteritis. An enlarged blind spot is also not a typical finding in
intraocular lymphoma.
35. c. Vitritis, subretinal (especially sub-RPE) infiltrates, and CNS
manifestations such as confusion are hallmarks of primary CNS
lymphoma. This disease typically occurs in older individuals.
A 40-year-old person with cotton-wool spots and exudates would more
likely have diabetic retinopathy; a hemorrhagic retinitis and retinal
vasculitis could be infectious or autoimmune, but is less likely to be
malignant; and a 29-year-old patient with pars plana exudates likely has
pars planitis.
36. b. A necrotizing retinitis in any immunocompromised person should
be presumed infectious until proven otherwise. Viral or parasitic (e.g.
Toxoplasma canis) agents are most likely, but any infectious pathogen
can be responsible.
Blood and urine cultures may show the presence of virus but do not
provide information about the intraocular process. These tests might be

useful in the negative; i.e. a negative result would argue against CMV as
the cause, but a positive result does not prove that it is the cause. In
addition, culturing samples is slow. Tuberculosis skin testing is
unreliable in patients with AIDS due to anergy.
Similar to the case with blood and urine cultures, serologic evidence of
herpes is not proof of intraocular infection. A direct sample from
intraocular fluid is the most specific way to determine the cause of an
infectious necrotizing retinitis.
37. d. Cytomegalovirus retinitis remains the most common intraocular
infection in patients with AIDS, despite a decline in the number of new
AIDS cases.
38. c. OCT can show vitreoretinal traction, which may require
vitreoretinal surgery. Fluorescein angiography may suggest the same (as
of course may clinical examination), but this possibility is best evaluated
by OCT.
Fluorescein angiography or OCT may suggest a subretinal neovascular
membrane, but that would be exceedingly rare in a patient with
intermediate uveitis (as opposed to chorioretinopathy).
MRI may be useful if demyelinating disease is suspected, but that would
not result in macular edema in and of itself.
Measurement of Lyme titers may be appropriate, but if the inflammation
is currently controlled even a positive test result would not suggest a
surgical treatment for the macular edema, and it is not clear that macular
edema in late Lyme disease would respond to antibiotics (although they
should be given to prevent possible systemic complications).

10 – Glaucoma
1. In which of the following conditions does increased episcleral venous
pressure not play a role in elevated intraocular pressure (IOP)?
a. superior vena cava syndrome
b. pseudotumor of the orbit
c. thyroid eye disease
d. primary open-angle glaucoma (POAG)
2. The highest prevalence of angle-closure glaucoma (ACG) is found in which
of the following?
a. individuals of Asian ancestry
b. individuals of African ancestry
c. individuals of European ancestry
d. the Alaskan Inuit
3. Which of the following risk factors is probably the least significant for
POAG?
a. myopia
b. race or ethnic origin
c. family history
d. level of IOP
4. All of the following statements regarding the Goldmann equation are true
except:
a. The facility of outflow is inversely related to the level of IOP.
b. F denotes the rate of aqueous formation and is typically 2.0-2.5 µ liters per
minute.
c. Episcleral venous pressure is normally 8-10 mm Hg and is directly related to
IOP, especially in acute situations.
d. C denotes the facility of outflow and is essentially the same as resistance to
outflow through the trabecular meshwork.
5. Which of the following is an accurate statement about IOP?
a. IOP is distributed normally when measured in large epidemiologic studies.
b. IOP varies 2 to 6 mm Hg in individuals without glaucoma over the course of 24
hours.
c. IOP is often transiently increased following alcohol consumption.
d. IOP is linearly related to central corneal thickness.

6. The measurement of IOP
a. can be obtained via applanation methods, which are based on the Imbert-Fick
principle
b. shows almost no variation throughout the day
c. using applanation puts the patient at significant risk of permanent corneal
damage
d. is not affected by corneal edema, as long as the patient is lying down
7. Factors that may increase IOP include all of the following except:
a. Valsalva maneuver
b. aerobic exercise
c. ketamine
d. blepharospasm
8. during automated static perimetry, a patient responds when no stimulus is
presented. What type of error is this?
a. short-term fluctuation
b. fixation loss
c. false -negative error
d. false -positive error
9. Which one of the following visual field testing strategies may allow an
earlier detection of glaucoma compared with standard automated perimetry?
a. suprathreshold testing
b. optical coherence tomography (OCT)
c. frequency-doubling technology (FDT)
d. confocal scanning laser ophthalmoscopy (CSLO)
10. The optic nerve finding most suggestive of glaucoma is
a. asymmetry of the cups
b. progressive enlargement of the cup
c. generalized pallor
d. exposed lamina cribrosa
11. What is the mode of inheritance of Axenfeld-Rieger syndrome?
a. X-linked
b. sporadic
c. autosomal recessive
d. autosomal dominant

12. Which one of the following types of perimetry has been used to detect
glaucomatous visual field loss earlier than conventional white-on-white
perimetry?
a. static suprathreshold testing
b. tangent screen
c. Goldmann perimetry
d. short-wavelength automated perimetry (SWAP)
13. Which ocular condition is associated with an increased risk of
complications with cataract surgery?
a. exfoliation syndrome
b. ocular hypertension
c. pigment dispersion syndrome
d. angle recession
14. Which multicenter randomized clinical trial evaluated the long-term
effect of treating patients with newly diagnosed OAG with trabeculectomy
versus medical therapy?
a. Early Manifest Glaucoma Trial (EMGT)
b. Collaborative Initial Glaucoma Treatment Study (CIGTS)
c. European Glaucoma Prevention Study (EGPS)
d. Ocular Hypertension Treatment Study (OHTS)
15. According to OHTS, which one of the following is associated with an
increased risk of converting from ocular hypertension to POAG?
a. a history of diabetes mellitus
b. decreasing age
c. smaller cup-disc ratio
d. lower central corneal thickness
16. Which glaucoma is caused by the leakage of lens proteins through the
capsule of a mature or hypermature cataract?
a. phacomorphic glaucoma
b. lens particle glaucoma
c. ectopia lentis
d. phacolytic glaucoma

17. Which is the correct order of normal angle structures viewed anteriorly
to posteriorly during gonioscopy?
a. cornea, non pigmented trabecular meshwork, Schwalbe line, pigmented
Trabecular meshwork, scleral spur, ciliary body band, iris root
b. cornea, scleral spur, non pigmented trabecular meshwork, pigmented trabecular
meshwork, Schwalbe line, ciliary body band, iris root
c. cornea, Schwalbe line, pigmented trabecular meshwork, non pigmented
Trabecular meshwork, scleral spur, ciliary body band, iris root
d. cornea, Schwalbe line, non pigmented trabecular meshwork, pigmented
Trabecular meshwork, scleral spur, ciliary body band, iris root
18. Which of the following is the best method to determine whether a patient
is at risk of angle closure?
a. gonioscopy
b. darkroom prone-position test
c. pharmacologic pupillary dilation
d. darkroom test
19. In which of the following is peripheral iridotomy the treatment of choice?
a. secondary angle closure following dense panretinal photocoagulation
b. iridocorneal endothelial dystrophy
c. phacoanaphylactic glaucoma
d. phacomorphic glaucoma
20. In an eye with a narrow angle, which of the following most strongly
argues in favor of performing a laser peripheral iridotomy?
a. gonioscopic findings
b. amount of glaucomatous optic nerve cupping
c. amount of glaucomatous visual field loss
d. IOP level
21. A 14-year-old boy with bilateral iris atrophy and corectopia is found to
have elevated IOPs.
His father has a similar condition. Which of the following is the most likely
diagnosis?
a. iridocorneal endothelial syndrome
b. Lowe syndrome
c. Axenfeld- Rieger syndrome
d. Hallermann- Streiff syndrome
22. What anatomical modification is found in increased frequency in primary
congenital glaucoma?
a. increased axial length
b. hyperopia
c. hypoplastic optic nerve
d. decreased corneal diameter
23. Which one of the following is the preferred initial surgical procedure for
an infant with primary congenital (infantile) glaucoma and corneal clouding?
a. goniotomy
b. trabeculectomy
c. cyclophotocoagulation
d. trabeculotomy
24. Mutations in the TIGR/myocilin gene are associated with which of the
following disorders?
a. pigment dispersion syndrome
b. exfoliation syndrome (or pseudoexfoliation)
c. juvenile OAG (JOAG)
d. nanophthalmos
25. Which of the following medications is contraindicated in the treatment of
glaucoma in a toddler?
a. dorzolamide
b. brimonidine
c. latanoprost
d. timolol
26. Which class of glaucoma medications can induce uterine smooth muscle
contraction and should therefore be avoided during pregnancy?
a. Beta-blockers
b. carbonic anhydrase inhibitors
c. alpha-agonists
d. prostaglandins

27. A 21-year-old woman with JOAG and 7 diopters of myopia complains of
severe blurring of vision after using 1 drop of pilocarpine. What is the most
likely cause of her symptom?
a. increased hyperopia
b. retinal detachment
c. increased myopia
d. a small pupil
28. Which of the following categories of primary ACG occurs without
pupillary block?
a. acute ACG
b. intermittent ACG
c. plateau iris syndrome
d. subacute ACG
29. A 52-year-old woman with ocular hypertension is started on a monocular
trial with a glaucoma medication. Which glaucoma medication is most likely
to produce a decrease in IOP in the contralateral (untreated) eye?
a. brimonidine
b. timolol
c. dorzolamide
d. latanoprost
30. Which one of the following patients with a preoperative IOP of 50 mm Hg
would be at greatest risk for developing a suprachoroidal hemorrhage
following a trabeculectomy?
a. aphakic patient with a postoperative IOP of 18 mm Hg
b. an aphakic patient with a postoperative IOP of 5 mm Hg
c. aphakic patient with a postoperative IOP of 5 mm Hg
d. an aphakic patient with a postoperative IOP of 18 mm Hg
31 . Which of the following glaucomas might not resolve after cataract
extraction?
a. primary ACG
b. phacolytic glaucoma
c. an eye with angle recession and phacodonesis after blunt trauma
d. microspherophakia with glaucoma

32. The use of adjunctive antifibrotic agents is more commonly associated
with which complication that can occur years after a trabeculectomy?
a. encapsulated bleb
b. aqueous misdirection
c. bleb infection
d. cystoid macular edema

Answers
1. d. The primary mechanism of outflow resistance in primary open-angle
glaucoma (POAG) is thought to be within the inner wall of the Schlem canal,
although some alterations in the uveoscleral pathway may also exist. In the other
conditions, there is an increase in the venous pressure in the orbit, which is
transmitted to the episcleral veins.
2. d. Available data show that, among white populations in the United States and
Europe, the prevalence of primary angle-closure glaucoma (PACG) is
approximately 0.1 %; the prevalence of PACG among the Inuit population of the
Arctic regions is 20 to 40 times higher.
For most Asian population groups, the prevalence of PACG is between that for
whites and that for the Inuit. Groups of African ancestry have a higher prevalence
of OAG.
3. a. Although glaucoma is not equated with elevated intraocular pressure (IOP),
elevated IOP is probably the most important risk factor for vision loss. Family
history and racial orethnic background are also highly important risk factors.
Black Americans have a greater prevalence of OAG at all ages. There is mounting
evidence for the genetic basis of many of the glaucoma. Other factors, such as
myopia and diabetes mellitus, are probably less important risk factors for POAG.
4. d. The facility of outflow is the inverse of the resistance to outflow.
5. b. In individuals without glaucoma, IOP varies 2-6 mm Hg over a 24-hour
period. IOP has a non-Gaussian distribution with a positive skew (tail to the
right), and it is normally decreased after alcohol consumption, not increased.
Although there is a direct correlation between corneal thickness and measured
IOP, it is not linear.
6. a. Applanation tonometry is based on the Imbert-Fick principle and, performed
correctly, is a very low-risk procedure. The other choices are incorrect because
IOP varies 2 to 6 mm Hg throughout the day, and corneal edema can significantly
alter the measurement of IOP no matter the patient's position.
7. b. Aerobic exercise has been shown to decrease IOP.

8. d. Automated static perimetry determines the threshold sensitivities at multiple
points in the visual field. When a patient responds at a time when no test stimulus
is presented, a false-positive error is recorded. When a patient fails to respond to a
stimulus presented in a location where a dimmer stimulus was previously seen, a
false-negative response is recorded.
Short-term fluctuation is a measure of normal physiologic variation and intratest
reliability. It is measured when the visual field analyzer double-determines 10
preselected points during the course of the test session. Fixation losses are
identified when the patient fails to look at the central fixation light during testing.
9. c. Frequency-doubling technology (PDT) perimetry presents a low spatial
frequency grating during visual field testing that preferentially activates the M
cells.
Whether it is because of isolation of specific cell populations that are susceptible
to early damage in glaucoma or because of the reduced redundancy allowing
earlier detection of defects, FDT perimetry may allow earlier detection of
glaucoma than does standard automated (white-on-white) perimetry.
Suprathreshold testing presents a stimulus at an intensity expected to be brighter
than the patient's threshold and is designed for screening purposes to detect
moderate to severe visual field defects. Optical coherence tomography (OCT)
and confocal scanning laser ophthalmoscopy (CSLO) are newer techniques that
can provide quantitative measurement of the optic nerve head and retinal nerve
fiber layer, which may aid clinicians in making an earlier diagnosis of glaucoma.
OCT and CSLO are not visual field testing strategies.
10. b. Progressive enlargement of the cup is the optic nerve finding most
suggestive of glaucoma.
Although asymmetry of the cups can be a sign of early glaucoma, it can be seen in
individuals without glaucoma as well and is often due to differences in the size of
the neural canal.
Generalized pallor is more commonly a sign of non glaucomatous optic nerve
injury. Exposed lamina cribrosa can be seen in glaucoma, but it is also present in
individuals with physiologic cupping.
11. d.
12. d. In short-wavelength automated perimetry (SWAP), a blue stimulus is
projected onto a yellow background designed to preferentially activate the konio
cellular ganglion cell population and measure the sensitivity of short-wavelength
mechanisms throughout the visual field. SWAP provides a more sensitive method

than does white-on-white perimetry for detecting early visual dysfunction in
glaucoma.
13. a. Patients with exfoliation syndrome (also termed pseudoexfoliation
syndrome) are at increased risk of lens subluxation and vitreous loss during
cataract surgery because of the reduced integrity of the lens zonular fibers.
Patients with exfoliation syndrome should be carefully examined preoperatively
for signs of phacodonesis. Segmental and complete tension rings are helpful intra
operative tools for stabilizing the lens capsule. In addition, these patients have a
higher incidence of IOP spikes postoperatively and are more vulnerable
to corneal edema and decompansation.
14. b. The Collaborative Initial Glaucoma Treatment Study (CIGTS) enrolled
patients with newly diagnosed OAG and randomized them to initial
trabeculectomy or treatment with glaucoma medications.
After 5 years of follow-up, the rates of visual field progression were similar in the
medical treatment group (10.7%) and surgical treatment group (13.5%).
The Early Manifest Glaucoma Trial assessed the efficacy of glaucoma medical
and laser therapy in patients with newly diagnosed glaucoma.
The Ocular Hypertension Treatment Study (OHTS) and the European Glaucoma
Prevention Study evaluated the efficacy of topical ocular hypotensive medications
in delaying or preventing the onset of POAG in patients with ocular hypertension.
15. d. OHTS is a multicenter randomized clinical trial designed to evaluate the
safety and efficacy of topical ocular hypotensive medications in preventing or
delaying the development of POAG in subjects with ocular hypertension. This
study identified baseline demographic and clinical features that predicted which
participants were more likely to progress to POAG.
Enrolled patients were randomized to observation or treatment with topical
glaucoma medications to lower IOP by 20% and maintain an IOP of 24 mm Hg or
lower. After 5 years of follow-up, 4.4% of treated patients developed glaucoma,
compared with 9.5% in the untreated observation group.
Higher IOP, lower central corneal thickness, larger cup-disc ratio, older age, and
higher pattern standard deviation on visual field testing were identified as
significant risk factors for the development of POAG in patients with ocular
hypertension. In OHTS, diabetes mellitus was found to be associated with a lower
risk of conversion to glaucoma.

16. d. In a mature or hypermature lens, soluble lens protein molecules are released
through microscopic openings in the lens capsule into the anterior chamber.
Secondary OAG may develop as lens proteins, phagocytizing macrophages, and
other inflammatory debris obstruct the trabecular meshwork.
Although medications should be used to treat the IOP elevation, definitive therapy
requires cataract extraction. In phacomorphic glaucoma, a large, intumescent lens
induces ACG. Lens particle glaucoma occurs when lens cortex particles obstruct
the trabecular meshwork following disruption of the lens capsule with cataract
extraction or ocular trauma. Ectopia lentis refers to displacement of the lens from
its normal anatomical position.
17. d. Knowledge of normal angle structures is essential for a proper
understanding of gonioscopy.
Expert opinion varies as to the best landmark to use for properly orienting the
clinician to the angle structures, but most prefer to first identify either the scleral
spur or the Schwalbe line. The Schwalbe line is best identified by observing the
corneal light wedge reflection (the parallelopiped, or corneal light wedge,
technique), which marks the junction of the corneal endothelium and the anterior
border of the trabecular endothelium.
For more information on and a video of normal angle structures, go to
gonioscopy.org, a website dedicated to teaching gonioscopy through videography,
and select "The Normal Angle:'
18. a. Most clinicians find gonioscopy to be the best method for identifying angles
that are potentially at risk for angle closure. Results of provocative testing may
supplement gonioscopic findings, but gonioscopy is considered the gold standard
by most experts.
19. d. Laser iridotomy is useful for treating angle closure when there is an element
of pupillary block (e.g. in phacomorphic glaucoma). Iridotomy is of no benefit
when angle closure is caused by other mechanisms and may exacerbate the
condition if outflow is further diminished by the inflammation inherent in the
procedure.
20. a. In chronic ACG with relative pupillary block, gonioscopic findings are the
key to diagnosis and management. IOP may be normal or elevated. In an eye with
a narrow angle, the presence of elevated pressure alone is not an indication for
laser iridotomy.

In this case, coexisting OAG may be causing the IOP elevation, not the narrow
angle. The extent of visual field loss or optic nerve damage does not indicate
whether an iridotomy is needed.
Patients with appositional angle closure or areas of peripheral anterior synechiae
with relative pupillary block have a high risk of developing chronic angle closure
and should have a laser iridotomy.
21. c. Axenfeld-Rieger syndrome is a group of bilateral congenital anomalies
involving anterior segment structures of neural crest origin. Approximately 50%
of cases are associated with glaucoma. Although this syndrome was initially
separated into Axenfeld anomaly (posterior embryotoxon with multiple iris
processes), Rieger anomaly (Axenfeld anomaly plus iris hypoplasia and
corectopia), and Rieger syndrome (Rieger anomaly plus developmental
defects of the teeth or facial bones, redundant periumbilical skin, pituitary
abnormalities or hypospadias), these disorders are now considered to be variations
of the same clinical entity and are combined under the name Axenfeld-Rieger
syndrome. In iridocorneal endothelial (ICE) syndrome, iris atrophy and corectopia
may be present, but this condition is unilateral and not inherited. Lowe syndrome
and Hallermann-Streiff syndrome are systemic congenital disorders that are
commonly associated with glaucoma; however, iris atrophy and corectopia are not
features of these syndromes.
22. a. Primary congenital glaucoma is caused by abnormal development of the
anterior chamber angle. It is a rare disease, occurring in 1 in 10,000 births, but it
accounts for approximately 50%-70% of congenital glaucoma cases. During the
first 3 years of life, the collagen fibers of the e) e are more elastic than they are
later in life. As a result, elevated IOP causes the cornea to stretch, which leads to
increased corneal diameter and enlargement of the globe (buphthalmos). Optic
nerve cupping and pallor are generally seen, but optic disc hypoplasia is not a
characteristic feature of congenital glaucoma. An increase in axial length usually
induces myopia, not hyperopia.
23. d. Primary congenital glaucoma is generally managed surgically, and
goniotomy and trabeculotomy ab externo are the procedures of choice.
Either is appropriate if the cornea is clear; a trabeculotomy should be performed if
the cornea is cloudy. A goniotomy involves incising the anterior aspect of the
trabecular meshwork via an ab interno approach under gonioscopic guidance. A
clear cornea is required for adequate visualization of the anterior chamber angle
during goniotomy. In a trabeculotomy, a trabeculotome or prolene suture is
inserted into the Schlemm canal from an external incision and passed into the

anterior chamber. Trabeculotomy is a type of angle surgery that can be performed
with or without a clear cornea. Trabeculectomy and cyclodestruction are usually
used in the management of primary congenital glaucoma when angle surgery has
failed.
24. c. The first OAG gene identified was GLC1A, which was initially mapped in a
large juvenile glaucoma family and has been localized to chromosome l.
Mutations in this gene produce the protein myocilin, which was also found to be
upregulated in trabecular meshwork cells following dexamethasone exposure.
For this reason, the gene was functionally termed trabecular meshwork inducible
glucocorticoid response (TIGR). Mutations in the TIGR/myocilin gene have been
reported in 3% of individuals with adult-onset POAG.
25. b. Brimonidine has been shown to cause systemic hypotension and apnea in
children younger than 2 years.
26. d. Prostaglandins contract uterine smooth muscle and are used therapeutically
to induce labor. They should therefore be avoided in the treatment of glaucoma
during pregnancy, if possible.
27. c. Young, highly myopic patients may have substantially increased myopia
with miotic therapy. This occurs because of a miotic-induced increased convexity
of the lens and forward movement of the lens. Retinal detachment can occur after
miotic therapy, but it would not be the most likely cause of severe visual blurring
in this case.
All patients with a normal iris develop a small pupil on miotic therapy.
This can cause nyctalopia and is more troublesome in older patients with a
cataract or other media opacity.
28. c. Elevation of IOP occurs with plateau iris syndrome without pupillary block
and may occur despite a patent iridotomy.
29. b. The contralateral effect of topical timolol and of topical β-blockers in
general, is clinically significant and has been reported in a number of clinical
trials, including OHTS (Piltz J, Gross R, Shin DH, et al. Contralateral effect of
topical beta -adrenergic antagonists in initial one-eyed trials in the Ocular
Hypertension Treatment Study. Am l Ophthalmol. 2000; 130(4):441-453).
30. b. Suprachoroidal hemorrhage can be one of the most devastating
complications of trabeculectomy.
Bleeding originates from the short or long posterior ciliary arteries as they
enter the suprachoroidal space from the intrascleral canal.
Delayed suprachoroidal hemorrhage is usually preceded by hypotony and the
development of serous ciliochoroidal effusions, which stretch and rupture one of
the vessels where the vessel bridges the suprachoroidal space.
Conditions that are associated with an increased risk of suprachoroidal
hemorrhage include high myopia, aphakia or pseudophakia, hypotony, prior
vitrectomy, advanced age, hypertension, anticoagulant therapy, and history of
suprachoroidal hemorrhage in the fellow eye.
The Fluorouracil Filtering Surgery Study found that the risk of suprachoroidal
hemorrhage was strongly associated with the level of preoperative IOP and the
magnitude of IOP reduction. Reducing the IOP as much as possible before
filtering surgery and decreasing the magnitude of the immediate IOP reduction
through the use of releasable sutures or laser suture lysis can help reduce the risk
of this complication.
31. c. Cataract extraction would not be expected to improve pressure control in an
eye with blunt trauma and direct trabecular damage. Angle recession may be
present and would be evidence of trabecular damage. Phacodonesis is evidence of
zonular disruption. In this patient, the lens is not contributing to the IOP elevation.
In chronic PACG, relative pupillary block is induced by the tension of the iris
sphincter muscle against the lens, which is positioned slightly anteriorly, in an eye
with a relatively short axial length. Cataract surgery may improve glaucoma
control or may completely eliminate glaucoma in these eyes.
In phacolytic glaucoma, proteinaceous lens material that is released through
microscopic openings in the lens capsule and engulfed by macro phages clogs the
trabecular meshwork and causes secondary elevation of IOP. Cataract surgery
may cure this form of glaucoma.
In microspherophakia, the abnormal, spherical shape of the lens induces pupillary
block, which a laser peripheral iridotomy or lens removal would be expected to
relieve.
32. c. The incidence of encapsulated filtering blebs after guarded filtering surgical
procedures without adjunctive antifibrotics is 8% to 28%. When a trabeculectomy
with mitomycin C is performed, the incidence of encapsulation decreases to 2.5%.
Aqueous misdirection can occur following guarded filtering surgery, with an
incidence of2% to 4%. However, aqueous misdirection tends to occur soon after
the surgery and in patients with a history of chronic ACG, hyperopia, or

nanophthalmos or after laser suture lysis or cessation of cycloplegic therapy.
Cystoid macular edema may occur after trabeculectomy, but its incidence
does not appear to be increased with the use of antifibrotic agents. The reported
incidence of bleb-related infections is 5.7% per year, and this percentage increases
significantly with the use of adjunctive antifibrotic therapy.

11 - Lens and Cataract
1. Which of the following is not a function of the crystalline lens?
a. maintaining clarity
b. providing accommodation
c. metabolizing toxins
d. refracting light
2. What is a normal change in the normal human crystalline lens as it ages?
a. It develops an increasingly curved shape, resulting in more refractive power.
b. It develops an increasingly flatter shape, resulting in less refractive power.
c. It undergoes an increase in the index of refraction as a result of the decreasing
presence of insoluble protein particles.
d. It undergoes a decrease in the index of refraction as a result of the decreasing
presence of insoluble protein particles.
3. What occurs during terminal differentiation?
a. Lens epithelial cells elongate into lens fibers.
b. The mass of cellular proteins is decreased.
c. Glycolysis assumes a lesser role in metabolism.
d. Cell organelles increase their metabolic activity.
4. What is the first presenting sign of Marfan syndrome in the eye?
a. pupillary block glaucoma
b. monocular diplopia
c. the need for aphakic correction
d. inferonasal subluxation
5. Why are glutathione and vitamins A and C present in the anterior
chamber?
a. to adjust the pH and act as a buffer
b. to protect the corneal endothelium
c. to scavenge free radicals
d. to induce DNA damage

6. What occurs when the ciliary muscle contracts?
a. The diameter of the muscle ring is reduced, thereby increasing tension on the
zonular fibers, allowing the lens to become more spherical.
b. The diameter of the muscle ring is increased, thereby increasing tension on the
zonular fibers, allowing the lens to become more spherical.
c. The diameter of the muscle ring is reduced, thereby relaxing tension on the
zonular fibers, allowing the lens to become more spherical.
d. The diameter of the muscle ring is increased, thereby relaxing tension on the
zonular fibers, allowing the lens to become more spherical.
7. The Y-sutures seen in the adult lens are the result of which of the following?
a. the junction of the adult nucleus with the surrounding cortex
b. scarring from the tunica vasculosa lentis
c. the elaboration of the adult nucleus around the fetal nucleus
d. fusion of the embryonic cells within the fetal nucleus
8. Which of the following systemic diseases is not associated with ectopia
lentis?
a. homocystinuria
b. Ehlers-Danlos syndrome
c. Marfan syndrome
d. myotonic dystrophy
9. What is a typical characteristic of a lens coloboma?
a. usually associated with previous lens trauma
b. typically located superiorly
c. typically associated with normal zonular attachments
d. often associated with cortical lens opacification
10. Which of the following is seen in Peters anomaly?
a. treatment with rigid gas-permeable contact lenses
b. defects in the corneal endothelium and Descemet membrane
c. identification of PAX6 mutation in all cases
d. bilaterality in 10% of cases

11. "Oil droplet;' crystalline, and "snowflake" cataracts are characteristic of
which diseases, respectively?
a. diabetes, myotonic dystrophy, galactosemia
b. myotonic dystrophy, galactosemia, diabetes
c. galactosemia, diabetes, myotonic dystrophy
d. galactosemia, myotonic dystrophy, diabetes
12. A patient presents with a mature lens and secondary glaucoma without
evidence of pupillary block. What is the most likely diagnosis?
a. phacomorphic glaucoma
b. phacolytic glaucoma
c. phacoantigenic uveitis
d. lens particle glaucoma
13. Which change is most characteristic of exfoliation syndrome?
a. exfoliative material confined to the lens capsule
b. strong zonular fibers
c. increased pigmentation of the trabecular meshwork
d. hypotony
14. A 65-year-old patient presents with a gradual reduction in vision 1 year
after Vitrectomy to repair a retinal detachment. What is the most likely
explanation?
a. Redetachment of the retina
b. posterior subcapsular cataract from intensive steroid therapy
c. nuclear cataract after vitrectomy to repair the retinal detachment
d. phacoantigenic uveitis from leakage of lens protein
15. Which of the following is true regarding the epidemiology of cataracts?
a. They are more prevalent in persons younger than 65 years.
b. They are more prevalent in men.
c. They occur only as a consequence of age.
d. They are the leading cause of reversible blindness.
16. In the developing world, which of the following could apply to a patient
who develops a visually significant cataract?
a. An additional person may be removed from the workforce for care of the patient.
b. The patient must receive prompt attention to have the cataract removed.
c. The patient is at lower risk for falls.
d. The patient is older than 65 years.

17. What did the Beaver Dam Eye Study determine regarding visually
significant cataracts?
a. They occur earlier in men than in women.
b. They interfere with vision only after patients are older than 75 years.
c. They are more likely to be cortical than nuclear.
d. The incidence of visually significant cataract increases slowly from age 54 to 75.
18. If the best -corrected visual acuity for a patient with cataract is 20/100, a
surgeon would be most likely to recommend surgery if
a. pinhole acuity is also 20/100
b. potential acuity meter (PAM) acuity is 20/25
c. laser interferometry reveals that the patient has no ability to recognize the
orientation of the diffraction pattern
d. a Maddox rod test shows multiple interruptions in the red light streak
19. If a patient has a dense white cataract and the posterior pole is not visible,
which of the following would be most helpful for the clinician in deciding
whether to perform surgery?
a. Specular microscopy
b. B-scan ultrasonography
c. laser interferometry
d. Maddox rod test
20. If a patient is found to have a best-corrected visual acuity of20/40 in each
eye but reports that vision is adequate for his needs, which factor would cause
the ophthalmologist to consider cataract surgery?
a. The level of lens opacity equals the level of vision loss.
b. The patient has no medical problems that would contraindicate surgery.
c. The ophthalmologist is unable to see the patient's retina well enough to evaluate
it.
d. The patient would be able to perform his activities of daily living more easily
with better vision.
21 . In a highly myopic patient, which of the following best describes an
appropriate step in decreasing operative risks?
a. raising the height of the irrigating bottle
b. maintaining a loose incision to allow for increased leakage
c. carefully examining the peripheral retina preoperatively
d. warning the patient of blurred vision from postoperative anisometropia

22. Which of the following is a source of potential complications during
cataract surgery in a uveitis patient?
a. shallow anterior chamber
b. zonular laxity
c. endogenous endophthalmitis
d. phacolytic glaucoma
23. Which one of the following steps would reduce the operative risks of
surgery for a mature, white cataract?
a. placing a small initial incision in the anterior capsule and injecting sufficient
viscoelastic into the lens to expel liquid cortex prior to completing the
capsulorrhexis
b. steepening the dome of the anterior capsule by removing the viscoelastic after
the initial capsule puncture
c. staining the capsule with trypan blue or indocyanine green dye
d. creating numerous radial relaxing incisions in the anterior capsule with long
Vannas scissors
24. A patient with visually significant cataract is found to dilate poorly on
preoperative examination.
Which of the following is the most likely cause of this poor dilation?
a. pigment dispersion syndrome
b. atopic dermatitis
c. exfoliation syndrome
d. hypertension
25. Which of the following would be the best initial treatment of a
postoperative shallow anterior chamber caused by ciliary block glaucoma?
a. miotics and peripheral iridotomy
b. cycloplegia and aqueous suppressants
c. emergent vitrectomy
d. cyclophotocoagulation
26. In operating on a patient with exfoliation syndrome, a surgeon chooses to
make a large anterior continuous curvilinear capsulorrhexis (CCC).
What postoperative complication will most likely be avoided?
a. opacification of the posterior lens capsule
b. postoperative phimosis of the anterior capsule
c. postoperative spike in intraocular pressure
d. glare and halos

27. In cataract surgery in which the posterior lens capsule ruptures and
vitreous presents in the anterior chamber, when is anterior Vitrectomy
complete?
a. when vitreous is removed from the wound
b. when a posterior chamber intraocular lens (IOL) can be placed
c. when the surgeon can see the retina
d. when vitreous is removed anterior to the posterior lens capsule

Answers
1. c. Lens cells have no mechanism for metabolizing toxins. The lens remains clear
because the lens fibers contain no nuclei or organelles that would scatter light. The
lens refracts light because the relative density of the lens is greater than that of the
fluids (aqueous and vitreous) surrounding it. The lens, until the onset of
presbyopia, remains flexible to provide accommodation in response to the tension
placed on the capsule from the ciliary muscle and zonular fibers.
2. a. With age, the human lens develops an increasingly curved shape, which
results in more refractive power. This change may be accompanied by- and
sometimes offset by-a decrease in the index of refraction of the lens, probably
resulting from an increase in water insoluble proteins.
3. a. Terminal differentiation involves elongation of the lens epithelial cells into
lens fibers.
This change is associated with a tremendous increase in the mass of cellular
proteins in each cell. The cells lose organelles, including nuclei, mitochondria, and
ribosomes.
The loss of cell organelles is optically advantageous; however, the cells then
become more dependent on glycolysis for energy production and less active
metabolically.
4. b. Monocular diplopia occurs when the lens is partially dislocated, and light can
pass both through and around the edge of the lens. Pupillary block glaucoma from
anterior dislocation of the lens is a rare event. Aphakic correction is required when
the lens is totally subluxed into the vitreous. When the lens subluxates, it usually
does so superotemporally.
5. c. Glutathione and vitamins A and C are powerful free radical scavengers. They
have no effect on the pH or the corneal endothelium. They actually protect DNA
from being damaged by free radicals.
6. c. The ciliary muscle is a ring, but upon contraction it does not have the effect
that one would intuitively expect of a sphincter. When it contracts, the diameter of
the muscle ring is reduced, thereby relaxing tension on the zonular fibers, allowing
the lens to become more spherical.

7. d. The Y-sutures represent the edges of the secondary lens fibers of the fetal
nucleus. The anterior Y is erect and the posterior one is inverted. They can be seen
in the center of the adult nucleus in a clear lens. The junction of the adult nucleus
and surrounding cortex is invisible until the nucleus develops sclerosis. The tunica
vasculosa lentis surrounds the lens as it grows. The Y-sutures are within the fetal
nucleus, not around it.
8. d. Myotonic dystrophy is not associated with ectopia lentis.
9. d. A lens coloboma is a wedge-shaped defect or indentation of the lens periphery
that occurs as an isolated anomaly or is secondary to the lack of ciliary body or
zonular development.
Cortical lens opacification or thickening of the lens capsule may appear adjacent
to the defect.
Lens colobomas are typically located inferiorly and may be associated with
colobomas of the uvea.
10. b. Peter’s anomaly is bilateral in 80% of cases. PAX6 mutations occur in
patients with Peter’s anomaly, but many cases are associated with mutations in
other alleles. Treatment usually involves sector iridectomy and/or penetrating
keratoplasty as well as management of coexisting glaucoma. Rigid gas-permeable
contact lenses would be ineffective since they do not address the effects of the
central corneal opacity.
11. d. Galactosemia produces an "oil droplet" cataract that appears within the first
few weeks of life. Untreated, galactosemia is rapidly fatal. Crystalline cataracts in
myotonic dystrophy develop a Christmas tree-appearing cortical cataract as well as
posterior subcapsular changes that will lead to complete opacification. The acute
cataract of uncontrolled diabetes has a snowflake appearance in the anterior and
posterior subcapsular region.
12. b. Phacolytic glaucoma occurs when denatured lens protein leaks through an
intact but permeable capsule. In phacomorphic glaucoma, the mature lens causes
pupillary block and secondary angle closure. In phacoantigenic uveitis, leaking of
lens protein produces a granulomatous inflammatory reaction. Lens particle
glaucoma is associated with penetrating lens injury or surgery.

13. c. Increased pigmentation of the trabeculum and reduced outflow occur
frequently in exfoliation syndrome. Exfoliative material has been found in many
bodily organs as well as on the iris and corneal endothelium. Intraocular pressure
may rise as a result of the obstruction of the trabecular meshwork by the exfoliative
material.
14. c. Nuclear cataract is common in patients older than 50 years if vitrectomy has
been used to repair a retinal detachment. Redetachment of the retina is an acute
phenomenon and unlikely 1 year after repair. Steroid therapy after retinal
detachment is usually brief and unlikely to cause nuclear cataract. Phacoantigenic
uveitis produces an inflammatory reaction and is extremely rare.
15. d. Census data confirm that cataracts are the leading cause of reversible
blindness. Cataracts increase in prevalence with increasing age and are a leading
cause of blindness worldwide. They can occur as a congenital condition or as a
result of trauma, metabolic diseases, or medications. Major epidemiologic studies
confirm an increased prevalence in women.
16. a. When 1 individual is incapacitated by blindness, the care that is required to
provide for that person may remove the caregiver from the workforce as well. The
ratio of surgeries to population in the developing world is as low as 50 per million.
Reduced vision is a primary factor in decreasing mobility and increasing the risk of
falls. Cataracts form earlier in life in populations in which nutrition is not optimal.
17. d. Cataracts begin to interfere with vision in persons aged 43-54 years, and,
from that age range, the incidence increases 13-fold in those aged 75 years or older.
The overall incidence of cataract is greater in women than in men. Nuclear
cataracts are more frequent than cortical cataracts at all ages.
18. b. The potential acuity meter (PAM) projects the equivalent of a Snellen visual
acuity chart into the eye, specifically through clear spaces in the lens, by means of
a beam of light to allow an estimate of macular function. The pinhole test
approximates the PAM; a reduced acuity would signal other ocular conditions that
cataract surgery might not improve.
Laser interferometry usually is beneficial in denser cataracts: the patient's failure to
discern the orientation of the diffraction pattern would indicate reduced visual
potential.
The patient's inability to see a continuous red line on a Maddox rod test would
suggest areas of decreased retinal sensitivity in the macula.

19. b. B-scan ultrasonography is indicated to evaluate for occult tumors, retinal
detachment, and posterior staphyloma or other posterior pathology that could affect
the visual outcome.
Laser interferometry and Maddox rod testing are not reliable with such a dense
cataract. Specular microscopy would be indicated only if signs of corneal
endothelial dysfunction were present.
20. c. The only consideration that would prompt the surgeon to consider operating
would be the inability to evaluate the patient's retina. This would be the case even if
the cataract explained the vision loss and the patient appeared well enough to
undergo surgery. If the patient reports that his vision is adequate for his needs,
surgery should be postponed.
21. c. Careful examination of the retinal periphery may reveal the presence of
lattice degeneration, retinal holes, and other abnormalities that warrant
consideration of preoperative treatment and/or diligent postoperative evaluation.
Lowering the height of the irrigating bottle produces less stress on the zonular
fibers and reduces the risk of posterior capsule tears. All incisions should be
carefully closed to reduce the risk of infection. Myopic patients do need to be
cautioned about anisometropia, and intolerable imbalances may prompt
consideration of second-eye surgery.
22. b. Chronic ciliary body inflammation at the zonular fibers may lead to zonular
laxity similar to that seen in exfoliation syndrome. The technical aspects of cataract
surgery can be more difficult in patients with uveitis. There may be limited access
to the lens because of posterior synechiae, a pupillary membrane, pupillary
sphincter fibrosis, and a floppy iris. Lysing synechiae, excising pupillary
membranes, and using pupil expanders and viscoelastic can counteract and
overcome the effects of an abnormal iris. Rupture of the capsulorrhexis with
extension to the zonular fibers can further complicate the procedure, and capsular
dyes may be necessary to maintain a continuous capsular tear during the rhexis.
23. c. When cataract surgery is performed on a patient with a white lens, there is
little or no red reflection. This makes it difficult to perform a circular
capsulorrhexis. Utilizing a capsular dye improves visualization of the capsule,
facilitating the creation of an anterior capsulorrhexis. The other methods described
increase the operative risks. Steepening the dome of the anterior capsule increases
the propensity for radial anterior capsule tearing and therefore should be avoided.
Maximally filling the anterior chamber with viscoelastic during the capsulorrhexis
can reduce leakage of white lens material into the anterior chamber, improving the
view of the anterior capsule. Creation of numerous radial relaxing incisions is a
method used when the initial capsulorrhexis is unsuccessful; it would not be the
primary step in creation of a capsulorrhexis. A small puncture in the anterior
capsule with injection of viscoelastic to expel liquid cortex prior to the completion
of the capsulorrhexis can be used initially but is not considered necessary with the
advent of capsular dyes.
24. c. Exfoliation syndrome is a common disorder associated with the deposition of
a fibrillo granular material on the anterior surface of the lens and elsewhere in the
anterior segment. With respect to cataract surgery, patients with this condition may
have zonular laxity, capsular fragility, and poor pupillary dilation.
25. b. Causes of a shallow chamber postoperatively include wound leak, pupillary
block, suprachoroidal effusion or hemorrhage, and ciliary block glaucoma with
aqueous misdirection into the vitreous cavity. If the cause is known to be ciliary
block glaucoma, initia treatment with cycloplegia and aqueous suppressants may
relieve the condition. Surgical disruption of the vitreous face by YAG laser or a
Vitrectomy may be necessary at a later time to permanently restore normal aqueous
circulation and anterior chamber depth if the initial treatment fails.
26. b. A large capsulorrhexis will reduce the risk of phimosis and increased tension
on the weakened zonular fibers of the patient, also reducing the risk of late
posterior dislocation of the intraocular lens. Opacification of the posterior lens
capsule is dependent not on the size of the capsulorrhexis but rather on the anterior
capsule overlapping the edge of the intraocular lens. Postoperative pressure spikes
are not dependent on capsulorrhexis size, although they are more common in
patients with exfoliation. Glare and halos are also not caused by a large anterior
capsulorrhexis.
27. d. Loss of vitreous is not a problem for the eye; vitreous traction is. The goal of
vitreous removal is to reduce the possibility of traction. The clinician may prevent
traction by removing enough vitreous to keep it away from the incision. Therefore,
a Vitrectomy is not complete until all vitreous is removed anterior to the posterior
capsule. This ensures a lower risk of traction, and it is also the best way to decrease
the risk of postoperative cystoid macular edema (CME).

12 - Retina and Vitreous
1. What is a posterior extension of the pars plana epithelium onto the retinal
side of the ora serrata?
a. enclosed ora bay
b. meridional complex
c. dentate process
d. peripheral retinal excavation
2. Which of the following diagnostic studies is indicated in the evaluation of
age-related macular degeneration (AMD) to detect the presence of choroidal
neovascularization (CNV)?
a. fluorescein angiography
b. magnetic resonance imaging
c. corneal topography
d. computerized axial tomography
3. Which of the following interventions is the most appropriate management
of a patient who has undergone fluorescein angiography?
a. administer aspirin
b. observe patient for late adverse reactions
c. advise patient to avoid sunlight for 5 days after the procedure
d. order urine culture and sensitivity test for urine color change
4. The technique of fluorescein angiography includes which of the following
procedures?
a. intramuscular injection of 5 mL of 10% sodium fluorescein
b. intravenous injection of 5 mL of indocyanine green solution
c. intravenous injection of 5 mL of 10% sodium fluorescein
d. coadministration of oral or intravenous diphenhydramine
5. The electro-oculogram (EOG) is most useful in the diagnosis of which
retinal dystrophy or degeneration?
a. Best disease
b. rubella retinopathy
c. pattern dystrophy
d. fundus flavimaculatus

6. Which agent with potential retinal toxicity may be associated with an
irreversible abnormal electroretinogram (ERG) result?
a. hydroxychloroquine
b. canthaxanthine
c. sildenafil
d. talc
7. Which of the following findings constitutes a pertinent clinical feature of
neovascular A MD?
a. subretinal fluid
b. geographic retinal pigment epithelium (RPE) atrophy
c. drusen
d. RPE pigmentary changes
8. The most appropriate workup for ocular histoplasmosis includes which
one of the following components?
a. C-reactive protein measurement
b. white blood cell count with differential count
c. erythrocyte sedimentation rate determination
d. thorough examination for CNV
9. Which of the following patients has been determined to benefit from Age-
Related Eye Disease Study (AREDS) vitamin supplementation?
a. 40-year-old man with numerous large drusen
b. 14-year-old girl with Stargardt disease
c. 62-year-old man with geographic atrophy in 1 eye
d. 78-year-old patient with previous bilateral CNV
10. Which of the following statements about patients who inherit sickle cell
hemoglobin (Hb SC) is least accurate?
a. "Salmon patch'' lesions, "black sunburst" lesions, and "sea fans" are all signs of
proliferative sickle cell retinopathy.
b. Those with hemoglobin SS have the most severe systemic complications.
c. Those with hemoglobin C and sickle cell thalassemia have the most serious
ocular complications.
d. Sickling of red blood cells occurs under conditions of decreased oxygen
tension.

11. Which of the following statements does not accurately describe the use of
indirect ophthalmoscopy to screen for retinopathy of prematurity (ROP)?
a. Screening should be performed on all premature neonates of less than 30 weeks
gestation.
b. Screening should be repeated biweekly on neonates who demonstrate ROP on
initial examination.
c. Screening should be performed before hospital discharge or by 4- 6 weeks of
age.
d. Screening should be performed on all premature neonates with a birth weight
<1500 g.
12. Which of the following factors is an important risk factor for ocular
toxoplasmosis?
a. consumption of undercooked meat
b. exposure to ticks
c. exposure to mosquitoes
d. living in the Ohio River Valley
13. A 25-year-old woman recently received a diagnosis of pars planitis. Her
visual acuity is 20/20 OD, 20/50 OS. Examination reveals vitreous cells and
cystoid edema in the left eye. Which of the following options is the most
appropriate management plan?
a. argon laser treatment of the peripheral retina in the left eye
b. sub-Tenon steroid injection in the left eye
c. oral methotrexate administration
d. pars plana vitrectomy in the left eye
14. What is a clinical feature of the multiple evanescent white dot syndrome
(MEWDS)?
a. RPE scarring
b. gray-white, poorly demarcated, patchy, outer-retinal lesions
c. severe vitreous cellular reaction
d. gray, granular pigmentation of the fovea

15. The parents of a 2-year-old girl report that she has had "bobbing eyes"
and light sensitivity since birth. In your office, the girl shows good visual
attention but has bilateral pendular nystagmus and squints in bright light.
The retina appears normal, but the foveal reflex is blunted. Dark-adapted
scotopic ERG responses are normal, but light-adapted photopic signals are
greatly diminished. No relatives are similarly affected. What condition does
this patient most likely have?
a. Stargardt disease
b. congenital stationary night blindness
c. Leber congenital amaurosis
d. achromatopsia
16. Acetazolamide is most beneficial when used to treat cystoid macular
edema (CME) associated with which of the following disorders?
a. retinitis pigmentosa
b. central retinal vein occlusion
c. hypotony
d. vitreomacular traction syndrome
17. Which of the following tests most often yields a normal result in Best
disease?
a. optical coherence tomography (OCT)
b. ERG
c. fluorescein angiography
d. EOG
18. Which of the following diagnostic procedures is most likely to reveal a
carrier for Best disease?
a. EOG
b. OCT
c. ERG
d. fluorescein angiography
19. Which of the following disorders would be least likely to be considered in
the differential diagnosis of chloroquine phosphate and hydroxychloroquine
toxicity?
a. AMD with geographic atrophy
b. Stargardt disease
c. Tay-Sachs disease
d. cone dystrophy

20. What predisposing factor contributes to an accelerated development of
hydroxychloroquine maculopathy?
a. adolescence
b. northern European ancestry
c. lean body weight
d. renal and/or hepatic disease
21. A patient taking thioridazine complains of blurred central vision.
Macular evaluation reveals pigmentary stippling.
What is the preferred management?
a. switch medication to trifluoperazine hydrochloride
b. switch medication to chlorpromazine
c. decrease dosage of thioridazine
d. discontinue use of thioridazine
22. An atypical form of CME may be seen as an adverse effect of which of the
following medications?
a. sildenafil
b. amiodorone
c. hydroxychloroquine
d. niacin
23. For a patient with a diabetic mid peripheral tractional retinal
detachment, what complication is of primary concern in the application of
initial panretinal photocoagulation?
a. rhegmatogenous retinal detachment
b. cortical cataract
c. retinal neovascularization
d. tractional macular detachment

24. Which of the following scenarios offers the strongest indication for
prophylactic treatment (cryopexy or laser surgery) to prevent
rhegmatogenous retinal detachment?
a. high myopia and lattice degeneration with new onset of floaters in a phakic
patient
b. lattice degeneration in a pseudophakic patient with a family history of retinal
detachment
c. an atrophic hole in aphakic patient whose other eye developed a retinal
detachment
d. an asymptomatic flap tear in an eye with a cataract that is about to be rendered
pseudophakic
25. A 42-year-old man has a total retinal detachment and a circumferential,
150° peripheral retinal tear with an inverted flap. What surgical approach
would be most appropriate?
a. intra vitreal injection 0.3 mL of sulfur hexafluoride (SF6) gas
b. 360° peripheral laser photocoagulation
c. pars plana vitrectomy, retinal reattachment with perfluorocarbon liquid, laser
photocoagulation, and complete fluid - gas exchange
d. scleral buckle with intra vitreal injection of SF 6 gas
26. In the repair of an acute-onset rhegmatogenous retinal detachment that
involves the macula, what period of delay between diagnosis and surgery has
been shown to worsen visual prognosis?
a. 3 weeks
b. 1 day
c. 1 month
d. 1 week
27. If pars plana vitrectomy is performed on a patient whose fundus has a
macular Epiretinal membrane, what is the most likely postsurgical
complication to occur?
a. nuclear sclerosis
b. retinal tear/detachment
c. endophthalmitis
d. macular pucker

28. What are the characteristics of a stage 3 macular hole?
a. small, perifoveal hole with no posterior vitreous separation
b. full-thickness hole with surrounding subretinal fluid and no posterior vitreous
separation
c. reopened stage 2 macular hole
d. full-thickness hole with surrounding sub retinal fluid and a posterior vitreous
separation
29. An epiretinal membrane developed in a 63-year-old woman over several
years after scatter laser treatment for a branch retinal vein occlusion. You
are preparing to counsel her regarding potential pars plana vitrectomy and
membrane peeling. Which of the following complications associated with
surgery need not be addressed?
a. cataract
b. high rates of epiretinal membrane recurrence
c. retinal pigment epithelial disturbance
d. macular edema
30. Which of the following choices has been reported as a complication of
face-down positioning after macular hole surgery?
a. compressive optic nerve injury
b. ulnar neuropathy
c. cyclodialysis cleft
d. cavernous sinus thrombosis
31. What is the preferred treatment for Bacillus cereus endophthalmitis?
a. intravitreal vancomycin or clindamycin
b. intravitreal amphotericin B
c. intravitreal ganciclovir
d. intravitreal gentamicin or tobramycin
32. What condition should be suspected in an 8-month-old baby presenting
with lethargy, seizures, bruises on the upper arms, retinal hemorrhages, and
cotton-wool spots?
a. shaken baby syndrome
b. sickle cell retinopathy
c. retinopathy of prematurity
d. Von Hippel-Lindau disease

33. What is a benefit of red laser photocoagulation compared with other
wavelengths?
a. better penetration through nuclear sclerotic cataracts
b. less patient discomfort
c. reduced risk of a "pop effect" from inhomogeneous absorption at the level of
the choroid
d. maximal absorption by xanthophyll
34. What laser wavelength is best absorbed by xanthophyll?
a. blue
b. red
c. yellow
d. infrared
35. What parameter increases the risk of Bruch membrane ruptures during
application of laser photocoagulation?
a. small spot size
b. long duration
c. low intensity
d. green wavelength
36. In the immediate postoperative period after vitrectomy, which of the
following findings is most commonly observed?
a. elevation of intraocular pressure
b. acceleration of cataract development
c. hyphema
d. retinal detachment
37. The risk of hemorrhagic choroidal detachment is increased by which one
of the following factors?
a. younger age
b. hyperopia
c. elevated intraocular pressure during surgery
d. hypertension

38. Development of an epiretinal membrane is most commonly associated
with which one of the following findings?
a. glaucoma
b. posterior vitreous detachment
c. cataract
d. facial clefts
39. Panretinal photocoagulation therapy is used in a young patient with
poorly controlled diabetes mellitus and arcade tractional retinal
detachments, moderate subhyaloid hemorrhage, and retrolenticular blood.
Which of the following complications could result in irreversible loss of vision
after such treatment? a. aggravation of hyperglycemia
b. cortical cataract
c. new vitreous hemorrhage
d. tractional retinal detachment involving the fovea

Answers
1. a. A dentate process is an anterior extension of retinal tissue that separates
adjacent ora bays in pars plana and is aligned with but does not reach a minor
ciliary process.
A meridional complex is a hyperplastic dentate process that extends across the
entire length of the pars plana and merges with a ciliary process.
A peripheral retinal excavation is a small, oval retinal depression posterior to the
ora and is often aligned with a meridional fold or complex. It is excavated because
of hypoplasia of inner retinal layers, similar to lattice degeneration.
2. a. Fluorescein angiography is indicated in the evaluation of age-related macular
degeneration (AMD) to detect the presence of choroidal neovascularization
(CNV).
3. b. Allergic reactions to fluorescein dye may occur immediately or several hours
after the administration of the dye. Adverse effects of the dye are usually mild but
in rare cases can be serious or even fatal.
4. c. Fluorescein angiography involves intravenous injection (or, less commonly,
oral administration) of fluorescein dye, followed by photography of the retinal
vasculature. Intramuscular administration of fluorescein is never appropriate.
Indocyanine green (ICG) is used intravenously in ICG angiography.
Diphenhydramine may be used if an allergic reaction to fluorescein is anticipated.
5. a. The electro-oculogram (EOG) is most specific as a test for Best disease,
which produces a severely reduced light-peak, dark-trough (Arden) ratio. In
fundus flavimaculatus and pattern dystrophy, the light-dark ratio is normal or only
mildly subnormal. In rubella retinopathy, the retinal pigment epithelium (RPE)
can be diffusely altered, but the EOG pattern is normal.
6. a. The full -field electroretinogram (ERG) response is a test of the mass
response of the retina and is not a direct test of macular function. It is important
for diagnosing and following diffuse diseases, such as retinal dystrophies, retinal
degenerations, central retinal artery occlusion, and retinal drug toxicities,
including some cases of hydroxychloroquine retinal toxicity.
The multifocal ERG has been shown to be more specific than the full –field ERG
in the diagnosis of hydroxychloroquine retinal toxicity. The ERG response is less
likely to be affected by more focal diseases such as macular holes, epiretinal
membranes, branch retinal vein occlusions, or regional uveitis damage. The

retinal toxicity associated with canthaxanthine, sildenafil, and talc has not been
shown to result in an irreversible abnormal ERG result.
7. a. Neovascular AMD is characterized by the development of CNV.
This exudative neovascular complex commonly results in the accumulation of
subretinal fluid, blood, and lipid. Drusen, RPE pigmentary changes, and
geographic RPE atrophy are characteristics of non neovascular AMD.
8. d. There are 4 signs of ocular histoplasmosis: "punched-out" chorioretinal
scars, juxta papillary pigmentary changes, no vitritis, and CNV. Untreated CNV
may lead to severe and permanent loss of vision.
9. c. Patients at the time of enrollment into the Age-Related Eye Disease Study
(AREDS) was 55-80 years old.
The AREDS showed a 25% reduction in the risk of progression to advanced
AMD for patients with advanced unilateral AMD who were randomly assigned to
the combination supplement group.
10. a. "Salmon patch" and iridescent spot lesions represent areas of intraretinal
hemorrhage, while "black sunburst" lesions are localized areas of intra- and
subretinal hemorrhage and arise from hyperplasia and intraretinal migration of the
RPE.
"Sea fans" are fronds of neovascularization that extend from the retina into the
vitreous and are therefore signs of proliferative retinopathy.
A prospective clinical trial has demonstrated the efficacy of argon laser scatter
photocoagulation therapy for proliferative sickle cell retinopathy. Prolonged loss
of visual acuity and vitreous hemorrhage were reduced in treated eyes compared
with control eyes. Scatter photocoagulation proved to be effective and safe in the
treatment of patients with sea fan neovascularization.
11. b. Several risk factors have been associated with the development of
retinopathy of prematurity (ROP) in premature neonates, including low birth
weight, low gestational age, oxygen therapy apnea, sepsis, and others. Premature
infants with a birth weight of 1500 g or less, of gestational age of 30 weeks or
less, or who require supplemental oxygen are particularly at risk of developing
ROP.
Initial examination of the peripheral retina by indirect ophthalmoscopy in these
neonates is recommended before hospital discharge, or by 4-6 weeks of postnatal
age (or within the 31st to 33rd week of post conceptional or postmenstrual age,
whichever is later).

Retinal examinations are repeated every 1- 2 weeks until the retina becomes fully
vascularized or ROP is noted.
If ROP develops, weekly examinations should be performed to watch for possible
progression to threshold disease.
12. a. Consumption of undercooked or raw meat or of substances contaminated
with cat feces is a risk factor for ocular toxoplasmosis.
Exposure to ticks increases the risk of Lyme disease, whereas exposure to
mosquitoes increases the risk of acquiring various infectious disease- causing
organisms (e.g. parasites that cause malaria and West Nile virus).
The Ohio River Valley is endemic for the ocular histoplasmosis syndrome.
13. b. Sub-Tenon steroid injection is a local treatment that is effective in
managing inflammation and macular edema associated with pars planitis,
especially when only 1 eye is involved.
Immunomodulation is reserved for persistent or refractory cases. Argon laser
treatment is utilized for peripheral retinal neovascularization associated with the
disease.
Pars plana vitrectomy is reserved for serious complications such as retinal
detachment, advanced uveitis, cataract, and/or severe cystoid macular edema
(CME) unresponsive to corticosteroid therapy.
14. b. Multiple evanescent white dot syndrome (MEWDS) is characterized by the
presence of multiple small gray-white dots at the level of the deep retina/RPE in
the posterior pole.
Foveal granularity, when present, appears as tiny yellow-orange dots.
Vitritis may or may not be present, but it is not severe.
RPE scarring is not a feature, as the condition typically resolves spontaneously
over 2- 6 weeks.
15. d. The early onset of photophobia and nystagmus points to a congenital cone
dysfunction.
The loss of photopic ERG response, including photopic flicker response, and the
patient's essentially normal rod function confirm the generalized cone
abnormality.
Although congenital stationary night blindness (CSNB) can reduce visual acuity
and cause nystagmus, the congenital loss of night vision from rod system
abnormalities would cause an abnormal scotopic ERG response.
CSNB is frequently an X-linked recessive trait that affects males.

In Leber congenital amaurosis, overall vision is very limited because of
generalized retinal dysfunction that causes loss of both rod and cone ERG
responses.
Stargardt disease often becomes evident during the grade school and teenage
years and typically shows a nearly normal rod and cone ERG response.
Achromatopsia causes total color blindness as a result of a congenital absence of
cone photoreceptors.
It has an autosomal recessive inheritance pattern, and its appearance in more than
the current generation is rare.
Ultimate visual acuity ranges from 20/100 to 20/200 and is best in dimmer light or
with sunglasses.
16. a. Acetazolamide has been shown to reduce CME in patients with hereditary
retinal degeneration (retinitis pigmentosa).
CME caused by a central retinal vein occlusion can be treated with intravitreal
injections of steroids or anti-vascular endothelial growth factor drugs.
Underlying causes of hypotony should be treated to reduce CME.
In patients with CME caused by vitreomacular traction, surgery may be indicated
to relieve the traction on the retina.
17. b. In patients with Best disease, the optical coherence tomogram and
fluorescein angiogram can help delineate the structure of vitelliform lesions, and
the EOG is often abnormal.
The ERG pattern, however, does not usually reveal any characteristic defects.
18. a. EOG is most helpful in identifying patients with, or carriers of, Best
disease. Results of optical coherence tomography, ERG, and fluorescein
angiography are typically normal in carriers of the disease.
19. c. AMD, Stargardt disease, and cone dystrophy can all cause RPE changes
similar to those found in chloroquine and hydroxychloroquine toxicity.
Tay-Sachs disease typically causes a cherry-red-spot appearance of the macula,
related to intraretinal storage of ganglioside.
20. d. The coexistence of renal and/or hepatic disease represents a risk factor for
the development of hydroxychloroquine maculopathy; youth, lean body weight,
and northern European ancestry do not.

21. d. The other medications can also cause pigmentary retinopathy. Thus, the
recommendation is to discontinue thioridazine as soon as toxicity is suspected.
Late atrophic changes of the macula can occur after discontinuation.
22. d. Niacin can cause a form of CME in which no late leakage is apparent on the
fluorescein angiogram. The other medications listed are not associated with an
atypical CME.
23. d. In proliferative diabetic retinopathy, panretinal photocoagulation may result
in the contraction of fibrovascular tissue, exacerbating tractional retinal
detachment, resulting in macular detachment.
Although this may also result in retinal breaks and combined tractional-
rhegmatogenous retinal detachment, this is uncommon.
Panretinal photocoagulation reduces retinal neovascularization and has no known
direct impact on cortical cataract formation.
24. d. The subject of prophylaxis for rhegmatogenous retinal detachment is an
area of some controversy among vitreoretinal specialists.
As with any surgical decision, the decision to treat must rest on an educated
assessment of the risks of treatment versus the risks of leaving the patient
untreated, as well as on knowledge of how much the treatment can actually reduce
the risk of detachment.
A thorough exploration is beyond the scope of this discussion, but factors that
prompt treatment are evidence of acute onset of symptoms and the presence of
vitreous traction.
Less compelling indications are a history of detachment in the other eye and
imminent cataract surgery, but the combination of the latter with evidence of
traction becomes a strong indication to treat.
25. c. Retinal detachments from giant retinal tears, tears of greater than 90°, have
a high redetachment rate due to proliferative vitreoretinopathy.
Because of the high risk of failure, the preferred approach would usually include
pars plana vitrectomy, use of perfluorocarbon liquid, laser photocoagulation
demarcation, and complete fluid-gas exchange.
The other options, performed alone, would not be likely to temporarily t1atten or
reattach the retina.

26. d. Repair for acute retinal detachment soon after diagnosis is important to
optimize outcome. Retrospective studies have shown a worsened prognosis in
cases for which surgery was delayed for about 7 days or more from the time of
diagnosis.
However, compared with emergency (same-day) surgery, scheduled surgery has
been associated with similar outcomes and complication rates, and with lower
cost. Nevertheless, because no prospective randomized studies have addressed
this topic, clinical judgment must be exercised.
Eyes with attached maculae or recently detached maculae may benefit from
earlier surgery. In addition, detachments associated with acute giant retinal tears
or superior bullous detachments with the macula remaining attached should be
repaired as soon as possible.
A good peripheral examination at diagnosis of retinal detachment is important to
assess for these factors.
27. a. Pars plana vitrectomy is indicated for patients with an epiretinal
membrane/macular pucker that produce metamorphopsia or a significant decrease
in visual acuity.
Visual acuity improves in most eyes after surgery but usually does not return to
normal. Complications after pars plana vitrectomy for epiretinal
membrane/macular pucker include peripheral retinal break formation (4%-6%);
retinal detachment (3%-6%), which may occur immediately postoperatively or
months after surgery; endophthalmitis ( 1% ); recurrent macular pucker that
affects visual acuity (5%); and progression of nuclear sclerosis (12%- 68%).
28. b. The staging system applies only to idiopathic macular holes, not traumatic
or disorder associated macular holes.
A stage 2 macular hole is defined as a perifoveal or "can opener" -like hole.
A stage 3 idiopathic macular hole is characterized by an adjacent annulus of
subretinal fluid without a posterior vitreous separation.
A stage 4 macular hole is a full -thickness hole with a posterior vitreous
separation.
Occasionally, idiopathic macular holes that have been repaired surgically will
reopen spontaneously or in relation to cataract surgery.
However, hole reopening is not included in the staging system.
29. b. Vitrectomy for removal of epiretinal membranes is a highly successful
surgery.
The procedure is associated with improvement in visual acuity, reduction in
metamorphopsia, and low rates of recurrent membrane formation. Accelerated
cataract development is the most common complication after vitrectomy for
epiretinal membrane removal.
Other postoperative risks include atrophy, hypertrophy, and migration of RPE
cells, macular edema, glaucoma, and retinal breaks.
Hypotony is a rare postoperative complication. However, when present, it is
usually due to decreased aqueous production or a wound leak rather than
increased trabecular filtration.
RPE disturbances are reported after successful vitrectomy and membrane peeling.
Indistinguishable RPE changes may develop after long-standing venous occlusive
disease.
Cautioning the patient regarding these postoperative complications would be
appropriate given the clinical setting.
30. b. Commonly reported complications of macular hole surgery include retinal
tear, retinal detachment, cataract, phototoxicity, and visual field loss. Cavernous
sinus thrombosis, compressive optic nerve injury, and cyclodialysis cleft have not
been reported.
In 1999, Holekamp and colleagues reported 7 cases of ulnar neuropathy from
face-down positioning after macular hole surgery.
All patients had positioned themselves with elbows flexed for at least 1 week.
The proposed mechanism was compression of the ulnar nerve while the nerve was
stretched in the condylar groove plus entrapment of the nerve in a narrowed
cubital tunnel during elbow t1exion.
At least 3 additional cases of this complication have been reported as the result of
face-down positioning after vitrectomy.
31. a. Bacillus cereus, which rarely causes endophthalmitis in other settings,
accounts for almost 25% of cases of traumatic bacterial endophthalmitis.
Endophthalmitis caused by B cereus has a rapid and severe course if untreated but
is sensitive to intravitreal vancomycin or clindamycin. Amphotericin B is an
antifungal drug.
Ganciclovir is an antiviral drug. Although B cereus may be sensitive to
gentamicin and tobramycin, the risk of retinal toxicity from these drugs precludes
their use in the treatment of this condition.

32. a. Shaken baby syndrome is a form of non accidental trauma, typically in a
baby less than a year old, frequently less than 6 months of age. Systemic signs
include bradycardia, apnea, hypothermia, lethargy, seizures, and bulging
fontanelles. Skin bruises may be present, particularly on the upper arms, chest, or
thighs, as may long-bone fractures and subdural and subarachnoid hemorrhages.
Ocular signs include retinal hemorrhages, cotton-wool spots, retinal folds, and
hemorrhagic schisis cavities.
33. a. The red laser penetrates through nuclear sclerotic cataracts better than other
wavelengths.
It is minimally absorbed by xanthophyll, possibly reducing the risk of thermal
damage in the treatment of CNV adjacent to the fovea.
It causes deeper burns with a higher rate of patient discomfort and a higher risk of
a "pop effect:'
34. a. Macular xanthophyll readily absorbs blue but minimally absorbs yellow,
red, and infrared wavelengths.
Therefore, the blue wavelength should be avoided during macular laser
photocoagulation in order to minimize thermal retinal damage.
35. a. Small spot size, high intensity, and short duration of laser applications all
increase the risk of a Bruch membrane rupture.
The red laser causes deeper burns with a higher risk of inhomogeneous choroidal
absorption and focal disruption.
36. a. Immediate postoperative elevation of intraocular pressure is not uncommon
after pars plana vitrectomy, especially in gas-filled eyes.
Although cataract progression is the most common complication of vitrectomy,
the onset occurs over months, with 90% of eyes in patients over age 50 years
showing visually significant nuclear sclerosis within the 2 years following
surgery.
Hyphema is not commonly observed after vitrectomy. Retinal detachment occurs
in 1%-5% of vitrectomy cases overall; the presentation is generally not immediate
owing to the time involved for tear formation as well as the time involved
between tear formation and subretinal fluid accumulation.

37. d. Hypertension is the only risk factor for choroidal detachment listed;
additional risk factors include advanced age, glaucoma, myopia, aphakia,
cardiovascular disease, Sturge Weber associated choroidal hemangioma, and intra
operative tachycardia. Transient Hypotony during surgery may cause rupture of a
posterior ciliary or choroidal artery.
38. b. Idiopathic epiretinal membrane formation is associated with posterior
vitreous detachment involving an abnormality of the vitreoretinal interface in
which retained cortical vitreous contracts and distorts the underlying retina.
39. d. The patient described represents a difficult challenge to the clinician.
Panretinal photocoagulation may result in contraction and regression of epiretinal
and disc neovascularization that has a fibrovascular component.
The resulting traction may aggravate or initiate tractional retinal detachments. If
the fovea becomes detached, the vision loss may not be reversible with vitrectomy
and membrane peeling.
Vitreous hemorrhage may follow scatter photocoagulation but does not cause
irreversible vision loss and may present an indication for pars plana vitrectomy.
Photocoagulation does not aggravate hyperglycemia.
Cortical cataract may result from absorption of laser energy at the posterior lens
surface, or by hemorrhage adjacent to the posterior capsule. Most
photocoagulation-related crystalline lens laser burns occur within the anterior
cortex and in preexisting cataractous areas.
Regardless, any associated vision loss is reversible with cataract surgery.

13 - Refractive Surgery
l. The most common technique used clinically to measure wavefront
aberrations employs the Hartmann-Shack wavefront sensor.
What are the ocular structures that affect wavefront analysis?
a. cornea, anterior chamber, and lens
b. cornea and anterior chamber
c. cornea, anterior chamber, lens, and vitreous
d. cornea
2. What condition might prevent a 25-year-old patient from being a good
candidate for photorefractive keratectomy (PRK)?
a. pregnancy
b. posterior corneal scar
c. asthma
d. anterior corneal scar
3. What is the best way to diagnose epithelial basement membrane dystrophy
(EBMD, or map-dot-fingerprint dystrophy) using a slit lamp?
a. slit-lamp examination using direct illumination
b. Hruby lens evaluation
c. lissamine green staining
d. rose bengal staining
4. What is a common long-term complication of radial keratotomy (RK)?
a. infection
b. progressive hyperopia
c. development of nuclear sclerotic cataracts
d. globe perforation
5. What is the correct definition of coupling?
a. corneal change that occurs in the peripheral cornea on both sides adjacent to a
clear corneal incision
b. corneal change that occurs only with arcuate keratotomy (AK) incisions
c. when 1 meridian is steepened at the site of an astigmatic incision, which thus
induces corneal flattening in the meridian 90° from the axis of incision
d. when 1 meridian is flattened at the site of an astigmatic incision, which thus
induces steepening in the meridian 90° from the axis of incision

6. What characteristic of an astigmatic incision would result in a greater
magnitude of astigmatic correction?
a. shorter incision
b. incision placed at a larger optical zone
c. shallow incision
d. incision placed at a smaller optical zone
7. What is the most common indication for the use of intrastromal corneal ring
segments?
a. hyperopia
b. keratoconus
c. Fuchs dystrophy
d. astigmatism
8. Intrastromal corneal ring segments are made from which material?
a. collamer
b. silicone
c. polymethylmethacrylate (PMMA)
d. porcelain
9. Orthokeratology causes a temporary reduction in myopia by what
mechanism?
a. steepening of the corneal epithelium
b. flattening of the corneal stroma
c. steepening of the corneal stroma
d. flattening of the corneal epithelium
10. What optical effect is observed following wavefront-guided and wavefront-
optimized ablations but not with conventional excimer laser ablations?
a. better contrast sensitivity
b. more nighttime glare and halos
c. greater postoperative higher-order aberrations
d. more postoperative spherical aberration
11. When considering a patient for excimer laser surgery, most surgeons
prefer what minimum safe thickness for the residual stromal bed?
a. 150 µm
b. 225 µm
c. 200 µm
d. 250 µm

12. What is the risk of cutting a laser in situ keratomileusis (LASIK) flap with
a mechanical microkeratome on a cornea flatter than 40.00 D?
a. larger than expected diameter flap, with increased risk for a "buttonhole"
b. larger than expected diameter flap, with increased risk for a free cap
c. smaller than expected diameter flap, with increased risk for a "buttonhole"
d. smaller than expected diameter flap, with increased risk for a free cap
13. What is the principal mechanism by which collagen cross linking stabilizes
the cornea?
a. keratocyte apoptosis
b. compaction of stromal lamellae
c. collagen polymerization
d. covalent bonding
14. What possible postoperative effect of collagen cross linking should a
refractive surgeon advise patients to anticipate?
a. improvement in corrected distance visual acuity
b. potential endothelial cell damage with resultant corneal edema
c. altered index of refraction with subsequent change in spectacle correction
d. corneal steepening
15. Which one of the following statements about corneal cross linking is true?
a. It was shown to be safe and effective in post-refractive surgery patients in US
Food and Drug Administration (FDA) trials.
b. It cannot be combined with insertion of intrastromal ring segments.
c. It is an option for patients with keratoconus who have a corneal thickness of
275 µm.
d. It may be utilized as a treatment for infectious keratitis.
16. What do all cases of phakic intraocular lens implantation require?
a. intra operative dilation
b. preoperative lens calculations
c. preoperative Schirmer testing
d. general anesthesia
17. What is the best refractive surgical option for a 45-year-old patient with a
manifest refraction of +5.00 D sphere and a central corneal thickness of 560
11m?
a. LASIK
b. PRK
c. refractive lens exchange
d. conductive keratoplasty
18. What preoperative test is most crucial for determining the available
strategies for astigmatism correction in the evaluation of a patient for
refractive lens exchange?
a. manual keratometry
b. simulated keratometry from an autorefactor or topographer
c. topography for pattern evaluation
d. Scheimpflug measurement of lenticular astigmatism
19. A 42-year-old man with diabetes mellitus reports worsening distance vision
for 6 months; his findings are as follows: most recent hemoglobin A1c
(HgbA1J value, 9.5; corrected distance visual acuity (CDVA, also called best-
corrected visual acuity), 20/15 in each eye (OD, -2.50 sphere; OS, -2.00 sphere);
and normal ophthalmologic evaluation.
What is the most appropriate refractive treatment?
a. contact lens fitting
b. eyeglass correction
c. repeat refraction in 3- 6 weeks
d. laser refractive surgery
20. What is the best initial therapy for a 53-year-old woman with intermittent
blurred vision and corneal punctate epitheliopathy who underwent
uncomplicated bilateral LASIK 6 weeks previously?
a. antibiotic drops
b. corticosteroid drops
c. non steroidal anti-inflammatory drops
d. preservative-free artificial tear drops

21. A 22-year-old man is referred for a LASIK evaluation. He has noted
worsening visual acuity over the past 3 years that has required several
eyeglass prescription changes. He states that he had good vision with soft
contact lenses as a teenager but that he cannot see well with his current soft
contact lens prescription. A manifest refraction reveals 3.00 D of non
orthogonal astigmatism, and manual keratometry shows irregular mires.
What is the most appropriate test for establishing a diagnosis of forme fruste
keratoconus?
a. corneal pachymetry
b. corneal topography
c. cycloplegic refraction
d. slit-lamp photography
22. A 65-year-old man had uncomplicated bilateral, 16-incision RK with a 3-
mm optical zone 15 years previously. Currently, his CDVA has decreased to
20/50 OU due to clinically significant posterior subcapsular cataracts; cataract
surgery with intraocular lens (IOL) implantation is planned.
What method is best for determining the appropriate IOL power in this
situation?
a. historical clinical history method utilizing keratometry readings from before and
after radial keratometry and the change in refraction
b. hard contact lens method to calculate the change in refraction with and without a
hard contact lens
c. American Society of Cataract and Refractive Surgery (ASCRS) Online Post-
Refractive IOL Power Calculator
d. Placido disk-based automated keratometry system to determine keratometry
values

Answers
1. c. Wavefront analysis with a Hartmann-Shack aberrometer measures the
wavefront error of the entire visual system, from the tear film to the retina.
With this device, a low-power laser beam is focused on the retina, and the reflected
light is then propagated back through the optical elements of the eye, at which
point the resultant wavefront is measured and analyzed.
2. a. Pregnancy can cause a temporary change in the refraction, which makes
refractive surgery potentially less accurate. It is generally recommended that
surgeons wait approximately 3 months after delivery to obtain a stable preoperative
refraction and perform refractive surgery.
Because breastfeeding is also associated with changes that may affect the
refraction, many surgeons recommend waiting for several months after the
cessation of breastfeeding before proceeding with refractive surgery.
As laser in situ keratomileusis (LASIK) requires cutting a flap in the anterior
cornea, patients with stromal scarring in the anterior cornea may experience
problems during flap creation whether by microkeratome or femtosecond laser;
thus, photorefractive keratectomy (PRK) may be preferable for these patients.
Additionally, patients with small anterior stromal scars may preferentially benefit
from PRK, as it may be possible to reduce the scar with the refractive ablation-
especially with myopic treatments. Controlled asthma is not a contraindication to
PRK.
3. a. Epithelial basement membrane dystrophy (EBMD; also called anterior
basement membrane dystrophy) occurs when the epithelial layer of the cornea is
not well attached to the Bowman layer. Eyes with EBMD are predisposed to
epithelial loosening or sloughing and even frank epithelial defects during the
LASIK procedure. Epithelial problems after LASIK increase the risk of diffuse
lamellar keratitis (DLK) and epithelial ingrowth under the flap.
The best method to detect EBMD is using a broad slit beam from the side to see the
irregular epithelium. Other techniques include using retroillumination or
fluorescein dye to identify subtle changes in the epithelium. Eyes with significant
EBMD may do best with a surface ablation procedure rather than LASIK.

4. b. Although infection, loss of corrected distance visual acuity, and globe
perforation can occur in rare instances after radial keratotomy (RK), progressive
hyperopia due to progressive corneal flattening is much more common.
The Prospective Evaluation of Radial Keratotomy study found that, 10 years
postoperatively, 43% of eyes were overcorrected by more than 1.00 D. Also,
diurnal fluctuation of vision is a common adverse effect of RK.
5. d. When 1 meridian is flattened from an astigmatic incision, an amount of
steepening occurs in the meridian 90° away; this phenomenon is the concept of
coupling.
6. d. The longer the incision, deeper the incision, and smaller the optical zone, the
greater the astigmatic correction.
7. b. Initially, intrastromal corneal ring segments were approved by the US Food
and Drug Administration (FDA) and used for the correction of myopia; because of
reduced predictability, however, they have fallen out of favor for treatment of
myopia.
They are now used almost exclusively in patients with keratoconus.
8. c. Intrastromal corneal ring segments have always been made of
polymethylmethacrylate (PMMA).
9. d. Orthokeratology involves the overnight wearing of rigid contact lenses to
create a temporary flattening effect on the corneal epithelium.
10. a. Wavefront-guided and wavefront-optimized ablations offer better contrast
sensitivity than conventional excimer laser ablations do because they reduce the
amount of higher order aberrations.
11. d. Leaving a residual stromal bed of less than 250 µm thickness puts the patient
at risk for corneal ectasia.
12. d. Corneas flatter than 40.00 D are more likely to have smaller-diameter flaps
and are at increased risk for creation of a free cap. Remember that cutting a flap
with the same blade in a second eye usually results in a thinner (not thicker) flap.

13. d. Corneal collagen cross linking combines riboflavin (vitamin B2), which is a
naturally occurring photosensitizer found in all human cells, and ultraviolet A
(UVA) light to strengthen the biomechanical properties of the cornea via covalent
bonding of the collagen fibrils. Although there may also be a slight flattening of the
cornea, the most important effect of the cross linking is that it stabilizes the corneal
curvature and prevents further steepening and bulging of the corneal stroma.
14. b. The UVA light used to activate riboflavin in the cross linking procedure is
toxic to corneal endothelial cells. In the presence of riboflavin, approximately 95%
of the UVA light irradiance is absorbed in the anterior 300 µm of the corneal
stroma.
Therefore, most studies require a minimal corneal thickness of 400 µm after
epithelial removal to prevent corneal endothelial damage and secondary corneal
edema by the UVA irradiation.
Thinner corneas may be thickened temporarily with application of a hypotonic
riboflavin formulation prior to UVA treatment.
15. d. Corneal collagen cross linking has had good results in stabilizing ectasia and
reducing both myopia and astigmatism resulting from post- refractive surgical
causes as well as naturally occurring conditions such as keratoconus; it has not yet
been approved by the FDA as safe and effective.
Some investigators have combined cross linking with other refractive modalities
(such as intrastromal rings) with promising early results. Patients with thin corneas
are not candidates for this procedure because of the endothelial toxicity of the UVA
irradiation.
Interestingly, there have been reports of collagen cross linking employed
successfully to treat fungal and bacterial infections of the cornea.
This use may represent a potential new application of this technology.
16. b. Implantation of posterior chamber phakic intraocular lenses (PIOLs) requires
intra operative pupillary dilation in order for the lenses to be inserted behind the
iris, whereas implantation of iris-fixated or anterior chamber PIOLs does not. As
PIOLs are not associated with significant dry eye, a preoperative Schirmer test is
not required for patients not suspected of having dry eye.
PIOLs can be inserted using topical anesthesia, making general anesthesia
unnecessary for most patients. All PIOLs currently require a peripheral
iridotomy/iridectomy either preoperatively or intra operatively to prevent pupillary
block.
All PIOLs also require preoperative calculations to determine the correct lens
power.

17. c. Compared with other refractive surgery procedures, refractive lens exchange
carries a higher risk of retinal detachment and an overall higher complication rate;
therefore, it is usually reserved for patients who fall outside the treatment ranges
for other surgical techniques.
Most patients with refractive errors ranging from +3.00 D to -6.00 D are reasonable
candidates for LASIK or PRK, and patients with normal accommodation stand to
incur diminished near visual acuity even with use of multifocal intraocular lenses
(IOLs).
Patients with high hyperopia generally are not good candidates for LASIK and
would thus benefit more from refractive lens exchange.
18. c. Manual keratometry and simulated keratometry values can both provide
information on the amount of regular corneal astigmatism present.
However, neither evaluation can determine irregular corneal astigmatism or
identify a corneal ectatic disorder such as keratoconus or pellucid marginal
degeneration.
Such disorders must be recognized preoperatively in order to decide what treatment
options are available for any residual astigmatism.
Whereas patients with regular astigmatism are potential candidates for a variety of
treatment strategies, including toric IOLs or multifocal IOLs with bioptics
(utilizing LASIK or PRK postoperatively), patients with significant irregular
astigmatism are not candidates for bioptics and may not be suitable for toric IOLs if
the irregularity is too great.
19. c. Elective ocular surgery should not be performed in a diabetic patient with
poor or erratic blood glucose control.
The blood sugar of a patient with diabetes mellitus must be well controlled at the
time of examination to ensure an accurate refraction, as the refractive error may
fluctuate with changes in the blood glucose level.
For this reason, it is also not advised to prescribe eyeglasses or contact lenses in
patients with diabetes mellitus whose blood glucose control is labile.
20. d. Dry eye symptoms after LASIK and PRK (advanced surface ablation) are the
most common adverse effects of refractive surgery.
Corneal nerves are severed when the flap is made, and the cornea overlying the flap
is significantly anesthetic for 3-6 months and even as long as 1 year
postoperatively.
As a result, most patients experience a decrease in tear production. Patients who
had dry eyes prior to surgery or whose eyes were marginally compensated before

surgery may experience more severe symptoms afterward. In addition, patients who
develop dry eyes after LASIK or surface ablation have an abnormal tear film and a
poor ocular surface, leading to reports of fluctuating vision between blinks
intermittently throughout the day.
Frequent application of preservative-free artificial tears often alleviates symptoms.
Additional treatments include topical cyclosporine, lubricant ointments, and
punctal occlusion.
21. b. Keratoconus is considered a contraindication to LASIK and surface ablation.
Creating a LASIK flap and removing stromal tissue results in a loss of structural
integrity of the cornea and increases the risk of ectasia, even if keratoconus had
been stable prior to treatment.
Forme fruste keratoconus is important to diagnose during the screening
examination for refractive surgery.
Although keratoconus can be diagnosed through slit-lamp examination and manual
keratometry, more sensitive analyses using corneal topography and corneal
pachymetry can reveal findings consistent with early keratoconus.
No specific agreed-upon test or measurement is diagnostic of a corneal ectatic
disorder, but both corneal topography and corneal pachymetry should be part of the
evaluation because subtle corneal thinning or curvature changes can be overlooked
on slit-lamp evaluation.
The existing literature on ectasia and longitudinal studies of the fellow eye of
unilateral keratoconus patients indicate that asymmetric inferior corneal steepening
or asymmetric bow-tie topographic patterns with skewed steep radial axes above
and below the horizontal meridian are risk factors for progression to keratoconus
and post-LASIK ectasia. With current technology, LASIK should not be considered
for these patients.
22. c. There are numerous ways to perform IOL calculations in eyes that have
undergone refractive surgery.
Unfortunately, none is perfect. Small, effective central optical zones after refractive
surgery (especially after RK) can lead to inaccurate measurements, because
keratometers and Placido disk-based corneal topography units measure the corneal
curvature several millimeters away from the center of the cornea.
Also, the relationship between the anterior and posterior corneal curvatures may be
altered after refractive surgery (especially after laser ablative procedures), leading
to inaccurate results.
Historical methods and rigid contact lens over refractions are often fairly accurate.
Manual keratometry is often less accurate than automated keratometry. Currently,
the best option for calculation of IOL powers in post-refractive surgery patients is

probably the American Society of Cataract and Refractive Surgery (ASCRS)
Online Post-Refractive IOL Power Calculator. This resource is available on the
websites of the ASCRS and the American Academy of Ophthalmology (AAO) and
is updated with new formulas and information as they become available.