1 health care reform & oncology bobbi buell, principal, onpoint oncology peyton howell,...
TRANSCRIPT

1
Health Care Reform & OncologyBobbi Buell, Principal, OnPoint Oncology
Peyton Howell, President, Consulting Services, ABC

2
“The View”: Health Care Reform, Medicare Changes and Oncology
• 3 Key Health Reform Updates for Oncology • Hot Topics Including the Highlights from the Proposed
2011 Medicare Physician Fee Schedule
• Our efforts in Washington
• What your practice should be doing now
• Questions & Discussion

3
3 Key Health Reform Updates for Oncology
4
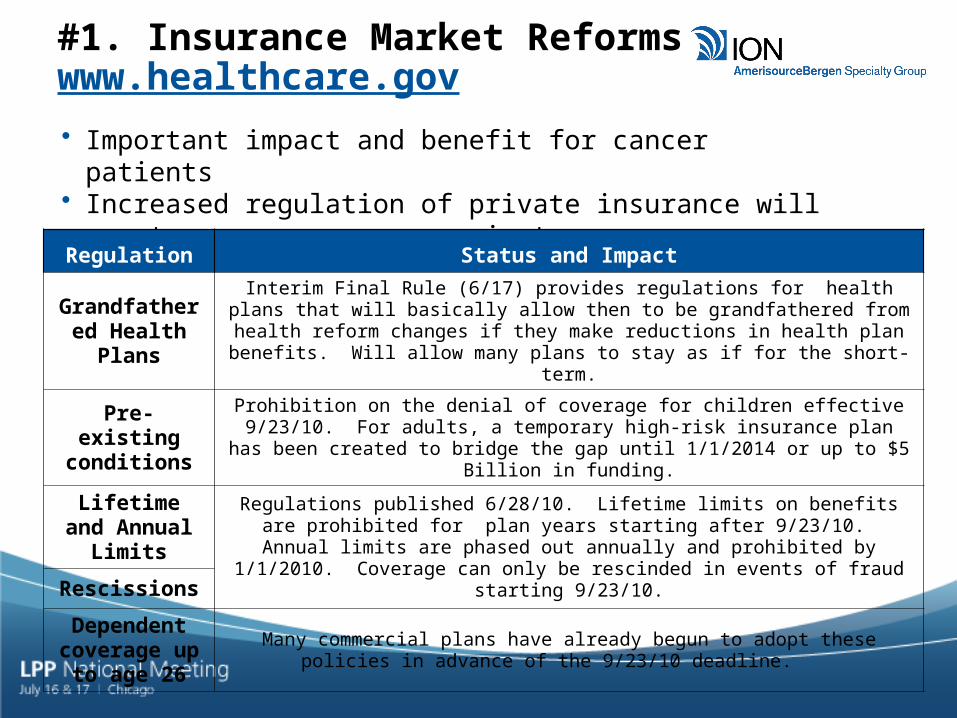
#1. Insurance Market Reforms www.healthcare.gov
• Important impact and benefit for cancer patients• Increased regulation of private insurance will create new
pressure on private payers
Regulation Status and Impact
Grandfathered Health Plans
Interim Final Rule (6/17) provides regulations for health plans that will basically allow then to be grandfathered from health reform changes if they make reductions
in health plan benefits. Will allow many plans to stay as if for the short-term.
Pre-existing conditions
Prohibition on the denial of coverage for children effective 9/23/10. For adults, a temporary high-risk insurance plan has been created to bridge the gap until
1/1/2014 or up to $5 Billion in funding.
Lifetime and Annual Limits Regulations published 6/28/10. Lifetime limits on benefits are prohibited for plan
years starting after 9/23/10. Annual limits are phased out annually and prohibited by 1/1/2010. Coverage can only be rescinded in events of fraud starting 9/23/10.Rescissions
Dependent coverage up to
age 26Many commercial plans have already begun to adopt these policies in advance of
the 9/23/10 deadline.

5
#2. Delivery System Changes Will Have Longer-term Impact
• Accountable Care Organizations (ACOs) (Medicare Shared Savings Program)
- CMS Special Open Door Forum- Questions and concerns regarding how ACOs can work
including Stark, anti-kickback, distribution of shared savings, structure and types of ACOs
• Center for Medicare & Medicaid Payment Innovation- Potential alignment of Part B and Part D benefits
• Comparative Effectiveness Research (CER) (Patient Centered Outcomes Research Institute)
- New focus on value-based data from private payers• Independent Payment Advisory Board
- Hospital delayed until 2019; Other providers 2015

6
#3. New Questions Emerge for 2014
• What is the purpose of 340B pricing post 2014?- Will program be narrowed dramatically to only remaining indigent/uninsured
patients? - Will it go away?
• What is the role of Disproportionate Share Hospitals (DSH) post 2014?
• How will Medicaid need to change if it represents a significant percentage of the overall payer mix?
• Will health provider that serve the uninsured benefit most from health reform? Will some providers be overwhelmed?

7
Health Care Reform 1.0
• We are expecting over 20,000 pages of regulations related to this first phase of health reform
• List of deadlines for 2010-2011 is challenging, including:- Restrictions on medical loss ratios- Eliminating the cost share for certain preventative services- Establishing tax credits for certain small employers- Creating a temporary reinsurance program- Medicare Part D changes related to coverage gap- Developing a premium rate review process- Setting limits on physician-owned hospitals- Establishing new state options for Medicaid- Establishing a new patient-centered outcomes research institute (aka CER)- Establishing a process for the FDA to approve biosimilars

8
Hot Topics including the Proposed 2011 Medicare Physician Fee Schedule
9
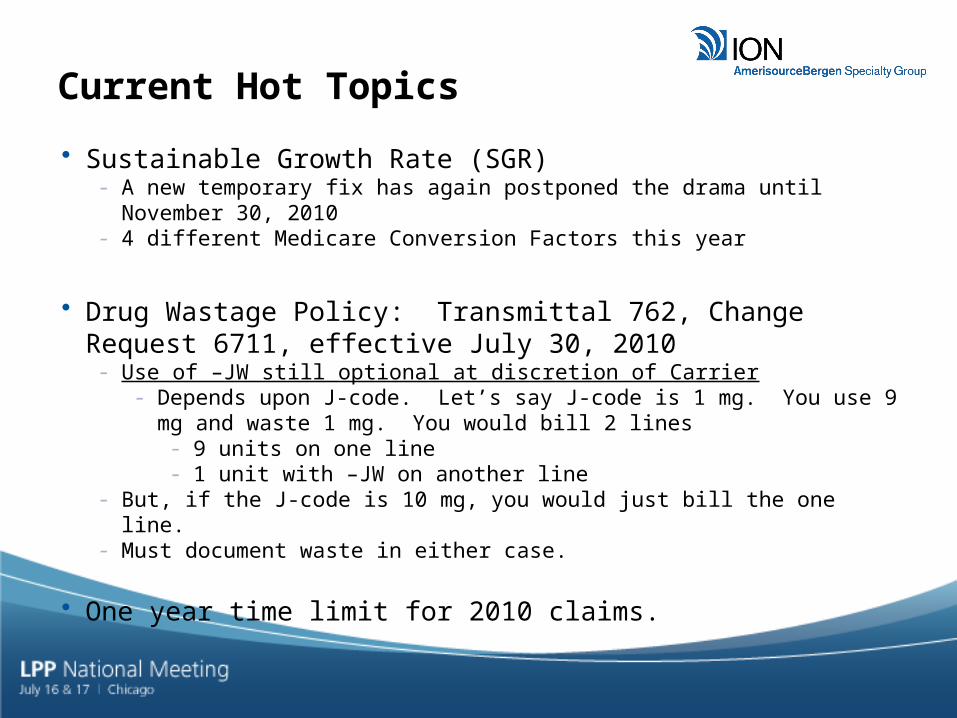
Current Hot Topics
• Sustainable Growth Rate (SGR)- A new temporary fix has again postponed the drama until November 30, 2010- 4 different Medicare Conversion Factors this year
• Drug Wastage Policy: Transmittal 762, Change Request 6711, effective July 30, 2010
- Use of –JW still optional at discretion of Carrier- Depends upon J-code. Let’s say J-code is 1 mg. You use 9 mg and waste 1
mg. You would bill 2 lines- 9 units on one line- 1 unit with –JW on another line
- But, if the J-code is 10 mg, you would just bill the one line.- Must document waste in either case.
• One year time limit for 2010 claims.

10
• On June 25, 2010, the Centers for Medicare & Medicaid Services (CMS) posted a proposed notice for Medicare payments in the physician fee schedule for calendar year (CY) 2011.
• CMS published this information in the July 13, 2010 Federal Register. An additional cut of 6.1% is proposed for the conversion factor.
• Many of these provisions were specified in Health Reform (“ACA”) and the rule affects physicians and office payment for services paid under the resource-based relative value scale/system (RBRVS), also known as, the Medicare Physician Fee Schedule.
• These are select highlights of the PROPOSED RULE. Remember that this is a proposal, not the law.
• Comments are due by August 24th
Proposed MPFS 2011
https://www.cms.gov/PhysicianFeeSched/PFSFRN/list.asp#TopOfPage
11
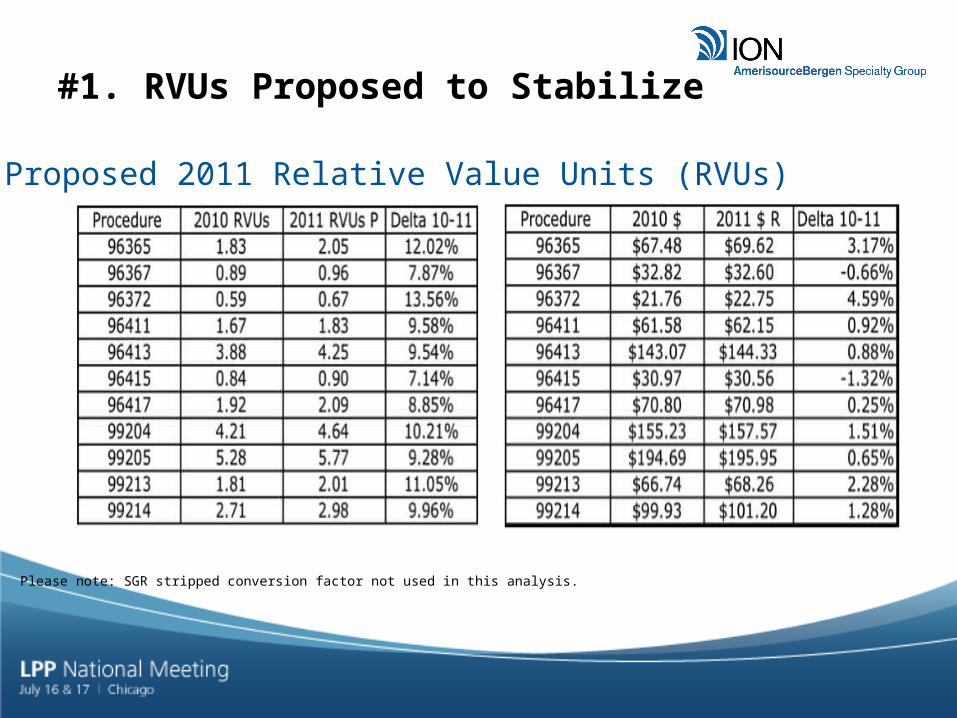
#1. RVUs Proposed to Stabilize
Proposed 2011 Relative Value Units (RVUs)he MEI
Please note: SGR stripped conversion factor not used in this analysis.

12
#2. Waiver of Cost Sharing for Preventative Services

13
• Imaging reductions for –TC of Related Procedures starting at the end of this month for multiple related procedures.
• Self-Referral Disclosure Law (starting 1/1/2011): The Affordable Care Act (ACA) amends the in-office ancillary services exception to the self-referral law as applied to magnetic resonance imaging, computed tomography, and positron emission tomography, to require a physician to disclose to a patient in writing at the time of the referral a list of other suppliers:
- A list of ten alternative ‘suppliers’ (not a hospital) within a 25-mile radius of the physician’s office who provide the same imaging services. The list must include no less than 10 suppliers.
- The list must include, name, address, phone number and distance from the physician’s office at the time of the referral. If there is no one they can go to, tell the patient they can get these tests in other facilities.
- The list is to be given to the patient at the time of referral.- A signature on the disclosure is required and must be maintained in the medical record. CMS is
currently not proposing to expand the list of procedures affected by this policy.- Emergency situations are not an exception.- Exceptions include patients who are not on Medicare at the time of the referral.
• Equipment Utilization Rate: Medicare law requires CMS to implement a 75 percent equipment utilization rate assumption to expensive diagnostic imaging equipment in a non-budget neutral manner for CY 2011, and the changes to PE RVUs will not be transitioned over a period of years. All other codes will remain at the 50 percent equipment assumption rate. In general, the codes affected by the 75 percent utilization rate are PET, CT and MRI codes.
#3. Imaging Changes

14
The proposed rule maintains the current ASP +6% reimbursement for Part B drugs, but it does propose some changes to ASP reporting and thresholds.
• Manufacturer reporting: If the manufacturer is late with quarterly reporting, the CMS proposes to update ASPs by carrying over the previously reported manufacturer ASP for applicable national drug code(s) (NDC(s)).
• CMS also proposes to update the regulations to clearly state that Medicare will not pay for amounts of “overfill”, i.e. product in excess of the amount reflected on the FDA-approved label. The ASP plus 6% will be paid for actual vial contents.
• Partial quarter ASPs for new drugs were also discussed in the proposed rule. Single-source drugs will be priced at WAC, plus 6% for that quarter and multisource and line extension drugs will be added to the weighted average of applicable NDCs.
• CMS also proposes to maintain the applicable threshold percentage for price substitution of WAMP or AMP for two consecutive quarters at 5%, and outlines a new proposal for price substitution at 103% of average manufacturer price (AMP) in certain circumstances when the ASP exceeds the AMP by 5% or more.
#4. Drug Reimbursement
Opportunity to comment on the flaws and inadequacies of current ASP reporting and reimbursement

15
• Still an opportunity to benefit before these become requirements or penalties
• PQRI –EPs who successfully report on quality measures in PQRI are eligible for a 1 percent incentive payment for the 2011 reporting period, down from 2 percent in 2010. EPs will receive PQRI incentive payments of 0.5 percent for years 2012-2014. EPs are eligible for an additional 0.5 percent incentive payment for years 2011-2014 for successfully participating in PQRI and a
Maintenance of Certification.• E-Prescribing: E-prescribing will pay 1% of the providers’ billed and allowed
fee schedule services (all services paid by RVUs) in 2011. 2011 is the last year where you will not be penalized,
- Measures: Exactly the same as in 2010, unless you are reporting under GPROI or GPROII, i.e. as a group practice. Then, the number depends entirely upon your group’s size.
- Reporting period: Calendar year, but data 1/1/2011-6/30/2011 will be used to identify those who should be penalized. So, you must report at least 50% before 6/30/11.
- Reporting mechanisms: Registries, claims, or EHR (if you are reporting PQRI this way)- Hardship exceptions—there will be new G-codes for these:
- Rural practices with no high speed internet OR- Providers near pharmacies that do not process e-rx.
#5. PQRI and E-Prescribing Incentives

16
Our Efforts in Washington

17
• Voice on the realities of challenges facing community oncology practices- ASP – Distributor prompt pay terms and bona fide
service fees must be excluded from ASP reporting.- Broader SGR Issues- Challenges facing practices- Patient access issues (uninsured and underinsured)- AMP as a potential reference price for ASP
• Ability to share experience based on working with practices across the country
Key Priorities

18
• AmerisourceBergen Washington DC office- ABC Leadership involvement and direct support
• Leveraging support for key associations and coalitions- Healthcare Distribution Management Association (HDMA)
- Specialty Biotech Distribution Council- Prompt Pay Coalition includes broad alliance of support
(HDMA, COA, ASCO, ACCC, NPAF)
• Leadership support for Community Oncology Alliance (COA)
Our support in Washington
19
What your practice should be doing now

20
Your To Do List July, 2010

21
Questions and Discussion